User login
ADHD in the long term
Parents whose kids are diagnosed with ADHD face important questions about what to expect in the long term and how that might inform treatment. Studies find that ADHD diagnosed in childhood tends to persist in up to 65% of adolescents (some estimates are lower depending on criteria used),1 and about 50% of people are estimated to continue to meet criteria for ADHD as adults.2 Many studies have attempted to understand what long-term risks are associated with ADHD, as well as the factors that help better predict which characteristics in childhood might predict those risks. A recent article was published on a cohort of boys followed over 33 years.3 This, as well as other large prospective studies, such as the Multimodal Treatment of ADHD (MTA) provide us with helpful long-range data that inform this article.4-6 This article reviews risks in adolescence and adulthood and the factors thought to be associated with them.

What predicts persistence of ADHD symptoms in adolescence?
Several factors emerge consistently, including higher symptom severity, comorbid conduct disorder, and lower childhood IQ; other findings include family-related factors, such as lower parental mental health, less-positive parenting, and lower rates of parental education. In general, hyperactivity and impulsivity wanes, while inattention symptoms remain more stable.
What does ADHD predict for adolescents?
Adolescents with ADHD are more than twice as likely to be involved in pregnancies under the age of 18 years, true for both male and female genders.7 This finding also is associated with increased substance use and low academic achievement but not completely explained by it. Adolescents with persistent ADHD symptoms experience poorer educational success than do kids without ADHD symptoms, according to teacher reports of performance and measurements of grade point average. They are more likely to repeat a grade.8 Related but independent is the relationship of substance use disorders in kids with ADHD. Adolescents with ADHD are more likely to use nicotine or marijuana or meet criteria for any substance use disorder than adolescents without ADHD. Finally, adolescents aged 12-18 years with ADHD are at higher risk for motor vehicle accidents and all types of accidental injuries.9
What predicts persistence of ADHD symptoms in adulthood?
A follow-up study of the MTA trial 16 years later looked at ADHD diagnosed before age 12 years and the association with symptom persistence in adulthood, defined by the DSM-5 cutoff criteria of five symptoms. The following factors related to symptom persistence: childhood psychiatric comorbidity, higher ADHD symptom severity, and parental mental health problems. Notably, family socioeconomic status, child IQ, and parental education were not associated. In addition to looking at symptom persistence, other studies have looked at predictors of functional impairment in adulthood following a childhood ADHD diagnosis (independent of whether people continue to meet criteria for the disorder). The main findings that seem consistently related to all functional outcomes, including social, occupational, and educational, are lower childhood IQ and history of conduct problems (in the absence of meeting criteria for full childhood conduct disorder). Educational family-related factors, such as socioeconomic status and lower parental education, were related to lower educational functioning only.
What does ADHD predict for adults?
It appears that overall, adults who were diagnosed with ADHD as children show poorer functional outcomes than did those who weren’t, and there is a step-wise relationship when considering adults whose symptoms persist, with more severe outcomes compared with adults whose symptoms have desisted, who in turn have worse outcomes than adults who were never diagnosed with ADHD. Educational attainments follow this pattern with the highest average levels of education in the non-ADHD group and the lowest average years in the group with persistent symptoms. Occupational success and percent receiving public assistance again separated between each group, with the symptom persisters faring the worst, the symptom desisters better, and those never affected by ADHD, the best. In terms of emotional disorders, it was only the symptom persisters who suffered from higher rates of mood and anxiety disorders. Similarly, only the symptom persisters had significantly more marijuana use disorders. No other substance use disorders or legal outcomes were significant.
How does this affect how we approach treatment?
Clinicians and researchers who specialize in ADHD have been arguing for ADHD to be treated as more of a chronic disease and for impairment to be the focus of treatment, rather than simply symptom control.10 With what we know about long-term functional impairment, there is reason to consider a more holistic picture of a child or an adolescent and how they are functioning in their academic, emotional, and social domains. A meta-analysis of treatment and long-term outcomes suggests that psychostimulant treatment, psychotherapy treatment, and combined treatment all improve long-term functioning, especially self-esteem, social functioning, and academic functioning, with combined psychotherapeutic and pharmacologic treatments associated with the highest effect sizes.11

For those who treat ADHD, it is our job to provide education to families about the chronic risks associated with the diagnosis, and the importance of offering multimodal therapy that can address family factors that might be contributing to risks, as well as the child’s overall well-being. If we are to make sense of how adults may experience impairment even in the absence of ongoing symptoms, we might look at how their overall wellness was interrupted during development. Maybe they fell into a different crowd of kids? Maybe they stopped achieving at school in a way that changed the achievement trajectory they were on? Maybe they impulsively picked up substances or got in trouble with the law? These events can have lasting impacts on well-being. We must use medicine and psychotherapy to help with symptoms, but we must look beyond treating illness and use evidence-based strategies to promote wellness at the level of the entire family.
Dr. Guth is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and the University of Vermont, both in Burlington. She works with children and adolescents as well as women in the perinatal period. She has no relevant financial disclosures.
References
1. Psychol Med. 2006 Feb;36(2):159-65.
2. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):937-44.e4.
3. J Am Acad Child Adolesc Psychiatry. 2018 Aug;57(8):571-82.e1.
4. J Am Acad Child Adolesc Psychiatry. 2017 Aug;56(8):687-95.e7.
5. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):945-52.e2.
6. J Am Acad Child Adolesc Psychiatry. 2009 May;48(5):484-500.
7. J Atten Disord. 2017 Sep 1:1087054717730610. doi: 10.1177/1087054717730610.
8. J Atten Disord. 2016 May;20(5):383-9.
9. Eur Child Adolesc Psychiatry. 2014 Feb;23(2):95-102.
10. JAMA Pediatr. 2018 Aug 13. doi: 10.1001/jamapediatrics.2018.1642.
11. PLoS One. 2015 Feb 25;10(2):e0116407.
Parents whose kids are diagnosed with ADHD face important questions about what to expect in the long term and how that might inform treatment. Studies find that ADHD diagnosed in childhood tends to persist in up to 65% of adolescents (some estimates are lower depending on criteria used),1 and about 50% of people are estimated to continue to meet criteria for ADHD as adults.2 Many studies have attempted to understand what long-term risks are associated with ADHD, as well as the factors that help better predict which characteristics in childhood might predict those risks. A recent article was published on a cohort of boys followed over 33 years.3 This, as well as other large prospective studies, such as the Multimodal Treatment of ADHD (MTA) provide us with helpful long-range data that inform this article.4-6 This article reviews risks in adolescence and adulthood and the factors thought to be associated with them.
What predicts persistence of ADHD symptoms in adolescence?
Several factors emerge consistently, including higher symptom severity, comorbid conduct disorder, and lower childhood IQ; other findings include family-related factors, such as lower parental mental health, less-positive parenting, and lower rates of parental education. In general, hyperactivity and impulsivity wanes, while inattention symptoms remain more stable.
What does ADHD predict for adolescents?
Adolescents with ADHD are more than twice as likely to be involved in pregnancies under the age of 18 years, true for both male and female genders.7 This finding also is associated with increased substance use and low academic achievement but not completely explained by it. Adolescents with persistent ADHD symptoms experience poorer educational success than do kids without ADHD symptoms, according to teacher reports of performance and measurements of grade point average. They are more likely to repeat a grade.8 Related but independent is the relationship of substance use disorders in kids with ADHD. Adolescents with ADHD are more likely to use nicotine or marijuana or meet criteria for any substance use disorder than adolescents without ADHD. Finally, adolescents aged 12-18 years with ADHD are at higher risk for motor vehicle accidents and all types of accidental injuries.9
What predicts persistence of ADHD symptoms in adulthood?
A follow-up study of the MTA trial 16 years later looked at ADHD diagnosed before age 12 years and the association with symptom persistence in adulthood, defined by the DSM-5 cutoff criteria of five symptoms. The following factors related to symptom persistence: childhood psychiatric comorbidity, higher ADHD symptom severity, and parental mental health problems. Notably, family socioeconomic status, child IQ, and parental education were not associated. In addition to looking at symptom persistence, other studies have looked at predictors of functional impairment in adulthood following a childhood ADHD diagnosis (independent of whether people continue to meet criteria for the disorder). The main findings that seem consistently related to all functional outcomes, including social, occupational, and educational, are lower childhood IQ and history of conduct problems (in the absence of meeting criteria for full childhood conduct disorder). Educational family-related factors, such as socioeconomic status and lower parental education, were related to lower educational functioning only.
What does ADHD predict for adults?
It appears that overall, adults who were diagnosed with ADHD as children show poorer functional outcomes than did those who weren’t, and there is a step-wise relationship when considering adults whose symptoms persist, with more severe outcomes compared with adults whose symptoms have desisted, who in turn have worse outcomes than adults who were never diagnosed with ADHD. Educational attainments follow this pattern with the highest average levels of education in the non-ADHD group and the lowest average years in the group with persistent symptoms. Occupational success and percent receiving public assistance again separated between each group, with the symptom persisters faring the worst, the symptom desisters better, and those never affected by ADHD, the best. In terms of emotional disorders, it was only the symptom persisters who suffered from higher rates of mood and anxiety disorders. Similarly, only the symptom persisters had significantly more marijuana use disorders. No other substance use disorders or legal outcomes were significant.
How does this affect how we approach treatment?
Clinicians and researchers who specialize in ADHD have been arguing for ADHD to be treated as more of a chronic disease and for impairment to be the focus of treatment, rather than simply symptom control.10 With what we know about long-term functional impairment, there is reason to consider a more holistic picture of a child or an adolescent and how they are functioning in their academic, emotional, and social domains. A meta-analysis of treatment and long-term outcomes suggests that psychostimulant treatment, psychotherapy treatment, and combined treatment all improve long-term functioning, especially self-esteem, social functioning, and academic functioning, with combined psychotherapeutic and pharmacologic treatments associated with the highest effect sizes.11
For those who treat ADHD, it is our job to provide education to families about the chronic risks associated with the diagnosis, and the importance of offering multimodal therapy that can address family factors that might be contributing to risks, as well as the child’s overall well-being. If we are to make sense of how adults may experience impairment even in the absence of ongoing symptoms, we might look at how their overall wellness was interrupted during development. Maybe they fell into a different crowd of kids? Maybe they stopped achieving at school in a way that changed the achievement trajectory they were on? Maybe they impulsively picked up substances or got in trouble with the law? These events can have lasting impacts on well-being. We must use medicine and psychotherapy to help with symptoms, but we must look beyond treating illness and use evidence-based strategies to promote wellness at the level of the entire family.
Dr. Guth is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and the University of Vermont, both in Burlington. She works with children and adolescents as well as women in the perinatal period. She has no relevant financial disclosures.
References
1. Psychol Med. 2006 Feb;36(2):159-65.
2. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):937-44.e4.
3. J Am Acad Child Adolesc Psychiatry. 2018 Aug;57(8):571-82.e1.
4. J Am Acad Child Adolesc Psychiatry. 2017 Aug;56(8):687-95.e7.
5. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):945-52.e2.
6. J Am Acad Child Adolesc Psychiatry. 2009 May;48(5):484-500.
7. J Atten Disord. 2017 Sep 1:1087054717730610. doi: 10.1177/1087054717730610.
8. J Atten Disord. 2016 May;20(5):383-9.
9. Eur Child Adolesc Psychiatry. 2014 Feb;23(2):95-102.
10. JAMA Pediatr. 2018 Aug 13. doi: 10.1001/jamapediatrics.2018.1642.
11. PLoS One. 2015 Feb 25;10(2):e0116407.
Parents whose kids are diagnosed with ADHD face important questions about what to expect in the long term and how that might inform treatment. Studies find that ADHD diagnosed in childhood tends to persist in up to 65% of adolescents (some estimates are lower depending on criteria used),1 and about 50% of people are estimated to continue to meet criteria for ADHD as adults.2 Many studies have attempted to understand what long-term risks are associated with ADHD, as well as the factors that help better predict which characteristics in childhood might predict those risks. A recent article was published on a cohort of boys followed over 33 years.3 This, as well as other large prospective studies, such as the Multimodal Treatment of ADHD (MTA) provide us with helpful long-range data that inform this article.4-6 This article reviews risks in adolescence and adulthood and the factors thought to be associated with them.
What predicts persistence of ADHD symptoms in adolescence?
Several factors emerge consistently, including higher symptom severity, comorbid conduct disorder, and lower childhood IQ; other findings include family-related factors, such as lower parental mental health, less-positive parenting, and lower rates of parental education. In general, hyperactivity and impulsivity wanes, while inattention symptoms remain more stable.
What does ADHD predict for adolescents?
Adolescents with ADHD are more than twice as likely to be involved in pregnancies under the age of 18 years, true for both male and female genders.7 This finding also is associated with increased substance use and low academic achievement but not completely explained by it. Adolescents with persistent ADHD symptoms experience poorer educational success than do kids without ADHD symptoms, according to teacher reports of performance and measurements of grade point average. They are more likely to repeat a grade.8 Related but independent is the relationship of substance use disorders in kids with ADHD. Adolescents with ADHD are more likely to use nicotine or marijuana or meet criteria for any substance use disorder than adolescents without ADHD. Finally, adolescents aged 12-18 years with ADHD are at higher risk for motor vehicle accidents and all types of accidental injuries.9
What predicts persistence of ADHD symptoms in adulthood?
