User login
Phrenic nerve paralysis induced by brachial plexus block
A 72-year-old man underwent elective ambulatory arthroscopic repair of the right shoulder rotator cuff. To manage postoperative pain, a supraclavicular catheter was placed for brachial plexus block, and he was sent home with a ropivacaine infusion pump.
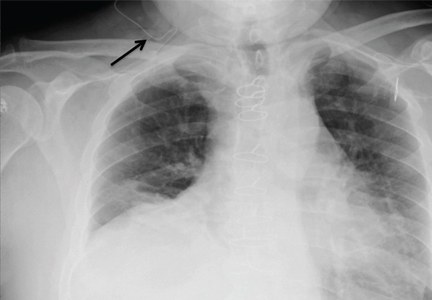
The next day, he presented to the emergency department with right-sided chest pain and mild shortness of breath. He had normal vital signs and adequate oxygen saturation on room air. On physical examination, breath sounds were decreased at the right lung base, and chest radiography (Figure 1) revealed an isolated elevated right hemidiaphragm, a clear indication of phrenic nerve paralysis from local infiltration of the infusion.
The ropivacaine infusion was stopped, and the supraclavicular catheter was removed under anesthesia. He was admitted to the hospital for observation, and over the course of 8 to 12 hours his shortness of breath resolved, and his findings on lung examination normalized. Repeat chest radiography 24 hours after his emergency room presentation showed regular positioning of his diaphragm (Figure 2).
RECOGNIZING AND MANAGING PHRENIC NERVE PARALYSIS
The scenario described here illustrates the importance of recognizing symptomatic phrenic nerve paralysis as a result of local infiltration of anesthetic from supraclavicular brachial plexus block. Regional anesthesia is commonly used for perioperative analgesia for minor shoulder surgeries. Because these blocks anesthetize the trunks formed by the C5–T1 nerve roots, infiltration of the anesthetic agent to the proximal nerve roots resulting in phrenic nerve paralysis is a common complication.
Although phrenic nerve paralysis has been reported to some degree in nearly all patients, reports of significant shortness of breath and radiographic evidence of hemidiaphragm are few.1–4 When it occurs, the analgesic regimen must be changed from regional anesthesia to oral or parenteral pain medications. Resolution of symptoms and radiographic abnormalities usually occurs spontaneously.
When available, an ultrasonographically guided approach for supraclavicular brachial plexus blocks is preferred over a blind approach and is associated with a higher success rate and a lower rate of complications.5,6
A potentially life-threatening complication of brachial plexus block is pneumothorax.
Contraindications to brachial plexus block include severe lung disease and previous surgery or interventions with the potential for phrenic nerve injury that could result in bilateral paralysis of the diaphragm. Ultimately, preprocedural chest radiography in selected patients at high risk should be considered to mitigate this risk.
- Tran QH, Clemente A, Doan J, Finlayson RJ. Brachial plexus blocks: a review of approaches and techniques. Can J Anaesth 2007; 54:662–674.
- Mian A, Chaudhry I, Huang R, Rizk E, Tubbs RS, Loukas M. Brachial plexus anesthesia: a review of the relevant anatomy, complications, and anatomical variations. Clin Anat 2014; 27:210–221.
- Knoblanche GE. The incidence and aetiology of phrenic nerve blockade associated with supraclavicular brachial plexus block. Anaesth Intensive Care 1979; 7:346–349.
- Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg 1991; 72:498–503.
- Gelfand HJ, Ouanes JP, Lesley MR, et al. Analgesic efficacy of ultrasound-guided regional anesthesia: a meta-analysis. J Clin Anesth 2011; 23:90–96.
- Sandhu NS, Capan LM. Ultrasound-guided infraclavicular brachial plexus block. Br J Anaesth 2002; 89:254–259.
A 72-year-old man underwent elective ambulatory arthroscopic repair of the right shoulder rotator cuff. To manage postoperative pain, a supraclavicular catheter was placed for brachial plexus block, and he was sent home with a ropivacaine infusion pump.
The next day, he presented to the emergency department with right-sided chest pain and mild shortness of breath. He had normal vital signs and adequate oxygen saturation on room air. On physical examination, breath sounds were decreased at the right lung base, and chest radiography (Figure 1) revealed an isolated elevated right hemidiaphragm, a clear indication of phrenic nerve paralysis from local infiltration of the infusion.
The ropivacaine infusion was stopped, and the supraclavicular catheter was removed under anesthesia. He was admitted to the hospital for observation, and over the course of 8 to 12 hours his shortness of breath resolved, and his findings on lung examination normalized. Repeat chest radiography 24 hours after his emergency room presentation showed regular positioning of his diaphragm (Figure 2).
RECOGNIZING AND MANAGING PHRENIC NERVE PARALYSIS
The scenario described here illustrates the importance of recognizing symptomatic phrenic nerve paralysis as a result of local infiltration of anesthetic from supraclavicular brachial plexus block. Regional anesthesia is commonly used for perioperative analgesia for minor shoulder surgeries. Because these blocks anesthetize the trunks formed by the C5–T1 nerve roots, infiltration of the anesthetic agent to the proximal nerve roots resulting in phrenic nerve paralysis is a common complication.
Although phrenic nerve paralysis has been reported to some degree in nearly all patients, reports of significant shortness of breath and radiographic evidence of hemidiaphragm are few.1–4 When it occurs, the analgesic regimen must be changed from regional anesthesia to oral or parenteral pain medications. Resolution of symptoms and radiographic abnormalities usually occurs spontaneously.
When available, an ultrasonographically guided approach for supraclavicular brachial plexus blocks is preferred over a blind approach and is associated with a higher success rate and a lower rate of complications.5,6
A potentially life-threatening complication of brachial plexus block is pneumothorax.
Contraindications to brachial plexus block include severe lung disease and previous surgery or interventions with the potential for phrenic nerve injury that could result in bilateral paralysis of the diaphragm. Ultimately, preprocedural chest radiography in selected patients at high risk should be considered to mitigate this risk.
A 72-year-old man underwent elective ambulatory arthroscopic repair of the right shoulder rotator cuff. To manage postoperative pain, a supraclavicular catheter was placed for brachial plexus block, and he was sent home with a ropivacaine infusion pump.
The next day, he presented to the emergency department with right-sided chest pain and mild shortness of breath. He had normal vital signs and adequate oxygen saturation on room air. On physical examination, breath sounds were decreased at the right lung base, and chest radiography (Figure 1) revealed an isolated elevated right hemidiaphragm, a clear indication of phrenic nerve paralysis from local infiltration of the infusion.
The ropivacaine infusion was stopped, and the supraclavicular catheter was removed under anesthesia. He was admitted to the hospital for observation, and over the course of 8 to 12 hours his shortness of breath resolved, and his findings on lung examination normalized. Repeat chest radiography 24 hours after his emergency room presentation showed regular positioning of his diaphragm (Figure 2).
RECOGNIZING AND MANAGING PHRENIC NERVE PARALYSIS
The scenario described here illustrates the importance of recognizing symptomatic phrenic nerve paralysis as a result of local infiltration of anesthetic from supraclavicular brachial plexus block. Regional anesthesia is commonly used for perioperative analgesia for minor shoulder surgeries. Because these blocks anesthetize the trunks formed by the C5–T1 nerve roots, infiltration of the anesthetic agent to the proximal nerve roots resulting in phrenic nerve paralysis is a common complication.
