User login
What underlies post–bariatric surgery bone fragility?
BOSTON – Charting a healthy path for patients after bariatric surgery can be complicated and addressing bone health is an important part of the endocrinologist’s role in keeping patients safe from postsurgical fractures, according to John Bilezikian, MD.
said Dr. Bilezikian, speaking during a bariatric surgery–focused session at the annual scientific & clinical congress of the American Academy of Clinical Endocrinologists.
It’s not easy to assess bone health, even before surgery, said Dr. Bilezikian. Even objective measures of bone density, such as dual-energy x-ray absorptiometry (DXA), may be skewed: very high fat mass causes artifact that interferes with accurate measurement of bone density, and DXA can’t distinguish between cortical and trabecular bone. The latter is a particular issue in high body mass index patients, since obesity is known to be associated with a more fragile bone microarchitecture, said Dr. Bilezikian, the Dorothy L. and Daniel H. Silberberg Professor of Medicine and director of the metabolic bone diseases unit at Columbia University, New York.
With these caveats in mind, Dr. Bilezikian said, there are some lessons to be learned from existing research to better manage bone health in bariatric patients.
After Roux-en-Y gastric bypass surgery (RYGB), bone turnover soon increases, with bone resorption markers increasing by up to 200% in the first 12-18 months after surgery. Bone formation markers also are elevated but to a lesser extent, said Dr. Bilezikian. Over time, the weight loss from RYGB is associated with a significant drop in bone mineral density (BMD) at weight-bearing sites. Weight loss was associated with bone loss at the total hip (r = 0.70; P less than .0003) and femoral neck (r = 0.47; P = .03 (J Clin Endocrinol Metab. 2013 Feb;98[2] 541-9).
A newer-technology, high-resolution peripheral quantitative CT (HR-pQCT) offers a noninvasive look not just at bone size and density but also at microarchitecture, including cortical thickness and details of trabecular structure. This technology “can help elucidate the structural basis for fragility,” said Dr. Bilezikian.
HR-pQCT was used in a recent study (J Bone Min Res. 2017 Dec. 27. doi: 10.1002/jbmr.3371) that followed 48 patients for 1 year after RYGB. Using HR-pQCT, DXA, and serum markers of bone turnover, the researchers found significant decrease in BMD and estimated decrease in bone strength after RYGB. Bone cortex became increasingly porous as well. Taken together, these changes may indicate an increased fracture risk, concluded the investigators.
A longer study that followed RYGB recipients for 2 years and used similar imaging and serum parameters also found that participants had decreased BMD. Tellingly, these investigators saw more marked increase in cortical porosity in the second year after bypass. Estimated bone strength continued to decline during the study period, even after weight loss had stopped.
All of these findings, said Dr. Bilezikian, point to a pathogenetic process other than weight loss that promotes the deteriorating bone microarchitecture seen years after RYGB. “Loss of bone mass and skeletal deterioration after gastric bypass surgery cannot be explained by weight loss alone,” said Dr. Bilezikian.
Another recent study was able to follow a small cohort of patients for a full 5 years, using DXA, lumbar CT, and Hr-pQCT. Though weight loss stabilized after 2 years and 25-OH D and calcium levels were unchanged from presurgical baseline, bone density continued to drop, and bone microarchitecture further deteriorated, said Dr. Bilezikian (Greenblatt L et al. ASBMR 2017, Abstract 1125).
Initially, post–bariatric surgery weight loss may induce bone changes because of skeletal unloading; further down the road, estrogen production by adipose tissue is decreased with ongoing fat loss, and sarcopenia may have an adverse effect on bone microarchitecture. Postsurgical malabsorption may also be an early mechanism of bone loss.
Other hormonal changes can include secondary hyperparathyroidism. Leptin, adiponectin, and peptide YY levels also may be altered.
Do these changes in BMD and bone architecture result in increased fracture risk? This question is difficult to answer, for the same reasons that other bariatric surgery research can be challenging, said Dr. Bilezikian. There is heterogeneity of procedures and supplement regimens, sample sizes can be small, follow-up times short, and adherence often is not tracked.
However, there are some clues that RYGB may be associated with an increased risk of all fractures and of fragility fractures, with appendicular fractures seen most frequently (Osteoporos Int. 2014 Jan; 25[1]:151-8). A larger study that tracked 12,676 patients receiving bariatric surgery, 38,028 patients with obesity, and 126,760 nonobese participants found that the bariatric patients had a 4.1% risk of fracture at 4 years post surgery, compared with 2.7% and 2.4% fracture rates in the participants with and without obesity, respectively (BMJ. 2016;354:i3794).
Other retrospective studies have found “a time-dependent increase in nonvertebral fractures with Roux-en-Y gastric bypass compared to gastric banding,” said Dr. Bilezikian.
How can these risks be managed after gastric bypass surgery? “Strive for nutritional adequacy” as the first step, said Dr. Bilezikian, meaning that calcium and vitamin D should be prescribed – and adherence encouraged – as indicated. Levels of 25-OH D should be checked regularly, with supplementation managed to keep levels over 30 ng/mL, he said.
All patients should be encouraged to develop and maintain an appropriate exercise regimen, and BMD should be followed over time. Those caring for post–gastric bypass patients can still use a bisphosphonate or other bone-health medication, if indicated using standard parameters. However, “You probably shouldn’t use an oral bisphosphonate in this population,” said Dr. Bilezikian.
Dr. Bilezikian reported that he has consulting or advisory relationships with Amgen, Radius Pharmaceuticals, Shire Pharmaceuticals, and Ultragenyx, and serves on a data safety monitoring board for Regeneron.
BOSTON – Charting a healthy path for patients after bariatric surgery can be complicated and addressing bone health is an important part of the endocrinologist’s role in keeping patients safe from postsurgical fractures, according to John Bilezikian, MD.
said Dr. Bilezikian, speaking during a bariatric surgery–focused session at the annual scientific & clinical congress of the American Academy of Clinical Endocrinologists.
It’s not easy to assess bone health, even before surgery, said Dr. Bilezikian. Even objective measures of bone density, such as dual-energy x-ray absorptiometry (DXA), may be skewed: very high fat mass causes artifact that interferes with accurate measurement of bone density, and DXA can’t distinguish between cortical and trabecular bone. The latter is a particular issue in high body mass index patients, since obesity is known to be associated with a more fragile bone microarchitecture, said Dr. Bilezikian, the Dorothy L. and Daniel H. Silberberg Professor of Medicine and director of the metabolic bone diseases unit at Columbia University, New York.
With these caveats in mind, Dr. Bilezikian said, there are some lessons to be learned from existing research to better manage bone health in bariatric patients.
After Roux-en-Y gastric bypass surgery (RYGB), bone turnover soon increases, with bone resorption markers increasing by up to 200% in the first 12-18 months after surgery. Bone formation markers also are elevated but to a lesser extent, said Dr. Bilezikian. Over time, the weight loss from RYGB is associated with a significant drop in bone mineral density (BMD) at weight-bearing sites. Weight loss was associated with bone loss at the total hip (r = 0.70; P less than .0003) and femoral neck (r = 0.47; P = .03 (J Clin Endocrinol Metab. 2013 Feb;98[2] 541-9).
A newer-technology, high-resolution peripheral quantitative CT (HR-pQCT) offers a noninvasive look not just at bone size and density but also at microarchitecture, including cortical thickness and details of trabecular structure. This technology “can help elucidate the structural basis for fragility,” said Dr. Bilezikian.
HR-pQCT was used in a recent study (J Bone Min Res. 2017 Dec. 27. doi: 10.1002/jbmr.3371) that followed 48 patients for 1 year after RYGB. Using HR-pQCT, DXA, and serum markers of bone turnover, the researchers found significant decrease in BMD and estimated decrease in bone strength after RYGB. Bone cortex became increasingly porous as well. Taken together, these changes may indicate an increased fracture risk, concluded the investigators.
A longer study that followed RYGB recipients for 2 years and used similar imaging and serum parameters also found that participants had decreased BMD. Tellingly, these investigators saw more marked increase in cortical porosity in the second year after bypass. Estimated bone strength continued to decline during the study period, even after weight loss had stopped.
All of these findings, said Dr. Bilezikian, point to a pathogenetic process other than weight loss that promotes the deteriorating bone microarchitecture seen years after RYGB. “Loss of bone mass and skeletal deterioration after gastric bypass surgery cannot be explained by weight loss alone,” said Dr. Bilezikian.
Another recent study was able to follow a small cohort of patients for a full 5 years, using DXA, lumbar CT, and Hr-pQCT. Though weight loss stabilized after 2 years and 25-OH D and calcium levels were unchanged from presurgical baseline, bone density continued to drop, and bone microarchitecture further deteriorated, said Dr. Bilezikian (Greenblatt L et al. ASBMR 2017, Abstract 1125).
Initially, post–bariatric surgery weight loss may induce bone changes because of skeletal unloading; further down the road, estrogen production by adipose tissue is decreased with ongoing fat loss, and sarcopenia may have an adverse effect on bone microarchitecture. Postsurgical malabsorption may also be an early mechanism of bone loss.
Other hormonal changes can include secondary hyperparathyroidism. Leptin, adiponectin, and peptide YY levels also may be altered.
Do these changes in BMD and bone architecture result in increased fracture risk? This question is difficult to answer, for the same reasons that other bariatric surgery research can be challenging, said Dr. Bilezikian. There is heterogeneity of procedures and supplement regimens, sample sizes can be small, follow-up times short, and adherence often is not tracked.
However, there are some clues that RYGB may be associated with an increased risk of all fractures and of fragility fractures, with appendicular fractures seen most frequently (Osteoporos Int. 2014 Jan; 25[1]:151-8). A larger study that tracked 12,676 patients receiving bariatric surgery, 38,028 patients with obesity, and 126,760 nonobese participants found that the bariatric patients had a 4.1% risk of fracture at 4 years post surgery, compared with 2.7% and 2.4% fracture rates in the participants with and without obesity, respectively (BMJ. 2016;354:i3794).
Other retrospective studies have found “a time-dependent increase in nonvertebral fractures with Roux-en-Y gastric bypass compared to gastric banding,” said Dr. Bilezikian.
How can these risks be managed after gastric bypass surgery? “Strive for nutritional adequacy” as the first step, said Dr. Bilezikian, meaning that calcium and vitamin D should be prescribed – and adherence encouraged – as indicated. Levels of 25-OH D should be checked regularly, with supplementation managed to keep levels over 30 ng/mL, he said.
All patients should be encouraged to develop and maintain an appropriate exercise regimen, and BMD should be followed over time. Those caring for post–gastric bypass patients can still use a bisphosphonate or other bone-health medication, if indicated using standard parameters. However, “You probably shouldn’t use an oral bisphosphonate in this population,” said Dr. Bilezikian.
Dr. Bilezikian reported that he has consulting or advisory relationships with Amgen, Radius Pharmaceuticals, Shire Pharmaceuticals, and Ultragenyx, and serves on a data safety monitoring board for Regeneron.
BOSTON – Charting a healthy path for patients after bariatric surgery can be complicated and addressing bone health is an important part of the endocrinologist’s role in keeping patients safe from postsurgical fractures, according to John Bilezikian, MD.
said Dr. Bilezikian, speaking during a bariatric surgery–focused session at the annual scientific & clinical congress of the American Academy of Clinical Endocrinologists.
It’s not easy to assess bone health, even before surgery, said Dr. Bilezikian. Even objective measures of bone density, such as dual-energy x-ray absorptiometry (DXA), may be skewed: very high fat mass causes artifact that interferes with accurate measurement of bone density, and DXA can’t distinguish between cortical and trabecular bone. The latter is a particular issue in high body mass index patients, since obesity is known to be associated with a more fragile bone microarchitecture, said Dr. Bilezikian, the Dorothy L. and Daniel H. Silberberg Professor of Medicine and director of the metabolic bone diseases unit at Columbia University, New York.
With these caveats in mind, Dr. Bilezikian said, there are some lessons to be learned from existing research to better manage bone health in bariatric patients.
