User login
‘Shed the Lead’ and the Injuries. Should Cath Labs Go Lead-Free?
“I’d probably be a quadriplegic,” Dean J. Kereiakes, MD, an interventional cardiologist, said when asked what would have happened if two top neurosurgeons at his hospital hadn’t rushed him to the operating room (OR) for a cervical decompression in February this year.
Dr. Kereiakes had orthopedic problems for years due to the heavy lead aprons he wore in the cath lab. He regularly dosed himself with steroids for disc pain so he could stand up straight and continue to do procedures. “Several times a year I’d go on a tapering dose of prednisone of about 10 days to 2 weeks, and this would take care of it.”
But then his luck ran out. “I’m told in retrospect that my gait — the way I walked — was different, and I was also having some myoclonic jerking in my legs when I was going to sleep. I thought it was peculiar, but I didn’t really tie it together that this was an upper tract injury response.”
At a restaurant with his wife, he found himself unable to sign the check. “I couldn’t write my name.” By the next morning, “I had a floppy right foot, and as I turned around to put my scrubs on, everything fell apart. My arms began to not function and my legs — I couldn’t walk.”
Admitted to The Christ Hospital Heart & Vascular Center in Cincinnati — the very hospital he works in — Dr. Kereiakes had CT and MRI scans and consulted with neurosurgeons he counts as friends. He was given extremely high doses of intravenous steroids. “But instead of getting better, the pain came back, and I started posturing — when you posture, it looks like a praying mantis, your arms are flexed up, your wrists are flexed, and your fingers are spasmed together.” His wife and the nurses couldn’t pull his fingers open, “so they rolled me back, and the posturing started to go away.”
This prompted the neurosurgeons to bring him to the OR “by 6 a.m., and they are ‘unzipping me in the back’ to basically get my spinal cord off my spine. I had cord compression at C2-3 and C 6-7.”
Postop, Dr. Kereiakes couldn’t move his right leg and couldn’t close any of his fingers. “You lose control of things like bladder and bowel function — you have a catheter in — and you say to yourself, ‘How am I going to live like this?.’ ”
The quick-thinking of his neurosurgeons prevented permanent paralysis, and after a long 6-month recovery, Dr. Kereiakes is back in the cath lab, performing procedures. But crucially, he will no longer have to wear a lead apron.
Ending Careers Early. A Catalyst for Change
Typically, interventional cardiologists, interventional radiologists, electrophysiologists, and others working in labs where they are exposed to ionizing radiation wear lead aprons and garments, such as thyroid collars, leaded caps, and glasses, to protect them during procedures.
Long-term occupational exposure to radiation is linked to cataracts; brain tumors; cancers, including leukemia, multiple myelomas, lymphomas, and thyroid cancers; and left-sided breast cancers in women because the aprons don’t always cover the left side of the chest adequately.
Individual states set the standards in terms of the thickness of the lead required, varying from 0.25- to 0.5-mm–lead-equivalent aprons, which reduce exposure by 85%-95%. Radiation safety officers monitor the badges that staff wear to record their radiation exposure and will warn them when their levels are too high.
But — as Dr. Kereiakes freely admits — ambitious interventionalists don’t always take much notice. “They would come and say, ‘Hey your badge is really high,’ and so I would just put it in a drawer and carry on,” he said. “When you are younger, you feel immortal.”
James B. Hermiller Jr., MD, president of the Society for Cardiovascular Angiography & Interventions (SCAI), agrees: “The feeling is that, with lead, you are indestructible, and no one wants to show any weakness.”
Another occupational hazard related to those protective lead aprons was also being ignored, that of orthopedic injury. In surveys done by SCAI, around half of interventional cardiology respondents report cervical, lumbar, hip, knee, or ankle joint injuries.
While Dr. Kereiakes recognizes likely bias — with those afflicted more likely to complete these surveys — he believes that the problem is huge and “is ending careers early.”
“It’s interesting that radiation is at the forefront of protection and occupational safety, but you are much more likely to be taken out of work because of orthopedic injury,” explained Dr. Hermiller, director of Structural Heart Program at Ascension St. Vincent Heart Center in Indianapolis.
His own story “is not as compelling as Dean’s, but 17 years ago, I ruptured a disk in my lower spine and had emergent surgery and I now need a neck surgery.”
Dr. Hermiller’s hospital, too, has purchased multiple radiation protection systems. “If you want to do this job for 30 years, you have to protect yourself early and at all times,” he said.
His focus as SCAI president is to help get these protection systems in place at more hospitals.
But significant challenges remain, not least the cost, which can be $150,000-$200,000 per lab. He estimates that fewer than 10% US hospitals with cath and other labs using radiation have installed such systems.
Most systems are not US Food and Drug Administration (FDA) approved because they are not attached to equipment in the cath lab, something that Nadia Sutton, MD, MPH, chair of the SCAI Women in Innovations committee, said many physicians are not aware of. “The companies [marketing the systems] are telling us that we can ‘shed our lead,’ ” she said. “It could be safe, but we are using the data provided by the companies.”
How Do the Lead-Free Systems Work?
Currently, there are three main radiation protection systems available. The Protego Radiation Protection System (Image Diagnostics), the EggNest Protect (Egg Medical), and the Rampart (Rampart ic).
According to Dr. Kereiakes, they differ somewhat in whether they allow immediate access to the patient or whether you can see and interact with them. He explained that in high-risk procedures, easy access is desirable. “If you get a perforation or tamponade and the patient suddenly goes ‘out,’ you need to be able to get to them quickly, and you can’t be spending a lot of time taking the shielding down.”
Dr. Kereiakes was recovering in the hospital when his colleagues plumped for the EggNest system. He thinks they chose it because it offers visibility and access to the patient and “takes 4-5 minutes, maximum, to set up.” So far, he agrees with the choice but wants to “give it a real, volume-driven try.”
If they are satisfied with the system, the hospital will order six more by the end of the year, he said. A significant financial undertaking, he acknowledged.
Dr. Hermiller cited data for the Rampart system showing a 95% reduction in radiation without any lead. For an average 1-GRAY radiation exposure case, “if you wear lead, you reach the maximum dose of radiation around 850 cases in a year. If you do it with one of these protection systems, in this case Rampart, you can do 14,500 cases in a year. Not that anyone would do that [many].”
The Protego system has very similar data, he noted. The systems protect the operator and whoever is scrubbing in at the table, so those on the other side of the protector still need to wear lead, Dr. Hermiller stressed.
Data for the EggNest Protect are available but are as yet unpublished.
Dr. Hermiller acknowledged that there is still a long way to go in getting hospitals to spend the money on these systems, but he thinks cath lab operators will drive the change.
“At our SCAI meeting this year, the biggest attendance was at a session about a lead-free cath lab environment.”
Regulation at the State Level
Despite the excitement among the profession, Dr. Sutton — director of Interventional Cardiology Research in the Division of Cardiovascular Medicine at Vanderbilt University Medical Center, Nashville, Tennessee — still has concerns about the lack of FDA regulation.
There is one newer system, called the Radiaction shield system, that attaches to the existing equipment so that is regulated by the FDA as a class II device, she noted. “But it is my understanding that the Protego, Rampart, and EggNest are Class I Exempt. That is the same category as Band-Aid.”
James Beabout, MBA, chief marketing officer, Egg Medical, confirmed that the EggNest “is classified as a Class I device which does not require FDA approval. That leaves regulation to each state regarding the requirements for protective aprons.” And Mark Hansen, vice president business development, of Image Diagnostics — the manufacturer of the Protego Radiation Protection System — confirmed that “the real governance is at the state level.”
The company petitions the state regulator for an exemption letter to the wearing of lead aprons. “In some cases, the state will come to the site directly and validate the systems integrity and to confirm their decision. Once the exemption is granted, the state sends a document, and it’s the responsibility of the sites’ Radiation Safety Officer (RSO) to change the labs safety process and rules,” Mr. Hansen explained.
“What really makes this work is a real-time dosimetry from Fluke Medical. Staff wear one to two badges that instantly detects exposure,” Mr. Hansen stressed.
Similarly, said Mr. Beabout, Egg Medical has data from over 1000 real-world cases collected using real-time dosimetry (RaySafe i3 system) which demonstrate that it is possible to get some people in the room out of protective aprons, where allowed. They recommend real-time dosimetry anytime people are removing their aprons, “since the patient BMI, x-ray system type/age, and complexity of the case all have a significant effect on the radiation dose in each case.” Their goal is for exposure to be zero or as close to zero as possible, “otherwise we recommend use of protective aprons. With the EggNest, operators can use much lighter aprons (0.125 mm sold by Burlington Medical) than what has traditionally been used, so that is also an option,” he said.
Dr. Hermiller said the SCAI plan is to produce several statements on going lead-free, with all other interested professional societies — such as those representing interventional radiologists and vascular surgeons, as well as all the major cardiology societies.
“We want to make an intellectual foundation for this,” Dr. Hermiller explained. Guidelines “are in the making,” he said, with the expectation that they will be ready by the end of this year or early next year.
SCAI will also work with the 50 US states to facilitate lead-free labs, “as each one has a different way to be approved to go without lead,” he noted.
“This is not going to go away, it’s going to build in force, through the societies,” said Dr. Kereiakes. “It’s a matter of workplace safety.” He doesn’t think that the federal Occupational Health and Safety Administration does much to protect doctors, nurses, and technicians in the cath and other labs.
Dr. Hermiller agreed: “I always say that if we were a GM car plant, they would shut us down.”
Dr. Hermiller also stressed the expense of having doctors and other staff off work with occupation-related injuries. He has already observed that “it’s much easier to recruit cath lab staff to a place where they don’t have to wear lead.”
He anticipates that the next generation of physicians “are going to demand places where they don’t have to wear lead.” He is also hopeful that it will result in more women choosing interventional cardiology: “Women are safe in the cath lab with current lead systems, but if we could move to this, there would be even more women participating.”
Pregnancy Safe in the Cath Lab
Dr. Sutton reiterated his point: “The number-one message that I want to get across is that it is considered safe for the unborn baby, being in the cath lab, under lead,” she said, noting that there are very good data that the amount of lead that is required by states results in negligible radiation exposure to the developing fetus.
She had her children before working in the cath lab, “but I’ve heard from other women: It’s heavy and its sweaty for prolonged periods of time, but it can be done and you can get through it,” she said. Although the promise of radiation protection systems “is exciting, we have to approach this with some level of caution or awareness,” she said. “Cardiologists come from a cardiology background. We are not radiologists who go through a radiology residency, like IRs do. They get a lot of training on radiation exposure and what it means,” Dr. Sutton stressed.
Dr. Kereiakes, for his part, remains enthusiastic. He returned to the cath lab in August, just 6 months after his brush with near quadriplegia. “This is what I’ve spent my life doing and I love doing it, and I’m not ready to quit.”
Dr. Hermiller, Dr. Kereiakes, and Dr. Sutton reported having no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
“I’d probably be a quadriplegic,” Dean J. Kereiakes, MD, an interventional cardiologist, said when asked what would have happened if two top neurosurgeons at his hospital hadn’t rushed him to the operating room (OR) for a cervical decompression in February this year.
Dr. Kereiakes had orthopedic problems for years due to the heavy lead aprons he wore in the cath lab. He regularly dosed himself with steroids for disc pain so he could stand up straight and continue to do procedures. “Several times a year I’d go on a tapering dose of prednisone of about 10 days to 2 weeks, and this would take care of it.”
But then his luck ran out. “I’m told in retrospect that my gait — the way I walked — was different, and I was also having some myoclonic jerking in my legs when I was going to sleep. I thought it was peculiar, but I didn’t really tie it together that this was an upper tract injury response.”
At a restaurant with his wife, he found himself unable to sign the check. “I couldn’t write my name.” By the next morning, “I had a floppy right foot, and as I turned around to put my scrubs on, everything fell apart. My arms began to not function and my legs — I couldn’t walk.”
Admitted to The Christ Hospital Heart & Vascular Center in Cincinnati — the very hospital he works in — Dr. Kereiakes had CT and MRI scans and consulted with neurosurgeons he counts as friends. He was given extremely high doses of intravenous steroids. “But instead of getting better, the pain came back, and I started posturing — when you posture, it looks like a praying mantis, your arms are flexed up, your wrists are flexed, and your fingers are spasmed together.” His wife and the nurses couldn’t pull his fingers open, “so they rolled me back, and the posturing started to go away.”
This prompted the neurosurgeons to bring him to the OR “by 6 a.m., and they are ‘unzipping me in the back’ to basically get my spinal cord off my spine. I had cord compression at C2-3 and C 6-7.”
Postop, Dr. Kereiakes couldn’t move his right leg and couldn’t close any of his fingers. “You lose control of things like bladder and bowel function — you have a catheter in — and you say to yourself, ‘How am I going to live like this?.’ ”
The quick-thinking of his neurosurgeons prevented permanent paralysis, and after a long 6-month recovery, Dr. Kereiakes is back in the cath lab, performing procedures. But crucially, he will no longer have to wear a lead apron.
Ending Careers Early. A Catalyst for Change
Typically, interventional cardiologists, interventional radiologists, electrophysiologists, and others working in labs where they are exposed to ionizing radiation wear lead aprons and garments, such as thyroid collars, leaded caps, and glasses, to protect them during procedures.
Long-term occupational exposure to radiation is linked to cataracts; brain tumors; cancers, including leukemia, multiple myelomas, lymphomas, and thyroid cancers; and left-sided breast cancers in women because the aprons don’t always cover the left side of the chest adequately.
Individual states set the standards in terms of the thickness of the lead required, varying from 0.25- to 0.5-mm–lead-equivalent aprons, which reduce exposure by 85%-95%. Radiation safety officers monitor the badges that staff wear to record their radiation exposure and will warn them when their levels are too high.
But — as Dr. Kereiakes freely admits — ambitious interventionalists don’t always take much notice. “They would come and say, ‘Hey your badge is really high,’ and so I would just put it in a drawer and carry on,” he said. “When you are younger, you feel immortal.”
James B. Hermiller Jr., MD, president of the Society for Cardiovascular Angiography & Interventions (SCAI), agrees: “The feeling is that, with lead, you are indestructible, and no one wants to show any weakness.”
Another occupational hazard related to those protective lead aprons was also being ignored, that of orthopedic injury. In surveys done by SCAI, around half of interventional cardiology respondents report cervical, lumbar, hip, knee, or ankle joint injuries.
While Dr. Kereiakes recognizes likely bias — with those afflicted more likely to complete these surveys — he believes that the problem is huge and “is ending careers early.”
“It’s interesting that radiation is at the forefront of protection and occupational safety, but you are much more likely to be taken out of work because of orthopedic injury,” explained Dr. Hermiller, director of Structural Heart Program at Ascension St. Vincent Heart Center in Indianapolis.
His own story “is not as compelling as Dean’s, but 17 years ago, I ruptured a disk in my lower spine and had emergent surgery and I now need a neck surgery.”
Dr. Hermiller’s hospital, too, has purchased multiple radiation protection systems. “If you want to do this job for 30 years, you have to protect yourself early and at all times,” he said.
His focus as SCAI president is to help get these protection systems in place at more hospitals.
But significant challenges remain, not least the cost, which can be $150,000-$200,000 per lab. He estimates that fewer than 10% US hospitals with cath and other labs using radiation have installed such systems.
Most systems are not US Food and Drug Administration (FDA) approved because they are not attached to equipment in the cath lab, something that Nadia Sutton, MD, MPH, chair of the SCAI Women in Innovations committee, said many physicians are not aware of. “The companies [marketing the systems] are telling us that we can ‘shed our lead,’ ” she said. “It could be safe, but we are using the data provided by the companies.”
How Do the Lead-Free Systems Work?
Currently, there are three main radiation protection systems available. The Protego Radiation Protection System (Image Diagnostics), the EggNest Protect (Egg Medical), and the Rampart (Rampart ic).
According to Dr. Kereiakes, they differ somewhat in whether they allow immediate access to the patient or whether you can see and interact with them. He explained that in high-risk procedures, easy access is desirable. “If you get a perforation or tamponade and the patient suddenly goes ‘out,’ you need to be able to get to them quickly, and you can’t be spending a lot of time taking the shielding down.”
Dr. Kereiakes was recovering in the hospital when his colleagues plumped for the EggNest system. He thinks they chose it because it offers visibility and access to the patient and “takes 4-5 minutes, maximum, to set up.” So far, he agrees with the choice but wants to “give it a real, volume-driven try.”
If they are satisfied with the system, the hospital will order six more by the end of the year, he said. A significant financial undertaking, he acknowledged.
Dr. Hermiller cited data for the Rampart system showing a 95% reduction in radiation without any lead. For an average 1-GRAY radiation exposure case, “if you wear lead, you reach the maximum dose of radiation around 850 cases in a year. If you do it with one of these protection systems, in this case Rampart, you can do 14,500 cases in a year. Not that anyone would do that [many].”
The Protego system has very similar data, he noted. The systems protect the operator and whoever is scrubbing in at the table, so those on the other side of the protector still need to wear lead, Dr. Hermiller stressed.
Data for the EggNest Protect are available but are as yet unpublished.
Dr. Hermiller acknowledged that there is still a long way to go in getting hospitals to spend the money on these systems, but he thinks cath lab operators will drive the change.
“At our SCAI meeting this year, the biggest attendance was at a session about a lead-free cath lab environment.”
Regulation at the State Level
Despite the excitement among the profession, Dr. Sutton — director of Interventional Cardiology Research in the Division of Cardiovascular Medicine at Vanderbilt University Medical Center, Nashville, Tennessee — still has concerns about the lack of FDA regulation.
There is one newer system, called the Radiaction shield system, that attaches to the existing equipment so that is regulated by the FDA as a class II device, she noted. “But it is my understanding that the Protego, Rampart, and EggNest are Class I Exempt. That is the same category as Band-Aid.”
James Beabout, MBA, chief marketing officer, Egg Medical, confirmed that the EggNest “is classified as a Class I device which does not require FDA approval. That leaves regulation to each state regarding the requirements for protective aprons.” And Mark Hansen, vice president business development, of Image Diagnostics — the manufacturer of the Protego Radiation Protection System — confirmed that “the real governance is at the state level.”
The company petitions the state regulator for an exemption letter to the wearing of lead aprons. “In some cases, the state will come to the site directly and validate the systems integrity and to confirm their decision. Once the exemption is granted, the state sends a document, and it’s the responsibility of the sites’ Radiation Safety Officer (RSO) to change the labs safety process and rules,” Mr. Hansen explained.
“What really makes this work is a real-time dosimetry from Fluke Medical. Staff wear one to two badges that instantly detects exposure,” Mr. Hansen stressed.
Similarly, said Mr. Beabout, Egg Medical has data from over 1000 real-world cases collected using real-time dosimetry (RaySafe i3 system) which demonstrate that it is possible to get some people in the room out of protective aprons, where allowed. They recommend real-time dosimetry anytime people are removing their aprons, “since the patient BMI, x-ray system type/age, and complexity of the case all have a significant effect on the radiation dose in each case.” Their goal is for exposure to be zero or as close to zero as possible, “otherwise we recommend use of protective aprons. With the EggNest, operators can use much lighter aprons (0.125 mm sold by Burlington Medical) than what has traditionally been used, so that is also an option,” he said.
Dr. Hermiller said the SCAI plan is to produce several statements on going lead-free, with all other interested professional societies — such as those representing interventional radiologists and vascular surgeons, as well as all the major cardiology societies.
“We want to make an intellectual foundation for this,” Dr. Hermiller explained. Guidelines “are in the making,” he said, with the expectation that they will be ready by the end of this year or early next year.
SCAI will also work with the 50 US states to facilitate lead-free labs, “as each one has a different way to be approved to go without lead,” he noted.
“This is not going to go away, it’s going to build in force, through the societies,” said Dr. Kereiakes. “It’s a matter of workplace safety.” He doesn’t think that the federal Occupational Health and Safety Administration does much to protect doctors, nurses, and technicians in the cath and other labs.
Dr. Hermiller agreed: “I always say that if we were a GM car plant, they would shut us down.”
Dr. Hermiller also stressed the expense of having doctors and other staff off work with occupation-related injuries. He has already observed that “it’s much easier to recruit cath lab staff to a place where they don’t have to wear lead.”
He anticipates that the next generation of physicians “are going to demand places where they don’t have to wear lead.” He is also hopeful that it will result in more women choosing interventional cardiology: “Women are safe in the cath lab with current lead systems, but if we could move to this, there would be even more women participating.”
Pregnancy Safe in the Cath Lab
Dr. Sutton reiterated his point: “The number-one message that I want to get across is that it is considered safe for the unborn baby, being in the cath lab, under lead,” she said, noting that there are very good data that the amount of lead that is required by states results in negligible radiation exposure to the developing fetus.
She had her children before working in the cath lab, “but I’ve heard from other women: It’s heavy and its sweaty for prolonged periods of time, but it can be done and you can get through it,” she said. Although the promise of radiation protection systems “is exciting, we have to approach this with some level of caution or awareness,” she said. “Cardiologists come from a cardiology background. We are not radiologists who go through a radiology residency, like IRs do. They get a lot of training on radiation exposure and what it means,” Dr. Sutton stressed.
Dr. Kereiakes, for his part, remains enthusiastic. He returned to the cath lab in August, just 6 months after his brush with near quadriplegia. “This is what I’ve spent my life doing and I love doing it, and I’m not ready to quit.”
Dr. Hermiller, Dr. Kereiakes, and Dr. Sutton reported having no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
“I’d probably be a quadriplegic,” Dean J. Kereiakes, MD, an interventional cardiologist, said when asked what would have happened if two top neurosurgeons at his hospital hadn’t rushed him to the operating room (OR) for a cervical decompression in February this year.
Dr. Kereiakes had orthopedic problems for years due to the heavy lead aprons he wore in the cath lab. He regularly dosed himself with steroids for disc pain so he could stand up straight and continue to do procedures. “Several times a year I’d go on a tapering dose of prednisone of about 10 days to 2 weeks, and this would take care of it.”
But then his luck ran out. “I’m told in retrospect that my gait — the way I walked — was different, and I was also having some myoclonic jerking in my legs when I was going to sleep. I thought it was peculiar, but I didn’t really tie it together that this was an upper tract injury response.”
At a restaurant with his wife, he found himself unable to sign the check. “I couldn’t write my name.” By the next morning, “I had a floppy right foot, and as I turned around to put my scrubs on, everything fell apart. My arms began to not function and my legs — I couldn’t walk.”