Although phrenic nerve paralysis has been reported to some degree in nearly all patients, reports of significant shortness of breath and radiographic evidence of hemidiaphragm are few.1–4 When it occurs, the analgesic regimen must be changed from regional anesthesia to oral or parenteral pain medications. Resolution of symptoms and radiographic abnormalities usually occurs spontaneously.
When available, an ultrasonographically guided approach for supraclavicular brachial plexus blocks is preferred over a blind approach and is associated with a higher success rate and a lower rate of complications.5,6
A potentially life-threatening complication of brachial plexus block is pneumothorax.
Contraindications to brachial plexus block include severe lung disease and previous surgery or interventions with the potential for phrenic nerve injury that could result in bilateral paralysis of the diaphragm. Ultimately, preprocedural chest radiography in selected patients at high risk should be considered to mitigate this risk.
- Tran QH, Clemente A, Doan J, Finlayson RJ. Brachial plexus blocks: a review of approaches and techniques. Can J Anaesth 2007; 54:662–674.
- Mian A, Chaudhry I, Huang R, Rizk E, Tubbs RS, Loukas M. Brachial plexus anesthesia: a review of the relevant anatomy, complications, and anatomical variations. Clin Anat 2014; 27:210–221.
- Knoblanche GE. The incidence and aetiology of phrenic nerve blockade associated with supraclavicular brachial plexus block. Anaesth Intensive Care 1979; 7:346–349.
- Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg 1991; 72:498–503.
- Gelfand HJ, Ouanes JP, Lesley MR, et al. Analgesic efficacy of ultrasound-guided regional anesthesia: a meta-analysis. J Clin Anesth 2011; 23:90–96.
- Sandhu NS, Capan LM. Ultrasound-guided infraclavicular brachial plexus block. Br J Anaesth 2002; 89:254–259.
- Tran QH, Clemente A, Doan J, Finlayson RJ. Brachial plexus blocks: a review of approaches and techniques. Can J Anaesth 2007; 54:662–674.
- Mian A, Chaudhry I, Huang R, Rizk E, Tubbs RS, Loukas M. Brachial plexus anesthesia: a review of the relevant anatomy, complications, and anatomical variations. Clin Anat 2014; 27:210–221.
- Knoblanche GE. The incidence and aetiology of phrenic nerve blockade associated with supraclavicular brachial plexus block. Anaesth Intensive Care 1979; 7:346–349.
- Urmey WF, Talts KH, Sharrock NE. One hundred percent incidence of hemidiaphragmatic paresis associated with interscalene brachial plexus anesthesia as diagnosed by ultrasonography. Anesth Analg 1991; 72:498–503.
- Gelfand HJ, Ouanes JP, Lesley MR, et al. Analgesic efficacy of ultrasound-guided regional anesthesia: a meta-analysis. J Clin Anesth 2011; 23:90–96.
- Sandhu NS, Capan LM. Ultrasound-guided infraclavicular brachial plexus block. Br J Anaesth 2002; 89:254–259.
Fluid Resuscitation in Sepsis: A Systematic Review and Network Meta-Analysis
Clinical question: Is there any difference between different resuscitative fluids (crystalloids or colloids) on mortality in critically ill sepsis patients?
Background: Fluid resuscitation, in addition to antibiotics and source control, is a cornerstone of initial management of sepsis. Resuscitation with crystalloids compared with colloids for critically ill patients has been evaluated in large randomized controlled trials and meta-analyses; however, whether any of these fluid properties translates into a survival advantage, particularly regarding the optimal fluid for resuscitation in critically ill sepsis patients, remains unclear.
Study design: Systematic review, network meta-analysis (NMA).
Setting: Database search in MEDLINE, Embase, ACP Journal Club, Cumulative Index to Nursing and Allied Health Literature (CINAHL), HealthSTAR, the Allied and Complementary Medicine Database (AMED), and the Cochrane Central Register of Controlled Trials (CENTRAL).
Synopsis: Of 9,875 records that involved adult (age =16 years) critically ill patients with severe sepsis or septic shock who required fluid resuscitation, with no restrictions on language or publication date, 14 randomized controlled trials were considered eligible. Interventions studied included any fluid or fluid strategy used for resuscitation compared with another fluid or fluid strategy. The endpoint was 90-day mortality or, if not available, 30-day intensive care unit or hospital mortality, whichever was longest.
The analysis classified fluids as crystalloids or colloids. The relevant analyses were a four-node NMA (crystalloids versus albumin versus hydroxyethyl starch [HES] versus gelatin) and a six-node NMA (crystalloids versus albumin versus HES versus gelatin, with crystalloids divided into balanced or unbalanced and HES divided into low or high molecular weight), and a conventional fixed-effects meta-analytic comparison of crystalloids versus colloids.
In the four-node analysis, the results suggested higher mortality with starches (versus crystalloids) and lower mortality with albumin (versus crystalloids and starches). In the six-node analysis, the results suggested that albumin is superior to saline and low-molecular-weight starch and that balanced crystalloids are superior to saline and starch (both high and low molecular weight).
These results highlight potentially important differences in mortality among solutions; they suggest an advantage of balanced crystalloids versus saline and low- or high-molecular-weight starch, with similar mortality results for balanced crystalloids and albumin. These differences were not detectable using a standard meta-analytic approach directly comparing “any crystalloids versus any colloids.” Biological rationale is consistent with the findings of lower mortality with balanced crystalloid solutions than with saline as it mimics the homeostatic composition of body fluids to a greater extent than unbalanced fluids. These results raise concerns about using unbalanced crystalloids in the acute resuscitation of patients with sepsis.
Bottom line: Among patients with sepsis, resuscitation with balanced crystalloids or albumin is associated with reduced mortality compared to other fluids.
Clinical question: Is there any difference between different resuscitative fluids (crystalloids or colloids) on mortality in critically ill sepsis patients?
Background: Fluid resuscitation, in addition to antibiotics and source control, is a cornerstone of initial management of sepsis. Resuscitation with crystalloids compared with colloids for critically ill patients has been evaluated in large randomized controlled trials and meta-analyses; however, whether any of these fluid properties translates into a survival advantage, particularly regarding the optimal fluid for resuscitation in critically ill sepsis patients, remains unclear.
Study design: Systematic review, network meta-analysis (NMA).
Setting: Database search in MEDLINE, Embase, ACP Journal Club, Cumulative Index to Nursing and Allied Health Literature (CINAHL), HealthSTAR, the Allied and Complementary Medicine Database (AMED), and the Cochrane Central Register of Controlled Trials (CENTRAL).
Synopsis: Of 9,875 records that involved adult (age =16 years) critically ill patients with severe sepsis or septic shock who required fluid resuscitation, with no restrictions on language or publication date, 14 randomized controlled trials were considered eligible. Interventions studied included any fluid or fluid strategy used for resuscitation compared with another fluid or fluid strategy. The endpoint was 90-day mortality or, if not available, 30-day intensive care unit or hospital mortality, whichever was longest.
