VAIL, Colo. – A patient arrives at the clinic with a recognized tick bite. To use prophylaxis for Lyme disease or not?
“This is actually a fairly common call to our infectious diseases division in the summertime: ‘I had a child come into the office. We’ve got the tick. What do we do?’ ” Dr. Sean O’Leary said at the annual conference on pediatric infectious diseases sponsored by the Children’s Hospital, Denver.
The answer he and his pediatric infectious disease colleagues at the hospital almost always provide is a strong “no” to antimicrobial prophylaxis. That’s consistent with detailed Infectious Diseases Society of America guidelines on the topic, Dr. O’Leary noted.
 Photo Courtesy of Scott Bauer/USDA
Photo Courtesy of Scott Bauer/USDA
IDSA recommends prophylaxis for Lyme disease if the deer tick (shown in photo) has been attached to the skin for more than 36 hours.
The risk/benefit numbers argue against prophylaxis under most circumstances, he continued. Assuming a 1.4% attack rate of Lyme disease following a tick bite in an endemic area, the number needed to treat in order to prevent 1 infection is 83 patients – a hefty NNT. With the use of amoxicillin for prophylaxis, for every 10 cases of early Lyme disease prevented, it’s to be expected that 1 patient would develop a severe, life-threatening drug reaction and 10 would experience a drug-induced rash. And, in a study involving prophylaxis with doxycycline, 30% of patients had adverse events.
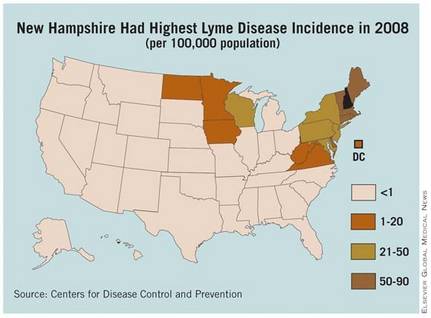
The Infectious Disease Society of America guidelines specify the limited circumstances in which prophylaxis is “moderately” favored. The tick must be reliably identified as an adult or nymphal Ixodes scapularis, commonly known as the deer tick, that’s been attached to the skin for more than 36 hours based upon the extent of engorgement with blood. The local rate of infection of this tick species with Borrelia burgdorferi has to exceed 20%, as is generally true in areas of New England, the Mid-Atlantic states, and the upper Midwest. And prophylaxis can be started less than 72 hours after removal of the tick.
When all those conditions are met, the IDSA guidelines state that it’s reasonable to offer a single dose of doxycycline in patients without a contraindication to the drug. The dose for Lyme prevention is 200 mg in adults and 4 mg/kg up to a maximum of 200 mg in children above 8 years of age.
As for prophylaxis against other tick-borne pathogens, Dr. O’Leary said that fewer than 1 in 1,000 Dermacentor ticks carry Rickettsia rickettsii, the cause of Rocky Mountain spotted fever. And while there are very few studies on other tick-borne diseases, the risk is considered “very, very low,” he noted.
“In general, the risk of prophylaxis far outweighs any potential benefit,” Dr. O’Leary stressed.
He disclosed having no relevant financial conflicts.