User login
Transcatheter tricuspid valve repair in real-world setting replicates trials
Data support benefit and safety
For the TriClip system (Abbott), the data were drawn from a prospective postmarketing registry, and for the EVOQUE system (Edwards Lifesciences), data were generated by a compassionate use program.
The TriClip system is approved and available in Europe, but neither system has regulatory approval in the United States.
The two sets of data, each presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, are consistent with controlled trials. Each system was associated with high rates of procedural success, low rates of adverse events, and sustained improvements in quality of life.
Real-world backup for TRILUMINATE
Presented just days before the pivotal multinational TRILUMINATE trial was published in the New England Journal of Medicine, the bRIGHT postmarketing study of the TriClip device demonstrated a procedural rate of success and a subsequent reduction in TR that was at least as good but in a substantially sicker patient population.
“To appreciate these results, you have to put into perspective the baseline TR in our population,” reported Philipp Lurz, MD, PhD, of the Heart Center Leipzig, University of Leipzig, Germany. Whereas only 70% of those randomized in TRILUMINATE had grade 4 (massive) or 5 (torrential) TR, the proportion was 90% in bRIGHT.
The proportion with TR of moderate or less severity was 77% when assessed at 30 days in bRIGHT versus 72%, however, when assessed at 1 year in TRILUMINATE. In addition, procedural success was 99% in both studies even though patients in bRIGHT were on average older and had more comorbidities. At baseline, 80% of bRIGHT patients were in New York Heart Association (NYHA) class III or IV heart failure versus 59% of those in TRILUMINATE.
TRILUMINATE data, presented prior to publication at the annual meeting of the American College of Cardiology earlier this year, did not associate the transcatheter TR repair with a reduction in mortality or a reduction in hospitalization for heart failure, which were the first two of three hierarchical endpoints, but it did show benefit on the third, which was quality of life. As measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ), patients in the transcatheter repair group gained 12.3 points versus 0.6 points (P < .001) on medical therapy.
In the bRIGHT registry, patients gained 19 points in the KCCQ score after treatment. By 30 days, the proportion of patients in NHYA class III/IV had fallen from 80% to 20%. The major adverse event rate of 2.5% at 30 days was only modestly higher than the 1.7% rate at 30 days in TRILUMINATE.
“The safety profile remained strong despite the sicker population treated in the registry,” reported Dr. Lurz, whose results were simultaneously published in the Journal of the American College of Cardiology (JACC).
The bRIGHT registry analysis was based on 511 patients treated at 26 sites in Europe. Dr. Lurz characterized it as “the first prospective, single-arm, open-label, multicenter, postmarket registry to evaluate the safety and performance of any transcatheter tricuspid valve repair system.”
In a panel discussion following the presentation, Nicole Karam, MD, PhD, codirector of the heart valve unit, Hospital Georges Pompidou, Paris, praised a study of TEER tricuspid valve device in the real world, but she pointed out that the question of who to treat remains unanswered. Although symptom relief has value for a condition that can impose large deficits in quality of life, she called for more data to identify optimal candidates, particularly in the persistent absence of a major effect on hard endpoints.
Dr. Lurz agreed. In bRIGHT, predictors of a moderate or less TR at discharge included a smaller tethering distance, a smaller right ventricular end diastolic dimension, a smaller right atrial volume, and a smaller tricuspid annular diameter.
Each of these predictors argues for earlier treatment, he said, even if later treatment in a clinical trial provides a greater likelihood of eventually demonstrating benefits on hard endpoints.
‘Remarkable reduction’
The data from the much smaller compassionate use evaluation of the EVOQUE system generated similar evidence of safety and benefit while also making the point that earlier intervention offers a greater opportunity for preventing irreversible progression. With much longer follow up, the compassionate-use analysis, which involved patients even sicker than those included in bRIGHT, suggested these repairs are durable.
In this retrospective analysis of 38 patients treated at eight centers in Europe, the United States, and Canada, the mortality climbed steadily over 2 years of follow-up, reaching 29% at 2 years despite the fact that TR was reduced to < 1% after the procedure and remained durably suppressed at a median follow-up of 520 days.
The tricuspid valve repair with the EVOQUE system “was associated with a remarkable reduction in heart failure symptoms and significant improvement in NYHA functional class up to a maximum of 1,074 days after the intervention,” reported Lukas Stolz, MD, an interventional cardiologist at Ludwig-Maximilians-University, Munich.
In the data he presented at EuroPCR, which was published simultaneously as a letter in JACC, he said that favorable reverse remodeling of the right ventricle, which was observed as early as 30 days after the procedure, was maintained at long-term follow up.
The uncontrolled data from the compassionate analysis, like the bRIGHT registry, could not confirm that tricuspid valve repair changes the trajectory of progressive heart disease, but the favorable effects Dr. Stolz reported on cardiovascular function, not just symptoms, support this idea.
Dr. Lutz has financial relationships with Edwards Lifesciences, ReCor, and Abbott, which funded the bRIGHT registry. Dr. Karam reports financial relationships with Abbott, Edwards Lifesciences, and Medtronic. Dr. Stolz reports no potential conflicts of interest, but other coinvestigators of the retrospective analysis have financial relationships with Edwards Lifesciences, which is developing the EVOQUE system.
Data support benefit and safety
Data support benefit and safety
For the TriClip system (Abbott), the data were drawn from a prospective postmarketing registry, and for the EVOQUE system (Edwards Lifesciences), data were generated by a compassionate use program.
The TriClip system is approved and available in Europe, but neither system has regulatory approval in the United States.
The two sets of data, each presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, are consistent with controlled trials. Each system was associated with high rates of procedural success, low rates of adverse events, and sustained improvements in quality of life.
Real-world backup for TRILUMINATE
Presented just days before the pivotal multinational TRILUMINATE trial was published in the New England Journal of Medicine, the bRIGHT postmarketing study of the TriClip device demonstrated a procedural rate of success and a subsequent reduction in TR that was at least as good but in a substantially sicker patient population.
“To appreciate these results, you have to put into perspective the baseline TR in our population,” reported Philipp Lurz, MD, PhD, of the Heart Center Leipzig, University of Leipzig, Germany. Whereas only 70% of those randomized in TRILUMINATE had grade 4 (massive) or 5 (torrential) TR, the proportion was 90% in bRIGHT.
The proportion with TR of moderate or less severity was 77% when assessed at 30 days in bRIGHT versus 72%, however, when assessed at 1 year in TRILUMINATE. In addition, procedural success was 99% in both studies even though patients in bRIGHT were on average older and had more comorbidities. At baseline, 80% of bRIGHT patients were in New York Heart Association (NYHA) class III or IV heart failure versus 59% of those in TRILUMINATE.
TRILUMINATE data, presented prior to publication at the annual meeting of the American College of Cardiology earlier this year, did not associate the transcatheter TR repair with a reduction in mortality or a reduction in hospitalization for heart failure, which were the first two of three hierarchical endpoints, but it did show benefit on the third, which was quality of life. As measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ), patients in the transcatheter repair group gained 12.3 points versus 0.6 points (P < .001) on medical therapy.
In the bRIGHT registry, patients gained 19 points in the KCCQ score after treatment. By 30 days, the proportion of patients in NHYA class III/IV had fallen from 80% to 20%. The major adverse event rate of 2.5% at 30 days was only modestly higher than the 1.7% rate at 30 days in TRILUMINATE.
“The safety profile remained strong despite the sicker population treated in the registry,” reported Dr. Lurz, whose results were simultaneously published in the Journal of the American College of Cardiology (JACC).
The bRIGHT registry analysis was based on 511 patients treated at 26 sites in Europe. Dr. Lurz characterized it as “the first prospective, single-arm, open-label, multicenter, postmarket registry to evaluate the safety and performance of any transcatheter tricuspid valve repair system.”
In a panel discussion following the presentation, Nicole Karam, MD, PhD, codirector of the heart valve unit, Hospital Georges Pompidou, Paris, praised a study of TEER tricuspid valve device in the real world, but she pointed out that the question of who to treat remains unanswered. Although symptom relief has value for a condition that can impose large deficits in quality of life, she called for more data to identify optimal candidates, particularly in the persistent absence of a major effect on hard endpoints.
Dr. Lurz agreed. In bRIGHT, predictors of a moderate or less TR at discharge included a smaller tethering distance, a smaller right ventricular end diastolic dimension, a smaller right atrial volume, and a smaller tricuspid annular diameter.
Each of these predictors argues for earlier treatment, he said, even if later treatment in a clinical trial provides a greater likelihood of eventually demonstrating benefits on hard endpoints.
‘Remarkable reduction’
The data from the much smaller compassionate use evaluation of the EVOQUE system generated similar evidence of safety and benefit while also making the point that earlier intervention offers a greater opportunity for preventing irreversible progression. With much longer follow up, the compassionate-use analysis, which involved patients even sicker than those included in bRIGHT, suggested these repairs are durable.
In this retrospective analysis of 38 patients treated at eight centers in Europe, the United States, and Canada, the mortality climbed steadily over 2 years of follow-up, reaching 29% at 2 years despite the fact that TR was reduced to < 1% after the procedure and remained durably suppressed at a median follow-up of 520 days.
The tricuspid valve repair with the EVOQUE system “was associated with a remarkable reduction in heart failure symptoms and significant improvement in NYHA functional class up to a maximum of 1,074 days after the intervention,” reported Lukas Stolz, MD, an interventional cardiologist at Ludwig-Maximilians-University, Munich.
In the data he presented at EuroPCR, which was published simultaneously as a letter in JACC, he said that favorable reverse remodeling of the right ventricle, which was observed as early as 30 days after the procedure, was maintained at long-term follow up.
The uncontrolled data from the compassionate analysis, like the bRIGHT registry, could not confirm that tricuspid valve repair changes the trajectory of progressive heart disease, but the favorable effects Dr. Stolz reported on cardiovascular function, not just symptoms, support this idea.
Dr. Lutz has financial relationships with Edwards Lifesciences, ReCor, and Abbott, which funded the bRIGHT registry. Dr. Karam reports financial relationships with Abbott, Edwards Lifesciences, and Medtronic. Dr. Stolz reports no potential conflicts of interest, but other coinvestigators of the retrospective analysis have financial relationships with Edwards Lifesciences, which is developing the EVOQUE system.
For the TriClip system (Abbott), the data were drawn from a prospective postmarketing registry, and for the EVOQUE system (Edwards Lifesciences), data were generated by a compassionate use program.
The TriClip system is approved and available in Europe, but neither system has regulatory approval in the United States.
The two sets of data, each presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions, are consistent with controlled trials. Each system was associated with high rates of procedural success, low rates of adverse events, and sustained improvements in quality of life.
Real-world backup for TRILUMINATE
Presented just days before the pivotal multinational TRILUMINATE trial was published in the New England Journal of Medicine, the bRIGHT postmarketing study of the TriClip device demonstrated a procedural rate of success and a subsequent reduction in TR that was at least as good but in a substantially sicker patient population.
“To appreciate these results, you have to put into perspective the baseline TR in our population,” reported Philipp Lurz, MD, PhD, of the Heart Center Leipzig, University of Leipzig, Germany. Whereas only 70% of those randomized in TRILUMINATE had grade 4 (massive) or 5 (torrential) TR, the proportion was 90% in bRIGHT.
The proportion with TR of moderate or less severity was 77% when assessed at 30 days in bRIGHT versus 72%, however, when assessed at 1 year in TRILUMINATE. In addition, procedural success was 99% in both studies even though patients in bRIGHT were on average older and had more comorbidities. At baseline, 80% of bRIGHT patients were in New York Heart Association (NYHA) class III or IV heart failure versus 59% of those in TRILUMINATE.
TRILUMINATE data, presented prior to publication at the annual meeting of the American College of Cardiology earlier this year, did not associate the transcatheter TR repair with a reduction in mortality or a reduction in hospitalization for heart failure, which were the first two of three hierarchical endpoints, but it did show benefit on the third, which was quality of life. As measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ), patients in the transcatheter repair group gained 12.3 points versus 0.6 points (P < .001) on medical therapy.
In the bRIGHT registry, patients gained 19 points in the KCCQ score after treatment. By 30 days, the proportion of patients in NHYA class III/IV had fallen from 80% to 20%. The major adverse event rate of 2.5% at 30 days was only modestly higher than the 1.7% rate at 30 days in TRILUMINATE.
“The safety profile remained strong despite the sicker population treated in the registry,” reported Dr. Lurz, whose results were simultaneously published in the Journal of the American College of Cardiology (JACC).
The bRIGHT registry analysis was based on 511 patients treated at 26 sites in Europe. Dr. Lurz characterized it as “the first prospective, single-arm, open-label, multicenter, postmarket registry to evaluate the safety and performance of any transcatheter tricuspid valve repair system.”
In a panel discussion following the presentation, Nicole Karam, MD, PhD, codirector of the heart valve unit, Hospital Georges Pompidou, Paris, praised a study of TEER tricuspid valve device in the real world, but she pointed out that the question of who to treat remains unanswered. Although symptom relief has value for a condition that can impose large deficits in quality of life, she called for more data to identify optimal candidates, particularly in the persistent absence of a major effect on hard endpoints.
Dr. Lurz agreed. In bRIGHT, predictors of a moderate or less TR at discharge included a smaller tethering distance, a smaller right ventricular end diastolic dimension, a smaller right atrial volume, and a smaller tricuspid annular diameter.
Each of these predictors argues for earlier treatment, he said, even if later treatment in a clinical trial provides a greater likelihood of eventually demonstrating benefits on hard endpoints.
‘Remarkable reduction’
The data from the much smaller compassionate use evaluation of the EVOQUE system generated similar evidence of safety and benefit while also making the point that earlier intervention offers a greater opportunity for preventing irreversible progression. With much longer follow up, the compassionate-use analysis, which involved patients even sicker than those included in bRIGHT, suggested these repairs are durable.
In this retrospective analysis of 38 patients treated at eight centers in Europe, the United States, and Canada, the mortality climbed steadily over 2 years of follow-up, reaching 29% at 2 years despite the fact that TR was reduced to < 1% after the procedure and remained durably suppressed at a median follow-up of 520 days.
The tricuspid valve repair with the EVOQUE system “was associated with a remarkable reduction in heart failure symptoms and significant improvement in NYHA functional class up to a maximum of 1,074 days after the intervention,” reported Lukas Stolz, MD, an interventional cardiologist at Ludwig-Maximilians-University, Munich.
In the data he presented at EuroPCR, which was published simultaneously as a letter in JACC, he said that favorable reverse remodeling of the right ventricle, which was observed as early as 30 days after the procedure, was maintained at long-term follow up.
