
Endovascular repair of ruptured abdominal aortic aneurysms confers no acute or late mortality benefit over open surgery, according to the results of a retrospective study using propensity-score matching by researchers at the University of Pittsburgh Medical Center.
Given these results and the massive systemic change and resources needed to organize and sustain an endovascular program, widespread adoption and routine use of endovascular repair of ruptured AAA (REVAR) should be deferred until there is good evidence of its superiority, according to Dr. Jae-Sung Cho and his colleagues.
 ©Elsevier Inc.
©Elsevier Inc.
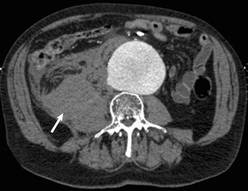
Axial slice of a CT scan showing an abdominal aortic aneurysm and a right retroperitoneal hematoma (arrow) due to contained rupture of the aneurysm.
Currently, the majority of ruptured AAAs are repaired using open surgery, but there is increasing enthusiasm for REVAR based on results from case reports and single-center series that used a standard REVAR protocol, according to the researchers. Those results are suspect because of the problem of selection bias and limited follow-up, the investigators said.
In an attempt to clarify the situation, Dr. Cho and his colleagues reviewed 312 patients who underwent ruptured abdominal aortic aneurysm (rAAA) repair from January 2001 to November 2010 at the University of Pittsburgh Medical Center (UPMC), a regional tertiary referral hospital with a high volume of open and emergent aortic surgery cases, according to the report in the September issue of the Journal of Vascular Surgery (2012;56:614-19).
A total of 34 patients were excluded owing to prior open or endovascular repair or because they were symptomatic without actual rupture. The remaining 288 patients formed the basis of the analysis: 37 underwent REVAR and 251 were treated with open surgical repair (OSR).
The researchers used propensity score–based matching to reduce the confounding effects of covariate imbalance between the REVAR and OSR as well as potential selection bias. A 1:3 ratio was used in the matching because of the various sample sizes of the REVAR and OSR patients and their distributions of propensity scores, yielding 37 REVAR patients matched to 111 OSR patients for analysis.
The matched cohorts did not significantly differ according to sex (the majority were men: 70.3% of the REVAR group, 62.2% of the OSR group); age (around 75 years in both groups); or history of comorbidities, including chronic obstructive pulmonary disease, cerebrovascular accident, hypertension, peripheral vascular disease, diabetes, smoking, hemodialysis, and coronary artery disease.
The only significant demographic difference between the patient groups was presentation with hemodynamic instability, defined as a systolic blood pressure less than 80 mm Hg. Such patients were more likely to undergo OSR (44%, compared with 24% of patients who underwent REVAR).
The outcomes measured comprised operative mortality (defined as intraoperative, in-hospital, and 30-day mortality), postoperative morbidity, length of stay, and transfusion of blood products. Long-term mortality was determined by evaluating against the Social Security Death Index. Late survival was estimated by Kaplan-Meier methods.
Although operative time and blood replacement were higher with OSR, overall complication rates were not significantly different (54% with REVAR vs. 66% with OSR). However, tracheostomies (21% vs. 3%), myocardial infarction (38% vs. 18%), and acute tubular necrosis (47% vs. 21%) were all significantly higher with OSR.
"Operative mortality rates were similar," according to the authors: 22% with REVAR vs. 32% with OSR (odds ratio, 0.63 for REVAR; 95% confidence interval, 0.24-1.48), and the incidences of secondary interventions for aneurysm- or graft-related complications were identical at 22%.
Kaplan-Meier estimates of 1-, 2-, and 3-year survival rates were not significantly different at 50%, 50%, and 42%, respectively, for REVAR and 54%, 52%, and 47% for OSR (P = .66).
The investigators discussed these results within the scope of several prospective, randomized trials that have been conducted or are currently underway comparing REVAR with OSR. The Nottingham trial and the Amsterdam Acute Aneurysm (AJAX) trial also failed to demonstrate any survival benefits from REVAR. The ongoing IMPROVE trial should be large enough (600 randomized patients) and should be able to address the question of whether or not a REVAR first approach provides a survival benefit over OSR.
Widespread adoption of a REVAR first approach is attractive, according to the researchers, who detail the value of its minimally invasive nature and the lower rates of complications, as demonstrated in their own study.
"However, implementation of such a protocol involves massive systemic changes, such as stocking of endovascular stent grafts and auxiliaries, and around-the-clock availability of skilled endovascular, radiologic, and nursing teams. It is not pragmatic to undertake such systemic and systematic changes in the absence of clear evidence of REVAR’s superiority," they said. For these reasons, no such change was established at the UPMC system, which would represent "a monumental task in a variety of ways."