After Roux-en-Y gastric bypass surgery (RYGB), bone turnover soon increases, with bone resorption markers increasing by up to 200% in the first 12-18 months after surgery. Bone formation markers also are elevated but to a lesser extent, said Dr. Bilezikian. Over time, the weight loss from RYGB is associated with a significant drop in bone mineral density (BMD) at weight-bearing sites. Weight loss was associated with bone loss at the total hip (r = 0.70; P less than .0003) and femoral neck (r = 0.47; P = .03 (J Clin Endocrinol Metab. 2013 Feb;98[2] 541-9).
A newer-technology, high-resolution peripheral quantitative CT (HR-pQCT) offers a noninvasive look not just at bone size and density but also at microarchitecture, including cortical thickness and details of trabecular structure. This technology “can help elucidate the structural basis for fragility,” said Dr. Bilezikian.
HR-pQCT was used in a recent study (J Bone Min Res. 2017 Dec. 27. doi: 10.1002/jbmr.3371) that followed 48 patients for 1 year after RYGB. Using HR-pQCT, DXA, and serum markers of bone turnover, the researchers found significant decrease in BMD and estimated decrease in bone strength after RYGB. Bone cortex became increasingly porous as well. Taken together, these changes may indicate an increased fracture risk, concluded the investigators.
A longer study that followed RYGB recipients for 2 years and used similar imaging and serum parameters also found that participants had decreased BMD. Tellingly, these investigators saw more marked increase in cortical porosity in the second year after bypass. Estimated bone strength continued to decline during the study period, even after weight loss had stopped.
All of these findings, said Dr. Bilezikian, point to a pathogenetic process other than weight loss that promotes the deteriorating bone microarchitecture seen years after RYGB. “Loss of bone mass and skeletal deterioration after gastric bypass surgery cannot be explained by weight loss alone,” said Dr. Bilezikian.
Another recent study was able to follow a small cohort of patients for a full 5 years, using DXA, lumbar CT, and Hr-pQCT. Though weight loss stabilized after 2 years and 25-OH D and calcium levels were unchanged from presurgical baseline, bone density continued to drop, and bone microarchitecture further deteriorated, said Dr. Bilezikian (Greenblatt L et al. ASBMR 2017, Abstract 1125).
Initially, post–bariatric surgery weight loss may induce bone changes because of skeletal unloading; further down the road, estrogen production by adipose tissue is decreased with ongoing fat loss, and sarcopenia may have an adverse effect on bone microarchitecture. Postsurgical malabsorption may also be an early mechanism of bone loss.
Other hormonal changes can include secondary hyperparathyroidism. Leptin, adiponectin, and peptide YY levels also may be altered.
Do these changes in BMD and bone architecture result in increased fracture risk? This question is difficult to answer, for the same reasons that other bariatric surgery research can be challenging, said Dr. Bilezikian. There is heterogeneity of procedures and supplement regimens, sample sizes can be small, follow-up times short, and adherence often is not tracked.
However, there are some clues that RYGB may be associated with an increased risk of all fractures and of fragility fractures, with appendicular fractures seen most frequently (Osteoporos Int. 2014 Jan; 25[1]:151-8). A larger study that tracked 12,676 patients receiving bariatric surgery, 38,028 patients with obesity, and 126,760 nonobese participants found that the bariatric patients had a 4.1% risk of fracture at 4 years post surgery, compared with 2.7% and 2.4% fracture rates in the participants with and without obesity, respectively (BMJ. 2016;354:i3794).
Other retrospective studies have found “a time-dependent increase in nonvertebral fractures with Roux-en-Y gastric bypass compared to gastric banding,” said Dr. Bilezikian.
How can these risks be managed after gastric bypass surgery? “Strive for nutritional adequacy” as the first step, said Dr. Bilezikian, meaning that calcium and vitamin D should be prescribed – and adherence encouraged – as indicated. Levels of 25-OH D should be checked regularly, with supplementation managed to keep levels over 30 ng/mL, he said.
All patients should be encouraged to develop and maintain an appropriate exercise regimen, and BMD should be followed over time. Those caring for post–gastric bypass patients can still use a bisphosphonate or other bone-health medication, if indicated using standard parameters. However, “You probably shouldn’t use an oral bisphosphonate in this population,” said Dr. Bilezikian.
Dr. Bilezikian reported that he has consulting or advisory relationships with Amgen, Radius Pharmaceuticals, Shire Pharmaceuticals, and Ultragenyx, and serves on a data safety monitoring board for Regeneron.
REPORTING FROM AACE 2018
The case for bariatric surgery to manage CV risk in diabetes
BOSTON – For patients with obesity and metabolic syndrome or type 2 diabetes ( health over the lifespan.
“Behavioral changes in diet and activity may be effective over the short term, but they are often ineffective over the long term,” said Daniel L. Hurley, MD. By contrast, “Bariatric surgery is very effective long-term,” he said.
At the annual clinical and scientific meeting of the American Association of Clinical Endocrinologists, Dr. Hurley made the case for bariatric surgery in effective and durable management of type 2 diabetes and cardiovascular risk, weighing risks and benefits for those with higher and lower levels of obesity.
Speaking during a morning session focused on bariatric surgery, Dr. Hurley, an endocrionologist at the Mayo Clinic, Rochester, Minn., noted that bariatric surgery reduces not just weight, but also visceral adiposity. This, he said, is important when thinking about type 2 diabetes (T2D), because diabetes prevalence has climbed in the United States as obesity has also increased, according to examination of data from the National Health and Nutrition Examination Survey (NHANES).
Additionally, increased abdominal adiposity is associated with increased risk for cardiovascular-related deaths, myocardial infarctions, and all-cause deaths. Some of this relationship is mediated by T2D, which itself “is a major cause of cardiovascular-related morbidity and mortality,” said Dr. Hurley.
From a population health perspective, the increased prevalence of T2D – expected to reach 10% in the United States by 2030 – will also boost cardiovascular morbidity and mortality, said Dr. Hurley. Those with T2D die 5 to 10 years earlier, and have double the risk for heart attack and stroke of their peers without diabetes. The risk of lower limb amputation can be as much as 40 times greater for an individual with T2D across the lifespan, he said.
The National Institutes of Health recognizes bariatric surgery as an appropriate weight loss therapy for individuals with a body mass index (BMI) of at least 35 kg/m2 and comorbidity. Whether bariatric surgery might be appropriate for individuals with T2D and BMIs of less than 35 kg/m2 is less settled, though at least some RCTs support the surgical approach, said Dr. Hurley.
The body of data that support long-term metabolic and cardiovascular benefits of bariatric surgery as obesity therapy is growing, said Dr. Hurley. A large prospective observational study by the American College of Surgeons’ Bariatric Surgery Center Network followed 28,616 patients, finding that Roux-en-Y gastric bypass (RYGB) was most effective in improving or resolving CVD comorbidities. At 1 year post surgery, 83% of RYGB patients saw improvement or resolution of T2D; the figure was 79% for hypertension and 66% for dyslipidemia (Ann Surg. 2011;254[3]:410-20).
Weight loss for patients receiving bariatric procedures has generally been durable: for laparoscopic RYGB patients tracked to 7 years after surgery, 75% had maintained at least a 20% weight loss (JAMA Surg. 2018;153[5]427-34).
Longer-term clinical follow-up points toward favorable metabolic and cardiovascular outcomes, said Dr. Hurley, citing data from the Swedish Obese Subjects (SOS) trial. This study followed over 4,000 patients with high BMIs (at least 34 kg/m2 for men and 38 kg/m2 for women) over 10 years. At that point, 36% of gastric bypass patients, compared with 13% of non-surgical high BMI patients, saw resolution of T2D, a significant difference. Triglyceride levels also fell significantly more for the bypass recipients. Hypertension was resolved in just 19% of patients at 10 years, a non-significant difference from the 11% of control patients. Data from the same patient set also showed a significant reduction in total cardiovascular events in the surgical versus non-surgical patients (n = 49 vs. 28, hazard ratio 0.83, log-rank P = .05). Fatal cardiovascular events were significantly lower for patients who had received bariatric surgery, with a 24% decline in mortality for bariatric surgery patients at about 11 years post surgery.
Canadian data showed even greater reductions in mortality, with an 89% decrease in mortality after RYGB, compared with non-surgical patients at the 5-year mark (Ann Surg 2004;240:416-24).
In trials that afforded a direct comparison of medical therapy and bariatric surgery obesity and diabetes, Dr. Hurley said that randomized trials generally show no change to modest change in HbA1c levels with medical management. By contrast, patients in the surgical arms showed a range of improvement ranging from a reduction of just under 1% to reductions of over 5%, with an average reduction of more than 2% across the trials.
Separating out data from the randomized controlled trials with patient BMIs averaging 35 kg/m2 or less, odds ratios still favored bariatric surgery over medication therapy for diabetes-related outcomes in this lower-BMI population, said Dr. Hurley (Diabetes Care 2016;39:924-33).
More data come from a recently reported randomized trial that assigned patients with T2D and a mean BMI of 37 kg/m2 (range, 27-43) to intensive medical therapy, or either sleeve gastrectomy (SG) or RYGB. The study, which had a 90% completion rate at the 5-year mark, found that both surgical procedures were significantly more effective at reducing HbA1c to 6% or less 12 months into the study (P less than .001).
At the 60-month mark, 45% of the RYGB and 25% of the SG patients were on no diabetes medications, while just 2% of the medical therapy arm had stopped all medications, and 40% of this group remained on insulin 5 years into the study, said Dr. Hurley (N Engl J Med. 2017;376:641-651).
“For treatment of type 2 diabetes and cardiovascular co-morbidities, long-term goals often are met following bariatric surgery versus behavior change,” said Dr. Hurley.
Dr. Hurley reported that he had no financial disclosures.
koakes@mdedge.com
SOURCE: Hurley, D. AACE 2018, Session SGS-4.
BOSTON – For patients with obesity and metabolic syndrome or type 2 diabetes ( health over the lifespan.
“Behavioral changes in diet and activity may be effective over the short term, but they are often ineffective over the long term,” said Daniel L. Hurley, MD. By contrast, “Bariatric surgery is very effective long-term,” he said.
At the annual clinical and scientific meeting of the American Association of Clinical Endocrinologists, Dr. Hurley made the case for bariatric surgery in effective and durable management of type 2 diabetes and cardiovascular risk, weighing risks and benefits for those with higher and lower levels of obesity.
Speaking during a morning session focused on bariatric surgery, Dr. Hurley, an endocrionologist at the Mayo Clinic, Rochester, Minn., noted that bariatric surgery reduces not just weight, but also visceral adiposity. This, he said, is important when thinking about type 2 diabetes (T2D), because diabetes prevalence has climbed in the United States as obesity has also increased, according to examination of data from the National Health and Nutrition Examination Survey (NHANES).
Additionally, increased abdominal adiposity is associated with increased risk for cardiovascular-related deaths, myocardial infarctions, and all-cause deaths. Some of this relationship is mediated by T2D, which itself “is a major cause of cardiovascular-related morbidity and mortality,” said Dr. Hurley.
From a population health perspective, the increased prevalence of T2D – expected to reach 10% in the United States by 2030 – will also boost cardiovascular morbidity and mortality, said Dr. Hurley. Those with T2D die 5 to 10 years earlier, and have double the risk for heart attack and stroke of their peers without diabetes. The risk of lower limb amputation can be as much as 40 times greater for an individual with T2D across the lifespan, he said.
The National Institutes of Health recognizes bariatric surgery as an appropriate weight loss therapy for individuals with a body mass index (BMI) of at least 35 kg/m2 and comorbidity. Whether bariatric surgery might be appropriate for individuals with T2D and BMIs of less than 35 kg/m2 is less settled, though at least some RCTs support the surgical approach, said Dr. Hurley.