The uncontrolled data from the compassionate analysis, like the bRIGHT registry, could not confirm that tricuspid valve repair changes the trajectory of progressive heart disease, but the favorable effects Dr. Stolz reported on cardiovascular function, not just symptoms, support this idea.
Dr. Lutz has financial relationships with Edwards Lifesciences, ReCor, and Abbott, which funded the bRIGHT registry. Dr. Karam reports financial relationships with Abbott, Edwards Lifesciences, and Medtronic. Dr. Stolz reports no potential conflicts of interest, but other coinvestigators of the retrospective analysis have financial relationships with Edwards Lifesciences, which is developing the EVOQUE system.
FROM EUROPCR 2023
Evidence of TAVR benefit extends to cardiogenic shock
Early risks outweighed at 1 year
For patients undergoing transcatheter aortic valve replacement (TAVR), adverse outcomes are more common in those who are in cardiogenic shock than those who are not, but the greater risks appear to be completely concentrated in the early period of recovery, suggests a propensity-matched study.
reported Abhijeet Dhoble, MD, associate professor and an interventional cardiologist at McGovern Medical School, University of Texas Health Science Center, Houston.
Their results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
The study, which drew data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement (STS/ACC TVR) Registry, looked only at patients who underwent TAVR with the Sapien3 or Sapience3 Ultra device. Patients with CS were propensity matched to Sapien device-treated patients in the registry without CS.
Taken from a pool of 9,348 patients with CS and 299,600 patients without, the matching included a large array of clinically relevant covariates, including age, gender, prior cardiovascular events, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) class.
After matching, there were 4,952 patients in each arm. The baseline Society of Thoracic Surgeons (STS) risk score was approximately 10.0 in both arms. About half had atrial fibrillation and 90% were in NYHA class III or IV. The median LVEF in both groups was 39.9%.
Mortality more than twofold higher in CS patients
At 30 days, outcomes were worse in patients with CS, including the proportion who died (12.9% vs. 4.9%; P < .0001) and the proportion with stroke (3.3% vs. 1.9%; P < .0001).
The only major study endpoint not significantly different, although higher in the CS group, was the rate of readmission (12.0% vs. 11.0%; P = .25).
At 1 year, the differences in the rates of mortality (29.7% vs. 22.6%; P < .0001) and stroke (4.3% vs. 3.1%; P = .0004) had narrowed modestly but remained highly significant. A closer analysis indicated that almost all of the difference in the rate of events occurred prior to hospital discharge.
In fact, mortality (9.9% vs. 2.7%; P < .0001), stroke (2.9% vs. 1.5%; P < .0001), major vascular complications (2.3% vs. 1.9%; P = .0002), life-threatening bleeding (2.5% vs. 0.7%; P < .0001), new dialysis (3.5% vs. 1.1%; P < .0001) and new onset atrial fibrillation (3.8% vs. 1.6%; P < .0001) were all significantly higher in the CS group in this very early time period. By hazard ratio (HR), the risk of a major event prior to leaving the hospital was nearly threefold higher (HR 2.3; P < .0001) in the CS group.
Yet, there was no significant difference in the accumulation of adverse events after discharge. When compared for major events in the landmark analysis, the event curves were essentially superimposable from 30 days to 1 year. During this period, event rates were 19.3% versus 18.5% for CS and non-CS patients (HR 1.07; P = .2640).
The higher rate of events was unrelated to procedural complications, which were very low in both groups and did not differ significantly. Transition to open surgery, annular disruption, aortic dissection, coronary occlusion, and device embolization occurred in < 1% of patients in both groups.
Predictors of a poor outcome identified
On multivariate analysis, the predictors of events in the CS patients were comorbidities. Despite propensity matching, being on dialysis, having a permanent pacemaker, or having a mechanical assist device were all independent predictors of mortality risk specific to the CS group.
Age and baseline Kansas City Cardiomyopathy Questionnaire (KCCQ) score were not predictors.
These risk factors deserve consideration when evaluating CS candidates for TAVR, but Dr. Dhoble said that none are absolute contraindications. Rather, he advised that they should be considered in the context of the entire clinical picture, including the expected benefit from TAVR. Indeed, the benefit-to-risk ratio generally favors TAVR in CS patients, particularly those with obstructive CS caused by aortic stenosis, according to Dr. Dhoble.
“Efforts should be made not only to avoid delaying TAVR in such patients but also to prevent CS by early definitive treatment of patients with aortic stenosis,” he said.
These data are useful and important, said Jonathan Schwartz, MD, medical director, interventional cardiology, Atrium Health, Charlotte, N.C.
CS candidates for TAVR “are some of the sickest patients we treat. It is nice to finally have some data for this group,” he said. He agreed that CS patients can derive major benefit from TAVR if appropriately selected.
While many CS patients are already considered for TAVR, one source of hesitation has been the exclusion of CS patients from major TAVR trials, said Dr. Dhoble. He hopes these data will provide a framework for clinical decisions.
Ironically, the first TAVR patient and half of the initial series of 38 TAVR patients had CS, noted Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. As the primary investigator of that initial TAVR study, conducted more than 20 years ago, he said he was not surprised by the favorable results of the propensity analysis.
“There is an almost miraculous clinical improvement to be achieved when you succeed with the procedure,” said Dr. Cribier, recounting his own experience. Improvements in LVEF of up to 30% can be achieved “within a day or two or even the first day,” he said.
Dr. Dhoble reports financial relationships with Abbott Vascular and Edwards Lifesciences. Dr. Schwartz reports that he has financial relationships with Abbott Vascular, Boston Scientific, Cordis, Edwards Lifesciences and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences.
Early risks outweighed at 1 year
Early risks outweighed at 1 year
For patients undergoing transcatheter aortic valve replacement (TAVR), adverse outcomes are more common in those who are in cardiogenic shock than those who are not, but the greater risks appear to be completely concentrated in the early period of recovery, suggests a propensity-matched study.
reported Abhijeet Dhoble, MD, associate professor and an interventional cardiologist at McGovern Medical School, University of Texas Health Science Center, Houston.
Their results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
The study, which drew data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement (STS/ACC TVR) Registry, looked only at patients who underwent TAVR with the Sapien3 or Sapience3 Ultra device. Patients with CS were propensity matched to Sapien device-treated patients in the registry without CS.
Taken from a pool of 9,348 patients with CS and 299,600 patients without, the matching included a large array of clinically relevant covariates, including age, gender, prior cardiovascular events, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) class.
After matching, there were 4,952 patients in each arm. The baseline Society of Thoracic Surgeons (STS) risk score was approximately 10.0 in both arms. About half had atrial fibrillation and 90% were in NYHA class III or IV. The median LVEF in both groups was 39.9%.
Mortality more than twofold higher in CS patients
At 30 days, outcomes were worse in patients with CS, including the proportion who died (12.9% vs. 4.9%; P < .0001) and the proportion with stroke (3.3% vs. 1.9%; P < .0001).
The only major study endpoint not significantly different, although higher in the CS group, was the rate of readmission (12.0% vs. 11.0%; P = .25).
At 1 year, the differences in the rates of mortality (29.7% vs. 22.6%; P < .0001) and stroke (4.3% vs. 3.1%; P = .0004) had narrowed modestly but remained highly significant. A closer analysis indicated that almost all of the difference in the rate of events occurred prior to hospital discharge.
In fact, mortality (9.9% vs. 2.7%; P < .0001), stroke (2.9% vs. 1.5%; P < .0001), major vascular complications (2.3% vs. 1.9%; P = .0002), life-threatening bleeding (2.5% vs. 0.7%; P < .0001), new dialysis (3.5% vs. 1.1%; P < .0001) and new onset atrial fibrillation (3.8% vs. 1.6%; P < .0001) were all significantly higher in the CS group in this very early time period. By hazard ratio (HR), the risk of a major event prior to leaving the hospital was nearly threefold higher (HR 2.3; P < .0001) in the CS group.
Yet, there was no significant difference in the accumulation of adverse events after discharge. When compared for major events in the landmark analysis, the event curves were essentially superimposable from 30 days to 1 year. During this period, event rates were 19.3% versus 18.5% for CS and non-CS patients (HR 1.07; P = .2640).
The higher rate of events was unrelated to procedural complications, which were very low in both groups and did not differ significantly. Transition to open surgery, annular disruption, aortic dissection, coronary occlusion, and device embolization occurred in < 1% of patients in both groups.
Predictors of a poor outcome identified
On multivariate analysis, the predictors of events in the CS patients were comorbidities. Despite propensity matching, being on dialysis, having a permanent pacemaker, or having a mechanical assist device were all independent predictors of mortality risk specific to the CS group.
Age and baseline Kansas City Cardiomyopathy Questionnaire (KCCQ) score were not predictors.
These risk factors deserve consideration when evaluating CS candidates for TAVR, but Dr. Dhoble said that none are absolute contraindications. Rather, he advised that they should be considered in the context of the entire clinical picture, including the expected benefit from TAVR. Indeed, the benefit-to-risk ratio generally favors TAVR in CS patients, particularly those with obstructive CS caused by aortic stenosis, according to Dr. Dhoble.
“Efforts should be made not only to avoid delaying TAVR in such patients but also to prevent CS by early definitive treatment of patients with aortic stenosis,” he said.
These data are useful and important, said Jonathan Schwartz, MD, medical director, interventional cardiology, Atrium Health, Charlotte, N.C.
CS candidates for TAVR “are some of the sickest patients we treat. It is nice to finally have some data for this group,” he said. He agreed that CS patients can derive major benefit from TAVR if appropriately selected.
While many CS patients are already considered for TAVR, one source of hesitation has been the exclusion of CS patients from major TAVR trials, said Dr. Dhoble. He hopes these data will provide a framework for clinical decisions.
Ironically, the first TAVR patient and half of the initial series of 38 TAVR patients had CS, noted Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. As the primary investigator of that initial TAVR study, conducted more than 20 years ago, he said he was not surprised by the favorable results of the propensity analysis.
“There is an almost miraculous clinical improvement to be achieved when you succeed with the procedure,” said Dr. Cribier, recounting his own experience. Improvements in LVEF of up to 30% can be achieved “within a day or two or even the first day,” he said.
Dr. Dhoble reports financial relationships with Abbott Vascular and Edwards Lifesciences. Dr. Schwartz reports that he has financial relationships with Abbott Vascular, Boston Scientific, Cordis, Edwards Lifesciences and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences.
For patients undergoing transcatheter aortic valve replacement (TAVR), adverse outcomes are more common in those who are in cardiogenic shock than those who are not, but the greater risks appear to be completely concentrated in the early period of recovery, suggests a propensity-matched study.
reported Abhijeet Dhoble, MD, associate professor and an interventional cardiologist at McGovern Medical School, University of Texas Health Science Center, Houston.
Their results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
The study, which drew data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement (STS/ACC TVR) Registry, looked only at patients who underwent TAVR with the Sapien3 or Sapience3 Ultra device. Patients with CS were propensity matched to Sapien device-treated patients in the registry without CS.
Taken from a pool of 9,348 patients with CS and 299,600 patients without, the matching included a large array of clinically relevant covariates, including age, gender, prior cardiovascular events, left ventricular ejection fraction (LVEF), and New York Heart Association (NYHA) class.
After matching, there were 4,952 patients in each arm. The baseline Society of Thoracic Surgeons (STS) risk score was approximately 10.0 in both arms. About half had atrial fibrillation and 90% were in NYHA class III or IV. The median LVEF in both groups was 39.9%.
Mortality more than twofold higher in CS patients
At 30 days, outcomes were worse in patients with CS, including the proportion who died (12.9% vs. 4.9%; P < .0001) and the proportion with stroke (3.3% vs. 1.9%; P < .0001).
The only major study endpoint not significantly different, although higher in the CS group, was the rate of readmission (12.0% vs. 11.0%; P = .25).
At 1 year, the differences in the rates of mortality (29.7% vs. 22.6%; P < .0001) and stroke (4.3% vs. 3.1%; P = .0004) had narrowed modestly but remained highly significant. A closer analysis indicated that almost all of the difference in the rate of events occurred prior to hospital discharge.
In fact, mortality (9.9% vs. 2.7%; P < .0001), stroke (2.9% vs. 1.5%; P < .0001), major vascular complications (2.3% vs. 1.9%; P = .0002), life-threatening bleeding (2.5% vs. 0.7%; P < .0001), new dialysis (3.5% vs. 1.1%; P < .0001) and new onset atrial fibrillation (3.8% vs. 1.6%; P < .0001) were all significantly higher in the CS group in this very early time period. By hazard ratio (HR), the risk of a major event prior to leaving the hospital was nearly threefold higher (HR 2.3; P < .0001) in the CS group.
Yet, there was no significant difference in the accumulation of adverse events after discharge. When compared for major events in the landmark analysis, the event curves were essentially superimposable from 30 days to 1 year. During this period, event rates were 19.3% versus 18.5% for CS and non-CS patients (HR 1.07; P = .2640).
The higher rate of events was unrelated to procedural complications, which were very low in both groups and did not differ significantly. Transition to open surgery, annular disruption, aortic dissection, coronary occlusion, and device embolization occurred in < 1% of patients in both groups.
Predictors of a poor outcome identified
On multivariate analysis, the predictors of events in the CS patients were comorbidities. Despite propensity matching, being on dialysis, having a permanent pacemaker, or having a mechanical assist device were all independent predictors of mortality risk specific to the CS group.
Age and baseline Kansas City Cardiomyopathy Questionnaire (KCCQ) score were not predictors.
These risk factors deserve consideration when evaluating CS candidates for TAVR, but Dr. Dhoble said that none are absolute contraindications. Rather, he advised that they should be considered in the context of the entire clinical picture, including the expected benefit from TAVR. Indeed, the benefit-to-risk ratio generally favors TAVR in CS patients, particularly those with obstructive CS caused by aortic stenosis, according to Dr. Dhoble.
“Efforts should be made not only to avoid delaying TAVR in such patients but also to prevent CS by early definitive treatment of patients with aortic stenosis,” he said.
These data are useful and important, said Jonathan Schwartz, MD, medical director, interventional cardiology, Atrium Health, Charlotte, N.C.
CS candidates for TAVR “are some of the sickest patients we treat. It is nice to finally have some data for this group,” he said. He agreed that CS patients can derive major benefit from TAVR if appropriately selected.
While many CS patients are already considered for TAVR, one source of hesitation has been the exclusion of CS patients from major TAVR trials, said Dr. Dhoble. He hopes these data will provide a framework for clinical decisions.
