David Kealy, MSW Paul I. Steinberg, MD, FRCPC John S. Ogrodniczuk, PhD Department of Psychiatry, University of British Columbia, Vancouver david.kealy@ubc.ca
The authors reported no potential conflict of interest relevant to this article.
The patient who always seems to be in crisis may actually have a personality disorder. Employing these techniques can benefit the patient and your interaction with him.
› Evaluate a patient’s sense of identity and interpersonal relationships for clues of a personality disorder (PD). A › Use validation, promote mentalization, and manage countertransference to help patients with PDs. A › Consider medications such as antidepressants or antipsychotics for patients with PDs, but only as adjuncts to psychotherapy, and only to target specific symptoms, such as impulsive aggression. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence B Inconsistent or limited-quality patient-oriented evidence C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Bob A, age 48, comes to his family physician (FP) to ask for authorization for extended medical leave from his job as an electrician. He frequently misses days at work and complains of stress on the job, saying his coworkers look down on him and make cruel jokes at his expense. He reports having chronic interpersonal conflicts and no significant relationships with family members or friends. Mr. A refuses a referral to a psychiatrist because he fears he will be “locked up and forced to take medications.”
If Mr. A were your patient, how would you proceed?
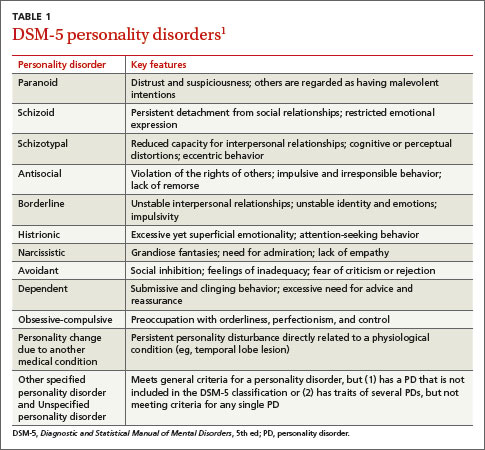
Personality disorders (PDs) are patterns of inflexible and maladaptive personality traits and behaviors that cause subjective distress and significant social or occupational impairment.1 An individual with a PD tends to have a limited repertoire of responses to the rough-and-tumble of life, with coping mechanisms that often perpetuate difficulty and distress. Examples include distrust and suspiciousness of others’ motives (paranoid PD); disregard and violation of the rights of others (antisocial PD); instability in interpersonal relationships, self-image, and affect (borderline PD); and social inhibition, feelings of inadequacy, and hypersensitivity to negative evaluation (avoidant PD).1
FPs may view patients with PDs as “difficult patients” because of their frequent crises and the interpersonal problems they bring into the physician-patient relationship.2,3 Help, of course, can come in the way of a referral to a psychotherapist who specializes in treating PDs. But you can also make use of some evidence-based psychotherapy techniques to improve your patients’ lives and the quality of the physician-patient relationship. This article focuses on identifying and managing PDs in family practice, using practical strategies drawn from empirically supported therapies.
PDs are more common than you might suspect
Personality disorders are associated with a greater incidence of serious medical illness and reduced social functioning. The overall prevalence of PD in the community ranges from 4.4% to 14.8%, with no consistent pattern of sex differences.4 Between 31.4% and 45.5% of psychiatric outpatients and up to 24% of primary care patients likely meet criteria for at least one PD.5-7 PDs impede recovery from other mental disorders,8 increase the risk for suicide,9 and are associated with substance abuse, impulsivity, and violence.10,11 Personality pathology also is associated with greater incidence of serious medical illness12,13 and reduced social functioning.14 Not surprisingly, patients with PDs frequently use medical and social services.15
PDs tend to be underdiagnosed, perhaps partly because of concern about stigmatization, but also due to difficulties in identifying and classifying these disorders. Published in 2013, the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) originally was to include a major revision of PDs—reflecting concern about the limitations of PD categories—but ultimately the existing categories were retained (TABLE 1).1 There is considerable overlap among PD categories; many patients meet the criteria for more than one PD, but it is unlikely that they actually suffer from several distinct PDs. Other patients—perhaps even the majority—are best diagnosed with “unspecified personality disorder” because they do not neatly fit into one of these categories.
Suspect your patient has a PD? Evaluate these 2 areas
Identifying patients who have PDs in primary care is useful for 2 reasons: to explore the option of specialty treatment for patients who may be amenable to it, and to improve management of the patient’s complaints in the primary care setting, including a smoother doctor-patient interaction. In either case, determining the specific DSM-5 diagnosis is less important than recognizing core personality impairment: an ingrained disturbance in one’s perceptions of self and others. This can be done by paying attention to how the patient adapts to life’s challenges and if he or she has problematic interpersonal tendencies, including difficulties in the doctor-patient relationship.
Unfortunately, assessing and diagnosing PDs in the primary care setting can be challenging. Limited time doesn’t allow for extensive, personality-focused interviews. Self-report screening tools are limited, because patients may underreport key interpersonal problems such as lack of empathy. Furthermore, very few patients seek help from their FP in addressing personality dysfunction; PDs typically are identified while investigating other complaints.