User login
Reimagining Inpatient Care in Canadian Teaching Hospitals: Bold Initiatives or Tinkering at the Margins?
Canada’s 17 medical schools and their affiliated teaching hospitals are instrumental in serving local communities and providing regional and national access to specialized therapies. Akin to many other countries, patients in Canadian teaching hospitals typically receive care from trainees supervised by attending physicians on teams that Canadians refer to as clinical teaching units (CTUs).1 For more than 50 years, the CTU model has served trainees, attendings, and patients well.2 The success of the CTU model has been dependent on several factors including the crucial balance between the number of trainees and volume of patients. However, Canadian teaching hospitals are increasingly challenged by an imbalance in the trainee-to-patient volume equilibrium spurred by increasing patient volumes and declining house staff availability. The challenges we are facing today in Canada are similar to those teaching hospitals in the United States have faced and adapted to over the last 15 years. Can we build a new, sustainable model of inpatient care through attending-directed inpatient services much as has happened in the US?
Canada’s population of 36 million people is growing by approximately 1% per year, largely driven by immigration.3 At the same time, Canada’s population is aging and becoming increasingly medically complex; the percentage of Canadians age 65 years and older is anticipated to rise from approximately 17% today to 25% in 2035.4 Canada’s healthcare system historically functioned with relatively few inpatient beds, encouraging efficiency particularly with respect to which patients require hospital admission and which do not.5 Although data suggest that the number of hospital admissions declined in Canada between 1980 and 1995, recent data documented that General Internal Medicine admissions increased by 32% between 2010 and 2015 and accounted for 24% of total hospital bed days.6,7 The effects of population growth and aging on admission volumes might be mitigated to some extent by innovations in healthcare delivery such as improved access to primary care (largely family physicians in Canada). However, even with these innovations, a growing and aging population is likely to have a disproportionate effect on the types of undifferentiated illnesses that are typically admitted to General Internal Medicine in Canadian teaching hospitals.
Increasing volumes and complexity are occurring at the same time that residency training in Canada is undergoing an extraordinary shift, mirroring trends in other countries.8 CTUs in Canada typically have a census of 20 or more patients and are staffed by an attending, one senior resident, two to three junior residents, and medical students. Recognition that physician fatigue is associated with patient safety events and physician burnout has led to shorter resident shifts, though Canadian hospitals typically operate without concrete work hour limits or “hard” caps on team size.8 To fulfill accreditation standards set by the Royal College of Physicians and Surgeons of Canada, residency programs have required increases in formal teaching sessions during working hours, further reducing resident presence at the bedside. Many specialty training programs (eg, anesthesiology and ophthalmology) that traditionally required trainees to rotate through General Medicine have eliminated this requirement. Moreover, postgraduate training now requires additional time be spent in ambulatory and community hospital settings to better prepare residents for practice.9 There is little enthusiasm for increasing the number of residents, as postgraduate training spots increased by 85% between 2000 and 2013, before stabilizing in recent years.10
These factors are leading to a substantial decline in resident availability on CTUs, shifting increasing amounts of direct patient care to attending physicians in Canadian teaching hospitals across virtually all specialties. Unsurprisingly, increased rates of burnout and decreases in job satisfactio
Canadian teaching hospitals currently find themselves facing a confluence of factors nearly identical to those faced by teaching hospitals in the United States during 2003 when the Accreditation Council for Graduate Medical Education instituted resident duty hour restrictions to address concerns over trainee wellness, shift length, and patient safety.8 Instantly, hundreds of US teaching hospitals faced uncertainty over who would provide patient care when residents were unavailable. Virtually all US teaching hospitals responded with a creativity and speed that we are unaccustomed to in academic medicine. Hospitals reallocated money to finance attending-directed services where patient care was provided directly by attending physicians often working without trainees12 but frequently supported by nurse practitioners or physician assistants.13 Despite the differences between US and Canadian healthcare, 15 years later, we in Canada can and should learn from the US experience.14
Attending-directed services offer several advantages. First, attending-directed services offer patient outcomes including ICU transfer, mortality, readmissions, and satisfaction that are similar, if not modestly improved, when compared with traditional teaching services.15 Results also suggest potential reductions in hospital length of stay and diagnostic testing.16 Attending-directed services can enhance trainee education by insuring attending physician presence and oversight in-hospital 24-hours per day.17 Although not well studied, attending-directed services may reduce variation in CTU patient census so that excess volumes can be absorbed by attending-directed teams even with seasonal surges (eg, influenza). Recognizing that many specialties were experiencing the same challenges as General Medicine in 2003, attending-directed services in the US have been designed to care for a wide spectrum of patients drawn from an array of different specialties with evidence of improved outcomes.12 Building attending-directed services in Canadian teaching hospitals may expand to include patients from multiple specialties and subspecialties (surgery, orthopedics, and cardiology) where patient volumes are increasing and resident coverage is increasingly scarce.
The challenges that accompany the implementation of attending-directed teams must be acknowledged. First, while attending-directed teams solve many problems for teaching hospitals, physician billings may not generate sufficient income to be self-sustaining and require additional financial support.18 Without investment from hospitals or government, attending-directed models cannot flourish in teaching hospitals. US hospitals typically provide substantial financial support ($50,000-$100,000 per physician) to hospitalist programs, but Canadian teaching hospitals have been reluctant to follow suit.
Second, attending-directed services require a sustainable workforce. In Canada, inpatient care is provided predominately by family physician hospitalists in community hospitals, whereas internists typically fulfill these roles in teaching hospitals.19 Family physician hospitalists are commonly represented by the Canadian Society for Hospital Medicine, which is the Canadian branch of the Society of Hospital Medicine. Hospital medicine in Canada is typically organized around physician training (family physician vs internist) rather than clinical focus (outpatient vs inpatient). Collaborative models of care that unite hospitalists from all training streams (family physician, internist, and pediatrics) are only just emerging in Canadian teaching hospitals. How these programs are developed will be critical to the successful growth of attending-directed services. Third, if attending-directed services expand in teaching hospitals, the physicians who staff these services must come from somewhere. Either the “production” of physicians will need to increase or physicians will migrate to attending-directed services from outpatient practice or from community hospitals.20 Canadian teaching hospitals can also explore nurse practitioners and physician assistants, a previously underutilized resource. Though the costs of such programs can be significant,21 the payoff in safety, quality, and efficiency may be worth it—as demonstrated in the US system. Fourth, teaching hospitals and medical schools must create academic homes to support and mentor the physicians working on attending-directed services. Although physicians hired for attending-directed services primarily provide direct patient care, few will join academic medical centers solely for this purpose. Teaching hospitals and medical schools need to carefully consider job descriptions, mentoring, and career advancement opportunities as they build attending-directed services. Finally, the interactions between teaching and attending-directed services are complex. There is an inevitable learning curve as clinical operations and protocols are built and developed. For example, decisions need to be made about how patients are divided between services and whether nocturnists are responsible for teaching overnight residents.17 Successful programs have the potential to benefit hospitals, patients, learners, and faculty alike.
The risks associated with the status quo in Canada must also be addressed. Patient volumes and complexity in Canada are likely to continue to slowly increase, while the number of trainees in Canadian teaching hospitals will remain stable at best. Forcing more patients onto already overtaxed teaching services is likely to worsen hospital efficiency, patient outcomes, and educational experiences.22 Forcing additional patient care onto overstretched faculty will slowly erode the academic work (teaching and research) that has characterized excellence in Canadian medicine.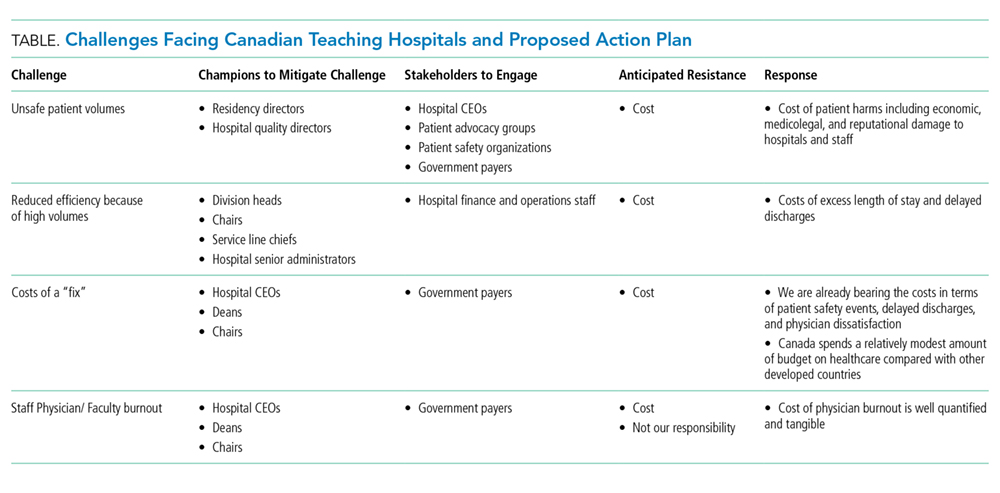
The changes we propose to overcome the challenges facing Canadian teaching hospitals are neither cheap nor easy (Table). We expect resistance on many fronts. Implementing them will likely require concerted advocacy from a diverse group of champions shining a bright spotlight on the sizable challenges Canadian teaching hospitals are confronting. We believe that each challenge maps to a discrete group of champions with discrete targets within hospital leadership, medical school administration, and government who will need to be engaged. In our opinion, organizing around these challenges offers the best opportunity to overcome the perpetual resistance around costs. Canadian teaching hospitals and their CTUs are under unprecedented pressure. Do we act boldly and embrace attending-directed models of care or continue tinkering at the margins?
Acknowledgments
The authors thank Chaim Bell for his advice and suggestions.
Disclosures
The authors have nothing to disclose.
1. Schrewe B, Pratt DD, McKellin WH. Adapting the forms of yesterday to the functions of today and the needs of tomorrow: a genealogical case study of clinical teaching units in Canada. Adv Health Sci Educ Theory Pract. 2016;21(2):475-499. PubMed
2. Maudsley RF. The clinical teaching unit in transition. CMAJ. 1993;148(9):1564-1566. PubMed
3. Statistics Canada. Recent Changes in Demographic Trends in Canada. Ottawa: Ontario, 2015. https://www150.statcan.gc.ca/n1/pub/75-006-x/2015001/article/14240-eng.htm. Accessed December 9, 2018
4. Statistics Canada. Census, Age and Sex. Ottawa: Ontario, 2016. https://www12.statcan.gc.ca/census-recensement/2016/rt-td/as-eng.cfm. Accessed December 10, 2018.
5. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA. 2018;319(10):1024-1039. PubMed
6. van Walraven C. Trends in 1-year survival of people admitted to hospital in Ontario, 1994-2009. CMAJ. 2013;185(16):E755-E762. PubMed
7. Verma AA, Guo Y, Kwan JL, et al. Patient characteristics, resource use and outcomes associated with general internal medicine hospital care: the General Medicine Inpatient Initiative (GEMINI) retrospective cohort study. CMAJ Open. 2017;5(4):E842-E849. PubMed
8. Pattani R, Wu PE, Dhalla IA. Resident duty hours in Canada: past, present and future. CMAJ. 2014;186(10):761-765. PubMed
9. Royal College of Physicians and Surgeons. Specialty Training Requirements in Internal medicine 2015. http://www.royalcollege.ca/cs/groups/public/documents/document/mdaw/mdg4/~edisp/088402.pdf. Accessed December 12, 2018.
10. Freeman TR, Petterson S, Finnegan S, Bazemore A. Shifting tides in the emigration patterns of Canadian physicians to the United States: a cross-sectional secondary data analysis. BMC Health Serv Res. 2016;16(1):678. PubMed
11. Wong BM, Imrie K. Why resident duty hours regulations must address attending physicians’ workload. Acad Med. 2013;88(9):1209-1211. PubMed
12. Flanders SA, Centor B, Weber V, McGinn T, DeSalvo K, Auerbach A. Challenges and opportunities in academic hospital medicine: report from the Academic Hospital Medicine Summit. J Hosp Med. 2009;4(4):240-246. PubMed
13. Torok H, Lackner C, Landis R, Wright S. Learning needs of physician assistants working in hospital medicine. J Hosp Med. 2012;7(3):190-194. PubMed
14. Ivers N, Brown AD, Detsky AS. Lessons from the Canadian experience with single-payer health insurance: just comfortable enough with the status quo. JAMA Intern Med. 2018;178(9):1250-1255. PubMed
15. Wray CM, Flores A, Padula WV, Prochaska MT, Meltzer DO, Arora VM. Measuring patient experiences on hospitalist and teaching services: patient responses to a 30-day postdischarge questionnaire. J Hosp Med. 2016;11(2):99-104. PubMed
16. Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859-865. PubMed
17. Farnan JM, Burger A, Boonyasai RT, et al. Survey of overnight academic hospitalist supervision of trainees. J Hosp Med. 2012;7(7):521-523. PubMed
18. Gonzalo JD, Kuperman EF, Chuang CH, Lehman E, Glasser F, Abendroth T. Impact of an overnight internal medicine academic hospitalist program on patient outcomes. J Gen Intern Med. 2015;30(12):1795-1802. PubMed
19. Soong C, Fan E, Howell EE, et al. Characteristics of Hospitalists and Hospitalist Programs in the United States and Canada 2009. J Clin Outcomes Meas. 2009; 16 (2): 69-74.
20. Yousefi V, Maslowski R. Health system drivers of hospital medicine in Canada: systematic review. Can Fam Phys Med Fam Can. 2013;59(7):762-767. PubMed
21. Nuckols TK, Escarce JJ. Cost implications of ACGME’s 2011 changes to resident duty hours and the training environment. J Gen Intern Med. 2012;27(2):241-249. PubMed
22. Elliott DJ, Young RS, Brice J, Aguiar R, Kolm P. Effect of hospitalist workload on the quality and efficiency of care. JAMA Intern Med. 2014;174(5):786-793. PubMed
Canada’s 17 medical schools and their affiliated teaching hospitals are instrumental in serving local communities and providing regional and national access to specialized therapies. Akin to many other countries, patients in Canadian teaching hospitals typically receive care from trainees supervised by attending physicians on teams that Canadians refer to as clinical teaching units (CTUs).1 For more than 50 years, the CTU model has served trainees, attendings, and patients well.2 The success of the CTU model has been dependent on several factors including the crucial balance between the number of trainees and volume of patients. However, Canadian teaching hospitals are increasingly challenged by an imbalance in the trainee-to-patient volume equilibrium spurred by increasing patient volumes and declining house staff availability. The challenges we are facing today in Canada are similar to those teaching hospitals in the United States have faced and adapted to over the last 15 years. Can we build a new, sustainable model of inpatient care through attending-directed inpatient services much as has happened in the US?
Canada’s population of 36 million people is growing by approximately 1% per year, largely driven by immigration.3 At the same time, Canada’s population is aging and becoming increasingly medically complex; the percentage of Canadians age 65 years and older is anticipated to rise from approximately 17% today to 25% in 2035.4 Canada’s healthcare system historically functioned with relatively few inpatient beds, encouraging efficiency particularly with respect to which patients require hospital admission and which do not.5 Although data suggest that the number of hospital admissions declined in Canada between 1980 and 1995, recent data documented that General Internal Medicine admissions increased by 32% between 2010 and 2015 and accounted for 24% of total hospital bed days.6,7 The effects of population growth and aging on admission volumes might be mitigated to some extent by innovations in healthcare delivery such as improved access to primary care (largely family physicians in Canada). However, even with these innovations, a growing and aging population is likely to have a disproportionate effect on the types of undifferentiated illnesses that are typically admitted to General Internal Medicine in Canadian teaching hospitals.
Increasing volumes and complexity are occurring at the same time that residency training in Canada is undergoing an extraordinary shift, mirroring trends in other countries.8 CTUs in Canada typically have a census of 20 or more patients and are staffed by an attending, one senior resident, two to three junior residents, and medical students. Recognition that physician fatigue is associated with patient safety events and physician burnout has led to shorter resident shifts, though Canadian hospitals typically operate without concrete work hour limits or “hard” caps on team size.8 To fulfill accreditation standards set by the Royal College of Physicians and Surgeons of Canada, residency programs have required increases in formal teaching sessions during working hours, further reducing resident presence at the bedside. Many specialty training programs (eg, anesthesiology and ophthalmology) that traditionally required trainees to rotate through General Medicine have eliminated this requirement. Moreover, postgraduate training now requires additional time be spent in ambulatory and community hospital settings to better prepare residents for practice.9 There is little enthusiasm for increasing the number of residents, as postgraduate training spots increased by 85% between 2000 and 2013, before stabilizing in recent years.10
These factors are leading to a substantial decline in resident availability on CTUs, shifting increasing amounts of direct patient care to attending physicians in Canadian teaching hospitals across virtually all specialties. Unsurprisingly, increased rates of burnout and decreases in job satisfactio
Canadian teaching hospitals currently find themselves facing a confluence of factors nearly identical to those faced by teaching hospitals in the United States during 2003 when the Accreditation Council for Graduate Medical Education instituted resident duty hour restrictions to address concerns over trainee wellness, shift length, and patient safety.8 Instantly, hundreds of US teaching hospitals faced uncertainty over who would provide patient care when residents were unavailable. Virtually all US teaching hospitals responded with a creativity and speed that we are unaccustomed to in academic medicine. Hospitals reallocated money to finance attending-directed services where patient care was provided directly by attending physicians often working without trainees12 but frequently supported by nurse practitioners or physician assistants.13 Despite the differences between US and Canadian healthcare, 15 years later, we in Canada can and should learn from the US experience.14
Attending-directed services offer several advantages. First, attending-directed services offer patient outcomes including ICU transfer, mortality, readmissions, and satisfaction that are similar, if not modestly improved, when compared with traditional teaching services.15 Results also suggest potential reductions in hospital length of stay and diagnostic testing.16 Attending-directed services can enhance trainee education by insuring attending physician presence and oversight in-hospital 24-hours per day.17 Although not well studied, attending-directed services may reduce variation in CTU patient census so that excess volumes can be absorbed by attending-directed teams even with seasonal surges (eg, influenza). Recognizing that many specialties were experiencing the same challenges as General Medicine in 2003, attending-directed services in the US have been designed to care for a wide spectrum of patients drawn from an array of different specialties with evidence of improved outcomes.12 Building attending-directed services in Canadian teaching hospitals may expand to include patients from multiple specialties and subspecialties (surgery, orthopedics, and cardiology) where patient volumes are increasing and resident coverage is increasingly scarce.
The challenges that accompany the implementation of attending-directed teams must be acknowledged. First, while attending-directed teams solve many problems for teaching hospitals, physician billings may not generate sufficient income to be self-sustaining and require additional financial support.18 Without investment from hospitals or government, attending-directed models cannot flourish in teaching hospitals. US hospitals typically provide substantial financial support ($50,000-$100,000 per physician) to hospitalist programs, but Canadian teaching hospitals have been reluctant to follow suit.
Second, attending-directed services require a sustainable workforce. In Canada, inpatient care is provided predominately by family physician hospitalists in community hospitals, whereas internists typically fulfill these roles in teaching hospitals.19 Family physician hospitalists are commonly represented by the Canadian Society for Hospital Medicine, which is the Canadian branch of the Society of Hospital Medicine. Hospital medicine in Canada is typically organized around physician training (family physician vs internist) rather than clinical focus (outpatient vs inpatient). Collaborative models of care that unite hospitalists from all training streams (family physician, internist, and pediatrics) are only just emerging in Canadian teaching hospitals. How these programs are developed will be critical to the successful growth of attending-directed services. Third, if attending-directed services expand in teaching hospitals, the physicians who staff these services must come from somewhere. Either the “production” of physicians will need to increase or physicians will migrate to attending-directed services from outpatient practice or from community hospitals.20 Canadian teaching hospitals can also explore nurse practitioners and physician assistants, a previously underutilized resource. Though the costs of such programs can be significant,21 the payoff in safety, quality, and efficiency may be worth it—as demonstrated in the US system. Fourth, teaching hospitals and medical schools must create academic homes to support and mentor the physicians working on attending-directed services. Although physicians hired for attending-directed services primarily provide direct patient care, few will join academic medical centers solely for this purpose. Teaching hospitals and medical schools need to carefully consider job descriptions, mentoring, and career advancement opportunities as they build attending-directed services. Finally, the interactions between teaching and attending-directed services are complex. There is an inevitable learning curve as clinical operations and protocols are built and developed. For example, decisions need to be made about how patients are divided between services and whether nocturnists are responsible for teaching overnight residents.17 Successful programs have the potential to benefit hospitals, patients, learners, and faculty alike.