Ironically, the first TAVR patient and half of the initial series of 38 TAVR patients had CS, noted Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. As the primary investigator of that initial TAVR study, conducted more than 20 years ago, he said he was not surprised by the favorable results of the propensity analysis.
“There is an almost miraculous clinical improvement to be achieved when you succeed with the procedure,” said Dr. Cribier, recounting his own experience. Improvements in LVEF of up to 30% can be achieved “within a day or two or even the first day,” he said.
Dr. Dhoble reports financial relationships with Abbott Vascular and Edwards Lifesciences. Dr. Schwartz reports that he has financial relationships with Abbott Vascular, Boston Scientific, Cordis, Edwards Lifesciences and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences.
FROM EUROPCR 2023
Redo-TAVR in U.S. database yields good news: Outcomes rival first intervention
Data support redo if needed.
Even after 3 years of follow-up, redo transcatheter aortic valve replacement (TAVR) performs about as well as the first procedure, whether compared for hard endpoints, such as death and stroke, or for softer endpoints, such as function and quality of life, new registry data suggest.
reported Rajendra Makkar, MD, associate director, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
The results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
Data for this analysis were drawn from 348,338 TAVR procedures with the Edwards balloon-expandable valves in the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement Registry.
Of these, 1,216 were redo procedures. In 475 of the cases, the redo was performed in a patient whose first procedure was with an Edwards device. In the remaining 741 cases, the Edwards device replaced a different prosthetic heart valve. The median time to the redo from the first procedure was 26 months.
For the analysis, the redo-TAVRs were compared with native TAVR patients through 1:1 propensity matching employing 35 covariates, such as age, body mass index (BMI), baseline comorbidities, prior cardiovascular procedures, valve size, and Society of Thoracic Surgeons risk score.
Low death and stroke rates following TAVR redos
The rates of all-cause death or stroke within hospital (4.7% vs. 3.9%; P = .32) and at 30 days (6.1% vs. 5.9%; P = .77) were numerically but not statistically higher in the redo group.
At 1 year, the rates of death (17.3% vs. 17.7%; P = .961) and stroke (3.3% vs. 3.5%; P = .982) were numerically but not significantly lower among those who underwent a redo procedure.
The secondary endpoints told the same story. The one exception was the higher aortic valve reintervention rate (0.61% vs. 0.09%; P = .03) at 30 days in the redo group. This did reach statistical significance, but Dr. Makkar pointed out rates were very low regardless. The rates climbed in both groups by 1 year (1.09% vs. 0.21%; P = .01).
No other secondary endpoints differed significantly at 30 days or at 1 year. Even though some were numerically higher after redo at 1 year, such as major vascular complications (1.25 vs. 1.60; P = .51), others were lower, such as new-start dialysis (1.62 vs. 0.98; P = .26). All-cause readmission rates at 1 year were nearly identical (32.56% vs. 32.23%; P = .82).
Consistent with the comparable outcomes on the hard endpoints, major and similar improvements were seen in both the redo and the propensity-matched native TAVR patients on the Kansas City Cardiomyopathy Questionnaire Overall Summary. The slight advantage for the redo group was not significant at 30 days, but the degree of improvement was greater after the redo than after native TAVR at 1 year (15% vs. 10%; P = .03).
“You bring good news,” said Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. Widely regarded as the father of TAVR for his first-in-human series in 2002, Dr. Cribier said that there are several reassuring take-home messages from this study.
“First, these data tell us that the redo rate is extremely low,” he said, noting that the registry data suggests a risk well below 1%. “Second, we are seeing from this data that there are no more complications [than TAVR in a native valve] if you need to do this.”
Redo patients are generally sicker
The propensity matching was designed to eliminate baseline differences for the outcome comparisons, but Dr. Makkar did point out that redo-TAVR patients were sicker than the native TAVR patients. For example, when compared prior to propensity matching, the STS score was higher (8.3 vs. 5.2; P < .01), more patients had atrial fibrillation (47.9% vs. 36.2%; P < .01), and more patients had a prior stroke (15.0% vs. 10.7%; P < .01).
The registry only has follow-up out to 1 year, but participating patients were matched to a claims database to capture outcomes out to 3 years. Mortality rates at long-term follow-up were not significantly different for redo vs. native TAVR (42.2% vs. 40.3% respectively; P = .98); for the entire dataset or when compared in subgroups defined by Edwards valve redo of an Edwards valve (P = .909) or an Edwards valve redo of a non-Edwards device (P = .871).
Whether an early redo, defined as 12 months after the index TAVR procedure, or a late redo, the rate of mortality ranged from approximately 16% to 18% with no significant difference between redo and native TAVR.
A moderator for the late-breaking trials session where these data were presented, Darren Mylotte, MD, a consultant in cardiology for the Galway University Hospitals, Ireland, challenged Dr. Makkar about the potential for selection bias. He said redo patients might be the ones that interventionalists feel confident about helping, making this comparison unrepresentative.
“I think that the selection bias is likely to cut both ways,” Dr. Makkar replied. For many patients with a failed TAVR, he explained that clinicians might think, “There is nothing to be done for this patient except to try a redo.”
Dr. Makkar reports financial relationships with Abbott, Cordis, Edwards Lifesciences, and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences. Dr. Mylotte reports no potential conflicts of interest.
Data support redo if needed.
Data support redo if needed.
Even after 3 years of follow-up, redo transcatheter aortic valve replacement (TAVR) performs about as well as the first procedure, whether compared for hard endpoints, such as death and stroke, or for softer endpoints, such as function and quality of life, new registry data suggest.
reported Rajendra Makkar, MD, associate director, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
The results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
Data for this analysis were drawn from 348,338 TAVR procedures with the Edwards balloon-expandable valves in the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement Registry.
Of these, 1,216 were redo procedures. In 475 of the cases, the redo was performed in a patient whose first procedure was with an Edwards device. In the remaining 741 cases, the Edwards device replaced a different prosthetic heart valve. The median time to the redo from the first procedure was 26 months.
For the analysis, the redo-TAVRs were compared with native TAVR patients through 1:1 propensity matching employing 35 covariates, such as age, body mass index (BMI), baseline comorbidities, prior cardiovascular procedures, valve size, and Society of Thoracic Surgeons risk score.
Low death and stroke rates following TAVR redos
The rates of all-cause death or stroke within hospital (4.7% vs. 3.9%; P = .32) and at 30 days (6.1% vs. 5.9%; P = .77) were numerically but not statistically higher in the redo group.
At 1 year, the rates of death (17.3% vs. 17.7%; P = .961) and stroke (3.3% vs. 3.5%; P = .982) were numerically but not significantly lower among those who underwent a redo procedure.
The secondary endpoints told the same story. The one exception was the higher aortic valve reintervention rate (0.61% vs. 0.09%; P = .03) at 30 days in the redo group. This did reach statistical significance, but Dr. Makkar pointed out rates were very low regardless. The rates climbed in both groups by 1 year (1.09% vs. 0.21%; P = .01).
No other secondary endpoints differed significantly at 30 days or at 1 year. Even though some were numerically higher after redo at 1 year, such as major vascular complications (1.25 vs. 1.60; P = .51), others were lower, such as new-start dialysis (1.62 vs. 0.98; P = .26). All-cause readmission rates at 1 year were nearly identical (32.56% vs. 32.23%; P = .82).
Consistent with the comparable outcomes on the hard endpoints, major and similar improvements were seen in both the redo and the propensity-matched native TAVR patients on the Kansas City Cardiomyopathy Questionnaire Overall Summary. The slight advantage for the redo group was not significant at 30 days, but the degree of improvement was greater after the redo than after native TAVR at 1 year (15% vs. 10%; P = .03).
“You bring good news,” said Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. Widely regarded as the father of TAVR for his first-in-human series in 2002, Dr. Cribier said that there are several reassuring take-home messages from this study.
“First, these data tell us that the redo rate is extremely low,” he said, noting that the registry data suggests a risk well below 1%. “Second, we are seeing from this data that there are no more complications [than TAVR in a native valve] if you need to do this.”
Redo patients are generally sicker
The propensity matching was designed to eliminate baseline differences for the outcome comparisons, but Dr. Makkar did point out that redo-TAVR patients were sicker than the native TAVR patients. For example, when compared prior to propensity matching, the STS score was higher (8.3 vs. 5.2; P < .01), more patients had atrial fibrillation (47.9% vs. 36.2%; P < .01), and more patients had a prior stroke (15.0% vs. 10.7%; P < .01).
The registry only has follow-up out to 1 year, but participating patients were matched to a claims database to capture outcomes out to 3 years. Mortality rates at long-term follow-up were not significantly different for redo vs. native TAVR (42.2% vs. 40.3% respectively; P = .98); for the entire dataset or when compared in subgroups defined by Edwards valve redo of an Edwards valve (P = .909) or an Edwards valve redo of a non-Edwards device (P = .871).
Whether an early redo, defined as 12 months after the index TAVR procedure, or a late redo, the rate of mortality ranged from approximately 16% to 18% with no significant difference between redo and native TAVR.
A moderator for the late-breaking trials session where these data were presented, Darren Mylotte, MD, a consultant in cardiology for the Galway University Hospitals, Ireland, challenged Dr. Makkar about the potential for selection bias. He said redo patients might be the ones that interventionalists feel confident about helping, making this comparison unrepresentative.
“I think that the selection bias is likely to cut both ways,” Dr. Makkar replied. For many patients with a failed TAVR, he explained that clinicians might think, “There is nothing to be done for this patient except to try a redo.”
Dr. Makkar reports financial relationships with Abbott, Cordis, Edwards Lifesciences, and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences. Dr. Mylotte reports no potential conflicts of interest.
Even after 3 years of follow-up, redo transcatheter aortic valve replacement (TAVR) performs about as well as the first procedure, whether compared for hard endpoints, such as death and stroke, or for softer endpoints, such as function and quality of life, new registry data suggest.
reported Rajendra Makkar, MD, associate director, Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles.
The results were presented at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
Data for this analysis were drawn from 348,338 TAVR procedures with the Edwards balloon-expandable valves in the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Replacement Registry.
Of these, 1,216 were redo procedures. In 475 of the cases, the redo was performed in a patient whose first procedure was with an Edwards device. In the remaining 741 cases, the Edwards device replaced a different prosthetic heart valve. The median time to the redo from the first procedure was 26 months.
For the analysis, the redo-TAVRs were compared with native TAVR patients through 1:1 propensity matching employing 35 covariates, such as age, body mass index (BMI), baseline comorbidities, prior cardiovascular procedures, valve size, and Society of Thoracic Surgeons risk score.
Low death and stroke rates following TAVR redos
The rates of all-cause death or stroke within hospital (4.7% vs. 3.9%; P = .32) and at 30 days (6.1% vs. 5.9%; P = .77) were numerically but not statistically higher in the redo group.
At 1 year, the rates of death (17.3% vs. 17.7%; P = .961) and stroke (3.3% vs. 3.5%; P = .982) were numerically but not significantly lower among those who underwent a redo procedure.
The secondary endpoints told the same story. The one exception was the higher aortic valve reintervention rate (0.61% vs. 0.09%; P = .03) at 30 days in the redo group. This did reach statistical significance, but Dr. Makkar pointed out rates were very low regardless. The rates climbed in both groups by 1 year (1.09% vs. 0.21%; P = .01).
No other secondary endpoints differed significantly at 30 days or at 1 year. Even though some were numerically higher after redo at 1 year, such as major vascular complications (1.25 vs. 1.60; P = .51), others were lower, such as new-start dialysis (1.62 vs. 0.98; P = .26). All-cause readmission rates at 1 year were nearly identical (32.56% vs. 32.23%; P = .82).
Consistent with the comparable outcomes on the hard endpoints, major and similar improvements were seen in both the redo and the propensity-matched native TAVR patients on the Kansas City Cardiomyopathy Questionnaire Overall Summary. The slight advantage for the redo group was not significant at 30 days, but the degree of improvement was greater after the redo than after native TAVR at 1 year (15% vs. 10%; P = .03).
“You bring good news,” said Alain G. Cribier, MD, director of cardiology, Charles Nicolle Hospital, University of Rouen, France. Widely regarded as the father of TAVR for his first-in-human series in 2002, Dr. Cribier said that there are several reassuring take-home messages from this study.
“First, these data tell us that the redo rate is extremely low,” he said, noting that the registry data suggests a risk well below 1%. “Second, we are seeing from this data that there are no more complications [than TAVR in a native valve] if you need to do this.”
Redo patients are generally sicker
The propensity matching was designed to eliminate baseline differences for the outcome comparisons, but Dr. Makkar did point out that redo-TAVR patients were sicker than the native TAVR patients. For example, when compared prior to propensity matching, the STS score was higher (8.3 vs. 5.2; P < .01), more patients had atrial fibrillation (47.9% vs. 36.2%; P < .01), and more patients had a prior stroke (15.0% vs. 10.7%; P < .01).
The registry only has follow-up out to 1 year, but participating patients were matched to a claims database to capture outcomes out to 3 years. Mortality rates at long-term follow-up were not significantly different for redo vs. native TAVR (42.2% vs. 40.3% respectively; P = .98); for the entire dataset or when compared in subgroups defined by Edwards valve redo of an Edwards valve (P = .909) or an Edwards valve redo of a non-Edwards device (P = .871).
Whether an early redo, defined as 12 months after the index TAVR procedure, or a late redo, the rate of mortality ranged from approximately 16% to 18% with no significant difference between redo and native TAVR.
A moderator for the late-breaking trials session where these data were presented, Darren Mylotte, MD, a consultant in cardiology for the Galway University Hospitals, Ireland, challenged Dr. Makkar about the potential for selection bias. He said redo patients might be the ones that interventionalists feel confident about helping, making this comparison unrepresentative.
“I think that the selection bias is likely to cut both ways,” Dr. Makkar replied. For many patients with a failed TAVR, he explained that clinicians might think, “There is nothing to be done for this patient except to try a redo.”
Dr. Makkar reports financial relationships with Abbott, Cordis, Edwards Lifesciences, and Medtronic. Dr. Cribier reports a financial relationship with Edwards Lifesciences. Dr. Mylotte reports no potential conflicts of interest.
FROM EUROPCR 2023
A call to revamp revascularization trial endpoints
The time has come to rethink the conventional primary endpoints investigators use in coronary revascularization trials – a composite of major adverse cardiovascular events (MACE), death or MI, and other endpoints – and shift toward greater emphasis on quality of life, two clinical trial investigators say.