Admitted to The Christ Hospital Heart & Vascular Center in Cincinnati — the very hospital he works in — Dr. Kereiakes had CT and MRI scans and consulted with neurosurgeons he counts as friends. He was given extremely high doses of intravenous steroids. “But instead of getting better, the pain came back, and I started posturing — when you posture, it looks like a praying mantis, your arms are flexed up, your wrists are flexed, and your fingers are spasmed together.” His wife and the nurses couldn’t pull his fingers open, “so they rolled me back, and the posturing started to go away.”
This prompted the neurosurgeons to bring him to the OR “by 6 a.m., and they are ‘unzipping me in the back’ to basically get my spinal cord off my spine. I had cord compression at C2-3 and C 6-7.”
Postop, Dr. Kereiakes couldn’t move his right leg and couldn’t close any of his fingers. “You lose control of things like bladder and bowel function — you have a catheter in — and you say to yourself, ‘How am I going to live like this?.’ ”
The quick-thinking of his neurosurgeons prevented permanent paralysis, and after a long 6-month recovery, Dr. Kereiakes is back in the cath lab, performing procedures. But crucially, he will no longer have to wear a lead apron.
Ending Careers Early. A Catalyst for Change
Typically, interventional cardiologists, interventional radiologists, electrophysiologists, and others working in labs where they are exposed to ionizing radiation wear lead aprons and garments, such as thyroid collars, leaded caps, and glasses, to protect them during procedures.
Long-term occupational exposure to radiation is linked to cataracts; brain tumors; cancers, including leukemia, multiple myelomas, lymphomas, and thyroid cancers; and left-sided breast cancers in women because the aprons don’t always cover the left side of the chest adequately.
Individual states set the standards in terms of the thickness of the lead required, varying from 0.25- to 0.5-mm–lead-equivalent aprons, which reduce exposure by 85%-95%. Radiation safety officers monitor the badges that staff wear to record their radiation exposure and will warn them when their levels are too high.
But — as Dr. Kereiakes freely admits — ambitious interventionalists don’t always take much notice. “They would come and say, ‘Hey your badge is really high,’ and so I would just put it in a drawer and carry on,” he said. “When you are younger, you feel immortal.”
James B. Hermiller Jr., MD, president of the Society for Cardiovascular Angiography & Interventions (SCAI), agrees: “The feeling is that, with lead, you are indestructible, and no one wants to show any weakness.”
Another occupational hazard related to those protective lead aprons was also being ignored, that of orthopedic injury. In surveys done by SCAI, around half of interventional cardiology respondents report cervical, lumbar, hip, knee, or ankle joint injuries.
While Dr. Kereiakes recognizes likely bias — with those afflicted more likely to complete these surveys — he believes that the problem is huge and “is ending careers early.”
“It’s interesting that radiation is at the forefront of protection and occupational safety, but you are much more likely to be taken out of work because of orthopedic injury,” explained Dr. Hermiller, director of Structural Heart Program at Ascension St. Vincent Heart Center in Indianapolis.
His own story “is not as compelling as Dean’s, but 17 years ago, I ruptured a disk in my lower spine and had emergent surgery and I now need a neck surgery.”
Dr. Hermiller’s hospital, too, has purchased multiple radiation protection systems. “If you want to do this job for 30 years, you have to protect yourself early and at all times,” he said.
His focus as SCAI president is to help get these protection systems in place at more hospitals.
But significant challenges remain, not least the cost, which can be $150,000-$200,000 per lab. He estimates that fewer than 10% US hospitals with cath and other labs using radiation have installed such systems.
Most systems are not US Food and Drug Administration (FDA) approved because they are not attached to equipment in the cath lab, something that Nadia Sutton, MD, MPH, chair of the SCAI Women in Innovations committee, said many physicians are not aware of. “The companies [marketing the systems] are telling us that we can ‘shed our lead,’ ” she said. “It could be safe, but we are using the data provided by the companies.”
How Do the Lead-Free Systems Work?
Currently, there are three main radiation protection systems available. The Protego Radiation Protection System (Image Diagnostics), the EggNest Protect (Egg Medical), and the Rampart (Rampart ic).
According to Dr. Kereiakes, they differ somewhat in whether they allow immediate access to the patient or whether you can see and interact with them. He explained that in high-risk procedures, easy access is desirable. “If you get a perforation or tamponade and the patient suddenly goes ‘out,’ you need to be able to get to them quickly, and you can’t be spending a lot of time taking the shielding down.”
Dr. Kereiakes was recovering in the hospital when his colleagues plumped for the EggNest system. He thinks they chose it because it offers visibility and access to the patient and “takes 4-5 minutes, maximum, to set up.” So far, he agrees with the choice but wants to “give it a real, volume-driven try.”
If they are satisfied with the system, the hospital will order six more by the end of the year, he said. A significant financial undertaking, he acknowledged.
Dr. Hermiller cited data for the Rampart system showing a 95% reduction in radiation without any lead. For an average 1-GRAY radiation exposure case, “if you wear lead, you reach the maximum dose of radiation around 850 cases in a year. If you do it with one of these protection systems, in this case Rampart, you can do 14,500 cases in a year. Not that anyone would do that [many].”
The Protego system has very similar data, he noted. The systems protect the operator and whoever is scrubbing in at the table, so those on the other side of the protector still need to wear lead, Dr. Hermiller stressed.
Data for the EggNest Protect are available but are as yet unpublished.
Dr. Hermiller acknowledged that there is still a long way to go in getting hospitals to spend the money on these systems, but he thinks cath lab operators will drive the change.
“At our SCAI meeting this year, the biggest attendance was at a session about a lead-free cath lab environment.”
Regulation at the State Level
Despite the excitement among the profession, Dr. Sutton — director of Interventional Cardiology Research in the Division of Cardiovascular Medicine at Vanderbilt University Medical Center, Nashville, Tennessee — still has concerns about the lack of FDA regulation.
There is one newer system, called the Radiaction shield system, that attaches to the existing equipment so that is regulated by the FDA as a class II device, she noted. “But it is my understanding that the Protego, Rampart, and EggNest are Class I Exempt. That is the same category as Band-Aid.”
James Beabout, MBA, chief marketing officer, Egg Medical, confirmed that the EggNest “is classified as a Class I device which does not require FDA approval. That leaves regulation to each state regarding the requirements for protective aprons.” And Mark Hansen, vice president business development, of Image Diagnostics — the manufacturer of the Protego Radiation Protection System — confirmed that “the real governance is at the state level.”
The company petitions the state regulator for an exemption letter to the wearing of lead aprons. “In some cases, the state will come to the site directly and validate the systems integrity and to confirm their decision. Once the exemption is granted, the state sends a document, and it’s the responsibility of the sites’ Radiation Safety Officer (RSO) to change the labs safety process and rules,” Mr. Hansen explained.
“What really makes this work is a real-time dosimetry from Fluke Medical. Staff wear one to two badges that instantly detects exposure,” Mr. Hansen stressed.
Similarly, said Mr. Beabout, Egg Medical has data from over 1000 real-world cases collected using real-time dosimetry (RaySafe i3 system) which demonstrate that it is possible to get some people in the room out of protective aprons, where allowed. They recommend real-time dosimetry anytime people are removing their aprons, “since the patient BMI, x-ray system type/age, and complexity of the case all have a significant effect on the radiation dose in each case.” Their goal is for exposure to be zero or as close to zero as possible, “otherwise we recommend use of protective aprons. With the EggNest, operators can use much lighter aprons (0.125 mm sold by Burlington Medical) than what has traditionally been used, so that is also an option,” he said.
Dr. Hermiller said the SCAI plan is to produce several statements on going lead-free, with all other interested professional societies — such as those representing interventional radiologists and vascular surgeons, as well as all the major cardiology societies.
“We want to make an intellectual foundation for this,” Dr. Hermiller explained. Guidelines “are in the making,” he said, with the expectation that they will be ready by the end of this year or early next year.
SCAI will also work with the 50 US states to facilitate lead-free labs, “as each one has a different way to be approved to go without lead,” he noted.
“This is not going to go away, it’s going to build in force, through the societies,” said Dr. Kereiakes. “It’s a matter of workplace safety.” He doesn’t think that the federal Occupational Health and Safety Administration does much to protect doctors, nurses, and technicians in the cath and other labs.
Dr. Hermiller agreed: “I always say that if we were a GM car plant, they would shut us down.”
Dr. Hermiller also stressed the expense of having doctors and other staff off work with occupation-related injuries. He has already observed that “it’s much easier to recruit cath lab staff to a place where they don’t have to wear lead.”
He anticipates that the next generation of physicians “are going to demand places where they don’t have to wear lead.” He is also hopeful that it will result in more women choosing interventional cardiology: “Women are safe in the cath lab with current lead systems, but if we could move to this, there would be even more women participating.”
Pregnancy Safe in the Cath Lab
Dr. Sutton reiterated his point: “The number-one message that I want to get across is that it is considered safe for the unborn baby, being in the cath lab, under lead,” she said, noting that there are very good data that the amount of lead that is required by states results in negligible radiation exposure to the developing fetus.
She had her children before working in the cath lab, “but I’ve heard from other women: It’s heavy and its sweaty for prolonged periods of time, but it can be done and you can get through it,” she said. Although the promise of radiation protection systems “is exciting, we have to approach this with some level of caution or awareness,” she said. “Cardiologists come from a cardiology background. We are not radiologists who go through a radiology residency, like IRs do. They get a lot of training on radiation exposure and what it means,” Dr. Sutton stressed.
Dr. Kereiakes, for his part, remains enthusiastic. He returned to the cath lab in August, just 6 months after his brush with near quadriplegia. “This is what I’ve spent my life doing and I love doing it, and I’m not ready to quit.”
Dr. Hermiller, Dr. Kereiakes, and Dr. Sutton reported having no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
Old, Frail Patients: Study More, Intervene Less?
Lessons From SENIOR-RITA
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lessons From SENIOR-RITA
Lessons From SENIOR-RITA
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The ability to save cardiac muscle during an acute coronary syndrome with percutaneous coronary intervention (PCI) made cardiology one of the most popular fields in medicine.
But acute coronary syndromes come in different categories. While rapid PCI clearly benefits patients with ST-segment elevation myocardial infarction (STEMI), the best use of angiography and PCI for patients with non–ST-segment elevation myocardial infarction (NSTEMI) is more complex.
There have been many trials and meta-analyses, and generally, outcomes are similar with either approach. Perhaps if one looks with enough optimism, there is a benefit for the more aggressive approach in higher-risk patients.
Despite the similar outcomes with the two strategies, most patients are treated with the early invasive approach. Early and invasive fit the spirit of modern cardiology.
Yet, older patients with acute coronary syndromes present a different challenge. NSTEMI trials, like most trials, enrolled mostly younger adults.
Whether evidence obtained in young people applies to older patients is one of the most common and important questions in all of medical practice. Older patients may be at higher risk for a primary outcome, but they also have greater risks for harm from therapy as well as more competing causes of morbidity and mortality.
Only a handful of smaller trials have enrolled older patients with NSTEMI. These trials have produced little evidence that an early invasive approach should be preferred.
The SENIOR-RITA Trial
At ESC, Vijay Kunadian, MD, from Newcastle, England, presented results of SENIOR-RITA, a large trial comparing an invasive vs conservative strategy in NSTEMI patients 75 years of age or older.
In the conservative arm, coronary angiography was allowed if the patient deteriorated and the procedure was clinically indicated in the judgment of the treating physicians.
Slightly more than 1500 patients with NSTEMI were randomly assigned to either strategy in 48 centers in the United Kingdom. Their mean age was 82 years, nearly half were women, and about a third were frail.
Over 4 years of follow-up, the primary outcome of cardiovascular (CV) death or MI occurred at a similar rate in both arms: 25.6% vs 26.3% for invasive vs conservative, respectively (HR, 0.94; 95% CI, 0.77-1.14; P =.53).
Rates of CV death were also not significantly different (15.8% vs 14.2%; HR, 1.11; 95% CI, 0.86-1.44).
The rate of nonfatal MI was slightly lower in the invasive arm (11.7% vs 15.0%; HR, 0.75; 95% CI, 0.57-0.99).
Some other notable findings: Fewer than half of patients in the invasive arm underwent revascularization. Coronary angiography was done in about a quarter of patients in the conservative arm, and revascularization in only 14%.
Comments
Because medicine has improved and patients live longer, cardiologists increasingly see older adults with frailty. It’s important to study these patients.
The authors tell us that 1 in 5 patients screened were enrolled, and those not enrolled were similar in age and were treated nearly equally with either strategy. Not all trials offer this information; it’s important because knowing that patients in a trial are representative helps us translate evidence to our actual patients.
Another positive was the investigators’ smart choice of cardiovascular death and MI as their primary outcome. Strategy trials are usually open label. If they had included an outcome that requires a decision from a clinician, such as unplanned revascularization, then bias becomes a possibility when patients and clinicians are aware of the treatment assignment. (I wrote about poor endpoint choice in the ABYSS trial.)
The most notable finding in SENIOR-RITA was that approximately 76% of patients in the conservative arm did not have a coronary angiogram and 86% were not revascularized.
Yet, the rate of CV death and MI were similar during 4 years of follow-up. This observation is nearly identical to the findings in chronic stable disease, seen in the ISCHEMIA trial. (See Figure 6a in the paper’s supplement.)
I take two messages from this consistent observation: One is that medical therapy is quite good at treating coronary artery disease not associated with acute vessel closure in STEMI.
The other is that using coronary angiography and revascularization as a bailout, in only a fraction of cases, achieves the same result, so the conservative strategy should be preferred.
I am not sure that the SENIOR-RITA researchers see it this way. They write in their discussion that “clinicians are often reluctant to offer an invasive strategy to frail older adults.” They then remind readers that modern PCI techniques (radial approach) have low rates of adverse events.
Perhaps I misread their message, but that paragraph seemed like it was reinforcing our tendency to offer invasive approaches to patients with NSTEMI.
I feel differently. When a trial reports similar outcomes with two strategies, I think we should favor the one with less intervention. I feel even more strongly about this philosophy in older patients with frailty.
Are we not in the business of helping people with the least amount of intervention?
The greatest challenge for the cardiologist of today is not a lack of treatment options, but whether we should use all options in older, frailer adults.
Good on the SENIOR-RITA investigators, for they have shown that we can avoid intervention in the vast majority of older adults presenting with NSTEMI.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Kentucky, and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Do Cannabis Users Need More Anesthesia During Surgery?
TOPLINE:
However, the clinical relevance of this difference remains unclear.
METHODOLOGY:
- To assess if cannabis use leads to higher doses of inhalational anesthesia during surgery, the researchers conducted a retrospective cohort study comparing the average intraoperative minimum alveolar concentrations of volatile anesthetics (isoflurane and sevoflurane) between older adults who used cannabis products and those who did not.
- The researchers reviewed electronic health records of 22,476 patients aged 65 years or older who underwent surgery at the University of Florida Health System between 2018 and 2020.
- Overall, 268 patients who reported using cannabis within 60 days of surgery (median age, 69 years; 35% women) were matched to 1072 nonusers.
- The median duration of anesthesia was 175 minutes.
- The primary outcome was the intraoperative time-weighted average of isoflurane or sevoflurane minimum alveolar concentration equivalents.
TAKEAWAY:
- Cannabis users had significantly higher average minimum alveolar concentrations of isoflurane or sevoflurane than nonusers (mean, 0.58 vs 0.54; mean difference, 0.04; P = .021).
- The findings were confirmed in a sensitivity analysis that revealed higher mean average minimum alveolar concentrations of anesthesia in cannabis users than in nonusers (0.57 vs 0.53; P = .029).
- Although the 0.04 difference in minimum alveolar concentration between cannabis users and nonusers was statistically significant, its clinical importance is unclear.
IN PRACTICE:
“While recent guidelines underscore the importance of universal screening for cannabinoids before surgery, caution is paramount to prevent clinical bias leading to the administration of unnecessary higher doses of inhalational anesthesia, especially as robust evidence supporting such practices remains lacking,” the authors of the study wrote.
SOURCE:
This study was led by Ruba Sajdeya, MD, PhD, of the Department of Epidemiology at the University of Florida, Gainesville, and was published online in August 2024 in Anesthesiology.
LIMITATIONS:
This study lacked access to prescription or dispensed medications, including opioids, which may have introduced residual confounding. Potential underdocumentation of cannabis use in medical records could have led to exposure misclassification. The causality between cannabis usage and increased anesthetic dosing could not be established due to the observational nature of this study.
DISCLOSURES:
This study was supported by the National Institute on Aging, the National Institutes of Health, and in part by the University of Florida Clinical and Translational Science Institute. Some authors declared receiving research support, consulting fees, and honoraria and having other ties with pharmaceutical companies and various other sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
However, the clinical relevance of this difference remains unclear.
METHODOLOGY:
- To assess if cannabis use leads to higher doses of inhalational anesthesia during surgery, the researchers conducted a retrospective cohort study comparing the average intraoperative minimum alveolar concentrations of volatile anesthetics (isoflurane and sevoflurane) between older adults who used cannabis products and those who did not.
- The researchers reviewed electronic health records of 22,476 patients aged 65 years or older who underwent surgery at the University of Florida Health System between 2018 and 2020.
- Overall, 268 patients who reported using cannabis within 60 days of surgery (median age, 69 years; 35% women) were matched to 1072 nonusers.
- The median duration of anesthesia was 175 minutes.
- The primary outcome was the intraoperative time-weighted average of isoflurane or sevoflurane minimum alveolar concentration equivalents.
TAKEAWAY:
- Cannabis users had significantly higher average minimum alveolar concentrations of isoflurane or sevoflurane than nonusers (mean, 0.58 vs 0.54; mean difference, 0.04; P = .021).
- The findings were confirmed in a sensitivity analysis that revealed higher mean average minimum alveolar concentrations of anesthesia in cannabis users than in nonusers (0.57 vs 0.53; P = .029).
- Although the 0.04 difference in minimum alveolar concentration between cannabis users and nonusers was statistically significant, its clinical importance is unclear.
IN PRACTICE:
“While recent guidelines underscore the importance of universal screening for cannabinoids before surgery, caution is paramount to prevent clinical bias leading to the administration of unnecessary higher doses of inhalational anesthesia, especially as robust evidence supporting such practices remains lacking,” the authors of the study wrote.
SOURCE:
This study was led by Ruba Sajdeya, MD, PhD, of the Department of Epidemiology at the University of Florida, Gainesville, and was published online in August 2024 in Anesthesiology.
LIMITATIONS:
This study lacked access to prescription or dispensed medications, including opioids, which may have introduced residual confounding. Potential underdocumentation of cannabis use in medical records could have led to exposure misclassification. The causality between cannabis usage and increased anesthetic dosing could not be established due to the observational nature of this study.
DISCLOSURES:
This study was supported by the National Institute on Aging, the National Institutes of Health, and in part by the University of Florida Clinical and Translational Science Institute. Some authors declared receiving research support, consulting fees, and honoraria and having other ties with pharmaceutical companies and various other sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
However, the clinical relevance of this difference remains unclear.
METHODOLOGY:
- To assess if cannabis use leads to higher doses of inhalational anesthesia during surgery, the researchers conducted a retrospective cohort study comparing the average intraoperative minimum alveolar concentrations of volatile anesthetics (isoflurane and sevoflurane) between older adults who used cannabis products and those who did not.
- The researchers reviewed electronic health records of 22,476 patients aged 65 years or older who underwent surgery at the University of Florida Health System between 2018 and 2020.
- Overall, 268 patients who reported using cannabis within 60 days of surgery (median age, 69 years; 35% women) were matched to 1072 nonusers.
- The median duration of anesthesia was 175 minutes.
- The primary outcome was the intraoperative time-weighted average of isoflurane or sevoflurane minimum alveolar concentration equivalents.
TAKEAWAY:
- Cannabis users had significantly higher average minimum alveolar concentrations of isoflurane or sevoflurane than nonusers (mean, 0.58 vs 0.54; mean difference, 0.04; P = .021).
- The findings were confirmed in a sensitivity analysis that revealed higher mean average minimum alveolar concentrations of anesthesia in cannabis users than in nonusers (0.57 vs 0.53; P = .029).
- Although the 0.04 difference in minimum alveolar concentration between cannabis users and nonusers was statistically significant, its clinical importance is unclear.
IN PRACTICE:
“While recent guidelines underscore the importance of universal screening for cannabinoids before surgery, caution is paramount to prevent clinical bias leading to the administration of unnecessary higher doses of inhalational anesthesia, especially as robust evidence supporting such practices remains lacking,” the authors of the study wrote.
SOURCE:
This study was led by Ruba Sajdeya, MD, PhD, of the Department of Epidemiology at the University of Florida, Gainesville, and was published online in August 2024 in Anesthesiology.
LIMITATIONS:
This study lacked access to prescription or dispensed medications, including opioids, which may have introduced residual confounding. Potential underdocumentation of cannabis use in medical records could have led to exposure misclassification. The causality between cannabis usage and increased anesthetic dosing could not be established due to the observational nature of this study.
DISCLOSURES:
This study was supported by the National Institute on Aging, the National Institutes of Health, and in part by the University of Florida Clinical and Translational Science Institute. Some authors declared receiving research support, consulting fees, and honoraria and having other ties with pharmaceutical companies and various other sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Not Kidding: Yellow Dye 5 May Lead to Invisibility
Applying the dye to lab mice made their skin temporarily transparent, allowing Stanford University researchers to observe the rodents’ digestive system, muscle fibers, and blood vessels, according to a study published in Science.
“It’s a stunning result,” said senior author Guosong Hong, PhD, who is assistant professor of materials science and engineering at Stanford University in California. “If the same technique could be applied to humans, it could offer a variety of benefits in biology, diagnostics, and even cosmetics.”
The work drew upon optical concepts first described in the early 20th century to form a surprising theory: Applying a light-absorbing substance could render skin transparent by reducing the chaotic scattering of light as it strikes proteins, fats, and water in tissue.
A search for a suitable light absorber led to FD&C Yellow 5, also called tartrazine, a synthetic color additive certified by the Food and Drug Administration (FDA) for use in foods, cosmetics, and medications.
Rubbed on live mice (after areas of fur were removed using a drugstore depilatory cream), tartrazine rendered skin on their bellies, hind legs, and heads transparent within 5 minutes. With the naked eye, the researchers watched a mouse’s intestines, bladder, and liver at work. Using a microscope, they observed muscle fibers and saw blood vessels in a living mouse’s brain — all without making incisions. Transparency faded quickly when the dye was washed off.
