Drs. M. Lennox, Rizzo, and L. Lennox are from the School of Medicine and Biomedical Sciences, State University of New York at Buffalo. Dr. Rothman is from Women & Children’s Hospital of Buffalo.
The authors report no conflict of interest.
Correspondence: Luke Lennox, MD, 782 Potomac Ave, Buffalo, NY 14209 (lennox1988@gmail.com).
We report a case of subcorneal hematomas caused by excessive video game play in a 19-year-old man. The hematomas occurred in a setting of thrombocytopenia secondary to induction chemotherapy for acute myeloid leukemia. It was concluded that thrombocytopenia subsequent to prior friction from heavy use of a video game controller allowed for traumatic subcorneal hemorrhage of the hands. Using our case as a springboard, we summarize other reports with video game associated pathologies in the medical literature. Overall, cognizance of the popularity of video games and related pathologies can be an asset for dermatologists who evaluate pediatric patients.
Video game play has been reported as an etiologic factor in multiple musculoskeletal and dermatologic conditions.
More than two-thirds of US children aged 2 to 18 years live in a home with a video game system.
Cognizance of the popularity of video games and related pathologies can be an asset for dermatologists who evaluate pediatric patients.
References
Case Report
A 19-year-old man was admitted to our hospital to begin treatment for acute myeloid leukemia that had been diagnosed 2 days prior. Three days after completing a 10-day regimen of induction chemotherapy, he developed bilateral, well-demarcated erythematous patches on the palmar surfaces of the proximal phalanges of the third, fourth, and fifth fingers (Figure 1) and 2 patches on the right palm. The patient was referred to dermatology for evaluation. He recalled no trauma to these sites although he reported pushing his intravenous pole with the right hand when walking. Of note, he had become neutropenic and thrombocytopenic following chemotherapy
Figure 1. Bilateral, well-demarcated erythematous patches on the palmar surfaces of the proximal phalanges of the third, fourth, and fifth fingers and on the right palm.
On physical examination, the patches measured 1- to 1.5-cm in diameter and were mildly tender to palpation. The 2 patches on the right palm were much smaller than those on the fingers but were otherwise similar in appearance.
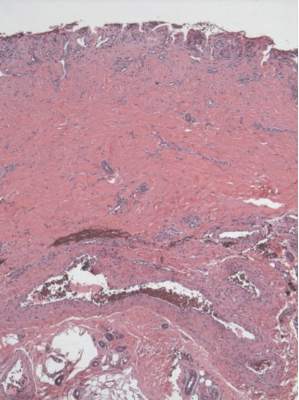
A punch biopsy of the erythematous lesion on the left third digit was performed. Histologic examination revealed extensive epidermal denudation associated with vascular proliferation and congestion as well as hemorrhage and a sparse lymphocytic infiltrate (Figures 2–4). There was no evidence of a leukemic infiltrate, and stains for fungal elements and bacteria were negative. Eccrine ducts appeared normal with no evidence of necrosis or metaplasia. These findings were suggestive of a frictional etiology.
Figure 2. Loss of epidermis with prominent dermal papillae and minimal inflammation (H&E, original magnification ×4).
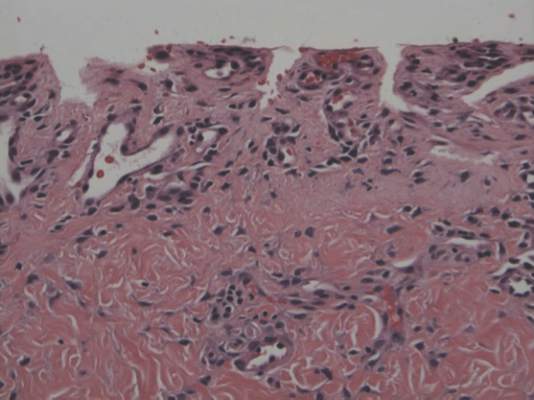
Figure 3. Loss of epidermis with preservation of dermal papillae. Vascular ectasia and congestion along with a paucicellular inflammatory infiltrate are noted (H&E, original magnification ×20).
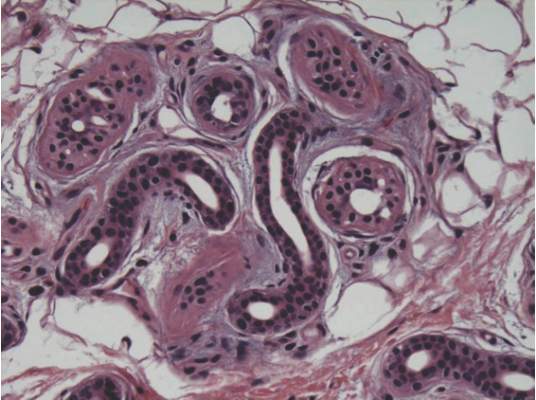
Figure 4. Eccrine sweat gland with normal secretory coils and excretory ducts. No inflammation or syringosquamous metaplasia were noted (H&E, original magnification ×20).
Due to the distribution of the skin lesions on the hands, it was suspected that the source of friction was a video game controller. Although the patient denied playing video games since his admission to the hospital, he reported heavy video game use during the weeks prior to admission. We postulated that the thrombocytopenia the patient developed following chemotherapy along with prior friction injury sustained from heavy video game play led to traumatic subcorneal hemorrhage on the hands at the points of contact with the video game controller (Figure 5). The subcorneal hematomas resolved completely over the next 2 months during which the patient abstained from video game play.
Figure 5. Points of contact on the hands are demonstrated when holding a video game controller.
This case demonstrates the importance of obtaining a detailed patient history, as our patient’s history of video game play prior to hospitalization proved to be of major diagnostic importance. Although the location, distribution, and well-demarcated nature of the patient’s lesions suggested an external source of trauma and biopsy definitively ruled out leukemia cutis, Sweet syndrome, and eccrine hidradenitis,1 the final diagnosis of traumatic subcorneal hematomas was only possible with specific knowledge of the patient’s video game controller use.