User login
CO2 laser guided by confocal microscopy effectively treated superficial BCC
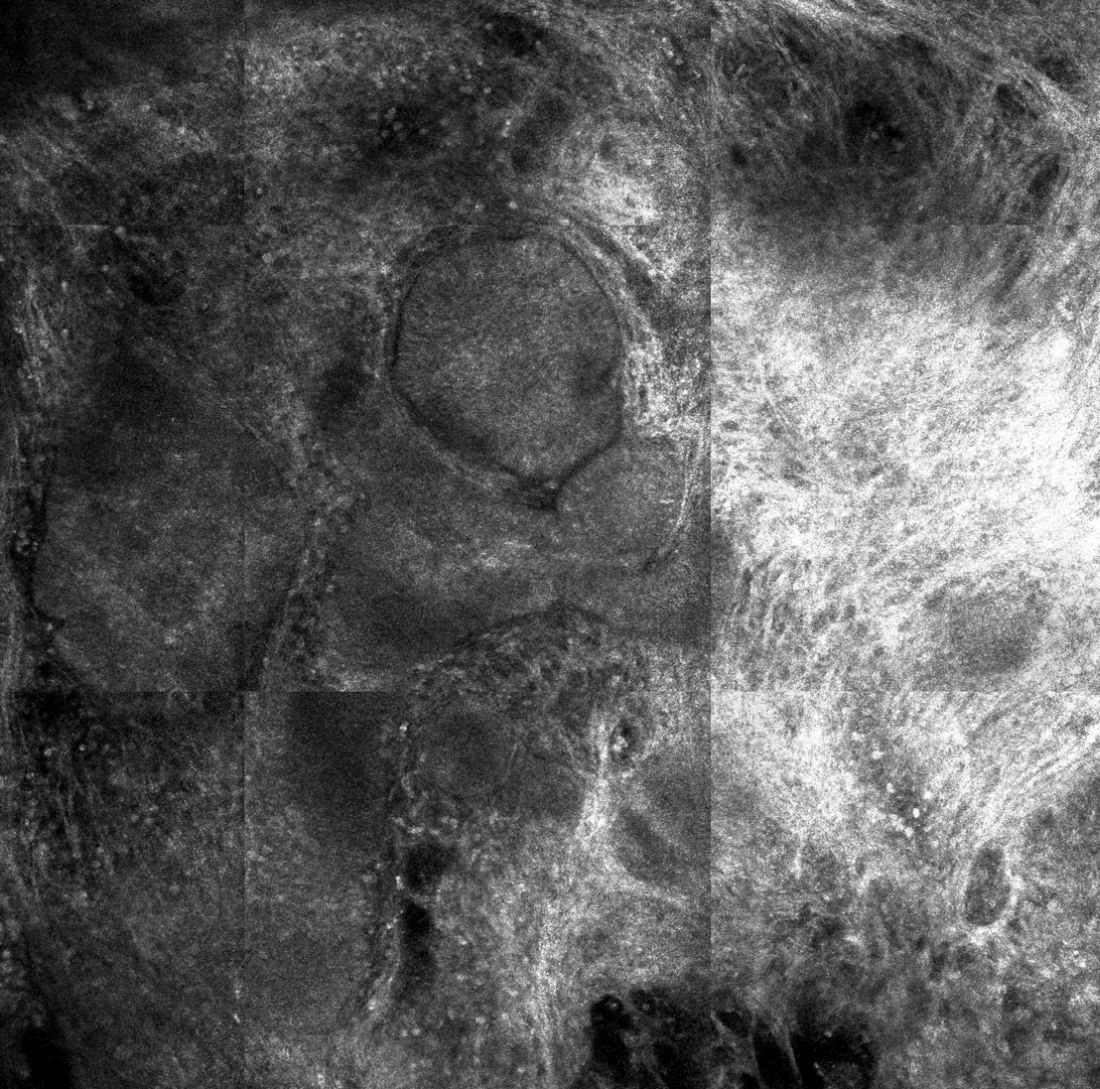
DALLAS – The use of CO2 laser ablation guided by reflectance confocal microscopy is an effective, minimally invasive treatment for superficial and early nodular basal cell carcinoma (BCC), according to results from an ongoing study.
“While surgery is the gold standard for many basal cell carcinomas, nonsurgical therapies may be a good option for the superficial and early nodular subtypes,” lead study author Anthony M. Rossi, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “Laser ablation was used many years ago, so this is not a novel concept, but we’re bringing it back and we’re trying to use confocal microscopy to hone in on the basal cell and selectively target the tumor.”

For the current analysis, he and his associates used with a mean age of 55 years. Of the 20 lesions, 18 were located on the limbs and trunk, while two were on the head and neck. The median lesion diameter was 7 mm. Prior to laser ablation, the researchers performed reflectance confocal microscopy to define lateral and deep margins and define the laser parameters.

The median number of laser passes was three, and ranged from two to eight, delivered at a fluence of 7.5 J/cm2. Reflectance confocal microscopy was repeated immediately after the laser treatment to the skin wound margins and deep margins, and it was performed every 3-6 months thereafter. “If you do confocal microscopy too early, you’ll see mainly inflammation and you may see residual tumor that hasn’t been fully resolved yet,” Dr. Rossi said.
As for future directions, he and his colleagues are developing contrast agents to enhance the ability to detect BCC tumors in vivo, to highlight tumor islands, and to differentiate sebaceous glands and hair follicles. Dr. Rossi reported having no relevant disclosures.
DALLAS – The use of CO2 laser ablation guided by reflectance confocal microscopy is an effective, minimally invasive treatment for superficial and early nodular basal cell carcinoma (BCC), according to results from an ongoing study.
“While surgery is the gold standard for many basal cell carcinomas, nonsurgical therapies may be a good option for the superficial and early nodular subtypes,” lead study author Anthony M. Rossi, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “Laser ablation was used many years ago, so this is not a novel concept, but we’re bringing it back and we’re trying to use confocal microscopy to hone in on the basal cell and selectively target the tumor.”
For the current analysis, he and his associates used with a mean age of 55 years. Of the 20 lesions, 18 were located on the limbs and trunk, while two were on the head and neck. The median lesion diameter was 7 mm. Prior to laser ablation, the researchers performed reflectance confocal microscopy to define lateral and deep margins and define the laser parameters.
