User login
First EDition: News for and about the practice of emergency medicine
CDC Issues New Opioid Prescribing Guideline
BY SHARON WORCESTER
Frontline Medical News
Nonopioid therapy is the preferred approach for managing chronic pain outside of active cancer, palliative, and end-of-life care, according to a new guideline released by the Centers for Disease Control and Prevention (CDC).
The 12 recommendations included in the guideline, which is available at http://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1er.htm, center around this principle and two others: using the lowest possible effective dosage when opioids are used, and exercising caution and monitoring patients closely when prescribing opioids.
Specifically, the guideline states that “clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient” and that “treatment should be combined with nonpharmacologic and nonopioid therapy, as appropriate.”
The guideline also addresses steps to take before starting or continuing opioid therapy, and drug selection, dosage, duration, follow-up, and discontinuation. Recommendations for assessing risk and addressing harms of opioid use are also included.
The CDC developed the guideline as part of the US government’s urgent response to the epidemic of overdose deaths, which has been fueled by a quadrupling of the prescribing and sales of opioids since 1999, according to a CDC press statement. The guideline’s purpose is to help prevent opioid misuse and overdose.
“The CDC Guideline for Prescribing Opioids for Chronic Pain, United States, 2016 will help primary care providers ensure the safest and most effective treatment for their patients,” according to the statement. The CDC’s director, Dr Tom Frieden, noted that “overprescribing opioids—largely for chronic pain—is a key driver of America’s drug-overdose epidemic.”
In a CDC teleconference marking the release of the guideline, Dr Frieden said it has become increasingly clear that opioids “carry substantial risks but only uncertain benefits, especially compared with other treatments for chronic pain.
“Beginning treatment with an opioid is a momentous decision, and it should only be done with full understanding by both the clinician and the patient of the substantial risks and uncertain benefits involved,” Dr Frieden said. He added that he knows of no other medication “that’s routinely used for a nonfatal condition [and] that kills patients so frequently.
“With more than 250 million prescriptions written each year, it’s so important that doctors understand that any one of those prescriptions could potentially end a patient’s life,” he cautioned.
A 2015 study showed that 1 of every 550 patients treated with opioids for noncancer pain—and 1 of 32 who received the highest doses (more than 200 morphine milligram equivalents per day)—died within 2.5 years of the first prescription.
Dr Frieden noted that opioids do have a place when the potential benefits outweigh the potential harms. “But for most patients—the vast majority of patients—the risks will outweigh the benefits,” he said.
The opioid epidemic is one of the most pressing public health issues in the United States today, said Sylvia M. Burwell, secretary of the Department of Health & Human Services (HHS). A year ago, she announced an HHS initiative to reduce prescription opioid and heroin-related drug overdose, death, and dependence.
“Last year, more Americans died from drug overdoses than car crashes,” Ms Burwell said during the teleconference, noting that families across the nation and from all walks of life have been affected.
Combating the opioid epidemic is a national priority, she said, and the CDC guideline will help in that effort.
“We believe this guideline will help health care professionals provide safer and more effective care for patients dealing with chronic pain, and we also believe it will help these providers drive down the rates of opioid use disorder, overdose, and...death,” she said.
Of note, the guideline stresses the right of patients with chronic pain to receive safe and effective pain management, and focuses on giving primary care providers (PCPs)—who account for about half of all opioid prescriptions—a road map for providing such pain management by increasing the use of effective nonopioid and nonpharmacological therapies.
It was developed through a “rigorous scientific process using the best available scientific evidence, consulting with experts, and listening to comments from the public and partner organizations,” according to the CDC statement. The organization “is dedicated to working with partners to improve the evidence base and will refine the recommendations as new research becomes available.
“In conjunction with the release of the guideline, the CDC has provided a checklist for prescribing opioids for chronic pain (available at http://stacks.cdc.gov/view/cdc/38025), and a Web site (http://www.cdc.gov/drugoverdose/prescribing/resources.html) with additional tools for implementing the recommendations within the guideline.
Patients of PCPs who follow these new guidelines and alter their opioid prescribing practices might subsequently present more frequently to the ED seeking opioid pain medications.
Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. MMWR Recomm Rep. ePub: 15 March 2016. doi:http://dx.doi.org/10.15585/mmwr.rr6501e1er.
Legalization of Marijuana in Colorado Is Followed by an Increase in Marijuana-related ED Visits by Nonresidents
BY JEFF BAUER
FROM N ENGL J MED
"Marijuana tourism”—when individuals travel to a state where marijuana is legal for purpose of consuming the drug—may be responsible for a steep increase in marijuana-related visits by out-of-state residents observed at a Colorado ED from 2013 to 2014. Colorado legalized marijuana in 2012, and retail sales began in 2014.
Researchers looked at the rates of marijuana-related visits (determined by International Classification of Diseases, Ninth Revision codes) to the ED of a single urban academic hospital hospital in Aurora, CO from 2012 to 2014. Researchers compared the rate of such visits by Colorado residents versus out-of-state residents based on the ZIP code patients provided when they registered in the ED.
The rate of marijuana-related ED visits among out-of-state residents roughly doubled from 85 per 10,000 visits in 2013 to 168 per 10,000 visits in 2014. The rate of such visits among Colorado residents did not change significantly during that time: it was 106 per 10,000 visits in 2013 and 112 per 10,000 visits in 2014. From 2012 to 2013—before marijuana was legalized—the rate of marijuana-related ED visits did not change significantly among Colorado residents or out-of-state residents.
Statewide, according to data from the Colorado Hospital Association, the rate of marijuana-related ED visits by out-of-state residents increased from 112 per 10,000 visits in 2013 to 163 per 10,000 visits in 2014. Among Colorado residents, this rate increased from 86 per 10,000 visits in 2013 to 101 per 10,000 visits in 2014.
Kim HS, Hall KE, Genco EK, Van Dyke M, Barker E, Monte AA. Marijuana tourism and emergency department visits in Colorado. N Engl J Med. 2016;374(8):797-798. doi:10.1056/NEJMc1515009.
CDC Issues New Opioid Prescribing Guideline
BY SHARON WORCESTER
Frontline Medical News
Nonopioid therapy is the preferred approach for managing chronic pain outside of active cancer, palliative, and end-of-life care, according to a new guideline released by the Centers for Disease Control and Prevention (CDC).
The 12 recommendations included in the guideline, which is available at http://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1er.htm, center around this principle and two others: using the lowest possible effective dosage when opioids are used, and exercising caution and monitoring patients closely when prescribing opioids.
Specifically, the guideline states that “clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient” and that “treatment should be combined with nonpharmacologic and nonopioid therapy, as appropriate.”
The guideline also addresses steps to take before starting or continuing opioid therapy, and drug selection, dosage, duration, follow-up, and discontinuation. Recommendations for assessing risk and addressing harms of opioid use are also included.
The CDC developed the guideline as part of the US government’s urgent response to the epidemic of overdose deaths, which has been fueled by a quadrupling of the prescribing and sales of opioids since 1999, according to a CDC press statement. The guideline’s purpose is to help prevent opioid misuse and overdose.
“The CDC Guideline for Prescribing Opioids for Chronic Pain, United States, 2016 will help primary care providers ensure the safest and most effective treatment for their patients,” according to the statement. The CDC’s director, Dr Tom Frieden, noted that “overprescribing opioids—largely for chronic pain—is a key driver of America’s drug-overdose epidemic.”
In a CDC teleconference marking the release of the guideline, Dr Frieden said it has become increasingly clear that opioids “carry substantial risks but only uncertain benefits, especially compared with other treatments for chronic pain.
“Beginning treatment with an opioid is a momentous decision, and it should only be done with full understanding by both the clinician and the patient of the substantial risks and uncertain benefits involved,” Dr Frieden said. He added that he knows of no other medication “that’s routinely used for a nonfatal condition [and] that kills patients so frequently.
“With more than 250 million prescriptions written each year, it’s so important that doctors understand that any one of those prescriptions could potentially end a patient’s life,” he cautioned.
A 2015 study showed that 1 of every 550 patients treated with opioids for noncancer pain—and 1 of 32 who received the highest doses (more than 200 morphine milligram equivalents per day)—died within 2.5 years of the first prescription.
Dr Frieden noted that opioids do have a place when the potential benefits outweigh the potential harms. “But for most patients—the vast majority of patients—the risks will outweigh the benefits,” he said.
The opioid epidemic is one of the most pressing public health issues in the United States today, said Sylvia M. Burwell, secretary of the Department of Health & Human Services (HHS). A year ago, she announced an HHS initiative to reduce prescription opioid and heroin-related drug overdose, death, and dependence.
“Last year, more Americans died from drug overdoses than car crashes,” Ms Burwell said during the teleconference, noting that families across the nation and from all walks of life have been affected.
Combating the opioid epidemic is a national priority, she said, and the CDC guideline will help in that effort.
“We believe this guideline will help health care professionals provide safer and more effective care for patients dealing with chronic pain, and we also believe it will help these providers drive down the rates of opioid use disorder, overdose, and...death,” she said.
Of note, the guideline stresses the right of patients with chronic pain to receive safe and effective pain management, and focuses on giving primary care providers (PCPs)—who account for about half of all opioid prescriptions—a road map for providing such pain management by increasing the use of effective nonopioid and nonpharmacological therapies.
It was developed through a “rigorous scientific process using the best available scientific evidence, consulting with experts, and listening to comments from the public and partner organizations,” according to the CDC statement. The organization “is dedicated to working with partners to improve the evidence base and will refine the recommendations as new research becomes available.
“In conjunction with the release of the guideline, the CDC has provided a checklist for prescribing opioids for chronic pain (available at http://stacks.cdc.gov/view/cdc/38025), and a Web site (http://www.cdc.gov/drugoverdose/prescribing/resources.html) with additional tools for implementing the recommendations within the guideline.
Patients of PCPs who follow these new guidelines and alter their opioid prescribing practices might subsequently present more frequently to the ED seeking opioid pain medications.
Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. MMWR Recomm Rep. ePub: 15 March 2016. doi:http://dx.doi.org/10.15585/mmwr.rr6501e1er.
Legalization of Marijuana in Colorado Is Followed by an Increase in Marijuana-related ED Visits by Nonresidents
BY JEFF BAUER
FROM N ENGL J MED
"Marijuana tourism”—when individuals travel to a state where marijuana is legal for purpose of consuming the drug—may be responsible for a steep increase in marijuana-related visits by out-of-state residents observed at a Colorado ED from 2013 to 2014. Colorado legalized marijuana in 2012, and retail sales began in 2014.
Researchers looked at the rates of marijuana-related visits (determined by International Classification of Diseases, Ninth Revision codes) to the ED of a single urban academic hospital hospital in Aurora, CO from 2012 to 2014. Researchers compared the rate of such visits by Colorado residents versus out-of-state residents based on the ZIP code patients provided when they registered in the ED.
The rate of marijuana-related ED visits among out-of-state residents roughly doubled from 85 per 10,000 visits in 2013 to 168 per 10,000 visits in 2014. The rate of such visits among Colorado residents did not change significantly during that time: it was 106 per 10,000 visits in 2013 and 112 per 10,000 visits in 2014. From 2012 to 2013—before marijuana was legalized—the rate of marijuana-related ED visits did not change significantly among Colorado residents or out-of-state residents.
Statewide, according to data from the Colorado Hospital Association, the rate of marijuana-related ED visits by out-of-state residents increased from 112 per 10,000 visits in 2013 to 163 per 10,000 visits in 2014. Among Colorado residents, this rate increased from 86 per 10,000 visits in 2013 to 101 per 10,000 visits in 2014.
Kim HS, Hall KE, Genco EK, Van Dyke M, Barker E, Monte AA. Marijuana tourism and emergency department visits in Colorado. N Engl J Med. 2016;374(8):797-798. doi:10.1056/NEJMc1515009.
CDC Issues New Opioid Prescribing Guideline
BY SHARON WORCESTER
Frontline Medical News
Nonopioid therapy is the preferred approach for managing chronic pain outside of active cancer, palliative, and end-of-life care, according to a new guideline released by the Centers for Disease Control and Prevention (CDC).
The 12 recommendations included in the guideline, which is available at http://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1er.htm, center around this principle and two others: using the lowest possible effective dosage when opioids are used, and exercising caution and monitoring patients closely when prescribing opioids.
Specifically, the guideline states that “clinicians should consider opioid therapy only if expected benefits for both pain and function are anticipated to outweigh risks to the patient” and that “treatment should be combined with nonpharmacologic and nonopioid therapy, as appropriate.”
The guideline also addresses steps to take before starting or continuing opioid therapy, and drug selection, dosage, duration, follow-up, and discontinuation. Recommendations for assessing risk and addressing harms of opioid use are also included.
The CDC developed the guideline as part of the US government’s urgent response to the epidemic of overdose deaths, which has been fueled by a quadrupling of the prescribing and sales of opioids since 1999, according to a CDC press statement. The guideline’s purpose is to help prevent opioid misuse and overdose.
“The CDC Guideline for Prescribing Opioids for Chronic Pain, United States, 2016 will help primary care providers ensure the safest and most effective treatment for their patients,” according to the statement. The CDC’s director, Dr Tom Frieden, noted that “overprescribing opioids—largely for chronic pain—is a key driver of America’s drug-overdose epidemic.”
In a CDC teleconference marking the release of the guideline, Dr Frieden said it has become increasingly clear that opioids “carry substantial risks but only uncertain benefits, especially compared with other treatments for chronic pain.
“Beginning treatment with an opioid is a momentous decision, and it should only be done with full understanding by both the clinician and the patient of the substantial risks and uncertain benefits involved,” Dr Frieden said. He added that he knows of no other medication “that’s routinely used for a nonfatal condition [and] that kills patients so frequently.
“With more than 250 million prescriptions written each year, it’s so important that doctors understand that any one of those prescriptions could potentially end a patient’s life,” he cautioned.
A 2015 study showed that 1 of every 550 patients treated with opioids for noncancer pain—and 1 of 32 who received the highest doses (more than 200 morphine milligram equivalents per day)—died within 2.5 years of the first prescription.
Dr Frieden noted that opioids do have a place when the potential benefits outweigh the potential harms. “But for most patients—the vast majority of patients—the risks will outweigh the benefits,” he said.
The opioid epidemic is one of the most pressing public health issues in the United States today, said Sylvia M. Burwell, secretary of the Department of Health & Human Services (HHS). A year ago, she announced an HHS initiative to reduce prescription opioid and heroin-related drug overdose, death, and dependence.
“Last year, more Americans died from drug overdoses than car crashes,” Ms Burwell said during the teleconference, noting that families across the nation and from all walks of life have been affected.
Combating the opioid epidemic is a national priority, she said, and the CDC guideline will help in that effort.
“We believe this guideline will help health care professionals provide safer and more effective care for patients dealing with chronic pain, and we also believe it will help these providers drive down the rates of opioid use disorder, overdose, and...death,” she said.
Of note, the guideline stresses the right of patients with chronic pain to receive safe and effective pain management, and focuses on giving primary care providers (PCPs)—who account for about half of all opioid prescriptions—a road map for providing such pain management by increasing the use of effective nonopioid and nonpharmacological therapies.
It was developed through a “rigorous scientific process using the best available scientific evidence, consulting with experts, and listening to comments from the public and partner organizations,” according to the CDC statement. The organization “is dedicated to working with partners to improve the evidence base and will refine the recommendations as new research becomes available.
“In conjunction with the release of the guideline, the CDC has provided a checklist for prescribing opioids for chronic pain (available at http://stacks.cdc.gov/view/cdc/38025), and a Web site (http://www.cdc.gov/drugoverdose/prescribing/resources.html) with additional tools for implementing the recommendations within the guideline.
Patients of PCPs who follow these new guidelines and alter their opioid prescribing practices might subsequently present more frequently to the ED seeking opioid pain medications.
Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain—United States, 2016. MMWR Recomm Rep. ePub: 15 March 2016. doi:http://dx.doi.org/10.15585/mmwr.rr6501e1er.
Legalization of Marijuana in Colorado Is Followed by an Increase in Marijuana-related ED Visits by Nonresidents
BY JEFF BAUER
FROM N ENGL J MED
"Marijuana tourism”—when individuals travel to a state where marijuana is legal for purpose of consuming the drug—may be responsible for a steep increase in marijuana-related visits by out-of-state residents observed at a Colorado ED from 2013 to 2014. Colorado legalized marijuana in 2012, and retail sales began in 2014.
Researchers looked at the rates of marijuana-related visits (determined by International Classification of Diseases, Ninth Revision codes) to the ED of a single urban academic hospital hospital in Aurora, CO from 2012 to 2014. Researchers compared the rate of such visits by Colorado residents versus out-of-state residents based on the ZIP code patients provided when they registered in the ED.
The rate of marijuana-related ED visits among out-of-state residents roughly doubled from 85 per 10,000 visits in 2013 to 168 per 10,000 visits in 2014. The rate of such visits among Colorado residents did not change significantly during that time: it was 106 per 10,000 visits in 2013 and 112 per 10,000 visits in 2014. From 2012 to 2013—before marijuana was legalized—the rate of marijuana-related ED visits did not change significantly among Colorado residents or out-of-state residents.
Statewide, according to data from the Colorado Hospital Association, the rate of marijuana-related ED visits by out-of-state residents increased from 112 per 10,000 visits in 2013 to 163 per 10,000 visits in 2014. Among Colorado residents, this rate increased from 86 per 10,000 visits in 2013 to 101 per 10,000 visits in 2014.
Kim HS, Hall KE, Genco EK, Van Dyke M, Barker E, Monte AA. Marijuana tourism and emergency department visits in Colorado. N Engl J Med. 2016;374(8):797-798. doi:10.1056/NEJMc1515009.

First EDition: News for and about the practice of emergency medicine
WHO Declares ‘Public Health Emergency’ for Microcephaly Linked to Zika Virus
BY MARY ELLEN SCHNEIDER
Frontline Medical News
The World Health Organization (WHO) has declared a “public health emergency of international concern” related to the clusters of microcephaly and other neurological complications reported in Brazil and earlier in French Polynesia. Though there is a strong association between these cases and the Zika virus, a causal link still has not been scientifically proven, according to the WHO.
The WHO’s emergency declaration clears the way for the international health community to move forward with a coordinated response. Dr Margaret Chan, WHO Director-General, said her organization plans to take a number of precautionary measures, including improving surveillance and detection of infections, congenital malformations, and neurological complications. They will also work with countries to intensify control of mosquito populations and help expedite the development of diagnostic tests and vaccines to protect at-risk populations.
The recommendations came after a February 1 meeting of the International Health Regulations Emergency Committee, which Dr Chan convened in response to the Zika virus outbreak and the observed increase in neurological disorders and neonatal malformations.
The group of 18 experts advised that the clusters of microcephaly and other complications constitute an “extraordinary event and a public health threat to other parts of the world.” The group did not recommend any restrictions on travel or trade with areas where the Zika virus transmission is ongoing, however.
“At present, the most important protective measures are the control of mosquito populations and the prevention of mosquito bites in at-risk individuals, especially pregnant women,” Dr Chan said during a press briefing.
Dr Chan said it’s unclear how long it will take to determine if Zika virus is causing the uptick in microcephaly and other congenital malformations and neurological abnormalities, but health officials are working to set up case-control studies.
Preparing for Zika Virus Outbreaks
BY DEEPAK CHITNIS
Frontline Medical News
The recent spike in Zika virus cases in Central and South America brings with it the alarming risk— and even the expectation—of outbreaks occuring in the United States. How should US-based clinicians prepare for the inevitable?
“The current outbreaks of Zika virus are the first of their kind in the Americas, so there isn’t a previous history of Zika virus spreading into the [United States],” explained Dr Joy St. John, director of surveillance, disease prevention, and control at the Caribbean Public Health Agency in Trinidad.
But now that the virus has hit the United States, with a confirmed case in Texas and more emerging since then, Dr St. John said the most important thing is for US health care providers to recognize the signs and symptoms of Zika virus infection. Carried and transmitted by the Aedes aegypti species of mosquito, Zika virus symptoms are relatively mild, consisting predominantly of maculopapular rash, fever, arthralgia, myalgia, and conjunctivitis. Only one in five individuals with a Zika virus infection develop symptoms, but patients who present as such and who have traveled to Central or South America in the week prior to the onset of symptoms should be considered likely infected.
“At present, there is no rapid test available for diagnosis of Zika,” said Dr St. John. “Diagnosis is primarily based on detection of viral RNA from clinical serum specimens in acutely ill patients.”
To that end, polymerase chain reaction (PCR) testing can be conducted on serum samples collected within 3 to 5 days of symptom onset. Beyond that, elevated levels of immunoglobulin M antibodies can be confirmed by serology, based on the neutralization, seroconversion or four-fold increase of Zika-specific antibodies in paired samples. However, Dr St. John warned that “Due to the possibility of cross reactivity with other viruses, for example, dengue, it is strongly recommended samples be collected early enough for PCR testing.”
Zika and Pregnancy
Zika virus has now been identified in 14 countries and territories worldwide, and while most infected patients experience relatively mild symptoms, Zika becomes very concerning when it infects a pregnant woman, as there have been cases of microcephaly in children whose mothers were infected with Zika virus during pregnancy. Although the association of microcephaly with Zika virus infection during pregnancy has not been definitively confirmed, the Centers for Disease Control and Prevention (CDC) have already issued a warning to Americans—particularly pregnant women—about traveling to high-risk areas.
“Scientifically, we’re not 100% sure if Zika virus is causing microcephaly, [but] what we’re seeing is in certain Brazilian districts, there’s been a 20-fold increase in rates of microcephaly at the same time that there’s been a lot more Zika virus in pregnant women,” explained Dr Sanjaya Senanayake of Australian National University in Canberra.
According to data from the CDC, 1,248 suspected cases of microcephaly had been reported in Brazil as of November 28, 2015, compared to the annual rate of just 150 to 200 such cases during 2010 through 2014. “Examination of the fetus [and] amniotic fluid, in some cases, has shown Zika virus, so there seems to be an association,” Dr Senanayake clarified, adding that “the [ANVISA – Brazilian Health Surveillance Agency] has told women in certain districts where there’s been a lot of microcephaly not to get pregnant.”
Brazil is set to host millions of guests from around the world as the 2016 Olympics get underway in only a few months’ time. Women who are pregnant or anticipate becoming pregnant should consider the risks if they are planning to travel to Rio de Janeiro. The risk of microcephaly does not apply to infected women who are not pregnant, however, as the CDC states that “Zika virus usually remains in the blood of an infected person for only a few days to a week,” and therefore “does not pose a risk of birth defects for future pregnancies.”
Dr St. Joy also stated that “public health personnel are still cautioning pregnant women to take special care to avoid mosquito bites during their pregnancies,” adding that the “[Pan-American Health Organization] is working on its guidelines for surveillance of congenital abnormalities.”
Clinical Insights
With treatment options so sparse—there is no vaccine or drug available specifically meant to combat a Zika virus infection—what can healthcare providers do for their patients? The CDC advises health care providers to “treat the symptoms,” which means telling patients to stay in bed, stay hydrated, and, most importantly, stay away from aspirins and NSAIDs “until dengue can be ruled out to reduce the risk of hemorrhage.” Acetaminophen or paracetamol are safe to use, in order to mitigate fever symptoms.
Those who are infected are also advised to stay indoors and remain as isolated as possible for at least a week after symptoms first present. While the risk of a domestic outbreak is probably low, Dr St. John said, the more exposure a Zika virus-infected individual has to the outside world, the more likely they are to be bitten by another mosquito, which can then carry and transmit the virus to another person.
“Chikungunya and dengue virus, which are transmitted by the same vectors [as Zika virus], have not managed to establish ongoing transmission in the United States despite repeated importations, [so] it is likely that Zika virus’ spread would follow a similar pattern,” Dr St. John noted.
Though rare, sexual transmission of Zika virus has also been found in at least one case, although it had been previously suspected for some time. In December 2013, a 44-year-old Tahitian man sought treatment for hematospermia. Analysis of his sperm, however, found Zika virus, indicating possible sexual transmission of the virus.
“The observation that [Zika virus] RNA was detectable in urine after viremia clearance in blood suggests that, as found for [dengue] and [West Nile virus] infections, urine samples can yield evidence of [Zika virus] for late diagnosis, but more investigation is needed,” the study concluded.
“The best way to control all this is to control the mosquito,” said Dr Senanayake. “You get a four-for-one deal; not only do you get rid of Zika virus, but also chikungunya, dengue, and yellow fever.” Dr Senanayake added that advanced research is currently underway in mosquito control efforts, including the idea of releasing mosquitoes into the wild that have been genetically modified so they cannot breed.
Now that the Illinois Department of Health has confirmed two new cases of Zika virus infection in that state, with other new cases cropping up in Saint Martin, Guadeloupe, and El Salvador, providers should remain vigilant, taking note of patients who have traveled to afflicted regions and show mosquito bites. Person-to-person transmission is “rare as hen’s teeth,” said Dr Senanayake, which is to say, it is highly unlikely to occur. Nonetheless, he said information and communication is the best way to ensure that Zika virus does not spread widely in the United States.
Study Characterizes Intracerebral Hemorrhage With New Oral Anticoagulants
BY MARY ANN MOON
FROM JAMA NEUROLOGY
Vitals Key clinical point: Intracerebral hemorrhage (ICH) related to new oral anticoagulants frequently involves hematoma expansion and does not appear to respond to prothrombin complex concentrate. Major finding: Mortality was 28%; 65% of survivors had unfavorable outcomes; and substantial hematoma expansion occurred in 38% of patients. Data source: A prospective, multicenter, observational study involving 61 patients treated during a 3-year period in Germany. Disclosures: The RASUNOA registry was supported by the University Hospital Heidelberg. Dr Purrucker reported receiving support from Pfizer unrelated to this study, and his associates reported ties to numerous industry sources. |
Intracerebral hemorrhage related to non–vitamin-K antagonist oral anticoagulants carries a high mortality and frequently involves hematoma expansion, according to a report published online December 14 in JAMA Neurology.1
The characteristics and natural history of acute-phase non–vitamin-K antagonist oral anticoagulant (NOAC)-associated intracerebral hemorrhage “are largely unknown,” and there are no prospective data concerning hematoma expansion or the effectiveness of prothrombin complex concentrate in limiting that expansion by reversing anticoagulation. Nevertheless, current recommendations suggest that clinicians consider administering prothrombin complex concentrate in this patient population, said Dr Jan C. Purrucker of the department of neurology at Heidelberg (Germany) University and his associates.1
Dr Purrucker and his associates performed the ICH substudy of the Registry of Acute Stroke Under New Oral Anticoagulants (RASUNOA), a prospective registry with certified stroke units in Germany. For their substudy, the investigators focused on 61 adults with a mean age of 76 years (range, 46-97 years) who were taking novel anticoagulants (NOACs; [apixaban, dabigatran etexilate, or rivaroxaban]) and had moderate to severe neurologic deficits and a median hematoma volume of 10.8 mL at presentation. Prothrombin complex concentrate was given to 35 (57%).
Mortality was high; 10 (16%) patients died during the acute inpatient stay and 17 (28%) at 3 months. Of the survivors, 65% had an unfavorable outcome. Substantial hematoma expansion—defined as a 33% or greater relative increase or 6 mL or greater absolute increase in intracerebral hemorrhage volume—affected 38% of patients. “This proportion was within the range reported for vitamin-K antagonist–associated intracerebral hemorrhage (36%-56%) and is higher, compared with that related to intracerebral hemorrhage in patients not receiving anticoagulation (12%-26%),” the researchers wrote.
Both larger hematoma volume at baseline (odds ratio [OR], 2.37) and intraventricular extension at baseline (OR, 8.13) strongly correlated with adverse outcomes. In contrast, prothrombin-complex concentrate failed to limit lesion expansion or avert adverse outcomes. This might be because patients given the treatment tended to have more severe initial neurologic deficits and more unfavorable hematoma location than did those who were not given prothrombin complex concentrate. In any case, “our study design, the limited sample size, and the potential for confounding by indication do not allow any [firm] conclusions regarding a potential association between prothrombin-complex concentrate treatment and outcome,” they noted.
It is important to note that in the study by Dr Purrucker and his colleagues, the median time from symptom onset to the first brain imaging was 14 hours and that fully 25% of patients presented for treatment more than 22 hours after noticing their initial symptoms. In contrast, patients with spontaneous hypertensive intracerebral hemorrhage present much earlier, usually within 6 hours. This indicates that the bleeding in NOAC-associated hemorrhagic stroke often is gradual and prolonged, an “oozing” process rather than the explosive type of process seen in spontaneous hemorrhagic stroke.
It is almost certain that if this cohort had undergone imaging at 3 hours rather than at 14 hours after symptom onset, the frequency of hematoma expansion would have approached 100% rather than 38%.
Dr Stephan A. Mayer is at Mount Sinai University, New York. He reported having no relevant financial disclosures. Dr Mayer made these remarks in an editorial accompanying Dr Purrucker’s report (Mayer, SA. Emergency Reversal of Novel Oral Anticoagulants. Help Is on the Way. JAMA Neurol. doi:10.1001/jamaneurol.2015.3884).
FDA Approves Treatment for Chemotherapy, Overdoses, Life-threatening Toxicities
BY ELIZABETH MECHCATIE
Frontline Medical News
Uridine triacetate, a pyrimidine analogue, has been approved for the emergency treatment of fluorouracil or capecitabine overdoses in adults and children, and for patients who develop “certain severe or life-threatening toxicities within 4 days of receiving” these treatments, the Food and Drug Administration (FDA) announced on December 11, 2015.
“Today’s approval is a first-of-its-kind therapy that can potentially save lives following overdose or life-threatening toxicity from these chemotherapy agents,” Dr Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, said in the FDA statement.1 It will be marketed as Vistogard by Wellstat Therapeutics.
Uridine comes in an oral granule formulation that can be mixed into soft foods or, when necessary, administered via a nasogastric or gastrostomy tube, the prescribing information states. The indication is for use after an overdose “regardless of the presence of symptoms,” and for treating “early-onset, severe, or life-threatening toxicity affecting the cardiac or central nervous system, and/or early-onset, unusually severe adverse reactions (eg, gastrointestinal toxicity and/or neutropenia) within 96 hours following the end of fluorouracil or capecitabine administration,” according to the prescribing information.
Uridine blocks cell damage and cell death caused by fluorouracil chemotherapy, according to the statement.
Uridine was evaluated in two studies of 135 adults and children with cancer treated for a fluorouracil or capecitabine overdose or for early-onset severe or life-threatening toxicities within 96 hours after receiving fluorouracil. Among those treated for an overdose, 97% were alive 30 days after treatment, and among those treated for early-onset severe or life-threatening toxicity, 89% were alive 30 days after treatment. In addition, 33% of the patients resumed chemotherapy within 30 days, according to the FDA statement. Diarrhea, vomiting, and nausea were the most common adverse events associated with treatment.
FDA Advisory Committees Support Changing Codeine Contraindications for Children
BY DEEPAK CHITNIS
AT AN FDA ADVISORY COMMITTEE MEETING
SILVER SPRING, MD—Food and Drug Administration advisory committees have voted overwhelmingly to support expanding the current contraindication for codeine to preclude its use for any pain management in all children under age 18 years.
Twenty members of the FDA’s Pulmonary-Allergy Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee voted on December 10 for the contraindication. Six members elected to contraindicate for any pain management in children younger than 12 years old, and another two members voted only to contraindicate for children younger than age 6 years. One committee member voted not to make any changes to the current contraindications for codeine.
The joint advisory panel also voted to contraindicate the use of codeine for the treatment of cough in all children younger than age 18 years by a similarly robust margin: 20 members voted for contraindicating in all pediatric patients, five voted to contraindicate only in patients younger than age 12 years, one voted to contraindicate in children younger than age 6 years, and three members voted not to make any changes at all.
The final voting question, asking whether to remove codeine from the FDA monograph for over-the-counter use in treating cough in children, was almost unanimously supported by the voting members of both committees. One member supported removing codeine from the monograph only for children under age 2 years.
The decision to vote on approving amendments to the contraindications for codeine use—which would affect not just the monogram, but labeling as well—comes on the heels of the FDA announcing last summer that they would be investigating the safety of codeine-containing drugs in children.
The joint advisory panel cited reports of respiratory depression and death in pediatric patients, variability of codeine metabolism based upon CYP2D6 activity, and the fact that “some regulatory agencies have restricted use of codeine for both cough and analgesia in pediatric patients” as their key reasons for considering the changes to current contraindications, according to Dr Sally Seymour, the FDA’s Deputy Director for Safety.
The FDA is not required to follow the advice of its advisory panels. No members of the panel reported any relevant financial conflicts of interest.
80% of Emergency Physicians Say Mental Health Crisis Response Needs Overhaul
BY WHITNEY MCKNIGHT
Frontline Medical News
Vitals Key clinical point: A new model of psychiatric ED care is being developed by the Coalition on Psychiatric Emergencies (COPE), to improve care, outcomes, and net costs. Major finding: 8 in 10 emergency physicians (EPs) believe a lack of training and resources keep them from meeting a growing demand for emergency mental health services. Data source: American College of Emergency Physicians (ACEP) survey of 1,500 EPs nationwide. Disclosures: COPE is underwritten in part by Teva Pharmaceuticals. |
Emergency medicine professionals have teamed up with mental health workers and patient advocates to call for a new model of care for ED patients in mental health crisis.
The Coalition on Psychiatric Emergencies,” is focused on improving the delivery of emergency psychiatric care, and is supported by more than 30 national emergency medicine, mental health, and patient advocate groups, including the ACEP, the American Psychiatric Association, and the National Alliance on Mental Illness (NAMI). The action comes on the heels of a survey that found 80% of 1,500 US EPs think the system for treating people in acute mental health crisis is broken.
“It’s time we think about doing things differently,” Dr Michael Gerardi, COPE Steering Committee Chair and immediate past president of ACEP, said in a statement. “Through this unique collaboration, the Coalition on Psychiatric Emergencies will focus on developing a more unified treatment model and improving the treatment experience for both patients and health care providers. We want to provide the best care for all our patients and reduce health care costs.”
Among its several goals, the coalition seeks to shorten the time between when a person in mental health crisis presents to the ED and is admitted to an inpatient psychiatric bed. In a recent NAMI survey of 1,400 families, 38% waited more than 7 hours in the ED before seeing a mental health professional. For 21% of those families, the wait was more than 10 hours.
The Coalition on Psychiatric Emergencies also seeks adequate education and training for all emergency personnel who care for patients experiencing psychiatric emergencies.
“Emergency department staff need proper training not only on how to handle behavioral health emergencies, but also on how to initiate care for patients who may remain in the ED setting for long periods of time,” Dr Lorenzo Norris, director of inpatient psychiatric services at George Washington University Hospital in Washington, DC, said in an interview. “Establishing these new systems will likely require robust funding efforts.”
‘‘There is a growing need for change. At our hospital, we have definitely seen an uptick in the number of patients seeking emergency psychiatric care,” Dr Norris said. “Our approach has been to hire a clinician whose sole duty is to work collaboratively with patients and ED staff. It’s the first step in our ultimate goal of creating an ED behavioral health team that includes a psychiatrist, an emergency physician, nursing staff, social worker, and others who can provide the patient with comprehensive care at the initial point of contact.”
Currently in the United States, there are no standard protocols for a psychiatric emergency, according to the National Institute of Mental Health. The online survey was conducted within the ACEP membership between July 1 through 31, 2015. The response rate was 6% and the margin of error of 2.5%.
- Study Characterizes Intracerebral Hemorrhage With New Oral Anticoagulants
- Parrucker JC, Haas K, Rizos T, et al. Early Clinical and Radiological Course, Management, and Outcome of Intracerebral Hemorrhage Related to New Oral Anticoagulants. JAMA Neurol. doi:10.1001/jamaneurol.2015.3682.
- FDA Approves Treatment for Chemotherapy, Overdoses, Life-threatening Toxicities
- US Food and Drug Administration. FDA approves first emergency treatment for overdose of certain types of chemotherapy [FDA News Release]. December 11, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm476919.htm.
WHO Declares ‘Public Health Emergency’ for Microcephaly Linked to Zika Virus
BY MARY ELLEN SCHNEIDER
Frontline Medical News
The World Health Organization (WHO) has declared a “public health emergency of international concern” related to the clusters of microcephaly and other neurological complications reported in Brazil and earlier in French Polynesia. Though there is a strong association between these cases and the Zika virus, a causal link still has not been scientifically proven, according to the WHO.
The WHO’s emergency declaration clears the way for the international health community to move forward with a coordinated response. Dr Margaret Chan, WHO Director-General, said her organization plans to take a number of precautionary measures, including improving surveillance and detection of infections, congenital malformations, and neurological complications. They will also work with countries to intensify control of mosquito populations and help expedite the development of diagnostic tests and vaccines to protect at-risk populations.
The recommendations came after a February 1 meeting of the International Health Regulations Emergency Committee, which Dr Chan convened in response to the Zika virus outbreak and the observed increase in neurological disorders and neonatal malformations.
The group of 18 experts advised that the clusters of microcephaly and other complications constitute an “extraordinary event and a public health threat to other parts of the world.” The group did not recommend any restrictions on travel or trade with areas where the Zika virus transmission is ongoing, however.
“At present, the most important protective measures are the control of mosquito populations and the prevention of mosquito bites in at-risk individuals, especially pregnant women,” Dr Chan said during a press briefing.
Dr Chan said it’s unclear how long it will take to determine if Zika virus is causing the uptick in microcephaly and other congenital malformations and neurological abnormalities, but health officials are working to set up case-control studies.
Preparing for Zika Virus Outbreaks
BY DEEPAK CHITNIS
Frontline Medical News
The recent spike in Zika virus cases in Central and South America brings with it the alarming risk— and even the expectation—of outbreaks occuring in the United States. How should US-based clinicians prepare for the inevitable?
“The current outbreaks of Zika virus are the first of their kind in the Americas, so there isn’t a previous history of Zika virus spreading into the [United States],” explained Dr Joy St. John, director of surveillance, disease prevention, and control at the Caribbean Public Health Agency in Trinidad.
But now that the virus has hit the United States, with a confirmed case in Texas and more emerging since then, Dr St. John said the most important thing is for US health care providers to recognize the signs and symptoms of Zika virus infection. Carried and transmitted by the Aedes aegypti species of mosquito, Zika virus symptoms are relatively mild, consisting predominantly of maculopapular rash, fever, arthralgia, myalgia, and conjunctivitis. Only one in five individuals with a Zika virus infection develop symptoms, but patients who present as such and who have traveled to Central or South America in the week prior to the onset of symptoms should be considered likely infected.
“At present, there is no rapid test available for diagnosis of Zika,” said Dr St. John. “Diagnosis is primarily based on detection of viral RNA from clinical serum specimens in acutely ill patients.”
To that end, polymerase chain reaction (PCR) testing can be conducted on serum samples collected within 3 to 5 days of symptom onset. Beyond that, elevated levels of immunoglobulin M antibodies can be confirmed by serology, based on the neutralization, seroconversion or four-fold increase of Zika-specific antibodies in paired samples. However, Dr St. John warned that “Due to the possibility of cross reactivity with other viruses, for example, dengue, it is strongly recommended samples be collected early enough for PCR testing.”
Zika and Pregnancy
Zika virus has now been identified in 14 countries and territories worldwide, and while most infected patients experience relatively mild symptoms, Zika becomes very concerning when it infects a pregnant woman, as there have been cases of microcephaly in children whose mothers were infected with Zika virus during pregnancy. Although the association of microcephaly with Zika virus infection during pregnancy has not been definitively confirmed, the Centers for Disease Control and Prevention (CDC) have already issued a warning to Americans—particularly pregnant women—about traveling to high-risk areas.
“Scientifically, we’re not 100% sure if Zika virus is causing microcephaly, [but] what we’re seeing is in certain Brazilian districts, there’s been a 20-fold increase in rates of microcephaly at the same time that there’s been a lot more Zika virus in pregnant women,” explained Dr Sanjaya Senanayake of Australian National University in Canberra.
According to data from the CDC, 1,248 suspected cases of microcephaly had been reported in Brazil as of November 28, 2015, compared to the annual rate of just 150 to 200 such cases during 2010 through 2014. “Examination of the fetus [and] amniotic fluid, in some cases, has shown Zika virus, so there seems to be an association,” Dr Senanayake clarified, adding that “the [ANVISA – Brazilian Health Surveillance Agency] has told women in certain districts where there’s been a lot of microcephaly not to get pregnant.”
Brazil is set to host millions of guests from around the world as the 2016 Olympics get underway in only a few months’ time. Women who are pregnant or anticipate becoming pregnant should consider the risks if they are planning to travel to Rio de Janeiro. The risk of microcephaly does not apply to infected women who are not pregnant, however, as the CDC states that “Zika virus usually remains in the blood of an infected person for only a few days to a week,” and therefore “does not pose a risk of birth defects for future pregnancies.”
Dr St. Joy also stated that “public health personnel are still cautioning pregnant women to take special care to avoid mosquito bites during their pregnancies,” adding that the “[Pan-American Health Organization] is working on its guidelines for surveillance of congenital abnormalities.”
Clinical Insights
With treatment options so sparse—there is no vaccine or drug available specifically meant to combat a Zika virus infection—what can healthcare providers do for their patients? The CDC advises health care providers to “treat the symptoms,” which means telling patients to stay in bed, stay hydrated, and, most importantly, stay away from aspirins and NSAIDs “until dengue can be ruled out to reduce the risk of hemorrhage.” Acetaminophen or paracetamol are safe to use, in order to mitigate fever symptoms.
Those who are infected are also advised to stay indoors and remain as isolated as possible for at least a week after symptoms first present. While the risk of a domestic outbreak is probably low, Dr St. John said, the more exposure a Zika virus-infected individual has to the outside world, the more likely they are to be bitten by another mosquito, which can then carry and transmit the virus to another person.
“Chikungunya and dengue virus, which are transmitted by the same vectors [as Zika virus], have not managed to establish ongoing transmission in the United States despite repeated importations, [so] it is likely that Zika virus’ spread would follow a similar pattern,” Dr St. John noted.
Though rare, sexual transmission of Zika virus has also been found in at least one case, although it had been previously suspected for some time. In December 2013, a 44-year-old Tahitian man sought treatment for hematospermia. Analysis of his sperm, however, found Zika virus, indicating possible sexual transmission of the virus.
“The observation that [Zika virus] RNA was detectable in urine after viremia clearance in blood suggests that, as found for [dengue] and [West Nile virus] infections, urine samples can yield evidence of [Zika virus] for late diagnosis, but more investigation is needed,” the study concluded.
“The best way to control all this is to control the mosquito,” said Dr Senanayake. “You get a four-for-one deal; not only do you get rid of Zika virus, but also chikungunya, dengue, and yellow fever.” Dr Senanayake added that advanced research is currently underway in mosquito control efforts, including the idea of releasing mosquitoes into the wild that have been genetically modified so they cannot breed.
Now that the Illinois Department of Health has confirmed two new cases of Zika virus infection in that state, with other new cases cropping up in Saint Martin, Guadeloupe, and El Salvador, providers should remain vigilant, taking note of patients who have traveled to afflicted regions and show mosquito bites. Person-to-person transmission is “rare as hen’s teeth,” said Dr Senanayake, which is to say, it is highly unlikely to occur. Nonetheless, he said information and communication is the best way to ensure that Zika virus does not spread widely in the United States.
Study Characterizes Intracerebral Hemorrhage With New Oral Anticoagulants
BY MARY ANN MOON
FROM JAMA NEUROLOGY
Vitals Key clinical point: Intracerebral hemorrhage (ICH) related to new oral anticoagulants frequently involves hematoma expansion and does not appear to respond to prothrombin complex concentrate. Major finding: Mortality was 28%; 65% of survivors had unfavorable outcomes; and substantial hematoma expansion occurred in 38% of patients. Data source: A prospective, multicenter, observational study involving 61 patients treated during a 3-year period in Germany. Disclosures: The RASUNOA registry was supported by the University Hospital Heidelberg. Dr Purrucker reported receiving support from Pfizer unrelated to this study, and his associates reported ties to numerous industry sources. |
Intracerebral hemorrhage related to non–vitamin-K antagonist oral anticoagulants carries a high mortality and frequently involves hematoma expansion, according to a report published online December 14 in JAMA Neurology.1
The characteristics and natural history of acute-phase non–vitamin-K antagonist oral anticoagulant (NOAC)-associated intracerebral hemorrhage “are largely unknown,” and there are no prospective data concerning hematoma expansion or the effectiveness of prothrombin complex concentrate in limiting that expansion by reversing anticoagulation. Nevertheless, current recommendations suggest that clinicians consider administering prothrombin complex concentrate in this patient population, said Dr Jan C. Purrucker of the department of neurology at Heidelberg (Germany) University and his associates.1
Dr Purrucker and his associates performed the ICH substudy of the Registry of Acute Stroke Under New Oral Anticoagulants (RASUNOA), a prospective registry with certified stroke units in Germany. For their substudy, the investigators focused on 61 adults with a mean age of 76 years (range, 46-97 years) who were taking novel anticoagulants (NOACs; [apixaban, dabigatran etexilate, or rivaroxaban]) and had moderate to severe neurologic deficits and a median hematoma volume of 10.8 mL at presentation. Prothrombin complex concentrate was given to 35 (57%).
Mortality was high; 10 (16%) patients died during the acute inpatient stay and 17 (28%) at 3 months. Of the survivors, 65% had an unfavorable outcome. Substantial hematoma expansion—defined as a 33% or greater relative increase or 6 mL or greater absolute increase in intracerebral hemorrhage volume—affected 38% of patients. “This proportion was within the range reported for vitamin-K antagonist–associated intracerebral hemorrhage (36%-56%) and is higher, compared with that related to intracerebral hemorrhage in patients not receiving anticoagulation (12%-26%),” the researchers wrote.
Both larger hematoma volume at baseline (odds ratio [OR], 2.37) and intraventricular extension at baseline (OR, 8.13) strongly correlated with adverse outcomes. In contrast, prothrombin-complex concentrate failed to limit lesion expansion or avert adverse outcomes. This might be because patients given the treatment tended to have more severe initial neurologic deficits and more unfavorable hematoma location than did those who were not given prothrombin complex concentrate. In any case, “our study design, the limited sample size, and the potential for confounding by indication do not allow any [firm] conclusions regarding a potential association between prothrombin-complex concentrate treatment and outcome,” they noted.
It is important to note that in the study by Dr Purrucker and his colleagues, the median time from symptom onset to the first brain imaging was 14 hours and that fully 25% of patients presented for treatment more than 22 hours after noticing their initial symptoms. In contrast, patients with spontaneous hypertensive intracerebral hemorrhage present much earlier, usually within 6 hours. This indicates that the bleeding in NOAC-associated hemorrhagic stroke often is gradual and prolonged, an “oozing” process rather than the explosive type of process seen in spontaneous hemorrhagic stroke.
It is almost certain that if this cohort had undergone imaging at 3 hours rather than at 14 hours after symptom onset, the frequency of hematoma expansion would have approached 100% rather than 38%.
Dr Stephan A. Mayer is at Mount Sinai University, New York. He reported having no relevant financial disclosures. Dr Mayer made these remarks in an editorial accompanying Dr Purrucker’s report (Mayer, SA. Emergency Reversal of Novel Oral Anticoagulants. Help Is on the Way. JAMA Neurol. doi:10.1001/jamaneurol.2015.3884).
FDA Approves Treatment for Chemotherapy, Overdoses, Life-threatening Toxicities
BY ELIZABETH MECHCATIE
Frontline Medical News
Uridine triacetate, a pyrimidine analogue, has been approved for the emergency treatment of fluorouracil or capecitabine overdoses in adults and children, and for patients who develop “certain severe or life-threatening toxicities within 4 days of receiving” these treatments, the Food and Drug Administration (FDA) announced on December 11, 2015.
“Today’s approval is a first-of-its-kind therapy that can potentially save lives following overdose or life-threatening toxicity from these chemotherapy agents,” Dr Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, said in the FDA statement.1 It will be marketed as Vistogard by Wellstat Therapeutics.
Uridine comes in an oral granule formulation that can be mixed into soft foods or, when necessary, administered via a nasogastric or gastrostomy tube, the prescribing information states. The indication is for use after an overdose “regardless of the presence of symptoms,” and for treating “early-onset, severe, or life-threatening toxicity affecting the cardiac or central nervous system, and/or early-onset, unusually severe adverse reactions (eg, gastrointestinal toxicity and/or neutropenia) within 96 hours following the end of fluorouracil or capecitabine administration,” according to the prescribing information.
Uridine blocks cell damage and cell death caused by fluorouracil chemotherapy, according to the statement.
Uridine was evaluated in two studies of 135 adults and children with cancer treated for a fluorouracil or capecitabine overdose or for early-onset severe or life-threatening toxicities within 96 hours after receiving fluorouracil. Among those treated for an overdose, 97% were alive 30 days after treatment, and among those treated for early-onset severe or life-threatening toxicity, 89% were alive 30 days after treatment. In addition, 33% of the patients resumed chemotherapy within 30 days, according to the FDA statement. Diarrhea, vomiting, and nausea were the most common adverse events associated with treatment.
FDA Advisory Committees Support Changing Codeine Contraindications for Children
BY DEEPAK CHITNIS
AT AN FDA ADVISORY COMMITTEE MEETING
SILVER SPRING, MD—Food and Drug Administration advisory committees have voted overwhelmingly to support expanding the current contraindication for codeine to preclude its use for any pain management in all children under age 18 years.
Twenty members of the FDA’s Pulmonary-Allergy Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee voted on December 10 for the contraindication. Six members elected to contraindicate for any pain management in children younger than 12 years old, and another two members voted only to contraindicate for children younger than age 6 years. One committee member voted not to make any changes to the current contraindications for codeine.
The joint advisory panel also voted to contraindicate the use of codeine for the treatment of cough in all children younger than age 18 years by a similarly robust margin: 20 members voted for contraindicating in all pediatric patients, five voted to contraindicate only in patients younger than age 12 years, one voted to contraindicate in children younger than age 6 years, and three members voted not to make any changes at all.
The final voting question, asking whether to remove codeine from the FDA monograph for over-the-counter use in treating cough in children, was almost unanimously supported by the voting members of both committees. One member supported removing codeine from the monograph only for children under age 2 years.
The decision to vote on approving amendments to the contraindications for codeine use—which would affect not just the monogram, but labeling as well—comes on the heels of the FDA announcing last summer that they would be investigating the safety of codeine-containing drugs in children.
The joint advisory panel cited reports of respiratory depression and death in pediatric patients, variability of codeine metabolism based upon CYP2D6 activity, and the fact that “some regulatory agencies have restricted use of codeine for both cough and analgesia in pediatric patients” as their key reasons for considering the changes to current contraindications, according to Dr Sally Seymour, the FDA’s Deputy Director for Safety.
The FDA is not required to follow the advice of its advisory panels. No members of the panel reported any relevant financial conflicts of interest.
80% of Emergency Physicians Say Mental Health Crisis Response Needs Overhaul
BY WHITNEY MCKNIGHT
Frontline Medical News
Vitals Key clinical point: A new model of psychiatric ED care is being developed by the Coalition on Psychiatric Emergencies (COPE), to improve care, outcomes, and net costs. Major finding: 8 in 10 emergency physicians (EPs) believe a lack of training and resources keep them from meeting a growing demand for emergency mental health services. Data source: American College of Emergency Physicians (ACEP) survey of 1,500 EPs nationwide. Disclosures: COPE is underwritten in part by Teva Pharmaceuticals. |
Emergency medicine professionals have teamed up with mental health workers and patient advocates to call for a new model of care for ED patients in mental health crisis.
The Coalition on Psychiatric Emergencies,” is focused on improving the delivery of emergency psychiatric care, and is supported by more than 30 national emergency medicine, mental health, and patient advocate groups, including the ACEP, the American Psychiatric Association, and the National Alliance on Mental Illness (NAMI). The action comes on the heels of a survey that found 80% of 1,500 US EPs think the system for treating people in acute mental health crisis is broken.
“It’s time we think about doing things differently,” Dr Michael Gerardi, COPE Steering Committee Chair and immediate past president of ACEP, said in a statement. “Through this unique collaboration, the Coalition on Psychiatric Emergencies will focus on developing a more unified treatment model and improving the treatment experience for both patients and health care providers. We want to provide the best care for all our patients and reduce health care costs.”
Among its several goals, the coalition seeks to shorten the time between when a person in mental health crisis presents to the ED and is admitted to an inpatient psychiatric bed. In a recent NAMI survey of 1,400 families, 38% waited more than 7 hours in the ED before seeing a mental health professional. For 21% of those families, the wait was more than 10 hours.
The Coalition on Psychiatric Emergencies also seeks adequate education and training for all emergency personnel who care for patients experiencing psychiatric emergencies.
“Emergency department staff need proper training not only on how to handle behavioral health emergencies, but also on how to initiate care for patients who may remain in the ED setting for long periods of time,” Dr Lorenzo Norris, director of inpatient psychiatric services at George Washington University Hospital in Washington, DC, said in an interview. “Establishing these new systems will likely require robust funding efforts.”
‘‘There is a growing need for change. At our hospital, we have definitely seen an uptick in the number of patients seeking emergency psychiatric care,” Dr Norris said. “Our approach has been to hire a clinician whose sole duty is to work collaboratively with patients and ED staff. It’s the first step in our ultimate goal of creating an ED behavioral health team that includes a psychiatrist, an emergency physician, nursing staff, social worker, and others who can provide the patient with comprehensive care at the initial point of contact.”
Currently in the United States, there are no standard protocols for a psychiatric emergency, according to the National Institute of Mental Health. The online survey was conducted within the ACEP membership between July 1 through 31, 2015. The response rate was 6% and the margin of error of 2.5%.
WHO Declares ‘Public Health Emergency’ for Microcephaly Linked to Zika Virus
BY MARY ELLEN SCHNEIDER
Frontline Medical News
The World Health Organization (WHO) has declared a “public health emergency of international concern” related to the clusters of microcephaly and other neurological complications reported in Brazil and earlier in French Polynesia. Though there is a strong association between these cases and the Zika virus, a causal link still has not been scientifically proven, according to the WHO.
The WHO’s emergency declaration clears the way for the international health community to move forward with a coordinated response. Dr Margaret Chan, WHO Director-General, said her organization plans to take a number of precautionary measures, including improving surveillance and detection of infections, congenital malformations, and neurological complications. They will also work with countries to intensify control of mosquito populations and help expedite the development of diagnostic tests and vaccines to protect at-risk populations.
The recommendations came after a February 1 meeting of the International Health Regulations Emergency Committee, which Dr Chan convened in response to the Zika virus outbreak and the observed increase in neurological disorders and neonatal malformations.
The group of 18 experts advised that the clusters of microcephaly and other complications constitute an “extraordinary event and a public health threat to other parts of the world.” The group did not recommend any restrictions on travel or trade with areas where the Zika virus transmission is ongoing, however.
“At present, the most important protective measures are the control of mosquito populations and the prevention of mosquito bites in at-risk individuals, especially pregnant women,” Dr Chan said during a press briefing.
Dr Chan said it’s unclear how long it will take to determine if Zika virus is causing the uptick in microcephaly and other congenital malformations and neurological abnormalities, but health officials are working to set up case-control studies.
Preparing for Zika Virus Outbreaks
BY DEEPAK CHITNIS
Frontline Medical News
The recent spike in Zika virus cases in Central and South America brings with it the alarming risk— and even the expectation—of outbreaks occuring in the United States. How should US-based clinicians prepare for the inevitable?
“The current outbreaks of Zika virus are the first of their kind in the Americas, so there isn’t a previous history of Zika virus spreading into the [United States],” explained Dr Joy St. John, director of surveillance, disease prevention, and control at the Caribbean Public Health Agency in Trinidad.
But now that the virus has hit the United States, with a confirmed case in Texas and more emerging since then, Dr St. John said the most important thing is for US health care providers to recognize the signs and symptoms of Zika virus infection. Carried and transmitted by the Aedes aegypti species of mosquito, Zika virus symptoms are relatively mild, consisting predominantly of maculopapular rash, fever, arthralgia, myalgia, and conjunctivitis. Only one in five individuals with a Zika virus infection develop symptoms, but patients who present as such and who have traveled to Central or South America in the week prior to the onset of symptoms should be considered likely infected.
“At present, there is no rapid test available for diagnosis of Zika,” said Dr St. John. “Diagnosis is primarily based on detection of viral RNA from clinical serum specimens in acutely ill patients.”
To that end, polymerase chain reaction (PCR) testing can be conducted on serum samples collected within 3 to 5 days of symptom onset. Beyond that, elevated levels of immunoglobulin M antibodies can be confirmed by serology, based on the neutralization, seroconversion or four-fold increase of Zika-specific antibodies in paired samples. However, Dr St. John warned that “Due to the possibility of cross reactivity with other viruses, for example, dengue, it is strongly recommended samples be collected early enough for PCR testing.”
Zika and Pregnancy
Zika virus has now been identified in 14 countries and territories worldwide, and while most infected patients experience relatively mild symptoms, Zika becomes very concerning when it infects a pregnant woman, as there have been cases of microcephaly in children whose mothers were infected with Zika virus during pregnancy. Although the association of microcephaly with Zika virus infection during pregnancy has not been definitively confirmed, the Centers for Disease Control and Prevention (CDC) have already issued a warning to Americans—particularly pregnant women—about traveling to high-risk areas.
“Scientifically, we’re not 100% sure if Zika virus is causing microcephaly, [but] what we’re seeing is in certain Brazilian districts, there’s been a 20-fold increase in rates of microcephaly at the same time that there’s been a lot more Zika virus in pregnant women,” explained Dr Sanjaya Senanayake of Australian National University in Canberra.
According to data from the CDC, 1,248 suspected cases of microcephaly had been reported in Brazil as of November 28, 2015, compared to the annual rate of just 150 to 200 such cases during 2010 through 2014. “Examination of the fetus [and] amniotic fluid, in some cases, has shown Zika virus, so there seems to be an association,” Dr Senanayake clarified, adding that “the [ANVISA – Brazilian Health Surveillance Agency] has told women in certain districts where there’s been a lot of microcephaly not to get pregnant.”
Brazil is set to host millions of guests from around the world as the 2016 Olympics get underway in only a few months’ time. Women who are pregnant or anticipate becoming pregnant should consider the risks if they are planning to travel to Rio de Janeiro. The risk of microcephaly does not apply to infected women who are not pregnant, however, as the CDC states that “Zika virus usually remains in the blood of an infected person for only a few days to a week,” and therefore “does not pose a risk of birth defects for future pregnancies.”
Dr St. Joy also stated that “public health personnel are still cautioning pregnant women to take special care to avoid mosquito bites during their pregnancies,” adding that the “[Pan-American Health Organization] is working on its guidelines for surveillance of congenital abnormalities.”
Clinical Insights
With treatment options so sparse—there is no vaccine or drug available specifically meant to combat a Zika virus infection—what can healthcare providers do for their patients? The CDC advises health care providers to “treat the symptoms,” which means telling patients to stay in bed, stay hydrated, and, most importantly, stay away from aspirins and NSAIDs “until dengue can be ruled out to reduce the risk of hemorrhage.” Acetaminophen or paracetamol are safe to use, in order to mitigate fever symptoms.
Those who are infected are also advised to stay indoors and remain as isolated as possible for at least a week after symptoms first present. While the risk of a domestic outbreak is probably low, Dr St. John said, the more exposure a Zika virus-infected individual has to the outside world, the more likely they are to be bitten by another mosquito, which can then carry and transmit the virus to another person.
“Chikungunya and dengue virus, which are transmitted by the same vectors [as Zika virus], have not managed to establish ongoing transmission in the United States despite repeated importations, [so] it is likely that Zika virus’ spread would follow a similar pattern,” Dr St. John noted.
Though rare, sexual transmission of Zika virus has also been found in at least one case, although it had been previously suspected for some time. In December 2013, a 44-year-old Tahitian man sought treatment for hematospermia. Analysis of his sperm, however, found Zika virus, indicating possible sexual transmission of the virus.
“The observation that [Zika virus] RNA was detectable in urine after viremia clearance in blood suggests that, as found for [dengue] and [West Nile virus] infections, urine samples can yield evidence of [Zika virus] for late diagnosis, but more investigation is needed,” the study concluded.
“The best way to control all this is to control the mosquito,” said Dr Senanayake. “You get a four-for-one deal; not only do you get rid of Zika virus, but also chikungunya, dengue, and yellow fever.” Dr Senanayake added that advanced research is currently underway in mosquito control efforts, including the idea of releasing mosquitoes into the wild that have been genetically modified so they cannot breed.
Now that the Illinois Department of Health has confirmed two new cases of Zika virus infection in that state, with other new cases cropping up in Saint Martin, Guadeloupe, and El Salvador, providers should remain vigilant, taking note of patients who have traveled to afflicted regions and show mosquito bites. Person-to-person transmission is “rare as hen’s teeth,” said Dr Senanayake, which is to say, it is highly unlikely to occur. Nonetheless, he said information and communication is the best way to ensure that Zika virus does not spread widely in the United States.
Study Characterizes Intracerebral Hemorrhage With New Oral Anticoagulants
BY MARY ANN MOON
FROM JAMA NEUROLOGY
Vitals Key clinical point: Intracerebral hemorrhage (ICH) related to new oral anticoagulants frequently involves hematoma expansion and does not appear to respond to prothrombin complex concentrate. Major finding: Mortality was 28%; 65% of survivors had unfavorable outcomes; and substantial hematoma expansion occurred in 38% of patients. Data source: A prospective, multicenter, observational study involving 61 patients treated during a 3-year period in Germany. Disclosures: The RASUNOA registry was supported by the University Hospital Heidelberg. Dr Purrucker reported receiving support from Pfizer unrelated to this study, and his associates reported ties to numerous industry sources. |
Intracerebral hemorrhage related to non–vitamin-K antagonist oral anticoagulants carries a high mortality and frequently involves hematoma expansion, according to a report published online December 14 in JAMA Neurology.1
The characteristics and natural history of acute-phase non–vitamin-K antagonist oral anticoagulant (NOAC)-associated intracerebral hemorrhage “are largely unknown,” and there are no prospective data concerning hematoma expansion or the effectiveness of prothrombin complex concentrate in limiting that expansion by reversing anticoagulation. Nevertheless, current recommendations suggest that clinicians consider administering prothrombin complex concentrate in this patient population, said Dr Jan C. Purrucker of the department of neurology at Heidelberg (Germany) University and his associates.1
Dr Purrucker and his associates performed the ICH substudy of the Registry of Acute Stroke Under New Oral Anticoagulants (RASUNOA), a prospective registry with certified stroke units in Germany. For their substudy, the investigators focused on 61 adults with a mean age of 76 years (range, 46-97 years) who were taking novel anticoagulants (NOACs; [apixaban, dabigatran etexilate, or rivaroxaban]) and had moderate to severe neurologic deficits and a median hematoma volume of 10.8 mL at presentation. Prothrombin complex concentrate was given to 35 (57%).
Mortality was high; 10 (16%) patients died during the acute inpatient stay and 17 (28%) at 3 months. Of the survivors, 65% had an unfavorable outcome. Substantial hematoma expansion—defined as a 33% or greater relative increase or 6 mL or greater absolute increase in intracerebral hemorrhage volume—affected 38% of patients. “This proportion was within the range reported for vitamin-K antagonist–associated intracerebral hemorrhage (36%-56%) and is higher, compared with that related to intracerebral hemorrhage in patients not receiving anticoagulation (12%-26%),” the researchers wrote.
Both larger hematoma volume at baseline (odds ratio [OR], 2.37) and intraventricular extension at baseline (OR, 8.13) strongly correlated with adverse outcomes. In contrast, prothrombin-complex concentrate failed to limit lesion expansion or avert adverse outcomes. This might be because patients given the treatment tended to have more severe initial neurologic deficits and more unfavorable hematoma location than did those who were not given prothrombin complex concentrate. In any case, “our study design, the limited sample size, and the potential for confounding by indication do not allow any [firm] conclusions regarding a potential association between prothrombin-complex concentrate treatment and outcome,” they noted.
It is important to note that in the study by Dr Purrucker and his colleagues, the median time from symptom onset to the first brain imaging was 14 hours and that fully 25% of patients presented for treatment more than 22 hours after noticing their initial symptoms. In contrast, patients with spontaneous hypertensive intracerebral hemorrhage present much earlier, usually within 6 hours. This indicates that the bleeding in NOAC-associated hemorrhagic stroke often is gradual and prolonged, an “oozing” process rather than the explosive type of process seen in spontaneous hemorrhagic stroke.
It is almost certain that if this cohort had undergone imaging at 3 hours rather than at 14 hours after symptom onset, the frequency of hematoma expansion would have approached 100% rather than 38%.
Dr Stephan A. Mayer is at Mount Sinai University, New York. He reported having no relevant financial disclosures. Dr Mayer made these remarks in an editorial accompanying Dr Purrucker’s report (Mayer, SA. Emergency Reversal of Novel Oral Anticoagulants. Help Is on the Way. JAMA Neurol. doi:10.1001/jamaneurol.2015.3884).
FDA Approves Treatment for Chemotherapy, Overdoses, Life-threatening Toxicities
BY ELIZABETH MECHCATIE
Frontline Medical News
Uridine triacetate, a pyrimidine analogue, has been approved for the emergency treatment of fluorouracil or capecitabine overdoses in adults and children, and for patients who develop “certain severe or life-threatening toxicities within 4 days of receiving” these treatments, the Food and Drug Administration (FDA) announced on December 11, 2015.
“Today’s approval is a first-of-its-kind therapy that can potentially save lives following overdose or life-threatening toxicity from these chemotherapy agents,” Dr Richard Pazdur, director of the office of hematology and oncology products in the FDA’s Center for Drug Evaluation and Research, said in the FDA statement.1 It will be marketed as Vistogard by Wellstat Therapeutics.
Uridine comes in an oral granule formulation that can be mixed into soft foods or, when necessary, administered via a nasogastric or gastrostomy tube, the prescribing information states. The indication is for use after an overdose “regardless of the presence of symptoms,” and for treating “early-onset, severe, or life-threatening toxicity affecting the cardiac or central nervous system, and/or early-onset, unusually severe adverse reactions (eg, gastrointestinal toxicity and/or neutropenia) within 96 hours following the end of fluorouracil or capecitabine administration,” according to the prescribing information.
Uridine blocks cell damage and cell death caused by fluorouracil chemotherapy, according to the statement.
Uridine was evaluated in two studies of 135 adults and children with cancer treated for a fluorouracil or capecitabine overdose or for early-onset severe or life-threatening toxicities within 96 hours after receiving fluorouracil. Among those treated for an overdose, 97% were alive 30 days after treatment, and among those treated for early-onset severe or life-threatening toxicity, 89% were alive 30 days after treatment. In addition, 33% of the patients resumed chemotherapy within 30 days, according to the FDA statement. Diarrhea, vomiting, and nausea were the most common adverse events associated with treatment.
FDA Advisory Committees Support Changing Codeine Contraindications for Children
BY DEEPAK CHITNIS
AT AN FDA ADVISORY COMMITTEE MEETING
SILVER SPRING, MD—Food and Drug Administration advisory committees have voted overwhelmingly to support expanding the current contraindication for codeine to preclude its use for any pain management in all children under age 18 years.
Twenty members of the FDA’s Pulmonary-Allergy Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee voted on December 10 for the contraindication. Six members elected to contraindicate for any pain management in children younger than 12 years old, and another two members voted only to contraindicate for children younger than age 6 years. One committee member voted not to make any changes to the current contraindications for codeine.
The joint advisory panel also voted to contraindicate the use of codeine for the treatment of cough in all children younger than age 18 years by a similarly robust margin: 20 members voted for contraindicating in all pediatric patients, five voted to contraindicate only in patients younger than age 12 years, one voted to contraindicate in children younger than age 6 years, and three members voted not to make any changes at all.
The final voting question, asking whether to remove codeine from the FDA monograph for over-the-counter use in treating cough in children, was almost unanimously supported by the voting members of both committees. One member supported removing codeine from the monograph only for children under age 2 years.
The decision to vote on approving amendments to the contraindications for codeine use—which would affect not just the monogram, but labeling as well—comes on the heels of the FDA announcing last summer that they would be investigating the safety of codeine-containing drugs in children.
The joint advisory panel cited reports of respiratory depression and death in pediatric patients, variability of codeine metabolism based upon CYP2D6 activity, and the fact that “some regulatory agencies have restricted use of codeine for both cough and analgesia in pediatric patients” as their key reasons for considering the changes to current contraindications, according to Dr Sally Seymour, the FDA’s Deputy Director for Safety.
The FDA is not required to follow the advice of its advisory panels. No members of the panel reported any relevant financial conflicts of interest.
80% of Emergency Physicians Say Mental Health Crisis Response Needs Overhaul
BY WHITNEY MCKNIGHT
Frontline Medical News
Vitals Key clinical point: A new model of psychiatric ED care is being developed by the Coalition on Psychiatric Emergencies (COPE), to improve care, outcomes, and net costs. Major finding: 8 in 10 emergency physicians (EPs) believe a lack of training and resources keep them from meeting a growing demand for emergency mental health services. Data source: American College of Emergency Physicians (ACEP) survey of 1,500 EPs nationwide. Disclosures: COPE is underwritten in part by Teva Pharmaceuticals. |
Emergency medicine professionals have teamed up with mental health workers and patient advocates to call for a new model of care for ED patients in mental health crisis.
The Coalition on Psychiatric Emergencies,” is focused on improving the delivery of emergency psychiatric care, and is supported by more than 30 national emergency medicine, mental health, and patient advocate groups, including the ACEP, the American Psychiatric Association, and the National Alliance on Mental Illness (NAMI). The action comes on the heels of a survey that found 80% of 1,500 US EPs think the system for treating people in acute mental health crisis is broken.
“It’s time we think about doing things differently,” Dr Michael Gerardi, COPE Steering Committee Chair and immediate past president of ACEP, said in a statement. “Through this unique collaboration, the Coalition on Psychiatric Emergencies will focus on developing a more unified treatment model and improving the treatment experience for both patients and health care providers. We want to provide the best care for all our patients and reduce health care costs.”
Among its several goals, the coalition seeks to shorten the time between when a person in mental health crisis presents to the ED and is admitted to an inpatient psychiatric bed. In a recent NAMI survey of 1,400 families, 38% waited more than 7 hours in the ED before seeing a mental health professional. For 21% of those families, the wait was more than 10 hours.
The Coalition on Psychiatric Emergencies also seeks adequate education and training for all emergency personnel who care for patients experiencing psychiatric emergencies.
“Emergency department staff need proper training not only on how to handle behavioral health emergencies, but also on how to initiate care for patients who may remain in the ED setting for long periods of time,” Dr Lorenzo Norris, director of inpatient psychiatric services at George Washington University Hospital in Washington, DC, said in an interview. “Establishing these new systems will likely require robust funding efforts.”
‘‘There is a growing need for change. At our hospital, we have definitely seen an uptick in the number of patients seeking emergency psychiatric care,” Dr Norris said. “Our approach has been to hire a clinician whose sole duty is to work collaboratively with patients and ED staff. It’s the first step in our ultimate goal of creating an ED behavioral health team that includes a psychiatrist, an emergency physician, nursing staff, social worker, and others who can provide the patient with comprehensive care at the initial point of contact.”
Currently in the United States, there are no standard protocols for a psychiatric emergency, according to the National Institute of Mental Health. The online survey was conducted within the ACEP membership between July 1 through 31, 2015. The response rate was 6% and the margin of error of 2.5%.
- Study Characterizes Intracerebral Hemorrhage With New Oral Anticoagulants
- Parrucker JC, Haas K, Rizos T, et al. Early Clinical and Radiological Course, Management, and Outcome of Intracerebral Hemorrhage Related to New Oral Anticoagulants. JAMA Neurol. doi:10.1001/jamaneurol.2015.3682.
- FDA Approves Treatment for Chemotherapy, Overdoses, Life-threatening Toxicities
- US Food and Drug Administration. FDA approves first emergency treatment for overdose of certain types of chemotherapy [FDA News Release]. December 11, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm476919.htm.
- Study Characterizes Intracerebral Hemorrhage With New Oral Anticoagulants
- Parrucker JC, Haas K, Rizos T, et al. Early Clinical and Radiological Course, Management, and Outcome of Intracerebral Hemorrhage Related to New Oral Anticoagulants. JAMA Neurol. doi:10.1001/jamaneurol.2015.3682.
- FDA Approves Treatment for Chemotherapy, Overdoses, Life-threatening Toxicities
- US Food and Drug Administration. FDA approves first emergency treatment for overdose of certain types of chemotherapy [FDA News Release]. December 11, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm476919.htm.