The body of data that support long-term metabolic and cardiovascular benefits of bariatric surgery as obesity therapy is growing, said Dr. Hurley. A large prospective observational study by the American College of Surgeons’ Bariatric Surgery Center Network followed 28,616 patients, finding that Roux-en-Y gastric bypass (RYGB) was most effective in improving or resolving CVD comorbidities. At 1 year post surgery, 83% of RYGB patients saw improvement or resolution of T2D; the figure was 79% for hypertension and 66% for dyslipidemia (Ann Surg. 2011;254[3]:410-20).
Weight loss for patients receiving bariatric procedures has generally been durable: for laparoscopic RYGB patients tracked to 7 years after surgery, 75% had maintained at least a 20% weight loss (JAMA Surg. 2018;153[5]427-34).
Longer-term clinical follow-up points toward favorable metabolic and cardiovascular outcomes, said Dr. Hurley, citing data from the Swedish Obese Subjects (SOS) trial. This study followed over 4,000 patients with high BMIs (at least 34 kg/m2 for men and 38 kg/m2 for women) over 10 years. At that point, 36% of gastric bypass patients, compared with 13% of non-surgical high BMI patients, saw resolution of T2D, a significant difference. Triglyceride levels also fell significantly more for the bypass recipients. Hypertension was resolved in just 19% of patients at 10 years, a non-significant difference from the 11% of control patients. Data from the same patient set also showed a significant reduction in total cardiovascular events in the surgical versus non-surgical patients (n = 49 vs. 28, hazard ratio 0.83, log-rank P = .05). Fatal cardiovascular events were significantly lower for patients who had received bariatric surgery, with a 24% decline in mortality for bariatric surgery patients at about 11 years post surgery.
Canadian data showed even greater reductions in mortality, with an 89% decrease in mortality after RYGB, compared with non-surgical patients at the 5-year mark (Ann Surg 2004;240:416-24).
In trials that afforded a direct comparison of medical therapy and bariatric surgery obesity and diabetes, Dr. Hurley said that randomized trials generally show no change to modest change in HbA1c levels with medical management. By contrast, patients in the surgical arms showed a range of improvement ranging from a reduction of just under 1% to reductions of over 5%, with an average reduction of more than 2% across the trials.
Separating out data from the randomized controlled trials with patient BMIs averaging 35 kg/m2 or less, odds ratios still favored bariatric surgery over medication therapy for diabetes-related outcomes in this lower-BMI population, said Dr. Hurley (Diabetes Care 2016;39:924-33).
More data come from a recently reported randomized trial that assigned patients with T2D and a mean BMI of 37 kg/m2 (range, 27-43) to intensive medical therapy, or either sleeve gastrectomy (SG) or RYGB. The study, which had a 90% completion rate at the 5-year mark, found that both surgical procedures were significantly more effective at reducing HbA1c to 6% or less 12 months into the study (P less than .001).
At the 60-month mark, 45% of the RYGB and 25% of the SG patients were on no diabetes medications, while just 2% of the medical therapy arm had stopped all medications, and 40% of this group remained on insulin 5 years into the study, said Dr. Hurley (N Engl J Med. 2017;376:641-651).
“For treatment of type 2 diabetes and cardiovascular co-morbidities, long-term goals often are met following bariatric surgery versus behavior change,” said Dr. Hurley.
Dr. Hurley reported that he had no financial disclosures.
koakes@mdedge.com
SOURCE: Hurley, D. AACE 2018, Session SGS-4.
BOSTON – For patients with obesity and metabolic syndrome or type 2 diabetes ( health over the lifespan.
“Behavioral changes in diet and activity may be effective over the short term, but they are often ineffective over the long term,” said Daniel L. Hurley, MD. By contrast, “Bariatric surgery is very effective long-term,” he said.
At the annual clinical and scientific meeting of the American Association of Clinical Endocrinologists, Dr. Hurley made the case for bariatric surgery in effective and durable management of type 2 diabetes and cardiovascular risk, weighing risks and benefits for those with higher and lower levels of obesity.
Speaking during a morning session focused on bariatric surgery, Dr. Hurley, an endocrionologist at the Mayo Clinic, Rochester, Minn., noted that bariatric surgery reduces not just weight, but also visceral adiposity. This, he said, is important when thinking about type 2 diabetes (T2D), because diabetes prevalence has climbed in the United States as obesity has also increased, according to examination of data from the National Health and Nutrition Examination Survey (NHANES).
Additionally, increased abdominal adiposity is associated with increased risk for cardiovascular-related deaths, myocardial infarctions, and all-cause deaths. Some of this relationship is mediated by T2D, which itself “is a major cause of cardiovascular-related morbidity and mortality,” said Dr. Hurley.
From a population health perspective, the increased prevalence of T2D – expected to reach 10% in the United States by 2030 – will also boost cardiovascular morbidity and mortality, said Dr. Hurley. Those with T2D die 5 to 10 years earlier, and have double the risk for heart attack and stroke of their peers without diabetes. The risk of lower limb amputation can be as much as 40 times greater for an individual with T2D across the lifespan, he said.
The National Institutes of Health recognizes bariatric surgery as an appropriate weight loss therapy for individuals with a body mass index (BMI) of at least 35 kg/m2 and comorbidity. Whether bariatric surgery might be appropriate for individuals with T2D and BMIs of less than 35 kg/m2 is less settled, though at least some RCTs support the surgical approach, said Dr. Hurley.
The body of data that support long-term metabolic and cardiovascular benefits of bariatric surgery as obesity therapy is growing, said Dr. Hurley. A large prospective observational study by the American College of Surgeons’ Bariatric Surgery Center Network followed 28,616 patients, finding that Roux-en-Y gastric bypass (RYGB) was most effective in improving or resolving CVD comorbidities. At 1 year post surgery, 83% of RYGB patients saw improvement or resolution of T2D; the figure was 79% for hypertension and 66% for dyslipidemia (Ann Surg. 2011;254[3]:410-20).
Weight loss for patients receiving bariatric procedures has generally been durable: for laparoscopic RYGB patients tracked to 7 years after surgery, 75% had maintained at least a 20% weight loss (JAMA Surg. 2018;153[5]427-34).
Longer-term clinical follow-up points toward favorable metabolic and cardiovascular outcomes, said Dr. Hurley, citing data from the Swedish Obese Subjects (SOS) trial. This study followed over 4,000 patients with high BMIs (at least 34 kg/m2 for men and 38 kg/m2 for women) over 10 years. At that point, 36% of gastric bypass patients, compared with 13% of non-surgical high BMI patients, saw resolution of T2D, a significant difference. Triglyceride levels also fell significantly more for the bypass recipients. Hypertension was resolved in just 19% of patients at 10 years, a non-significant difference from the 11% of control patients. Data from the same patient set also showed a significant reduction in total cardiovascular events in the surgical versus non-surgical patients (n = 49 vs. 28, hazard ratio 0.83, log-rank P = .05). Fatal cardiovascular events were significantly lower for patients who had received bariatric surgery, with a 24% decline in mortality for bariatric surgery patients at about 11 years post surgery.
Canadian data showed even greater reductions in mortality, with an 89% decrease in mortality after RYGB, compared with non-surgical patients at the 5-year mark (Ann Surg 2004;240:416-24).
In trials that afforded a direct comparison of medical therapy and bariatric surgery obesity and diabetes, Dr. Hurley said that randomized trials generally show no change to modest change in HbA1c levels with medical management. By contrast, patients in the surgical arms showed a range of improvement ranging from a reduction of just under 1% to reductions of over 5%, with an average reduction of more than 2% across the trials.
Separating out data from the randomized controlled trials with patient BMIs averaging 35 kg/m2 or less, odds ratios still favored bariatric surgery over medication therapy for diabetes-related outcomes in this lower-BMI population, said Dr. Hurley (Diabetes Care 2016;39:924-33).
More data come from a recently reported randomized trial that assigned patients with T2D and a mean BMI of 37 kg/m2 (range, 27-43) to intensive medical therapy, or either sleeve gastrectomy (SG) or RYGB. The study, which had a 90% completion rate at the 5-year mark, found that both surgical procedures were significantly more effective at reducing HbA1c to 6% or less 12 months into the study (P less than .001).
At the 60-month mark, 45% of the RYGB and 25% of the SG patients were on no diabetes medications, while just 2% of the medical therapy arm had stopped all medications, and 40% of this group remained on insulin 5 years into the study, said Dr. Hurley (N Engl J Med. 2017;376:641-651).
“For treatment of type 2 diabetes and cardiovascular co-morbidities, long-term goals often are met following bariatric surgery versus behavior change,” said Dr. Hurley.
Dr. Hurley reported that he had no financial disclosures.
koakes@mdedge.com
SOURCE: Hurley, D. AACE 2018, Session SGS-4.
EXPERT ANALYSIS FROM AACE 2018
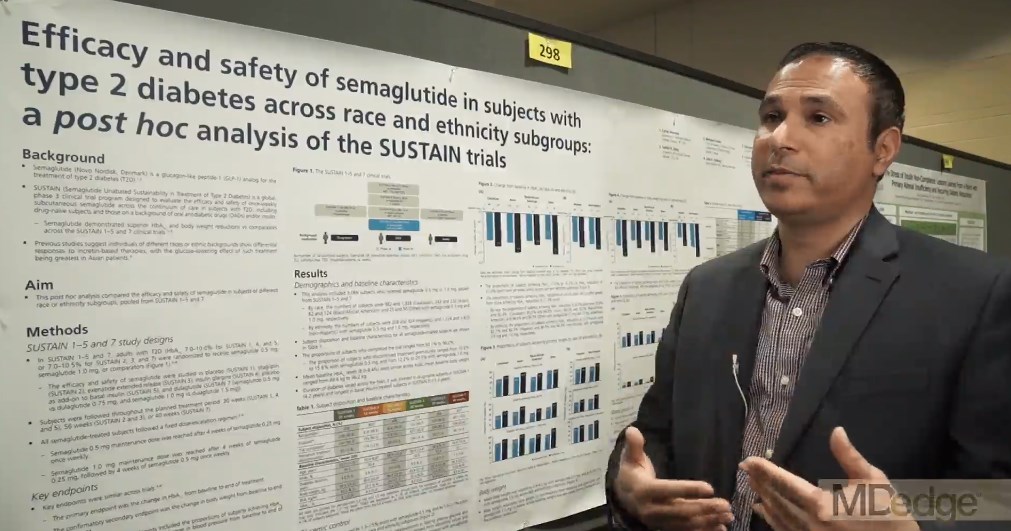
Semaglutide drops HbA1c, weight, across ethnicities
BOSTON – studied in a series of clinical trials; the efficacy did not come at the cost of frequent hypoglycemia or other serious adverse events, according to a pooled subgroup analysis of the SUSTAIN trials.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The trials investigated the safety and efficacy of semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, in the treatment of T2DM. Cyrus V. Desouza, MBBS, presented results of a post hoc analysis of racial and ethnic subgroups, drawing on SUSTAIN trials 1-5 and 7 (SUSTAIN 6 had a different design, focusing on cardiovascular outcomes).
“The trials incorporated patients on the whole spectrum of diabetes, starting from people who are newly diagnosed ... all the way to patients who were on a combination of oral antidiabetic drugs plus insulin,” Dr. Desouza explained in an interview at the annual scientific & clinical congress of the American Association of Clinical Endocrinologists.
The mean time since diagnosis in the SUSTAIN trials varied from 4.2 years in SUSTAIN 1 to 13.3 years in SUSTAIN 5. Dr. Desouza and his colleagues pooled data from the six trials to conduct the subgroup analyses.
Patients in the intervention arms of all trials received once weekly subcutaneous semaglutide, at a dose of either 0.5 mg or 1.0 mg, according to Dr. Desouza, professor of diabetes, endocrinology, and metabolism and Schultz Professor of Diabetes Research, Diabetes, Endocrinology, and Metabolism at the University of Nebraska, Lincoln.
In all, data from 3,066 patients were available. In the racial analysis, 982 low- and 1,328 high-dose semaglutide recipients were white, 243 and 232 were Asian, 82 and 124 were African American, and 25 and 50 identified as “other,” respectively.