The median number of laser passes was three, and ranged from two to eight, delivered at a fluence of 7.5 J/cm2. Reflectance confocal microscopy was repeated immediately after the laser treatment to the skin wound margins and deep margins, and it was performed every 3-6 months thereafter. “If you do confocal microscopy too early, you’ll see mainly inflammation and you may see residual tumor that hasn’t been fully resolved yet,” Dr. Rossi said.
As for future directions, he and his colleagues are developing contrast agents to enhance the ability to detect BCC tumors in vivo, to highlight tumor islands, and to differentiate sebaceous glands and hair follicles. Dr. Rossi reported having no relevant disclosures.
DALLAS – The use of CO2 laser ablation guided by reflectance confocal microscopy is an effective, minimally invasive treatment for superficial and early nodular basal cell carcinoma (BCC), according to results from an ongoing study.
“While surgery is the gold standard for many basal cell carcinomas, nonsurgical therapies may be a good option for the superficial and early nodular subtypes,” lead study author Anthony M. Rossi, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “Laser ablation was used many years ago, so this is not a novel concept, but we’re bringing it back and we’re trying to use confocal microscopy to hone in on the basal cell and selectively target the tumor.”
For the current analysis, he and his associates used with a mean age of 55 years. Of the 20 lesions, 18 were located on the limbs and trunk, while two were on the head and neck. The median lesion diameter was 7 mm. Prior to laser ablation, the researchers performed reflectance confocal microscopy to define lateral and deep margins and define the laser parameters.
The median number of laser passes was three, and ranged from two to eight, delivered at a fluence of 7.5 J/cm2. Reflectance confocal microscopy was repeated immediately after the laser treatment to the skin wound margins and deep margins, and it was performed every 3-6 months thereafter. “If you do confocal microscopy too early, you’ll see mainly inflammation and you may see residual tumor that hasn’t been fully resolved yet,” Dr. Rossi said.
As for future directions, he and his colleagues are developing contrast agents to enhance the ability to detect BCC tumors in vivo, to highlight tumor islands, and to differentiate sebaceous glands and hair follicles. Dr. Rossi reported having no relevant disclosures.
REPORTING FROM ASLMS 2018
Key clinical point: Reflectance confocal microscopy-guided CO2 laser ablation of basal cell carcinoma (BCC) was found to be effective.
Major finding: After an average follow-up of 17 months, no recurrence of BCC has been detected clinically, dermoscopically, or by reflectance confocal microscopy.
Study details: A clinical analysis of seven adults with superficial BCC who were treated with a CO2 laser guided by confocal microscopy.
Disclosures: Dr. Rossi reported having no financial disclosures.
Noninvasive 1060-nm diode laser found effective for axillary hyperhidrosis
DALLAS – , a condition that affects an estimated 1.4% people in the United States.
“Newer treatments such as microwave technology, botulinum toxin injections, and lasers have emerged as effective methods,” lead study author Bruce E. Katz, MD, who directs the Juva Skin & Laser Center in New York, said at the annual conference of the American Society for Laser Medicine and Surgery Inc.
In a prospective pilot study, Dr. Katz and his associates examined the use of a noninvasive 1060-nm diode laser (SculpSure, Cynosure) in 10 subjects with moderate to severe hyperhidrosis of the axilla, which was defined as having Hyperhidrosis Disease Severity Scale (HDSS) scores of 3 or 4. The subjects, whose mean age was 42 years, received two laser treatments on the axillary area at 6-week intervals, and the researchers performed starch iodine tests and took two-dimensional photography of the axilla before and after treatment. Subjects were asked to rate their conditions on the HDSS and satisfaction with treatment. Two blinded dermatologist evaluators graded the reduction in sweat production on photos of starch iodine tests. The researchers also performed a retrospective analysis on all subjects to assess safety and efficacy of treatment.
The 1060-nm diode laser used for the study features four flat, nonsuction applicators. Dr. Katz and his associates positioned two applicators on the axilla simultaneously for 25 minutes. “The 1060-nm wavelength has minimal absorption in the melanin, so we can really treat any skin type,” he said. “It has a high affinity for adipose tissue, and we believe that its targeted effect at the level of the eccrine and apocrine glands should help improve hyperhidrosis. It works by elevating the tissue temperature to about 42 to 47 degrees Centigrade, without damaging surrounding tissue. The device has a sapphire cooling plate, so it’s comfortable for the patient.”
The retrospective analysis revealed minimal adverse events such as pain, mild erythema, and edema, which were transient and resolved without intervention in a day or two. To date, no cases have recurred, “which we were surprised by,” Dr. Katz said. “We were surprised that the effect lasted that long.”

SOURCE: Katz et. al. ASLMS 2018.
DALLAS – , a condition that affects an estimated 1.4% people in the United States.
“Newer treatments such as microwave technology, botulinum toxin injections, and lasers have emerged as effective methods,” lead study author Bruce E. Katz, MD, who directs the Juva Skin & Laser Center in New York, said at the annual conference of the American Society for Laser Medicine and Surgery Inc.
In a prospective pilot study, Dr. Katz and his associates examined the use of a noninvasive 1060-nm diode laser (SculpSure, Cynosure) in 10 subjects with moderate to severe hyperhidrosis of the axilla, which was defined as having Hyperhidrosis Disease Severity Scale (HDSS) scores of 3 or 4. The subjects, whose mean age was 42 years, received two laser treatments on the axillary area at 6-week intervals, and the researchers performed starch iodine tests and took two-dimensional photography of the axilla before and after treatment. Subjects were asked to rate their conditions on the HDSS and satisfaction with treatment. Two blinded dermatologist evaluators graded the reduction in sweat production on photos of starch iodine tests. The researchers also performed a retrospective analysis on all subjects to assess safety and efficacy of treatment.
The 1060-nm diode laser used for the study features four flat, nonsuction applicators. Dr. Katz and his associates positioned two applicators on the axilla simultaneously for 25 minutes. “The 1060-nm wavelength has minimal absorption in the melanin, so we can really treat any skin type,” he said. “It has a high affinity for adipose tissue, and we believe that its targeted effect at the level of the eccrine and apocrine glands should help improve hyperhidrosis. It works by elevating the tissue temperature to about 42 to 47 degrees Centigrade, without damaging surrounding tissue. The device has a sapphire cooling plate, so it’s comfortable for the patient.”
The retrospective analysis revealed minimal adverse events such as pain, mild erythema, and edema, which were transient and resolved without intervention in a day or two. To date, no cases have recurred, “which we were surprised by,” Dr. Katz said. “We were surprised that the effect lasted that long.”