Gregg Stone, MD, and Mario Gaudino, MD, MSCE, PhD, made their case in the Journal of the American College of Cardiology, writing: “The classic academic exercise of comparing revascularization modalities in an elusive search for a clear ‘winner’ has failed.” Dr. Stone was the principal investigator of the landmark EXCEL trial and an investigator for the ISCHEMIA trial, the latter of which Dr. Gaudino was also an investigator. Both trials evaluated percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) as treatments for coronary artery disease.
In an interview, Dr. Stone, a cardiologist at the Icahn School of Medicine at Mount Sinai, New York, said: “We’re proposing a new endpoint called a composite endpoint measured in a hierarchical fashion of death or quality of life [QOL].” Dr. Gaudino is a cardiac surgeon at Weill Cornell Medicine, New York.
Quality of life as a validation tool
As a measure of revascularization after PCI or CABG, Dr. Stone said, QOL is ready for prime time. “Over the last 20 years there’s been a very rich literature of science developed linking certain quality of life instruments to improved outcomes, in particularly health but also heart failure.”
Those instruments include the Seattle Angina Questionnaire, the Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy questionnaire. “All of these are sufficiently validated that the [Food and Drug Administration] considers them ‘validated tools’ for use in clinical trials.” Dr. Stone also noted that substudies of three landmark trials comparing PCI and CABG – EXCEL, SYNTAX, and FREEDOM – used those instruments to evaluate QOL as an endpoint alongside “hard” outcomes such as death, MI or stroke. “So quality of life already is being used and it is already widely accepted. What we’re saying is, when you think about the information you need for medical studies, we believe it’s time to elevate that from secondary supportive information to primary.”
He and Dr. Gaudino are putting their money where their mouths are. They’ve applied for a grant through the Patient-Centered Outcomes Research Institute to use QOL as an outcomes measure in a trial of revascularization strategies in women and minority patients.
Shortcomings with traditional endpoints
Dr. Stone explained some of the shortcomings with the traditional endpoints revascularization studies have used. “Everybody agrees that mortality or survival is the most important endpoint, but studies can never be large enough to be powered for that. So we always end up combining them with myocardial infarction, stroke, and often with repeat revascularization” into one MACE endpoint.
But those four types of events are “very, very different,” Dr. Stone said. The severity of MIs and strokes can range from minor, almost inconsequential events to major, debilitating events. “Some strokes resolve in a few days but we count them all the same.”
He ticked off a list of the other outcomes the traditional endpoints don’t account for: atrial fibrillation, kidney dysfunction, musculoskeletal disorders, depression, cognitive changes, and vascular complications. They all can all have a significant impact on a patient’s QOL, Dr. Stone said.
“We’ve now entered an era that is much more patient centered,” Dr. Stone said. “My goal as a physician is to try to impart my knowledge of the evidence that’s out there so that the patient can make the decision that gives them the best chance of meeting their life goals and objectives. When you ask patients what they want, they all want to live longer and they want to live better.”
MACE as a composite endpoint has its shortcomings, but using QOL can also be fraught with problems, said Suzanne Baron, MD, director of interventional cardiology research at Massachusetts General Hospital, Boston.
With regards to MACE, she echoed some of Dr. Stone’s concerns. “Patients and clinicians likely would not consider a repeat stenting procedure to be the same as having a stroke, and so weighting these two outcomes equally within a composite endpoint can potentially result in a skewed trial conclusion.”
One potential issue with QOL as an endpoint is that it can vary from day to day. “If quality of life is only measured at a few time points, such as annually, it is possible that those measurements may only reflect a small portion of the patient’s overall quality of life,” she said. “Accordingly, I think that it will be important to incorporate frequent assessments of a patient’s quality of life if these measures will be used as a primary endpoint in cardiac revascularization trials.”
And, in a cost-conscious health care system, quantity (length) of life tends to carry more weight than QOL, she said. “So it will be important that a trial using quality-of-life improvement as a primary endpoint mandates that the degree of improvement be large enough to ensure that the treatment remains high-value from a health economics standpoint.”
Dr. Stone disclosed financial relationships with numerous pharmaceutical companies. Dr. Baron reported financial relationships with Abiomed, Acarix, Boston Scientific, Medtronic, Zoll Medical, Biotronik, Edwards Lifesciences, and Janssen.
The time has come to rethink the conventional primary endpoints investigators use in coronary revascularization trials – a composite of major adverse cardiovascular events (MACE), death or MI, and other endpoints – and shift toward greater emphasis on quality of life, two clinical trial investigators say.
Gregg Stone, MD, and Mario Gaudino, MD, MSCE, PhD, made their case in the Journal of the American College of Cardiology, writing: “The classic academic exercise of comparing revascularization modalities in an elusive search for a clear ‘winner’ has failed.” Dr. Stone was the principal investigator of the landmark EXCEL trial and an investigator for the ISCHEMIA trial, the latter of which Dr. Gaudino was also an investigator. Both trials evaluated percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) as treatments for coronary artery disease.
In an interview, Dr. Stone, a cardiologist at the Icahn School of Medicine at Mount Sinai, New York, said: “We’re proposing a new endpoint called a composite endpoint measured in a hierarchical fashion of death or quality of life [QOL].” Dr. Gaudino is a cardiac surgeon at Weill Cornell Medicine, New York.
Quality of life as a validation tool
As a measure of revascularization after PCI or CABG, Dr. Stone said, QOL is ready for prime time. “Over the last 20 years there’s been a very rich literature of science developed linking certain quality of life instruments to improved outcomes, in particularly health but also heart failure.”
Those instruments include the Seattle Angina Questionnaire, the Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy questionnaire. “All of these are sufficiently validated that the [Food and Drug Administration] considers them ‘validated tools’ for use in clinical trials.” Dr. Stone also noted that substudies of three landmark trials comparing PCI and CABG – EXCEL, SYNTAX, and FREEDOM – used those instruments to evaluate QOL as an endpoint alongside “hard” outcomes such as death, MI or stroke. “So quality of life already is being used and it is already widely accepted. What we’re saying is, when you think about the information you need for medical studies, we believe it’s time to elevate that from secondary supportive information to primary.”
He and Dr. Gaudino are putting their money where their mouths are. They’ve applied for a grant through the Patient-Centered Outcomes Research Institute to use QOL as an outcomes measure in a trial of revascularization strategies in women and minority patients.
Shortcomings with traditional endpoints
Dr. Stone explained some of the shortcomings with the traditional endpoints revascularization studies have used. “Everybody agrees that mortality or survival is the most important endpoint, but studies can never be large enough to be powered for that. So we always end up combining them with myocardial infarction, stroke, and often with repeat revascularization” into one MACE endpoint.
But those four types of events are “very, very different,” Dr. Stone said. The severity of MIs and strokes can range from minor, almost inconsequential events to major, debilitating events. “Some strokes resolve in a few days but we count them all the same.”
He ticked off a list of the other outcomes the traditional endpoints don’t account for: atrial fibrillation, kidney dysfunction, musculoskeletal disorders, depression, cognitive changes, and vascular complications. They all can all have a significant impact on a patient’s QOL, Dr. Stone said.
“We’ve now entered an era that is much more patient centered,” Dr. Stone said. “My goal as a physician is to try to impart my knowledge of the evidence that’s out there so that the patient can make the decision that gives them the best chance of meeting their life goals and objectives. When you ask patients what they want, they all want to live longer and they want to live better.”
MACE as a composite endpoint has its shortcomings, but using QOL can also be fraught with problems, said Suzanne Baron, MD, director of interventional cardiology research at Massachusetts General Hospital, Boston.
With regards to MACE, she echoed some of Dr. Stone’s concerns. “Patients and clinicians likely would not consider a repeat stenting procedure to be the same as having a stroke, and so weighting these two outcomes equally within a composite endpoint can potentially result in a skewed trial conclusion.”
One potential issue with QOL as an endpoint is that it can vary from day to day. “If quality of life is only measured at a few time points, such as annually, it is possible that those measurements may only reflect a small portion of the patient’s overall quality of life,” she said. “Accordingly, I think that it will be important to incorporate frequent assessments of a patient’s quality of life if these measures will be used as a primary endpoint in cardiac revascularization trials.”
And, in a cost-conscious health care system, quantity (length) of life tends to carry more weight than QOL, she said. “So it will be important that a trial using quality-of-life improvement as a primary endpoint mandates that the degree of improvement be large enough to ensure that the treatment remains high-value from a health economics standpoint.”
Dr. Stone disclosed financial relationships with numerous pharmaceutical companies. Dr. Baron reported financial relationships with Abiomed, Acarix, Boston Scientific, Medtronic, Zoll Medical, Biotronik, Edwards Lifesciences, and Janssen.
The time has come to rethink the conventional primary endpoints investigators use in coronary revascularization trials – a composite of major adverse cardiovascular events (MACE), death or MI, and other endpoints – and shift toward greater emphasis on quality of life, two clinical trial investigators say.
Gregg Stone, MD, and Mario Gaudino, MD, MSCE, PhD, made their case in the Journal of the American College of Cardiology, writing: “The classic academic exercise of comparing revascularization modalities in an elusive search for a clear ‘winner’ has failed.” Dr. Stone was the principal investigator of the landmark EXCEL trial and an investigator for the ISCHEMIA trial, the latter of which Dr. Gaudino was also an investigator. Both trials evaluated percutaneous coronary intervention (PCI) and coronary artery bypass surgery (CABG) as treatments for coronary artery disease.
In an interview, Dr. Stone, a cardiologist at the Icahn School of Medicine at Mount Sinai, New York, said: “We’re proposing a new endpoint called a composite endpoint measured in a hierarchical fashion of death or quality of life [QOL].” Dr. Gaudino is a cardiac surgeon at Weill Cornell Medicine, New York.
Quality of life as a validation tool
As a measure of revascularization after PCI or CABG, Dr. Stone said, QOL is ready for prime time. “Over the last 20 years there’s been a very rich literature of science developed linking certain quality of life instruments to improved outcomes, in particularly health but also heart failure.”
Those instruments include the Seattle Angina Questionnaire, the Minnesota Living with Heart Failure Questionnaire and the Kansas City Cardiomyopathy questionnaire. “All of these are sufficiently validated that the [Food and Drug Administration] considers them ‘validated tools’ for use in clinical trials.” Dr. Stone also noted that substudies of three landmark trials comparing PCI and CABG – EXCEL, SYNTAX, and FREEDOM – used those instruments to evaluate QOL as an endpoint alongside “hard” outcomes such as death, MI or stroke. “So quality of life already is being used and it is already widely accepted. What we’re saying is, when you think about the information you need for medical studies, we believe it’s time to elevate that from secondary supportive information to primary.”
He and Dr. Gaudino are putting their money where their mouths are. They’ve applied for a grant through the Patient-Centered Outcomes Research Institute to use QOL as an outcomes measure in a trial of revascularization strategies in women and minority patients.
Shortcomings with traditional endpoints
Dr. Stone explained some of the shortcomings with the traditional endpoints revascularization studies have used. “Everybody agrees that mortality or survival is the most important endpoint, but studies can never be large enough to be powered for that. So we always end up combining them with myocardial infarction, stroke, and often with repeat revascularization” into one MACE endpoint.
But those four types of events are “very, very different,” Dr. Stone said. The severity of MIs and strokes can range from minor, almost inconsequential events to major, debilitating events. “Some strokes resolve in a few days but we count them all the same.”
He ticked off a list of the other outcomes the traditional endpoints don’t account for: atrial fibrillation, kidney dysfunction, musculoskeletal disorders, depression, cognitive changes, and vascular complications. They all can all have a significant impact on a patient’s QOL, Dr. Stone said.
“We’ve now entered an era that is much more patient centered,” Dr. Stone said. “My goal as a physician is to try to impart my knowledge of the evidence that’s out there so that the patient can make the decision that gives them the best chance of meeting their life goals and objectives. When you ask patients what they want, they all want to live longer and they want to live better.”
MACE as a composite endpoint has its shortcomings, but using QOL can also be fraught with problems, said Suzanne Baron, MD, director of interventional cardiology research at Massachusetts General Hospital, Boston.
With regards to MACE, she echoed some of Dr. Stone’s concerns. “Patients and clinicians likely would not consider a repeat stenting procedure to be the same as having a stroke, and so weighting these two outcomes equally within a composite endpoint can potentially result in a skewed trial conclusion.”
One potential issue with QOL as an endpoint is that it can vary from day to day. “If quality of life is only measured at a few time points, such as annually, it is possible that those measurements may only reflect a small portion of the patient’s overall quality of life,” she said. “Accordingly, I think that it will be important to incorporate frequent assessments of a patient’s quality of life if these measures will be used as a primary endpoint in cardiac revascularization trials.”
And, in a cost-conscious health care system, quantity (length) of life tends to carry more weight than QOL, she said. “So it will be important that a trial using quality-of-life improvement as a primary endpoint mandates that the degree of improvement be large enough to ensure that the treatment remains high-value from a health economics standpoint.”
Dr. Stone disclosed financial relationships with numerous pharmaceutical companies. Dr. Baron reported financial relationships with Abiomed, Acarix, Boston Scientific, Medtronic, Zoll Medical, Biotronik, Edwards Lifesciences, and Janssen.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
LAA closure outcomes improve with CCTA: Swiss-Apero subanalysis
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
The largest multicenter randomized trial to date of CT angiography before left atrial appendage closure (LAAC) to treat atrial fibrillation has added to the evidence that the imaging technique on top of transesophageal echocardiography achieves a higher degree of short- and long-term success than TEE alone.
The results are from a subanalysis of the Swiss-Apero trial, a randomized comparative trial of the Watchman and Amulet devices for LAAC, which published results in Circulation.
“Our observational data support to use of CT for LAAC procedure planning,” senior investigator Lorenz Räber, MD, PhD, said in an interview. “This is not very surprising given the high variability of the LAA anatomy and the associated complexity of the procedure.” Dr. Räber is director of the catheterization laboratory at Inselspital, Bern (Switzerland) University Hospital.
The study, published online in JACC: Cardiovascular Interventions, included 219 LAAC procedures in which the operators performed coronary CT angiography (CTTA) beforehand. When the investigators designed the study, LAAC procedures were typically planned using TEE alone, and so participating operators were blinded to preprocedural CCTA imaging. Soon after the study launch, European cardiology societies issued a consensus statement that included CCTA as an option for procedure planning. So the Swiss-Apero investigators changed the subanalysis protocol to unblind the operators – that is, they were permitted to plan LAAC procedures with CCTA imaging in addition to TEE. In this subanalysis, most patients had implantation with blinding to CCTA (57.9% vs. 41.2%).