The analysis classified fluids as crystalloids or colloids. The relevant analyses were a four-node NMA (crystalloids versus albumin versus hydroxyethyl starch [HES] versus gelatin) and a six-node NMA (crystalloids versus albumin versus HES versus gelatin, with crystalloids divided into balanced or unbalanced and HES divided into low or high molecular weight), and a conventional fixed-effects meta-analytic comparison of crystalloids versus colloids.
In the four-node analysis, the results suggested higher mortality with starches (versus crystalloids) and lower mortality with albumin (versus crystalloids and starches). In the six-node analysis, the results suggested that albumin is superior to saline and low-molecular-weight starch and that balanced crystalloids are superior to saline and starch (both high and low molecular weight).
These results highlight potentially important differences in mortality among solutions; they suggest an advantage of balanced crystalloids versus saline and low- or high-molecular-weight starch, with similar mortality results for balanced crystalloids and albumin. These differences were not detectable using a standard meta-analytic approach directly comparing “any crystalloids versus any colloids.” Biological rationale is consistent with the findings of lower mortality with balanced crystalloid solutions than with saline as it mimics the homeostatic composition of body fluids to a greater extent than unbalanced fluids. These results raise concerns about using unbalanced crystalloids in the acute resuscitation of patients with sepsis.
Bottom line: Among patients with sepsis, resuscitation with balanced crystalloids or albumin is associated with reduced mortality compared to other fluids.
Clinical question: Is there any difference between different resuscitative fluids (crystalloids or colloids) on mortality in critically ill sepsis patients?
Background: Fluid resuscitation, in addition to antibiotics and source control, is a cornerstone of initial management of sepsis. Resuscitation with crystalloids compared with colloids for critically ill patients has been evaluated in large randomized controlled trials and meta-analyses; however, whether any of these fluid properties translates into a survival advantage, particularly regarding the optimal fluid for resuscitation in critically ill sepsis patients, remains unclear.
Study design: Systematic review, network meta-analysis (NMA).
Setting: Database search in MEDLINE, Embase, ACP Journal Club, Cumulative Index to Nursing and Allied Health Literature (CINAHL), HealthSTAR, the Allied and Complementary Medicine Database (AMED), and the Cochrane Central Register of Controlled Trials (CENTRAL).
Synopsis: Of 9,875 records that involved adult (age =16 years) critically ill patients with severe sepsis or septic shock who required fluid resuscitation, with no restrictions on language or publication date, 14 randomized controlled trials were considered eligible. Interventions studied included any fluid or fluid strategy used for resuscitation compared with another fluid or fluid strategy. The endpoint was 90-day mortality or, if not available, 30-day intensive care unit or hospital mortality, whichever was longest.
The analysis classified fluids as crystalloids or colloids. The relevant analyses were a four-node NMA (crystalloids versus albumin versus hydroxyethyl starch [HES] versus gelatin) and a six-node NMA (crystalloids versus albumin versus HES versus gelatin, with crystalloids divided into balanced or unbalanced and HES divided into low or high molecular weight), and a conventional fixed-effects meta-analytic comparison of crystalloids versus colloids.
In the four-node analysis, the results suggested higher mortality with starches (versus crystalloids) and lower mortality with albumin (versus crystalloids and starches). In the six-node analysis, the results suggested that albumin is superior to saline and low-molecular-weight starch and that balanced crystalloids are superior to saline and starch (both high and low molecular weight).
These results highlight potentially important differences in mortality among solutions; they suggest an advantage of balanced crystalloids versus saline and low- or high-molecular-weight starch, with similar mortality results for balanced crystalloids and albumin. These differences were not detectable using a standard meta-analytic approach directly comparing “any crystalloids versus any colloids.” Biological rationale is consistent with the findings of lower mortality with balanced crystalloid solutions than with saline as it mimics the homeostatic composition of body fluids to a greater extent than unbalanced fluids. These results raise concerns about using unbalanced crystalloids in the acute resuscitation of patients with sepsis.
Bottom line: Among patients with sepsis, resuscitation with balanced crystalloids or albumin is associated with reduced mortality compared to other fluids.
Medical Consultants Provide Benefits for Hospitalized Surgical Patients
Clinical question: How are medical consultants used for hospitalized surgical patients, and how does this vary among regions and hospitals in the U.S.?
Background: Reimbursement for surgical procedures is moving toward bundled payments, making it increasingly important to understand the use of resources in order to improve efficiency and quality of care.
Study design: Observational, retrospective, cohort study.
Setting: Fee-for-service Medicare patients undergoing colectomy or total hip replacement (THR) at U.S. acute care hospitals.
Synopsis: Using the Medicare Provider Analysis and Review (MEDPAR) File, the Carrier File, and the 2007 American Hospital Association’s annual survey, researchers evaluated a sample of 91,684 colectomy patients at 930 hospitals and 339,319 THR patients at 1,589 hospitals between the ages of 65 and 99 who were enrolled in Medicare parts A and B between 2007 and 2010. Sixty-nine percent of colectomy patients saw a consultant (50% medicine and 56% specialists). Sixty-three percent of THR patients saw a consultant (53% medicine and 24% specialists).
Patient factors for consults included older age, comorbidities, and nonelective admission. Hospital factors for consults included Midwest location, nonteaching, for-profit status, and hospital size. Greater use of consultants was associated with higher rates of post-operative complications.
Additional research on the association between mortality after complications (including type and timing) and number of consultants may help to improve future efficiency and outcomes. Creating a consensus about the use of medical consultants in healthy patients would also be beneficial.
Limitations of the study include a lack of detail on consult indications, unknown effect of pre-operative outpatient medical consults, major differences in median visits by site and surgery type, and the sole use of administrative claims data.
Bottom line: With the procedural fee for service changing to bundled payments, guidelines may be necessary for appropriate use of consultants, to improve both efficiency and quality of care provided by hospitals.
Clinical question: How are medical consultants used for hospitalized surgical patients, and how does this vary among regions and hospitals in the U.S.?
Background: Reimbursement for surgical procedures is moving toward bundled payments, making it increasingly important to understand the use of resources in order to improve efficiency and quality of care.
Study design: Observational, retrospective, cohort study.
Setting: Fee-for-service Medicare patients undergoing colectomy or total hip replacement (THR) at U.S. acute care hospitals.
Synopsis: Using the Medicare Provider Analysis and Review (MEDPAR) File, the Carrier File, and the 2007 American Hospital Association’s annual survey, researchers evaluated a sample of 91,684 colectomy patients at 930 hospitals and 339,319 THR patients at 1,589 hospitals between the ages of 65 and 99 who were enrolled in Medicare parts A and B between 2007 and 2010. Sixty-nine percent of colectomy patients saw a consultant (50% medicine and 56% specialists). Sixty-three percent of THR patients saw a consultant (53% medicine and 24% specialists).
Patient factors for consults included older age, comorbidities, and nonelective admission. Hospital factors for consults included Midwest location, nonteaching, for-profit status, and hospital size. Greater use of consultants was associated with higher rates of post-operative complications.
Additional research on the association between mortality after complications (including type and timing) and number of consultants may help to improve future efficiency and outcomes. Creating a consensus about the use of medical consultants in healthy patients would also be beneficial.