An analysis by ethnicity found that 208 low- and 324 high-dose recipients were Hispanic.
At baseline in all trials, mean hemoglobin A1c levels were similar, ranging from 8% to 8.4%; weights at baseline were a mean 89.6 kg to 96.2 kg across the trials.
The range of reductions in HbA1c was similar across racial and ethnic groups. “If you look at the proportion of patients who actually achieved an A1c below 7[%], it’s pretty impressive – it’s between 70% to 80%.” Between 50% and 60% of patients reached an HbA1c less than 6.5%, said Dr. Desouza.
Looking at the data another way, 62.2%-72.4% of patients saw an HbA1c reduction of at least 1% on low-dose semaglutide; the range across ethnicities was 74.2%-87.1% on high-dose semaglutide. Dr. Desouza said that the sample sizes weren’t large enough to calculate statistical significance for these subgroup differences.
“But I think what is impressive is that over 50% of patients in all the races and ethnicities were able to achieve a 5% body weight loss, which is metabolically significant in terms of improving outcomes,” he said. “I think that’s a really important fact.” A smaller proportion – around 20% – lost at least 10% of body weight, mostly on high-dose semaglutide.
Severe hypoglycemia, as defined by American Diabetes Association classification, was very rare across trials, except that 4.7% of African Americans saw this adverse event on high-dose semaglutide. Incidence in other subgroups, at either dose, ranged from 0% to 2.4%.
Otherwise, the medication was generally well tolerated, though gastrointestinal side effects were seen. “Asian people have a little higher GI side effects – up to 50% of Asians did develop GI side effects, and between 10% and 13% of Asians had to stop medication due to side effects,” said Dr. Desouza. “So I think that would be the one caveat in terms of tolerance that we did learn.”
The SUSTAIN trials were sponsored by Novo Nordisk. Dr. Desouza has received consulting fees for Novo Nordisk and has received grant support from several other pharmaceutical companies. Two coauthors are Novo Nordisk employees.
SOURCE: Desouza C et al. AACE 2018, Abstract 298
BOSTON – studied in a series of clinical trials; the efficacy did not come at the cost of frequent hypoglycemia or other serious adverse events, according to a pooled subgroup analysis of the SUSTAIN trials.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The trials investigated the safety and efficacy of semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, in the treatment of T2DM. Cyrus V. Desouza, MBBS, presented results of a post hoc analysis of racial and ethnic subgroups, drawing on SUSTAIN trials 1-5 and 7 (SUSTAIN 6 had a different design, focusing on cardiovascular outcomes).
“The trials incorporated patients on the whole spectrum of diabetes, starting from people who are newly diagnosed ... all the way to patients who were on a combination of oral antidiabetic drugs plus insulin,” Dr. Desouza explained in an interview at the annual scientific & clinical congress of the American Association of Clinical Endocrinologists.
The mean time since diagnosis in the SUSTAIN trials varied from 4.2 years in SUSTAIN 1 to 13.3 years in SUSTAIN 5. Dr. Desouza and his colleagues pooled data from the six trials to conduct the subgroup analyses.
Patients in the intervention arms of all trials received once weekly subcutaneous semaglutide, at a dose of either 0.5 mg or 1.0 mg, according to Dr. Desouza, professor of diabetes, endocrinology, and metabolism and Schultz Professor of Diabetes Research, Diabetes, Endocrinology, and Metabolism at the University of Nebraska, Lincoln.
In all, data from 3,066 patients were available. In the racial analysis, 982 low- and 1,328 high-dose semaglutide recipients were white, 243 and 232 were Asian, 82 and 124 were African American, and 25 and 50 identified as “other,” respectively.
An analysis by ethnicity found that 208 low- and 324 high-dose recipients were Hispanic.
At baseline in all trials, mean hemoglobin A1c levels were similar, ranging from 8% to 8.4%; weights at baseline were a mean 89.6 kg to 96.2 kg across the trials.
The range of reductions in HbA1c was similar across racial and ethnic groups. “If you look at the proportion of patients who actually achieved an A1c below 7[%], it’s pretty impressive – it’s between 70% to 80%.” Between 50% and 60% of patients reached an HbA1c less than 6.5%, said Dr. Desouza.
Looking at the data another way, 62.2%-72.4% of patients saw an HbA1c reduction of at least 1% on low-dose semaglutide; the range across ethnicities was 74.2%-87.1% on high-dose semaglutide. Dr. Desouza said that the sample sizes weren’t large enough to calculate statistical significance for these subgroup differences.
“But I think what is impressive is that over 50% of patients in all the races and ethnicities were able to achieve a 5% body weight loss, which is metabolically significant in terms of improving outcomes,” he said. “I think that’s a really important fact.” A smaller proportion – around 20% – lost at least 10% of body weight, mostly on high-dose semaglutide.
Severe hypoglycemia, as defined by American Diabetes Association classification, was very rare across trials, except that 4.7% of African Americans saw this adverse event on high-dose semaglutide. Incidence in other subgroups, at either dose, ranged from 0% to 2.4%.
Otherwise, the medication was generally well tolerated, though gastrointestinal side effects were seen. “Asian people have a little higher GI side effects – up to 50% of Asians did develop GI side effects, and between 10% and 13% of Asians had to stop medication due to side effects,” said Dr. Desouza. “So I think that would be the one caveat in terms of tolerance that we did learn.”
The SUSTAIN trials were sponsored by Novo Nordisk. Dr. Desouza has received consulting fees for Novo Nordisk and has received grant support from several other pharmaceutical companies. Two coauthors are Novo Nordisk employees.
SOURCE: Desouza C et al. AACE 2018, Abstract 298
BOSTON – studied in a series of clinical trials; the efficacy did not come at the cost of frequent hypoglycemia or other serious adverse events, according to a pooled subgroup analysis of the SUSTAIN trials.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The trials investigated the safety and efficacy of semaglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, in the treatment of T2DM. Cyrus V. Desouza, MBBS, presented results of a post hoc analysis of racial and ethnic subgroups, drawing on SUSTAIN trials 1-5 and 7 (SUSTAIN 6 had a different design, focusing on cardiovascular outcomes).
“The trials incorporated patients on the whole spectrum of diabetes, starting from people who are newly diagnosed ... all the way to patients who were on a combination of oral antidiabetic drugs plus insulin,” Dr. Desouza explained in an interview at the annual scientific & clinical congress of the American Association of Clinical Endocrinologists.
The mean time since diagnosis in the SUSTAIN trials varied from 4.2 years in SUSTAIN 1 to 13.3 years in SUSTAIN 5. Dr. Desouza and his colleagues pooled data from the six trials to conduct the subgroup analyses.
Patients in the intervention arms of all trials received once weekly subcutaneous semaglutide, at a dose of either 0.5 mg or 1.0 mg, according to Dr. Desouza, professor of diabetes, endocrinology, and metabolism and Schultz Professor of Diabetes Research, Diabetes, Endocrinology, and Metabolism at the University of Nebraska, Lincoln.
In all, data from 3,066 patients were available. In the racial analysis, 982 low- and 1,328 high-dose semaglutide recipients were white, 243 and 232 were Asian, 82 and 124 were African American, and 25 and 50 identified as “other,” respectively.
An analysis by ethnicity found that 208 low- and 324 high-dose recipients were Hispanic.
At baseline in all trials, mean hemoglobin A1c levels were similar, ranging from 8% to 8.4%; weights at baseline were a mean 89.6 kg to 96.2 kg across the trials.
The range of reductions in HbA1c was similar across racial and ethnic groups. “If you look at the proportion of patients who actually achieved an A1c below 7[%], it’s pretty impressive – it’s between 70% to 80%.” Between 50% and 60% of patients reached an HbA1c less than 6.5%, said Dr. Desouza.
Looking at the data another way, 62.2%-72.4% of patients saw an HbA1c reduction of at least 1% on low-dose semaglutide; the range across ethnicities was 74.2%-87.1% on high-dose semaglutide. Dr. Desouza said that the sample sizes weren’t large enough to calculate statistical significance for these subgroup differences.
“But I think what is impressive is that over 50% of patients in all the races and ethnicities were able to achieve a 5% body weight loss, which is metabolically significant in terms of improving outcomes,” he said. “I think that’s a really important fact.” A smaller proportion – around 20% – lost at least 10% of body weight, mostly on high-dose semaglutide.
Severe hypoglycemia, as defined by American Diabetes Association classification, was very rare across trials, except that 4.7% of African Americans saw this adverse event on high-dose semaglutide. Incidence in other subgroups, at either dose, ranged from 0% to 2.4%.
Otherwise, the medication was generally well tolerated, though gastrointestinal side effects were seen. “Asian people have a little higher GI side effects – up to 50% of Asians did develop GI side effects, and between 10% and 13% of Asians had to stop medication due to side effects,” said Dr. Desouza. “So I think that would be the one caveat in terms of tolerance that we did learn.”
The SUSTAIN trials were sponsored by Novo Nordisk. Dr. Desouza has received consulting fees for Novo Nordisk and has received grant support from several other pharmaceutical companies. Two coauthors are Novo Nordisk employees.
SOURCE: Desouza C et al. AACE 2018, Abstract 298
REPORTING FROM AACE 2018
Endocrinologists well positioned to be experts on changes in transgender care
according to Joshua D. Safer, MD, executive director of the Mount Sinai Center for Transgender Medicine and Surgery, New York.
“It’s not that we have to be the experts on making diagnoses or other elements of transgender care, necessarily,” Dr. Safer said in an interview here at the annual scientific & clinical congress of the American Association of Clinical Endocrinologists.
In a meet-the-expert session at AACE, Dr. Safer talked about the “change in landscape” in transgender medical care that precipitated the Endocrine Society clinical practice guideline on endocrine treatment of gender-dysphoric/gender-incongruent individuals.
The new guidelines, published just this past fall, updated guidance published by the society back in 2009.
One big change for pediatrics in the new guidelines is the recognition that there may be “compelling reasons” to start cross-sex hormonal therapy prior to 16 years, the former age cut-off. Sixteen years is “very late if you’re thinking about it from a biological perspective,” said Dr. Safer, who was a coauthor of the new guidelines.
While there are only limited data on using gender-affirming hormones in younger adolescents, there are potential risks of waiting until age 16 years in some cases, according to the guidelines.
For example, an individual who reaches Tanner stage 2 at age 9-10 years might be at risk of bone health issues if puberty is suppressed for 6-7 years before initiating sex hormones. Other risks could include inappropriate height or emotional/social isolation if the adolescent has to wait until age 16 years for initiation of secondary sex characteristics. On the adult side, one of the biggest changes is removing the idea that a mental health professional is necessary to make the diagnosis. In truth, any knowledgeable clinician could make that diagnosis, according to Dr. Safer.
A transgender individual’s treatment team should include several providers, according to guidelines: a medical provider who is knowledgeable in transgender hormone therapy, a mental health provider who is knowledgeable in gender dysphoria/gender incongruence and transition-associated mental health concerns, plus a primary care provider who can provide care appropriate to transgender needs.
Nonbinary persons (that is, those not exclusively identifying as either male or female) might need some “special tailoring” of treatment within accepted safety guidelines, Dr. Safer noted. Endocrinologists should provide education regarding onset and time course of physical changes induced by sex hormones for transgender individuals undergoing treatment, the guidelines also recommend.
It’s very important for endocrinologists to be familiar with why the landscape has changed for transgender health care, Dr. Safer said at the meeting.
“It’s not that we’ve all decided to be more tolerant or something along those lines,” he said in the interview. “It’s that even those of us who have been very skeptical in the medical and scientific community have recognized that there is clearly a biological component to gender identity.”
according to Joshua D. Safer, MD, executive director of the Mount Sinai Center for Transgender Medicine and Surgery, New York.
“It’s not that we have to be the experts on making diagnoses or other elements of transgender care, necessarily,” Dr. Safer said in an interview here at the annual scientific & clinical congress of the American Association of Clinical Endocrinologists.