A follow-up study of the MTA trial 16 years later looked at ADHD diagnosed before age 12 years and the association with symptom persistence in adulthood, defined by the DSM-5 cutoff criteria of five symptoms. The following factors related to symptom persistence: childhood psychiatric comorbidity, higher ADHD symptom severity, and parental mental health problems. Notably, family socioeconomic status, child IQ, and parental education were not associated. In addition to looking at symptom persistence, other studies have looked at predictors of functional impairment in adulthood following a childhood ADHD diagnosis (independent of whether people continue to meet criteria for the disorder). The main findings that seem consistently related to all functional outcomes, including social, occupational, and educational, are lower childhood IQ and history of conduct problems (in the absence of meeting criteria for full childhood conduct disorder). Educational family-related factors, such as socioeconomic status and lower parental education, were related to lower educational functioning only.
What does ADHD predict for adults?
It appears that overall, adults who were diagnosed with ADHD as children show poorer functional outcomes than did those who weren’t, and there is a step-wise relationship when considering adults whose symptoms persist, with more severe outcomes compared with adults whose symptoms have desisted, who in turn have worse outcomes than adults who were never diagnosed with ADHD. Educational attainments follow this pattern with the highest average levels of education in the non-ADHD group and the lowest average years in the group with persistent symptoms. Occupational success and percent receiving public assistance again separated between each group, with the symptom persisters faring the worst, the symptom desisters better, and those never affected by ADHD, the best. In terms of emotional disorders, it was only the symptom persisters who suffered from higher rates of mood and anxiety disorders. Similarly, only the symptom persisters had significantly more marijuana use disorders. No other substance use disorders or legal outcomes were significant.
How does this affect how we approach treatment?
Clinicians and researchers who specialize in ADHD have been arguing for ADHD to be treated as more of a chronic disease and for impairment to be the focus of treatment, rather than simply symptom control.10 With what we know about long-term functional impairment, there is reason to consider a more holistic picture of a child or an adolescent and how they are functioning in their academic, emotional, and social domains. A meta-analysis of treatment and long-term outcomes suggests that psychostimulant treatment, psychotherapy treatment, and combined treatment all improve long-term functioning, especially self-esteem, social functioning, and academic functioning, with combined psychotherapeutic and pharmacologic treatments associated with the highest effect sizes.11
For those who treat ADHD, it is our job to provide education to families about the chronic risks associated with the diagnosis, and the importance of offering multimodal therapy that can address family factors that might be contributing to risks, as well as the child’s overall well-being. If we are to make sense of how adults may experience impairment even in the absence of ongoing symptoms, we might look at how their overall wellness was interrupted during development. Maybe they fell into a different crowd of kids? Maybe they stopped achieving at school in a way that changed the achievement trajectory they were on? Maybe they impulsively picked up substances or got in trouble with the law? These events can have lasting impacts on well-being. We must use medicine and psychotherapy to help with symptoms, but we must look beyond treating illness and use evidence-based strategies to promote wellness at the level of the entire family.
Dr. Guth is an assistant professor in the department of psychiatry at the University of Vermont Medical Center and the University of Vermont, both in Burlington. She works with children and adolescents as well as women in the perinatal period. She has no relevant financial disclosures.
References
1. Psychol Med. 2006 Feb;36(2):159-65.
2. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):937-44.e4.
3. J Am Acad Child Adolesc Psychiatry. 2018 Aug;57(8):571-82.e1.
4. J Am Acad Child Adolesc Psychiatry. 2017 Aug;56(8):687-95.e7.
5. J Am Acad Child Adolesc Psychiatry. 2016 Nov;55(11):945-52.e2.
6. J Am Acad Child Adolesc Psychiatry. 2009 May;48(5):484-500.
7. J Atten Disord. 2017 Sep 1:1087054717730610. doi: 10.1177/1087054717730610.
8. J Atten Disord. 2016 May;20(5):383-9.
9. Eur Child Adolesc Psychiatry. 2014 Feb;23(2):95-102.
10. JAMA Pediatr. 2018 Aug 13. doi: 10.1001/jamapediatrics.2018.1642.
11. PLoS One. 2015 Feb 25;10(2):e0116407.
Over past 20 years, the percentage of children with ADHD nearly doubles
The number of children diagnosed with ADHD has reached more than 10%, a significant increase during the past 20 years, according to a recent study in JAMA.
The rise was most pronounced in minority groups, suggesting that better access to health insurance and mental health treatment through the Affordable Care Act might have played some role in the increase. The rate of diagnosis during that time period doubled in girls, although it was still much lower than in boys.
But the researchers say they found no evidence confirming frequent complaints that the condition is overdiagnosed or misdiagnosed.
The United States has significantly more instances of ADHD than do other developed countries, which researchers said has led some to think Americans are overdiagnosing children. Wei Bao, MD, PhD, lead author of the study, said in an interview that a review of studies around the world does not support that.
”I don’t think overdiagnosis is the main issue,” he said.
Nonetheless, those doubts persist. Stephen Hinshaw, MD, who coauthored a 2014 book called “The ADHD Explosion: Myths, Medication, Money, and Today’s Push for Performance,” compared ADHD with depression. He said in an interview that neither condition has unequivocal biological markers, which makes it hard to determine if a patient truly has the condition without lengthy psychological evaluations. Symptoms of ADHD can include inattention, fidgety behavior, and impulsivity.
“It’s probably not a true epidemic of ADHD,” said Dr. Hinshaw, a professor of psychology at the University of California, Berkeley, and a professor of psychiatry at University of California, San Francisco. “It might be an epidemic of diagnosing it.”
In interpreting their results, however, the study’s authors tied the higher numbers to better understanding of the condition by doctors and the public, new standards for diagnosis and an increase in access to health insurance through the ACA.
Because of the ACA, “some low-income families have improved access to services and referrals,” said Dr. Bao, an epidemiologist at the University of Iowa College of Public Health in Iowa City.
The study, published in JAMA Network Open, used data from the National Health Interview Survey, an annual federal survey of about 35,000 households. It found a steady increase in diagnoses in children from about 6% during 1997-1998 to more than 10% during 2015-2016.
Advances in medical technology also may have contributed to the increase, according to the research. Twenty years ago, preterm or low-birth-weight babies had a harder time surviving. Those factors increase the risk of being diagnosed with ADHD.
The study also suggests that fewer stigmas about mental health care in minority communities also may lead to more people receiving an ADHD diagnosis.
In the late 1990s, 7.2% of non-Hispanic white children, 4.7% of non-Hispanic black children, and 3.6% of Hispanic children were diagnosed with ADHD, according to the study. By 2016, it was 12% of white kids, 12.8% of blacks, and 6.1% of Hispanics.
Over the past several decades, Dr. Hinshaw said, there’s been an expanded view of who can develop ADHD. It’s no longer viewed as a disease that affects only white middle-class boys, as eating disorders are no longer seen as afflicting only white middle-class girls.
Still, he cautioned against overdiagnosing ADHD in communities in which behavioral issues could be the result of social or environmental factors such as overcrowded classrooms.
The study found rates of ADHD among girls rose from 3% to more than 6% over the study period. It said that was partly a result of a change in how the condition is classified. For years, ADHD pertained to children who were hyperactive. But in recent years, the American Psychiatric Association added to its guide of mental health conditions that diagnosis should also include some children who are inattentive, Dr. Bao said. That raised the number of girls, he explained, because it seems they are more likely to be in that second subtype.
“If we compare these two, you can easily imagine people will easily recognize hyperactivity,” he said.
That rang true for Ruth Hay, a 25-year-old student and cook from New York who now lives in Jerusalem. She was diagnosed with what was then called ADD the summer between second and third grade.
Ms. Hay said her hyperactive tendencies aren’t as “loud” as some people’s. She’s less likely to bounce around a room than she is to bounce in her chair, she said.
Yet, despite her early diagnosis, Ms. Hay said, no one ever told her about other symptoms. For example, she said, she suffers from executive dysfunction, which leaves her feeling unable to accomplish tasks, no matter how much she wanted to or tried.
“I grew up being called lazy in periods of time when I wasn’t,” Ms. Hay said. “If you look at a list of all the various ADHD symptoms, I have all of them to one degree or another, but the only ones ever discussed with me was you might be less focused and more fidgety.”
“I don’t know how my brain would be if I didn’t have it,” she added. “I don’t know if I’d still be me, but all it has been for me is a disability.”
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The number of children diagnosed with ADHD has reached more than 10%, a significant increase during the past 20 years, according to a recent study in JAMA.
The rise was most pronounced in minority groups, suggesting that better access to health insurance and mental health treatment through the Affordable Care Act might have played some role in the increase. The rate of diagnosis during that time period doubled in girls, although it was still much lower than in boys.
But the researchers say they found no evidence confirming frequent complaints that the condition is overdiagnosed or misdiagnosed.
The United States has significantly more instances of ADHD than do other developed countries, which researchers said has led some to think Americans are overdiagnosing children. Wei Bao, MD, PhD, lead author of the study, said in an interview that a review of studies around the world does not support that.
”I don’t think overdiagnosis is the main issue,” he said.
Nonetheless, those doubts persist. Stephen Hinshaw, MD, who coauthored a 2014 book called “The ADHD Explosion: Myths, Medication, Money, and Today’s Push for Performance,” compared ADHD with depression. He said in an interview that neither condition has unequivocal biological markers, which makes it hard to determine if a patient truly has the condition without lengthy psychological evaluations. Symptoms of ADHD can include inattention, fidgety behavior, and impulsivity.
“It’s probably not a true epidemic of ADHD,” said Dr. Hinshaw, a professor of psychology at the University of California, Berkeley, and a professor of psychiatry at University of California, San Francisco. “It might be an epidemic of diagnosing it.”
In interpreting their results, however, the study’s authors tied the higher numbers to better understanding of the condition by doctors and the public, new standards for diagnosis and an increase in access to health insurance through the ACA.
Because of the ACA, “some low-income families have improved access to services and referrals,” said Dr. Bao, an epidemiologist at the University of Iowa College of Public Health in Iowa City.
The study, published in JAMA Network Open, used data from the National Health Interview Survey, an annual federal survey of about 35,000 households. It found a steady increase in diagnoses in children from about 6% during 1997-1998 to more than 10% during 2015-2016.
Advances in medical technology also may have contributed to the increase, according to the research. Twenty years ago, preterm or low-birth-weight babies had a harder time surviving. Those factors increase the risk of being diagnosed with ADHD.
The study also suggests that fewer stigmas about mental health care in minority communities also may lead to more people receiving an ADHD diagnosis.
In the late 1990s, 7.2% of non-Hispanic white children, 4.7% of non-Hispanic black children, and 3.6% of Hispanic children were diagnosed with ADHD, according to the study. By 2016, it was 12% of white kids, 12.8% of blacks, and 6.1% of Hispanics.
Over the past several decades, Dr. Hinshaw said, there’s been an expanded view of who can develop ADHD. It’s no longer viewed as a disease that affects only white middle-class boys, as eating disorders are no longer seen as afflicting only white middle-class girls.
Still, he cautioned against overdiagnosing ADHD in communities in which behavioral issues could be the result of social or environmental factors such as overcrowded classrooms.
The study found rates of ADHD among girls rose from 3% to more than 6% over the study period. It said that was partly a result of a change in how the condition is classified. For years, ADHD pertained to children who were hyperactive. But in recent years, the American Psychiatric Association added to its guide of mental health conditions that diagnosis should also include some children who are inattentive, Dr. Bao said. That raised the number of girls, he explained, because it seems they are more likely to be in that second subtype.
“If we compare these two, you can easily imagine people will easily recognize hyperactivity,” he said.
That rang true for Ruth Hay, a 25-year-old student and cook from New York who now lives in Jerusalem. She was diagnosed with what was then called ADD the summer between second and third grade.
Ms. Hay said her hyperactive tendencies aren’t as “loud” as some people’s. She’s less likely to bounce around a room than she is to bounce in her chair, she said.
Yet, despite her early diagnosis, Ms. Hay said, no one ever told her about other symptoms. For example, she said, she suffers from executive dysfunction, which leaves her feeling unable to accomplish tasks, no matter how much she wanted to or tried.
“I grew up being called lazy in periods of time when I wasn’t,” Ms. Hay said. “If you look at a list of all the various ADHD symptoms, I have all of them to one degree or another, but the only ones ever discussed with me was you might be less focused and more fidgety.”
“I don’t know how my brain would be if I didn’t have it,” she added. “I don’t know if I’d still be me, but all it has been for me is a disability.”
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The number of children diagnosed with ADHD has reached more than 10%, a significant increase during the past 20 years, according to a recent study in JAMA.
The rise was most pronounced in minority groups, suggesting that better access to health insurance and mental health treatment through the Affordable Care Act might have played some role in the increase. The rate of diagnosis during that time period doubled in girls, although it was still much lower than in boys.