Limitations of the study include a lack of detail on consult indications, unknown effect of pre-operative outpatient medical consults, major differences in median visits by site and surgery type, and the sole use of administrative claims data.
Bottom line: With the procedural fee for service changing to bundled payments, guidelines may be necessary for appropriate use of consultants, to improve both efficiency and quality of care provided by hospitals.
Clinical question: How are medical consultants used for hospitalized surgical patients, and how does this vary among regions and hospitals in the U.S.?
Background: Reimbursement for surgical procedures is moving toward bundled payments, making it increasingly important to understand the use of resources in order to improve efficiency and quality of care.
Study design: Observational, retrospective, cohort study.
Setting: Fee-for-service Medicare patients undergoing colectomy or total hip replacement (THR) at U.S. acute care hospitals.
Synopsis: Using the Medicare Provider Analysis and Review (MEDPAR) File, the Carrier File, and the 2007 American Hospital Association’s annual survey, researchers evaluated a sample of 91,684 colectomy patients at 930 hospitals and 339,319 THR patients at 1,589 hospitals between the ages of 65 and 99 who were enrolled in Medicare parts A and B between 2007 and 2010. Sixty-nine percent of colectomy patients saw a consultant (50% medicine and 56% specialists). Sixty-three percent of THR patients saw a consultant (53% medicine and 24% specialists).
Patient factors for consults included older age, comorbidities, and nonelective admission. Hospital factors for consults included Midwest location, nonteaching, for-profit status, and hospital size. Greater use of consultants was associated with higher rates of post-operative complications.
Additional research on the association between mortality after complications (including type and timing) and number of consultants may help to improve future efficiency and outcomes. Creating a consensus about the use of medical consultants in healthy patients would also be beneficial.
Limitations of the study include a lack of detail on consult indications, unknown effect of pre-operative outpatient medical consults, major differences in median visits by site and surgery type, and the sole use of administrative claims data.
Bottom line: With the procedural fee for service changing to bundled payments, guidelines may be necessary for appropriate use of consultants, to improve both efficiency and quality of care provided by hospitals.
Fluid Resuscitation in Sepsis: Systematic Review and Network Meta-Analysis
Clinical question: Is there any difference between different resuscitative fluids (crystalloids or colloids) on mortality in critically ill sepsis patients?
Background: Fluid resuscitation, in addition to antibiotics and source control, is a cornerstone of initial management of sepsis. Resuscitation with crystalloids compared with colloids for critically ill patients has been evaluated in large randomized, controlled trials and meta-analyses; however, whether any of these fluid properties translates into a survival advantage, particularly regarding the optimal fluid for resuscitation in critically ill sepsis patients, remains unclear.
Study design: Systematic review, network meta-analysis (NMA).
Setting: Database search in MEDLINE, Embase, ACP Journal Club, Cumulative Index to Nursing and Allied Health Literature (CINAHL), HealthSTAR, the Allied and Complementary Medicine Database (AMED), and the Cochrane Central Register of Controlled Trials (CENTRAL).
Synopsis: Of 9,875 records that involved adult (aged ≥16 years) critically ill patients with severe sepsis or septic shock who required fluid resuscitation, with no restrictions on language or publication date, 14 randomized controlled trials were considered eligible. Interventions studied included any fluid or fluid strategy used for resuscitation compared with another fluid or fluid strategy. The endpoint was 90-day mortality or, if not available, 30-day intensive care unit or hospital mortality, whichever was longest. The analysis classified fluids as crystalloids or colloids. The relevant analyses were a four-node NMA (crystalloids vs. albumin vs. HES [hydroxyethyl starch] vs. gelatin) and a six-node NMA (crystalloids vs. albumin vs. HES vs. gelatin, with crystalloids divided into balanced or unbalanced and HES divided into low or high molecular weight), and a conventional fixed-effects meta-analytic comparison of crystalloids vs. colloids.
In the four-node analysis, the results suggested higher mortality with starches (vs. crystalloids) and lower mortality with albumin (vs. crystalloids and starches). In the six-node analysis, the results suggested that albumin is superior to saline and low molecular weight starch, and balanced crystalloids are superior to saline and starch (both high and low molecular weight).
These results highlight potentially important differences in mortality among solutions; it suggests an advantage of balanced crystalloids versus saline and low or high molecular weight starch, with similar mortality results for balanced crystalloids and albumin. These differences were not detectable using a standard meta-analytic approach directly comparing “any crystalloids vs. any colloids.” Biological rationale is consistent with the findings of lower mortality with balanced crystalloid solutions than with saline, as it mimics the homeostatic composition of body fluids to a greater extent than unbalanced fluids.
These results raise concerns about using unbalanced crystalloids in the acute resuscitation of patients with sepsis.
Bottom line: Among patients with sepsis, resuscitation with balanced crystalloids or albumin is associated with reduced mortality compared to other fluids.
Clinical question: Is there any difference between different resuscitative fluids (crystalloids or colloids) on mortality in critically ill sepsis patients?
Background: Fluid resuscitation, in addition to antibiotics and source control, is a cornerstone of initial management of sepsis. Resuscitation with crystalloids compared with colloids for critically ill patients has been evaluated in large randomized, controlled trials and meta-analyses; however, whether any of these fluid properties translates into a survival advantage, particularly regarding the optimal fluid for resuscitation in critically ill sepsis patients, remains unclear.
Study design: Systematic review, network meta-analysis (NMA).
Setting: Database search in MEDLINE, Embase, ACP Journal Club, Cumulative Index to Nursing and Allied Health Literature (CINAHL), HealthSTAR, the Allied and Complementary Medicine Database (AMED), and the Cochrane Central Register of Controlled Trials (CENTRAL).
Synopsis: Of 9,875 records that involved adult (aged ≥16 years) critically ill patients with severe sepsis or septic shock who required fluid resuscitation, with no restrictions on language or publication date, 14 randomized controlled trials were considered eligible. Interventions studied included any fluid or fluid strategy used for resuscitation compared with another fluid or fluid strategy. The endpoint was 90-day mortality or, if not available, 30-day intensive care unit or hospital mortality, whichever was longest. The analysis classified fluids as crystalloids or colloids. The relevant analyses were a four-node NMA (crystalloids vs. albumin vs. HES [hydroxyethyl starch] vs. gelatin) and a six-node NMA (crystalloids vs. albumin vs. HES vs. gelatin, with crystalloids divided into balanced or unbalanced and HES divided into low or high molecular weight), and a conventional fixed-effects meta-analytic comparison of crystalloids vs. colloids.
In the four-node analysis, the results suggested higher mortality with starches (vs. crystalloids) and lower mortality with albumin (vs. crystalloids and starches). In the six-node analysis, the results suggested that albumin is superior to saline and low molecular weight starch, and balanced crystalloids are superior to saline and starch (both high and low molecular weight).
These results highlight potentially important differences in mortality among solutions; it suggests an advantage of balanced crystalloids versus saline and low or high molecular weight starch, with similar mortality results for balanced crystalloids and albumin. These differences were not detectable using a standard meta-analytic approach directly comparing “any crystalloids vs. any colloids.” Biological rationale is consistent with the findings of lower mortality with balanced crystalloid solutions than with saline, as it mimics the homeostatic composition of body fluids to a greater extent than unbalanced fluids.