SOURCE: Katz et. al. ASLMS 2018.
DALLAS – , a condition that affects an estimated 1.4% people in the United States.
“Newer treatments such as microwave technology, botulinum toxin injections, and lasers have emerged as effective methods,” lead study author Bruce E. Katz, MD, who directs the Juva Skin & Laser Center in New York, said at the annual conference of the American Society for Laser Medicine and Surgery Inc.
In a prospective pilot study, Dr. Katz and his associates examined the use of a noninvasive 1060-nm diode laser (SculpSure, Cynosure) in 10 subjects with moderate to severe hyperhidrosis of the axilla, which was defined as having Hyperhidrosis Disease Severity Scale (HDSS) scores of 3 or 4. The subjects, whose mean age was 42 years, received two laser treatments on the axillary area at 6-week intervals, and the researchers performed starch iodine tests and took two-dimensional photography of the axilla before and after treatment. Subjects were asked to rate their conditions on the HDSS and satisfaction with treatment. Two blinded dermatologist evaluators graded the reduction in sweat production on photos of starch iodine tests. The researchers also performed a retrospective analysis on all subjects to assess safety and efficacy of treatment.
The 1060-nm diode laser used for the study features four flat, nonsuction applicators. Dr. Katz and his associates positioned two applicators on the axilla simultaneously for 25 minutes. “The 1060-nm wavelength has minimal absorption in the melanin, so we can really treat any skin type,” he said. “It has a high affinity for adipose tissue, and we believe that its targeted effect at the level of the eccrine and apocrine glands should help improve hyperhidrosis. It works by elevating the tissue temperature to about 42 to 47 degrees Centigrade, without damaging surrounding tissue. The device has a sapphire cooling plate, so it’s comfortable for the patient.”
The retrospective analysis revealed minimal adverse events such as pain, mild erythema, and edema, which were transient and resolved without intervention in a day or two. To date, no cases have recurred, “which we were surprised by,” Dr. Katz said. “We were surprised that the effect lasted that long.”
SOURCE: Katz et. al. ASLMS 2018.
REPORTING FROM ASLMS 2018
Few physicians report adverse events related to body contouring devices
DALLAS – Most physicians do not report adverse events related to noninvasive body contouring devices to the Food and Drug Administration, a database review showed.
“The FDA mandates that manufacturers and device operators disclose medical device reports to monitor suspected injuries and device malfunctions to the Manufacturer and User Facility Device Experience [MAUDE] database,” study author Adam J. Wulkan, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “Given the rapid growth in the noninvasive fat reduction market, it is essential physicians be aware of associated adverse events.”
“Given that this is the largest database for adverse events, I was surprised how few reports were done by physicians,” Dr. Wulkan said in an interview.
He reported results from 83 of the 98 MDRs. A total of 26 MDRs reported on cryolipolysis and included newly diagnosed or exacerbation of prior umbilical hernias (10), neuropathies (5), paradoxical fat hyperplasias (4), blisters (3), rashes (1), flu-like symptoms (1), gastroenteritis (1), and prolapsed bladder/uterus/rectum (1). Of the 11 MDRs for radio-frequency devices, 10 were burns/blisters and 1 fire.
Dr. Wulkan went on to note that 17 MDRs were reported for 1060-nm laser lipolysis, including burns/blisters (5), nodules (4), pain (3), cellulitis/abscesses (2), excessive swelling (1), neuropathy (1), and vomiting (1). There were four cases of burns on MDRs from focused/pulsed ultrasound procedures. One was on a non–FDA approved body site and another after combination radio-frequency/infrared treatment for cellulite reduction.
There were eight MDRs reported with 1440-nm laser cellulite reduction, including burn (5), unacceptable cosmesis (2), and faulty power supply (1). In addition, there were 12 MDRs reported on high-frequency ultrasound, including burns/blisters (9), subcutaneous nodules (2), and excoriation (1). Finally, vacuum-assisted submission was associated with five MDRs, including festooning/unacceptable cosmesis (2), seroma/hematoma (1), laceration (1), and nodules (1).
Dr. Wulkan acknowledged certain limitations of the study, including the fact that not all MDRs are reported to MAUDE, and that the reliability of patient reporting can be questionable. “We have to figure out if there is a natural causation between the adverse event and the treatment itself,” he said at the meeting. “The number of MDRs for any given device must be correlated to the number of procedures performed before we jump to conclusions about the safety of any given device.”
He reported having no financial disclosures. One study coauthor holds positions on advisory boards of, is a consultant for, and has intellectual property and/or stock options with various industry companies, such as Soliton and Allergan.
SOURCE: Wulkan et. al., ASLMS 2018.
DALLAS – Most physicians do not report adverse events related to noninvasive body contouring devices to the Food and Drug Administration, a database review showed.
“The FDA mandates that manufacturers and device operators disclose medical device reports to monitor suspected injuries and device malfunctions to the Manufacturer and User Facility Device Experience [MAUDE] database,” study author Adam J. Wulkan, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “Given the rapid growth in the noninvasive fat reduction market, it is essential physicians be aware of associated adverse events.”
“Given that this is the largest database for adverse events, I was surprised how few reports were done by physicians,” Dr. Wulkan said in an interview.
He reported results from 83 of the 98 MDRs. A total of 26 MDRs reported on cryolipolysis and included newly diagnosed or exacerbation of prior umbilical hernias (10), neuropathies (5), paradoxical fat hyperplasias (4), blisters (3), rashes (1), flu-like symptoms (1), gastroenteritis (1), and prolapsed bladder/uterus/rectum (1). Of the 11 MDRs for radio-frequency devices, 10 were burns/blisters and 1 fire.
Dr. Wulkan went on to note that 17 MDRs were reported for 1060-nm laser lipolysis, including burns/blisters (5), nodules (4), pain (3), cellulitis/abscesses (2), excessive swelling (1), neuropathy (1), and vomiting (1). There were four cases of burns on MDRs from focused/pulsed ultrasound procedures. One was on a non–FDA approved body site and another after combination radio-frequency/infrared treatment for cellulite reduction.
There were eight MDRs reported with 1440-nm laser cellulite reduction, including burn (5), unacceptable cosmesis (2), and faulty power supply (1). In addition, there were 12 MDRs reported on high-frequency ultrasound, including burns/blisters (9), subcutaneous nodules (2), and excoriation (1). Finally, vacuum-assisted submission was associated with five MDRs, including festooning/unacceptable cosmesis (2), seroma/hematoma (1), laceration (1), and nodules (1).
