To the Editor:
Keratoacanthoma (KA)–type squamous cell carcinomas (SCCs) are rapidly evolving neoplasms of the epithelium that often spontaneously regress but rarely metastasize.1,2 Keratoacanthomas are thought to ascend from the hair follicle,1 and they clinically present as an enlarging solitary crateriform nodule with a keratin-filled center. Multiple KAs are rare2; histologically, KAs can be difficult to distinguish from conventional SCCs and are frequently treated by standard surgical excision.1 Reactive KAs are a subtype of KA that are induced by trauma including UV exposure, electromagnetic radiation, surgical procedures, chemical peels, laser treatments, and rarely tattoos.3-5
A 56-year-old man presented to the clinic with 3 asymptomatic enlarging papulonodules within a multicolored tattoo along the right forearm and elbow of 5 months’ duration (Figure 1). The lesions developed 1 month after the tattoo was placed and were localized to the areas of red pigment. The patient had several other tattoos. Histologic examination of the lesions revealed a well-differentiated squamous neoplasm with a crateriform invagination consistent with the superficial portion of a KA (Figures 2A–C). The specimen also revealed exogenous red pigment that was consistent with the background tattoo (Figure 2D). The patient underwent excisions of all 3 KAs, and free surgical margins were obtained.

Figure 1. Three hyperkeratotic papulonodules within the red portions of a multicolored tattoo on the right forearm and elbow.
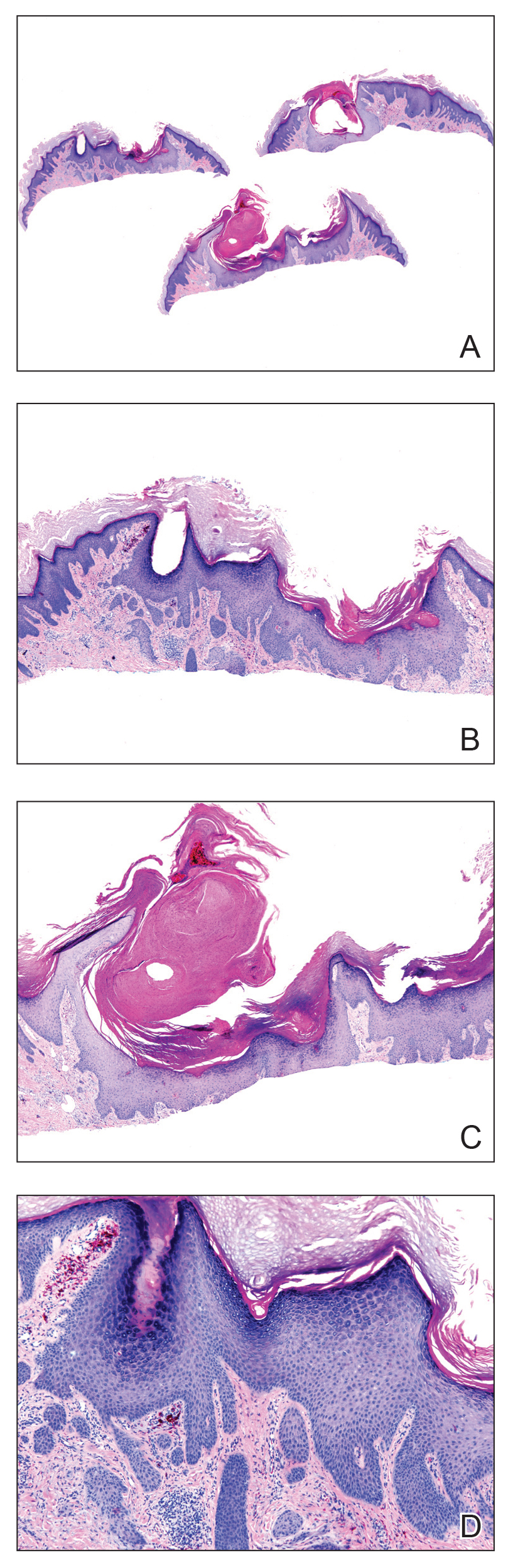
Figure 2. A–C, Histopathology demonstrated a well-differentiated squamous neoplasm with a crateriform invagination, consistent with a keratoacanthoma (all H&E; original magnifications ×1.25, ×4, and ×4, respectively). D, Exogenous red pigment within the dermis, consistent with an underlying tattoo (H&E, original magnification ×10).
Tattooing is a popular practice dating back to 3000 bc.6 It is estimated that 24% of the US adult population has a tattoo7 and as many as 20% of individuals with tattoos (approximately 50 million individuals) have experienced an adverse cutaneous reaction after the introduction of exogenous pigments into the skin.8 Cutaneous tattoo reactions include allergic contact dermatitis, eczematous and lichenoid dermatoses, pseudolymphomatous and granulomatous reactions, pseudoepitheliomatous hyperplasia, and KAs.9 Red pigment is reported to cause the greatest number of adverse cutaneous tattoo reactions.3 Reactions to mercury sulfide in red dye are well documented, and the use of this pigment has been eliminated by major manufacturers3; however, it is possible that other inorganic pigments that may contribute to these adverse cutaneous reactions have not been identified.4 Notably, our patient has other red tattoos with no adverse reactions, but in this new multicolored tattoo, all 3 KAs only appeared in areas of red pigment, suggesting that the reaction was specific to a component of this red dye.
Cipollaro10 reported the first case of a KA in a tattoo in 1973. Although there have been reports of melanoma and basal cell carcinoma occurring within tattoos, KAs and conventional SCCs are the most common cutaneous neoplasms arising in tattoos.
The pathogenesis underlying the development of malignancies in tattoos is unclear. It has been hypothesized that trauma from tattooing may play a role given the temporal relationship between tattoo placement and malignancy development.11 Another theory is that tattoo pigment causes a chronic inflammatory foreign body reaction that triggers carcinogenesis.12 Lastly, it has been postulated that tattoo pigment may alter UV light absorption in the skin that could potentially impact mutagenesis.11
The most common treatment of KAs is standard surgical excision.4 Mohs micrographic surgery is an option if the KA is located in a cosmetically sensitive area. Although there are no reports of recurrence after excision of tattoo-related KAs, new KAs forming adjacent to a previously excised KA have been reported.13
Currently, tattoos are not regulated by the US Food and Drug Administration before going to market. Although many states regulate the practice of tattooing, few regulate the contents of tattoo ink, and ink is only investigated when safety issues arise.14 This case provides further evidence of an association between KAs, tattooing, and potentially carcinogenic pigments, especially in red dye, supporting the need for further research on the safety of pigment components and more regulation of tattoo ink.