User login
Easing the discomfort of a speculum exam
Put lubricating gel, not water, on the speculum every time you do a pelvic exam.1
STRENGTH OF RECOMMENDATION
B: Based on one good-quality, randomized controlled trial (RCT).
Hill DA, Lamvu G. Effect of lubricating gel on patient comfort during vaginal speculum examination. Obstet Gynecol. 2012;119(2 pt 1): 227-231.
ILLUSTRATIVE CASE
A 24-year-old woman comes in for an annual exam, including Pap smear and testing for sexually transmitted diseases (STD). She tells you how painful her previous speculum exam was and how worried she is about having another. Should you apply lubricating gel or water to the speculum before vaginal insertion to ease her discomfort?
Physiology teaches us that vaginal entry requires lubrication. But traditional teaching has held that lubricating gel on a speculum can interfere with the results of a Pap smear and chlamydia tesing.2 Pelvic exams performed without lubricating gel on the speculum can cause significant discomfort—possibly bad enough to prevent some women from undergoing the recommended screening tests.3
Until now, we’ve only evaluated gel’s impact on test results
Studies comparing lubricating gel and water have conclusively shown that a small amount of gel, used on the outside of the speculum blades, does not interfere with either Pap testing or detection of Chlamydia trachomatis.4,5 One liquid-based cytology manufacturer, however, discourages the use of lubricants with “carbomers” or “carbopol polymers,” but states that water-based lubricants have not been shown to interfere with Pap smear results.6 No studies have evaluated lubricants from a patient perspective—until now.
STUDY SUMMARY: Lubricating gel eases discomfort
The study by Hill and Lamvu was a 6-month, single-blind, randomized trial of women ages 18 to 50 years who sought care at an Orlando, Florida obstetrics and gynecology department for conditions requiring vaginal speculum examination.1 The study excluded women who might have an altered perception of pain during speculum insertion— those who were menopausal, pregnant, or within 6 weeks’ postpartum; had dyspareunia, vaginitis, vulvar pain, or vulvar lesions; were undergoing a procedure; or had never had vaginal intercourse. Women who were not fluent in English were excluded, as well.
The study included 120 women who underwent computer-generated randomization into 2 groups with no marked differences in demographics. A single examiner did all the speculum exams, using a standard protocol with a medium-size Graves speculum. The examiner applied 0.3 mL water-based lubricating gel to the speculum before insertion for the women in one group, and used 3 mL water for the other.
Immediately after the speculum was inserted and opened—before the examiner attempted to visualize the cervix—patients were given a visual analog scale and told to indicate the level of pain with insertion, using a scale of 0 (no pain) to 10 (the worst pain imaginable). The gel group had lower pain scores for speculum insertion compared with the water group (1.41±1.55 vs 2.15±1.93; P<.01), a statistically significant difference of 0.74. Twenty of the 59 patients in the gel group (33.9%) rated their pain as 0, compared with 6 of 60 (10%) in the water group (P=.002). Although pain, rather than sampling quality, was the primary outcome of the study, the authors also reported that all of the women who underwent Pap screening (73) had adequate cytology.
WHAT’S NEW?: It’s time for lubrication to become standard practice
This trial is the first to study speculum lubrication from this patient-oriented outcome, and to show that women experience less pain when lubricating gel is applied to the speculum, rather than water. This knowledge, combined with previous studies showing that a small amount of water-based lubricating gel does not interfere with liquid-based cytology or chlamydia test results, should make the use of lubricating gel standard practice when performing speculum examinations.
CAVEATS: We see no downside
The exclusion criteria of this study were meant to eliminate women who had an altered pain perception that could skew study results. Yet those who met the exclusion criteria may also benefit from a pelvic exam with gel lubrication. We see no harm in trying a small amount of lubricant when examining them, as well.
In addition, the study did not compare various types and sizes of specula. However, we see no reason why the benefit of a gel lubricant would be limited to the type of speculum used by the examiner.
Studies in emergency departments that have used visual analog scales to measure interventions that decrease pain have used a 0.9 mean difference as “clinically meaningful.”7,8 By that criteria, the 0.74 difference observed in this study does not rise to the level of clinical meaningfulness. However, one in 3 patients in the gel group marked 0 on the pain scale, indicating that they had no pain, vs only one in 10 in the water group. We believe that the higher proportion of women experiencing no pain and the mean difference of 0.74 on the pain scale (both statistically significant), combined with the lack of risk associated with the use of a water-based lubricant, makes this a clinically useful practice changer.
CHALLENGES TO IMPLEMENTATION: There aren’t any
Other than clinical inertia, we see no challenges to the implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National center for Research Resources, a clinical Translational Science Award to the University of chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National center for Research Resources or the National Institutes of health.
1. Hill DA, Lamvu G. Effect of lubricating gel on patient comfort during vaginal speculum examination. Obstet Gynecol. 2012;119 (2 pt 1):227-231.
2. Harmanli O, Jones KA. Using lubricant for speculum insertion. Obstet Gynecol. 2010;116:415-417.
3. Hoyo C, Yarnall KSH, Skinner CS, et al. Pain predicts non-adherence to pap smear screening among middle-aged African American women. Prev Med. 2005;41:439-445.
4. Amies AE, Miller L, Lee S, et al. The effect of vaginal speculum lubrication on the rate of unsatisfactory cervical cytology diagnosis. Obstet Gynecol. 2002;100:889-892.
5. Griffith WF, Stuart GS, Gluck KL, et al. Vaginal speculum lubrication and its effects on cervical cytology and microbiology. Contraception. 2005;72:60-604.
6. Evantash E. Lubricant use during Pap test collection. Bedford, Mass: Hologic, Inc; 2009. Available at: www.thinprep.com/pdfs/Lubricant_Letter_Rev_3.doc. Accessed June 8, 2012.
7. Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med. 2001;8:1153-1157.
8. Kelly AM. Does the clinically significant difference in visual analog scale pain scores vary with gender, age, or cause of pain? Acad Emerg Med. 1998;5:1086-1090.
Put lubricating gel, not water, on the speculum every time you do a pelvic exam.1
STRENGTH OF RECOMMENDATION
B: Based on one good-quality, randomized controlled trial (RCT).
Hill DA, Lamvu G. Effect of lubricating gel on patient comfort during vaginal speculum examination. Obstet Gynecol. 2012;119(2 pt 1): 227-231.
ILLUSTRATIVE CASE
A 24-year-old woman comes in for an annual exam, including Pap smear and testing for sexually transmitted diseases (STD). She tells you how painful her previous speculum exam was and how worried she is about having another. Should you apply lubricating gel or water to the speculum before vaginal insertion to ease her discomfort?
Physiology teaches us that vaginal entry requires lubrication. But traditional teaching has held that lubricating gel on a speculum can interfere with the results of a Pap smear and chlamydia tesing.2 Pelvic exams performed without lubricating gel on the speculum can cause significant discomfort—possibly bad enough to prevent some women from undergoing the recommended screening tests.3
Until now, we’ve only evaluated gel’s impact on test results
Studies comparing lubricating gel and water have conclusively shown that a small amount of gel, used on the outside of the speculum blades, does not interfere with either Pap testing or detection of Chlamydia trachomatis.4,5 One liquid-based cytology manufacturer, however, discourages the use of lubricants with “carbomers” or “carbopol polymers,” but states that water-based lubricants have not been shown to interfere with Pap smear results.6 No studies have evaluated lubricants from a patient perspective—until now.
STUDY SUMMARY: Lubricating gel eases discomfort
The study by Hill and Lamvu was a 6-month, single-blind, randomized trial of women ages 18 to 50 years who sought care at an Orlando, Florida obstetrics and gynecology department for conditions requiring vaginal speculum examination.1 The study excluded women who might have an altered perception of pain during speculum insertion— those who were menopausal, pregnant, or within 6 weeks’ postpartum; had dyspareunia, vaginitis, vulvar pain, or vulvar lesions; were undergoing a procedure; or had never had vaginal intercourse. Women who were not fluent in English were excluded, as well.
The study included 120 women who underwent computer-generated randomization into 2 groups with no marked differences in demographics. A single examiner did all the speculum exams, using a standard protocol with a medium-size Graves speculum. The examiner applied 0.3 mL water-based lubricating gel to the speculum before insertion for the women in one group, and used 3 mL water for the other.
Immediately after the speculum was inserted and opened—before the examiner attempted to visualize the cervix—patients were given a visual analog scale and told to indicate the level of pain with insertion, using a scale of 0 (no pain) to 10 (the worst pain imaginable). The gel group had lower pain scores for speculum insertion compared with the water group (1.41±1.55 vs 2.15±1.93; P<.01), a statistically significant difference of 0.74. Twenty of the 59 patients in the gel group (33.9%) rated their pain as 0, compared with 6 of 60 (10%) in the water group (P=.002). Although pain, rather than sampling quality, was the primary outcome of the study, the authors also reported that all of the women who underwent Pap screening (73) had adequate cytology.
WHAT’S NEW?: It’s time for lubrication to become standard practice
This trial is the first to study speculum lubrication from this patient-oriented outcome, and to show that women experience less pain when lubricating gel is applied to the speculum, rather than water. This knowledge, combined with previous studies showing that a small amount of water-based lubricating gel does not interfere with liquid-based cytology or chlamydia test results, should make the use of lubricating gel standard practice when performing speculum examinations.
CAVEATS: We see no downside
The exclusion criteria of this study were meant to eliminate women who had an altered pain perception that could skew study results. Yet those who met the exclusion criteria may also benefit from a pelvic exam with gel lubrication. We see no harm in trying a small amount of lubricant when examining them, as well.
In addition, the study did not compare various types and sizes of specula. However, we see no reason why the benefit of a gel lubricant would be limited to the type of speculum used by the examiner.
Studies in emergency departments that have used visual analog scales to measure interventions that decrease pain have used a 0.9 mean difference as “clinically meaningful.”7,8 By that criteria, the 0.74 difference observed in this study does not rise to the level of clinical meaningfulness. However, one in 3 patients in the gel group marked 0 on the pain scale, indicating that they had no pain, vs only one in 10 in the water group. We believe that the higher proportion of women experiencing no pain and the mean difference of 0.74 on the pain scale (both statistically significant), combined with the lack of risk associated with the use of a water-based lubricant, makes this a clinically useful practice changer.
CHALLENGES TO IMPLEMENTATION: There aren’t any
Other than clinical inertia, we see no challenges to the implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National center for Research Resources, a clinical Translational Science Award to the University of chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National center for Research Resources or the National Institutes of health.
Put lubricating gel, not water, on the speculum every time you do a pelvic exam.1
STRENGTH OF RECOMMENDATION
B: Based on one good-quality, randomized controlled trial (RCT).
Hill DA, Lamvu G. Effect of lubricating gel on patient comfort during vaginal speculum examination. Obstet Gynecol. 2012;119(2 pt 1): 227-231.
ILLUSTRATIVE CASE
A 24-year-old woman comes in for an annual exam, including Pap smear and testing for sexually transmitted diseases (STD). She tells you how painful her previous speculum exam was and how worried she is about having another. Should you apply lubricating gel or water to the speculum before vaginal insertion to ease her discomfort?
Physiology teaches us that vaginal entry requires lubrication. But traditional teaching has held that lubricating gel on a speculum can interfere with the results of a Pap smear and chlamydia tesing.2 Pelvic exams performed without lubricating gel on the speculum can cause significant discomfort—possibly bad enough to prevent some women from undergoing the recommended screening tests.3
Until now, we’ve only evaluated gel’s impact on test results
Studies comparing lubricating gel and water have conclusively shown that a small amount of gel, used on the outside of the speculum blades, does not interfere with either Pap testing or detection of Chlamydia trachomatis.4,5 One liquid-based cytology manufacturer, however, discourages the use of lubricants with “carbomers” or “carbopol polymers,” but states that water-based lubricants have not been shown to interfere with Pap smear results.6 No studies have evaluated lubricants from a patient perspective—until now.