These results raise concerns about using unbalanced crystalloids in the acute resuscitation of patients with sepsis.
Bottom line: Among patients with sepsis, resuscitation with balanced crystalloids or albumin is associated with reduced mortality compared to other fluids.
Clinical question: Is there any difference between different resuscitative fluids (crystalloids or colloids) on mortality in critically ill sepsis patients?
Background: Fluid resuscitation, in addition to antibiotics and source control, is a cornerstone of initial management of sepsis. Resuscitation with crystalloids compared with colloids for critically ill patients has been evaluated in large randomized, controlled trials and meta-analyses; however, whether any of these fluid properties translates into a survival advantage, particularly regarding the optimal fluid for resuscitation in critically ill sepsis patients, remains unclear.
Study design: Systematic review, network meta-analysis (NMA).
Setting: Database search in MEDLINE, Embase, ACP Journal Club, Cumulative Index to Nursing and Allied Health Literature (CINAHL), HealthSTAR, the Allied and Complementary Medicine Database (AMED), and the Cochrane Central Register of Controlled Trials (CENTRAL).
Synopsis: Of 9,875 records that involved adult (aged ≥16 years) critically ill patients with severe sepsis or septic shock who required fluid resuscitation, with no restrictions on language or publication date, 14 randomized controlled trials were considered eligible. Interventions studied included any fluid or fluid strategy used for resuscitation compared with another fluid or fluid strategy. The endpoint was 90-day mortality or, if not available, 30-day intensive care unit or hospital mortality, whichever was longest. The analysis classified fluids as crystalloids or colloids. The relevant analyses were a four-node NMA (crystalloids vs. albumin vs. HES [hydroxyethyl starch] vs. gelatin) and a six-node NMA (crystalloids vs. albumin vs. HES vs. gelatin, with crystalloids divided into balanced or unbalanced and HES divided into low or high molecular weight), and a conventional fixed-effects meta-analytic comparison of crystalloids vs. colloids.
In the four-node analysis, the results suggested higher mortality with starches (vs. crystalloids) and lower mortality with albumin (vs. crystalloids and starches). In the six-node analysis, the results suggested that albumin is superior to saline and low molecular weight starch, and balanced crystalloids are superior to saline and starch (both high and low molecular weight).
These results highlight potentially important differences in mortality among solutions; it suggests an advantage of balanced crystalloids versus saline and low or high molecular weight starch, with similar mortality results for balanced crystalloids and albumin. These differences were not detectable using a standard meta-analytic approach directly comparing “any crystalloids vs. any colloids.” Biological rationale is consistent with the findings of lower mortality with balanced crystalloid solutions than with saline, as it mimics the homeostatic composition of body fluids to a greater extent than unbalanced fluids.
These results raise concerns about using unbalanced crystalloids in the acute resuscitation of patients with sepsis.
Bottom line: Among patients with sepsis, resuscitation with balanced crystalloids or albumin is associated with reduced mortality compared to other fluids.
Hip Fracture Adverse Outcomes Among Nursing Home Residents
Clinical question: What are the risk factors for mortality and functional decline following hip fracture among nursing home residents?
Background: Little is known about the survival and functional outcomes of nursing home residents who sustain hip fracture. Previous studies on hip fracture have either excluded nursing home residents or have been limited by small sample size.
Study design: Retrospective cohort study.
Setting: Fee-for-service Medicare beneficiaries.
Synopsis: This retrospective study of 60,111 patients residing in nursing homes who were hospitalized for hip fracture between 2005 and 2010 found that 36.2% died within six months. Within this cohort, 53.5% of the patients who did not have total dependence prior to the hip fracture either died or became totally disabled within six months.
Specifically, patients older than 90 years (vs. those younger than 75 years: RR 1.42; P<0.001), with severe cognitive impairment (vs. intact cognition: RR 1.66, P<0.001), and receiving nonoperative management (vs. internal fixation: RR 1.48, P<0.001) had a higher combined risk of death or new total dependence in locomotion within six months of the hip fracture.
The findings suggest there is substantial mortality and functional decline following hip fracture among residents in nursing homes. A profound decrease in activities of daily living across the spectrum was observed. Interestingly, patients who underwent nonoperative treatment, even after risk adjustment, were more likely to have adverse outcomes, suggesting surgery should be considered, if consistent with the patient’s overall goal of care.
Bottom line: Significant mortality and functional decline occurs following hip fracture among nursing home patients. Patients with severe cognitive impairment, older age (more than 90 years), and receiving nonoperative treatment are more likely to die or develop complete dependence in locomotion.
Clinical question: What are the risk factors for mortality and functional decline following hip fracture among nursing home residents?
Background: Little is known about the survival and functional outcomes of nursing home residents who sustain hip fracture. Previous studies on hip fracture have either excluded nursing home residents or have been limited by small sample size.
Study design: Retrospective cohort study.
Setting: Fee-for-service Medicare beneficiaries.
Synopsis: This retrospective study of 60,111 patients residing in nursing homes who were hospitalized for hip fracture between 2005 and 2010 found that 36.2% died within six months. Within this cohort, 53.5% of the patients who did not have total dependence prior to the hip fracture either died or became totally disabled within six months.
Specifically, patients older than 90 years (vs. those younger than 75 years: RR 1.42; P<0.001), with severe cognitive impairment (vs. intact cognition: RR 1.66, P<0.001), and receiving nonoperative management (vs. internal fixation: RR 1.48, P<0.001) had a higher combined risk of death or new total dependence in locomotion within six months of the hip fracture.
The findings suggest there is substantial mortality and functional decline following hip fracture among residents in nursing homes. A profound decrease in activities of daily living across the spectrum was observed. Interestingly, patients who underwent nonoperative treatment, even after risk adjustment, were more likely to have adverse outcomes, suggesting surgery should be considered, if consistent with the patient’s overall goal of care.
Bottom line: Significant mortality and functional decline occurs following hip fracture among nursing home patients. Patients with severe cognitive impairment, older age (more than 90 years), and receiving nonoperative treatment are more likely to die or develop complete dependence in locomotion.
Clinical question: What are the risk factors for mortality and functional decline following hip fracture among nursing home residents?
Background: Little is known about the survival and functional outcomes of nursing home residents who sustain hip fracture. Previous studies on hip fracture have either excluded nursing home residents or have been limited by small sample size.
Study design: Retrospective cohort study.
Setting: Fee-for-service Medicare beneficiaries.
Synopsis: This retrospective study of 60,111 patients residing in nursing homes who were hospitalized for hip fracture between 2005 and 2010 found that 36.2% died within six months. Within this cohort, 53.5% of the patients who did not have total dependence prior to the hip fracture either died or became totally disabled within six months.
Specifically, patients older than 90 years (vs. those younger than 75 years: RR 1.42; P<0.001), with severe cognitive impairment (vs. intact cognition: RR 1.66, P<0.001), and receiving nonoperative management (vs. internal fixation: RR 1.48, P<0.001) had a higher combined risk of death or new total dependence in locomotion within six months of the hip fracture.
