
News

‘Praise Diabetes’: Support programs in Black churches yield lasting A1c changes
Statistically significant reductions in A1c and diabetes distress were seen in the Praise Diabetes Project, a 33-month randomized trial, an...
News
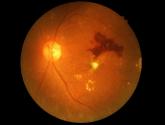
Anti-VEGF injections for diabetic retinopathy linked to mortality risk
Results suggest a need to be “very careful” with treatment choice in certain patients, investigator says, though much more research is needed to...
News

'Full throttle': 'Diabetes Garage' workshops boost Mexican American men's self-management
Infusing diabetes education with concepts and lingo from car culture is a promising approach to improving self-management behaviors, and might...
News

Intervention opens access to care for minority youths with type 1 diabetes
Program adds support for children with diabetes and their families who are struggling because of lack of resources or marginalization in the...
News

Type 1 diabetes amputation rates fall in Sweden, rise in U.S.
Coupled with renal and A1c data, the findings suggest improved prognosis for these patients, Swedish investigators say.
News

Unmanaged diabetes, high blood glucose tied to COVID-19 severity
Findings suggest in part that hospitalized COVID-19 patients need aggressive treatment of hyperglycemia, regardless of the diagnosis of diabetes...
News

FDA approves OTC antihistamine nasal spray
Nasal antihistamines “work quickly, whereas the nasal steroids don’t, and I think a lot of people who go to the drugstore looking for allergy...
News
GI symptoms and chronic fatigue may persist months after COVID-19
Loose stools, somatization, and chronic fatigue risks increased at a mean of 5 months after SARS-CoV-2 infection, suggesting a common...