But the researchers say they found no evidence confirming frequent complaints that the condition is overdiagnosed or misdiagnosed.
The United States has significantly more instances of ADHD than do other developed countries, which researchers said has led some to think Americans are overdiagnosing children. Wei Bao, MD, PhD, lead author of the study, said in an interview that a review of studies around the world does not support that.
”I don’t think overdiagnosis is the main issue,” he said.
Nonetheless, those doubts persist. Stephen Hinshaw, MD, who coauthored a 2014 book called “The ADHD Explosion: Myths, Medication, Money, and Today’s Push for Performance,” compared ADHD with depression. He said in an interview that neither condition has unequivocal biological markers, which makes it hard to determine if a patient truly has the condition without lengthy psychological evaluations. Symptoms of ADHD can include inattention, fidgety behavior, and impulsivity.
“It’s probably not a true epidemic of ADHD,” said Dr. Hinshaw, a professor of psychology at the University of California, Berkeley, and a professor of psychiatry at University of California, San Francisco. “It might be an epidemic of diagnosing it.”
In interpreting their results, however, the study’s authors tied the higher numbers to better understanding of the condition by doctors and the public, new standards for diagnosis and an increase in access to health insurance through the ACA.
Because of the ACA, “some low-income families have improved access to services and referrals,” said Dr. Bao, an epidemiologist at the University of Iowa College of Public Health in Iowa City.
The study, published in JAMA Network Open, used data from the National Health Interview Survey, an annual federal survey of about 35,000 households. It found a steady increase in diagnoses in children from about 6% during 1997-1998 to more than 10% during 2015-2016.
Advances in medical technology also may have contributed to the increase, according to the research. Twenty years ago, preterm or low-birth-weight babies had a harder time surviving. Those factors increase the risk of being diagnosed with ADHD.
The study also suggests that fewer stigmas about mental health care in minority communities also may lead to more people receiving an ADHD diagnosis.
In the late 1990s, 7.2% of non-Hispanic white children, 4.7% of non-Hispanic black children, and 3.6% of Hispanic children were diagnosed with ADHD, according to the study. By 2016, it was 12% of white kids, 12.8% of blacks, and 6.1% of Hispanics.
Over the past several decades, Dr. Hinshaw said, there’s been an expanded view of who can develop ADHD. It’s no longer viewed as a disease that affects only white middle-class boys, as eating disorders are no longer seen as afflicting only white middle-class girls.
Still, he cautioned against overdiagnosing ADHD in communities in which behavioral issues could be the result of social or environmental factors such as overcrowded classrooms.
The study found rates of ADHD among girls rose from 3% to more than 6% over the study period. It said that was partly a result of a change in how the condition is classified. For years, ADHD pertained to children who were hyperactive. But in recent years, the American Psychiatric Association added to its guide of mental health conditions that diagnosis should also include some children who are inattentive, Dr. Bao said. That raised the number of girls, he explained, because it seems they are more likely to be in that second subtype.
“If we compare these two, you can easily imagine people will easily recognize hyperactivity,” he said.
That rang true for Ruth Hay, a 25-year-old student and cook from New York who now lives in Jerusalem. She was diagnosed with what was then called ADD the summer between second and third grade.
Ms. Hay said her hyperactive tendencies aren’t as “loud” as some people’s. She’s less likely to bounce around a room than she is to bounce in her chair, she said.
Yet, despite her early diagnosis, Ms. Hay said, no one ever told her about other symptoms. For example, she said, she suffers from executive dysfunction, which leaves her feeling unable to accomplish tasks, no matter how much she wanted to or tried.
“I grew up being called lazy in periods of time when I wasn’t,” Ms. Hay said. “If you look at a list of all the various ADHD symptoms, I have all of them to one degree or another, but the only ones ever discussed with me was you might be less focused and more fidgety.”
“I don’t know how my brain would be if I didn’t have it,” she added. “I don’t know if I’d still be me, but all it has been for me is a disability.”
KHN’s coverage of children’s health care issues is supported in part by the Heising-Simons Foundation.
Kaiser Health News is a nonprofit national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Schools’ cell phone policies: What’s best for students?
Schools across the country – or around the world, for that matter – are grappling with policies and regulations tied to their students’ use of cell phones during school hours.

These policies run the gamut, from allowing students to use smartphones as learning tools to requiring them to keep the devices turned off. One public high school’s action on cell phones, initiated this year by a parent, has prompted one parent’s thumbs-up. This school is phasing in a lock-up-your-cell-phone policy.
NPR reporter Jennifer Ludden said that when the idea was first floated toward the end of the last school year, it provoked a parental outcry at her sons’ school. “My generation is used to 24/7 access to our kids, wherever they are. I confess, I’ve texted mine at school. It was about a doctor’s appointment,” Ms. Ludden says.
Meanwhile, she says, some asked: “ ‘What if there’s an emergency?’ It’s a fair question. We’ve all heard about students hiding from a gunman, posting updates, and texting to let friends and family know they’re safe,” she says.
Yet, evidence suggests that a cell-free classroom is a safer classroom, without the distraction of that screen to divert attention instructions that come in the wake of a school emergency. And, in a chilling mental image, a phone’s ringtone or vibration on a desk could be a beacon for a shooter.
Putting aside the horrific potential of school violence, a no-phone policy could have other tangible benefits that would help students in real life. The rejigging of adolescent brains away from the umbilical cord of their phone would be welcome. Imagine social interactions, instead of that face-down, thumbs-poised posture that is everywhere! And it could also help curb the electronic version of passing notes during tests.
Ms. Ludden mentions another benefit. “ Invaluable time to relax, and connect, without phones. I’m grateful to see some schools investing in that,” Ms. Ludden says.
Click here to listen to Ms. Ludden’s take.
Schools across the country – or around the world, for that matter – are grappling with policies and regulations tied to their students’ use of cell phones during school hours.
These policies run the gamut, from allowing students to use smartphones as learning tools to requiring them to keep the devices turned off. One public high school’s action on cell phones, initiated this year by a parent, has prompted one parent’s thumbs-up. This school is phasing in a lock-up-your-cell-phone policy.
NPR reporter Jennifer Ludden said that when the idea was first floated toward the end of the last school year, it provoked a parental outcry at her sons’ school. “My generation is used to 24/7 access to our kids, wherever they are. I confess, I’ve texted mine at school. It was about a doctor’s appointment,” Ms. Ludden says.
Meanwhile, she says, some asked: “ ‘What if there’s an emergency?’ It’s a fair question. We’ve all heard about students hiding from a gunman, posting updates, and texting to let friends and family know they’re safe,” she says.
Yet, evidence suggests that a cell-free classroom is a safer classroom, without the distraction of that screen to divert attention instructions that come in the wake of a school emergency. And, in a chilling mental image, a phone’s ringtone or vibration on a desk could be a beacon for a shooter.
Putting aside the horrific potential of school violence, a no-phone policy could have other tangible benefits that would help students in real life. The rejigging of adolescent brains away from the umbilical cord of their phone would be welcome. Imagine social interactions, instead of that face-down, thumbs-poised posture that is everywhere! And it could also help curb the electronic version of passing notes during tests.
Ms. Ludden mentions another benefit. “ Invaluable time to relax, and connect, without phones. I’m grateful to see some schools investing in that,” Ms. Ludden says.
Click here to listen to Ms. Ludden’s take.
Schools across the country – or around the world, for that matter – are grappling with policies and regulations tied to their students’ use of cell phones during school hours.
These policies run the gamut, from allowing students to use smartphones as learning tools to requiring them to keep the devices turned off. One public high school’s action on cell phones, initiated this year by a parent, has prompted one parent’s thumbs-up. This school is phasing in a lock-up-your-cell-phone policy.
NPR reporter Jennifer Ludden said that when the idea was first floated toward the end of the last school year, it provoked a parental outcry at her sons’ school. “My generation is used to 24/7 access to our kids, wherever they are. I confess, I’ve texted mine at school. It was about a doctor’s appointment,” Ms. Ludden says.
Meanwhile, she says, some asked: “ ‘What if there’s an emergency?’ It’s a fair question. We’ve all heard about students hiding from a gunman, posting updates, and texting to let friends and family know they’re safe,” she says.
Yet, evidence suggests that a cell-free classroom is a safer classroom, without the distraction of that screen to divert attention instructions that come in the wake of a school emergency. And, in a chilling mental image, a phone’s ringtone or vibration on a desk could be a beacon for a shooter.
Putting aside the horrific potential of school violence, a no-phone policy could have other tangible benefits that would help students in real life. The rejigging of adolescent brains away from the umbilical cord of their phone would be welcome. Imagine social interactions, instead of that face-down, thumbs-poised posture that is everywhere! And it could also help curb the electronic version of passing notes during tests.
Ms. Ludden mentions another benefit. “ Invaluable time to relax, and connect, without phones. I’m grateful to see some schools investing in that,” Ms. Ludden says.
Click here to listen to Ms. Ludden’s take.
Alopecia areata linked to mental health disorders
Alopecia areata is associated with greater frequency of mental health disorders, according to a new analysis of U.S. hospitalizations.
Specifically, the analysis found, alopecia areata patients are at risk for any mental health disorder, anxiety disorders, attention-deficit/hyperactivity disorder, dementia, mood disorders, personality disorders, and suicide or intentionally self-inflicted injury. The report was published in the Journal of the American Academy of Dermatology.
The researchers worked with 87,053,155 adult and child records from the 2002-2012 National Inpatient Sample, which represents 20% of U.S. hospitalizations.
Overall, 5,605 patients had alopecia areata, which was the secondary diagnosis more than 99% of the time. Compared with inpatients without alopecia areata, those with the disorder were more likely to be younger (42.2 vs. 47.9 years; P less than .0001), female (61.7% vs. 58.6%; P = .0297), and uninsured (8.1% vs. 5.5%; P less than .0001). In addition, inpatients with alopecia areata had a greater frequency of mental health disorders (32.8% vs. 20.0%; P less than .0001) and were more likely to have a primary mental health diagnosis (5.5% vs. 2.2%; P less than .0001), reported Vivek Singam of Northwestern University, Chicago, and his associates.
Among 15 mental health or classes of disorders examined, alopecia areata patients were at greater risk in 13 of them. The only exceptions were delirium/dementia/amnestic/cognitive disorders and disorders diagnosed in infancy, childhood, or adolescence.
Alopecia areata patients with a mental health disorder had a mean hospital stay of 6.0 days (95% confidence interval, 5.4.-6.6) and hospitalization cost of $11,907 (95% CI, $10,312-$13,503).
Previous studies had shown similar relationships. However, previous studies showed lower risk of alopecia areata and schizophrenia and no increased risk of ADHD, compared with the current study’s findings. The authors could offer no explanation for those differences.
The strengths of the current analysis include its use of a large-scale, nationally representative cohort and its large sample size, as well its inclusion of a broad range of mental health disorders. Because of its cross-sectional design, the study could not establish the temporal relationship between alopecia areata and mental health disorders.
It is unclear whether psychosocial stress might cause or exacerbate alopecia areata, or whether alopecia areata can lead to or worsen mental health disorders.
The researchers called for additional studies to understand this relationship and potential mechanisms.
The Agency for Healthcare Research and Quality and the Dermatology Foundation funded the study. The researchers declared having no conflicts of interest.
SOURCE: Singam V et al. J Am Acad Dermatol. 2018 Aug 6. doi: 10.1016/j.jaad.2018.07.044.
Alopecia areata is associated with greater frequency of mental health disorders, according to a new analysis of U.S. hospitalizations.
Specifically, the analysis found, alopecia areata patients are at risk for any mental health disorder, anxiety disorders, attention-deficit/hyperactivity disorder, dementia, mood disorders, personality disorders, and suicide or intentionally self-inflicted injury. The report was published in the Journal of the American Academy of Dermatology.
The researchers worked with 87,053,155 adult and child records from the 2002-2012 National Inpatient Sample, which represents 20% of U.S. hospitalizations.
Overall, 5,605 patients had alopecia areata, which was the secondary diagnosis more than 99% of the time. Compared with inpatients without alopecia areata, those with the disorder were more likely to be younger (42.2 vs. 47.9 years; P less than .0001), female (61.7% vs. 58.6%; P = .0297), and uninsured (8.1% vs. 5.5%; P less than .0001). In addition, inpatients with alopecia areata had a greater frequency of mental health disorders (32.8% vs. 20.0%; P less than .0001) and were more likely to have a primary mental health diagnosis (5.5% vs. 2.2%; P less than .0001), reported Vivek Singam of Northwestern University, Chicago, and his associates.
Among 15 mental health or classes of disorders examined, alopecia areata patients were at greater risk in 13 of them. The only exceptions were delirium/dementia/amnestic/cognitive disorders and disorders diagnosed in infancy, childhood, or adolescence.
Alopecia areata patients with a mental health disorder had a mean hospital stay of 6.0 days (95% confidence interval, 5.4.-6.6) and hospitalization cost of $11,907 (95% CI, $10,312-$13,503).
