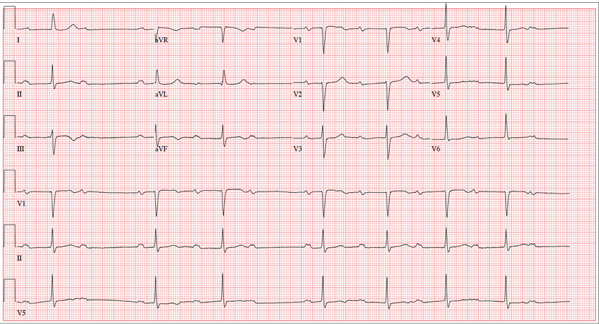
A 74-year-old man presents to your outpatient clinic for a routine appointment. He’s been your patient for years, but you’ve had difficulty convincing him of the importance of taking his hypertension medications regularly. For the most part, he has been compliant; however, recently, with finances becoming tight toward the end of the month, he often takes his β-blocker and diuretic every other day in order to stretch his prescription before refilling it. His health has remained excellent since you last saw him a year ago. However, while performing a review of systems, you learn that his heart rhythm has been “funny” in the past two weeks. He states it hasn’t affected his ability to perform his daily activities, including farming, but it was just “strange.” He denies chest pain, shortness of breath, dizziness, syncope or near-syncope, and peripheral edema. He still manages his 450-acre farm, as he has for most of his adult life. Medical history includes hypertension but no angina, MI, or other cardiac disease. Surgical history is remarkable for a right inguinal hernia repair, an appendectomy, and a right hip replacement. His medications include furosemide, potassium chloride, and metoprolol. He has no known drug allergies and does not use recreational drugs or naturopathic herbs. The patient has been a widower for 12 years. His two sons live nearby and help him on his farm. Due to his religious affiliation, he has never used alcohol or tobacco. Review of systems is remarkable for palpitations and an occasional skipped beat. Vital signs include a blood pressure of 108/58 mm Hg; pulse, 50 beats/min and “irregular”; respiratory rate, 14 breaths/min-1; temperature, 98.4°F; and O2 saturation, 96% on room air. His weight is 176 lb and his height, 74 in. Physical exam reveals a pulse that is regularly irregular at a rate of 56 beats/min. There are no murmurs, rubs, or gallops. The neck veins are not distended, and there is no peripheral edema. His lungs are clear to auscultation, and the remainder of his physical exam is unchanged from his previous visit. Given the change in his heart rhythm since his previous visit, you order an ECG and note the following: a ventricular rate of 44 beats/min; PR interval, not measured; QRS duration, 106 ms; QT/QTc interval, 484/413 ms; P axis, 65°; R axis, 11°; and T axis, 6°. What is your interpretation of this ECG?