Study results
The subanalysis determined that operator unblinding to preprocedural CCTA resulted in better success with LAAC, both in the short term, at 93.5% vs. 81.1% (P = .009; adjusted odds ratio, 2.76; 95% confidence interval, 1.05-7.29; P = .40) and the long term, at 83.7% vs. 72.4% (P = .050; aOR, 2.12; 95% CI, 1.03-4.35; P = .041).
Dr. Räber noted that this is only the third study to date that examined the potential impact of preprocedural CCTA plus TEE. One was a small study of 24 consecutive LAAC procedures with the Watchman device that compared TEE alone and CCTA plus TEE, finding better outcomes in the group that had both imaging modalities . A larger, single-center cohort study of 485 LAAC Watchman procedures found that CCTA resulted in faster operation times and higher successful device implantation rates, but no significant difference in procedural complications.
Dr. Räber explained why his group’s subanalysis may have found a clinical benefit with CCTA on top of TEE. “Our study was much larger, as compared to the randomized clinical trial, and there was no selection bias as in the second study mentioned before, as operators did not have the option to decide whether or not to assess the CCTA prior to the procedure,” he said. “Finally, in the previous studies there was no random allocation of device type” – that is, Amulet versus Watchman.
One study limitation Dr. Räber noted was that significantly more patients in the blinded group were discharged with dual-antiplatelet therapy. “The lower rate of procedure complications observed in unblinded procedures was mostly driven by a lower number of major bleedings and in particular of pericardial tamponade,” he said. “We cannot therefore exclude that the higher percentage of patients under dual-antiplatelet therapy in the CCTA-blinded group might have favored this difference.”
However, he noted the investigators corrected their analysis to account for differences between the groups. “Importantly, the numerical excess in major procedural bleeding was observed within both the single-antiplatelet therapy and dual-antiplatelet therapy subgroups of the TEE-only group.”
In an accompanying editorial, coauthors Brian O’Neill, MD, and Dee Dee Wang, MD, both with the Center for Structural Heard Disease at Henry Ford Hospital in Detroit, noted that the Swiss-Apero subanalysis “reinforced” the benefit of CCTA before LAAC.
“This study demonstrated, for the first time, improved short- and long-term procedural success using CT in addition to TEE for left atrial appendage occlusion,” Dr. O’Neill said in an interview. “This particular study may serve as a guide to an adequately powered randomized trial of CT versus TEE in left atrial appendage occlusion.” Future LAAC trials should incorporate preprocedural CCTA.
Dr. O’Neill noted that, as a subanalysis of a randomized trial, the “results are hypothesis generating.” However, he added, “the results are in line with several previous studies of CT versus TEE in left atrial appendage occlusion.”
Dr Räber disclosed financial relationships with Abbott Vascular, Boston Scientific, Biotronik, Infraredx, Heartflow, Sanofi, Regeneron, Amgen, AstraZeneca, CSL Behring, Canon, Occlutech, and Vifor. Dr. O’Neill disclosed financial relationships with Edwards Lifesciences, Medtronic, and Abbott Vascular.
FROM JACC: CARDIOVASCULAR INTERVENTIONS
Novel strategy could improve heart transplant allocation
Prediction models that incorporate more than just treatment status could rank order heart transplant candidates by urgency more effectively than the current system, a modeling study suggests.
Since 2018, the U.S. heart transplant allocation system has ranked heart candidates according to six treatment-based “statuses” (up from three used previously), ignoring many objective patient characteristics, the authors write.
Their study showed no significant difference in survival between statuses four and six, and status five had lower survival than status four.
“We expected multivariable prediction models to outperform the six-status system when it comes to rank ordering patients by how likely they are to die on the wait list (medical urgency),” William F. Parker, MD, MS, PhD, of the University of Chicago, told this news organization.
“However, we were surprised to see that the statuses were out of order,” he said. “Status five patients are more urgent than status three or status four patients,” mainly because most are in renal failure and listed for multiorgan transplantation with a kidney.
Objective physiologic measurements, such as glomerular filtration rate (GFR), had high variable importance, offering a minimally invasive measurement with predictive power in assessing medical urgency. Therefore, including GFR and other variables such as extracorporeal membrane oxygenation (ECMO) could improve the accuracy of the allocation system in identifying the most medically urgent candidates, Dr. Parker and colleagues suggest.
The study was published online in JACC: Heart Failure.
‘Moderate ability’ to rank order
The investigators assessed the effectiveness of the standard six-status ranking system and several novel prediction models in identifying the most urgent heart transplant candidates. The primary outcome was death before receipt of a heart transplant.
The final data set contained 32,294 candidates (mean age, 53 years; 74%, men); 27,200 made up the prepolicy training set and 5,094 were included in the postpolicy test set.
The team evaluated the accuracy of the six-status system using Harrell’s C-index and log-rank tests of Kaplan-Meier estimated survival by status for candidates listed after the policy change (November 2018 to March 2020) in the Scientific Registry of Transplant Recipients data set.
They then developed Cox proportional hazards models and random survival forest models using prepolicy data (2010-2017). Predictor variables included age, diagnosis, laboratory measurements, hemodynamics, and supportive treatment at the time of listing.
They found that the six-status ranking at listing has had “moderate ability” to rank order candidates.
As Dr. Parker indicated, statuses four and six had no significant difference in survival, and status five had lower survival than status four.
The investigators’ multivariable prediction models derived with prepolicy data ranked candidates correctly more often than the six-status rankings. Objective physiologic measurements, such as GFR and ECMO, were identified as having significant importance with regard to ranking by urgency.
“The novel prediction models we developed … could be implemented by the Organ Procurement and Transplantation Network (OPTN) as allocation policy and would be better than the status quo,” Dr. Parker said. “However, I think we could do even better using the newer data collected after 2018.”
Modifications underway
The OPTN Heart Transplantation Committee is currently working on developing a new framework for allocating deceased donor hearts called Continuous Distribution.
“The six-tiered system works well, and it better stratifies the most medically urgent candidates than the previous allocation framework,” the leadership of the United Network for Organ Sharing Heart Transplantation Committee, including Chair Richard C. Daly, MD, Mayo Clinic; Vice-Chair Jondavid Menteer, MD, University of Southern California, Los Angeles; and former Chair Shelley Hall, MD, Baylor University Medical Center, told this news organization.
“That said, it is always appropriate to review and adjust variables that affect the medical urgency attribute for heart allocation.”
The new framework will change how patients are prioritized, they said. “Continuous distribution will consider all patient factors, including medical urgency, together to determine the order of an organ offer, and no single factor will decide an organ match.
“The goal is to increase fairness by moving to a points-based allocation framework that allows candidates to be compared using a single score composed of multiple factors.
“Furthermore,” they added, “continuous distribution provides a framework that will allow modifications of the criteria defining medical urgency (and other attributes of allocation) to a finer degree than the current policy. … Once continuous distribution is in place and the OPTN has policy monitoring data, the committee may consider and model different ways of defining medical urgency.”
Kiran K. Khush, MD, of Stanford (Calif.) University School of Medicine, coauthor of a related commentary, elaborated. “The composite allocation score (CAS) will consist of a ‘points-based system,’ in which candidates will be assigned points based on (1) medical urgency, (2) anticipated posttransplant survival, (3) candidate biology (eg., special characteristics that may result in higher prioritization, such as blood type O and allosensitization), (4) access (eg., prior living donor, pediatric patient), and (5) placement efficacy (travel, proximity).”
Candidates will be assigned points based on these categories, and will be rank ordered for each donor offer.
Dr. Khush and colleagues propose that a multivariable model – such as the ones described in the study – would be the best way to assign points for medical urgency.
“This system will be more equitable than the current system,” Dr. Khush said, “because it will better prioritize the sickest candidates while improving access for patients who are currently at a disadvantage [for example, blood O, highly sensitized patients], and will also remove artificial geographic boundaries [for example, the current 500-mile rule for heart allocation].”
Going further
Jesse D. Schold, PhD, of the University of Colorado at Denver, Aurora, raises concerns about other aspects of the heart allocation system in another related commentary.
“One big issue with our data in transplantation … is that, while it is very comprehensive for capturing transplant candidates and recipients, there is no data collection for patients and processes of care for patients prior to wait list placement,” he told this news organization. This phase of care is subject to wide variation in practice, he said, “and is likely as important as any to patients – the ability to be referred, evaluated, and placed on a waiting list.”
Report cards that measure quality of care after wait list placement ignore key phases prior to wait list placement, he said. “This may have the unintended consequences of limiting access to care and to the waiting list for patients perceived to be at higher risk, or the use of higher-risk donors, despite their potential survival advantage.
“In contrast,” he said, “quality report cards that incentivize treatment for all patients who may benefit would likely have a greater beneficial impact on patients with end-organ disease.”
There is also significant risk of underlying differences in patient populations between centers, despite the use of multivariable models, he added. This heterogeneity “may not be reflected accurately in the report cards [which] have significant impact for regulatory review, private payer contracting, and center reputation.”
Some of these concerns may be addressed in the new OPTN Modernization Initiative, according to David Bowman, a public affairs specialist at the Health Resources and Services Administration. One of the goals of the initiative “is to ensure that the OPTN Board of Directors is high functioning, has greater independence, and represents the diversity of communities served by the OPTN,” he told this news organization. “Strengthened governance will lead to effective policy development and implementation, and enhanced transparency and accountability of the process.”
Addressing another concern about the system, Savitri Fedson, MD, of the Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, wonders in a related editorial whether organ donors and recipients should know more about each other, and if so, could that reverse the ongoing downward trend in organ acceptance?
Although some organizations are in favor of sharing more information, Dr. Fedson notes that “less information may have the greater benefit.” She writes, “We might realize that the simplest approach is often the best: a fulsome thank you for the donor’s gift that is willingly given to a stranger without expectation of payment, and on the recipient side, the knowledge that an organ is of good quality.
“The transplant patient can be comforted with the understanding that the risk of disease transmission, while not zero, is low, and that their survival following acceptance of an organ is better than languishing on a waiting list.”
The study received no commercial funding. Dr. Parker, Dr. Khush, Dr. Schold, and Dr. Fedson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prediction models that incorporate more than just treatment status could rank order heart transplant candidates by urgency more effectively than the current system, a modeling study suggests.
Since 2018, the U.S. heart transplant allocation system has ranked heart candidates according to six treatment-based “statuses” (up from three used previously), ignoring many objective patient characteristics, the authors write.
Their study showed no significant difference in survival between statuses four and six, and status five had lower survival than status four.
“We expected multivariable prediction models to outperform the six-status system when it comes to rank ordering patients by how likely they are to die on the wait list (medical urgency),” William F. Parker, MD, MS, PhD, of the University of Chicago, told this news organization.
“However, we were surprised to see that the statuses were out of order,” he said. “Status five patients are more urgent than status three or status four patients,” mainly because most are in renal failure and listed for multiorgan transplantation with a kidney.
Objective physiologic measurements, such as glomerular filtration rate (GFR), had high variable importance, offering a minimally invasive measurement with predictive power in assessing medical urgency. Therefore, including GFR and other variables such as extracorporeal membrane oxygenation (ECMO) could improve the accuracy of the allocation system in identifying the most medically urgent candidates, Dr. Parker and colleagues suggest.
The study was published online in JACC: Heart Failure.
‘Moderate ability’ to rank order
The investigators assessed the effectiveness of the standard six-status ranking system and several novel prediction models in identifying the most urgent heart transplant candidates. The primary outcome was death before receipt of a heart transplant.
The final data set contained 32,294 candidates (mean age, 53 years; 74%, men); 27,200 made up the prepolicy training set and 5,094 were included in the postpolicy test set.
The team evaluated the accuracy of the six-status system using Harrell’s C-index and log-rank tests of Kaplan-Meier estimated survival by status for candidates listed after the policy change (November 2018 to March 2020) in the Scientific Registry of Transplant Recipients data set.
They then developed Cox proportional hazards models and random survival forest models using prepolicy data (2010-2017). Predictor variables included age, diagnosis, laboratory measurements, hemodynamics, and supportive treatment at the time of listing.
They found that the six-status ranking at listing has had “moderate ability” to rank order candidates.
As Dr. Parker indicated, statuses four and six had no significant difference in survival, and status five had lower survival than status four.
The investigators’ multivariable prediction models derived with prepolicy data ranked candidates correctly more often than the six-status rankings. Objective physiologic measurements, such as GFR and ECMO, were identified as having significant importance with regard to ranking by urgency.
“The novel prediction models we developed … could be implemented by the Organ Procurement and Transplantation Network (OPTN) as allocation policy and would be better than the status quo,” Dr. Parker said. “However, I think we could do even better using the newer data collected after 2018.”
Modifications underway
The OPTN Heart Transplantation Committee is currently working on developing a new framework for allocating deceased donor hearts called Continuous Distribution.
“The six-tiered system works well, and it better stratifies the most medically urgent candidates than the previous allocation framework,” the leadership of the United Network for Organ Sharing Heart Transplantation Committee, including Chair Richard C. Daly, MD, Mayo Clinic; Vice-Chair Jondavid Menteer, MD, University of Southern California, Los Angeles; and former Chair Shelley Hall, MD, Baylor University Medical Center, told this news organization.
“That said, it is always appropriate to review and adjust variables that affect the medical urgency attribute for heart allocation.”
The new framework will change how patients are prioritized, they said. “Continuous distribution will consider all patient factors, including medical urgency, together to determine the order of an organ offer, and no single factor will decide an organ match.
“The goal is to increase fairness by moving to a points-based allocation framework that allows candidates to be compared using a single score composed of multiple factors.
“Furthermore,” they added, “continuous distribution provides a framework that will allow modifications of the criteria defining medical urgency (and other attributes of allocation) to a finer degree than the current policy. … Once continuous distribution is in place and the OPTN has policy monitoring data, the committee may consider and model different ways of defining medical urgency.”
Kiran K. Khush, MD, of Stanford (Calif.) University School of Medicine, coauthor of a related commentary, elaborated. “The composite allocation score (CAS) will consist of a ‘points-based system,’ in which candidates will be assigned points based on (1) medical urgency, (2) anticipated posttransplant survival, (3) candidate biology (eg., special characteristics that may result in higher prioritization, such as blood type O and allosensitization), (4) access (eg., prior living donor, pediatric patient), and (5) placement efficacy (travel, proximity).”
Candidates will be assigned points based on these categories, and will be rank ordered for each donor offer.
Dr. Khush and colleagues propose that a multivariable model – such as the ones described in the study – would be the best way to assign points for medical urgency.
“This system will be more equitable than the current system,” Dr. Khush said, “because it will better prioritize the sickest candidates while improving access for patients who are currently at a disadvantage [for example, blood O, highly sensitized patients], and will also remove artificial geographic boundaries [for example, the current 500-mile rule for heart allocation].”