The findings suggest there is substantial mortality and functional decline following hip fracture among residents in nursing homes. A profound decrease in activities of daily living across the spectrum was observed. Interestingly, patients who underwent nonoperative treatment, even after risk adjustment, were more likely to have adverse outcomes, suggesting surgery should be considered, if consistent with the patient’s overall goal of care.
Bottom line: Significant mortality and functional decline occurs following hip fracture among nursing home patients. Patients with severe cognitive impairment, older age (more than 90 years), and receiving nonoperative treatment are more likely to die or develop complete dependence in locomotion.
Post-Operative Pneumonia Reduced by Standardization in Noncritical Surgical Patients
Clinical question: What is the long-term effectiveness of a standardized pneumonia prevention program among surgical noncritical inpatients?
Background: Few studies have focused on the prevention of post-operative pneumonia in non-mechanically ventilated patients. The current study describes the effectiveness of an intervention designed to reduce post-operative pneumonia among noncritical patients who did not require mechanical ventilation.
Study design: Retrospective, cohort study.
Setting: University-affiliated VA hospital involving all noncardiac surgical patients.
Synopsis: A standardized pneumonia prevention program was implemented in 2007 in noncritical care settings for noncardiac surgery patients. Post-operative pneumonia rates were compared to pre-intervention and to American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) benchmarks. Rates of post-operative pneumonia following the intervention dropped from 0.78% to 0.44%, a 43% decrease (P=0.01). Both pre- and post-intervention rates were significantly better than those reported in the ACS-NSQIP database (2.56%).
It was proposed that widespread implementation of the program could lead to a 43% reduction of pneumonia cases in the ACS-NSQIP population, which would translate into a cost savings of more than $280 million.
Bottom line: A sustained reduction of post-operative pneumonia among noncritical surgical patients can be achieved by a standardized pneumonia prevention program, which may lead to improved outcomes and substantial cost savings.
Clinical question: What is the long-term effectiveness of a standardized pneumonia prevention program among surgical noncritical inpatients?
Background: Few studies have focused on the prevention of post-operative pneumonia in non-mechanically ventilated patients. The current study describes the effectiveness of an intervention designed to reduce post-operative pneumonia among noncritical patients who did not require mechanical ventilation.
Study design: Retrospective, cohort study.
Setting: University-affiliated VA hospital involving all noncardiac surgical patients.
Synopsis: A standardized pneumonia prevention program was implemented in 2007 in noncritical care settings for noncardiac surgery patients. Post-operative pneumonia rates were compared to pre-intervention and to American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) benchmarks. Rates of post-operative pneumonia following the intervention dropped from 0.78% to 0.44%, a 43% decrease (P=0.01). Both pre- and post-intervention rates were significantly better than those reported in the ACS-NSQIP database (2.56%).
It was proposed that widespread implementation of the program could lead to a 43% reduction of pneumonia cases in the ACS-NSQIP population, which would translate into a cost savings of more than $280 million.
Bottom line: A sustained reduction of post-operative pneumonia among noncritical surgical patients can be achieved by a standardized pneumonia prevention program, which may lead to improved outcomes and substantial cost savings.
Clinical question: What is the long-term effectiveness of a standardized pneumonia prevention program among surgical noncritical inpatients?
Background: Few studies have focused on the prevention of post-operative pneumonia in non-mechanically ventilated patients. The current study describes the effectiveness of an intervention designed to reduce post-operative pneumonia among noncritical patients who did not require mechanical ventilation.
Study design: Retrospective, cohort study.
Setting: University-affiliated VA hospital involving all noncardiac surgical patients.
Synopsis: A standardized pneumonia prevention program was implemented in 2007 in noncritical care settings for noncardiac surgery patients. Post-operative pneumonia rates were compared to pre-intervention and to American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) benchmarks. Rates of post-operative pneumonia following the intervention dropped from 0.78% to 0.44%, a 43% decrease (P=0.01). Both pre- and post-intervention rates were significantly better than those reported in the ACS-NSQIP database (2.56%).
It was proposed that widespread implementation of the program could lead to a 43% reduction of pneumonia cases in the ACS-NSQIP population, which would translate into a cost savings of more than $280 million.
Bottom line: A sustained reduction of post-operative pneumonia among noncritical surgical patients can be achieved by a standardized pneumonia prevention program, which may lead to improved outcomes and substantial cost savings.
Aspirin vs. Anticoagulation for VTE Prevention in Lower Extremity Orthopedic Surgery
Clinical question: What are rates of venous thromboembolism (VTE) and bleeding among adult patients receiving aspirin versus anticoagulants after major lower extremity orthopedic surgery?
Background: VTE is common after hip fracture surgery and elective total knee/hip arthroplasty. National guidelines recommend pharmacologic thromboprophylaxis but leave clinicians to select the specific agents. The efficiency and safety of aspirin in these patient populations, compared to other anticoagulants, has been a source of great controversy.
Study design: Meta-analysis.
Setting: Eight randomized trials in the U.S., Spain, Sweden, and Canada.
Synopsis: The trials included 1,408 subjects; aspirin was compared with other anticoagulants for VTE prevention and bleeding after major lower extremity orthopedic surgery. The primary outcome was the rate of proximal deep vein thrombosis (DVT). The different classes of anticoagulants included warfarin, heparin, low molecular weight heparin (LMWH), and danaparoid. Treatment duration was seven to 21 days with clinical follow-up extended up to six months.
Overall rates of DVT did not differ statistically between aspirin and anticoagulants (10.4% vs. 9.2%); however, the balance of risk versus benefit of aspirin compared to anticoagulation differed according to type of surgery; there was a nonsignificant trend favoring anticoagulation for VTE prevention following hip fracture repair, but no difference was found for knee/hip arthroplasty. The risk of bleeding was lower with aspirin than with anticoagulants following hip fracture repair (3.1% vs. 10%) and knee/hip arthroplasty (3.9% vs. 7.8%).
Rates of pulmonary embolism were too low in all the groups to provide reliable estimates.
Bottom line: Aspirin may be associated with higher risk of VTE following hip fracture repair compared to anticoagulants, although bleeding rates were substantially lower. Aspirin was similarly effective compared to anticoagulants for VTE prevention after knee/hip arthroplasty and may be associated with lower bleeding risk.
Clinical question: What are rates of venous thromboembolism (VTE) and bleeding among adult patients receiving aspirin versus anticoagulants after major lower extremity orthopedic surgery?
Background: VTE is common after hip fracture surgery and elective total knee/hip arthroplasty. National guidelines recommend pharmacologic thromboprophylaxis but leave clinicians to select the specific agents. The efficiency and safety of aspirin in these patient populations, compared to other anticoagulants, has been a source of great controversy.
Study design: Meta-analysis.
Setting: Eight randomized trials in the U.S., Spain, Sweden, and Canada.
Synopsis: The trials included 1,408 subjects; aspirin was compared with other anticoagulants for VTE prevention and bleeding after major lower extremity orthopedic surgery. The primary outcome was the rate of proximal deep vein thrombosis (DVT). The different classes of anticoagulants included warfarin, heparin, low molecular weight heparin (LMWH), and danaparoid. Treatment duration was seven to 21 days with clinical follow-up extended up to six months.