Dr. Wulkan acknowledged certain limitations of the study, including the fact that not all MDRs are reported to MAUDE, and that the reliability of patient reporting can be questionable. “We have to figure out if there is a natural causation between the adverse event and the treatment itself,” he said at the meeting. “The number of MDRs for any given device must be correlated to the number of procedures performed before we jump to conclusions about the safety of any given device.”
He reported having no financial disclosures. One study coauthor holds positions on advisory boards of, is a consultant for, and has intellectual property and/or stock options with various industry companies, such as Soliton and Allergan.
SOURCE: Wulkan et. al., ASLMS 2018.
DALLAS – Most physicians do not report adverse events related to noninvasive body contouring devices to the Food and Drug Administration, a database review showed.
“The FDA mandates that manufacturers and device operators disclose medical device reports to monitor suspected injuries and device malfunctions to the Manufacturer and User Facility Device Experience [MAUDE] database,” study author Adam J. Wulkan, MD, said at the annual conference of the American Society for Laser Medicine and Surgery. “Given the rapid growth in the noninvasive fat reduction market, it is essential physicians be aware of associated adverse events.”
“Given that this is the largest database for adverse events, I was surprised how few reports were done by physicians,” Dr. Wulkan said in an interview.
He reported results from 83 of the 98 MDRs. A total of 26 MDRs reported on cryolipolysis and included newly diagnosed or exacerbation of prior umbilical hernias (10), neuropathies (5), paradoxical fat hyperplasias (4), blisters (3), rashes (1), flu-like symptoms (1), gastroenteritis (1), and prolapsed bladder/uterus/rectum (1). Of the 11 MDRs for radio-frequency devices, 10 were burns/blisters and 1 fire.
Dr. Wulkan went on to note that 17 MDRs were reported for 1060-nm laser lipolysis, including burns/blisters (5), nodules (4), pain (3), cellulitis/abscesses (2), excessive swelling (1), neuropathy (1), and vomiting (1). There were four cases of burns on MDRs from focused/pulsed ultrasound procedures. One was on a non–FDA approved body site and another after combination radio-frequency/infrared treatment for cellulite reduction.
There were eight MDRs reported with 1440-nm laser cellulite reduction, including burn (5), unacceptable cosmesis (2), and faulty power supply (1). In addition, there were 12 MDRs reported on high-frequency ultrasound, including burns/blisters (9), subcutaneous nodules (2), and excoriation (1). Finally, vacuum-assisted submission was associated with five MDRs, including festooning/unacceptable cosmesis (2), seroma/hematoma (1), laceration (1), and nodules (1).
Dr. Wulkan acknowledged certain limitations of the study, including the fact that not all MDRs are reported to MAUDE, and that the reliability of patient reporting can be questionable. “We have to figure out if there is a natural causation between the adverse event and the treatment itself,” he said at the meeting. “The number of MDRs for any given device must be correlated to the number of procedures performed before we jump to conclusions about the safety of any given device.”
He reported having no financial disclosures. One study coauthor holds positions on advisory boards of, is a consultant for, and has intellectual property and/or stock options with various industry companies, such as Soliton and Allergan.
SOURCE: Wulkan et. al., ASLMS 2018.
REPORTING FROM ASLMS 2018
Key clinical point: Most physicians do not report adverse events related to noninvasive body contouring devices to the FDA .
Major finding: Of 83 medical device reports, 26 were related to cryolipolysis.
Study details: An analysis of 83 complications of noninvasive fat reduction and cellulite reduction devices reported to the FDA.
Disclosures: Dr. Wulkan reported having no financial disclosures. One study coauthor holds positions on advisory boards of, is a consultant for, and has intellectual property and/or stock options with various industry companies, such as Soliton and Allergan.
Source: Wulkan et al. ASLMS 2018.
Laser treatment of port wine stains in infancy found safe, effective
DALLAS – Laser treatment of port wine stains in infancy is both safe and effective, with no incidence of scarring or pigmentary changes, according to results from a single-center analysis.
“Early intervention allows for treatment without general anesthesia, with faster and more complete clearance than what has been reported for treatments begun at older ages,” Hana Jeon, MD, said at the annual conference of the American Society for Laser Medicine and Surgery.
A recent Food and Drug Administration Drug Safety Communication warned that “repeated or lengthy used of general anesthetic and sedation drugs during surgeries or procedures in children younger than 3 years or in pregnant women during their third trimester may affect the development of children’s brains.” Dr. Jeon, a dermatologist in private practice in New York, noted that the FDA warning “places a greater importance on the already controversial topic of when to initiate port wine stain [PWS] treatments in pediatric patients, which requires repeated treatments and are often performed with general anesthesia. Without treatment, these lesions tend to get larger and thicker with time. Starting the treatment during infancy has the potential to limit the use of general anesthesia and to facilitate clearing.”
In what she said is the largest retrospective study of its kind to date, Dr. Jeon and her associates evaluated the success and safety of treating PWSs with a pulsed dye laser at the age of 1 year or younger in the office setting without general anesthesia. The patients received their first PWS treatment at their center during 2000-2017. They reviewed the charts of 197 patients to extract relevant data, including demographic information, age at the time of procedure, and treatment dates. The data cutoff was at 1 year following the initial treatment. Four physicians independently reviewed before and after photos and used the visual analogue scale to grade them.
The pulsed dye laser with dynamic cooling spray was used to minimize patient discomfort. No topical, local, or general anesthesia was used. Patients were immobilized by ancillary staff with parents present in most cases. Ocular shields were placed to allow treatment of periocular lesions.
Of the 197 patients, 63% were female, 90.1% had Fitzpatrick skin types I-III, 8.1% had type IV skin, and the rest had type V-VI skin. Most of the lesions were facial (75.6%), and 41.1% had periocular involvement. The average lesion size was 61 cm2.
The treatment settings for the pulsed dye laser were a 10-12 mm spot size delivered at a fluence of 6.5-9 J/cm2 in a pulse duration of 0.45-1.5 milliseconds. The average age at the time of first treatment was 3.4 months (range, 5-355 days), and the average number of treatments was 9.8 (range, 2-23). Most of the patients (116) were aged 0-3 months at the time of first treatment, followed by 51 aged 3-6 months, 19 aged 6-9 months, and 11 aged 9-12 months.
According to the averaged scores on the visual analogue scale assigned by physicians, 27.4% showed a 100% clearance, 39.1% showed 76%-99% improvement, 15.1% showed 51%-75% improvement, 10.7% showed 26%-50% improvement, and 7.7% showed 0%-25% improvement. No scarring or pigmentary changes were observed.