Going further
Jesse D. Schold, PhD, of the University of Colorado at Denver, Aurora, raises concerns about other aspects of the heart allocation system in another related commentary.
“One big issue with our data in transplantation … is that, while it is very comprehensive for capturing transplant candidates and recipients, there is no data collection for patients and processes of care for patients prior to wait list placement,” he told this news organization. This phase of care is subject to wide variation in practice, he said, “and is likely as important as any to patients – the ability to be referred, evaluated, and placed on a waiting list.”
Report cards that measure quality of care after wait list placement ignore key phases prior to wait list placement, he said. “This may have the unintended consequences of limiting access to care and to the waiting list for patients perceived to be at higher risk, or the use of higher-risk donors, despite their potential survival advantage.
“In contrast,” he said, “quality report cards that incentivize treatment for all patients who may benefit would likely have a greater beneficial impact on patients with end-organ disease.”
There is also significant risk of underlying differences in patient populations between centers, despite the use of multivariable models, he added. This heterogeneity “may not be reflected accurately in the report cards [which] have significant impact for regulatory review, private payer contracting, and center reputation.”
Some of these concerns may be addressed in the new OPTN Modernization Initiative, according to David Bowman, a public affairs specialist at the Health Resources and Services Administration. One of the goals of the initiative “is to ensure that the OPTN Board of Directors is high functioning, has greater independence, and represents the diversity of communities served by the OPTN,” he told this news organization. “Strengthened governance will lead to effective policy development and implementation, and enhanced transparency and accountability of the process.”
Addressing another concern about the system, Savitri Fedson, MD, of the Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, wonders in a related editorial whether organ donors and recipients should know more about each other, and if so, could that reverse the ongoing downward trend in organ acceptance?
Although some organizations are in favor of sharing more information, Dr. Fedson notes that “less information may have the greater benefit.” She writes, “We might realize that the simplest approach is often the best: a fulsome thank you for the donor’s gift that is willingly given to a stranger without expectation of payment, and on the recipient side, the knowledge that an organ is of good quality.
“The transplant patient can be comforted with the understanding that the risk of disease transmission, while not zero, is low, and that their survival following acceptance of an organ is better than languishing on a waiting list.”
The study received no commercial funding. Dr. Parker, Dr. Khush, Dr. Schold, and Dr. Fedson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Prediction models that incorporate more than just treatment status could rank order heart transplant candidates by urgency more effectively than the current system, a modeling study suggests.
Since 2018, the U.S. heart transplant allocation system has ranked heart candidates according to six treatment-based “statuses” (up from three used previously), ignoring many objective patient characteristics, the authors write.
Their study showed no significant difference in survival between statuses four and six, and status five had lower survival than status four.
“We expected multivariable prediction models to outperform the six-status system when it comes to rank ordering patients by how likely they are to die on the wait list (medical urgency),” William F. Parker, MD, MS, PhD, of the University of Chicago, told this news organization.
“However, we were surprised to see that the statuses were out of order,” he said. “Status five patients are more urgent than status three or status four patients,” mainly because most are in renal failure and listed for multiorgan transplantation with a kidney.
Objective physiologic measurements, such as glomerular filtration rate (GFR), had high variable importance, offering a minimally invasive measurement with predictive power in assessing medical urgency. Therefore, including GFR and other variables such as extracorporeal membrane oxygenation (ECMO) could improve the accuracy of the allocation system in identifying the most medically urgent candidates, Dr. Parker and colleagues suggest.
The study was published online in JACC: Heart Failure.
‘Moderate ability’ to rank order
The investigators assessed the effectiveness of the standard six-status ranking system and several novel prediction models in identifying the most urgent heart transplant candidates. The primary outcome was death before receipt of a heart transplant.
The final data set contained 32,294 candidates (mean age, 53 years; 74%, men); 27,200 made up the prepolicy training set and 5,094 were included in the postpolicy test set.
The team evaluated the accuracy of the six-status system using Harrell’s C-index and log-rank tests of Kaplan-Meier estimated survival by status for candidates listed after the policy change (November 2018 to March 2020) in the Scientific Registry of Transplant Recipients data set.
They then developed Cox proportional hazards models and random survival forest models using prepolicy data (2010-2017). Predictor variables included age, diagnosis, laboratory measurements, hemodynamics, and supportive treatment at the time of listing.
They found that the six-status ranking at listing has had “moderate ability” to rank order candidates.
As Dr. Parker indicated, statuses four and six had no significant difference in survival, and status five had lower survival than status four.
The investigators’ multivariable prediction models derived with prepolicy data ranked candidates correctly more often than the six-status rankings. Objective physiologic measurements, such as GFR and ECMO, were identified as having significant importance with regard to ranking by urgency.
“The novel prediction models we developed … could be implemented by the Organ Procurement and Transplantation Network (OPTN) as allocation policy and would be better than the status quo,” Dr. Parker said. “However, I think we could do even better using the newer data collected after 2018.”
Modifications underway
The OPTN Heart Transplantation Committee is currently working on developing a new framework for allocating deceased donor hearts called Continuous Distribution.
“The six-tiered system works well, and it better stratifies the most medically urgent candidates than the previous allocation framework,” the leadership of the United Network for Organ Sharing Heart Transplantation Committee, including Chair Richard C. Daly, MD, Mayo Clinic; Vice-Chair Jondavid Menteer, MD, University of Southern California, Los Angeles; and former Chair Shelley Hall, MD, Baylor University Medical Center, told this news organization.
“That said, it is always appropriate to review and adjust variables that affect the medical urgency attribute for heart allocation.”
The new framework will change how patients are prioritized, they said. “Continuous distribution will consider all patient factors, including medical urgency, together to determine the order of an organ offer, and no single factor will decide an organ match.
“The goal is to increase fairness by moving to a points-based allocation framework that allows candidates to be compared using a single score composed of multiple factors.
“Furthermore,” they added, “continuous distribution provides a framework that will allow modifications of the criteria defining medical urgency (and other attributes of allocation) to a finer degree than the current policy. … Once continuous distribution is in place and the OPTN has policy monitoring data, the committee may consider and model different ways of defining medical urgency.”
Kiran K. Khush, MD, of Stanford (Calif.) University School of Medicine, coauthor of a related commentary, elaborated. “The composite allocation score (CAS) will consist of a ‘points-based system,’ in which candidates will be assigned points based on (1) medical urgency, (2) anticipated posttransplant survival, (3) candidate biology (eg., special characteristics that may result in higher prioritization, such as blood type O and allosensitization), (4) access (eg., prior living donor, pediatric patient), and (5) placement efficacy (travel, proximity).”
Candidates will be assigned points based on these categories, and will be rank ordered for each donor offer.
Dr. Khush and colleagues propose that a multivariable model – such as the ones described in the study – would be the best way to assign points for medical urgency.
“This system will be more equitable than the current system,” Dr. Khush said, “because it will better prioritize the sickest candidates while improving access for patients who are currently at a disadvantage [for example, blood O, highly sensitized patients], and will also remove artificial geographic boundaries [for example, the current 500-mile rule for heart allocation].”
Going further
Jesse D. Schold, PhD, of the University of Colorado at Denver, Aurora, raises concerns about other aspects of the heart allocation system in another related commentary.
“One big issue with our data in transplantation … is that, while it is very comprehensive for capturing transplant candidates and recipients, there is no data collection for patients and processes of care for patients prior to wait list placement,” he told this news organization. This phase of care is subject to wide variation in practice, he said, “and is likely as important as any to patients – the ability to be referred, evaluated, and placed on a waiting list.”
Report cards that measure quality of care after wait list placement ignore key phases prior to wait list placement, he said. “This may have the unintended consequences of limiting access to care and to the waiting list for patients perceived to be at higher risk, or the use of higher-risk donors, despite their potential survival advantage.
“In contrast,” he said, “quality report cards that incentivize treatment for all patients who may benefit would likely have a greater beneficial impact on patients with end-organ disease.”
There is also significant risk of underlying differences in patient populations between centers, despite the use of multivariable models, he added. This heterogeneity “may not be reflected accurately in the report cards [which] have significant impact for regulatory review, private payer contracting, and center reputation.”
Some of these concerns may be addressed in the new OPTN Modernization Initiative, according to David Bowman, a public affairs specialist at the Health Resources and Services Administration. One of the goals of the initiative “is to ensure that the OPTN Board of Directors is high functioning, has greater independence, and represents the diversity of communities served by the OPTN,” he told this news organization. “Strengthened governance will lead to effective policy development and implementation, and enhanced transparency and accountability of the process.”
Addressing another concern about the system, Savitri Fedson, MD, of the Michael E. DeBakey VA Medical Center and Baylor College of Medicine, Houston, wonders in a related editorial whether organ donors and recipients should know more about each other, and if so, could that reverse the ongoing downward trend in organ acceptance?
Although some organizations are in favor of sharing more information, Dr. Fedson notes that “less information may have the greater benefit.” She writes, “We might realize that the simplest approach is often the best: a fulsome thank you for the donor’s gift that is willingly given to a stranger without expectation of payment, and on the recipient side, the knowledge that an organ is of good quality.
“The transplant patient can be comforted with the understanding that the risk of disease transmission, while not zero, is low, and that their survival following acceptance of an organ is better than languishing on a waiting list.”
The study received no commercial funding. Dr. Parker, Dr. Khush, Dr. Schold, and Dr. Fedson report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JACC: HEART FAILURE
Hybrid ablation superior for persistent AFib: CEASE-AF
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”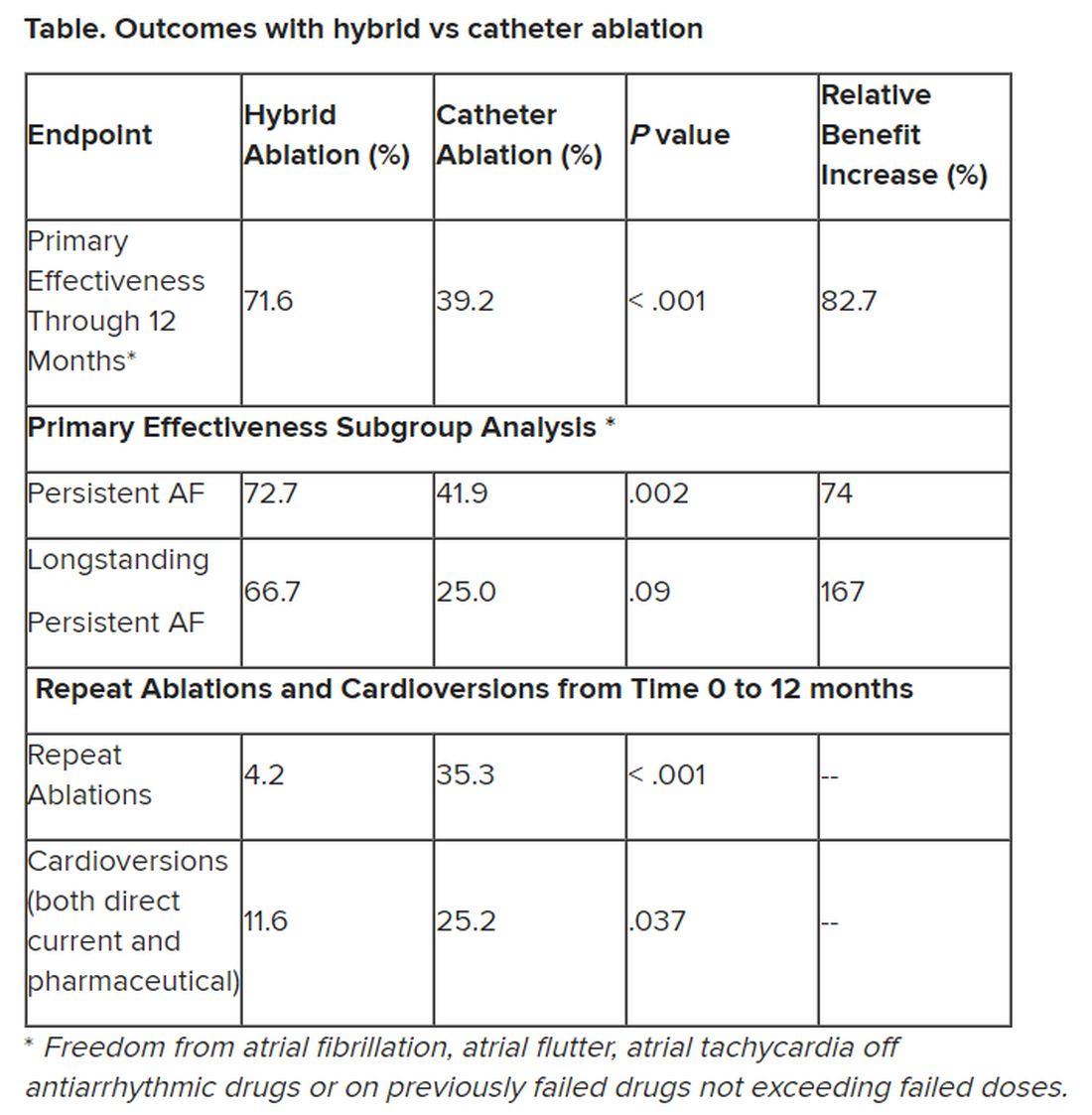
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AT EHRA 2023
AHA statement targets nuance in CVD risk assessment of women
In a new scientific statement, the American Heart Association highlighted the importance of incorporating nonbiological risk factors and social determinants of health in cardiovascular disease (CVD) risk assessment for women, particularly women from different racial and ethnic backgrounds.
CVD risk assessment in women is multifaceted and goes well beyond traditional risk factors to include sex-specific biological risk factors, as well as social, behavioral, and environmental factors, the writing group noted.
They said a greater focus on addressing all CVD risk factors among women from underrepresented races and ethnicities is warranted to avert future CVD.
The scientific statement was published online in Circulation.
Look beyond traditional risk factors
“Risk assessment is the first step in preventing heart disease, yet there are many limitations to traditional risk factors and their ability to comprehensively estimate a woman’s risk for cardiovascular disease,” Jennifer H. Mieres, MD, vice chair of the writing group and professor of cardiology at Hofstra University, Hempstead, N.Y., said in a news release.
“The delivery of equitable cardiovascular health care for women depends on improving the knowledge and awareness of all members of the healthcare team about the full spectrum of cardiovascular risk factors for women, including female-specific and female-predominant risk factors,” Dr. Mieres added.