The risks associated with the status quo in Canada must also be addressed. Patient volumes and complexity in Canada are likely to continue to slowly increase, while the number of trainees in Canadian teaching hospitals will remain stable at best. Forcing more patients onto already overtaxed teaching services is likely to worsen hospital efficiency, patient outcomes, and educational experiences.22 Forcing additional patient care onto overstretched faculty will slowly erode the academic work (teaching and research) that has characterized excellence in Canadian medicine.
The changes we propose to overcome the challenges facing Canadian teaching hospitals are neither cheap nor easy (Table). We expect resistance on many fronts. Implementing them will likely require concerted advocacy from a diverse group of champions shining a bright spotlight on the sizable challenges Canadian teaching hospitals are confronting. We believe that each challenge maps to a discrete group of champions with discrete targets within hospital leadership, medical school administration, and government who will need to be engaged. In our opinion, organizing around these challenges offers the best opportunity to overcome the perpetual resistance around costs. Canadian teaching hospitals and their CTUs are under unprecedented pressure. Do we act boldly and embrace attending-directed models of care or continue tinkering at the margins?
Acknowledgments
The authors thank Chaim Bell for his advice and suggestions.
Disclosures
The authors have nothing to disclose.
Canada’s 17 medical schools and their affiliated teaching hospitals are instrumental in serving local communities and providing regional and national access to specialized therapies. Akin to many other countries, patients in Canadian teaching hospitals typically receive care from trainees supervised by attending physicians on teams that Canadians refer to as clinical teaching units (CTUs).1 For more than 50 years, the CTU model has served trainees, attendings, and patients well.2 The success of the CTU model has been dependent on several factors including the crucial balance between the number of trainees and volume of patients. However, Canadian teaching hospitals are increasingly challenged by an imbalance in the trainee-to-patient volume equilibrium spurred by increasing patient volumes and declining house staff availability. The challenges we are facing today in Canada are similar to those teaching hospitals in the United States have faced and adapted to over the last 15 years. Can we build a new, sustainable model of inpatient care through attending-directed inpatient services much as has happened in the US?
Canada’s population of 36 million people is growing by approximately 1% per year, largely driven by immigration.3 At the same time, Canada’s population is aging and becoming increasingly medically complex; the percentage of Canadians age 65 years and older is anticipated to rise from approximately 17% today to 25% in 2035.4 Canada’s healthcare system historically functioned with relatively few inpatient beds, encouraging efficiency particularly with respect to which patients require hospital admission and which do not.5 Although data suggest that the number of hospital admissions declined in Canada between 1980 and 1995, recent data documented that General Internal Medicine admissions increased by 32% between 2010 and 2015 and accounted for 24% of total hospital bed days.6,7 The effects of population growth and aging on admission volumes might be mitigated to some extent by innovations in healthcare delivery such as improved access to primary care (largely family physicians in Canada). However, even with these innovations, a growing and aging population is likely to have a disproportionate effect on the types of undifferentiated illnesses that are typically admitted to General Internal Medicine in Canadian teaching hospitals.
Increasing volumes and complexity are occurring at the same time that residency training in Canada is undergoing an extraordinary shift, mirroring trends in other countries.8 CTUs in Canada typically have a census of 20 or more patients and are staffed by an attending, one senior resident, two to three junior residents, and medical students. Recognition that physician fatigue is associated with patient safety events and physician burnout has led to shorter resident shifts, though Canadian hospitals typically operate without concrete work hour limits or “hard” caps on team size.8 To fulfill accreditation standards set by the Royal College of Physicians and Surgeons of Canada, residency programs have required increases in formal teaching sessions during working hours, further reducing resident presence at the bedside. Many specialty training programs (eg, anesthesiology and ophthalmology) that traditionally required trainees to rotate through General Medicine have eliminated this requirement. Moreover, postgraduate training now requires additional time be spent in ambulatory and community hospital settings to better prepare residents for practice.9 There is little enthusiasm for increasing the number of residents, as postgraduate training spots increased by 85% between 2000 and 2013, before stabilizing in recent years.10
These factors are leading to a substantial decline in resident availability on CTUs, shifting increasing amounts of direct patient care to attending physicians in Canadian teaching hospitals across virtually all specialties. Unsurprisingly, increased rates of burnout and decreases in job satisfactio
Canadian teaching hospitals currently find themselves facing a confluence of factors nearly identical to those faced by teaching hospitals in the United States during 2003 when the Accreditation Council for Graduate Medical Education instituted resident duty hour restrictions to address concerns over trainee wellness, shift length, and patient safety.8 Instantly, hundreds of US teaching hospitals faced uncertainty over who would provide patient care when residents were unavailable. Virtually all US teaching hospitals responded with a creativity and speed that we are unaccustomed to in academic medicine. Hospitals reallocated money to finance attending-directed services where patient care was provided directly by attending physicians often working without trainees12 but frequently supported by nurse practitioners or physician assistants.13 Despite the differences between US and Canadian healthcare, 15 years later, we in Canada can and should learn from the US experience.14
Attending-directed services offer several advantages. First, attending-directed services offer patient outcomes including ICU transfer, mortality, readmissions, and satisfaction that are similar, if not modestly improved, when compared with traditional teaching services.15 Results also suggest potential reductions in hospital length of stay and diagnostic testing.16 Attending-directed services can enhance trainee education by insuring attending physician presence and oversight in-hospital 24-hours per day.17 Although not well studied, attending-directed services may reduce variation in CTU patient census so that excess volumes can be absorbed by attending-directed teams even with seasonal surges (eg, influenza). Recognizing that many specialties were experiencing the same challenges as General Medicine in 2003, attending-directed services in the US have been designed to care for a wide spectrum of patients drawn from an array of different specialties with evidence of improved outcomes.12 Building attending-directed services in Canadian teaching hospitals may expand to include patients from multiple specialties and subspecialties (surgery, orthopedics, and cardiology) where patient volumes are increasing and resident coverage is increasingly scarce.
The challenges that accompany the implementation of attending-directed teams must be acknowledged. First, while attending-directed teams solve many problems for teaching hospitals, physician billings may not generate sufficient income to be self-sustaining and require additional financial support.18 Without investment from hospitals or government, attending-directed models cannot flourish in teaching hospitals. US hospitals typically provide substantial financial support ($50,000-$100,000 per physician) to hospitalist programs, but Canadian teaching hospitals have been reluctant to follow suit.
Second, attending-directed services require a sustainable workforce. In Canada, inpatient care is provided predominately by family physician hospitalists in community hospitals, whereas internists typically fulfill these roles in teaching hospitals.19 Family physician hospitalists are commonly represented by the Canadian Society for Hospital Medicine, which is the Canadian branch of the Society of Hospital Medicine. Hospital medicine in Canada is typically organized around physician training (family physician vs internist) rather than clinical focus (outpatient vs inpatient). Collaborative models of care that unite hospitalists from all training streams (family physician, internist, and pediatrics) are only just emerging in Canadian teaching hospitals. How these programs are developed will be critical to the successful growth of attending-directed services. Third, if attending-directed services expand in teaching hospitals, the physicians who staff these services must come from somewhere. Either the “production” of physicians will need to increase or physicians will migrate to attending-directed services from outpatient practice or from community hospitals.20 Canadian teaching hospitals can also explore nurse practitioners and physician assistants, a previously underutilized resource. Though the costs of such programs can be significant,21 the payoff in safety, quality, and efficiency may be worth it—as demonstrated in the US system. Fourth, teaching hospitals and medical schools must create academic homes to support and mentor the physicians working on attending-directed services. Although physicians hired for attending-directed services primarily provide direct patient care, few will join academic medical centers solely for this purpose. Teaching hospitals and medical schools need to carefully consider job descriptions, mentoring, and career advancement opportunities as they build attending-directed services. Finally, the interactions between teaching and attending-directed services are complex. There is an inevitable learning curve as clinical operations and protocols are built and developed. For example, decisions need to be made about how patients are divided between services and whether nocturnists are responsible for teaching overnight residents.17 Successful programs have the potential to benefit hospitals, patients, learners, and faculty alike.
The risks associated with the status quo in Canada must also be addressed. Patient volumes and complexity in Canada are likely to continue to slowly increase, while the number of trainees in Canadian teaching hospitals will remain stable at best. Forcing more patients onto already overtaxed teaching services is likely to worsen hospital efficiency, patient outcomes, and educational experiences.22 Forcing additional patient care onto overstretched faculty will slowly erode the academic work (teaching and research) that has characterized excellence in Canadian medicine.
The changes we propose to overcome the challenges facing Canadian teaching hospitals are neither cheap nor easy (Table). We expect resistance on many fronts. Implementing them will likely require concerted advocacy from a diverse group of champions shining a bright spotlight on the sizable challenges Canadian teaching hospitals are confronting. We believe that each challenge maps to a discrete group of champions with discrete targets within hospital leadership, medical school administration, and government who will need to be engaged. In our opinion, organizing around these challenges offers the best opportunity to overcome the perpetual resistance around costs. Canadian teaching hospitals and their CTUs are under unprecedented pressure. Do we act boldly and embrace attending-directed models of care or continue tinkering at the margins?
Acknowledgments
The authors thank Chaim Bell for his advice and suggestions.
Disclosures
The authors have nothing to disclose.
1. Schrewe B, Pratt DD, McKellin WH. Adapting the forms of yesterday to the functions of today and the needs of tomorrow: a genealogical case study of clinical teaching units in Canada. Adv Health Sci Educ Theory Pract. 2016;21(2):475-499. PubMed
2. Maudsley RF. The clinical teaching unit in transition. CMAJ. 1993;148(9):1564-1566. PubMed
3. Statistics Canada. Recent Changes in Demographic Trends in Canada. Ottawa: Ontario, 2015. https://www150.statcan.gc.ca/n1/pub/75-006-x/2015001/article/14240-eng.htm. Accessed December 9, 2018
4. Statistics Canada. Census, Age and Sex. Ottawa: Ontario, 2016. https://www12.statcan.gc.ca/census-recensement/2016/rt-td/as-eng.cfm. Accessed December 10, 2018.
5. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA. 2018;319(10):1024-1039. PubMed
6. van Walraven C. Trends in 1-year survival of people admitted to hospital in Ontario, 1994-2009. CMAJ. 2013;185(16):E755-E762. PubMed
7. Verma AA, Guo Y, Kwan JL, et al. Patient characteristics, resource use and outcomes associated with general internal medicine hospital care: the General Medicine Inpatient Initiative (GEMINI) retrospective cohort study. CMAJ Open. 2017;5(4):E842-E849. PubMed
8. Pattani R, Wu PE, Dhalla IA. Resident duty hours in Canada: past, present and future. CMAJ. 2014;186(10):761-765. PubMed
9. Royal College of Physicians and Surgeons. Specialty Training Requirements in Internal medicine 2015. http://www.royalcollege.ca/cs/groups/public/documents/document/mdaw/mdg4/~edisp/088402.pdf. Accessed December 12, 2018.
10. Freeman TR, Petterson S, Finnegan S, Bazemore A. Shifting tides in the emigration patterns of Canadian physicians to the United States: a cross-sectional secondary data analysis. BMC Health Serv Res. 2016;16(1):678. PubMed
11. Wong BM, Imrie K. Why resident duty hours regulations must address attending physicians’ workload. Acad Med. 2013;88(9):1209-1211. PubMed
12. Flanders SA, Centor B, Weber V, McGinn T, DeSalvo K, Auerbach A. Challenges and opportunities in academic hospital medicine: report from the Academic Hospital Medicine Summit. J Hosp Med. 2009;4(4):240-246. PubMed
13. Torok H, Lackner C, Landis R, Wright S. Learning needs of physician assistants working in hospital medicine. J Hosp Med. 2012;7(3):190-194. PubMed
14. Ivers N, Brown AD, Detsky AS. Lessons from the Canadian experience with single-payer health insurance: just comfortable enough with the status quo. JAMA Intern Med. 2018;178(9):1250-1255. PubMed
15. Wray CM, Flores A, Padula WV, Prochaska MT, Meltzer DO, Arora VM. Measuring patient experiences on hospitalist and teaching services: patient responses to a 30-day postdischarge questionnaire. J Hosp Med. 2016;11(2):99-104. PubMed
16. Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859-865. PubMed
17. Farnan JM, Burger A, Boonyasai RT, et al. Survey of overnight academic hospitalist supervision of trainees. J Hosp Med. 2012;7(7):521-523. PubMed
18. Gonzalo JD, Kuperman EF, Chuang CH, Lehman E, Glasser F, Abendroth T. Impact of an overnight internal medicine academic hospitalist program on patient outcomes. J Gen Intern Med. 2015;30(12):1795-1802. PubMed
19. Soong C, Fan E, Howell EE, et al. Characteristics of Hospitalists and Hospitalist Programs in the United States and Canada 2009. J Clin Outcomes Meas. 2009; 16 (2): 69-74.
20. Yousefi V, Maslowski R. Health system drivers of hospital medicine in Canada: systematic review. Can Fam Phys Med Fam Can. 2013;59(7):762-767. PubMed
21. Nuckols TK, Escarce JJ. Cost implications of ACGME’s 2011 changes to resident duty hours and the training environment. J Gen Intern Med. 2012;27(2):241-249. PubMed
22. Elliott DJ, Young RS, Brice J, Aguiar R, Kolm P. Effect of hospitalist workload on the quality and efficiency of care. JAMA Intern Med. 2014;174(5):786-793. PubMed
1. Schrewe B, Pratt DD, McKellin WH. Adapting the forms of yesterday to the functions of today and the needs of tomorrow: a genealogical case study of clinical teaching units in Canada. Adv Health Sci Educ Theory Pract. 2016;21(2):475-499. PubMed
2. Maudsley RF. The clinical teaching unit in transition. CMAJ. 1993;148(9):1564-1566. PubMed
3. Statistics Canada. Recent Changes in Demographic Trends in Canada. Ottawa: Ontario, 2015. https://www150.statcan.gc.ca/n1/pub/75-006-x/2015001/article/14240-eng.htm. Accessed December 9, 2018
4. Statistics Canada. Census, Age and Sex. Ottawa: Ontario, 2016. https://www12.statcan.gc.ca/census-recensement/2016/rt-td/as-eng.cfm. Accessed December 10, 2018.
5. Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. JAMA. 2018;319(10):1024-1039. PubMed
6. van Walraven C. Trends in 1-year survival of people admitted to hospital in Ontario, 1994-2009. CMAJ. 2013;185(16):E755-E762. PubMed
7. Verma AA, Guo Y, Kwan JL, et al. Patient characteristics, resource use and outcomes associated with general internal medicine hospital care: the General Medicine Inpatient Initiative (GEMINI) retrospective cohort study. CMAJ Open. 2017;5(4):E842-E849. PubMed
8. Pattani R, Wu PE, Dhalla IA. Resident duty hours in Canada: past, present and future. CMAJ. 2014;186(10):761-765. PubMed
9. Royal College of Physicians and Surgeons. Specialty Training Requirements in Internal medicine 2015. http://www.royalcollege.ca/cs/groups/public/documents/document/mdaw/mdg4/~edisp/088402.pdf. Accessed December 12, 2018.
10. Freeman TR, Petterson S, Finnegan S, Bazemore A. Shifting tides in the emigration patterns of Canadian physicians to the United States: a cross-sectional secondary data analysis. BMC Health Serv Res. 2016;16(1):678. PubMed
11. Wong BM, Imrie K. Why resident duty hours regulations must address attending physicians’ workload. Acad Med. 2013;88(9):1209-1211. PubMed
12. Flanders SA, Centor B, Weber V, McGinn T, DeSalvo K, Auerbach A. Challenges and opportunities in academic hospital medicine: report from the Academic Hospital Medicine Summit. J Hosp Med. 2009;4(4):240-246. PubMed
13. Torok H, Lackner C, Landis R, Wright S. Learning needs of physician assistants working in hospital medicine. J Hosp Med. 2012;7(3):190-194. PubMed
14. Ivers N, Brown AD, Detsky AS. Lessons from the Canadian experience with single-payer health insurance: just comfortable enough with the status quo. JAMA Intern Med. 2018;178(9):1250-1255. PubMed
15. Wray CM, Flores A, Padula WV, Prochaska MT, Meltzer DO, Arora VM. Measuring patient experiences on hospitalist and teaching services: patient responses to a 30-day postdischarge questionnaire. J Hosp Med. 2016;11(2):99-104. PubMed
16. Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859-865. PubMed
17. Farnan JM, Burger A, Boonyasai RT, et al. Survey of overnight academic hospitalist supervision of trainees. J Hosp Med. 2012;7(7):521-523. PubMed
18. Gonzalo JD, Kuperman EF, Chuang CH, Lehman E, Glasser F, Abendroth T. Impact of an overnight internal medicine academic hospitalist program on patient outcomes. J Gen Intern Med. 2015;30(12):1795-1802. PubMed
19. Soong C, Fan E, Howell EE, et al. Characteristics of Hospitalists and Hospitalist Programs in the United States and Canada 2009. J Clin Outcomes Meas. 2009; 16 (2): 69-74.
