User login
Patient history: The patient is a 53-year-old woman, 70 days status post-allogenic stem-cell transplantation for multiple myeloma. She presents with fever, mental status changes, and abdominal distension. Abdominal films are ordered.
Salient Findings
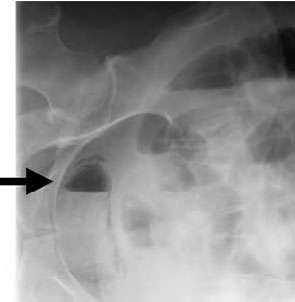
The patient has air within the wall of the bladder (see Figure 1 below, white arrow) and within the bladder lumen, diagnostic for emphysematous cystitis. On the lateral film the intravesicular air layers with a gravity dependent air-fluid level (see Figure 2 below, black arrow). The gas in the bladder wall is seen circumferentially. Because the lucency (air) remains in the dependent portions of the bladder, it must be in the bladder wall itself.

Patient population and disease history
Fifty to 80% of patients with emphysematous cystitis are diabetic. Other predisposing factors include immunosuppression, indwelling catheters, neutropenic bladders, female gender, and bladder outlet obstruction.
Most cases are caused by E. coli; less common pathogens are Enterobacter aerogenes and Klebsiella pneumoniae.
Management
Emphysematous infections are gas-forming infections of unknown mechanism. Common symptoms of emphysematous cystitis include abdominal pain, dysuria, and pneumaturia. Most patients with emphysematous cystitis (involvement of bladder only) respond well to systemic antibiotics, good bladder drainage, and excellent glycemic control.
On occasion, patients require cystectomy if unresponsive to medical management alone. Emphysematous pyelonephritis (involvement of renal parenchymal, intrarenal collecting system, and/or perinephric tissues), on the other hand, requires antibiotics along with surgical intervention. Percutaneous catheter placement is indicated for gas in the collecting system or renal parenchyma. Further extension of the gas or abscess formation may require surgical resection and/or total nephrectomy. Patients with emphysematous pyelonephritis should have a CT scan to define the extent of involvement.
Take-home points:
- Emphysematous cystitis is most common in diabetics;
- Pathogenesis is unclear at present;
- Emphysematous cystitis typically responds to IV antibiotics; and
- Emphysematous pyelonephritis requires systemic antibiotics and surgical intervention (percutaneous catheterization, resection of involved tissue, or total nephrectomy). CT can characterize the extent of tissue involvement and guide treatment. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
References
- Stamm WE; Harrison’s Textbook of Internal Medicine, 16th ed; 2005, McGraw-Hill. Chapter 269.
- Huang JJ, Tseng CC. Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000;Mar 27;160(6):797-805.
- Evanoff GV, Thompson CS, Foley R, Weinman EJ. Spectrum of gas within the kidney. Emphysematous pyelonephritis and emphysematous pyelitis. Am J Med. 1987 Jul;83(1):149-154.
Patient history: The patient is a 53-year-old woman, 70 days status post-allogenic stem-cell transplantation for multiple myeloma. She presents with fever, mental status changes, and abdominal distension. Abdominal films are ordered.
Salient Findings
The patient has air within the wall of the bladder (see Figure 1 below, white arrow) and within the bladder lumen, diagnostic for emphysematous cystitis. On the lateral film the intravesicular air layers with a gravity dependent air-fluid level (see Figure 2 below, black arrow). The gas in the bladder wall is seen circumferentially. Because the lucency (air) remains in the dependent portions of the bladder, it must be in the bladder wall itself.
Patient population and disease history
Fifty to 80% of patients with emphysematous cystitis are diabetic. Other predisposing factors include immunosuppression, indwelling catheters, neutropenic bladders, female gender, and bladder outlet obstruction.
Most cases are caused by E. coli; less common pathogens are Enterobacter aerogenes and Klebsiella pneumoniae.
Management
Emphysematous infections are gas-forming infections of unknown mechanism. Common symptoms of emphysematous cystitis include abdominal pain, dysuria, and pneumaturia. Most patients with emphysematous cystitis (involvement of bladder only) respond well to systemic antibiotics, good bladder drainage, and excellent glycemic control.