In a meet-the-expert session at AACE, Dr. Safer talked about the “change in landscape” in transgender medical care that precipitated the Endocrine Society clinical practice guideline on endocrine treatment of gender-dysphoric/gender-incongruent individuals.
The new guidelines, published just this past fall, updated guidance published by the society back in 2009.
One big change for pediatrics in the new guidelines is the recognition that there may be “compelling reasons” to start cross-sex hormonal therapy prior to 16 years, the former age cut-off. Sixteen years is “very late if you’re thinking about it from a biological perspective,” said Dr. Safer, who was a coauthor of the new guidelines.
While there are only limited data on using gender-affirming hormones in younger adolescents, there are potential risks of waiting until age 16 years in some cases, according to the guidelines.
For example, an individual who reaches Tanner stage 2 at age 9-10 years might be at risk of bone health issues if puberty is suppressed for 6-7 years before initiating sex hormones. Other risks could include inappropriate height or emotional/social isolation if the adolescent has to wait until age 16 years for initiation of secondary sex characteristics. On the adult side, one of the biggest changes is removing the idea that a mental health professional is necessary to make the diagnosis. In truth, any knowledgeable clinician could make that diagnosis, according to Dr. Safer.
A transgender individual’s treatment team should include several providers, according to guidelines: a medical provider who is knowledgeable in transgender hormone therapy, a mental health provider who is knowledgeable in gender dysphoria/gender incongruence and transition-associated mental health concerns, plus a primary care provider who can provide care appropriate to transgender needs.
Nonbinary persons (that is, those not exclusively identifying as either male or female) might need some “special tailoring” of treatment within accepted safety guidelines, Dr. Safer noted. Endocrinologists should provide education regarding onset and time course of physical changes induced by sex hormones for transgender individuals undergoing treatment, the guidelines also recommend.
It’s very important for endocrinologists to be familiar with why the landscape has changed for transgender health care, Dr. Safer said at the meeting.
“It’s not that we’ve all decided to be more tolerant or something along those lines,” he said in the interview. “It’s that even those of us who have been very skeptical in the medical and scientific community have recognized that there is clearly a biological component to gender identity.”
according to Joshua D. Safer, MD, executive director of the Mount Sinai Center for Transgender Medicine and Surgery, New York.
“It’s not that we have to be the experts on making diagnoses or other elements of transgender care, necessarily,” Dr. Safer said in an interview here at the annual scientific & clinical congress of the American Association of Clinical Endocrinologists.
In a meet-the-expert session at AACE, Dr. Safer talked about the “change in landscape” in transgender medical care that precipitated the Endocrine Society clinical practice guideline on endocrine treatment of gender-dysphoric/gender-incongruent individuals.
The new guidelines, published just this past fall, updated guidance published by the society back in 2009.
One big change for pediatrics in the new guidelines is the recognition that there may be “compelling reasons” to start cross-sex hormonal therapy prior to 16 years, the former age cut-off. Sixteen years is “very late if you’re thinking about it from a biological perspective,” said Dr. Safer, who was a coauthor of the new guidelines.
While there are only limited data on using gender-affirming hormones in younger adolescents, there are potential risks of waiting until age 16 years in some cases, according to the guidelines.
For example, an individual who reaches Tanner stage 2 at age 9-10 years might be at risk of bone health issues if puberty is suppressed for 6-7 years before initiating sex hormones. Other risks could include inappropriate height or emotional/social isolation if the adolescent has to wait until age 16 years for initiation of secondary sex characteristics. On the adult side, one of the biggest changes is removing the idea that a mental health professional is necessary to make the diagnosis. In truth, any knowledgeable clinician could make that diagnosis, according to Dr. Safer.
A transgender individual’s treatment team should include several providers, according to guidelines: a medical provider who is knowledgeable in transgender hormone therapy, a mental health provider who is knowledgeable in gender dysphoria/gender incongruence and transition-associated mental health concerns, plus a primary care provider who can provide care appropriate to transgender needs.
Nonbinary persons (that is, those not exclusively identifying as either male or female) might need some “special tailoring” of treatment within accepted safety guidelines, Dr. Safer noted. Endocrinologists should provide education regarding onset and time course of physical changes induced by sex hormones for transgender individuals undergoing treatment, the guidelines also recommend.
It’s very important for endocrinologists to be familiar with why the landscape has changed for transgender health care, Dr. Safer said at the meeting.
“It’s not that we’ve all decided to be more tolerant or something along those lines,” he said in the interview. “It’s that even those of us who have been very skeptical in the medical and scientific community have recognized that there is clearly a biological component to gender identity.”
REPORTING FROM AACE 2018
Genes, not adiposity, may be driving appetite differences in obesity
BOSTON – Evidence from a twin study points to genes, rather than just adiposity, as the underlying factor in differences in appetite and satiety that have been observed in obesity.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The work adds a new dimension – and some questions – to previous research, which suggested individuals with obesity show heightened brain activation to food cues, especially calorically dense food.
“We thought it was fat mass…but when we controlled for everything that monozygotic pairs have in common, that relationship went away, implicating something that the monozygotic twins have in common, i.e., genetics,” said first author Jennifer Rosenbaum, MD, in a video interview at the annual meeting of the American Academy of Clinical Endocrinologists.
Dr. Rosenbaum, a fellow in the department of metabolism, endocrinology, and nutrition at the University of Washington, Seattle, and her collaborators made use of a statewide twin registry to conduct an extensive investigation of subjective and objective measures of appetite and satiety in the 42 twin pairs.
Twins had a mean age of 31 years; 27 of the twin pairs were monozygotic, Dr. Rosenbaum said. At least one member of each twin pair met criteria for obesity, and participants had a mean body mass index of 32.8 kg/m2.
On the study day, participants arrived in fasting state, and had a fixed-calorie breakfast equivalent to 10% of their daily caloric needs. They then underwent dual-energy x-ray absorptiometry scanning to determine adiposity, and also filled out a behavioral questionnaire.
Then, participants received the first of two functional MRI scans; during the scan, they were shown images of high calorie foods, low calorie foods, and nonfood objects, completing ratings of how appealing they found each image. After consuming another standardized meal equivalent to 20% of daily caloric needs, the fMRI scan was repeated.
Finally, participants were given access to a buffet meal and allowed to eat as much as they chose; consumption was measured. Before and after each meal and scan, and at various points during the day, the investigators also obtained blood samples and asked participants to rate their hunger on a visual analog scale.
“When compared with how much fat mass they had, there was no relationship between how hungry or full they were when they were fasting, how hungry or full they were with a snack, or when they ate the buffet. It just didn’t matter how much fat mass they had” for subjective reporting of hunger and fullness, said Dr. Rosenbaum.
However, there was a direct correlation between fat mass and amount consumed at the ad libitum buffet. Additionally, the fMRI analysis showed that “the brain activation that we would expect to go down, didn’t seem to go down as much if you had more adiposity,” she said.
As fat mass went up, areas of the brain implicated in appetite and reward showed more activity when participants were presented with the tempting images of high calorie foods, regardless of the calories consumed. These areas include the ventral and dorsal striata, the amygdala, the insula, the ventral tegmental area, and the medial orbitofrontal cortex.
Next, the researchers looked for differences within the monozygotic twin pairs, who essentially share a genome. They compared the brain activation of the twin with the higher fat mass with that of the twin with lower fat mass. Instead of seeing the same correlation between higher adiposity and greater brain activation with tempting stimuli, “Suddenly, we lost that relationship between how many calories they would eat and how their brain activated with the food,” said Dr. Rosenbaum. This is a clue, she said, that genetics, rather than simple adiposity, is driving the different responses to food cues.
The study was funded by the National Institutes of Health. Dr. Rosenbaum reported no financial disclosures.
BOSTON – Evidence from a twin study points to genes, rather than just adiposity, as the underlying factor in differences in appetite and satiety that have been observed in obesity.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The work adds a new dimension – and some questions – to previous research, which suggested individuals with obesity show heightened brain activation to food cues, especially calorically dense food.
“We thought it was fat mass…but when we controlled for everything that monozygotic pairs have in common, that relationship went away, implicating something that the monozygotic twins have in common, i.e., genetics,” said first author Jennifer Rosenbaum, MD, in a video interview at the annual meeting of the American Academy of Clinical Endocrinologists.
Dr. Rosenbaum, a fellow in the department of metabolism, endocrinology, and nutrition at the University of Washington, Seattle, and her collaborators made use of a statewide twin registry to conduct an extensive investigation of subjective and objective measures of appetite and satiety in the 42 twin pairs.
Twins had a mean age of 31 years; 27 of the twin pairs were monozygotic, Dr. Rosenbaum said. At least one member of each twin pair met criteria for obesity, and participants had a mean body mass index of 32.8 kg/m2.
On the study day, participants arrived in fasting state, and had a fixed-calorie breakfast equivalent to 10% of their daily caloric needs. They then underwent dual-energy x-ray absorptiometry scanning to determine adiposity, and also filled out a behavioral questionnaire.
Then, participants received the first of two functional MRI scans; during the scan, they were shown images of high calorie foods, low calorie foods, and nonfood objects, completing ratings of how appealing they found each image. After consuming another standardized meal equivalent to 20% of daily caloric needs, the fMRI scan was repeated.
Finally, participants were given access to a buffet meal and allowed to eat as much as they chose; consumption was measured. Before and after each meal and scan, and at various points during the day, the investigators also obtained blood samples and asked participants to rate their hunger on a visual analog scale.
“When compared with how much fat mass they had, there was no relationship between how hungry or full they were when they were fasting, how hungry or full they were with a snack, or when they ate the buffet. It just didn’t matter how much fat mass they had” for subjective reporting of hunger and fullness, said Dr. Rosenbaum.
However, there was a direct correlation between fat mass and amount consumed at the ad libitum buffet. Additionally, the fMRI analysis showed that “the brain activation that we would expect to go down, didn’t seem to go down as much if you had more adiposity,” she said.
As fat mass went up, areas of the brain implicated in appetite and reward showed more activity when participants were presented with the tempting images of high calorie foods, regardless of the calories consumed. These areas include the ventral and dorsal striata, the amygdala, the insula, the ventral tegmental area, and the medial orbitofrontal cortex.
Next, the researchers looked for differences within the monozygotic twin pairs, who essentially share a genome. They compared the brain activation of the twin with the higher fat mass with that of the twin with lower fat mass. Instead of seeing the same correlation between higher adiposity and greater brain activation with tempting stimuli, “Suddenly, we lost that relationship between how many calories they would eat and how their brain activated with the food,” said Dr. Rosenbaum. This is a clue, she said, that genetics, rather than simple adiposity, is driving the different responses to food cues.
The study was funded by the National Institutes of Health. Dr. Rosenbaum reported no financial disclosures.
BOSTON – Evidence from a twin study points to genes, rather than just adiposity, as the underlying factor in differences in appetite and satiety that have been observed in obesity.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The work adds a new dimension – and some questions – to previous research, which suggested individuals with obesity show heightened brain activation to food cues, especially calorically dense food.
“We thought it was fat mass…but when we controlled for everything that monozygotic pairs have in common, that relationship went away, implicating something that the monozygotic twins have in common, i.e., genetics,” said first author Jennifer Rosenbaum, MD, in a video interview at the annual meeting of the American Academy of Clinical Endocrinologists.
Dr. Rosenbaum, a fellow in the department of metabolism, endocrinology, and nutrition at the University of Washington, Seattle, and her collaborators made use of a statewide twin registry to conduct an extensive investigation of subjective and objective measures of appetite and satiety in the 42 twin pairs.
Twins had a mean age of 31 years; 27 of the twin pairs were monozygotic, Dr. Rosenbaum said. At least one member of each twin pair met criteria for obesity, and participants had a mean body mass index of 32.8 kg/m2.
On the study day, participants arrived in fasting state, and had a fixed-calorie breakfast equivalent to 10% of their daily caloric needs. They then underwent dual-energy x-ray absorptiometry scanning to determine adiposity, and also filled out a behavioral questionnaire.