An analysis of dermatomal distribution revealed that the presence of a V1 lesion was a statistically significant predictor of a higher clearance rate, while the presence of a V3 lesion was a statistically significant predictor of a low clearance rate. “Regardless of where the lesion was, all patients did well,” she said.
Given the small proportion of patients who received their first treatment between the ages of 6 and 12 months of age, Dr. Jeon said that “further studies would be needed to elucidate whether earlier intervention helps to achieve better results.”*
Advantages of early treatment, she said, include the ability to “treat lesions before they get larger and thicker, which also decreases the risk of spontaneous bleeding. Thinner skin allows for better penetration of the laser beam, and we can also avoid using general anesthesia. Psychologically, if we’re able to clear these lesions, it can result in improved quality of life and self-esteem; not just for the patient but for the family as well.”
Dr. Jeon acknowledged certain limitations of the study, including its retrospective design, variable follow-up times, and non-standardization of photographs.
She reported having no financial disclosures.
SOURCE: Jeon H et al. ASLMS 2018.
Correction, 4/18/18: An earlier version of this article misstated the age range of the study participants.
DALLAS – Laser treatment of port wine stains in infancy is both safe and effective, with no incidence of scarring or pigmentary changes, according to results from a single-center analysis.
“Early intervention allows for treatment without general anesthesia, with faster and more complete clearance than what has been reported for treatments begun at older ages,” Hana Jeon, MD, said at the annual conference of the American Society for Laser Medicine and Surgery.
A recent Food and Drug Administration Drug Safety Communication warned that “repeated or lengthy used of general anesthetic and sedation drugs during surgeries or procedures in children younger than 3 years or in pregnant women during their third trimester may affect the development of children’s brains.” Dr. Jeon, a dermatologist in private practice in New York, noted that the FDA warning “places a greater importance on the already controversial topic of when to initiate port wine stain [PWS] treatments in pediatric patients, which requires repeated treatments and are often performed with general anesthesia. Without treatment, these lesions tend to get larger and thicker with time. Starting the treatment during infancy has the potential to limit the use of general anesthesia and to facilitate clearing.”
In what she said is the largest retrospective study of its kind to date, Dr. Jeon and her associates evaluated the success and safety of treating PWSs with a pulsed dye laser at the age of 1 year or younger in the office setting without general anesthesia. The patients received their first PWS treatment at their center during 2000-2017. They reviewed the charts of 197 patients to extract relevant data, including demographic information, age at the time of procedure, and treatment dates. The data cutoff was at 1 year following the initial treatment. Four physicians independently reviewed before and after photos and used the visual analogue scale to grade them.
The pulsed dye laser with dynamic cooling spray was used to minimize patient discomfort. No topical, local, or general anesthesia was used. Patients were immobilized by ancillary staff with parents present in most cases. Ocular shields were placed to allow treatment of periocular lesions.
Of the 197 patients, 63% were female, 90.1% had Fitzpatrick skin types I-III, 8.1% had type IV skin, and the rest had type V-VI skin. Most of the lesions were facial (75.6%), and 41.1% had periocular involvement. The average lesion size was 61 cm2.
The treatment settings for the pulsed dye laser were a 10-12 mm spot size delivered at a fluence of 6.5-9 J/cm2 in a pulse duration of 0.45-1.5 milliseconds. The average age at the time of first treatment was 3.4 months (range, 5-355 days), and the average number of treatments was 9.8 (range, 2-23). Most of the patients (116) were aged 0-3 months at the time of first treatment, followed by 51 aged 3-6 months, 19 aged 6-9 months, and 11 aged 9-12 months.
According to the averaged scores on the visual analogue scale assigned by physicians, 27.4% showed a 100% clearance, 39.1% showed 76%-99% improvement, 15.1% showed 51%-75% improvement, 10.7% showed 26%-50% improvement, and 7.7% showed 0%-25% improvement. No scarring or pigmentary changes were observed.
An analysis of dermatomal distribution revealed that the presence of a V1 lesion was a statistically significant predictor of a higher clearance rate, while the presence of a V3 lesion was a statistically significant predictor of a low clearance rate. “Regardless of where the lesion was, all patients did well,” she said.
Given the small proportion of patients who received their first treatment between the ages of 6 and 12 months of age, Dr. Jeon said that “further studies would be needed to elucidate whether earlier intervention helps to achieve better results.”*
Advantages of early treatment, she said, include the ability to “treat lesions before they get larger and thicker, which also decreases the risk of spontaneous bleeding. Thinner skin allows for better penetration of the laser beam, and we can also avoid using general anesthesia. Psychologically, if we’re able to clear these lesions, it can result in improved quality of life and self-esteem; not just for the patient but for the family as well.”
Dr. Jeon acknowledged certain limitations of the study, including its retrospective design, variable follow-up times, and non-standardization of photographs.
She reported having no financial disclosures.
SOURCE: Jeon H et al. ASLMS 2018.
Correction, 4/18/18: An earlier version of this article misstated the age range of the study participants.
DALLAS – Laser treatment of port wine stains in infancy is both safe and effective, with no incidence of scarring or pigmentary changes, according to results from a single-center analysis.
“Early intervention allows for treatment without general anesthesia, with faster and more complete clearance than what has been reported for treatments begun at older ages,” Hana Jeon, MD, said at the annual conference of the American Society for Laser Medicine and Surgery.
A recent Food and Drug Administration Drug Safety Communication warned that “repeated or lengthy used of general anesthetic and sedation drugs during surgeries or procedures in children younger than 3 years or in pregnant women during their third trimester may affect the development of children’s brains.” Dr. Jeon, a dermatologist in private practice in New York, noted that the FDA warning “places a greater importance on the already controversial topic of when to initiate port wine stain [PWS] treatments in pediatric patients, which requires repeated treatments and are often performed with general anesthesia. Without treatment, these lesions tend to get larger and thicker with time. Starting the treatment during infancy has the potential to limit the use of general anesthesia and to facilitate clearing.”
In what she said is the largest retrospective study of its kind to date, Dr. Jeon and her associates evaluated the success and safety of treating PWSs with a pulsed dye laser at the age of 1 year or younger in the office setting without general anesthesia. The patients received their first PWS treatment at their center during 2000-2017. They reviewed the charts of 197 patients to extract relevant data, including demographic information, age at the time of procedure, and treatment dates. The data cutoff was at 1 year following the initial treatment. Four physicians independently reviewed before and after photos and used the visual analogue scale to grade them.