Someday, the concept could be used in doctors’ offices and hospitals, Dr. Hong said.
“Instead of relying on invasive biopsies, doctors might be able to diagnose deep-seated tumors by simply examining a person’s tissue without the need for invasive surgical removal,” he said. “This technique could potentially make blood draws less painful by helping phlebotomists easily locate veins under the skin. It could also enhance procedures like laser tattoo removal by allowing more precise targeting of the pigment beneath the skin.”
From Cake Frosting to Groundbreaking Research
Yellow 5 food dye can be found in everything from cereal, soda, spices, and cake frosting to lipstick, mouthwash, shampoo, dietary supplements, and house paint. Although it’s in some topical medications, more research is needed before it could be used in human diagnostics, said Christopher J. Rowlands, PhD, a senior lecturer in the Department of Bioengineering at Imperial College London, England, where he studies biophotonic instrumentation — ways to image structures inside the body more quickly and clearly.
But the finding could prove useful in research. In a commentary published in Science, Dr. Rowlands and his colleague Jon Gorecki, PhD, an experimental optical physicist also at Imperial College London, noted that the dye could be an alternative to other optical clearing agents currently used in lab studies, such as glycerol, fructose, or acetic acid. Advantages are the effect is reversible and works at lower concentrations with fewer side effects. This could broaden the types of studies possible in lab animals, so researchers don’t have to rely on naturally transparent creatures like nematodes and zebrafish.
The dye could also be paired with imaging techniques such as MRI or electron microscopy.
“Imaging techniques all have pros and cons,” Dr. Rowlands said. “MRI can see all the way through the body albeit with limited resolution and contrast. Electron microscopy has excellent resolution but limited compatibility with live tissue and penetration depth. Optical microscopy has subcellular resolution, the ability to label things, excellent biocompatibility but less than 1 millimeter of penetration depth. This clearing method will give a substantial boost to optical imaging for medicine and biology.”
The discovery could improve the depth imaging equipment can achieve by tenfold, according to the commentary.
Brain research especially stands to benefit. “Neurobiology in particular will have great use for combinations of multiphoton, optogenetics, and tissue clearing to record and control neural activity over (potentially) the whole mouse brain,” he said.
Refraction, Absorption, and The Invisible Man
The dye discovery has distant echoes in H.G. Wells’ 1897 novel The Invisible Man, Dr. Rowlands noted. In the book, a serum makes the main character invisible by changing the light scattering — or refractive index (RI) — of his cells to match the air around him.
The Stanford engineers looked to the past for inspiration, but not to fiction. They turned to a concept first described in the 1920s called the Kramers-Kronig relations, a mathematical principle that can be applied to relationships between the way light is refracted and absorbed in different materials. They also read up on Lorentz oscillation, which describes how electrons and atoms inside molecules react to light.
They reasoned that light-absorbing compounds could equalize the differences between the light-scattering properties of proteins, lipids, and water that make skin opaque.
With that, the search was on. The study’s first author, postdoctoral researcher Zihao Ou, PhD, began testing strong dyes to find a candidate. Tartrazine was a front-runner.
“We found that dye molecules are more efficient in raising the refractive index of water than conventional RI-matching agents, thus resulting in transparency at a much lower concentration,” Dr. Hong said. “The underlying physics, explained by the Lorentz oscillator model and Kramers-Kronig relations, reveals that conventional RI matching agents like fructose are not as efficient because they are not ‘colored’ enough.”
What’s Next
Though the dye is already in products that people consume and apply to their skin, medical use is years away. In some people, tartrazine can cause skin or respiratory reactions.
The National Science Foundation (NSF), which helped fund the research, posted a home or classroom activity related to the work on its website. It involves painting a tartrazine solution on a thin slice of raw chicken breast, making it transparent. The experiment should only be done while wearing a mask, eye protection, lab coat, and lab-quality nitrile gloves for protection, according to the NSF.
Meanwhile, Dr. Hong said his lab is looking for new compounds that will improve visibility through transparent skin, removing a red tone seen in the current experiments. And they’re looking for ways to induce cells to make their own “see-through” compounds.
“We are exploring methods for cells to express intensely absorbing molecules endogenously, enabling genetically encoded tissue transparency in live animals,” he said.
A version of this article first appeared on Medscape.com.
Applying the dye to lab mice made their skin temporarily transparent, allowing Stanford University researchers to observe the rodents’ digestive system, muscle fibers, and blood vessels, according to a study published in Science.
“It’s a stunning result,” said senior author Guosong Hong, PhD, who is assistant professor of materials science and engineering at Stanford University in California. “If the same technique could be applied to humans, it could offer a variety of benefits in biology, diagnostics, and even cosmetics.”
The work drew upon optical concepts first described in the early 20th century to form a surprising theory: Applying a light-absorbing substance could render skin transparent by reducing the chaotic scattering of light as it strikes proteins, fats, and water in tissue.
A search for a suitable light absorber led to FD&C Yellow 5, also called tartrazine, a synthetic color additive certified by the Food and Drug Administration (FDA) for use in foods, cosmetics, and medications.
Rubbed on live mice (after areas of fur were removed using a drugstore depilatory cream), tartrazine rendered skin on their bellies, hind legs, and heads transparent within 5 minutes. With the naked eye, the researchers watched a mouse’s intestines, bladder, and liver at work. Using a microscope, they observed muscle fibers and saw blood vessels in a living mouse’s brain — all without making incisions. Transparency faded quickly when the dye was washed off.
Someday, the concept could be used in doctors’ offices and hospitals, Dr. Hong said.
“Instead of relying on invasive biopsies, doctors might be able to diagnose deep-seated tumors by simply examining a person’s tissue without the need for invasive surgical removal,” he said. “This technique could potentially make blood draws less painful by helping phlebotomists easily locate veins under the skin. It could also enhance procedures like laser tattoo removal by allowing more precise targeting of the pigment beneath the skin.”
From Cake Frosting to Groundbreaking Research
Yellow 5 food dye can be found in everything from cereal, soda, spices, and cake frosting to lipstick, mouthwash, shampoo, dietary supplements, and house paint. Although it’s in some topical medications, more research is needed before it could be used in human diagnostics, said Christopher J. Rowlands, PhD, a senior lecturer in the Department of Bioengineering at Imperial College London, England, where he studies biophotonic instrumentation — ways to image structures inside the body more quickly and clearly.
But the finding could prove useful in research. In a commentary published in Science, Dr. Rowlands and his colleague Jon Gorecki, PhD, an experimental optical physicist also at Imperial College London, noted that the dye could be an alternative to other optical clearing agents currently used in lab studies, such as glycerol, fructose, or acetic acid. Advantages are the effect is reversible and works at lower concentrations with fewer side effects. This could broaden the types of studies possible in lab animals, so researchers don’t have to rely on naturally transparent creatures like nematodes and zebrafish.
The dye could also be paired with imaging techniques such as MRI or electron microscopy.
“Imaging techniques all have pros and cons,” Dr. Rowlands said. “MRI can see all the way through the body albeit with limited resolution and contrast. Electron microscopy has excellent resolution but limited compatibility with live tissue and penetration depth. Optical microscopy has subcellular resolution, the ability to label things, excellent biocompatibility but less than 1 millimeter of penetration depth. This clearing method will give a substantial boost to optical imaging for medicine and biology.”
The discovery could improve the depth imaging equipment can achieve by tenfold, according to the commentary.
Brain research especially stands to benefit. “Neurobiology in particular will have great use for combinations of multiphoton, optogenetics, and tissue clearing to record and control neural activity over (potentially) the whole mouse brain,” he said.
Refraction, Absorption, and The Invisible Man
The dye discovery has distant echoes in H.G. Wells’ 1897 novel The Invisible Man, Dr. Rowlands noted. In the book, a serum makes the main character invisible by changing the light scattering — or refractive index (RI) — of his cells to match the air around him.
The Stanford engineers looked to the past for inspiration, but not to fiction. They turned to a concept first described in the 1920s called the Kramers-Kronig relations, a mathematical principle that can be applied to relationships between the way light is refracted and absorbed in different materials. They also read up on Lorentz oscillation, which describes how electrons and atoms inside molecules react to light.
They reasoned that light-absorbing compounds could equalize the differences between the light-scattering properties of proteins, lipids, and water that make skin opaque.
With that, the search was on. The study’s first author, postdoctoral researcher Zihao Ou, PhD, began testing strong dyes to find a candidate. Tartrazine was a front-runner.
“We found that dye molecules are more efficient in raising the refractive index of water than conventional RI-matching agents, thus resulting in transparency at a much lower concentration,” Dr. Hong said. “The underlying physics, explained by the Lorentz oscillator model and Kramers-Kronig relations, reveals that conventional RI matching agents like fructose are not as efficient because they are not ‘colored’ enough.”
What’s Next
Though the dye is already in products that people consume and apply to their skin, medical use is years away. In some people, tartrazine can cause skin or respiratory reactions.
The National Science Foundation (NSF), which helped fund the research, posted a home or classroom activity related to the work on its website. It involves painting a tartrazine solution on a thin slice of raw chicken breast, making it transparent. The experiment should only be done while wearing a mask, eye protection, lab coat, and lab-quality nitrile gloves for protection, according to the NSF.
Meanwhile, Dr. Hong said his lab is looking for new compounds that will improve visibility through transparent skin, removing a red tone seen in the current experiments. And they’re looking for ways to induce cells to make their own “see-through” compounds.
“We are exploring methods for cells to express intensely absorbing molecules endogenously, enabling genetically encoded tissue transparency in live animals,” he said.
A version of this article first appeared on Medscape.com.
Applying the dye to lab mice made their skin temporarily transparent, allowing Stanford University researchers to observe the rodents’ digestive system, muscle fibers, and blood vessels, according to a study published in Science.
“It’s a stunning result,” said senior author Guosong Hong, PhD, who is assistant professor of materials science and engineering at Stanford University in California. “If the same technique could be applied to humans, it could offer a variety of benefits in biology, diagnostics, and even cosmetics.”
The work drew upon optical concepts first described in the early 20th century to form a surprising theory: Applying a light-absorbing substance could render skin transparent by reducing the chaotic scattering of light as it strikes proteins, fats, and water in tissue.
A search for a suitable light absorber led to FD&C Yellow 5, also called tartrazine, a synthetic color additive certified by the Food and Drug Administration (FDA) for use in foods, cosmetics, and medications.
Rubbed on live mice (after areas of fur were removed using a drugstore depilatory cream), tartrazine rendered skin on their bellies, hind legs, and heads transparent within 5 minutes. With the naked eye, the researchers watched a mouse’s intestines, bladder, and liver at work. Using a microscope, they observed muscle fibers and saw blood vessels in a living mouse’s brain — all without making incisions. Transparency faded quickly when the dye was washed off.
Someday, the concept could be used in doctors’ offices and hospitals, Dr. Hong said.
“Instead of relying on invasive biopsies, doctors might be able to diagnose deep-seated tumors by simply examining a person’s tissue without the need for invasive surgical removal,” he said. “This technique could potentially make blood draws less painful by helping phlebotomists easily locate veins under the skin. It could also enhance procedures like laser tattoo removal by allowing more precise targeting of the pigment beneath the skin.”
From Cake Frosting to Groundbreaking Research
Yellow 5 food dye can be found in everything from cereal, soda, spices, and cake frosting to lipstick, mouthwash, shampoo, dietary supplements, and house paint. Although it’s in some topical medications, more research is needed before it could be used in human diagnostics, said Christopher J. Rowlands, PhD, a senior lecturer in the Department of Bioengineering at Imperial College London, England, where he studies biophotonic instrumentation — ways to image structures inside the body more quickly and clearly.
But the finding could prove useful in research. In a commentary published in Science, Dr. Rowlands and his colleague Jon Gorecki, PhD, an experimental optical physicist also at Imperial College London, noted that the dye could be an alternative to other optical clearing agents currently used in lab studies, such as glycerol, fructose, or acetic acid. Advantages are the effect is reversible and works at lower concentrations with fewer side effects. This could broaden the types of studies possible in lab animals, so researchers don’t have to rely on naturally transparent creatures like nematodes and zebrafish.
The dye could also be paired with imaging techniques such as MRI or electron microscopy.
“Imaging techniques all have pros and cons,” Dr. Rowlands said. “MRI can see all the way through the body albeit with limited resolution and contrast. Electron microscopy has excellent resolution but limited compatibility with live tissue and penetration depth. Optical microscopy has subcellular resolution, the ability to label things, excellent biocompatibility but less than 1 millimeter of penetration depth. This clearing method will give a substantial boost to optical imaging for medicine and biology.”
The discovery could improve the depth imaging equipment can achieve by tenfold, according to the commentary.
Brain research especially stands to benefit. “Neurobiology in particular will have great use for combinations of multiphoton, optogenetics, and tissue clearing to record and control neural activity over (potentially) the whole mouse brain,” he said.
Refraction, Absorption, and The Invisible Man
The dye discovery has distant echoes in H.G. Wells’ 1897 novel The Invisible Man, Dr. Rowlands noted. In the book, a serum makes the main character invisible by changing the light scattering — or refractive index (RI) — of his cells to match the air around him.
The Stanford engineers looked to the past for inspiration, but not to fiction. They turned to a concept first described in the 1920s called the Kramers-Kronig relations, a mathematical principle that can be applied to relationships between the way light is refracted and absorbed in different materials. They also read up on Lorentz oscillation, which describes how electrons and atoms inside molecules react to light.
They reasoned that light-absorbing compounds could equalize the differences between the light-scattering properties of proteins, lipids, and water that make skin opaque.
With that, the search was on. The study’s first author, postdoctoral researcher Zihao Ou, PhD, began testing strong dyes to find a candidate. Tartrazine was a front-runner.
“We found that dye molecules are more efficient in raising the refractive index of water than conventional RI-matching agents, thus resulting in transparency at a much lower concentration,” Dr. Hong said. “The underlying physics, explained by the Lorentz oscillator model and Kramers-Kronig relations, reveals that conventional RI matching agents like fructose are not as efficient because they are not ‘colored’ enough.”
What’s Next
Though the dye is already in products that people consume and apply to their skin, medical use is years away. In some people, tartrazine can cause skin or respiratory reactions.
The National Science Foundation (NSF), which helped fund the research, posted a home or classroom activity related to the work on its website. It involves painting a tartrazine solution on a thin slice of raw chicken breast, making it transparent. The experiment should only be done while wearing a mask, eye protection, lab coat, and lab-quality nitrile gloves for protection, according to the NSF.
Meanwhile, Dr. Hong said his lab is looking for new compounds that will improve visibility through transparent skin, removing a red tone seen in the current experiments. And they’re looking for ways to induce cells to make their own “see-through” compounds.
“We are exploring methods for cells to express intensely absorbing molecules endogenously, enabling genetically encoded tissue transparency in live animals,” he said.
A version of this article first appeared on Medscape.com.
FROM SCIENCE
Cell Phone Use Linked to Higher Heart Disease Risk
“We found that a poor sleep pattern, psychological distress, and neuroticism significantly mediated the positive association between weekly mobile phone usage time and the risk for incident CVD, with a mediating proportion of 5.11%, 11.50%, and 2.25%, respectively,” said principal investigator Xianhui Qin, MD, professor of nephrology at Southern Medical University, Guangzhou, China.
Poor sleep patterns and poor mental health could disrupt circadian rhythms and endocrine and metabolic functions, as well as increase inflammation, he explained.
In addition, chronic exposure to radiofrequency electromagnetic fields (RF-EMF) emitted from cell phones could lead to oxidative stress and an inflammatory response. Combined with smoking and diabetes, this exposure “may have a synergistic effect in increasing CVD risk,” Dr. Qin suggested.
The study was published online in the Canadian Journal of Cardiology.
Risk Underestimated?
The researchers aimed to examine the association of regular cell phone use with incident CVD and explore the mediating effects of sleep and mental health using linked hospital and mortality records.
Their analysis included 444,027 participants (mean age, 56 years; 44% men) without a history of CVD from the UK Biobank. A total of 378,161 participants were regular cell phone users.
Regular cell phone use was defined as at least one call per week. Weekly use was self-reported as the average time of calls per week during the previous 3 months.
The primary outcome was incident CVD. Secondary outcomes were each component of CVD (ie, coronary heart disease, stroke, atrial fibrillation, and heart failure) and increased carotid intima media thickness (CIMT).
Compared with nonregular cell phone users, regular users were younger, had higher proportions of current smokers and urban residents, and had lower proportions of history of hypertension and diabetes. They also had higher income, Townsend deprivation index, and body mass index, and lower education levels.
During a median follow-up of 12.3 years, 56,181 participants developed incident CVD. Compared with nonregular cell phone users, regular users had a significantly higher risk for incident CVD (hazard ratio, 1.04) and increased CIMT (odds ratio, 1.11).
Among regular cell phone users, the duration of cell phone use and hands-free device/speakerphone use during calls was not significantly associated with incident CVD. Yet a significant and positive dose-response relationship was seen between weekly cell phone usage time and the risk for CVD. The positive association was stronger in current vs noncurrent smokers and people with vs without diabetes.
To different extents, sleep patterns (5.11%), psychologic distress (11.5%), and neuroticism (2.25%) mediated the relationship between weekly cell phone usage time and the risk for incident CVD.
“Our study suggests that despite the advantages of mobile phone use, we should also pay attention to the potential harm of mobile phone use to cardiovascular health,” Dr. Qin said. “Future studies to assess the risk-benefit balance will help promote mobile phone use patterns that are conducive to cardiovascular health.”
Meanwhile, he added, “We encourage measures to reduce time spent on mobile phones to promote the primary prevention of CVD. On the other hand, improving sleep and mental health status may help reduce the higher risk of CVD associated with mobile phone use.”
There are several limitations to the study in addition to its observational nature, which cannot show cause and effect. The questionnaires on cell phone use were restricted to phone calls; other use patterns of cell phones (eg, messaging, watching videos, and browsing the web) were not considered. Although the researchers adjusted for many potential confounders, unmeasured confounding bias (eg, the type of cell phone used and other sources of RF-EMF) cannot be eliminated.
Weak Link?
In a comment, Nicholas Grubic, MSc, a PhD student in epidemiology at the University of Toronto, Ontario, Canada, and coauthor of a related editorial, said, “I found it interesting that there was a connection observed between mobile phone use and CVD. However, it is crucial to understand that this link appeared to be much weaker compared with other well-known cardiovascular risk factors, such as smoking, diabetes, and high blood pressure. For now, mobile phone use should not be a major concern for most people.”
Nevertheless, clinicians should encourage patients to practice healthy habits around their screen time, he advised. “This could include limiting mobile phone use before bedtime and taking regular breaks to engage in activities that promote heart health, such as exercising or spending time outdoors.
“For the time being, we probably won’t see mobile phone use included in standard assessments for cardiovascular risk or as a focal point of cardiovascular health promotion initiatives,” he added. Instead, clinicians should “focus on established risk factors that have a stronger impact on patients’ cardiovascular health.”
Nieca Goldberg, MD, a clinical associate professor of medicine at NYU Grossman School of Medicine in New York City and American Heart Association volunteer expert, had a similar message. “You don’t have to go back to using a landline,” she said. “Instead, patients should be more mindful of how much phone use is taking away from their physical activity, keeping them from sleeping, and causing them stress.” Clinicians should also remember to counsel smokers on smoking cessation.
“It would be important for future studies to look at time spent on the phone and the type of activities patients are doing on their phones, such as social media, calls, texts, movies, or streaming TV shows,” she said. “It would be important to see how phone use is leading to a sedentary lifestyle” and what that means for a larger, more diverse population.
The study was supported by the National Key R&D Program, the National Natural Science Foundation of China, and the Outstanding Youth Development Scheme of Nanfang Hospital, Southern Medical University. Dr. Qin, Dr. Grubic, and Dr. Goldberg reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We found that a poor sleep pattern, psychological distress, and neuroticism significantly mediated the positive association between weekly mobile phone usage time and the risk for incident CVD, with a mediating proportion of 5.11%, 11.50%, and 2.25%, respectively,” said principal investigator Xianhui Qin, MD, professor of nephrology at Southern Medical University, Guangzhou, China.
Poor sleep patterns and poor mental health could disrupt circadian rhythms and endocrine and metabolic functions, as well as increase inflammation, he explained.
In addition, chronic exposure to radiofrequency electromagnetic fields (RF-EMF) emitted from cell phones could lead to oxidative stress and an inflammatory response. Combined with smoking and diabetes, this exposure “may have a synergistic effect in increasing CVD risk,” Dr. Qin suggested.
The study was published online in the Canadian Journal of Cardiology.
Risk Underestimated?
The researchers aimed to examine the association of regular cell phone use with incident CVD and explore the mediating effects of sleep and mental health using linked hospital and mortality records.
Their analysis included 444,027 participants (mean age, 56 years; 44% men) without a history of CVD from the UK Biobank. A total of 378,161 participants were regular cell phone users.
Regular cell phone use was defined as at least one call per week. Weekly use was self-reported as the average time of calls per week during the previous 3 months.
The primary outcome was incident CVD. Secondary outcomes were each component of CVD (ie, coronary heart disease, stroke, atrial fibrillation, and heart failure) and increased carotid intima media thickness (CIMT).
Compared with nonregular cell phone users, regular users were younger, had higher proportions of current smokers and urban residents, and had lower proportions of history of hypertension and diabetes. They also had higher income, Townsend deprivation index, and body mass index, and lower education levels.
During a median follow-up of 12.3 years, 56,181 participants developed incident CVD. Compared with nonregular cell phone users, regular users had a significantly higher risk for incident CVD (hazard ratio, 1.04) and increased CIMT (odds ratio, 1.11).
Among regular cell phone users, the duration of cell phone use and hands-free device/speakerphone use during calls was not significantly associated with incident CVD. Yet a significant and positive dose-response relationship was seen between weekly cell phone usage time and the risk for CVD. The positive association was stronger in current vs noncurrent smokers and people with vs without diabetes.
To different extents, sleep patterns (5.11%), psychologic distress (11.5%), and neuroticism (2.25%) mediated the relationship between weekly cell phone usage time and the risk for incident CVD.
“Our study suggests that despite the advantages of mobile phone use, we should also pay attention to the potential harm of mobile phone use to cardiovascular health,” Dr. Qin said. “Future studies to assess the risk-benefit balance will help promote mobile phone use patterns that are conducive to cardiovascular health.”
