A Multipronged Approach to Decrease the Risk of Clostridium difficile Infection at a Community Hospital and Long-Term Care Facility
Journal of Clinical Outcomes Management. 2015 September;22(9)
References
cases during the study period. Initially, we examined the occurrence of C. difficile cases from the period prior to our initiatives (July 2008) through the end of 2013. Looking at the number of cases per quarter and breaking up the analysis into 2 time periods, the earlier period being the data up
to the 4th quarter of 2010, and the later time period being the data from 2011 on, we have the interrupted time series displayed in Figure 2 and Figure 3 . Linear regression was performed on each of the segments (Figure 3). The regression for the first segment (earlier time period) was significant (intercept 15.87, 95% confidence interval [CI] 9.31 to 22.42, t = 5.58, P = 0.001; slope –1.19, 95% CI –2.25 to –0.14. t = –2.61, P = 0.031) for the reduction in the number of C. difficile cases, while the regression for the second segment (later time period) was not (intercept 4.35, 95% CI 0.29 to 8.41, t = 2.39, P = 0.038; slope –0.16, 95% CI –0.40 to 0.08, t = –1.46, P = 0.176). Examination of the number of cases per quarter between the 2 time periods (July 2008–December 2010 and January 2011–December 2013) revealed that they differed significantly (Wilcoxon rank sum test, z = 3.91, P < 0.001) (Figure 3).
Within the population of patients having a CDI or recurrence, we found that those patients in the later time period (2011–2013) were significantly less likely to have a recurrence than those in the earlier time period (pre- Jan 2011) (chi square = 5.975, df = 1, P = 0.015). The odds ratio (OR) was 0.35 (95% CI 0.15 to 0.83).