Previous studies had shown similar relationships. However, previous studies showed lower risk of alopecia areata and schizophrenia and no increased risk of ADHD, compared with the current study’s findings. The authors could offer no explanation for those differences.
The strengths of the current analysis include its use of a large-scale, nationally representative cohort and its large sample size, as well its inclusion of a broad range of mental health disorders. Because of its cross-sectional design, the study could not establish the temporal relationship between alopecia areata and mental health disorders.
It is unclear whether psychosocial stress might cause or exacerbate alopecia areata, or whether alopecia areata can lead to or worsen mental health disorders.
The researchers called for additional studies to understand this relationship and potential mechanisms.
The Agency for Healthcare Research and Quality and the Dermatology Foundation funded the study. The researchers declared having no conflicts of interest.
SOURCE: Singam V et al. J Am Acad Dermatol. 2018 Aug 6. doi: 10.1016/j.jaad.2018.07.044.
Alopecia areata is associated with greater frequency of mental health disorders, according to a new analysis of U.S. hospitalizations.
Specifically, the analysis found, alopecia areata patients are at risk for any mental health disorder, anxiety disorders, attention-deficit/hyperactivity disorder, dementia, mood disorders, personality disorders, and suicide or intentionally self-inflicted injury. The report was published in the Journal of the American Academy of Dermatology.
The researchers worked with 87,053,155 adult and child records from the 2002-2012 National Inpatient Sample, which represents 20% of U.S. hospitalizations.
Overall, 5,605 patients had alopecia areata, which was the secondary diagnosis more than 99% of the time. Compared with inpatients without alopecia areata, those with the disorder were more likely to be younger (42.2 vs. 47.9 years; P less than .0001), female (61.7% vs. 58.6%; P = .0297), and uninsured (8.1% vs. 5.5%; P less than .0001). In addition, inpatients with alopecia areata had a greater frequency of mental health disorders (32.8% vs. 20.0%; P less than .0001) and were more likely to have a primary mental health diagnosis (5.5% vs. 2.2%; P less than .0001), reported Vivek Singam of Northwestern University, Chicago, and his associates.
Among 15 mental health or classes of disorders examined, alopecia areata patients were at greater risk in 13 of them. The only exceptions were delirium/dementia/amnestic/cognitive disorders and disorders diagnosed in infancy, childhood, or adolescence.
Alopecia areata patients with a mental health disorder had a mean hospital stay of 6.0 days (95% confidence interval, 5.4.-6.6) and hospitalization cost of $11,907 (95% CI, $10,312-$13,503).
Previous studies had shown similar relationships. However, previous studies showed lower risk of alopecia areata and schizophrenia and no increased risk of ADHD, compared with the current study’s findings. The authors could offer no explanation for those differences.
The strengths of the current analysis include its use of a large-scale, nationally representative cohort and its large sample size, as well its inclusion of a broad range of mental health disorders. Because of its cross-sectional design, the study could not establish the temporal relationship between alopecia areata and mental health disorders.
It is unclear whether psychosocial stress might cause or exacerbate alopecia areata, or whether alopecia areata can lead to or worsen mental health disorders.
The researchers called for additional studies to understand this relationship and potential mechanisms.
The Agency for Healthcare Research and Quality and the Dermatology Foundation funded the study. The researchers declared having no conflicts of interest.
SOURCE: Singam V et al. J Am Acad Dermatol. 2018 Aug 6. doi: 10.1016/j.jaad.2018.07.044.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: Alopecia areata patients should be monitored closely for mental health disorders.
Major finding: Overall, 32.8% of hospitalized alopecia areata patients had a mental health disorder, compared with 20.0% of controls.
Study details: Retrospective analysis of 87,053,155 U.S. adults and children.
Disclosures: The Agency for Healthcare Research & Quality and the Dermatology Foundation funded the study. The researchers declared having no conflicts of interest.
Source: Singam V et al. J Am Acad Dermatol. 2018 Aug 6. doi: 10.1016/j.jaad.2018.07.044.
Concurrent stimulant and opioid use ‘common’ in adult ADHD
A significant number of adults with attention-deficit/hyperactivity disorder are concurrently using stimulants and opioids, highlighting a need for research into the risks and benefits of long-term coadministration of these medications.
Researchers reported the results of a cross-sectional study using Medicaid Analytic eXtract data from 66,406 adults with ADHD across 29 states.
Overall, 32.7% used stimulants, and 5.4% had used both stimulants and opioids long term, defined as at least 30 consecutive days of use. Long-term opioid use was more common among adults who used stimulants, compared with those who did not use stimulants (16.5% vs. 13%), wrote Yu-Jung “Jenny” Wei, PhD, and her associates. The report was published in JAMA Network Open.
Most of the adults who used both stimulants and opioids concurrently long term were using short-acting opioids (81.8%) rather than long-acting (20.6%). However, nearly one-quarter (23.2%) had prescriptions for both long- and short-acting opioids.
The researchers noted a significant 12% increase in the prevalence of concurrent use of stimulants and opioids from 1999 to 2010.
“Our findings suggest that long-term concurrent use of stimulants and opioids has become an increasingly common practice among adult patients with ADHD,” wrote Dr. Wei, of the College of Pharmacy at the University of Florida, Gainesville, and her associates.
The researchers also found an increase in these trends with age: Adults in their 30s showed a 7% higher prevalence of long-term concurrent use, compared with adults in their 20s. In addition, those aged 41-50 years had a 14% higher prevalence, and those aged 51-64 years had a 17% higher prevalence.
Adults with pain had a 10% higher prevalence of concurrent use, while other People with schizophrenia appeared to have a 5% lower incidence of concurrent use.
“Although the concurrent use of stimulants and opioids may initially have been prompted by ADHD symptoms and comorbid chronic pain, continued use of opioids alone or combined with central nervous system stimulants may result in drug dependence and other adverse effects (e.g., overdose) because of the high potential for abuse and misuse,” the authors wrote. “Identifying these high-risk patients allows for early intervention and may reduce the number of adverse events associated with the long-term use of these medications.”
Among the limitations cited is that only prescription medications filled and reimbursed by Medicaid were included in the analysis. “Considering that opioid prescription fills are commonly paid out of pocket, our reported prevalence of concurrent stimulant-opioid use may be too low,” they wrote.
The authors reported no conflicts of interest. One author was supported by an award from the National Institute on Aging.
SOURCE: Wei Y-J et al. JAMA Network Open. 2018. Aug 10. doi: 10.1001/jamanetworkopen.2018.1152.
A significant number of adults with attention-deficit/hyperactivity disorder are concurrently using stimulants and opioids, highlighting a need for research into the risks and benefits of long-term coadministration of these medications.
Researchers reported the results of a cross-sectional study using Medicaid Analytic eXtract data from 66,406 adults with ADHD across 29 states.
Overall, 32.7% used stimulants, and 5.4% had used both stimulants and opioids long term, defined as at least 30 consecutive days of use. Long-term opioid use was more common among adults who used stimulants, compared with those who did not use stimulants (16.5% vs. 13%), wrote Yu-Jung “Jenny” Wei, PhD, and her associates. The report was published in JAMA Network Open.
Most of the adults who used both stimulants and opioids concurrently long term were using short-acting opioids (81.8%) rather than long-acting (20.6%). However, nearly one-quarter (23.2%) had prescriptions for both long- and short-acting opioids.
The researchers noted a significant 12% increase in the prevalence of concurrent use of stimulants and opioids from 1999 to 2010.
“Our findings suggest that long-term concurrent use of stimulants and opioids has become an increasingly common practice among adult patients with ADHD,” wrote Dr. Wei, of the College of Pharmacy at the University of Florida, Gainesville, and her associates.
The researchers also found an increase in these trends with age: Adults in their 30s showed a 7% higher prevalence of long-term concurrent use, compared with adults in their 20s. In addition, those aged 41-50 years had a 14% higher prevalence, and those aged 51-64 years had a 17% higher prevalence.
Adults with pain had a 10% higher prevalence of concurrent use, while other People with schizophrenia appeared to have a 5% lower incidence of concurrent use.
“Although the concurrent use of stimulants and opioids may initially have been prompted by ADHD symptoms and comorbid chronic pain, continued use of opioids alone or combined with central nervous system stimulants may result in drug dependence and other adverse effects (e.g., overdose) because of the high potential for abuse and misuse,” the authors wrote. “Identifying these high-risk patients allows for early intervention and may reduce the number of adverse events associated with the long-term use of these medications.”
Among the limitations cited is that only prescription medications filled and reimbursed by Medicaid were included in the analysis. “Considering that opioid prescription fills are commonly paid out of pocket, our reported prevalence of concurrent stimulant-opioid use may be too low,” they wrote.
The authors reported no conflicts of interest. One author was supported by an award from the National Institute on Aging.
SOURCE: Wei Y-J et al. JAMA Network Open. 2018. Aug 10. doi: 10.1001/jamanetworkopen.2018.1152.
A significant number of adults with attention-deficit/hyperactivity disorder are concurrently using stimulants and opioids, highlighting a need for research into the risks and benefits of long-term coadministration of these medications.
Researchers reported the results of a cross-sectional study using Medicaid Analytic eXtract data from 66,406 adults with ADHD across 29 states.
Overall, 32.7% used stimulants, and 5.4% had used both stimulants and opioids long term, defined as at least 30 consecutive days of use. Long-term opioid use was more common among adults who used stimulants, compared with those who did not use stimulants (16.5% vs. 13%), wrote Yu-Jung “Jenny” Wei, PhD, and her associates. The report was published in JAMA Network Open.
Most of the adults who used both stimulants and opioids concurrently long term were using short-acting opioids (81.8%) rather than long-acting (20.6%). However, nearly one-quarter (23.2%) had prescriptions for both long- and short-acting opioids.
The researchers noted a significant 12% increase in the prevalence of concurrent use of stimulants and opioids from 1999 to 2010.
“Our findings suggest that long-term concurrent use of stimulants and opioids has become an increasingly common practice among adult patients with ADHD,” wrote Dr. Wei, of the College of Pharmacy at the University of Florida, Gainesville, and her associates.
The researchers also found an increase in these trends with age: Adults in their 30s showed a 7% higher prevalence of long-term concurrent use, compared with adults in their 20s. In addition, those aged 41-50 years had a 14% higher prevalence, and those aged 51-64 years had a 17% higher prevalence.
Adults with pain had a 10% higher prevalence of concurrent use, while other People with schizophrenia appeared to have a 5% lower incidence of concurrent use.
“Although the concurrent use of stimulants and opioids may initially have been prompted by ADHD symptoms and comorbid chronic pain, continued use of opioids alone or combined with central nervous system stimulants may result in drug dependence and other adverse effects (e.g., overdose) because of the high potential for abuse and misuse,” the authors wrote. “Identifying these high-risk patients allows for early intervention and may reduce the number of adverse events associated with the long-term use of these medications.”
Among the limitations cited is that only prescription medications filled and reimbursed by Medicaid were included in the analysis. “Considering that opioid prescription fills are commonly paid out of pocket, our reported prevalence of concurrent stimulant-opioid use may be too low,” they wrote.
The authors reported no conflicts of interest. One author was supported by an award from the National Institute on Aging.
SOURCE: Wei Y-J et al. JAMA Network Open. 2018. Aug 10. doi: 10.1001/jamanetworkopen.2018.1152.
FROM JAMA NETWORK OPEN
Key clinical point: Identifying high-risk patients “allows for early intervention and may reduce the number of adverse events associated with the long-term use.”
Major finding: About 5% of adults with ADHD are on both opioids and stimulants long term.
Study details: Cross-sectional study of 66,406 adults with ADHD.
Disclosures: The authors reported no conflicts of interest. One author was supported by an award from the National Institute on Aging.
Source: Wei Y-J et al. JAMA Network Open. 2018. Aug 10. doi: 10.1001/jamanetworkopen.2018.1152.
Methylphenidate deemed best first-line option for ADHD in children
Methylphenidate appears to be the safest and most effective treatment option for attention-deficit/hyperactivity disorder in children and adolescents, while amphetamines are the preferred first-line choice in adults, a systematic review and meta-analysis have found.
Researchers reported the results of a network meta-analysis of 133 double-blind randomized controlled trials – 81 in children and adolescents, 51 in adults, and 1 in both – involving a total of 10,068 children and adolescents, and 8,131 adults. The included studies all compared a range of medications to placebo or in head-to-head trials. The meta-analysis was published online Aug. 7 in The Lancet Psychiatry.
At 12 weeks, all the medications, which included amphetamines, atomoxetine, bupropion, clonidine, guanfacine, methylphenidate, and modafinil, were found to be better than placebo in reducing core ADHD symptoms in children and adolescents, according to clinicians’ ratings. However, when teachers’ ratings were used, only methylphenidate and modafinil were better than placebo.
In adults, clinicians’ ratings found that amphetamines, methylphenidate, bupropion, and atomoxetine – but not modafinil – were better than placebo.
In head-to-head trials, clinicians’ ratings favored amphetamines over modafinil, atomoxetine, and methylphenidate in children, adolescents, and adults.