The pulsed dye laser with dynamic cooling spray was used to minimize patient discomfort. No topical, local, or general anesthesia was used. Patients were immobilized by ancillary staff with parents present in most cases. Ocular shields were placed to allow treatment of periocular lesions.
Of the 197 patients, 63% were female, 90.1% had Fitzpatrick skin types I-III, 8.1% had type IV skin, and the rest had type V-VI skin. Most of the lesions were facial (75.6%), and 41.1% had periocular involvement. The average lesion size was 61 cm2.
The treatment settings for the pulsed dye laser were a 10-12 mm spot size delivered at a fluence of 6.5-9 J/cm2 in a pulse duration of 0.45-1.5 milliseconds. The average age at the time of first treatment was 3.4 months (range, 5-355 days), and the average number of treatments was 9.8 (range, 2-23). Most of the patients (116) were aged 0-3 months at the time of first treatment, followed by 51 aged 3-6 months, 19 aged 6-9 months, and 11 aged 9-12 months.
According to the averaged scores on the visual analogue scale assigned by physicians, 27.4% showed a 100% clearance, 39.1% showed 76%-99% improvement, 15.1% showed 51%-75% improvement, 10.7% showed 26%-50% improvement, and 7.7% showed 0%-25% improvement. No scarring or pigmentary changes were observed.
An analysis of dermatomal distribution revealed that the presence of a V1 lesion was a statistically significant predictor of a higher clearance rate, while the presence of a V3 lesion was a statistically significant predictor of a low clearance rate. “Regardless of where the lesion was, all patients did well,” she said.
Given the small proportion of patients who received their first treatment between the ages of 6 and 12 months of age, Dr. Jeon said that “further studies would be needed to elucidate whether earlier intervention helps to achieve better results.”*
Advantages of early treatment, she said, include the ability to “treat lesions before they get larger and thicker, which also decreases the risk of spontaneous bleeding. Thinner skin allows for better penetration of the laser beam, and we can also avoid using general anesthesia. Psychologically, if we’re able to clear these lesions, it can result in improved quality of life and self-esteem; not just for the patient but for the family as well.”
Dr. Jeon acknowledged certain limitations of the study, including its retrospective design, variable follow-up times, and non-standardization of photographs.
She reported having no financial disclosures.
SOURCE: Jeon H et al. ASLMS 2018.
Correction, 4/18/18: An earlier version of this article misstated the age range of the study participants.
REPORTING FROM ASLMS 2018
Key clinical point:
Major finding: On the visual analogue scale, 27.4% of infants achieved complete clearance of their port wine lesion after treatment.
Study details: An analysis of 197 infants aged 1 year or younger with port wine stains who were treated with a pulsed dye laser during 2000-2017.
Disclosures: Dr. Jeon reported having no financial disclosures.
Source: Jeon H et al. ASLMS 2018.
Carboxytherapy caused small yet transient subcutaneous fat reduction
DALLAS – , a small randomized, controlled trial demonstrated.
“Carboxytherapy has been previously used therapeutically to reduce fat, and studies of carboxytherapy have been done in the past as well,” the study’s senior author, Murad Alam, MD, said in an interview in advance of a poster session at the annual conference of the American Society for Laser Medicine and Surgery Inc. “However, earlier studies have not been controlled trials.”
For the split-body study, he and his associates enrolled 16 adults and randomized one side of their body to receive infusions of 1,000 cc of CO2 every week for 5 weeks in the flank region, while the contralateral side received sham treatments. Outcomes of interest included fat layer thickness using a diagnostic ultrasound, total circumference, and body weight, said Dr. Alam, vice-chair of the department of dermatology and chief of the division of cutaneous and aesthetic surgery at Northwestern University, Chicago. He reported that a significant difference in fat thickness was observed in the carboxytherapy-treated side 1 week after the last treatment (P = .011), but this difference was not maintained at 28 weeks as measured by diagnostic ultrasound. Total circumference decreased nominally but not significantly. Body weights did not significantly change throughout the study.
Dr. Alam acknowledged that the study’s small sample size is a limitation. “We do think we did enough treatments, five per side, to obtain an effect if one were to be seen,” he said. The researchers reported having no financial disclosures.
DALLAS – , a small randomized, controlled trial demonstrated.
“Carboxytherapy has been previously used therapeutically to reduce fat, and studies of carboxytherapy have been done in the past as well,” the study’s senior author, Murad Alam, MD, said in an interview in advance of a poster session at the annual conference of the American Society for Laser Medicine and Surgery Inc. “However, earlier studies have not been controlled trials.”
For the split-body study, he and his associates enrolled 16 adults and randomized one side of their body to receive infusions of 1,000 cc of CO2 every week for 5 weeks in the flank region, while the contralateral side received sham treatments. Outcomes of interest included fat layer thickness using a diagnostic ultrasound, total circumference, and body weight, said Dr. Alam, vice-chair of the department of dermatology and chief of the division of cutaneous and aesthetic surgery at Northwestern University, Chicago. He reported that a significant difference in fat thickness was observed in the carboxytherapy-treated side 1 week after the last treatment (P = .011), but this difference was not maintained at 28 weeks as measured by diagnostic ultrasound. Total circumference decreased nominally but not significantly. Body weights did not significantly change throughout the study.
Dr. Alam acknowledged that the study’s small sample size is a limitation. “We do think we did enough treatments, five per side, to obtain an effect if one were to be seen,” he said. The researchers reported having no financial disclosures.
DALLAS – , a small randomized, controlled trial demonstrated.
“Carboxytherapy has been previously used therapeutically to reduce fat, and studies of carboxytherapy have been done in the past as well,” the study’s senior author, Murad Alam, MD, said in an interview in advance of a poster session at the annual conference of the American Society for Laser Medicine and Surgery Inc. “However, earlier studies have not been controlled trials.”
For the split-body study, he and his associates enrolled 16 adults and randomized one side of their body to receive infusions of 1,000 cc of CO2 every week for 5 weeks in the flank region, while the contralateral side received sham treatments. Outcomes of interest included fat layer thickness using a diagnostic ultrasound, total circumference, and body weight, said Dr. Alam, vice-chair of the department of dermatology and chief of the division of cutaneous and aesthetic surgery at Northwestern University, Chicago. He reported that a significant difference in fat thickness was observed in the carboxytherapy-treated side 1 week after the last treatment (P = .011), but this difference was not maintained at 28 weeks as measured by diagnostic ultrasound. Total circumference decreased nominally but not significantly. Body weights did not significantly change throughout the study.