First EDition: News for and about the practice of emergency medicine
Federal rule could cut payments for out-of-network emergency services
BY ALICIA GALLEGOS
Frontline Medical News
Emergency physician leaders expressed outrage over a new federal regulation that they say could drastically lower payments for out-of-network emergency services. The final regulation, which affirms interim regulations by the US Department of Health & Human Services (HHS), allows health plans to use a vague methodology to calculate reimbursement for out-of-network emergency services.
The American College of Emergency Physicians has worked for years to have the rule’s language revised, said Dr Jeffrey Bettinger, a member of ACEP’s reimbursement committee and founder of a health care business consulting firm in Pinecrest, Florida. “They released final regulations which not only kept worrisome language...but actually made it worse.”
The regulation, published November 18 in the Federal Register, outlines patient protections under the Affordable Care Act, including how health plans must calculate coverage for out-of-network emergency services.1 The regulation states that a patient’s group health plan must reimburse out-of-network emergency services by paying the greatest of three possible (GOT) amounts:
- The median amount negotiated with in-network providers for the emergency service furnished.
- The amount for the emergency service calculated using the same method the plan generally uses to determine payments for out-of-network services (such as the usual, customary, and reasonable amount).
- The amount that would be paid under Medicare for the emergency service.
Under these options, the second choice is nearly always the greatest of the three amounts, and the last option–Medicare’s rate–is likely to be lowest, Dr Bettinger said.
ACEP has long been concerned about the second option because it lacks specificity and essentially leaves it up to health insurance plans to establish a Medicare-related method to reimburse emergency physicians for out-of-network services. The college lobbied for government officials to require more transparency from insurers who chose to pay under option two– for instance, by tying their methods to a usual, customary, and reasonable database or another model that was academically validated, Dr Bettinger said. The interim rule used the language, “such as the usual, customary, and reasonable charges,” rather than “amount” under option two. Under the final rule, the phrase “usual, customary, and reasonable amount,” is even more ambiguous than the proposed language, Dr Bettinger said.
“It’s a nebulous term,” he said. “It’s totally nontransparent. There’s no database that we know of that keeps track of what that number is. Honestly, it’s interpreted by the insurance companies to dramatically lower the payments they are making for out-of-network emergency services.”
In the final regulation, HHS acknowledged concerns by health providers about the level of payment for out-of-network emergency services and the need for more transparency by insurers.
“The departments believe that this concern is addressed by our requirement that the amount be the greatest of the three amounts specified,” according to the regulation.

The final regulation does not prohibit balance billing; however, if a patient resides in a state that bans balance billing, the “greatest of three” rule does not apply. Rather, emergency physicians in such states would be reimbursed based on the unique reimbursement method for out-of-network emergency services in their state, Dr Bettinger said.
“Some states that have specific payment regulations won’t be impacted to a large degree,” he said. “Other states that have prohibitions have less clearly defined payment formulas. These states will be impacted by the final rule.”
ACEP is considering taking legal action against the government over the rule, said ACEP President Jay A. Kaplan, MD, FACEP.
“This new ruling will significantly benefit health insurance companies at the expense of physicians, because they know hospital emergency departments have a federal mandate to care for everyone, regardless of ability to pay,” Dr Kaplan said in a statement.3 “They will continue to shift costs onto patients and medical providers, as well as shrink the number of doctors available in plans. Instead of requiring health plans to pay fairly, this ruling guarantees that insurance companies can pay whatever they want for emergency care. If history tells us anything, it’s that insurance companies prefer to pay as close to nothing as possible, while building their war chest for profits and litigation.”3
HHS officials did not respond to requests for comment.
Senate calls for childproof packaging for ‘e-cig juice’
BY GREGORY TWACHTMAN
Frontline Medical News
The Senate passed a bill that would require childproof packaging for liquid nicotine products.
The Child Nicotine Poisoning Prevention Act of 2015 (S. 142), also would codify Food and Drug Administration authority to regulate the packaging of liquid nicotine that is used to refill various electronic nicotine delivery systems.
S. 142 passed by unanimous consent in the Senate on December 10. The House of Representatives has not taken action on the bill.
“Just a small amount of this stuff can injure or even kill a small child,” Sen. Bill Nelson (D-Fla.), the bill’s sponsor, said in a statement. “Making these bottles childproof is just common sense.”
In 2014, poison control centers received more than 3,000 calls related to e-cigarette nicotine exposure, including one toddler death, according to a statement1 from the American Academy of Pediatrics.
“With e-cigarettes becoming more and more common in households across the country, we cannot afford to wait another day to protect children from poisonous liquid nicotine,” AAP President Dr Sandra Hassink said in the statement.1
- Federal rule could cut payments for out-of-network emergency services
- Federal Register. Final Rules for Grandfathered Plans, Preexisting Condition Exclusions, Lifetime and Annual Limits, Rescissions, Dependent Coverage, Appeals, and Patient Protections Under the Affordable Care Act. https://www.federalregister.gov/articles/2015/11/18/2015-29294/final-rules-for-grandfathered-plans-preexisting-condition-exclusions-lifetime-and-annual-limits. Published November 18, 2015.
- America’s Health Insurance Plans. Charges Billed by Out-of-Network Providers: Implications for Affordability. September, 2015. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahUKEwjW4ZrEzOPJAhXJoD4KHQq_BHMQFggdMAA&url=https%3A%2F%2Fwww.ahip.org%2FWorkarea%2FDownloadAsset.aspx%3Fid%3D4294973660&usg=AFQjCNEzsdxahTetw0_BMDROQG2d2R2Lbg&sig2=5xkmsLx5jLmAkv1o2X9E4Q. Accessed December 17, 2015.
- Health Plans Not Required To Pay Fairly for Emergency Care, Under New Regulation. Washington, DC: American College of Emergency Physicians; December 1, 2015. http://newsroom.acep.org/2015-12-01-Health-Plans-Not-Required-To-Pay-Fairly-for-Emergency-Care-Under-New-Regulation. Accessed December 17, 2015.
- Senate calls for childproof packaging for ‘e-cig juice’
- American Academy of Pediatrics. Pediatricians Applaud Senate Passage of the Child Nicotine Poisoning Prevention Act of 2015 [Press Release]. December 11, 2015. https://www.aap.org/en-us/about-the-aap/aap-press-room/Pages/Pediatricians-Applaud-Senate-Passage-of-the-Child-Nicotine-Poisoning-Prevention-Act-of-2015.aspx.
Federal rule could cut payments for out-of-network emergency services
BY ALICIA GALLEGOS
Frontline Medical News
Emergency physician leaders expressed outrage over a new federal regulation that they say could drastically lower payments for out-of-network emergency services. The final regulation, which affirms interim regulations by the US Department of Health & Human Services (HHS), allows health plans to use a vague methodology to calculate reimbursement for out-of-network emergency services.
The American College of Emergency Physicians has worked for years to have the rule’s language revised, said Dr Jeffrey Bettinger, a member of ACEP’s reimbursement committee and founder of a health care business consulting firm in Pinecrest, Florida. “They released final regulations which not only kept worrisome language...but actually made it worse.”
The regulation, published November 18 in the Federal Register, outlines patient protections under the Affordable Care Act, including how health plans must calculate coverage for out-of-network emergency services.1 The regulation states that a patient’s group health plan must reimburse out-of-network emergency services by paying the greatest of three possible (GOT) amounts:
- The median amount negotiated with in-network providers for the emergency service furnished.
- The amount for the emergency service calculated using the same method the plan generally uses to determine payments for out-of-network services (such as the usual, customary, and reasonable amount).
- The amount that would be paid under Medicare for the emergency service.
Under these options, the second choice is nearly always the greatest of the three amounts, and the last option–Medicare’s rate–is likely to be lowest, Dr Bettinger said.
ACEP has long been concerned about the second option because it lacks specificity and essentially leaves it up to health insurance plans to establish a Medicare-related method to reimburse emergency physicians for out-of-network services. The college lobbied for government officials to require more transparency from insurers who chose to pay under option two– for instance, by tying their methods to a usual, customary, and reasonable database or another model that was academically validated, Dr Bettinger said. The interim rule used the language, “such as the usual, customary, and reasonable charges,” rather than “amount” under option two. Under the final rule, the phrase “usual, customary, and reasonable amount,” is even more ambiguous than the proposed language, Dr Bettinger said.
“It’s a nebulous term,” he said. “It’s totally nontransparent. There’s no database that we know of that keeps track of what that number is. Honestly, it’s interpreted by the insurance companies to dramatically lower the payments they are making for out-of-network emergency services.”
In the final regulation, HHS acknowledged concerns by health providers about the level of payment for out-of-network emergency services and the need for more transparency by insurers.
“The departments believe that this concern is addressed by our requirement that the amount be the greatest of the three amounts specified,” according to the regulation.
The final regulation does not prohibit balance billing; however, if a patient resides in a state that bans balance billing, the “greatest of three” rule does not apply. Rather, emergency physicians in such states would be reimbursed based on the unique reimbursement method for out-of-network emergency services in their state, Dr Bettinger said.
“Some states that have specific payment regulations won’t be impacted to a large degree,” he said. “Other states that have prohibitions have less clearly defined payment formulas. These states will be impacted by the final rule.”
ACEP is considering taking legal action against the government over the rule, said ACEP President Jay A. Kaplan, MD, FACEP.
“This new ruling will significantly benefit health insurance companies at the expense of physicians, because they know hospital emergency departments have a federal mandate to care for everyone, regardless of ability to pay,” Dr Kaplan said in a statement.3 “They will continue to shift costs onto patients and medical providers, as well as shrink the number of doctors available in plans. Instead of requiring health plans to pay fairly, this ruling guarantees that insurance companies can pay whatever they want for emergency care. If history tells us anything, it’s that insurance companies prefer to pay as close to nothing as possible, while building their war chest for profits and litigation.”3
HHS officials did not respond to requests for comment.
Senate calls for childproof packaging for ‘e-cig juice’
BY GREGORY TWACHTMAN
Frontline Medical News
The Senate passed a bill that would require childproof packaging for liquid nicotine products.
The Child Nicotine Poisoning Prevention Act of 2015 (S. 142), also would codify Food and Drug Administration authority to regulate the packaging of liquid nicotine that is used to refill various electronic nicotine delivery systems.
S. 142 passed by unanimous consent in the Senate on December 10. The House of Representatives has not taken action on the bill.
“Just a small amount of this stuff can injure or even kill a small child,” Sen. Bill Nelson (D-Fla.), the bill’s sponsor, said in a statement. “Making these bottles childproof is just common sense.”
In 2014, poison control centers received more than 3,000 calls related to e-cigarette nicotine exposure, including one toddler death, according to a statement1 from the American Academy of Pediatrics.
“With e-cigarettes becoming more and more common in households across the country, we cannot afford to wait another day to protect children from poisonous liquid nicotine,” AAP President Dr Sandra Hassink said in the statement.1
Federal rule could cut payments for out-of-network emergency services
BY ALICIA GALLEGOS
Frontline Medical News
Emergency physician leaders expressed outrage over a new federal regulation that they say could drastically lower payments for out-of-network emergency services. The final regulation, which affirms interim regulations by the US Department of Health & Human Services (HHS), allows health plans to use a vague methodology to calculate reimbursement for out-of-network emergency services.
The American College of Emergency Physicians has worked for years to have the rule’s language revised, said Dr Jeffrey Bettinger, a member of ACEP’s reimbursement committee and founder of a health care business consulting firm in Pinecrest, Florida. “They released final regulations which not only kept worrisome language...but actually made it worse.”
The regulation, published November 18 in the Federal Register, outlines patient protections under the Affordable Care Act, including how health plans must calculate coverage for out-of-network emergency services.1 The regulation states that a patient’s group health plan must reimburse out-of-network emergency services by paying the greatest of three possible (GOT) amounts:
- The median amount negotiated with in-network providers for the emergency service furnished.
- The amount for the emergency service calculated using the same method the plan generally uses to determine payments for out-of-network services (such as the usual, customary, and reasonable amount).
- The amount that would be paid under Medicare for the emergency service.
Under these options, the second choice is nearly always the greatest of the three amounts, and the last option–Medicare’s rate–is likely to be lowest, Dr Bettinger said.
ACEP has long been concerned about the second option because it lacks specificity and essentially leaves it up to health insurance plans to establish a Medicare-related method to reimburse emergency physicians for out-of-network services. The college lobbied for government officials to require more transparency from insurers who chose to pay under option two– for instance, by tying their methods to a usual, customary, and reasonable database or another model that was academically validated, Dr Bettinger said. The interim rule used the language, “such as the usual, customary, and reasonable charges,” rather than “amount” under option two. Under the final rule, the phrase “usual, customary, and reasonable amount,” is even more ambiguous than the proposed language, Dr Bettinger said.
“It’s a nebulous term,” he said. “It’s totally nontransparent. There’s no database that we know of that keeps track of what that number is. Honestly, it’s interpreted by the insurance companies to dramatically lower the payments they are making for out-of-network emergency services.”
In the final regulation, HHS acknowledged concerns by health providers about the level of payment for out-of-network emergency services and the need for more transparency by insurers.
“The departments believe that this concern is addressed by our requirement that the amount be the greatest of the three amounts specified,” according to the regulation.
The final regulation does not prohibit balance billing; however, if a patient resides in a state that bans balance billing, the “greatest of three” rule does not apply. Rather, emergency physicians in such states would be reimbursed based on the unique reimbursement method for out-of-network emergency services in their state, Dr Bettinger said.
“Some states that have specific payment regulations won’t be impacted to a large degree,” he said. “Other states that have prohibitions have less clearly defined payment formulas. These states will be impacted by the final rule.”
ACEP is considering taking legal action against the government over the rule, said ACEP President Jay A. Kaplan, MD, FACEP.
“This new ruling will significantly benefit health insurance companies at the expense of physicians, because they know hospital emergency departments have a federal mandate to care for everyone, regardless of ability to pay,” Dr Kaplan said in a statement.3 “They will continue to shift costs onto patients and medical providers, as well as shrink the number of doctors available in plans. Instead of requiring health plans to pay fairly, this ruling guarantees that insurance companies can pay whatever they want for emergency care. If history tells us anything, it’s that insurance companies prefer to pay as close to nothing as possible, while building their war chest for profits and litigation.”3
HHS officials did not respond to requests for comment.
Senate calls for childproof packaging for ‘e-cig juice’
BY GREGORY TWACHTMAN
Frontline Medical News
The Senate passed a bill that would require childproof packaging for liquid nicotine products.
The Child Nicotine Poisoning Prevention Act of 2015 (S. 142), also would codify Food and Drug Administration authority to regulate the packaging of liquid nicotine that is used to refill various electronic nicotine delivery systems.
S. 142 passed by unanimous consent in the Senate on December 10. The House of Representatives has not taken action on the bill.
“Just a small amount of this stuff can injure or even kill a small child,” Sen. Bill Nelson (D-Fla.), the bill’s sponsor, said in a statement. “Making these bottles childproof is just common sense.”
In 2014, poison control centers received more than 3,000 calls related to e-cigarette nicotine exposure, including one toddler death, according to a statement1 from the American Academy of Pediatrics.
“With e-cigarettes becoming more and more common in households across the country, we cannot afford to wait another day to protect children from poisonous liquid nicotine,” AAP President Dr Sandra Hassink said in the statement.1
- Federal rule could cut payments for out-of-network emergency services
- Federal Register. Final Rules for Grandfathered Plans, Preexisting Condition Exclusions, Lifetime and Annual Limits, Rescissions, Dependent Coverage, Appeals, and Patient Protections Under the Affordable Care Act. https://www.federalregister.gov/articles/2015/11/18/2015-29294/final-rules-for-grandfathered-plans-preexisting-condition-exclusions-lifetime-and-annual-limits. Published November 18, 2015.
- America’s Health Insurance Plans. Charges Billed by Out-of-Network Providers: Implications for Affordability. September, 2015. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahUKEwjW4ZrEzOPJAhXJoD4KHQq_BHMQFggdMAA&url=https%3A%2F%2Fwww.ahip.org%2FWorkarea%2FDownloadAsset.aspx%3Fid%3D4294973660&usg=AFQjCNEzsdxahTetw0_BMDROQG2d2R2Lbg&sig2=5xkmsLx5jLmAkv1o2X9E4Q. Accessed December 17, 2015.
- Health Plans Not Required To Pay Fairly for Emergency Care, Under New Regulation. Washington, DC: American College of Emergency Physicians; December 1, 2015. http://newsroom.acep.org/2015-12-01-Health-Plans-Not-Required-To-Pay-Fairly-for-Emergency-Care-Under-New-Regulation. Accessed December 17, 2015.
- Senate calls for childproof packaging for ‘e-cig juice’
- American Academy of Pediatrics. Pediatricians Applaud Senate Passage of the Child Nicotine Poisoning Prevention Act of 2015 [Press Release]. December 11, 2015. https://www.aap.org/en-us/about-the-aap/aap-press-room/Pages/Pediatricians-Applaud-Senate-Passage-of-the-Child-Nicotine-Poisoning-Prevention-Act-of-2015.aspx.
- Federal rule could cut payments for out-of-network emergency services
- Federal Register. Final Rules for Grandfathered Plans, Preexisting Condition Exclusions, Lifetime and Annual Limits, Rescissions, Dependent Coverage, Appeals, and Patient Protections Under the Affordable Care Act. https://www.federalregister.gov/articles/2015/11/18/2015-29294/final-rules-for-grandfathered-plans-preexisting-condition-exclusions-lifetime-and-annual-limits. Published November 18, 2015.
- America’s Health Insurance Plans. Charges Billed by Out-of-Network Providers: Implications for Affordability. September, 2015. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0ahUKEwjW4ZrEzOPJAhXJoD4KHQq_BHMQFggdMAA&url=https%3A%2F%2Fwww.ahip.org%2FWorkarea%2FDownloadAsset.aspx%3Fid%3D4294973660&usg=AFQjCNEzsdxahTetw0_BMDROQG2d2R2Lbg&sig2=5xkmsLx5jLmAkv1o2X9E4Q. Accessed December 17, 2015.
- Health Plans Not Required To Pay Fairly for Emergency Care, Under New Regulation. Washington, DC: American College of Emergency Physicians; December 1, 2015. http://newsroom.acep.org/2015-12-01-Health-Plans-Not-Required-To-Pay-Fairly-for-Emergency-Care-Under-New-Regulation. Accessed December 17, 2015.
- Senate calls for childproof packaging for ‘e-cig juice’
- American Academy of Pediatrics. Pediatricians Applaud Senate Passage of the Child Nicotine Poisoning Prevention Act of 2015 [Press Release]. December 11, 2015. https://www.aap.org/en-us/about-the-aap/aap-press-room/Pages/Pediatricians-Applaud-Senate-Passage-of-the-Child-Nicotine-Poisoning-Prevention-Act-of-2015.aspx.

First EDition: News for and about the practice of emergency medicine
FDA approves first naloxone nasal spray for opioid overdose
BY DEEPAK CHITNIS
Frontline Medical News
The US Food and Drug Administration (FDA) has approved the first nasal spray variant of the opioid-overdose drug naloxone hydrochloride.
Marketed in the United States as Narcan (Adapt Pharma, a partner of Lightlake Therapeutics, Radnor, Pennsylvania) the nasal spray is known to stop or, in some cases, reverse the effects of opioid overdosing in patients. Narcan is the first naloxone hydrochloride nasal spray approved by the FDA.
“Combating the opioid abuse epidemic is a top priority for the FDA,” Dr Stephen Ostroff, FDA acting commissioner, said in a statement released with the November 18 approval announcement. “While naloxone will not solve the underlying problems of the opioid epidemic, we are speeding to review new formulations that will ultimately save lives that might otherwise be lost to drug addiction and overdose.”1
The nasal spray itself is available only with a prescription, and is safe for use by both adults and children, according to the FDA.
The spray delivers a dose of 4 mg naloxone in a single 0.1-mL nasal spray, which comes in a ready-to-use, needle-free device, according to Adapt Pharma. Administration of Narcan, which is sprayed into one nostril while the patient is lying on his or her back, does not require special training.
The FDA warned that body aches, diarrhea, tachycardia, fever, piloerection, nausea, nervousness, abdominal cramps, weakness, and increased blood pressure, among other conditions, are all possible side effects of Narcan.
Narcan’s approval is one step of many that must be taken to adequately address and ultimately end the problem of opioid abuse in the US, cautioned Dr Peter Friedmann, an addiction medicine specialist and chief research officer at Baystate Health in Springfield, Massachusetts. He expressed concern regarding the pricing of Narcan, noting that the drug’s affordability is crucial to its success.
“Right now, nasal atomizers with syringes are used off label, and the prices have been going up with increasing demand,” he said. “But [Narcan] is a commercial product based around what is essentially a generic medication, so [I] hope it’s priced at a price point that’s accessible to the great majority of patients and their families who are facing addiction, many of whom don’t have huge means.”
Therapeutic hypothermia after nonshockable-rhythm cardiac arrest
BY MARY ANN MOON
FROM CIRCULATION
Vitals Key clinical point: Therapeutic hypothermia raises the rate of survival with a good neurologic outcome in comatose patients after a cardiac arrest with a nonshockable initial rhythm. Major finding: The rate of survival-to-hospital discharge was significantly higher with therapeutic hypothermia (29%) than without it (15%), as was the rate of survival with a favorable neurologic outcome (21% vs 10%). Data source: A retrospective cohort study involving 519 adults enrolled in a therapeutic hypothermia registry during a 3-year period. Disclosures: This study was supported by the National Institutes of Health. Dr Perman and her associates reported having no financial disclosures. |
Therapeutic hypothermia significantly raises the rate of survival with a good neurologic outcome among patients who are comatose after a cardiac arrest with a nonshockable initial rhythm, according to a report published online November 16 in Circulation.1
Many observational and retrospective cohort studies have examined the possible benefits of therapeutic hypothermia in this patient population, but they have produced conflicting results. No prospective randomized clinical trials have been published, and some clinicians insist the treatment should be reserved for patients who meet the narrow criteria for which there is good supportive evidence; others, eager for any clinical strategy that can improve the outcomes of these critically ill patients, routinely expand its use to comatose patients regardless of their initial heart rhythm or the location of the cardiac arrest, wrote Dr Sarah M. Perman of the department of emergency medicine, University of Colorado, Aurora, and her associates.
They studied the issue using data from a national registry of patients treated at 16 medical centers that sometimes use therapeutic hypothermia after cardiac arrest. They assessed the records of 519 adults who had a nontraumatic cardiac arrest and initially registered either pulseless electrical activity or asystole, then had a return of spontaneous circulation but remained comatose. Approximately half of these comatose survivors (262 patients) were treated with therapeutic hypothermia according to their hospital’s usual protocols, and the other half (257 control subjects) received standard care without therapeutic hypothermia.

