Antimicrobial Stewardship Programs: Effects on Clinical and Economic Outcomes and Future Directions
Journal of Clinical Outcomes Management. 2017 July;24(7)
References
Prior authorization, also referred to as a “front-end” intervention, is the process of approving medications before they are used. Interventions include a restricted formulary for antimicrobials that can be managed through a paging system or a built-in computer restriction program, as well as other guidelines and protocols for dosing and duration of therapy. Restrictions typically focus on broad spectrum antibiotics as well as the more costly drugs on formularies. These solutions reduce the need for manual intervention as technology makes it possible to create automated restriction-based services that prevent inappropriate prescribing [6].
Aside from these main techniques, other strategies are taken to achieve the goal of attaining optimal clinical outcomes while limiting further antimicrobial resistance and adverse effects. Different clinical settings have different needs, and ASPs are customized to each setting’s resources, prescribing habits, and other local specificities [1]. These differences present difficulty with interpreting diverse datasets, but certain themes arise in the literature: commonly assessed clinical outcomes of inpatient ASPs include hospital length of stay (LOS) and readmission, reinfection, mortality, and resistance rates. These outcomes are putatively driven by the more prudent use of antimicrobials, particularly by decreased rates of antimicrobial consumption.
ASP Team Members
While ASPs may differ between institutions, the staff members involved are typically the same, and leadership is always an important aspect of a program. The CDC recommends that ASP leadership consist of a program leader (an ID physician) and a pharmacy leader, who co-lead the team [18]. In addition, the Joint Commission recommends that the multidisciplinary team should include an infection preventionist (ie, infection control and hospital epidemiologist) and practitioner [17]; these specialists have a role in prevention, awareness, and policy [19]. The integration of infection control with stewardship yields the best results [15], as infection control aims to prevent antibiotic use altogether, while stewardship increases the quality of antibiotic regimens that are being prescribed [20].
It is also beneficial to incorporate a microbiologist as an integral part of the team, responsible for performing and interpreting laboratory data (ie, cultures). Nurses should be integrated into ASPs due to the overlap of their routine activities with ASP interventions [21]; other clinicians (regardless of their infectious disease clinical background), quality control, information technology, and environmental services should all collaborate in the hospital-wide systems related to the program where appropriate [18].
Evidence Review
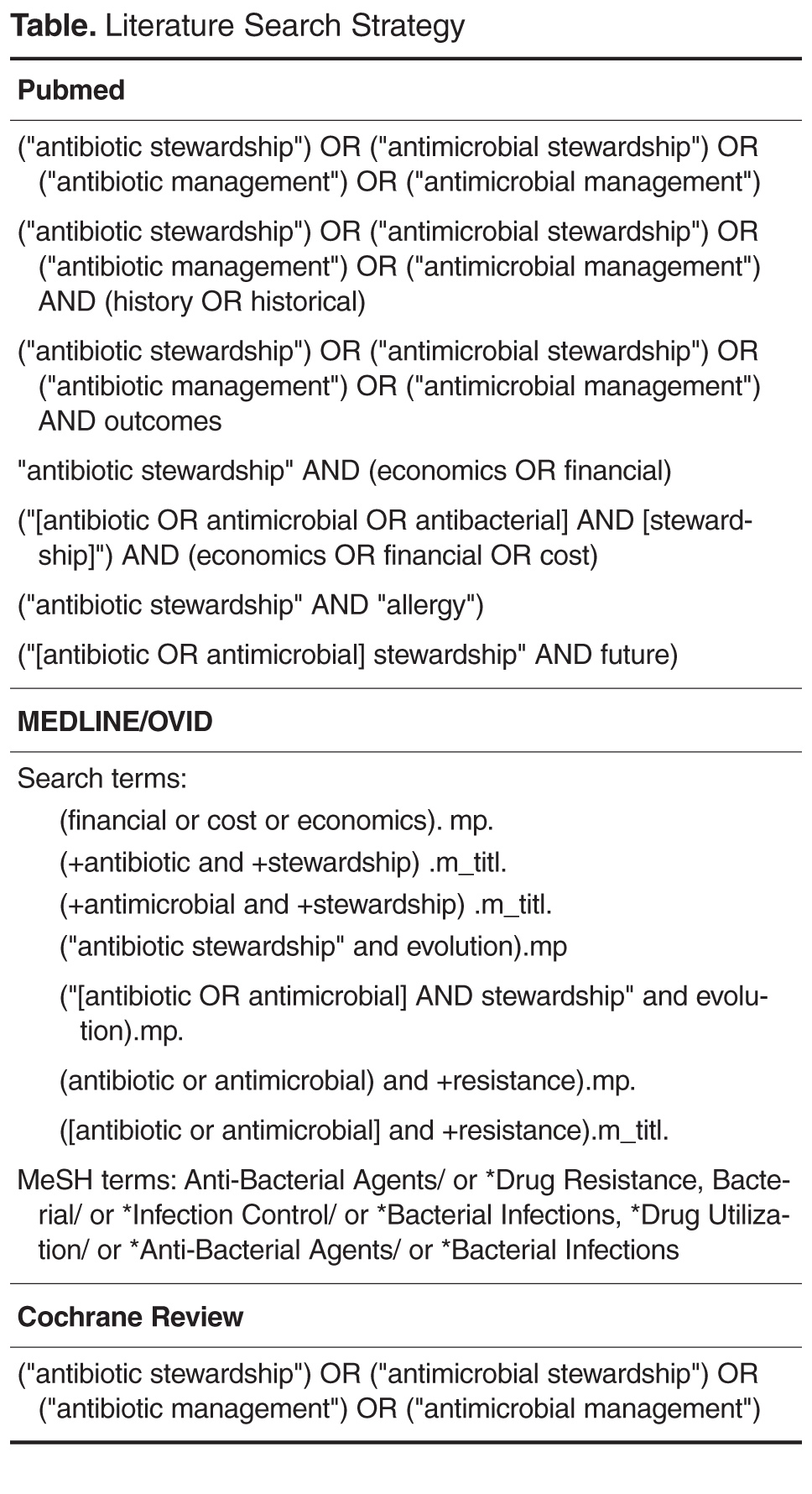
To assess the effectiveness of inpatient ASPs, we performed a literature search using Pubmed, Cochrane Database of Systematic Reviews, and MEDLINE/OVIDSp up to 1 September 2016. The search terms used are listed in the Table. Included in this review were studies evaluating clinical or economic outcomes related to inpatient ASPs; excluded were editorials, opinion pieces, articles not containing original clinical or economic ASP outcome data, ASPs not performed in the inpatient setting, and studies that were included in identified systematic reviews or meta-analyses. Also excluded from this review were studies that reviewed ASPs performed in niche settings or for applications in which ASPs were not yet prevalent, as assessed by the authors. The search initially yielded 182 articles. After removing duplicates and excluded articles, 18 articles were identified for review: 8 meta-analyses and systematic reviews and 10 additional clinical studies (2 randomized controlled, 5 observational, and 3 quasi-experimental studies) evaluating clinical and economic outcomes not contained in the identified aggregated studies. Systematic reviews, meta-analyses, and other studies were screened to identify any other relevant literature not captured in the original search. The articles included in this review are summarized in 2 Tables, which may be accessed at www.turner-white.com/pdf/jcom_jul17_antimicrobial_appendix.pdf