On occasion, patients require cystectomy if unresponsive to medical management alone. Emphysematous pyelonephritis (involvement of renal parenchymal, intrarenal collecting system, and/or perinephric tissues), on the other hand, requires antibiotics along with surgical intervention. Percutaneous catheter placement is indicated for gas in the collecting system or renal parenchyma. Further extension of the gas or abscess formation may require surgical resection and/or total nephrectomy. Patients with emphysematous pyelonephritis should have a CT scan to define the extent of involvement.
Take-home points:
- Emphysematous cystitis is most common in diabetics;
- Pathogenesis is unclear at present;
- Emphysematous cystitis typically responds to IV antibiotics; and
- Emphysematous pyelonephritis requires systemic antibiotics and surgical intervention (percutaneous catheterization, resection of involved tissue, or total nephrectomy). CT can characterize the extent of tissue involvement and guide treatment. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
References
- Stamm WE; Harrison’s Textbook of Internal Medicine, 16th ed; 2005, McGraw-Hill. Chapter 269.
- Huang JJ, Tseng CC. Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000;Mar 27;160(6):797-805.
- Evanoff GV, Thompson CS, Foley R, Weinman EJ. Spectrum of gas within the kidney. Emphysematous pyelonephritis and emphysematous pyelitis. Am J Med. 1987 Jul;83(1):149-154.
Patient history: The patient is a 53-year-old woman, 70 days status post-allogenic stem-cell transplantation for multiple myeloma. She presents with fever, mental status changes, and abdominal distension. Abdominal films are ordered.
Salient Findings
The patient has air within the wall of the bladder (see Figure 1 below, white arrow) and within the bladder lumen, diagnostic for emphysematous cystitis. On the lateral film the intravesicular air layers with a gravity dependent air-fluid level (see Figure 2 below, black arrow). The gas in the bladder wall is seen circumferentially. Because the lucency (air) remains in the dependent portions of the bladder, it must be in the bladder wall itself.
Patient population and disease history
Fifty to 80% of patients with emphysematous cystitis are diabetic. Other predisposing factors include immunosuppression, indwelling catheters, neutropenic bladders, female gender, and bladder outlet obstruction.
Most cases are caused by E. coli; less common pathogens are Enterobacter aerogenes and Klebsiella pneumoniae.
Management
Emphysematous infections are gas-forming infections of unknown mechanism. Common symptoms of emphysematous cystitis include abdominal pain, dysuria, and pneumaturia. Most patients with emphysematous cystitis (involvement of bladder only) respond well to systemic antibiotics, good bladder drainage, and excellent glycemic control.
On occasion, patients require cystectomy if unresponsive to medical management alone. Emphysematous pyelonephritis (involvement of renal parenchymal, intrarenal collecting system, and/or perinephric tissues), on the other hand, requires antibiotics along with surgical intervention. Percutaneous catheter placement is indicated for gas in the collecting system or renal parenchyma. Further extension of the gas or abscess formation may require surgical resection and/or total nephrectomy. Patients with emphysematous pyelonephritis should have a CT scan to define the extent of involvement.
Take-home points:
- Emphysematous cystitis is most common in diabetics;
- Pathogenesis is unclear at present;
- Emphysematous cystitis typically responds to IV antibiotics; and
- Emphysematous pyelonephritis requires systemic antibiotics and surgical intervention (percutaneous catheterization, resection of involved tissue, or total nephrectomy). CT can characterize the extent of tissue involvement and guide treatment. TH
Helena Summers is a radiology resident and Erik Summers is a hospitalist at the Mayo Clinic College of Medicine, Rochester, Minn.
References
- Stamm WE; Harrison’s Textbook of Internal Medicine, 16th ed; 2005, McGraw-Hill. Chapter 269.
- Huang JJ, Tseng CC. Emphysematous pyelonephritis: clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000;Mar 27;160(6):797-805.
- Evanoff GV, Thompson CS, Foley R, Weinman EJ. Spectrum of gas within the kidney. Emphysematous pyelonephritis and emphysematous pyelitis. Am J Med. 1987 Jul;83(1):149-154.