STUDY SUMMARY: Lubricating gel eases discomfort
The study by Hill and Lamvu was a 6-month, single-blind, randomized trial of women ages 18 to 50 years who sought care at an Orlando, Florida obstetrics and gynecology department for conditions requiring vaginal speculum examination.1 The study excluded women who might have an altered perception of pain during speculum insertion— those who were menopausal, pregnant, or within 6 weeks’ postpartum; had dyspareunia, vaginitis, vulvar pain, or vulvar lesions; were undergoing a procedure; or had never had vaginal intercourse. Women who were not fluent in English were excluded, as well.
The study included 120 women who underwent computer-generated randomization into 2 groups with no marked differences in demographics. A single examiner did all the speculum exams, using a standard protocol with a medium-size Graves speculum. The examiner applied 0.3 mL water-based lubricating gel to the speculum before insertion for the women in one group, and used 3 mL water for the other.
Immediately after the speculum was inserted and opened—before the examiner attempted to visualize the cervix—patients were given a visual analog scale and told to indicate the level of pain with insertion, using a scale of 0 (no pain) to 10 (the worst pain imaginable). The gel group had lower pain scores for speculum insertion compared with the water group (1.41±1.55 vs 2.15±1.93; P<.01), a statistically significant difference of 0.74. Twenty of the 59 patients in the gel group (33.9%) rated their pain as 0, compared with 6 of 60 (10%) in the water group (P=.002). Although pain, rather than sampling quality, was the primary outcome of the study, the authors also reported that all of the women who underwent Pap screening (73) had adequate cytology.
WHAT’S NEW?: It’s time for lubrication to become standard practice
This trial is the first to study speculum lubrication from this patient-oriented outcome, and to show that women experience less pain when lubricating gel is applied to the speculum, rather than water. This knowledge, combined with previous studies showing that a small amount of water-based lubricating gel does not interfere with liquid-based cytology or chlamydia test results, should make the use of lubricating gel standard practice when performing speculum examinations.
CAVEATS: We see no downside
The exclusion criteria of this study were meant to eliminate women who had an altered pain perception that could skew study results. Yet those who met the exclusion criteria may also benefit from a pelvic exam with gel lubrication. We see no harm in trying a small amount of lubricant when examining them, as well.
In addition, the study did not compare various types and sizes of specula. However, we see no reason why the benefit of a gel lubricant would be limited to the type of speculum used by the examiner.
Studies in emergency departments that have used visual analog scales to measure interventions that decrease pain have used a 0.9 mean difference as “clinically meaningful.”7,8 By that criteria, the 0.74 difference observed in this study does not rise to the level of clinical meaningfulness. However, one in 3 patients in the gel group marked 0 on the pain scale, indicating that they had no pain, vs only one in 10 in the water group. We believe that the higher proportion of women experiencing no pain and the mean difference of 0.74 on the pain scale (both statistically significant), combined with the lack of risk associated with the use of a water-based lubricant, makes this a clinically useful practice changer.
CHALLENGES TO IMPLEMENTATION: There aren’t any
Other than clinical inertia, we see no challenges to the implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National center for Research Resources, a clinical Translational Science Award to the University of chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National center for Research Resources or the National Institutes of health.
1. Hill DA, Lamvu G. Effect of lubricating gel on patient comfort during vaginal speculum examination. Obstet Gynecol. 2012;119 (2 pt 1):227-231.
2. Harmanli O, Jones KA. Using lubricant for speculum insertion. Obstet Gynecol. 2010;116:415-417.
3. Hoyo C, Yarnall KSH, Skinner CS, et al. Pain predicts non-adherence to pap smear screening among middle-aged African American women. Prev Med. 2005;41:439-445.
4. Amies AE, Miller L, Lee S, et al. The effect of vaginal speculum lubrication on the rate of unsatisfactory cervical cytology diagnosis. Obstet Gynecol. 2002;100:889-892.
5. Griffith WF, Stuart GS, Gluck KL, et al. Vaginal speculum lubrication and its effects on cervical cytology and microbiology. Contraception. 2005;72:60-604.
6. Evantash E. Lubricant use during Pap test collection. Bedford, Mass: Hologic, Inc; 2009. Available at: www.thinprep.com/pdfs/Lubricant_Letter_Rev_3.doc. Accessed June 8, 2012.
7. Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med. 2001;8:1153-1157.
8. Kelly AM. Does the clinically significant difference in visual analog scale pain scores vary with gender, age, or cause of pain? Acad Emerg Med. 1998;5:1086-1090.
1. Hill DA, Lamvu G. Effect of lubricating gel on patient comfort during vaginal speculum examination. Obstet Gynecol. 2012;119 (2 pt 1):227-231.
2. Harmanli O, Jones KA. Using lubricant for speculum insertion. Obstet Gynecol. 2010;116:415-417.
3. Hoyo C, Yarnall KSH, Skinner CS, et al. Pain predicts non-adherence to pap smear screening among middle-aged African American women. Prev Med. 2005;41:439-445.
4. Amies AE, Miller L, Lee S, et al. The effect of vaginal speculum lubrication on the rate of unsatisfactory cervical cytology diagnosis. Obstet Gynecol. 2002;100:889-892.
5. Griffith WF, Stuart GS, Gluck KL, et al. Vaginal speculum lubrication and its effects on cervical cytology and microbiology. Contraception. 2005;72:60-604.
6. Evantash E. Lubricant use during Pap test collection. Bedford, Mass: Hologic, Inc; 2009. Available at: www.thinprep.com/pdfs/Lubricant_Letter_Rev_3.doc. Accessed June 8, 2012.
7. Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med. 2001;8:1153-1157.
8. Kelly AM. Does the clinically significant difference in visual analog scale pain scores vary with gender, age, or cause of pain? Acad Emerg Med. 1998;5:1086-1090.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
The shrinking case for saw palmetto
Advise men with benign prostatic hyperplasia (BPH) not to take saw palmetto for urinary symptoms. Explain that it has not been found to alleviate symptoms, even at triple the standard dose.1
A: Based on evidence from a high-quality randomized controlled trial (RCT)1 and a 2009 meta-analysis.2
1. Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344-1351.
ILLUSTRATIVE CASE
A 66-year-old man comes to your office complaining of urinary frequency and straining to begin urination. He was recently diagnosed with BPh by a urologist, but is hesitant to begin taking a prescription drug. The patient, who is on a fixed income, asks you if saw palmetto extract might relieve his urinary symptoms. What should you tell him?
Roughly 40% of American men older than 60 years and nearly 90% of men older than 80 suffer from BPH and the troublesome lower urinary tract symptoms (LUTS) that it causes.3 Established medical and surgical options, as well as over-the-counter (OTC) plant-based products, are used for symptom relief. The OTC remedy most commonly used for BPH is Serenoa repens, derived from the saw palmetto dwarf palm tree. In a 2007 survey, 1.6 million US adults reported using saw palmetto extract, often as a treatment for BPH, in the 30 days prior to the survey.4
Until now, more questions than answers
As a family physician, you undoubtedly have many patients who are taking or considering taking saw palmetto for relief of BPH symptoms. The significant adverse effects of alpha-blockers and 5-alpha-reductase inhibitors, which are typically prescribed for LUTS—including decreased libido and dizziness—may help account for their interest in this alternative treatment.5,6
Until recently, evidence of saw palmetto’s efficacy has been limited and conflicting, despite widespread use of the extract. That has left many of us wondering whether we should recommend that men with BPH try saw palmetto despite the limited evidence; whether it is effective for some, but not all, BPH symptoms; and whether an increase in dose would increase its efficacy.
A 2002 Cochrane meta-analysis of 21 trials of saw palmetto extract for LUTS reported reduced nocturia, improved self-reported symptoms, and increased peak uroflow compared with placebo, without significant adverse effects.7 An updated Cochrane review published in 2009 included several more rigorous trials—and had very different results: This meta-analysis, which was based on 30 trials, found a reduction in nocturia, but failed to show improvement in other self-reported symptoms or peak uroflow.2
The largest trial included in the 2009 review was the Saw Palmetto Treatment for Enlarged Prostates (STEP) study,8 a one-year study with 225 participants. Its findings: no improvement in the treatment group compared with the placebo group in symptom scores or any secondary endpoints, and no important toxicity.8 Of note, the STEP study and most trials included in the 2009 Cochrane review used the standard saw palmetto extract dose of 160 mg twice daily.1,2
STUDY SUMMARY: Saw palmetto is ineffective, even at triple the dose
Barry et al conducted a 72-week double-blind, multicenter placebo-controlled trial to assess the effect of double (640 mg/d) and triple (960 mg/d) the standard dose of saw palmetto extract on BPH symptoms.1 The study included 369 men with moderate LUTS who had not recently received treatment for BPH. Exclusion criteria included a history of invasive BPH treatment, recent treatment with either an alpha-blocker or a 5-alpha-reductase inhibitor; recent phytotherapy, including saw palmetto; and a history of prostate or bladder cancer. Participants were randomized to receive either saw palmetto extract or an identical-looking placebo gel cap. Doses started at 320 mg/d and were increased to 640 mg/d at 24 weeks and 960 mg/d at 48 weeks.
The primary outcome was the change in the American Urological Association Symptom Index (AUASI) score from baseline to 72 weeks. AUASI, a scale of 0 to 35 in which higher numbers represent increased symptoms, is the same scoring tool used in both the Cochrane review and the STEP trial. Secondary measures included other symptom scales, peak uroflow, and poststudy satisfaction. The treatment and placebo groups had statistically identical baseline characteristics, and the sample size was large enough to detect clinically significant differences.
The AUASI score decreased by a mean of 2.20 points (95% confidence interval [CI], -3.04 to -0.36) in the group that received saw palmetto and by 2.99 points (95% CI, -3.81 to -2.17) in the placebo group—a mean difference of 0.79 in favor of the placebo group (P=.91). The proportion of participants achieving a 3-point reduction in AUASI score was statistically similar between the 2 groups (P=0.66). There was no significant dose response difference between the 2 groups, and saw palmetto proved to be no better than placebo for any of the secondary outcomes.
Subgroup analysis did not reveal any results that differed from the main outcomes. The only adverse events that were significantly different between the 2 groups related to physical injury or trauma, which were unlikely to be due to the intervention.1
By using the same symptom scoring system (AUASI) as many studies in the previous Cochrane reviews, Barry et al were able to compare their findings with those of other high-quality studies with similar methodologies and outcome measures. Despite using an even higher dose of the extract, the results of this trial are remarkably consistent with previous conclusions: Saw palmetto is not an effective treatment for symptoms associated with BPH. Moreover, this trial had a broad base of participants similar to the population in a primary care practice, including patients who would typically choose a natural remedy for LUTS.1
WHAT’S NEW: We now have answers to queries about saw palmetto
This trial is the first to compare higher doses of saw palmetto with placebo to assess a dosage threshold for effectiveness. While the study found no evidence of saw palmetto toxicity even at these higher doses, the extract did not outperform placebo for any measured outcome.1
This high-quality study confirmed the recent series of rigorous studies with negative outcomes by showing that the use of a standard dosage was not a study limitation and that saw palmetto extract is not effective for treating LUTS at any dosage. This trial should substantially affect future guideline recommendations that were limited by methodological concerns in the past.9-11
CAVEATS: In theory, individual preparations could work differently
It is not possible to be absolutely certain that these findings apply to all saw palmetto extract preparations, given the unknown active ingredients and unknown mechanism of action. However, the researchers used a high-quality preparation (a proprietary lipidic ethanolic extract) of saw palmetto at higher doses than the STEP trial and came to a similar conclusion, making it highly unlikely that another preparation would perform differently.
CHALLENGES TO IMPLEMENTATION: There are none
We see no challenges to implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344-1351.
2. Tacklind J, MacDonald R, Rutks I, et al. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2009;(2):CD001423.-
3. Roehrborn CG, McConnell JD. Etiology, Pathophysiology, Epidemiology, and Natural History of Benign Prostatic Hyperplasia. 8th ed. Philadelphia, Pa: Campbell’s Urology; 2002.
4. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;(12):1-23.
5. Traish AM, Hassani J, Guay AT, et al. Adverse side effects of 5-alpha-reductase inhibitors therapy: persistent diminished libido and erectile dysfunction and depression in a subset of patients. J Sex Med. 2011;8:872-884.
6. Clifford GM, Farmer RD. Medical therapy for benign prostatic hyperplasia: a review of the literature. Eur Urol. 2000;38:2-19.
7. Wilt T, Ishani A, MacDonald R. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002;(3):CD001423.-
8. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566.
9. Benign prostatic hyperplasia: treatment {saw palmetto}. In: DynaMed. Available at: http://www.DynamicMedical.com. Accessed April 16, 2012.
10. Saper R. Clinical use of saw palmetto {saw palmetto}. In: Basow DS, ed. UpToDate [database online]. Waltham, Mass: UpToDate 2012. Available at: http://www.uptodate.com. Accessed April 16, 2012.
11. Agency for Healthcare Research and Quality. Guidelines on the treatment of non-neurogenic male LUTS. Available at: http://www.guideline.gov/content.aspx?id=34066. Accessed June 17, 2012.
Advise men with benign prostatic hyperplasia (BPH) not to take saw palmetto for urinary symptoms. Explain that it has not been found to alleviate symptoms, even at triple the standard dose.1
A: Based on evidence from a high-quality randomized controlled trial (RCT)1 and a 2009 meta-analysis.2
1. Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344-1351.
ILLUSTRATIVE CASE
A 66-year-old man comes to your office complaining of urinary frequency and straining to begin urination. He was recently diagnosed with BPh by a urologist, but is hesitant to begin taking a prescription drug. The patient, who is on a fixed income, asks you if saw palmetto extract might relieve his urinary symptoms. What should you tell him?
Roughly 40% of American men older than 60 years and nearly 90% of men older than 80 suffer from BPH and the troublesome lower urinary tract symptoms (LUTS) that it causes.3 Established medical and surgical options, as well as over-the-counter (OTC) plant-based products, are used for symptom relief. The OTC remedy most commonly used for BPH is Serenoa repens, derived from the saw palmetto dwarf palm tree. In a 2007 survey, 1.6 million US adults reported using saw palmetto extract, often as a treatment for BPH, in the 30 days prior to the survey.4
Until now, more questions than answers
As a family physician, you undoubtedly have many patients who are taking or considering taking saw palmetto for relief of BPH symptoms. The significant adverse effects of alpha-blockers and 5-alpha-reductase inhibitors, which are typically prescribed for LUTS—including decreased libido and dizziness—may help account for their interest in this alternative treatment.5,6
Until recently, evidence of saw palmetto’s efficacy has been limited and conflicting, despite widespread use of the extract. That has left many of us wondering whether we should recommend that men with BPH try saw palmetto despite the limited evidence; whether it is effective for some, but not all, BPH symptoms; and whether an increase in dose would increase its efficacy.
A 2002 Cochrane meta-analysis of 21 trials of saw palmetto extract for LUTS reported reduced nocturia, improved self-reported symptoms, and increased peak uroflow compared with placebo, without significant adverse effects.7 An updated Cochrane review published in 2009 included several more rigorous trials—and had very different results: This meta-analysis, which was based on 30 trials, found a reduction in nocturia, but failed to show improvement in other self-reported symptoms or peak uroflow.2
The largest trial included in the 2009 review was the Saw Palmetto Treatment for Enlarged Prostates (STEP) study,8 a one-year study with 225 participants. Its findings: no improvement in the treatment group compared with the placebo group in symptom scores or any secondary endpoints, and no important toxicity.8 Of note, the STEP study and most trials included in the 2009 Cochrane review used the standard saw palmetto extract dose of 160 mg twice daily.1,2
STUDY SUMMARY: Saw palmetto is ineffective, even at triple the dose
Barry et al conducted a 72-week double-blind, multicenter placebo-controlled trial to assess the effect of double (640 mg/d) and triple (960 mg/d) the standard dose of saw palmetto extract on BPH symptoms.1 The study included 369 men with moderate LUTS who had not recently received treatment for BPH. Exclusion criteria included a history of invasive BPH treatment, recent treatment with either an alpha-blocker or a 5-alpha-reductase inhibitor; recent phytotherapy, including saw palmetto; and a history of prostate or bladder cancer. Participants were randomized to receive either saw palmetto extract or an identical-looking placebo gel cap. Doses started at 320 mg/d and were increased to 640 mg/d at 24 weeks and 960 mg/d at 48 weeks.
The primary outcome was the change in the American Urological Association Symptom Index (AUASI) score from baseline to 72 weeks. AUASI, a scale of 0 to 35 in which higher numbers represent increased symptoms, is the same scoring tool used in both the Cochrane review and the STEP trial. Secondary measures included other symptom scales, peak uroflow, and poststudy satisfaction. The treatment and placebo groups had statistically identical baseline characteristics, and the sample size was large enough to detect clinically significant differences.
The AUASI score decreased by a mean of 2.20 points (95% confidence interval [CI], -3.04 to -0.36) in the group that received saw palmetto and by 2.99 points (95% CI, -3.81 to -2.17) in the placebo group—a mean difference of 0.79 in favor of the placebo group (P=.91). The proportion of participants achieving a 3-point reduction in AUASI score was statistically similar between the 2 groups (P=0.66). There was no significant dose response difference between the 2 groups, and saw palmetto proved to be no better than placebo for any of the secondary outcomes.
Subgroup analysis did not reveal any results that differed from the main outcomes. The only adverse events that were significantly different between the 2 groups related to physical injury or trauma, which were unlikely to be due to the intervention.1
By using the same symptom scoring system (AUASI) as many studies in the previous Cochrane reviews, Barry et al were able to compare their findings with those of other high-quality studies with similar methodologies and outcome measures. Despite using an even higher dose of the extract, the results of this trial are remarkably consistent with previous conclusions: Saw palmetto is not an effective treatment for symptoms associated with BPH. Moreover, this trial had a broad base of participants similar to the population in a primary care practice, including patients who would typically choose a natural remedy for LUTS.1
WHAT’S NEW: We now have answers to queries about saw palmetto
This trial is the first to compare higher doses of saw palmetto with placebo to assess a dosage threshold for effectiveness. While the study found no evidence of saw palmetto toxicity even at these higher doses, the extract did not outperform placebo for any measured outcome.1
This high-quality study confirmed the recent series of rigorous studies with negative outcomes by showing that the use of a standard dosage was not a study limitation and that saw palmetto extract is not effective for treating LUTS at any dosage. This trial should substantially affect future guideline recommendations that were limited by methodological concerns in the past.9-11
CAVEATS: In theory, individual preparations could work differently
It is not possible to be absolutely certain that these findings apply to all saw palmetto extract preparations, given the unknown active ingredients and unknown mechanism of action. However, the researchers used a high-quality preparation (a proprietary lipidic ethanolic extract) of saw palmetto at higher doses than the STEP trial and came to a similar conclusion, making it highly unlikely that another preparation would perform differently.
CHALLENGES TO IMPLEMENTATION: There are none
We see no challenges to implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Advise men with benign prostatic hyperplasia (BPH) not to take saw palmetto for urinary symptoms. Explain that it has not been found to alleviate symptoms, even at triple the standard dose.1
A: Based on evidence from a high-quality randomized controlled trial (RCT)1 and a 2009 meta-analysis.2
1. Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344-1351.
ILLUSTRATIVE CASE
A 66-year-old man comes to your office complaining of urinary frequency and straining to begin urination. He was recently diagnosed with BPh by a urologist, but is hesitant to begin taking a prescription drug. The patient, who is on a fixed income, asks you if saw palmetto extract might relieve his urinary symptoms. What should you tell him?
Roughly 40% of American men older than 60 years and nearly 90% of men older than 80 suffer from BPH and the troublesome lower urinary tract symptoms (LUTS) that it causes.3 Established medical and surgical options, as well as over-the-counter (OTC) plant-based products, are used for symptom relief. The OTC remedy most commonly used for BPH is Serenoa repens, derived from the saw palmetto dwarf palm tree. In a 2007 survey, 1.6 million US adults reported using saw palmetto extract, often as a treatment for BPH, in the 30 days prior to the survey.4
Until now, more questions than answers
As a family physician, you undoubtedly have many patients who are taking or considering taking saw palmetto for relief of BPH symptoms. The significant adverse effects of alpha-blockers and 5-alpha-reductase inhibitors, which are typically prescribed for LUTS—including decreased libido and dizziness—may help account for their interest in this alternative treatment.5,6
Until recently, evidence of saw palmetto’s efficacy has been limited and conflicting, despite widespread use of the extract. That has left many of us wondering whether we should recommend that men with BPH try saw palmetto despite the limited evidence; whether it is effective for some, but not all, BPH symptoms; and whether an increase in dose would increase its efficacy.
A 2002 Cochrane meta-analysis of 21 trials of saw palmetto extract for LUTS reported reduced nocturia, improved self-reported symptoms, and increased peak uroflow compared with placebo, without significant adverse effects.7 An updated Cochrane review published in 2009 included several more rigorous trials—and had very different results: This meta-analysis, which was based on 30 trials, found a reduction in nocturia, but failed to show improvement in other self-reported symptoms or peak uroflow.2
The largest trial included in the 2009 review was the Saw Palmetto Treatment for Enlarged Prostates (STEP) study,8 a one-year study with 225 participants. Its findings: no improvement in the treatment group compared with the placebo group in symptom scores or any secondary endpoints, and no important toxicity.8 Of note, the STEP study and most trials included in the 2009 Cochrane review used the standard saw palmetto extract dose of 160 mg twice daily.1,2
STUDY SUMMARY: Saw palmetto is ineffective, even at triple the dose
Barry et al conducted a 72-week double-blind, multicenter placebo-controlled trial to assess the effect of double (640 mg/d) and triple (960 mg/d) the standard dose of saw palmetto extract on BPH symptoms.1 The study included 369 men with moderate LUTS who had not recently received treatment for BPH. Exclusion criteria included a history of invasive BPH treatment, recent treatment with either an alpha-blocker or a 5-alpha-reductase inhibitor; recent phytotherapy, including saw palmetto; and a history of prostate or bladder cancer. Participants were randomized to receive either saw palmetto extract or an identical-looking placebo gel cap. Doses started at 320 mg/d and were increased to 640 mg/d at 24 weeks and 960 mg/d at 48 weeks.
The primary outcome was the change in the American Urological Association Symptom Index (AUASI) score from baseline to 72 weeks. AUASI, a scale of 0 to 35 in which higher numbers represent increased symptoms, is the same scoring tool used in both the Cochrane review and the STEP trial. Secondary measures included other symptom scales, peak uroflow, and poststudy satisfaction. The treatment and placebo groups had statistically identical baseline characteristics, and the sample size was large enough to detect clinically significant differences.
The AUASI score decreased by a mean of 2.20 points (95% confidence interval [CI], -3.04 to -0.36) in the group that received saw palmetto and by 2.99 points (95% CI, -3.81 to -2.17) in the placebo group—a mean difference of 0.79 in favor of the placebo group (P=.91). The proportion of participants achieving a 3-point reduction in AUASI score was statistically similar between the 2 groups (P=0.66). There was no significant dose response difference between the 2 groups, and saw palmetto proved to be no better than placebo for any of the secondary outcomes.