Female-specific factors that should be included in CVD risk assessment include pregnancy-related conditions such as preeclampsia, preterm delivery, and gestational diabetes, the writing group said.
Other factors include menstrual cycle history; types of birth control and/or hormone replacement therapy used; polycystic ovarian syndrome (PCOS), which affects 10% of women of reproductive age and is associated with increased CVD risk; and autoimmune disorders, depression, and PTSD, all of which are more common in women and are also associated with higher risk for CVD.
The statement also highlights the key role that social determinants of health (SDOH) play in the development of CVD in women, particularly women from diverse racial and ethnic backgrounds. SDOH include education level, economic stability, neighborhood safety, working conditions, environmental hazards, and access to quality health care.
“It is critical that risk assessment be expanded to include [SDOH] as risk factors if we are to improve health outcomes in all women,” Laxmi Mehta, MD, chair of the writing group and director of preventative cardiology and women’s cardiovascular health at Ohio State University Wexner Medical Center, Columbus, said in the news release.
“It is also important for the health care team to consider [SDOH] when working with women on shared decisions about cardiovascular disease prevention and treatment,” Dr. Mehta noted.
No one-size-fits-all approach
The statement highlighted significant differences in CVD risk among women of different racial and ethnic backgrounds and provides detailed CV risk factor profiles for non-Hispanic Black, Hispanic/Latinx, Asian and American Indian/Alaska Native women.
It noted that language barriers, discrimination, acculturation, and health care access disproportionately affect women of underrepresented racial and ethnic groups. These factors result in a higher prevalence of CVD and significant challenges in CVD diagnosis and treatment.
“When customizing CVD prevention and treatment strategies to improve cardiovascular health for women, a one-size-fits-all approach is unlikely to be successful,” Dr. Mieres said.
“We must be cognizant of the complex interplay of sex, race and ethnicity, as well as social determinants of health, and how they impact the risk of cardiovascular disease and adverse outcomes in order to avert future CVD morbidity and mortality,” Dr. Mieres added.
Looking ahead, the writing group said future CVD prevention guidelines could be strengthened by including culturally-specific lifestyle recommendations.
They also said community-based approaches, faith-based community partnerships, and peer support to encourage a healthy lifestyle could play a key role in preventing CVD among all women.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifelong Congenital Heart Disease and Heart Health in the Young, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article first appeared on Medscape.com.
In a new scientific statement, the American Heart Association highlighted the importance of incorporating nonbiological risk factors and social determinants of health in cardiovascular disease (CVD) risk assessment for women, particularly women from different racial and ethnic backgrounds.
CVD risk assessment in women is multifaceted and goes well beyond traditional risk factors to include sex-specific biological risk factors, as well as social, behavioral, and environmental factors, the writing group noted.
They said a greater focus on addressing all CVD risk factors among women from underrepresented races and ethnicities is warranted to avert future CVD.
The scientific statement was published online in Circulation.
Look beyond traditional risk factors
“Risk assessment is the first step in preventing heart disease, yet there are many limitations to traditional risk factors and their ability to comprehensively estimate a woman’s risk for cardiovascular disease,” Jennifer H. Mieres, MD, vice chair of the writing group and professor of cardiology at Hofstra University, Hempstead, N.Y., said in a news release.
“The delivery of equitable cardiovascular health care for women depends on improving the knowledge and awareness of all members of the healthcare team about the full spectrum of cardiovascular risk factors for women, including female-specific and female-predominant risk factors,” Dr. Mieres added.
Female-specific factors that should be included in CVD risk assessment include pregnancy-related conditions such as preeclampsia, preterm delivery, and gestational diabetes, the writing group said.
Other factors include menstrual cycle history; types of birth control and/or hormone replacement therapy used; polycystic ovarian syndrome (PCOS), which affects 10% of women of reproductive age and is associated with increased CVD risk; and autoimmune disorders, depression, and PTSD, all of which are more common in women and are also associated with higher risk for CVD.
The statement also highlights the key role that social determinants of health (SDOH) play in the development of CVD in women, particularly women from diverse racial and ethnic backgrounds. SDOH include education level, economic stability, neighborhood safety, working conditions, environmental hazards, and access to quality health care.
“It is critical that risk assessment be expanded to include [SDOH] as risk factors if we are to improve health outcomes in all women,” Laxmi Mehta, MD, chair of the writing group and director of preventative cardiology and women’s cardiovascular health at Ohio State University Wexner Medical Center, Columbus, said in the news release.
“It is also important for the health care team to consider [SDOH] when working with women on shared decisions about cardiovascular disease prevention and treatment,” Dr. Mehta noted.
No one-size-fits-all approach
The statement highlighted significant differences in CVD risk among women of different racial and ethnic backgrounds and provides detailed CV risk factor profiles for non-Hispanic Black, Hispanic/Latinx, Asian and American Indian/Alaska Native women.
It noted that language barriers, discrimination, acculturation, and health care access disproportionately affect women of underrepresented racial and ethnic groups. These factors result in a higher prevalence of CVD and significant challenges in CVD diagnosis and treatment.
“When customizing CVD prevention and treatment strategies to improve cardiovascular health for women, a one-size-fits-all approach is unlikely to be successful,” Dr. Mieres said.
“We must be cognizant of the complex interplay of sex, race and ethnicity, as well as social determinants of health, and how they impact the risk of cardiovascular disease and adverse outcomes in order to avert future CVD morbidity and mortality,” Dr. Mieres added.
Looking ahead, the writing group said future CVD prevention guidelines could be strengthened by including culturally-specific lifestyle recommendations.
They also said community-based approaches, faith-based community partnerships, and peer support to encourage a healthy lifestyle could play a key role in preventing CVD among all women.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifelong Congenital Heart Disease and Heart Health in the Young, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article first appeared on Medscape.com.
In a new scientific statement, the American Heart Association highlighted the importance of incorporating nonbiological risk factors and social determinants of health in cardiovascular disease (CVD) risk assessment for women, particularly women from different racial and ethnic backgrounds.
CVD risk assessment in women is multifaceted and goes well beyond traditional risk factors to include sex-specific biological risk factors, as well as social, behavioral, and environmental factors, the writing group noted.
They said a greater focus on addressing all CVD risk factors among women from underrepresented races and ethnicities is warranted to avert future CVD.
The scientific statement was published online in Circulation.
Look beyond traditional risk factors
“Risk assessment is the first step in preventing heart disease, yet there are many limitations to traditional risk factors and their ability to comprehensively estimate a woman’s risk for cardiovascular disease,” Jennifer H. Mieres, MD, vice chair of the writing group and professor of cardiology at Hofstra University, Hempstead, N.Y., said in a news release.
“The delivery of equitable cardiovascular health care for women depends on improving the knowledge and awareness of all members of the healthcare team about the full spectrum of cardiovascular risk factors for women, including female-specific and female-predominant risk factors,” Dr. Mieres added.
Female-specific factors that should be included in CVD risk assessment include pregnancy-related conditions such as preeclampsia, preterm delivery, and gestational diabetes, the writing group said.
Other factors include menstrual cycle history; types of birth control and/or hormone replacement therapy used; polycystic ovarian syndrome (PCOS), which affects 10% of women of reproductive age and is associated with increased CVD risk; and autoimmune disorders, depression, and PTSD, all of which are more common in women and are also associated with higher risk for CVD.
The statement also highlights the key role that social determinants of health (SDOH) play in the development of CVD in women, particularly women from diverse racial and ethnic backgrounds. SDOH include education level, economic stability, neighborhood safety, working conditions, environmental hazards, and access to quality health care.
“It is critical that risk assessment be expanded to include [SDOH] as risk factors if we are to improve health outcomes in all women,” Laxmi Mehta, MD, chair of the writing group and director of preventative cardiology and women’s cardiovascular health at Ohio State University Wexner Medical Center, Columbus, said in the news release.
“It is also important for the health care team to consider [SDOH] when working with women on shared decisions about cardiovascular disease prevention and treatment,” Dr. Mehta noted.
No one-size-fits-all approach
The statement highlighted significant differences in CVD risk among women of different racial and ethnic backgrounds and provides detailed CV risk factor profiles for non-Hispanic Black, Hispanic/Latinx, Asian and American Indian/Alaska Native women.
It noted that language barriers, discrimination, acculturation, and health care access disproportionately affect women of underrepresented racial and ethnic groups. These factors result in a higher prevalence of CVD and significant challenges in CVD diagnosis and treatment.
“When customizing CVD prevention and treatment strategies to improve cardiovascular health for women, a one-size-fits-all approach is unlikely to be successful,” Dr. Mieres said.
“We must be cognizant of the complex interplay of sex, race and ethnicity, as well as social determinants of health, and how they impact the risk of cardiovascular disease and adverse outcomes in order to avert future CVD morbidity and mortality,” Dr. Mieres added.
Looking ahead, the writing group said future CVD prevention guidelines could be strengthened by including culturally-specific lifestyle recommendations.
They also said community-based approaches, faith-based community partnerships, and peer support to encourage a healthy lifestyle could play a key role in preventing CVD among all women.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA’s Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, the Council on Lifelong Congenital Heart Disease and Heart Health in the Young, the Council on Lifestyle and Cardiometabolic Health, the Council on Peripheral Vascular Disease, and the Stroke Council.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
New ASE guideline on interventional echocardiography training
The American Society of Echocardiography (ASE) has issued guidance on all critical aspects of training for cardiology and anesthesiology trainees and postgraduate echocardiographers who plan to specialize in interventional echocardiography (IE).
The guideline outlines requirements of the training institution, the duration and core competencies of training, minimal procedural volume for competency in IE, and knowledge of specific structural health disease (SHD) procedures.
The 16-page guideline was published online in the Journal of the American Society of Echocardiography.
Specific skill set
IE is the primary imaging modality used to support and guide SHD interventions, such as heart valve replacements and other cardiac catheterization procedures, the writing group notes.
They say the “emerging specialty” of IE requires a specific set of skills to support an array of transcatheter therapies, with successful outcomes highly dependent on the skill of the echocardiography team.
“IE techniques are unique since imaging is performed in real-time, it is highly dependent on 3D and non-standard views, and it has immediate and profound implications for patient management,” Stephen H. Little, MD, ASE president and co-chair of the guideline writing group, says in a news release.
“Additionally, IE requires candid, accurate, and timely communication with other members of the multidisciplinary SHD team,” Dr. Little adds.
The new ASE guideline expands on the 2019 statement on echocardiography training put forward by the American College of Cardiology, American Heart Association, and ASE, by focusing specifically on interventional echocardiographers.
It outlines core competencies common to all transcatheter therapies, as well as specific transcatheter procedures. It provides consensus recommendations for specific knowledge, experience, and skills to be learned and demonstrated within an IE training program or during postgraduate training.
A “core principle” in the guideline states that the length of IE training or achieved number of procedures performed are less important than the demonstration of procedure-specific competencies within the milestone domains of knowledge, skill, and communication.
“Transcatheter therapies for SHD continue to grow at a rapid pace, which means that the demand for skilled interventional echocardiographers has steadily increased,” Vera H. Rigolin, MD, co-chair of the guideline writing, says in the release.
“Training standards are needed to ensure that interventional echocardiographers have the necessary expertise to provide fast, accurate, and high-quality image acquisition and interpretation in real-time,” Dr. Rigolin adds.
In addition, the guidelines states that use of simulation training has a role in IE training.
Virtual and simulation training could shorten the learning curve for trainees and, when combined with remote learning, could permit societies to standardize a teaching curriculum and allow the trainee to complete training in a reasonable timeframe. Simulator training may also improve access to training and thus promote diversity and inclusivity, the writing group says.
The guideline has been endorsed by 21 ASE international partners.
Writing group co-chairs Little and Rigolin have declared no conflicts of interest. A complete list of disclosures for the writing group is available with the original article.
A version of this article first appeared on Medscape.com.
The American Society of Echocardiography (ASE) has issued guidance on all critical aspects of training for cardiology and anesthesiology trainees and postgraduate echocardiographers who plan to specialize in interventional echocardiography (IE).
The guideline outlines requirements of the training institution, the duration and core competencies of training, minimal procedural volume for competency in IE, and knowledge of specific structural health disease (SHD) procedures.
The 16-page guideline was published online in the Journal of the American Society of Echocardiography.
Specific skill set
IE is the primary imaging modality used to support and guide SHD interventions, such as heart valve replacements and other cardiac catheterization procedures, the writing group notes.
They say the “emerging specialty” of IE requires a specific set of skills to support an array of transcatheter therapies, with successful outcomes highly dependent on the skill of the echocardiography team.
“IE techniques are unique since imaging is performed in real-time, it is highly dependent on 3D and non-standard views, and it has immediate and profound implications for patient management,” Stephen H. Little, MD, ASE president and co-chair of the guideline writing group, says in a news release.
“Additionally, IE requires candid, accurate, and timely communication with other members of the multidisciplinary SHD team,” Dr. Little adds.
The new ASE guideline expands on the 2019 statement on echocardiography training put forward by the American College of Cardiology, American Heart Association, and ASE, by focusing specifically on interventional echocardiographers.
It outlines core competencies common to all transcatheter therapies, as well as specific transcatheter procedures. It provides consensus recommendations for specific knowledge, experience, and skills to be learned and demonstrated within an IE training program or during postgraduate training.
A “core principle” in the guideline states that the length of IE training or achieved number of procedures performed are less important than the demonstration of procedure-specific competencies within the milestone domains of knowledge, skill, and communication.
“Transcatheter therapies for SHD continue to grow at a rapid pace, which means that the demand for skilled interventional echocardiographers has steadily increased,” Vera H. Rigolin, MD, co-chair of the guideline writing, says in the release.
“Training standards are needed to ensure that interventional echocardiographers have the necessary expertise to provide fast, accurate, and high-quality image acquisition and interpretation in real-time,” Dr. Rigolin adds.
In addition, the guidelines states that use of simulation training has a role in IE training.
Virtual and simulation training could shorten the learning curve for trainees and, when combined with remote learning, could permit societies to standardize a teaching curriculum and allow the trainee to complete training in a reasonable timeframe. Simulator training may also improve access to training and thus promote diversity and inclusivity, the writing group says.
The guideline has been endorsed by 21 ASE international partners.
Writing group co-chairs Little and Rigolin have declared no conflicts of interest. A complete list of disclosures for the writing group is available with the original article.
A version of this article first appeared on Medscape.com.
The American Society of Echocardiography (ASE) has issued guidance on all critical aspects of training for cardiology and anesthesiology trainees and postgraduate echocardiographers who plan to specialize in interventional echocardiography (IE).
