Radiographic Imaging
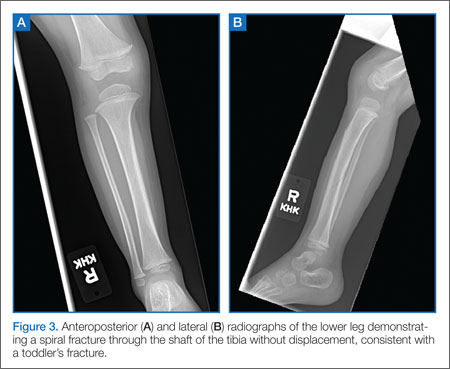
Quality anteroposterior (AP) or lateral radiographs of the affected leg may show a hairline fracture, but these can easily be missed on initial plain films in almost a third of patients.21 An internal oblique view can aid in identifying nondisplaced toddler fractures.17 The AP view is the best view for observing the nondisplaced spiral fracture along the distal tibia (Figure 3).6 Occasionally, a fracture line is not identified on initial plain films and the first evidence of fracture becomes apparent on X-ray when new periosteal bone forms 7 to 10 days after the initial injury.
Definitive Treatment
Children with a classic history for a toddler’s fracture and an inability to bear weight should be immobilized with a long-leg splint or cast—even when X-rays are negative—until a definitive diagnosis can be made. Such fractures usually become visible on X-ray 7 to 10 days after injury as a result of new bone growth.22
When definitive diagnosis of a toddler’s fracture is made on plain radiographs, the child should either be immobilized in a long-leg splint with referral to an orthopedist within 5 to 7 days, or immediately casted.16
Conclusion
Fractures in both children and adults are among the most common injury-related presentations to the ED. Based on the structure and increased elasticity of bone in the pediatric patient, there are several fracture patterns unique to this population. Appropriate evaluation, diagnosis, and management in the ED helps to maximize and ensure long-term function and healing while minimizing trauma to the patient.
Dr McBride is an associate professor of pediatrics and pediatric emergency medicine, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.
Dr Sutton is a pediatric resident, Wake Forest Baptist Health, Brenner Children’s Hospital, Winston-Salem, North Carolina.