Subgroup analysis did not reveal any results that differed from the main outcomes. The only adverse events that were significantly different between the 2 groups related to physical injury or trauma, which were unlikely to be due to the intervention.1
By using the same symptom scoring system (AUASI) as many studies in the previous Cochrane reviews, Barry et al were able to compare their findings with those of other high-quality studies with similar methodologies and outcome measures. Despite using an even higher dose of the extract, the results of this trial are remarkably consistent with previous conclusions: Saw palmetto is not an effective treatment for symptoms associated with BPH. Moreover, this trial had a broad base of participants similar to the population in a primary care practice, including patients who would typically choose a natural remedy for LUTS.1
WHAT’S NEW: We now have answers to queries about saw palmetto
This trial is the first to compare higher doses of saw palmetto with placebo to assess a dosage threshold for effectiveness. While the study found no evidence of saw palmetto toxicity even at these higher doses, the extract did not outperform placebo for any measured outcome.1
This high-quality study confirmed the recent series of rigorous studies with negative outcomes by showing that the use of a standard dosage was not a study limitation and that saw palmetto extract is not effective for treating LUTS at any dosage. This trial should substantially affect future guideline recommendations that were limited by methodological concerns in the past.9-11
CAVEATS: In theory, individual preparations could work differently
It is not possible to be absolutely certain that these findings apply to all saw palmetto extract preparations, given the unknown active ingredients and unknown mechanism of action. However, the researchers used a high-quality preparation (a proprietary lipidic ethanolic extract) of saw palmetto at higher doses than the STEP trial and came to a similar conclusion, making it highly unlikely that another preparation would perform differently.
CHALLENGES TO IMPLEMENTATION: There are none
We see no challenges to implementation of this recommendation.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344-1351.
2. Tacklind J, MacDonald R, Rutks I, et al. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2009;(2):CD001423.-
3. Roehrborn CG, McConnell JD. Etiology, Pathophysiology, Epidemiology, and Natural History of Benign Prostatic Hyperplasia. 8th ed. Philadelphia, Pa: Campbell’s Urology; 2002.
4. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;(12):1-23.
5. Traish AM, Hassani J, Guay AT, et al. Adverse side effects of 5-alpha-reductase inhibitors therapy: persistent diminished libido and erectile dysfunction and depression in a subset of patients. J Sex Med. 2011;8:872-884.
6. Clifford GM, Farmer RD. Medical therapy for benign prostatic hyperplasia: a review of the literature. Eur Urol. 2000;38:2-19.
7. Wilt T, Ishani A, MacDonald R. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002;(3):CD001423.-
8. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566.
9. Benign prostatic hyperplasia: treatment {saw palmetto}. In: DynaMed. Available at: http://www.DynamicMedical.com. Accessed April 16, 2012.
10. Saper R. Clinical use of saw palmetto {saw palmetto}. In: Basow DS, ed. UpToDate [database online]. Waltham, Mass: UpToDate 2012. Available at: http://www.uptodate.com. Accessed April 16, 2012.
11. Agency for Healthcare Research and Quality. Guidelines on the treatment of non-neurogenic male LUTS. Available at: http://www.guideline.gov/content.aspx?id=34066. Accessed June 17, 2012.
1. Barry MJ, Meleth S, Lee JY, et al. Effect of increasing doses of saw palmetto extract on lower urinary tract symptoms: a randomized trial. JAMA. 2011;306:1344-1351.
2. Tacklind J, MacDonald R, Rutks I, et al. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2009;(2):CD001423.-
3. Roehrborn CG, McConnell JD. Etiology, Pathophysiology, Epidemiology, and Natural History of Benign Prostatic Hyperplasia. 8th ed. Philadelphia, Pa: Campbell’s Urology; 2002.
4. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;(12):1-23.
5. Traish AM, Hassani J, Guay AT, et al. Adverse side effects of 5-alpha-reductase inhibitors therapy: persistent diminished libido and erectile dysfunction and depression in a subset of patients. J Sex Med. 2011;8:872-884.
6. Clifford GM, Farmer RD. Medical therapy for benign prostatic hyperplasia: a review of the literature. Eur Urol. 2000;38:2-19.
7. Wilt T, Ishani A, MacDonald R. Serenoa repens for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002;(3):CD001423.-
8. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566.
9. Benign prostatic hyperplasia: treatment {saw palmetto}. In: DynaMed. Available at: http://www.DynamicMedical.com. Accessed April 16, 2012.
10. Saper R. Clinical use of saw palmetto {saw palmetto}. In: Basow DS, ed. UpToDate [database online]. Waltham, Mass: UpToDate 2012. Available at: http://www.uptodate.com. Accessed April 16, 2012.
11. Agency for Healthcare Research and Quality. Guidelines on the treatment of non-neurogenic male LUTS. Available at: http://www.guideline.gov/content.aspx?id=34066. Accessed June 17, 2012.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
Should breastfeeding babies be given pacifiers?
Do not discourage the use of pacifiers by healthy infants who are breastfeeding.1
STRENGTH OF RECOMMENDATION
A: Based on a good-quality meta-analysis
Jaafar SH, Jahanfar S, Angolkar M, et al. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011;(3):CD007202.
ILLUSTRATIVE CASE
A 28-year-old first-time mother brings her 1-week-old full-term, healthy daughter to your clinic for a routine check-up. The baby is growing as expected. The mother is breastfeeding exclusively and would like to continue until the baby is at least 6 months old. She has begun giving the infant a pacifier and asks whether that’s OK. What should you tell her?
Breast milk is superior to formula for infant nutrition,2,3 and the American Academy of Pediatrics (AAP), World Health Organization (WHO), and UNICEF recommend exclusive breastfeeding through the first 6 months of life.4,5 “Ten steps to successful breastfeeding,” a document developed by the WHO and UNICEF, specifically states that artificial teats and pacifiers should not be given to breastfeeding infants.5
Concern about pacifiers for breastfeeding infants focuses on “nipple confusion”—that is, that pacifiers (and supplemental bottles) do not facilitate effective breast sucking and may contribute to incorrect latch.6,7 Findings from earlier observational stud-ies suggest that early exposure to pacifiers leads to cessation of exclusive breastfeeding by 3 to 6 months and an end to all breastfeeding by 12 months.8,9
Pacifiers have become a cultural norm in many parts of the world,10 and their use appears to be associated with a decrease in the incidence of sudden infant death syndrome (SIDS).11 But both the AAP and the American Academy of Family Physicians recommend delaying paci-fier use until breastfeeding is established.4,12
STUDY SUMMARY: Pacifier or no pacifier— no significant difference
Cochrane reviewers conducted a meta-analysis of randomized controlled trials (RCTs) that assessed the effects of pacifier use on healthy full-term infants whose mothers had initiated breastfeeding and intended to exclusively breastfeed.1
The primary outcome was the duration of breastfeeding, as measured by (1) mean duration of full breastfeeding (in months); (2) mean duration of any or partial breastfeeding; or (3) the prevalence or proportion of infants who were fully or partially breastfed at 3, 4, and 6 months of age. Secondary outcomes were (1) rate of breastfeeding difficulties (cracked nipples, breast engorgement, mastitis); (2) maternal satisfaction and level of confidence in parenting; (3) frequency of infant crying and fussiness; and (4) infant health, including SIDS, oral candidiasis, otitis media, and dental malocclusion. Infants who were given pacifiers (ie, those who had unrestricted or actively encouraged pacifier use) were compared with infants who were not given pacifiers (ie, whose mothers were advised against pacifier use).
Two studies, with a combined total of 1302 infants, were included in the meta-analysis (a third was excluded because the method by which allocation was concealed was un-clear). Both reported blinding of the research nurses and outcome assessors. Blinding of par-ticipants was not feasible.
Each trial measured at least one primary outcome. The dropout rate was <10% in each arm of both studies.
When pacifier use was compared with no pacifier use, no significant difference was found in the proportion of infants who were exclusively breastfed at 3 months (risk ratio [RR]=1.00; 95% confidence interval [CI], 0.95-1.06) or 4 months of age (RR=0.99; 95% CI, 0.92-1.06). Nor was there a significant difference in the proportion of infants who were partially breastfed at 3 months (RR=1.00; 95% CI, 0.97-1.02) or 4 months (RR=1.01; 95% CI, 0.98-1.03).
Neither study reported on any of the secondary outcomes.
WHAT’S NEW: Now we know: Pacifier use by breastfeeding infants is fine
This meta-analysis shows that pacifier use does not decrease breastfeeding duration in full-term infants. The new evidence contradicts current WHO recom-mendations, however, which are based on less rigorous studies.8,9,13,14 The AAP now recommends that pacifier use be implemented after breastfeeding is established.4 Based on the evidence, we think mothers who are motivated to breastfeed their infants should be allowed to make their own decisions regarding pacifier use, and pacifier use should not be discouraged.
CAVEATS: Effects on infant health still unaddressed
This meta-analysis did not report on the potential harms of pacifi-ers to infants >4 months old or to their lactating mothers. Potential problems of prolonged pacifier use (>4 months), such as increased risk of recurrent acute otitis media, oral candidiasis, and dental malocclusion, should be addressed with mothers, but should not lead to discouraging pacifier use in early infancy.15-17
CHALLENGES TO IMPLEMENTATION: There aren’t any
We see no challenges to implementation of this practice changer.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Jaafar SH, Jahanfar S, Angolkar M, et al. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011;(3):CD007202.-
2. Chandra RK. Prospective studies on the effect of breastfeeding on the incidence of infection and allergy. Acta Paediatr Scand. 1979;68:691-694.
3. Oddy WH. Breastfeeding protects against illness and infection in infants and children: a review of the evidence. Breastfeed Rev. 2001;9:11-18.
4. American Academy of Pediatrics Section on breastfeeding. Policy Statement. Breastfeeding and the use of human milk. Pediatrics. 2012;129:e827-e841.
5. World Health Organization. Ten steps to successful breastfeeding. WHO/UNICEF statement. Available at: http://www.unicef.org/newsline/tenstps.htm. Accessed April 12, 2012.
6. Gomes CF, Trezza EM, Murade EC, et al. Surface electromyography of facial muscles during natural and artificial feeding of infants. J Pediatr (Rio J). 2006;82:103-109.
7. Righard L. Are breastfeeding problems related to incorrect breastfeeding technique and the use of pacifiers and bottles? Birth. 1998;25:40-44.
8. Mascarenhes ML, Albernaz EP, DaSilva MB, et al. Prevalence of exclusive breastfeeding and its determiners in the first 3 months of life in the South of Brazil. J Pediatr (Rio J). 2006;82:289-294.
9. Scott JA, Binns CW, Oddy WH, et al. Predictors of breastfeeding duration: evidence from a cohort study. Pediatrics. 2006;117:e646-e655.
10. Barros FC, Victora CG, Semer TC, et al. Use of pacifiers is associated with decreased breast-feeding duration. Pediatrics. 1995;95:497-499.
11. American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. The changing concept of sudden infant death syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics. 2005;116:1245-1255.
12. American Academy of Family Physicians. Breastfeeding, family physicians supporting (position paper). Available at: www.aafp.org/online/en/home/policy/policies/b/breastfeedingpositionpaper.html. Accessed April 17, 2012.
13. Howard CR, Howard FM, Lanphear B, et al. The effects of early pacifier use on breastfeeding duration. Pediatrics. 1999;103:E133.-
14. Karabulut E, Yalcin SS, Ozdemir-Geyik P, et al. Effect of pacifier use on exclusive and any breastfeeding: a meta-analysis. Turk J Pediatr. 2009;51:35-43.
15. Jackson JM, Mourino AP. Pacifier use and otitis media in infants twelve months of age or younger. Pediatr Dent. 1999;21:255-260.
16. Darwazeh AM, al-Bashir A. Oral candidal flora in healthy infants. J Oral Pathol Med. 1995;24:361-364.
17. Caglar E, Larsson E, Andersson EM, et al. Feeding, artificial sucking habits, and malocclusions in 3-year-old girls in different regions of the world. J Dent Child (Chic). 2005;72:25-30.
Do not discourage the use of pacifiers by healthy infants who are breastfeeding.1
STRENGTH OF RECOMMENDATION
A: Based on a good-quality meta-analysis
Jaafar SH, Jahanfar S, Angolkar M, et al. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011;(3):CD007202.
ILLUSTRATIVE CASE
A 28-year-old first-time mother brings her 1-week-old full-term, healthy daughter to your clinic for a routine check-up. The baby is growing as expected. The mother is breastfeeding exclusively and would like to continue until the baby is at least 6 months old. She has begun giving the infant a pacifier and asks whether that’s OK. What should you tell her?
