ANSWER
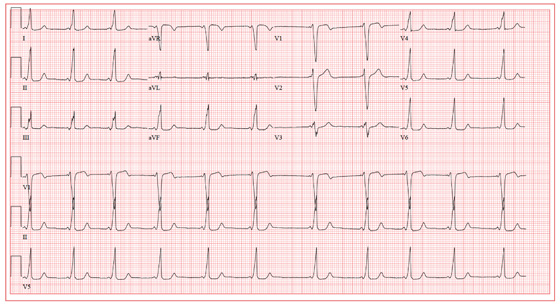
The ECG shows a sinus rhythm with a sinus arrhythmia and a short PR interval with ventricular pre-excitation, consistent with Wolff-Parkinson-White syndrome.
Ventricular pre-excitation occurs when conduction proceeds from the atria to the ventricles via an accessory pathway without involving the atrioventricular node, and is evident from a short PR interval and a delta wave immediately preceding the QRS complex. The delta wave illustrates conduction down the accessory pathway.
Careful examination reveals positive delta waves in the limb leads and the precordial leads, with an R-wave transition occurring in lead V4. This suggests the location of the accessory pathway to be on the tricuspid annulus (right sided) in an anteroseptal location. This location was confirmed by electrophysiology study, as was the pathway’s participation in an orthodromic reentry tachycardia responsible for the patient’s episodes of near-syncope and syncope. It was successfully ablated.
The sinus arrhythmia seen on the ECG is a normal variant.