In the propensity-matched cohort, the rate of survival-to-hospital discharge was significantly higher with therapeutic hypothermia (29%) than without it (15%), as was the rate of survival with a favorable neurologic outcome (21% vs 10%). And in a multivariate analysis of factors contributing to positive patient outcomes, the intervention was associated with a 3.5-fold increase in favorable neurologic outcomes. A further analysis of the data showed that therapeutic hypothermia was associated with improved survival, with an odds ratio (OR) of 2.8, the investigators said.
In addition, an analysis of outcomes across various subgroups of patients showed that regardless of the location of their cardiac arrest, patients were consistently more likely to survive to hospital discharge neurologically intact if they received therapeutic hypothermia (OR, 2.1 for out-of-hospital cardiac rest; OR, 4.2 for in-hospital cardiac arrest).
“These results lend support to a broadening of indications for therapeutic hypothermia in comatose post-arrest patients with initial nonshockable rhythms,” Dr Perman and her associates said.
Andexanet reverses anticoagulant effects of factor Xa inhibitors
BY BIANCA NOGRADY
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Andexanet reverses the anticoagulant effects of factor Xa inhibitors rivaroxaban and apixaban in healthy older adults. Major finding: Andexanet achieved a 92% to 94% reduction in antifactor Xa activity, compared with an 18% to 21% reduction with placebo. Data source: A two-part randomized, placebo-controlled study in 145 healthy individuals. Disclosures: The study was supported by Portola Pharmaceuticals, Bayer, Bristol-Myers Squibb, Johnson & Johnson, and Pfizer. Several authors are employees of Portola, one with stock options and a related patent. Other authors declared grants and personal fees from the pharmaceutical industry, including the study supporters. |
Andexanet alfa has been found to reverse the anticoagulant effects of factor Xa inhibitors rivaroxaban and apixaban, according to a study presented at the American Heart Association scientific sessions and published simultaneously in the November 11 issue of the New England Journal of Medicine.1
In a two-part randomized, placebo-controlled study involving 145 healthy individuals with a mean age of 58 years, patients treated first with apixaban and then given a bolus of andexanet had a 94% reduction in anti-factor Xa activity, compared with a 21% reduction with placebo. Thrombin generation was restored in 100% of patients within 2 to 5 minutes.
In the patients treated with rivaroxaban, treatment with andexanet reduced antifactor Xa activity by 92%, compared to 18% with placebo. Thrombin generation was restored in 96% of participants in the andexanet group, compared with 7% in the placebo group.
Adverse events associated with andexanet were minor, including constipation, feeling hot, or a strange taste in the mouth. The effects of the andexanet also were sustained over the course of a 2-hour infusion in addition to the bolus.1
“The rapid onset and offset of action of andexanet and the ability to administer it as a bolus or as a bolus plus an infusion may provide flexibility with regard to the restoration of hemostasis when urgent factor Xa inhibitor reversal is required,” Dr Deborah M. Siegal of McMaster University, Hamilton, Ontario, Canada and coauthors wrote.
Continuous no better than interrupted chest compressions
BY MARY ANN MOON
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Continuous chest compressions during CPR didn’t improve survival or neurologic function compared with standard compressions briefly interrupted for ventilation. Major finding: The primary outcome – the rate of survival to hospital discharge – was 9.0% for continuous chest compressions and 9.7% for interrupted compressions, a nonsignificant difference. Data source: A cluster-randomized crossover trial involving 23,711 adults treated by 114 North American EMS agencies for nontraumatic out-of-hospital cardiac arrest. Disclosures: This study was supported by the US National Heart, Lung, and Blood Institute, the US Army Medical Research and Materiel Command, the Canadian Institutes of Health Research, the Institute of Circulatory and Respiratory Health, Defence Research and Development Canada, the Heart and Stroke Foundation of Canada, the American Heart Association, and the Medic One Foundation. Dr Nichol and his associates reported ties to numerous industry sources. |
Continuous chest compressions during CPR failed to improve survival or neurologic function compared with standard chest compressions that are briefly interrupted for ventilation, based on findings in the first large randomized trial to compare the two strategies for out-of-hospital, nontraumatic cardiac arrest.
In a presentation at the American Heart Association scientific sessions, simultaneously published online November 9 in the New England Journal of Medicine, Dr Graham Nichol and his associates analyzed data from the Resuscitation Outcomes Consortium, a network of clinical centers and EMS agencies that have expertise in conducting research on out-of-hospital cardiac arrest.1
Data were analyzed for 23,711 adults treated by 114 EMS agencies affiliated with eight clinical centers across the United States and Canada. These agencies were grouped into 47 clusters that were randomly assigned to perform CPR using either continuous chest compressions (100 per minute) with asynchronous positive-pressure ventilations (10 per minute) or standard chest compressions interrupted for ventilations (at a rate of 30 compressions per two ventilations) at every response to an out-of-hospital cardiac arrest. Twice per year, each cluster crossed over to the other resuscitation strategy, said Dr Nichol of the University of Washington–Harborview Center for Prehospital Emergency Care and Clinical Trial Center in Seattle.
A total of 12,653 patients were assigned to continuous chest compressions (the intervention group) and 11,058 to interrupted chest compressions (the control group). The primary outcome—the rate of survival to hospital discharge—was 9.0% in the intervention group and 9.7% in the control group, a nonsignificant difference. Similarly, the rate of survival with favorable neurologic function did not differ significantly, at 7.0% and 7.7%, respectively, the investigators said.1

However, it is also possible that three important limitations of this trial unduly influenced the results.
First, the per-protocol analysis, which used an automated algorithm to assess adherence to the compression assignments, could not classify many patients as having received either continuous or interrupted chest compressions. Second, the quality of postresuscitation care, which certainly influences outcomes, was not monitored. And third, actual oxygenation levels were not measured, nor were minutes of ventilation delivered. Thus, “we do not know whether there were important differences in oxygenation or ventilation between the two treatment strategies,” he said.
It is not yet clear why this large randomized trial1 showed no benefit from continuous chest compressions when previous observational research showed the opposite. One possibility is that many of the previous studies assessed not just chest compressions but an entire bundle of care related to CPR, so the benefits they reported may not be attributable to chest compressions alone.
In addition, in this study the mean chest-compression fraction – the proportion of each minute during which compressions are given, an important marker of interruptions in chest compressions – was already high in the control group (0.77) and not much different from that in the intervention group (0.83). Both of these are much higher than the target recommended by both American and European guidelines, which is only 0.60.
And of course a third reason may be that the interruptions for ventilation during CPR aren’t all that critical, and may be less detrimental to survival, than is currently believed.
Dr Rudolph W. Koster is in the department of cardiology at Amsterdam Academic Medical Center. He reported having no relevant financial disclosures. Dr Koster made these remarks in an editorial accompanying Dr Nichol’s report (Koster RW. Continuous or interrupted chest compressions for cardiac arrest [published online ahead of print November 9, 2015]. N Engl J Med).
Answers elusive in quest for better chlamydia treatment
BY BRUCE JANCIN
EXPERT ANALYSIS FROM ICAAC 2015
SAN DIEGO – The hottest topic today in the treatment of sexually transmitted diseases caused by Chlamydia trachomatis is the unresolved question of whether azithromycin is still as effective as doxycycline, the other current guideline-recommended, first-line therapy, Dr Kimberly Workowski said at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
“This is important, because doxycycline is administered twice a day for 7 days, and azithromycin is given as a single pill suitable for directly observed therapy,” noted Dr Workowski, professor of medicine at Emory University in Atlanta and lead author of the 2015 Centers for Disease Control and Prevention STD treatment guidelines.1
Several recent retrospective case series have suggested azithromycin is less effective, with the biggest efficacy gap being seen in rectal C. trachomatis infections. These nonrandomized studies were further supported by an Australian meta-analysis of six randomized, controlled trials comparing the two antibiotics for the treatment of genital chlamydia. The investigators found roughly 3% greater efficacy for doxycycline, compared with azithromycin, for urogenital chlamydia, and a 7% advantage for doxycycline in treating symptomatic urethral infection in men.
However, the investigators were quick to add the caveat that “the quality of the evidence varies considerably.”2
There’s a pressing need for better data. Dr Workowski and her colleagues on the STD guidelines panel are eagerly awaiting the results of a well-structured randomized trial led by Dr William M. Geisler, professor of medicine at the University of Alabama, Birmingham. The investigators randomized more than 300 chlamydia-infected male and female inmates in youth correctional facilities to guideline-recommended azithromycin at 1 g orally in a single dose or oral doxycycline at 100 mg twice daily for 7 days. The results, which are anticipated soon, should influence clinical practice, Dr Workowski said.
Here’s what else is new in chlamydia:
Pregnancy: For treatment of chlamydia in pregnancy, amoxicillin at 500 mg orally t.i.d. for 7 days has been demoted from a first-line recommended therapy to alternative-regimen status. Now, the sole recommended first-line treatment in pregnancy is oral azithromycin at 1 g orally in a single dose.
“We did this based on in vitro studies showing Chlamydia trachomatis is not well-killed by amoxicillin. Instead, the drug induces persistent viable noninfectious forms which can sometimes reactivate,” Dr Workowski explained.
Delayed-release doxycycline: This FDA-approved drug, known as Doryx, administered as a 200-mg tablet once daily for 7 days, “might be an alternative” to the standard generic doxycycline regimen of 100 mg twice daily for 7 days, according to the current Centers for Disease Control and Prevention guidelines. In a randomized, double-blind trial, the new agent was as effective as twice-daily generic doxycycline in men and women with urogenital C. trachomatis infection, and it had fewer gastrointestinal side effects. Doryx is costlier than the twice-daily alternatives.
Lymphogranuloma venereum: The current guidelines repeat a point made in previous editions, but one Dr Workowski believes remains underappreciated and thus worthy of emphasis: Rectal exposure to C. trachomatis serovars L1, L2, and L3 in men who have sex with men or in women who have rectal sex can cause lymphogranuloma venereum, which takes the form of proctocolitis mimicking inflammatory bowel disease.
Patients suspected of having lymphogranuloma venereum should be started presumptively on the recommended regimen for this STD, which is oral doxycycline at 100 mg b.i.d. for 21 days.
“If you also see painful ulcers or, on anoscopy, mucosal ulcers, you should also treat empirically for herpes simplex until your culture results come back,” she added.
Dr Workowski reported having no financial conflicts of interest.
Catheter-directed thrombolysis trumps systemic for acute pulmonary embolism
BY MITCHEL L. ZOLER
AT CHEST 2015
Vitals Key clinical point: Catheter-directed thrombolysis was linked to reduced mortality, compared with systemic thrombolysis in patients with an acute pulmonary embolism. Major finding: In-hospital mortality in acute pulmonary embolism patients ran 10% with catheter-directed thrombolysis and 17% with systemic thrombolysis. Data source: Review of 1,521 US patients treated for acute pulmonary embolism during 2010-2012 in the National Inpatient Sample. Disclosures: Dr Saqib and Dr Muthiah had no disclosures. |
MONTREAL – Catheter-directed thrombolysis surpassed systemic thrombolysis for minimizing in-hospital mortality of patients with an acute pulmonary embolism in a review of more than 1,500 United States patients.
The review also found evidence that US pulmonary embolism (PE) patients increasingly undergo catheter-directed thrombolysis, with usage jumping by more than 50% from 2010 to 2012, although in 2012 US clinicians performed catheter-directed thrombolysis on 160 patients with an acute pulmonary embolism (PE) who were included in a national US registry of hospitalized patients, Dr Amina Saqib said at the annual meeting of the American College of Chest Physicians.
Catheter-directed thrombolysis resulted in a 9% in-hospital mortality rate and a 10% combined rate of in-hospital mortality plus intracerebral hemorrhages, rates significantly below those tallied in propensity score-matched patients who underwent systemic thrombolysis of their acute PE. The matched group with systemic thrombolysis had a 17% in-hospital mortality rate and a 17% combined mortality plus intracerebral hemorrhage rate, said Dr Saqib, a researcher at Staten Island (New York) University Hospital.
“To the best of our knowledge, this is the first, large, nationwide, observational study that compared safety and efficacy outcomes between systemic thrombolysis and catheter-directed thrombolysis in acute PE,”
Dr Saqib said.
The US data, collected during 2010-2012, also showed that, after adjustment for clinical and demographic variables, each acute PE treatment by catheter-directed thrombolysis cost an average $9,428 above the cost for systemic thrombolysis, she said.

Dr Saqib and her associates used data collected by the Federal National Inpatient Sample. Among US patients hospitalized during 2010-2012 and entered into this database, they identified 1,169 adult acute PE patients who underwent systemic thrombolysis and 352 patients who received catheter-directed thrombolysis. The patients averaged about 58 years old and just under half were men.
The propensity score-adjusted analysis also showed no statistically significant difference between the two treatment approaches for the incidence of intracerebral hemorrhage, any hemorrhages requiring a transfusion, new-onset acute renal failure, or hospital length of stay. Among the patients treated by catheter-directed thrombolysis, all the intracerebral hemorrhages occurred during 2010; during 2011 and 2012 none of the patients treated this way had an intracerebral hemorrhage, Dr Saqib noted.
Although the findings were consistent with results from prior analyses, the propensity-score adjustment used in the current study cannot fully account for all unmeasured confounding factors. The best way to compare catheter-directed thrombolysis and systemic thrombolysis for treating acute PE would be in a prospective, randomized study, Dr Saqib said.
Survivors of out-of-hospital cardiac arrest usually had intact brain function
BY AMY KARON
FROM THE AHA SCIENTIFIC SESSIONS

Vitals Key clinical point: Most adults who survived out-of-hospital cardiac arrests remained neurologically intact, regardless of duration of CPR in the field. Major finding: Only 12% of patients survived, but 84% of survivors had a cerebral performance category of 1 or 2, including 10% who underwent more than 35 minutes of CPR before reaching the hospital. Data source: A retrospective observational study of 3,814 adults who had an out-of-hospital cardiac arrest between 2005 and 2014. Disclosures: Dr Williams had no disclosures. The senior author disclosed research funding from the Medtronic Foundation. |
Most adults who survived out-of-hospital cardiac arrests remained neurologically intact, even if cardiopulmonary resuscitation lasted longer than has been recommended, authors of a retrospective observational study reported at the American Heart Association scientific sessions.
Dr Jefferson Williams of the Wake County Department of Emergency Medical Services in Raleigh, North Carolina, and his associates studied 3,814 adults who had a cardiac arrest outside the hospital between 2005 and 2014. Only 12% of patients survived, but 84% of survivors had a cerebral performance category of 1 or 2, including 10% who underwent more than 35 minutes of CPR before reaching the hospital.
Neurologically intact survival was associated with having an initial shockable rhythm, a bystander-witnessed arrest, and return of spontaneous circulation in the field rather than in the hospital. Age, basic airway management, and therapeutic hypothermia phase also predicted survival with intact brain function, but duration of CPR did not.
Procalcitonin assay detects invasive bacterial infection
BY MARY ANN MOON
FROM JAMA PEDIATRICS
Vitals Key clinical point: The procalcitonin assay was superior to three other tests at detecting invasive bacterial infection in febrile infants aged 7-91 days. Major finding: At a threshold of 0.3 ng/mL or more, procalcitonin level detected invasive bacterial infections with a sensitivity of 90%, a specificity of 78%, and a negative predictive value of 0.1. Data source: A multicenter prospective cohort study involving 2,047 infants treated at pediatric EDs in France during a 30-month period. Disclosures: The French Health Ministry funded the study. Dr Milcent and her associates reported having no financial disclosures. |
The procalcitonin assay was superior to C-reactive protein, neutrophil, and white blood cell measurements at identifying invasive bacterial infections in very young febrile infants, according to a study published in JAMA Pediatrics.1
Compared with other biomarker assays, procalcitonin assays allow earlier detection of certain infections in older children. A few small studies have hinted at the usefulness of procalcitonin assays in infants, but to date no large prospective studies have assessed these assays in the youngest infants. For this prospective study, researchers evaluated the diagnostic accuracy of procalcitonin and other biomarkers in a study of 2,047 febrile infants aged 7-91 days who presented to 15 pediatric emergency departments in France during a 30-month period.
“We did not include infants 6 days or younger because they are likely to have early-onset sepsis related to perinatal factors and because physiologic procalcitonin concentrations during the first [few] days of life are higher than thereafter,” said Dr Karen Milcent of Hôpital Antoine Béclère, Clamart (France), and her associates.
Serum samples were collected at the initial clinical examination, but procalcitonin assays were not performed at that time. Attending physicians diagnosed the infants as having either bacterial or nonbacterial infections without knowing the procalcitonin results. Then, procalcitonin tests were done retrospectively on frozen serum samples by lab personnel who were blinded to the infants’ clinical features. Thirteen (1.0%) infants had bacteremia and 8 (0.6%) had bacterial meningitis.
The procalcitonin assay was significantly more accurate at identifying invasive bacterial infections than was C-reactive protein level, absolute neutrophil count, or white blood cell count. At a threshold of 0.3 ng/mL or more, the procalcitonin level had a sensitivity of 90%, a specificity of 78%, and a negative predictive value of 0.1. In addition, the procalcitonin assay was the most accurate in a subgroup analysis restricted to patients whose fever duration was less than 6 hours and another subgroup analysis restricted to patients younger than 1 month of age, the researchers said.1
For young febrile infants, combining procalcitonin assay results with a careful case history, a thorough physical examination, and other appropriate testing offers the potential of avoiding lumbar punctures. These study findings “should encourage the development of decision-making rules that incorporate procalcitonin,” Dr Milcent and her associates said.
The findings by Milcent et al are an important step forward in managing very young febrile infants, which remains a vexing problem.
A vital next step is to find alternatives to culture-based testing of blood, urine, and CSF. Genomic technologies that reliably detect molecular signatures in small amounts of biologic samples may be one such alternative. They may offer the additional benefit of identifying the pathogen and the host’s response to the presence of the pathogen.
Dr Nathan Kuppermann is in the departments of emergency medicine and pediatrics at the University of California–Davis. Dr Prashant Mahajan is in the departments of pediatrics and emergency medicine at Children’s Hospital of Michigan and Wayne State University, Detroit. They have no relevant financial disclosures. They made these remarks in an editorial accompanying Dr Milcent’s report (Kuppermann N, Mahajan P. Role of serum procalcitonin in identifying young febrile infants with invasive bacterial infections: one step closer to the holy grail [published online ahead of print November 23, 2015]? JAMA Ped. doi:10.1001/jamapediatrics.2015.3267).
Out-of-hospital MI survival is best in the Midwest
BY BRUCE JANCIN
AT THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Substantial and as-yet unexplained regional differences in survival and total hospital charges following out-of-hospital cardiac arrest exist across the United States. Major finding: Mortality among adults hospitalized after experiencing out-of-hospital cardiac arrest was 14% lower in the Midwest than in the Northeast. Data source: A retrospective analysis of data from the Nationwide Inpatient Sample for 2002-2012 that included 155,592 adults with out-of-hospital cardiac arrest who survived to hospital admission. Disclosures: The presenter reported having no financial conflicts of interest. |
ORLANDO – Considerable regional variation exists across the United States in outcomes, including survival and hospital charges following out-of-hospital cardiac arrest, Dr Aiham Albaeni reported at the American Heart Association scientific sessions.1
He presented an analysis of 155,592 adults who survived at least until hospital admission following non-trauma-related out-of-hospital cardiac arrest (OHCA) during 2002-2012. The data came from the Agency for Healthcare Research and Quality’s Nationwide Inpatient Sample, the largest all-payer US inpatient database.
Mortality was lowest among patients whose OHCA occurred in the Midwest. Indeed, taking the Northeast region as the reference point in a multivariate analysis, the adjusted mortality risk was 14% lower in the Midwest and 9% lower in the South. There was no difference in survival rates between the West and Northeast in this analysis adjusted for age, gender, race, primary diagnosis, income, Charlson Comorbidity Index, primary payer, and hospital size and teaching status, reported Dr Albaeni of Johns Hopkins University, Baltimore, Maryland.
Total hospital charges for patients admitted following OHCA were far and away highest in the West, and this increased expenditure didn’t pay off in terms of a survival advantage. The Consumer Price Index–adjusted mean total hospital charges averaged $85,592 per patient in the West, $66,290 in the Northeast, $55,257 in the Midwest, and $54,878 in the South.
Outliers in terms of cost of care—that is, patients admitted with OHCA whose total hospital charges exceeded $109,000 per admission—were 85% more common in the West than the other three regions, he noted.
Hospital length of stay greater than 8 days occurred most often in the Northeast. These lengthier stays were 10% to 12% less common in the other regions.
The explanation for the marked regional differences observed in this study remains unknown.
“These findings call for more efforts to identify a high-quality model of excellence that standardizes health care delivery and improves quality of care in low-performing regions,” said Dr Albaeni.
He reported having no financial conflicts of interest regarding his study.
Modified Valsalva more than doubled conversion rate in supraventricular tachycardia
BY AMY KARON
FROM THE LANCET
Vitals Key clinical point: A modified version of the Valsalva maneuver, in which patients were immediately laid flat afterward with their legs passively raised, more than doubled the rate of conversion from acute supraventricular tachycardia to normal sinus rhythm as compared with the standard Valsalva maneuver. Major finding: The conversion rate was 43% for the modified Valsalva group and 17% for patients undergoing the standard maneuver (adjusted OR, 3.7; P < .0001). Data source: Multicenter, randomized, controlled, parallel-group trial of 428 patients presenting to emergency departments with acute SVT. Disclosures: The National Institute for Health Research funded the study. The investigators declared no competing interests. |
A modified version of the Valsalva maneuver more than doubled the rate of conversion from acute supraventricular tachycardia to normal sinus rhythm when compared with the standard maneuver, said authors of a randomized, controlled trial published in the Lancet.
In all, 93 of 214 (43%) emergency department patients with acute supraventricular tachycardia (SVT) achieved cardioversion a minute after treatment with the modified Valsalva maneuver, compared with 37 (17%) of patients treated with standard Valsalva (adjusted odds ratio, 3.7; 95% CI, 2.3-5.8; P < .0001), reported Dr Andrew Appelboam of Royal Devon and Exeter (England) Hospital NHS Foundation Trust and his associates.
Standard Valsalva is safe, but achieves cardioversion for only 5% to 20% of patients with acute SVT. Nonresponders usually receive intravenous adenosine, which causes transient asystole and has other side effects, including a sense of “impending doom” or imminent death, the investigators noted.1
For the modified Valsalva maneuver, patients underwent standardized strain at 40 mm Hg pressure for 15 seconds while semi-recumbent, but then immediately laid flat while a staff member raised their legs to a 45-degree angle for 15 seconds. They returned to the semi-recumbent position for another 45 seconds before their cardiac rhythm was reassessed. The control group simply remained semirecumbent for 60 seconds after 15 seconds of Valsalva strain.
The adapted technique should achieve the same rate of cardioversion in community practice, and clinicians should repeat it once if it is not initially effective, said the researchers. “As long as individuals can safely undertake a Valsalva strain and be repositioned as described, this maneuver can be used as the routine initial treatment for episodes of supraventricular tachycardia regardless of location,” they said. Patients did not experience serious adverse effects, and transient cardiac events were self-limited and affected similar proportions of both groups, they added.
The National Institute for Health Research funded the study. The researchers declared no competing interests.
Off-label prescriptions link to more adverse events
BY MARY ANN MOON
FROM JAMA INTERNAL MEDICINE
Vitals Key clinical point: Off-label prescribing in adults is common and very likely to cause adverse events. Major finding: The incidence of adverse events was 44% higher for off-label use (19.7 per 10,000 person-months) than for on-label use (12.5 per 10,000 person-months) of prescription drugs. Data source: A prospective cohort study of 46,021 adults who received 151,305 incident prescriptions from primary care clinicians in Quebec during a 5-year period. Disclosures: No sponsors were identified for this study. Dr Tewodros Eguale and his associates reported having no relevant financial disclosures. |
Off-label prescribing of drugs is common and very likely to cause adverse events, particularly when no strong scientific evidence supports the off-label use, according to a report published in JAMA Internal Medicine.
No systematic investigation of the off-label use of prescription drugs has been done to date, in part because physicians aren’t required to document intended indications. Recent innovations in electronic health records provided an opportunity to track off-label prescribing and its influence on adverse drug events for all 8.5 million residents in the Canadian province of Quebec. There, physicians must provide the indication for every new prescription, the reason for any dose changes or drug discontinuation, and the nature of any adverse events, said Dr Tewodros Eguale of the department of epidemiology, biostatistics, and occupational health at McGill University, Montreal, and his associates.
“Selected examples of adverse events associated with the most frequently used off-label drugs include akathisia resulting from the use of gabapentin for neurogenic pain; agitation associated with the use of amitriptyline hydrochloride for migraine; hallucinations with the use of trazodone hydrochloride for insomnia; QT interval prolongation with the use of quetiapine fumarate for depression; and weight gain with the use of olanzapine for depression,” the authors reported.
Prescribing information in electronic medical records of 46,021 adults (mean age 58 years) given 151,305 new prescriptions was analyzed during a 5-year period. Physicians reported off-label use in 17,847 (12%) of these prescriptions, and that off-label use lacked strong scientific evidence in 81% of cases. The median follow-up time for use of prescribed medications was 386 days (range, 1 day to 6 years).