Breast milk is superior to formula for infant nutrition,2,3 and the American Academy of Pediatrics (AAP), World Health Organization (WHO), and UNICEF recommend exclusive breastfeeding through the first 6 months of life.4,5 “Ten steps to successful breastfeeding,” a document developed by the WHO and UNICEF, specifically states that artificial teats and pacifiers should not be given to breastfeeding infants.5
Concern about pacifiers for breastfeeding infants focuses on “nipple confusion”—that is, that pacifiers (and supplemental bottles) do not facilitate effective breast sucking and may contribute to incorrect latch.6,7 Findings from earlier observational stud-ies suggest that early exposure to pacifiers leads to cessation of exclusive breastfeeding by 3 to 6 months and an end to all breastfeeding by 12 months.8,9
Pacifiers have become a cultural norm in many parts of the world,10 and their use appears to be associated with a decrease in the incidence of sudden infant death syndrome (SIDS).11 But both the AAP and the American Academy of Family Physicians recommend delaying paci-fier use until breastfeeding is established.4,12
STUDY SUMMARY: Pacifier or no pacifier— no significant difference
Cochrane reviewers conducted a meta-analysis of randomized controlled trials (RCTs) that assessed the effects of pacifier use on healthy full-term infants whose mothers had initiated breastfeeding and intended to exclusively breastfeed.1
The primary outcome was the duration of breastfeeding, as measured by (1) mean duration of full breastfeeding (in months); (2) mean duration of any or partial breastfeeding; or (3) the prevalence or proportion of infants who were fully or partially breastfed at 3, 4, and 6 months of age. Secondary outcomes were (1) rate of breastfeeding difficulties (cracked nipples, breast engorgement, mastitis); (2) maternal satisfaction and level of confidence in parenting; (3) frequency of infant crying and fussiness; and (4) infant health, including SIDS, oral candidiasis, otitis media, and dental malocclusion. Infants who were given pacifiers (ie, those who had unrestricted or actively encouraged pacifier use) were compared with infants who were not given pacifiers (ie, whose mothers were advised against pacifier use).
Two studies, with a combined total of 1302 infants, were included in the meta-analysis (a third was excluded because the method by which allocation was concealed was un-clear). Both reported blinding of the research nurses and outcome assessors. Blinding of par-ticipants was not feasible.
Each trial measured at least one primary outcome. The dropout rate was <10% in each arm of both studies.
When pacifier use was compared with no pacifier use, no significant difference was found in the proportion of infants who were exclusively breastfed at 3 months (risk ratio [RR]=1.00; 95% confidence interval [CI], 0.95-1.06) or 4 months of age (RR=0.99; 95% CI, 0.92-1.06). Nor was there a significant difference in the proportion of infants who were partially breastfed at 3 months (RR=1.00; 95% CI, 0.97-1.02) or 4 months (RR=1.01; 95% CI, 0.98-1.03).
Neither study reported on any of the secondary outcomes.
WHAT’S NEW: Now we know: Pacifier use by breastfeeding infants is fine
This meta-analysis shows that pacifier use does not decrease breastfeeding duration in full-term infants. The new evidence contradicts current WHO recom-mendations, however, which are based on less rigorous studies.8,9,13,14 The AAP now recommends that pacifier use be implemented after breastfeeding is established.4 Based on the evidence, we think mothers who are motivated to breastfeed their infants should be allowed to make their own decisions regarding pacifier use, and pacifier use should not be discouraged.
CAVEATS: Effects on infant health still unaddressed
This meta-analysis did not report on the potential harms of pacifi-ers to infants >4 months old or to their lactating mothers. Potential problems of prolonged pacifier use (>4 months), such as increased risk of recurrent acute otitis media, oral candidiasis, and dental malocclusion, should be addressed with mothers, but should not lead to discouraging pacifier use in early infancy.15-17
CHALLENGES TO IMPLEMENTATION: There aren’t any
We see no challenges to implementation of this practice changer.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Do not discourage the use of pacifiers by healthy infants who are breastfeeding.1
STRENGTH OF RECOMMENDATION
A: Based on a good-quality meta-analysis
Jaafar SH, Jahanfar S, Angolkar M, et al. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011;(3):CD007202.
ILLUSTRATIVE CASE
A 28-year-old first-time mother brings her 1-week-old full-term, healthy daughter to your clinic for a routine check-up. The baby is growing as expected. The mother is breastfeeding exclusively and would like to continue until the baby is at least 6 months old. She has begun giving the infant a pacifier and asks whether that’s OK. What should you tell her?
Breast milk is superior to formula for infant nutrition,2,3 and the American Academy of Pediatrics (AAP), World Health Organization (WHO), and UNICEF recommend exclusive breastfeeding through the first 6 months of life.4,5 “Ten steps to successful breastfeeding,” a document developed by the WHO and UNICEF, specifically states that artificial teats and pacifiers should not be given to breastfeeding infants.5
Concern about pacifiers for breastfeeding infants focuses on “nipple confusion”—that is, that pacifiers (and supplemental bottles) do not facilitate effective breast sucking and may contribute to incorrect latch.6,7 Findings from earlier observational stud-ies suggest that early exposure to pacifiers leads to cessation of exclusive breastfeeding by 3 to 6 months and an end to all breastfeeding by 12 months.8,9
Pacifiers have become a cultural norm in many parts of the world,10 and their use appears to be associated with a decrease in the incidence of sudden infant death syndrome (SIDS).11 But both the AAP and the American Academy of Family Physicians recommend delaying paci-fier use until breastfeeding is established.4,12
STUDY SUMMARY: Pacifier or no pacifier— no significant difference
Cochrane reviewers conducted a meta-analysis of randomized controlled trials (RCTs) that assessed the effects of pacifier use on healthy full-term infants whose mothers had initiated breastfeeding and intended to exclusively breastfeed.1
The primary outcome was the duration of breastfeeding, as measured by (1) mean duration of full breastfeeding (in months); (2) mean duration of any or partial breastfeeding; or (3) the prevalence or proportion of infants who were fully or partially breastfed at 3, 4, and 6 months of age. Secondary outcomes were (1) rate of breastfeeding difficulties (cracked nipples, breast engorgement, mastitis); (2) maternal satisfaction and level of confidence in parenting; (3) frequency of infant crying and fussiness; and (4) infant health, including SIDS, oral candidiasis, otitis media, and dental malocclusion. Infants who were given pacifiers (ie, those who had unrestricted or actively encouraged pacifier use) were compared with infants who were not given pacifiers (ie, whose mothers were advised against pacifier use).
Two studies, with a combined total of 1302 infants, were included in the meta-analysis (a third was excluded because the method by which allocation was concealed was un-clear). Both reported blinding of the research nurses and outcome assessors. Blinding of par-ticipants was not feasible.
Each trial measured at least one primary outcome. The dropout rate was <10% in each arm of both studies.
When pacifier use was compared with no pacifier use, no significant difference was found in the proportion of infants who were exclusively breastfed at 3 months (risk ratio [RR]=1.00; 95% confidence interval [CI], 0.95-1.06) or 4 months of age (RR=0.99; 95% CI, 0.92-1.06). Nor was there a significant difference in the proportion of infants who were partially breastfed at 3 months (RR=1.00; 95% CI, 0.97-1.02) or 4 months (RR=1.01; 95% CI, 0.98-1.03).
Neither study reported on any of the secondary outcomes.
WHAT’S NEW: Now we know: Pacifier use by breastfeeding infants is fine
This meta-analysis shows that pacifier use does not decrease breastfeeding duration in full-term infants. The new evidence contradicts current WHO recom-mendations, however, which are based on less rigorous studies.8,9,13,14 The AAP now recommends that pacifier use be implemented after breastfeeding is established.4 Based on the evidence, we think mothers who are motivated to breastfeed their infants should be allowed to make their own decisions regarding pacifier use, and pacifier use should not be discouraged.
CAVEATS: Effects on infant health still unaddressed
This meta-analysis did not report on the potential harms of pacifi-ers to infants >4 months old or to their lactating mothers. Potential problems of prolonged pacifier use (>4 months), such as increased risk of recurrent acute otitis media, oral candidiasis, and dental malocclusion, should be addressed with mothers, but should not lead to discouraging pacifier use in early infancy.15-17
CHALLENGES TO IMPLEMENTATION: There aren’t any
We see no challenges to implementation of this practice changer.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Jaafar SH, Jahanfar S, Angolkar M, et al. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011;(3):CD007202.-
2. Chandra RK. Prospective studies on the effect of breastfeeding on the incidence of infection and allergy. Acta Paediatr Scand. 1979;68:691-694.
3. Oddy WH. Breastfeeding protects against illness and infection in infants and children: a review of the evidence. Breastfeed Rev. 2001;9:11-18.
4. American Academy of Pediatrics Section on breastfeeding. Policy Statement. Breastfeeding and the use of human milk. Pediatrics. 2012;129:e827-e841.
5. World Health Organization. Ten steps to successful breastfeeding. WHO/UNICEF statement. Available at: http://www.unicef.org/newsline/tenstps.htm. Accessed April 12, 2012.
6. Gomes CF, Trezza EM, Murade EC, et al. Surface electromyography of facial muscles during natural and artificial feeding of infants. J Pediatr (Rio J). 2006;82:103-109.
7. Righard L. Are breastfeeding problems related to incorrect breastfeeding technique and the use of pacifiers and bottles? Birth. 1998;25:40-44.
8. Mascarenhes ML, Albernaz EP, DaSilva MB, et al. Prevalence of exclusive breastfeeding and its determiners in the first 3 months of life in the South of Brazil. J Pediatr (Rio J). 2006;82:289-294.
9. Scott JA, Binns CW, Oddy WH, et al. Predictors of breastfeeding duration: evidence from a cohort study. Pediatrics. 2006;117:e646-e655.
10. Barros FC, Victora CG, Semer TC, et al. Use of pacifiers is associated with decreased breast-feeding duration. Pediatrics. 1995;95:497-499.
11. American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. The changing concept of sudden infant death syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics. 2005;116:1245-1255.
12. American Academy of Family Physicians. Breastfeeding, family physicians supporting (position paper). Available at: www.aafp.org/online/en/home/policy/policies/b/breastfeedingpositionpaper.html. Accessed April 17, 2012.
13. Howard CR, Howard FM, Lanphear B, et al. The effects of early pacifier use on breastfeeding duration. Pediatrics. 1999;103:E133.-
14. Karabulut E, Yalcin SS, Ozdemir-Geyik P, et al. Effect of pacifier use on exclusive and any breastfeeding: a meta-analysis. Turk J Pediatr. 2009;51:35-43.
15. Jackson JM, Mourino AP. Pacifier use and otitis media in infants twelve months of age or younger. Pediatr Dent. 1999;21:255-260.
16. Darwazeh AM, al-Bashir A. Oral candidal flora in healthy infants. J Oral Pathol Med. 1995;24:361-364.
17. Caglar E, Larsson E, Andersson EM, et al. Feeding, artificial sucking habits, and malocclusions in 3-year-old girls in different regions of the world. J Dent Child (Chic). 2005;72:25-30.
1. Jaafar SH, Jahanfar S, Angolkar M, et al. Pacifier use versus no pacifier use in breastfeeding term infants for increasing duration of breastfeeding. Cochrane Database Syst Rev. 2011;(3):CD007202.-
2. Chandra RK. Prospective studies on the effect of breastfeeding on the incidence of infection and allergy. Acta Paediatr Scand. 1979;68:691-694.
3. Oddy WH. Breastfeeding protects against illness and infection in infants and children: a review of the evidence. Breastfeed Rev. 2001;9:11-18.
4. American Academy of Pediatrics Section on breastfeeding. Policy Statement. Breastfeeding and the use of human milk. Pediatrics. 2012;129:e827-e841.