Meanwhile, he added, “We encourage measures to reduce time spent on mobile phones to promote the primary prevention of CVD. On the other hand, improving sleep and mental health status may help reduce the higher risk of CVD associated with mobile phone use.”
There are several limitations to the study in addition to its observational nature, which cannot show cause and effect. The questionnaires on cell phone use were restricted to phone calls; other use patterns of cell phones (eg, messaging, watching videos, and browsing the web) were not considered. Although the researchers adjusted for many potential confounders, unmeasured confounding bias (eg, the type of cell phone used and other sources of RF-EMF) cannot be eliminated.
Weak Link?
In a comment, Nicholas Grubic, MSc, a PhD student in epidemiology at the University of Toronto, Ontario, Canada, and coauthor of a related editorial, said, “I found it interesting that there was a connection observed between mobile phone use and CVD. However, it is crucial to understand that this link appeared to be much weaker compared with other well-known cardiovascular risk factors, such as smoking, diabetes, and high blood pressure. For now, mobile phone use should not be a major concern for most people.”
Nevertheless, clinicians should encourage patients to practice healthy habits around their screen time, he advised. “This could include limiting mobile phone use before bedtime and taking regular breaks to engage in activities that promote heart health, such as exercising or spending time outdoors.
“For the time being, we probably won’t see mobile phone use included in standard assessments for cardiovascular risk or as a focal point of cardiovascular health promotion initiatives,” he added. Instead, clinicians should “focus on established risk factors that have a stronger impact on patients’ cardiovascular health.”
Nieca Goldberg, MD, a clinical associate professor of medicine at NYU Grossman School of Medicine in New York City and American Heart Association volunteer expert, had a similar message. “You don’t have to go back to using a landline,” she said. “Instead, patients should be more mindful of how much phone use is taking away from their physical activity, keeping them from sleeping, and causing them stress.” Clinicians should also remember to counsel smokers on smoking cessation.
“It would be important for future studies to look at time spent on the phone and the type of activities patients are doing on their phones, such as social media, calls, texts, movies, or streaming TV shows,” she said. “It would be important to see how phone use is leading to a sedentary lifestyle” and what that means for a larger, more diverse population.
The study was supported by the National Key R&D Program, the National Natural Science Foundation of China, and the Outstanding Youth Development Scheme of Nanfang Hospital, Southern Medical University. Dr. Qin, Dr. Grubic, and Dr. Goldberg reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We found that a poor sleep pattern, psychological distress, and neuroticism significantly mediated the positive association between weekly mobile phone usage time and the risk for incident CVD, with a mediating proportion of 5.11%, 11.50%, and 2.25%, respectively,” said principal investigator Xianhui Qin, MD, professor of nephrology at Southern Medical University, Guangzhou, China.
Poor sleep patterns and poor mental health could disrupt circadian rhythms and endocrine and metabolic functions, as well as increase inflammation, he explained.
In addition, chronic exposure to radiofrequency electromagnetic fields (RF-EMF) emitted from cell phones could lead to oxidative stress and an inflammatory response. Combined with smoking and diabetes, this exposure “may have a synergistic effect in increasing CVD risk,” Dr. Qin suggested.
The study was published online in the Canadian Journal of Cardiology.
Risk Underestimated?
The researchers aimed to examine the association of regular cell phone use with incident CVD and explore the mediating effects of sleep and mental health using linked hospital and mortality records.
Their analysis included 444,027 participants (mean age, 56 years; 44% men) without a history of CVD from the UK Biobank. A total of 378,161 participants were regular cell phone users.
Regular cell phone use was defined as at least one call per week. Weekly use was self-reported as the average time of calls per week during the previous 3 months.
The primary outcome was incident CVD. Secondary outcomes were each component of CVD (ie, coronary heart disease, stroke, atrial fibrillation, and heart failure) and increased carotid intima media thickness (CIMT).
Compared with nonregular cell phone users, regular users were younger, had higher proportions of current smokers and urban residents, and had lower proportions of history of hypertension and diabetes. They also had higher income, Townsend deprivation index, and body mass index, and lower education levels.
During a median follow-up of 12.3 years, 56,181 participants developed incident CVD. Compared with nonregular cell phone users, regular users had a significantly higher risk for incident CVD (hazard ratio, 1.04) and increased CIMT (odds ratio, 1.11).
Among regular cell phone users, the duration of cell phone use and hands-free device/speakerphone use during calls was not significantly associated with incident CVD. Yet a significant and positive dose-response relationship was seen between weekly cell phone usage time and the risk for CVD. The positive association was stronger in current vs noncurrent smokers and people with vs without diabetes.
To different extents, sleep patterns (5.11%), psychologic distress (11.5%), and neuroticism (2.25%) mediated the relationship between weekly cell phone usage time and the risk for incident CVD.
“Our study suggests that despite the advantages of mobile phone use, we should also pay attention to the potential harm of mobile phone use to cardiovascular health,” Dr. Qin said. “Future studies to assess the risk-benefit balance will help promote mobile phone use patterns that are conducive to cardiovascular health.”
Meanwhile, he added, “We encourage measures to reduce time spent on mobile phones to promote the primary prevention of CVD. On the other hand, improving sleep and mental health status may help reduce the higher risk of CVD associated with mobile phone use.”
There are several limitations to the study in addition to its observational nature, which cannot show cause and effect. The questionnaires on cell phone use were restricted to phone calls; other use patterns of cell phones (eg, messaging, watching videos, and browsing the web) were not considered. Although the researchers adjusted for many potential confounders, unmeasured confounding bias (eg, the type of cell phone used and other sources of RF-EMF) cannot be eliminated.
Weak Link?
In a comment, Nicholas Grubic, MSc, a PhD student in epidemiology at the University of Toronto, Ontario, Canada, and coauthor of a related editorial, said, “I found it interesting that there was a connection observed between mobile phone use and CVD. However, it is crucial to understand that this link appeared to be much weaker compared with other well-known cardiovascular risk factors, such as smoking, diabetes, and high blood pressure. For now, mobile phone use should not be a major concern for most people.”
Nevertheless, clinicians should encourage patients to practice healthy habits around their screen time, he advised. “This could include limiting mobile phone use before bedtime and taking regular breaks to engage in activities that promote heart health, such as exercising or spending time outdoors.
“For the time being, we probably won’t see mobile phone use included in standard assessments for cardiovascular risk or as a focal point of cardiovascular health promotion initiatives,” he added. Instead, clinicians should “focus on established risk factors that have a stronger impact on patients’ cardiovascular health.”
Nieca Goldberg, MD, a clinical associate professor of medicine at NYU Grossman School of Medicine in New York City and American Heart Association volunteer expert, had a similar message. “You don’t have to go back to using a landline,” she said. “Instead, patients should be more mindful of how much phone use is taking away from their physical activity, keeping them from sleeping, and causing them stress.” Clinicians should also remember to counsel smokers on smoking cessation.
“It would be important for future studies to look at time spent on the phone and the type of activities patients are doing on their phones, such as social media, calls, texts, movies, or streaming TV shows,” she said. “It would be important to see how phone use is leading to a sedentary lifestyle” and what that means for a larger, more diverse population.
The study was supported by the National Key R&D Program, the National Natural Science Foundation of China, and the Outstanding Youth Development Scheme of Nanfang Hospital, Southern Medical University. Dr. Qin, Dr. Grubic, and Dr. Goldberg reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE CANADIAN JOURNAL OF CARDIOLOGY
Skip Potassium After Cardiac Surgery
LONDON —
“The widespread practice of giving patients potassium after bypass heart surgery even though their blood levels are within the normal range can be abandoned,” said Benjamin O’Brien, MD, PhD, director of the Clinic for Cardioanesthesiology and Intensive Care Medicine at Charité Hospital in Berlin, Germany.
Results from the randomized TIGHT-K trial that assessed two levels of potassium supplementation were presented at the annual congress of the European Society of Cardiology.
In the tight-control group, supplementation was provided to maintain high-normal levels of potassium (> 4.5 mEq/L). In the relaxed-control group, supplementation was provided only when potassium levels fell below the low-normal threshold (< 3.6 mEq/L).
Trial Upending Popular Practice
The multinational trial involved 23 centers in Germany and the United Kingdom. All 1690 participants enrolled were scheduled to undergo a coronary artery bypass graft procedure, but Dr. O’Brien said he considers the results of TIGHT-K to be broadly applicable.
“There is no physiological basis to expect a different result in patients undergoing different types of cardiac surgery,” he said.
The primary endpoint was clinically and electrocardiography confirmed new-onset atrial fibrillation that occurred in the 5 days after the bypass procedure.
For the primary atrial fibrillation endpoint, event rates were similar in the tight-control and the relaxed-control groups (26.2% vs 27.8%); the 1.7% difference did not approach statistical significance (P = .44). The difference in dysrhythmias other than atrial fibrillation, although numerically lower in the tight-control group, was also not significant (19.1% vs 21.1%; P = .26).
There were no significant differences in several secondary endpoints, including length of hospital stay and in-patient mortality, but cost, a prespecified secondary endpoint, was approximately $120 lower per patient in the relaxed-control group than in the tight-control group (P < .001).
Lowering Cost Across Cardiac Surgeries
During the 5-day follow-up, median potassium levels were higher in the tight-control group. Levels in both groups fell gradually, but essentially in parallel, over the study period, so median potassium levels were always higher in the tight-control group than in the relaxed-control group. At the end of the observation period, mean potassium levels were 4.34 mEq/L in the tight-control group and 4.08 mEq/L in the relaxed-control group.
Prior to the development of atrial fibrillation, participants in the tight-control group received a medium of seven potassium administrations (range, 4-12), whereas those in the relaxed-control group received a medium of zero.
There were no significant differences in episodes in any subgroup evaluated, including those divided by age, sex, baseline left ventricular ejection fraction, and the absence or presence of beta blockers or loop diuretics. A per-protocol analysis also failed to show any advantage for tight potassium control.
Atrial fibrillation occurs in about one third of patients after bypass surgery, as it does after many types of cardiac surgery. Institutions often have strategies in place to reduce the risk after cardiac surgery, and potassium supplementation is one of the most common, despite the lack of supportive evidence, Dr. O’Brien said.
Narrow Window for Optimal Potassium Levels
The difference in potassium levels between the tight-control group and the relaxed-control group were modest in this study, said Subodh Verma, MD, a cardiac surgeon at St Michael’s Hospital and professor at the University of Toronto, Ontario, Canada.
However, this is unavoidable and central to the question being posed, Dr. O’Brien pointed out. Because of the risks for both hypokalemia and hyperkalemia, the window for safe supplementation is short. Current practice is to achieve high-normal levels to reduce atrial fibrillation, but TIGHT-K demonstrates this has no benefit.
The conclusion of TIGHT-K is appropriate, said Faiez Zannad, MD, PhD, professor of therapeutics in the Division of Cardiology at the University of Lorraine in Nancy, France, who praised the design and conduct of the study.
He acknowledged an unmet need for effective methods to reduce the risk for atrial fibrillation after cardiac surgery, but the ESC invited discussant said it is now necessary to look at other strategies. Several are under current evaluation, such as supplementary magnesium and the use of sodium-glucose transporter-2 inhibitors.
Although Dr. Zannad encouraged more studies of methods to reduce atrial fibrillation risk after cardiac surgery, he said that TIGHT-K has answered the question of whether potassium supplementation is beneficial.
Potassium supplementation should no longer be offered, he said, which will “reduce healthcare costs and decrease patient risk from an unnecessary intervention.”
A version of this article first appeared on Medscape.com.
LONDON —
“The widespread practice of giving patients potassium after bypass heart surgery even though their blood levels are within the normal range can be abandoned,” said Benjamin O’Brien, MD, PhD, director of the Clinic for Cardioanesthesiology and Intensive Care Medicine at Charité Hospital in Berlin, Germany.
Results from the randomized TIGHT-K trial that assessed two levels of potassium supplementation were presented at the annual congress of the European Society of Cardiology.
In the tight-control group, supplementation was provided to maintain high-normal levels of potassium (> 4.5 mEq/L). In the relaxed-control group, supplementation was provided only when potassium levels fell below the low-normal threshold (< 3.6 mEq/L).
Trial Upending Popular Practice
The multinational trial involved 23 centers in Germany and the United Kingdom. All 1690 participants enrolled were scheduled to undergo a coronary artery bypass graft procedure, but Dr. O’Brien said he considers the results of TIGHT-K to be broadly applicable.
“There is no physiological basis to expect a different result in patients undergoing different types of cardiac surgery,” he said.
The primary endpoint was clinically and electrocardiography confirmed new-onset atrial fibrillation that occurred in the 5 days after the bypass procedure.
For the primary atrial fibrillation endpoint, event rates were similar in the tight-control and the relaxed-control groups (26.2% vs 27.8%); the 1.7% difference did not approach statistical significance (P = .44). The difference in dysrhythmias other than atrial fibrillation, although numerically lower in the tight-control group, was also not significant (19.1% vs 21.1%; P = .26).
There were no significant differences in several secondary endpoints, including length of hospital stay and in-patient mortality, but cost, a prespecified secondary endpoint, was approximately $120 lower per patient in the relaxed-control group than in the tight-control group (P < .001).
Lowering Cost Across Cardiac Surgeries
During the 5-day follow-up, median potassium levels were higher in the tight-control group. Levels in both groups fell gradually, but essentially in parallel, over the study period, so median potassium levels were always higher in the tight-control group than in the relaxed-control group. At the end of the observation period, mean potassium levels were 4.34 mEq/L in the tight-control group and 4.08 mEq/L in the relaxed-control group.
Prior to the development of atrial fibrillation, participants in the tight-control group received a medium of seven potassium administrations (range, 4-12), whereas those in the relaxed-control group received a medium of zero.
There were no significant differences in episodes in any subgroup evaluated, including those divided by age, sex, baseline left ventricular ejection fraction, and the absence or presence of beta blockers or loop diuretics. A per-protocol analysis also failed to show any advantage for tight potassium control.
Atrial fibrillation occurs in about one third of patients after bypass surgery, as it does after many types of cardiac surgery. Institutions often have strategies in place to reduce the risk after cardiac surgery, and potassium supplementation is one of the most common, despite the lack of supportive evidence, Dr. O’Brien said.
Narrow Window for Optimal Potassium Levels
The difference in potassium levels between the tight-control group and the relaxed-control group were modest in this study, said Subodh Verma, MD, a cardiac surgeon at St Michael’s Hospital and professor at the University of Toronto, Ontario, Canada.
However, this is unavoidable and central to the question being posed, Dr. O’Brien pointed out. Because of the risks for both hypokalemia and hyperkalemia, the window for safe supplementation is short. Current practice is to achieve high-normal levels to reduce atrial fibrillation, but TIGHT-K demonstrates this has no benefit.
The conclusion of TIGHT-K is appropriate, said Faiez Zannad, MD, PhD, professor of therapeutics in the Division of Cardiology at the University of Lorraine in Nancy, France, who praised the design and conduct of the study.
He acknowledged an unmet need for effective methods to reduce the risk for atrial fibrillation after cardiac surgery, but the ESC invited discussant said it is now necessary to look at other strategies. Several are under current evaluation, such as supplementary magnesium and the use of sodium-glucose transporter-2 inhibitors.
Although Dr. Zannad encouraged more studies of methods to reduce atrial fibrillation risk after cardiac surgery, he said that TIGHT-K has answered the question of whether potassium supplementation is beneficial.
Potassium supplementation should no longer be offered, he said, which will “reduce healthcare costs and decrease patient risk from an unnecessary intervention.”
A version of this article first appeared on Medscape.com.
LONDON —
“The widespread practice of giving patients potassium after bypass heart surgery even though their blood levels are within the normal range can be abandoned,” said Benjamin O’Brien, MD, PhD, director of the Clinic for Cardioanesthesiology and Intensive Care Medicine at Charité Hospital in Berlin, Germany.
Results from the randomized TIGHT-K trial that assessed two levels of potassium supplementation were presented at the annual congress of the European Society of Cardiology.
In the tight-control group, supplementation was provided to maintain high-normal levels of potassium (> 4.5 mEq/L). In the relaxed-control group, supplementation was provided only when potassium levels fell below the low-normal threshold (< 3.6 mEq/L).
Trial Upending Popular Practice
The multinational trial involved 23 centers in Germany and the United Kingdom. All 1690 participants enrolled were scheduled to undergo a coronary artery bypass graft procedure, but Dr. O’Brien said he considers the results of TIGHT-K to be broadly applicable.
“There is no physiological basis to expect a different result in patients undergoing different types of cardiac surgery,” he said.
The primary endpoint was clinically and electrocardiography confirmed new-onset atrial fibrillation that occurred in the 5 days after the bypass procedure.
For the primary atrial fibrillation endpoint, event rates were similar in the tight-control and the relaxed-control groups (26.2% vs 27.8%); the 1.7% difference did not approach statistical significance (P = .44). The difference in dysrhythmias other than atrial fibrillation, although numerically lower in the tight-control group, was also not significant (19.1% vs 21.1%; P = .26).
There were no significant differences in several secondary endpoints, including length of hospital stay and in-patient mortality, but cost, a prespecified secondary endpoint, was approximately $120 lower per patient in the relaxed-control group than in the tight-control group (P < .001).
Lowering Cost Across Cardiac Surgeries
During the 5-day follow-up, median potassium levels were higher in the tight-control group. Levels in both groups fell gradually, but essentially in parallel, over the study period, so median potassium levels were always higher in the tight-control group than in the relaxed-control group. At the end of the observation period, mean potassium levels were 4.34 mEq/L in the tight-control group and 4.08 mEq/L in the relaxed-control group.
Prior to the development of atrial fibrillation, participants in the tight-control group received a medium of seven potassium administrations (range, 4-12), whereas those in the relaxed-control group received a medium of zero.
There were no significant differences in episodes in any subgroup evaluated, including those divided by age, sex, baseline left ventricular ejection fraction, and the absence or presence of beta blockers or loop diuretics. A per-protocol analysis also failed to show any advantage for tight potassium control.
Atrial fibrillation occurs in about one third of patients after bypass surgery, as it does after many types of cardiac surgery. Institutions often have strategies in place to reduce the risk after cardiac surgery, and potassium supplementation is one of the most common, despite the lack of supportive evidence, Dr. O’Brien said.
Narrow Window for Optimal Potassium Levels
The difference in potassium levels between the tight-control group and the relaxed-control group were modest in this study, said Subodh Verma, MD, a cardiac surgeon at St Michael’s Hospital and professor at the University of Toronto, Ontario, Canada.
However, this is unavoidable and central to the question being posed, Dr. O’Brien pointed out. Because of the risks for both hypokalemia and hyperkalemia, the window for safe supplementation is short. Current practice is to achieve high-normal levels to reduce atrial fibrillation, but TIGHT-K demonstrates this has no benefit.
The conclusion of TIGHT-K is appropriate, said Faiez Zannad, MD, PhD, professor of therapeutics in the Division of Cardiology at the University of Lorraine in Nancy, France, who praised the design and conduct of the study.
He acknowledged an unmet need for effective methods to reduce the risk for atrial fibrillation after cardiac surgery, but the ESC invited discussant said it is now necessary to look at other strategies. Several are under current evaluation, such as supplementary magnesium and the use of sodium-glucose transporter-2 inhibitors.
Although Dr. Zannad encouraged more studies of methods to reduce atrial fibrillation risk after cardiac surgery, he said that TIGHT-K has answered the question of whether potassium supplementation is beneficial.
Potassium supplementation should no longer be offered, he said, which will “reduce healthcare costs and decrease patient risk from an unnecessary intervention.”
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2024
FDA ‘Recalls’ Often Leave Targeted Medical Devices in Use
In 2016, medical device giant Abbott issued a recall for its MitraClip cardiac device — “a Class I recall, the most serious type,” the FDA said.
“Use of this device may cause serious injuries or death,” an FDA notice about the recall said.
But neither the manufacturer nor the FDA actually recalled the device or suspended its use. They allowed doctors to continue implanting the clips in leaky heart valves in what has become a common procedure.
In a notice, the manufacturer explained, “Abbott is not removing product from commercial distribution.” Rather, Abbott revised instructions for use and required doctors who implant the clips to undergo training.
“It’s very oxymoronic,” said Rita Redberg, a cardiologist at the University of California-San Francisco and former editor-in-chief of the journal JAMA Internal Medicine. “A recall makes it sound like it’s recalled. But that is not actually what it means.”
Though the FDA and federal regulations call these actions recalls, they might be described more aptly as “non-recalls.” And they have happened repeatedly in recent years. For instance, in addition to other Abbott devices, products made by Medtronic, Abiomed, and Getinge have had recalls that left them in use.
Safeguarding the Public
Recalls that leave what the FDA identifies as potentially dangerous products in the marketplace can raise the question: Do they do enough to protect the public?
There are other ways to handle recalls. In announcements about products as varied as crib bumpers, pool drain covers, bicycle helmets, and coffee mugs, the Consumer Product Safety Commission routinely alerts consumers to stop using recalled products and contact the manufacturers for refunds, repairs, or replacements. The National Highway Traffic Safety Administration regularly advises consumers to bring recalled cars back to the dealer to have them fixed. When the U.S. Department of Agriculture and the FDA announce food recalls, they routinely tell consumers to return or discard the food.
In some cases, a medical device that is the subject of a recall can be kept on the market safely because there is a simple fix, said Sanket Dhruva, a cardiologist and an associate professor at UCSF who has studied FDA oversight of devices. In other cases, recalls that don’t remove devices from the market can provide unwarranted reassurance and leave the public at risk, Dhruva said.
From 2019 through 2023, there were 338 Class I medical device recalls, 164 of which were corrections and 174 of which were removals, FDA spokesperson Amanda Hils said.
Some products undergo recall after recall while they remain on the market. Products in the MitraClip line have been the subject of three rounds of recalls, none of which removed devices from use.
“When deciding whether a recall warrants device removal from the field, the FDA considers the frequency and severity of adverse events, effectiveness of the corrective actions that have been executed, and the benefits and risks of preserving patient access to the device,” FDA spokesperson Audra Harrison said.
Where recalled devices have already been implanted, “removal” doesn’t necessarily mean removing them from patients’ bodies. “When an implanted device has the potential to fail unexpectedly, companies often tell doctors to contact their patients to discuss the risk of removing the device compared to the risk of leaving it in place,” the FDA website says.
