Case Report
A 44-year-old woman presented with a localized patch of hair loss on the frontal scalp of several month’s duration. She had been bitten by a tick at this site during the summer. Two months later a primary care provider prescribed triamcinolone cream because of intense itching at the bite site. The patient returned to her primary care provider 2 weeks later due to persistent itching, hyperpigmentation, and hair loss. At that time, the clinician probed the central portion of the lesion because of a concern for retained tick parts. A few weeks later, a dermatologist evaluated the patient and found a roughly circular zone of alopecia measuring approximately 5 cm in diameter that was just posterior to the left frontal hairline (Figure 1). In the center of the plaque there was a small eschar surrounded by a zone of hyperpigmentation, mild induration, and almost complete loss of terminal hairs. At the periphery of the lesion, hair density gradually increased and skin pigmentation normalized.

Figure 1. A centrally located eschar that is typical of tick bite alopecia.
A punch biopsy was obtained from an indurated area of hyperpigmentation adjacent to the eschar. Both vertical and horizontal sections were obtained, revealing a relatively normal epidermis, a marked decrease in follicular structures with loss of sebaceous glands, and dense perifollicular lymphocytic inflammation with a few scattered eosinophils (Figures 2 and 3).
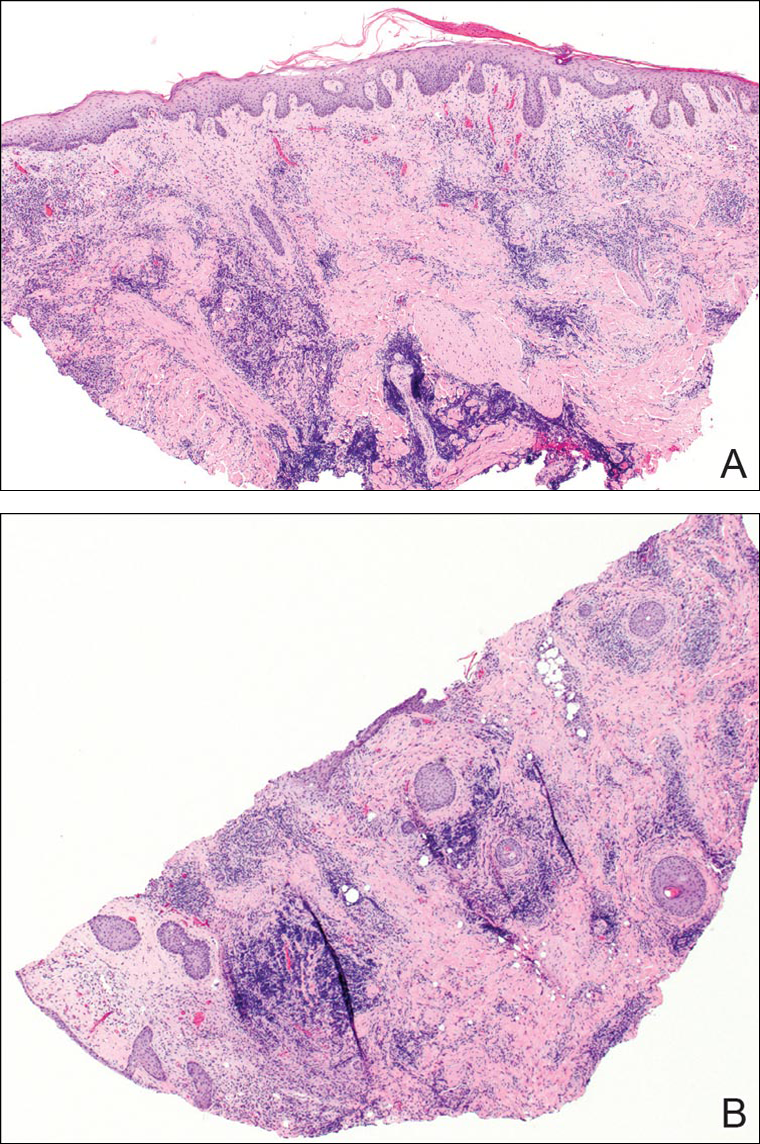
Figure 2. Vertical section (A) and horizontal section (B) of a biopsy from the lesion (both H&E, original magnification ×40).