5. World Health Organization. Ten steps to successful breastfeeding. WHO/UNICEF statement. Available at: http://www.unicef.org/newsline/tenstps.htm. Accessed April 12, 2012.
6. Gomes CF, Trezza EM, Murade EC, et al. Surface electromyography of facial muscles during natural and artificial feeding of infants. J Pediatr (Rio J). 2006;82:103-109.
7. Righard L. Are breastfeeding problems related to incorrect breastfeeding technique and the use of pacifiers and bottles? Birth. 1998;25:40-44.
8. Mascarenhes ML, Albernaz EP, DaSilva MB, et al. Prevalence of exclusive breastfeeding and its determiners in the first 3 months of life in the South of Brazil. J Pediatr (Rio J). 2006;82:289-294.
9. Scott JA, Binns CW, Oddy WH, et al. Predictors of breastfeeding duration: evidence from a cohort study. Pediatrics. 2006;117:e646-e655.
10. Barros FC, Victora CG, Semer TC, et al. Use of pacifiers is associated with decreased breast-feeding duration. Pediatrics. 1995;95:497-499.
11. American Academy of Pediatrics Task Force on Sudden Infant Death Syndrome. The changing concept of sudden infant death syndrome: diagnostic coding shifts, controversies regarding the sleeping environment, and new variables to consider in reducing risk. Pediatrics. 2005;116:1245-1255.
12. American Academy of Family Physicians. Breastfeeding, family physicians supporting (position paper). Available at: www.aafp.org/online/en/home/policy/policies/b/breastfeedingpositionpaper.html. Accessed April 17, 2012.
13. Howard CR, Howard FM, Lanphear B, et al. The effects of early pacifier use on breastfeeding duration. Pediatrics. 1999;103:E133.-
14. Karabulut E, Yalcin SS, Ozdemir-Geyik P, et al. Effect of pacifier use on exclusive and any breastfeeding: a meta-analysis. Turk J Pediatr. 2009;51:35-43.
15. Jackson JM, Mourino AP. Pacifier use and otitis media in infants twelve months of age or younger. Pediatr Dent. 1999;21:255-260.
16. Darwazeh AM, al-Bashir A. Oral candidal flora in healthy infants. J Oral Pathol Med. 1995;24:361-364.
17. Caglar E, Larsson E, Andersson EM, et al. Feeding, artificial sucking habits, and malocclusions in 3-year-old girls in different regions of the world. J Dent Child (Chic). 2005;72:25-30.
Copyright © 2012 The Family Physicians Inquiries Network. All rights reserved.
Statins for patients with nonalcoholic fatty liver?
Treat patients with hyperlipidemia and presumed nonalcoholic fatty liver disease with atorvastatin to reduce the risk of cardiovascular events.1
STRENGTH OF RECOMMENDATION
B: Based on a single prospective randomized controlled trial (RCT).
Athyros VG, Tziomalos K, Gossios TD, et al. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post hoc analysis. Lancet. 2010; 376:1916-1922.
ILLUSTRATIVE CASE
An obese 58-year-old man with type 2 diabetes comes to your office for follow-up. His low-density lipoprotein cholesterol (LDL-C) is 130 mg/dL; triglycerides, 300 mg/dL; alanine transaminase (ALT), 110 units/L; and aspartate transaminase (AST), 120 units/L. The patient’s work-up for chronic hepatitis B and C, autoimmune hepatitis, hemochromatosis, and Wilson’s disease are negative, and you rule out alcohol misuse based on his medical history. An ultrasound of the patient’s liver reveals hepatic steatosis, and you diagnose nonalcoholic fatty liver disease (NAFLD). Should you start him on a statin?
Patients with central obesity, diabetes, hypertension, hyperlipidemia, and metabolic syndrome are at high risk of developing NAFLD. These conditions have increased in prevalence, and NAFLD is now the most common cause of liver disease in the United States.2 In Western industrialized countries, approximately 30% of the general population and 70% to 90% of patients with diabetes will develop NAFLD.3 Although most patients are asymptomatic, their liver enzymes are elevated. To diagnose NAFLD, it is necessary to rule out alcoholic hepatitis with a medical history, and viral hepatitis, hereditary hemochromatosis, Wilson’s disease, and autoimmune hepatitis with laboratory testing. Ultrasound reveals fat accumulation in the liver.
Treatment for NAFLD has little evidence of benefit
Patients with NAFLD have a much higher mortality rate than that of the general public, primarily because of cardiovascular disease.4-6 Increased physical activity and weight loss is the only therapy that has solid evidence of a benefit,7 although other treatments, such as insulin-sensitizing drugs (metformin or pioglitazone), may be beneficial.8 Surprisingly, atorvastatin has been found to reduce aminotransferase levels in patients with NAFLD,9,10 but clinicians are often concerned about prescribing a statin for patients with elevated liver enzymes. In one study, 50% of primary care physicians said they would not prescribe statins for patients whose liver enzymes are 1.5× the upper limit of normal (ULN).11
STUDY SUMMARY: Statins lower risk of cardiovascular morbidity and mortality
The Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) study was a randomized, prospective open-label, intention-to-treat trial involving 1600 patients. All had established coronary heart disease (CHD), were younger than 75 years, and had triglycerides <400 mg/dL and LDL-C >100 mg/dL. The study reviewed here—evaluating the risk-to-benefit ratio of using a statin to treat hyperlipidemia in patients with NAFLD—was a post hoc analysis of the GREACE study.1
Participants were randomized to either usual care or structured care with atorvastatin, starting at 10 mg/d and adjusted to 80 mg/d to bring the LDL-C level below 100 mg/dL. In the usual care group, treatment included lifestyle changes plus necessary drug treatments (only 30% of those in the usual care group received hyperlipidemia drugs). Patients were followed after medication dose titration, then every 6 months for 3 years. Serum ALT and AST were measured at baseline, at 6 weeks, and every 6 months.
At baseline, mild-to-moderate increases (<3× ULN) in ALT/AST were noted in 437 of the 1600 patients. For these patients, alcoholic hepatitis, chronic hepatitis B and C, Wilson’s disease, and autoimmune hepatitis were excluded by history, laboratory tests, and ultrasound, and the elevated liver enzymes were attributed to NAFLD.
The primary endpoints were the first occurrence of any cardiovascular event, including nonfatal myocardial infarction, revascularization, unstable angina, heart failure, and stroke; all-cause mortality; and CHD mortality. The relative risk (RR) for such events was calculated for the 437 patients with elevated liver enzymes, compared with that of patients without abnormal liver tests. Elevated liver enzymes and liver-related adverse events were secondary endpoints.
A cardiovascular event occurred in 10% (22/227) of the patients with elevated liver enzymes who received a statin, and 30% (63/210) of patients who had elevated liver enzymes but did not receive a statin.
There were 3.2 events per 100 patient-years in the atorvastatin group, compared with 10 events per 100 patient-years in those not on atorvastatin, a 68% reduction in RR (P<.0001) and an NNT of 15 per year to prevent one cardiovascular event. The risk reduction in cardiovascular events was greater in patients with NAFLD (68%) than in patients with normal liver tests (39%).
An added benefit was the reduction in ALT/AST levels during treatment for patients with NAFLD who were taking a statin, an average decrease of 47% in AST levels and 35% in ALT levels. In addition, 89% of the patients in the statin group had normal ALT, AST, and gamma-glutamyl transferase levels by the end of the 3-year follow-up. Patients with NAFLD who did not receive statins had a 12% increase in AST and ALT by the end of the 3-year study.
Only 10 of 880 patients taking statins developed liver enzymes more than 3× ULN. In 3 of these patients, dose adjustments brought the liver enzymes back to normal. Only 7 (<1%) patients who received a statin had to discontinue therapy because of liver-related adverse effects.
WHAT’S NEW: Liver enzymes improve, with few adverse effects
Preliminary studies have shown an improvement in liver enzymes in patients with NAFLD treated with a statin.9,10 This is the first study to show survival benefits and significant reduction in major cardiovascular morbidity for such patients, as well.
This is also the first large-scale study that shows that treating NAFLD patients with a statin decreases liver enzyme levels, with minimal adverse effects.
CAVEATS: Differences in groups, few women could skew results
This study cannot be considered the final word on this topic. Patients in the “structured care” group were followed at a university clinic, while those in the “usual care” group were followed by either a family physician or a cardiologist outside the hospital, based on their choice. There may have been other differences in the care received by the 2 groups that could account for the difference in mortality and morbidity reduction.
In addition, study participants had coronary artery disease, and atorvastatin was not used for primary prevention. Moreover, nearly 80% of the study participants were male, which raises the question of generalizability. And this study was a post hoc analysis of the larger GREACE study, which also raises concerns about the validity of findings.
In the absence of a larger prospective RCT, however, this is the best available evidence to support the use of statins in this population, and suggests that treating patients with NAFLD with statins is safe and effective.
CHALLENGES TO IMPLEMENTATION: Extensive Dx tests are costly
Study participants were evaluated to rule out other causes of their abnormal liver tests, with extensive laboratory tests and an ultrasound evaluation of the liver. Such extensive testing may be cost prohibitive in some situations.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Athyros VG, Tziomalos K, Gossios TD, et al. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post hoc analysis. Lancet. 2010;376:1916-1922.
2. Kim CH, Younossi ZM. Nonalcoholic fatty liver disease: a manifestation of the metabolic syndrome. Cleve Clin J Med. 2008;75:721-728.
3. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221-1231.
4. Adams LA, LympJ F, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113-121.
5. Soderberg C, Stal P, Askling J, et al. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology. 2010;51:595-602.
6. Targher G, Day CP, Bonora E. Risk of cardiovascular diseases in patients with nonalcoholic fatty liver. N Engl J Med. 2010;363:1341-1350.
7. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51:121-129.
8. Angelico F, Burattin M, Alessandri C, et al. Drugs improving insulin resistance for nonalcoholic fatty liver disease and/or non-alcoholic steatohepatitis. Cochrane Database Syst Rev. 2007;(1):CD005166.-
9. Hyogo H, Tazuma S, Arihiro K, et al. Efficacy of atorvastatin for the treatment of nonalcoholic steatohepatitis with dyslipidemia. Metabolism. 2008;57:1711-1718.
10. Georgescu EF, Georgescu M. Therapeutic options in non-alcoholic steatohepatitis (NASH). Are all agents alike? Results of a preliminary study. J Gastrointestin Liver Dis. 2007;16:39-46.
11. Rzouq FS, Volk ML, Hatoum HH, et al. Hepatotoxicity fears contribute to underutilization of statin medications by primary care physicians. Am J Med Sci. 2010;340:89-93.
Treat patients with hyperlipidemia and presumed nonalcoholic fatty liver disease with atorvastatin to reduce the risk of cardiovascular events.1
STRENGTH OF RECOMMENDATION
B: Based on a single prospective randomized controlled trial (RCT).
Athyros VG, Tziomalos K, Gossios TD, et al. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post hoc analysis. Lancet. 2010; 376:1916-1922.
ILLUSTRATIVE CASE
An obese 58-year-old man with type 2 diabetes comes to your office for follow-up. His low-density lipoprotein cholesterol (LDL-C) is 130 mg/dL; triglycerides, 300 mg/dL; alanine transaminase (ALT), 110 units/L; and aspartate transaminase (AST), 120 units/L. The patient’s work-up for chronic hepatitis B and C, autoimmune hepatitis, hemochromatosis, and Wilson’s disease are negative, and you rule out alcohol misuse based on his medical history. An ultrasound of the patient’s liver reveals hepatic steatosis, and you diagnose nonalcoholic fatty liver disease (NAFLD). Should you start him on a statin?
Patients with central obesity, diabetes, hypertension, hyperlipidemia, and metabolic syndrome are at high risk of developing NAFLD. These conditions have increased in prevalence, and NAFLD is now the most common cause of liver disease in the United States.2 In Western industrialized countries, approximately 30% of the general population and 70% to 90% of patients with diabetes will develop NAFLD.3 Although most patients are asymptomatic, their liver enzymes are elevated. To diagnose NAFLD, it is necessary to rule out alcoholic hepatitis with a medical history, and viral hepatitis, hereditary hemochromatosis, Wilson’s disease, and autoimmune hepatitis with laboratory testing. Ultrasound reveals fat accumulation in the liver.
