Does the patient’s hip make a snapping sound?
Patients with snapping of the hip can be categorized into those whose injuries are painful, and those whose injuries are not. Reassure patients with pain-free snapping that there is no reason to be concerned.
External snapping is usually related to the iliotibial band moving over the greater trochanteric bursa, which can lead to a painful bursa.17 The key symptom, in addition to the snapping, is lateral hip pain of gradual onset. Examination reproduces the pain with the snapping hip maneuver (FIGURES 3A AND 3B).
Internal snapping is related to the iliopsoas tendon passing over the femoral head and hip capsule or over the iliopectineal eminence and bony ridge of the lesser trochanter.17 Inflammation of the iliopsoas bursa may lead to painful snapping. This pain is anterior in location, and the snap can be reproduced with the patient lying on the unaffected side, bringing the affected hip passively from flexed, abducted, and externally rotated to a medial position of extension, adduction, and internal rotation.
Internal and external snapping usually occurs in patients whose activities involve the repetitive motions done in the exam maneuvers. Intra-articular snapping is due to loose bodies or acetabular labral tears.
Imaging for the patient with painful hip snapping consists of hip radiographs—usually negative—and ultrasound. MRI is done if intra-articular pathology is suspected.17 Treatment of snapping hips includes activity modification, NSAIDs, physical therapy, and possible steroid injection. Rarely is the condition surgically treated.
FIGURE 3
Snapping maneuver can help identify source of pain
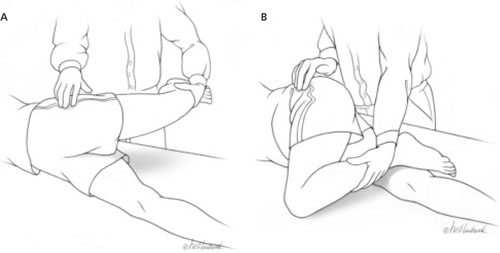
With the patient lying with the unaffected side down, passively abduct the affected hip (A), then move from full extension to 90° of flexion (B). External snapping is usually related to the iliotibial band moving over the greater trochanter, which can lead to a painful bursa.
Avulsion fractures, acetabular tears, and bursitis
Avulsion fractures are a separation of the secondary growth center, the apophyses, from the underlying bone in skeletally immature athletes. They occur because the athlete’s tendons are stronger than the cartilaginous growth centers,10,11,16,18 and are produced by sudden forceful contraction of the muscle. The patient will complain of acute pain and swelling. The exam will be positive for palpable tenderness at the bony site and for muscle weakness. The most common sites of avulsion fractures causing hip pain are the sartorius attachment at the ASIS, the rectus femoris attachment at the anterior inferior iliac spine, and the hamstring attachment onto the ischial tuberosity.10 Radiographs are diagnostic.16,18
Treatment is conservative, including rest, ice, analgesics, and ROM exercises. Advise the patient to refrain from stretching the injured muscle attachment for 6 weeks, then gradually return to activity. Surgery is needed only if there is a large separation (>2 cm).
Acetabular labral tears are seen in athletes of all ages. Pain may be acute from a traumatic event or insidious from repetitive trauma.10 Structural or developmental abnormalities may also predispose certain athletes to injury.10 Patients will complain of pain, snapping, or a “giving way” sensation in the anteromedial area of the hip. On examination, the impingement test—forced flexion/adduction and internal rotation— may reproduce the groin pain, or the snapping maneuver may produce an audible sound.10,16,19
Radiographs are obtained initially to rule out other causes of hip pain and to assess for predisposing abnormalities, such as femoroacetabular impingement. Magnetic resonance arthrogram is a highly sensitive test for labral tears and is usually diagnostic.10 Labral tears are rarely an isolated event, however, and are usually seen in combination with a chondral injury, ligamentum teres tear, synovitis, or loose bodies.10
After diagnosis, a trial of activity modification, NSAIDs, and physical therapy is acceptable. If there is no improvement after 4 to 6 weeks, patients should be referred to an orthopedist for hip arthroscopy. A few studies have found that arthroscopy provides excellent symptom relief in 70% to 90% of patients,10,19 with a return to full activity in 6 to 12 weeks.
Trochanteric bursitis is commonly seen in older adults, but can occur in children. It has been associated with leg length discrepancy and obesity—and, in younger athletes, it is often linked to running and climbing.
The condition is caused by repetitive trauma from contraction of the muscles inserting on the greater trochanter. Patients develop chronic, intermittent lateral hip pain, which may be worse with direct pressure. The predominant physical exam finding is pain with direct pressure over the greater trochanter. One study reported that >50% of patients with trochanteric bursitis had a positive Patrick’s test—the presence of pain with Flexion, ABduction, and External Rotation (FABER) of the affected hip.20