Abnormal Uterine Bleeding in Reproductive-Aged Women
Journal of Clinical Outcomes Management. 2015 February;22(2)
References
What is the likely diagnosis?
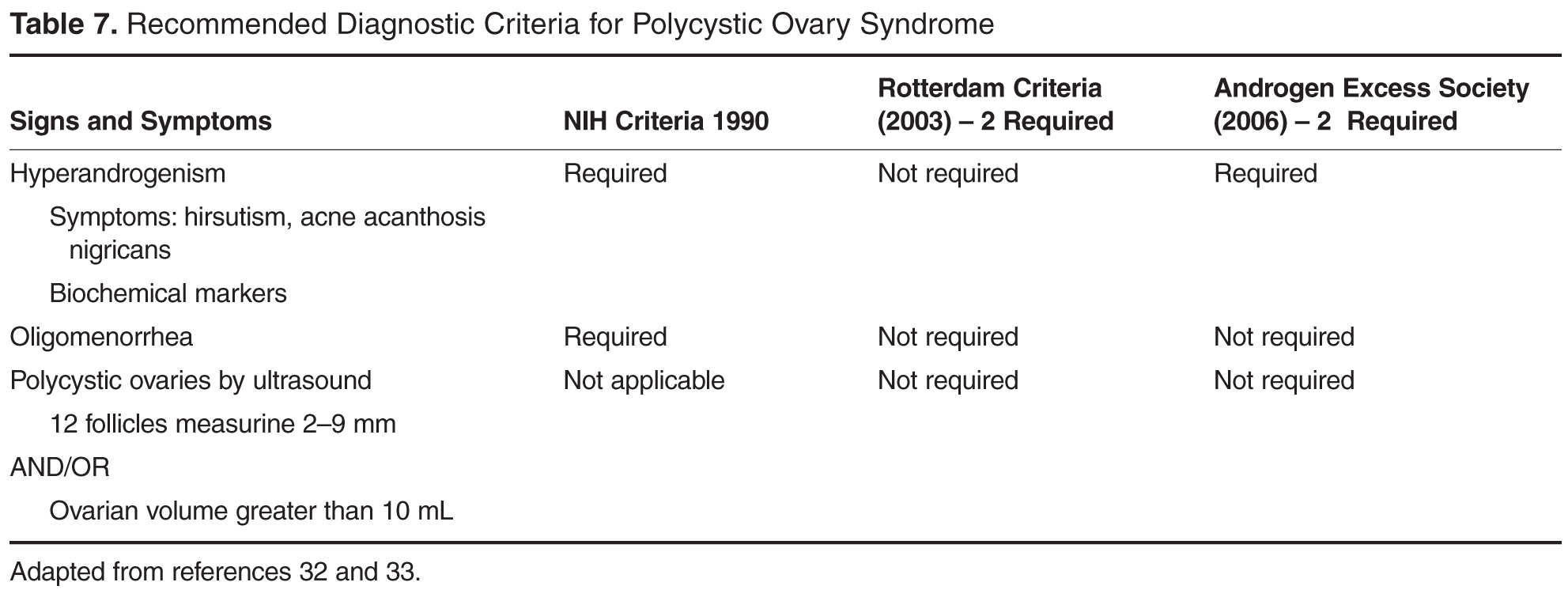
Based on her history and physical, this patient has a high likelihood of having PCOS. PCOS is a common cause of anovulation [32,35].The cause is considered multifactorial. PCOS is a hyperandrogen state that includes anovulation and increased ovarian androgen production. Several sets of diagnostic criteria have been proposed, all including some combination of oligo- or anovulation, clinical or biochemical signs of excess androgen, and ultrasound evidence of polycystic ovaries. Currently it is diagnosed when at least 2 criteria are met. These include olio- or anovulation, biochemical signs of excess androgen, and ultrasound evidence of polycystic ovaries [32,35] ( Table 7). Secondary causes of hyperandrogenism such as androgen-producing neoplasm, hyperprolactinemia and adult onset congenital adrenal hyperplasia should be ruled out but these are less likely than PCOS when classic symptoms and signs are found.
Women with PCOS are at increased risk for metabolic syndrome, nonalcoholic fatty liver disease, type 2 diabetes and cardiovascular disease, endometrial cancer, and infertility. Women with PCOS who become pregnant have increased risk of pregnancy complications such as hypertensive disorders and gestational diabetes.
What tests are indicated in this patient?