Dr. Alam acknowledged that the study’s small sample size is a limitation. “We do think we did enough treatments, five per side, to obtain an effect if one were to be seen,” he said. The researchers reported having no financial disclosures.
REPORTING FROM ASLMS 2018
Key clinical point: Carboxytherapy yielded a modest reduction in fat that went away after a few months.
Major finding: A significant difference in fat thickness was observed in the carboxytherapy-treated flank region 1 week after the last treatment (P = .011).
Study details: A randomized, split-body study of 16 adults.
Disclosures: Dr. Alam reported having no financial disclosures.
Liability claims from cutaneous laser surgery continue to rise
DALLAS – , and the average indemnity claim is close to $320,000, results from an analysis of national data have shown.
“Physicians seeking to undertake laser surgery in their practice should ensure they have proper training in the physics, safety, and techniques of each procedure,” study author Saami Khalifian, MD, said in an interview in advance of the annual meeting of the American Society for Laser Medicine and Surgery. “Legal precedent has demonstrated that nonphysicians performing laser surgery will likely be held to a standard of care and training corresponding to a physician with appropriate training. Therefore, physicians who delegate laser operations to their nonphysician agents are ultimately responsible for the actions of their agents.”
For the period between June 2012 and December 2017, Dr. Khalifian and his colleagues identified 32 cases with public decision related to injury secondary to cutaneous laser surgery. The incidence of litigation related to laser surgery demonstrates an increasing trend since 1985, with peak occurrence in 2010 (total of 22 cases, which represents 10.7% of 206 cases reported in the entire data set since 1985). Laser hair removal was the most common litigated procedure prior to 2012, but since then has been surpassed by laser rejuvenation, which includes ablative and nonablative resurfacing, fractionated lasers, and intense pulsed light (47% of cases since mid-2012). Nonphysician operators accounted for a substantial subset of these cases (66% of all cases since mid-2012), with their physician supervisors named as defendants, despite not performing the procedure.
Dr. Khalifian noted that medical spas in the study “uniformly had unsupervised nonphysician operators in nonmedical office settings,” and therefore “had one of the highest litigation rates and number of cases. What is interesting about this, however, is that medical spas that are run by nonphysicians are also less likely to have medical liability insurance to satisfy a potential malpractice claim and therefore would be less likely to be pursued by a plaintiff’s attorney. Despite this, they had one of the highest patient injury rates, which is likely underrepresented based on the lack of malpractice insurance to be pursued in a legal claim.”
The researchers also found that delegated procedures were most frequently litigated against regardless of subspecialty of supervising physician (66%). Of the preventable causes of action, the most common was failure to obtain an informed consent (34%) and negligence (50%). Of the 32 cases with public decisions, 17 (53.1%) resulted in decisions in favor of the plaintiff. The mean indemnity payment was $318,832.
“Our current work evaluating data from 2012-2017 is consistent with our prior work dating back to 1985 and demonstrates again that nonphysician operators account for the majority of cases of legal action,” Dr. Khalifian said. “In fact, there is an increasing trend since about 2008 for a higher proportion of cases being performed by physician extenders and nonphysician operators. Despite physicians acting as supervisors and not the actual laser operator they are nonetheless named as defendants in legal claims,” he added.
The data on allegations and causes of legal action “should serve as a guide to help improve patient safety and decrease professional liability,” he pointed out. “It is critical that physicians take steps to mitigate risk to patients by ensuring robust and adequate training for their agents and by directly supervising procedures. However, the data clearly show that the safest treatments are performed directly by physicians who have had such dedicated training in laser and light sources.”
Dr. Khalifian acknowledged certain limitations of the study, including the fact that the data were extracted from only one legal database and did not include cases settled outside of the justice system through third-party arbitration or other means. “It is also limited by search terms in our query,” he said. “It is possible that some cases did not include the terms we used. Finally, only incomplete information was available for some cases even when supplemented through other resources and additional research.”
He reported having no financial disclosures. Study coauthor Mathew M. Avram, MD, JD, serves on the medical advisory board of Sciton and on the scientific advisory boards of Sienna Biopharmaceuticals, Cytrellis, and Allergan. He is also consultant for Merz Aesthetics, Allergan, Soliton, Invasix, and Revance, and has intellectual property with Cytrellis. He also holds stock options with Cytrellis, Invasix, and Zalea.
SOURCE: Khalifian et al. ASLMS 2018.
DALLAS – , and the average indemnity claim is close to $320,000, results from an analysis of national data have shown.
“Physicians seeking to undertake laser surgery in their practice should ensure they have proper training in the physics, safety, and techniques of each procedure,” study author Saami Khalifian, MD, said in an interview in advance of the annual meeting of the American Society for Laser Medicine and Surgery. “Legal precedent has demonstrated that nonphysicians performing laser surgery will likely be held to a standard of care and training corresponding to a physician with appropriate training. Therefore, physicians who delegate laser operations to their nonphysician agents are ultimately responsible for the actions of their agents.”
For the period between June 2012 and December 2017, Dr. Khalifian and his colleagues identified 32 cases with public decision related to injury secondary to cutaneous laser surgery. The incidence of litigation related to laser surgery demonstrates an increasing trend since 1985, with peak occurrence in 2010 (total of 22 cases, which represents 10.7% of 206 cases reported in the entire data set since 1985). Laser hair removal was the most common litigated procedure prior to 2012, but since then has been surpassed by laser rejuvenation, which includes ablative and nonablative resurfacing, fractionated lasers, and intense pulsed light (47% of cases since mid-2012). Nonphysician operators accounted for a substantial subset of these cases (66% of all cases since mid-2012), with their physician supervisors named as defendants, despite not performing the procedure.
Dr. Khalifian noted that medical spas in the study “uniformly had unsupervised nonphysician operators in nonmedical office settings,” and therefore “had one of the highest litigation rates and number of cases. What is interesting about this, however, is that medical spas that are run by nonphysicians are also less likely to have medical liability insurance to satisfy a potential malpractice claim and therefore would be less likely to be pursued by a plaintiff’s attorney. Despite this, they had one of the highest patient injury rates, which is likely underrepresented based on the lack of malpractice insurance to be pursued in a legal claim.”