The class of drugs with the highest rate of adverse effects was anti-infective agents (66.2 per 10,000 person-months), followed by central nervous system drugs such as antidepressants, anxiolytics, and antimigraine medicine (18.1 per 10,000); cardiovascular drugs (15.9 per 10,000); hormonal agents (12.7); autonomic drugs including albuterol and terbutaline (8.4); gastrointestinal drugs (6.1); ear, nose, and throat medications (2.8); and “other” agents such as antihistamines, blood thinners, and antineoplastics (1.3).
“Off-label use may be clinically appropriate given the complexity of the patient’s condition, the lack of alternative effective drugs, or after exhausting approved drugs.” However, previous research has shown that physicians’ lack of knowledge of approved treatment indications was one important factor contributing to off-label prescribing. And one study showed that physicians are finding it difficult to keep up with rapidly changing medication information, and this lack of knowledge is affecting treatment, Dr Eguale and his associates said.
That knowledge gap could be filled by supplying clinicians with information regarding drug approval status and the quality of supporting scientific evidence at the point of care, when they write prescriptions into patients’ electronic health records, the investigators noted. This would have the added advantage of facilitating communication among physicians, pharmacists, and patients, and could reduce medication errors such as those caused by giving drugs to the wrong patients or by giving patients sound-alike or look-alike drugs.
No sponsors were identified for this study. Dr Tewodros Eguale and his associates reported having no relevant financial disclosures.
This study, the most extensive and informative one to evaluate the safety of off-label drug use in adults to date, shows that clinicians often enter an arena of the unknown when they expand prescribing beyond the carefully devised confines of the labeled indication. It provides compelling evidence that off-label prescribing is frequently inappropriate and substantially raises the risk for an adverse event.
Even in cases in which an off-label indication has been studied, the pharmacokinetics, drug-disease interactions, drug-drug interactions, and other safety considerations weren’t studied to the degree required during the drug approval process. Moreover, how many clinicians have the time or motivation to review the evidence for those off-label indications, arriving at a balanced assessment of risks and benefits?
Dr Chester B. Good is in pharmacy benefits management services at the US Department of Veterans Affairs in Hines, Illinois, and the department of pharmacy and therapeutics at the University of Pittsburgh. Dr Good and Dr Walid F. Gellad are in the department of medicine at the University of Pittsburgh and at the Center for Health Equity Research and Promotion in the Veterans Affairs Pittsburgh Healthcare System. Dr Good and Dr Gellad reported serving as unpaid advisers to the Food and Drug Administration’s Drug Safety Oversight Board. They made these remarks in an Invited Commentary accompanying Dr Eguale’s report (Good CB, Gellad WF. Off-label drug use and adverse drug events: turning up the heat on off-label prescribing [published online ahead of print November 2, 2014]. JAMA Intern Med. doi:10.1001/jamainternmed.2015.6068).
Dr Lappin is an assistant professor and an attending physician, department of mergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical College, New York.
- FDA approves first naloxone nasal spray for opioid overdose
- FDA moves quickly to approve easy-to-use nasal spray to treat opioid overdose [press release]. Silver Spring, MD: US Food and Drug Administration; November 18, 2015. Updated November 19, 2015.
- Therapeutic hypothermia after nonshockable-rhythm cardiac arrest
- Perman SM, Grossestreuer AV, Wiee DJ, Carr BG, Abella BS, Gaieski DF. The utility of therapeutic hypothermia for post-cardiac arrest syndrome patients with an initial non-shockable rhythm [published online ahead of print November 16, 2015]. Circulation. pii:CIRCULATIONAHA.115.016317.
- Andexanet reverses anticoagulant effects of factor Xa inhibitors
- Siegal DM, Cornutte JT, Connolly SJ, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity [published online ahead of print November 11, 2015]. N Engl J Med.
- Continuous no better than interrupted chest compressions
- Nichol G, Leroux B, Wang H, et al; ROC Investigators. Trial of continuous or interrupted chest compressions during CPR [published online ahead of print November 9, 2015]. N Engl J Med.
- Answers elusive in quest for better chlamydia treatment
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1-137.
- Kong FY, Tabrizi SN, Law M, et al. Azithrmycin versus doxycycline for the treatment of genital chlamydia infection: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014;59(2):193-205.
- Procalcitonin assay detects invasive bacterial infection
- Milcent K, Faesch S, Gras-Le Guen C, et al. Use of procalcitonin assays to predict serious bacterial infection in young febrile infants [published online ahead of print November 23, 2015]. JAMA Pediatr. doi: 10.1001/jamapediatrics.2015.3210.
- Out-of-hospital MI survival is best in the Midwest
- Shaker M, Albaeni A, Rios R. Impact of Change in Resuscitation Guidelines on National Out-of-hospital Cardiac Arrest Outcomes: Fulfilled Expectations? Paper presented at: American Heart Association 2015 Scientific Sessions; November 7-11, 2015; Orlando, Florida.
- Modified Valsalva more than doubled conversion rate in supraventricular tachycardia
- Appelboam A, Reuben A, Mann C, et al; REVERT trial collaborators. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015;386(10005):1747-1753.
- Off-label prescriptions link to more adverse events
- Eguale T, Buckeridge DL, Verma A, et al. Association of off-label drug use and adverse drug events in an adult population [published online ahead of print November 2, 2015]. JAMA Intern Med. doi: 10.1001/jamainternmed.2015.6058.
FDA approves first naloxone nasal spray for opioid overdose
BY DEEPAK CHITNIS
Frontline Medical News
The US Food and Drug Administration (FDA) has approved the first nasal spray variant of the opioid-overdose drug naloxone hydrochloride.
Marketed in the United States as Narcan (Adapt Pharma, a partner of Lightlake Therapeutics, Radnor, Pennsylvania) the nasal spray is known to stop or, in some cases, reverse the effects of opioid overdosing in patients. Narcan is the first naloxone hydrochloride nasal spray approved by the FDA.
“Combating the opioid abuse epidemic is a top priority for the FDA,” Dr Stephen Ostroff, FDA acting commissioner, said in a statement released with the November 18 approval announcement. “While naloxone will not solve the underlying problems of the opioid epidemic, we are speeding to review new formulations that will ultimately save lives that might otherwise be lost to drug addiction and overdose.”1
The nasal spray itself is available only with a prescription, and is safe for use by both adults and children, according to the FDA.
The spray delivers a dose of 4 mg naloxone in a single 0.1-mL nasal spray, which comes in a ready-to-use, needle-free device, according to Adapt Pharma. Administration of Narcan, which is sprayed into one nostril while the patient is lying on his or her back, does not require special training.
The FDA warned that body aches, diarrhea, tachycardia, fever, piloerection, nausea, nervousness, abdominal cramps, weakness, and increased blood pressure, among other conditions, are all possible side effects of Narcan.
Narcan’s approval is one step of many that must be taken to adequately address and ultimately end the problem of opioid abuse in the US, cautioned Dr Peter Friedmann, an addiction medicine specialist and chief research officer at Baystate Health in Springfield, Massachusetts. He expressed concern regarding the pricing of Narcan, noting that the drug’s affordability is crucial to its success.
“Right now, nasal atomizers with syringes are used off label, and the prices have been going up with increasing demand,” he said. “But [Narcan] is a commercial product based around what is essentially a generic medication, so [I] hope it’s priced at a price point that’s accessible to the great majority of patients and their families who are facing addiction, many of whom don’t have huge means.”
Therapeutic hypothermia after nonshockable-rhythm cardiac arrest
BY MARY ANN MOON
FROM CIRCULATION
Vitals Key clinical point: Therapeutic hypothermia raises the rate of survival with a good neurologic outcome in comatose patients after a cardiac arrest with a nonshockable initial rhythm. Major finding: The rate of survival-to-hospital discharge was significantly higher with therapeutic hypothermia (29%) than without it (15%), as was the rate of survival with a favorable neurologic outcome (21% vs 10%). Data source: A retrospective cohort study involving 519 adults enrolled in a therapeutic hypothermia registry during a 3-year period. Disclosures: This study was supported by the National Institutes of Health. Dr Perman and her associates reported having no financial disclosures. |
Therapeutic hypothermia significantly raises the rate of survival with a good neurologic outcome among patients who are comatose after a cardiac arrest with a nonshockable initial rhythm, according to a report published online November 16 in Circulation.1
Many observational and retrospective cohort studies have examined the possible benefits of therapeutic hypothermia in this patient population, but they have produced conflicting results. No prospective randomized clinical trials have been published, and some clinicians insist the treatment should be reserved for patients who meet the narrow criteria for which there is good supportive evidence; others, eager for any clinical strategy that can improve the outcomes of these critically ill patients, routinely expand its use to comatose patients regardless of their initial heart rhythm or the location of the cardiac arrest, wrote Dr Sarah M. Perman of the department of emergency medicine, University of Colorado, Aurora, and her associates.
They studied the issue using data from a national registry of patients treated at 16 medical centers that sometimes use therapeutic hypothermia after cardiac arrest. They assessed the records of 519 adults who had a nontraumatic cardiac arrest and initially registered either pulseless electrical activity or asystole, then had a return of spontaneous circulation but remained comatose. Approximately half of these comatose survivors (262 patients) were treated with therapeutic hypothermia according to their hospital’s usual protocols, and the other half (257 control subjects) received standard care without therapeutic hypothermia.
In the propensity-matched cohort, the rate of survival-to-hospital discharge was significantly higher with therapeutic hypothermia (29%) than without it (15%), as was the rate of survival with a favorable neurologic outcome (21% vs 10%). And in a multivariate analysis of factors contributing to positive patient outcomes, the intervention was associated with a 3.5-fold increase in favorable neurologic outcomes. A further analysis of the data showed that therapeutic hypothermia was associated with improved survival, with an odds ratio (OR) of 2.8, the investigators said.
In addition, an analysis of outcomes across various subgroups of patients showed that regardless of the location of their cardiac arrest, patients were consistently more likely to survive to hospital discharge neurologically intact if they received therapeutic hypothermia (OR, 2.1 for out-of-hospital cardiac rest; OR, 4.2 for in-hospital cardiac arrest).
“These results lend support to a broadening of indications for therapeutic hypothermia in comatose post-arrest patients with initial nonshockable rhythms,” Dr Perman and her associates said.
Andexanet reverses anticoagulant effects of factor Xa inhibitors
BY BIANCA NOGRADY
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Andexanet reverses the anticoagulant effects of factor Xa inhibitors rivaroxaban and apixaban in healthy older adults. Major finding: Andexanet achieved a 92% to 94% reduction in antifactor Xa activity, compared with an 18% to 21% reduction with placebo. Data source: A two-part randomized, placebo-controlled study in 145 healthy individuals. Disclosures: The study was supported by Portola Pharmaceuticals, Bayer, Bristol-Myers Squibb, Johnson & Johnson, and Pfizer. Several authors are employees of Portola, one with stock options and a related patent. Other authors declared grants and personal fees from the pharmaceutical industry, including the study supporters. |
Andexanet alfa has been found to reverse the anticoagulant effects of factor Xa inhibitors rivaroxaban and apixaban, according to a study presented at the American Heart Association scientific sessions and published simultaneously in the November 11 issue of the New England Journal of Medicine.1
In a two-part randomized, placebo-controlled study involving 145 healthy individuals with a mean age of 58 years, patients treated first with apixaban and then given a bolus of andexanet had a 94% reduction in anti-factor Xa activity, compared with a 21% reduction with placebo. Thrombin generation was restored in 100% of patients within 2 to 5 minutes.
In the patients treated with rivaroxaban, treatment with andexanet reduced antifactor Xa activity by 92%, compared to 18% with placebo. Thrombin generation was restored in 96% of participants in the andexanet group, compared with 7% in the placebo group.
Adverse events associated with andexanet were minor, including constipation, feeling hot, or a strange taste in the mouth. The effects of the andexanet also were sustained over the course of a 2-hour infusion in addition to the bolus.1
“The rapid onset and offset of action of andexanet and the ability to administer it as a bolus or as a bolus plus an infusion may provide flexibility with regard to the restoration of hemostasis when urgent factor Xa inhibitor reversal is required,” Dr Deborah M. Siegal of McMaster University, Hamilton, Ontario, Canada and coauthors wrote.
Continuous no better than interrupted chest compressions
BY MARY ANN MOON
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Continuous chest compressions during CPR didn’t improve survival or neurologic function compared with standard compressions briefly interrupted for ventilation. Major finding: The primary outcome – the rate of survival to hospital discharge – was 9.0% for continuous chest compressions and 9.7% for interrupted compressions, a nonsignificant difference. Data source: A cluster-randomized crossover trial involving 23,711 adults treated by 114 North American EMS agencies for nontraumatic out-of-hospital cardiac arrest. Disclosures: This study was supported by the US National Heart, Lung, and Blood Institute, the US Army Medical Research and Materiel Command, the Canadian Institutes of Health Research, the Institute of Circulatory and Respiratory Health, Defence Research and Development Canada, the Heart and Stroke Foundation of Canada, the American Heart Association, and the Medic One Foundation. Dr Nichol and his associates reported ties to numerous industry sources. |
Continuous chest compressions during CPR failed to improve survival or neurologic function compared with standard chest compressions that are briefly interrupted for ventilation, based on findings in the first large randomized trial to compare the two strategies for out-of-hospital, nontraumatic cardiac arrest.
In a presentation at the American Heart Association scientific sessions, simultaneously published online November 9 in the New England Journal of Medicine, Dr Graham Nichol and his associates analyzed data from the Resuscitation Outcomes Consortium, a network of clinical centers and EMS agencies that have expertise in conducting research on out-of-hospital cardiac arrest.1
Data were analyzed for 23,711 adults treated by 114 EMS agencies affiliated with eight clinical centers across the United States and Canada. These agencies were grouped into 47 clusters that were randomly assigned to perform CPR using either continuous chest compressions (100 per minute) with asynchronous positive-pressure ventilations (10 per minute) or standard chest compressions interrupted for ventilations (at a rate of 30 compressions per two ventilations) at every response to an out-of-hospital cardiac arrest. Twice per year, each cluster crossed over to the other resuscitation strategy, said Dr Nichol of the University of Washington–Harborview Center for Prehospital Emergency Care and Clinical Trial Center in Seattle.
A total of 12,653 patients were assigned to continuous chest compressions (the intervention group) and 11,058 to interrupted chest compressions (the control group). The primary outcome—the rate of survival to hospital discharge—was 9.0% in the intervention group and 9.7% in the control group, a nonsignificant difference. Similarly, the rate of survival with favorable neurologic function did not differ significantly, at 7.0% and 7.7%, respectively, the investigators said.1
However, it is also possible that three important limitations of this trial unduly influenced the results.
First, the per-protocol analysis, which used an automated algorithm to assess adherence to the compression assignments, could not classify many patients as having received either continuous or interrupted chest compressions. Second, the quality of postresuscitation care, which certainly influences outcomes, was not monitored. And third, actual oxygenation levels were not measured, nor were minutes of ventilation delivered. Thus, “we do not know whether there were important differences in oxygenation or ventilation between the two treatment strategies,” he said.
It is not yet clear why this large randomized trial1 showed no benefit from continuous chest compressions when previous observational research showed the opposite. One possibility is that many of the previous studies assessed not just chest compressions but an entire bundle of care related to CPR, so the benefits they reported may not be attributable to chest compressions alone.
In addition, in this study the mean chest-compression fraction – the proportion of each minute during which compressions are given, an important marker of interruptions in chest compressions – was already high in the control group (0.77) and not much different from that in the intervention group (0.83). Both of these are much higher than the target recommended by both American and European guidelines, which is only 0.60.
And of course a third reason may be that the interruptions for ventilation during CPR aren’t all that critical, and may be less detrimental to survival, than is currently believed.
Dr Rudolph W. Koster is in the department of cardiology at Amsterdam Academic Medical Center. He reported having no relevant financial disclosures. Dr Koster made these remarks in an editorial accompanying Dr Nichol’s report (Koster RW. Continuous or interrupted chest compressions for cardiac arrest [published online ahead of print November 9, 2015]. N Engl J Med).
Answers elusive in quest for better chlamydia treatment
BY BRUCE JANCIN
EXPERT ANALYSIS FROM ICAAC 2015
SAN DIEGO – The hottest topic today in the treatment of sexually transmitted diseases caused by Chlamydia trachomatis is the unresolved question of whether azithromycin is still as effective as doxycycline, the other current guideline-recommended, first-line therapy, Dr Kimberly Workowski said at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
“This is important, because doxycycline is administered twice a day for 7 days, and azithromycin is given as a single pill suitable for directly observed therapy,” noted Dr Workowski, professor of medicine at Emory University in Atlanta and lead author of the 2015 Centers for Disease Control and Prevention STD treatment guidelines.1
Several recent retrospective case series have suggested azithromycin is less effective, with the biggest efficacy gap being seen in rectal C. trachomatis infections. These nonrandomized studies were further supported by an Australian meta-analysis of six randomized, controlled trials comparing the two antibiotics for the treatment of genital chlamydia. The investigators found roughly 3% greater efficacy for doxycycline, compared with azithromycin, for urogenital chlamydia, and a 7% advantage for doxycycline in treating symptomatic urethral infection in men.
However, the investigators were quick to add the caveat that “the quality of the evidence varies considerably.”2
There’s a pressing need for better data. Dr Workowski and her colleagues on the STD guidelines panel are eagerly awaiting the results of a well-structured randomized trial led by Dr William M. Geisler, professor of medicine at the University of Alabama, Birmingham. The investigators randomized more than 300 chlamydia-infected male and female inmates in youth correctional facilities to guideline-recommended azithromycin at 1 g orally in a single dose or oral doxycycline at 100 mg twice daily for 7 days. The results, which are anticipated soon, should influence clinical practice, Dr Workowski said.
Here’s what else is new in chlamydia:
Pregnancy: For treatment of chlamydia in pregnancy, amoxicillin at 500 mg orally t.i.d. for 7 days has been demoted from a first-line recommended therapy to alternative-regimen status. Now, the sole recommended first-line treatment in pregnancy is oral azithromycin at 1 g orally in a single dose.
“We did this based on in vitro studies showing Chlamydia trachomatis is not well-killed by amoxicillin. Instead, the drug induces persistent viable noninfectious forms which can sometimes reactivate,” Dr Workowski explained.
Delayed-release doxycycline: This FDA-approved drug, known as Doryx, administered as a 200-mg tablet once daily for 7 days, “might be an alternative” to the standard generic doxycycline regimen of 100 mg twice daily for 7 days, according to the current Centers for Disease Control and Prevention guidelines. In a randomized, double-blind trial, the new agent was as effective as twice-daily generic doxycycline in men and women with urogenital C. trachomatis infection, and it had fewer gastrointestinal side effects. Doryx is costlier than the twice-daily alternatives.
Lymphogranuloma venereum: The current guidelines repeat a point made in previous editions, but one Dr Workowski believes remains underappreciated and thus worthy of emphasis: Rectal exposure to C. trachomatis serovars L1, L2, and L3 in men who have sex with men or in women who have rectal sex can cause lymphogranuloma venereum, which takes the form of proctocolitis mimicking inflammatory bowel disease.
Patients suspected of having lymphogranuloma venereum should be started presumptively on the recommended regimen for this STD, which is oral doxycycline at 100 mg b.i.d. for 21 days.
“If you also see painful ulcers or, on anoscopy, mucosal ulcers, you should also treat empirically for herpes simplex until your culture results come back,” she added.
Dr Workowski reported having no financial conflicts of interest.
Catheter-directed thrombolysis trumps systemic for acute pulmonary embolism
BY MITCHEL L. ZOLER
AT CHEST 2015
Vitals Key clinical point: Catheter-directed thrombolysis was linked to reduced mortality, compared with systemic thrombolysis in patients with an acute pulmonary embolism. Major finding: In-hospital mortality in acute pulmonary embolism patients ran 10% with catheter-directed thrombolysis and 17% with systemic thrombolysis. Data source: Review of 1,521 US patients treated for acute pulmonary embolism during 2010-2012 in the National Inpatient Sample. Disclosures: Dr Saqib and Dr Muthiah had no disclosures. |
MONTREAL – Catheter-directed thrombolysis surpassed systemic thrombolysis for minimizing in-hospital mortality of patients with an acute pulmonary embolism in a review of more than 1,500 United States patients.
The review also found evidence that US pulmonary embolism (PE) patients increasingly undergo catheter-directed thrombolysis, with usage jumping by more than 50% from 2010 to 2012, although in 2012 US clinicians performed catheter-directed thrombolysis on 160 patients with an acute pulmonary embolism (PE) who were included in a national US registry of hospitalized patients, Dr Amina Saqib said at the annual meeting of the American College of Chest Physicians.
Catheter-directed thrombolysis resulted in a 9% in-hospital mortality rate and a 10% combined rate of in-hospital mortality plus intracerebral hemorrhages, rates significantly below those tallied in propensity score-matched patients who underwent systemic thrombolysis of their acute PE. The matched group with systemic thrombolysis had a 17% in-hospital mortality rate and a 17% combined mortality plus intracerebral hemorrhage rate, said Dr Saqib, a researcher at Staten Island (New York) University Hospital.
“To the best of our knowledge, this is the first, large, nationwide, observational study that compared safety and efficacy outcomes between systemic thrombolysis and catheter-directed thrombolysis in acute PE,”
Dr Saqib said.
The US data, collected during 2010-2012, also showed that, after adjustment for clinical and demographic variables, each acute PE treatment by catheter-directed thrombolysis cost an average $9,428 above the cost for systemic thrombolysis, she said.
Dr Saqib and her associates used data collected by the Federal National Inpatient Sample. Among US patients hospitalized during 2010-2012 and entered into this database, they identified 1,169 adult acute PE patients who underwent systemic thrombolysis and 352 patients who received catheter-directed thrombolysis. The patients averaged about 58 years old and just under half were men.
The propensity score-adjusted analysis also showed no statistically significant difference between the two treatment approaches for the incidence of intracerebral hemorrhage, any hemorrhages requiring a transfusion, new-onset acute renal failure, or hospital length of stay. Among the patients treated by catheter-directed thrombolysis, all the intracerebral hemorrhages occurred during 2010; during 2011 and 2012 none of the patients treated this way had an intracerebral hemorrhage, Dr Saqib noted.
Although the findings were consistent with results from prior analyses, the propensity-score adjustment used in the current study cannot fully account for all unmeasured confounding factors. The best way to compare catheter-directed thrombolysis and systemic thrombolysis for treating acute PE would be in a prospective, randomized study, Dr Saqib said.
Survivors of out-of-hospital cardiac arrest usually had intact brain function
BY AMY KARON
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Most adults who survived out-of-hospital cardiac arrests remained neurologically intact, regardless of duration of CPR in the field. Major finding: Only 12% of patients survived, but 84% of survivors had a cerebral performance category of 1 or 2, including 10% who underwent more than 35 minutes of CPR before reaching the hospital. Data source: A retrospective observational study of 3,814 adults who had an out-of-hospital cardiac arrest between 2005 and 2014. Disclosures: Dr Williams had no disclosures. The senior author disclosed research funding from the Medtronic Foundation. |
Most adults who survived out-of-hospital cardiac arrests remained neurologically intact, even if cardiopulmonary resuscitation lasted longer than has been recommended, authors of a retrospective observational study reported at the American Heart Association scientific sessions.
Dr Jefferson Williams of the Wake County Department of Emergency Medical Services in Raleigh, North Carolina, and his associates studied 3,814 adults who had a cardiac arrest outside the hospital between 2005 and 2014. Only 12% of patients survived, but 84% of survivors had a cerebral performance category of 1 or 2, including 10% who underwent more than 35 minutes of CPR before reaching the hospital.
Neurologically intact survival was associated with having an initial shockable rhythm, a bystander-witnessed arrest, and return of spontaneous circulation in the field rather than in the hospital. Age, basic airway management, and therapeutic hypothermia phase also predicted survival with intact brain function, but duration of CPR did not.
Procalcitonin assay detects invasive bacterial infection
BY MARY ANN MOON
FROM JAMA PEDIATRICS
Vitals Key clinical point: The procalcitonin assay was superior to three other tests at detecting invasive bacterial infection in febrile infants aged 7-91 days. Major finding: At a threshold of 0.3 ng/mL or more, procalcitonin level detected invasive bacterial infections with a sensitivity of 90%, a specificity of 78%, and a negative predictive value of 0.1. Data source: A multicenter prospective cohort study involving 2,047 infants treated at pediatric EDs in France during a 30-month period. Disclosures: The French Health Ministry funded the study. Dr Milcent and her associates reported having no financial disclosures. |
The procalcitonin assay was superior to C-reactive protein, neutrophil, and white blood cell measurements at identifying invasive bacterial infections in very young febrile infants, according to a study published in JAMA Pediatrics.1
Compared with other biomarker assays, procalcitonin assays allow earlier detection of certain infections in older children. A few small studies have hinted at the usefulness of procalcitonin assays in infants, but to date no large prospective studies have assessed these assays in the youngest infants. For this prospective study, researchers evaluated the diagnostic accuracy of procalcitonin and other biomarkers in a study of 2,047 febrile infants aged 7-91 days who presented to 15 pediatric emergency departments in France during a 30-month period.
“We did not include infants 6 days or younger because they are likely to have early-onset sepsis related to perinatal factors and because physiologic procalcitonin concentrations during the first [few] days of life are higher than thereafter,” said Dr Karen Milcent of Hôpital Antoine Béclère, Clamart (France), and her associates.
Serum samples were collected at the initial clinical examination, but procalcitonin assays were not performed at that time. Attending physicians diagnosed the infants as having either bacterial or nonbacterial infections without knowing the procalcitonin results. Then, procalcitonin tests were done retrospectively on frozen serum samples by lab personnel who were blinded to the infants’ clinical features. Thirteen (1.0%) infants had bacteremia and 8 (0.6%) had bacterial meningitis.
The procalcitonin assay was significantly more accurate at identifying invasive bacterial infections than was C-reactive protein level, absolute neutrophil count, or white blood cell count. At a threshold of 0.3 ng/mL or more, the procalcitonin level had a sensitivity of 90%, a specificity of 78%, and a negative predictive value of 0.1. In addition, the procalcitonin assay was the most accurate in a subgroup analysis restricted to patients whose fever duration was less than 6 hours and another subgroup analysis restricted to patients younger than 1 month of age, the researchers said.1
For young febrile infants, combining procalcitonin assay results with a careful case history, a thorough physical examination, and other appropriate testing offers the potential of avoiding lumbar punctures. These study findings “should encourage the development of decision-making rules that incorporate procalcitonin,” Dr Milcent and her associates said.
The findings by Milcent et al are an important step forward in managing very young febrile infants, which remains a vexing problem.
A vital next step is to find alternatives to culture-based testing of blood, urine, and CSF. Genomic technologies that reliably detect molecular signatures in small amounts of biologic samples may be one such alternative. They may offer the additional benefit of identifying the pathogen and the host’s response to the presence of the pathogen.
Dr Nathan Kuppermann is in the departments of emergency medicine and pediatrics at the University of California–Davis. Dr Prashant Mahajan is in the departments of pediatrics and emergency medicine at Children’s Hospital of Michigan and Wayne State University, Detroit. They have no relevant financial disclosures. They made these remarks in an editorial accompanying Dr Milcent’s report (Kuppermann N, Mahajan P. Role of serum procalcitonin in identifying young febrile infants with invasive bacterial infections: one step closer to the holy grail [published online ahead of print November 23, 2015]? JAMA Ped. doi:10.1001/jamapediatrics.2015.3267).
Out-of-hospital MI survival is best in the Midwest
BY BRUCE JANCIN
AT THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Substantial and as-yet unexplained regional differences in survival and total hospital charges following out-of-hospital cardiac arrest exist across the United States. Major finding: Mortality among adults hospitalized after experiencing out-of-hospital cardiac arrest was 14% lower in the Midwest than in the Northeast. Data source: A retrospective analysis of data from the Nationwide Inpatient Sample for 2002-2012 that included 155,592 adults with out-of-hospital cardiac arrest who survived to hospital admission. Disclosures: The presenter reported having no financial conflicts of interest. |
ORLANDO – Considerable regional variation exists across the United States in outcomes, including survival and hospital charges following out-of-hospital cardiac arrest, Dr Aiham Albaeni reported at the American Heart Association scientific sessions.1
He presented an analysis of 155,592 adults who survived at least until hospital admission following non-trauma-related out-of-hospital cardiac arrest (OHCA) during 2002-2012. The data came from the Agency for Healthcare Research and Quality’s Nationwide Inpatient Sample, the largest all-payer US inpatient database.
Mortality was lowest among patients whose OHCA occurred in the Midwest. Indeed, taking the Northeast region as the reference point in a multivariate analysis, the adjusted mortality risk was 14% lower in the Midwest and 9% lower in the South. There was no difference in survival rates between the West and Northeast in this analysis adjusted for age, gender, race, primary diagnosis, income, Charlson Comorbidity Index, primary payer, and hospital size and teaching status, reported Dr Albaeni of Johns Hopkins University, Baltimore, Maryland.
Total hospital charges for patients admitted following OHCA were far and away highest in the West, and this increased expenditure didn’t pay off in terms of a survival advantage. The Consumer Price Index–adjusted mean total hospital charges averaged $85,592 per patient in the West, $66,290 in the Northeast, $55,257 in the Midwest, and $54,878 in the South.
Outliers in terms of cost of care—that is, patients admitted with OHCA whose total hospital charges exceeded $109,000 per admission—were 85% more common in the West than the other three regions, he noted.
Hospital length of stay greater than 8 days occurred most often in the Northeast. These lengthier stays were 10% to 12% less common in the other regions.
The explanation for the marked regional differences observed in this study remains unknown.
“These findings call for more efforts to identify a high-quality model of excellence that standardizes health care delivery and improves quality of care in low-performing regions,” said Dr Albaeni.
He reported having no financial conflicts of interest regarding his study.
Modified Valsalva more than doubled conversion rate in supraventricular tachycardia
BY AMY KARON
FROM THE LANCET
Vitals Key clinical point: A modified version of the Valsalva maneuver, in which patients were immediately laid flat afterward with their legs passively raised, more than doubled the rate of conversion from acute supraventricular tachycardia to normal sinus rhythm as compared with the standard Valsalva maneuver. Major finding: The conversion rate was 43% for the modified Valsalva group and 17% for patients undergoing the standard maneuver (adjusted OR, 3.7; P < .0001). Data source: Multicenter, randomized, controlled, parallel-group trial of 428 patients presenting to emergency departments with acute SVT. Disclosures: The National Institute for Health Research funded the study. The investigators declared no competing interests. |
A modified version of the Valsalva maneuver more than doubled the rate of conversion from acute supraventricular tachycardia to normal sinus rhythm when compared with the standard maneuver, said authors of a randomized, controlled trial published in the Lancet.
In all, 93 of 214 (43%) emergency department patients with acute supraventricular tachycardia (SVT) achieved cardioversion a minute after treatment with the modified Valsalva maneuver, compared with 37 (17%) of patients treated with standard Valsalva (adjusted odds ratio, 3.7; 95% CI, 2.3-5.8; P < .0001), reported Dr Andrew Appelboam of Royal Devon and Exeter (England) Hospital NHS Foundation Trust and his associates.
Standard Valsalva is safe, but achieves cardioversion for only 5% to 20% of patients with acute SVT. Nonresponders usually receive intravenous adenosine, which causes transient asystole and has other side effects, including a sense of “impending doom” or imminent death, the investigators noted.1
For the modified Valsalva maneuver, patients underwent standardized strain at 40 mm Hg pressure for 15 seconds while semi-recumbent, but then immediately laid flat while a staff member raised their legs to a 45-degree angle for 15 seconds. They returned to the semi-recumbent position for another 45 seconds before their cardiac rhythm was reassessed. The control group simply remained semirecumbent for 60 seconds after 15 seconds of Valsalva strain.
The adapted technique should achieve the same rate of cardioversion in community practice, and clinicians should repeat it once if it is not initially effective, said the researchers. “As long as individuals can safely undertake a Valsalva strain and be repositioned as described, this maneuver can be used as the routine initial treatment for episodes of supraventricular tachycardia regardless of location,” they said. Patients did not experience serious adverse effects, and transient cardiac events were self-limited and affected similar proportions of both groups, they added.
The National Institute for Health Research funded the study. The researchers declared no competing interests.
Off-label prescriptions link to more adverse events
BY MARY ANN MOON
FROM JAMA INTERNAL MEDICINE
Vitals Key clinical point: Off-label prescribing in adults is common and very likely to cause adverse events. Major finding: The incidence of adverse events was 44% higher for off-label use (19.7 per 10,000 person-months) than for on-label use (12.5 per 10,000 person-months) of prescription drugs. Data source: A prospective cohort study of 46,021 adults who received 151,305 incident prescriptions from primary care clinicians in Quebec during a 5-year period. Disclosures: No sponsors were identified for this study. Dr Tewodros Eguale and his associates reported having no relevant financial disclosures. |
Off-label prescribing of drugs is common and very likely to cause adverse events, particularly when no strong scientific evidence supports the off-label use, according to a report published in JAMA Internal Medicine.
No systematic investigation of the off-label use of prescription drugs has been done to date, in part because physicians aren’t required to document intended indications. Recent innovations in electronic health records provided an opportunity to track off-label prescribing and its influence on adverse drug events for all 8.5 million residents in the Canadian province of Quebec. There, physicians must provide the indication for every new prescription, the reason for any dose changes or drug discontinuation, and the nature of any adverse events, said Dr Tewodros Eguale of the department of epidemiology, biostatistics, and occupational health at McGill University, Montreal, and his associates.
“Selected examples of adverse events associated with the most frequently used off-label drugs include akathisia resulting from the use of gabapentin for neurogenic pain; agitation associated with the use of amitriptyline hydrochloride for migraine; hallucinations with the use of trazodone hydrochloride for insomnia; QT interval prolongation with the use of quetiapine fumarate for depression; and weight gain with the use of olanzapine for depression,” the authors reported.
Prescribing information in electronic medical records of 46,021 adults (mean age 58 years) given 151,305 new prescriptions was analyzed during a 5-year period. Physicians reported off-label use in 17,847 (12%) of these prescriptions, and that off-label use lacked strong scientific evidence in 81% of cases. The median follow-up time for use of prescribed medications was 386 days (range, 1 day to 6 years).
The class of drugs with the highest rate of adverse effects was anti-infective agents (66.2 per 10,000 person-months), followed by central nervous system drugs such as antidepressants, anxiolytics, and antimigraine medicine (18.1 per 10,000); cardiovascular drugs (15.9 per 10,000); hormonal agents (12.7); autonomic drugs including albuterol and terbutaline (8.4); gastrointestinal drugs (6.1); ear, nose, and throat medications (2.8); and “other” agents such as antihistamines, blood thinners, and antineoplastics (1.3).
“Off-label use may be clinically appropriate given the complexity of the patient’s condition, the lack of alternative effective drugs, or after exhausting approved drugs.” However, previous research has shown that physicians’ lack of knowledge of approved treatment indications was one important factor contributing to off-label prescribing. And one study showed that physicians are finding it difficult to keep up with rapidly changing medication information, and this lack of knowledge is affecting treatment, Dr Eguale and his associates said.
That knowledge gap could be filled by supplying clinicians with information regarding drug approval status and the quality of supporting scientific evidence at the point of care, when they write prescriptions into patients’ electronic health records, the investigators noted. This would have the added advantage of facilitating communication among physicians, pharmacists, and patients, and could reduce medication errors such as those caused by giving drugs to the wrong patients or by giving patients sound-alike or look-alike drugs.
No sponsors were identified for this study. Dr Tewodros Eguale and his associates reported having no relevant financial disclosures.
This study, the most extensive and informative one to evaluate the safety of off-label drug use in adults to date, shows that clinicians often enter an arena of the unknown when they expand prescribing beyond the carefully devised confines of the labeled indication. It provides compelling evidence that off-label prescribing is frequently inappropriate and substantially raises the risk for an adverse event.
Even in cases in which an off-label indication has been studied, the pharmacokinetics, drug-disease interactions, drug-drug interactions, and other safety considerations weren’t studied to the degree required during the drug approval process. Moreover, how many clinicians have the time or motivation to review the evidence for those off-label indications, arriving at a balanced assessment of risks and benefits?
Dr Chester B. Good is in pharmacy benefits management services at the US Department of Veterans Affairs in Hines, Illinois, and the department of pharmacy and therapeutics at the University of Pittsburgh. Dr Good and Dr Walid F. Gellad are in the department of medicine at the University of Pittsburgh and at the Center for Health Equity Research and Promotion in the Veterans Affairs Pittsburgh Healthcare System. Dr Good and Dr Gellad reported serving as unpaid advisers to the Food and Drug Administration’s Drug Safety Oversight Board. They made these remarks in an Invited Commentary accompanying Dr Eguale’s report (Good CB, Gellad WF. Off-label drug use and adverse drug events: turning up the heat on off-label prescribing [published online ahead of print November 2, 2014]. JAMA Intern Med. doi:10.1001/jamainternmed.2015.6068).
Dr Lappin is an assistant professor and an attending physician, department of mergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical College, New York.
FDA approves first naloxone nasal spray for opioid overdose
BY DEEPAK CHITNIS
Frontline Medical News
The US Food and Drug Administration (FDA) has approved the first nasal spray variant of the opioid-overdose drug naloxone hydrochloride.
Marketed in the United States as Narcan (Adapt Pharma, a partner of Lightlake Therapeutics, Radnor, Pennsylvania) the nasal spray is known to stop or, in some cases, reverse the effects of opioid overdosing in patients. Narcan is the first naloxone hydrochloride nasal spray approved by the FDA.
“Combating the opioid abuse epidemic is a top priority for the FDA,” Dr Stephen Ostroff, FDA acting commissioner, said in a statement released with the November 18 approval announcement. “While naloxone will not solve the underlying problems of the opioid epidemic, we are speeding to review new formulations that will ultimately save lives that might otherwise be lost to drug addiction and overdose.”1
The nasal spray itself is available only with a prescription, and is safe for use by both adults and children, according to the FDA.
The spray delivers a dose of 4 mg naloxone in a single 0.1-mL nasal spray, which comes in a ready-to-use, needle-free device, according to Adapt Pharma. Administration of Narcan, which is sprayed into one nostril while the patient is lying on his or her back, does not require special training.
The FDA warned that body aches, diarrhea, tachycardia, fever, piloerection, nausea, nervousness, abdominal cramps, weakness, and increased blood pressure, among other conditions, are all possible side effects of Narcan.
Narcan’s approval is one step of many that must be taken to adequately address and ultimately end the problem of opioid abuse in the US, cautioned Dr Peter Friedmann, an addiction medicine specialist and chief research officer at Baystate Health in Springfield, Massachusetts. He expressed concern regarding the pricing of Narcan, noting that the drug’s affordability is crucial to its success.
“Right now, nasal atomizers with syringes are used off label, and the prices have been going up with increasing demand,” he said. “But [Narcan] is a commercial product based around what is essentially a generic medication, so [I] hope it’s priced at a price point that’s accessible to the great majority of patients and their families who are facing addiction, many of whom don’t have huge means.”
Therapeutic hypothermia after nonshockable-rhythm cardiac arrest
BY MARY ANN MOON
FROM CIRCULATION
Vitals Key clinical point: Therapeutic hypothermia raises the rate of survival with a good neurologic outcome in comatose patients after a cardiac arrest with a nonshockable initial rhythm. Major finding: The rate of survival-to-hospital discharge was significantly higher with therapeutic hypothermia (29%) than without it (15%), as was the rate of survival with a favorable neurologic outcome (21% vs 10%). Data source: A retrospective cohort study involving 519 adults enrolled in a therapeutic hypothermia registry during a 3-year period. Disclosures: This study was supported by the National Institutes of Health. Dr Perman and her associates reported having no financial disclosures. |
Therapeutic hypothermia significantly raises the rate of survival with a good neurologic outcome among patients who are comatose after a cardiac arrest with a nonshockable initial rhythm, according to a report published online November 16 in Circulation.1
Many observational and retrospective cohort studies have examined the possible benefits of therapeutic hypothermia in this patient population, but they have produced conflicting results. No prospective randomized clinical trials have been published, and some clinicians insist the treatment should be reserved for patients who meet the narrow criteria for which there is good supportive evidence; others, eager for any clinical strategy that can improve the outcomes of these critically ill patients, routinely expand its use to comatose patients regardless of their initial heart rhythm or the location of the cardiac arrest, wrote Dr Sarah M. Perman of the department of emergency medicine, University of Colorado, Aurora, and her associates.
They studied the issue using data from a national registry of patients treated at 16 medical centers that sometimes use therapeutic hypothermia after cardiac arrest. They assessed the records of 519 adults who had a nontraumatic cardiac arrest and initially registered either pulseless electrical activity or asystole, then had a return of spontaneous circulation but remained comatose. Approximately half of these comatose survivors (262 patients) were treated with therapeutic hypothermia according to their hospital’s usual protocols, and the other half (257 control subjects) received standard care without therapeutic hypothermia.
In the propensity-matched cohort, the rate of survival-to-hospital discharge was significantly higher with therapeutic hypothermia (29%) than without it (15%), as was the rate of survival with a favorable neurologic outcome (21% vs 10%). And in a multivariate analysis of factors contributing to positive patient outcomes, the intervention was associated with a 3.5-fold increase in favorable neurologic outcomes. A further analysis of the data showed that therapeutic hypothermia was associated with improved survival, with an odds ratio (OR) of 2.8, the investigators said.
In addition, an analysis of outcomes across various subgroups of patients showed that regardless of the location of their cardiac arrest, patients were consistently more likely to survive to hospital discharge neurologically intact if they received therapeutic hypothermia (OR, 2.1 for out-of-hospital cardiac rest; OR, 4.2 for in-hospital cardiac arrest).
“These results lend support to a broadening of indications for therapeutic hypothermia in comatose post-arrest patients with initial nonshockable rhythms,” Dr Perman and her associates said.
Andexanet reverses anticoagulant effects of factor Xa inhibitors
BY BIANCA NOGRADY
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Andexanet reverses the anticoagulant effects of factor Xa inhibitors rivaroxaban and apixaban in healthy older adults. Major finding: Andexanet achieved a 92% to 94% reduction in antifactor Xa activity, compared with an 18% to 21% reduction with placebo. Data source: A two-part randomized, placebo-controlled study in 145 healthy individuals. Disclosures: The study was supported by Portola Pharmaceuticals, Bayer, Bristol-Myers Squibb, Johnson & Johnson, and Pfizer. Several authors are employees of Portola, one with stock options and a related patent. Other authors declared grants and personal fees from the pharmaceutical industry, including the study supporters. |
Andexanet alfa has been found to reverse the anticoagulant effects of factor Xa inhibitors rivaroxaban and apixaban, according to a study presented at the American Heart Association scientific sessions and published simultaneously in the November 11 issue of the New England Journal of Medicine.1
In a two-part randomized, placebo-controlled study involving 145 healthy individuals with a mean age of 58 years, patients treated first with apixaban and then given a bolus of andexanet had a 94% reduction in anti-factor Xa activity, compared with a 21% reduction with placebo. Thrombin generation was restored in 100% of patients within 2 to 5 minutes.
In the patients treated with rivaroxaban, treatment with andexanet reduced antifactor Xa activity by 92%, compared to 18% with placebo. Thrombin generation was restored in 96% of participants in the andexanet group, compared with 7% in the placebo group.
Adverse events associated with andexanet were minor, including constipation, feeling hot, or a strange taste in the mouth. The effects of the andexanet also were sustained over the course of a 2-hour infusion in addition to the bolus.1
“The rapid onset and offset of action of andexanet and the ability to administer it as a bolus or as a bolus plus an infusion may provide flexibility with regard to the restoration of hemostasis when urgent factor Xa inhibitor reversal is required,” Dr Deborah M. Siegal of McMaster University, Hamilton, Ontario, Canada and coauthors wrote.
Continuous no better than interrupted chest compressions
BY MARY ANN MOON
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Continuous chest compressions during CPR didn’t improve survival or neurologic function compared with standard compressions briefly interrupted for ventilation. Major finding: The primary outcome – the rate of survival to hospital discharge – was 9.0% for continuous chest compressions and 9.7% for interrupted compressions, a nonsignificant difference. Data source: A cluster-randomized crossover trial involving 23,711 adults treated by 114 North American EMS agencies for nontraumatic out-of-hospital cardiac arrest. Disclosures: This study was supported by the US National Heart, Lung, and Blood Institute, the US Army Medical Research and Materiel Command, the Canadian Institutes of Health Research, the Institute of Circulatory and Respiratory Health, Defence Research and Development Canada, the Heart and Stroke Foundation of Canada, the American Heart Association, and the Medic One Foundation. Dr Nichol and his associates reported ties to numerous industry sources. |
Continuous chest compressions during CPR failed to improve survival or neurologic function compared with standard chest compressions that are briefly interrupted for ventilation, based on findings in the first large randomized trial to compare the two strategies for out-of-hospital, nontraumatic cardiac arrest.
In a presentation at the American Heart Association scientific sessions, simultaneously published online November 9 in the New England Journal of Medicine, Dr Graham Nichol and his associates analyzed data from the Resuscitation Outcomes Consortium, a network of clinical centers and EMS agencies that have expertise in conducting research on out-of-hospital cardiac arrest.1
Data were analyzed for 23,711 adults treated by 114 EMS agencies affiliated with eight clinical centers across the United States and Canada. These agencies were grouped into 47 clusters that were randomly assigned to perform CPR using either continuous chest compressions (100 per minute) with asynchronous positive-pressure ventilations (10 per minute) or standard chest compressions interrupted for ventilations (at a rate of 30 compressions per two ventilations) at every response to an out-of-hospital cardiac arrest. Twice per year, each cluster crossed over to the other resuscitation strategy, said Dr Nichol of the University of Washington–Harborview Center for Prehospital Emergency Care and Clinical Trial Center in Seattle.
A total of 12,653 patients were assigned to continuous chest compressions (the intervention group) and 11,058 to interrupted chest compressions (the control group). The primary outcome—the rate of survival to hospital discharge—was 9.0% in the intervention group and 9.7% in the control group, a nonsignificant difference. Similarly, the rate of survival with favorable neurologic function did not differ significantly, at 7.0% and 7.7%, respectively, the investigators said.1
However, it is also possible that three important limitations of this trial unduly influenced the results.
First, the per-protocol analysis, which used an automated algorithm to assess adherence to the compression assignments, could not classify many patients as having received either continuous or interrupted chest compressions. Second, the quality of postresuscitation care, which certainly influences outcomes, was not monitored. And third, actual oxygenation levels were not measured, nor were minutes of ventilation delivered. Thus, “we do not know whether there were important differences in oxygenation or ventilation between the two treatment strategies,” he said.
It is not yet clear why this large randomized trial1 showed no benefit from continuous chest compressions when previous observational research showed the opposite. One possibility is that many of the previous studies assessed not just chest compressions but an entire bundle of care related to CPR, so the benefits they reported may not be attributable to chest compressions alone.
In addition, in this study the mean chest-compression fraction – the proportion of each minute during which compressions are given, an important marker of interruptions in chest compressions – was already high in the control group (0.77) and not much different from that in the intervention group (0.83). Both of these are much higher than the target recommended by both American and European guidelines, which is only 0.60.
And of course a third reason may be that the interruptions for ventilation during CPR aren’t all that critical, and may be less detrimental to survival, than is currently believed.
Dr Rudolph W. Koster is in the department of cardiology at Amsterdam Academic Medical Center. He reported having no relevant financial disclosures. Dr Koster made these remarks in an editorial accompanying Dr Nichol’s report (Koster RW. Continuous or interrupted chest compressions for cardiac arrest [published online ahead of print November 9, 2015]. N Engl J Med).
Answers elusive in quest for better chlamydia treatment
BY BRUCE JANCIN
EXPERT ANALYSIS FROM ICAAC 2015
SAN DIEGO – The hottest topic today in the treatment of sexually transmitted diseases caused by Chlamydia trachomatis is the unresolved question of whether azithromycin is still as effective as doxycycline, the other current guideline-recommended, first-line therapy, Dr Kimberly Workowski said at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy.
“This is important, because doxycycline is administered twice a day for 7 days, and azithromycin is given as a single pill suitable for directly observed therapy,” noted Dr Workowski, professor of medicine at Emory University in Atlanta and lead author of the 2015 Centers for Disease Control and Prevention STD treatment guidelines.1
Several recent retrospective case series have suggested azithromycin is less effective, with the biggest efficacy gap being seen in rectal C. trachomatis infections. These nonrandomized studies were further supported by an Australian meta-analysis of six randomized, controlled trials comparing the two antibiotics for the treatment of genital chlamydia. The investigators found roughly 3% greater efficacy for doxycycline, compared with azithromycin, for urogenital chlamydia, and a 7% advantage for doxycycline in treating symptomatic urethral infection in men.
However, the investigators were quick to add the caveat that “the quality of the evidence varies considerably.”2
There’s a pressing need for better data. Dr Workowski and her colleagues on the STD guidelines panel are eagerly awaiting the results of a well-structured randomized trial led by Dr William M. Geisler, professor of medicine at the University of Alabama, Birmingham. The investigators randomized more than 300 chlamydia-infected male and female inmates in youth correctional facilities to guideline-recommended azithromycin at 1 g orally in a single dose or oral doxycycline at 100 mg twice daily for 7 days. The results, which are anticipated soon, should influence clinical practice, Dr Workowski said.
Here’s what else is new in chlamydia:
Pregnancy: For treatment of chlamydia in pregnancy, amoxicillin at 500 mg orally t.i.d. for 7 days has been demoted from a first-line recommended therapy to alternative-regimen status. Now, the sole recommended first-line treatment in pregnancy is oral azithromycin at 1 g orally in a single dose.
“We did this based on in vitro studies showing Chlamydia trachomatis is not well-killed by amoxicillin. Instead, the drug induces persistent viable noninfectious forms which can sometimes reactivate,” Dr Workowski explained.
Delayed-release doxycycline: This FDA-approved drug, known as Doryx, administered as a 200-mg tablet once daily for 7 days, “might be an alternative” to the standard generic doxycycline regimen of 100 mg twice daily for 7 days, according to the current Centers for Disease Control and Prevention guidelines. In a randomized, double-blind trial, the new agent was as effective as twice-daily generic doxycycline in men and women with urogenital C. trachomatis infection, and it had fewer gastrointestinal side effects. Doryx is costlier than the twice-daily alternatives.
Lymphogranuloma venereum: The current guidelines repeat a point made in previous editions, but one Dr Workowski believes remains underappreciated and thus worthy of emphasis: Rectal exposure to C. trachomatis serovars L1, L2, and L3 in men who have sex with men or in women who have rectal sex can cause lymphogranuloma venereum, which takes the form of proctocolitis mimicking inflammatory bowel disease.
Patients suspected of having lymphogranuloma venereum should be started presumptively on the recommended regimen for this STD, which is oral doxycycline at 100 mg b.i.d. for 21 days.
“If you also see painful ulcers or, on anoscopy, mucosal ulcers, you should also treat empirically for herpes simplex until your culture results come back,” she added.
Dr Workowski reported having no financial conflicts of interest.
Catheter-directed thrombolysis trumps systemic for acute pulmonary embolism
BY MITCHEL L. ZOLER
AT CHEST 2015
Vitals Key clinical point: Catheter-directed thrombolysis was linked to reduced mortality, compared with systemic thrombolysis in patients with an acute pulmonary embolism. Major finding: In-hospital mortality in acute pulmonary embolism patients ran 10% with catheter-directed thrombolysis and 17% with systemic thrombolysis. Data source: Review of 1,521 US patients treated for acute pulmonary embolism during 2010-2012 in the National Inpatient Sample. Disclosures: Dr Saqib and Dr Muthiah had no disclosures. |
MONTREAL – Catheter-directed thrombolysis surpassed systemic thrombolysis for minimizing in-hospital mortality of patients with an acute pulmonary embolism in a review of more than 1,500 United States patients.
The review also found evidence that US pulmonary embolism (PE) patients increasingly undergo catheter-directed thrombolysis, with usage jumping by more than 50% from 2010 to 2012, although in 2012 US clinicians performed catheter-directed thrombolysis on 160 patients with an acute pulmonary embolism (PE) who were included in a national US registry of hospitalized patients, Dr Amina Saqib said at the annual meeting of the American College of Chest Physicians.
Catheter-directed thrombolysis resulted in a 9% in-hospital mortality rate and a 10% combined rate of in-hospital mortality plus intracerebral hemorrhages, rates significantly below those tallied in propensity score-matched patients who underwent systemic thrombolysis of their acute PE. The matched group with systemic thrombolysis had a 17% in-hospital mortality rate and a 17% combined mortality plus intracerebral hemorrhage rate, said Dr Saqib, a researcher at Staten Island (New York) University Hospital.
“To the best of our knowledge, this is the first, large, nationwide, observational study that compared safety and efficacy outcomes between systemic thrombolysis and catheter-directed thrombolysis in acute PE,”
Dr Saqib said.
The US data, collected during 2010-2012, also showed that, after adjustment for clinical and demographic variables, each acute PE treatment by catheter-directed thrombolysis cost an average $9,428 above the cost for systemic thrombolysis, she said.
Dr Saqib and her associates used data collected by the Federal National Inpatient Sample. Among US patients hospitalized during 2010-2012 and entered into this database, they identified 1,169 adult acute PE patients who underwent systemic thrombolysis and 352 patients who received catheter-directed thrombolysis. The patients averaged about 58 years old and just under half were men.
The propensity score-adjusted analysis also showed no statistically significant difference between the two treatment approaches for the incidence of intracerebral hemorrhage, any hemorrhages requiring a transfusion, new-onset acute renal failure, or hospital length of stay. Among the patients treated by catheter-directed thrombolysis, all the intracerebral hemorrhages occurred during 2010; during 2011 and 2012 none of the patients treated this way had an intracerebral hemorrhage, Dr Saqib noted.
Although the findings were consistent with results from prior analyses, the propensity-score adjustment used in the current study cannot fully account for all unmeasured confounding factors. The best way to compare catheter-directed thrombolysis and systemic thrombolysis for treating acute PE would be in a prospective, randomized study, Dr Saqib said.
Survivors of out-of-hospital cardiac arrest usually had intact brain function
BY AMY KARON
FROM THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Most adults who survived out-of-hospital cardiac arrests remained neurologically intact, regardless of duration of CPR in the field. Major finding: Only 12% of patients survived, but 84% of survivors had a cerebral performance category of 1 or 2, including 10% who underwent more than 35 minutes of CPR before reaching the hospital. Data source: A retrospective observational study of 3,814 adults who had an out-of-hospital cardiac arrest between 2005 and 2014. Disclosures: Dr Williams had no disclosures. The senior author disclosed research funding from the Medtronic Foundation. |
Most adults who survived out-of-hospital cardiac arrests remained neurologically intact, even if cardiopulmonary resuscitation lasted longer than has been recommended, authors of a retrospective observational study reported at the American Heart Association scientific sessions.
Dr Jefferson Williams of the Wake County Department of Emergency Medical Services in Raleigh, North Carolina, and his associates studied 3,814 adults who had a cardiac arrest outside the hospital between 2005 and 2014. Only 12% of patients survived, but 84% of survivors had a cerebral performance category of 1 or 2, including 10% who underwent more than 35 minutes of CPR before reaching the hospital.
Neurologically intact survival was associated with having an initial shockable rhythm, a bystander-witnessed arrest, and return of spontaneous circulation in the field rather than in the hospital. Age, basic airway management, and therapeutic hypothermia phase also predicted survival with intact brain function, but duration of CPR did not.
Procalcitonin assay detects invasive bacterial infection
BY MARY ANN MOON
FROM JAMA PEDIATRICS
Vitals Key clinical point: The procalcitonin assay was superior to three other tests at detecting invasive bacterial infection in febrile infants aged 7-91 days. Major finding: At a threshold of 0.3 ng/mL or more, procalcitonin level detected invasive bacterial infections with a sensitivity of 90%, a specificity of 78%, and a negative predictive value of 0.1. Data source: A multicenter prospective cohort study involving 2,047 infants treated at pediatric EDs in France during a 30-month period. Disclosures: The French Health Ministry funded the study. Dr Milcent and her associates reported having no financial disclosures. |
The procalcitonin assay was superior to C-reactive protein, neutrophil, and white blood cell measurements at identifying invasive bacterial infections in very young febrile infants, according to a study published in JAMA Pediatrics.1
Compared with other biomarker assays, procalcitonin assays allow earlier detection of certain infections in older children. A few small studies have hinted at the usefulness of procalcitonin assays in infants, but to date no large prospective studies have assessed these assays in the youngest infants. For this prospective study, researchers evaluated the diagnostic accuracy of procalcitonin and other biomarkers in a study of 2,047 febrile infants aged 7-91 days who presented to 15 pediatric emergency departments in France during a 30-month period.
“We did not include infants 6 days or younger because they are likely to have early-onset sepsis related to perinatal factors and because physiologic procalcitonin concentrations during the first [few] days of life are higher than thereafter,” said Dr Karen Milcent of Hôpital Antoine Béclère, Clamart (France), and her associates.
Serum samples were collected at the initial clinical examination, but procalcitonin assays were not performed at that time. Attending physicians diagnosed the infants as having either bacterial or nonbacterial infections without knowing the procalcitonin results. Then, procalcitonin tests were done retrospectively on frozen serum samples by lab personnel who were blinded to the infants’ clinical features. Thirteen (1.0%) infants had bacteremia and 8 (0.6%) had bacterial meningitis.
The procalcitonin assay was significantly more accurate at identifying invasive bacterial infections than was C-reactive protein level, absolute neutrophil count, or white blood cell count. At a threshold of 0.3 ng/mL or more, the procalcitonin level had a sensitivity of 90%, a specificity of 78%, and a negative predictive value of 0.1. In addition, the procalcitonin assay was the most accurate in a subgroup analysis restricted to patients whose fever duration was less than 6 hours and another subgroup analysis restricted to patients younger than 1 month of age, the researchers said.1
For young febrile infants, combining procalcitonin assay results with a careful case history, a thorough physical examination, and other appropriate testing offers the potential of avoiding lumbar punctures. These study findings “should encourage the development of decision-making rules that incorporate procalcitonin,” Dr Milcent and her associates said.
The findings by Milcent et al are an important step forward in managing very young febrile infants, which remains a vexing problem.
A vital next step is to find alternatives to culture-based testing of blood, urine, and CSF. Genomic technologies that reliably detect molecular signatures in small amounts of biologic samples may be one such alternative. They may offer the additional benefit of identifying the pathogen and the host’s response to the presence of the pathogen.
Dr Nathan Kuppermann is in the departments of emergency medicine and pediatrics at the University of California–Davis. Dr Prashant Mahajan is in the departments of pediatrics and emergency medicine at Children’s Hospital of Michigan and Wayne State University, Detroit. They have no relevant financial disclosures. They made these remarks in an editorial accompanying Dr Milcent’s report (Kuppermann N, Mahajan P. Role of serum procalcitonin in identifying young febrile infants with invasive bacterial infections: one step closer to the holy grail [published online ahead of print November 23, 2015]? JAMA Ped. doi:10.1001/jamapediatrics.2015.3267).
Out-of-hospital MI survival is best in the Midwest
BY BRUCE JANCIN
AT THE AHA SCIENTIFIC SESSIONS
Vitals Key clinical point: Substantial and as-yet unexplained regional differences in survival and total hospital charges following out-of-hospital cardiac arrest exist across the United States. Major finding: Mortality among adults hospitalized after experiencing out-of-hospital cardiac arrest was 14% lower in the Midwest than in the Northeast. Data source: A retrospective analysis of data from the Nationwide Inpatient Sample for 2002-2012 that included 155,592 adults with out-of-hospital cardiac arrest who survived to hospital admission. Disclosures: The presenter reported having no financial conflicts of interest. |
ORLANDO – Considerable regional variation exists across the United States in outcomes, including survival and hospital charges following out-of-hospital cardiac arrest, Dr Aiham Albaeni reported at the American Heart Association scientific sessions.1
He presented an analysis of 155,592 adults who survived at least until hospital admission following non-trauma-related out-of-hospital cardiac arrest (OHCA) during 2002-2012. The data came from the Agency for Healthcare Research and Quality’s Nationwide Inpatient Sample, the largest all-payer US inpatient database.
Mortality was lowest among patients whose OHCA occurred in the Midwest. Indeed, taking the Northeast region as the reference point in a multivariate analysis, the adjusted mortality risk was 14% lower in the Midwest and 9% lower in the South. There was no difference in survival rates between the West and Northeast in this analysis adjusted for age, gender, race, primary diagnosis, income, Charlson Comorbidity Index, primary payer, and hospital size and teaching status, reported Dr Albaeni of Johns Hopkins University, Baltimore, Maryland.
Total hospital charges for patients admitted following OHCA were far and away highest in the West, and this increased expenditure didn’t pay off in terms of a survival advantage. The Consumer Price Index–adjusted mean total hospital charges averaged $85,592 per patient in the West, $66,290 in the Northeast, $55,257 in the Midwest, and $54,878 in the South.
Outliers in terms of cost of care—that is, patients admitted with OHCA whose total hospital charges exceeded $109,000 per admission—were 85% more common in the West than the other three regions, he noted.
Hospital length of stay greater than 8 days occurred most often in the Northeast. These lengthier stays were 10% to 12% less common in the other regions.
The explanation for the marked regional differences observed in this study remains unknown.
“These findings call for more efforts to identify a high-quality model of excellence that standardizes health care delivery and improves quality of care in low-performing regions,” said Dr Albaeni.
He reported having no financial conflicts of interest regarding his study.
Modified Valsalva more than doubled conversion rate in supraventricular tachycardia
BY AMY KARON
FROM THE LANCET
Vitals Key clinical point: A modified version of the Valsalva maneuver, in which patients were immediately laid flat afterward with their legs passively raised, more than doubled the rate of conversion from acute supraventricular tachycardia to normal sinus rhythm as compared with the standard Valsalva maneuver. Major finding: The conversion rate was 43% for the modified Valsalva group and 17% for patients undergoing the standard maneuver (adjusted OR, 3.7; P < .0001). Data source: Multicenter, randomized, controlled, parallel-group trial of 428 patients presenting to emergency departments with acute SVT. Disclosures: The National Institute for Health Research funded the study. The investigators declared no competing interests. |
A modified version of the Valsalva maneuver more than doubled the rate of conversion from acute supraventricular tachycardia to normal sinus rhythm when compared with the standard maneuver, said authors of a randomized, controlled trial published in the Lancet.
In all, 93 of 214 (43%) emergency department patients with acute supraventricular tachycardia (SVT) achieved cardioversion a minute after treatment with the modified Valsalva maneuver, compared with 37 (17%) of patients treated with standard Valsalva (adjusted odds ratio, 3.7; 95% CI, 2.3-5.8; P < .0001), reported Dr Andrew Appelboam of Royal Devon and Exeter (England) Hospital NHS Foundation Trust and his associates.
Standard Valsalva is safe, but achieves cardioversion for only 5% to 20% of patients with acute SVT. Nonresponders usually receive intravenous adenosine, which causes transient asystole and has other side effects, including a sense of “impending doom” or imminent death, the investigators noted.1
For the modified Valsalva maneuver, patients underwent standardized strain at 40 mm Hg pressure for 15 seconds while semi-recumbent, but then immediately laid flat while a staff member raised their legs to a 45-degree angle for 15 seconds. They returned to the semi-recumbent position for another 45 seconds before their cardiac rhythm was reassessed. The control group simply remained semirecumbent for 60 seconds after 15 seconds of Valsalva strain.
The adapted technique should achieve the same rate of cardioversion in community practice, and clinicians should repeat it once if it is not initially effective, said the researchers. “As long as individuals can safely undertake a Valsalva strain and be repositioned as described, this maneuver can be used as the routine initial treatment for episodes of supraventricular tachycardia regardless of location,” they said. Patients did not experience serious adverse effects, and transient cardiac events were self-limited and affected similar proportions of both groups, they added.
The National Institute for Health Research funded the study. The researchers declared no competing interests.
Off-label prescriptions link to more adverse events
BY MARY ANN MOON
FROM JAMA INTERNAL MEDICINE
Vitals Key clinical point: Off-label prescribing in adults is common and very likely to cause adverse events. Major finding: The incidence of adverse events was 44% higher for off-label use (19.7 per 10,000 person-months) than for on-label use (12.5 per 10,000 person-months) of prescription drugs. Data source: A prospective cohort study of 46,021 adults who received 151,305 incident prescriptions from primary care clinicians in Quebec during a 5-year period. Disclosures: No sponsors were identified for this study. Dr Tewodros Eguale and his associates reported having no relevant financial disclosures. |
Off-label prescribing of drugs is common and very likely to cause adverse events, particularly when no strong scientific evidence supports the off-label use, according to a report published in JAMA Internal Medicine.
No systematic investigation of the off-label use of prescription drugs has been done to date, in part because physicians aren’t required to document intended indications. Recent innovations in electronic health records provided an opportunity to track off-label prescribing and its influence on adverse drug events for all 8.5 million residents in the Canadian province of Quebec. There, physicians must provide the indication for every new prescription, the reason for any dose changes or drug discontinuation, and the nature of any adverse events, said Dr Tewodros Eguale of the department of epidemiology, biostatistics, and occupational health at McGill University, Montreal, and his associates.
“Selected examples of adverse events associated with the most frequently used off-label drugs include akathisia resulting from the use of gabapentin for neurogenic pain; agitation associated with the use of amitriptyline hydrochloride for migraine; hallucinations with the use of trazodone hydrochloride for insomnia; QT interval prolongation with the use of quetiapine fumarate for depression; and weight gain with the use of olanzapine for depression,” the authors reported.
Prescribing information in electronic medical records of 46,021 adults (mean age 58 years) given 151,305 new prescriptions was analyzed during a 5-year period. Physicians reported off-label use in 17,847 (12%) of these prescriptions, and that off-label use lacked strong scientific evidence in 81% of cases. The median follow-up time for use of prescribed medications was 386 days (range, 1 day to 6 years).
The class of drugs with the highest rate of adverse effects was anti-infective agents (66.2 per 10,000 person-months), followed by central nervous system drugs such as antidepressants, anxiolytics, and antimigraine medicine (18.1 per 10,000); cardiovascular drugs (15.9 per 10,000); hormonal agents (12.7); autonomic drugs including albuterol and terbutaline (8.4); gastrointestinal drugs (6.1); ear, nose, and throat medications (2.8); and “other” agents such as antihistamines, blood thinners, and antineoplastics (1.3).
“Off-label use may be clinically appropriate given the complexity of the patient’s condition, the lack of alternative effective drugs, or after exhausting approved drugs.” However, previous research has shown that physicians’ lack of knowledge of approved treatment indications was one important factor contributing to off-label prescribing. And one study showed that physicians are finding it difficult to keep up with rapidly changing medication information, and this lack of knowledge is affecting treatment, Dr Eguale and his associates said.
That knowledge gap could be filled by supplying clinicians with information regarding drug approval status and the quality of supporting scientific evidence at the point of care, when they write prescriptions into patients’ electronic health records, the investigators noted. This would have the added advantage of facilitating communication among physicians, pharmacists, and patients, and could reduce medication errors such as those caused by giving drugs to the wrong patients or by giving patients sound-alike or look-alike drugs.
No sponsors were identified for this study. Dr Tewodros Eguale and his associates reported having no relevant financial disclosures.
This study, the most extensive and informative one to evaluate the safety of off-label drug use in adults to date, shows that clinicians often enter an arena of the unknown when they expand prescribing beyond the carefully devised confines of the labeled indication. It provides compelling evidence that off-label prescribing is frequently inappropriate and substantially raises the risk for an adverse event.
Even in cases in which an off-label indication has been studied, the pharmacokinetics, drug-disease interactions, drug-drug interactions, and other safety considerations weren’t studied to the degree required during the drug approval process. Moreover, how many clinicians have the time or motivation to review the evidence for those off-label indications, arriving at a balanced assessment of risks and benefits?
Dr Chester B. Good is in pharmacy benefits management services at the US Department of Veterans Affairs in Hines, Illinois, and the department of pharmacy and therapeutics at the University of Pittsburgh. Dr Good and Dr Walid F. Gellad are in the department of medicine at the University of Pittsburgh and at the Center for Health Equity Research and Promotion in the Veterans Affairs Pittsburgh Healthcare System. Dr Good and Dr Gellad reported serving as unpaid advisers to the Food and Drug Administration’s Drug Safety Oversight Board. They made these remarks in an Invited Commentary accompanying Dr Eguale’s report (Good CB, Gellad WF. Off-label drug use and adverse drug events: turning up the heat on off-label prescribing [published online ahead of print November 2, 2014]. JAMA Intern Med. doi:10.1001/jamainternmed.2015.6068).
Dr Lappin is an assistant professor and an attending physician, department of mergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical College, New York.
- FDA approves first naloxone nasal spray for opioid overdose
- FDA moves quickly to approve easy-to-use nasal spray to treat opioid overdose [press release]. Silver Spring, MD: US Food and Drug Administration; November 18, 2015. Updated November 19, 2015.
- Therapeutic hypothermia after nonshockable-rhythm cardiac arrest
- Perman SM, Grossestreuer AV, Wiee DJ, Carr BG, Abella BS, Gaieski DF. The utility of therapeutic hypothermia for post-cardiac arrest syndrome patients with an initial non-shockable rhythm [published online ahead of print November 16, 2015]. Circulation. pii:CIRCULATIONAHA.115.016317.
- Andexanet reverses anticoagulant effects of factor Xa inhibitors
- Siegal DM, Cornutte JT, Connolly SJ, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity [published online ahead of print November 11, 2015]. N Engl J Med.
- Continuous no better than interrupted chest compressions
- Nichol G, Leroux B, Wang H, et al; ROC Investigators. Trial of continuous or interrupted chest compressions during CPR [published online ahead of print November 9, 2015]. N Engl J Med.
- Answers elusive in quest for better chlamydia treatment
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1-137.
- Kong FY, Tabrizi SN, Law M, et al. Azithrmycin versus doxycycline for the treatment of genital chlamydia infection: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014;59(2):193-205.
- Procalcitonin assay detects invasive bacterial infection
- Milcent K, Faesch S, Gras-Le Guen C, et al. Use of procalcitonin assays to predict serious bacterial infection in young febrile infants [published online ahead of print November 23, 2015]. JAMA Pediatr. doi: 10.1001/jamapediatrics.2015.3210.
- Out-of-hospital MI survival is best in the Midwest
- Shaker M, Albaeni A, Rios R. Impact of Change in Resuscitation Guidelines on National Out-of-hospital Cardiac Arrest Outcomes: Fulfilled Expectations? Paper presented at: American Heart Association 2015 Scientific Sessions; November 7-11, 2015; Orlando, Florida.
- Modified Valsalva more than doubled conversion rate in supraventricular tachycardia
- Appelboam A, Reuben A, Mann C, et al; REVERT trial collaborators. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015;386(10005):1747-1753.
- Off-label prescriptions link to more adverse events
- Eguale T, Buckeridge DL, Verma A, et al. Association of off-label drug use and adverse drug events in an adult population [published online ahead of print November 2, 2015]. JAMA Intern Med. doi: 10.1001/jamainternmed.2015.6058.
- FDA approves first naloxone nasal spray for opioid overdose
- FDA moves quickly to approve easy-to-use nasal spray to treat opioid overdose [press release]. Silver Spring, MD: US Food and Drug Administration; November 18, 2015. Updated November 19, 2015.
- Therapeutic hypothermia after nonshockable-rhythm cardiac arrest
- Perman SM, Grossestreuer AV, Wiee DJ, Carr BG, Abella BS, Gaieski DF. The utility of therapeutic hypothermia for post-cardiac arrest syndrome patients with an initial non-shockable rhythm [published online ahead of print November 16, 2015]. Circulation. pii:CIRCULATIONAHA.115.016317.
- Andexanet reverses anticoagulant effects of factor Xa inhibitors
- Siegal DM, Cornutte JT, Connolly SJ, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity [published online ahead of print November 11, 2015]. N Engl J Med.
- Continuous no better than interrupted chest compressions
- Nichol G, Leroux B, Wang H, et al; ROC Investigators. Trial of continuous or interrupted chest compressions during CPR [published online ahead of print November 9, 2015]. N Engl J Med.
- Answers elusive in quest for better chlamydia treatment
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1-137.
- Kong FY, Tabrizi SN, Law M, et al. Azithrmycin versus doxycycline for the treatment of genital chlamydia infection: a meta-analysis of randomized controlled trials. Clin Infect Dis. 2014;59(2):193-205.
- Procalcitonin assay detects invasive bacterial infection
- Milcent K, Faesch S, Gras-Le Guen C, et al. Use of procalcitonin assays to predict serious bacterial infection in young febrile infants [published online ahead of print November 23, 2015]. JAMA Pediatr. doi: 10.1001/jamapediatrics.2015.3210.
- Out-of-hospital MI survival is best in the Midwest
- Shaker M, Albaeni A, Rios R. Impact of Change in Resuscitation Guidelines on National Out-of-hospital Cardiac Arrest Outcomes: Fulfilled Expectations? Paper presented at: American Heart Association 2015 Scientific Sessions; November 7-11, 2015; Orlando, Florida.
- Modified Valsalva more than doubled conversion rate in supraventricular tachycardia
- Appelboam A, Reuben A, Mann C, et al; REVERT trial collaborators. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial. Lancet. 2015;386(10005):1747-1753.
- Off-label prescriptions link to more adverse events
- Eguale T, Buckeridge DL, Verma A, et al. Association of off-label drug use and adverse drug events in an adult population [published online ahead of print November 2, 2015]. JAMA Intern Med. doi: 10.1001/jamainternmed.2015.6058.