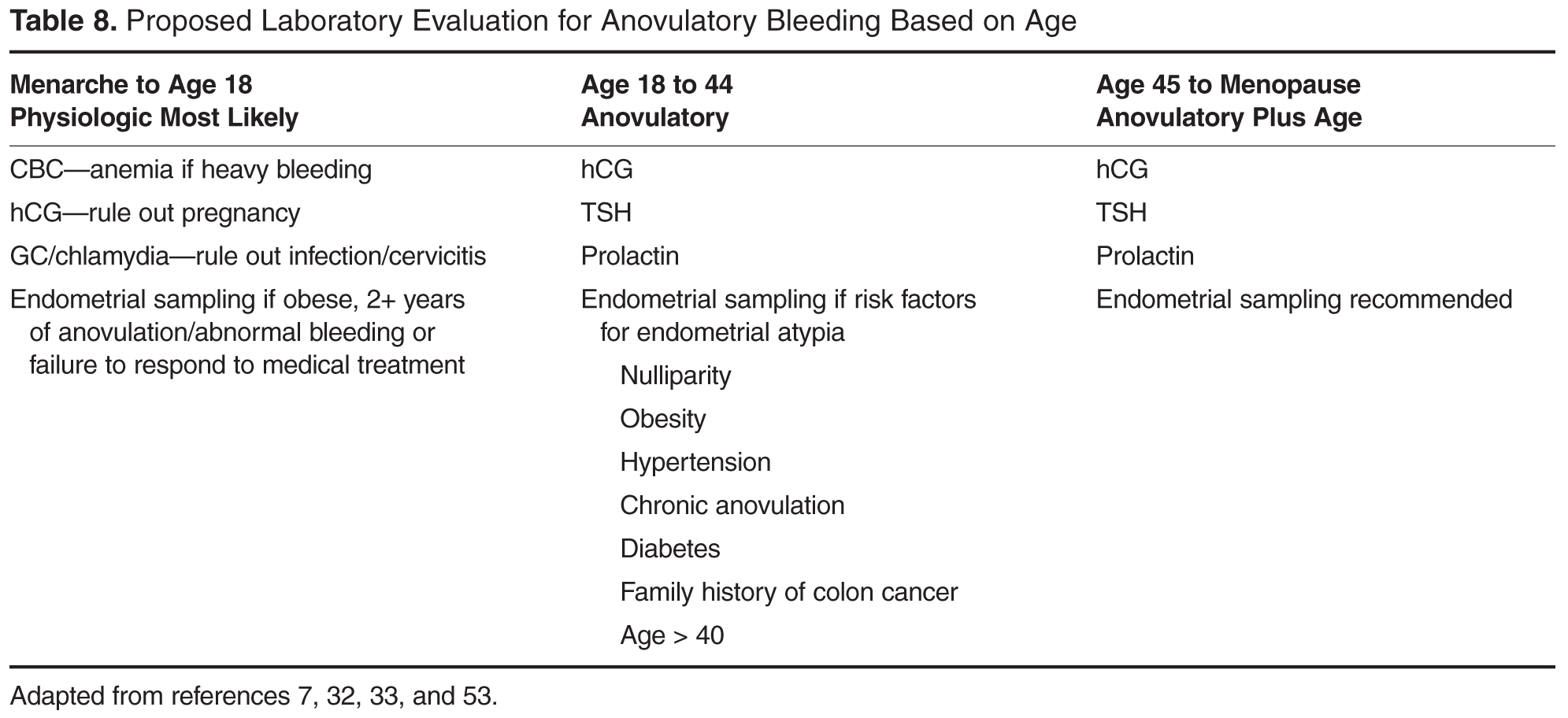
Appropriate laboratory testing is often determined based on findings in the history and physical as well as the patient’s age. Anovulation in the first 18 months to 3 years after menarche is common and testing for pregnancy, infection, and anemia are often sufficient. Menorrhagia in adolescents warrants testing for bleeding disorders as well [7].Within 3 years of menarche, menstrual cycles should become more regular. Persistent anovulatory cycles increase the likelihood of pathologic causes and warrant additional evaluation. Pregnancy testing, thyroid stimulation hormone and prolactin levels are recommended first line evaluation [7,32,34].If PCOS is suspected an ultrasound can be performed but as noted above, polycystic ovaries are not required to make the diagnosis after adolescence.
Additional testing includes testosterone levels to look for androgen secreting tumors. Late onset congenital adrenal hyperplasia is an uncommon cause of hyperandrogenism but is more common in women of Ashkenazi Jewish descent and those with a family history [34].Morning hydroxyprogesterone can be performed to evaluate for this. If women exhibit abrupt change in menstrual pattern and other signs of cortisol excess (hypertension, abdominal striae) 24-hour urine cortisol can detect Cushing’s syndrome [34].
In patients with PCOS, additional testing to evaluate for medical comorbidities is recommended. This includes screening for diabetes, dyslipidemia, and liver dysfunction.
The decision to perform endometrial evaluation depends on age, symptoms and other risk factors for endometrial hyperplasia or cancer. In women over 40, the risk is increased and chronic anovulation becomes more concerning. Even though endometrial cancer is rare in women age 19 to 39, those with increased risk for endometrial cancer such as nulliparity, hypertension, obesity, family history endometrial sampling could be considered, especially for patients who do not respond to initial treatment [7] (Table 8).
Case Continued
The patient’s prolactin and TSH are normal. Tests for diabetes are normal. Her LDL is elevated to 162, triglycerides are 200, and her HDL is 38. The physician informs her that she meets criteria for PCOS and also that she has obesity and metabolic syndrome.