The guideline outlines requirements of the training institution, the duration and core competencies of training, minimal procedural volume for competency in IE, and knowledge of specific structural health disease (SHD) procedures.
The 16-page guideline was published online in the Journal of the American Society of Echocardiography.
Specific skill set
IE is the primary imaging modality used to support and guide SHD interventions, such as heart valve replacements and other cardiac catheterization procedures, the writing group notes.
They say the “emerging specialty” of IE requires a specific set of skills to support an array of transcatheter therapies, with successful outcomes highly dependent on the skill of the echocardiography team.
“IE techniques are unique since imaging is performed in real-time, it is highly dependent on 3D and non-standard views, and it has immediate and profound implications for patient management,” Stephen H. Little, MD, ASE president and co-chair of the guideline writing group, says in a news release.
“Additionally, IE requires candid, accurate, and timely communication with other members of the multidisciplinary SHD team,” Dr. Little adds.
The new ASE guideline expands on the 2019 statement on echocardiography training put forward by the American College of Cardiology, American Heart Association, and ASE, by focusing specifically on interventional echocardiographers.
It outlines core competencies common to all transcatheter therapies, as well as specific transcatheter procedures. It provides consensus recommendations for specific knowledge, experience, and skills to be learned and demonstrated within an IE training program or during postgraduate training.
A “core principle” in the guideline states that the length of IE training or achieved number of procedures performed are less important than the demonstration of procedure-specific competencies within the milestone domains of knowledge, skill, and communication.
“Transcatheter therapies for SHD continue to grow at a rapid pace, which means that the demand for skilled interventional echocardiographers has steadily increased,” Vera H. Rigolin, MD, co-chair of the guideline writing, says in the release.
“Training standards are needed to ensure that interventional echocardiographers have the necessary expertise to provide fast, accurate, and high-quality image acquisition and interpretation in real-time,” Dr. Rigolin adds.
In addition, the guidelines states that use of simulation training has a role in IE training.
Virtual and simulation training could shorten the learning curve for trainees and, when combined with remote learning, could permit societies to standardize a teaching curriculum and allow the trainee to complete training in a reasonable timeframe. Simulator training may also improve access to training and thus promote diversity and inclusivity, the writing group says.
The guideline has been endorsed by 21 ASE international partners.
Writing group co-chairs Little and Rigolin have declared no conflicts of interest. A complete list of disclosures for the writing group is available with the original article.
A version of this article first appeared on Medscape.com.
Spherical heart may predict cardiomyopathy, AFib
A round heart, or left ventricle sphericity, predicted cardiomyopathy and atrial fibrillation (AFib) in a deep learning analysis of MRI images from close to 39,000 participants in the UK Biobank, a new study shows.
An increase of 1 standard deviation in the sphericity index (short axis length/long axis length) was associated with a 47% increased incidence of cardiomyopathy and a 20% increased incidence of AFib, independent of clinical factors and traditional MRI measures.
Furthermore, a genetic analysis suggested a shared architecture between sphericity and nonischemic cardiomyopathy, pointing to NICM as a possible causal factor for left ventricle sphericity among individuals with normal LV size and function.
“Physicians have known the heart gets rounder after heart attacks and as we get older,” David Ouyang, MD, a cardiologist in the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, and a researcher in the division of artificial intelligence in medicine, said in an interview. “We wanted to see if this sphericity is prognostic of future disease even in healthy individuals.”
Although it is too early to recommend heart shape assessment in healthy asymptomatic people, he said, “physicians should be extra careful and think about treatments when they notice a patient’s heart is particularly round.”
The study was published online March 29 in the journal Med.
Sphericity index key
The investigators hypothesized that there is variation in LV sphericity within the spectrum of normal LV chamber size and systolic function, and that such variation might be a marker of cardiac risk with genetic influences.
To test this hypothesis, they used automated deep-learning segmentation of cardiac MRI data to estimate and analyze the sphericity index in a cohort of 38,897 individuals participating in the UK Biobank.
After adjustment for age at MRI and sex, an increased sphericity index was associated with an increased risk for cardiomyopathy (hazard ratio, 1.57), AFib (HR, 1.35), and heart failure (HR, 1.37).
No significant association was seen with cardiac arrest.
The team then stratified the cohort into quintiles and compared the top 20%, middle 60%, and bottom 20%. The relationship between the sphericity index and risk extended across the distribution; individuals with higher than median sphericity had increased disease incidence, and those with lower than median sphericity had decreased incidence.
Overall, a single standard deviation in the sphericity index was associated with increased risk of cardiomyopathy (HR, 1.47) and of AFib (HR, 1.20), independent of clinical factors and usual MRI measurements.
In a minimally adjusted model, the sphericity index was a predictor of incident cardiomyopathy, AFib, and heart failure.
Adjustment for clinical factors partially attenuated the heart failure association; additional adjustment for MRI measurements fully attenuated that association and partially attenuated the association with AFib.
However, in all adjusted models, the association with cardiomyopathy showed little attenuation.
Furthermore, the team identified four loci associated with sphericity at genomewide significance – PLN, ANGPT1, PDZRN3, and HLA DR/DQ – and Mendelian randomization supported NICM as a cause of LV sphericity.
Looking ahead
“While conventional imaging metrics have significant diagnostic and prognostic value, some of these measurements have been adopted out of convenience or tradition,” the authors noted. “By representing a specific multidimensional remodeling phenotype, sphericity has emerged as a distinct morphologic trait with features not adequately captured by conventional measurements.
“We expect that the search space of potential imaging measurements is vast, and we have only begun to scratch at the surface of disease associations.”
Indeed, Dr. Ouyang said his group is “trying to evaluate the sphericity in echocardiograms or heart ultrasounds, which are more common and cheaper than MRI.”
“The main caveat is translating the information directly to patient care,” Richard C. Becker, MD, director and physician-in-chief of the University of Cincinnati Heart, Lung, and Vascular Institute, said in an interview. “Near-term yield could include using the spherical calculation in routine MRI of the heart, and based on the findings, following patients more closely if there is an abnormal shape. Or performing an MRI and targeted gene testing if there is a family history of cardiomyopathy or [of] an abnormal shape of the heart.”
“Validation of the findings and large-scale evaluation of the genes identified, and how they interact with patient and environmental factors, will be very important,” he added.
Nevertheless, “the study was well done and may serve as a foundation for future research,” Dr. Becker said. “The investigators used several powerful tools, including MRI, genomics, and [artificial intelligence] to draw their conclusions. This is precisely the way that ‘big data’ should be used – in a complementary fashion.”
The study authors and Dr. Becker reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A round heart, or left ventricle sphericity, predicted cardiomyopathy and atrial fibrillation (AFib) in a deep learning analysis of MRI images from close to 39,000 participants in the UK Biobank, a new study shows.
An increase of 1 standard deviation in the sphericity index (short axis length/long axis length) was associated with a 47% increased incidence of cardiomyopathy and a 20% increased incidence of AFib, independent of clinical factors and traditional MRI measures.
Furthermore, a genetic analysis suggested a shared architecture between sphericity and nonischemic cardiomyopathy, pointing to NICM as a possible causal factor for left ventricle sphericity among individuals with normal LV size and function.
“Physicians have known the heart gets rounder after heart attacks and as we get older,” David Ouyang, MD, a cardiologist in the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, and a researcher in the division of artificial intelligence in medicine, said in an interview. “We wanted to see if this sphericity is prognostic of future disease even in healthy individuals.”
Although it is too early to recommend heart shape assessment in healthy asymptomatic people, he said, “physicians should be extra careful and think about treatments when they notice a patient’s heart is particularly round.”
The study was published online March 29 in the journal Med.
Sphericity index key
The investigators hypothesized that there is variation in LV sphericity within the spectrum of normal LV chamber size and systolic function, and that such variation might be a marker of cardiac risk with genetic influences.
To test this hypothesis, they used automated deep-learning segmentation of cardiac MRI data to estimate and analyze the sphericity index in a cohort of 38,897 individuals participating in the UK Biobank.
After adjustment for age at MRI and sex, an increased sphericity index was associated with an increased risk for cardiomyopathy (hazard ratio, 1.57), AFib (HR, 1.35), and heart failure (HR, 1.37).
No significant association was seen with cardiac arrest.
The team then stratified the cohort into quintiles and compared the top 20%, middle 60%, and bottom 20%. The relationship between the sphericity index and risk extended across the distribution; individuals with higher than median sphericity had increased disease incidence, and those with lower than median sphericity had decreased incidence.
Overall, a single standard deviation in the sphericity index was associated with increased risk of cardiomyopathy (HR, 1.47) and of AFib (HR, 1.20), independent of clinical factors and usual MRI measurements.
In a minimally adjusted model, the sphericity index was a predictor of incident cardiomyopathy, AFib, and heart failure.
Adjustment for clinical factors partially attenuated the heart failure association; additional adjustment for MRI measurements fully attenuated that association and partially attenuated the association with AFib.
However, in all adjusted models, the association with cardiomyopathy showed little attenuation.
Furthermore, the team identified four loci associated with sphericity at genomewide significance – PLN, ANGPT1, PDZRN3, and HLA DR/DQ – and Mendelian randomization supported NICM as a cause of LV sphericity.
Looking ahead
“While conventional imaging metrics have significant diagnostic and prognostic value, some of these measurements have been adopted out of convenience or tradition,” the authors noted. “By representing a specific multidimensional remodeling phenotype, sphericity has emerged as a distinct morphologic trait with features not adequately captured by conventional measurements.
“We expect that the search space of potential imaging measurements is vast, and we have only begun to scratch at the surface of disease associations.”
Indeed, Dr. Ouyang said his group is “trying to evaluate the sphericity in echocardiograms or heart ultrasounds, which are more common and cheaper than MRI.”
“The main caveat is translating the information directly to patient care,” Richard C. Becker, MD, director and physician-in-chief of the University of Cincinnati Heart, Lung, and Vascular Institute, said in an interview. “Near-term yield could include using the spherical calculation in routine MRI of the heart, and based on the findings, following patients more closely if there is an abnormal shape. Or performing an MRI and targeted gene testing if there is a family history of cardiomyopathy or [of] an abnormal shape of the heart.”
“Validation of the findings and large-scale evaluation of the genes identified, and how they interact with patient and environmental factors, will be very important,” he added.
Nevertheless, “the study was well done and may serve as a foundation for future research,” Dr. Becker said. “The investigators used several powerful tools, including MRI, genomics, and [artificial intelligence] to draw their conclusions. This is precisely the way that ‘big data’ should be used – in a complementary fashion.”
The study authors and Dr. Becker reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A round heart, or left ventricle sphericity, predicted cardiomyopathy and atrial fibrillation (AFib) in a deep learning analysis of MRI images from close to 39,000 participants in the UK Biobank, a new study shows.
An increase of 1 standard deviation in the sphericity index (short axis length/long axis length) was associated with a 47% increased incidence of cardiomyopathy and a 20% increased incidence of AFib, independent of clinical factors and traditional MRI measures.
Furthermore, a genetic analysis suggested a shared architecture between sphericity and nonischemic cardiomyopathy, pointing to NICM as a possible causal factor for left ventricle sphericity among individuals with normal LV size and function.
“Physicians have known the heart gets rounder after heart attacks and as we get older,” David Ouyang, MD, a cardiologist in the Smidt Heart Institute at Cedars-Sinai Medical Center, Los Angeles, and a researcher in the division of artificial intelligence in medicine, said in an interview. “We wanted to see if this sphericity is prognostic of future disease even in healthy individuals.”
Although it is too early to recommend heart shape assessment in healthy asymptomatic people, he said, “physicians should be extra careful and think about treatments when they notice a patient’s heart is particularly round.”
The study was published online March 29 in the journal Med.
Sphericity index key
The investigators hypothesized that there is variation in LV sphericity within the spectrum of normal LV chamber size and systolic function, and that such variation might be a marker of cardiac risk with genetic influences.
To test this hypothesis, they used automated deep-learning segmentation of cardiac MRI data to estimate and analyze the sphericity index in a cohort of 38,897 individuals participating in the UK Biobank.
After adjustment for age at MRI and sex, an increased sphericity index was associated with an increased risk for cardiomyopathy (hazard ratio, 1.57), AFib (HR, 1.35), and heart failure (HR, 1.37).
No significant association was seen with cardiac arrest.
The team then stratified the cohort into quintiles and compared the top 20%, middle 60%, and bottom 20%. The relationship between the sphericity index and risk extended across the distribution; individuals with higher than median sphericity had increased disease incidence, and those with lower than median sphericity had decreased incidence.
Overall, a single standard deviation in the sphericity index was associated with increased risk of cardiomyopathy (HR, 1.47) and of AFib (HR, 1.20), independent of clinical factors and usual MRI measurements.
In a minimally adjusted model, the sphericity index was a predictor of incident cardiomyopathy, AFib, and heart failure.
Adjustment for clinical factors partially attenuated the heart failure association; additional adjustment for MRI measurements fully attenuated that association and partially attenuated the association with AFib.
However, in all adjusted models, the association with cardiomyopathy showed little attenuation.
Furthermore, the team identified four loci associated with sphericity at genomewide significance – PLN, ANGPT1, PDZRN3, and HLA DR/DQ – and Mendelian randomization supported NICM as a cause of LV sphericity.
Looking ahead
“While conventional imaging metrics have significant diagnostic and prognostic value, some of these measurements have been adopted out of convenience or tradition,” the authors noted. “By representing a specific multidimensional remodeling phenotype, sphericity has emerged as a distinct morphologic trait with features not adequately captured by conventional measurements.
“We expect that the search space of potential imaging measurements is vast, and we have only begun to scratch at the surface of disease associations.”
Indeed, Dr. Ouyang said his group is “trying to evaluate the sphericity in echocardiograms or heart ultrasounds, which are more common and cheaper than MRI.”
“The main caveat is translating the information directly to patient care,” Richard C. Becker, MD, director and physician-in-chief of the University of Cincinnati Heart, Lung, and Vascular Institute, said in an interview. “Near-term yield could include using the spherical calculation in routine MRI of the heart, and based on the findings, following patients more closely if there is an abnormal shape. Or performing an MRI and targeted gene testing if there is a family history of cardiomyopathy or [of] an abnormal shape of the heart.”
“Validation of the findings and large-scale evaluation of the genes identified, and how they interact with patient and environmental factors, will be very important,” he added.
Nevertheless, “the study was well done and may serve as a foundation for future research,” Dr. Becker said. “The investigators used several powerful tools, including MRI, genomics, and [artificial intelligence] to draw their conclusions. This is precisely the way that ‘big data’ should be used – in a complementary fashion.”
The study authors and Dr. Becker reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MED