20. Yousefi V, Maslowski R. Health system drivers of hospital medicine in Canada: systematic review. Can Fam Phys Med Fam Can. 2013;59(7):762-767. PubMed
21. Nuckols TK, Escarce JJ. Cost implications of ACGME’s 2011 changes to resident duty hours and the training environment. J Gen Intern Med. 2012;27(2):241-249. PubMed
22. Elliott DJ, Young RS, Brice J, Aguiar R, Kolm P. Effect of hospitalist workload on the quality and efficiency of care. JAMA Intern Med. 2014;174(5):786-793. PubMed
© 2019 Society of Hospital Medicine
A Matter of Urgency: Reducing Clinical Text Message Interruptions During Educational Sessions
On general medical wards, effective interprofessional communication is essential for high-quality patient care. Hospitals increasingly adopt secure text-messaging systems for healthcare team members to communicate with physicians in lieu of paging.1-3 Text messages facilitate bidirectional communication4,5 and increase perceived efficiency6-8 and are thus preferred over paging by nurses and trainees. However, this novel technology unintentionally causes high volumes of interruptions.9,10 Compared to paging, sending text messages and calling smartphones are more convenient and encourage communication of issues in real time, regardless of urgency.11 Interrupting messages are often perceived as nonurgent by physicians.6,12 In particular, 73%-93% of pages or messages sent to physicians are found to be nonurgent.13-17
Pages, text messages, or calls not only interrupt day-to-day tasks on the ward6,7,10,11,17,18 but also educational sessions,18-21 which are essential to the clinical teaching unit (CTU). Interruptions reduce learning and retention22 and are disruptive to the medical learning climate.18-20,23
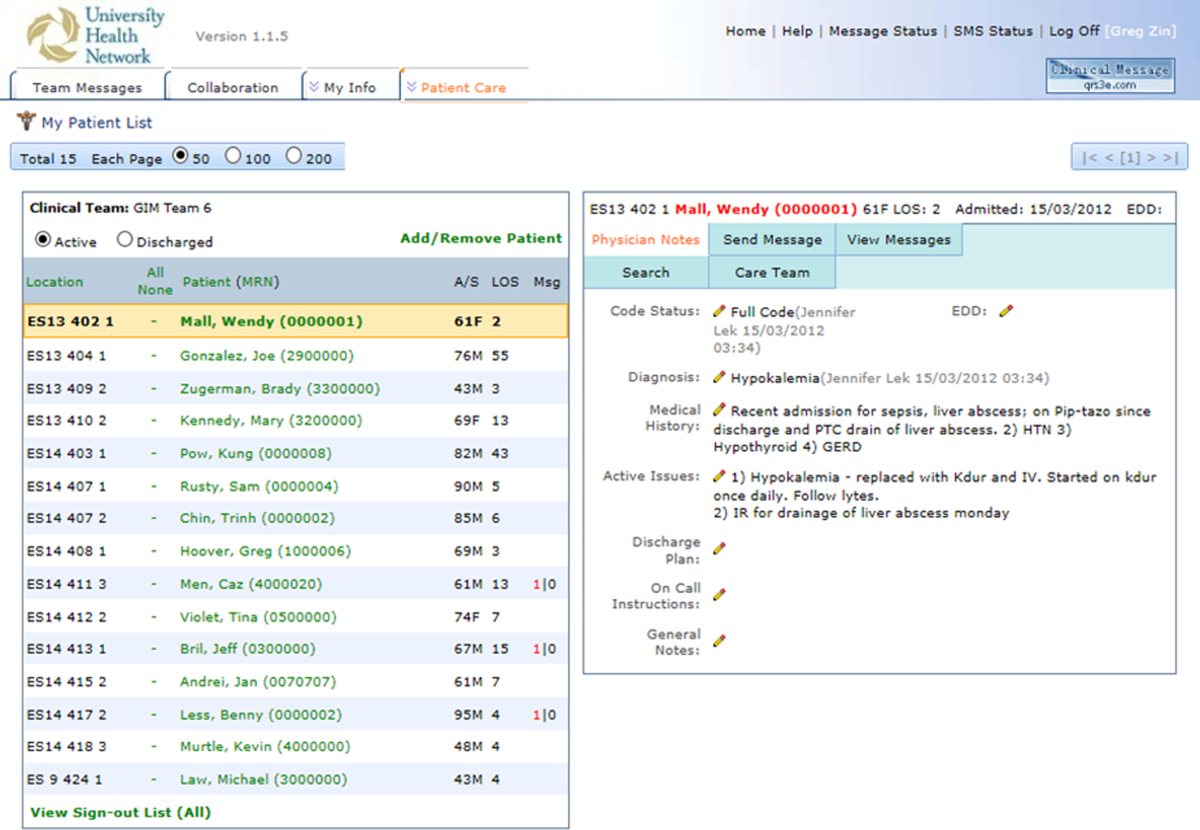
Internal medicine CTUs at our large urban academic hospital network utilize a smartphone-based text messaging tool for interdisciplinary communication. Nonurgent interruptions are frequent during educational seminars, which occur at our institution between 8 AM and 9 AM and 12 PM and 1 PM on weekdays.10,11,19 In a preliminary analysis at one hospital site, an average of three text messages (range 1-11), 2 calls (range 0-8), and 3 emails (range 0-13) interrupted each educational session. Physicians and nurses can disagree on the urgency of messages or calls for the purposes of patient care and workflow.6,11,12,24 Nurses have expressed a desire for guidance regarding what constitutes an urgent clinical communication.6
This project aimed to reduce nonurgent text message interruptions during educational rounds. We hypothesized that improved decision support around clinical prioritization and reminders about educational hours could reduce unnecessary interruptions.
METHODS
This study was approved by the institution’s Research Ethics Board and conducted across 8 general medical CTU teams at an academic hospital network (Sites 1 and 2). Each CTU team provides 24-hour coverage of approximately 20–28 patients. The most responsible resident from each team carries an institution-provided smartphone, which receives secure texts, phone calls, and emails from nurses, social workers, physiotherapists, speech language pathologists, dieticians, pharmacists, and other physicians. Close collaboration with the platform developer permitted changes to be made to the system when needed. Prior to our interventions, a nurse could send a text message as either an “immediate interrupt” or a “delayed interrupt” message. Messages sent via the “delayed interrupt” option would be added to a queue and would eventually lead to an interrupting message if not replied to after a defined period. Direct phone calls were reserved for especially urgent or emergent communications.
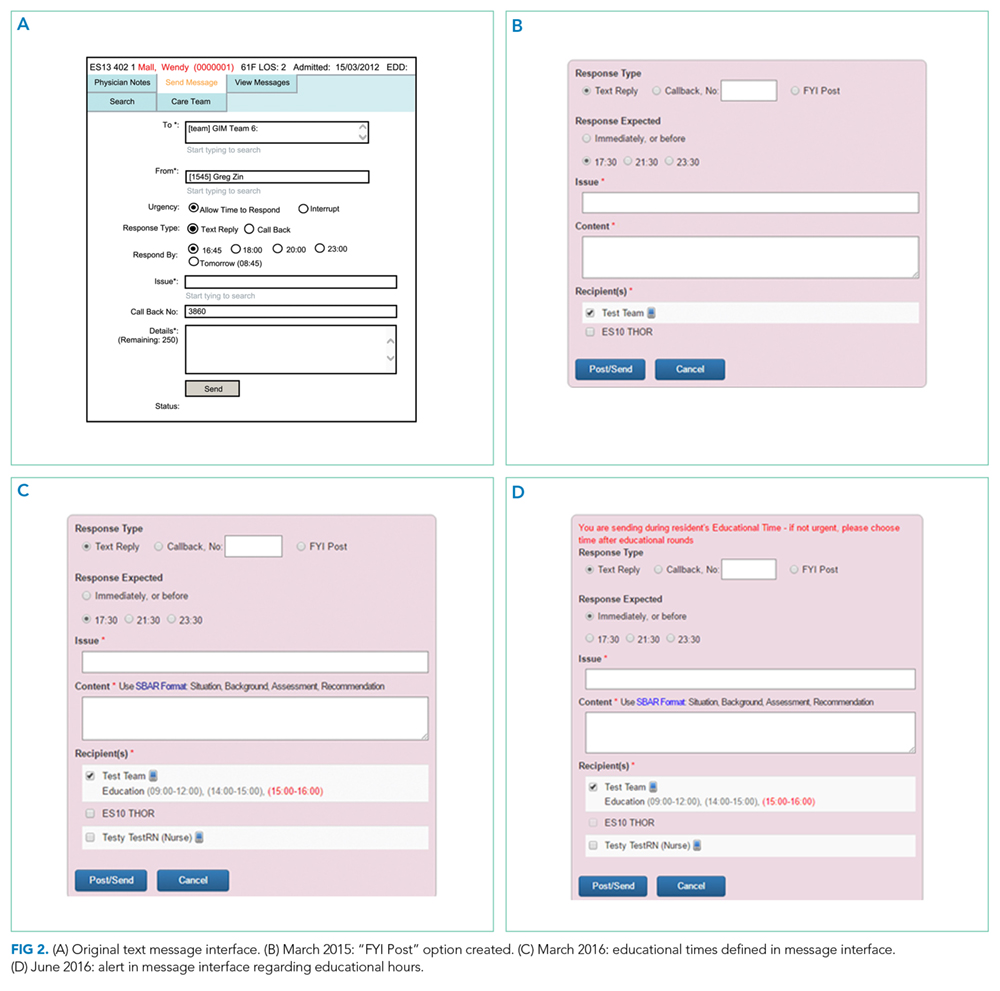
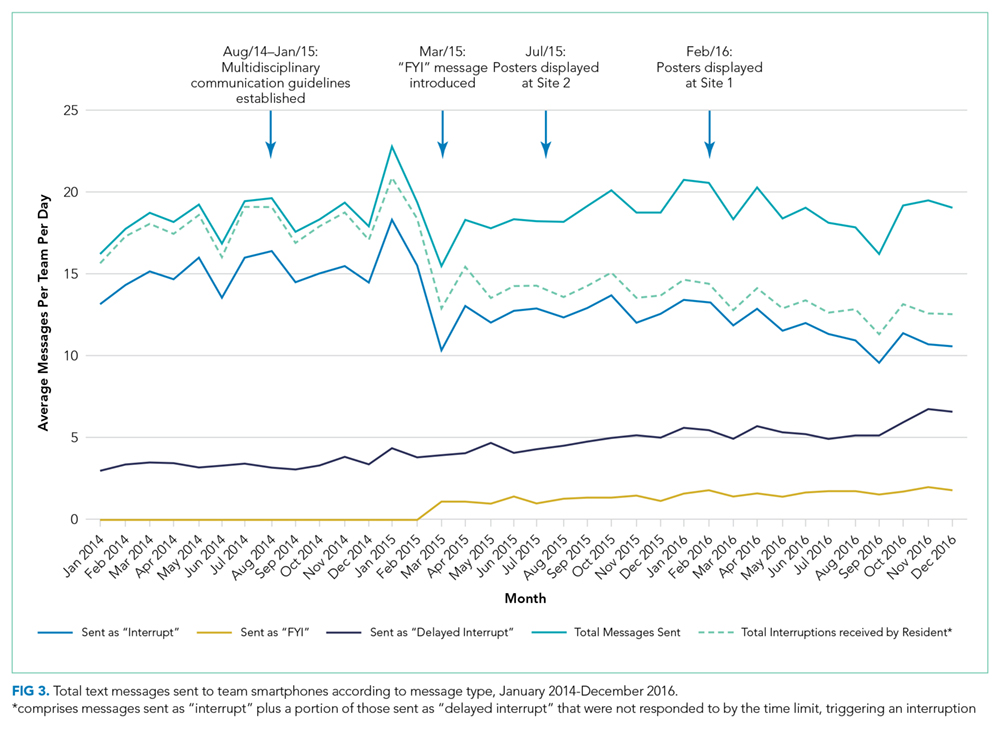
Meetings were held with physicians and nursing managers at Site 1 (August 2014) and Site 2 (January 2015) to establish consensus on the communication process and determine clinical scenarios, regardless of time of day, that warrant a phone call, an “immediate interrupt” text, or a “delayed interrupt” text. In March 2015, resident feedback led to the addition of a third option to the sender interface. This option allowed messages to be sent as “For Your Information (FYI)” only, which would not lead to an interruption. “FYI” messages (for example, to notify that an ambulance had been booked for a patient), were instead placed in an electronic message board that could be viewed by the resident through the application. This change relied upon interdisciplinary trust and a commitment from residents to ensure that “FYI” messages were reviewed regularly.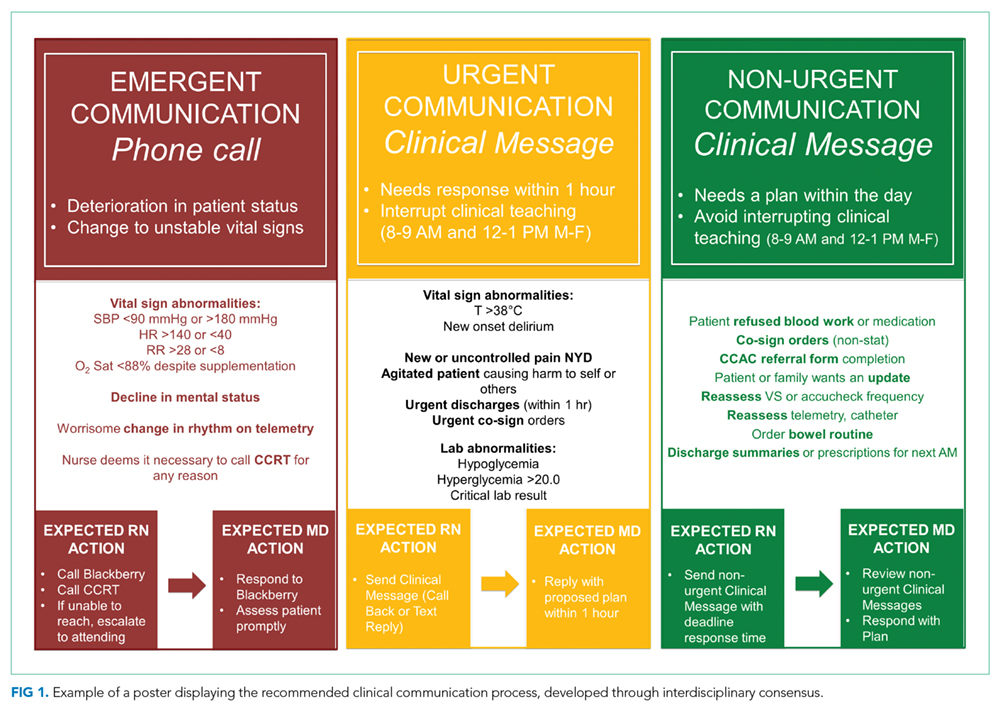
Statistical process control charts (u charts) assessed the frequency of each type of educational interruption (text, call, or email) per team on a monthly basis. The total educational interruptions per month were divided by the number of educational hours per month to account for variation in educational hours each month (for example, during holidays when educational rounds do not take place). If call logs or email data were unavailable for individual teams or time periods, then the denominator was adjusted to reflect the number of teams and educational hours in the sample for that month.
Two 4-week samples of interrupting text messages received by the 8 teams during educational hours were deidentified, analyzed, and compared in terms of content and urgency. A preintervention sample (November 17 to December 14, 2014) was compared to a postintervention sample (November 14 to December 11, 2016). Messages from the 2014 and 2016 samples were randomized, deidentified for date and time, and analyzed for urgency by 3 independent adjudicators (2 senior residents and 1 staff physician) to avoid biasing the postintervention analysis toward improvement. Messages were classified as “urgent” if the adjudicator felt a response or action was required within 1 hour. Messages not meeting these criteria were classified as “nonurgent” or “indeterminate” if the urgency of the message could not be assessed because it required further context. Fleiss kappa statistic evaluated agreement among adjudicators. Individual urgency designations were compared for each message, and discrepant rankings were addressed through repeated joint assessments. Disagreements were resolved through discussion and comparison against communication guidelines. In addition, messages reporting a “critical lab,” requiring physician notification as per institutional policy, were reclassified as “urgent.” The proportion of “nonurgent” messages sent during educational hours was compared between baseline and post-intervention periods using the Chi-square test.
“FYI” messages sent from November 14 to December 11, 2016 were audited using the same adjudication process to determine if “FYI” designations were appropriate and did not contain urgent patient care communications.
RESULTS

Incoming phone call logs were available from April 2015 to December 2016, with a mean of 0.62 (95% CI, 0.56 to 0.67) calls per team per educational hour, which did not change over the study period (Supplementary Figure 2). The overall number of calls to team smartphones also did not change during the measurement period. Incoming email data were available from October 2014 to December 2016, with a mean of 0.94 (95% CI, 0.88 to 1.0) emails per team per educational hour, which did not change over the study period (Supplementary Figure 3). Internal medicine service discharges, “Code Blue” announcements, and Critical Care Outreach Team consultations remained stable over the measurement period.
Independent ranking of the combined 4-week samples of educational text interruptions from 2014 and 2016 revealed an initial 3-way agreement on 257/455 (56%) messages (Fleiss Kappa 0.298, fair agreement), which increased to 405/455 (89%) messages after the first joint assessment and reached full consensus after a third joint assessment that included classifying all messages that communicated institution-defined “critical lab” values as “urgent.”
Overall, 71 (16%) messages were classified as “urgent,” 346 (76%) as “nonurgent,” and 38 (8%) as “indeterminate.” After unblinding of the message date and time, 273 text messages were received during the baseline measurement period (November 17 to December 14, 2014) and 182 messages were received during the equivalent time period 2 years later (November 14 to December 11, 2016), consistent with the reduced volume of educational interruptions observed (Figure 4). A total of 426 (94%) messages were sent by nurses, and the remaining ones were sent by pharmacists (n = 20), ward clerks (n = 3), social workers (n = 4), speech language pathologist (n = 1), or device administrator (n = 1).
The proportion of “nonurgent” messages decreased from 223/273 (82%) in 2014 to 123/182 (68%) in 2016 (P ≤ .01). Although the absolute number of urgent messages remained similar (33 in 2014 and 38 in 2016), the proportion of “urgent” messages increased from 12% to 21% of the total messages received (P = .02). Seventeen (6%) messages had indeterminate frequency in 2014 compared to 21 (11.5%) in 2016 (NS).
An audit of consecutive “FYI” messages (November 14-December 11, 2016) revealed an initial agreement in 384/431 (89%), reaching full consensus after repeated joint assessments. A total of 406 (94%) “FYI” messages were appropriately sent, while 10 (2%) represented urgent communications that should have been sent as interruptions. In 15 (4%) cases, the appropriateness of the message was indeterminate.
DISCUSSION
Sequential interventions over a 36-month period were associated with reduced nonurgent text message interruptions during educational hours. A clinical communication process was formally defined to accurately match message urgency with communication modality. A “noninterrupt” option allowed nonurgent text messages to be posted to an electronic message board, rather than causing real-time interruption, thereby reducing the overall volume of interrupting text messages. Modifying the interface to alert potential senders to protected educational hours was associated with reductions in educational interruptions. Through a blinded analysis of the text message content between 2014 and 2016, we determined that nonurgent educational interruptions were significantly reduced, and the number of urgent communications remained constant. Reduced nonurgent interruptions have the potential to improve the learning climate on the medical teaching unit during protected educational hours.
At baseline, 82% of the sampled text messages sent during educational hours across both sites were considered nonurgent. The estimated proportion of urgent messages varies in the literature (5%-34%)13-18 possibly due to center-specific methods of defining and measuring urgent messages. For example, different assessor training backgrounds, different numbers of assessors, and varying institutional policies are described.13-17 We considered an urgent message to require a response or action within 1 hour or to represent an established “critical lab value” as per the institution. The high proportion of nonurgent interruptions found in this study and other works demonstrates the widespread nature of this problem within inpatient hospital settings; this phenomenon could potentially lead to unintended consequences on efficiency and medical education.
Few other initiatives have aimed to reduce interruptions to medical trainees during educational sessions. At one center, replacing numeric pagers with alphanumeric pagers decreased the need to return pages during educational sessions but did not decrease the overall number of pages.21 Another center implemented an inbox tool that reduced daytime nonurgent numeric pages.15 Similar to our center’s previous experience,11 the total number of communications increased with the creation of the inbox tool.15 Unexpectedly, the introduction of an “FYI” option for senders in March 2015 did not increase the total number of messages.
Increasing use of text messages for communication between physicians and allied health professions has resulted in higher volumes of interruptions compared with conventional paging.6,7,9 Excessive interruptions create a “crisis mode” work climate,10 which could compromise patient safety25-27 and hamper trainees’ attainment of educational objectives.18-20,23 During educational sessions, audible text, phone call, and email interruptions disrupt all learners in addition to the resident receiving the message. The creation of the “FYI” message option in March 2015 was associated with reduced overall daily interruptions, which may improve efficiency in residents’ clinical duties17,18 and minimize multi-tasking that could lead to errors.28 However, adding a real-time notification during educational hours (March 2016, modified June 2016) exerted the greatest impact specifically on educational interruptions. Engaging physicians in the creation and ongoing modification of instant-messaging interfaces can help customize technology to meet the needs of users.15,29 Our work provides a strategy for improving communication between nurses and physicians in a teaching hospital setting, by achieving consensus on levels of urgency of different messages, providing a non-interrupting message option, and providing nurses with real-time information about educational hours.
Potential unintended consequences of the interventions require consideration. Discouraging interruptions may have reduced urgent patient care communications but were mitigated by enabling senders to ignore/override interruption warnings. We did not observe an increase in the number of overall calls to team devices, “Code Blues,” or critical care team consultations. However, we found that a very small (2%) but important group of “FYI” messages should have been sent as urgent interrupting messages, thereby underscoring the necessity for continuous feedback to senders on the clinical communication process.
Our study has limitations. Although educational interruptions can cause fragmented learning at our institution,19 the impact of reduced interruptions on the quality of educational sessions can only be inferred because we did not formally assess resident or staff physician perceptions on this outcome during the interventions. Moreover, we were unable to quantify interruptions received through personal smartphones, a frequent method of physician-physician communication.30 Phone calls are the most intrusive of interruptions but were not the focus of interventions. Future work must consider documenting perceived appropriateness of calls in real time, similar to previous studies assessing paging urgency.13,14,18 Biased ranking of message urgency was minimized by utilizing 3 independent adjudicators blinded to message date throughout the adjudication process and by applying established communication guidelines where available. Nevertheless, retrospective assessment of message urgency could be limited by a lack of clinical context, which may have been more apparent to the original sender and the recipient. Finally, at our center, a close relationship with the communication platform programmer made sequential modifications possible, while other institutions may have limited ability to make such changes. A different approach may be useful in some cases, such as modifying academic teaching times to limit interruptions.23
In a large academic center, a high number of interrupting smartphone messages cause unnecessary distractions and reduce learning during educational hours. “Nonurgent” educational interruptions were reduced through successive improvement cycles, and ultimately by modifying the program interface to alert senders of educational hours. Further reduction in interruptions and sustainability may be achieved by studying phone call interruptions and by formalizing audit and feedback of sender’s adherence to standardized clinical communication methods.
