Pantea Hashemi, MD; Grace F. Kao, MD; Thomas Konia, MD; Lisa C. Kauffman, MD; Christine C. Tam, MD; Bahram Sina, MD
Dr. Hashemi is from the Department of Dermatology, New York Medical College, New York. Dr. Kao is from VA Maryland Health Care System, Baltimore. Dr. Konia is from University of California at Davis Medical Center, Sacramento. Dr. Kauffman is in private practice, Washington, DC. Dr. Tam is from the Department of Dermatology, University of Cincinnati, Ohio. Dr. Sina is from the Department of Dermatology, University of Maryland Medical Center, Baltimore.
The authors report no conflict of interest.
Correspondence: Pantea Hashemi, MD, 1901 1st Ave, New York, NY 10029 (panteahashemi@gmail.com).
Toker cells are epithelial clear cells found in the areolar and nipple areas of the breast, vulvar region, and other apocrine gland–bearing areas of the skin. Toker cells have been implicated in the pathogenesis of clear cell papulosis, cutaneous hamartoma with pagetoid cells, and rare cases of primary extramammary Paget disease (EMPD) but not in secondary EMPD with underlying adenocarcinoma. The pathogenesis of primary EMPD is not well defined. We report a case of multicentric primary EMPD with evidence of Toker cell proliferation and nonaggressive biologic behavior in a 63-year-old white man. A detailed description of the morphologic and biologic features of Toker cells and their possible carcinogenetic links also are discussed. Based on the observation and follow-up of our patient, we hypothesize that multicentric primary EMPD starts with Toker cell hyperplasia and can potentially evolve to carcinoma in the genital region.
Toker cells are epithelial clear cells found in apocrine gland–bearing areas of the skin.
Toker cell hyperplasia may be a precursor to primary extramammary Paget disease (EMPD).
In patients with established EMPD, it is important to examine other parts of the skin with apocrine glands for multicentric disease.
Primary multicentric EMPD has a favorable outcome.
References
Extramammary Paget disease (EMPD), which was first described by Crocker1 in a patient with erythematous patches on the penis and scrotum, is morphologically identical to mammary Paget disease (MPD) of the nipple. The principal difference between EMPD and MPD is anatomic location. Extramammary Paget disease predominantly affects apocrine gland–bearing areas including the vulva, scrotum, and perianal areas. Although EMPD is not a common condition, it must be considered in the differential diagnosis for patients with chronic genital or perianal dermatitis. Primary EMPD must be distinguished from secondary epithelial involvement by an underlying invasive carcinoma that originates from sites such as the gastrointestinal or genitourinary systems (secondary EMPD).
Although multicentric primary EMPD is not uncommon among Eastern Asians, as there have been several reports in the literature from Japan,2-5 multicentric EMPD in white individuals is rare.6 We report a case of primary EMPD that was established when no underlying malignancies were detected.
Case Report A 63-year-old white man presented to the dermatology clinic with a pruritic rash involving the groin of 8 years’ duration. Over-the-counter antifungal agents provided no improvement. Confluent erythematous and macerated plaques on the scrotum, shaft of the penis, bilateral inguinal areas, and perineum were noted on clinical examination (Figure 1). There also were well-demarcated, 4×5-cm, erythematous, velvety plaques on the right axilla and a small erythematous plaque on the left axilla. Systemic workup including colonoscopy, cystoscopy, and magnetic resonance imaging of the abdomen and pelvis were unremarkable. A positron emission tomography–computed tomography scan revealed foci of hypermetabolic activity in the bilateral inguinal nodes that were interpreted as evidence of an inflammatory process.
Figure 1. Confluent erythematous and macerated plaques on the scrotum, shaft of the penis, bilateral inguinal areas, and perineum.
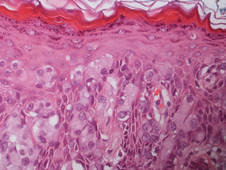
Fourteen biopsies were taken from the clinically involved regions in the genital area to delineate the extent of involvement. They all showed intraepidermal carcinoma characterized by large cells with clear cytoplasm and large hyperchromatic nuclei throughout the epidermis, which were more abundant in the basilar and lower portions of the epidermis (Figure 2). There was no evidence of underlying carcinoma in the dermis.
Figure 2. Histopathologic examination of the genital region showed Paget cells with large round and oval hyperchromatic nuclei and abundant pale cytoplasm (H&E, original magnification ×400).
On immunohistochemical staining, the neoplastic cells were diffusely and strongly positive for cytokeratin 7 (Figure 3) and moderately positive for carcinoembryonic antigen, estrogen and progesterone receptors, and ERBB2 (formerly HER-2/neu). Additional immunostaining for cytokeratin 20 and gross cystic disease fluid protein 15 were negative. High-molecular-weight keratin staining highlighted background epithelium and spared neoplastic cells. Mucicarmine staining highlighted mucin within the cytoplasm of neoplastic cells. Ultrastructural studies showed evidence of apocrine differentiation in the neoplastic cells with deeply indented, bean-shaped nuclei and clear cytoplasm with inconspicuous organelles. Clinically unaffected skin from the periumbilical region also was biopsied. The histology demonstrated Toker cells characterized by clear cytoplasm, small vesicular nuclei, and the absence of hyperchromasia (Figure 4).
Figure 3. Immunohistochemical staining for cytokeratin 7 showed diffusely positive clear cells in the epidermis (H&E, original magnification ×200).
The patient was treated with 6 cycles of 5-aminolevulinic acid 20% photodynamic therapy but showed no improvement. Imiquimod cream 5% resulted in mild clinical improvement in the axillae but caused severe irritation in the groin and was discontinued after 3 months. A radiology consultation obtained 6 years prior to presentation determined that the risk associated with radiation therapy outweighed any possible benefits. Although localized disease persisted, repeated biopsies and positron emission tomography–computed tomography scans did not show any evidence of invasion or metastasis, respectively. Three years after initial presentation, groin lesions progressed to become more erythematous and vegetative. The corresponding histology demonstrated EMPD. An ancillary test (polymerase chain reaction analysis) for low- and high-risk human papillomavirus was negative.
Comment Primary EMPD has been well documented in the literature to have a favorable prognosis if adequately treated. The few cases reported from Japan on EMPD without underlying adenocarcinoma had good outcomes.2,3 Further reports of multicentric EMPD involving 2 or 3 sites in the axillae and/or genital region did not reveal any progression to invasive carcinomas after adequate follow-up.3-9 Indeed, many of these cases, particularly those in the genital region, were aggressively treated with surgery, topical chemotherapy, immunomodulatory agents, and radiation; therefore, their natural course is not known.2 A Japanese studyconducted at 75 medical institutions (1987-1991) included 46 EMPD patients with multiple (ie, 2 or 3) sites of involvement.10 Some of the patients with a combination of genital and axillary lesions were followed without any treatment. None of the EMPD patients with axillary involvement developed invasive carcinoma after 4- to 12-year follow-up.10