
.")
Dermpath Diagnosis
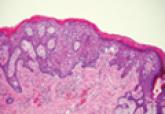
Extramammary Paget Disease
Extramammary Paget disease (EMPD) is an uncommon condition that usually presents in apocrine sweat gland–rich areas, most commonly the vulva...
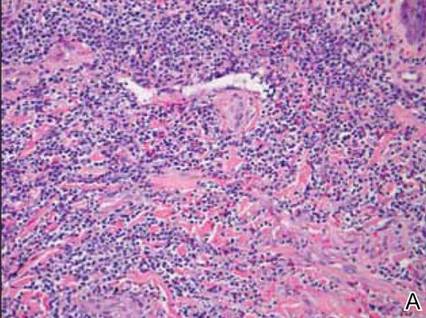
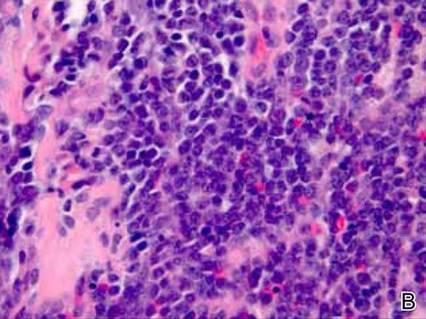
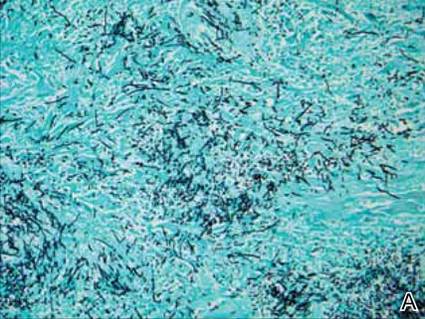
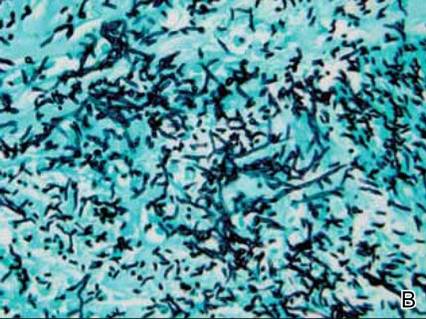
Leukemia cutis (LC) is characterized by the infiltration of malignant neoplastic leukocytes or their precursors into the skin and is most often seen in conjunction with systemic leukemia. Patients with LC frequently are in a relative or absolute immunocompromised state. We report the case of a 52-year-old man with primary refractory acute myelogenous leukemia (AML) following allogeneic stem cell transplant (SCT) who presented with a progressive reddish purple nodule with surrounding erythema and central necrosis in the setting of leukocytosis and possible fungal pneumonia. Histopathologic examination revealed an ulcerated dense diffuse dermal infiltrate of large atypical lymphocytes consistent with LC and septate hyphae with acute-angle branching in the dermal blood vessels. Cultures from a biopsied lesion grew Paecilomyces species, a rare but emerging opportunistic infection, despite the patient being on antifungal prophylaxis. This novel report of a rare angioinvasive infection occurring within a lesion of LC supports the need to maintain a high index of suspicion for invasive infection in patients with hematologic malignancy, even those on antifungal prophylaxis.
Practice Points
Extramammary Paget disease (EMPD) is an uncommon condition that usually presents in apocrine sweat gland–rich areas, most commonly the vulva...

Cutaneous manifestations of leukemia can be defined as specific or nonspecific skin lesions.