ACKNOWLEDGMENT
Dr. Wu is supported by an award from the Mak Pak Chiu and Mak-Soo Lai Hing Chair in General Internal Medicine, University of Toronto. The authors would like to acknowledge Jason Uppal for his ongoing contribution to the improvement of clinical text message communications at our institution.
Disclosures
The authors have nothing to disclose.
1. Wu R, Lo V, Morra D, et al. A smartphone-enabled communication system to improve hospital communication: usage and perceptions of medical trainees and nurses on general internal medicine wards. J Hosp Med. 2015;10(2):83-89. PubMed
2. Smith CN, Quan SD, Morra D, et al. Understanding interprofessional communication: a content analysis of email communications between doctors and nurses. Appl Clin Inform. 2012;3(1):38-51. PubMed
3. Frizzell JD, Ahmed B. Text messaging versus paging: new technology for the next generation. J Am Coll Cardiol. 2014;64(24):2703-2705. PubMed
4. Wu RC, Morra D, Quan S, et al. The use of smartphones for clinical communication on internal medicine wards. J Hosp Med. 2010;5(9):553-559. PubMed
5. Ighani F, Kapoor KG, Gibran SK, et al. A comparison of two-way text versus conventional paging systems in an academic ophthalmology department. J Med Syst. 2010;34(4):677-684. PubMed
6. Wu R, Rossos P, Quan S, et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed-methods study. J Med Internet Res. 2011;13(3):e59. PubMed
7. Wu RC, Lo V, Morra D, et al. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. J Am Med Inform Assoc. 2013;20(4):766-777. PubMed
8. Patel N, Siegler JE, Stromberg N, Ravitz N, Hanson CW. Perfect storm of inpatient communication needs and an innovative solution utilizing smartphones and secured messaging. Appl Clin Inform. 2016;7(3):777-789. PubMed
9. Aungst TD, Belliveau P. Leveraging mobile smart devices to improve interprofessional communications in inpatient practice setting: A literature review. J Interprof Care. 2015;29(6):570-578. PubMed
10. Vaisman A, Wu RC. Analysis of Smartphone Interruptions on Academic General Internal Medicine Wards. Frequent Interruptions may cause a ‘Crisis Mode’ Work Climate. Appl Clin Inform. 2017;8(1):1-11. PubMed
11. Quan SD, Wu RC, Rossos PG, et al. It’s not about pager replacement: an in-depth look at the interprofessional nature of communication in healthcare. J Hosp Med. 2013;8(3):137-143. PubMed
12. Quan SD, Morra D, Lau FY, et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82(5):378-386. PubMed
13. Katz MH, Schroeder SA. The sounds of the hospital. Paging patterns in three teaching hospitals. N Engl J Med. 1988;319(24):1585-1589. PubMed
14. Patel R, Reilly K, Old A, Naden G, Child S. Appropriate use of pagers in a New Zealand tertiary hospital. N Z Med J. 2006;119(1231):U1912. PubMed
15. Ferguson A, Aaronson B, Anuradhika A. Inbox messaging: an effective tool for minimizing non-urgent paging related interruptions in hospital medicine provider workflow. BMJ Qual Improv Rep. 2016;5(1):u215856.w7316. PubMed
16. Luxenberg A, Chan B, Khanna R, Sarkar U. Efficiency and interpretability of text paging communication for medical inpatients: A mixed-methods analysis. JAMA Intern Med. 2017;177(8):1218-1220. PubMed
17. Ly T, Korb-Wells CS, Sumpton D, Russo RR, Barnsley L. Nature and impact of interruptions on clinical workflow of medical residents in the inpatient setting. J Grad Med Educ. 2013;5(2):232-237. PubMed
18. Blum NJ, Lieu TA. Interrupted care. The effects of paging on pediatric resident activities. Am J Dis Child. 1992;146(7):806-808. PubMed
19. Wu RC, Tzanetos K, Morra D, Quan S, Lo V, Wong BM. Educational impact of using smartphones for clinical communication on general medicine: more global, less local. J Hosp Med. 2013;8(7):365-372. PubMed
20. Katz-Sidlow RJ, Ludwig A, Miller S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595-599. PubMed
21. Wong BM, Quan S, Shadowitz S, Etchells E. Implementation and evaluation of an alpha-numeric paging system on a resident inpatient teaching service. J Hosp Med. 2009;4(8):E34-E40. PubMed
22. Conard MA MR. Interest level improves learning but does not moderate the effects of interruptions: An experiment using simultaneous multitasking. Learn Individ Differ. 2014;30:112-117.
23. Zastoupil L, McIntosh A, Sopfe J, et al. Positive impact of transition from noon conference to academic half day in a pediatric residency program. Acad Pediatr. 2017;17(4):436-442. PubMed
24. Lo V, Wu RC, Morra D, Lee L, Reeves S. The use of smartphones in general and internal medicine units: a boon or a bane to the promotion of interprofessional collaboration? J Interprof Care. 2012;26(4):276-282. PubMed
25. Patterson ME, Bogart MS, Starr KR. Associations between perceived crisis mode work climate and poor information exchange within hospitals. J Hosp Med. 2015;10(3):152-159. PubMed
26. Laxmisan A, Hakimzada F, Sayan OR, Green RA, Zhang J, Patel VL. The multitasking clinician: decision-making and cognitive demand during and after team handoffs in emergency care. Int J Med Inform. 2007;76(11-12):801-811. PubMed
27. Westbrook JI, Woods A, Rob MI, Dunsmuir WT, Day RO. Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683-690. PubMed
28. Collins S, Currie L, Patel V, Bakken S, Cimino JJ. Multitasking by clinicians in the context of CPOE and CIS use. Stud Health Technol Inform. 2007;129(Pt 2):958-962. PubMed
29. Huang ME. It is from mars and physicians from venus: Bridging the gap. PM R. 2017;9(5S):S19-S25. PubMed
30. Tran K, Morra D, Lo V, Quan S, Wu R. The use of smartphones on General Internal Medicine wards: A mixed methods study. Appl Clin Inform. 2014;5(3):814-823. PubMed
On general medical wards, effective interprofessional communication is essential for high-quality patient care. Hospitals increasingly adopt secure text-messaging systems for healthcare team members to communicate with physicians in lieu of paging.1-3 Text messages facilitate bidirectional communication4,5 and increase perceived efficiency6-8 and are thus preferred over paging by nurses and trainees. However, this novel technology unintentionally causes high volumes of interruptions.9,10 Compared to paging, sending text messages and calling smartphones are more convenient and encourage communication of issues in real time, regardless of urgency.11 Interrupting messages are often perceived as nonurgent by physicians.6,12 In particular, 73%-93% of pages or messages sent to physicians are found to be nonurgent.13-17
Pages, text messages, or calls not only interrupt day-to-day tasks on the ward6,7,10,11,17,18 but also educational sessions,18-21 which are essential to the clinical teaching unit (CTU). Interruptions reduce learning and retention22 and are disruptive to the medical learning climate.18-20,23
Internal medicine CTUs at our large urban academic hospital network utilize a smartphone-based text messaging tool for interdisciplinary communication. Nonurgent interruptions are frequent during educational seminars, which occur at our institution between 8 AM and 9 AM and 12 PM and 1 PM on weekdays.10,11,19 In a preliminary analysis at one hospital site, an average of three text messages (range 1-11), 2 calls (range 0-8), and 3 emails (range 0-13) interrupted each educational session. Physicians and nurses can disagree on the urgency of messages or calls for the purposes of patient care and workflow.6,11,12,24 Nurses have expressed a desire for guidance regarding what constitutes an urgent clinical communication.6
This project aimed to reduce nonurgent text message interruptions during educational rounds. We hypothesized that improved decision support around clinical prioritization and reminders about educational hours could reduce unnecessary interruptions.
METHODS
This study was approved by the institution’s Research Ethics Board and conducted across 8 general medical CTU teams at an academic hospital network (Sites 1 and 2). Each CTU team provides 24-hour coverage of approximately 20–28 patients. The most responsible resident from each team carries an institution-provided smartphone, which receives secure texts, phone calls, and emails from nurses, social workers, physiotherapists, speech language pathologists, dieticians, pharmacists, and other physicians. Close collaboration with the platform developer permitted changes to be made to the system when needed. Prior to our interventions, a nurse could send a text message as either an “immediate interrupt” or a “delayed interrupt” message. Messages sent via the “delayed interrupt” option would be added to a queue and would eventually lead to an interrupting message if not replied to after a defined period. Direct phone calls were reserved for especially urgent or emergent communications.
Meetings were held with physicians and nursing managers at Site 1 (August 2014) and Site 2 (January 2015) to establish consensus on the communication process and determine clinical scenarios, regardless of time of day, that warrant a phone call, an “immediate interrupt” text, or a “delayed interrupt” text. In March 2015, resident feedback led to the addition of a third option to the sender interface. This option allowed messages to be sent as “For Your Information (FYI)” only, which would not lead to an interruption. “FYI” messages (for example, to notify that an ambulance had been booked for a patient), were instead placed in an electronic message board that could be viewed by the resident through the application. This change relied upon interdisciplinary trust and a commitment from residents to ensure that “FYI” messages were reviewed regularly.
Statistical process control charts (u charts) assessed the frequency of each type of educational interruption (text, call, or email) per team on a monthly basis. The total educational interruptions per month were divided by the number of educational hours per month to account for variation in educational hours each month (for example, during holidays when educational rounds do not take place). If call logs or email data were unavailable for individual teams or time periods, then the denominator was adjusted to reflect the number of teams and educational hours in the sample for that month.
Two 4-week samples of interrupting text messages received by the 8 teams during educational hours were deidentified, analyzed, and compared in terms of content and urgency. A preintervention sample (November 17 to December 14, 2014) was compared to a postintervention sample (November 14 to December 11, 2016). Messages from the 2014 and 2016 samples were randomized, deidentified for date and time, and analyzed for urgency by 3 independent adjudicators (2 senior residents and 1 staff physician) to avoid biasing the postintervention analysis toward improvement. Messages were classified as “urgent” if the adjudicator felt a response or action was required within 1 hour. Messages not meeting these criteria were classified as “nonurgent” or “indeterminate” if the urgency of the message could not be assessed because it required further context. Fleiss kappa statistic evaluated agreement among adjudicators. Individual urgency designations were compared for each message, and discrepant rankings were addressed through repeated joint assessments. Disagreements were resolved through discussion and comparison against communication guidelines. In addition, messages reporting a “critical lab,” requiring physician notification as per institutional policy, were reclassified as “urgent.” The proportion of “nonurgent” messages sent during educational hours was compared between baseline and post-intervention periods using the Chi-square test.
“FYI” messages sent from November 14 to December 11, 2016 were audited using the same adjudication process to determine if “FYI” designations were appropriate and did not contain urgent patient care communications.
RESULTS
Incoming phone call logs were available from April 2015 to December 2016, with a mean of 0.62 (95% CI, 0.56 to 0.67) calls per team per educational hour, which did not change over the study period (Supplementary Figure 2). The overall number of calls to team smartphones also did not change during the measurement period. Incoming email data were available from October 2014 to December 2016, with a mean of 0.94 (95% CI, 0.88 to 1.0) emails per team per educational hour, which did not change over the study period (Supplementary Figure 3). Internal medicine service discharges, “Code Blue” announcements, and Critical Care Outreach Team consultations remained stable over the measurement period.
Independent ranking of the combined 4-week samples of educational text interruptions from 2014 and 2016 revealed an initial 3-way agreement on 257/455 (56%) messages (Fleiss Kappa 0.298, fair agreement), which increased to 405/455 (89%) messages after the first joint assessment and reached full consensus after a third joint assessment that included classifying all messages that communicated institution-defined “critical lab” values as “urgent.”
Overall, 71 (16%) messages were classified as “urgent,” 346 (76%) as “nonurgent,” and 38 (8%) as “indeterminate.” After unblinding of the message date and time, 273 text messages were received during the baseline measurement period (November 17 to December 14, 2014) and 182 messages were received during the equivalent time period 2 years later (November 14 to December 11, 2016), consistent with the reduced volume of educational interruptions observed (Figure 4). A total of 426 (94%) messages were sent by nurses, and the remaining ones were sent by pharmacists (n = 20), ward clerks (n = 3), social workers (n = 4), speech language pathologist (n = 1), or device administrator (n = 1).
The proportion of “nonurgent” messages decreased from 223/273 (82%) in 2014 to 123/182 (68%) in 2016 (P ≤ .01). Although the absolute number of urgent messages remained similar (33 in 2014 and 38 in 2016), the proportion of “urgent” messages increased from 12% to 21% of the total messages received (P = .02). Seventeen (6%) messages had indeterminate frequency in 2014 compared to 21 (11.5%) in 2016 (NS).
An audit of consecutive “FYI” messages (November 14-December 11, 2016) revealed an initial agreement in 384/431 (89%), reaching full consensus after repeated joint assessments. A total of 406 (94%) “FYI” messages were appropriately sent, while 10 (2%) represented urgent communications that should have been sent as interruptions. In 15 (4%) cases, the appropriateness of the message was indeterminate.
DISCUSSION
Sequential interventions over a 36-month period were associated with reduced nonurgent text message interruptions during educational hours. A clinical communication process was formally defined to accurately match message urgency with communication modality. A “noninterrupt” option allowed nonurgent text messages to be posted to an electronic message board, rather than causing real-time interruption, thereby reducing the overall volume of interrupting text messages. Modifying the interface to alert potential senders to protected educational hours was associated with reductions in educational interruptions. Through a blinded analysis of the text message content between 2014 and 2016, we determined that nonurgent educational interruptions were significantly reduced, and the number of urgent communications remained constant. Reduced nonurgent interruptions have the potential to improve the learning climate on the medical teaching unit during protected educational hours.
At baseline, 82% of the sampled text messages sent during educational hours across both sites were considered nonurgent. The estimated proportion of urgent messages varies in the literature (5%-34%)13-18 possibly due to center-specific methods of defining and measuring urgent messages. For example, different assessor training backgrounds, different numbers of assessors, and varying institutional policies are described.13-17 We considered an urgent message to require a response or action within 1 hour or to represent an established “critical lab value” as per the institution. The high proportion of nonurgent interruptions found in this study and other works demonstrates the widespread nature of this problem within inpatient hospital settings; this phenomenon could potentially lead to unintended consequences on efficiency and medical education.
Few other initiatives have aimed to reduce interruptions to medical trainees during educational sessions. At one center, replacing numeric pagers with alphanumeric pagers decreased the need to return pages during educational sessions but did not decrease the overall number of pages.21 Another center implemented an inbox tool that reduced daytime nonurgent numeric pages.15 Similar to our center’s previous experience,11 the total number of communications increased with the creation of the inbox tool.15 Unexpectedly, the introduction of an “FYI” option for senders in March 2015 did not increase the total number of messages.
Increasing use of text messages for communication between physicians and allied health professions has resulted in higher volumes of interruptions compared with conventional paging.6,7,9 Excessive interruptions create a “crisis mode” work climate,10 which could compromise patient safety25-27 and hamper trainees’ attainment of educational objectives.18-20,23 During educational sessions, audible text, phone call, and email interruptions disrupt all learners in addition to the resident receiving the message. The creation of the “FYI” message option in March 2015 was associated with reduced overall daily interruptions, which may improve efficiency in residents’ clinical duties17,18 and minimize multi-tasking that could lead to errors.28 However, adding a real-time notification during educational hours (March 2016, modified June 2016) exerted the greatest impact specifically on educational interruptions. Engaging physicians in the creation and ongoing modification of instant-messaging interfaces can help customize technology to meet the needs of users.15,29 Our work provides a strategy for improving communication between nurses and physicians in a teaching hospital setting, by achieving consensus on levels of urgency of different messages, providing a non-interrupting message option, and providing nurses with real-time information about educational hours.
Potential unintended consequences of the interventions require consideration. Discouraging interruptions may have reduced urgent patient care communications but were mitigated by enabling senders to ignore/override interruption warnings. We did not observe an increase in the number of overall calls to team devices, “Code Blues,” or critical care team consultations. However, we found that a very small (2%) but important group of “FYI” messages should have been sent as urgent interrupting messages, thereby underscoring the necessity for continuous feedback to senders on the clinical communication process.
Our study has limitations. Although educational interruptions can cause fragmented learning at our institution,19 the impact of reduced interruptions on the quality of educational sessions can only be inferred because we did not formally assess resident or staff physician perceptions on this outcome during the interventions. Moreover, we were unable to quantify interruptions received through personal smartphones, a frequent method of physician-physician communication.30 Phone calls are the most intrusive of interruptions but were not the focus of interventions. Future work must consider documenting perceived appropriateness of calls in real time, similar to previous studies assessing paging urgency.13,14,18 Biased ranking of message urgency was minimized by utilizing 3 independent adjudicators blinded to message date throughout the adjudication process and by applying established communication guidelines where available. Nevertheless, retrospective assessment of message urgency could be limited by a lack of clinical context, which may have been more apparent to the original sender and the recipient. Finally, at our center, a close relationship with the communication platform programmer made sequential modifications possible, while other institutions may have limited ability to make such changes. A different approach may be useful in some cases, such as modifying academic teaching times to limit interruptions.23
In a large academic center, a high number of interrupting smartphone messages cause unnecessary distractions and reduce learning during educational hours. “Nonurgent” educational interruptions were reduced through successive improvement cycles, and ultimately by modifying the program interface to alert senders of educational hours. Further reduction in interruptions and sustainability may be achieved by studying phone call interruptions and by formalizing audit and feedback of sender’s adherence to standardized clinical communication methods.
ACKNOWLEDGMENT
Dr. Wu is supported by an award from the Mak Pak Chiu and Mak-Soo Lai Hing Chair in General Internal Medicine, University of Toronto. The authors would like to acknowledge Jason Uppal for his ongoing contribution to the improvement of clinical text message communications at our institution.
Disclosures
The authors have nothing to disclose.
On general medical wards, effective interprofessional communication is essential for high-quality patient care. Hospitals increasingly adopt secure text-messaging systems for healthcare team members to communicate with physicians in lieu of paging.1-3 Text messages facilitate bidirectional communication4,5 and increase perceived efficiency6-8 and are thus preferred over paging by nurses and trainees. However, this novel technology unintentionally causes high volumes of interruptions.9,10 Compared to paging, sending text messages and calling smartphones are more convenient and encourage communication of issues in real time, regardless of urgency.11 Interrupting messages are often perceived as nonurgent by physicians.6,12 In particular, 73%-93% of pages or messages sent to physicians are found to be nonurgent.13-17
Pages, text messages, or calls not only interrupt day-to-day tasks on the ward6,7,10,11,17,18 but also educational sessions,18-21 which are essential to the clinical teaching unit (CTU). Interruptions reduce learning and retention22 and are disruptive to the medical learning climate.18-20,23
Internal medicine CTUs at our large urban academic hospital network utilize a smartphone-based text messaging tool for interdisciplinary communication. Nonurgent interruptions are frequent during educational seminars, which occur at our institution between 8 AM and 9 AM and 12 PM and 1 PM on weekdays.10,11,19 In a preliminary analysis at one hospital site, an average of three text messages (range 1-11), 2 calls (range 0-8), and 3 emails (range 0-13) interrupted each educational session. Physicians and nurses can disagree on the urgency of messages or calls for the purposes of patient care and workflow.6,11,12,24 Nurses have expressed a desire for guidance regarding what constitutes an urgent clinical communication.6
This project aimed to reduce nonurgent text message interruptions during educational rounds. We hypothesized that improved decision support around clinical prioritization and reminders about educational hours could reduce unnecessary interruptions.