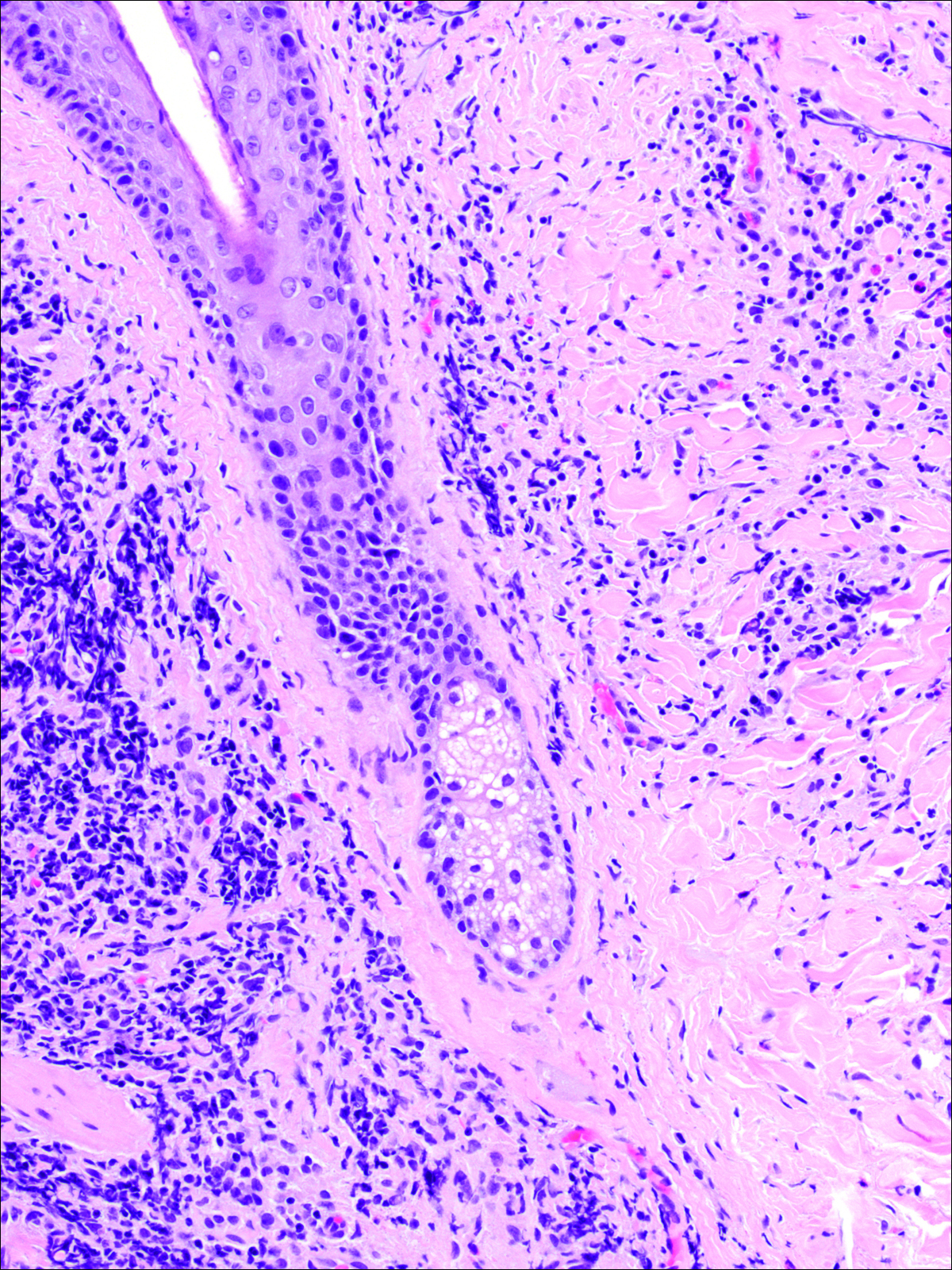
Figure 3. Perifollicular, predominantly lymphocytic inflammation surrounding a catagen follicle. A few eosinophils also were present in the infiltrate (original magnification ×100).
Clear-cut follicular scars surrounded by dense inflammation could be found (Figure 4). Horizontal sections revealed loss of most terminal hairs, with a few residual vellus telogen hairs present. At the sites of former follicles, some foci of dense inflammation showed evidence of germinal center formation as revealed by immunohistochemical staining (Figure 5).