Then, participants received the first of two functional MRI scans; during the scan, they were shown images of high calorie foods, low calorie foods, and nonfood objects, completing ratings of how appealing they found each image. After consuming another standardized meal equivalent to 20% of daily caloric needs, the fMRI scan was repeated.
Finally, participants were given access to a buffet meal and allowed to eat as much as they chose; consumption was measured. Before and after each meal and scan, and at various points during the day, the investigators also obtained blood samples and asked participants to rate their hunger on a visual analog scale.
“When compared with how much fat mass they had, there was no relationship between how hungry or full they were when they were fasting, how hungry or full they were with a snack, or when they ate the buffet. It just didn’t matter how much fat mass they had” for subjective reporting of hunger and fullness, said Dr. Rosenbaum.
However, there was a direct correlation between fat mass and amount consumed at the ad libitum buffet. Additionally, the fMRI analysis showed that “the brain activation that we would expect to go down, didn’t seem to go down as much if you had more adiposity,” she said.
As fat mass went up, areas of the brain implicated in appetite and reward showed more activity when participants were presented with the tempting images of high calorie foods, regardless of the calories consumed. These areas include the ventral and dorsal striata, the amygdala, the insula, the ventral tegmental area, and the medial orbitofrontal cortex.
Next, the researchers looked for differences within the monozygotic twin pairs, who essentially share a genome. They compared the brain activation of the twin with the higher fat mass with that of the twin with lower fat mass. Instead of seeing the same correlation between higher adiposity and greater brain activation with tempting stimuli, “Suddenly, we lost that relationship between how many calories they would eat and how their brain activated with the food,” said Dr. Rosenbaum. This is a clue, she said, that genetics, rather than simple adiposity, is driving the different responses to food cues.
The study was funded by the National Institutes of Health. Dr. Rosenbaum reported no financial disclosures.
REPORTING FROM AACE 2018
SUSTAIN-7: GLP-1 receptor agonists effective in elderly
BOSTON – Efficacy and safety of two glucagonlike peptide 1 (GLP-1) receptor agonists in type 2 diabetes mellitus were similar between older and younger adults, according to a post hoc analysis of the SUSTAIN 7 clinical trial data.
However, said the study’s first author, Vanita Aroda, MD, associate director for clinical diabetes research at Brigham and Women’s Hospital, Boston.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The SUSTAIN 7 trial compared low-dose semaglutide (0.5 mg) with low-dose dulaglutide (0.75 mg), and high-dose semaglutide (1.0 mg) with high-dose dulaglutide (1.5 mg) as add-on therapy to metformin for adults with type 2 diabetes. All medications were given as once-weekly subcutaneous injections.
Dr. Aroda and her collaborators performed a subgroup analysis of the SUSTAIN 7 data that compared 260 patients aged 65 years and older (mean, 69.3 years) with 939 patients younger than 65 years (mean, 51.9 years).
“What we found is that the efficacy results … were similar to what we saw in the general population. We did not lose the efficacy in the older adult population,” said Dr. Aroda in an interview at the annual meeting of the American Association for Clinical Endocrinology.
Weight loss was similar in older and younger patients, though there was “maybe a tiny bit more in the older adults,” said Dr. Aroda: Older participants had a 4.4-kg reduction in weight, compared with 4.9-kg reduction in the younger population, on low-dose semaglutide. For low-dose dulaglutide, losses were an average 2.6 kg in the elderly versus 2.2 kg in the younger participants.
The higher doses of each resulted in greater weight loss, up to a mean 6.7 kg in elderly participants on high-dose semaglutide, with the same marginally greater losses seen in older participants.
Both agents were efficacious in the older population, Dr. Aroda said, with slightly better efficacy than in younger patients. As a caveat, she noted that the older patients came into the study with slightly better glycemic control and slightly lower body weight.
An array of endpoints for the 40-week study included achieving hemoglobin A1c less than 7%, less than or equal to 6.5%, and less than 7% without weight gain or hypoglycemia. A higher proportion of elderly patients met these endpoints; for example, 83% of elderly patients on high-dose semaglutide reached the composite endpoint of HbA1c less than 7% with no weight gain or hypoglycemia, compared to 72.1% of younger participants.
The analysis also looked at safety data for SUSTAIN 7. “The next question is, are you seeing this efficacy in terms of glycemic change and weight loss, at any cost of hypoglycemia? And the answer to that was no,” said Dr. Aroda. There were very rare to zero hypoglycemic events in the various study arms, she said.
However, older adults taking the higher doses of both GLP-1 receptor agonists had a high incidence of nausea, vomiting, and other gastrointestinal disturbances. These adverse events were seen in 52.8% of older patients on high-dose semaglutide and 52.2% of those on high-dose dulaglutide. Rates for the younger study population at these doses were 42.5% for semaglutide and 46.6% for dulaglutide.
The clinical take-home message? Don’t be afraid to reach for a GLP-1 receptor agonist for an older patient who’s not reaching target on metformin. “You have good efficacy with both of the therapies … but you just need to watch out for tolerability at the higher doses,” said Dr. Aroda.
Dr. Aroda reported receiving research funding from AstraZeneca, Calibri, Eisai, Novo Nordisk, Sanofi, and Theracos. She was formerly affiliated with Medstar Health Research Institute, Hyattsville, Md.
SOURCE: Aroda V et al. AACE 2018. Abstract 245.
BOSTON – Efficacy and safety of two glucagonlike peptide 1 (GLP-1) receptor agonists in type 2 diabetes mellitus were similar between older and younger adults, according to a post hoc analysis of the SUSTAIN 7 clinical trial data.
However, said the study’s first author, Vanita Aroda, MD, associate director for clinical diabetes research at Brigham and Women’s Hospital, Boston.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The SUSTAIN 7 trial compared low-dose semaglutide (0.5 mg) with low-dose dulaglutide (0.75 mg), and high-dose semaglutide (1.0 mg) with high-dose dulaglutide (1.5 mg) as add-on therapy to metformin for adults with type 2 diabetes. All medications were given as once-weekly subcutaneous injections.
Dr. Aroda and her collaborators performed a subgroup analysis of the SUSTAIN 7 data that compared 260 patients aged 65 years and older (mean, 69.3 years) with 939 patients younger than 65 years (mean, 51.9 years).
“What we found is that the efficacy results … were similar to what we saw in the general population. We did not lose the efficacy in the older adult population,” said Dr. Aroda in an interview at the annual meeting of the American Association for Clinical Endocrinology.
Weight loss was similar in older and younger patients, though there was “maybe a tiny bit more in the older adults,” said Dr. Aroda: Older participants had a 4.4-kg reduction in weight, compared with 4.9-kg reduction in the younger population, on low-dose semaglutide. For low-dose dulaglutide, losses were an average 2.6 kg in the elderly versus 2.2 kg in the younger participants.
The higher doses of each resulted in greater weight loss, up to a mean 6.7 kg in elderly participants on high-dose semaglutide, with the same marginally greater losses seen in older participants.
Both agents were efficacious in the older population, Dr. Aroda said, with slightly better efficacy than in younger patients. As a caveat, she noted that the older patients came into the study with slightly better glycemic control and slightly lower body weight.
An array of endpoints for the 40-week study included achieving hemoglobin A1c less than 7%, less than or equal to 6.5%, and less than 7% without weight gain or hypoglycemia. A higher proportion of elderly patients met these endpoints; for example, 83% of elderly patients on high-dose semaglutide reached the composite endpoint of HbA1c less than 7% with no weight gain or hypoglycemia, compared to 72.1% of younger participants.
The analysis also looked at safety data for SUSTAIN 7. “The next question is, are you seeing this efficacy in terms of glycemic change and weight loss, at any cost of hypoglycemia? And the answer to that was no,” said Dr. Aroda. There were very rare to zero hypoglycemic events in the various study arms, she said.
However, older adults taking the higher doses of both GLP-1 receptor agonists had a high incidence of nausea, vomiting, and other gastrointestinal disturbances. These adverse events were seen in 52.8% of older patients on high-dose semaglutide and 52.2% of those on high-dose dulaglutide. Rates for the younger study population at these doses were 42.5% for semaglutide and 46.6% for dulaglutide.
The clinical take-home message? Don’t be afraid to reach for a GLP-1 receptor agonist for an older patient who’s not reaching target on metformin. “You have good efficacy with both of the therapies … but you just need to watch out for tolerability at the higher doses,” said Dr. Aroda.
Dr. Aroda reported receiving research funding from AstraZeneca, Calibri, Eisai, Novo Nordisk, Sanofi, and Theracos. She was formerly affiliated with Medstar Health Research Institute, Hyattsville, Md.
SOURCE: Aroda V et al. AACE 2018. Abstract 245.
BOSTON – Efficacy and safety of two glucagonlike peptide 1 (GLP-1) receptor agonists in type 2 diabetes mellitus were similar between older and younger adults, according to a post hoc analysis of the SUSTAIN 7 clinical trial data.
However, said the study’s first author, Vanita Aroda, MD, associate director for clinical diabetes research at Brigham and Women’s Hospital, Boston.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The SUSTAIN 7 trial compared low-dose semaglutide (0.5 mg) with low-dose dulaglutide (0.75 mg), and high-dose semaglutide (1.0 mg) with high-dose dulaglutide (1.5 mg) as add-on therapy to metformin for adults with type 2 diabetes. All medications were given as once-weekly subcutaneous injections.
Dr. Aroda and her collaborators performed a subgroup analysis of the SUSTAIN 7 data that compared 260 patients aged 65 years and older (mean, 69.3 years) with 939 patients younger than 65 years (mean, 51.9 years).
“What we found is that the efficacy results … were similar to what we saw in the general population. We did not lose the efficacy in the older adult population,” said Dr. Aroda in an interview at the annual meeting of the American Association for Clinical Endocrinology.
Weight loss was similar in older and younger patients, though there was “maybe a tiny bit more in the older adults,” said Dr. Aroda: Older participants had a 4.4-kg reduction in weight, compared with 4.9-kg reduction in the younger population, on low-dose semaglutide. For low-dose dulaglutide, losses were an average 2.6 kg in the elderly versus 2.2 kg in the younger participants.
The higher doses of each resulted in greater weight loss, up to a mean 6.7 kg in elderly participants on high-dose semaglutide, with the same marginally greater losses seen in older participants.
Both agents were efficacious in the older population, Dr. Aroda said, with slightly better efficacy than in younger patients. As a caveat, she noted that the older patients came into the study with slightly better glycemic control and slightly lower body weight.
An array of endpoints for the 40-week study included achieving hemoglobin A1c less than 7%, less than or equal to 6.5%, and less than 7% without weight gain or hypoglycemia. A higher proportion of elderly patients met these endpoints; for example, 83% of elderly patients on high-dose semaglutide reached the composite endpoint of HbA1c less than 7% with no weight gain or hypoglycemia, compared to 72.1% of younger participants.
The analysis also looked at safety data for SUSTAIN 7. “The next question is, are you seeing this efficacy in terms of glycemic change and weight loss, at any cost of hypoglycemia? And the answer to that was no,” said Dr. Aroda. There were very rare to zero hypoglycemic events in the various study arms, she said.
However, older adults taking the higher doses of both GLP-1 receptor agonists had a high incidence of nausea, vomiting, and other gastrointestinal disturbances. These adverse events were seen in 52.8% of older patients on high-dose semaglutide and 52.2% of those on high-dose dulaglutide. Rates for the younger study population at these doses were 42.5% for semaglutide and 46.6% for dulaglutide.
The clinical take-home message? Don’t be afraid to reach for a GLP-1 receptor agonist for an older patient who’s not reaching target on metformin. “You have good efficacy with both of the therapies … but you just need to watch out for tolerability at the higher doses,” said Dr. Aroda.
Dr. Aroda reported receiving research funding from AstraZeneca, Calibri, Eisai, Novo Nordisk, Sanofi, and Theracos. She was formerly affiliated with Medstar Health Research Institute, Hyattsville, Md.
SOURCE: Aroda V et al. AACE 2018. Abstract 245.