But in adults, amphetamines, bupropion, and methylphenidate all beat placebo.
When it came to tolerability in children and adolescents, guanfacine and amphetamines were the only two treatments that were less well tolerated than placebo. However, a post hoc analysis suggested lisdexamfetamine had a lower tolerability relative to other amphetamines, at least in children and adolescents. In adults, modafinil, amphetamines, methylphenidate, and atomoxetine were beaten by placebo for tolerability.
“Overall, all medications, except modafinil in adults, were more efficacious than placebo for the short-term treatment of ADHD, and they were less efficacious and less well tolerated in adults than in children and adolescents,” wrote Samuele Cortese, MD, PhD, of the University of Southampton (England), and his coauthors. “However, the included medications were not equivalent in relation to their mean effect size, which ranged from moderate to high and varied according to the type of rater.”
For example, while atomoxetine had the lowest mean effect size in children and adolescents based on clinicians’ ratings, in adults, it was on par with methylphenidate. Amphetamines increased diastolic blood pressure in children but not in adults.
“Taking into account both efficacy and safety, evidence from this meta-analysis supports methylphenidate in children and adolescents, and amphetamines in adults, as preferred first-choice medications for the short-term treatment of ADHD,” the authors wrote.
Dr. Cortese and his coauthors cited a few limitations. One is that the most recent study included in their meta-analysis was published in April 2017. When the researchers conducted a PubMed search in May 2018, they found three additional studies that met their criteria. “Since we already had 133 included studies, we decided that adding these three studies would not have changed the final results materially,” they wrote.
The study was supported by the Stichting Eunethydis (European Network for Hyperkinetic Disorders), and the U.K. National Institute for Health Research Oxford Health Biomedical Research Centre. Nine authors declared support, funding, or advisory roles with a range of organizations or the pharmaceutical industry.
SOURCE: Cortese S et al. Lancet Psychiatry. 2018 Aug 7. doi: 10.1016/S2215-0366(18)30269-4.
Methylphenidate appears to be the safest and most effective treatment option for attention-deficit/hyperactivity disorder in children and adolescents, while amphetamines are the preferred first-line choice in adults, a systematic review and meta-analysis have found.
Researchers reported the results of a network meta-analysis of 133 double-blind randomized controlled trials – 81 in children and adolescents, 51 in adults, and 1 in both – involving a total of 10,068 children and adolescents, and 8,131 adults. The included studies all compared a range of medications to placebo or in head-to-head trials. The meta-analysis was published online Aug. 7 in The Lancet Psychiatry.
At 12 weeks, all the medications, which included amphetamines, atomoxetine, bupropion, clonidine, guanfacine, methylphenidate, and modafinil, were found to be better than placebo in reducing core ADHD symptoms in children and adolescents, according to clinicians’ ratings. However, when teachers’ ratings were used, only methylphenidate and modafinil were better than placebo.
In adults, clinicians’ ratings found that amphetamines, methylphenidate, bupropion, and atomoxetine – but not modafinil – were better than placebo.
In head-to-head trials, clinicians’ ratings favored amphetamines over modafinil, atomoxetine, and methylphenidate in children, adolescents, and adults.
But in adults, amphetamines, bupropion, and methylphenidate all beat placebo.
When it came to tolerability in children and adolescents, guanfacine and amphetamines were the only two treatments that were less well tolerated than placebo. However, a post hoc analysis suggested lisdexamfetamine had a lower tolerability relative to other amphetamines, at least in children and adolescents. In adults, modafinil, amphetamines, methylphenidate, and atomoxetine were beaten by placebo for tolerability.
“Overall, all medications, except modafinil in adults, were more efficacious than placebo for the short-term treatment of ADHD, and they were less efficacious and less well tolerated in adults than in children and adolescents,” wrote Samuele Cortese, MD, PhD, of the University of Southampton (England), and his coauthors. “However, the included medications were not equivalent in relation to their mean effect size, which ranged from moderate to high and varied according to the type of rater.”
For example, while atomoxetine had the lowest mean effect size in children and adolescents based on clinicians’ ratings, in adults, it was on par with methylphenidate. Amphetamines increased diastolic blood pressure in children but not in adults.
“Taking into account both efficacy and safety, evidence from this meta-analysis supports methylphenidate in children and adolescents, and amphetamines in adults, as preferred first-choice medications for the short-term treatment of ADHD,” the authors wrote.
Dr. Cortese and his coauthors cited a few limitations. One is that the most recent study included in their meta-analysis was published in April 2017. When the researchers conducted a PubMed search in May 2018, they found three additional studies that met their criteria. “Since we already had 133 included studies, we decided that adding these three studies would not have changed the final results materially,” they wrote.
The study was supported by the Stichting Eunethydis (European Network for Hyperkinetic Disorders), and the U.K. National Institute for Health Research Oxford Health Biomedical Research Centre. Nine authors declared support, funding, or advisory roles with a range of organizations or the pharmaceutical industry.
SOURCE: Cortese S et al. Lancet Psychiatry. 2018 Aug 7. doi: 10.1016/S2215-0366(18)30269-4.
Methylphenidate appears to be the safest and most effective treatment option for attention-deficit/hyperactivity disorder in children and adolescents, while amphetamines are the preferred first-line choice in adults, a systematic review and meta-analysis have found.
Researchers reported the results of a network meta-analysis of 133 double-blind randomized controlled trials – 81 in children and adolescents, 51 in adults, and 1 in both – involving a total of 10,068 children and adolescents, and 8,131 adults. The included studies all compared a range of medications to placebo or in head-to-head trials. The meta-analysis was published online Aug. 7 in The Lancet Psychiatry.
At 12 weeks, all the medications, which included amphetamines, atomoxetine, bupropion, clonidine, guanfacine, methylphenidate, and modafinil, were found to be better than placebo in reducing core ADHD symptoms in children and adolescents, according to clinicians’ ratings. However, when teachers’ ratings were used, only methylphenidate and modafinil were better than placebo.
In adults, clinicians’ ratings found that amphetamines, methylphenidate, bupropion, and atomoxetine – but not modafinil – were better than placebo.
In head-to-head trials, clinicians’ ratings favored amphetamines over modafinil, atomoxetine, and methylphenidate in children, adolescents, and adults.
But in adults, amphetamines, bupropion, and methylphenidate all beat placebo.
When it came to tolerability in children and adolescents, guanfacine and amphetamines were the only two treatments that were less well tolerated than placebo. However, a post hoc analysis suggested lisdexamfetamine had a lower tolerability relative to other amphetamines, at least in children and adolescents. In adults, modafinil, amphetamines, methylphenidate, and atomoxetine were beaten by placebo for tolerability.
“Overall, all medications, except modafinil in adults, were more efficacious than placebo for the short-term treatment of ADHD, and they were less efficacious and less well tolerated in adults than in children and adolescents,” wrote Samuele Cortese, MD, PhD, of the University of Southampton (England), and his coauthors. “However, the included medications were not equivalent in relation to their mean effect size, which ranged from moderate to high and varied according to the type of rater.”
For example, while atomoxetine had the lowest mean effect size in children and adolescents based on clinicians’ ratings, in adults, it was on par with methylphenidate. Amphetamines increased diastolic blood pressure in children but not in adults.
“Taking into account both efficacy and safety, evidence from this meta-analysis supports methylphenidate in children and adolescents, and amphetamines in adults, as preferred first-choice medications for the short-term treatment of ADHD,” the authors wrote.
Dr. Cortese and his coauthors cited a few limitations. One is that the most recent study included in their meta-analysis was published in April 2017. When the researchers conducted a PubMed search in May 2018, they found three additional studies that met their criteria. “Since we already had 133 included studies, we decided that adding these three studies would not have changed the final results materially,” they wrote.
The study was supported by the Stichting Eunethydis (European Network for Hyperkinetic Disorders), and the U.K. National Institute for Health Research Oxford Health Biomedical Research Centre. Nine authors declared support, funding, or advisory roles with a range of organizations or the pharmaceutical industry.
SOURCE: Cortese S et al. Lancet Psychiatry. 2018 Aug 7. doi: 10.1016/S2215-0366(18)30269-4.
FROM THE LANCET PSYCHIATRY
Key clinical point: “All medications, except modafinil in adults, were more efficacious than placebo for the short-term treatment of ADHD.”
Major finding: Methylphenidate showed the greatest tolerability and efficacy of ADHD treatments for children and adolescents.
Study details: Systematic review and meta-analysis of 133 double-blind randomized controlled trials.
Disclosures: The study was supported by the Stichting Eunethydis (European Network for Hyperkinetic Disorders), and the U.K. National Institute for Health Research Oxford Health Biomedical Research Centre. Nine authors declared support, funding, or advisory roles with a range of organizations or the pharmaceutical industry.
Source: Cortese S et al. Lancet Psychiatry. 2018 Aug 7. doi: 10.1016/S2215-0366(18)30269-4.
Social media use linked to 10% increase in risk of new ADHD symptoms among teens
according to results from a prospective, longitudinal cohort study published in JAMA. 
“Further research is needed to determine whether this association is causal,” cautioned the investigators.
Between fall 2014 (10th grade) and fall 2016 (12th grade), researchers studied 3,051 students from 10 different Los Angeles schools who were enrolled in the Happiness & Health Study and did not have significant ADHD symptoms; of these students, 2,587 adolescents (mean age 16 years, 54% girls) self-reported digital media use activities from 14 different types through surveys administered at baseline and again at 6-month, 12-month, 18-month and 24-month follow-up. Digital use activities included checking social media sites, engaging with social media content, texting, streaming music, and browsing or viewing images or videos, among others.
“Although some emerging research indicates that ADHD levels and use of certain forms of modern media may be concurrently associated, the role of modern digital media use in ADHD risk largely remains unclear from the prior literature due to limitations in exposure assessment and the application of designs incapable of supporting temporal or causal inferences,” wrote Chaelin K. Ra, MPH, of the University of Southern California, Los Angeles, and his colleagues. “The current study provides new longitudinal evidence on this topic using a 5-wave prospective design and comprehensive assessment across a wide continuum of digital media exposure, including numerous media platforms currently popular among youth.”
Students ranked their activities in a cumulative index and indicated whether they participated in those activities “0, 1-2 times per week, 1-2 times per day, or many times per day.” They also filled out the DSM-IV Current Symptoms Self-Report Form, which asked them to report whether they experienced any of nine different hyperactivity-impulsivity symptoms such as “difficulty organizing and completing tasks.”
Mr. Ra and his colleagues found that 81% of adolescents reported at least one digital media activity performed at a high-frequency rate, with 54% reporting they checked social media at a high-frequency rate. There was a mean of four baseline digital media activities performed at a high-frequency rate among students surveyed. Each additional digital media activity used at a high-frequency rate carried a statistically significant association of subsequent ADHD symptoms over the follow-up period (odds ratio 1.1; 95% confidence interval, 1.06-1.16), which remained after adjustment for covariates including age, sex, and subsidized lunch availability tied to family income (OR 1.1; 95% CI, 1.05-1.15). The researchers noted that there was a 5% mean prevalence of subsequent ADHD symptoms in follow-up among patients who reported no baseline high-frequency rate of digital media use, compared with 10% in students indicating 7 high-frequency activities and 11% in students indicating 14 high-frequency activities.
Limitations of the study included potential inaccuracies in self-reporting ADHD symptoms as opposed to students receiving a diagnosis through a clinical interview, the possibility of the association being influenced by ADHD symptoms not detected in the study, the fact that the media use measure in the study had not been validated, and use of a targeted age range in the sample of students that excluded students without surveys who had differing demographic data from the rest of the cohort, according to the researchers.
The authors reported having no relevant financial disclosures. The study was supported by a grant from the National Institutes of Health.
SOURCE: Ra CK et al. JAMA. 2018 Jul 17. doi: 10.1001/jama.2018.8931.
This study is among the first to capture current media use because technology tends to outpace researchers’ ability to publish data “within relevant time frames,” Jenny Radesky, MD of the University of Michigan in Ann Arbor, said in an editorial.
While previous studies linking ADHD symptoms and media use analyzed use of media such as television shows and video games, this study analyzes smartphone use and “always-on” media such as social media in addition to traditional media, she said.
It should be noted that “high-frequency media use was associated with only a 10% increased risk of later ADHD symptoms overall.
“Although the authors were able to adjust for income and mental health symptoms, they did not assess parent media use or whether the parents were involved in how the adolescents used media,” Dr. Radesky said. “Parent media use correlates with child media use, may interrupt parent-child activities, and is associated with child behavior difficulties in younger children.”
She said the study affirms guidelines from the American Academy of Pediatrics to “prioritize activities that promote adolescent executive functioning and well-being, including sleep, physical activity, distraction-free homework, and positive interactions with family and friends.
“Although not directly addressed by this study, the American Academy of Pediatrics recommendations for parent involvement in their adolescent’s media use – including discussions about prosocial uses of media, digital citizenship, misinformation, and persuasion awareness – are relevant to the cognitive and emotional reactions to digital media of adolescents,” she added.
