David Kealy, MSW Paul I. Steinberg, MD, FRCPC John S. Ogrodniczuk, PhD Department of Psychiatry, University of British Columbia, Vancouver david.kealy@ubc.ca
The authors reported no potential conflict of interest relevant to this article.
Recognizing countertransference can guard against extreme reactions and maintain an appropriate clinical focus. Psychodynamic approaches consider managing countertransference to be a therapeutic intervention, even when psychotherapy is not explicitly being carried out. Strong emotional responses may reflect something that the patient needs the physician to experience, as the patient cannot bear to experience it himself. The patient needs to see—and learn from—the physician’s handling of unbearable (for the patient) feelings. This occurs at a level of unconscious communication and may be repeated over time. Although not discussed with the patient, a physician’s capacity for self-containment and provision of undisrupted, good medical care is in itself a psychotherapeutic accomplishment.
CASE › Based on Mr. A’s history of interpersonal conflicts and perceived persecution by coworkers, the FP consults with a psychotherapist colleague, who says Mr. A’s chronic mistrust and social isolation suggest he may have a severe identity disturbance and unspecified PD with paranoid and schizoid features. Because Mr. A refuses to see a therapist, his FP decides to focus on promoting small improvements in Mr. A’s interpersonal interactions and reducing absenteeism at work.
The FP validates Mr. A’s feelings (“it can be very stressful to constantly feel like others are at odds with you”) and tries to promote mentalizing (“I want to understand more about what you think regarding your work situation and your coworkers. Let’s try to look at this from all perspectives—maybe we can come up with some new ideas.”)
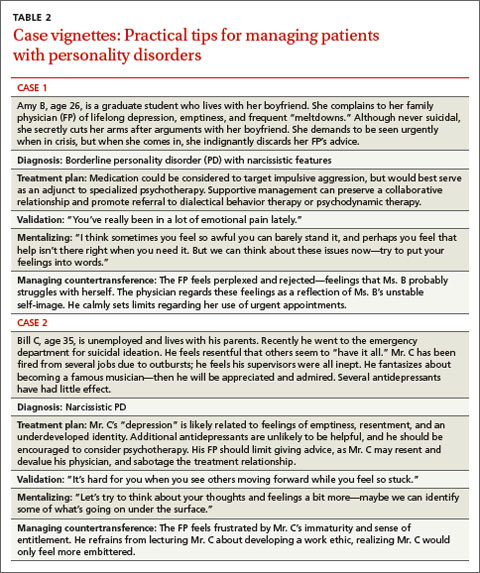
Despite wanting to help his patient, the FP feels uneasy and reluctant to engage with Mr. A, who likely evokes such feelings to keep others at a distance. The FP tactfully seeks to remain Mr. A’s ally without endorsing his distorted interpretation of events. Given Mr. A’s paranoid rejection of therapy, the FP refrains from making further such recommendations. The FP’s interventions, however, may help Mr. A warm to the idea of further help over time, and the FP’s supportive stance will help to ameliorate the patient’s distress. (For 2 additional examples of how FPs can use the strategies described in this article to help patients with PDs, see TABLE 2.)
CORRESPONDENCE David Kealy, MSW, Psychotherapy Program, Department of Psychiatry, University of British Columbia, #420-5950 University Boulevard, Vancouver, BC Canada V6T 1Z3; david.kealy@ubc.ca