Dr. Salgado is from the Department of Dermatology and Pathology, Rutgers New Jersey Medical School, Newark. Dr. Elston is from the Department of Dermatology and Dermatologic Surgery, Medical University of South Carolina, Charleston.
The authors report no conflict of interest.
Correspondence: Dirk M. Elston, MD, Department of Dermatology and Dermatologic Surgery, Medical University of South Carolina, MSC 578, 135 Rutledge Ave, 11th Floor, Charleston, SC 29425-5780 (elstond@musc.edu).
Scabies infestation is a major cause of impetigo and subsequent renal failure in the developing world, and efforts to eradicate widespread infestation are underway. Ivermectin, topical sulfur, and topical benzyl benzoate often are used to treat widespread outbreaks.
Scabies infestation is one of the world’s leading causes of chronic kidney disease.
Ivermectin can be used to treat mass infestations, and older topical therapies also are commonly used.
References
Scabies is caused by the mite Sarcoptes scabiei var hominis.1 It is in the arthropod class Arachnida, subclass Acari, and family Sarcoptidae.2 Historically, scabies was first described in the Old Testament and by Aristotle,2 but the causative organism was not identified until 1687 using a light microscope.3 Scabies affects all age groups, races, and social classes and is globally widespread. It is most prevalent in developing tropical countries.1 It is estimated that 300 million individuals worldwide are infested with scabies mites annually, with the highest burden in young children.4-7 In industrialized societies, infections often are seen in young adults and in institutional settings such as nursing homes.8 Scabies disproportionately impacts impoverished communities with crowded living conditions, poor hygiene and nutrition, and substandard housing.5,9 Controlling the spread of the disease in these communities presents challenges but is important because of the connection between scabies and chronic kidney disease.10 As such, scabies represents a major health problem in the developing world and has been the focus of major health initiatives.1,11
Identifying Characteristics
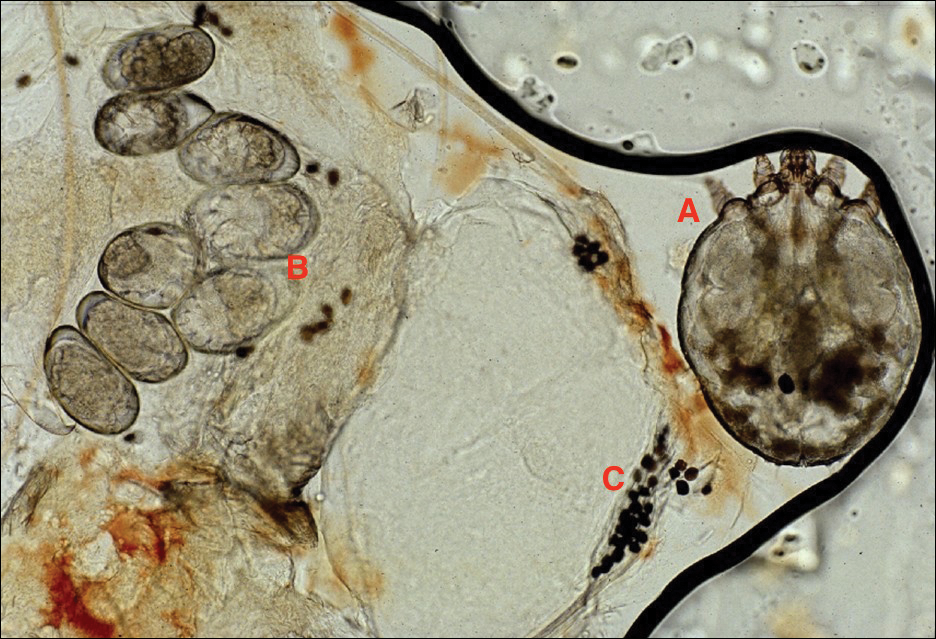
Adult females are 0.4-mm long and 0.3-mm wide, with males being smaller. Adult nymphs have 8 legs and larvae have 6 legs. Scabies mites are distinguishable from other arachnids by the position of a distinct gnathosoma and the lack of a division between the abdomen and cephalothorax.12 They are ovoid with a small anterior cephalic and caudal thoracoabdominal portion with hairlike projections coming off from the rudimentary legs. They can crawl as fast as 2.5 cm per minute on warm skin.2 The life cycle of the mite begins after mating: the male mite dies, and the female lays up to 3 eggs per day, which hatch in 3 to 4 days,2 in skin burrows within the stratum granulosum.12 Maturation from larva to adult takes 10 to 14 days.12 A female mite can live for 4 to 6 weeks and can produce up to 40 ova (Figure 1).