Treatment for NAFLD has little evidence of benefit
Patients with NAFLD have a much higher mortality rate than that of the general public, primarily because of cardiovascular disease.4-6 Increased physical activity and weight loss is the only therapy that has solid evidence of a benefit,7 although other treatments, such as insulin-sensitizing drugs (metformin or pioglitazone), may be beneficial.8 Surprisingly, atorvastatin has been found to reduce aminotransferase levels in patients with NAFLD,9,10 but clinicians are often concerned about prescribing a statin for patients with elevated liver enzymes. In one study, 50% of primary care physicians said they would not prescribe statins for patients whose liver enzymes are 1.5× the upper limit of normal (ULN).11
STUDY SUMMARY: Statins lower risk of cardiovascular morbidity and mortality
The Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) study was a randomized, prospective open-label, intention-to-treat trial involving 1600 patients. All had established coronary heart disease (CHD), were younger than 75 years, and had triglycerides <400 mg/dL and LDL-C >100 mg/dL. The study reviewed here—evaluating the risk-to-benefit ratio of using a statin to treat hyperlipidemia in patients with NAFLD—was a post hoc analysis of the GREACE study.1
Participants were randomized to either usual care or structured care with atorvastatin, starting at 10 mg/d and adjusted to 80 mg/d to bring the LDL-C level below 100 mg/dL. In the usual care group, treatment included lifestyle changes plus necessary drug treatments (only 30% of those in the usual care group received hyperlipidemia drugs). Patients were followed after medication dose titration, then every 6 months for 3 years. Serum ALT and AST were measured at baseline, at 6 weeks, and every 6 months.
At baseline, mild-to-moderate increases (<3× ULN) in ALT/AST were noted in 437 of the 1600 patients. For these patients, alcoholic hepatitis, chronic hepatitis B and C, Wilson’s disease, and autoimmune hepatitis were excluded by history, laboratory tests, and ultrasound, and the elevated liver enzymes were attributed to NAFLD.
The primary endpoints were the first occurrence of any cardiovascular event, including nonfatal myocardial infarction, revascularization, unstable angina, heart failure, and stroke; all-cause mortality; and CHD mortality. The relative risk (RR) for such events was calculated for the 437 patients with elevated liver enzymes, compared with that of patients without abnormal liver tests. Elevated liver enzymes and liver-related adverse events were secondary endpoints.
A cardiovascular event occurred in 10% (22/227) of the patients with elevated liver enzymes who received a statin, and 30% (63/210) of patients who had elevated liver enzymes but did not receive a statin.
There were 3.2 events per 100 patient-years in the atorvastatin group, compared with 10 events per 100 patient-years in those not on atorvastatin, a 68% reduction in RR (P<.0001) and an NNT of 15 per year to prevent one cardiovascular event. The risk reduction in cardiovascular events was greater in patients with NAFLD (68%) than in patients with normal liver tests (39%).
An added benefit was the reduction in ALT/AST levels during treatment for patients with NAFLD who were taking a statin, an average decrease of 47% in AST levels and 35% in ALT levels. In addition, 89% of the patients in the statin group had normal ALT, AST, and gamma-glutamyl transferase levels by the end of the 3-year follow-up. Patients with NAFLD who did not receive statins had a 12% increase in AST and ALT by the end of the 3-year study.
Only 10 of 880 patients taking statins developed liver enzymes more than 3× ULN. In 3 of these patients, dose adjustments brought the liver enzymes back to normal. Only 7 (<1%) patients who received a statin had to discontinue therapy because of liver-related adverse effects.
WHAT’S NEW: Liver enzymes improve, with few adverse effects
Preliminary studies have shown an improvement in liver enzymes in patients with NAFLD treated with a statin.9,10 This is the first study to show survival benefits and significant reduction in major cardiovascular morbidity for such patients, as well.
This is also the first large-scale study that shows that treating NAFLD patients with a statin decreases liver enzyme levels, with minimal adverse effects.
CAVEATS: Differences in groups, few women could skew results
This study cannot be considered the final word on this topic. Patients in the “structured care” group were followed at a university clinic, while those in the “usual care” group were followed by either a family physician or a cardiologist outside the hospital, based on their choice. There may have been other differences in the care received by the 2 groups that could account for the difference in mortality and morbidity reduction.
In addition, study participants had coronary artery disease, and atorvastatin was not used for primary prevention. Moreover, nearly 80% of the study participants were male, which raises the question of generalizability. And this study was a post hoc analysis of the larger GREACE study, which also raises concerns about the validity of findings.
In the absence of a larger prospective RCT, however, this is the best available evidence to support the use of statins in this population, and suggests that treating patients with NAFLD with statins is safe and effective.
CHALLENGES TO IMPLEMENTATION: Extensive Dx tests are costly
Study participants were evaluated to rule out other causes of their abnormal liver tests, with extensive laboratory tests and an ultrasound evaluation of the liver. Such extensive testing may be cost prohibitive in some situations.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Treat patients with hyperlipidemia and presumed nonalcoholic fatty liver disease with atorvastatin to reduce the risk of cardiovascular events.1
STRENGTH OF RECOMMENDATION
B: Based on a single prospective randomized controlled trial (RCT).
Athyros VG, Tziomalos K, Gossios TD, et al. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post hoc analysis. Lancet. 2010; 376:1916-1922.
ILLUSTRATIVE CASE
An obese 58-year-old man with type 2 diabetes comes to your office for follow-up. His low-density lipoprotein cholesterol (LDL-C) is 130 mg/dL; triglycerides, 300 mg/dL; alanine transaminase (ALT), 110 units/L; and aspartate transaminase (AST), 120 units/L. The patient’s work-up for chronic hepatitis B and C, autoimmune hepatitis, hemochromatosis, and Wilson’s disease are negative, and you rule out alcohol misuse based on his medical history. An ultrasound of the patient’s liver reveals hepatic steatosis, and you diagnose nonalcoholic fatty liver disease (NAFLD). Should you start him on a statin?
Patients with central obesity, diabetes, hypertension, hyperlipidemia, and metabolic syndrome are at high risk of developing NAFLD. These conditions have increased in prevalence, and NAFLD is now the most common cause of liver disease in the United States.2 In Western industrialized countries, approximately 30% of the general population and 70% to 90% of patients with diabetes will develop NAFLD.3 Although most patients are asymptomatic, their liver enzymes are elevated. To diagnose NAFLD, it is necessary to rule out alcoholic hepatitis with a medical history, and viral hepatitis, hereditary hemochromatosis, Wilson’s disease, and autoimmune hepatitis with laboratory testing. Ultrasound reveals fat accumulation in the liver.
Treatment for NAFLD has little evidence of benefit
Patients with NAFLD have a much higher mortality rate than that of the general public, primarily because of cardiovascular disease.4-6 Increased physical activity and weight loss is the only therapy that has solid evidence of a benefit,7 although other treatments, such as insulin-sensitizing drugs (metformin or pioglitazone), may be beneficial.8 Surprisingly, atorvastatin has been found to reduce aminotransferase levels in patients with NAFLD,9,10 but clinicians are often concerned about prescribing a statin for patients with elevated liver enzymes. In one study, 50% of primary care physicians said they would not prescribe statins for patients whose liver enzymes are 1.5× the upper limit of normal (ULN).11
STUDY SUMMARY: Statins lower risk of cardiovascular morbidity and mortality
The Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) study was a randomized, prospective open-label, intention-to-treat trial involving 1600 patients. All had established coronary heart disease (CHD), were younger than 75 years, and had triglycerides <400 mg/dL and LDL-C >100 mg/dL. The study reviewed here—evaluating the risk-to-benefit ratio of using a statin to treat hyperlipidemia in patients with NAFLD—was a post hoc analysis of the GREACE study.1
Participants were randomized to either usual care or structured care with atorvastatin, starting at 10 mg/d and adjusted to 80 mg/d to bring the LDL-C level below 100 mg/dL. In the usual care group, treatment included lifestyle changes plus necessary drug treatments (only 30% of those in the usual care group received hyperlipidemia drugs). Patients were followed after medication dose titration, then every 6 months for 3 years. Serum ALT and AST were measured at baseline, at 6 weeks, and every 6 months.
At baseline, mild-to-moderate increases (<3× ULN) in ALT/AST were noted in 437 of the 1600 patients. For these patients, alcoholic hepatitis, chronic hepatitis B and C, Wilson’s disease, and autoimmune hepatitis were excluded by history, laboratory tests, and ultrasound, and the elevated liver enzymes were attributed to NAFLD.
The primary endpoints were the first occurrence of any cardiovascular event, including nonfatal myocardial infarction, revascularization, unstable angina, heart failure, and stroke; all-cause mortality; and CHD mortality. The relative risk (RR) for such events was calculated for the 437 patients with elevated liver enzymes, compared with that of patients without abnormal liver tests. Elevated liver enzymes and liver-related adverse events were secondary endpoints.
A cardiovascular event occurred in 10% (22/227) of the patients with elevated liver enzymes who received a statin, and 30% (63/210) of patients who had elevated liver enzymes but did not receive a statin.
There were 3.2 events per 100 patient-years in the atorvastatin group, compared with 10 events per 100 patient-years in those not on atorvastatin, a 68% reduction in RR (P<.0001) and an NNT of 15 per year to prevent one cardiovascular event. The risk reduction in cardiovascular events was greater in patients with NAFLD (68%) than in patients with normal liver tests (39%).
An added benefit was the reduction in ALT/AST levels during treatment for patients with NAFLD who were taking a statin, an average decrease of 47% in AST levels and 35% in ALT levels. In addition, 89% of the patients in the statin group had normal ALT, AST, and gamma-glutamyl transferase levels by the end of the 3-year follow-up. Patients with NAFLD who did not receive statins had a 12% increase in AST and ALT by the end of the 3-year study.
Only 10 of 880 patients taking statins developed liver enzymes more than 3× ULN. In 3 of these patients, dose adjustments brought the liver enzymes back to normal. Only 7 (<1%) patients who received a statin had to discontinue therapy because of liver-related adverse effects.
WHAT’S NEW: Liver enzymes improve, with few adverse effects
Preliminary studies have shown an improvement in liver enzymes in patients with NAFLD treated with a statin.9,10 This is the first study to show survival benefits and significant reduction in major cardiovascular morbidity for such patients, as well.
This is also the first large-scale study that shows that treating NAFLD patients with a statin decreases liver enzyme levels, with minimal adverse effects.
CAVEATS: Differences in groups, few women could skew results
This study cannot be considered the final word on this topic. Patients in the “structured care” group were followed at a university clinic, while those in the “usual care” group were followed by either a family physician or a cardiologist outside the hospital, based on their choice. There may have been other differences in the care received by the 2 groups that could account for the difference in mortality and morbidity reduction.
In addition, study participants had coronary artery disease, and atorvastatin was not used for primary prevention. Moreover, nearly 80% of the study participants were male, which raises the question of generalizability. And this study was a post hoc analysis of the larger GREACE study, which also raises concerns about the validity of findings.
In the absence of a larger prospective RCT, however, this is the best available evidence to support the use of statins in this population, and suggests that treating patients with NAFLD with statins is safe and effective.
CHALLENGES TO IMPLEMENTATION: Extensive Dx tests are costly
Study participants were evaluated to rule out other causes of their abnormal liver tests, with extensive laboratory tests and an ultrasound evaluation of the liver. Such extensive testing may be cost prohibitive in some situations.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Athyros VG, Tziomalos K, Gossios TD, et al. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post hoc analysis. Lancet. 2010;376:1916-1922.
2. Kim CH, Younossi ZM. Nonalcoholic fatty liver disease: a manifestation of the metabolic syndrome. Cleve Clin J Med. 2008;75:721-728.
3. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221-1231.