Dr. Radesky noted that the potential for the association between media use and ADHD symptoms to be influenced by confounders not measured in the study is a “major limitation.”
Dr. Radesky is at the University of Michigan, Ann Arbor. She receives grant support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. These comments summarize her editorial accompanying the article by Ra et al. ( JAMA. 2018;320:237-39 ).
This study is among the first to capture current media use because technology tends to outpace researchers’ ability to publish data “within relevant time frames,” Jenny Radesky, MD of the University of Michigan in Ann Arbor, said in an editorial.
While previous studies linking ADHD symptoms and media use analyzed use of media such as television shows and video games, this study analyzes smartphone use and “always-on” media such as social media in addition to traditional media, she said.
It should be noted that “high-frequency media use was associated with only a 10% increased risk of later ADHD symptoms overall.
“Although the authors were able to adjust for income and mental health symptoms, they did not assess parent media use or whether the parents were involved in how the adolescents used media,” Dr. Radesky said. “Parent media use correlates with child media use, may interrupt parent-child activities, and is associated with child behavior difficulties in younger children.”
She said the study affirms guidelines from the American Academy of Pediatrics to “prioritize activities that promote adolescent executive functioning and well-being, including sleep, physical activity, distraction-free homework, and positive interactions with family and friends.
“Although not directly addressed by this study, the American Academy of Pediatrics recommendations for parent involvement in their adolescent’s media use – including discussions about prosocial uses of media, digital citizenship, misinformation, and persuasion awareness – are relevant to the cognitive and emotional reactions to digital media of adolescents,” she added.
Dr. Radesky noted that the potential for the association between media use and ADHD symptoms to be influenced by confounders not measured in the study is a “major limitation.”
Dr. Radesky is at the University of Michigan, Ann Arbor. She receives grant support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. These comments summarize her editorial accompanying the article by Ra et al. ( JAMA. 2018;320:237-39 ).
This study is among the first to capture current media use because technology tends to outpace researchers’ ability to publish data “within relevant time frames,” Jenny Radesky, MD of the University of Michigan in Ann Arbor, said in an editorial.
While previous studies linking ADHD symptoms and media use analyzed use of media such as television shows and video games, this study analyzes smartphone use and “always-on” media such as social media in addition to traditional media, she said.
It should be noted that “high-frequency media use was associated with only a 10% increased risk of later ADHD symptoms overall.
“Although the authors were able to adjust for income and mental health symptoms, they did not assess parent media use or whether the parents were involved in how the adolescents used media,” Dr. Radesky said. “Parent media use correlates with child media use, may interrupt parent-child activities, and is associated with child behavior difficulties in younger children.”
She said the study affirms guidelines from the American Academy of Pediatrics to “prioritize activities that promote adolescent executive functioning and well-being, including sleep, physical activity, distraction-free homework, and positive interactions with family and friends.
“Although not directly addressed by this study, the American Academy of Pediatrics recommendations for parent involvement in their adolescent’s media use – including discussions about prosocial uses of media, digital citizenship, misinformation, and persuasion awareness – are relevant to the cognitive and emotional reactions to digital media of adolescents,” she added.
Dr. Radesky noted that the potential for the association between media use and ADHD symptoms to be influenced by confounders not measured in the study is a “major limitation.”
Dr. Radesky is at the University of Michigan, Ann Arbor. She receives grant support from the Eunice Kennedy Shriver National Institute of Child Health and Human Development. These comments summarize her editorial accompanying the article by Ra et al. ( JAMA. 2018;320:237-39 ).
according to results from a prospective, longitudinal cohort study published in JAMA.
“Further research is needed to determine whether this association is causal,” cautioned the investigators.
Between fall 2014 (10th grade) and fall 2016 (12th grade), researchers studied 3,051 students from 10 different Los Angeles schools who were enrolled in the Happiness & Health Study and did not have significant ADHD symptoms; of these students, 2,587 adolescents (mean age 16 years, 54% girls) self-reported digital media use activities from 14 different types through surveys administered at baseline and again at 6-month, 12-month, 18-month and 24-month follow-up. Digital use activities included checking social media sites, engaging with social media content, texting, streaming music, and browsing or viewing images or videos, among others.
“Although some emerging research indicates that ADHD levels and use of certain forms of modern media may be concurrently associated, the role of modern digital media use in ADHD risk largely remains unclear from the prior literature due to limitations in exposure assessment and the application of designs incapable of supporting temporal or causal inferences,” wrote Chaelin K. Ra, MPH, of the University of Southern California, Los Angeles, and his colleagues. “The current study provides new longitudinal evidence on this topic using a 5-wave prospective design and comprehensive assessment across a wide continuum of digital media exposure, including numerous media platforms currently popular among youth.”
Students ranked their activities in a cumulative index and indicated whether they participated in those activities “0, 1-2 times per week, 1-2 times per day, or many times per day.” They also filled out the DSM-IV Current Symptoms Self-Report Form, which asked them to report whether they experienced any of nine different hyperactivity-impulsivity symptoms such as “difficulty organizing and completing tasks.”
Mr. Ra and his colleagues found that 81% of adolescents reported at least one digital media activity performed at a high-frequency rate, with 54% reporting they checked social media at a high-frequency rate. There was a mean of four baseline digital media activities performed at a high-frequency rate among students surveyed. Each additional digital media activity used at a high-frequency rate carried a statistically significant association of subsequent ADHD symptoms over the follow-up period (odds ratio 1.1; 95% confidence interval, 1.06-1.16), which remained after adjustment for covariates including age, sex, and subsidized lunch availability tied to family income (OR 1.1; 95% CI, 1.05-1.15). The researchers noted that there was a 5% mean prevalence of subsequent ADHD symptoms in follow-up among patients who reported no baseline high-frequency rate of digital media use, compared with 10% in students indicating 7 high-frequency activities and 11% in students indicating 14 high-frequency activities.
Limitations of the study included potential inaccuracies in self-reporting ADHD symptoms as opposed to students receiving a diagnosis through a clinical interview, the possibility of the association being influenced by ADHD symptoms not detected in the study, the fact that the media use measure in the study had not been validated, and use of a targeted age range in the sample of students that excluded students without surveys who had differing demographic data from the rest of the cohort, according to the researchers.
The authors reported having no relevant financial disclosures. The study was supported by a grant from the National Institutes of Health.
SOURCE: Ra CK et al. JAMA. 2018 Jul 17. doi: 10.1001/jama.2018.8931.
according to results from a prospective, longitudinal cohort study published in JAMA.
“Further research is needed to determine whether this association is causal,” cautioned the investigators.
Between fall 2014 (10th grade) and fall 2016 (12th grade), researchers studied 3,051 students from 10 different Los Angeles schools who were enrolled in the Happiness & Health Study and did not have significant ADHD symptoms; of these students, 2,587 adolescents (mean age 16 years, 54% girls) self-reported digital media use activities from 14 different types through surveys administered at baseline and again at 6-month, 12-month, 18-month and 24-month follow-up. Digital use activities included checking social media sites, engaging with social media content, texting, streaming music, and browsing or viewing images or videos, among others.
“Although some emerging research indicates that ADHD levels and use of certain forms of modern media may be concurrently associated, the role of modern digital media use in ADHD risk largely remains unclear from the prior literature due to limitations in exposure assessment and the application of designs incapable of supporting temporal or causal inferences,” wrote Chaelin K. Ra, MPH, of the University of Southern California, Los Angeles, and his colleagues. “The current study provides new longitudinal evidence on this topic using a 5-wave prospective design and comprehensive assessment across a wide continuum of digital media exposure, including numerous media platforms currently popular among youth.”
Students ranked their activities in a cumulative index and indicated whether they participated in those activities “0, 1-2 times per week, 1-2 times per day, or many times per day.” They also filled out the DSM-IV Current Symptoms Self-Report Form, which asked them to report whether they experienced any of nine different hyperactivity-impulsivity symptoms such as “difficulty organizing and completing tasks.”
Mr. Ra and his colleagues found that 81% of adolescents reported at least one digital media activity performed at a high-frequency rate, with 54% reporting they checked social media at a high-frequency rate. There was a mean of four baseline digital media activities performed at a high-frequency rate among students surveyed. Each additional digital media activity used at a high-frequency rate carried a statistically significant association of subsequent ADHD symptoms over the follow-up period (odds ratio 1.1; 95% confidence interval, 1.06-1.16), which remained after adjustment for covariates including age, sex, and subsidized lunch availability tied to family income (OR 1.1; 95% CI, 1.05-1.15). The researchers noted that there was a 5% mean prevalence of subsequent ADHD symptoms in follow-up among patients who reported no baseline high-frequency rate of digital media use, compared with 10% in students indicating 7 high-frequency activities and 11% in students indicating 14 high-frequency activities.
Limitations of the study included potential inaccuracies in self-reporting ADHD symptoms as opposed to students receiving a diagnosis through a clinical interview, the possibility of the association being influenced by ADHD symptoms not detected in the study, the fact that the media use measure in the study had not been validated, and use of a targeted age range in the sample of students that excluded students without surveys who had differing demographic data from the rest of the cohort, according to the researchers.
The authors reported having no relevant financial disclosures. The study was supported by a grant from the National Institutes of Health.
SOURCE: Ra CK et al. JAMA. 2018 Jul 17. doi: 10.1001/jama.2018.8931.
FROM JAMA
Key clinical point: High-frequency digital media use carries a statistically significant association with subsequent ADHD symptoms in adolescent students without previous significant ADHD symptoms at baseline.
Major finding: Of the adolescent students without significant ADHD symptoms,
Study details: A prospective, longitudinal study of 3,051 adolescent students (mean age, 16 years) in the Happiness & Health Study, followed for 24 months.
Disclosures: The authors reported having no relevant financial disclosures. The study was supported by a grant from the National Institutes of Health.
Source: Ra CK et al. JAMA. 2018 Jul 17. doi: 10.1001/jama.2018.8931.
It’s not about time
Like most couples of retirement age, rituals dominate our breakfasts. I eat eggs. Marilyn leans toward baked goods. We each have a bowl of fruit and finish by working the New York Times mini-crossword on our electronic devices. Solving it usually takes somewhere between 40 seconds and 4 minutes. The challenge lies in how fast one can complete the puzzle. And, being who we are, Marilyn and I have ritualized this into a serious competition. She usually takes the first turn and then tries to psyche me out by announcing, “I did it in 2:34, but you should be able to solve it in less than 2 minutes.” This bit of gamesmanship often means that I am going to start the day with thin layer of nervous perspiration.
The claimed disabilities range from an anxiety disorder and ADHD to a problem with reading comprehension. The number of students requesting a test environment modification at Pomona College, Claremont, Calif., is 22% up from 5% in 2014. At Marlboro College in Vermont, one in three students asks for more time or a less distracting setting.
This phenomenon raises two obvious questions. First, what has happened to the bell-shaped curve? Was it too boring hanging out with all those people under the bell? Do folks feel safer and more secure in the tails? I guess we have to be happy that young people are less afraid to admit they are different. But it does make one wonder how we should go about defining a disability.
The second question is whether timed tests deserve a place in our educational toolbox? How often is processing speed important? I would like the woman piloting my flight to San Francisco to be quick-witted. But what about the research chemist working on a more durable tire compound? Is it a problem that it took him 30% longer than his classmates to successfully finish his college statistics final exam?
What about the lawyer who bills you $500 per hour to review the contract with your employer? It might have been helpful to know before you hired him that he routinely requested an extra hour and a half to complete his exams in law school. But I suspect that for the most part timed tests probably don’t produce better graduates. In the past they may have been used to thin oversubscribed disciplines, and certainly time limits have been the norm at every level of education I encountered. However, the best taught courses had exams with an abundance of time. Either you knew the information or you didn’t. An extra 2 hours wasn’t going to make a difference.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Like most couples of retirement age, rituals dominate our breakfasts. I eat eggs. Marilyn leans toward baked goods. We each have a bowl of fruit and finish by working the New York Times mini-crossword on our electronic devices. Solving it usually takes somewhere between 40 seconds and 4 minutes. The challenge lies in how fast one can complete the puzzle. And, being who we are, Marilyn and I have ritualized this into a serious competition. She usually takes the first turn and then tries to psyche me out by announcing, “I did it in 2:34, but you should be able to solve it in less than 2 minutes.” This bit of gamesmanship often means that I am going to start the day with thin layer of nervous perspiration.
The claimed disabilities range from an anxiety disorder and ADHD to a problem with reading comprehension. The number of students requesting a test environment modification at Pomona College, Claremont, Calif., is 22% up from 5% in 2014. At Marlboro College in Vermont, one in three students asks for more time or a less distracting setting.
This phenomenon raises two obvious questions. First, what has happened to the bell-shaped curve? Was it too boring hanging out with all those people under the bell? Do folks feel safer and more secure in the tails? I guess we have to be happy that young people are less afraid to admit they are different. But it does make one wonder how we should go about defining a disability.
The second question is whether timed tests deserve a place in our educational toolbox? How often is processing speed important? I would like the woman piloting my flight to San Francisco to be quick-witted. But what about the research chemist working on a more durable tire compound? Is it a problem that it took him 30% longer than his classmates to successfully finish his college statistics final exam?