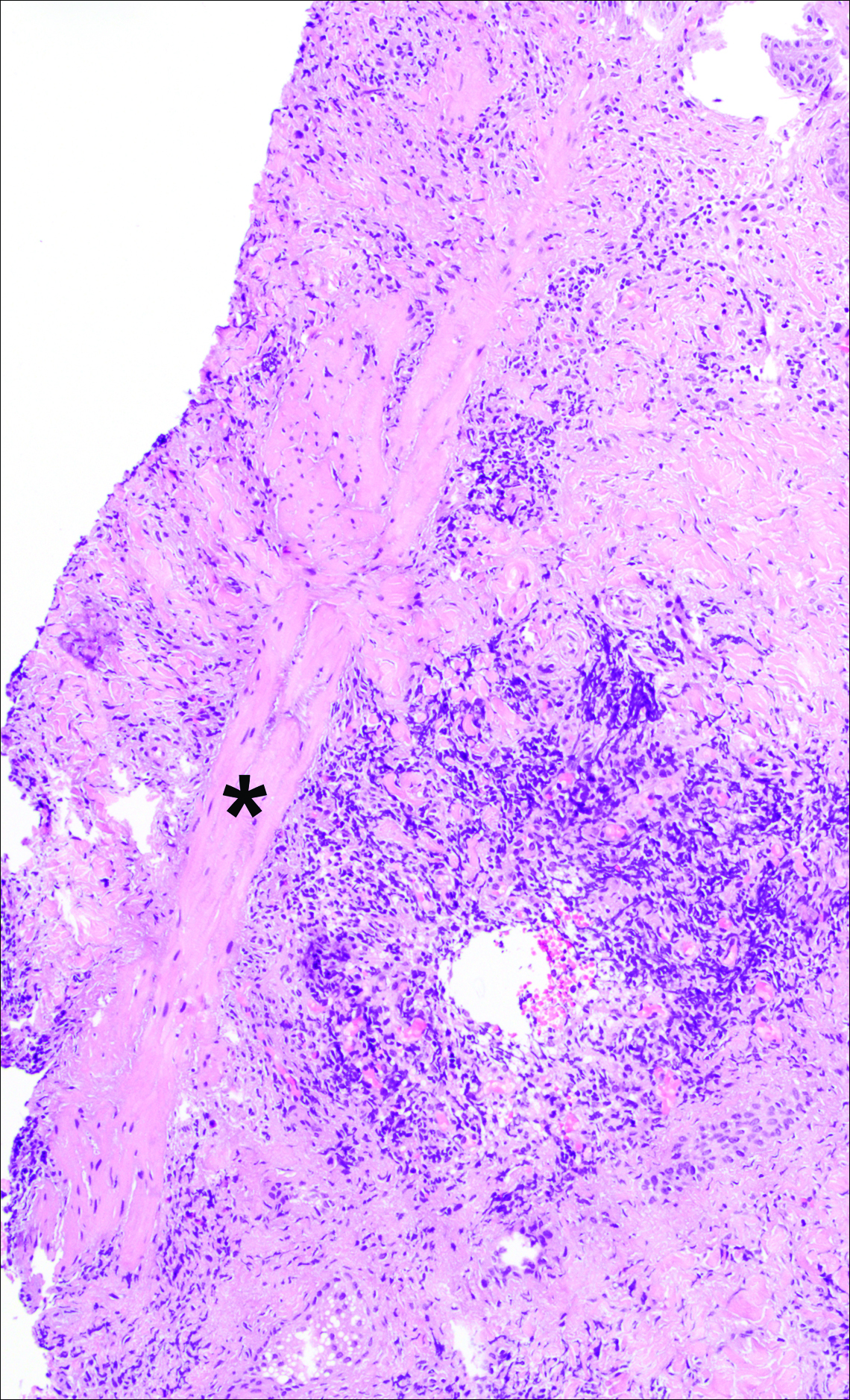
Figure 4. Nodular aggregate of chronic inflammation adjacent to a follicular scar (identified with an asterisk) (original magnification ×100).
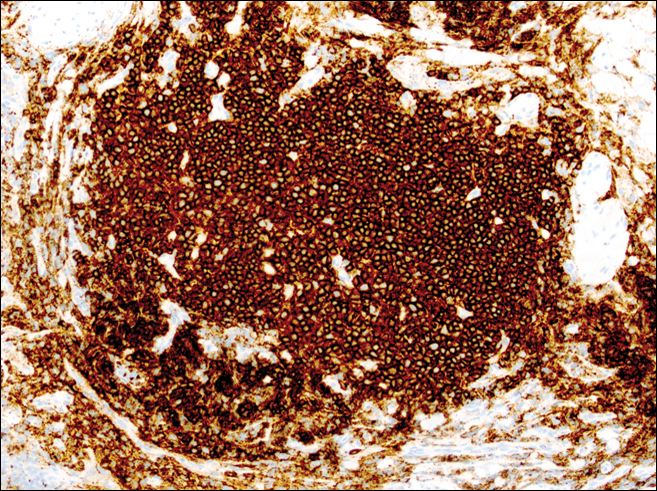
Figure 5. CD20 immunohistochemical stain of a nodular aggregate of inflammation (original magnification ×200). The dominant cells are B lymphocytes. CD4 and CD8 staining (not shown) was confirmatory.
Historical Perspective
Tick bite alopecia was first described in the French literature in 19211 and in the English-language literature in 1955.2 A few additional cases were subsequently reported.3-5 In 2008, Castelli et al6 described the histologic and immunohistochemical features of 25 tick bite cases, a few of which resulted in alopecia. Other than these reports, little original information has been written about tick bite alopecia.