Figure 1. Sarcoptes scabiei mite (A), ova (B) and scybala (fecal material)(C).
Disease Transmission
Without a host, mites are able to survive and remain capable of infestation for 24 to 36 hours at 21°C and 40% to 80% relative humidity. Lower temperatures and higher humidity prolong survival, but infectivity decreases the longer they are without a host.13
An adult human with ordinary scabies will have an average of 12 adult female mites on the body surface at a given time.14 However, hundreds of mites can be found in neglected children in underprivileged communities and millions in patients with crusted scabies.13 Transmission of typical scabies requires close direct skin-to-skin contact for 15 to 20 minutes.2,8 Transmission from clothing or fomites are an unlikely source of infestation with the exception of patients who are heavily infested such as in crusted scabies.12 In adults, sexual contact is an important method of transmission,12 and patients with scabies should be screened for other sexually transmitted diseases.8
Clinical Manifestations
Signs of scabies on the skin include burrows, erythematous papules, and generalized pruritus (Figure 2).12 The scalp, face, and neck frequently are involved in infants and children,2 and the hands, wrists, elbows, genitalia, axillae, umbilicus, belt line, nipples, and buttocks commonly are involved in adults.12 Itching is characteristically worse at night.8 In tropical climates, patients with scabies are predisposed to secondary bacterial skin infections, particularly Streptococcus pyogenes (group A streptococci). The association between scabies and pyoderma caused by group A streptococci has been well established.15,16 Mika et al10 suggested that local complement inhibition plays an important role in the development of pyoderma in scabies-infested skin. A relationship between scabies and poststreptococcal glomerulonephritis (PSGN) has been established.11,17 An outbreak of PSGN in Brazil following an epidemic of Streptococcus zooepidemicus resulted in a high prevalence of renal abnormalities (mean follow-up, 5.4 years).18 In an aboriginal population with high rates of end-stage renal disease, follow-up in children 6 to 18 years after an epidemic of PSGN (mean follow-up, 14.6 years) showed that risk for overt proteinuria was more than 6 times greater than in healthy controls (95% confidence interval, 2.2-16.9).19 Scabies skin infestations and infections are endemic in many remote aboriginal communities20 where 70% of children younger than 2 years have chronic scabies and skin sores.21 In Dhaka, an urban slum in Bangladesh, the incidence of at least one scabies infection in children younger than 6 years was 952 per 1000 per year. In urban settlements in Dhaka, 49% (288/589) of infested children were not treated for up to 44 weeks after the characteristic signs and symptoms had developed due to restricted access to health care.22 In Brazil, scabies is hyperendemic in many poor communities and slums and is commonly associated with considerable morbidity.23 Edison et al24 reported that scabies and bacterial superinfections cause substantial morbidity among American Samoan children, with superinfections present in 53% (604/1139) of children diagnosed with scabies. Steer et al25 found that impetigo and scabies had been underestimated in Fiji where 25.6% and 18.5% of primary school children and 12.2% and 14.0% of infants had impetigo and scabies, respectively. In a systematic review of scabies and impetigo prevalence, Romani et al26 concluded that scabies and associated impetigo are common problems in the developing world that disproportionately affect children and communities in underprivileged areas and tropical countries, with the Pacific and Latin American regions having the highest prevalence of scabies. Scabies represents a major health concern worldwide due to the strong relationship between scabies and secondary infection.27
Figure 2. Scabies rash in an infant with burrows and erythematous papules.