REPORTING FROM AACE 2018
VIDEO: Health advisers boost type 2 diabetes adherence
BOSTON – A company that partners patients and health advisers claims to help patients with type 2 diabetes to manage their symptoms and lower their HbA1c levels.
The Pack Health program connects each patient with a health adviser, who contacts them five times a week using a mix of phone calls, text messages, and emails. The goals include helping patients to find clinicians in their area, make appointments, and adhere to treatment, Dhiren Patel, PharmD, medical director at Pack Health, said at the annual meeting of the American Association of Clinical Endocrinologists.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Patients lost an average of 5 pounds, and annual eye and foot exams increased by 17% and 19%, respectively.
Similar remote health coach initiatives are being used to help other patients with chronic health conditions as part of the Pack Health services, which Dr. Patel discussed in a video interview.
SOURCE: Patel D et al. AACE 2018. Abstract 1209.
BOSTON – A company that partners patients and health advisers claims to help patients with type 2 diabetes to manage their symptoms and lower their HbA1c levels.
The Pack Health program connects each patient with a health adviser, who contacts them five times a week using a mix of phone calls, text messages, and emails. The goals include helping patients to find clinicians in their area, make appointments, and adhere to treatment, Dhiren Patel, PharmD, medical director at Pack Health, said at the annual meeting of the American Association of Clinical Endocrinologists.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Patients lost an average of 5 pounds, and annual eye and foot exams increased by 17% and 19%, respectively.
Similar remote health coach initiatives are being used to help other patients with chronic health conditions as part of the Pack Health services, which Dr. Patel discussed in a video interview.
SOURCE: Patel D et al. AACE 2018. Abstract 1209.
BOSTON – A company that partners patients and health advisers claims to help patients with type 2 diabetes to manage their symptoms and lower their HbA1c levels.
The Pack Health program connects each patient with a health adviser, who contacts them five times a week using a mix of phone calls, text messages, and emails. The goals include helping patients to find clinicians in their area, make appointments, and adhere to treatment, Dhiren Patel, PharmD, medical director at Pack Health, said at the annual meeting of the American Association of Clinical Endocrinologists.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Patients lost an average of 5 pounds, and annual eye and foot exams increased by 17% and 19%, respectively.
Similar remote health coach initiatives are being used to help other patients with chronic health conditions as part of the Pack Health services, which Dr. Patel discussed in a video interview.
SOURCE: Patel D et al. AACE 2018. Abstract 1209.
REPORTING FROM AACE 2018
Canagliflozin linked to lower HbA1c levels in younger patients
BOSTON – The effects of canagliflozin on hemoglobin A1c levels were greater in participants under age 65 years in randomized clinical trials of the SGLT2 inhibitor, according to results of a prespecified subgroup analysis.
Some cardiovascular, renal, and mortality outcomes also varied by age group, according to the analysis of participants in the CANVAS (Canagliflozin Cardiovascular Assessment Study) program. Despite those differences, the effect of canagliflozin was generally consistent on other outcomes, such as body weight and blood pressure, in patient grouped into those aged less than 65 years and those aged 65 years and older, investigators reported at the annual meeting of the American Association of Clinical Endocrinologists.
Nonfatal MI, nonfatal stroke, and the composite of doubling of serum creatine, end-stage renal disease, or renal death were lower in study participants aged 65 and older on canagliflozin. Lower risks of cardiovascular death and all-cause mortality were seen in participants under age 65 years who were taking canagliflozin. However, “these results should be interpreted with caution given the large number of subgroup analyses performed,” wrote Fernando Ovalle, MD, director of the multidisciplinary comprehensive diabetes clinic at the University of Alabama at Birmingham, and his colleagues.
Canagliflozin was found to reduce risk of the composite endpoint of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke versus placebo in previously published results of the CANVAS study, which included individuals with type 2 diabetes mellitus who either had or were at high risk for having cardiovascular disease.
The two multicenter, randomized, controlled trials, CANVAS and CANVAS-R, included more than 10,000 patients. The subgroup analysis presented here at the AACE meeting included 5,578 patients aged less than 65 years (55%) and 4,564 patients aged 65 years or older (45%).
The subgroup analysis found that placebo-subtracted differences in HbA1c were greater in patients under 65 years than those in patients 65 or older (–0.7% and –0.5%, respectively; P less than .0001). However, there were no significant differences by age group in body weight changes, systolic blood pressure, or diastolic blood pressure.
Patients aged 65 years or older at baseline had a lower risk of nonfatal MI and nonfatal stroke with canagliflozin versus placebo (P for heterogeneity, .02 and.01, respectively), according to investigators. Older patients also had lower risk of the composite of serum creatinine doubling, end-stage kidney disease, or renal death with canagliflozin versus placebo (P = .01).
Patients aged less than 65 years at baseline had lower risk of cardiovascular death (P = .01) and all cause mortality (P = .01) for canagliflozin versus placebo.
Dr. Ovalle reported disclosures related to Merck, AstraZeneca, Sanofi Pasteur, Novo Nordisk, GlaxoSmithKline, Janssen, Eli Lilly, Medtronic, Pfizer, and GI Dynamics, along with the National Institutes of Health and Juvenile Diabetes Research Foundation.
SOURCE: Ovalle F et al. AACE 2018, Abstract 233.
BOSTON – The effects of canagliflozin on hemoglobin A1c levels were greater in participants under age 65 years in randomized clinical trials of the SGLT2 inhibitor, according to results of a prespecified subgroup analysis.
Some cardiovascular, renal, and mortality outcomes also varied by age group, according to the analysis of participants in the CANVAS (Canagliflozin Cardiovascular Assessment Study) program. Despite those differences, the effect of canagliflozin was generally consistent on other outcomes, such as body weight and blood pressure, in patient grouped into those aged less than 65 years and those aged 65 years and older, investigators reported at the annual meeting of the American Association of Clinical Endocrinologists.
Nonfatal MI, nonfatal stroke, and the composite of doubling of serum creatine, end-stage renal disease, or renal death were lower in study participants aged 65 and older on canagliflozin. Lower risks of cardiovascular death and all-cause mortality were seen in participants under age 65 years who were taking canagliflozin. However, “these results should be interpreted with caution given the large number of subgroup analyses performed,” wrote Fernando Ovalle, MD, director of the multidisciplinary comprehensive diabetes clinic at the University of Alabama at Birmingham, and his colleagues.
Canagliflozin was found to reduce risk of the composite endpoint of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke versus placebo in previously published results of the CANVAS study, which included individuals with type 2 diabetes mellitus who either had or were at high risk for having cardiovascular disease.
The two multicenter, randomized, controlled trials, CANVAS and CANVAS-R, included more than 10,000 patients. The subgroup analysis presented here at the AACE meeting included 5,578 patients aged less than 65 years (55%) and 4,564 patients aged 65 years or older (45%).
The subgroup analysis found that placebo-subtracted differences in HbA1c were greater in patients under 65 years than those in patients 65 or older (–0.7% and –0.5%, respectively; P less than .0001). However, there were no significant differences by age group in body weight changes, systolic blood pressure, or diastolic blood pressure.
Patients aged 65 years or older at baseline had a lower risk of nonfatal MI and nonfatal stroke with canagliflozin versus placebo (P for heterogeneity, .02 and.01, respectively), according to investigators. Older patients also had lower risk of the composite of serum creatinine doubling, end-stage kidney disease, or renal death with canagliflozin versus placebo (P = .01).
Patients aged less than 65 years at baseline had lower risk of cardiovascular death (P = .01) and all cause mortality (P = .01) for canagliflozin versus placebo.
Dr. Ovalle reported disclosures related to Merck, AstraZeneca, Sanofi Pasteur, Novo Nordisk, GlaxoSmithKline, Janssen, Eli Lilly, Medtronic, Pfizer, and GI Dynamics, along with the National Institutes of Health and Juvenile Diabetes Research Foundation.
SOURCE: Ovalle F et al. AACE 2018, Abstract 233.
BOSTON – The effects of canagliflozin on hemoglobin A1c levels were greater in participants under age 65 years in randomized clinical trials of the SGLT2 inhibitor, according to results of a prespecified subgroup analysis.
Some cardiovascular, renal, and mortality outcomes also varied by age group, according to the analysis of participants in the CANVAS (Canagliflozin Cardiovascular Assessment Study) program. Despite those differences, the effect of canagliflozin was generally consistent on other outcomes, such as body weight and blood pressure, in patient grouped into those aged less than 65 years and those aged 65 years and older, investigators reported at the annual meeting of the American Association of Clinical Endocrinologists.
Nonfatal MI, nonfatal stroke, and the composite of doubling of serum creatine, end-stage renal disease, or renal death were lower in study participants aged 65 and older on canagliflozin. Lower risks of cardiovascular death and all-cause mortality were seen in participants under age 65 years who were taking canagliflozin. However, “these results should be interpreted with caution given the large number of subgroup analyses performed,” wrote Fernando Ovalle, MD, director of the multidisciplinary comprehensive diabetes clinic at the University of Alabama at Birmingham, and his colleagues.
Canagliflozin was found to reduce risk of the composite endpoint of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke versus placebo in previously published results of the CANVAS study, which included individuals with type 2 diabetes mellitus who either had or were at high risk for having cardiovascular disease.
The two multicenter, randomized, controlled trials, CANVAS and CANVAS-R, included more than 10,000 patients. The subgroup analysis presented here at the AACE meeting included 5,578 patients aged less than 65 years (55%) and 4,564 patients aged 65 years or older (45%).
The subgroup analysis found that placebo-subtracted differences in HbA1c were greater in patients under 65 years than those in patients 65 or older (–0.7% and –0.5%, respectively; P less than .0001). However, there were no significant differences by age group in body weight changes, systolic blood pressure, or diastolic blood pressure.
Patients aged 65 years or older at baseline had a lower risk of nonfatal MI and nonfatal stroke with canagliflozin versus placebo (P for heterogeneity, .02 and.01, respectively), according to investigators. Older patients also had lower risk of the composite of serum creatinine doubling, end-stage kidney disease, or renal death with canagliflozin versus placebo (P = .01).
Patients aged less than 65 years at baseline had lower risk of cardiovascular death (P = .01) and all cause mortality (P = .01) for canagliflozin versus placebo.
Dr. Ovalle reported disclosures related to Merck, AstraZeneca, Sanofi Pasteur, Novo Nordisk, GlaxoSmithKline, Janssen, Eli Lilly, Medtronic, Pfizer, and GI Dynamics, along with the National Institutes of Health and Juvenile Diabetes Research Foundation.
SOURCE: Ovalle F et al. AACE 2018, Abstract 233.
REPORTING FROM AACE 2018
Key clinical point: Placebo-subtracted differences in HbA1c were greater in patients under age 65 years versus patients age 65 years and older, while some cardiovascular, renal, and mortality outcomes varied by age group.
Major finding: Placebo-subtracted differences in HbA1c were greater in patients under 65 years versus patients 65 or older (-0.7% and -0.5%, respectively; P less than 0.0001).
Study details: A prespecified subset analysis of the 2 multicenter randomized controlled trials in the CANVAS Program (CANVAS and CANVAS-R studies) including more than 10,000 individuals with type 2 diabetes mellitus and either established CV disease or high risk for CV disease.
Disclosures: Dr. Ovalle reported disclosures related to Merck, AstraZeneca, Sanofi Pasteur, Novo Nordisk, GlaxoSmithKline, Janssen, Eli Lilly, Medtronic, Pfizer, and GI Dynamics, along with the National Institutes of Health and Juvenile Diabetes Research Foundation.
Source: Ovalle F, et al. AACE 2018, Abstract 233
VIDEO: Canagliflozin’s HbA1c effect muted over time by placebo group effects
BOSTON – In a large, long-term study of canagliflozin versus placebo, an excess of discontinuations in the placebo group contributed to a dampening in the magnitude of improvement in hemoglobin A1c.
That’s according to investigators who reported the findings at the annual meeting of the American Association of Clinical Endocrinologists.