First EDition: News for and about the practice of emergency medicine
New CPR Guide Sets Compression Limits, Scratches Vasopressin
By Shannon Aymes
From Circulation
New guidelines on cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) set upper limits on chest compression rate and depth, add naloxone to the care of suspected opioid abusers, and remove vasopressin from the advanced cardiac life support (ACLS) algorithm.
Vitals Key clinical point: The percentage of nonmedical use of prescription opioids declined during the last decade, but the prevalence of use disorders, the frequency of abuse, and related mortality all increased. Major finding: The 1-year prevalence of opioid use disorders rose from 0.6% to 0.9%, that of high-frequency use increased from 0.3% to 0.4%, and that of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. Data source: An analysis of time trends in prescription opioid use, based on two nationally representative data sets involving 472,200 adults. Disclosures: The Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse, and the US Food and Drug Administration (FDA) sponsored the study. Dr Han reported having no relevant disclosures; an associate reported owning stock in General Electric, 3M Company, and Pfizer. |
The American Heart Association (AHA) published its revised guidelines October 15 in Circulation.1 The AHA released its previous guidelines in 2010.2
“When everyone knows their role, knows CPR, and works together, we can dramatically improve cardiac arrest victims’ chances of survival,” Dr Mark Creager, AHA president and director of the Heart and Vascular Center at Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, said in a statement.
The 2015 guidelines’ new recommendations include the following:
Resuscitation pathways. The guidelines note that the resuscitation pathways are very different for patients who experience cardiac arrest present in either a hospital setting (IHCA) or out-of-hospital setting (OHCA). In an OHCA, the patient depends on lay rescuers to not only recognize the situation but also call for help, initiate CPR, and, if available, administer defibrillation until emergency medical personnel arrive. However, IHCA involves prevention of cardiac arrest and smooth delivery of care in a multidisciplinary setting.

Compression rate and depth. The new guidelines set upper limits on chest compression depth and heart rate, recommending a compression rate of 100-120 compressions per minute with a depth of at least 2 inches, not to exceed 2.4 inches in adults.
Social media dispatching. Despite limited evidence, the guideline authors said that it may be reasonable for communities to use social media technologies to alert lay rescuers with mobile phones about nearby OHCA cases.
Naloxone and opioid addiction. Also new to the guidelines is the recommended use of naloxone for patients with suspected or known opioid addiction by appropriately trained lay rescuers or basic life support (BLS) providers.
CPR training. The guidelines highlight several changes to simplify health care provider training in CPR. For example, trained rescuers can simultaneously perform some tasks to reduce the time to initiate chest compressions. Likewise, in a team of trained rescuers, multiple steps—such as activating the emergency response system, chest compression, ventilation, and defibrillator retrieval—can be accomplished simultaneously.
High-quality CPR. The guidelines focus on emphasizing high-quality CPR with adequate compression rate and depth, complete chest recoil, few interruptions to compressions, and appropriate ventilation.
The guidelines offer several changes to advanced cardiac life support (ACLS). The algorithm was simplified by removing vasopressin, because the authors note that “the combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest.”
Likewise, the guidelines note conflicting studies to support the use of lidocaine after return of spontaneous circulation (ROSC). “However, the initiation or continuation of lidocaine may be considered immediately after ROSC from VF/pulseless ventricular tachycardia cardiac arrest,” the guideline authors wrote.
Finally, the guidelines highlight updates in post–cardiac arrest care, including a wider range of target temperatures, between 32°C and 36°C, to be maintained for at least 24 hours in comatose adults with ROSC after cardiac arrest. In comparison, the 2010 guidelines called for a target temperature range of 32°C to 34°C for 12 to 24 hours.
The guidelines also detail new updates for acute coronary syndrome, pediatric BLS, pediatric ACLS, and neonatal resuscitation.
Complex Picture Emerges of Prescription Opioid Abuse
By Mary Ann Moon
From JAMA

These findings—from an analysis of two large nationally representative data sets—paint a picture that is complex and more nuanced than that suggested by some recent reports. For example, a study of the Researched Abuse, Diversion, and Addiction-Related Surveillance (RADARS) System found that the abuse and diversion of prescription opioids plateaued or decreased in recent years.3 “The nationally representative results in our study may be especially important in providing an accurate picture of the current status of the epidemic,” said Dr Beth Han of the Substance Abuse and Mental Health Services Administration (SAMHSA), Rockville, Maryland, and her associates.
The nonmedical use of prescription opioids is an acknowledged epidemic, but that epidemic’s changing pattern over time needed to be updated. The investigators assessed the changes in use during the most recent decade for which data are available (2003-2013) using annual surveys conducted by SAMHSA and cause of death files from the National Vital Statistics System.
Based on responses from 472,200 people aged 18 to 64 years, the 1-year prevalence of nonmedical use of prescription opioids decreased from 5.4% to 4.9% during the study period. However, the 1-year prevalence of use disorders rose from 0.6% to 0.9%, the 1-year prevalence of high-frequency use (200 days or more per year) increased from 0.3% to 0.4%, and the rate of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. In addition, the mean number of days of opioid abuse increased from 2.1 to 2.6 per year in the general population and from 40.0 to 54.2 days per year among acknowledged opioid users, the investigators said.1
Compared with white users of prescription opioids, both black and Hispanic users had a lower prevalence of use disorders. The prevalence of use disorders was higher among less-educated than more-educated adults, among those with no health insurance or Medicaid as opposed to private health insurance, and among smokers than nonsmokers, Dr Han and her associates added.
Previous research has shown that most adults who abuse prescription opioids neither receive treatment nor perceive that they need treatment. Clinicians can help by using prescription-drug monitoring programs to identify inappropriate receipt of prescription opioids, then offering treatments, which are highly effective, for patients who need them, the investigators noted.
The slight decline (approximately 0.4% over 10 years) in opioid initiation reported by Han et al1 may be encouraging, but their other findings suggest that more patients are experiencing an inexorable progression from initial opioid use to frequent use to highly frequent use to a use disorder.
The source of most opioid abuse is often a seemingly legitimate prescription, and the key to addressing the opioid-abuse epidemic is to keep opioid-naive patients opioid naive. It is still unclear why clinicians continue to prescribe opioids, despite recommendations to the contrary and the fact that these agents provide little or no long-term benefit for most types of chronic pain.
Lewis S. Nelson, MD, is in the Ronald O. Perelman department of emergency medicine at New York University. He and his associates made these remarks in an editorial2 accompanying Dr Han’s report.1
US Injury Costs Topped $671 Billion in 2013
By Richard Franki
From MMWR
Over 30 million injuries were treated in US EDs in 2013, costing an estimated $671 billion, the CDC reported.
The largest share of that cost—almost $290 billion, or about 43%—came from the 3 million persons with nonfatal injuries who were hospitalized. Costs for the 27 million people who were treated and released from EDs were $167 billion, which was just under 25% of the total. The lifetime cost estimate for the almost 193,000 injury-associated deaths in 2013 was over $214 billion (32%), said Curtis Florence, PhD, of the CDC’s National Center for Injury Prevention and Control, Atlanta, Georgia, and associates.
For each ED-treated injury-related death, the mean cost in terms of lost lifetime earnings and medical care provided was just over $1.1 million: Homicides cost over $1.6 million, suicides were $1.2 million each, and each unintentional injury death cost just under $1 million, they said.1
Drug poisonings, including prescription drug overdoses, accounted for the largest share of fatal injury costs (27%), followed by transportation-related deaths (23%) and firearm-related deaths (22%), Dr Florence and associates noted.
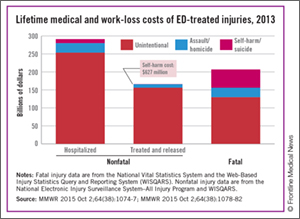
“Injuries cost Americans far too much money, suffering, and preventable death,” CDC Director Tom Frieden said in a written statement. “The doubling of deaths by drug poisoning, including prescription drug overdose and heroin, is particularly alarming.”
The investigators used data from the National Vital Statistics System and the Web-Based Injury Statistics Query and Reporting System (WISQARS) for injury-related deaths and the National Electronic Injury Surveillance System–All Injury Program and WISQARS for nonfatal injuries.
Peramivir Effective Against Most Flu Viruses Circulating Globally
By Doug Brunk
AT ICAAC 2015
Vitals Key clinical point: Peramivir is potently effective against seasonal influenza viruses circulating globally. Major finding: During the 2013-2014 and 2014-2015 influenza seasons, about 99% of influenza type A and B viruses were inhibited by peramivir. Data source: An analysis of 8,426 influenza viruses that were tested during the 2013-2014 and 2014-2015 influenza seasons as part of the World Health Organization Global Influenza Surveillance and Response System.1 Disclosures: The researchers reporting having no financial disclosures. |
SAN DIEGO – The neuraminidase inhibitor peramivir inhibited about 99% of seasonal influenza A and B viruses circulating globally during the 2013 to 2014 and 2014 to 2015 influenza seasons, a large analysis demonstrated.
“The frequency of H1N1pdm09 viruses carrying neuraminidase (NA) H275Y remained low during both seasons; this mutation confers resistance to oseltamivir and peramivir,” said Margaret Okomo-Adhiambo, PhD, at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC/ICC 2015). In addition, “a small proportion of viruses contained other neuraminidase changes that affect binding of peramivir to viral enzymes and may decrease virus susceptibility. These changes need to be closely monitored.”
Approved by the FDA in December of 2014, peramivir (Rapivab) is the only antiviral agent for influenza treatment to come to market in nearly 20 years. Approved for intravenous administration as a single dose, it is indicated for adults with acute uncomplicated influenza who may have trouble taking orally administered or inhaled neuraminidase (NA) inhibitors. Other NA inhibitors approved by the FDA for influenza infection include oseltamivir, which is orally administered, and zanamivir, which is inhaled.
For the current analysis, Dr Okomo-Adhiambo of the influenza division at the US Centers for Disease Control and Prevention (CDC), Atlanta, and her associates tested influenza virus susceptibility to peramivir during the 2013-2014 and 2014-2015 influenza seasons as part of the World Health Organization Global Influenza Surveillance and Response System. A total of 8,426 viruses were tested, 75% of which were circulating in the United States.1
Dr Okomo-Adhiambo reported that during the 2013-2014 and 2014-2015 influenza seasons, about 99% of influenza type A and B viruses were inhibited by peramivir, except for a few viruses belonging to subtype A(H1N1)pdm09 (1.5%), subtype A(H3N2) (0.2%), and type B (0.4%). In addition, NA activity of type A viruses was five to six times more sensitive to inhibition by peramivir, compared with type B NA.
Parasitic Infection Emerging in the Southwestern United States
By Doug Brunk
At IDWEEK 2015
Vitals Key clinical point: Lesions containing a zoonotic parasite known as Onchocerca lupi are appearing in humans who reside in the Southwestern United States. Major finding: In three of six human cases, nodules containing Onchocerca lupi were located in the cervical spinal canal. Data source: A case report of the first six people in the United States to be infected with Onchocerca lupi. Disclosures: The researchers reported having no financial disclosures. |
SAN DIEGO – Onchocerca lupi, a zoonotic parasite previously described as causing eye disease in cats and dogs, as well as in humans from Europe, Asia, and the Middle East, is emerging in the Southwestern United States.
“The life cycle of this organism is not yet clearly defined, but likely includes a canine and/or feline animal reservoir, as well as an insect vector,” Dr Christiana Smith said in an interview at an annual scientific meeting on infectious diseases.1 “No specific risk factors for developing this disease have been identified, other than residing in or traveling through the Southwestern US.”
To date, six cases of humans infected by Onchocerca lupi have come to the attention of health officials, including those at the CDC, due to symptoms from a nodule containing the parasite, according to Dr Smith, a pediatrician with the University of Colorado School of Medicine and Children’s Hospital Colorado, Aurora. The affected patients range in age from 22 months to 50 years of age; three of the six reside in Arizona, two in New Mexico, and one in Texas.
In three of the six cases, the nodule was located in the cervical spinal canal. In the remaining three cases, nodules were located on the scalp, the forearm, and the superior rectus muscle of the orbit. Two of the patients reported insect bites at the nodule site years prior to presentation, while another patient owned a dog with eye lesions.
“No previous Onchocerca parasites are known to have tropism for the central nervous system,” Dr Smith said. “In addition, five of the six cases presented in children. It is not clear whether children are disproportionately affected by this disease, or whether they are diagnosed more frequently.”
Treatment included surgical excision and antiparasitic treatment for most cases. To date, all patients have remained asymptomatic following treatment. Dr Smith said that more information about Onchocerca lupi will become available as additional cases are described. “Continued epidemiologic investigation will help define the life cycle of this organism, describe the spectrum of human disease, develop approaches to diagnosis and management, and design prevention strategies,” she said.
IDWeek marks the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society. The researchers reported having no financial disclosures.
Europeans Adopt 1-Hour ED Chest Pain Triage
By Bruce Jancin
At the ESC Congress 2015
LONDON – The positive findings of the Biomarkers in Acute Cardiovascular Care (BACC) study1 reinforce a key change contained in the brand-new European Society of Cardiology guidelines for management of patients with acute coronary syndrome without ST-segment elevation: namely, that it’s appropriate to assess such patients using two measurements of a validated high-sensitivity cardiac troponin assay taken just 1 hour apart, according to Dr Kurt Huber.
The BACC results are the evidence-based icing on the cake in support of the new recommendation in the guidelines, released at the annual congress of the European Society of Cardiology. The BACC study, which included 1,045 patients who presented to a university ED with acute chest pain suggestive of an acute coronary syndrome without ST-segment elevation, was the latest of several studies to show that most such patients can either be safely sent home from the ED or ruled-in for acute MI in just 1 hour when evaluated using a high-sensitivity troponin assay backed by a validated patient-management algorithm. The result means reduced pressure on overcrowded EDs and less patient anxiety because of delayed diagnosis, Dr Huber, director of cardiology and emergency medicine at Wilhelminen Hospital in Vienna, observed during an interview at the meeting.
The BACC study, presented by Dr Dirk Westermann of the University Heart Center Hamburg (Germany), utilized a high-sensitivity cardiac troponin I assay. The 1-hour algorithm had a 99.7% negative predictive value for acute MI. A total of 53% of patients were ruled out or in for MI at the 1-hour mark; the rest required further evaluation.2
To view the video, search “Huber” at http://www.emed-journal.com/
- New CPR Guide Sets Compression Limits, Scratches Vasopressin
- Bhanji F, Donoghue AJ, Wolff MS, et al. Part 14: Education: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S561-S573.
- Cave DM, Gazmuri RJ, Otto CW, et al. Part 7: CPR techniques and devices: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 Suppl 3):S720-S728.
- Complex Picture Emerges of Prescription Opioid Abuse
- Han B, Compton WM, Jones CM, Cai R. Nonmedical prescription opioid use and use disorders among adults aged 18 through 64 years in the United States, 2003-2013. JAMA. 2015;314(14):1468-1478.
- Nelson LS, Juurlink DN, Perrone J. Addressing the opioid epidemic. JAMA. 2015;314(14):1453-1454.
- Severtson SG, Bartelson BB, Davis JM, et al. Reduced abuse, therapeutic errors, and diversion following reformulation of extended-release ocycodone in 2010. J Pain. 2013;14(10):1122-1130.
- US Injury Costs Topped $671 Billion in 2013
- Florence C, Simon T, Haegerich T, Luo F, Zhou C. Estimated lifetime medical and work-loss costs of fatal injuries – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;46(38):1074-1077.
- Florence C, Haegerich T, Simon T, Zhou C, Luo F. Estimated lifetime medical and work-loss costs of emergency department-treated nonfatal injuries – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(38):1078-1082.
- Peramivir Effective Against Most Flu Viruses Circulating Globally
- Okomo-Adhiambo M, Daniels J, Nguyen HT, et al. Peramivir Susceptibility Surveillance of Influenza A and B Viruses Circulated Globally, 2013-2015. Presented at: Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC) and the International Society of Chemotherapy (ISC)’s International Congress of Chemotherapy and Infection (ICC) 2015; September 17-21, 2015; San Diego, California
- Parasitic Infection Emerging in the Southwestern United States
- Smith C, Rao S, Dehority W, et al. Onchocerca lupi: An Emerging Parasitic Infection in the Southwestern United States. Poster presented at: Infectious Disease (ID) Week 2015; October 7-11, 2015; San Diego, California; Abstract 1971.
- Europeans Adopt 1-Hour ED Chest Pain Triage
- Universitätsklinikum Hamburg-Eppendorf. Biomarkers in Acute Cardiac Care (BACC). In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Available from: https://clinicaltrials.gov/ct2/show/NCT02355457. NLM Identifier: NCT02355457.
- Westermann D. Accurate and rapid diagnosis of myocardial infarction using a high sensitivity Troponin I 1-hour algorithm. Presented at: European Society of Cardiology (ESC) Congress; August 29 - September 2, 2015; London, England. FP NR 1161.
New CPR Guide Sets Compression Limits, Scratches Vasopressin
By Shannon Aymes
From Circulation
New guidelines on cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) set upper limits on chest compression rate and depth, add naloxone to the care of suspected opioid abusers, and remove vasopressin from the advanced cardiac life support (ACLS) algorithm.
Vitals Key clinical point: The percentage of nonmedical use of prescription opioids declined during the last decade, but the prevalence of use disorders, the frequency of abuse, and related mortality all increased. Major finding: The 1-year prevalence of opioid use disorders rose from 0.6% to 0.9%, that of high-frequency use increased from 0.3% to 0.4%, and that of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. Data source: An analysis of time trends in prescription opioid use, based on two nationally representative data sets involving 472,200 adults. Disclosures: The Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse, and the US Food and Drug Administration (FDA) sponsored the study. Dr Han reported having no relevant disclosures; an associate reported owning stock in General Electric, 3M Company, and Pfizer. |
The American Heart Association (AHA) published its revised guidelines October 15 in Circulation.1 The AHA released its previous guidelines in 2010.2
“When everyone knows their role, knows CPR, and works together, we can dramatically improve cardiac arrest victims’ chances of survival,” Dr Mark Creager, AHA president and director of the Heart and Vascular Center at Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, said in a statement.
The 2015 guidelines’ new recommendations include the following:
Resuscitation pathways. The guidelines note that the resuscitation pathways are very different for patients who experience cardiac arrest present in either a hospital setting (IHCA) or out-of-hospital setting (OHCA). In an OHCA, the patient depends on lay rescuers to not only recognize the situation but also call for help, initiate CPR, and, if available, administer defibrillation until emergency medical personnel arrive. However, IHCA involves prevention of cardiac arrest and smooth delivery of care in a multidisciplinary setting.
Compression rate and depth. The new guidelines set upper limits on chest compression depth and heart rate, recommending a compression rate of 100-120 compressions per minute with a depth of at least 2 inches, not to exceed 2.4 inches in adults.
Social media dispatching. Despite limited evidence, the guideline authors said that it may be reasonable for communities to use social media technologies to alert lay rescuers with mobile phones about nearby OHCA cases.
Naloxone and opioid addiction. Also new to the guidelines is the recommended use of naloxone for patients with suspected or known opioid addiction by appropriately trained lay rescuers or basic life support (BLS) providers.
CPR training. The guidelines highlight several changes to simplify health care provider training in CPR. For example, trained rescuers can simultaneously perform some tasks to reduce the time to initiate chest compressions. Likewise, in a team of trained rescuers, multiple steps—such as activating the emergency response system, chest compression, ventilation, and defibrillator retrieval—can be accomplished simultaneously.
High-quality CPR. The guidelines focus on emphasizing high-quality CPR with adequate compression rate and depth, complete chest recoil, few interruptions to compressions, and appropriate ventilation.
The guidelines offer several changes to advanced cardiac life support (ACLS). The algorithm was simplified by removing vasopressin, because the authors note that “the combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest.”
Likewise, the guidelines note conflicting studies to support the use of lidocaine after return of spontaneous circulation (ROSC). “However, the initiation or continuation of lidocaine may be considered immediately after ROSC from VF/pulseless ventricular tachycardia cardiac arrest,” the guideline authors wrote.
Finally, the guidelines highlight updates in post–cardiac arrest care, including a wider range of target temperatures, between 32°C and 36°C, to be maintained for at least 24 hours in comatose adults with ROSC after cardiac arrest. In comparison, the 2010 guidelines called for a target temperature range of 32°C to 34°C for 12 to 24 hours.
The guidelines also detail new updates for acute coronary syndrome, pediatric BLS, pediatric ACLS, and neonatal resuscitation.
Complex Picture Emerges of Prescription Opioid Abuse
By Mary Ann Moon
From JAMA
These findings—from an analysis of two large nationally representative data sets—paint a picture that is complex and more nuanced than that suggested by some recent reports. For example, a study of the Researched Abuse, Diversion, and Addiction-Related Surveillance (RADARS) System found that the abuse and diversion of prescription opioids plateaued or decreased in recent years.3 “The nationally representative results in our study may be especially important in providing an accurate picture of the current status of the epidemic,” said Dr Beth Han of the Substance Abuse and Mental Health Services Administration (SAMHSA), Rockville, Maryland, and her associates.
The nonmedical use of prescription opioids is an acknowledged epidemic, but that epidemic’s changing pattern over time needed to be updated. The investigators assessed the changes in use during the most recent decade for which data are available (2003-2013) using annual surveys conducted by SAMHSA and cause of death files from the National Vital Statistics System.
Based on responses from 472,200 people aged 18 to 64 years, the 1-year prevalence of nonmedical use of prescription opioids decreased from 5.4% to 4.9% during the study period. However, the 1-year prevalence of use disorders rose from 0.6% to 0.9%, the 1-year prevalence of high-frequency use (200 days or more per year) increased from 0.3% to 0.4%, and the rate of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. In addition, the mean number of days of opioid abuse increased from 2.1 to 2.6 per year in the general population and from 40.0 to 54.2 days per year among acknowledged opioid users, the investigators said.1
Compared with white users of prescription opioids, both black and Hispanic users had a lower prevalence of use disorders. The prevalence of use disorders was higher among less-educated than more-educated adults, among those with no health insurance or Medicaid as opposed to private health insurance, and among smokers than nonsmokers, Dr Han and her associates added.
Previous research has shown that most adults who abuse prescription opioids neither receive treatment nor perceive that they need treatment. Clinicians can help by using prescription-drug monitoring programs to identify inappropriate receipt of prescription opioids, then offering treatments, which are highly effective, for patients who need them, the investigators noted.
The slight decline (approximately 0.4% over 10 years) in opioid initiation reported by Han et al1 may be encouraging, but their other findings suggest that more patients are experiencing an inexorable progression from initial opioid use to frequent use to highly frequent use to a use disorder.
The source of most opioid abuse is often a seemingly legitimate prescription, and the key to addressing the opioid-abuse epidemic is to keep opioid-naive patients opioid naive. It is still unclear why clinicians continue to prescribe opioids, despite recommendations to the contrary and the fact that these agents provide little or no long-term benefit for most types of chronic pain.
Lewis S. Nelson, MD, is in the Ronald O. Perelman department of emergency medicine at New York University. He and his associates made these remarks in an editorial2 accompanying Dr Han’s report.1
US Injury Costs Topped $671 Billion in 2013
By Richard Franki
From MMWR
Over 30 million injuries were treated in US EDs in 2013, costing an estimated $671 billion, the CDC reported.
The largest share of that cost—almost $290 billion, or about 43%—came from the 3 million persons with nonfatal injuries who were hospitalized. Costs for the 27 million people who were treated and released from EDs were $167 billion, which was just under 25% of the total. The lifetime cost estimate for the almost 193,000 injury-associated deaths in 2013 was over $214 billion (32%), said Curtis Florence, PhD, of the CDC’s National Center for Injury Prevention and Control, Atlanta, Georgia, and associates.
For each ED-treated injury-related death, the mean cost in terms of lost lifetime earnings and medical care provided was just over $1.1 million: Homicides cost over $1.6 million, suicides were $1.2 million each, and each unintentional injury death cost just under $1 million, they said.1
Drug poisonings, including prescription drug overdoses, accounted for the largest share of fatal injury costs (27%), followed by transportation-related deaths (23%) and firearm-related deaths (22%), Dr Florence and associates noted.
“Injuries cost Americans far too much money, suffering, and preventable death,” CDC Director Tom Frieden said in a written statement. “The doubling of deaths by drug poisoning, including prescription drug overdose and heroin, is particularly alarming.”
The investigators used data from the National Vital Statistics System and the Web-Based Injury Statistics Query and Reporting System (WISQARS) for injury-related deaths and the National Electronic Injury Surveillance System–All Injury Program and WISQARS for nonfatal injuries.
Peramivir Effective Against Most Flu Viruses Circulating Globally
By Doug Brunk
AT ICAAC 2015
Vitals Key clinical point: Peramivir is potently effective against seasonal influenza viruses circulating globally. Major finding: During the 2013-2014 and 2014-2015 influenza seasons, about 99% of influenza type A and B viruses were inhibited by peramivir. Data source: An analysis of 8,426 influenza viruses that were tested during the 2013-2014 and 2014-2015 influenza seasons as part of the World Health Organization Global Influenza Surveillance and Response System.1 Disclosures: The researchers reporting having no financial disclosures. |
SAN DIEGO – The neuraminidase inhibitor peramivir inhibited about 99% of seasonal influenza A and B viruses circulating globally during the 2013 to 2014 and 2014 to 2015 influenza seasons, a large analysis demonstrated.
“The frequency of H1N1pdm09 viruses carrying neuraminidase (NA) H275Y remained low during both seasons; this mutation confers resistance to oseltamivir and peramivir,” said Margaret Okomo-Adhiambo, PhD, at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC/ICC 2015). In addition, “a small proportion of viruses contained other neuraminidase changes that affect binding of peramivir to viral enzymes and may decrease virus susceptibility. These changes need to be closely monitored.”
Approved by the FDA in December of 2014, peramivir (Rapivab) is the only antiviral agent for influenza treatment to come to market in nearly 20 years. Approved for intravenous administration as a single dose, it is indicated for adults with acute uncomplicated influenza who may have trouble taking orally administered or inhaled neuraminidase (NA) inhibitors. Other NA inhibitors approved by the FDA for influenza infection include oseltamivir, which is orally administered, and zanamivir, which is inhaled.
For the current analysis, Dr Okomo-Adhiambo of the influenza division at the US Centers for Disease Control and Prevention (CDC), Atlanta, and her associates tested influenza virus susceptibility to peramivir during the 2013-2014 and 2014-2015 influenza seasons as part of the World Health Organization Global Influenza Surveillance and Response System. A total of 8,426 viruses were tested, 75% of which were circulating in the United States.1
Dr Okomo-Adhiambo reported that during the 2013-2014 and 2014-2015 influenza seasons, about 99% of influenza type A and B viruses were inhibited by peramivir, except for a few viruses belonging to subtype A(H1N1)pdm09 (1.5%), subtype A(H3N2) (0.2%), and type B (0.4%). In addition, NA activity of type A viruses was five to six times more sensitive to inhibition by peramivir, compared with type B NA.
Parasitic Infection Emerging in the Southwestern United States
By Doug Brunk
At IDWEEK 2015
Vitals Key clinical point: Lesions containing a zoonotic parasite known as Onchocerca lupi are appearing in humans who reside in the Southwestern United States. Major finding: In three of six human cases, nodules containing Onchocerca lupi were located in the cervical spinal canal. Data source: A case report of the first six people in the United States to be infected with Onchocerca lupi. Disclosures: The researchers reported having no financial disclosures. |
SAN DIEGO – Onchocerca lupi, a zoonotic parasite previously described as causing eye disease in cats and dogs, as well as in humans from Europe, Asia, and the Middle East, is emerging in the Southwestern United States.
“The life cycle of this organism is not yet clearly defined, but likely includes a canine and/or feline animal reservoir, as well as an insect vector,” Dr Christiana Smith said in an interview at an annual scientific meeting on infectious diseases.1 “No specific risk factors for developing this disease have been identified, other than residing in or traveling through the Southwestern US.”
To date, six cases of humans infected by Onchocerca lupi have come to the attention of health officials, including those at the CDC, due to symptoms from a nodule containing the parasite, according to Dr Smith, a pediatrician with the University of Colorado School of Medicine and Children’s Hospital Colorado, Aurora. The affected patients range in age from 22 months to 50 years of age; three of the six reside in Arizona, two in New Mexico, and one in Texas.
In three of the six cases, the nodule was located in the cervical spinal canal. In the remaining three cases, nodules were located on the scalp, the forearm, and the superior rectus muscle of the orbit. Two of the patients reported insect bites at the nodule site years prior to presentation, while another patient owned a dog with eye lesions.
“No previous Onchocerca parasites are known to have tropism for the central nervous system,” Dr Smith said. “In addition, five of the six cases presented in children. It is not clear whether children are disproportionately affected by this disease, or whether they are diagnosed more frequently.”
Treatment included surgical excision and antiparasitic treatment for most cases. To date, all patients have remained asymptomatic following treatment. Dr Smith said that more information about Onchocerca lupi will become available as additional cases are described. “Continued epidemiologic investigation will help define the life cycle of this organism, describe the spectrum of human disease, develop approaches to diagnosis and management, and design prevention strategies,” she said.
IDWeek marks the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society. The researchers reported having no financial disclosures.
Europeans Adopt 1-Hour ED Chest Pain Triage
By Bruce Jancin
At the ESC Congress 2015
LONDON – The positive findings of the Biomarkers in Acute Cardiovascular Care (BACC) study1 reinforce a key change contained in the brand-new European Society of Cardiology guidelines for management of patients with acute coronary syndrome without ST-segment elevation: namely, that it’s appropriate to assess such patients using two measurements of a validated high-sensitivity cardiac troponin assay taken just 1 hour apart, according to Dr Kurt Huber.
The BACC results are the evidence-based icing on the cake in support of the new recommendation in the guidelines, released at the annual congress of the European Society of Cardiology. The BACC study, which included 1,045 patients who presented to a university ED with acute chest pain suggestive of an acute coronary syndrome without ST-segment elevation, was the latest of several studies to show that most such patients can either be safely sent home from the ED or ruled-in for acute MI in just 1 hour when evaluated using a high-sensitivity troponin assay backed by a validated patient-management algorithm. The result means reduced pressure on overcrowded EDs and less patient anxiety because of delayed diagnosis, Dr Huber, director of cardiology and emergency medicine at Wilhelminen Hospital in Vienna, observed during an interview at the meeting.
The BACC study, presented by Dr Dirk Westermann of the University Heart Center Hamburg (Germany), utilized a high-sensitivity cardiac troponin I assay. The 1-hour algorithm had a 99.7% negative predictive value for acute MI. A total of 53% of patients were ruled out or in for MI at the 1-hour mark; the rest required further evaluation.2
To view the video, search “Huber” at http://www.emed-journal.com/
New CPR Guide Sets Compression Limits, Scratches Vasopressin
By Shannon Aymes
From Circulation
New guidelines on cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) set upper limits on chest compression rate and depth, add naloxone to the care of suspected opioid abusers, and remove vasopressin from the advanced cardiac life support (ACLS) algorithm.
Vitals Key clinical point: The percentage of nonmedical use of prescription opioids declined during the last decade, but the prevalence of use disorders, the frequency of abuse, and related mortality all increased. Major finding: The 1-year prevalence of opioid use disorders rose from 0.6% to 0.9%, that of high-frequency use increased from 0.3% to 0.4%, and that of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. Data source: An analysis of time trends in prescription opioid use, based on two nationally representative data sets involving 472,200 adults. Disclosures: The Substance Abuse and Mental Health Services Administration, the National Institute on Drug Abuse, and the US Food and Drug Administration (FDA) sponsored the study. Dr Han reported having no relevant disclosures; an associate reported owning stock in General Electric, 3M Company, and Pfizer. |
The American Heart Association (AHA) published its revised guidelines October 15 in Circulation.1 The AHA released its previous guidelines in 2010.2
“When everyone knows their role, knows CPR, and works together, we can dramatically improve cardiac arrest victims’ chances of survival,” Dr Mark Creager, AHA president and director of the Heart and Vascular Center at Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, said in a statement.
The 2015 guidelines’ new recommendations include the following:
Resuscitation pathways. The guidelines note that the resuscitation pathways are very different for patients who experience cardiac arrest present in either a hospital setting (IHCA) or out-of-hospital setting (OHCA). In an OHCA, the patient depends on lay rescuers to not only recognize the situation but also call for help, initiate CPR, and, if available, administer defibrillation until emergency medical personnel arrive. However, IHCA involves prevention of cardiac arrest and smooth delivery of care in a multidisciplinary setting.
Compression rate and depth. The new guidelines set upper limits on chest compression depth and heart rate, recommending a compression rate of 100-120 compressions per minute with a depth of at least 2 inches, not to exceed 2.4 inches in adults.
Social media dispatching. Despite limited evidence, the guideline authors said that it may be reasonable for communities to use social media technologies to alert lay rescuers with mobile phones about nearby OHCA cases.
Naloxone and opioid addiction. Also new to the guidelines is the recommended use of naloxone for patients with suspected or known opioid addiction by appropriately trained lay rescuers or basic life support (BLS) providers.
CPR training. The guidelines highlight several changes to simplify health care provider training in CPR. For example, trained rescuers can simultaneously perform some tasks to reduce the time to initiate chest compressions. Likewise, in a team of trained rescuers, multiple steps—such as activating the emergency response system, chest compression, ventilation, and defibrillator retrieval—can be accomplished simultaneously.
High-quality CPR. The guidelines focus on emphasizing high-quality CPR with adequate compression rate and depth, complete chest recoil, few interruptions to compressions, and appropriate ventilation.
The guidelines offer several changes to advanced cardiac life support (ACLS). The algorithm was simplified by removing vasopressin, because the authors note that “the combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest.”
Likewise, the guidelines note conflicting studies to support the use of lidocaine after return of spontaneous circulation (ROSC). “However, the initiation or continuation of lidocaine may be considered immediately after ROSC from VF/pulseless ventricular tachycardia cardiac arrest,” the guideline authors wrote.
Finally, the guidelines highlight updates in post–cardiac arrest care, including a wider range of target temperatures, between 32°C and 36°C, to be maintained for at least 24 hours in comatose adults with ROSC after cardiac arrest. In comparison, the 2010 guidelines called for a target temperature range of 32°C to 34°C for 12 to 24 hours.
The guidelines also detail new updates for acute coronary syndrome, pediatric BLS, pediatric ACLS, and neonatal resuscitation.
Complex Picture Emerges of Prescription Opioid Abuse
By Mary Ann Moon
From JAMA
These findings—from an analysis of two large nationally representative data sets—paint a picture that is complex and more nuanced than that suggested by some recent reports. For example, a study of the Researched Abuse, Diversion, and Addiction-Related Surveillance (RADARS) System found that the abuse and diversion of prescription opioids plateaued or decreased in recent years.3 “The nationally representative results in our study may be especially important in providing an accurate picture of the current status of the epidemic,” said Dr Beth Han of the Substance Abuse and Mental Health Services Administration (SAMHSA), Rockville, Maryland, and her associates.
The nonmedical use of prescription opioids is an acknowledged epidemic, but that epidemic’s changing pattern over time needed to be updated. The investigators assessed the changes in use during the most recent decade for which data are available (2003-2013) using annual surveys conducted by SAMHSA and cause of death files from the National Vital Statistics System.
Based on responses from 472,200 people aged 18 to 64 years, the 1-year prevalence of nonmedical use of prescription opioids decreased from 5.4% to 4.9% during the study period. However, the 1-year prevalence of use disorders rose from 0.6% to 0.9%, the 1-year prevalence of high-frequency use (200 days or more per year) increased from 0.3% to 0.4%, and the rate of opioid-related deaths increased from 4.5 per 100,000 to 7.8 per 100,000. In addition, the mean number of days of opioid abuse increased from 2.1 to 2.6 per year in the general population and from 40.0 to 54.2 days per year among acknowledged opioid users, the investigators said.1
Compared with white users of prescription opioids, both black and Hispanic users had a lower prevalence of use disorders. The prevalence of use disorders was higher among less-educated than more-educated adults, among those with no health insurance or Medicaid as opposed to private health insurance, and among smokers than nonsmokers, Dr Han and her associates added.
Previous research has shown that most adults who abuse prescription opioids neither receive treatment nor perceive that they need treatment. Clinicians can help by using prescription-drug monitoring programs to identify inappropriate receipt of prescription opioids, then offering treatments, which are highly effective, for patients who need them, the investigators noted.
The slight decline (approximately 0.4% over 10 years) in opioid initiation reported by Han et al1 may be encouraging, but their other findings suggest that more patients are experiencing an inexorable progression from initial opioid use to frequent use to highly frequent use to a use disorder.
The source of most opioid abuse is often a seemingly legitimate prescription, and the key to addressing the opioid-abuse epidemic is to keep opioid-naive patients opioid naive. It is still unclear why clinicians continue to prescribe opioids, despite recommendations to the contrary and the fact that these agents provide little or no long-term benefit for most types of chronic pain.
Lewis S. Nelson, MD, is in the Ronald O. Perelman department of emergency medicine at New York University. He and his associates made these remarks in an editorial2 accompanying Dr Han’s report.1
US Injury Costs Topped $671 Billion in 2013
By Richard Franki
From MMWR
Over 30 million injuries were treated in US EDs in 2013, costing an estimated $671 billion, the CDC reported.
The largest share of that cost—almost $290 billion, or about 43%—came from the 3 million persons with nonfatal injuries who were hospitalized. Costs for the 27 million people who were treated and released from EDs were $167 billion, which was just under 25% of the total. The lifetime cost estimate for the almost 193,000 injury-associated deaths in 2013 was over $214 billion (32%), said Curtis Florence, PhD, of the CDC’s National Center for Injury Prevention and Control, Atlanta, Georgia, and associates.
For each ED-treated injury-related death, the mean cost in terms of lost lifetime earnings and medical care provided was just over $1.1 million: Homicides cost over $1.6 million, suicides were $1.2 million each, and each unintentional injury death cost just under $1 million, they said.1
Drug poisonings, including prescription drug overdoses, accounted for the largest share of fatal injury costs (27%), followed by transportation-related deaths (23%) and firearm-related deaths (22%), Dr Florence and associates noted.
“Injuries cost Americans far too much money, suffering, and preventable death,” CDC Director Tom Frieden said in a written statement. “The doubling of deaths by drug poisoning, including prescription drug overdose and heroin, is particularly alarming.”
The investigators used data from the National Vital Statistics System and the Web-Based Injury Statistics Query and Reporting System (WISQARS) for injury-related deaths and the National Electronic Injury Surveillance System–All Injury Program and WISQARS for nonfatal injuries.
Peramivir Effective Against Most Flu Viruses Circulating Globally
By Doug Brunk
AT ICAAC 2015
Vitals Key clinical point: Peramivir is potently effective against seasonal influenza viruses circulating globally. Major finding: During the 2013-2014 and 2014-2015 influenza seasons, about 99% of influenza type A and B viruses were inhibited by peramivir. Data source: An analysis of 8,426 influenza viruses that were tested during the 2013-2014 and 2014-2015 influenza seasons as part of the World Health Organization Global Influenza Surveillance and Response System.1 Disclosures: The researchers reporting having no financial disclosures. |
SAN DIEGO – The neuraminidase inhibitor peramivir inhibited about 99% of seasonal influenza A and B viruses circulating globally during the 2013 to 2014 and 2014 to 2015 influenza seasons, a large analysis demonstrated.
“The frequency of H1N1pdm09 viruses carrying neuraminidase (NA) H275Y remained low during both seasons; this mutation confers resistance to oseltamivir and peramivir,” said Margaret Okomo-Adhiambo, PhD, at the annual Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC/ICC 2015). In addition, “a small proportion of viruses contained other neuraminidase changes that affect binding of peramivir to viral enzymes and may decrease virus susceptibility. These changes need to be closely monitored.”
Approved by the FDA in December of 2014, peramivir (Rapivab) is the only antiviral agent for influenza treatment to come to market in nearly 20 years. Approved for intravenous administration as a single dose, it is indicated for adults with acute uncomplicated influenza who may have trouble taking orally administered or inhaled neuraminidase (NA) inhibitors. Other NA inhibitors approved by the FDA for influenza infection include oseltamivir, which is orally administered, and zanamivir, which is inhaled.
For the current analysis, Dr Okomo-Adhiambo of the influenza division at the US Centers for Disease Control and Prevention (CDC), Atlanta, and her associates tested influenza virus susceptibility to peramivir during the 2013-2014 and 2014-2015 influenza seasons as part of the World Health Organization Global Influenza Surveillance and Response System. A total of 8,426 viruses were tested, 75% of which were circulating in the United States.1
Dr Okomo-Adhiambo reported that during the 2013-2014 and 2014-2015 influenza seasons, about 99% of influenza type A and B viruses were inhibited by peramivir, except for a few viruses belonging to subtype A(H1N1)pdm09 (1.5%), subtype A(H3N2) (0.2%), and type B (0.4%). In addition, NA activity of type A viruses was five to six times more sensitive to inhibition by peramivir, compared with type B NA.
Parasitic Infection Emerging in the Southwestern United States
By Doug Brunk
At IDWEEK 2015
Vitals Key clinical point: Lesions containing a zoonotic parasite known as Onchocerca lupi are appearing in humans who reside in the Southwestern United States. Major finding: In three of six human cases, nodules containing Onchocerca lupi were located in the cervical spinal canal. Data source: A case report of the first six people in the United States to be infected with Onchocerca lupi. Disclosures: The researchers reported having no financial disclosures. |
SAN DIEGO – Onchocerca lupi, a zoonotic parasite previously described as causing eye disease in cats and dogs, as well as in humans from Europe, Asia, and the Middle East, is emerging in the Southwestern United States.
“The life cycle of this organism is not yet clearly defined, but likely includes a canine and/or feline animal reservoir, as well as an insect vector,” Dr Christiana Smith said in an interview at an annual scientific meeting on infectious diseases.1 “No specific risk factors for developing this disease have been identified, other than residing in or traveling through the Southwestern US.”
To date, six cases of humans infected by Onchocerca lupi have come to the attention of health officials, including those at the CDC, due to symptoms from a nodule containing the parasite, according to Dr Smith, a pediatrician with the University of Colorado School of Medicine and Children’s Hospital Colorado, Aurora. The affected patients range in age from 22 months to 50 years of age; three of the six reside in Arizona, two in New Mexico, and one in Texas.
In three of the six cases, the nodule was located in the cervical spinal canal. In the remaining three cases, nodules were located on the scalp, the forearm, and the superior rectus muscle of the orbit. Two of the patients reported insect bites at the nodule site years prior to presentation, while another patient owned a dog with eye lesions.
“No previous Onchocerca parasites are known to have tropism for the central nervous system,” Dr Smith said. “In addition, five of the six cases presented in children. It is not clear whether children are disproportionately affected by this disease, or whether they are diagnosed more frequently.”
Treatment included surgical excision and antiparasitic treatment for most cases. To date, all patients have remained asymptomatic following treatment. Dr Smith said that more information about Onchocerca lupi will become available as additional cases are described. “Continued epidemiologic investigation will help define the life cycle of this organism, describe the spectrum of human disease, develop approaches to diagnosis and management, and design prevention strategies,” she said.
IDWeek marks the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society. The researchers reported having no financial disclosures.
Europeans Adopt 1-Hour ED Chest Pain Triage
By Bruce Jancin
At the ESC Congress 2015
LONDON – The positive findings of the Biomarkers in Acute Cardiovascular Care (BACC) study1 reinforce a key change contained in the brand-new European Society of Cardiology guidelines for management of patients with acute coronary syndrome without ST-segment elevation: namely, that it’s appropriate to assess such patients using two measurements of a validated high-sensitivity cardiac troponin assay taken just 1 hour apart, according to Dr Kurt Huber.
The BACC results are the evidence-based icing on the cake in support of the new recommendation in the guidelines, released at the annual congress of the European Society of Cardiology. The BACC study, which included 1,045 patients who presented to a university ED with acute chest pain suggestive of an acute coronary syndrome without ST-segment elevation, was the latest of several studies to show that most such patients can either be safely sent home from the ED or ruled-in for acute MI in just 1 hour when evaluated using a high-sensitivity troponin assay backed by a validated patient-management algorithm. The result means reduced pressure on overcrowded EDs and less patient anxiety because of delayed diagnosis, Dr Huber, director of cardiology and emergency medicine at Wilhelminen Hospital in Vienna, observed during an interview at the meeting.
The BACC study, presented by Dr Dirk Westermann of the University Heart Center Hamburg (Germany), utilized a high-sensitivity cardiac troponin I assay. The 1-hour algorithm had a 99.7% negative predictive value for acute MI. A total of 53% of patients were ruled out or in for MI at the 1-hour mark; the rest required further evaluation.2
To view the video, search “Huber” at http://www.emed-journal.com/
- New CPR Guide Sets Compression Limits, Scratches Vasopressin
- Bhanji F, Donoghue AJ, Wolff MS, et al. Part 14: Education: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S561-S573.
- Cave DM, Gazmuri RJ, Otto CW, et al. Part 7: CPR techniques and devices: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 Suppl 3):S720-S728.
- Complex Picture Emerges of Prescription Opioid Abuse
- Han B, Compton WM, Jones CM, Cai R. Nonmedical prescription opioid use and use disorders among adults aged 18 through 64 years in the United States, 2003-2013. JAMA. 2015;314(14):1468-1478.
- Nelson LS, Juurlink DN, Perrone J. Addressing the opioid epidemic. JAMA. 2015;314(14):1453-1454.
- Severtson SG, Bartelson BB, Davis JM, et al. Reduced abuse, therapeutic errors, and diversion following reformulation of extended-release ocycodone in 2010. J Pain. 2013;14(10):1122-1130.
- US Injury Costs Topped $671 Billion in 2013
- Florence C, Simon T, Haegerich T, Luo F, Zhou C. Estimated lifetime medical and work-loss costs of fatal injuries – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;46(38):1074-1077.
- Florence C, Haegerich T, Simon T, Zhou C, Luo F. Estimated lifetime medical and work-loss costs of emergency department-treated nonfatal injuries – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(38):1078-1082.
- Peramivir Effective Against Most Flu Viruses Circulating Globally
- Okomo-Adhiambo M, Daniels J, Nguyen HT, et al. Peramivir Susceptibility Surveillance of Influenza A and B Viruses Circulated Globally, 2013-2015. Presented at: Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC) and the International Society of Chemotherapy (ISC)’s International Congress of Chemotherapy and Infection (ICC) 2015; September 17-21, 2015; San Diego, California
- Parasitic Infection Emerging in the Southwestern United States
- Smith C, Rao S, Dehority W, et al. Onchocerca lupi: An Emerging Parasitic Infection in the Southwestern United States. Poster presented at: Infectious Disease (ID) Week 2015; October 7-11, 2015; San Diego, California; Abstract 1971.
- Europeans Adopt 1-Hour ED Chest Pain Triage
- Universitätsklinikum Hamburg-Eppendorf. Biomarkers in Acute Cardiac Care (BACC). In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Available from: https://clinicaltrials.gov/ct2/show/NCT02355457. NLM Identifier: NCT02355457.
- Westermann D. Accurate and rapid diagnosis of myocardial infarction using a high sensitivity Troponin I 1-hour algorithm. Presented at: European Society of Cardiology (ESC) Congress; August 29 - September 2, 2015; London, England. FP NR 1161.
- New CPR Guide Sets Compression Limits, Scratches Vasopressin
- Bhanji F, Donoghue AJ, Wolff MS, et al. Part 14: Education: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2):S561-S573.
- Cave DM, Gazmuri RJ, Otto CW, et al. Part 7: CPR techniques and devices: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 Suppl 3):S720-S728.
- Complex Picture Emerges of Prescription Opioid Abuse
- Han B, Compton WM, Jones CM, Cai R. Nonmedical prescription opioid use and use disorders among adults aged 18 through 64 years in the United States, 2003-2013. JAMA. 2015;314(14):1468-1478.
- Nelson LS, Juurlink DN, Perrone J. Addressing the opioid epidemic. JAMA. 2015;314(14):1453-1454.
- Severtson SG, Bartelson BB, Davis JM, et al. Reduced abuse, therapeutic errors, and diversion following reformulation of extended-release ocycodone in 2010. J Pain. 2013;14(10):1122-1130.
- US Injury Costs Topped $671 Billion in 2013
- Florence C, Simon T, Haegerich T, Luo F, Zhou C. Estimated lifetime medical and work-loss costs of fatal injuries – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;46(38):1074-1077.
- Florence C, Haegerich T, Simon T, Zhou C, Luo F. Estimated lifetime medical and work-loss costs of emergency department-treated nonfatal injuries – United States, 2013. MMWR Morb Mortal Wkly Rep. 2015;64(38):1078-1082.
- Peramivir Effective Against Most Flu Viruses Circulating Globally
- Okomo-Adhiambo M, Daniels J, Nguyen HT, et al. Peramivir Susceptibility Surveillance of Influenza A and B Viruses Circulated Globally, 2013-2015. Presented at: Interscience Conference of Antimicrobial Agents and Chemotherapy (ICAAC) and the International Society of Chemotherapy (ISC)’s International Congress of Chemotherapy and Infection (ICC) 2015; September 17-21, 2015; San Diego, California
- Parasitic Infection Emerging in the Southwestern United States
- Smith C, Rao S, Dehority W, et al. Onchocerca lupi: An Emerging Parasitic Infection in the Southwestern United States. Poster presented at: Infectious Disease (ID) Week 2015; October 7-11, 2015; San Diego, California; Abstract 1971.
- Europeans Adopt 1-Hour ED Chest Pain Triage
- Universitätsklinikum Hamburg-Eppendorf. Biomarkers in Acute Cardiac Care (BACC). In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Available from: https://clinicaltrials.gov/ct2/show/NCT02355457. NLM Identifier: NCT02355457.
- Westermann D. Accurate and rapid diagnosis of myocardial infarction using a high sensitivity Troponin I 1-hour algorithm. Presented at: European Society of Cardiology (ESC) Congress; August 29 - September 2, 2015; London, England. FP NR 1161.