METHODS
This study was approved by the institution’s Research Ethics Board and conducted across 8 general medical CTU teams at an academic hospital network (Sites 1 and 2). Each CTU team provides 24-hour coverage of approximately 20–28 patients. The most responsible resident from each team carries an institution-provided smartphone, which receives secure texts, phone calls, and emails from nurses, social workers, physiotherapists, speech language pathologists, dieticians, pharmacists, and other physicians. Close collaboration with the platform developer permitted changes to be made to the system when needed. Prior to our interventions, a nurse could send a text message as either an “immediate interrupt” or a “delayed interrupt” message. Messages sent via the “delayed interrupt” option would be added to a queue and would eventually lead to an interrupting message if not replied to after a defined period. Direct phone calls were reserved for especially urgent or emergent communications.
Meetings were held with physicians and nursing managers at Site 1 (August 2014) and Site 2 (January 2015) to establish consensus on the communication process and determine clinical scenarios, regardless of time of day, that warrant a phone call, an “immediate interrupt” text, or a “delayed interrupt” text. In March 2015, resident feedback led to the addition of a third option to the sender interface. This option allowed messages to be sent as “For Your Information (FYI)” only, which would not lead to an interruption. “FYI” messages (for example, to notify that an ambulance had been booked for a patient), were instead placed in an electronic message board that could be viewed by the resident through the application. This change relied upon interdisciplinary trust and a commitment from residents to ensure that “FYI” messages were reviewed regularly.
Statistical process control charts (u charts) assessed the frequency of each type of educational interruption (text, call, or email) per team on a monthly basis. The total educational interruptions per month were divided by the number of educational hours per month to account for variation in educational hours each month (for example, during holidays when educational rounds do not take place). If call logs or email data were unavailable for individual teams or time periods, then the denominator was adjusted to reflect the number of teams and educational hours in the sample for that month.
Two 4-week samples of interrupting text messages received by the 8 teams during educational hours were deidentified, analyzed, and compared in terms of content and urgency. A preintervention sample (November 17 to December 14, 2014) was compared to a postintervention sample (November 14 to December 11, 2016). Messages from the 2014 and 2016 samples were randomized, deidentified for date and time, and analyzed for urgency by 3 independent adjudicators (2 senior residents and 1 staff physician) to avoid biasing the postintervention analysis toward improvement. Messages were classified as “urgent” if the adjudicator felt a response or action was required within 1 hour. Messages not meeting these criteria were classified as “nonurgent” or “indeterminate” if the urgency of the message could not be assessed because it required further context. Fleiss kappa statistic evaluated agreement among adjudicators. Individual urgency designations were compared for each message, and discrepant rankings were addressed through repeated joint assessments. Disagreements were resolved through discussion and comparison against communication guidelines. In addition, messages reporting a “critical lab,” requiring physician notification as per institutional policy, were reclassified as “urgent.” The proportion of “nonurgent” messages sent during educational hours was compared between baseline and post-intervention periods using the Chi-square test.
“FYI” messages sent from November 14 to December 11, 2016 were audited using the same adjudication process to determine if “FYI” designations were appropriate and did not contain urgent patient care communications.
RESULTS
Incoming phone call logs were available from April 2015 to December 2016, with a mean of 0.62 (95% CI, 0.56 to 0.67) calls per team per educational hour, which did not change over the study period (Supplementary Figure 2). The overall number of calls to team smartphones also did not change during the measurement period. Incoming email data were available from October 2014 to December 2016, with a mean of 0.94 (95% CI, 0.88 to 1.0) emails per team per educational hour, which did not change over the study period (Supplementary Figure 3). Internal medicine service discharges, “Code Blue” announcements, and Critical Care Outreach Team consultations remained stable over the measurement period.
Independent ranking of the combined 4-week samples of educational text interruptions from 2014 and 2016 revealed an initial 3-way agreement on 257/455 (56%) messages (Fleiss Kappa 0.298, fair agreement), which increased to 405/455 (89%) messages after the first joint assessment and reached full consensus after a third joint assessment that included classifying all messages that communicated institution-defined “critical lab” values as “urgent.”
Overall, 71 (16%) messages were classified as “urgent,” 346 (76%) as “nonurgent,” and 38 (8%) as “indeterminate.” After unblinding of the message date and time, 273 text messages were received during the baseline measurement period (November 17 to December 14, 2014) and 182 messages were received during the equivalent time period 2 years later (November 14 to December 11, 2016), consistent with the reduced volume of educational interruptions observed (Figure 4). A total of 426 (94%) messages were sent by nurses, and the remaining ones were sent by pharmacists (n = 20), ward clerks (n = 3), social workers (n = 4), speech language pathologist (n = 1), or device administrator (n = 1).
The proportion of “nonurgent” messages decreased from 223/273 (82%) in 2014 to 123/182 (68%) in 2016 (P ≤ .01). Although the absolute number of urgent messages remained similar (33 in 2014 and 38 in 2016), the proportion of “urgent” messages increased from 12% to 21% of the total messages received (P = .02). Seventeen (6%) messages had indeterminate frequency in 2014 compared to 21 (11.5%) in 2016 (NS).
An audit of consecutive “FYI” messages (November 14-December 11, 2016) revealed an initial agreement in 384/431 (89%), reaching full consensus after repeated joint assessments. A total of 406 (94%) “FYI” messages were appropriately sent, while 10 (2%) represented urgent communications that should have been sent as interruptions. In 15 (4%) cases, the appropriateness of the message was indeterminate.
DISCUSSION
Sequential interventions over a 36-month period were associated with reduced nonurgent text message interruptions during educational hours. A clinical communication process was formally defined to accurately match message urgency with communication modality. A “noninterrupt” option allowed nonurgent text messages to be posted to an electronic message board, rather than causing real-time interruption, thereby reducing the overall volume of interrupting text messages. Modifying the interface to alert potential senders to protected educational hours was associated with reductions in educational interruptions. Through a blinded analysis of the text message content between 2014 and 2016, we determined that nonurgent educational interruptions were significantly reduced, and the number of urgent communications remained constant. Reduced nonurgent interruptions have the potential to improve the learning climate on the medical teaching unit during protected educational hours.
At baseline, 82% of the sampled text messages sent during educational hours across both sites were considered nonurgent. The estimated proportion of urgent messages varies in the literature (5%-34%)13-18 possibly due to center-specific methods of defining and measuring urgent messages. For example, different assessor training backgrounds, different numbers of assessors, and varying institutional policies are described.13-17 We considered an urgent message to require a response or action within 1 hour or to represent an established “critical lab value” as per the institution. The high proportion of nonurgent interruptions found in this study and other works demonstrates the widespread nature of this problem within inpatient hospital settings; this phenomenon could potentially lead to unintended consequences on efficiency and medical education.
Few other initiatives have aimed to reduce interruptions to medical trainees during educational sessions. At one center, replacing numeric pagers with alphanumeric pagers decreased the need to return pages during educational sessions but did not decrease the overall number of pages.21 Another center implemented an inbox tool that reduced daytime nonurgent numeric pages.15 Similar to our center’s previous experience,11 the total number of communications increased with the creation of the inbox tool.15 Unexpectedly, the introduction of an “FYI” option for senders in March 2015 did not increase the total number of messages.
Increasing use of text messages for communication between physicians and allied health professions has resulted in higher volumes of interruptions compared with conventional paging.6,7,9 Excessive interruptions create a “crisis mode” work climate,10 which could compromise patient safety25-27 and hamper trainees’ attainment of educational objectives.18-20,23 During educational sessions, audible text, phone call, and email interruptions disrupt all learners in addition to the resident receiving the message. The creation of the “FYI” message option in March 2015 was associated with reduced overall daily interruptions, which may improve efficiency in residents’ clinical duties17,18 and minimize multi-tasking that could lead to errors.28 However, adding a real-time notification during educational hours (March 2016, modified June 2016) exerted the greatest impact specifically on educational interruptions. Engaging physicians in the creation and ongoing modification of instant-messaging interfaces can help customize technology to meet the needs of users.15,29 Our work provides a strategy for improving communication between nurses and physicians in a teaching hospital setting, by achieving consensus on levels of urgency of different messages, providing a non-interrupting message option, and providing nurses with real-time information about educational hours.
Potential unintended consequences of the interventions require consideration. Discouraging interruptions may have reduced urgent patient care communications but were mitigated by enabling senders to ignore/override interruption warnings. We did not observe an increase in the number of overall calls to team devices, “Code Blues,” or critical care team consultations. However, we found that a very small (2%) but important group of “FYI” messages should have been sent as urgent interrupting messages, thereby underscoring the necessity for continuous feedback to senders on the clinical communication process.
Our study has limitations. Although educational interruptions can cause fragmented learning at our institution,19 the impact of reduced interruptions on the quality of educational sessions can only be inferred because we did not formally assess resident or staff physician perceptions on this outcome during the interventions. Moreover, we were unable to quantify interruptions received through personal smartphones, a frequent method of physician-physician communication.30 Phone calls are the most intrusive of interruptions but were not the focus of interventions. Future work must consider documenting perceived appropriateness of calls in real time, similar to previous studies assessing paging urgency.13,14,18 Biased ranking of message urgency was minimized by utilizing 3 independent adjudicators blinded to message date throughout the adjudication process and by applying established communication guidelines where available. Nevertheless, retrospective assessment of message urgency could be limited by a lack of clinical context, which may have been more apparent to the original sender and the recipient. Finally, at our center, a close relationship with the communication platform programmer made sequential modifications possible, while other institutions may have limited ability to make such changes. A different approach may be useful in some cases, such as modifying academic teaching times to limit interruptions.23
In a large academic center, a high number of interrupting smartphone messages cause unnecessary distractions and reduce learning during educational hours. “Nonurgent” educational interruptions were reduced through successive improvement cycles, and ultimately by modifying the program interface to alert senders of educational hours. Further reduction in interruptions and sustainability may be achieved by studying phone call interruptions and by formalizing audit and feedback of sender’s adherence to standardized clinical communication methods.
ACKNOWLEDGMENT
Dr. Wu is supported by an award from the Mak Pak Chiu and Mak-Soo Lai Hing Chair in General Internal Medicine, University of Toronto. The authors would like to acknowledge Jason Uppal for his ongoing contribution to the improvement of clinical text message communications at our institution.
Disclosures
The authors have nothing to disclose.
1. Wu R, Lo V, Morra D, et al. A smartphone-enabled communication system to improve hospital communication: usage and perceptions of medical trainees and nurses on general internal medicine wards. J Hosp Med. 2015;10(2):83-89. PubMed
2. Smith CN, Quan SD, Morra D, et al. Understanding interprofessional communication: a content analysis of email communications between doctors and nurses. Appl Clin Inform. 2012;3(1):38-51. PubMed
3. Frizzell JD, Ahmed B. Text messaging versus paging: new technology for the next generation. J Am Coll Cardiol. 2014;64(24):2703-2705. PubMed
4. Wu RC, Morra D, Quan S, et al. The use of smartphones for clinical communication on internal medicine wards. J Hosp Med. 2010;5(9):553-559. PubMed
5. Ighani F, Kapoor KG, Gibran SK, et al. A comparison of two-way text versus conventional paging systems in an academic ophthalmology department. J Med Syst. 2010;34(4):677-684. PubMed
6. Wu R, Rossos P, Quan S, et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed-methods study. J Med Internet Res. 2011;13(3):e59. PubMed
7. Wu RC, Lo V, Morra D, et al. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. J Am Med Inform Assoc. 2013;20(4):766-777. PubMed
8. Patel N, Siegler JE, Stromberg N, Ravitz N, Hanson CW. Perfect storm of inpatient communication needs and an innovative solution utilizing smartphones and secured messaging. Appl Clin Inform. 2016;7(3):777-789. PubMed
9. Aungst TD, Belliveau P. Leveraging mobile smart devices to improve interprofessional communications in inpatient practice setting: A literature review. J Interprof Care. 2015;29(6):570-578. PubMed
10. Vaisman A, Wu RC. Analysis of Smartphone Interruptions on Academic General Internal Medicine Wards. Frequent Interruptions may cause a ‘Crisis Mode’ Work Climate. Appl Clin Inform. 2017;8(1):1-11. PubMed
11. Quan SD, Wu RC, Rossos PG, et al. It’s not about pager replacement: an in-depth look at the interprofessional nature of communication in healthcare. J Hosp Med. 2013;8(3):137-143. PubMed
12. Quan SD, Morra D, Lau FY, et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82(5):378-386. PubMed
13. Katz MH, Schroeder SA. The sounds of the hospital. Paging patterns in three teaching hospitals. N Engl J Med. 1988;319(24):1585-1589. PubMed
14. Patel R, Reilly K, Old A, Naden G, Child S. Appropriate use of pagers in a New Zealand tertiary hospital. N Z Med J. 2006;119(1231):U1912. PubMed
15. Ferguson A, Aaronson B, Anuradhika A. Inbox messaging: an effective tool for minimizing non-urgent paging related interruptions in hospital medicine provider workflow. BMJ Qual Improv Rep. 2016;5(1):u215856.w7316. PubMed
16. Luxenberg A, Chan B, Khanna R, Sarkar U. Efficiency and interpretability of text paging communication for medical inpatients: A mixed-methods analysis. JAMA Intern Med. 2017;177(8):1218-1220. PubMed
17. Ly T, Korb-Wells CS, Sumpton D, Russo RR, Barnsley L. Nature and impact of interruptions on clinical workflow of medical residents in the inpatient setting. J Grad Med Educ. 2013;5(2):232-237. PubMed
18. Blum NJ, Lieu TA. Interrupted care. The effects of paging on pediatric resident activities. Am J Dis Child. 1992;146(7):806-808. PubMed
19. Wu RC, Tzanetos K, Morra D, Quan S, Lo V, Wong BM. Educational impact of using smartphones for clinical communication on general medicine: more global, less local. J Hosp Med. 2013;8(7):365-372. PubMed
20. Katz-Sidlow RJ, Ludwig A, Miller S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595-599. PubMed
21. Wong BM, Quan S, Shadowitz S, Etchells E. Implementation and evaluation of an alpha-numeric paging system on a resident inpatient teaching service. J Hosp Med. 2009;4(8):E34-E40. PubMed
22. Conard MA MR. Interest level improves learning but does not moderate the effects of interruptions: An experiment using simultaneous multitasking. Learn Individ Differ. 2014;30:112-117.
23. Zastoupil L, McIntosh A, Sopfe J, et al. Positive impact of transition from noon conference to academic half day in a pediatric residency program. Acad Pediatr. 2017;17(4):436-442. PubMed
24. Lo V, Wu RC, Morra D, Lee L, Reeves S. The use of smartphones in general and internal medicine units: a boon or a bane to the promotion of interprofessional collaboration? J Interprof Care. 2012;26(4):276-282. PubMed
25. Patterson ME, Bogart MS, Starr KR. Associations between perceived crisis mode work climate and poor information exchange within hospitals. J Hosp Med. 2015;10(3):152-159. PubMed
26. Laxmisan A, Hakimzada F, Sayan OR, Green RA, Zhang J, Patel VL. The multitasking clinician: decision-making and cognitive demand during and after team handoffs in emergency care. Int J Med Inform. 2007;76(11-12):801-811. PubMed
27. Westbrook JI, Woods A, Rob MI, Dunsmuir WT, Day RO. Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683-690. PubMed
28. Collins S, Currie L, Patel V, Bakken S, Cimino JJ. Multitasking by clinicians in the context of CPOE and CIS use. Stud Health Technol Inform. 2007;129(Pt 2):958-962. PubMed
29. Huang ME. It is from mars and physicians from venus: Bridging the gap. PM R. 2017;9(5S):S19-S25. PubMed
30. Tran K, Morra D, Lo V, Quan S, Wu R. The use of smartphones on General Internal Medicine wards: A mixed methods study. Appl Clin Inform. 2014;5(3):814-823. PubMed
1. Wu R, Lo V, Morra D, et al. A smartphone-enabled communication system to improve hospital communication: usage and perceptions of medical trainees and nurses on general internal medicine wards. J Hosp Med. 2015;10(2):83-89. PubMed
2. Smith CN, Quan SD, Morra D, et al. Understanding interprofessional communication: a content analysis of email communications between doctors and nurses. Appl Clin Inform. 2012;3(1):38-51. PubMed
3. Frizzell JD, Ahmed B. Text messaging versus paging: new technology for the next generation. J Am Coll Cardiol. 2014;64(24):2703-2705. PubMed
4. Wu RC, Morra D, Quan S, et al. The use of smartphones for clinical communication on internal medicine wards. J Hosp Med. 2010;5(9):553-559. PubMed
5. Ighani F, Kapoor KG, Gibran SK, et al. A comparison of two-way text versus conventional paging systems in an academic ophthalmology department. J Med Syst. 2010;34(4):677-684. PubMed
6. Wu R, Rossos P, Quan S, et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed-methods study. J Med Internet Res. 2011;13(3):e59. PubMed
7. Wu RC, Lo V, Morra D, et al. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. J Am Med Inform Assoc. 2013;20(4):766-777. PubMed
8. Patel N, Siegler JE, Stromberg N, Ravitz N, Hanson CW. Perfect storm of inpatient communication needs and an innovative solution utilizing smartphones and secured messaging. Appl Clin Inform. 2016;7(3):777-789. PubMed
9. Aungst TD, Belliveau P. Leveraging mobile smart devices to improve interprofessional communications in inpatient practice setting: A literature review. J Interprof Care. 2015;29(6):570-578. PubMed
10. Vaisman A, Wu RC. Analysis of Smartphone Interruptions on Academic General Internal Medicine Wards. Frequent Interruptions may cause a ‘Crisis Mode’ Work Climate. Appl Clin Inform. 2017;8(1):1-11. PubMed
11. Quan SD, Wu RC, Rossos PG, et al. It’s not about pager replacement: an in-depth look at the interprofessional nature of communication in healthcare. J Hosp Med. 2013;8(3):137-143. PubMed
12. Quan SD, Morra D, Lau FY, et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82(5):378-386. PubMed
13. Katz MH, Schroeder SA. The sounds of the hospital. Paging patterns in three teaching hospitals. N Engl J Med. 1988;319(24):1585-1589. PubMed
14. Patel R, Reilly K, Old A, Naden G, Child S. Appropriate use of pagers in a New Zealand tertiary hospital. N Z Med J. 2006;119(1231):U1912. PubMed
15. Ferguson A, Aaronson B, Anuradhika A. Inbox messaging: an effective tool for minimizing non-urgent paging related interruptions in hospital medicine provider workflow. BMJ Qual Improv Rep. 2016;5(1):u215856.w7316. PubMed
16. Luxenberg A, Chan B, Khanna R, Sarkar U. Efficiency and interpretability of text paging communication for medical inpatients: A mixed-methods analysis. JAMA Intern Med. 2017;177(8):1218-1220. PubMed
17. Ly T, Korb-Wells CS, Sumpton D, Russo RR, Barnsley L. Nature and impact of interruptions on clinical workflow of medical residents in the inpatient setting. J Grad Med Educ. 2013;5(2):232-237. PubMed
18. Blum NJ, Lieu TA. Interrupted care. The effects of paging on pediatric resident activities. Am J Dis Child. 1992;146(7):806-808. PubMed
19. Wu RC, Tzanetos K, Morra D, Quan S, Lo V, Wong BM. Educational impact of using smartphones for clinical communication on general medicine: more global, less local. J Hosp Med. 2013;8(7):365-372. PubMed
20. Katz-Sidlow RJ, Ludwig A, Miller S, Sidlow R. Smartphone use during inpatient attending rounds: prevalence, patterns and potential for distraction. J Hosp Med. 2012;7(8):595-599. PubMed
21. Wong BM, Quan S, Shadowitz S, Etchells E. Implementation and evaluation of an alpha-numeric paging system on a resident inpatient teaching service. J Hosp Med. 2009;4(8):E34-E40. PubMed
22. Conard MA MR. Interest level improves learning but does not moderate the effects of interruptions: An experiment using simultaneous multitasking. Learn Individ Differ. 2014;30:112-117.