The FDA allowed the recalled MitraClip devices to remain in use “because the agency believed that the overall benefits of the device continued to outweigh the risks and the firm’s recall strategy was appropriate and adequate,” Harrison said.
The FDA reviews the recall strategies that manufacturers propose and often provides input to ensure the public will be protected, Hils said. The agency also monitors the effectiveness of recalls and, before terminating them, makes sure the strategy was carried out, Hils said.
Abbott, the maker of MitraClip, said the device has been proven safe and effective “based on more than 20 years of clinical evidence and has profoundly improved the lives of people living with mitral regurgitation,” a condition in which blood flows backward through the heart’s mitral valve. The condition can lead to heart failure and death.
“With MitraClip, we’re addressing the needs of people with MR who often have no other options,” company spokesperson Brent Tippen said.
Speaking of the MitraClip recalls, Redberg said, “So hard to imagine these are effective actions in protecting patients.”
In 2021, for Medtronic’s StealthStation S7 cranial software, the company and the FDA sent a different message.
StealthStation is an elaborate system of screens and other equipment that guides neurosurgeons using instruments in the brain — for instance, to biopsy or cut out tumors. Drawing from CT scans, MRIs, and other imaging, it’s meant to show the location of the surgical instruments.
In connection with a Class I November 2021 recall, the FDA website said potential inaccuracies in a biopsy depth gauge could result in “life-threatening injury (such as hemorrhage, unintended tissue damage, or permanent neurological injury), which could lead to death.”
The FDA website explained what Medtronic was doing about it.
“The recalling firm will provide a warning and instructional placard to be applied to impacted systems,” the website said. “Until a software update is available, ensure you are following the instructions below to prevent the issue from occurring,” it advised doctors.
In a statement to KFF Health News, Medtronic spokesperson Erika Winkels said the safety and well-being of patients is the company’s primary concern, and certain issues “can be safely and effectively remedied with a correction on site.”
Richard Everson, a neurosurgeon and an assistant professor at UCLA, noted that the 2021 recall allowed doctors to continue using unaffected StealthStation features, a benefit for patients and facilities depending on them.
“But, I mean, then you could ask, ‘Well, why don’t they just disable the view [of the brain] that’s bugged?’” Everson said. “Why would they give you the option of looking at an inaccurate one?”
“That’s kind of a strange solution,” he said.
The FDA lists the 2021 recall as still open, explaining “not all products have been corrected or removed.”
That recall was not the last word on problems with StealthStation. Since then, the manufacturer has submitted adverse event reports to the FDA describing trouble in cases involving various versions of StealthStation.
In a September 2022 case, guidance provided by a StealthStation device was allegedly off the mark, a procedure was aborted, and, when the patient awoke, they “had almost no speech for two days,” according to a Medtronic report. In the report, Medtronic said there was “insufficient information to determine the relationship of the software to the reported issue.”
In a February 2024 case, after brain surgery, an MRI found that the operation “missed the tumor” and that other tissue was removed instead, according to a report Medtronic submitted to the FDA. In the report, Medtronic said that when a company representative tested the system, it performed as intended.
In March 2024, Medtronic recalled versions of StealthStation S8 without removing them from hospitals. The company said at the time that it would provide a software update.
“Software updates are available to correct the anomalies identified in the 2021 S7 and 2024 S8 recalls and are actively being deployed,” Medtronic’s Winkels told KFF Health News in a July email. “While the software updates for the 2021 S7 recall are complete in the US, they remain ongoing in some international regions.”
In June 2023, Abiomed issued an urgent medical device correction for its Impella 2.5 intravascular micro axial blood pump, which supports the heart. In patients with a certain type of replacement heart valve, there was a risk of “destruction of the impeller blades,” which could cause “low flow” and “embolization of the fractured impeller material,” an entry on the FDA website said.
“Clinicians are cautioned to position the Impella system carefully in patients,” the FDA website said, among other instructions.
The updated instructions “provide technical guidance to mitigate the risk of rare complications,” Abiomed spokesperson Ryan Carbain said. There were no product removals and no reports of adverse events “related to product design or manufacturing,” Carbain said.
Another set of medical devices, Cardiosave Hybrid and Rescue Intra-Aortic Balloon Pumps made by Getinge of Sweden, have failed persistently, according to FDA records.
The devices — which are placed in the aorta, a major artery, to assist the heart — were the subject of eight Class I recalls from December 2022 to July 2023. All were corrections rather than removals, a KFF Health News analysis found.
In a May 2024 letter to health care providers, the FDA said that, in the previous 12 months, it had received almost 3,000 adverse event reports related to the balloon pumps. It was referring to reports of malfunctions and cases in which the products might have caused or contributed to a death or injury. Of those, 15 reportedly involved serious injury or death, the FDA said.
During the summer of 2023, the FDA noted that “alternative treatments are limited” and said the devices could continue to be used.
But, in May, the FDA changed its stance. The agency advised health care facilities to “transition away from these devices and seek alternatives, if possible.”
“These recommendations are based on our continued concerns” that the manufacturer “has not sufficiently addressed the problems and risks with these recalled devices.”
Getinge sent KFF Health News written answers from Elin Frostehav, the company’s president of Acute Care Therapies.
“There is no question that we would have liked to have solved these issues in full much earlier,” she said.
As a result of the FDA’s May action, the company “immediately paused proactive marketing” of the balloon pumps in the United States, and it is selling them only to customers who have no alternatives, Frostehav said.
“We are working with the agency to finalize remediation and product update solutions,” Frostehav said.
‘Known Possible Complications’
Abbott’s MitraClip system includes tiny clips implanted in the heart’s mitral valve and the equipment used to implant them. The apparatus features a steering mechanism with hand controls and a catheter that is threaded through a major vein, typically from an incision in the groin, to place one or more clips in the heart.
Worldwide, more than 200,000 people have been treated with MitraClip, according to an Abbott website.
The 2016 MitraClip recall described cases in which “the user was unable to separate the implantable Clip from the delivery system.”
In a news release at the time, Abbott said it had “received a small number of reports” in which that happened.
Those cases “resulted in surgical interventions to remove the delivery system or replace the mitral valve, and it is expected that any future similar incidents would also require surgery to correct the problem,” the FDA said in a 2016 notice. “There was one patient death in these cases as a result of severe comorbidities following surgery.”
Years later, something similar happened.
In February 2021, a clip was implanted in an 81-year-old patient but the doctor couldn’t separate the clip from the delivery system, according to a report Abbott filed with the FDA. The patient was transferred to surgery, where the delivery system “had to be cut down in order to detach the clip.”
The patient then underwent an operation to replace the mitral valve, and, hours later, the patient was brought back to surgery to address bleeding, the report said.
The patient “coded” the next day and died from an aortic bleed, the report said.
In the report to the FDA, the manufacturer blamed “case-specific circumstances.”
“Cardiac arrest, hemorrhage and death are listed” in the device instructions “as known possible complications associated with mitraclip procedures,” the company said. “There is no indication of a product issue with respect to manufacture, design or labeling.”
The third MitraClip recall, initiated in September 2022, cited an “increase in clip locking malfunctions.”
Most of the reported malfunctions were not associated with adverse outcomes, the FDA said then. Treatment with MitraClip “remains within the anticipated risk levels,” the company told customers.
As with the two earlier recalls, the third advised doctors to follow the device’s instructions. But the 2022 recall identified a contributing factor: the way the device was made.
“Abbott has identified a contributing cause … as a change in the material properties of one of the Clip locking components,” the company said in a 2022 letter to customers.
“Abbott is working on producing new lots with updated manufacturing processing and raw material,” the company wrote. In the same letter, Abbott told doctors that, in the meantime, they could use the devices they had in stock.
Six days later, a clip opened while locked and a patient died, according to a report the manufacturer submitted to the FDA.
“There is no evidence that death was related to the device but it was likely related to the procedure,” Abbott wrote.
Now, almost two years later, the 2022 recall remains open, according to the FDA website, and “not all products have been corrected or removed.”
KFF Health News data editor Holly K. Hacker contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
In 2016, medical device giant Abbott issued a recall for its MitraClip cardiac device — “a Class I recall, the most serious type,” the FDA said.
“Use of this device may cause serious injuries or death,” an FDA notice about the recall said.
But neither the manufacturer nor the FDA actually recalled the device or suspended its use. They allowed doctors to continue implanting the clips in leaky heart valves in what has become a common procedure.
In a notice, the manufacturer explained, “Abbott is not removing product from commercial distribution.” Rather, Abbott revised instructions for use and required doctors who implant the clips to undergo training.
“It’s very oxymoronic,” said Rita Redberg, a cardiologist at the University of California-San Francisco and former editor-in-chief of the journal JAMA Internal Medicine. “A recall makes it sound like it’s recalled. But that is not actually what it means.”
Though the FDA and federal regulations call these actions recalls, they might be described more aptly as “non-recalls.” And they have happened repeatedly in recent years. For instance, in addition to other Abbott devices, products made by Medtronic, Abiomed, and Getinge have had recalls that left them in use.
Safeguarding the Public
Recalls that leave what the FDA identifies as potentially dangerous products in the marketplace can raise the question: Do they do enough to protect the public?
There are other ways to handle recalls. In announcements about products as varied as crib bumpers, pool drain covers, bicycle helmets, and coffee mugs, the Consumer Product Safety Commission routinely alerts consumers to stop using recalled products and contact the manufacturers for refunds, repairs, or replacements. The National Highway Traffic Safety Administration regularly advises consumers to bring recalled cars back to the dealer to have them fixed. When the U.S. Department of Agriculture and the FDA announce food recalls, they routinely tell consumers to return or discard the food.
In some cases, a medical device that is the subject of a recall can be kept on the market safely because there is a simple fix, said Sanket Dhruva, a cardiologist and an associate professor at UCSF who has studied FDA oversight of devices. In other cases, recalls that don’t remove devices from the market can provide unwarranted reassurance and leave the public at risk, Dhruva said.
From 2019 through 2023, there were 338 Class I medical device recalls, 164 of which were corrections and 174 of which were removals, FDA spokesperson Amanda Hils said.
Some products undergo recall after recall while they remain on the market. Products in the MitraClip line have been the subject of three rounds of recalls, none of which removed devices from use.
“When deciding whether a recall warrants device removal from the field, the FDA considers the frequency and severity of adverse events, effectiveness of the corrective actions that have been executed, and the benefits and risks of preserving patient access to the device,” FDA spokesperson Audra Harrison said.
Where recalled devices have already been implanted, “removal” doesn’t necessarily mean removing them from patients’ bodies. “When an implanted device has the potential to fail unexpectedly, companies often tell doctors to contact their patients to discuss the risk of removing the device compared to the risk of leaving it in place,” the FDA website says.
The FDA allowed the recalled MitraClip devices to remain in use “because the agency believed that the overall benefits of the device continued to outweigh the risks and the firm’s recall strategy was appropriate and adequate,” Harrison said.
The FDA reviews the recall strategies that manufacturers propose and often provides input to ensure the public will be protected, Hils said. The agency also monitors the effectiveness of recalls and, before terminating them, makes sure the strategy was carried out, Hils said.
Abbott, the maker of MitraClip, said the device has been proven safe and effective “based on more than 20 years of clinical evidence and has profoundly improved the lives of people living with mitral regurgitation,” a condition in which blood flows backward through the heart’s mitral valve. The condition can lead to heart failure and death.
“With MitraClip, we’re addressing the needs of people with MR who often have no other options,” company spokesperson Brent Tippen said.
Speaking of the MitraClip recalls, Redberg said, “So hard to imagine these are effective actions in protecting patients.”
In 2021, for Medtronic’s StealthStation S7 cranial software, the company and the FDA sent a different message.
StealthStation is an elaborate system of screens and other equipment that guides neurosurgeons using instruments in the brain — for instance, to biopsy or cut out tumors. Drawing from CT scans, MRIs, and other imaging, it’s meant to show the location of the surgical instruments.
In connection with a Class I November 2021 recall, the FDA website said potential inaccuracies in a biopsy depth gauge could result in “life-threatening injury (such as hemorrhage, unintended tissue damage, or permanent neurological injury), which could lead to death.”
The FDA website explained what Medtronic was doing about it.
“The recalling firm will provide a warning and instructional placard to be applied to impacted systems,” the website said. “Until a software update is available, ensure you are following the instructions below to prevent the issue from occurring,” it advised doctors.
In a statement to KFF Health News, Medtronic spokesperson Erika Winkels said the safety and well-being of patients is the company’s primary concern, and certain issues “can be safely and effectively remedied with a correction on site.”
Richard Everson, a neurosurgeon and an assistant professor at UCLA, noted that the 2021 recall allowed doctors to continue using unaffected StealthStation features, a benefit for patients and facilities depending on them.
“But, I mean, then you could ask, ‘Well, why don’t they just disable the view [of the brain] that’s bugged?’” Everson said. “Why would they give you the option of looking at an inaccurate one?”
“That’s kind of a strange solution,” he said.
The FDA lists the 2021 recall as still open, explaining “not all products have been corrected or removed.”
That recall was not the last word on problems with StealthStation. Since then, the manufacturer has submitted adverse event reports to the FDA describing trouble in cases involving various versions of StealthStation.
In a September 2022 case, guidance provided by a StealthStation device was allegedly off the mark, a procedure was aborted, and, when the patient awoke, they “had almost no speech for two days,” according to a Medtronic report. In the report, Medtronic said there was “insufficient information to determine the relationship of the software to the reported issue.”
In a February 2024 case, after brain surgery, an MRI found that the operation “missed the tumor” and that other tissue was removed instead, according to a report Medtronic submitted to the FDA. In the report, Medtronic said that when a company representative tested the system, it performed as intended.
In March 2024, Medtronic recalled versions of StealthStation S8 without removing them from hospitals. The company said at the time that it would provide a software update.
“Software updates are available to correct the anomalies identified in the 2021 S7 and 2024 S8 recalls and are actively being deployed,” Medtronic’s Winkels told KFF Health News in a July email. “While the software updates for the 2021 S7 recall are complete in the US, they remain ongoing in some international regions.”
In June 2023, Abiomed issued an urgent medical device correction for its Impella 2.5 intravascular micro axial blood pump, which supports the heart. In patients with a certain type of replacement heart valve, there was a risk of “destruction of the impeller blades,” which could cause “low flow” and “embolization of the fractured impeller material,” an entry on the FDA website said.
“Clinicians are cautioned to position the Impella system carefully in patients,” the FDA website said, among other instructions.
The updated instructions “provide technical guidance to mitigate the risk of rare complications,” Abiomed spokesperson Ryan Carbain said. There were no product removals and no reports of adverse events “related to product design or manufacturing,” Carbain said.
Another set of medical devices, Cardiosave Hybrid and Rescue Intra-Aortic Balloon Pumps made by Getinge of Sweden, have failed persistently, according to FDA records.
The devices — which are placed in the aorta, a major artery, to assist the heart — were the subject of eight Class I recalls from December 2022 to July 2023. All were corrections rather than removals, a KFF Health News analysis found.
In a May 2024 letter to health care providers, the FDA said that, in the previous 12 months, it had received almost 3,000 adverse event reports related to the balloon pumps. It was referring to reports of malfunctions and cases in which the products might have caused or contributed to a death or injury. Of those, 15 reportedly involved serious injury or death, the FDA said.
During the summer of 2023, the FDA noted that “alternative treatments are limited” and said the devices could continue to be used.
But, in May, the FDA changed its stance. The agency advised health care facilities to “transition away from these devices and seek alternatives, if possible.”
“These recommendations are based on our continued concerns” that the manufacturer “has not sufficiently addressed the problems and risks with these recalled devices.”
Getinge sent KFF Health News written answers from Elin Frostehav, the company’s president of Acute Care Therapies.
“There is no question that we would have liked to have solved these issues in full much earlier,” she said.
As a result of the FDA’s May action, the company “immediately paused proactive marketing” of the balloon pumps in the United States, and it is selling them only to customers who have no alternatives, Frostehav said.
“We are working with the agency to finalize remediation and product update solutions,” Frostehav said.
‘Known Possible Complications’
Abbott’s MitraClip system includes tiny clips implanted in the heart’s mitral valve and the equipment used to implant them. The apparatus features a steering mechanism with hand controls and a catheter that is threaded through a major vein, typically from an incision in the groin, to place one or more clips in the heart.
Worldwide, more than 200,000 people have been treated with MitraClip, according to an Abbott website.
The 2016 MitraClip recall described cases in which “the user was unable to separate the implantable Clip from the delivery system.”
In a news release at the time, Abbott said it had “received a small number of reports” in which that happened.
Those cases “resulted in surgical interventions to remove the delivery system or replace the mitral valve, and it is expected that any future similar incidents would also require surgery to correct the problem,” the FDA said in a 2016 notice. “There was one patient death in these cases as a result of severe comorbidities following surgery.”
Years later, something similar happened.
In February 2021, a clip was implanted in an 81-year-old patient but the doctor couldn’t separate the clip from the delivery system, according to a report Abbott filed with the FDA. The patient was transferred to surgery, where the delivery system “had to be cut down in order to detach the clip.”
The patient then underwent an operation to replace the mitral valve, and, hours later, the patient was brought back to surgery to address bleeding, the report said.
The patient “coded” the next day and died from an aortic bleed, the report said.
In the report to the FDA, the manufacturer blamed “case-specific circumstances.”
“Cardiac arrest, hemorrhage and death are listed” in the device instructions “as known possible complications associated with mitraclip procedures,” the company said. “There is no indication of a product issue with respect to manufacture, design or labeling.”
The third MitraClip recall, initiated in September 2022, cited an “increase in clip locking malfunctions.”
Most of the reported malfunctions were not associated with adverse outcomes, the FDA said then. Treatment with MitraClip “remains within the anticipated risk levels,” the company told customers.
As with the two earlier recalls, the third advised doctors to follow the device’s instructions. But the 2022 recall identified a contributing factor: the way the device was made.
“Abbott has identified a contributing cause … as a change in the material properties of one of the Clip locking components,” the company said in a 2022 letter to customers.
“Abbott is working on producing new lots with updated manufacturing processing and raw material,” the company wrote. In the same letter, Abbott told doctors that, in the meantime, they could use the devices they had in stock.
Six days later, a clip opened while locked and a patient died, according to a report the manufacturer submitted to the FDA.
“There is no evidence that death was related to the device but it was likely related to the procedure,” Abbott wrote.
Now, almost two years later, the 2022 recall remains open, according to the FDA website, and “not all products have been corrected or removed.”
KFF Health News data editor Holly K. Hacker contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
In 2016, medical device giant Abbott issued a recall for its MitraClip cardiac device — “a Class I recall, the most serious type,” the FDA said.
“Use of this device may cause serious injuries or death,” an FDA notice about the recall said.
But neither the manufacturer nor the FDA actually recalled the device or suspended its use. They allowed doctors to continue implanting the clips in leaky heart valves in what has become a common procedure.
In a notice, the manufacturer explained, “Abbott is not removing product from commercial distribution.” Rather, Abbott revised instructions for use and required doctors who implant the clips to undergo training.
“It’s very oxymoronic,” said Rita Redberg, a cardiologist at the University of California-San Francisco and former editor-in-chief of the journal JAMA Internal Medicine. “A recall makes it sound like it’s recalled. But that is not actually what it means.”
Though the FDA and federal regulations call these actions recalls, they might be described more aptly as “non-recalls.” And they have happened repeatedly in recent years. For instance, in addition to other Abbott devices, products made by Medtronic, Abiomed, and Getinge have had recalls that left them in use.
Safeguarding the Public
Recalls that leave what the FDA identifies as potentially dangerous products in the marketplace can raise the question: Do they do enough to protect the public?
There are other ways to handle recalls. In announcements about products as varied as crib bumpers, pool drain covers, bicycle helmets, and coffee mugs, the Consumer Product Safety Commission routinely alerts consumers to stop using recalled products and contact the manufacturers for refunds, repairs, or replacements. The National Highway Traffic Safety Administration regularly advises consumers to bring recalled cars back to the dealer to have them fixed. When the U.S. Department of Agriculture and the FDA announce food recalls, they routinely tell consumers to return or discard the food.
In some cases, a medical device that is the subject of a recall can be kept on the market safely because there is a simple fix, said Sanket Dhruva, a cardiologist and an associate professor at UCSF who has studied FDA oversight of devices. In other cases, recalls that don’t remove devices from the market can provide unwarranted reassurance and leave the public at risk, Dhruva said.
From 2019 through 2023, there were 338 Class I medical device recalls, 164 of which were corrections and 174 of which were removals, FDA spokesperson Amanda Hils said.
Some products undergo recall after recall while they remain on the market. Products in the MitraClip line have been the subject of three rounds of recalls, none of which removed devices from use.
“When deciding whether a recall warrants device removal from the field, the FDA considers the frequency and severity of adverse events, effectiveness of the corrective actions that have been executed, and the benefits and risks of preserving patient access to the device,” FDA spokesperson Audra Harrison said.
Where recalled devices have already been implanted, “removal” doesn’t necessarily mean removing them from patients’ bodies. “When an implanted device has the potential to fail unexpectedly, companies often tell doctors to contact their patients to discuss the risk of removing the device compared to the risk of leaving it in place,” the FDA website says.
The FDA allowed the recalled MitraClip devices to remain in use “because the agency believed that the overall benefits of the device continued to outweigh the risks and the firm’s recall strategy was appropriate and adequate,” Harrison said.
The FDA reviews the recall strategies that manufacturers propose and often provides input to ensure the public will be protected, Hils said. The agency also monitors the effectiveness of recalls and, before terminating them, makes sure the strategy was carried out, Hils said.
Abbott, the maker of MitraClip, said the device has been proven safe and effective “based on more than 20 years of clinical evidence and has profoundly improved the lives of people living with mitral regurgitation,” a condition in which blood flows backward through the heart’s mitral valve. The condition can lead to heart failure and death.
“With MitraClip, we’re addressing the needs of people with MR who often have no other options,” company spokesperson Brent Tippen said.
Speaking of the MitraClip recalls, Redberg said, “So hard to imagine these are effective actions in protecting patients.”
In 2021, for Medtronic’s StealthStation S7 cranial software, the company and the FDA sent a different message.
StealthStation is an elaborate system of screens and other equipment that guides neurosurgeons using instruments in the brain — for instance, to biopsy or cut out tumors. Drawing from CT scans, MRIs, and other imaging, it’s meant to show the location of the surgical instruments.