First EDition: News for and about the practice of emergency medicine
Timely Epinephrine for Pediatric In-Hospital Cardiac Arrest
BY MARY ANN MOON
FROM JAMA
Vitals Key clinical point: Delay in administering epinephrine was linked to poorer outcomes in pediatric in-hospital cardiac arrest. Major finding: Delay in epinephrine treatment was significantly associated with a lower chance of survival to hospital discharge (relative risk [RR], 0.95 per minute of delay). Data source: A multicenter cohort study of 1,558 in-hospital cardiac arrests among pediatric patients across the United States during a 15-year period. Disclosures: The National Heart, Lung, and Blood Institute and the American Heart Association (AHA) supported the study. Dr Andersen and his associates reported having no conflicts of interest. |
Delay in administering epinephrine is associated with significantly poorer outcomes among pediatric patients who have in-hospital cardiac arrest with an nonshockable rhythm, according to a report published in JAMA.1
For the approximately 16,000 US children and adolescents in this patient population each year, epinephrine is the recommended first-line pharmacologic therapy, even though no randomized placebo-controlled trials have ever been performed to support this practice.
“It is highly unlikely that any such study will ever be done, given the ethical considerations; so to examine the effect of the timing of epinephrine therapy, investigators analyzed data from the Get With the Guidelines-Resuscitation registry concerning 1,558 patients aged 0-18 years who were treated during a 15-year period,” said Dr Lars W. Andersen of the department of emergency medicine at Beth Israel Deaconess Medical Center, Boston, Massachusetts and the department of anesthesiology at Aarhus (Denmark) University and his associates.1
All the patients received chest compressions and at least one epinephrine bolus while pulseless with a documented nonshockable initial rhythm. The median age was 9 months, and the median time to first epinephrine dose was 1 minute (range, 0-20 minutes). A total of 37% of these patients received their first dose of epinephrine within 1 minute after loss of pulse was noted, and 15% received their first dose more than 5 minutes afterward.
Delay in epinephrine treatment was significantly associated with a lower chance of survival to hospital discharge (RR, 0.95 per minute of delay), the primary outcome measure of the study. In addition, longer time to epinephrine delivery was significantly associated with a decreased chance of return to spontaneous circulation (RR, 0.97 per minute of delay), for survival at 24 hours (RR, 0.97 per minute of delay), and for survival with favorable neurologic outcome (RR, 0.95 per minute of delay).
In a further analysis of the data, patients were divided into two groups according to the length of time before epinephrine administration. The 1,325 patients who received epinephrine within 5 minutes had a 33.1% rate of survival to hospital discharge, while the 233 who received epinephrine after 5 minutes had elapsed had a significantly lower 21.0% rate of survival to hospital discharge, Dr Andersen and his associates said.
These findings suggest, but cannot establish, that treatment delay causes poorer outcomes because an observational study cannot determine causality. Even though the data were adjusted to account for numerous patient and hospital characteristics, and even though the results remained robust through multiple sensitivity analyses, it remains possible that time to epinephrine administration is not a causal mediator but a marker of other aspects of the resuscitation process, the researchers added.
The findings by Dr Andersen and his associates provide fairly strong evidence that following current guidelines for epinephrine timing is best practice, supporting an AHA class I strength of recommendation.1
The investigators are correct to note that observational data cannot establish causality. Almost all of these cardiac arrests were witnessed; approximately two-thirds occurred in the pediatric intensive care unit, operating room, or postanesthesia setting; and half of the patients were receiving mechanical ventilation. So it is possible that the link between timing of epinephrine and outcomes may simply reflect factors such as the circumstances of the cardiac arrest, the presence of an airway and intravenous access, or the quality of chest compressions.
Dr Robert C. Tasker and Dr Adriennne G. Randolph are with the division of critical care medicine, department of anesthesia, perioperative, and pain medicine at Boston Children’s Hospital and the department of anesthesia at Harvard Medical School. Dr Tasker is also with the department of neurology at both institutions and Dr Randolph is also with the department of pediatrics at Harvard. Both authors reported having no relevant financial conflicts of interest. Dr Tasker and Dr Randolph made these remarks in an accompanying editorial.2
ED Care Pathway Hastens Febrile Neutropenia Therapy
BY Kari Oakes
FROM THE JOURNAL OF ONCOLOGY PRACTICE
Vitals Key clinical point: Instituting a care pathway hastened antibiotic administration in cancer patients with fever in the ED. Major finding: Cancer patients treated according to a febrile neutropenia care pathway in the ED received antibiotics in 81 minutes, significantly sooner than did historical and direct admission comparison cohorts at 235 and 169 minutes, respectively (P<.001 for both differences). Data source: Prospective study of 276 febrile neutropenia episodes in 223 patients, compared with 107 episodes in 87 historical patients and 114 episodes in 101 direct admission cohort patients. Disclosures: The authors reported no relevant financial disclosures. |
Cancer patients who arrive in the ED with febrile neutropenia (FN) received antibiotics much more quickly when their condition was identified as a medical emergency and a care pathway was used to guide treatment. The set of simple interventions slashed average time to antibiotics from about 4 hours to less than 1.5 hours, compared with a historical cohort, and the inexpensive interventions have had durable results.
Dr Michael Keng and his coinvestigators at the Cleveland Clinic reported the results of a single-center prospective analysis that targeted FN, a common and serious chemotherapy complication with a mortality rate that can exceed 50% in medically fragile individuals.1
“With an increasing number of outpatient chemotherapy regimens, more patients are likely to present to the emergency department with FN,” wrote Dr Keng. The FN pathway devised by Dr Keng and his associates implemented key changes designed to identify FN as an emergency and guide prompt triage, assessment, and treatment.
Study coauthor Dr Mikkael Sekeres said, “The interventions were not complicated. We standardized our definition of fever, provided patients with wallet-sized cards alerting emergency departments to the potential of this serious condition, worked with our emergency department staff to change the triage level of fever and neutropenia to be equivalent to that observed for heart attack or stroke, designed standard febrile neutropenia order sets for our electronic medical record, and relocated the antibiotics used to treat febrile neutropenia to our emergency department.”
Febrile patients with cancer in the prospective cohort (n = 223) were compared with a historical cohort of patients presenting to the ED who received usual care (n = 87), as well as to a concurrent cohort of patients who were directly admitted to the hospital (n = 114). The total number of FN episodes for the cohorts was 276, 107, and 114, respectively. Multivariable analysis was used to account for some differences in patient characteristics across cohorts.