23. Zastoupil L, McIntosh A, Sopfe J, et al. Positive impact of transition from noon conference to academic half day in a pediatric residency program. Acad Pediatr. 2017;17(4):436-442. PubMed
24. Lo V, Wu RC, Morra D, Lee L, Reeves S. The use of smartphones in general and internal medicine units: a boon or a bane to the promotion of interprofessional collaboration? J Interprof Care. 2012;26(4):276-282. PubMed
25. Patterson ME, Bogart MS, Starr KR. Associations between perceived crisis mode work climate and poor information exchange within hospitals. J Hosp Med. 2015;10(3):152-159. PubMed
26. Laxmisan A, Hakimzada F, Sayan OR, Green RA, Zhang J, Patel VL. The multitasking clinician: decision-making and cognitive demand during and after team handoffs in emergency care. Int J Med Inform. 2007;76(11-12):801-811. PubMed
27. Westbrook JI, Woods A, Rob MI, Dunsmuir WT, Day RO. Association of interruptions with an increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683-690. PubMed
28. Collins S, Currie L, Patel V, Bakken S, Cimino JJ. Multitasking by clinicians in the context of CPOE and CIS use. Stud Health Technol Inform. 2007;129(Pt 2):958-962. PubMed
29. Huang ME. It is from mars and physicians from venus: Bridging the gap. PM R. 2017;9(5S):S19-S25. PubMed
30. Tran K, Morra D, Lo V, Quan S, Wu R. The use of smartphones on General Internal Medicine wards: A mixed methods study. Appl Clin Inform. 2014;5(3):814-823. PubMed
© 2018 Society of Hospital Medicine
Smartphone‐Enabled Communication System
Previous studies have advocated the importance of effective communication between clinicians as a critical component in the provision of high‐quality patient care.[1, 2, 3, 4] There is increasing interest in the use of information and communication technologies to improve how clinicians communicate in hospital settings. A number of hospitals have implemented different solutions to improve communication. These solutions include alphanumeric pagers,[5] smartphones,[6] e‐mail,[7] secure text messaging,[8] and a Web‐based interdisciplinary communication tool.[9]
These systems have different limitations that render them inefficient and likely inhibit collaborative care. Current systems, such as pagers, rely on the sender to ensure the message was received and are successful in delivering messages approximately 67% of the time.[5, 9, 10] Although alphanumeric pagers and secure text messaging can increase the likelihood of delivery, these messages are often isolated and not easily viewable by the whole care team.[11] Improved systems should also reduce unnecessary interruptions by providing support for both urgent and delayed messages. Finally, messages should be stored and retrievable to enable increased accountability and allow for review for quality improvement initiatives.
It is also important to consider the unintended consequences of technology implementations.[12] Moving communication to text messages and smartphones has the potential to reduce interprofessional relations and can increase confusion if used for complex issues.[10, 13] In this article, we present a system designed to improve interprofessional communication on general internal medicine wards by incorporating these desired features and describe the usage and attitudes toward the system, specifically assessing for effects on multiple domains including efficiency, interprofessional collaboration, and relationships.
METHODS
Research Question
Will nurses and physicians use a system designed to improve interprofessional communication and will they perceive it to be effective and improve workflow?
Setting
The study took place on the general internal medicine wards at Toronto General Hospital and Toronto Western Hospital, 2 large academic teaching hospitals. There are several general internal medicine wards at each site with approximately 80 beds at each site. At each site there are 4 clinical teaching units and 1 hospitalist team. The study was approved by the research ethics board at the University Health Network.
Intervention
To address issues with communication, we developed a systemClinical Message (CM)that included 2 main components: a physician handover tool and secure messaging module. The focus of CM was to improve communication and information flow among different healthcare providers (physicians, nurses, pharmacists, social workers and therapists) through a secure, shared platform.
Physician Handover
The physician handover tool was designed to facilitate the physician handover process at shift change and is used as a patient rounding tool for day‐to‐day management of patients. It is also accessed by nurses and other clinicians to view the physicians' notes and to stay informed on the overall care plan. The tool contains standard elements including a list of patients with the following information on each patient: demographics, diagnosis, code status, medical history, active issues, and discharge plans (Figure 1).

Secure Messaging
Secure messaging was designed around our dominant communication: nurses sending messages to physicians who would then respond. Nurses and other health professionals sent messages to the medical teams by accessing CM, selecting the appropriate patient, and filling out a message template. The system automatically populated the To field with the team assigned to the selected patient. Messaging for each team was centralized around a single team smartphone that was carried 24 hours a day, 7 days a week by a physician on that team. This removed the guesswork of trying to identify the individual physician responsible for that patient. For each message, a subject or issue and content were entered (Figure 2). Logic was also incorporated to reduce the amount of unnecessary interruptions. Senders would choose to send the message immediately as an interrupt message (urgent) for urgent/time sensitive issues or as an allow time to respond message (delayed). For the latter, the message was posted to the system where physicians could check and answer them. Interrupt messages were sent to the team smartphone using the Short Message Service (SMS) protocol. To try and ensure the communication loop on any issues was closed, when a message requested a response and did not receive it, the system sent another message. For urgent messages, a repeat message was initiated after 15 minutes. For delayed messages, the sender defined when they needed a response, typically within 2 to 8 hours. Senders were also able to select the mode of response that would best meet their needs from a workflow perspective: call back, text reply, or to specify that a reply was not required. Senders were also able to verify if the messages were received by the physician's smartphone. Physicians could view the messages within CM and reply. For messages that went to their team smartphone, physicians could respond from the smartphone through a secure Web link.
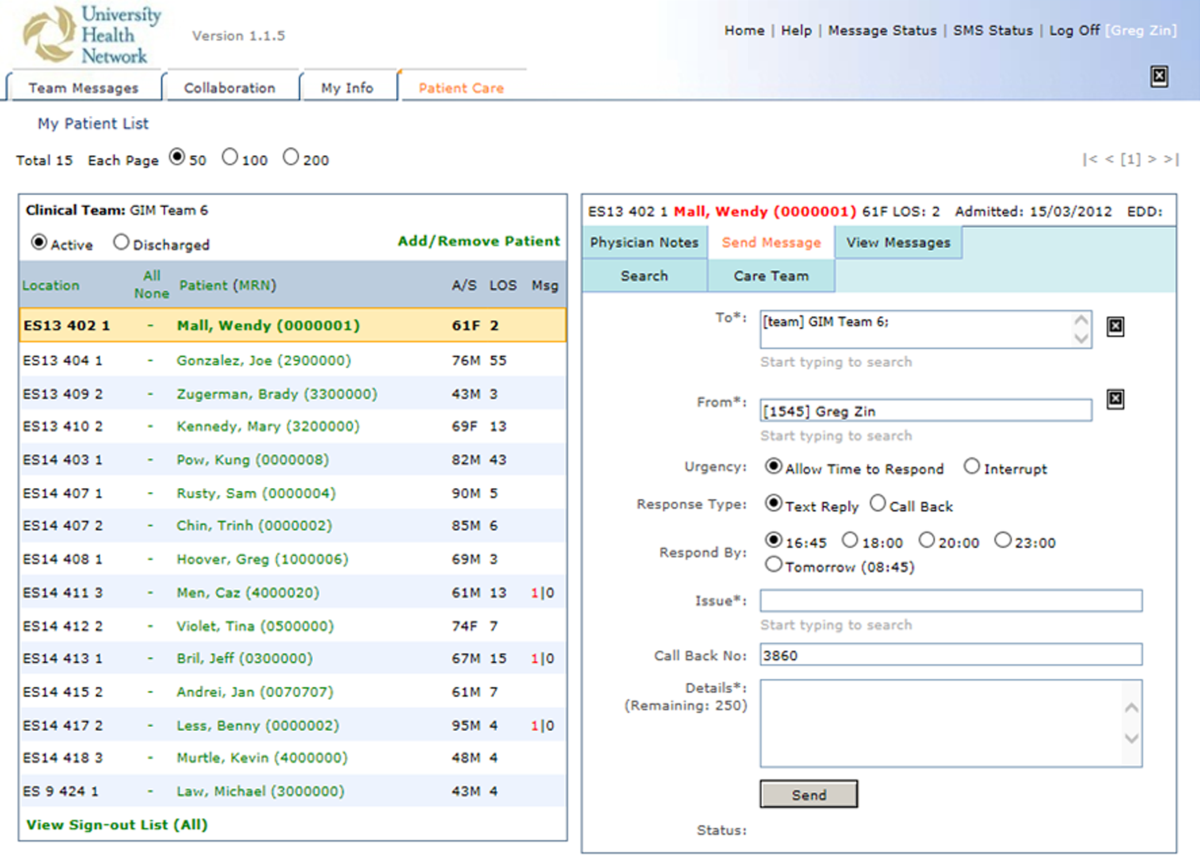
Because the messages were linked to the patients, they were visible to the entire care team, not just the message sender and recipient. If the care of the patient was transferred from 1 clinician to the next, the new clinician could easily review prior messages to understand recent patient events. The system was accessible through a browser on the intranet. The system regularly pulled patient demographic details such as name, age, medical record number, and location from our electronic medical record through a 1‐way interface. Information from this communication system was not considered part of the medical record but was retrievable.
The system was introduced as the new standard method of communication for nurses to reach physicians for all of the general internal medicine wards and for all medical teams at site 1 on May 2, 2011 and site 2 on June 6, 2011. The system replaced a text‐based Web‐paging system and supplemented the numeric pager carried by residents. Initial training of a half hour was provided to all nurses and residents.
Message Analysis for Usage Statistics
We analyzed messages created and sent via the CM system from May 2011 until August 2012. The extracted message information included date and time sent, issue, level of urgency, response type requested, roles of clinicians involved from the associated team, hospital site (senders and receivers), and message details. The following inclusion criteria were used for the analyses: (1) the senders and receivers of the messages could not be CM support staff, and (2) the messages sent were intended for the team smartphones used by the respective medical teams, not individual clinicians. Descriptive statistics and frequency analysis were performed using Microsoft Excel (Microsoft Corp., Redmond, WA) and IBM SPSS (IBM, Armonk, NY).
Survey
Development of the Survey
We used standard methods to develop a survey to assess staff perceptions on the impact of the new communication system. Relevant questionnaire items were compiled from a systematic review of the literature for communication surveys and communication issues that included the following domains: efficiency, accountability, accuracy, collaboration, timeliness, richness of the communication medium, and impact on interprofessional relationships and verbal communication.[10, 14, 15] We carried out pilot testing with 5 nurses and physicians, and modified the questionnaires based on their feedback.
Sampling and Data Collection of the Survey
Survey participants consisted of 2 groups of clinicians: (1) medical trainees that included medical residents, medical interns, and clinical fellows, and (2) nursing staff that included part‐time and full‐time nurses. To qualify for inclusion, participants had to have used the CM system for at least a month prior to administration of the questionnaire.
Data Analysis
Responses were recorded into an Excel spreadsheet that was imported into SPSS for analysis. Categorical variables were described using proportions. Survey comments were grouped into common themes, and themes mentioned by more than 1 respondent were reported.
RESULTS
Usage Analysis
A total of 60,969 messages were sent using CM between May 2, 2011 and August 19, 2012. On average, a team would receive 14.8 messages per day. Of all messages, 76.5% requested a text reply, 7.7% requested a call‐back, and 15.7% did not request a response. More than two‐thirds of messages at both hospitals were sent as immediate. Of the nonurgent messages, 86% were not replied to within the desired time, requiring a repeat message to be sent. Examples of different types of messages are shown in Table 1.
| Sender | Issue | Details | Priority | Desired Response Type | Time Created | Time Sent | Reply | Time Replied |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| Nurse | Vital sign | Pt's BP is 182/95, HR is 108 now. Previous at 0800 was 165/78; HR was 99. PT is not on antihypertensive meds. | Allow time to respond (23:00) | Text reply | 21:43 | 23:02 | OK. Will assess. | 23:03 |
| Nurse | NG tube | NG tube is in place. Can you please enter portable chest x‐ray to check placement ASAP? | Immediate | Text reply | 16:58 | 16:58 | Will do. | 17:00 |
| Nurse | Bloodwork | Pt creat=216. Pt has NS @ 75 cc/hr. Pt has noted crackles throughout lung fields and has productive cough; eating and drinking well. Would you like it continued as well? Pt O2Sat 93% RA; would you like 4 L of O2 continued? Pls call for telephone order. | Immediate | Call back | 12:53 | 13:04 | Dealt with it on phone. | 13:05 |
| Nurse | Pain control | Hello! Pt has been getting 1 mg hydromorphone IV q 1 hr and pain is still not controlled. Pt remains awake and alert. Thanks! | Immediate | Info only | 15:41 | 15:41 | Thank you. | 15:42 |
For messages requesting a text reply, 8.6% did not receive a reply. The median response time was 2.3 minutes (interquartile range of 5.8 minutes), but some messages did not receive a response even after a week, which skewed the distribution of response times. For those messages that did receive a reply, 68.9% of them were responded to within 5 minutes, and 84.5% were responded to within 15 minutes. Messages were predominantly received between 9 am and midnight (see Supporting Figure 1 in the online version of this article). Because the sending of some messages was delayed, there appeared to be fewer messages received during protected educational times (89 am and 121 pm) as well as between midnight and 7 am compared to other times.
Survey Results
Between April 2013 and June 2013, 82 of 86 medical trainees (95.3%) and 83 of 116 nurses (71.6%) completed the survey, for an overall response rate of 81.7%. Clinicians perceived that CM appeared to have a positive impact on efficiency. In particular, 82.8% of physicians and 78.3% of nurses agreed or strongly agreed that CM helped speed up daily work tasks (Table 2). The majority of physicians and nurses agreed that the system increased accountability, increased timeliness of communication, and improved interprofessional relationships. It was not seen to be effective for communicating complex patient issues.
| No. of Subitems in Survey | Physician (% Agree, Strongly Agree), n=82 | Nurse (% Agree, Strongly Agree), n=83 | |
|---|---|---|---|
| |||
| Positive impact on efficiency. | 7 | 58.9% | 66.6% |
| The CM system helps speed up my daily work tasks. | 82.8% | 78.3% | |
| Positive impact on physician‐nurse collaboration. | 6 | 55.3% | 58.5% |
| The CM system increases the amount of communication between nurses and physicians. | 50.6% | 67.1% | |
| Improved timeliness of communication. | 5 | 54.2% | 50.5% |
| Communication through the CM system helps me resolve patient issues within the appropriate time frames. | 66.7% | 55.6% | |
| Increased accountability. | 2 | 67.1% | 73.2% |
| Improved accuracy of communications. | 3 | 41.6% | 50.7% |
| Improved interprofessional relationships. | 2 | 62.2% | 53.6% |
| Increased verbal communications. | 2 | 35.1% | 25.3% |
| Richness of the communication medium. | 6 | 40.7% | 48.3% |
| I find the CM system useful for communicating complex patient issues. | 35.8% | 26.3% | |
| I would prefer CM over standard hospital communication methods such as numeric paging. | 1 | 68.3% | 76.5% |
| I enjoy using the CM system for clinical communication on the wards. | 1 | 63.0% | 79.0% |
| Communication through the CM system helps to reduce interruptions for physicians. | 1 | 45.7% | |
Survey comments revealed that nurses perceived a lack of desired response, whereas physicians noted being interrupted with low‐value information through the system (Table 3). Both commented that further functionality, such as an active message stream, would be of benefit. Difficulty in communicating complex issues was also noted.
| Issue | Occurrences | Example | ||
|---|---|---|---|---|
| MD | RN | Total | ||
| ||||
| Lack of response | 1 | 10 | 11 | It depends if they respond quickly or not. A few times I send the 2nd message to remind them of the issue. I also spend more time to check if they answer it or not. I even call their Blackberries at last to get a response. |
| Message stream | 3 | 4 | 7 | I wish that I could see follow‐up messages after my initial reply (ie, it would be nice to have an open message stream). |
| Difficult to communicate complex issues | 1 | 5 | 6 | Difficult to communicate complex issues. Takes a lot of time to respond, and it becomes inefficient when responding to nonurgent CM because it interrupts workflow. |
| Many messages are low‐value interrupts | 3 | 0 | 3 | CM is useful for handover between clinicians, but often it slows down the clinician when they are used for information‐related low‐value/noncritical messages between nurses and clinicians |
| Lack of detailed response | 0 | 3 | 3 | Specific messages regarding response to care is required most times. For example, acknowledged is not a favorable response. |
| Technical issues | 2 | 0 | 2 | I find CM very useful. We have had multiple issues with our Blackberry this month, and CM was not working. When it is up and running, however, it is a wonderful tool. |
| Discrepancy in perceived urgency | 2 | 0 | 2 | Discrepancy between what nurses find urgent and what we find urgent. |
DISCUSSION
We describe an implementation of a system to improve clinical communication in hospitals. The system was highly used and was perceived to improve communication by both nurses and physicians. Specifically, users found that the system increased efficiency, accountability, timeliness, and collaboration, but that there were issues with message clarity for complex medical issues.
Other systems and approaches have been implemented to improve communication. These included the use of alphanumeric pagers, e‐mail, secure texting, and smartphones. There is evidence that more advanced systems can improve efficiency for senders.[16] A recent randomized trial of secure text messaging found that it was perceived to be more efficient than paging, but overall usage was low and inconsistent.[8] There is also evidence that smartphones may increase interruptions, worsen interprofessional relationships, and cause issues with professional behavior.[10] Unfortunately, there are a limited number of interventions that improve communication, with some improving efficiency but none demonstrating improved patient‐oriented outcomes.[16, 17] This study evaluated a novel system, with functionality to link communication to patients, and created a system that aligned with the workflow of the clinicians. Messages were linked to the patient, not the sender or receiver, so other clinicians in the patient's circle of care could easily view the communication. Moreover, the system was designed to improve message response rates and allow for nonurgent messages.
Our communication system uses standard, commercially available components (smartphones, SMS), and relatively basic functionality (handover, secure messaging). Important findings are that the current system of paging can be transformed to a more efficient system that users will readily adopt. We found positive effects with components of the system. It appeared to improve efficiency and increase accountability. Accountability is crucial and moves from undocumented conversation to fully documented details of interactions. This can be used for both incident review and to review for quality improvement.
Using the system, physicians perceived that they were bothered by low‐value information, whereas nurses perceived a lack of response, and both found that the system was not ideal for complex messages. The mismatch between what physicians and nurses perceive as important has been attributed to their different timeframes and context.[18] For nurses with an upcoming change of shift, they wanted resolution of issues before handover. A physician on a different ward may not appreciate the context of a nurse having to directly interact with an irate family member. These different perceptions likely contributed to the lack of response to 8.6% of text messages. This is still better than other systems, such as paging, which can be as high as 33%.[10] For nonurgent items, clinicians would ideally check and clear items regularly from the system using a desktop computer, responding within the allotted timeframe. Unfortunately, this never became part of routine physician workflow, likely due to their busy workload, so many physicians would only respond when items became overdue. However, having a method to deal with nonurgent messages may have prevented some interruptions during protected educational times of trainees. The system was also not ideal for urgent or complex items. Complex items can be difficult to convey using the rarified communication medium of text messages.[19, 20] Urgent or complex issues are likely best resolved with a face‐to‐face or telephone conversation.
There are several limitations in our study that should be considered when interpreting the results. It is a study of usage and perceptions after implementation. Although more rigorous study is required to evaluate the effects, we see this as a first step in process improvement. Future research should measure the impact on improving patient care of this system and on patient outcomes such as adverse events. The study and intervention was limited to general internal medicine wards in 2 academic hospital settings where there are frequent rotations of medical personnel. The findings may not be generalizable to other hospital settings.
Future directions should be to further improve on the communication system and to educate and train staff on how to effectively communicate. Survey results showed that although users perceived increased efficiency, there was still significant opportunity to improve. One way to improve would be to have a mobile application in which physicians can easily review nonurgent items. Improvements could also be realized by educating clinicians on the use of the system and providing immediate feedback. Providing feedback to physicians on how well they respond could address nurses' issues around lack of timely response. By creating consensus between nurses and physicians on what is of high and low value to communicate could increase satisfaction for all users.
