The decrease in stomach size causes a decrease in intrinsic factor from parietal cells, with subsequent inability to appropriately transport vitamin B12. Exclusion of the duodenum also eliminates the site of absorption; therefore, B12 should be replaced orally.11 Megaloblastic anemia is a rarely reported sequela.17,18 Folate deficiency is less common because it can take place in the entire intestine after surgery, even though absorption occurs primarily in the proximal portion of the small intestine.10
Protein deficiency can result in loss of muscle mass and subsequent muscle weakness, edema, and anomalies of the skin, mucosa, and nails.12 It is seen after both types of procedures because of decreased dietary intake from intolerance. Malabsorptive procedures also decrease pepsinogen secretion and reduce the intestinal absorption surface.
Considerations for Orthopedic Surgeons
Wound Healing
Much of our knowledge of the effects of bariatric surgery on skin and wound healing has been gleaned from samples obtained from patients during abdominoplasty or other body-contouring procedures. These samples have all shown a decrease in hydroxyproline, the major constituent of collagen and the main factor in determining the tensile strength of a wound.19 D’Ettorre and colleagues20 performed biopsies of abdominal skin before and after biliopancreatic diversion and noted that tissue proteins, including hydroxyproline, were significantly reduced. Histologic examination revealed disorganized dermal elastic and collagen fibers. In addition, all patients involved in the study had wound-healing problems, with delayed healing of 25 days, compared with 12 days in nonbariatric patients. Deficiencies in vitamins B12, D, and E, as well as folate and total tissue protein, were implicated as causative factors.
Effects on Bone
Malabsorptive procedures decrease bone mineral density (BMD) through their effects on calcium and vitamin D. BMD is also decreased because these procedures lower levels of plasma leptin and ghrelin, increase adiponectin, and reduce estrogen in women.21 The BMD decline correlates with amount of weight lost.22 This complication is not seen in restrictive procedures, even though patients may have decreased calcium and vitamin D levels.23 The exact effect on BMD and on subsequent risk for osteopenia and osteoporosis is difficult to quantify, as obese patients have higher BMD than age-matched controls do, because of increased mechanical loading. In a prospective study, Vilarrasa and colleagues24 found a 10.9% decrease in femoral neck BMD in women 1 year after Roux-en-Y with 34% weight loss, despite supplementation with 800 IU of vitamin D and 1200 mg of calcium daily.
Fracture Healing
Although BMD is decreased in patients after gastric bypass surgery, there has been only 1 recorded case of fracture nonunion after bariatric surgery—involving a distal radius fracture in a patient who had undergone jejunoileal bypass surgery.25 Hypovitaminosis has a detrimental effect on bone repair and BMD, increasing the risk for fracture from minor trauma; however, delayed union and nonunion have not been reported as consequences.26
Pharmacology
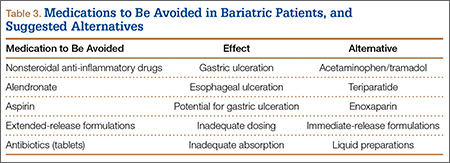
Both restrictive and malabsorptive procedures decrease drug bioavailabilty from tablet preparations by shortening the surface area available for absorption and diminishing stomach acidity.27 These consequences pose a problem particularly for extended-release formulations, as these formulations are not given enough time to dissolve and reach therapeutic concentrations.28 Also affected is warfarin, which requires a larger dose to maintain therapeutic international normalized ratio. Antibiotics may have reduced bioavailability because of decreased transit time. Therefore, liquid preparations are preferred, as they need not be dissolved.
As there is no reported change in intravenous bioavailability with preoperative and postoperative antimicrobial prophylaxis, this is the preferred administration method.29 However, obese patients in general may have altered pharmacokinetics, including increased glomerular filtration rate, and in most cases they should be treated with higher levels of antibiotics.30
Nonsteroidal anti-inflammatory drugs (NSAIDs) should be avoided in all patients. The acidic composition of NSAIDs causes direct injury to the gastric pouch. NSAIDs also injure the gastrointestinal lining by inhibiting prostaglandin synthesis, which thins the mucosa. In turn, erosions and ulcers may form in the epithelial layer.31 Acetaminophen or a centrally acting agent (eg, tramadol) is recommended instead. Aspirin has a chemical structure similar to that of NSAIDs and should not be used either. Alendronate causes esophageal ulceration; however, no such complication has been reported with teriparatide32 (Table 3).
Preoperative Evaluation
As already discussed, patients who undergo weight-loss surgery are at higher risk for wound-healing complications because of nutritional deficiencies. Total protein, albumin, and prealbumin levels and total lymphocyte count should be used to identify protein deficiency, which can decrease the likelihood of organized collagen formation. Huang and colleagues33 noted a statistically significant increase in complications after total knee arthroplasty (TKA) in patients with a prealbumin level under 3.5 mg/dL or a transferrin level under 200 mg/dL. Rates of prosthetic joint infection and development of hematoma or seroma requiring operative management were much higher, as were rates of postoperative neurovascular, renal, and cardiovascular complications.