Using the order set in the electronic health record (EHR) also made a difference: for those treated per the order set (n = 103), median time to antibiotics was 68 minutes, compared with 96 minutes when the order set was not used.
Secondary outcome measures included times to physician assessment, blood draw, and antibiotic order placement. All measures except time to physician assessment were significantly shorter for the FN pathway group than for the comparison cohorts (P<.001 for all).
Since so many changes were made at once, Dr Keng and his coauthors noted, “It is difficult to determine the impact of any one change.” Some institutions may have difficulty implementing all the interventions, but immediate triage, automated antibiotic ordering, and EHR use were the changes that had the most impact, he wrote.
“Instituting these changes took less than half a year, and the benefits have persisted for years afterward,” Dr Sekeres said in an interview.
ESC: Aldosterone Blockade Fails to Fly for Early MI in ALBATROSS
BY BRUCE JANCIN
AT THE European Society of Cardiology CONGRESS 2015
Vitals Key clinical point: Giving aldosterone antagonists to myocardial infarction (MI) patients without heart failure doesn’t improve clinical outcomes. Major finding: The 6-month rate of a multipronged composite clinical endpoint was closely similar, regardless of whether patients with acute MI without heart failure were placed on spironolactone within the first couple of days post-MI. Data source: The Aldosterone Lethal Effects Blockade in Acute Myocardial Infarction Treated With or Without Reperfusion to Improve Outcome and Survival at Six Months’ Follow-Up (ALBATROSS) trial was an open-label, multicenter French study in which 1,603 patients were randomized to 6 months of aldosterone blockade or not within the first hours after an acute MI without heart failure. Disclosures: The investigator-initiated ALBATROSS trial was funded by the French Ministry of Health. |
LONDON – Aldosterone blockade with oral spironolactone showed a disappointing lack of clinical benefit when initiated in the first hours after an acute MI without heart failure in the large, randomized ALBATROSS trial.
ALBATROSS did, however, flash a silver lining under one wing: A whopping 80% reduction in 6-month mortality in a prespecified subgroup analysis restricted to the 1,229 participants with ST-elevation MI, Dr Gilles Montalescot reported at the annual congress of the European Society of Cardiology.
Although this finding is intriguing, hypothesis-generating, and definitely warrants a confirmatory study, he continued, mortality was nevertheless merely a secondary endpoint in ALBATROSS.
In contrast, the primary composite outcome was negative, so the takeaway message is clear: “The results of the ALBATROSS study do not warrant the extension of aldosterone blockade to MI patients without heart failure,” said Dr Montalescot, professor of cardiology at the University of Paris.
ALBATROSS was a multicenter French trial that randomly assigned 1,603 acute MI patients to standard therapy alone or with added mineralocorticoid antagonist therapy started within the first 2 days of their coronary event. Often the aldosterone antagonist was begun in the ambulance en route to the hospital.1
The primary endpoint was a composite of death, resuscitated cardiac arrest, ventricular fibrillation or tachycardia, heart failure, or an indication for an implantable cardioverter defibrillator. There were 194 such events, and they occurred at a similar rate in the patients who got 25 mg/day of spironolactone and those who did not.
The rationale for ALBATROSS was sound, according to the cardiologist. Aldosterone is a stress hormone released in acute MI. It has deleterious cardiac effects, including arrhythmias, heart failure, and a dose-dependent increase in mortality, so it makes good sense to block it as soon as possible in MI patients. In the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) trial, the aldosterone antagonist eplerenone, when started 3-14 days post MI in patients with early heart failure, significantly reduced mortality,2 with the bulk of the benefit occurring in patients in whom the drug was started 3-7 days post MI.
Last year, Dr Montalescot and his coinvestigators published the Randomized, Placebo-Controlled Trial Evaluating The Safety and Efficacy of Early Treatment With Eplerenone in Patients With Acute Myocardial Infarction (REMINDER) study, in which 1,012 ST-elevation MI (STEMI) patients without heart failure were randomized to eplerenone or placebo within the first 24 hours. The study showed a significant reduction in levels of brain natriuretic peptide (BNP) or N-terminal pro-BNP in the eplerenone arm,2 but that’s not a clinical endpoint. ALBATROSS was the first study to look at the clinical impact of commencing mineralocorticoid antagonist therapy prior to day 3 post-MI.
Discussant Dr John McMurray, professor of cardiology at the University of Glasgow, Scotland, said that ALBATROSS was simply underpowered and thus leaves unanswered the clinically important question of whether early initiation of aldosterone blockade post MI in patients without heart failure confers clinical benefit. The investigators projected a total of 269 events in the composite endpoint but got only 194 because the study participants were so well treated and contemporary medical and interventional therapies are quite effective.
He dismissed the sharp reduction seen in 6-month mortality with spironolactone in the STEMI patients as “just implausible—we don’t know of any treatments in medicine that reduce mortality by 80%.”
Noting that there were only 28 deaths in the study, Dr McMurray asserted that “a subgroup analysis on such a small number of events is never going to give you a reliable result.” Moreover, he added, “subgroup analysis is even more treacherous when the overall trial is underpowered.”
Dr Montalescot replied that, while he considers the signal of a mortality benefit for aldosterone blockade in STEMI patients worthy of pursuit in a large randomized trial, the prospects for mounting such a study are poor. The medications are now available as generics, so there is no commercial incentive. The French Ministry of Health, which funded ALBATROSS, isn’t prepared to back a follow-up study. The best hope is that eventually one of the pharmaceutical companies developing third-generation aldosterone antagonists, now in phase II studies, will become interested, he said.
Dr Montalescot said that, while he receives research grants and consulting fees from numerous pharmaceutical companies, these commercial relationships aren’t relevant to the government-funded ALBATROSS trial.
Inpatient Mortality Down for High-Volume Conditions
BY RICHARD FRANKI
Frontline Medical News
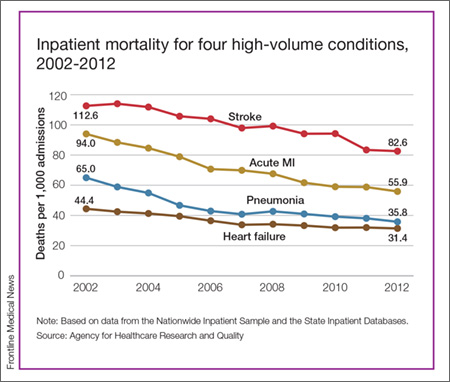
Over that period, mortality among adults hospitalized with pneumonia went from 65 per 1,000 admissions to 35.8 per 1,000 for a drop of 45%—the largest of the four high-volume conditions. Corresponding declines for the others were 41% for acute MI, 29% for heart failure, and 27% for stroke, the AHRQ noted.
Since “death following discharge from a hospital is not reflected in these data,” the report said, measures of inpatient mortality “can reflect both improvements in health care and shifts in where end-of-life care takes place over time.”
The estimates in the report are based on data from the Nationwide Inpatient Sample (2002-2011) and State Inpatient Databases (2012).1
- Timely Epinephrine for Pediatric In-Hospital Cardiac Arrest
- Andersen LW, Berg, KM, Saindon BZ, et al; American Heart Associaton Get With the Guidelines—Resuscitation Investigators. Time to epinephrine and survival after pediatric in-hospital cardiac arrest. JAMA. 2015;314(8):802-810.
- Tasker RC, Randolph AG. Pediatric pulseless arrest with “nonshockable” rhythm: does faster time to epinephrine improve outsome? JAMA. 2015;314(8):776-777.
- ED Care Pathway Hastens Febrile Neutropenia Therapy
- Keng MK, Thallner EA, Elson P, et al. Reducing time to antibiotic administration for febrile neutropenia in the emergency department [published online ahead of print July 28, 2015]. J Oncol Pract.
- ESC: Aldosterone Blockade Fails to Fly for Early MI in ALBATROSS
- Aldosterone Lethal Effects Blocked in AMI Treated With or Without Reperfusion to Improve Outcome and Survival at Six Months Follow-up: THE ALBATROSS TRIAL. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2015 September 14. Available from: https://clinicaltrials.gov/ct2/show/NCT01059136.
- Pitt B, Remme W, Zannad F, et al; Eplerenon Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14)1309-1321.
- Inpatient Mortality Down for High-Volume Conditions
- Statistical Brief #194. Trends in Observed Adult Inpatient Mortality for High-Volume Conditions, 2002-2012. Healthcare Cost and Utilization Project (HCUP). July 2015. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb194-Inpatient-Mortality-High-Volume-Conditions.jsp. Accessed August 20, 2015.
Timely Epinephrine for Pediatric In-Hospital Cardiac Arrest
BY MARY ANN MOON
FROM JAMA
Vitals Key clinical point: Delay in administering epinephrine was linked to poorer outcomes in pediatric in-hospital cardiac arrest. Major finding: Delay in epinephrine treatment was significantly associated with a lower chance of survival to hospital discharge (relative risk [RR], 0.95 per minute of delay). Data source: A multicenter cohort study of 1,558 in-hospital cardiac arrests among pediatric patients across the United States during a 15-year period. Disclosures: The National Heart, Lung, and Blood Institute and the American Heart Association (AHA) supported the study. Dr Andersen and his associates reported having no conflicts of interest. |
Delay in administering epinephrine is associated with significantly poorer outcomes among pediatric patients who have in-hospital cardiac arrest with an nonshockable rhythm, according to a report published in JAMA.1
For the approximately 16,000 US children and adolescents in this patient population each year, epinephrine is the recommended first-line pharmacologic therapy, even though no randomized placebo-controlled trials have ever been performed to support this practice.
“It is highly unlikely that any such study will ever be done, given the ethical considerations; so to examine the effect of the timing of epinephrine therapy, investigators analyzed data from the Get With the Guidelines-Resuscitation registry concerning 1,558 patients aged 0-18 years who were treated during a 15-year period,” said Dr Lars W. Andersen of the department of emergency medicine at Beth Israel Deaconess Medical Center, Boston, Massachusetts and the department of anesthesiology at Aarhus (Denmark) University and his associates.1
All the patients received chest compressions and at least one epinephrine bolus while pulseless with a documented nonshockable initial rhythm. The median age was 9 months, and the median time to first epinephrine dose was 1 minute (range, 0-20 minutes). A total of 37% of these patients received their first dose of epinephrine within 1 minute after loss of pulse was noted, and 15% received their first dose more than 5 minutes afterward.
Delay in epinephrine treatment was significantly associated with a lower chance of survival to hospital discharge (RR, 0.95 per minute of delay), the primary outcome measure of the study. In addition, longer time to epinephrine delivery was significantly associated with a decreased chance of return to spontaneous circulation (RR, 0.97 per minute of delay), for survival at 24 hours (RR, 0.97 per minute of delay), and for survival with favorable neurologic outcome (RR, 0.95 per minute of delay).
In a further analysis of the data, patients were divided into two groups according to the length of time before epinephrine administration. The 1,325 patients who received epinephrine within 5 minutes had a 33.1% rate of survival to hospital discharge, while the 233 who received epinephrine after 5 minutes had elapsed had a significantly lower 21.0% rate of survival to hospital discharge, Dr Andersen and his associates said.
These findings suggest, but cannot establish, that treatment delay causes poorer outcomes because an observational study cannot determine causality. Even though the data were adjusted to account for numerous patient and hospital characteristics, and even though the results remained robust through multiple sensitivity analyses, it remains possible that time to epinephrine administration is not a causal mediator but a marker of other aspects of the resuscitation process, the researchers added.
The findings by Dr Andersen and his associates provide fairly strong evidence that following current guidelines for epinephrine timing is best practice, supporting an AHA class I strength of recommendation.1
The investigators are correct to note that observational data cannot establish causality. Almost all of these cardiac arrests were witnessed; approximately two-thirds occurred in the pediatric intensive care unit, operating room, or postanesthesia setting; and half of the patients were receiving mechanical ventilation. So it is possible that the link between timing of epinephrine and outcomes may simply reflect factors such as the circumstances of the cardiac arrest, the presence of an airway and intravenous access, or the quality of chest compressions.
Dr Robert C. Tasker and Dr Adriennne G. Randolph are with the division of critical care medicine, department of anesthesia, perioperative, and pain medicine at Boston Children’s Hospital and the department of anesthesia at Harvard Medical School. Dr Tasker is also with the department of neurology at both institutions and Dr Randolph is also with the department of pediatrics at Harvard. Both authors reported having no relevant financial conflicts of interest. Dr Tasker and Dr Randolph made these remarks in an accompanying editorial.2
ED Care Pathway Hastens Febrile Neutropenia Therapy
BY Kari Oakes
FROM THE JOURNAL OF ONCOLOGY PRACTICE
Vitals Key clinical point: Instituting a care pathway hastened antibiotic administration in cancer patients with fever in the ED. Major finding: Cancer patients treated according to a febrile neutropenia care pathway in the ED received antibiotics in 81 minutes, significantly sooner than did historical and direct admission comparison cohorts at 235 and 169 minutes, respectively (P<.001 for both differences). Data source: Prospective study of 276 febrile neutropenia episodes in 223 patients, compared with 107 episodes in 87 historical patients and 114 episodes in 101 direct admission cohort patients. Disclosures: The authors reported no relevant financial disclosures. |
Cancer patients who arrive in the ED with febrile neutropenia (FN) received antibiotics much more quickly when their condition was identified as a medical emergency and a care pathway was used to guide treatment. The set of simple interventions slashed average time to antibiotics from about 4 hours to less than 1.5 hours, compared with a historical cohort, and the inexpensive interventions have had durable results.
Dr Michael Keng and his coinvestigators at the Cleveland Clinic reported the results of a single-center prospective analysis that targeted FN, a common and serious chemotherapy complication with a mortality rate that can exceed 50% in medically fragile individuals.1
“With an increasing number of outpatient chemotherapy regimens, more patients are likely to present to the emergency department with FN,” wrote Dr Keng. The FN pathway devised by Dr Keng and his associates implemented key changes designed to identify FN as an emergency and guide prompt triage, assessment, and treatment.
Study coauthor Dr Mikkael Sekeres said, “The interventions were not complicated. We standardized our definition of fever, provided patients with wallet-sized cards alerting emergency departments to the potential of this serious condition, worked with our emergency department staff to change the triage level of fever and neutropenia to be equivalent to that observed for heart attack or stroke, designed standard febrile neutropenia order sets for our electronic medical record, and relocated the antibiotics used to treat febrile neutropenia to our emergency department.”
Febrile patients with cancer in the prospective cohort (n = 223) were compared with a historical cohort of patients presenting to the ED who received usual care (n = 87), as well as to a concurrent cohort of patients who were directly admitted to the hospital (n = 114). The total number of FN episodes for the cohorts was 276, 107, and 114, respectively. Multivariable analysis was used to account for some differences in patient characteristics across cohorts.
Using the order set in the electronic health record (EHR) also made a difference: for those treated per the order set (n = 103), median time to antibiotics was 68 minutes, compared with 96 minutes when the order set was not used.
Secondary outcome measures included times to physician assessment, blood draw, and antibiotic order placement. All measures except time to physician assessment were significantly shorter for the FN pathway group than for the comparison cohorts (P<.001 for all).
Since so many changes were made at once, Dr Keng and his coauthors noted, “It is difficult to determine the impact of any one change.” Some institutions may have difficulty implementing all the interventions, but immediate triage, automated antibiotic ordering, and EHR use were the changes that had the most impact, he wrote.
“Instituting these changes took less than half a year, and the benefits have persisted for years afterward,” Dr Sekeres said in an interview.
ESC: Aldosterone Blockade Fails to Fly for Early MI in ALBATROSS
BY BRUCE JANCIN
AT THE European Society of Cardiology CONGRESS 2015
Vitals Key clinical point: Giving aldosterone antagonists to myocardial infarction (MI) patients without heart failure doesn’t improve clinical outcomes. Major finding: The 6-month rate of a multipronged composite clinical endpoint was closely similar, regardless of whether patients with acute MI without heart failure were placed on spironolactone within the first couple of days post-MI. Data source: The Aldosterone Lethal Effects Blockade in Acute Myocardial Infarction Treated With or Without Reperfusion to Improve Outcome and Survival at Six Months’ Follow-Up (ALBATROSS) trial was an open-label, multicenter French study in which 1,603 patients were randomized to 6 months of aldosterone blockade or not within the first hours after an acute MI without heart failure. Disclosures: The investigator-initiated ALBATROSS trial was funded by the French Ministry of Health. |
LONDON – Aldosterone blockade with oral spironolactone showed a disappointing lack of clinical benefit when initiated in the first hours after an acute MI without heart failure in the large, randomized ALBATROSS trial.
ALBATROSS did, however, flash a silver lining under one wing: A whopping 80% reduction in 6-month mortality in a prespecified subgroup analysis restricted to the 1,229 participants with ST-elevation MI, Dr Gilles Montalescot reported at the annual congress of the European Society of Cardiology.
Although this finding is intriguing, hypothesis-generating, and definitely warrants a confirmatory study, he continued, mortality was nevertheless merely a secondary endpoint in ALBATROSS.
In contrast, the primary composite outcome was negative, so the takeaway message is clear: “The results of the ALBATROSS study do not warrant the extension of aldosterone blockade to MI patients without heart failure,” said Dr Montalescot, professor of cardiology at the University of Paris.
ALBATROSS was a multicenter French trial that randomly assigned 1,603 acute MI patients to standard therapy alone or with added mineralocorticoid antagonist therapy started within the first 2 days of their coronary event. Often the aldosterone antagonist was begun in the ambulance en route to the hospital.1
The primary endpoint was a composite of death, resuscitated cardiac arrest, ventricular fibrillation or tachycardia, heart failure, or an indication for an implantable cardioverter defibrillator. There were 194 such events, and they occurred at a similar rate in the patients who got 25 mg/day of spironolactone and those who did not.
The rationale for ALBATROSS was sound, according to the cardiologist. Aldosterone is a stress hormone released in acute MI. It has deleterious cardiac effects, including arrhythmias, heart failure, and a dose-dependent increase in mortality, so it makes good sense to block it as soon as possible in MI patients. In the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) trial, the aldosterone antagonist eplerenone, when started 3-14 days post MI in patients with early heart failure, significantly reduced mortality,2 with the bulk of the benefit occurring in patients in whom the drug was started 3-7 days post MI.
Last year, Dr Montalescot and his coinvestigators published the Randomized, Placebo-Controlled Trial Evaluating The Safety and Efficacy of Early Treatment With Eplerenone in Patients With Acute Myocardial Infarction (REMINDER) study, in which 1,012 ST-elevation MI (STEMI) patients without heart failure were randomized to eplerenone or placebo within the first 24 hours. The study showed a significant reduction in levels of brain natriuretic peptide (BNP) or N-terminal pro-BNP in the eplerenone arm,2 but that’s not a clinical endpoint. ALBATROSS was the first study to look at the clinical impact of commencing mineralocorticoid antagonist therapy prior to day 3 post-MI.
Discussant Dr John McMurray, professor of cardiology at the University of Glasgow, Scotland, said that ALBATROSS was simply underpowered and thus leaves unanswered the clinically important question of whether early initiation of aldosterone blockade post MI in patients without heart failure confers clinical benefit. The investigators projected a total of 269 events in the composite endpoint but got only 194 because the study participants were so well treated and contemporary medical and interventional therapies are quite effective.
He dismissed the sharp reduction seen in 6-month mortality with spironolactone in the STEMI patients as “just implausible—we don’t know of any treatments in medicine that reduce mortality by 80%.”
Noting that there were only 28 deaths in the study, Dr McMurray asserted that “a subgroup analysis on such a small number of events is never going to give you a reliable result.” Moreover, he added, “subgroup analysis is even more treacherous when the overall trial is underpowered.”
Dr Montalescot replied that, while he considers the signal of a mortality benefit for aldosterone blockade in STEMI patients worthy of pursuit in a large randomized trial, the prospects for mounting such a study are poor. The medications are now available as generics, so there is no commercial incentive. The French Ministry of Health, which funded ALBATROSS, isn’t prepared to back a follow-up study. The best hope is that eventually one of the pharmaceutical companies developing third-generation aldosterone antagonists, now in phase II studies, will become interested, he said.
Dr Montalescot said that, while he receives research grants and consulting fees from numerous pharmaceutical companies, these commercial relationships aren’t relevant to the government-funded ALBATROSS trial.
Inpatient Mortality Down for High-Volume Conditions
BY RICHARD FRANKI
Frontline Medical News
Over that period, mortality among adults hospitalized with pneumonia went from 65 per 1,000 admissions to 35.8 per 1,000 for a drop of 45%—the largest of the four high-volume conditions. Corresponding declines for the others were 41% for acute MI, 29% for heart failure, and 27% for stroke, the AHRQ noted.
Since “death following discharge from a hospital is not reflected in these data,” the report said, measures of inpatient mortality “can reflect both improvements in health care and shifts in where end-of-life care takes place over time.”
The estimates in the report are based on data from the Nationwide Inpatient Sample (2002-2011) and State Inpatient Databases (2012).1
Timely Epinephrine for Pediatric In-Hospital Cardiac Arrest
BY MARY ANN MOON
FROM JAMA
Vitals Key clinical point: Delay in administering epinephrine was linked to poorer outcomes in pediatric in-hospital cardiac arrest. Major finding: Delay in epinephrine treatment was significantly associated with a lower chance of survival to hospital discharge (relative risk [RR], 0.95 per minute of delay). Data source: A multicenter cohort study of 1,558 in-hospital cardiac arrests among pediatric patients across the United States during a 15-year period. Disclosures: The National Heart, Lung, and Blood Institute and the American Heart Association (AHA) supported the study. Dr Andersen and his associates reported having no conflicts of interest. |
Delay in administering epinephrine is associated with significantly poorer outcomes among pediatric patients who have in-hospital cardiac arrest with an nonshockable rhythm, according to a report published in JAMA.1
For the approximately 16,000 US children and adolescents in this patient population each year, epinephrine is the recommended first-line pharmacologic therapy, even though no randomized placebo-controlled trials have ever been performed to support this practice.
“It is highly unlikely that any such study will ever be done, given the ethical considerations; so to examine the effect of the timing of epinephrine therapy, investigators analyzed data from the Get With the Guidelines-Resuscitation registry concerning 1,558 patients aged 0-18 years who were treated during a 15-year period,” said Dr Lars W. Andersen of the department of emergency medicine at Beth Israel Deaconess Medical Center, Boston, Massachusetts and the department of anesthesiology at Aarhus (Denmark) University and his associates.1
All the patients received chest compressions and at least one epinephrine bolus while pulseless with a documented nonshockable initial rhythm. The median age was 9 months, and the median time to first epinephrine dose was 1 minute (range, 0-20 minutes). A total of 37% of these patients received their first dose of epinephrine within 1 minute after loss of pulse was noted, and 15% received their first dose more than 5 minutes afterward.
Delay in epinephrine treatment was significantly associated with a lower chance of survival to hospital discharge (RR, 0.95 per minute of delay), the primary outcome measure of the study. In addition, longer time to epinephrine delivery was significantly associated with a decreased chance of return to spontaneous circulation (RR, 0.97 per minute of delay), for survival at 24 hours (RR, 0.97 per minute of delay), and for survival with favorable neurologic outcome (RR, 0.95 per minute of delay).
In a further analysis of the data, patients were divided into two groups according to the length of time before epinephrine administration. The 1,325 patients who received epinephrine within 5 minutes had a 33.1% rate of survival to hospital discharge, while the 233 who received epinephrine after 5 minutes had elapsed had a significantly lower 21.0% rate of survival to hospital discharge, Dr Andersen and his associates said.
These findings suggest, but cannot establish, that treatment delay causes poorer outcomes because an observational study cannot determine causality. Even though the data were adjusted to account for numerous patient and hospital characteristics, and even though the results remained robust through multiple sensitivity analyses, it remains possible that time to epinephrine administration is not a causal mediator but a marker of other aspects of the resuscitation process, the researchers added.
The findings by Dr Andersen and his associates provide fairly strong evidence that following current guidelines for epinephrine timing is best practice, supporting an AHA class I strength of recommendation.1
The investigators are correct to note that observational data cannot establish causality. Almost all of these cardiac arrests were witnessed; approximately two-thirds occurred in the pediatric intensive care unit, operating room, or postanesthesia setting; and half of the patients were receiving mechanical ventilation. So it is possible that the link between timing of epinephrine and outcomes may simply reflect factors such as the circumstances of the cardiac arrest, the presence of an airway and intravenous access, or the quality of chest compressions.
Dr Robert C. Tasker and Dr Adriennne G. Randolph are with the division of critical care medicine, department of anesthesia, perioperative, and pain medicine at Boston Children’s Hospital and the department of anesthesia at Harvard Medical School. Dr Tasker is also with the department of neurology at both institutions and Dr Randolph is also with the department of pediatrics at Harvard. Both authors reported having no relevant financial conflicts of interest. Dr Tasker and Dr Randolph made these remarks in an accompanying editorial.2
ED Care Pathway Hastens Febrile Neutropenia Therapy
BY Kari Oakes
FROM THE JOURNAL OF ONCOLOGY PRACTICE
Vitals Key clinical point: Instituting a care pathway hastened antibiotic administration in cancer patients with fever in the ED. Major finding: Cancer patients treated according to a febrile neutropenia care pathway in the ED received antibiotics in 81 minutes, significantly sooner than did historical and direct admission comparison cohorts at 235 and 169 minutes, respectively (P<.001 for both differences). Data source: Prospective study of 276 febrile neutropenia episodes in 223 patients, compared with 107 episodes in 87 historical patients and 114 episodes in 101 direct admission cohort patients. Disclosures: The authors reported no relevant financial disclosures. |
Cancer patients who arrive in the ED with febrile neutropenia (FN) received antibiotics much more quickly when their condition was identified as a medical emergency and a care pathway was used to guide treatment. The set of simple interventions slashed average time to antibiotics from about 4 hours to less than 1.5 hours, compared with a historical cohort, and the inexpensive interventions have had durable results.
Dr Michael Keng and his coinvestigators at the Cleveland Clinic reported the results of a single-center prospective analysis that targeted FN, a common and serious chemotherapy complication with a mortality rate that can exceed 50% in medically fragile individuals.1
“With an increasing number of outpatient chemotherapy regimens, more patients are likely to present to the emergency department with FN,” wrote Dr Keng. The FN pathway devised by Dr Keng and his associates implemented key changes designed to identify FN as an emergency and guide prompt triage, assessment, and treatment.
Study coauthor Dr Mikkael Sekeres said, “The interventions were not complicated. We standardized our definition of fever, provided patients with wallet-sized cards alerting emergency departments to the potential of this serious condition, worked with our emergency department staff to change the triage level of fever and neutropenia to be equivalent to that observed for heart attack or stroke, designed standard febrile neutropenia order sets for our electronic medical record, and relocated the antibiotics used to treat febrile neutropenia to our emergency department.”
Febrile patients with cancer in the prospective cohort (n = 223) were compared with a historical cohort of patients presenting to the ED who received usual care (n = 87), as well as to a concurrent cohort of patients who were directly admitted to the hospital (n = 114). The total number of FN episodes for the cohorts was 276, 107, and 114, respectively. Multivariable analysis was used to account for some differences in patient characteristics across cohorts.
Using the order set in the electronic health record (EHR) also made a difference: for those treated per the order set (n = 103), median time to antibiotics was 68 minutes, compared with 96 minutes when the order set was not used.
Secondary outcome measures included times to physician assessment, blood draw, and antibiotic order placement. All measures except time to physician assessment were significantly shorter for the FN pathway group than for the comparison cohorts (P<.001 for all).
Since so many changes were made at once, Dr Keng and his coauthors noted, “It is difficult to determine the impact of any one change.” Some institutions may have difficulty implementing all the interventions, but immediate triage, automated antibiotic ordering, and EHR use were the changes that had the most impact, he wrote.
“Instituting these changes took less than half a year, and the benefits have persisted for years afterward,” Dr Sekeres said in an interview.
ESC: Aldosterone Blockade Fails to Fly for Early MI in ALBATROSS
BY BRUCE JANCIN
AT THE European Society of Cardiology CONGRESS 2015
Vitals Key clinical point: Giving aldosterone antagonists to myocardial infarction (MI) patients without heart failure doesn’t improve clinical outcomes. Major finding: The 6-month rate of a multipronged composite clinical endpoint was closely similar, regardless of whether patients with acute MI without heart failure were placed on spironolactone within the first couple of days post-MI. Data source: The Aldosterone Lethal Effects Blockade in Acute Myocardial Infarction Treated With or Without Reperfusion to Improve Outcome and Survival at Six Months’ Follow-Up (ALBATROSS) trial was an open-label, multicenter French study in which 1,603 patients were randomized to 6 months of aldosterone blockade or not within the first hours after an acute MI without heart failure. Disclosures: The investigator-initiated ALBATROSS trial was funded by the French Ministry of Health. |
LONDON – Aldosterone blockade with oral spironolactone showed a disappointing lack of clinical benefit when initiated in the first hours after an acute MI without heart failure in the large, randomized ALBATROSS trial.
ALBATROSS did, however, flash a silver lining under one wing: A whopping 80% reduction in 6-month mortality in a prespecified subgroup analysis restricted to the 1,229 participants with ST-elevation MI, Dr Gilles Montalescot reported at the annual congress of the European Society of Cardiology.
Although this finding is intriguing, hypothesis-generating, and definitely warrants a confirmatory study, he continued, mortality was nevertheless merely a secondary endpoint in ALBATROSS.
In contrast, the primary composite outcome was negative, so the takeaway message is clear: “The results of the ALBATROSS study do not warrant the extension of aldosterone blockade to MI patients without heart failure,” said Dr Montalescot, professor of cardiology at the University of Paris.
ALBATROSS was a multicenter French trial that randomly assigned 1,603 acute MI patients to standard therapy alone or with added mineralocorticoid antagonist therapy started within the first 2 days of their coronary event. Often the aldosterone antagonist was begun in the ambulance en route to the hospital.1
The primary endpoint was a composite of death, resuscitated cardiac arrest, ventricular fibrillation or tachycardia, heart failure, or an indication for an implantable cardioverter defibrillator. There were 194 such events, and they occurred at a similar rate in the patients who got 25 mg/day of spironolactone and those who did not.
The rationale for ALBATROSS was sound, according to the cardiologist. Aldosterone is a stress hormone released in acute MI. It has deleterious cardiac effects, including arrhythmias, heart failure, and a dose-dependent increase in mortality, so it makes good sense to block it as soon as possible in MI patients. In the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) trial, the aldosterone antagonist eplerenone, when started 3-14 days post MI in patients with early heart failure, significantly reduced mortality,2 with the bulk of the benefit occurring in patients in whom the drug was started 3-7 days post MI.
Last year, Dr Montalescot and his coinvestigators published the Randomized, Placebo-Controlled Trial Evaluating The Safety and Efficacy of Early Treatment With Eplerenone in Patients With Acute Myocardial Infarction (REMINDER) study, in which 1,012 ST-elevation MI (STEMI) patients without heart failure were randomized to eplerenone or placebo within the first 24 hours. The study showed a significant reduction in levels of brain natriuretic peptide (BNP) or N-terminal pro-BNP in the eplerenone arm,2 but that’s not a clinical endpoint. ALBATROSS was the first study to look at the clinical impact of commencing mineralocorticoid antagonist therapy prior to day 3 post-MI.
Discussant Dr John McMurray, professor of cardiology at the University of Glasgow, Scotland, said that ALBATROSS was simply underpowered and thus leaves unanswered the clinically important question of whether early initiation of aldosterone blockade post MI in patients without heart failure confers clinical benefit. The investigators projected a total of 269 events in the composite endpoint but got only 194 because the study participants were so well treated and contemporary medical and interventional therapies are quite effective.
He dismissed the sharp reduction seen in 6-month mortality with spironolactone in the STEMI patients as “just implausible—we don’t know of any treatments in medicine that reduce mortality by 80%.”
Noting that there were only 28 deaths in the study, Dr McMurray asserted that “a subgroup analysis on such a small number of events is never going to give you a reliable result.” Moreover, he added, “subgroup analysis is even more treacherous when the overall trial is underpowered.”
Dr Montalescot replied that, while he considers the signal of a mortality benefit for aldosterone blockade in STEMI patients worthy of pursuit in a large randomized trial, the prospects for mounting such a study are poor. The medications are now available as generics, so there is no commercial incentive. The French Ministry of Health, which funded ALBATROSS, isn’t prepared to back a follow-up study. The best hope is that eventually one of the pharmaceutical companies developing third-generation aldosterone antagonists, now in phase II studies, will become interested, he said.
Dr Montalescot said that, while he receives research grants and consulting fees from numerous pharmaceutical companies, these commercial relationships aren’t relevant to the government-funded ALBATROSS trial.
Inpatient Mortality Down for High-Volume Conditions
BY RICHARD FRANKI
Frontline Medical News
Over that period, mortality among adults hospitalized with pneumonia went from 65 per 1,000 admissions to 35.8 per 1,000 for a drop of 45%—the largest of the four high-volume conditions. Corresponding declines for the others were 41% for acute MI, 29% for heart failure, and 27% for stroke, the AHRQ noted.
Since “death following discharge from a hospital is not reflected in these data,” the report said, measures of inpatient mortality “can reflect both improvements in health care and shifts in where end-of-life care takes place over time.”
The estimates in the report are based on data from the Nationwide Inpatient Sample (2002-2011) and State Inpatient Databases (2012).1
- Timely Epinephrine for Pediatric In-Hospital Cardiac Arrest
- Andersen LW, Berg, KM, Saindon BZ, et al; American Heart Associaton Get With the Guidelines—Resuscitation Investigators. Time to epinephrine and survival after pediatric in-hospital cardiac arrest. JAMA. 2015;314(8):802-810.
- Tasker RC, Randolph AG. Pediatric pulseless arrest with “nonshockable” rhythm: does faster time to epinephrine improve outsome? JAMA. 2015;314(8):776-777.
- ED Care Pathway Hastens Febrile Neutropenia Therapy
- Keng MK, Thallner EA, Elson P, et al. Reducing time to antibiotic administration for febrile neutropenia in the emergency department [published online ahead of print July 28, 2015]. J Oncol Pract.
- ESC: Aldosterone Blockade Fails to Fly for Early MI in ALBATROSS
- Aldosterone Lethal Effects Blocked in AMI Treated With or Without Reperfusion to Improve Outcome and Survival at Six Months Follow-up: THE ALBATROSS TRIAL. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2015 September 14. Available from: https://clinicaltrials.gov/ct2/show/NCT01059136.
- Pitt B, Remme W, Zannad F, et al; Eplerenon Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14)1309-1321.
- Inpatient Mortality Down for High-Volume Conditions
- Statistical Brief #194. Trends in Observed Adult Inpatient Mortality for High-Volume Conditions, 2002-2012. Healthcare Cost and Utilization Project (HCUP). July 2015. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb194-Inpatient-Mortality-High-Volume-Conditions.jsp. Accessed August 20, 2015.
- Timely Epinephrine for Pediatric In-Hospital Cardiac Arrest
- Andersen LW, Berg, KM, Saindon BZ, et al; American Heart Associaton Get With the Guidelines—Resuscitation Investigators. Time to epinephrine and survival after pediatric in-hospital cardiac arrest. JAMA. 2015;314(8):802-810.
- Tasker RC, Randolph AG. Pediatric pulseless arrest with “nonshockable” rhythm: does faster time to epinephrine improve outsome? JAMA. 2015;314(8):776-777.
- ED Care Pathway Hastens Febrile Neutropenia Therapy
- Keng MK, Thallner EA, Elson P, et al. Reducing time to antibiotic administration for febrile neutropenia in the emergency department [published online ahead of print July 28, 2015]. J Oncol Pract.
- ESC: Aldosterone Blockade Fails to Fly for Early MI in ALBATROSS
- Aldosterone Lethal Effects Blocked in AMI Treated With or Without Reperfusion to Improve Outcome and Survival at Six Months Follow-up: THE ALBATROSS TRIAL. In: ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). 2015 September 14. Available from: https://clinicaltrials.gov/ct2/show/NCT01059136.
- Pitt B, Remme W, Zannad F, et al; Eplerenon Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study Investigators. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14)1309-1321.
- Inpatient Mortality Down for High-Volume Conditions
- Statistical Brief #194. Trends in Observed Adult Inpatient Mortality for High-Volume Conditions, 2002-2012. Healthcare Cost and Utilization Project (HCUP). July 2015. Agency for Healthcare Research and Quality, Rockville, MD. www.hcup-us.ahrq.gov/reports/statbriefs/sb194-Inpatient-Mortality-High-Volume-Conditions.jsp. Accessed August 20, 2015.
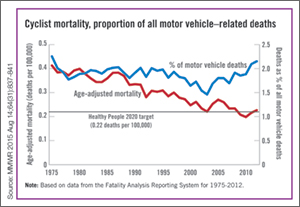
First EDition: News for and about the practice of Emergency Medicine
More bicyclists, more fatalities
BY RICHARD FRANKI
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
| The annual rate for bicyclist deaths associated with motor vehicles dropped 44% from 1975 to 2012, but the downward trend has slowed in recent years, the Centers for Disease Control and Prevention reported. |
Annual mortality among cyclists for all motor vehicle-related deaths was 0.23 per 100,000 in 2012, a decline of 44% since 1975 when the rate was 0.41 per 100,000. But the rate is up from just under 0.20 per 100,000 in 2010. In 2012, the rate topped the Healthy People 2020 goal of 0.22 for the first time since 2008, according to Jason Vargo, PhD, of the University of Wisconsin, Madison, and his associates.1
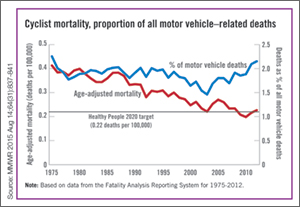
The explanation may be that the number of bicyclists has been steadily rising. “The share of total household trips taken by bicycle has doubled over the last 35 years,” with the largest share of that increase occurring in recent years. From 2000 to 2012, for example, “the number of US workers who traveled to work by bicycle increased 61%,” the researchers wrote.
The report was based on data from the Fatality Analysis Reporting System, which limits fatalities to those involving a motor vehicle on a public road.2
Surgical bolt cutters quickly cut titanium ring
BY AMY KARON
FROM EMERGENCY MEDICINE JOURNAL
| A pair of large surgical bolt cutters were used to safely and quickly cut a titanium ring from a patient’s swollen finger, according to a letter published online in the Emergency Medicine Journal. |
“Our method used simple equipment that is readily available in most hospitals at all times, took less than 30 seconds to perform, and could be performed by a sole operator without damage to the underlying finger,” wrote Dr Andrej Salibi and Dr Andrew Morritt at Sheffield (England) Teaching Hospital NHS Foundation.1
Ring constriction is a fairly common problem that can cause necrosis and loss of the digit if the ring is not removed. Basic ring cutters can sever gold and silver, but not titanium, which has become popular for rings because it is hypoallergenic, durable, lightweight, and strong—so strong that diamond-tipped saws or drills can take up to 15 minutes to cut these rings. Many facilities also lack access to such equipment, and it generates enough heat that an assistant must irrigate the surrounding skin to prevent burns.
The case report described a patient who bathed in warm water at a spa and developed a painful, swollen finger that was constricted by a titanium wedding band. Elevation and lubrication at the ED failed to remove the ring, as did finger binding, and use of a manual ring cutter.
“The fire service was called and attempted removal using specialized cutting equipment, which also failed,” the surgeons wrote. “The patient was then admitted under the plastic surgery service for hand elevation, and further attempts 8 hours later blunted two manual ring cutters.” At this point, the surgeons borrowed a large pair of bolt cutters from the operating room, and quickly severed the ring without harming the finger. Then they applied lateral traction with a pair of paper clips and removed the split ring.
The authors declared no funding sources or conflicts of interest.
Federal plan emphasizes heroin/opioid treatment over incarceration
BY WHITNEY MCKNIGHT
Frontline Medical News
| WASHINGTON—The Obama administration has announced that it will spend an additional $13.4 million fighting opioid and heroin abuse, emphasizing treatment over law enforcement. |
The increased emphasis will center on geographic areas where heroin and opioid abuse are rampant, specifically: Appalachia; New England; Philadelphia/Camden, New Jersey; metropolitan New York City, particularly northern New Jersey; and the Washington/Baltimore metropolitan region. Public safety officers and first responders will be trained in how to administer naloxone and provide other medical attention for those in the midst of a heroin or opioid overdose.
The 15 states in the targeted areas will share and leverage data to determine regional patterns of heroin and prescription painkiller-related overdose. These data are expected to delineate where the narcotics—especially those laced with other, more dangerous drugs—are being produced and distributed so that heroin response teams can disrupt the production and distribution of illegal drugs, and respond pre-emptively by expanding resources to communities hardest hit.
In a statement, Michael Botticelli, director of the White House Office of National Drug Control Policy, said the administration’s emphasis on “the national drug challenge as both a public health and public safety issue” is based on viewing drug addiction as “a chronic disease of the brain that can be successfully prevented and treated, and from which one can recover.”
The initiative also will provide additional funding for similar efforts to address opioid abuse and methamphetamine abuse in the Southwest and along the United States/Mexico border.
“This program demonstrates the importance of linking health to criminal justice in collaboration rather than seeing better, new drug policy as a choice between health and law enforcement,” Dr Robert L. DuPont, former director of the National Institute on Drug Abuse (NIDA) and president of the Institute for Behavior and Health, said in an interview.
Online resource is aid for preventing patient falls
BY MIKE BOCK
Frontline Medical News
| An online resource guide offers 21 targeted solutions for reducing the rate of falls in hospitals and urgent care settings,1 The Joint Commission Center for Transforming Healthcare announced in a statement. |
Developed in collaboration with seven hospitals and five health care organizations, the fall prevention methodology of the Targeted Solutions Tool could potentially reduce the number of patients injured from a fall from 117 to 45 in a typical 200-bed hospital, avoiding approximately $1 million in costs annually, the agency claims.
Some of the recommendations for reducing in-hospital falls include:
- Creating awareness among staff
- Using a validated fall risk assessment tool
- Engaging patients and their families in the fall safety program
- Hourly rounding with scheduled restroom use for patients
- Engaging all hospital staff and patients to ensure no patient walks without assistance
“Hundreds of thousands of patients fall in hospitals every year; and many of these falls result in moderate to severe injuries that can prolong hospital stays and require the patient to undergo additional treatment,” Dr Erin DuPree, vice president and chief medical officer of the Joint Commission Center for Transforming Healthcare, said in a statement.
The Joint Commission Center for Transforming Healthcare was created in 2008 as a nonprofit affiliate of The Joint Commission.
Dr Lappin is an assistant professor and an attending physician, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical College, New York.
Reference - CDC More bicyclists, more fatalities
- Vargo J, Gerhardstein BG, Whitfield GP, Wendel A. Bicyclist deaths associated with motor vehicle traffic – United States, 1975-2012. MMWR Morb Mortal Wkly Rep.2015;64(31):837-841.
- National Highway Traffic Safety Administration. Fatality Analysis Reporting System (FARS). http://www.nhtsa.gov/FARS. Accessed August 20, 2015.
Reference - Surgical bolt cutters quickly cut titanium ring
- Salibi A, Morritt AN. Removing a titanium wedding ring [published online ahead of print August 13, 2015]. Emerg Med J. doi: 10.1136/emermed-2015-204962.
Reference - Online resource is aid for preventing patient falls
- Joint Commission Center for Transforming Healthcare. New! Targeted Solutions Tool for Preventing Falls. http://www.centerfortransforminghealthcare.org/tst_pfi.aspx. Accessed August 20, 2015.
More bicyclists, more fatalities
BY RICHARD FRANKI
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
| The annual rate for bicyclist deaths associated with motor vehicles dropped 44% from 1975 to 2012, but the downward trend has slowed in recent years, the Centers for Disease Control and Prevention reported. |
Annual mortality among cyclists for all motor vehicle-related deaths was 0.23 per 100,000 in 2012, a decline of 44% since 1975 when the rate was 0.41 per 100,000. But the rate is up from just under 0.20 per 100,000 in 2010. In 2012, the rate topped the Healthy People 2020 goal of 0.22 for the first time since 2008, according to Jason Vargo, PhD, of the University of Wisconsin, Madison, and his associates.1
The explanation may be that the number of bicyclists has been steadily rising. “The share of total household trips taken by bicycle has doubled over the last 35 years,” with the largest share of that increase occurring in recent years. From 2000 to 2012, for example, “the number of US workers who traveled to work by bicycle increased 61%,” the researchers wrote.
The report was based on data from the Fatality Analysis Reporting System, which limits fatalities to those involving a motor vehicle on a public road.2
Surgical bolt cutters quickly cut titanium ring
BY AMY KARON
FROM EMERGENCY MEDICINE JOURNAL
| A pair of large surgical bolt cutters were used to safely and quickly cut a titanium ring from a patient’s swollen finger, according to a letter published online in the Emergency Medicine Journal. |
“Our method used simple equipment that is readily available in most hospitals at all times, took less than 30 seconds to perform, and could be performed by a sole operator without damage to the underlying finger,” wrote Dr Andrej Salibi and Dr Andrew Morritt at Sheffield (England) Teaching Hospital NHS Foundation.1
Ring constriction is a fairly common problem that can cause necrosis and loss of the digit if the ring is not removed. Basic ring cutters can sever gold and silver, but not titanium, which has become popular for rings because it is hypoallergenic, durable, lightweight, and strong—so strong that diamond-tipped saws or drills can take up to 15 minutes to cut these rings. Many facilities also lack access to such equipment, and it generates enough heat that an assistant must irrigate the surrounding skin to prevent burns.
The case report described a patient who bathed in warm water at a spa and developed a painful, swollen finger that was constricted by a titanium wedding band. Elevation and lubrication at the ED failed to remove the ring, as did finger binding, and use of a manual ring cutter.
“The fire service was called and attempted removal using specialized cutting equipment, which also failed,” the surgeons wrote. “The patient was then admitted under the plastic surgery service for hand elevation, and further attempts 8 hours later blunted two manual ring cutters.” At this point, the surgeons borrowed a large pair of bolt cutters from the operating room, and quickly severed the ring without harming the finger. Then they applied lateral traction with a pair of paper clips and removed the split ring.
The authors declared no funding sources or conflicts of interest.
Federal plan emphasizes heroin/opioid treatment over incarceration
BY WHITNEY MCKNIGHT
Frontline Medical News
| WASHINGTON—The Obama administration has announced that it will spend an additional $13.4 million fighting opioid and heroin abuse, emphasizing treatment over law enforcement. |
The increased emphasis will center on geographic areas where heroin and opioid abuse are rampant, specifically: Appalachia; New England; Philadelphia/Camden, New Jersey; metropolitan New York City, particularly northern New Jersey; and the Washington/Baltimore metropolitan region. Public safety officers and first responders will be trained in how to administer naloxone and provide other medical attention for those in the midst of a heroin or opioid overdose.
The 15 states in the targeted areas will share and leverage data to determine regional patterns of heroin and prescription painkiller-related overdose. These data are expected to delineate where the narcotics—especially those laced with other, more dangerous drugs—are being produced and distributed so that heroin response teams can disrupt the production and distribution of illegal drugs, and respond pre-emptively by expanding resources to communities hardest hit.
In a statement, Michael Botticelli, director of the White House Office of National Drug Control Policy, said the administration’s emphasis on “the national drug challenge as both a public health and public safety issue” is based on viewing drug addiction as “a chronic disease of the brain that can be successfully prevented and treated, and from which one can recover.”
The initiative also will provide additional funding for similar efforts to address opioid abuse and methamphetamine abuse in the Southwest and along the United States/Mexico border.
“This program demonstrates the importance of linking health to criminal justice in collaboration rather than seeing better, new drug policy as a choice between health and law enforcement,” Dr Robert L. DuPont, former director of the National Institute on Drug Abuse (NIDA) and president of the Institute for Behavior and Health, said in an interview.
Online resource is aid for preventing patient falls
BY MIKE BOCK
Frontline Medical News
| An online resource guide offers 21 targeted solutions for reducing the rate of falls in hospitals and urgent care settings,1 The Joint Commission Center for Transforming Healthcare announced in a statement. |
Developed in collaboration with seven hospitals and five health care organizations, the fall prevention methodology of the Targeted Solutions Tool could potentially reduce the number of patients injured from a fall from 117 to 45 in a typical 200-bed hospital, avoiding approximately $1 million in costs annually, the agency claims.
Some of the recommendations for reducing in-hospital falls include:
- Creating awareness among staff
- Using a validated fall risk assessment tool
- Engaging patients and their families in the fall safety program
- Hourly rounding with scheduled restroom use for patients
- Engaging all hospital staff and patients to ensure no patient walks without assistance
“Hundreds of thousands of patients fall in hospitals every year; and many of these falls result in moderate to severe injuries that can prolong hospital stays and require the patient to undergo additional treatment,” Dr Erin DuPree, vice president and chief medical officer of the Joint Commission Center for Transforming Healthcare, said in a statement.
The Joint Commission Center for Transforming Healthcare was created in 2008 as a nonprofit affiliate of The Joint Commission.
Dr Lappin is an assistant professor and an attending physician, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical College, New York.
More bicyclists, more fatalities
BY RICHARD FRANKI
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
| The annual rate for bicyclist deaths associated with motor vehicles dropped 44% from 1975 to 2012, but the downward trend has slowed in recent years, the Centers for Disease Control and Prevention reported. |
Annual mortality among cyclists for all motor vehicle-related deaths was 0.23 per 100,000 in 2012, a decline of 44% since 1975 when the rate was 0.41 per 100,000. But the rate is up from just under 0.20 per 100,000 in 2010. In 2012, the rate topped the Healthy People 2020 goal of 0.22 for the first time since 2008, according to Jason Vargo, PhD, of the University of Wisconsin, Madison, and his associates.1
The explanation may be that the number of bicyclists has been steadily rising. “The share of total household trips taken by bicycle has doubled over the last 35 years,” with the largest share of that increase occurring in recent years. From 2000 to 2012, for example, “the number of US workers who traveled to work by bicycle increased 61%,” the researchers wrote.
The report was based on data from the Fatality Analysis Reporting System, which limits fatalities to those involving a motor vehicle on a public road.2
Surgical bolt cutters quickly cut titanium ring
BY AMY KARON
FROM EMERGENCY MEDICINE JOURNAL
| A pair of large surgical bolt cutters were used to safely and quickly cut a titanium ring from a patient’s swollen finger, according to a letter published online in the Emergency Medicine Journal. |
“Our method used simple equipment that is readily available in most hospitals at all times, took less than 30 seconds to perform, and could be performed by a sole operator without damage to the underlying finger,” wrote Dr Andrej Salibi and Dr Andrew Morritt at Sheffield (England) Teaching Hospital NHS Foundation.1
Ring constriction is a fairly common problem that can cause necrosis and loss of the digit if the ring is not removed. Basic ring cutters can sever gold and silver, but not titanium, which has become popular for rings because it is hypoallergenic, durable, lightweight, and strong—so strong that diamond-tipped saws or drills can take up to 15 minutes to cut these rings. Many facilities also lack access to such equipment, and it generates enough heat that an assistant must irrigate the surrounding skin to prevent burns.
The case report described a patient who bathed in warm water at a spa and developed a painful, swollen finger that was constricted by a titanium wedding band. Elevation and lubrication at the ED failed to remove the ring, as did finger binding, and use of a manual ring cutter.
“The fire service was called and attempted removal using specialized cutting equipment, which also failed,” the surgeons wrote. “The patient was then admitted under the plastic surgery service for hand elevation, and further attempts 8 hours later blunted two manual ring cutters.” At this point, the surgeons borrowed a large pair of bolt cutters from the operating room, and quickly severed the ring without harming the finger. Then they applied lateral traction with a pair of paper clips and removed the split ring.
The authors declared no funding sources or conflicts of interest.
Federal plan emphasizes heroin/opioid treatment over incarceration
BY WHITNEY MCKNIGHT
Frontline Medical News
| WASHINGTON—The Obama administration has announced that it will spend an additional $13.4 million fighting opioid and heroin abuse, emphasizing treatment over law enforcement. |
The increased emphasis will center on geographic areas where heroin and opioid abuse are rampant, specifically: Appalachia; New England; Philadelphia/Camden, New Jersey; metropolitan New York City, particularly northern New Jersey; and the Washington/Baltimore metropolitan region. Public safety officers and first responders will be trained in how to administer naloxone and provide other medical attention for those in the midst of a heroin or opioid overdose.
The 15 states in the targeted areas will share and leverage data to determine regional patterns of heroin and prescription painkiller-related overdose. These data are expected to delineate where the narcotics—especially those laced with other, more dangerous drugs—are being produced and distributed so that heroin response teams can disrupt the production and distribution of illegal drugs, and respond pre-emptively by expanding resources to communities hardest hit.
In a statement, Michael Botticelli, director of the White House Office of National Drug Control Policy, said the administration’s emphasis on “the national drug challenge as both a public health and public safety issue” is based on viewing drug addiction as “a chronic disease of the brain that can be successfully prevented and treated, and from which one can recover.”
The initiative also will provide additional funding for similar efforts to address opioid abuse and methamphetamine abuse in the Southwest and along the United States/Mexico border.
“This program demonstrates the importance of linking health to criminal justice in collaboration rather than seeing better, new drug policy as a choice between health and law enforcement,” Dr Robert L. DuPont, former director of the National Institute on Drug Abuse (NIDA) and president of the Institute for Behavior and Health, said in an interview.
Online resource is aid for preventing patient falls
BY MIKE BOCK
Frontline Medical News
| An online resource guide offers 21 targeted solutions for reducing the rate of falls in hospitals and urgent care settings,1 The Joint Commission Center for Transforming Healthcare announced in a statement. |
Developed in collaboration with seven hospitals and five health care organizations, the fall prevention methodology of the Targeted Solutions Tool could potentially reduce the number of patients injured from a fall from 117 to 45 in a typical 200-bed hospital, avoiding approximately $1 million in costs annually, the agency claims.
Some of the recommendations for reducing in-hospital falls include:
- Creating awareness among staff
- Using a validated fall risk assessment tool
- Engaging patients and their families in the fall safety program
- Hourly rounding with scheduled restroom use for patients
- Engaging all hospital staff and patients to ensure no patient walks without assistance
“Hundreds of thousands of patients fall in hospitals every year; and many of these falls result in moderate to severe injuries that can prolong hospital stays and require the patient to undergo additional treatment,” Dr Erin DuPree, vice president and chief medical officer of the Joint Commission Center for Transforming Healthcare, said in a statement.
The Joint Commission Center for Transforming Healthcare was created in 2008 as a nonprofit affiliate of The Joint Commission.
Dr Lappin is an assistant professor and an attending physician, department of emergency medicine, New York-Presbyterian Hospital/Weill Cornell Medical College, New York.
Reference - CDC More bicyclists, more fatalities
- Vargo J, Gerhardstein BG, Whitfield GP, Wendel A. Bicyclist deaths associated with motor vehicle traffic – United States, 1975-2012. MMWR Morb Mortal Wkly Rep.2015;64(31):837-841.
- National Highway Traffic Safety Administration. Fatality Analysis Reporting System (FARS). http://www.nhtsa.gov/FARS. Accessed August 20, 2015.
Reference - Surgical bolt cutters quickly cut titanium ring
- Salibi A, Morritt AN. Removing a titanium wedding ring [published online ahead of print August 13, 2015]. Emerg Med J. doi: 10.1136/emermed-2015-204962.
Reference - Online resource is aid for preventing patient falls
- Joint Commission Center for Transforming Healthcare. New! Targeted Solutions Tool for Preventing Falls. http://www.centerfortransforminghealthcare.org/tst_pfi.aspx. Accessed August 20, 2015.
Reference - CDC More bicyclists, more fatalities
- Vargo J, Gerhardstein BG, Whitfield GP, Wendel A. Bicyclist deaths associated with motor vehicle traffic – United States, 1975-2012. MMWR Morb Mortal Wkly Rep.2015;64(31):837-841.
- National Highway Traffic Safety Administration. Fatality Analysis Reporting System (FARS). http://www.nhtsa.gov/FARS. Accessed August 20, 2015.
Reference - Surgical bolt cutters quickly cut titanium ring
- Salibi A, Morritt AN. Removing a titanium wedding ring [published online ahead of print August 13, 2015]. Emerg Med J. doi: 10.1136/emermed-2015-204962.
Reference - Online resource is aid for preventing patient falls
- Joint Commission Center for Transforming Healthcare. New! Targeted Solutions Tool for Preventing Falls. http://www.centerfortransforminghealthcare.org/tst_pfi.aspx. Accessed August 20, 2015.
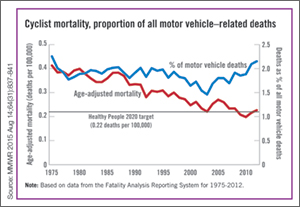
3-Month paliperidone palmitate for preventing relapse in schizophrenia
A 3-month paliperidone palmitate (PPM-3) extended-release injectable suspension was approved by the FDA in May 2015 for preventing relapse among patients with schizophrenia, under the brand name Invega Trinza (Table 1). Administered 4 times a year, PPM-3 provides the longest interval of any approved long-acting injectable antipsychotic (LAIA). PPM-3 can be administered to patients with schizophrenia who have been taking 1-month paliperidone palmitate (PPM-1) extended-release injectable suspension (brand name, Invega Sustenna), once a month, for at least 4 months.
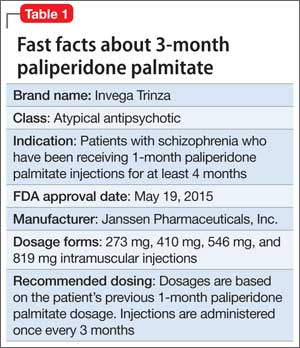
How it works
PPM-3 is a LAIA injection. Because of its low solubility in water, paliperidone palmitate dissolves slowly once injected before being hydrolyzed as paliperidone and absorbed into the bloodstream. From time of release on Day 1, PPM-3 remains active for as long 18 months.
PPM-3 reaches a maximum plasma concentration between Day 30 and Day 33. In clinical trials, PPM-3 had a median half-life of 84 to 95 days when injected into the deltoid muscle and a median half-life of 118 to 139 days when injected into the gluteal muscle.
Paliperidone is not extensively metabolized in the liver. Although results of a study suggest that cytochrome P450 (CYP) 2D6 and CYP3A4 might play a role in metabolizing paliperidone, there is no evidence that it has a significant role.
Dosing and administration
PPM-3 is administered intramuscularly by a licensed health care professional, once every 3 months. The recommended dosage is based on the patient’s previous dosage of PPM-1 (Table 2).
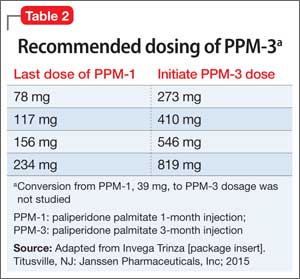
See the prescribing information for administration instructions.
Efficacy
The efficacy of PPM-3 was assessed in a long-term double-blind, placebo-controlled, randomized-withdrawal trial in adult patients with acute symptoms (previously treated with an oral antipsychotic) or adequately treated with a LAIA, either PPM-1 or another agent; patients receiving PPM-1, 39 mg, injections were ineligible. All patients entering the study received PPM-1 in place of the next scheduled injection.
The study comprised 3 treatment periods:
• 17-Week flexible-dose open-label period with PPM-1 (ie, first part of a 29-week open-label stabilization phase): Patients (N = 506) received PPM-1 with a flexible dose based on symptom response, tolerability, and medication history. Patients had to achieve a Positive and Negative Syndrome Scale (PANSS) total score of <70 at Week 17 to enter the second phase.
• 12-Week open-label with PPM-3 (ie, second part of the 29-week open-label stabilization phase): Patients (N = 379) received a single injection of PPM-3 that was 3.5 times the last dose of PPM-1. Patients had to achieve a PANSS total score of <70 and ≤4 for 7 specific PANSS items.
• A variable length double-blind treatment period: Patients (N = 305) were randomized 1:1 to continue treatment with PPM-3 (273 mg, 410 mg, 546 mg, or 819 mg) or placebo (administered once every 12 weeks) until relapse, early withdrawal, or end of the study. The primary efficacy measure was time to first relapse, defined as psychiatric hospitalization, ≥25% increase or a 10-point increase in total PANSS score on 2 consecutive assessments, deliberate self-injury, violent behavior, suicidal or homicidal ideation, or a score of ≥5 (if the maximum baseline score was ≤3) or ≥6 (if the maximum baseline score was 4) on 2 consecutive assessments of the specific PANSS items.
Among the patients in the third treatment period, 23% of those who received placebo and 7.4% of those who received PPM-3 experienced a relapse event. The time to relapse was significantly longer for patients who received PPM-3 than for those who received placebo.
See Table 3 for adverse reactions reported in patients who received PPM-3 and those taking placebo in the study.
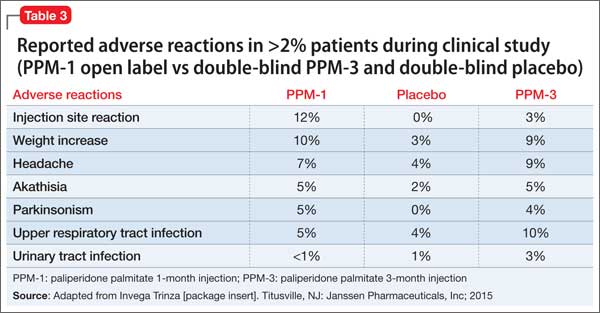
Contraindications
Allergic reactions. Patients who have a hypersensitivity to paliperidone, risperidone, or their components should not receive PPM-3. Anaphylactic reactions have been reported in patients who previously tolerated risperidone or oral paliperidone, which could be significant because the drug is slowly released over 3 months. Other adverse reactions, including angioedema, ileus, swollen tongue, thrombotic thrombocytopenic purpura, urinary incontinence, and urinary retention, were reported post-approval of paliperidone; however, these adverse effects were reported voluntarily from an unknown population size and, therefore, it is unknown whether there is a causal relationship to the drug or its frequency.
Drug-drug interactions. Although paliperidone is not expected to cause drug– drug interactions with medications that are metabolized by CYP isoenzymes, it is recommended to avoid using a strong inducer of CYP3A4 and/or P-glycoprotein.
Overdose. When assessing treatment options and recovery, consider the half-life of PPM-3 and its long-lasting effects.
Because PPM-3 is administered by a licensed health care provider, the potential for overdose is low. However, if overdose occurs, general treatment and management measures should be employed as with overdose of any drug and the possibility of multiple drug overdose should be considered. There is no specific antidote to paliperidone. Contact a certified poison control center for guidance on managing paliperidone and PPM-3 overdose. Generally, management consists of supportive care.
Black-box warning in dementia. As with all atypical antipsychotics, the black-box warning for PPM-3 states that it is not approved for, and should not be used in, patients with dementia-related psychosis. An analysis of placebo-controlled studies revealed that patients taking an antipsychotic had (1) 1.6 to 1.7 times the risk of death than those who received placebo and (2) a higher incidence of cerebrovascular adverse reactions.
Adverse reactions
The safety profile of PPM-3 is similar to that of PPM-1. The most common adverse reactions are:
• reaction at the injection site
• weight gain
• headache
• upper respiratory tract infection
• akathisia
• parkinsonism.
See the full prescribing information for a complete list of adverse effects.
Related Resources
• Sedky K, Nazir R, Lindenmayer JP, et al. Paliperidone palmitate: once monthly treatment option for schizophrenia. Current Psychiatry. 2010;9(3):48-49.
• Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial [published online March 29, 2015]. JAMA Psychiatry. doi: 10.1001/jamapsychiatry.2015.0241.
Drug Brand Names
Paliperidone palmitate • Invega Sustenna, Invega Trinza
Risperidone • Risperdal
Source: Invega Trinza [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2015.
A 3-month paliperidone palmitate (PPM-3) extended-release injectable suspension was approved by the FDA in May 2015 for preventing relapse among patients with schizophrenia, under the brand name Invega Trinza (Table 1). Administered 4 times a year, PPM-3 provides the longest interval of any approved long-acting injectable antipsychotic (LAIA). PPM-3 can be administered to patients with schizophrenia who have been taking 1-month paliperidone palmitate (PPM-1) extended-release injectable suspension (brand name, Invega Sustenna), once a month, for at least 4 months.
How it works
PPM-3 is a LAIA injection. Because of its low solubility in water, paliperidone palmitate dissolves slowly once injected before being hydrolyzed as paliperidone and absorbed into the bloodstream. From time of release on Day 1, PPM-3 remains active for as long 18 months.
PPM-3 reaches a maximum plasma concentration between Day 30 and Day 33. In clinical trials, PPM-3 had a median half-life of 84 to 95 days when injected into the deltoid muscle and a median half-life of 118 to 139 days when injected into the gluteal muscle.
Paliperidone is not extensively metabolized in the liver. Although results of a study suggest that cytochrome P450 (CYP) 2D6 and CYP3A4 might play a role in metabolizing paliperidone, there is no evidence that it has a significant role.
Dosing and administration
PPM-3 is administered intramuscularly by a licensed health care professional, once every 3 months. The recommended dosage is based on the patient’s previous dosage of PPM-1 (Table 2).
See the prescribing information for administration instructions.
Efficacy
The efficacy of PPM-3 was assessed in a long-term double-blind, placebo-controlled, randomized-withdrawal trial in adult patients with acute symptoms (previously treated with an oral antipsychotic) or adequately treated with a LAIA, either PPM-1 or another agent; patients receiving PPM-1, 39 mg, injections were ineligible. All patients entering the study received PPM-1 in place of the next scheduled injection.
The study comprised 3 treatment periods:
• 17-Week flexible-dose open-label period with PPM-1 (ie, first part of a 29-week open-label stabilization phase): Patients (N = 506) received PPM-1 with a flexible dose based on symptom response, tolerability, and medication history. Patients had to achieve a Positive and Negative Syndrome Scale (PANSS) total score of <70 at Week 17 to enter the second phase.
• 12-Week open-label with PPM-3 (ie, second part of the 29-week open-label stabilization phase): Patients (N = 379) received a single injection of PPM-3 that was 3.5 times the last dose of PPM-1. Patients had to achieve a PANSS total score of <70 and ≤4 for 7 specific PANSS items.
• A variable length double-blind treatment period: Patients (N = 305) were randomized 1:1 to continue treatment with PPM-3 (273 mg, 410 mg, 546 mg, or 819 mg) or placebo (administered once every 12 weeks) until relapse, early withdrawal, or end of the study. The primary efficacy measure was time to first relapse, defined as psychiatric hospitalization, ≥25% increase or a 10-point increase in total PANSS score on 2 consecutive assessments, deliberate self-injury, violent behavior, suicidal or homicidal ideation, or a score of ≥5 (if the maximum baseline score was ≤3) or ≥6 (if the maximum baseline score was 4) on 2 consecutive assessments of the specific PANSS items.
Among the patients in the third treatment period, 23% of those who received placebo and 7.4% of those who received PPM-3 experienced a relapse event. The time to relapse was significantly longer for patients who received PPM-3 than for those who received placebo.
See Table 3 for adverse reactions reported in patients who received PPM-3 and those taking placebo in the study.
Contraindications
Allergic reactions. Patients who have a hypersensitivity to paliperidone, risperidone, or their components should not receive PPM-3. Anaphylactic reactions have been reported in patients who previously tolerated risperidone or oral paliperidone, which could be significant because the drug is slowly released over 3 months. Other adverse reactions, including angioedema, ileus, swollen tongue, thrombotic thrombocytopenic purpura, urinary incontinence, and urinary retention, were reported post-approval of paliperidone; however, these adverse effects were reported voluntarily from an unknown population size and, therefore, it is unknown whether there is a causal relationship to the drug or its frequency.
Drug-drug interactions. Although paliperidone is not expected to cause drug– drug interactions with medications that are metabolized by CYP isoenzymes, it is recommended to avoid using a strong inducer of CYP3A4 and/or P-glycoprotein.
Overdose. When assessing treatment options and recovery, consider the half-life of PPM-3 and its long-lasting effects.
Because PPM-3 is administered by a licensed health care provider, the potential for overdose is low. However, if overdose occurs, general treatment and management measures should be employed as with overdose of any drug and the possibility of multiple drug overdose should be considered. There is no specific antidote to paliperidone. Contact a certified poison control center for guidance on managing paliperidone and PPM-3 overdose. Generally, management consists of supportive care.
Black-box warning in dementia. As with all atypical antipsychotics, the black-box warning for PPM-3 states that it is not approved for, and should not be used in, patients with dementia-related psychosis. An analysis of placebo-controlled studies revealed that patients taking an antipsychotic had (1) 1.6 to 1.7 times the risk of death than those who received placebo and (2) a higher incidence of cerebrovascular adverse reactions.
Adverse reactions
The safety profile of PPM-3 is similar to that of PPM-1. The most common adverse reactions are:
• reaction at the injection site
• weight gain
• headache
• upper respiratory tract infection
• akathisia
• parkinsonism.
See the full prescribing information for a complete list of adverse effects.
Related Resources
• Sedky K, Nazir R, Lindenmayer JP, et al. Paliperidone palmitate: once monthly treatment option for schizophrenia. Current Psychiatry. 2010;9(3):48-49.
• Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial [published online March 29, 2015]. JAMA Psychiatry. doi: 10.1001/jamapsychiatry.2015.0241.
Drug Brand Names
Paliperidone palmitate • Invega Sustenna, Invega Trinza
Risperidone • Risperdal
A 3-month paliperidone palmitate (PPM-3) extended-release injectable suspension was approved by the FDA in May 2015 for preventing relapse among patients with schizophrenia, under the brand name Invega Trinza (Table 1). Administered 4 times a year, PPM-3 provides the longest interval of any approved long-acting injectable antipsychotic (LAIA). PPM-3 can be administered to patients with schizophrenia who have been taking 1-month paliperidone palmitate (PPM-1) extended-release injectable suspension (brand name, Invega Sustenna), once a month, for at least 4 months.
How it works
PPM-3 is a LAIA injection. Because of its low solubility in water, paliperidone palmitate dissolves slowly once injected before being hydrolyzed as paliperidone and absorbed into the bloodstream. From time of release on Day 1, PPM-3 remains active for as long 18 months.
PPM-3 reaches a maximum plasma concentration between Day 30 and Day 33. In clinical trials, PPM-3 had a median half-life of 84 to 95 days when injected into the deltoid muscle and a median half-life of 118 to 139 days when injected into the gluteal muscle.
Paliperidone is not extensively metabolized in the liver. Although results of a study suggest that cytochrome P450 (CYP) 2D6 and CYP3A4 might play a role in metabolizing paliperidone, there is no evidence that it has a significant role.
Dosing and administration
PPM-3 is administered intramuscularly by a licensed health care professional, once every 3 months. The recommended dosage is based on the patient’s previous dosage of PPM-1 (Table 2).
See the prescribing information for administration instructions.
Efficacy
The efficacy of PPM-3 was assessed in a long-term double-blind, placebo-controlled, randomized-withdrawal trial in adult patients with acute symptoms (previously treated with an oral antipsychotic) or adequately treated with a LAIA, either PPM-1 or another agent; patients receiving PPM-1, 39 mg, injections were ineligible. All patients entering the study received PPM-1 in place of the next scheduled injection.
The study comprised 3 treatment periods:
• 17-Week flexible-dose open-label period with PPM-1 (ie, first part of a 29-week open-label stabilization phase): Patients (N = 506) received PPM-1 with a flexible dose based on symptom response, tolerability, and medication history. Patients had to achieve a Positive and Negative Syndrome Scale (PANSS) total score of <70 at Week 17 to enter the second phase.
• 12-Week open-label with PPM-3 (ie, second part of the 29-week open-label stabilization phase): Patients (N = 379) received a single injection of PPM-3 that was 3.5 times the last dose of PPM-1. Patients had to achieve a PANSS total score of <70 and ≤4 for 7 specific PANSS items.
• A variable length double-blind treatment period: Patients (N = 305) were randomized 1:1 to continue treatment with PPM-3 (273 mg, 410 mg, 546 mg, or 819 mg) or placebo (administered once every 12 weeks) until relapse, early withdrawal, or end of the study. The primary efficacy measure was time to first relapse, defined as psychiatric hospitalization, ≥25% increase or a 10-point increase in total PANSS score on 2 consecutive assessments, deliberate self-injury, violent behavior, suicidal or homicidal ideation, or a score of ≥5 (if the maximum baseline score was ≤3) or ≥6 (if the maximum baseline score was 4) on 2 consecutive assessments of the specific PANSS items.
Among the patients in the third treatment period, 23% of those who received placebo and 7.4% of those who received PPM-3 experienced a relapse event. The time to relapse was significantly longer for patients who received PPM-3 than for those who received placebo.
See Table 3 for adverse reactions reported in patients who received PPM-3 and those taking placebo in the study.
Contraindications
Allergic reactions. Patients who have a hypersensitivity to paliperidone, risperidone, or their components should not receive PPM-3. Anaphylactic reactions have been reported in patients who previously tolerated risperidone or oral paliperidone, which could be significant because the drug is slowly released over 3 months. Other adverse reactions, including angioedema, ileus, swollen tongue, thrombotic thrombocytopenic purpura, urinary incontinence, and urinary retention, were reported post-approval of paliperidone; however, these adverse effects were reported voluntarily from an unknown population size and, therefore, it is unknown whether there is a causal relationship to the drug or its frequency.
Drug-drug interactions. Although paliperidone is not expected to cause drug– drug interactions with medications that are metabolized by CYP isoenzymes, it is recommended to avoid using a strong inducer of CYP3A4 and/or P-glycoprotein.
Overdose. When assessing treatment options and recovery, consider the half-life of PPM-3 and its long-lasting effects.
Because PPM-3 is administered by a licensed health care provider, the potential for overdose is low. However, if overdose occurs, general treatment and management measures should be employed as with overdose of any drug and the possibility of multiple drug overdose should be considered. There is no specific antidote to paliperidone. Contact a certified poison control center for guidance on managing paliperidone and PPM-3 overdose. Generally, management consists of supportive care.
Black-box warning in dementia. As with all atypical antipsychotics, the black-box warning for PPM-3 states that it is not approved for, and should not be used in, patients with dementia-related psychosis. An analysis of placebo-controlled studies revealed that patients taking an antipsychotic had (1) 1.6 to 1.7 times the risk of death than those who received placebo and (2) a higher incidence of cerebrovascular adverse reactions.
Adverse reactions
The safety profile of PPM-3 is similar to that of PPM-1. The most common adverse reactions are:
• reaction at the injection site
• weight gain
• headache
• upper respiratory tract infection
• akathisia
• parkinsonism.
See the full prescribing information for a complete list of adverse effects.
Related Resources
• Sedky K, Nazir R, Lindenmayer JP, et al. Paliperidone palmitate: once monthly treatment option for schizophrenia. Current Psychiatry. 2010;9(3):48-49.
• Berwaerts J, Liu Y, Gopal S, et al. Efficacy and safety of the 3-month formulation of paliperidone palmitate vs placebo for relapse prevention of schizophrenia: a randomized clinical trial [published online March 29, 2015]. JAMA Psychiatry. doi: 10.1001/jamapsychiatry.2015.0241.
Drug Brand Names
Paliperidone palmitate • Invega Sustenna, Invega Trinza
Risperidone • Risperdal
Source: Invega Trinza [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2015.
Source: Invega Trinza [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2015.
Asenapine for pediatric bipolar disorder: New indication
Asenapine an atypical antipsychotic sold under the brand name Saphris, was granted a second, pediatric indication by the FDA in March 2015 as monotherapy for acute treatment of manic or mixed episodes of bipolar I disorder in children and adolescents age 10 to 17 (Table 1).1 (Asenapine was first approved in August 2009 as monotherapy or adjunctive therapy to lithium or valproate in adults for schizophrenia and bipolar I disorder.1,2)
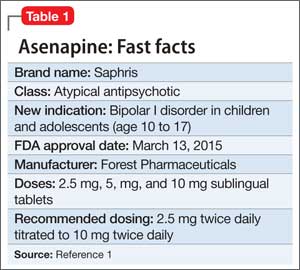
Dosage and administration
Asenapine is available as 2.5-, 5-, and 10-mg sublingual tablets, the only atypical antipsychotic with this formulation.1 The recommended dosage for the new indication is 2.5 mg twice daily for 3 days, titrated to 5 mg twice daily, titrated again to 10 mg twice daily after 3 days.3 In a phase I study, pediatric patients appeared to be more sensitive to dystonia when the recommended dosage escalation schedule was not followed.3
In clinical trials, drinking water 2 to 5 minutes after taking asenapine decreased exposure to the drug. Instruct patients not to swallow the tablet and to avoid eating and drinking for 10 minutes after administration.3
For full prescribing information for pediatric and adult patients, see Reference 3.
Safety and efficacy
In a 3-week, placebo-controlled, double-blind trial of 403 patients, 302 children and adolescents age 10 to 17 received asenapine at fixed dosages of 2.5 to 10 mg twice daily; the remainder were given placebo. The Young Mania Rating Scale (YMRS) total score and Clinical Global Impressions Severity of Illness scores of patients who received asenapine improved significantly compared with those who received placebo, as measured by change from baseline to week 3 (Table 2).1
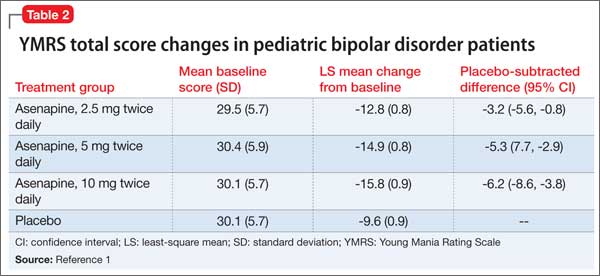
The safety and efficacy of asenapine has not been evaluated in pediatric bipolar disorder patients age ≤10 or pediatric schizophrenia patients age ≤12, or as an adjunctive therapy in pediatric bipolar disorder patients.
Asenapine was not shown to be effective in pediatric patients with schizophrenia in an 8-week, placebo-controlled, double-blind trial.
The pharmacokinetics of asenapine in pediatric patients are similar to those seen in adults.
Adverse effects
In pediatric patients, the most common reported adverse effects of asenapine are:
• dizziness
• dysgeusia
• fatigue
• increased appetite
• increased weight
• nausea
• oral paresthesia
• somnolence.
Similar adverse effects were reported in the pediatric bipolar disorder and adult bipolar disorder clinical trials (Table 3).3 A complete list of reported adverse effects is given in the package insert.3
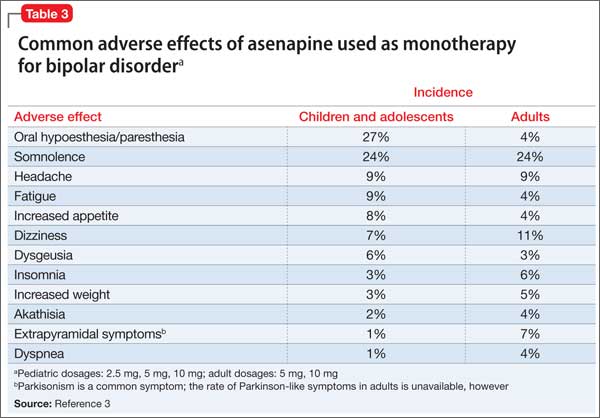
When treating pediatric patients, monitor the child’s weight gain against expected normal weight gain.
Asenapine is contraindicated in patients with hepatic impairment and those who have a hypersensitivity to asenapine or any components in its formulation.3
1. Actavis receives FDA approval of Saphris for pediatric patients with bipolar I disorder. Drugs.com. http://www.drugs.com/newdrugs/actavis-receivesfda-
approval-saphris-pediatric-patients-bipolardisorder-4188.html. Published March 2015. Accessed June 19, 2015.
2. Lincoln J, Preskon S. Asenapine for schizophrenia and bipolar I disorder. Current Psychiatry. 2009;12(8):75-76,83-85.
3. Saphris [package insert]. St. Louis, MO: Forest Pharmaceuticals; 2015.
Asenapine an atypical antipsychotic sold under the brand name Saphris, was granted a second, pediatric indication by the FDA in March 2015 as monotherapy for acute treatment of manic or mixed episodes of bipolar I disorder in children and adolescents age 10 to 17 (Table 1).1 (Asenapine was first approved in August 2009 as monotherapy or adjunctive therapy to lithium or valproate in adults for schizophrenia and bipolar I disorder.1,2)
Dosage and administration
Asenapine is available as 2.5-, 5-, and 10-mg sublingual tablets, the only atypical antipsychotic with this formulation.1 The recommended dosage for the new indication is 2.5 mg twice daily for 3 days, titrated to 5 mg twice daily, titrated again to 10 mg twice daily after 3 days.3 In a phase I study, pediatric patients appeared to be more sensitive to dystonia when the recommended dosage escalation schedule was not followed.3
In clinical trials, drinking water 2 to 5 minutes after taking asenapine decreased exposure to the drug. Instruct patients not to swallow the tablet and to avoid eating and drinking for 10 minutes after administration.3
For full prescribing information for pediatric and adult patients, see Reference 3.
Safety and efficacy
In a 3-week, placebo-controlled, double-blind trial of 403 patients, 302 children and adolescents age 10 to 17 received asenapine at fixed dosages of 2.5 to 10 mg twice daily; the remainder were given placebo. The Young Mania Rating Scale (YMRS) total score and Clinical Global Impressions Severity of Illness scores of patients who received asenapine improved significantly compared with those who received placebo, as measured by change from baseline to week 3 (Table 2).1
The safety and efficacy of asenapine has not been evaluated in pediatric bipolar disorder patients age ≤10 or pediatric schizophrenia patients age ≤12, or as an adjunctive therapy in pediatric bipolar disorder patients.
Asenapine was not shown to be effective in pediatric patients with schizophrenia in an 8-week, placebo-controlled, double-blind trial.
The pharmacokinetics of asenapine in pediatric patients are similar to those seen in adults.
Adverse effects
In pediatric patients, the most common reported adverse effects of asenapine are:
• dizziness
• dysgeusia
• fatigue
• increased appetite
• increased weight
• nausea
• oral paresthesia
• somnolence.
Similar adverse effects were reported in the pediatric bipolar disorder and adult bipolar disorder clinical trials (Table 3).3 A complete list of reported adverse effects is given in the package insert.3
When treating pediatric patients, monitor the child’s weight gain against expected normal weight gain.
Asenapine is contraindicated in patients with hepatic impairment and those who have a hypersensitivity to asenapine or any components in its formulation.3
Asenapine an atypical antipsychotic sold under the brand name Saphris, was granted a second, pediatric indication by the FDA in March 2015 as monotherapy for acute treatment of manic or mixed episodes of bipolar I disorder in children and adolescents age 10 to 17 (Table 1).1 (Asenapine was first approved in August 2009 as monotherapy or adjunctive therapy to lithium or valproate in adults for schizophrenia and bipolar I disorder.1,2)
Dosage and administration
Asenapine is available as 2.5-, 5-, and 10-mg sublingual tablets, the only atypical antipsychotic with this formulation.1 The recommended dosage for the new indication is 2.5 mg twice daily for 3 days, titrated to 5 mg twice daily, titrated again to 10 mg twice daily after 3 days.3 In a phase I study, pediatric patients appeared to be more sensitive to dystonia when the recommended dosage escalation schedule was not followed.3
In clinical trials, drinking water 2 to 5 minutes after taking asenapine decreased exposure to the drug. Instruct patients not to swallow the tablet and to avoid eating and drinking for 10 minutes after administration.3
For full prescribing information for pediatric and adult patients, see Reference 3.
Safety and efficacy
In a 3-week, placebo-controlled, double-blind trial of 403 patients, 302 children and adolescents age 10 to 17 received asenapine at fixed dosages of 2.5 to 10 mg twice daily; the remainder were given placebo. The Young Mania Rating Scale (YMRS) total score and Clinical Global Impressions Severity of Illness scores of patients who received asenapine improved significantly compared with those who received placebo, as measured by change from baseline to week 3 (Table 2).1
The safety and efficacy of asenapine has not been evaluated in pediatric bipolar disorder patients age ≤10 or pediatric schizophrenia patients age ≤12, or as an adjunctive therapy in pediatric bipolar disorder patients.
Asenapine was not shown to be effective in pediatric patients with schizophrenia in an 8-week, placebo-controlled, double-blind trial.
The pharmacokinetics of asenapine in pediatric patients are similar to those seen in adults.
Adverse effects
In pediatric patients, the most common reported adverse effects of asenapine are:
• dizziness
• dysgeusia
• fatigue
• increased appetite
• increased weight
• nausea
• oral paresthesia
• somnolence.
Similar adverse effects were reported in the pediatric bipolar disorder and adult bipolar disorder clinical trials (Table 3).3 A complete list of reported adverse effects is given in the package insert.3
When treating pediatric patients, monitor the child’s weight gain against expected normal weight gain.
Asenapine is contraindicated in patients with hepatic impairment and those who have a hypersensitivity to asenapine or any components in its formulation.3
1. Actavis receives FDA approval of Saphris for pediatric patients with bipolar I disorder. Drugs.com. http://www.drugs.com/newdrugs/actavis-receivesfda-
approval-saphris-pediatric-patients-bipolardisorder-4188.html. Published March 2015. Accessed June 19, 2015.
2. Lincoln J, Preskon S. Asenapine for schizophrenia and bipolar I disorder. Current Psychiatry. 2009;12(8):75-76,83-85.
3. Saphris [package insert]. St. Louis, MO: Forest Pharmaceuticals; 2015.
1. Actavis receives FDA approval of Saphris for pediatric patients with bipolar I disorder. Drugs.com. http://www.drugs.com/newdrugs/actavis-receivesfda-
approval-saphris-pediatric-patients-bipolardisorder-4188.html. Published March 2015. Accessed June 19, 2015.
2. Lincoln J, Preskon S. Asenapine for schizophrenia and bipolar I disorder. Current Psychiatry. 2009;12(8):75-76,83-85.
3. Saphris [package insert]. St. Louis, MO: Forest Pharmaceuticals; 2015.
First EDition: News for and about the practice of Emergency Medicine
Three lab tests predict serious bacterial infections in infants
BY JENNIE SMITH
AT SAEM 2015
SAN DIEGO – A simple three-variable prediction rule can accurately predict which febrile infants younger than age 2 months with fever who present to the ED have serious bacterial infections. Bacterial meningitis, urinary tract infections, and bacteremia are considered serious bacterial infections; many young infants with these infections are difficult to identify, and current laboratory protocols for identifying them include urinalysis, white blood cell counts, band counts, and sometimes cerebrospinal fluid.

Vitals Key clinical point: A rule comprising three lab measurements allows for the prediction of serious bacterial infections in infants under age 2 months presenting to the ED. Major finding: Positive urinalysis, ANC of 4.09 x 1,000/mm3 or higher, and serum procalcitonin of 1.71 ng/mL or greater are between 98% and 99% sensitive in predicting SBIs. Data source: A prospective observational cohort of 1,821 infants at 21 centers forming a pediatric emergency research network. Disclosures: The study was funded by federal government grants. The authors disclosed no conflicts of interest. |
In a presentation at the annual meeting of the Society for Academic Emergency Medicine, Dr Nathan Kuppermann of the University of California, Davis, demonstrated results from a large prospective cohort study of 1,821 febrile infants 60 days old and younger conducted at 21 EDs. Infants with underlying congenital anomalies or critical illness were excluded from the study.
The investigators evaluated 8 variables as potential predictors: age, temperature, Yale Observation Scale score, and clinician suspicion of SBI, along with 4 laboratory variables (urinalysis, white blood cell count, absolute neutrophil count [ANC], and procalcitonin). Band counts were available at some, but not all of the study centers, and therefore were not evaluated.
Dr Kuppermann and his colleagues found that positive urinalysis, ANC of 4.09 x 1,000/mm3 or higher, and serum procalcitonin of 1.71 ng/mL or higher were, taken together, 98% to 99% sensitive and about 60% specific, in predicting SBI in the cohort. Negative predictive values approached 100%. The rate of SBI was 9.3% of the cohort, in keeping with expected rates.
“The SBI positive group was more likely to have higher clinician suspicion of SBI, and all of the lab markers were more elevated in the SBI positive group than the SBI negative group,” Dr Kuppermann said at the meeting. However, after the researchers considered all of the predictors as a group, only the urinalysis, the ANC, and the procalcitonin remained important. Only 3 of 1,821 (0.2%) infants with SBIs were missed when the three-variable prediction tool was used.
To make the prediction rule easier to remember and use, the investigators evaluated lower, more standard, and easier to remember thresholds for the three variables. They reanalyzed their data using a lower cutoff point for ANC of 4.00 x 1,000/mm3, and a lowered procalcitonin cutoff of 0.5 ng/mL. The rule performed almost identically as the original rule, and did not miss any more patients with SBIs beyond the original three.