In connection with a Class I November 2021 recall, the FDA website said potential inaccuracies in a biopsy depth gauge could result in “life-threatening injury (such as hemorrhage, unintended tissue damage, or permanent neurological injury), which could lead to death.”
The FDA website explained what Medtronic was doing about it.
“The recalling firm will provide a warning and instructional placard to be applied to impacted systems,” the website said. “Until a software update is available, ensure you are following the instructions below to prevent the issue from occurring,” it advised doctors.
In a statement to KFF Health News, Medtronic spokesperson Erika Winkels said the safety and well-being of patients is the company’s primary concern, and certain issues “can be safely and effectively remedied with a correction on site.”
Richard Everson, a neurosurgeon and an assistant professor at UCLA, noted that the 2021 recall allowed doctors to continue using unaffected StealthStation features, a benefit for patients and facilities depending on them.
“But, I mean, then you could ask, ‘Well, why don’t they just disable the view [of the brain] that’s bugged?’” Everson said. “Why would they give you the option of looking at an inaccurate one?”
“That’s kind of a strange solution,” he said.
The FDA lists the 2021 recall as still open, explaining “not all products have been corrected or removed.”
That recall was not the last word on problems with StealthStation. Since then, the manufacturer has submitted adverse event reports to the FDA describing trouble in cases involving various versions of StealthStation.
In a September 2022 case, guidance provided by a StealthStation device was allegedly off the mark, a procedure was aborted, and, when the patient awoke, they “had almost no speech for two days,” according to a Medtronic report. In the report, Medtronic said there was “insufficient information to determine the relationship of the software to the reported issue.”
In a February 2024 case, after brain surgery, an MRI found that the operation “missed the tumor” and that other tissue was removed instead, according to a report Medtronic submitted to the FDA. In the report, Medtronic said that when a company representative tested the system, it performed as intended.
In March 2024, Medtronic recalled versions of StealthStation S8 without removing them from hospitals. The company said at the time that it would provide a software update.
“Software updates are available to correct the anomalies identified in the 2021 S7 and 2024 S8 recalls and are actively being deployed,” Medtronic’s Winkels told KFF Health News in a July email. “While the software updates for the 2021 S7 recall are complete in the US, they remain ongoing in some international regions.”
In June 2023, Abiomed issued an urgent medical device correction for its Impella 2.5 intravascular micro axial blood pump, which supports the heart. In patients with a certain type of replacement heart valve, there was a risk of “destruction of the impeller blades,” which could cause “low flow” and “embolization of the fractured impeller material,” an entry on the FDA website said.
“Clinicians are cautioned to position the Impella system carefully in patients,” the FDA website said, among other instructions.
The updated instructions “provide technical guidance to mitigate the risk of rare complications,” Abiomed spokesperson Ryan Carbain said. There were no product removals and no reports of adverse events “related to product design or manufacturing,” Carbain said.
Another set of medical devices, Cardiosave Hybrid and Rescue Intra-Aortic Balloon Pumps made by Getinge of Sweden, have failed persistently, according to FDA records.
The devices — which are placed in the aorta, a major artery, to assist the heart — were the subject of eight Class I recalls from December 2022 to July 2023. All were corrections rather than removals, a KFF Health News analysis found.
In a May 2024 letter to health care providers, the FDA said that, in the previous 12 months, it had received almost 3,000 adverse event reports related to the balloon pumps. It was referring to reports of malfunctions and cases in which the products might have caused or contributed to a death or injury. Of those, 15 reportedly involved serious injury or death, the FDA said.
During the summer of 2023, the FDA noted that “alternative treatments are limited” and said the devices could continue to be used.
But, in May, the FDA changed its stance. The agency advised health care facilities to “transition away from these devices and seek alternatives, if possible.”
“These recommendations are based on our continued concerns” that the manufacturer “has not sufficiently addressed the problems and risks with these recalled devices.”
Getinge sent KFF Health News written answers from Elin Frostehav, the company’s president of Acute Care Therapies.
“There is no question that we would have liked to have solved these issues in full much earlier,” she said.
As a result of the FDA’s May action, the company “immediately paused proactive marketing” of the balloon pumps in the United States, and it is selling them only to customers who have no alternatives, Frostehav said.
“We are working with the agency to finalize remediation and product update solutions,” Frostehav said.
‘Known Possible Complications’
Abbott’s MitraClip system includes tiny clips implanted in the heart’s mitral valve and the equipment used to implant them. The apparatus features a steering mechanism with hand controls and a catheter that is threaded through a major vein, typically from an incision in the groin, to place one or more clips in the heart.
Worldwide, more than 200,000 people have been treated with MitraClip, according to an Abbott website.
The 2016 MitraClip recall described cases in which “the user was unable to separate the implantable Clip from the delivery system.”
In a news release at the time, Abbott said it had “received a small number of reports” in which that happened.
Those cases “resulted in surgical interventions to remove the delivery system or replace the mitral valve, and it is expected that any future similar incidents would also require surgery to correct the problem,” the FDA said in a 2016 notice. “There was one patient death in these cases as a result of severe comorbidities following surgery.”
Years later, something similar happened.
In February 2021, a clip was implanted in an 81-year-old patient but the doctor couldn’t separate the clip from the delivery system, according to a report Abbott filed with the FDA. The patient was transferred to surgery, where the delivery system “had to be cut down in order to detach the clip.”
The patient then underwent an operation to replace the mitral valve, and, hours later, the patient was brought back to surgery to address bleeding, the report said.
The patient “coded” the next day and died from an aortic bleed, the report said.
In the report to the FDA, the manufacturer blamed “case-specific circumstances.”
“Cardiac arrest, hemorrhage and death are listed” in the device instructions “as known possible complications associated with mitraclip procedures,” the company said. “There is no indication of a product issue with respect to manufacture, design or labeling.”
The third MitraClip recall, initiated in September 2022, cited an “increase in clip locking malfunctions.”
Most of the reported malfunctions were not associated with adverse outcomes, the FDA said then. Treatment with MitraClip “remains within the anticipated risk levels,” the company told customers.
As with the two earlier recalls, the third advised doctors to follow the device’s instructions. But the 2022 recall identified a contributing factor: the way the device was made.
“Abbott has identified a contributing cause … as a change in the material properties of one of the Clip locking components,” the company said in a 2022 letter to customers.
“Abbott is working on producing new lots with updated manufacturing processing and raw material,” the company wrote. In the same letter, Abbott told doctors that, in the meantime, they could use the devices they had in stock.
Six days later, a clip opened while locked and a patient died, according to a report the manufacturer submitted to the FDA.
“There is no evidence that death was related to the device but it was likely related to the procedure,” Abbott wrote.
Now, almost two years later, the 2022 recall remains open, according to the FDA website, and “not all products have been corrected or removed.”
KFF Health News data editor Holly K. Hacker contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — the independent source for health policy research, polling, and journalism.
Less Invasive, Overlooked Option in Cardiac Surgery May Offer Benefit
Compared with traditional replacement valves, sutureless valves placed through minimally invasive cardiac surgery have less data supporting their use but offer unique features that might make them the preferred option for certain patients, reported specialists.
The sutureless device known as Perceval (Corcym) and a rapidly deployed device called Intuity (Edwards Lifesciences) are used as an alternative to surgical aortic valve replacement (SAVR) and transcatheter aortic valve replacement (TAVR). But despite being commercially available since 2016, the devices are still not being used much.
The devices are not discussed in substantial detail in either the joint guidelines from the American College of Cardiology and American Heart Association issued in 2020 or guidelines from the European Society of Cardiology issued in 2022.
Cristiano Spadaccio, MD, PhD, a cardiothoracic surgeon associated with Lancashire Cardiac Centre in Blackpool, England, and his colleagues reviewed the small number of studies evaluating the alternate approach to “make the cardiology world aware” of alternatives “that can relieve the surgical burden by minimizing the implantation time and length of the operation,” he said.
The comprehensive review is published in the Journal of the American College of Cardiology.
A Neglected Alternative
The sutureless Perceval device is held in place by a stent frame that self-expands. The Intuity device also relies primarily on its framework to anchor the valve in place but does involve three sutures. Both devices are still referred to as sutureless in the new review of them.
Only a small number of centers perform minimally invasive cardiac surgeries, and the main advantage of the devices — rapid deployment — has been eroded with the advent of automated knotting which has significantly reduced the time to implant and sutured valve.
The underuse of these devices is largely caused by the limited amount of comparative and prospective data, said Dr. Spadaccio. “The entire literature on sutureless aortic valve replacement with the exception of one randomized controlled trial is observational.”
That trial, PERSIST-AVR, found that the sutureless valves were just as good as conventional ones when it comes to major adverse cardiovascular events including all-cause death, myocardial infarction, stroke, or valve reintervention at 1 year.
In a subanalysis limited to patients who had isolated aortic valve replacement, the sutureless procedure was associated with lower adverse events (5.2% vs 10.8%) at the cost of a higher rate of pacemaker implantation (11% vs 1.6%).
There are also multiple retrospective studies and registries that have generated observational data comparing sutureless aortic valve replacement with SAVR and TAVR in various patient populations, said Dr. Spadaccio, and the review was based on more than a dozen studies published since 2015. Long-term follow-up data for sutureless aortic valve replacements, which now exceeds 10 years, suggest rates of structural valve deterioration and reintervention have been acceptably low.
The minimally invasive procedures have other advantages too. For example, relative to the greater trauma associated with open heart surgery, minimally invasive surgeries typically involve faster recovery, an advantage likely to appeal to many patients who are candidates for either.
Quicker Recovery
Collectively, these data suggest that sutureless aortic valve replacement might be a reasonable or even a more appropriate alternative to either SAVR or TAVR when considering specific patient characteristics and goals, according to the review, which included an algorithm identifying specifically where sutureless aortic valve replacement fits with SAVR and TAVR.
“The algorithm is based on different clinical scenarios and reflects current guidelines for SAVR,” said Dr. Spadaccio. For example, current guidelines identify SAVR as preferred in patients younger than 65 years and in older patients with a low Society of Thoracic Surgeons (STS) score, but there are many instances in which sutureless aortic valve replacement might be more attractive, such as in those also undergoing mitral valve repair, coronary artery bypass grafting, or another surgical procedure.
Dr. Spadaccio said that the STS score should not be considered in isolation when evaluating a patient for SAVR or TAVR. Other features such as mobility, frailty score, and comorbid liver or renal disease should also be considered when discussing the three options with patients. As a result, the algorithm emphasizes a detailed evaluation of patient characteristics in selecting one procedure over another.
“The treatment should be really tailored on the individual patient basis,” said Dr. Spadaccio.
Dr. Spadaccio acknowledged that there is a need for more comparative trials, particularly in regard to sutureless aortic valve replacement as an alternative to TAVR. “I really think that a 1:1 RCT on sutureless aortic valve replacement vs TAVR could give better answers to all of these interrogatives.”
But despite the limitations outlined in this review, Dr. Spadaccio and colleagues challenged the perception that current data are not sufficient to allow clinicians to consider sutureless aortic valve replacement in the mix of options.
A Viable Option
This comprehensive summary of what is known about sutureless aortic valve replacement compared with the other options addresses an important knowledge gap, said S. Chris Malaisrie, MD, a cardiac surgeon at Northwestern University Feinberg School of Medicine, Chicago, Illinois.
He said he agrees this option has unique qualities. “Minimally invasive surgery has been largely ignored by guideline writers, but patients certainly demand options that are less invasive than standard open heart surgery. Sutureless and rapid deployment valves facilitate minimally invasive surgery and offer an advantageous option for younger patients.”
Dr. Malaisrie said the review is generating discussion about a potentially valuable option within the cardiology community. And that is exactly what Dr. Spadaccio was hoping for. “This paper was meant to educate as much as possible on these details to assist and inform decision-making,” he said.
A version of this article first appeared on Medscape.com.
Compared with traditional replacement valves, sutureless valves placed through minimally invasive cardiac surgery have less data supporting their use but offer unique features that might make them the preferred option for certain patients, reported specialists.
The sutureless device known as Perceval (Corcym) and a rapidly deployed device called Intuity (Edwards Lifesciences) are used as an alternative to surgical aortic valve replacement (SAVR) and transcatheter aortic valve replacement (TAVR). But despite being commercially available since 2016, the devices are still not being used much.
The devices are not discussed in substantial detail in either the joint guidelines from the American College of Cardiology and American Heart Association issued in 2020 or guidelines from the European Society of Cardiology issued in 2022.
Cristiano Spadaccio, MD, PhD, a cardiothoracic surgeon associated with Lancashire Cardiac Centre in Blackpool, England, and his colleagues reviewed the small number of studies evaluating the alternate approach to “make the cardiology world aware” of alternatives “that can relieve the surgical burden by minimizing the implantation time and length of the operation,” he said.
The comprehensive review is published in the Journal of the American College of Cardiology.
A Neglected Alternative
The sutureless Perceval device is held in place by a stent frame that self-expands. The Intuity device also relies primarily on its framework to anchor the valve in place but does involve three sutures. Both devices are still referred to as sutureless in the new review of them.
Only a small number of centers perform minimally invasive cardiac surgeries, and the main advantage of the devices — rapid deployment — has been eroded with the advent of automated knotting which has significantly reduced the time to implant and sutured valve.
The underuse of these devices is largely caused by the limited amount of comparative and prospective data, said Dr. Spadaccio. “The entire literature on sutureless aortic valve replacement with the exception of one randomized controlled trial is observational.”
That trial, PERSIST-AVR, found that the sutureless valves were just as good as conventional ones when it comes to major adverse cardiovascular events including all-cause death, myocardial infarction, stroke, or valve reintervention at 1 year.
In a subanalysis limited to patients who had isolated aortic valve replacement, the sutureless procedure was associated with lower adverse events (5.2% vs 10.8%) at the cost of a higher rate of pacemaker implantation (11% vs 1.6%).
There are also multiple retrospective studies and registries that have generated observational data comparing sutureless aortic valve replacement with SAVR and TAVR in various patient populations, said Dr. Spadaccio, and the review was based on more than a dozen studies published since 2015. Long-term follow-up data for sutureless aortic valve replacements, which now exceeds 10 years, suggest rates of structural valve deterioration and reintervention have been acceptably low.
The minimally invasive procedures have other advantages too. For example, relative to the greater trauma associated with open heart surgery, minimally invasive surgeries typically involve faster recovery, an advantage likely to appeal to many patients who are candidates for either.
Quicker Recovery
Collectively, these data suggest that sutureless aortic valve replacement might be a reasonable or even a more appropriate alternative to either SAVR or TAVR when considering specific patient characteristics and goals, according to the review, which included an algorithm identifying specifically where sutureless aortic valve replacement fits with SAVR and TAVR.
“The algorithm is based on different clinical scenarios and reflects current guidelines for SAVR,” said Dr. Spadaccio. For example, current guidelines identify SAVR as preferred in patients younger than 65 years and in older patients with a low Society of Thoracic Surgeons (STS) score, but there are many instances in which sutureless aortic valve replacement might be more attractive, such as in those also undergoing mitral valve repair, coronary artery bypass grafting, or another surgical procedure.
Dr. Spadaccio said that the STS score should not be considered in isolation when evaluating a patient for SAVR or TAVR. Other features such as mobility, frailty score, and comorbid liver or renal disease should also be considered when discussing the three options with patients. As a result, the algorithm emphasizes a detailed evaluation of patient characteristics in selecting one procedure over another.
“The treatment should be really tailored on the individual patient basis,” said Dr. Spadaccio.
Dr. Spadaccio acknowledged that there is a need for more comparative trials, particularly in regard to sutureless aortic valve replacement as an alternative to TAVR. “I really think that a 1:1 RCT on sutureless aortic valve replacement vs TAVR could give better answers to all of these interrogatives.”
But despite the limitations outlined in this review, Dr. Spadaccio and colleagues challenged the perception that current data are not sufficient to allow clinicians to consider sutureless aortic valve replacement in the mix of options.
A Viable Option
This comprehensive summary of what is known about sutureless aortic valve replacement compared with the other options addresses an important knowledge gap, said S. Chris Malaisrie, MD, a cardiac surgeon at Northwestern University Feinberg School of Medicine, Chicago, Illinois.
He said he agrees this option has unique qualities. “Minimally invasive surgery has been largely ignored by guideline writers, but patients certainly demand options that are less invasive than standard open heart surgery. Sutureless and rapid deployment valves facilitate minimally invasive surgery and offer an advantageous option for younger patients.”
Dr. Malaisrie said the review is generating discussion about a potentially valuable option within the cardiology community. And that is exactly what Dr. Spadaccio was hoping for. “This paper was meant to educate as much as possible on these details to assist and inform decision-making,” he said.
A version of this article first appeared on Medscape.com.
Compared with traditional replacement valves, sutureless valves placed through minimally invasive cardiac surgery have less data supporting their use but offer unique features that might make them the preferred option for certain patients, reported specialists.
The sutureless device known as Perceval (Corcym) and a rapidly deployed device called Intuity (Edwards Lifesciences) are used as an alternative to surgical aortic valve replacement (SAVR) and transcatheter aortic valve replacement (TAVR). But despite being commercially available since 2016, the devices are still not being used much.
The devices are not discussed in substantial detail in either the joint guidelines from the American College of Cardiology and American Heart Association issued in 2020 or guidelines from the European Society of Cardiology issued in 2022.
Cristiano Spadaccio, MD, PhD, a cardiothoracic surgeon associated with Lancashire Cardiac Centre in Blackpool, England, and his colleagues reviewed the small number of studies evaluating the alternate approach to “make the cardiology world aware” of alternatives “that can relieve the surgical burden by minimizing the implantation time and length of the operation,” he said.
The comprehensive review is published in the Journal of the American College of Cardiology.
A Neglected Alternative
The sutureless Perceval device is held in place by a stent frame that self-expands. The Intuity device also relies primarily on its framework to anchor the valve in place but does involve three sutures. Both devices are still referred to as sutureless in the new review of them.
Only a small number of centers perform minimally invasive cardiac surgeries, and the main advantage of the devices — rapid deployment — has been eroded with the advent of automated knotting which has significantly reduced the time to implant and sutured valve.
The underuse of these devices is largely caused by the limited amount of comparative and prospective data, said Dr. Spadaccio. “The entire literature on sutureless aortic valve replacement with the exception of one randomized controlled trial is observational.”
That trial, PERSIST-AVR, found that the sutureless valves were just as good as conventional ones when it comes to major adverse cardiovascular events including all-cause death, myocardial infarction, stroke, or valve reintervention at 1 year.
In a subanalysis limited to patients who had isolated aortic valve replacement, the sutureless procedure was associated with lower adverse events (5.2% vs 10.8%) at the cost of a higher rate of pacemaker implantation (11% vs 1.6%).
There are also multiple retrospective studies and registries that have generated observational data comparing sutureless aortic valve replacement with SAVR and TAVR in various patient populations, said Dr. Spadaccio, and the review was based on more than a dozen studies published since 2015. Long-term follow-up data for sutureless aortic valve replacements, which now exceeds 10 years, suggest rates of structural valve deterioration and reintervention have been acceptably low.
The minimally invasive procedures have other advantages too. For example, relative to the greater trauma associated with open heart surgery, minimally invasive surgeries typically involve faster recovery, an advantage likely to appeal to many patients who are candidates for either.
Quicker Recovery
Collectively, these data suggest that sutureless aortic valve replacement might be a reasonable or even a more appropriate alternative to either SAVR or TAVR when considering specific patient characteristics and goals, according to the review, which included an algorithm identifying specifically where sutureless aortic valve replacement fits with SAVR and TAVR.
“The algorithm is based on different clinical scenarios and reflects current guidelines for SAVR,” said Dr. Spadaccio. For example, current guidelines identify SAVR as preferred in patients younger than 65 years and in older patients with a low Society of Thoracic Surgeons (STS) score, but there are many instances in which sutureless aortic valve replacement might be more attractive, such as in those also undergoing mitral valve repair, coronary artery bypass grafting, or another surgical procedure.
Dr. Spadaccio said that the STS score should not be considered in isolation when evaluating a patient for SAVR or TAVR. Other features such as mobility, frailty score, and comorbid liver or renal disease should also be considered when discussing the three options with patients. As a result, the algorithm emphasizes a detailed evaluation of patient characteristics in selecting one procedure over another.
“The treatment should be really tailored on the individual patient basis,” said Dr. Spadaccio.
Dr. Spadaccio acknowledged that there is a need for more comparative trials, particularly in regard to sutureless aortic valve replacement as an alternative to TAVR. “I really think that a 1:1 RCT on sutureless aortic valve replacement vs TAVR could give better answers to all of these interrogatives.”
But despite the limitations outlined in this review, Dr. Spadaccio and colleagues challenged the perception that current data are not sufficient to allow clinicians to consider sutureless aortic valve replacement in the mix of options.
A Viable Option
This comprehensive summary of what is known about sutureless aortic valve replacement compared with the other options addresses an important knowledge gap, said S. Chris Malaisrie, MD, a cardiac surgeon at Northwestern University Feinberg School of Medicine, Chicago, Illinois.
He said he agrees this option has unique qualities. “Minimally invasive surgery has been largely ignored by guideline writers, but patients certainly demand options that are less invasive than standard open heart surgery. Sutureless and rapid deployment valves facilitate minimally invasive surgery and offer an advantageous option for younger patients.”
Dr. Malaisrie said the review is generating discussion about a potentially valuable option within the cardiology community. And that is exactly what Dr. Spadaccio was hoping for. “This paper was meant to educate as much as possible on these details to assist and inform decision-making,” he said.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Trial of Impella Heart Pump Stopped
An international trial of the Impella heart pump in patients with ST elevation myocardial infarction (STEMI) and cardiogenic shock has been stopped by the sponsor, Abiomed Inc. The termination followed news that another international trial, DanGer Shock, found that the pump improved survival in these patients.
“I was convinced that the study could not continue,” one of the principal investigators William O’Neill, MD, an interventional cardiologist with the Henry Ford Health in Detroit, said in an interview. After 3.5 years of work and thousands of person-hours, he added, “It’s not a decision that people took lightly.”
The trial already had three sites in Europe and one in the United States up and running, with two more US sites slated to join the trial. It had started enrolling patients, although few to date.
DanGer Shock trial results were expected to have a serious effect on how RECOVER IV would unfold. It was previously uncertain whether the Impella heart pump would save lives vs existing approaches, said O’Neill and co-principal investigator Navin Kapur, MD, an interventional cardiologist at Tufts Medical Center in Boston. Once the DanGer Shock trial showed the benefits of using the heart pump, that equipoise vanished.