Patients in the earlier (2009–2010) vs. the later post-intervention group (2011–2013) had more likely received multiple antibiotic courses (chi square = 5.32, df = 1, P = 0.021, OR 2.56), a PPI (chi square = 8.86, df = 1, P = 0.003, OR 3.38), and had a health care facility–associated infection originating from our institution as opposed to outside facility transfers or community-acquired cases (chi square = 7.09, df = 1, P = 0.008, OR 2.94).
Antibiotic Pressure
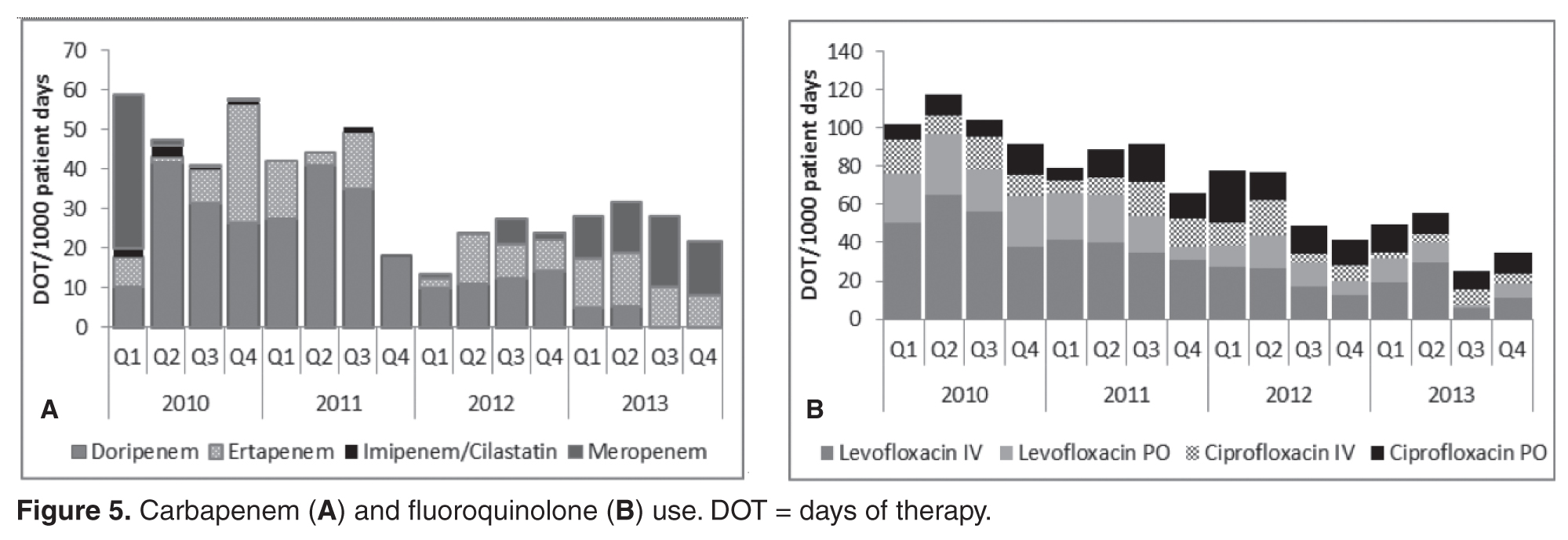
Certain antibiotic classes have been more associated with increased CDI risk. Antibiotics preceding each CDI infection are noted in Figure 4 . The data shows that proportionally more patients with CDI received fluoroquinolones as the preceding antibiotic, followed by third- or fourth-generation cephalosporins, extended-spectrum penicillins, and the carbapenem class. Some antibiotics were
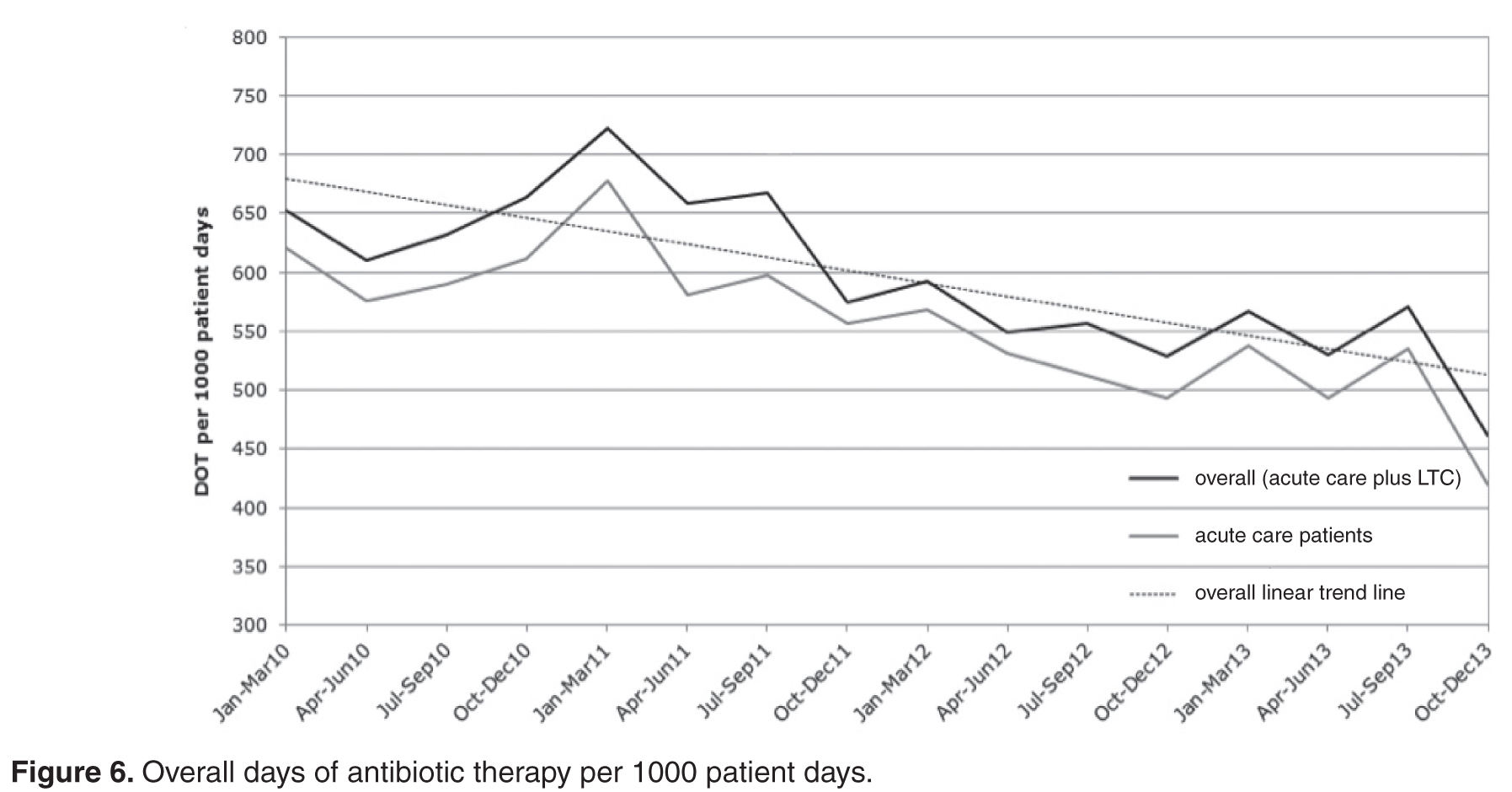
implicated simply by being combined with another higher risk class of antibiotics, eg, aminoglycosides. Our antibiotic stewardship program led to the streamlining of antibiotic therapy and reduced utilization of broad-spectrum antibiotics ( Figure 5 ). Patient days of antibiotic therapy per 1000 patient days were used for
trending antibiotic use. Since we began tracking this in 2010, we have seen a 30% reduction in overall days of therapy ( Figure 6 ). Multiple antibiotic courses also had a significant association with PPI administration in the patients who contracted CDI (chi square = 6.9, df = 1, P