Dr Kuppermann described the three-variable rule as “simple, objective, and highly accurate” in predicting or ruling out SBI. Nonetheless, it requires external validation in a large cohort, he acknowledged. He said he would continue to routinely perform lumbar punctures in infants younger than 30 days with fever until the findings could be further validated.
“But personally, in that second month of life, I would use these data to decide who actually needs a lumbar puncture and hospitalization,” he said.
Dr Kuppermann also noted as a limitation of the study that the cohort included few infants with bacterial meningitis.
ED revisits twice as frequent as expected
BY MARY ANN MOON
FROM ANNALS OF INTERNAL MEDICINE
The rate of adult revisits to EDs is more than twice as high as has been reported previously – 8% at 3 days and 20% at 30 days – in large part because until now researchers have failed to account for revisits to different hospitals, according to a report published online June 2 in Annals of Internal Medicine.
Vitals Key clinical point: Revisits to the emergency department were twice as frequent as previously reported: 8% at 3 days and 20% at 30 days. Major finding: At 3 days after an initial ED visit, the overall revisit rate was 8.2%, and at 30 days it was 20%, with one-third of these revisits occurring at a medical facility different from that of the initial visit. Data source: A longitudinal, population-based study of adult revisits to the ED after 57,530,239 initial visits in six states during 2006-2010. Disclosures: This study was supported by the US Agency for Healthcare Research and Quality. The researchers’ financial disclosures are available at www.acponline.org. |
Little is known about returns to an emergency department following an index ED visit because most studies have assessed only visits to a single institution or to hospitals within a single state or insurance plan. Now researchers have performed a broader examination of the issue by analyzing newly available multistate longitudinal data from the Healthcare Cost and Utilization Project, which allowed them to identify returns to any ED or acute-care hospital. They focused on acute-care revisits after 57,530,239 initial ED visits by adults in six states (Arizona, California, Florida, Nebraska, Utah, and Hawaii) during 2006-2010.
At 3 days after an initial ED visit, the overall revisit rate was 8.2%, with one-third of these revisits occurring at a medical facility different from that of the initial visit. Previously, estimates of 3-day revisits have ranged from 2.7% to 3.4%. At 30 days, the revisit rate was 20%, and approximately one-third of these revisits involved a different facility. Revisits to different institutions “may have special clinical and financial implications because fragmentation of care increases the likelihood of duplication of services and problems with care transitions,” said Dr Reena Duseja of the department of emergency medicine, University of California, San Francisco, and her associates.
Views on the News Highlighting an underappreciated problem The findings of Duseja et al highlight an underappreciated problem and also raise important questions. To what extent do ED revisits represent gaps in quality as opposed to reasonable strategies that prevent admissions? How often are revisits due to failures of transitional care, suboptimal patient education, or lack of timely follow-up? And why do patients so often seek care at different institutions? Are they dissatisfied with their initial encounter, exercising greater discretion in choosing a facility the second time around, or doing something else? Dr Kumar Dharmarajan and Dr Harlan M. Krumholz are at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Connecticut. Dr Dharmarajan reported receiving grant support from the National Institute on Aging and the American Federation for Aging Research. Dr Krumholz reported receiving grant support from the National Heart, Lung, and Blood Institute and the Center for Cardiovascular Outcomes Research at Yale. The investigators made these remarks in an editorial accompanying Dr Duseja’s report (Ann Intern Med. 2015;162(11):793-794. doi:10.7326/M15-0878). |
“The scope of revisits to outside institutions is much greater than previously suspected, which suggests that improving communication infrastructure across institutions (such as health information exchanges) may improve care and allow individual institutions to get a more accurate picture of their revisit rates,” they noted (Ann Intern Med. 2015;162(11):750-756. doi:10.7326/M14-1616).
Revisit rates varied substantially according to diagnosis. “Skin and subcutaneous tissue infection” accounted for 23% of revisits. “Abdominal pain” was the diagnosis with the next highest revisit rate (10%). The most frequent diagnosis among patients who revisited a different hospital was back pain (2.6%), and nonspecific chest pain was the diagnosis with the
highest rate of later admission to a different hospital (1.1%).

“Financial data from the Florida facilities showed that revisits accounted for more of the total costs of ED care than initial visits did. This demonstrates that revisits are a major, and unaccounted for, component of emergency care costs,” Dr Duseja and her associates said.
Because of insufficient data, they could not determine whether these revisits reflected inadequate access to primary care, patient nonadherence to treatment recommendations, poor quality of care at the initial visit, or other factors, the researchers noted.
Cefazolin ranks sixth as cause of drug-induced liver injury
BY AMY KARON
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
| A single intravenous infusion of cefazolin can cause drug-induced liver injury (DILI), and the antibiotic ranked sixth among pharmacologic causes of hepatic injury in an analysis of 1,212 patients. “Cephalosporins appear to be a relatively common cause of antibiotic-associated liver injury,” said Dr Saleh Alqahtani at the University of Texas Southwestern in Dallas and his associates. “The latency period is typically 1 to 3 weeks after exposure, and patients may not become symptomatic until after the antibiotic is stopped – this is particularly true in the unique clinical syndrome in which a single infusion of cefazolin leads to drug-induced liver injury.” |
Vitals Key clinical point: A single dose of cefazolin can cause drug-induced liver injury (DILI), and the agent is implicated more often than previously thought. Major finding: Cefazolin ranked sixth among causes of DILI, and signs and symptoms began 1 to 3 weeks after initial exposure. Data source: Registry-based study of 1,212 cases of DILI. Disclosures: The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, the National Cancer Institute, and by Clinical and Translational Science Award grants. The investigators reported having no conflicts of interest. |
“Cephalosporins have been reported as rare causes of DILI, but most data come from single case reports,” the researchers said. To study causes of DILI, they analyzed cases from the Drug-Induced Livery Injury Network, an ongoing prospective study at 8 US medical centers. Enrolled patients had strong clinical suspicion for liver injury caused by a drug or an herbal agent. Liver injury was defined based on specific criteria for liver enzymes, alkaline phosphatase (ALP), or total bilirubin levels, or as an international normalized ratio greater than 1.5 that was accompanied by elevated liver enzymes or ALP. Patients were followed for at least 6 months after their baseline visit (Clin Gastroenterol Hepatol. Published January 26, 2015. doi: 10.1016/j.cgh.2015.01.010).
Among the 1,212 cases of DILI in the analysis, one-third were linked to antimicrobial therapies, including 41 (3.3%) in which cephalosporins were implicated, the investigators reported. Nineteen of the cases were tied to a single dose of intravenous cefazolin given before surgery. These patients developed cholestatic or mixed hepatocellular-cholestatic injury 1 to 3 weeks after the cefazolin infusion. They almost always had jaundice and pruritus, and usually also had fever and nausea. Signs and symptoms were self-limiting, resolving within a few days to a few weeks.
“Because of confusion about the specific diagnosis, patients underwent substantial diagnostic testing (including multiple computed tomography scans, magnetic resonance imaging scans, endoscopic retrograde cholangiopancreatography exams, liver biopsies, and others), which often were unnecessary, and in some cases led to severe complications,” the investigators said.
“The study also identified barriers to identifying cefazolin as a cause of DILI,” they said. Patients often did not know they had received the antibiotic, and clinicians, including study investigators, often did not know that cefazolin could cause DILI. In more than half of cases, DILI was linked to cefazolin only after careful medical record reviews. “For these reasons, we speculate that cefazolin is and has been underappreciated as a cause of DILI,” the researchers noted. “The appearance of jaundice and pruritus 1 to 3 weeks after minor surgery should lead to a search of surgical records and medications that might have been given during surgery. These results also imply that the merits of routine use of cefazolin at the time of uncomplicated surgery should be reconsidered carefully.”

“Two patients died after receiving cephalosporins other than cefazolin, and another patient developed severe liver injury,” the researchers said. “However, in each of the fatal cases, patients had a complicated clinical course, with a severe hypersensitivity reaction on top of an underlying liver disease. Therefore, we urge caution in concluding that non-cefazolin cephalosporin-induced DILI may be severe or fatal,” they said. “Because cephalosporins are used commonly in clinical practice, it is likely that the overall mortality rate associated with cephalosporin use is low, but not nil, and it may be more likely in patients with underlying disorders.”
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, the National Cancer Institute, and by six Clinical and Translational Science Award grants. The investigators reported having no conflicts of interest.
Pelvic CT may not be needed to diagnose intra-abdominal injury in children
BY JENNIE SMITH
FROM SAEM 2015
| San DIEGO – Children who have suffered blunt trauma are routinely screened in EDs for intra-abdominal injury (IAI) via computed tomography of the abdomen and pelvis. |
Vitals Key clinical point: Abdominal CT scans without a pelvic portion may diagnose intra-abdominal injury in children as well as do full abdominopelvic scans, with less radiation exposure to patients. Major finding: Abdominal CT alone was 85% sensitive (95% CI, 65%-96%) and 99% specific (95% CI, 97%-100%) in identifying IAIs. The four missed injuries were solid organ injuries within the radiographic abdomen. Data source: A retrospective cohort study of 313 patients aged 3 to 17 years presenting to 12 EDs. Disclosures: The study was funded by the Carolinas Trauma Network Research Center of Excellence. None of the investigators disclosed conflicts of interest. |
But concerns about excess exposure to CT radiation, particularly to the gonads, led one group of researchers to question whether it’s necessary to scan the entire abdominopelvic region in all of these patients to identify IAI.
Dr Stacy Reynolds and her colleagues at the Carolinas Medical Center in Charlotte, North Carolina, hypothesized that CT limited to the radiographic abdomen – the region between the dome of the diaphragm to the top of the iliac crest – can capture the vast majority of IAIs in this population.
At the Society for Academic Emergency Medicine annual meeting, Dr Reynolds presented results from a retrospective cohort study enrolling 313 hemodynamically stable pediatric patients (median age 14 years, 64% male) presenting to 12 EDs after blunt trauma. Patients with known pelvic fractures or hip dislocation were excluded, as they would have had a clear indication for a full abdominopelvic CT.
All subjects underwent axial abdominopelvic CT imaging. Researchers created matched pairs of images comprising the original scans and those that had been altered with software that truncated the pelvic portion of the study to create CT abdomen-only studies. Study radiologists were blinded to the results of the original scans.
In all, 26 IAI’s were diagnosed in 24 patients: 8 hepatic injuries, 12 splenic injuries, 5 renal injuries, and 1 retroperitoneal hemorrhage. Abdominal CT alone was 85% sensitive (95% CI, 65%-96%) and 99% specific (95% CI, 97%-100%) in identifying IAIs. The four missed injuries were solid organ injuries within the radiographic abdomen. False positives occurred in two of the complete scans, both involving free fluid prompting suspicion of small bowel injury later ruled out by clinical observation.
Dr Reynolds said in an interview that the findings, while promising, were limited by the study’s small numbers, and its use of axial images alone, when sagittal images also would be required for the most accurate diagnoses. Also, physician suspicion of IAI prior to imaging was not captured because of the study’s retrospective design, she said. “The real key to whether or not this hypothesis is valuable is if physicians are able to target the right population of patients for application.”
Dr Reynolds cautioned that the findings would need to be validated in a larger trial before any changes could be made to clinical practice. “Some of the outcomes that we need to make sure whether we’re missing are still rare,” she said. “You couldn’t feel confident that this is the right way to go with a study this small, but it establishes that we can safely and ethically pursue a multicenter trial that would examine the issue with bigger numbers.”
Other groups of investigators, including members of the Pediatric Emergency Care Applied Research Network (PECARN), also have taken up the question of identifying children at low risk of IAI who may not need CT screening after blunt trauma. In 2013, PECARN published a prediction rule using only patient history and physical examination findings intended to obviate use of CT in the lowest-risk patients (Ann Emerg Med. 2013;62:107-116.e2).
Dr Reynolds said that while overuse of CT was a worrisome trend that could have long-term implications for patients, and that it was important to identify ways it might be limited, there is a reason it remains the go-to technology in the ED for detecting IAI. “It’s got very high sensitivity and specificity. If you’re a busy trauma surgeon who’s admitting 20 injured patients in a night, there’s no faster or more efficient way to determine whether the patient in front of you is injured.”
The ‘sad truth’ about suicide risk assessment scales
BY BRUCE JANCIN
EXPERT ANALYSIS FROM THE ANNUAL AAS CONFERENCE
ATLANTA – “Don’t – repeat, don’t – use risk assessment tools and scales in an effort to predict future suicide in patients who’ve committed intentional self-harm,” Dr Keith Hawton urged at the annual conference of the American Association of Suicidology.
He noted this isn’t simply a matter of his personal opinion; it’s also a strongly worded recommendation in the current UK NICE (National Institute for Health and Care Excellence) guidelines on the long-term management of patients who’ve committed self-harm. The various NICE guidelines, which address numerous areas of medical practice and are used to determine what’s reimbursable through the UK’s National Health Service, are famously evidence based and concerned with cost-effectiveness.
The NICE guidelines on management of self-harm further advise: “Do not use risk assessment tools and scales to determine who should and should not be offered treatment or who should be discharged from hospital.”
“Those are some fairly contentious statements about risk assessment scales. But those statements are based upon review of the evidence about the effectiveness of risk assessment scales,” according to Dr Hawton, professor of psychiatry and director of the Centre for Suicide Research at the University of Oxford (England).

“In our country, hospitals have become obsessed with risk assessment. And usually, it seems to be about protecting the organization rather than the patient, because so often the results aren’t linked to risk management, which is what we should be talking about,” he observed.
Dr Hawton and his colleagues provided some of the evidence that led to the NICE guideline committee’s thumbs-down on the use of suicide risk assessment scales in patients who’ve engaged in intentional self-harm. In a study provocatively titled “The sad truth about the SADPERSONS scale,” he and his coinvestigators essentially dismantled SADPERSONS, a widely used screening tool for suicide risk, concluding that it is without value.
The acronym stands for Sex (male), Age (<19 or >45), Depression, Previous attempts, Ethanol abuse, Rational thinking loss, Social supports lacking, Organized plan, No spouse, and Sickness. One point is given for each. Patients who score 7-10 are to be hospitalized, and those with a total of 5 or 6 points should be strongly considered for hospitalization.
Dr Hawton and coinvestigators tracked 126 consecutive patients who were evaluated for self-harm using the SADPERSONS scale in a general hospital emergency department and then followed them for 6 months. SADPERSONS performed miserably in predicting clinical management outcomes, such as admission to a psychiatric hospital or repetition of self-harm within 6 months. Indeed, the test failed to identify 4 of the 5 patients admitted to a psychiatric hospital, 65 of 70 who were referred from the ED to community psychiatric aftercare, and 28 of 31 who repeated self-harm within 6 months. Thus, its sensitivity as a predictor of repetition of self-harm was a lowly 6.6% (Emerg Med J. 2014;31:796-798).
And yet, a 32-hospital UK national study conducted by Dr Hawton and others found that SADPERSONS was the most widely used scale in EDs for risk assessment following self-harm (BMJ Open. 2014;4(5):e004732. doi:10.1136/bmjopen-2013-004732). “It’s a very crude tool,” Dr Hawton said. “How it found its way into common use in clinical practice is beyond me.”
bjancin@frontlinemedcom.com
Three lab tests predict serious bacterial infections in infants
BY JENNIE SMITH
AT SAEM 2015
SAN DIEGO – A simple three-variable prediction rule can accurately predict which febrile infants younger than age 2 months with fever who present to the ED have serious bacterial infections. Bacterial meningitis, urinary tract infections, and bacteremia are considered serious bacterial infections; many young infants with these infections are difficult to identify, and current laboratory protocols for identifying them include urinalysis, white blood cell counts, band counts, and sometimes cerebrospinal fluid.
Vitals Key clinical point: A rule comprising three lab measurements allows for the prediction of serious bacterial infections in infants under age 2 months presenting to the ED. Major finding: Positive urinalysis, ANC of 4.09 x 1,000/mm3 or higher, and serum procalcitonin of 1.71 ng/mL or greater are between 98% and 99% sensitive in predicting SBIs. Data source: A prospective observational cohort of 1,821 infants at 21 centers forming a pediatric emergency research network. Disclosures: The study was funded by federal government grants. The authors disclosed no conflicts of interest. |
In a presentation at the annual meeting of the Society for Academic Emergency Medicine, Dr Nathan Kuppermann of the University of California, Davis, demonstrated results from a large prospective cohort study of 1,821 febrile infants 60 days old and younger conducted at 21 EDs. Infants with underlying congenital anomalies or critical illness were excluded from the study.
The investigators evaluated 8 variables as potential predictors: age, temperature, Yale Observation Scale score, and clinician suspicion of SBI, along with 4 laboratory variables (urinalysis, white blood cell count, absolute neutrophil count [ANC], and procalcitonin). Band counts were available at some, but not all of the study centers, and therefore were not evaluated.
Dr Kuppermann and his colleagues found that positive urinalysis, ANC of 4.09 x 1,000/mm3 or higher, and serum procalcitonin of 1.71 ng/mL or higher were, taken together, 98% to 99% sensitive and about 60% specific, in predicting SBI in the cohort. Negative predictive values approached 100%. The rate of SBI was 9.3% of the cohort, in keeping with expected rates.
“The SBI positive group was more likely to have higher clinician suspicion of SBI, and all of the lab markers were more elevated in the SBI positive group than the SBI negative group,” Dr Kuppermann said at the meeting. However, after the researchers considered all of the predictors as a group, only the urinalysis, the ANC, and the procalcitonin remained important. Only 3 of 1,821 (0.2%) infants with SBIs were missed when the three-variable prediction tool was used.
To make the prediction rule easier to remember and use, the investigators evaluated lower, more standard, and easier to remember thresholds for the three variables. They reanalyzed their data using a lower cutoff point for ANC of 4.00 x 1,000/mm3, and a lowered procalcitonin cutoff of 0.5 ng/mL. The rule performed almost identically as the original rule, and did not miss any more patients with SBIs beyond the original three.
Dr Kuppermann described the three-variable rule as “simple, objective, and highly accurate” in predicting or ruling out SBI. Nonetheless, it requires external validation in a large cohort, he acknowledged. He said he would continue to routinely perform lumbar punctures in infants younger than 30 days with fever until the findings could be further validated.
“But personally, in that second month of life, I would use these data to decide who actually needs a lumbar puncture and hospitalization,” he said.
Dr Kuppermann also noted as a limitation of the study that the cohort included few infants with bacterial meningitis.
ED revisits twice as frequent as expected
BY MARY ANN MOON
FROM ANNALS OF INTERNAL MEDICINE
The rate of adult revisits to EDs is more than twice as high as has been reported previously – 8% at 3 days and 20% at 30 days – in large part because until now researchers have failed to account for revisits to different hospitals, according to a report published online June 2 in Annals of Internal Medicine.
Vitals Key clinical point: Revisits to the emergency department were twice as frequent as previously reported: 8% at 3 days and 20% at 30 days. Major finding: At 3 days after an initial ED visit, the overall revisit rate was 8.2%, and at 30 days it was 20%, with one-third of these revisits occurring at a medical facility different from that of the initial visit. Data source: A longitudinal, population-based study of adult revisits to the ED after 57,530,239 initial visits in six states during 2006-2010. Disclosures: This study was supported by the US Agency for Healthcare Research and Quality. The researchers’ financial disclosures are available at www.acponline.org. |
Little is known about returns to an emergency department following an index ED visit because most studies have assessed only visits to a single institution or to hospitals within a single state or insurance plan. Now researchers have performed a broader examination of the issue by analyzing newly available multistate longitudinal data from the Healthcare Cost and Utilization Project, which allowed them to identify returns to any ED or acute-care hospital. They focused on acute-care revisits after 57,530,239 initial ED visits by adults in six states (Arizona, California, Florida, Nebraska, Utah, and Hawaii) during 2006-2010.
At 3 days after an initial ED visit, the overall revisit rate was 8.2%, with one-third of these revisits occurring at a medical facility different from that of the initial visit. Previously, estimates of 3-day revisits have ranged from 2.7% to 3.4%. At 30 days, the revisit rate was 20%, and approximately one-third of these revisits involved a different facility. Revisits to different institutions “may have special clinical and financial implications because fragmentation of care increases the likelihood of duplication of services and problems with care transitions,” said Dr Reena Duseja of the department of emergency medicine, University of California, San Francisco, and her associates.
Views on the News Highlighting an underappreciated problem The findings of Duseja et al highlight an underappreciated problem and also raise important questions. To what extent do ED revisits represent gaps in quality as opposed to reasonable strategies that prevent admissions? How often are revisits due to failures of transitional care, suboptimal patient education, or lack of timely follow-up? And why do patients so often seek care at different institutions? Are they dissatisfied with their initial encounter, exercising greater discretion in choosing a facility the second time around, or doing something else? Dr Kumar Dharmarajan and Dr Harlan M. Krumholz are at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Connecticut. Dr Dharmarajan reported receiving grant support from the National Institute on Aging and the American Federation for Aging Research. Dr Krumholz reported receiving grant support from the National Heart, Lung, and Blood Institute and the Center for Cardiovascular Outcomes Research at Yale. The investigators made these remarks in an editorial accompanying Dr Duseja’s report (Ann Intern Med. 2015;162(11):793-794. doi:10.7326/M15-0878). |
“The scope of revisits to outside institutions is much greater than previously suspected, which suggests that improving communication infrastructure across institutions (such as health information exchanges) may improve care and allow individual institutions to get a more accurate picture of their revisit rates,” they noted (Ann Intern Med. 2015;162(11):750-756. doi:10.7326/M14-1616).
Revisit rates varied substantially according to diagnosis. “Skin and subcutaneous tissue infection” accounted for 23% of revisits. “Abdominal pain” was the diagnosis with the next highest revisit rate (10%). The most frequent diagnosis among patients who revisited a different hospital was back pain (2.6%), and nonspecific chest pain was the diagnosis with the
highest rate of later admission to a different hospital (1.1%).
“Financial data from the Florida facilities showed that revisits accounted for more of the total costs of ED care than initial visits did. This demonstrates that revisits are a major, and unaccounted for, component of emergency care costs,” Dr Duseja and her associates said.
Because of insufficient data, they could not determine whether these revisits reflected inadequate access to primary care, patient nonadherence to treatment recommendations, poor quality of care at the initial visit, or other factors, the researchers noted.
Cefazolin ranks sixth as cause of drug-induced liver injury
BY AMY KARON
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
| A single intravenous infusion of cefazolin can cause drug-induced liver injury (DILI), and the antibiotic ranked sixth among pharmacologic causes of hepatic injury in an analysis of 1,212 patients. “Cephalosporins appear to be a relatively common cause of antibiotic-associated liver injury,” said Dr Saleh Alqahtani at the University of Texas Southwestern in Dallas and his associates. “The latency period is typically 1 to 3 weeks after exposure, and patients may not become symptomatic until after the antibiotic is stopped – this is particularly true in the unique clinical syndrome in which a single infusion of cefazolin leads to drug-induced liver injury.” |
Vitals Key clinical point: A single dose of cefazolin can cause drug-induced liver injury (DILI), and the agent is implicated more often than previously thought. Major finding: Cefazolin ranked sixth among causes of DILI, and signs and symptoms began 1 to 3 weeks after initial exposure. Data source: Registry-based study of 1,212 cases of DILI. Disclosures: The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, the National Cancer Institute, and by Clinical and Translational Science Award grants. The investigators reported having no conflicts of interest. |
“Cephalosporins have been reported as rare causes of DILI, but most data come from single case reports,” the researchers said. To study causes of DILI, they analyzed cases from the Drug-Induced Livery Injury Network, an ongoing prospective study at 8 US medical centers. Enrolled patients had strong clinical suspicion for liver injury caused by a drug or an herbal agent. Liver injury was defined based on specific criteria for liver enzymes, alkaline phosphatase (ALP), or total bilirubin levels, or as an international normalized ratio greater than 1.5 that was accompanied by elevated liver enzymes or ALP. Patients were followed for at least 6 months after their baseline visit (Clin Gastroenterol Hepatol. Published January 26, 2015. doi: 10.1016/j.cgh.2015.01.010).
Among the 1,212 cases of DILI in the analysis, one-third were linked to antimicrobial therapies, including 41 (3.3%) in which cephalosporins were implicated, the investigators reported. Nineteen of the cases were tied to a single dose of intravenous cefazolin given before surgery. These patients developed cholestatic or mixed hepatocellular-cholestatic injury 1 to 3 weeks after the cefazolin infusion. They almost always had jaundice and pruritus, and usually also had fever and nausea. Signs and symptoms were self-limiting, resolving within a few days to a few weeks.
“Because of confusion about the specific diagnosis, patients underwent substantial diagnostic testing (including multiple computed tomography scans, magnetic resonance imaging scans, endoscopic retrograde cholangiopancreatography exams, liver biopsies, and others), which often were unnecessary, and in some cases led to severe complications,” the investigators said.
“The study also identified barriers to identifying cefazolin as a cause of DILI,” they said. Patients often did not know they had received the antibiotic, and clinicians, including study investigators, often did not know that cefazolin could cause DILI. In more than half of cases, DILI was linked to cefazolin only after careful medical record reviews. “For these reasons, we speculate that cefazolin is and has been underappreciated as a cause of DILI,” the researchers noted. “The appearance of jaundice and pruritus 1 to 3 weeks after minor surgery should lead to a search of surgical records and medications that might have been given during surgery. These results also imply that the merits of routine use of cefazolin at the time of uncomplicated surgery should be reconsidered carefully.”
“Two patients died after receiving cephalosporins other than cefazolin, and another patient developed severe liver injury,” the researchers said. “However, in each of the fatal cases, patients had a complicated clinical course, with a severe hypersensitivity reaction on top of an underlying liver disease. Therefore, we urge caution in concluding that non-cefazolin cephalosporin-induced DILI may be severe or fatal,” they said. “Because cephalosporins are used commonly in clinical practice, it is likely that the overall mortality rate associated with cephalosporin use is low, but not nil, and it may be more likely in patients with underlying disorders.”
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, the National Cancer Institute, and by six Clinical and Translational Science Award grants. The investigators reported having no conflicts of interest.
Pelvic CT may not be needed to diagnose intra-abdominal injury in children
BY JENNIE SMITH
FROM SAEM 2015
| San DIEGO – Children who have suffered blunt trauma are routinely screened in EDs for intra-abdominal injury (IAI) via computed tomography of the abdomen and pelvis. |
Vitals Key clinical point: Abdominal CT scans without a pelvic portion may diagnose intra-abdominal injury in children as well as do full abdominopelvic scans, with less radiation exposure to patients. Major finding: Abdominal CT alone was 85% sensitive (95% CI, 65%-96%) and 99% specific (95% CI, 97%-100%) in identifying IAIs. The four missed injuries were solid organ injuries within the radiographic abdomen. Data source: A retrospective cohort study of 313 patients aged 3 to 17 years presenting to 12 EDs. Disclosures: The study was funded by the Carolinas Trauma Network Research Center of Excellence. None of the investigators disclosed conflicts of interest. |
But concerns about excess exposure to CT radiation, particularly to the gonads, led one group of researchers to question whether it’s necessary to scan the entire abdominopelvic region in all of these patients to identify IAI.
Dr Stacy Reynolds and her colleagues at the Carolinas Medical Center in Charlotte, North Carolina, hypothesized that CT limited to the radiographic abdomen – the region between the dome of the diaphragm to the top of the iliac crest – can capture the vast majority of IAIs in this population.
At the Society for Academic Emergency Medicine annual meeting, Dr Reynolds presented results from a retrospective cohort study enrolling 313 hemodynamically stable pediatric patients (median age 14 years, 64% male) presenting to 12 EDs after blunt trauma. Patients with known pelvic fractures or hip dislocation were excluded, as they would have had a clear indication for a full abdominopelvic CT.
All subjects underwent axial abdominopelvic CT imaging. Researchers created matched pairs of images comprising the original scans and those that had been altered with software that truncated the pelvic portion of the study to create CT abdomen-only studies. Study radiologists were blinded to the results of the original scans.
In all, 26 IAI’s were diagnosed in 24 patients: 8 hepatic injuries, 12 splenic injuries, 5 renal injuries, and 1 retroperitoneal hemorrhage. Abdominal CT alone was 85% sensitive (95% CI, 65%-96%) and 99% specific (95% CI, 97%-100%) in identifying IAIs. The four missed injuries were solid organ injuries within the radiographic abdomen. False positives occurred in two of the complete scans, both involving free fluid prompting suspicion of small bowel injury later ruled out by clinical observation.
Dr Reynolds said in an interview that the findings, while promising, were limited by the study’s small numbers, and its use of axial images alone, when sagittal images also would be required for the most accurate diagnoses. Also, physician suspicion of IAI prior to imaging was not captured because of the study’s retrospective design, she said. “The real key to whether or not this hypothesis is valuable is if physicians are able to target the right population of patients for application.”
Dr Reynolds cautioned that the findings would need to be validated in a larger trial before any changes could be made to clinical practice. “Some of the outcomes that we need to make sure whether we’re missing are still rare,” she said. “You couldn’t feel confident that this is the right way to go with a study this small, but it establishes that we can safely and ethically pursue a multicenter trial that would examine the issue with bigger numbers.”
Other groups of investigators, including members of the Pediatric Emergency Care Applied Research Network (PECARN), also have taken up the question of identifying children at low risk of IAI who may not need CT screening after blunt trauma. In 2013, PECARN published a prediction rule using only patient history and physical examination findings intended to obviate use of CT in the lowest-risk patients (Ann Emerg Med. 2013;62:107-116.e2).
Dr Reynolds said that while overuse of CT was a worrisome trend that could have long-term implications for patients, and that it was important to identify ways it might be limited, there is a reason it remains the go-to technology in the ED for detecting IAI. “It’s got very high sensitivity and specificity. If you’re a busy trauma surgeon who’s admitting 20 injured patients in a night, there’s no faster or more efficient way to determine whether the patient in front of you is injured.”
The ‘sad truth’ about suicide risk assessment scales
BY BRUCE JANCIN
EXPERT ANALYSIS FROM THE ANNUAL AAS CONFERENCE
ATLANTA – “Don’t – repeat, don’t – use risk assessment tools and scales in an effort to predict future suicide in patients who’ve committed intentional self-harm,” Dr Keith Hawton urged at the annual conference of the American Association of Suicidology.
He noted this isn’t simply a matter of his personal opinion; it’s also a strongly worded recommendation in the current UK NICE (National Institute for Health and Care Excellence) guidelines on the long-term management of patients who’ve committed self-harm. The various NICE guidelines, which address numerous areas of medical practice and are used to determine what’s reimbursable through the UK’s National Health Service, are famously evidence based and concerned with cost-effectiveness.
The NICE guidelines on management of self-harm further advise: “Do not use risk assessment tools and scales to determine who should and should not be offered treatment or who should be discharged from hospital.”
“Those are some fairly contentious statements about risk assessment scales. But those statements are based upon review of the evidence about the effectiveness of risk assessment scales,” according to Dr Hawton, professor of psychiatry and director of the Centre for Suicide Research at the University of Oxford (England).
“In our country, hospitals have become obsessed with risk assessment. And usually, it seems to be about protecting the organization rather than the patient, because so often the results aren’t linked to risk management, which is what we should be talking about,” he observed.
Dr Hawton and his colleagues provided some of the evidence that led to the NICE guideline committee’s thumbs-down on the use of suicide risk assessment scales in patients who’ve engaged in intentional self-harm. In a study provocatively titled “The sad truth about the SADPERSONS scale,” he and his coinvestigators essentially dismantled SADPERSONS, a widely used screening tool for suicide risk, concluding that it is without value.
The acronym stands for Sex (male), Age (<19 or >45), Depression, Previous attempts, Ethanol abuse, Rational thinking loss, Social supports lacking, Organized plan, No spouse, and Sickness. One point is given for each. Patients who score 7-10 are to be hospitalized, and those with a total of 5 or 6 points should be strongly considered for hospitalization.
Dr Hawton and coinvestigators tracked 126 consecutive patients who were evaluated for self-harm using the SADPERSONS scale in a general hospital emergency department and then followed them for 6 months. SADPERSONS performed miserably in predicting clinical management outcomes, such as admission to a psychiatric hospital or repetition of self-harm within 6 months. Indeed, the test failed to identify 4 of the 5 patients admitted to a psychiatric hospital, 65 of 70 who were referred from the ED to community psychiatric aftercare, and 28 of 31 who repeated self-harm within 6 months. Thus, its sensitivity as a predictor of repetition of self-harm was a lowly 6.6% (Emerg Med J. 2014;31:796-798).
And yet, a 32-hospital UK national study conducted by Dr Hawton and others found that SADPERSONS was the most widely used scale in EDs for risk assessment following self-harm (BMJ Open. 2014;4(5):e004732. doi:10.1136/bmjopen-2013-004732). “It’s a very crude tool,” Dr Hawton said. “How it found its way into common use in clinical practice is beyond me.”
bjancin@frontlinemedcom.com
Three lab tests predict serious bacterial infections in infants
BY JENNIE SMITH
AT SAEM 2015
SAN DIEGO – A simple three-variable prediction rule can accurately predict which febrile infants younger than age 2 months with fever who present to the ED have serious bacterial infections. Bacterial meningitis, urinary tract infections, and bacteremia are considered serious bacterial infections; many young infants with these infections are difficult to identify, and current laboratory protocols for identifying them include urinalysis, white blood cell counts, band counts, and sometimes cerebrospinal fluid.
Vitals Key clinical point: A rule comprising three lab measurements allows for the prediction of serious bacterial infections in infants under age 2 months presenting to the ED. Major finding: Positive urinalysis, ANC of 4.09 x 1,000/mm3 or higher, and serum procalcitonin of 1.71 ng/mL or greater are between 98% and 99% sensitive in predicting SBIs. Data source: A prospective observational cohort of 1,821 infants at 21 centers forming a pediatric emergency research network. Disclosures: The study was funded by federal government grants. The authors disclosed no conflicts of interest. |
In a presentation at the annual meeting of the Society for Academic Emergency Medicine, Dr Nathan Kuppermann of the University of California, Davis, demonstrated results from a large prospective cohort study of 1,821 febrile infants 60 days old and younger conducted at 21 EDs. Infants with underlying congenital anomalies or critical illness were excluded from the study.
The investigators evaluated 8 variables as potential predictors: age, temperature, Yale Observation Scale score, and clinician suspicion of SBI, along with 4 laboratory variables (urinalysis, white blood cell count, absolute neutrophil count [ANC], and procalcitonin). Band counts were available at some, but not all of the study centers, and therefore were not evaluated.
Dr Kuppermann and his colleagues found that positive urinalysis, ANC of 4.09 x 1,000/mm3 or higher, and serum procalcitonin of 1.71 ng/mL or higher were, taken together, 98% to 99% sensitive and about 60% specific, in predicting SBI in the cohort. Negative predictive values approached 100%. The rate of SBI was 9.3% of the cohort, in keeping with expected rates.
“The SBI positive group was more likely to have higher clinician suspicion of SBI, and all of the lab markers were more elevated in the SBI positive group than the SBI negative group,” Dr Kuppermann said at the meeting. However, after the researchers considered all of the predictors as a group, only the urinalysis, the ANC, and the procalcitonin remained important. Only 3 of 1,821 (0.2%) infants with SBIs were missed when the three-variable prediction tool was used.
To make the prediction rule easier to remember and use, the investigators evaluated lower, more standard, and easier to remember thresholds for the three variables. They reanalyzed their data using a lower cutoff point for ANC of 4.00 x 1,000/mm3, and a lowered procalcitonin cutoff of 0.5 ng/mL. The rule performed almost identically as the original rule, and did not miss any more patients with SBIs beyond the original three.
Dr Kuppermann described the three-variable rule as “simple, objective, and highly accurate” in predicting or ruling out SBI. Nonetheless, it requires external validation in a large cohort, he acknowledged. He said he would continue to routinely perform lumbar punctures in infants younger than 30 days with fever until the findings could be further validated.
“But personally, in that second month of life, I would use these data to decide who actually needs a lumbar puncture and hospitalization,” he said.
Dr Kuppermann also noted as a limitation of the study that the cohort included few infants with bacterial meningitis.
ED revisits twice as frequent as expected
BY MARY ANN MOON
FROM ANNALS OF INTERNAL MEDICINE
The rate of adult revisits to EDs is more than twice as high as has been reported previously – 8% at 3 days and 20% at 30 days – in large part because until now researchers have failed to account for revisits to different hospitals, according to a report published online June 2 in Annals of Internal Medicine.
Vitals Key clinical point: Revisits to the emergency department were twice as frequent as previously reported: 8% at 3 days and 20% at 30 days. Major finding: At 3 days after an initial ED visit, the overall revisit rate was 8.2%, and at 30 days it was 20%, with one-third of these revisits occurring at a medical facility different from that of the initial visit. Data source: A longitudinal, population-based study of adult revisits to the ED after 57,530,239 initial visits in six states during 2006-2010. Disclosures: This study was supported by the US Agency for Healthcare Research and Quality. The researchers’ financial disclosures are available at www.acponline.org. |
Little is known about returns to an emergency department following an index ED visit because most studies have assessed only visits to a single institution or to hospitals within a single state or insurance plan. Now researchers have performed a broader examination of the issue by analyzing newly available multistate longitudinal data from the Healthcare Cost and Utilization Project, which allowed them to identify returns to any ED or acute-care hospital. They focused on acute-care revisits after 57,530,239 initial ED visits by adults in six states (Arizona, California, Florida, Nebraska, Utah, and Hawaii) during 2006-2010.
At 3 days after an initial ED visit, the overall revisit rate was 8.2%, with one-third of these revisits occurring at a medical facility different from that of the initial visit. Previously, estimates of 3-day revisits have ranged from 2.7% to 3.4%. At 30 days, the revisit rate was 20%, and approximately one-third of these revisits involved a different facility. Revisits to different institutions “may have special clinical and financial implications because fragmentation of care increases the likelihood of duplication of services and problems with care transitions,” said Dr Reena Duseja of the department of emergency medicine, University of California, San Francisco, and her associates.
Views on the News Highlighting an underappreciated problem The findings of Duseja et al highlight an underappreciated problem and also raise important questions. To what extent do ED revisits represent gaps in quality as opposed to reasonable strategies that prevent admissions? How often are revisits due to failures of transitional care, suboptimal patient education, or lack of timely follow-up? And why do patients so often seek care at different institutions? Are they dissatisfied with their initial encounter, exercising greater discretion in choosing a facility the second time around, or doing something else? Dr Kumar Dharmarajan and Dr Harlan M. Krumholz are at the Center for Outcomes Research and Evaluation, Yale University, New Haven, Connecticut. Dr Dharmarajan reported receiving grant support from the National Institute on Aging and the American Federation for Aging Research. Dr Krumholz reported receiving grant support from the National Heart, Lung, and Blood Institute and the Center for Cardiovascular Outcomes Research at Yale. The investigators made these remarks in an editorial accompanying Dr Duseja’s report (Ann Intern Med. 2015;162(11):793-794. doi:10.7326/M15-0878). |
“The scope of revisits to outside institutions is much greater than previously suspected, which suggests that improving communication infrastructure across institutions (such as health information exchanges) may improve care and allow individual institutions to get a more accurate picture of their revisit rates,” they noted (Ann Intern Med. 2015;162(11):750-756. doi:10.7326/M14-1616).
Revisit rates varied substantially according to diagnosis. “Skin and subcutaneous tissue infection” accounted for 23% of revisits. “Abdominal pain” was the diagnosis with the next highest revisit rate (10%). The most frequent diagnosis among patients who revisited a different hospital was back pain (2.6%), and nonspecific chest pain was the diagnosis with the
highest rate of later admission to a different hospital (1.1%).
“Financial data from the Florida facilities showed that revisits accounted for more of the total costs of ED care than initial visits did. This demonstrates that revisits are a major, and unaccounted for, component of emergency care costs,” Dr Duseja and her associates said.
Because of insufficient data, they could not determine whether these revisits reflected inadequate access to primary care, patient nonadherence to treatment recommendations, poor quality of care at the initial visit, or other factors, the researchers noted.
Cefazolin ranks sixth as cause of drug-induced liver injury
BY AMY KARON
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
| A single intravenous infusion of cefazolin can cause drug-induced liver injury (DILI), and the antibiotic ranked sixth among pharmacologic causes of hepatic injury in an analysis of 1,212 patients. “Cephalosporins appear to be a relatively common cause of antibiotic-associated liver injury,” said Dr Saleh Alqahtani at the University of Texas Southwestern in Dallas and his associates. “The latency period is typically 1 to 3 weeks after exposure, and patients may not become symptomatic until after the antibiotic is stopped – this is particularly true in the unique clinical syndrome in which a single infusion of cefazolin leads to drug-induced liver injury.” |
Vitals Key clinical point: A single dose of cefazolin can cause drug-induced liver injury (DILI), and the agent is implicated more often than previously thought. Major finding: Cefazolin ranked sixth among causes of DILI, and signs and symptoms began 1 to 3 weeks after initial exposure. Data source: Registry-based study of 1,212 cases of DILI. Disclosures: The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, the National Cancer Institute, and by Clinical and Translational Science Award grants. The investigators reported having no conflicts of interest. |
“Cephalosporins have been reported as rare causes of DILI, but most data come from single case reports,” the researchers said. To study causes of DILI, they analyzed cases from the Drug-Induced Livery Injury Network, an ongoing prospective study at 8 US medical centers. Enrolled patients had strong clinical suspicion for liver injury caused by a drug or an herbal agent. Liver injury was defined based on specific criteria for liver enzymes, alkaline phosphatase (ALP), or total bilirubin levels, or as an international normalized ratio greater than 1.5 that was accompanied by elevated liver enzymes or ALP. Patients were followed for at least 6 months after their baseline visit (Clin Gastroenterol Hepatol. Published January 26, 2015. doi: 10.1016/j.cgh.2015.01.010).
Among the 1,212 cases of DILI in the analysis, one-third were linked to antimicrobial therapies, including 41 (3.3%) in which cephalosporins were implicated, the investigators reported. Nineteen of the cases were tied to a single dose of intravenous cefazolin given before surgery. These patients developed cholestatic or mixed hepatocellular-cholestatic injury 1 to 3 weeks after the cefazolin infusion. They almost always had jaundice and pruritus, and usually also had fever and nausea. Signs and symptoms were self-limiting, resolving within a few days to a few weeks.
“Because of confusion about the specific diagnosis, patients underwent substantial diagnostic testing (including multiple computed tomography scans, magnetic resonance imaging scans, endoscopic retrograde cholangiopancreatography exams, liver biopsies, and others), which often were unnecessary, and in some cases led to severe complications,” the investigators said.
“The study also identified barriers to identifying cefazolin as a cause of DILI,” they said. Patients often did not know they had received the antibiotic, and clinicians, including study investigators, often did not know that cefazolin could cause DILI. In more than half of cases, DILI was linked to cefazolin only after careful medical record reviews. “For these reasons, we speculate that cefazolin is and has been underappreciated as a cause of DILI,” the researchers noted. “The appearance of jaundice and pruritus 1 to 3 weeks after minor surgery should lead to a search of surgical records and medications that might have been given during surgery. These results also imply that the merits of routine use of cefazolin at the time of uncomplicated surgery should be reconsidered carefully.”
“Two patients died after receiving cephalosporins other than cefazolin, and another patient developed severe liver injury,” the researchers said. “However, in each of the fatal cases, patients had a complicated clinical course, with a severe hypersensitivity reaction on top of an underlying liver disease. Therefore, we urge caution in concluding that non-cefazolin cephalosporin-induced DILI may be severe or fatal,” they said. “Because cephalosporins are used commonly in clinical practice, it is likely that the overall mortality rate associated with cephalosporin use is low, but not nil, and it may be more likely in patients with underlying disorders.”
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, the National Cancer Institute, and by six Clinical and Translational Science Award grants. The investigators reported having no conflicts of interest.
Pelvic CT may not be needed to diagnose intra-abdominal injury in children
BY JENNIE SMITH
FROM SAEM 2015
| San DIEGO – Children who have suffered blunt trauma are routinely screened in EDs for intra-abdominal injury (IAI) via computed tomography of the abdomen and pelvis. |
Vitals Key clinical point: Abdominal CT scans without a pelvic portion may diagnose intra-abdominal injury in children as well as do full abdominopelvic scans, with less radiation exposure to patients. Major finding: Abdominal CT alone was 85% sensitive (95% CI, 65%-96%) and 99% specific (95% CI, 97%-100%) in identifying IAIs. The four missed injuries were solid organ injuries within the radiographic abdomen. Data source: A retrospective cohort study of 313 patients aged 3 to 17 years presenting to 12 EDs. Disclosures: The study was funded by the Carolinas Trauma Network Research Center of Excellence. None of the investigators disclosed conflicts of interest. |
But concerns about excess exposure to CT radiation, particularly to the gonads, led one group of researchers to question whether it’s necessary to scan the entire abdominopelvic region in all of these patients to identify IAI.
Dr Stacy Reynolds and her colleagues at the Carolinas Medical Center in Charlotte, North Carolina, hypothesized that CT limited to the radiographic abdomen – the region between the dome of the diaphragm to the top of the iliac crest – can capture the vast majority of IAIs in this population.
At the Society for Academic Emergency Medicine annual meeting, Dr Reynolds presented results from a retrospective cohort study enrolling 313 hemodynamically stable pediatric patients (median age 14 years, 64% male) presenting to 12 EDs after blunt trauma. Patients with known pelvic fractures or hip dislocation were excluded, as they would have had a clear indication for a full abdominopelvic CT.
All subjects underwent axial abdominopelvic CT imaging. Researchers created matched pairs of images comprising the original scans and those that had been altered with software that truncated the pelvic portion of the study to create CT abdomen-only studies. Study radiologists were blinded to the results of the original scans.
In all, 26 IAI’s were diagnosed in 24 patients: 8 hepatic injuries, 12 splenic injuries, 5 renal injuries, and 1 retroperitoneal hemorrhage. Abdominal CT alone was 85% sensitive (95% CI, 65%-96%) and 99% specific (95% CI, 97%-100%) in identifying IAIs. The four missed injuries were solid organ injuries within the radiographic abdomen. False positives occurred in two of the complete scans, both involving free fluid prompting suspicion of small bowel injury later ruled out by clinical observation.
Dr Reynolds said in an interview that the findings, while promising, were limited by the study’s small numbers, and its use of axial images alone, when sagittal images also would be required for the most accurate diagnoses. Also, physician suspicion of IAI prior to imaging was not captured because of the study’s retrospective design, she said. “The real key to whether or not this hypothesis is valuable is if physicians are able to target the right population of patients for application.”
Dr Reynolds cautioned that the findings would need to be validated in a larger trial before any changes could be made to clinical practice. “Some of the outcomes that we need to make sure whether we’re missing are still rare,” she said. “You couldn’t feel confident that this is the right way to go with a study this small, but it establishes that we can safely and ethically pursue a multicenter trial that would examine the issue with bigger numbers.”
Other groups of investigators, including members of the Pediatric Emergency Care Applied Research Network (PECARN), also have taken up the question of identifying children at low risk of IAI who may not need CT screening after blunt trauma. In 2013, PECARN published a prediction rule using only patient history and physical examination findings intended to obviate use of CT in the lowest-risk patients (Ann Emerg Med. 2013;62:107-116.e2).
Dr Reynolds said that while overuse of CT was a worrisome trend that could have long-term implications for patients, and that it was important to identify ways it might be limited, there is a reason it remains the go-to technology in the ED for detecting IAI. “It’s got very high sensitivity and specificity. If you’re a busy trauma surgeon who’s admitting 20 injured patients in a night, there’s no faster or more efficient way to determine whether the patient in front of you is injured.”
The ‘sad truth’ about suicide risk assessment scales
BY BRUCE JANCIN
EXPERT ANALYSIS FROM THE ANNUAL AAS CONFERENCE
ATLANTA – “Don’t – repeat, don’t – use risk assessment tools and scales in an effort to predict future suicide in patients who’ve committed intentional self-harm,” Dr Keith Hawton urged at the annual conference of the American Association of Suicidology.
He noted this isn’t simply a matter of his personal opinion; it’s also a strongly worded recommendation in the current UK NICE (National Institute for Health and Care Excellence) guidelines on the long-term management of patients who’ve committed self-harm. The various NICE guidelines, which address numerous areas of medical practice and are used to determine what’s reimbursable through the UK’s National Health Service, are famously evidence based and concerned with cost-effectiveness.
The NICE guidelines on management of self-harm further advise: “Do not use risk assessment tools and scales to determine who should and should not be offered treatment or who should be discharged from hospital.”
“Those are some fairly contentious statements about risk assessment scales. But those statements are based upon review of the evidence about the effectiveness of risk assessment scales,” according to Dr Hawton, professor of psychiatry and director of the Centre for Suicide Research at the University of Oxford (England).
“In our country, hospitals have become obsessed with risk assessment. And usually, it seems to be about protecting the organization rather than the patient, because so often the results aren’t linked to risk management, which is what we should be talking about,” he observed.
Dr Hawton and his colleagues provided some of the evidence that led to the NICE guideline committee’s thumbs-down on the use of suicide risk assessment scales in patients who’ve engaged in intentional self-harm. In a study provocatively titled “The sad truth about the SADPERSONS scale,” he and his coinvestigators essentially dismantled SADPERSONS, a widely used screening tool for suicide risk, concluding that it is without value.
The acronym stands for Sex (male), Age (<19 or >45), Depression, Previous attempts, Ethanol abuse, Rational thinking loss, Social supports lacking, Organized plan, No spouse, and Sickness. One point is given for each. Patients who score 7-10 are to be hospitalized, and those with a total of 5 or 6 points should be strongly considered for hospitalization.
Dr Hawton and coinvestigators tracked 126 consecutive patients who were evaluated for self-harm using the SADPERSONS scale in a general hospital emergency department and then followed them for 6 months. SADPERSONS performed miserably in predicting clinical management outcomes, such as admission to a psychiatric hospital or repetition of self-harm within 6 months. Indeed, the test failed to identify 4 of the 5 patients admitted to a psychiatric hospital, 65 of 70 who were referred from the ED to community psychiatric aftercare, and 28 of 31 who repeated self-harm within 6 months. Thus, its sensitivity as a predictor of repetition of self-harm was a lowly 6.6% (Emerg Med J. 2014;31:796-798).
And yet, a 32-hospital UK national study conducted by Dr Hawton and others found that SADPERSONS was the most widely used scale in EDs for risk assessment following self-harm (BMJ Open. 2014;4(5):e004732. doi:10.1136/bmjopen-2013-004732). “It’s a very crude tool,” Dr Hawton said. “How it found its way into common use in clinical practice is beyond me.”
bjancin@frontlinemedcom.com