What about the lawyer who bills you $500 per hour to review the contract with your employer? It might have been helpful to know before you hired him that he routinely requested an extra hour and a half to complete his exams in law school. But I suspect that for the most part timed tests probably don’t produce better graduates. In the past they may have been used to thin oversubscribed disciplines, and certainly time limits have been the norm at every level of education I encountered. However, the best taught courses had exams with an abundance of time. Either you knew the information or you didn’t. An extra 2 hours wasn’t going to make a difference.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Like most couples of retirement age, rituals dominate our breakfasts. I eat eggs. Marilyn leans toward baked goods. We each have a bowl of fruit and finish by working the New York Times mini-crossword on our electronic devices. Solving it usually takes somewhere between 40 seconds and 4 minutes. The challenge lies in how fast one can complete the puzzle. And, being who we are, Marilyn and I have ritualized this into a serious competition. She usually takes the first turn and then tries to psyche me out by announcing, “I did it in 2:34, but you should be able to solve it in less than 2 minutes.” This bit of gamesmanship often means that I am going to start the day with thin layer of nervous perspiration.
The claimed disabilities range from an anxiety disorder and ADHD to a problem with reading comprehension. The number of students requesting a test environment modification at Pomona College, Claremont, Calif., is 22% up from 5% in 2014. At Marlboro College in Vermont, one in three students asks for more time or a less distracting setting.
This phenomenon raises two obvious questions. First, what has happened to the bell-shaped curve? Was it too boring hanging out with all those people under the bell? Do folks feel safer and more secure in the tails? I guess we have to be happy that young people are less afraid to admit they are different. But it does make one wonder how we should go about defining a disability.
The second question is whether timed tests deserve a place in our educational toolbox? How often is processing speed important? I would like the woman piloting my flight to San Francisco to be quick-witted. But what about the research chemist working on a more durable tire compound? Is it a problem that it took him 30% longer than his classmates to successfully finish his college statistics final exam?
What about the lawyer who bills you $500 per hour to review the contract with your employer? It might have been helpful to know before you hired him that he routinely requested an extra hour and a half to complete his exams in law school. But I suspect that for the most part timed tests probably don’t produce better graduates. In the past they may have been used to thin oversubscribed disciplines, and certainly time limits have been the norm at every level of education I encountered. However, the best taught courses had exams with an abundance of time. Either you knew the information or you didn’t. An extra 2 hours wasn’t going to make a difference.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Anxiety, depression prevalent in children with comorbid autism and ADHD
Children with comorbid autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) are at an increased risk of anxiety and mood disorders, a cross-sectional analysis has shown.
“Our study supports that anxiety and mood disorders, although highly prevalent in those with ASD alone, are even more prevalent in individuals who have ADHD,” wrote Eliza Gordon-Lipkin, MD, of the Kennedy Krieger Institute, Baltimore, and her associates. ”The identification of psychiatric conditions in children with ASD is important because these disorders are treatable and affect quality of life.”
The study was published in Pediatrics.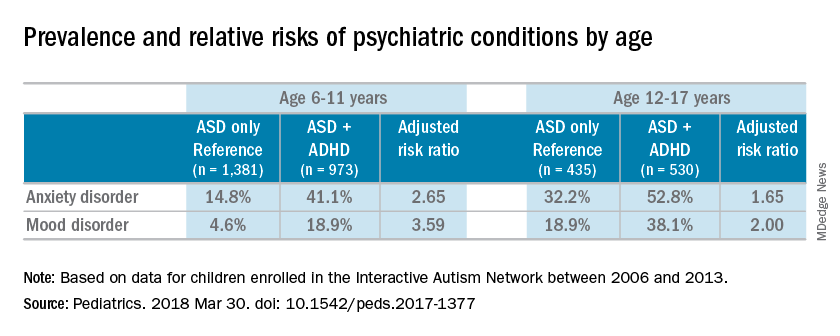
Most of the children were male (83%), white (87%), and non-Hispanic (92%); the mean age of the children was 10 years. Almost half of the children in the study had parent-reported ADHD (45%). Almost one-third of patients were diagnosed with an anxiety disorder (31%), and many also were reported to have been diagnosed with a mood disorder (16%). An increased risk of reported anxiety disorder was found in patients with both ADHD and ASD (adjusted relative risk, 2.20; 95% confidence interval, 1.97-2.46).
The researchers also found an increased risk of mood disorders (aRR, 2.72; 95% CI, 2.28-3.24) among children with comorbid conditions. Those risks increased with age (both P less than .001). An increased prevalence of anxiety and mood disorders was found in adolescents, compared with school-aged children with both ASD and ADHD or ASD alone. But higher relative risk ratios were found for the younger children, compared with the adolescents for those in the ADHD/ASD group and the ASD alone group.
“This suggests that or more likely to exhibit detectable symptoms at an earlier age,” reported Dr. Gordon-Lipkin, also with the department of pediatrics at Johns Hopkins University, in Baltimore.
The research team cited several limitations. For example, patient-reported data might be subject to recall or reporting biases. Also, computer and Internet access was required to complete the IAN questionnaires, which means that the findings could be biased toward people of higher socioeconomic status.
Nevertheless, the researchers wrote, their study is the largest to compare comorbidities in patients with ASD and ADHD, or ASD alone.
Further research is needed to better understand the relationship between ASD and ADHD. “ADHD affects nearly half of the children with ASD. This subgroup of individuals with ASD may represent a distinct clinical phenotype, with different diagnostic and therapeutic implications,” Dr. Gordon-Lipkin and her associates wrote. “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
None of the study authors had relevant financial disclosures to report. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
SOURCE: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
The work of Gordon-Lipkin et al. is one of the largest studies analyzing the relationships between autism, ADHD, and anxiety and mood disorders. But because of the inherent behavioral and biological complexity of autism, changes in the diagnostic criteria, and the use of parent-reported data, the current study might not reflect what is truly occurring in patients with autism, Christopher J. McDougle, MD, said in an interview.
“There are a number of things to say about [the study]. [One] of the strengths of the paper [is] the sample size,” Dr. McDougle said.“It’s always good to have a big sample size. The downside to having informant-databased information is that it is exactly what it is. This is fine, but the information may be inaccurate.”
In addition to parent-reported data, physicians are dealing with the relatively new diagnostic criteria. The May 2013 update of the Diagnostic and Statistical Manual of Mental Disorders to the DSM-5 brought with it the ability to diagnose ADHD with autism, when just the day before the DSM-5 was released, this differential diagnosis was not listed in the manual, Dr. McDougle said. “If something that important can change with the strike of the clock, it makes me concerned.” He also said listing the differential diagnosis in the diagnostic manual underscored the uncertainty of medicine’s understanding of comorbid autism and ADHD.
“That’s reflective of the field’s lack of knowledge. Sometimes I think we like to portray things as though we understand what’s going on, when I think it’s better to be honest and say we really don’t; we are just doing our best.”
Dr. McDougle is the director of the Lurie Center for Autism at Massachusetts General Hospital and is the Nancy Lurie Marks Professor of Psychiatry at Harvard Medical Center, both in Boston. He treats children, adolescents, and adults with autism spectrum disorder and other neurodevelopmental disorders. He was asked to comment on this study.
The work of Gordon-Lipkin et al. is one of the largest studies analyzing the relationships between autism, ADHD, and anxiety and mood disorders. But because of the inherent behavioral and biological complexity of autism, changes in the diagnostic criteria, and the use of parent-reported data, the current study might not reflect what is truly occurring in patients with autism, Christopher J. McDougle, MD, said in an interview.
“There are a number of things to say about [the study]. [One] of the strengths of the paper [is] the sample size,” Dr. McDougle said.“It’s always good to have a big sample size. The downside to having informant-databased information is that it is exactly what it is. This is fine, but the information may be inaccurate.”
In addition to parent-reported data, physicians are dealing with the relatively new diagnostic criteria. The May 2013 update of the Diagnostic and Statistical Manual of Mental Disorders to the DSM-5 brought with it the ability to diagnose ADHD with autism, when just the day before the DSM-5 was released, this differential diagnosis was not listed in the manual, Dr. McDougle said. “If something that important can change with the strike of the clock, it makes me concerned.” He also said listing the differential diagnosis in the diagnostic manual underscored the uncertainty of medicine’s understanding of comorbid autism and ADHD.
“That’s reflective of the field’s lack of knowledge. Sometimes I think we like to portray things as though we understand what’s going on, when I think it’s better to be honest and say we really don’t; we are just doing our best.”
Dr. McDougle is the director of the Lurie Center for Autism at Massachusetts General Hospital and is the Nancy Lurie Marks Professor of Psychiatry at Harvard Medical Center, both in Boston. He treats children, adolescents, and adults with autism spectrum disorder and other neurodevelopmental disorders. He was asked to comment on this study.
The work of Gordon-Lipkin et al. is one of the largest studies analyzing the relationships between autism, ADHD, and anxiety and mood disorders. But because of the inherent behavioral and biological complexity of autism, changes in the diagnostic criteria, and the use of parent-reported data, the current study might not reflect what is truly occurring in patients with autism, Christopher J. McDougle, MD, said in an interview.
“There are a number of things to say about [the study]. [One] of the strengths of the paper [is] the sample size,” Dr. McDougle said.“It’s always good to have a big sample size. The downside to having informant-databased information is that it is exactly what it is. This is fine, but the information may be inaccurate.”
In addition to parent-reported data, physicians are dealing with the relatively new diagnostic criteria. The May 2013 update of the Diagnostic and Statistical Manual of Mental Disorders to the DSM-5 brought with it the ability to diagnose ADHD with autism, when just the day before the DSM-5 was released, this differential diagnosis was not listed in the manual, Dr. McDougle said. “If something that important can change with the strike of the clock, it makes me concerned.” He also said listing the differential diagnosis in the diagnostic manual underscored the uncertainty of medicine’s understanding of comorbid autism and ADHD.
“That’s reflective of the field’s lack of knowledge. Sometimes I think we like to portray things as though we understand what’s going on, when I think it’s better to be honest and say we really don’t; we are just doing our best.”
Dr. McDougle is the director of the Lurie Center for Autism at Massachusetts General Hospital and is the Nancy Lurie Marks Professor of Psychiatry at Harvard Medical Center, both in Boston. He treats children, adolescents, and adults with autism spectrum disorder and other neurodevelopmental disorders. He was asked to comment on this study.
Children with comorbid autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) are at an increased risk of anxiety and mood disorders, a cross-sectional analysis has shown.
“Our study supports that anxiety and mood disorders, although highly prevalent in those with ASD alone, are even more prevalent in individuals who have ADHD,” wrote Eliza Gordon-Lipkin, MD, of the Kennedy Krieger Institute, Baltimore, and her associates. ”The identification of psychiatric conditions in children with ASD is important because these disorders are treatable and affect quality of life.”
The study was published in Pediatrics.
Most of the children were male (83%), white (87%), and non-Hispanic (92%); the mean age of the children was 10 years. Almost half of the children in the study had parent-reported ADHD (45%). Almost one-third of patients were diagnosed with an anxiety disorder (31%), and many also were reported to have been diagnosed with a mood disorder (16%). An increased risk of reported anxiety disorder was found in patients with both ADHD and ASD (adjusted relative risk, 2.20; 95% confidence interval, 1.97-2.46).
The researchers also found an increased risk of mood disorders (aRR, 2.72; 95% CI, 2.28-3.24) among children with comorbid conditions. Those risks increased with age (both P less than .001). An increased prevalence of anxiety and mood disorders was found in adolescents, compared with school-aged children with both ASD and ADHD or ASD alone. But higher relative risk ratios were found for the younger children, compared with the adolescents for those in the ADHD/ASD group and the ASD alone group.
“This suggests that or more likely to exhibit detectable symptoms at an earlier age,” reported Dr. Gordon-Lipkin, also with the department of pediatrics at Johns Hopkins University, in Baltimore.
The research team cited several limitations. For example, patient-reported data might be subject to recall or reporting biases. Also, computer and Internet access was required to complete the IAN questionnaires, which means that the findings could be biased toward people of higher socioeconomic status.
Nevertheless, the researchers wrote, their study is the largest to compare comorbidities in patients with ASD and ADHD, or ASD alone.
Further research is needed to better understand the relationship between ASD and ADHD. “ADHD affects nearly half of the children with ASD. This subgroup of individuals with ASD may represent a distinct clinical phenotype, with different diagnostic and therapeutic implications,” Dr. Gordon-Lipkin and her associates wrote. “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
None of the study authors had relevant financial disclosures to report. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
SOURCE: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
Children with comorbid autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD) are at an increased risk of anxiety and mood disorders, a cross-sectional analysis has shown.
“Our study supports that anxiety and mood disorders, although highly prevalent in those with ASD alone, are even more prevalent in individuals who have ADHD,” wrote Eliza Gordon-Lipkin, MD, of the Kennedy Krieger Institute, Baltimore, and her associates. ”The identification of psychiatric conditions in children with ASD is important because these disorders are treatable and affect quality of life.”
