From the Kaiser Permanente Center for Health Research Southeast, Atlanta, GA (Dr. Lewis) and the Division of General Internal Medicine, Johns Hopkins University School of Medicine, Baltimore, MD (Dr. Gudzune).
Abstract
Objective: To review challenges to obesity counseling in the primary care setting and suggest potential solutions.
Methods: Review of the literature.
Results: There are many challenges to obesity counseling in the primary care setting, including lack of primary care provider (PCP) training, provider weight bias, lack of reimbursement, lack of time during outpatient encounters, and limited ability to refer patients to structured weight loss support programs. However, there are potential solutions to overcome these challenges. By seeking continuing medical education on weight management and communication skills, PCPs can address any training gaps and establish rapport with patients when delivering obesity counseling. Recent policy changes including Medicare coverage of obesity counseling visits may reduce PCPs' concern about lack of reimbursement and time, and the rise of new models of care delivery and reimbursement, such as patient-centered medical homes or accountable care organizations, may facilitate referrals to ancillary providers like registered dietitians or multi-component weight loss programs.
Conclusion: Although providers face several challenges in delivering effective obesity counseling, PCPs may overcome these obstacles by pursuing continuing medical education in this area and taking advantage of new health care benefits coverage and care delivery models.
Over one-third of U.S. adults are now obese [1] and the prevalence of obesity is rising globally (2). In 2003 and 2012, the U.S. Preventive Services Task Force (USPSTF) issued a recommendation that health care providers screen all patients for obesity and offer intensive, multicomponent behavioral interventions to obese patients [3,4]. Screening for obesity typically involves assessment and classification of a patient’s body mass index (BMI). In the primary care setting, weight management may include a range of therapeutic options such as intensive behavioral counseling, prescription anti-obesity medications, and referral to bariatric surgery. Behavioral interventions typically include activities such as goal setting, diet and exercise change, and self-monitoring. A recent systematic review showed that primary care–based behavioral interventions could result in modest weight losses of 3 kg over a 12-month period, and prevent the development of diabetes and hypertension in at-risk patients [5].
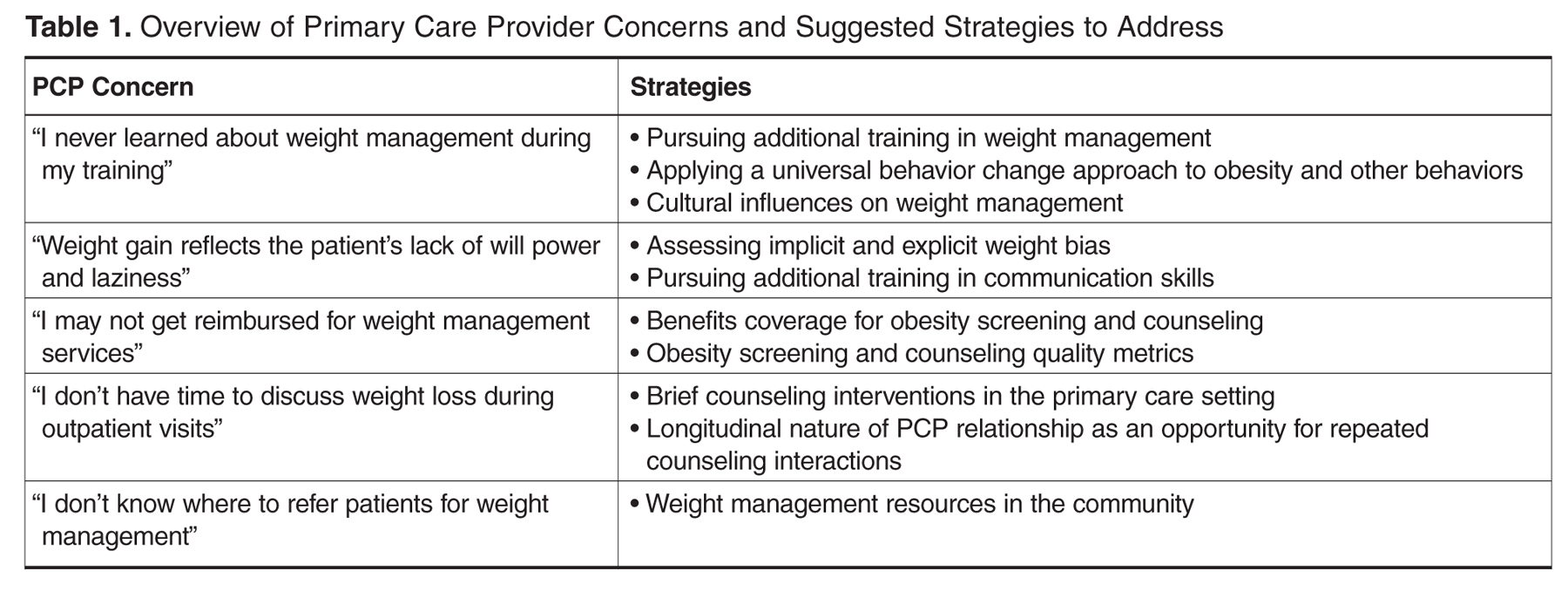
While primary care–based weight management interventions can successfully achieve modest weight loss, many obese patients do not receive the recommended treatment. Studies have found that the percentage of obese patients who received weight loss counseling from their primary care provider (PCP) varies from 20% to 40% [6–8]. Most recent estimates suggest that only 18% of obese patients receive counseling for weight reduction, 25% for dietary change, and 21% on exercise [8]. Obese patients have not reported increased rates of weight loss counseling since the USPSTF guidelines were first released in 2003 [9]. We have identified several challenges that may contribute to PCPs low rates of obesity counseling, as well as potential solutions to overcome these barriers ( Table 1 ).
PCP Concern: “I never learned about weight management during my training”
One of the most common barriers to providing the recommended counseling reported by health care providers is inadequate training in nutrition, exercise, and weight loss counseling [10–12]. Many providers have knowledge deficiencies in basic weight management [13,14]. In addition, few PCPs who have received obesity-related training rate that training as good quality during medical school (23%) and residency (35%) [15].