In summary, we present the usage and perceptions of a system designed to improve hospital communication. We found that there was high uptake, and that users perceived it to improve efficiency, collaboration, and accountability, but it may not be useful for communicating complex issues.
ACKNOWLEDGEMENTS
The authors acknowledge the nurses, physicians, residents, and other health professions on the general internal medicine ward for their patience and support as we continue to try to innovate. The authors also acknowledge the members of the information systems department (Shared Information Management Systems, University Health Network) who helped to support the Communication System, and the software developer, QRS, that helped to codevelop the software system.
Disclosures: The hospital was in a codevelopment agreement that has since terminated. No researcher or hospital received any funds from private industry for any purpose including personal or research. The authors report no conflicts of interest.
- . When conversation is better than computation. J Am Med Inform Assoc. 2000;7(3):277–286.
- , , , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324(6):370–376.
- , , , et al. Gaps in pediatric clinician communication and opportunities for improvement. J Healthc Qual. 2008;30(5):43–54.
- , , , , . Quality in Australian health care study. Med J Aust. 1996;164(12):754.
- , , , . Implementation and evaluation of an alphanumeric paging system on a resident inpatient teaching service. J Hosp Med. 2009;4(8):E34–E40.
- , , , et al. Demonstrating the BlackBerry as a clinical communication tool: a pilot study conducted through the Centre for Innovation in Complex Care. Healthc Q. 2008;11(4):94–98.
- , , , . The use of wireless email to improve healthcare team communication. J Am Med Inform Assoc. 2009;16(5):705–713.
- , , , , , . Smarter hospital communication: secure smartphone text messaging improves provider satisfaction and perception of efficacy, workflow. J Hosp Med. 2014;9(9):573–578.
- , , , , . Beyond paging: building a web‐based communication tool for nurses and physicians. J Gen Intern Med. 2009;24(1):105–110.
- , , , et al. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. J Am Med Inform Assoc. 2013;20(4):766–777.
- , , , et al. Improving hospital care and collaborative communications for the 21st century: key recommendations for general internal medicine. Interact J Med Res. 2012;1(2):e9.
- , , , , , . Anticipating and addressing the unintended consequences of health IT and policy: a report from the AMIA 2009 Health Policy Meeting. J Am Med Inform Assoc. 2011;18(1):82–90.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- , , , , . Organizational assessment in intensive care units (ICUs): construct development, reliability, and validity of the ICU nurse‐physician questionnaire. Med Care. 1991;29(8):709–726.
- . Impact of communication medium on task performance and satisfaction: an examination of media‐richness theory. Inform Manag. 1999;35:295–312.
- , , , et al. Effects of clinical communication interventions in hospitals: a systematic review of information and communication technology adoptions for improved communication between clinicians. Int J Med Inform. 2012;81(11):723–732.
- , , , et al. Provider‐to‐provider electronic communication in the era of meaningful use: a review of the evidence. J Hosp Med. 2013;8(10):589–597.
- , , , et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82(5):378–386.
- , , , , , . Short message service or disService: issues with text messaging in a complex medical environment. Int J Med Inform. 2014;83(4):278–284.
- , , . Instant messaging at the hospital: supporting articulation work? Int J Med Inform. 2013;82(9):753–761.
Previous studies have advocated the importance of effective communication between clinicians as a critical component in the provision of high‐quality patient care.[1, 2, 3, 4] There is increasing interest in the use of information and communication technologies to improve how clinicians communicate in hospital settings. A number of hospitals have implemented different solutions to improve communication. These solutions include alphanumeric pagers,[5] smartphones,[6] e‐mail,[7] secure text messaging,[8] and a Web‐based interdisciplinary communication tool.[9]
These systems have different limitations that render them inefficient and likely inhibit collaborative care. Current systems, such as pagers, rely on the sender to ensure the message was received and are successful in delivering messages approximately 67% of the time.[5, 9, 10] Although alphanumeric pagers and secure text messaging can increase the likelihood of delivery, these messages are often isolated and not easily viewable by the whole care team.[11] Improved systems should also reduce unnecessary interruptions by providing support for both urgent and delayed messages. Finally, messages should be stored and retrievable to enable increased accountability and allow for review for quality improvement initiatives.
It is also important to consider the unintended consequences of technology implementations.[12] Moving communication to text messages and smartphones has the potential to reduce interprofessional relations and can increase confusion if used for complex issues.[10, 13] In this article, we present a system designed to improve interprofessional communication on general internal medicine wards by incorporating these desired features and describe the usage and attitudes toward the system, specifically assessing for effects on multiple domains including efficiency, interprofessional collaboration, and relationships.
METHODS
Research Question
Will nurses and physicians use a system designed to improve interprofessional communication and will they perceive it to be effective and improve workflow?
Setting
The study took place on the general internal medicine wards at Toronto General Hospital and Toronto Western Hospital, 2 large academic teaching hospitals. There are several general internal medicine wards at each site with approximately 80 beds at each site. At each site there are 4 clinical teaching units and 1 hospitalist team. The study was approved by the research ethics board at the University Health Network.
Intervention
To address issues with communication, we developed a systemClinical Message (CM)that included 2 main components: a physician handover tool and secure messaging module. The focus of CM was to improve communication and information flow among different healthcare providers (physicians, nurses, pharmacists, social workers and therapists) through a secure, shared platform.
Physician Handover
The physician handover tool was designed to facilitate the physician handover process at shift change and is used as a patient rounding tool for day‐to‐day management of patients. It is also accessed by nurses and other clinicians to view the physicians' notes and to stay informed on the overall care plan. The tool contains standard elements including a list of patients with the following information on each patient: demographics, diagnosis, code status, medical history, active issues, and discharge plans (Figure 1).
Secure Messaging
Secure messaging was designed around our dominant communication: nurses sending messages to physicians who would then respond. Nurses and other health professionals sent messages to the medical teams by accessing CM, selecting the appropriate patient, and filling out a message template. The system automatically populated the To field with the team assigned to the selected patient. Messaging for each team was centralized around a single team smartphone that was carried 24 hours a day, 7 days a week by a physician on that team. This removed the guesswork of trying to identify the individual physician responsible for that patient. For each message, a subject or issue and content were entered (Figure 2). Logic was also incorporated to reduce the amount of unnecessary interruptions. Senders would choose to send the message immediately as an interrupt message (urgent) for urgent/time sensitive issues or as an allow time to respond message (delayed). For the latter, the message was posted to the system where physicians could check and answer them. Interrupt messages were sent to the team smartphone using the Short Message Service (SMS) protocol. To try and ensure the communication loop on any issues was closed, when a message requested a response and did not receive it, the system sent another message. For urgent messages, a repeat message was initiated after 15 minutes. For delayed messages, the sender defined when they needed a response, typically within 2 to 8 hours. Senders were also able to select the mode of response that would best meet their needs from a workflow perspective: call back, text reply, or to specify that a reply was not required. Senders were also able to verify if the messages were received by the physician's smartphone. Physicians could view the messages within CM and reply. For messages that went to their team smartphone, physicians could respond from the smartphone through a secure Web link.
Because the messages were linked to the patients, they were visible to the entire care team, not just the message sender and recipient. If the care of the patient was transferred from 1 clinician to the next, the new clinician could easily review prior messages to understand recent patient events. The system was accessible through a browser on the intranet. The system regularly pulled patient demographic details such as name, age, medical record number, and location from our electronic medical record through a 1‐way interface. Information from this communication system was not considered part of the medical record but was retrievable.
The system was introduced as the new standard method of communication for nurses to reach physicians for all of the general internal medicine wards and for all medical teams at site 1 on May 2, 2011 and site 2 on June 6, 2011. The system replaced a text‐based Web‐paging system and supplemented the numeric pager carried by residents. Initial training of a half hour was provided to all nurses and residents.
Message Analysis for Usage Statistics
We analyzed messages created and sent via the CM system from May 2011 until August 2012. The extracted message information included date and time sent, issue, level of urgency, response type requested, roles of clinicians involved from the associated team, hospital site (senders and receivers), and message details. The following inclusion criteria were used for the analyses: (1) the senders and receivers of the messages could not be CM support staff, and (2) the messages sent were intended for the team smartphones used by the respective medical teams, not individual clinicians. Descriptive statistics and frequency analysis were performed using Microsoft Excel (Microsoft Corp., Redmond, WA) and IBM SPSS (IBM, Armonk, NY).
Survey
Development of the Survey
We used standard methods to develop a survey to assess staff perceptions on the impact of the new communication system. Relevant questionnaire items were compiled from a systematic review of the literature for communication surveys and communication issues that included the following domains: efficiency, accountability, accuracy, collaboration, timeliness, richness of the communication medium, and impact on interprofessional relationships and verbal communication.[10, 14, 15] We carried out pilot testing with 5 nurses and physicians, and modified the questionnaires based on their feedback.
Sampling and Data Collection of the Survey
Survey participants consisted of 2 groups of clinicians: (1) medical trainees that included medical residents, medical interns, and clinical fellows, and (2) nursing staff that included part‐time and full‐time nurses. To qualify for inclusion, participants had to have used the CM system for at least a month prior to administration of the questionnaire.
Data Analysis
Responses were recorded into an Excel spreadsheet that was imported into SPSS for analysis. Categorical variables were described using proportions. Survey comments were grouped into common themes, and themes mentioned by more than 1 respondent were reported.
RESULTS
Usage Analysis
A total of 60,969 messages were sent using CM between May 2, 2011 and August 19, 2012. On average, a team would receive 14.8 messages per day. Of all messages, 76.5% requested a text reply, 7.7% requested a call‐back, and 15.7% did not request a response. More than two‐thirds of messages at both hospitals were sent as immediate. Of the nonurgent messages, 86% were not replied to within the desired time, requiring a repeat message to be sent. Examples of different types of messages are shown in Table 1.
| Sender | Issue | Details | Priority | Desired Response Type | Time Created | Time Sent | Reply | Time Replied |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| Nurse | Vital sign | Pt's BP is 182/95, HR is 108 now. Previous at 0800 was 165/78; HR was 99. PT is not on antihypertensive meds. | Allow time to respond (23:00) | Text reply | 21:43 | 23:02 | OK. Will assess. | 23:03 |
| Nurse | NG tube | NG tube is in place. Can you please enter portable chest x‐ray to check placement ASAP? | Immediate | Text reply | 16:58 | 16:58 | Will do. | 17:00 |
| Nurse | Bloodwork | Pt creat=216. Pt has NS @ 75 cc/hr. Pt has noted crackles throughout lung fields and has productive cough; eating and drinking well. Would you like it continued as well? Pt O2Sat 93% RA; would you like 4 L of O2 continued? Pls call for telephone order. | Immediate | Call back | 12:53 | 13:04 | Dealt with it on phone. | 13:05 |
| Nurse | Pain control | Hello! Pt has been getting 1 mg hydromorphone IV q 1 hr and pain is still not controlled. Pt remains awake and alert. Thanks! | Immediate | Info only | 15:41 | 15:41 | Thank you. | 15:42 |
For messages requesting a text reply, 8.6% did not receive a reply. The median response time was 2.3 minutes (interquartile range of 5.8 minutes), but some messages did not receive a response even after a week, which skewed the distribution of response times. For those messages that did receive a reply, 68.9% of them were responded to within 5 minutes, and 84.5% were responded to within 15 minutes. Messages were predominantly received between 9 am and midnight (see Supporting Figure 1 in the online version of this article). Because the sending of some messages was delayed, there appeared to be fewer messages received during protected educational times (89 am and 121 pm) as well as between midnight and 7 am compared to other times.
Survey Results
Between April 2013 and June 2013, 82 of 86 medical trainees (95.3%) and 83 of 116 nurses (71.6%) completed the survey, for an overall response rate of 81.7%. Clinicians perceived that CM appeared to have a positive impact on efficiency. In particular, 82.8% of physicians and 78.3% of nurses agreed or strongly agreed that CM helped speed up daily work tasks (Table 2). The majority of physicians and nurses agreed that the system increased accountability, increased timeliness of communication, and improved interprofessional relationships. It was not seen to be effective for communicating complex patient issues.
| No. of Subitems in Survey | Physician (% Agree, Strongly Agree), n=82 | Nurse (% Agree, Strongly Agree), n=83 | |
|---|---|---|---|
| |||
| Positive impact on efficiency. | 7 | 58.9% | 66.6% |
| The CM system helps speed up my daily work tasks. | 82.8% | 78.3% | |
| Positive impact on physician‐nurse collaboration. | 6 | 55.3% | 58.5% |
| The CM system increases the amount of communication between nurses and physicians. | 50.6% | 67.1% | |
| Improved timeliness of communication. | 5 | 54.2% | 50.5% |
| Communication through the CM system helps me resolve patient issues within the appropriate time frames. | 66.7% | 55.6% | |
| Increased accountability. | 2 | 67.1% | 73.2% |
| Improved accuracy of communications. | 3 | 41.6% | 50.7% |
| Improved interprofessional relationships. | 2 | 62.2% | 53.6% |
| Increased verbal communications. | 2 | 35.1% | 25.3% |
| Richness of the communication medium. | 6 | 40.7% | 48.3% |
| I find the CM system useful for communicating complex patient issues. | 35.8% | 26.3% | |
| I would prefer CM over standard hospital communication methods such as numeric paging. | 1 | 68.3% | 76.5% |
| I enjoy using the CM system for clinical communication on the wards. | 1 | 63.0% | 79.0% |
| Communication through the CM system helps to reduce interruptions for physicians. | 1 | 45.7% | |
Survey comments revealed that nurses perceived a lack of desired response, whereas physicians noted being interrupted with low‐value information through the system (Table 3). Both commented that further functionality, such as an active message stream, would be of benefit. Difficulty in communicating complex issues was also noted.
| Issue | Occurrences | Example | ||
|---|---|---|---|---|
| MD | RN | Total | ||
| ||||
| Lack of response | 1 | 10 | 11 | It depends if they respond quickly or not. A few times I send the 2nd message to remind them of the issue. I also spend more time to check if they answer it or not. I even call their Blackberries at last to get a response. |
| Message stream | 3 | 4 | 7 | I wish that I could see follow‐up messages after my initial reply (ie, it would be nice to have an open message stream). |
| Difficult to communicate complex issues | 1 | 5 | 6 | Difficult to communicate complex issues. Takes a lot of time to respond, and it becomes inefficient when responding to nonurgent CM because it interrupts workflow. |
| Many messages are low‐value interrupts | 3 | 0 | 3 | CM is useful for handover between clinicians, but often it slows down the clinician when they are used for information‐related low‐value/noncritical messages between nurses and clinicians |
| Lack of detailed response | 0 | 3 | 3 | Specific messages regarding response to care is required most times. For example, acknowledged is not a favorable response. |
| Technical issues | 2 | 0 | 2 | I find CM very useful. We have had multiple issues with our Blackberry this month, and CM was not working. When it is up and running, however, it is a wonderful tool. |
| Discrepancy in perceived urgency | 2 | 0 | 2 | Discrepancy between what nurses find urgent and what we find urgent. |
DISCUSSION
We describe an implementation of a system to improve clinical communication in hospitals. The system was highly used and was perceived to improve communication by both nurses and physicians. Specifically, users found that the system increased efficiency, accountability, timeliness, and collaboration, but that there were issues with message clarity for complex medical issues.
Other systems and approaches have been implemented to improve communication. These included the use of alphanumeric pagers, e‐mail, secure texting, and smartphones. There is evidence that more advanced systems can improve efficiency for senders.[16] A recent randomized trial of secure text messaging found that it was perceived to be more efficient than paging, but overall usage was low and inconsistent.[8] There is also evidence that smartphones may increase interruptions, worsen interprofessional relationships, and cause issues with professional behavior.[10] Unfortunately, there are a limited number of interventions that improve communication, with some improving efficiency but none demonstrating improved patient‐oriented outcomes.[16, 17] This study evaluated a novel system, with functionality to link communication to patients, and created a system that aligned with the workflow of the clinicians. Messages were linked to the patient, not the sender or receiver, so other clinicians in the patient's circle of care could easily view the communication. Moreover, the system was designed to improve message response rates and allow for nonurgent messages.
Our communication system uses standard, commercially available components (smartphones, SMS), and relatively basic functionality (handover, secure messaging). Important findings are that the current system of paging can be transformed to a more efficient system that users will readily adopt. We found positive effects with components of the system. It appeared to improve efficiency and increase accountability. Accountability is crucial and moves from undocumented conversation to fully documented details of interactions. This can be used for both incident review and to review for quality improvement.
Using the system, physicians perceived that they were bothered by low‐value information, whereas nurses perceived a lack of response, and both found that the system was not ideal for complex messages. The mismatch between what physicians and nurses perceive as important has been attributed to their different timeframes and context.[18] For nurses with an upcoming change of shift, they wanted resolution of issues before handover. A physician on a different ward may not appreciate the context of a nurse having to directly interact with an irate family member. These different perceptions likely contributed to the lack of response to 8.6% of text messages. This is still better than other systems, such as paging, which can be as high as 33%.[10] For nonurgent items, clinicians would ideally check and clear items regularly from the system using a desktop computer, responding within the allotted timeframe. Unfortunately, this never became part of routine physician workflow, likely due to their busy workload, so many physicians would only respond when items became overdue. However, having a method to deal with nonurgent messages may have prevented some interruptions during protected educational times of trainees. The system was also not ideal for urgent or complex items. Complex items can be difficult to convey using the rarified communication medium of text messages.[19, 20] Urgent or complex issues are likely best resolved with a face‐to‐face or telephone conversation.
There are several limitations in our study that should be considered when interpreting the results. It is a study of usage and perceptions after implementation. Although more rigorous study is required to evaluate the effects, we see this as a first step in process improvement. Future research should measure the impact on improving patient care of this system and on patient outcomes such as adverse events. The study and intervention was limited to general internal medicine wards in 2 academic hospital settings where there are frequent rotations of medical personnel. The findings may not be generalizable to other hospital settings.
Future directions should be to further improve on the communication system and to educate and train staff on how to effectively communicate. Survey results showed that although users perceived increased efficiency, there was still significant opportunity to improve. One way to improve would be to have a mobile application in which physicians can easily review nonurgent items. Improvements could also be realized by educating clinicians on the use of the system and providing immediate feedback. Providing feedback to physicians on how well they respond could address nurses' issues around lack of timely response. By creating consensus between nurses and physicians on what is of high and low value to communicate could increase satisfaction for all users.
In summary, we present the usage and perceptions of a system designed to improve hospital communication. We found that there was high uptake, and that users perceived it to improve efficiency, collaboration, and accountability, but it may not be useful for communicating complex issues.
ACKNOWLEDGEMENTS
The authors acknowledge the nurses, physicians, residents, and other health professions on the general internal medicine ward for their patience and support as we continue to try to innovate. The authors also acknowledge the members of the information systems department (Shared Information Management Systems, University Health Network) who helped to support the Communication System, and the software developer, QRS, that helped to codevelop the software system.
Disclosures: The hospital was in a codevelopment agreement that has since terminated. No researcher or hospital received any funds from private industry for any purpose including personal or research. The authors report no conflicts of interest.
Previous studies have advocated the importance of effective communication between clinicians as a critical component in the provision of high‐quality patient care.[1, 2, 3, 4] There is increasing interest in the use of information and communication technologies to improve how clinicians communicate in hospital settings. A number of hospitals have implemented different solutions to improve communication. These solutions include alphanumeric pagers,[5] smartphones,[6] e‐mail,[7] secure text messaging,[8] and a Web‐based interdisciplinary communication tool.[9]
These systems have different limitations that render them inefficient and likely inhibit collaborative care. Current systems, such as pagers, rely on the sender to ensure the message was received and are successful in delivering messages approximately 67% of the time.[5, 9, 10] Although alphanumeric pagers and secure text messaging can increase the likelihood of delivery, these messages are often isolated and not easily viewable by the whole care team.[11] Improved systems should also reduce unnecessary interruptions by providing support for both urgent and delayed messages. Finally, messages should be stored and retrievable to enable increased accountability and allow for review for quality improvement initiatives.