The researchers also found that delegated procedures were most frequently litigated against regardless of subspecialty of supervising physician (66%). Of the preventable causes of action, the most common was failure to obtain an informed consent (34%) and negligence (50%). Of the 32 cases with public decisions, 17 (53.1%) resulted in decisions in favor of the plaintiff. The mean indemnity payment was $318,832.
“Our current work evaluating data from 2012-2017 is consistent with our prior work dating back to 1985 and demonstrates again that nonphysician operators account for the majority of cases of legal action,” Dr. Khalifian said. “In fact, there is an increasing trend since about 2008 for a higher proportion of cases being performed by physician extenders and nonphysician operators. Despite physicians acting as supervisors and not the actual laser operator they are nonetheless named as defendants in legal claims,” he added.
The data on allegations and causes of legal action “should serve as a guide to help improve patient safety and decrease professional liability,” he pointed out. “It is critical that physicians take steps to mitigate risk to patients by ensuring robust and adequate training for their agents and by directly supervising procedures. However, the data clearly show that the safest treatments are performed directly by physicians who have had such dedicated training in laser and light sources.”
Dr. Khalifian acknowledged certain limitations of the study, including the fact that the data were extracted from only one legal database and did not include cases settled outside of the justice system through third-party arbitration or other means. “It is also limited by search terms in our query,” he said. “It is possible that some cases did not include the terms we used. Finally, only incomplete information was available for some cases even when supplemented through other resources and additional research.”
He reported having no financial disclosures. Study coauthor Mathew M. Avram, MD, JD, serves on the medical advisory board of Sciton and on the scientific advisory boards of Sienna Biopharmaceuticals, Cytrellis, and Allergan. He is also consultant for Merz Aesthetics, Allergan, Soliton, Invasix, and Revance, and has intellectual property with Cytrellis. He also holds stock options with Cytrellis, Invasix, and Zalea.
SOURCE: Khalifian et al. ASLMS 2018.
DALLAS – , and the average indemnity claim is close to $320,000, results from an analysis of national data have shown.
“Physicians seeking to undertake laser surgery in their practice should ensure they have proper training in the physics, safety, and techniques of each procedure,” study author Saami Khalifian, MD, said in an interview in advance of the annual meeting of the American Society for Laser Medicine and Surgery. “Legal precedent has demonstrated that nonphysicians performing laser surgery will likely be held to a standard of care and training corresponding to a physician with appropriate training. Therefore, physicians who delegate laser operations to their nonphysician agents are ultimately responsible for the actions of their agents.”
For the period between June 2012 and December 2017, Dr. Khalifian and his colleagues identified 32 cases with public decision related to injury secondary to cutaneous laser surgery. The incidence of litigation related to laser surgery demonstrates an increasing trend since 1985, with peak occurrence in 2010 (total of 22 cases, which represents 10.7% of 206 cases reported in the entire data set since 1985). Laser hair removal was the most common litigated procedure prior to 2012, but since then has been surpassed by laser rejuvenation, which includes ablative and nonablative resurfacing, fractionated lasers, and intense pulsed light (47% of cases since mid-2012). Nonphysician operators accounted for a substantial subset of these cases (66% of all cases since mid-2012), with their physician supervisors named as defendants, despite not performing the procedure.
Dr. Khalifian noted that medical spas in the study “uniformly had unsupervised nonphysician operators in nonmedical office settings,” and therefore “had one of the highest litigation rates and number of cases. What is interesting about this, however, is that medical spas that are run by nonphysicians are also less likely to have medical liability insurance to satisfy a potential malpractice claim and therefore would be less likely to be pursued by a plaintiff’s attorney. Despite this, they had one of the highest patient injury rates, which is likely underrepresented based on the lack of malpractice insurance to be pursued in a legal claim.”
The researchers also found that delegated procedures were most frequently litigated against regardless of subspecialty of supervising physician (66%). Of the preventable causes of action, the most common was failure to obtain an informed consent (34%) and negligence (50%). Of the 32 cases with public decisions, 17 (53.1%) resulted in decisions in favor of the plaintiff. The mean indemnity payment was $318,832.
“Our current work evaluating data from 2012-2017 is consistent with our prior work dating back to 1985 and demonstrates again that nonphysician operators account for the majority of cases of legal action,” Dr. Khalifian said. “In fact, there is an increasing trend since about 2008 for a higher proportion of cases being performed by physician extenders and nonphysician operators. Despite physicians acting as supervisors and not the actual laser operator they are nonetheless named as defendants in legal claims,” he added.
The data on allegations and causes of legal action “should serve as a guide to help improve patient safety and decrease professional liability,” he pointed out. “It is critical that physicians take steps to mitigate risk to patients by ensuring robust and adequate training for their agents and by directly supervising procedures. However, the data clearly show that the safest treatments are performed directly by physicians who have had such dedicated training in laser and light sources.”
Dr. Khalifian acknowledged certain limitations of the study, including the fact that the data were extracted from only one legal database and did not include cases settled outside of the justice system through third-party arbitration or other means. “It is also limited by search terms in our query,” he said. “It is possible that some cases did not include the terms we used. Finally, only incomplete information was available for some cases even when supplemented through other resources and additional research.”
He reported having no financial disclosures. Study coauthor Mathew M. Avram, MD, JD, serves on the medical advisory board of Sciton and on the scientific advisory boards of Sienna Biopharmaceuticals, Cytrellis, and Allergan. He is also consultant for Merz Aesthetics, Allergan, Soliton, Invasix, and Revance, and has intellectual property with Cytrellis. He also holds stock options with Cytrellis, Invasix, and Zalea.
SOURCE: Khalifian et al. ASLMS 2018.
REPORTING FROM ASLMS 2018
Key clinical point: Claims related to cutaneous laser surgery are steadily increasing, as are the average indemnity payments.
Major finding: Among cases with public decision related to injury secondary to cutaneous laser surgery, nearly half since mid-2012 (47%) have been due to laser rejuvenation.
Study details: An analysis of 32 medical professional liability claims related to cutaneous laser surgery June 2012 through December 2017.
Disclosures: Dr. Khalifian reported having no financial disclosures. Study coauthor Mathew Avram, MD, serves on the medical advisory board of Sciton and on the scientific advisory boards of Sienna Biopharmaceuticals, Cytrellis, and Allergan. He is also consultant for Merz Aesthetics, Allergan, Soliton, Invasix, and Revance, and has intellectual property with Cytrellis. He also holds stock options with Cytrellis, Invasix, and Zalea.
Source: Khalifian et al. ASLMS 2018.