A higher rate of starting new antihyperglycemic agents in the placebo arm also likely contributed to the decrease in the difference in HbA1c after 52 weeks in CANVAS (Canagliflozin Cardiovascular Assessment Study), according to investigator Carol Wysham, MD, of the University of Washington, Spokane.
As previously reported, the two randomized trials in the CANVAS program showed that canagliflozin reduced risk of cardiovascular events in patients with type 2 diabetes at elevated risk of cardiovascular disease.
While the CANVAS program was not designed to assess glucose lowering – and, in fact, allowed adjustment of background antihyperglycemic agents at any time – canagliflozin patients were more likely than placebo-treated patients to achieve HbA1c less than 7.0%.
However, the mean placebo-subtracted reduction in HbA1c peaked at –0.64% at week 26 but shrank to –0.24% by week 338, the end of the study.
“In this case, [the analysis] is helping to understand why we might have seen a deterioration in A1c control over a very long period of time,” Dr. Wysham explained.
The analysis showed that, after week 52 of the study, more patients discontinued placebo, compared with those taking canagliflozin. Over the entire CANVAS program, investigators said, the rate of discontinuation was 118.0 per 1,000 patient-years in the placebo group and 94.1 per 1,000 patient-years for canagliflozin.
In addition, while the concomitant use of antihyperglycemic agents was well balanced at baseline, the number of participants initiating new antihyperglycemic agents over the course of the study was 27% for the placebo-treated patients and 17.8% for the canagliflozin-treated patients, investigators found.
All together, the CANVAS program has provided the longest-term experience to date regarding glycemic control with canagliflozin, demonstrating greater reductions in HbA1c, versus placebo, over about 6.5 years, Dr. Wysham and her coinvestigators said in their poster presentation.
The new analysis provides better clarity on why the durability in HbA1c benefit seemed somewhat attenuated over time, according to Dr. Wysham.
“Most of us think that, if you start an SGLT2 inhibitor, especially starting it relatively early in diagnosis of diabetes, it gives you better durability than what you might see with other agents,” she said. “In fact, that’s been seen in many of the clinical trials, compared to sulphonylurea or DPP-4 inhibitor.”
Dr. Wysham reported disclosures related to AstraZeneca, Boehringer Ingelheim, Eli Lilly, Insulet, Janssen Scientific Affairs, Novo Nordisk, and Sanofi Pasteur.
SOURCE: Wysham C et al. AACE 2018, Abstract 262.
BOSTON – In a large, long-term study of canagliflozin versus placebo, an excess of discontinuations in the placebo group contributed to a dampening in the magnitude of improvement in hemoglobin A1c.
That’s according to investigators who reported the findings at the annual meeting of the American Association of Clinical Endocrinologists.
A higher rate of starting new antihyperglycemic agents in the placebo arm also likely contributed to the decrease in the difference in HbA1c after 52 weeks in CANVAS (Canagliflozin Cardiovascular Assessment Study), according to investigator Carol Wysham, MD, of the University of Washington, Spokane.
As previously reported, the two randomized trials in the CANVAS program showed that canagliflozin reduced risk of cardiovascular events in patients with type 2 diabetes at elevated risk of cardiovascular disease.
While the CANVAS program was not designed to assess glucose lowering – and, in fact, allowed adjustment of background antihyperglycemic agents at any time – canagliflozin patients were more likely than placebo-treated patients to achieve HbA1c less than 7.0%.
However, the mean placebo-subtracted reduction in HbA1c peaked at –0.64% at week 26 but shrank to –0.24% by week 338, the end of the study.
“In this case, [the analysis] is helping to understand why we might have seen a deterioration in A1c control over a very long period of time,” Dr. Wysham explained.
The analysis showed that, after week 52 of the study, more patients discontinued placebo, compared with those taking canagliflozin. Over the entire CANVAS program, investigators said, the rate of discontinuation was 118.0 per 1,000 patient-years in the placebo group and 94.1 per 1,000 patient-years for canagliflozin.
In addition, while the concomitant use of antihyperglycemic agents was well balanced at baseline, the number of participants initiating new antihyperglycemic agents over the course of the study was 27% for the placebo-treated patients and 17.8% for the canagliflozin-treated patients, investigators found.
All together, the CANVAS program has provided the longest-term experience to date regarding glycemic control with canagliflozin, demonstrating greater reductions in HbA1c, versus placebo, over about 6.5 years, Dr. Wysham and her coinvestigators said in their poster presentation.
The new analysis provides better clarity on why the durability in HbA1c benefit seemed somewhat attenuated over time, according to Dr. Wysham.
“Most of us think that, if you start an SGLT2 inhibitor, especially starting it relatively early in diagnosis of diabetes, it gives you better durability than what you might see with other agents,” she said. “In fact, that’s been seen in many of the clinical trials, compared to sulphonylurea or DPP-4 inhibitor.”
Dr. Wysham reported disclosures related to AstraZeneca, Boehringer Ingelheim, Eli Lilly, Insulet, Janssen Scientific Affairs, Novo Nordisk, and Sanofi Pasteur.
SOURCE: Wysham C et al. AACE 2018, Abstract 262.
BOSTON – In a large, long-term study of canagliflozin versus placebo, an excess of discontinuations in the placebo group contributed to a dampening in the magnitude of improvement in hemoglobin A1c.
That’s according to investigators who reported the findings at the annual meeting of the American Association of Clinical Endocrinologists.
A higher rate of starting new antihyperglycemic agents in the placebo arm also likely contributed to the decrease in the difference in HbA1c after 52 weeks in CANVAS (Canagliflozin Cardiovascular Assessment Study), according to investigator Carol Wysham, MD, of the University of Washington, Spokane.
As previously reported, the two randomized trials in the CANVAS program showed that canagliflozin reduced risk of cardiovascular events in patients with type 2 diabetes at elevated risk of cardiovascular disease.
While the CANVAS program was not designed to assess glucose lowering – and, in fact, allowed adjustment of background antihyperglycemic agents at any time – canagliflozin patients were more likely than placebo-treated patients to achieve HbA1c less than 7.0%.
However, the mean placebo-subtracted reduction in HbA1c peaked at –0.64% at week 26 but shrank to –0.24% by week 338, the end of the study.
“In this case, [the analysis] is helping to understand why we might have seen a deterioration in A1c control over a very long period of time,” Dr. Wysham explained.
The analysis showed that, after week 52 of the study, more patients discontinued placebo, compared with those taking canagliflozin. Over the entire CANVAS program, investigators said, the rate of discontinuation was 118.0 per 1,000 patient-years in the placebo group and 94.1 per 1,000 patient-years for canagliflozin.
In addition, while the concomitant use of antihyperglycemic agents was well balanced at baseline, the number of participants initiating new antihyperglycemic agents over the course of the study was 27% for the placebo-treated patients and 17.8% for the canagliflozin-treated patients, investigators found.
All together, the CANVAS program has provided the longest-term experience to date regarding glycemic control with canagliflozin, demonstrating greater reductions in HbA1c, versus placebo, over about 6.5 years, Dr. Wysham and her coinvestigators said in their poster presentation.
The new analysis provides better clarity on why the durability in HbA1c benefit seemed somewhat attenuated over time, according to Dr. Wysham.
“Most of us think that, if you start an SGLT2 inhibitor, especially starting it relatively early in diagnosis of diabetes, it gives you better durability than what you might see with other agents,” she said. “In fact, that’s been seen in many of the clinical trials, compared to sulphonylurea or DPP-4 inhibitor.”
Dr. Wysham reported disclosures related to AstraZeneca, Boehringer Ingelheim, Eli Lilly, Insulet, Janssen Scientific Affairs, Novo Nordisk, and Sanofi Pasteur.
SOURCE: Wysham C et al. AACE 2018, Abstract 262.
REPORTING FROM AACE 2018
Key clinical point: and a higher rate of starting new antihyperglycemic agents in the placebo arm.
Major finding: After week 52 of the study, more patients discontinued placebo versus canagliflozin. The number of participants initiating new antihyperglycemic agents over the course of the study was 17.8% for the canagliflozin arm and 27% for placebo.
Study details: An analysis of the effects of canagliflozin on HbA1c and changes in use of antihyperglycemic agents in the CANVAS study.
Disclosures: Dr. Wysham reported disclosures related to AstraZeneca, Boehringer Ingelheim, Eli Lilly, Insulet, Janssen Scientific Affairs, Novo Nordisk, and Sanofi Pasteur.
Source: Wysham C et al. AACE 2018, Abstract 262.
VIDEO: Acromegaly study reveals gender-specific differences
BOSTON – , according to study results presented at the annual meeting of the American Association of Clinical Endocrinologists.
The study was based on data for 112 patients (54 male, 58 female) operated on by one neurosurgeon between 1994 and 2016. The mean age at surgery was 43.6 years in men and 48.7 in women (P = .04), according to Talin Handa, Emory University, Atlanta, who presented the retrospective analysis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Men had higher mean IGF-1 levels (874 ng/mL vs. 716 ng/mL for women; P less than .01), and were more likely to have hypopituitarism.
Adjuvant treatment for acromegaly was needed in 57% of men and 49% of women. Following adjuvant treatment, 72% of men maintained surgical remission or achieved normal IGF-1 levels, compared with 89% of women (P = .03). Mean follow-up was shorter in men, 3.6 years, versus 5.2 years for women (P = .02), the researchers reported.
Six-year event-free survival was higher in women (P less than .01), according to the researchers.
For more study findings, watch our video interview.
SOURCE: Handa T et al. AACE 2018. Abstract #824.
BOSTON – , according to study results presented at the annual meeting of the American Association of Clinical Endocrinologists.
The study was based on data for 112 patients (54 male, 58 female) operated on by one neurosurgeon between 1994 and 2016. The mean age at surgery was 43.6 years in men and 48.7 in women (P = .04), according to Talin Handa, Emory University, Atlanta, who presented the retrospective analysis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Men had higher mean IGF-1 levels (874 ng/mL vs. 716 ng/mL for women; P less than .01), and were more likely to have hypopituitarism.
Adjuvant treatment for acromegaly was needed in 57% of men and 49% of women. Following adjuvant treatment, 72% of men maintained surgical remission or achieved normal IGF-1 levels, compared with 89% of women (P = .03). Mean follow-up was shorter in men, 3.6 years, versus 5.2 years for women (P = .02), the researchers reported.
Six-year event-free survival was higher in women (P less than .01), according to the researchers.
For more study findings, watch our video interview.
SOURCE: Handa T et al. AACE 2018. Abstract #824.
BOSTON – , according to study results presented at the annual meeting of the American Association of Clinical Endocrinologists.
The study was based on data for 112 patients (54 male, 58 female) operated on by one neurosurgeon between 1994 and 2016. The mean age at surgery was 43.6 years in men and 48.7 in women (P = .04), according to Talin Handa, Emory University, Atlanta, who presented the retrospective analysis.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Men had higher mean IGF-1 levels (874 ng/mL vs. 716 ng/mL for women; P less than .01), and were more likely to have hypopituitarism.
Adjuvant treatment for acromegaly was needed in 57% of men and 49% of women. Following adjuvant treatment, 72% of men maintained surgical remission or achieved normal IGF-1 levels, compared with 89% of women (P = .03). Mean follow-up was shorter in men, 3.6 years, versus 5.2 years for women (P = .02), the researchers reported.
Six-year event-free survival was higher in women (P less than .01), according to the researchers.
For more study findings, watch our video interview.
SOURCE: Handa T et al. AACE 2018. Abstract #824.
REPORTING FROM AACE 2018
Key clinical point: Men with acromegaly present at a younger age, have higher IGF-1 levels, and achieve lower biochemical control rates than do women with the disorder.
Major finding: Men were less likely than women to have surgical remissions or normal IGF-1 levels after adjuvant treatment (72% for men and 89% for women; P = .03).
Study details: A retrospective analysis of 112 patients (54 male, 58 female) operated on by one neurosurgeon during 1994-2016.
Disclosures: The presenter had no disclosures related to the presentation.
Source: Handa T et al. AACE 2018. Abstract #824.