The study was published in Pediatrics.
Most of the children were male (83%), white (87%), and non-Hispanic (92%); the mean age of the children was 10 years. Almost half of the children in the study had parent-reported ADHD (45%). Almost one-third of patients were diagnosed with an anxiety disorder (31%), and many also were reported to have been diagnosed with a mood disorder (16%). An increased risk of reported anxiety disorder was found in patients with both ADHD and ASD (adjusted relative risk, 2.20; 95% confidence interval, 1.97-2.46).
The researchers also found an increased risk of mood disorders (aRR, 2.72; 95% CI, 2.28-3.24) among children with comorbid conditions. Those risks increased with age (both P less than .001). An increased prevalence of anxiety and mood disorders was found in adolescents, compared with school-aged children with both ASD and ADHD or ASD alone. But higher relative risk ratios were found for the younger children, compared with the adolescents for those in the ADHD/ASD group and the ASD alone group.
“This suggests that or more likely to exhibit detectable symptoms at an earlier age,” reported Dr. Gordon-Lipkin, also with the department of pediatrics at Johns Hopkins University, in Baltimore.
The research team cited several limitations. For example, patient-reported data might be subject to recall or reporting biases. Also, computer and Internet access was required to complete the IAN questionnaires, which means that the findings could be biased toward people of higher socioeconomic status.
Nevertheless, the researchers wrote, their study is the largest to compare comorbidities in patients with ASD and ADHD, or ASD alone.
Further research is needed to better understand the relationship between ASD and ADHD. “ADHD affects nearly half of the children with ASD. This subgroup of individuals with ASD may represent a distinct clinical phenotype, with different diagnostic and therapeutic implications,” Dr. Gordon-Lipkin and her associates wrote. “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
None of the study authors had relevant financial disclosures to report. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
SOURCE: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
FROM PEDIATRICS
Key clinical point: “Better understanding the differences between children with ASD with and without ADHD is crucial to designing effective interventions.”
Major finding: Sixteen percent of the children with autistic spectrum disorder had a mood disorder, and 31% had an anxiety disorder.
Study details: A cross-sectional analysis of information on 3,319 patients, obtained between 2006 and 2013 in the Interactive Autism Network (IAN), an online autism research registry that uses parent report information.
Disclosures: None of the study authors reported relevant financial disclosures. The Interactive Autism Network is funded by the Simons Foundation and the Patient-Centered Outcomes Research Institute.
Source: Gordon-Lipkin E et al. Pediatrics. 2018 Mar 30. doi: 10.1542/ peds.2017-1377.
Early reading aloud, play reduced hyperactivity at school entry
and had sustained behavioral effects after the program was completed, according to results of a randomized clinical trial.
The Video Interaction Project (VIP), in which parents review and reflect upon recordings of themselves interacting with their children, is a low-cost, scalable intervention that has a “high potential” for enhancing social and emotional development by reducing disruptive behaviors, the study authors reported in Pediatrics.
The study included 675 parent-child dyads enrolled post partum at an urban public hospital serving low-income families. Of that group, 450 families were randomized to the VIP program from 0 to 3 years of age, a control group, or a third group that included a different intervention called Building Blocks that incorporates parenting education newsletters, learning materials, and parent questionnaires.
In the VIP intervention, parent-child dyads participated in up to 15 one-on-one sessions from 2 weeks of age to 3 years. In each 30-minute session, the parent and child were video recorded for 5 minutes of play or shared reading; immediately afterward, the parent would review the video with a bilingual facilitator to identify positive interactions and reflect on them.
As previously reported, the VIP intervention had enhanced children’s social and emotional development. Compared with controls, children in the VIP group had higher scores in imitation/play and attention at the end of the program and lower scores in separation distress, hyperactivity, and externalizing problems, according to investigators.
Now, investigators are reporting results that include a second phase of random assignment to VIP from 3-5 years or a control group. The second-phase VIP intervention included nine 30- to 45-minute sessions enhanced with new strategies designed to support the rapidly emerging developmental capacities of preschoolers, Dr. Mendelsohn and associates said. Ultimately, 252 families completed the 4.5 year assessment.
Those new strategies included building sessions around themes (such as birthday party), incorporation of writing into play (such as party invitations), focusing on story characters’ feelings, and video recording both reading and play, with the story serving as the basis for the play.
The initial VIP 0-3 year intervention and the VIP 3-5 year intervention were both independently associated with improved T-scores at 4.5 years on Behavior Assessment System for Children, Second Edition, rating scales, with Cohen’s d effect sizes ranging from approximately –0.25 to –0.30, according to investigators.
Participating in both VIP interventions was associated with a significant reduction in hyperactivity (effect size, –0.63; P = 0.001), Dr. Mendelsohn and his associates also reported.
Moreover, participation in the first VIP session was associated with a reduction in clinically significant hyperactivity (relative risk reduction, 69%; P = .03), they added.
The cost of the VIP program for 0-3 years is approximately $175-$200 per child per year, including staff, equipment, rent, and other expenses, according to the report, which notes that one interventionist can provide services for 400-500 families.
Taken together, these findings suggest the VIP intervention is a low-cost intervention that may prevent poverty-related disparities, investigators said.
“In this study, we provide strong support for the use of pediatric primary care to promote positive parenting activities such as reading aloud and play and the potential for such programs to promote social-emotional development as reflected through reductions in disruptive behaviors,” they wrote.
Dr. Mendelsohn and his coauthors reported no relevant financial disclosures. The study was supported by grants from the National Institutes of Health and the National Institute of Child Health and Human Development; the Tiger Foundation; the Marks Family Foundation; Children of Bellevue; KiDS of New York University Foundation; and Rhodebeck Charitable Trust. Several of the investigators were supported in part by awards or grants.
SOURCE: Mendelsohn AL et al. Pediatrics. 2018;141(5):e20173393.
and had sustained behavioral effects after the program was completed, according to results of a randomized clinical trial.
The Video Interaction Project (VIP), in which parents review and reflect upon recordings of themselves interacting with their children, is a low-cost, scalable intervention that has a “high potential” for enhancing social and emotional development by reducing disruptive behaviors, the study authors reported in Pediatrics.
The study included 675 parent-child dyads enrolled post partum at an urban public hospital serving low-income families. Of that group, 450 families were randomized to the VIP program from 0 to 3 years of age, a control group, or a third group that included a different intervention called Building Blocks that incorporates parenting education newsletters, learning materials, and parent questionnaires.
In the VIP intervention, parent-child dyads participated in up to 15 one-on-one sessions from 2 weeks of age to 3 years. In each 30-minute session, the parent and child were video recorded for 5 minutes of play or shared reading; immediately afterward, the parent would review the video with a bilingual facilitator to identify positive interactions and reflect on them.
As previously reported, the VIP intervention had enhanced children’s social and emotional development. Compared with controls, children in the VIP group had higher scores in imitation/play and attention at the end of the program and lower scores in separation distress, hyperactivity, and externalizing problems, according to investigators.
Now, investigators are reporting results that include a second phase of random assignment to VIP from 3-5 years or a control group. The second-phase VIP intervention included nine 30- to 45-minute sessions enhanced with new strategies designed to support the rapidly emerging developmental capacities of preschoolers, Dr. Mendelsohn and associates said. Ultimately, 252 families completed the 4.5 year assessment.
Those new strategies included building sessions around themes (such as birthday party), incorporation of writing into play (such as party invitations), focusing on story characters’ feelings, and video recording both reading and play, with the story serving as the basis for the play.
The initial VIP 0-3 year intervention and the VIP 3-5 year intervention were both independently associated with improved T-scores at 4.5 years on Behavior Assessment System for Children, Second Edition, rating scales, with Cohen’s d effect sizes ranging from approximately –0.25 to –0.30, according to investigators.
Participating in both VIP interventions was associated with a significant reduction in hyperactivity (effect size, –0.63; P = 0.001), Dr. Mendelsohn and his associates also reported.
Moreover, participation in the first VIP session was associated with a reduction in clinically significant hyperactivity (relative risk reduction, 69%; P = .03), they added.
The cost of the VIP program for 0-3 years is approximately $175-$200 per child per year, including staff, equipment, rent, and other expenses, according to the report, which notes that one interventionist can provide services for 400-500 families.
Taken together, these findings suggest the VIP intervention is a low-cost intervention that may prevent poverty-related disparities, investigators said.
“In this study, we provide strong support for the use of pediatric primary care to promote positive parenting activities such as reading aloud and play and the potential for such programs to promote social-emotional development as reflected through reductions in disruptive behaviors,” they wrote.
Dr. Mendelsohn and his coauthors reported no relevant financial disclosures. The study was supported by grants from the National Institutes of Health and the National Institute of Child Health and Human Development; the Tiger Foundation; the Marks Family Foundation; Children of Bellevue; KiDS of New York University Foundation; and Rhodebeck Charitable Trust. Several of the investigators were supported in part by awards or grants.
SOURCE: Mendelsohn AL et al. Pediatrics. 2018;141(5):e20173393.
and had sustained behavioral effects after the program was completed, according to results of a randomized clinical trial.
The Video Interaction Project (VIP), in which parents review and reflect upon recordings of themselves interacting with their children, is a low-cost, scalable intervention that has a “high potential” for enhancing social and emotional development by reducing disruptive behaviors, the study authors reported in Pediatrics.
The study included 675 parent-child dyads enrolled post partum at an urban public hospital serving low-income families. Of that group, 450 families were randomized to the VIP program from 0 to 3 years of age, a control group, or a third group that included a different intervention called Building Blocks that incorporates parenting education newsletters, learning materials, and parent questionnaires.
In the VIP intervention, parent-child dyads participated in up to 15 one-on-one sessions from 2 weeks of age to 3 years. In each 30-minute session, the parent and child were video recorded for 5 minutes of play or shared reading; immediately afterward, the parent would review the video with a bilingual facilitator to identify positive interactions and reflect on them.
As previously reported, the VIP intervention had enhanced children’s social and emotional development. Compared with controls, children in the VIP group had higher scores in imitation/play and attention at the end of the program and lower scores in separation distress, hyperactivity, and externalizing problems, according to investigators.
Now, investigators are reporting results that include a second phase of random assignment to VIP from 3-5 years or a control group. The second-phase VIP intervention included nine 30- to 45-minute sessions enhanced with new strategies designed to support the rapidly emerging developmental capacities of preschoolers, Dr. Mendelsohn and associates said. Ultimately, 252 families completed the 4.5 year assessment.
Those new strategies included building sessions around themes (such as birthday party), incorporation of writing into play (such as party invitations), focusing on story characters’ feelings, and video recording both reading and play, with the story serving as the basis for the play.
The initial VIP 0-3 year intervention and the VIP 3-5 year intervention were both independently associated with improved T-scores at 4.5 years on Behavior Assessment System for Children, Second Edition, rating scales, with Cohen’s d effect sizes ranging from approximately –0.25 to –0.30, according to investigators.
Participating in both VIP interventions was associated with a significant reduction in hyperactivity (effect size, –0.63; P = 0.001), Dr. Mendelsohn and his associates also reported.
Moreover, participation in the first VIP session was associated with a reduction in clinically significant hyperactivity (relative risk reduction, 69%; P = .03), they added.
The cost of the VIP program for 0-3 years is approximately $175-$200 per child per year, including staff, equipment, rent, and other expenses, according to the report, which notes that one interventionist can provide services for 400-500 families.
Taken together, these findings suggest the VIP intervention is a low-cost intervention that may prevent poverty-related disparities, investigators said.
“In this study, we provide strong support for the use of pediatric primary care to promote positive parenting activities such as reading aloud and play and the potential for such programs to promote social-emotional development as reflected through reductions in disruptive behaviors,” they wrote.
Dr. Mendelsohn and his coauthors reported no relevant financial disclosures. The study was supported by grants from the National Institutes of Health and the National Institute of Child Health and Human Development; the Tiger Foundation; the Marks Family Foundation; Children of Bellevue; KiDS of New York University Foundation; and Rhodebeck Charitable Trust. Several of the investigators were supported in part by awards or grants.
SOURCE: Mendelsohn AL et al. Pediatrics. 2018;141(5):e20173393.
FROM PEDIATRICS
Key clinical point: A video-based intervention designed to promote parent-child reading aloud and play reduced hyperactivity at school entry and had sustained behavioral effects over time.
Major finding: Parent-child participation in the Video Interaction Project (VIP) was independently associated with improved T-scores at 4.5 years on Behavior Assessment System for Children, Second Edition, rating scales, with effect sizes ranging from approximately –0.25 to –0.30.
Study details: A randomized controlled trial including 450 families enrolled at an urban public hospital that serves low-income families.
Disclosures: The researchers reported no relevant financial disclosures. The study was supported by grants from the National Institutes of Health and the National Institute of Child Health and Human Development; the Tiger Foundation; the Marks Family Foundation; Children of Bellevue; KiDS of New York University Foundation; and Rhodebeck Charitable Trust. Several of the investigators were supported in part by awards or grants.
Source: Mendelsohn AL et al. Pediatrics. 2018;141(5):e20173393.