Mark Zimmerman, MD Professor of Psychiatry and Human Behavior Warren Alpert Medical School of Brown University Rhode Island Hospital Providence, Rhode Island Member of the Current Psychiatry Editorial Board
Disclosure The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Screening for BPD as part of your diagnostic interview
An alternative approach to using self-administered questionnaires for screening is for clinicians to include questions in their evaluation as part of a psychiatric review of systems. When conducting a diagnostic interview, clinicians typically screen for disorders that are comorbid with the principal diagnosis by asking about the comorbid disorders’ necessary features or “gate criteria.” For example, in a patient with a principal diagnosis of MDD, the clinician would inquire about the presence of panic attacks, excessive worry, or substance use to screen for the presence of panic disorder, generalized anxiety disorder, or a substance use disorder. In contrast, for polythetically defined disorders such as BPD, there is no single gate criterion, because the disorder is diagnosed based on the presence of at least 5 of 9 criteria and no single one of these criteria is required to be present to establish the diagnosis.
As part of the MIDAS project, the psychometric properties of the BPD criteria were examined to determine if it was possible to identify 1 or 2 criteria that could serve as gate criteria to screen for the disorder. If the sensitivity of 1 criterion or a combination of 2 BPD criteria was sufficiently high (ie, >90%), then the assessment of this criterion (or these criteria) could be included in a psychiatric review of systems, thus potentially improving the detection of BPD. Researchers hypothesized that affective instability, considered first by Linehan53 and later by other theorists54 to be of central importance to the clinical manifestations of BPD, could function as a gate criterion. In the sample of 3,674 psychiatric outpatients who were evaluated with a semi-structured interview, the sensitivity of the affective instability criterion was 92.8%, and the negative predictive value of the criterion was 99%.
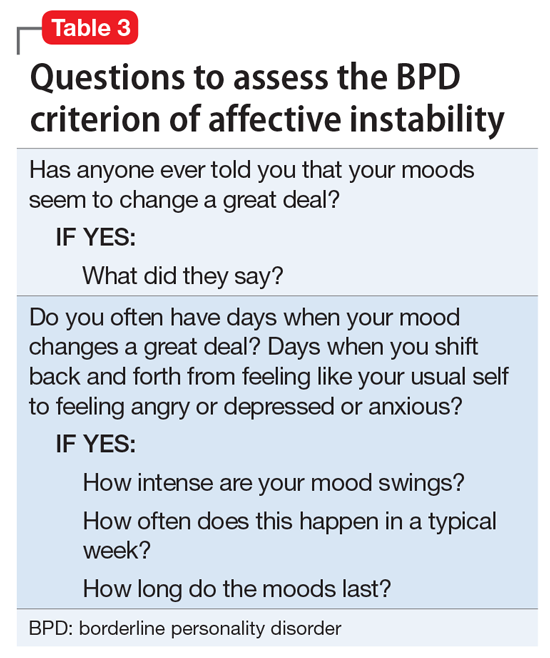
These results from the MIDAS project were consistent with the results of other, smaller studies that found that >90% of patients with BPD report affective instability, and it was the most frequent BPD criterion.55-62 The largest of these studies, the multisite Collaborative Longitudinal Investigation of Personality Study (CLPS), found that sensitivity of affective instability was 94%, which was higher than the sensitivity of the other BPD criteria.62 Moreover, the CLPS examined the sensitivity of the BPD criteria assessed at baseline in relation to a diagnosis of BPD that was made 2 years later.63 Affective instability had a 90% sensitivity and 95% negative predictive value in predicting a future diagnosis of BPD. Both of these figures were the highest of the BPD criteria. Other studies have found a negative predictive value >95%.55,58-61 Therefore,a clinician can be highly confident in ruling out a diagnosis of BPD in patients who do not report affective instability. Table 3 lists questions used to assess affective instability in semi-structured interviews.
Identifying a single BPD criterion that is present in the vast majority of patients diagnosed with BPD will allow clinicians to follow their usual clinical practice when conducting a psychiatric review of systems and inquire about the gate criteria of various disorders. Several studies have found that >90% of patients with BPD report affective instability. However, this does not mean that the diagnosis of BPD can be abbreviated to an assessment of the presence or absence of affective instability. Many patients who screen positive will not have BPD when a more definitive diagnostic evaluation is conducted. In the case of BPD, the more costly definitive diagnostic procedure simply entails inquiry of the other diagnostic criteria.
Bottom Line
BPD is underdiagnosed in clinical practice. Detection of BPD can be improved by careful clinical evaluations that inquire about the features of BPD and the use of screening questionnaires. Affective instability may serve as a gate criterion that can be used to rule out BPD or prompt a more definitive diagnostic evaluation
Related Resources
Leichsenring F, Leibing E, Kruse J, et al. Borderline personality disorder. Lancet. 2011;377(9759):74-84.