Overall rates of DVT did not differ statistically between aspirin and anticoagulants (10.4% vs. 9.2%); however, the balance of risk versus benefit of aspirin compared to anticoagulation differed according to type of surgery; there was a nonsignificant trend favoring anticoagulation for VTE prevention following hip fracture repair, but no difference was found for knee/hip arthroplasty. The risk of bleeding was lower with aspirin than with anticoagulants following hip fracture repair (3.1% vs. 10%) and knee/hip arthroplasty (3.9% vs. 7.8%).
Rates of pulmonary embolism were too low in all the groups to provide reliable estimates.
Bottom line: Aspirin may be associated with higher risk of VTE following hip fracture repair compared to anticoagulants, although bleeding rates were substantially lower. Aspirin was similarly effective compared to anticoagulants for VTE prevention after knee/hip arthroplasty and may be associated with lower bleeding risk.
Clinical question: What are rates of venous thromboembolism (VTE) and bleeding among adult patients receiving aspirin versus anticoagulants after major lower extremity orthopedic surgery?
Background: VTE is common after hip fracture surgery and elective total knee/hip arthroplasty. National guidelines recommend pharmacologic thromboprophylaxis but leave clinicians to select the specific agents. The efficiency and safety of aspirin in these patient populations, compared to other anticoagulants, has been a source of great controversy.
Study design: Meta-analysis.
Setting: Eight randomized trials in the U.S., Spain, Sweden, and Canada.
Synopsis: The trials included 1,408 subjects; aspirin was compared with other anticoagulants for VTE prevention and bleeding after major lower extremity orthopedic surgery. The primary outcome was the rate of proximal deep vein thrombosis (DVT). The different classes of anticoagulants included warfarin, heparin, low molecular weight heparin (LMWH), and danaparoid. Treatment duration was seven to 21 days with clinical follow-up extended up to six months.
Overall rates of DVT did not differ statistically between aspirin and anticoagulants (10.4% vs. 9.2%); however, the balance of risk versus benefit of aspirin compared to anticoagulation differed according to type of surgery; there was a nonsignificant trend favoring anticoagulation for VTE prevention following hip fracture repair, but no difference was found for knee/hip arthroplasty. The risk of bleeding was lower with aspirin than with anticoagulants following hip fracture repair (3.1% vs. 10%) and knee/hip arthroplasty (3.9% vs. 7.8%).
Rates of pulmonary embolism were too low in all the groups to provide reliable estimates.
Bottom line: Aspirin may be associated with higher risk of VTE following hip fracture repair compared to anticoagulants, although bleeding rates were substantially lower. Aspirin was similarly effective compared to anticoagulants for VTE prevention after knee/hip arthroplasty and may be associated with lower bleeding risk.
Depletive Fluid Management Strategy During Weaning from Mechanical Ventilation Can Lower VAP Rates
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Clinical question: What is the benefit associated with a depletive fluid management strategy on ventilator-associated complication (VAC) and ventilator-associated pneumonia (VAP) during weaning from mechanical ventilation?
Background: VAP is common in the ICU. Pulmonary edema predisposes patients to pneumonia by altering the alveolar microenvironment through enhancement of bacterial colonization and infectivity and a decrease in host bactericidal capacities. A fluid management strategy aimed at lowering lung fluid balance may prove useful in reducing both VAC and VAP.
Study design: Randomized controlled trial.
Setting: Nine ICUs in Europe and South America, between May 2007 and July 2009.
Synopsis: Data from the B-type Natriuretic Peptide for the Management of Weaning (BMW) trial was used to compare the cumulative incidence of VAC and VAP between the biomarker-driven, depletive fluid management group and the usual care group during the 14 days following randomization. The trial enrolled 304 randomized patients, 152 in each group.
Compared with usual care, the interventional strategy was associated with a higher proportion of patients receiving diuretics, in higher doses, resulting in a significantly more negative fluid balance during weaning and a shorter duration of mechanical ventilation. VAC (as defined by worsening oxygenation) occurred in 13.2% of patients during the 14 days following randomization: 17.8% in the usual care group and 8.6% in the interventional group. VAP occurred in 13.5% during the 14 days following randomization: 17.8% in the usual care group and 9.2% in the interventional group.
Bottom line: A biomarker-driven, depletive fluid strategy decreases the cumulative incidence of VAC and VAP.
Limitations of Best Practice Alerts on Curbing Blood Transfusions
Clinical question: Why do providers continue to transfuse blood products outside of recommended guidelines, despite best practice alerts (BPAs)?
Background: There is evidence that a restrictive approach to blood transfusion versus a liberal approach is beneficial in reducing cost, morbidity, and mortality. It is unclear why providers continue to order transfusions outside of recommended guidelines in spite of interruptive prompts.
Study design: Retrospective cohort.
Setting: Academic, tertiary care medical care center in California.
Synopsis: Researchers reviewed 10,642 blood transfusion-triggered BPAs. The BPA led to abortion of only 2% of the transfusions in this study. From the predefined institutional accepted transfusion indication list, acute bleeding was the most common (34%), followed by protocol-driven behaviors in specialty services, i.e., stem cell transplant service.
“Other” accounted for 56% of the responses; of these, only 37% entered a free text comment elaborating on the reason to override. Symptomatic anemia was the most common indication cited for these blood transfusions, followed by peri-operative transfusion and anticipation of imminent discharge. The vast majority of providers who interacted with the BPA were resident physicians (55%).
The major limitation of this study is the substantial portion (>60%) of nonspecific “other” overrides.
Bottom line: Protocol-driven behaviors and subjective indications for transfusion, such as symptomatic anemia, are unlikely to be influenced by BPAs.
Clinical question: Why do providers continue to transfuse blood products outside of recommended guidelines, despite best practice alerts (BPAs)?
Background: There is evidence that a restrictive approach to blood transfusion versus a liberal approach is beneficial in reducing cost, morbidity, and mortality. It is unclear why providers continue to order transfusions outside of recommended guidelines in spite of interruptive prompts.
Study design: Retrospective cohort.
Setting: Academic, tertiary care medical care center in California.
Synopsis: Researchers reviewed 10,642 blood transfusion-triggered BPAs. The BPA led to abortion of only 2% of the transfusions in this study. From the predefined institutional accepted transfusion indication list, acute bleeding was the most common (34%), followed by protocol-driven behaviors in specialty services, i.e., stem cell transplant service.
“Other” accounted for 56% of the responses; of these, only 37% entered a free text comment elaborating on the reason to override. Symptomatic anemia was the most common indication cited for these blood transfusions, followed by peri-operative transfusion and anticipation of imminent discharge. The vast majority of providers who interacted with the BPA were resident physicians (55%).
The major limitation of this study is the substantial portion (>60%) of nonspecific “other” overrides.
Bottom line: Protocol-driven behaviors and subjective indications for transfusion, such as symptomatic anemia, are unlikely to be influenced by BPAs.
Clinical question: Why do providers continue to transfuse blood products outside of recommended guidelines, despite best practice alerts (BPAs)?
Background: There is evidence that a restrictive approach to blood transfusion versus a liberal approach is beneficial in reducing cost, morbidity, and mortality. It is unclear why providers continue to order transfusions outside of recommended guidelines in spite of interruptive prompts.