Loss of Clinical Equipoise
“The clinicians were challenged in getting consent from patients where they had to say, ‘If you are randomized to the control arm, we are not able to use an Impella,’ ” said Dr. Kapur. He pointed out that patients would be unlikely to agree to participate in a trial where they might not get the treatment already shown to improve survival.
Dr. Kapur and Dr. O’Neill said the clinicians participating in the trial expressed discomfort at continuing. The RECOVER IV trial was expected to take many years to enroll the targeted number of patients. To participate, hospitals had to have the equipment and expertise to use the Impella heart pump, as well as the control treatments — balloon-pump support and extracorporeal membrane oxygenation (ECMO), Dr. Kapur explained. He said most patients with STEMI and cardiogenic shock would present to their nearest community hospitals, many of which would not have these treatments and would be unable to participate in the study.
Patients with STEMI and cardiogenic shock are uncommon. About 80,000 patients in the United States each year present with cardiogenic shock, of whom about 40% are not experiencing a STEMI, said Dr. O’Neill.
But those who do fit into the population of both STEMI and cardiogenic shock are at very high risk, said Dr. Kapur. “One in three or one in two patients with STEMI and cardiogenic shock will die in hospital.”
Getting Hearts Pumping
The Impella heart pump was originally developed by Impella Cardiosystems in Aachen, Germany, which was acquired by Abiomed in 2005, according to the Abiomed website. And Abiomed was acquired by Johnson & Johnson MedTech in 2022. The company has developed a series of models over the years and said that Impella CP — the model used in DanGer Shock and RECOVER IV trials — is the world’s smallest heart pump.
“Impella is the only heart pump that can be introduced percutaneously through the leg,” said Dr. O’Neill, whereas other pumps available are used only in open-heart surgery. While Impella is the first pump to be used this way, he said it won’t be the last. Other, more powerful pumps are being developed.
DanGer Shock: A Leap Forward
Despite leading to the halt of another trial, the DanGer Shock results are a good news story, said the RECOVER IV investigators.
“The DanGer trial is a huge advance,” said Dr. O’Neill. “It’s the first study this century that shows something that improves survival in cardiogenic shock. You treat eight patients, and you save one life.” Dr. O’Neill said this is one of the best outcomes he has seen during his long career.
Dr. Kapur said the DanGer trial is also a leap forward in designing trials for cardiogenic shock. He said previous trials of mechanical support in cardiogenic shock had neutral results, probably due to broad inclusion criteria for patients.
“The DanGer trial was selective in its inclusion and exclusion criteria. That made it more difficult to enroll the population, so it took a lot longer. But it used the right device at the right time in the right patient, and it was successful,” he said.
“The DanGer investigators need to be applauded,” he added. “The lesson is, we have to design the right trials.”
New Cardiogenic Shock Trials
Dr. O’Neill and Dr. Kapur said the groundwork they laid for RECOVER IV can be used for new trials.
“We have 50 sites in the US, Germany, and Denmark. They’re interested, and they’re waiting,” said Dr. O’Neill. The researchers are poised to begin new trials once protocols are developed.
What will the next trials investigate?
DanGer Shock results showed higher rates of adverse events following Impella use than after standard care. “We need to come up with strategies to decrease bleeding problems and renal failure,” said Dr. O’Neill, and these could be tested in trials.
Other questions he would like to see investigated are using the Impella heart pump before or after angioplasty, and multi-vessel vs culprit-vessel percutaneous coronary intervention in cardiogenic shock with Impella support.
Dr. Kapur mentioned studying patients excluded from the DanGer Shock trial — such as those needing right ventricular support — because DanGer Shock covered only left ventricular support and those suffering cardiac arrest outside hospital. He said trials could compare differences between models of Impella and investigate the role of ECMO.
“I’m optimistic that we can design more randomized controlled trials with the right patient population and right treatment algorithm,” Dr. Kapur said. This is a critical step toward better outcomes for patients, he added. Another step is optimizing the design of heart pumps, which should decrease the rates of adverse events, he said. “I have a lot of optimism for the future of device design.”
A version of this article first appeared on Medscape.com.
An international trial of the Impella heart pump in patients with ST elevation myocardial infarction (STEMI) and cardiogenic shock has been stopped by the sponsor, Abiomed Inc. The termination followed news that another international trial, DanGer Shock, found that the pump improved survival in these patients.
“I was convinced that the study could not continue,” one of the principal investigators William O’Neill, MD, an interventional cardiologist with the Henry Ford Health in Detroit, said in an interview. After 3.5 years of work and thousands of person-hours, he added, “It’s not a decision that people took lightly.”
The trial already had three sites in Europe and one in the United States up and running, with two more US sites slated to join the trial. It had started enrolling patients, although few to date.
DanGer Shock trial results were expected to have a serious effect on how RECOVER IV would unfold. It was previously uncertain whether the Impella heart pump would save lives vs existing approaches, said O’Neill and co-principal investigator Navin Kapur, MD, an interventional cardiologist at Tufts Medical Center in Boston. Once the DanGer Shock trial showed the benefits of using the heart pump, that equipoise vanished.
Loss of Clinical Equipoise
“The clinicians were challenged in getting consent from patients where they had to say, ‘If you are randomized to the control arm, we are not able to use an Impella,’ ” said Dr. Kapur. He pointed out that patients would be unlikely to agree to participate in a trial where they might not get the treatment already shown to improve survival.
Dr. Kapur and Dr. O’Neill said the clinicians participating in the trial expressed discomfort at continuing. The RECOVER IV trial was expected to take many years to enroll the targeted number of patients. To participate, hospitals had to have the equipment and expertise to use the Impella heart pump, as well as the control treatments — balloon-pump support and extracorporeal membrane oxygenation (ECMO), Dr. Kapur explained. He said most patients with STEMI and cardiogenic shock would present to their nearest community hospitals, many of which would not have these treatments and would be unable to participate in the study.
Patients with STEMI and cardiogenic shock are uncommon. About 80,000 patients in the United States each year present with cardiogenic shock, of whom about 40% are not experiencing a STEMI, said Dr. O’Neill.
But those who do fit into the population of both STEMI and cardiogenic shock are at very high risk, said Dr. Kapur. “One in three or one in two patients with STEMI and cardiogenic shock will die in hospital.”
Getting Hearts Pumping
The Impella heart pump was originally developed by Impella Cardiosystems in Aachen, Germany, which was acquired by Abiomed in 2005, according to the Abiomed website. And Abiomed was acquired by Johnson & Johnson MedTech in 2022. The company has developed a series of models over the years and said that Impella CP — the model used in DanGer Shock and RECOVER IV trials — is the world’s smallest heart pump.
“Impella is the only heart pump that can be introduced percutaneously through the leg,” said Dr. O’Neill, whereas other pumps available are used only in open-heart surgery. While Impella is the first pump to be used this way, he said it won’t be the last. Other, more powerful pumps are being developed.
DanGer Shock: A Leap Forward
Despite leading to the halt of another trial, the DanGer Shock results are a good news story, said the RECOVER IV investigators.
“The DanGer trial is a huge advance,” said Dr. O’Neill. “It’s the first study this century that shows something that improves survival in cardiogenic shock. You treat eight patients, and you save one life.” Dr. O’Neill said this is one of the best outcomes he has seen during his long career.
Dr. Kapur said the DanGer trial is also a leap forward in designing trials for cardiogenic shock. He said previous trials of mechanical support in cardiogenic shock had neutral results, probably due to broad inclusion criteria for patients.
“The DanGer trial was selective in its inclusion and exclusion criteria. That made it more difficult to enroll the population, so it took a lot longer. But it used the right device at the right time in the right patient, and it was successful,” he said.
“The DanGer investigators need to be applauded,” he added. “The lesson is, we have to design the right trials.”
New Cardiogenic Shock Trials
Dr. O’Neill and Dr. Kapur said the groundwork they laid for RECOVER IV can be used for new trials.
“We have 50 sites in the US, Germany, and Denmark. They’re interested, and they’re waiting,” said Dr. O’Neill. The researchers are poised to begin new trials once protocols are developed.
What will the next trials investigate?
DanGer Shock results showed higher rates of adverse events following Impella use than after standard care. “We need to come up with strategies to decrease bleeding problems and renal failure,” said Dr. O’Neill, and these could be tested in trials.
Other questions he would like to see investigated are using the Impella heart pump before or after angioplasty, and multi-vessel vs culprit-vessel percutaneous coronary intervention in cardiogenic shock with Impella support.
Dr. Kapur mentioned studying patients excluded from the DanGer Shock trial — such as those needing right ventricular support — because DanGer Shock covered only left ventricular support and those suffering cardiac arrest outside hospital. He said trials could compare differences between models of Impella and investigate the role of ECMO.
“I’m optimistic that we can design more randomized controlled trials with the right patient population and right treatment algorithm,” Dr. Kapur said. This is a critical step toward better outcomes for patients, he added. Another step is optimizing the design of heart pumps, which should decrease the rates of adverse events, he said. “I have a lot of optimism for the future of device design.”
A version of this article first appeared on Medscape.com.
An international trial of the Impella heart pump in patients with ST elevation myocardial infarction (STEMI) and cardiogenic shock has been stopped by the sponsor, Abiomed Inc. The termination followed news that another international trial, DanGer Shock, found that the pump improved survival in these patients.
“I was convinced that the study could not continue,” one of the principal investigators William O’Neill, MD, an interventional cardiologist with the Henry Ford Health in Detroit, said in an interview. After 3.5 years of work and thousands of person-hours, he added, “It’s not a decision that people took lightly.”
The trial already had three sites in Europe and one in the United States up and running, with two more US sites slated to join the trial. It had started enrolling patients, although few to date.
DanGer Shock trial results were expected to have a serious effect on how RECOVER IV would unfold. It was previously uncertain whether the Impella heart pump would save lives vs existing approaches, said O’Neill and co-principal investigator Navin Kapur, MD, an interventional cardiologist at Tufts Medical Center in Boston. Once the DanGer Shock trial showed the benefits of using the heart pump, that equipoise vanished.
Loss of Clinical Equipoise
“The clinicians were challenged in getting consent from patients where they had to say, ‘If you are randomized to the control arm, we are not able to use an Impella,’ ” said Dr. Kapur. He pointed out that patients would be unlikely to agree to participate in a trial where they might not get the treatment already shown to improve survival.
Dr. Kapur and Dr. O’Neill said the clinicians participating in the trial expressed discomfort at continuing. The RECOVER IV trial was expected to take many years to enroll the targeted number of patients. To participate, hospitals had to have the equipment and expertise to use the Impella heart pump, as well as the control treatments — balloon-pump support and extracorporeal membrane oxygenation (ECMO), Dr. Kapur explained. He said most patients with STEMI and cardiogenic shock would present to their nearest community hospitals, many of which would not have these treatments and would be unable to participate in the study.
Patients with STEMI and cardiogenic shock are uncommon. About 80,000 patients in the United States each year present with cardiogenic shock, of whom about 40% are not experiencing a STEMI, said Dr. O’Neill.
But those who do fit into the population of both STEMI and cardiogenic shock are at very high risk, said Dr. Kapur. “One in three or one in two patients with STEMI and cardiogenic shock will die in hospital.”
Getting Hearts Pumping
The Impella heart pump was originally developed by Impella Cardiosystems in Aachen, Germany, which was acquired by Abiomed in 2005, according to the Abiomed website. And Abiomed was acquired by Johnson & Johnson MedTech in 2022. The company has developed a series of models over the years and said that Impella CP — the model used in DanGer Shock and RECOVER IV trials — is the world’s smallest heart pump.
“Impella is the only heart pump that can be introduced percutaneously through the leg,” said Dr. O’Neill, whereas other pumps available are used only in open-heart surgery. While Impella is the first pump to be used this way, he said it won’t be the last. Other, more powerful pumps are being developed.
DanGer Shock: A Leap Forward
Despite leading to the halt of another trial, the DanGer Shock results are a good news story, said the RECOVER IV investigators.
“The DanGer trial is a huge advance,” said Dr. O’Neill. “It’s the first study this century that shows something that improves survival in cardiogenic shock. You treat eight patients, and you save one life.” Dr. O’Neill said this is one of the best outcomes he has seen during his long career.
Dr. Kapur said the DanGer trial is also a leap forward in designing trials for cardiogenic shock. He said previous trials of mechanical support in cardiogenic shock had neutral results, probably due to broad inclusion criteria for patients.
“The DanGer trial was selective in its inclusion and exclusion criteria. That made it more difficult to enroll the population, so it took a lot longer. But it used the right device at the right time in the right patient, and it was successful,” he said.
“The DanGer investigators need to be applauded,” he added. “The lesson is, we have to design the right trials.”
New Cardiogenic Shock Trials
Dr. O’Neill and Dr. Kapur said the groundwork they laid for RECOVER IV can be used for new trials.
“We have 50 sites in the US, Germany, and Denmark. They’re interested, and they’re waiting,” said Dr. O’Neill. The researchers are poised to begin new trials once protocols are developed.
What will the next trials investigate?
DanGer Shock results showed higher rates of adverse events following Impella use than after standard care. “We need to come up with strategies to decrease bleeding problems and renal failure,” said Dr. O’Neill, and these could be tested in trials.
Other questions he would like to see investigated are using the Impella heart pump before or after angioplasty, and multi-vessel vs culprit-vessel percutaneous coronary intervention in cardiogenic shock with Impella support.
Dr. Kapur mentioned studying patients excluded from the DanGer Shock trial — such as those needing right ventricular support — because DanGer Shock covered only left ventricular support and those suffering cardiac arrest outside hospital. He said trials could compare differences between models of Impella and investigate the role of ECMO.
“I’m optimistic that we can design more randomized controlled trials with the right patient population and right treatment algorithm,” Dr. Kapur said. This is a critical step toward better outcomes for patients, he added. Another step is optimizing the design of heart pumps, which should decrease the rates of adverse events, he said. “I have a lot of optimism for the future of device design.”
A version of this article first appeared on Medscape.com.
Why Cardiac Biomarkers Don’t Help Predict Heart Disease
This transcript has been edited for clarity.
It’s the counterintuitive stuff in epidemiology that always really interests me. One intuition many of us have is that if a risk factor is significantly associated with an outcome, knowledge of that risk factor would help to predict that outcome. Makes sense. Feels right.
But it’s not right. Not always.
Here’s a fake example to illustrate my point. Let’s say we have 10,000 individuals who we follow for 10 years and 2000 of them die. (It’s been a rough decade.) At baseline, I measured a novel biomarker, the Perry Factor, in everyone. To keep it simple, the Perry Factor has only two values: 0 or 1.
I then do a standard associational analysis and find that individuals who are positive for the Perry Factor have a 40-fold higher odds of death than those who are negative for it. I am beginning to reconsider ascribing my good name to this biomarker. This is a highly statistically significant result — a P value <.001.
Clearly, knowledge of the Perry Factor should help me predict who will die in the cohort. I evaluate predictive power using a metric called the area under the receiver operating characteristic curve (AUC, referred to as the C-statistic in time-to-event studies). It tells you, given two people — one who dies and one who doesn’t — how frequently you “pick” the right person, given the knowledge of their Perry Factor.
A C-statistic of 0.5, or 50%, would mean the Perry Factor gives you no better results than a coin flip; it’s chance. A C-statistic of 1 is perfect prediction. So, what will the C-statistic be, given the incredibly strong association of the Perry Factor with outcomes? 0.9? 0.95?
0.5024. Almost useless.

Let’s figure out why strength of association and usefulness for prediction are not always the same thing.
I constructed my fake Perry Factor dataset quite carefully to illustrate this point. Let me show you what happened. What you see here is a breakdown of the patients in my fake study. You can see that just 11 of them were Perry Factor positive, but 10 of those 11 ended up dying.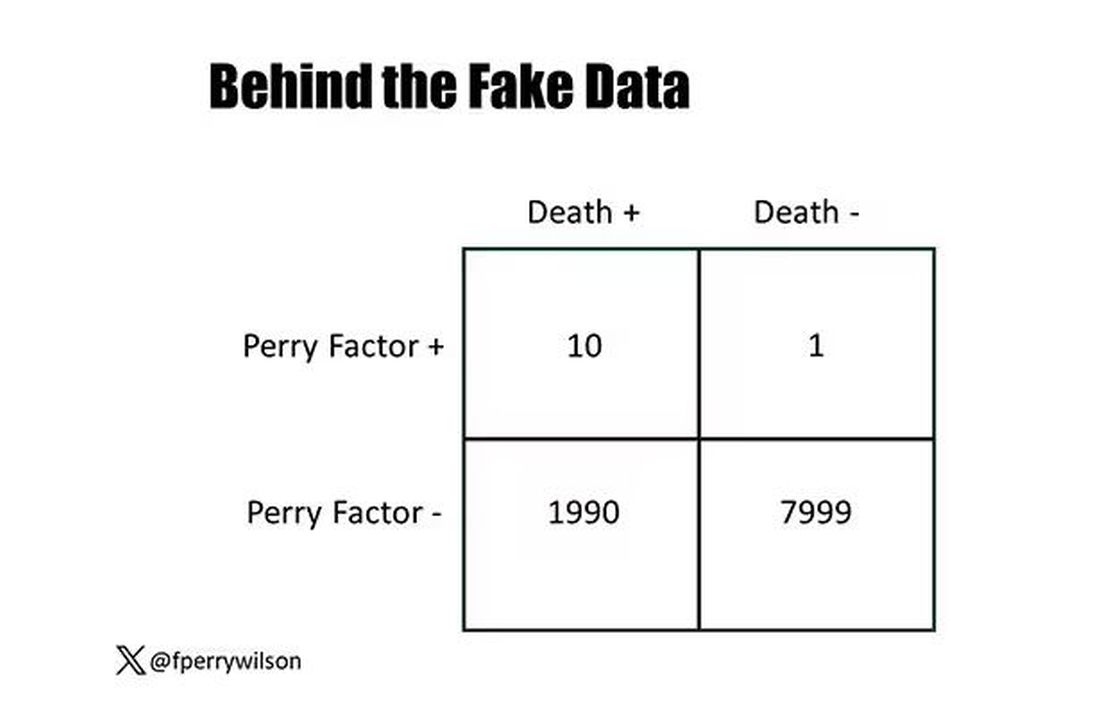
That’s quite unlikely by chance alone. It really does appear that if you have Perry Factor, your risk for death is much higher. But the reason that Perry Factor is a bad predictor is because it is so rare in the population. Sure, you can use it to correctly predict the outcome of 10 of the 11 people who have it, but the vast majority of people don’t have Perry Factor. It’s useless to distinguish who will die vs who will live in that population.
Why have I spent so much time trying to reverse our intuition that strength of association and strength of predictive power must be related? Because it helps to explain this paper, “Prognostic Value of Cardiovascular Biomarkers in the Population,” appearing in JAMA, which is a very nice piece of work trying to help us better predict cardiovascular disease.
I don’t need to tell you that cardiovascular disease is the number-one killer in this country and most of the world. I don’t need to tell you that we have really good preventive therapies and lifestyle interventions that can reduce the risk. But it would be nice to know in whom, specifically, we should use those interventions.
Cardiovascular risk scores, to date, are pretty simple. The most common one in use in the United States, the pooled cohort risk equation, has nine variables, two of which require a cholesterol panel and one a blood pressure test. It’s easy and it’s pretty accurate.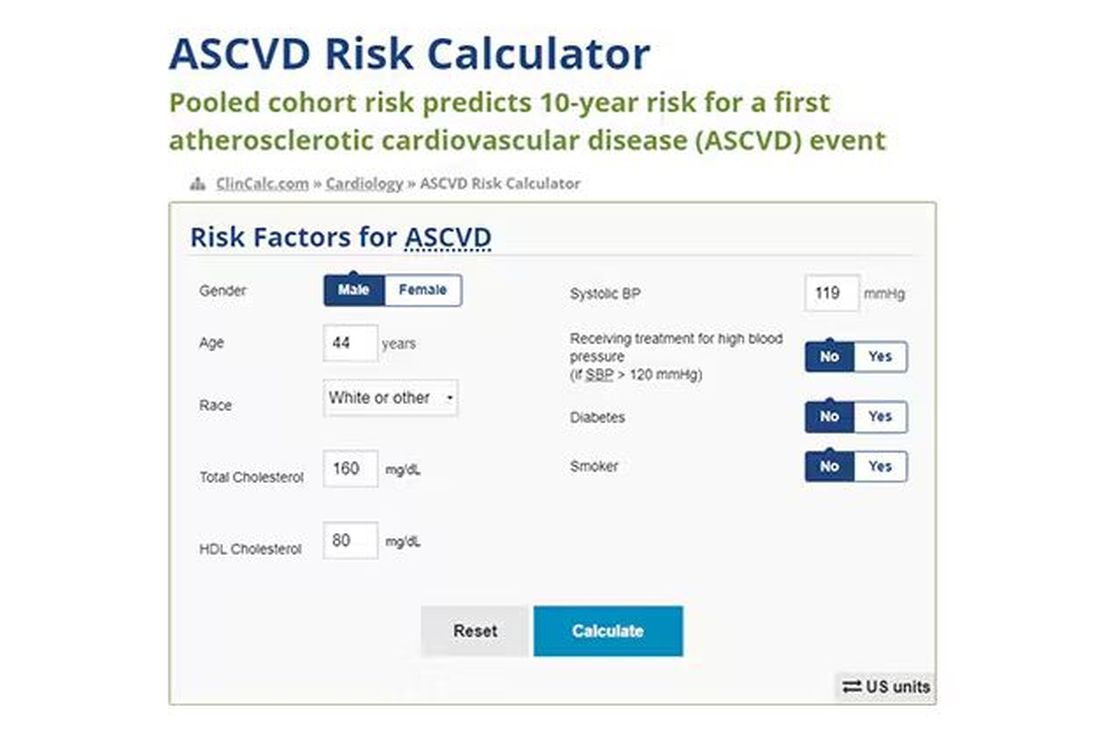
Using the score from the pooled cohort risk calculator, you get a C-statistic as high as 0.82 when applied to Black women, a low of 0.71 when applied to Black men. Non-Black individuals are in the middle. Not bad. But, clearly, not perfect.
And aren’t we in the era of big data, the era of personalized medicine? We have dozens, maybe hundreds, of quantifiable biomarkers that are associated with subsequent heart disease. Surely, by adding these biomarkers into the risk equation, we can improve prediction. Right?
