
News
T-VEC plus pembrolizumab yields promising response rate in phase 2 sarcoma study
About one in three patients had a response, translating into the highest objective response rate seen in a study of unselected sarcoma patients...
News
Start of myeloma therapy may be delayed for women, minorities
Timeliness of treatment should be addressed urgently because of potential effects on disease morbidity, quality of life, and survival.
News
‘Simple’ model predicts severe neutropenia risk in lung cancer patients
New tool performs favorably compared with existing, non–lung-cancer-specific model, though prospective validation is needed.
News
Decreased incidence, survival in low-grade serous ovarian cancer illustrate ‘diagnostic shift’
Relative to serous borderline ovarian tumors, low-grade serous ovarian cancer cases declined precipitously through 2000, with a trend toward...
News

Sharp declines for lung cancer, melanoma deaths fuel record drop in cancer mortality
Reductions in smoking are largely responsible for the lung cancer progress, while immunotherapy and targeted treatments have improved survival in...
News
Fewer interventions after sleeve gastrectomy vs. Roux-en-Y, real-world data show
Balanced by weight loss and health outcomes data, safety results may help inform decision making for prospective patients and physicians,...
News

Turoctocog alfa prevented, treated bleeds in previously untreated pediatric patients with severe hemophilia A
In guardian 4, the first trial in its series to evaluate previously untreated patients, recombinant factor VIII was well tolerated, and...
News
New toxicity subscale measures QOL in cancer patients on checkpoint inhibitors
With further validation, the instrument could become an important tool for evaluation of treatment-related toxicity.
News
Unique T cell populations pinpointed in hepatocellular carcinoma tissue
Cells identified in tumors could represent target of immunotherapy and serve as “prognostic indicator of therapy responsiveness,” according to...
News

CAR T-cell therapy advances in CLL
ORLANDO – The safety and clinical activity of the CD19-directed CAR T-cell agent justifies moving forward with phase 2 investigation, researchers...
News
LOXO-305: Next-gen BTK inhibitor safe and effective in B-cell malignancies
ORLANDO – The antitumor activity of the novel drug was significant among patients with chronic lymphocytic leukemia and mantle cell lymphoma.
News

D-RVd for frontline myeloma looks robust in GRIFFIN trial update
ORLANDO – The depth of response has improved over time, though further follow-up is needed to evaluate the durability of response and progression-...
News
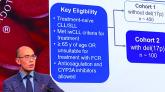
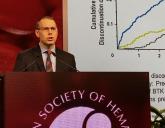
Zanubrutinib achieved high response rate in del(17p) CLL cohort
ORLANDO – The study looked at responses in a cohort of patients with historically poor prognosis and response to chemotherapy.
News

BCL11A-directed gene therapy advances in sickle cell disease
ORLANDO – A phase 2/3 study is planned to assess the gene therapy in a larger group of patients with sickle cell disease.