Study design: Retrospective cohort.
Setting: Academic, tertiary care medical care center in California.
Synopsis: Researchers reviewed 10,642 blood transfusion-triggered BPAs. The BPA led to abortion of only 2% of the transfusions in this study. From the predefined institutional accepted transfusion indication list, acute bleeding was the most common (34%), followed by protocol-driven behaviors in specialty services, i.e., stem cell transplant service.
“Other” accounted for 56% of the responses; of these, only 37% entered a free text comment elaborating on the reason to override. Symptomatic anemia was the most common indication cited for these blood transfusions, followed by peri-operative transfusion and anticipation of imminent discharge. The vast majority of providers who interacted with the BPA were resident physicians (55%).
The major limitation of this study is the substantial portion (>60%) of nonspecific “other” overrides.
Bottom line: Protocol-driven behaviors and subjective indications for transfusion, such as symptomatic anemia, are unlikely to be influenced by BPAs.
Peri-Operative Atrial Fibrillation, Long-Term Risk of Ischemic Stroke
Clinical question: Is there an association between peri-operative AF and long-term risk of ischemic stroke in patients undergoing any type of surgery?
Background: Peri-operative AF is usually viewed as a transient response to physiological stress, and the long-term risk of stroke after peri-operative AF is unclear. The incidence of peri-operative AF ranges widely, from 1% to 40%. Data are scarce regarding the long-term risk of stroke from peri-operative AF in patients undergoing various types of surgery.
Study design: Retrospective cohort.
Setting: Nonfederal California acute care hospitals.
Synopsis: The goal of this study was to evaluate the relationship between peri-operative AF and long-term post-operative ischemic stroke by measuring newly diagnosed AF during the index hospitalization among 1,729,360 adult patients who underwent inpatient cardiac and noncardiac surgeries between 2007 and 2010. The main outcome variable was ischemic stroke in any hospital discharge diagnosis, which was adjusted for age, sex, race, insurance status, and cardiovascular comorbidities (hypertension, diabetes mellitus, coronary heart disease, congestive heart failure, peripheral vascular disease, chronic kidney disease, and chronic obstructive pulmonary disease). Kaplan-Meier survival statistics were used to calculate cumulative rates of stroke after surgery; cumulative stroke rates were stratified by the CHA2DS2VASc score.
Of 1.73 million eligible patients with diagnoses of ischemic strokes after discharge from the index hospitalization for surgery, 24,711 had new-onset peri-operative AF during the index hospitalization, and 13,952 experienced a stroke after discharge.
At one year after hospitalization for cardiac surgery, cumulative rates of stroke were 0.99% in those with peri-operative AF and 0.83% in those without AF. At one year after noncardiac surgery, cumulative rates of stroke were 1.47% in those with peri-operative AF and 0.36% in those without AF.
In a Cox proportional hazards analysis accounting for potential confounders, peri-operative AF was associated with subsequent stroke after both cardiac and noncardiac surgery.
Bottom line: Among patients hospitalized for surgery, peri-operative AF was associated with an increased long-term risk of ischemic stroke, especially following noncardiac surgery.
Clinical question: Is there an association between peri-operative AF and long-term risk of ischemic stroke in patients undergoing any type of surgery?
Background: Peri-operative AF is usually viewed as a transient response to physiological stress, and the long-term risk of stroke after peri-operative AF is unclear. The incidence of peri-operative AF ranges widely, from 1% to 40%. Data are scarce regarding the long-term risk of stroke from peri-operative AF in patients undergoing various types of surgery.
Study design: Retrospective cohort.
Setting: Nonfederal California acute care hospitals.
Synopsis: The goal of this study was to evaluate the relationship between peri-operative AF and long-term post-operative ischemic stroke by measuring newly diagnosed AF during the index hospitalization among 1,729,360 adult patients who underwent inpatient cardiac and noncardiac surgeries between 2007 and 2010. The main outcome variable was ischemic stroke in any hospital discharge diagnosis, which was adjusted for age, sex, race, insurance status, and cardiovascular comorbidities (hypertension, diabetes mellitus, coronary heart disease, congestive heart failure, peripheral vascular disease, chronic kidney disease, and chronic obstructive pulmonary disease). Kaplan-Meier survival statistics were used to calculate cumulative rates of stroke after surgery; cumulative stroke rates were stratified by the CHA2DS2VASc score.
Of 1.73 million eligible patients with diagnoses of ischemic strokes after discharge from the index hospitalization for surgery, 24,711 had new-onset peri-operative AF during the index hospitalization, and 13,952 experienced a stroke after discharge.
At one year after hospitalization for cardiac surgery, cumulative rates of stroke were 0.99% in those with peri-operative AF and 0.83% in those without AF. At one year after noncardiac surgery, cumulative rates of stroke were 1.47% in those with peri-operative AF and 0.36% in those without AF.
In a Cox proportional hazards analysis accounting for potential confounders, peri-operative AF was associated with subsequent stroke after both cardiac and noncardiac surgery.
Bottom line: Among patients hospitalized for surgery, peri-operative AF was associated with an increased long-term risk of ischemic stroke, especially following noncardiac surgery.
Clinical question: Is there an association between peri-operative AF and long-term risk of ischemic stroke in patients undergoing any type of surgery?
Background: Peri-operative AF is usually viewed as a transient response to physiological stress, and the long-term risk of stroke after peri-operative AF is unclear. The incidence of peri-operative AF ranges widely, from 1% to 40%. Data are scarce regarding the long-term risk of stroke from peri-operative AF in patients undergoing various types of surgery.
Study design: Retrospective cohort.
Setting: Nonfederal California acute care hospitals.
Synopsis: The goal of this study was to evaluate the relationship between peri-operative AF and long-term post-operative ischemic stroke by measuring newly diagnosed AF during the index hospitalization among 1,729,360 adult patients who underwent inpatient cardiac and noncardiac surgeries between 2007 and 2010. The main outcome variable was ischemic stroke in any hospital discharge diagnosis, which was adjusted for age, sex, race, insurance status, and cardiovascular comorbidities (hypertension, diabetes mellitus, coronary heart disease, congestive heart failure, peripheral vascular disease, chronic kidney disease, and chronic obstructive pulmonary disease). Kaplan-Meier survival statistics were used to calculate cumulative rates of stroke after surgery; cumulative stroke rates were stratified by the CHA2DS2VASc score.
Of 1.73 million eligible patients with diagnoses of ischemic strokes after discharge from the index hospitalization for surgery, 24,711 had new-onset peri-operative AF during the index hospitalization, and 13,952 experienced a stroke after discharge.
At one year after hospitalization for cardiac surgery, cumulative rates of stroke were 0.99% in those with peri-operative AF and 0.83% in those without AF. At one year after noncardiac surgery, cumulative rates of stroke were 1.47% in those with peri-operative AF and 0.36% in those without AF.
In a Cox proportional hazards analysis accounting for potential confounders, peri-operative AF was associated with subsequent stroke after both cardiac and noncardiac surgery.
Bottom line: Among patients hospitalized for surgery, peri-operative AF was associated with an increased long-term risk of ischemic stroke, especially following noncardiac surgery.