It is also important to consider the unintended consequences of technology implementations.[12] Moving communication to text messages and smartphones has the potential to reduce interprofessional relations and can increase confusion if used for complex issues.[10, 13] In this article, we present a system designed to improve interprofessional communication on general internal medicine wards by incorporating these desired features and describe the usage and attitudes toward the system, specifically assessing for effects on multiple domains including efficiency, interprofessional collaboration, and relationships.
METHODS
Research Question
Will nurses and physicians use a system designed to improve interprofessional communication and will they perceive it to be effective and improve workflow?
Setting
The study took place on the general internal medicine wards at Toronto General Hospital and Toronto Western Hospital, 2 large academic teaching hospitals. There are several general internal medicine wards at each site with approximately 80 beds at each site. At each site there are 4 clinical teaching units and 1 hospitalist team. The study was approved by the research ethics board at the University Health Network.
Intervention
To address issues with communication, we developed a systemClinical Message (CM)that included 2 main components: a physician handover tool and secure messaging module. The focus of CM was to improve communication and information flow among different healthcare providers (physicians, nurses, pharmacists, social workers and therapists) through a secure, shared platform.
Physician Handover
The physician handover tool was designed to facilitate the physician handover process at shift change and is used as a patient rounding tool for day‐to‐day management of patients. It is also accessed by nurses and other clinicians to view the physicians' notes and to stay informed on the overall care plan. The tool contains standard elements including a list of patients with the following information on each patient: demographics, diagnosis, code status, medical history, active issues, and discharge plans (Figure 1).
Secure Messaging
Secure messaging was designed around our dominant communication: nurses sending messages to physicians who would then respond. Nurses and other health professionals sent messages to the medical teams by accessing CM, selecting the appropriate patient, and filling out a message template. The system automatically populated the To field with the team assigned to the selected patient. Messaging for each team was centralized around a single team smartphone that was carried 24 hours a day, 7 days a week by a physician on that team. This removed the guesswork of trying to identify the individual physician responsible for that patient. For each message, a subject or issue and content were entered (Figure 2). Logic was also incorporated to reduce the amount of unnecessary interruptions. Senders would choose to send the message immediately as an interrupt message (urgent) for urgent/time sensitive issues or as an allow time to respond message (delayed). For the latter, the message was posted to the system where physicians could check and answer them. Interrupt messages were sent to the team smartphone using the Short Message Service (SMS) protocol. To try and ensure the communication loop on any issues was closed, when a message requested a response and did not receive it, the system sent another message. For urgent messages, a repeat message was initiated after 15 minutes. For delayed messages, the sender defined when they needed a response, typically within 2 to 8 hours. Senders were also able to select the mode of response that would best meet their needs from a workflow perspective: call back, text reply, or to specify that a reply was not required. Senders were also able to verify if the messages were received by the physician's smartphone. Physicians could view the messages within CM and reply. For messages that went to their team smartphone, physicians could respond from the smartphone through a secure Web link.
Because the messages were linked to the patients, they were visible to the entire care team, not just the message sender and recipient. If the care of the patient was transferred from 1 clinician to the next, the new clinician could easily review prior messages to understand recent patient events. The system was accessible through a browser on the intranet. The system regularly pulled patient demographic details such as name, age, medical record number, and location from our electronic medical record through a 1‐way interface. Information from this communication system was not considered part of the medical record but was retrievable.
The system was introduced as the new standard method of communication for nurses to reach physicians for all of the general internal medicine wards and for all medical teams at site 1 on May 2, 2011 and site 2 on June 6, 2011. The system replaced a text‐based Web‐paging system and supplemented the numeric pager carried by residents. Initial training of a half hour was provided to all nurses and residents.
Message Analysis for Usage Statistics
We analyzed messages created and sent via the CM system from May 2011 until August 2012. The extracted message information included date and time sent, issue, level of urgency, response type requested, roles of clinicians involved from the associated team, hospital site (senders and receivers), and message details. The following inclusion criteria were used for the analyses: (1) the senders and receivers of the messages could not be CM support staff, and (2) the messages sent were intended for the team smartphones used by the respective medical teams, not individual clinicians. Descriptive statistics and frequency analysis were performed using Microsoft Excel (Microsoft Corp., Redmond, WA) and IBM SPSS (IBM, Armonk, NY).
Survey
Development of the Survey
We used standard methods to develop a survey to assess staff perceptions on the impact of the new communication system. Relevant questionnaire items were compiled from a systematic review of the literature for communication surveys and communication issues that included the following domains: efficiency, accountability, accuracy, collaboration, timeliness, richness of the communication medium, and impact on interprofessional relationships and verbal communication.[10, 14, 15] We carried out pilot testing with 5 nurses and physicians, and modified the questionnaires based on their feedback.
Sampling and Data Collection of the Survey
Survey participants consisted of 2 groups of clinicians: (1) medical trainees that included medical residents, medical interns, and clinical fellows, and (2) nursing staff that included part‐time and full‐time nurses. To qualify for inclusion, participants had to have used the CM system for at least a month prior to administration of the questionnaire.
Data Analysis
Responses were recorded into an Excel spreadsheet that was imported into SPSS for analysis. Categorical variables were described using proportions. Survey comments were grouped into common themes, and themes mentioned by more than 1 respondent were reported.
RESULTS
Usage Analysis
A total of 60,969 messages were sent using CM between May 2, 2011 and August 19, 2012. On average, a team would receive 14.8 messages per day. Of all messages, 76.5% requested a text reply, 7.7% requested a call‐back, and 15.7% did not request a response. More than two‐thirds of messages at both hospitals were sent as immediate. Of the nonurgent messages, 86% were not replied to within the desired time, requiring a repeat message to be sent. Examples of different types of messages are shown in Table 1.
| Sender | Issue | Details | Priority | Desired Response Type | Time Created | Time Sent | Reply | Time Replied |
|---|---|---|---|---|---|---|---|---|
| ||||||||
| Nurse | Vital sign | Pt's BP is 182/95, HR is 108 now. Previous at 0800 was 165/78; HR was 99. PT is not on antihypertensive meds. | Allow time to respond (23:00) | Text reply | 21:43 | 23:02 | OK. Will assess. | 23:03 |
| Nurse | NG tube | NG tube is in place. Can you please enter portable chest x‐ray to check placement ASAP? | Immediate | Text reply | 16:58 | 16:58 | Will do. | 17:00 |
| Nurse | Bloodwork | Pt creat=216. Pt has NS @ 75 cc/hr. Pt has noted crackles throughout lung fields and has productive cough; eating and drinking well. Would you like it continued as well? Pt O2Sat 93% RA; would you like 4 L of O2 continued? Pls call for telephone order. | Immediate | Call back | 12:53 | 13:04 | Dealt with it on phone. | 13:05 |
| Nurse | Pain control | Hello! Pt has been getting 1 mg hydromorphone IV q 1 hr and pain is still not controlled. Pt remains awake and alert. Thanks! | Immediate | Info only | 15:41 | 15:41 | Thank you. | 15:42 |
For messages requesting a text reply, 8.6% did not receive a reply. The median response time was 2.3 minutes (interquartile range of 5.8 minutes), but some messages did not receive a response even after a week, which skewed the distribution of response times. For those messages that did receive a reply, 68.9% of them were responded to within 5 minutes, and 84.5% were responded to within 15 minutes. Messages were predominantly received between 9 am and midnight (see Supporting Figure 1 in the online version of this article). Because the sending of some messages was delayed, there appeared to be fewer messages received during protected educational times (89 am and 121 pm) as well as between midnight and 7 am compared to other times.
Survey Results
Between April 2013 and June 2013, 82 of 86 medical trainees (95.3%) and 83 of 116 nurses (71.6%) completed the survey, for an overall response rate of 81.7%. Clinicians perceived that CM appeared to have a positive impact on efficiency. In particular, 82.8% of physicians and 78.3% of nurses agreed or strongly agreed that CM helped speed up daily work tasks (Table 2). The majority of physicians and nurses agreed that the system increased accountability, increased timeliness of communication, and improved interprofessional relationships. It was not seen to be effective for communicating complex patient issues.
| No. of Subitems in Survey | Physician (% Agree, Strongly Agree), n=82 | Nurse (% Agree, Strongly Agree), n=83 | |
|---|---|---|---|
| |||
| Positive impact on efficiency. | 7 | 58.9% | 66.6% |
| The CM system helps speed up my daily work tasks. | 82.8% | 78.3% | |
| Positive impact on physician‐nurse collaboration. | 6 | 55.3% | 58.5% |
| The CM system increases the amount of communication between nurses and physicians. | 50.6% | 67.1% | |
| Improved timeliness of communication. | 5 | 54.2% | 50.5% |
| Communication through the CM system helps me resolve patient issues within the appropriate time frames. | 66.7% | 55.6% | |
| Increased accountability. | 2 | 67.1% | 73.2% |
| Improved accuracy of communications. | 3 | 41.6% | 50.7% |
| Improved interprofessional relationships. | 2 | 62.2% | 53.6% |
| Increased verbal communications. | 2 | 35.1% | 25.3% |
| Richness of the communication medium. | 6 | 40.7% | 48.3% |
| I find the CM system useful for communicating complex patient issues. | 35.8% | 26.3% | |
| I would prefer CM over standard hospital communication methods such as numeric paging. | 1 | 68.3% | 76.5% |
| I enjoy using the CM system for clinical communication on the wards. | 1 | 63.0% | 79.0% |
| Communication through the CM system helps to reduce interruptions for physicians. | 1 | 45.7% | |
Survey comments revealed that nurses perceived a lack of desired response, whereas physicians noted being interrupted with low‐value information through the system (Table 3). Both commented that further functionality, such as an active message stream, would be of benefit. Difficulty in communicating complex issues was also noted.
| Issue | Occurrences | Example | ||
|---|---|---|---|---|
| MD | RN | Total | ||
| ||||
| Lack of response | 1 | 10 | 11 | It depends if they respond quickly or not. A few times I send the 2nd message to remind them of the issue. I also spend more time to check if they answer it or not. I even call their Blackberries at last to get a response. |
| Message stream | 3 | 4 | 7 | I wish that I could see follow‐up messages after my initial reply (ie, it would be nice to have an open message stream). |
| Difficult to communicate complex issues | 1 | 5 | 6 | Difficult to communicate complex issues. Takes a lot of time to respond, and it becomes inefficient when responding to nonurgent CM because it interrupts workflow. |
| Many messages are low‐value interrupts | 3 | 0 | 3 | CM is useful for handover between clinicians, but often it slows down the clinician when they are used for information‐related low‐value/noncritical messages between nurses and clinicians |
| Lack of detailed response | 0 | 3 | 3 | Specific messages regarding response to care is required most times. For example, acknowledged is not a favorable response. |
| Technical issues | 2 | 0 | 2 | I find CM very useful. We have had multiple issues with our Blackberry this month, and CM was not working. When it is up and running, however, it is a wonderful tool. |
| Discrepancy in perceived urgency | 2 | 0 | 2 | Discrepancy between what nurses find urgent and what we find urgent. |
DISCUSSION
We describe an implementation of a system to improve clinical communication in hospitals. The system was highly used and was perceived to improve communication by both nurses and physicians. Specifically, users found that the system increased efficiency, accountability, timeliness, and collaboration, but that there were issues with message clarity for complex medical issues.
Other systems and approaches have been implemented to improve communication. These included the use of alphanumeric pagers, e‐mail, secure texting, and smartphones. There is evidence that more advanced systems can improve efficiency for senders.[16] A recent randomized trial of secure text messaging found that it was perceived to be more efficient than paging, but overall usage was low and inconsistent.[8] There is also evidence that smartphones may increase interruptions, worsen interprofessional relationships, and cause issues with professional behavior.[10] Unfortunately, there are a limited number of interventions that improve communication, with some improving efficiency but none demonstrating improved patient‐oriented outcomes.[16, 17] This study evaluated a novel system, with functionality to link communication to patients, and created a system that aligned with the workflow of the clinicians. Messages were linked to the patient, not the sender or receiver, so other clinicians in the patient's circle of care could easily view the communication. Moreover, the system was designed to improve message response rates and allow for nonurgent messages.
Our communication system uses standard, commercially available components (smartphones, SMS), and relatively basic functionality (handover, secure messaging). Important findings are that the current system of paging can be transformed to a more efficient system that users will readily adopt. We found positive effects with components of the system. It appeared to improve efficiency and increase accountability. Accountability is crucial and moves from undocumented conversation to fully documented details of interactions. This can be used for both incident review and to review for quality improvement.
Using the system, physicians perceived that they were bothered by low‐value information, whereas nurses perceived a lack of response, and both found that the system was not ideal for complex messages. The mismatch between what physicians and nurses perceive as important has been attributed to their different timeframes and context.[18] For nurses with an upcoming change of shift, they wanted resolution of issues before handover. A physician on a different ward may not appreciate the context of a nurse having to directly interact with an irate family member. These different perceptions likely contributed to the lack of response to 8.6% of text messages. This is still better than other systems, such as paging, which can be as high as 33%.[10] For nonurgent items, clinicians would ideally check and clear items regularly from the system using a desktop computer, responding within the allotted timeframe. Unfortunately, this never became part of routine physician workflow, likely due to their busy workload, so many physicians would only respond when items became overdue. However, having a method to deal with nonurgent messages may have prevented some interruptions during protected educational times of trainees. The system was also not ideal for urgent or complex items. Complex items can be difficult to convey using the rarified communication medium of text messages.[19, 20] Urgent or complex issues are likely best resolved with a face‐to‐face or telephone conversation.
There are several limitations in our study that should be considered when interpreting the results. It is a study of usage and perceptions after implementation. Although more rigorous study is required to evaluate the effects, we see this as a first step in process improvement. Future research should measure the impact on improving patient care of this system and on patient outcomes such as adverse events. The study and intervention was limited to general internal medicine wards in 2 academic hospital settings where there are frequent rotations of medical personnel. The findings may not be generalizable to other hospital settings.
Future directions should be to further improve on the communication system and to educate and train staff on how to effectively communicate. Survey results showed that although users perceived increased efficiency, there was still significant opportunity to improve. One way to improve would be to have a mobile application in which physicians can easily review nonurgent items. Improvements could also be realized by educating clinicians on the use of the system and providing immediate feedback. Providing feedback to physicians on how well they respond could address nurses' issues around lack of timely response. By creating consensus between nurses and physicians on what is of high and low value to communicate could increase satisfaction for all users.
In summary, we present the usage and perceptions of a system designed to improve hospital communication. We found that there was high uptake, and that users perceived it to improve efficiency, collaboration, and accountability, but it may not be useful for communicating complex issues.
ACKNOWLEDGEMENTS
The authors acknowledge the nurses, physicians, residents, and other health professions on the general internal medicine ward for their patience and support as we continue to try to innovate. The authors also acknowledge the members of the information systems department (Shared Information Management Systems, University Health Network) who helped to support the Communication System, and the software developer, QRS, that helped to codevelop the software system.
Disclosures: The hospital was in a codevelopment agreement that has since terminated. No researcher or hospital received any funds from private industry for any purpose including personal or research. The authors report no conflicts of interest.
- . When conversation is better than computation. J Am Med Inform Assoc. 2000;7(3):277–286.
- , , , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324(6):370–376.
- , , , et al. Gaps in pediatric clinician communication and opportunities for improvement. J Healthc Qual. 2008;30(5):43–54.
- , , , , . Quality in Australian health care study. Med J Aust. 1996;164(12):754.
- , , , . Implementation and evaluation of an alphanumeric paging system on a resident inpatient teaching service. J Hosp Med. 2009;4(8):E34–E40.
- , , , et al. Demonstrating the BlackBerry as a clinical communication tool: a pilot study conducted through the Centre for Innovation in Complex Care. Healthc Q. 2008;11(4):94–98.
- , , , . The use of wireless email to improve healthcare team communication. J Am Med Inform Assoc. 2009;16(5):705–713.
- , , , , , . Smarter hospital communication: secure smartphone text messaging improves provider satisfaction and perception of efficacy, workflow. J Hosp Med. 2014;9(9):573–578.
- , , , , . Beyond paging: building a web‐based communication tool for nurses and physicians. J Gen Intern Med. 2009;24(1):105–110.
- , , , et al. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. J Am Med Inform Assoc. 2013;20(4):766–777.
- , , , et al. Improving hospital care and collaborative communications for the 21st century: key recommendations for general internal medicine. Interact J Med Res. 2012;1(2):e9.
- , , , , , . Anticipating and addressing the unintended consequences of health IT and policy: a report from the AMIA 2009 Health Policy Meeting. J Am Med Inform Assoc. 2011;18(1):82–90.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- , , , , . Organizational assessment in intensive care units (ICUs): construct development, reliability, and validity of the ICU nurse‐physician questionnaire. Med Care. 1991;29(8):709–726.
- . Impact of communication medium on task performance and satisfaction: an examination of media‐richness theory. Inform Manag. 1999;35:295–312.
- , , , et al. Effects of clinical communication interventions in hospitals: a systematic review of information and communication technology adoptions for improved communication between clinicians. Int J Med Inform. 2012;81(11):723–732.
- , , , et al. Provider‐to‐provider electronic communication in the era of meaningful use: a review of the evidence. J Hosp Med. 2013;8(10):589–597.
- , , , et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82(5):378–386.
- , , , , , . Short message service or disService: issues with text messaging in a complex medical environment. Int J Med Inform. 2014;83(4):278–284.
- , , . Instant messaging at the hospital: supporting articulation work? Int J Med Inform. 2013;82(9):753–761.
- . When conversation is better than computation. J Am Med Inform Assoc. 2000;7(3):277–286.
- , , , et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Engl J Med. 1991;324(6):370–376.
- , , , et al. Gaps in pediatric clinician communication and opportunities for improvement. J Healthc Qual. 2008;30(5):43–54.
- , , , , . Quality in Australian health care study. Med J Aust. 1996;164(12):754.
- , , , . Implementation and evaluation of an alphanumeric paging system on a resident inpatient teaching service. J Hosp Med. 2009;4(8):E34–E40.
- , , , et al. Demonstrating the BlackBerry as a clinical communication tool: a pilot study conducted through the Centre for Innovation in Complex Care. Healthc Q. 2008;11(4):94–98.
- , , , . The use of wireless email to improve healthcare team communication. J Am Med Inform Assoc. 2009;16(5):705–713.
- , , , , , . Smarter hospital communication: secure smartphone text messaging improves provider satisfaction and perception of efficacy, workflow. J Hosp Med. 2014;9(9):573–578.
- , , , , . Beyond paging: building a web‐based communication tool for nurses and physicians. J Gen Intern Med. 2009;24(1):105–110.
- , , , et al. The intended and unintended consequences of communication systems on general internal medicine inpatient care delivery: a prospective observational case study of five teaching hospitals. J Am Med Inform Assoc. 2013;20(4):766–777.
- , , , et al. Improving hospital care and collaborative communications for the 21st century: key recommendations for general internal medicine. Interact J Med Res. 2012;1(2):e9.
- , , , , , . Anticipating and addressing the unintended consequences of health IT and policy: a report from the AMIA 2009 Health Policy Meeting. J Am Med Inform Assoc. 2011;18(1):82–90.
- , , , et al. An evaluation of the use of smartphones to communicate between clinicians: a mixed‐methods study. J Med Internet Res. 2011;13(3):e59.
- , , , , . Organizational assessment in intensive care units (ICUs): construct development, reliability, and validity of the ICU nurse‐physician questionnaire. Med Care. 1991;29(8):709–726.
- . Impact of communication medium on task performance and satisfaction: an examination of media‐richness theory. Inform Manag. 1999;35:295–312.
- , , , et al. Effects of clinical communication interventions in hospitals: a systematic review of information and communication technology adoptions for improved communication between clinicians. Int J Med Inform. 2012;81(11):723–732.
- , , , et al. Provider‐to‐provider electronic communication in the era of meaningful use: a review of the evidence. J Hosp Med. 2013;8(10):589–597.
- , , , et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82(5):378–386.
- , , , , , . Short message service or disService: issues with text messaging in a complex medical environment. Int J Med Inform. 2014;83(4):278–284.
- , , . Instant messaging at the hospital: supporting articulation work? Int J Med Inform. 2013;82(9):753–761.
© 2014 Society of Hospital Medicine