The JAMA study includes 164,054 patients pooled from 28 cohort studies from 12 countries. All the studies measured various key biomarkers at baseline and followed their participants for cardiovascular events like heart attack, stroke, coronary revascularization, and so on.
The biomarkers in question are really the big guns in this space: troponin, a marker of stress on the heart muscle; NT-proBNP, a marker of stretch on the heart muscle; and C-reactive protein, a marker of inflammation. In every case, higher levels of these markers at baseline were associated with a higher risk for cardiovascular disease in the future.
Troponin T, shown here, has a basically linear risk with subsequent cardiovascular disease.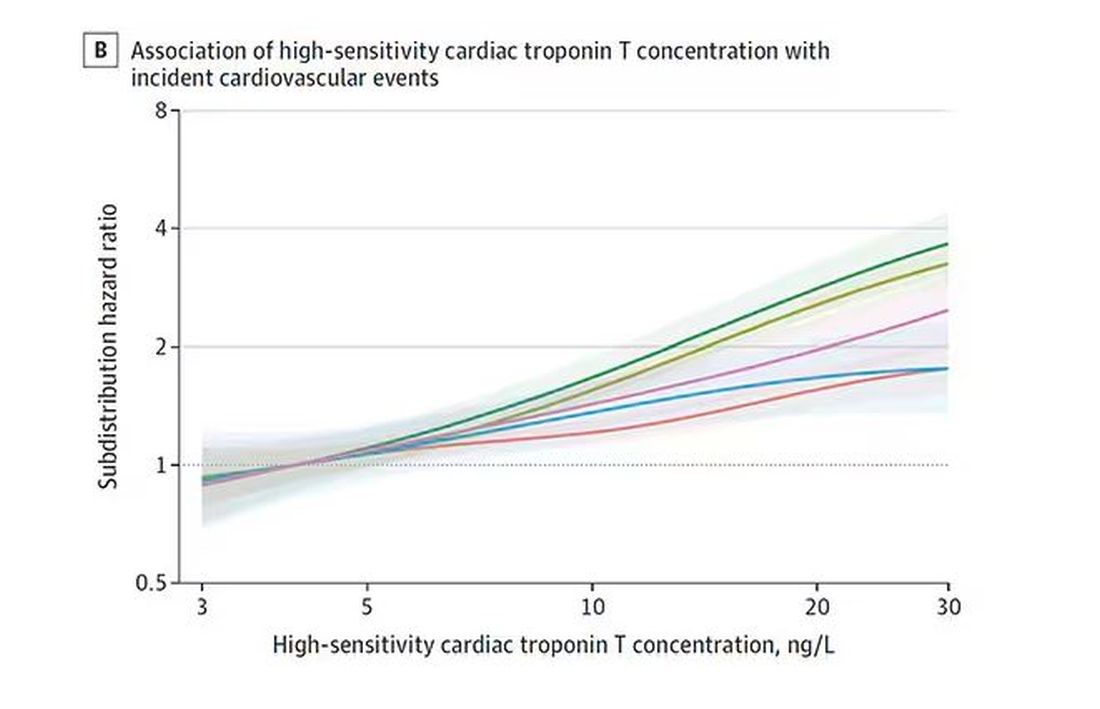
BNP seems to demonstrate more of a threshold effect, where levels above 60 start to associate with problems.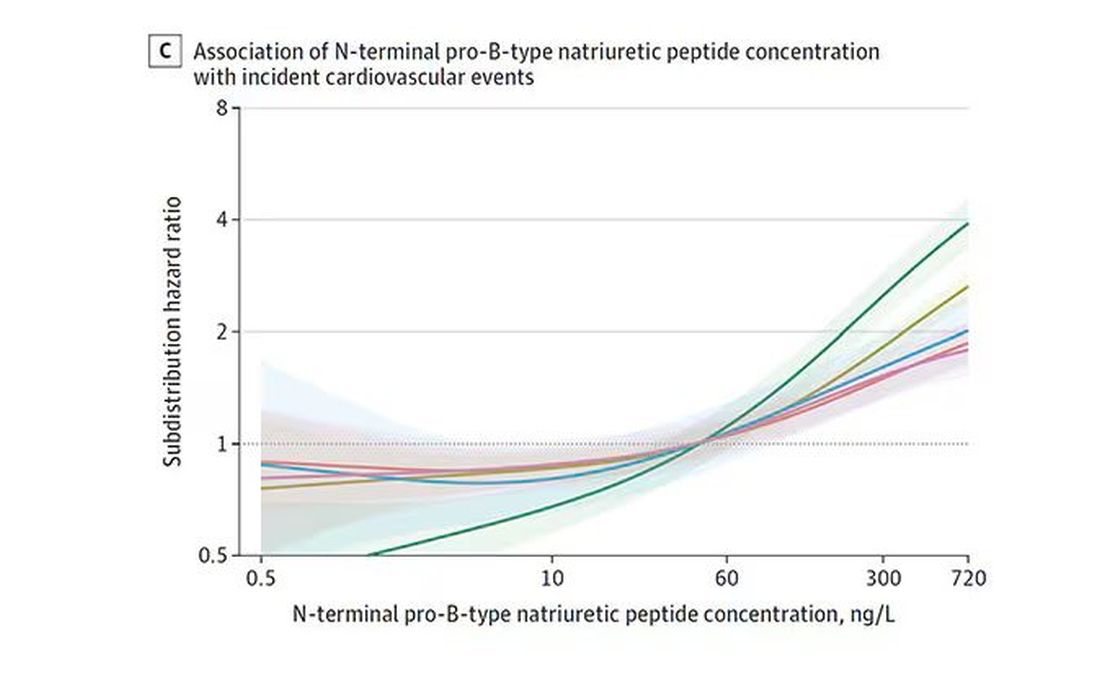
And CRP does a similar thing, with levels above 1.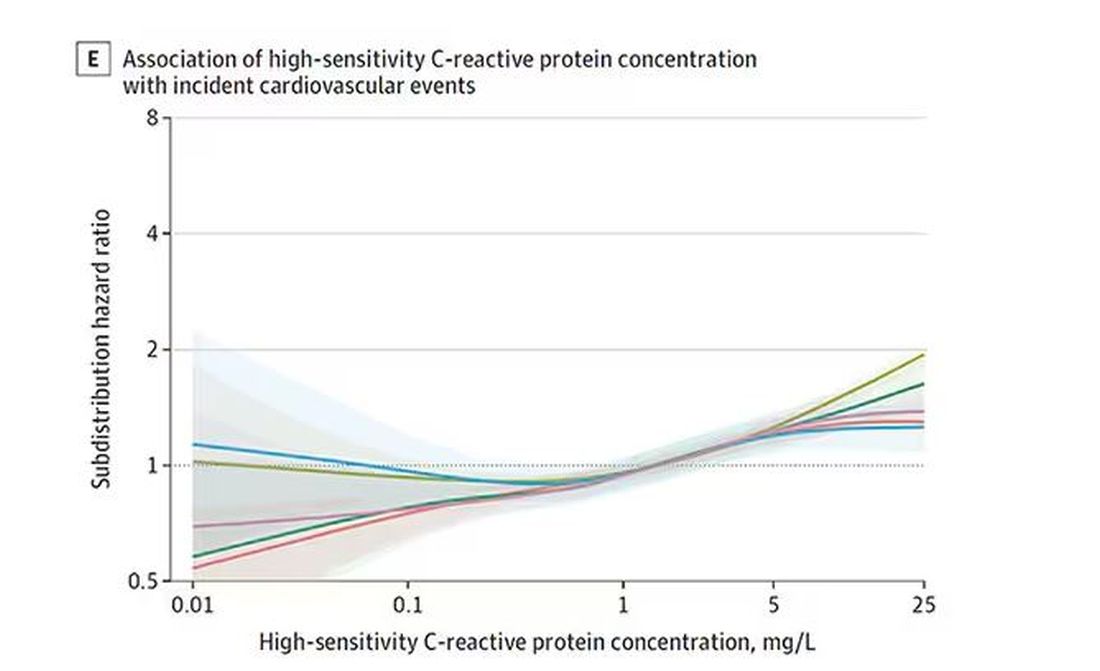
All of these findings were statistically significant. If you have higher levels of one or more of these biomarkers, you are more likely to have cardiovascular disease in the future.
Of course, our old friend the pooled cohort risk equation is still here — in the background — requiring just that one blood test and measurement of blood pressure. Let’s talk about predictive power.
The pooled cohort risk equation score, in this study, had a C-statistic of 0.812.
By adding troponin, BNP, and CRP to the equation, the new C-statistic is 0.819. Barely any change.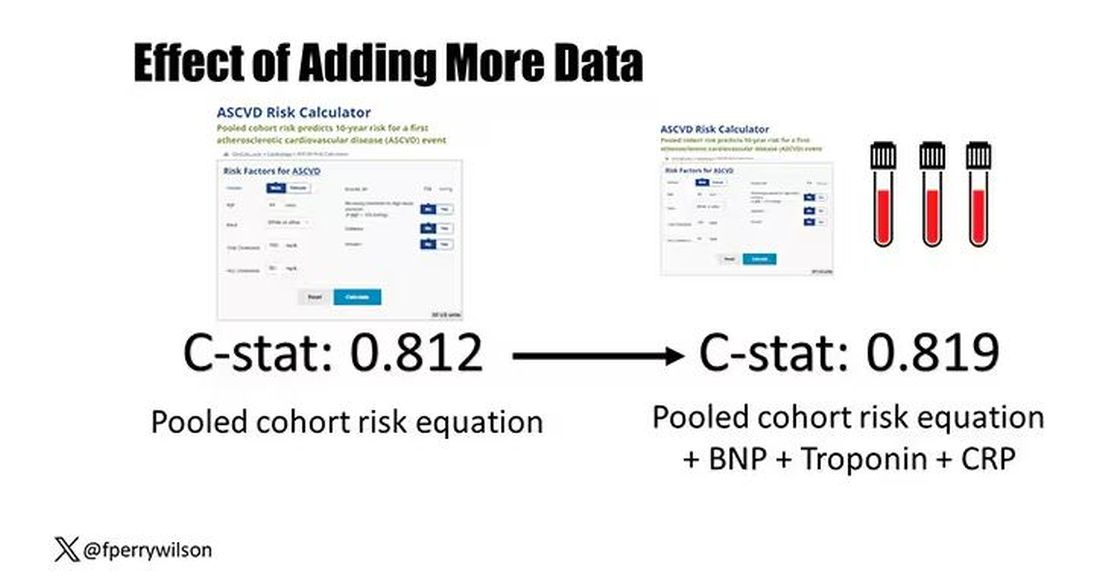
Now, the authors looked at different types of prediction here. The greatest improvement in the AUC was seen when they tried to predict heart failure within 1 year of measurement; there the AUC improved by 0.04. But the presence of BNP as a biomarker and the short time window of 1 year makes me wonder whether this is really prediction at all or whether they were essentially just diagnosing people with existing heart failure.
Why does this happen? Why do these promising biomarkers, clearly associated with bad outcomes, fail to improve our ability to predict the future? I already gave one example, which has to do with how the markers are distributed in the population. But even more relevant here is that the new markers will only improve prediction insofar as they are not already represented in the old predictive model.
Of course, BNP, for example, wasn’t in the old model. But smoking was. Diabetes was. Blood pressure was. All of that data might actually tell you something about the patient’s BNP through their mutual correlation. And improvement in prediction requires new information.
This is actually why I consider this a really successful study. We need to do studies like this to help us find what those new sources of information might be.
We will never get to a C-statistic of 1. Perfect prediction is the domain of palm readers and astrophysicists. But better prediction is always possible through data. The big question, of course, is which data?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s the counterintuitive stuff in epidemiology that always really interests me. One intuition many of us have is that if a risk factor is significantly associated with an outcome, knowledge of that risk factor would help to predict that outcome. Makes sense. Feels right.
But it’s not right. Not always.
Here’s a fake example to illustrate my point. Let’s say we have 10,000 individuals who we follow for 10 years and 2000 of them die. (It’s been a rough decade.) At baseline, I measured a novel biomarker, the Perry Factor, in everyone. To keep it simple, the Perry Factor has only two values: 0 or 1.
I then do a standard associational analysis and find that individuals who are positive for the Perry Factor have a 40-fold higher odds of death than those who are negative for it. I am beginning to reconsider ascribing my good name to this biomarker. This is a highly statistically significant result — a P value <.001.
Clearly, knowledge of the Perry Factor should help me predict who will die in the cohort. I evaluate predictive power using a metric called the area under the receiver operating characteristic curve (AUC, referred to as the C-statistic in time-to-event studies). It tells you, given two people — one who dies and one who doesn’t — how frequently you “pick” the right person, given the knowledge of their Perry Factor.
A C-statistic of 0.5, or 50%, would mean the Perry Factor gives you no better results than a coin flip; it’s chance. A C-statistic of 1 is perfect prediction. So, what will the C-statistic be, given the incredibly strong association of the Perry Factor with outcomes? 0.9? 0.95?
0.5024. Almost useless.
Let’s figure out why strength of association and usefulness for prediction are not always the same thing.
I constructed my fake Perry Factor dataset quite carefully to illustrate this point. Let me show you what happened. What you see here is a breakdown of the patients in my fake study. You can see that just 11 of them were Perry Factor positive, but 10 of those 11 ended up dying.
That’s quite unlikely by chance alone. It really does appear that if you have Perry Factor, your risk for death is much higher. But the reason that Perry Factor is a bad predictor is because it is so rare in the population. Sure, you can use it to correctly predict the outcome of 10 of the 11 people who have it, but the vast majority of people don’t have Perry Factor. It’s useless to distinguish who will die vs who will live in that population.
Why have I spent so much time trying to reverse our intuition that strength of association and strength of predictive power must be related? Because it helps to explain this paper, “Prognostic Value of Cardiovascular Biomarkers in the Population,” appearing in JAMA, which is a very nice piece of work trying to help us better predict cardiovascular disease.
I don’t need to tell you that cardiovascular disease is the number-one killer in this country and most of the world. I don’t need to tell you that we have really good preventive therapies and lifestyle interventions that can reduce the risk. But it would be nice to know in whom, specifically, we should use those interventions.
Cardiovascular risk scores, to date, are pretty simple. The most common one in use in the United States, the pooled cohort risk equation, has nine variables, two of which require a cholesterol panel and one a blood pressure test. It’s easy and it’s pretty accurate.
Using the score from the pooled cohort risk calculator, you get a C-statistic as high as 0.82 when applied to Black women, a low of 0.71 when applied to Black men. Non-Black individuals are in the middle. Not bad. But, clearly, not perfect.
And aren’t we in the era of big data, the era of personalized medicine? We have dozens, maybe hundreds, of quantifiable biomarkers that are associated with subsequent heart disease. Surely, by adding these biomarkers into the risk equation, we can improve prediction. Right?
The JAMA study includes 164,054 patients pooled from 28 cohort studies from 12 countries. All the studies measured various key biomarkers at baseline and followed their participants for cardiovascular events like heart attack, stroke, coronary revascularization, and so on.
The biomarkers in question are really the big guns in this space: troponin, a marker of stress on the heart muscle; NT-proBNP, a marker of stretch on the heart muscle; and C-reactive protein, a marker of inflammation. In every case, higher levels of these markers at baseline were associated with a higher risk for cardiovascular disease in the future.
Troponin T, shown here, has a basically linear risk with subsequent cardiovascular disease.
BNP seems to demonstrate more of a threshold effect, where levels above 60 start to associate with problems.
And CRP does a similar thing, with levels above 1.
All of these findings were statistically significant. If you have higher levels of one or more of these biomarkers, you are more likely to have cardiovascular disease in the future.
Of course, our old friend the pooled cohort risk equation is still here — in the background — requiring just that one blood test and measurement of blood pressure. Let’s talk about predictive power.
The pooled cohort risk equation score, in this study, had a C-statistic of 0.812.
By adding troponin, BNP, and CRP to the equation, the new C-statistic is 0.819. Barely any change.
Now, the authors looked at different types of prediction here. The greatest improvement in the AUC was seen when they tried to predict heart failure within 1 year of measurement; there the AUC improved by 0.04. But the presence of BNP as a biomarker and the short time window of 1 year makes me wonder whether this is really prediction at all or whether they were essentially just diagnosing people with existing heart failure.
Why does this happen? Why do these promising biomarkers, clearly associated with bad outcomes, fail to improve our ability to predict the future? I already gave one example, which has to do with how the markers are distributed in the population. But even more relevant here is that the new markers will only improve prediction insofar as they are not already represented in the old predictive model.
Of course, BNP, for example, wasn’t in the old model. But smoking was. Diabetes was. Blood pressure was. All of that data might actually tell you something about the patient’s BNP through their mutual correlation. And improvement in prediction requires new information.
This is actually why I consider this a really successful study. We need to do studies like this to help us find what those new sources of information might be.
We will never get to a C-statistic of 1. Perfect prediction is the domain of palm readers and astrophysicists. But better prediction is always possible through data. The big question, of course, is which data?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It’s the counterintuitive stuff in epidemiology that always really interests me. One intuition many of us have is that if a risk factor is significantly associated with an outcome, knowledge of that risk factor would help to predict that outcome. Makes sense. Feels right.
But it’s not right. Not always.
Here’s a fake example to illustrate my point. Let’s say we have 10,000 individuals who we follow for 10 years and 2000 of them die. (It’s been a rough decade.) At baseline, I measured a novel biomarker, the Perry Factor, in everyone. To keep it simple, the Perry Factor has only two values: 0 or 1.
I then do a standard associational analysis and find that individuals who are positive for the Perry Factor have a 40-fold higher odds of death than those who are negative for it. I am beginning to reconsider ascribing my good name to this biomarker. This is a highly statistically significant result — a P value <.001.
Clearly, knowledge of the Perry Factor should help me predict who will die in the cohort. I evaluate predictive power using a metric called the area under the receiver operating characteristic curve (AUC, referred to as the C-statistic in time-to-event studies). It tells you, given two people — one who dies and one who doesn’t — how frequently you “pick” the right person, given the knowledge of their Perry Factor.
A C-statistic of 0.5, or 50%, would mean the Perry Factor gives you no better results than a coin flip; it’s chance. A C-statistic of 1 is perfect prediction. So, what will the C-statistic be, given the incredibly strong association of the Perry Factor with outcomes? 0.9? 0.95?
0.5024. Almost useless.
Let’s figure out why strength of association and usefulness for prediction are not always the same thing.
I constructed my fake Perry Factor dataset quite carefully to illustrate this point. Let me show you what happened. What you see here is a breakdown of the patients in my fake study. You can see that just 11 of them were Perry Factor positive, but 10 of those 11 ended up dying.
That’s quite unlikely by chance alone. It really does appear that if you have Perry Factor, your risk for death is much higher. But the reason that Perry Factor is a bad predictor is because it is so rare in the population. Sure, you can use it to correctly predict the outcome of 10 of the 11 people who have it, but the vast majority of people don’t have Perry Factor. It’s useless to distinguish who will die vs who will live in that population.
Why have I spent so much time trying to reverse our intuition that strength of association and strength of predictive power must be related? Because it helps to explain this paper, “Prognostic Value of Cardiovascular Biomarkers in the Population,” appearing in JAMA, which is a very nice piece of work trying to help us better predict cardiovascular disease.
I don’t need to tell you that cardiovascular disease is the number-one killer in this country and most of the world. I don’t need to tell you that we have really good preventive therapies and lifestyle interventions that can reduce the risk. But it would be nice to know in whom, specifically, we should use those interventions.
Cardiovascular risk scores, to date, are pretty simple. The most common one in use in the United States, the pooled cohort risk equation, has nine variables, two of which require a cholesterol panel and one a blood pressure test. It’s easy and it’s pretty accurate.
Using the score from the pooled cohort risk calculator, you get a C-statistic as high as 0.82 when applied to Black women, a low of 0.71 when applied to Black men. Non-Black individuals are in the middle. Not bad. But, clearly, not perfect.
And aren’t we in the era of big data, the era of personalized medicine? We have dozens, maybe hundreds, of quantifiable biomarkers that are associated with subsequent heart disease. Surely, by adding these biomarkers into the risk equation, we can improve prediction. Right?
The JAMA study includes 164,054 patients pooled from 28 cohort studies from 12 countries. All the studies measured various key biomarkers at baseline and followed their participants for cardiovascular events like heart attack, stroke, coronary revascularization, and so on.
The biomarkers in question are really the big guns in this space: troponin, a marker of stress on the heart muscle; NT-proBNP, a marker of stretch on the heart muscle; and C-reactive protein, a marker of inflammation. In every case, higher levels of these markers at baseline were associated with a higher risk for cardiovascular disease in the future.
Troponin T, shown here, has a basically linear risk with subsequent cardiovascular disease.
BNP seems to demonstrate more of a threshold effect, where levels above 60 start to associate with problems.
And CRP does a similar thing, with levels above 1.
All of these findings were statistically significant. If you have higher levels of one or more of these biomarkers, you are more likely to have cardiovascular disease in the future.
Of course, our old friend the pooled cohort risk equation is still here — in the background — requiring just that one blood test and measurement of blood pressure. Let’s talk about predictive power.
The pooled cohort risk equation score, in this study, had a C-statistic of 0.812.
By adding troponin, BNP, and CRP to the equation, the new C-statistic is 0.819. Barely any change.
Now, the authors looked at different types of prediction here. The greatest improvement in the AUC was seen when they tried to predict heart failure within 1 year of measurement; there the AUC improved by 0.04. But the presence of BNP as a biomarker and the short time window of 1 year makes me wonder whether this is really prediction at all or whether they were essentially just diagnosing people with existing heart failure.
Why does this happen? Why do these promising biomarkers, clearly associated with bad outcomes, fail to improve our ability to predict the future? I already gave one example, which has to do with how the markers are distributed in the population. But even more relevant here is that the new markers will only improve prediction insofar as they are not already represented in the old predictive model.
Of course, BNP, for example, wasn’t in the old model. But smoking was. Diabetes was. Blood pressure was. All of that data might actually tell you something about the patient’s BNP through their mutual correlation. And improvement in prediction requires new information.
This is actually why I consider this a really successful study. We need to do studies like this to help us find what those new sources of information might be.
We will never get to a C-statistic of 1. Perfect prediction is the domain of palm readers and astrophysicists. But better prediction is always possible through data. The big question, of course, is which data?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.