4. Adams LA, LympJ F, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113-121.
5. Soderberg C, Stal P, Askling J, et al. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology. 2010;51:595-602.
6. Targher G, Day CP, Bonora E. Risk of cardiovascular diseases in patients with nonalcoholic fatty liver. N Engl J Med. 2010;363:1341-1350.
7. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51:121-129.
8. Angelico F, Burattin M, Alessandri C, et al. Drugs improving insulin resistance for nonalcoholic fatty liver disease and/or non-alcoholic steatohepatitis. Cochrane Database Syst Rev. 2007;(1):CD005166.-
9. Hyogo H, Tazuma S, Arihiro K, et al. Efficacy of atorvastatin for the treatment of nonalcoholic steatohepatitis with dyslipidemia. Metabolism. 2008;57:1711-1718.
10. Georgescu EF, Georgescu M. Therapeutic options in non-alcoholic steatohepatitis (NASH). Are all agents alike? Results of a preliminary study. J Gastrointestin Liver Dis. 2007;16:39-46.
11. Rzouq FS, Volk ML, Hatoum HH, et al. Hepatotoxicity fears contribute to underutilization of statin medications by primary care physicians. Am J Med Sci. 2010;340:89-93.
1. Athyros VG, Tziomalos K, Gossios TD, et al. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: a post hoc analysis. Lancet. 2010;376:1916-1922.
2. Kim CH, Younossi ZM. Nonalcoholic fatty liver disease: a manifestation of the metabolic syndrome. Cleve Clin J Med. 2008;75:721-728.
3. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med. 2002;346:1221-1231.
4. Adams LA, LympJ F, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113-121.
5. Soderberg C, Stal P, Askling J, et al. Decreased survival of subjects with elevated liver function tests during a 28-year follow-up. Hepatology. 2010;51:595-602.
6. Targher G, Day CP, Bonora E. Risk of cardiovascular diseases in patients with nonalcoholic fatty liver. N Engl J Med. 2010;363:1341-1350.
7. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology. 2010;51:121-129.
8. Angelico F, Burattin M, Alessandri C, et al. Drugs improving insulin resistance for nonalcoholic fatty liver disease and/or non-alcoholic steatohepatitis. Cochrane Database Syst Rev. 2007;(1):CD005166.-
9. Hyogo H, Tazuma S, Arihiro K, et al. Efficacy of atorvastatin for the treatment of nonalcoholic steatohepatitis with dyslipidemia. Metabolism. 2008;57:1711-1718.
10. Georgescu EF, Georgescu M. Therapeutic options in non-alcoholic steatohepatitis (NASH). Are all agents alike? Results of a preliminary study. J Gastrointestin Liver Dis. 2007;16:39-46.
11. Rzouq FS, Volk ML, Hatoum HH, et al. Hepatotoxicity fears contribute to underutilization of statin medications by primary care physicians. Am J Med Sci. 2010;340:89-93.
Copyright © 2011 The Family Physicians Inquiries Network.
All rights reserved.
Consider this option for heavy menstrual bleeding
Offer tranexamic acid to patients with heavy menstrual bleeding. The extended-release formulation is effective and well tolerated.1
STRENGTH OF RECOMMENDATION
A: Based on 1 good-quality randomized controlled trial (RCT).
Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116:865-875.
ILLUSTRATIVE CASE
A 32-year-old woman comes to your office complaining of heavy, but regular, menstrual bleeding, accompanied by clots and heavy cramping that often leave her drained and unable to work. She has taken oral contraceptives in the past, but they caused nausea, and nonsteroidal anti-inflammatory drugs (NSAIDs) did not provide adequate symptom relief.
A pelvic ultrasound shows that the patient has normal endometrial thickness and no fibroids. Aside from surgical intervention or the placement of a hormonal intrauterine device (IUD), what can you offer her?
Heavy menstrual bleeding is a frequent problem, common enough to cause an estimated 10% to 30% of women of reproductive age to seek treatment.2-4 Often the bleeding is severe enough to adversely affect the patient’s social, physical, and emotional well-being.
Adverse effects, variable efficacy limit use of other treatments
Quantitatively defined as blood loss ≥80 mL per cycle, heavy menstrual bleeding can also be diagnosed based on a patient’s perception of menstrual blood loss and its effect on her daily life.5,6 NSAIDs, hormonal medications, the placement of a hormonal IUD, and surgical procedures are all treatment options, but potential adverse effects, contraindications, personal preference, and variable efficacy can limit their use.7
The fibrinolysis-blood loss link
Fibrinolytic activity in menstrual blood, leading to increasing blood loss, has prompted the evaluation of hemostatic agents as potential therapeutic options.8 Oral tranexamic acid decreases fibrinolysis, thereby reducing menstrual blood loss;9 however, gastrointestinal (GI) side effects limit the usefulness of immediate-release tranexamic acid.9,10
This formulation of tranexamic acid has been used in Europe for heavy menstrual bleeding. A Cochrane review published in 2000 included 4 studies that compared immediate-release tranexamic acid therapy with placebo. The meta-analysis found a significant reduction in mean blood loss compared with placebo (weighted mean difference [WMD]=-94.0 mL; 95% confidence interval [CI], -151.4 to -36.5) and a significant change in mean reduction of blood loss (WMD=-110.2 mL; 95% CI, -146.5 to -73.8) compared with baseline in the treatment group. However, only one of the studies measured perceived improvement in monthly menstrual blood loss, and its sample size was inadequate to provide a precise estimate of the effect (relative risk [RR] 2.5; 95% CI, 0.9-7.3).11
An extended-release option. Oral extended-release (ER) tranexamic acid (Lysteda), approved by the US Food and Drug Administration in 2009,12 reduces blood loss with fewer GI effects than immediate-release tranexamic acid. In the RCT detailed below, Lukes et al assessed the efficacy and safety of this new formulation.
STUDY SUMMARY: ER formulation reduces blood loss, boosts quality of life
The researchers conducted a multicenter, randomized, double-blind placebo-controlled study comparing the effect of ER tranexamic acid on reduction of menstrual blood flow compared with placebo.1 Reduction in menstrual blood loss >50 mL and a reduction in menstrual blood loss ≥36 mL (an amount previously established to be perceived as meaningful to women) were related primary outcomes. Improvements in limitations in social or leisure and physical activities and in self-perceived menstrual blood loss were secondary outcomes.
Study participants were women ages 18 to 49 years who had heavy menstrual bleeding, a normal pelvic exam, and a normal transvaginal ultrasound; current use of a nonhormonal birth control method was also required. Women with fibroids were not excluded unless surgery was planned. Exclusion criteria included significant coagulation issues, endocrinopathy, ocular disease, pregnancy or lactation, endometrial abnormalities, cervical cancer, anovulatory dysfunctional uterine bleeding, metrorrhagia, menometrorrhagia, and polymenorrhea.
Participants were randomized to receive either tranexamic acid 1.3 g by mouth 3 times a day for 5 days per menstrual cycle, beginning with the onset of heavy bleeding, or a matched placebo. The use of anticoagulants or NSAIDs during the menstrual period was not permitted.
Heavy bleeding was defined as ≥60 mL of blood loss in one measured cycle and an average ≥80 mL of blood loss over 2 measured cycles.
Mean reduction in blood loss per cycle over 6 cycles was 70 mL (a 40.4% reduction) in the active treatment group vs 13 mL (an 8.2% reduction) in the placebo group (P<.001). The proportion of women with a ≥50% reduction from baseline in blood loss was greater in the tranexamic acid group compared with the placebo group (35% vs 7%; P<.001), yielding a number needed to treat of 4. The mean reduction in perceived blood loss was also greater in the treatment group, but the difference was not statistically significant.
The researchers used a validated menstrual quality-of-life scale that measured social and physical quality of life using a 5-point Likert scale. Women treated with tranexamic acid had a mean reduction of 0.89 points from baseline on the social and leisure activity question, compared with a mean reduction of 0.38 points for those in the placebo group. On the physical activity question, those in the tranexamic acid group had a mean reduction of 0.90 points from baseline, vs a mean decline of 0.35 points in the placebo group.
These findings indicate that the women who received tranexamic acid experienced significantly fewer limitations in social and physical activities. Responses to a question about limitations in work activities showed that the treatment group had significant improvements there, as well. The ER form of tranexamic acid used in the study was well tolerated, with no significant differences in adverse effects between the intervention and control groups.
WHAT’S NEW: Women with heavy menstrual bleeding have a new option
The ER formulation of tranexamic acid used in the study does not appear to have the GI side effects associated with the immediate-release formula.
Tranexamic acid is taken only during the menstrual cycle and does not interfere with ovulation. Thus, it can be used by women who desire fertility but are troubled by heavy bleeding.
CAVEATS: Questions about related conditions, use with hormones remain
The study included women with regular heavy menstrual periods (menorrhagia) and therefore may not be applicable to those with irregular heavy periods or anovulatory, dysfunctional uterine bleeding. In clinical practice, these conditions may overlap, but the safety and efficacy of tranexamic acid in such cases is unclear.
Another caveat, at least theoretically, is that research to date has neither identified nor excluded the possibility that tranexamic acid with concomitant use of hormonal agents might increase the risk of thrombotic events.13 This risk is low based on evidence to date, but the theoretical uncertainty leads us to be cautious about the combination of tranexamic acid and hormonal therapy for long-term use.
Xanodyne Pharmaceuticals (which manufactured Lysteda) and Ferring Pharmaceuticals (its current owner) were major sponsors of this study. While we cannot recognize any source of bias as a result of sponsorship, the independence of the investigators in publishing the findings was not clearly stated, so it is possible that future independent studies would contradict these findings.
CHALLENGES TO IMPLEMENTATION: The treatment is costly
Lysteda is expensive, costing about $170 for 30 tablets of 650 mg each.14 Cost aside, ER tranexamic acid appears to be safe, with no major barriers to its use.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116:865-875.
2. Coulter A, Peto V, Jenkinson C. Quality of life and patient satisfaction following treatment for menorrhagia. Fam Pract. 1994;11:394-401.
3. Liu Z, Doan QV, Blumenthal P, et al. A systematic review evaluating health-related quality of life, work impairment, and health-care costs and utilization in abnormal uterine bleeding. Value Health. 2007;10:183-194.
4. Shapley M, Jordan K, Croft PR. Increased vaginal bleeding: the reasons women give for consulting primary care. J Obstet Gynaecol. 2003;23:48-50.
5. Rees M. Menorrhagia. BMJ Clin Res Ed. 1987;294:759-762.
6. Wyatt KM, Dimmock PW, Walker TJ, et al. Determination of total menstrual blood loss. Fertil Steril. 2001;76:125-131.
7. Hurskainen R, Grenman S, Komi I, et al. Diagnosis and treatment of menorrhagia. Acta Obstet Gynecol Scand. 2007;86:749-757.
8. Dockeray CJ, Sheppard BL, Daly L, et al. The fibrinolytic enzyme system in normal menstruation and excessive uterine bleeding and the effect of tranexamic acid. Eur J Obstet Gynecol Reprod Biol. 1987;24:309-318.
9. Wellington K, Wagstaff AJ. Tranexamic acid: a review of its use in the management of menorrhagia. Drugs. 2003;63:1417-1433.
10. Winkler UH. The effect of tranexamic acid on the quality of life of women with heavy menstrual bleeding. Eur J Obstet Gynecol Reprod Biol. 2001;99:238-243.
11. Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy menstrual bleeding. Cochrane Database Syst Rev. 2000;(4):CD000249.-
12. US Food and Drug Administration. FDA approves Lysteda to treat heavy menstrual bleeding. November 13, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/Press Announcements/2009/ucm190551.htm. Accessed June 14, 2011.
13. Berntorp E, Floorud C, Lethagen S. No increased risk of venous thrombosis in women taking tranexamic acid. Thromb Haemost. 2001;86:714-715.
14. Lysteda Drugstore.com. Available at: http://www.drugstore.com/lysteda/650mg-tablets/qxn66479065001. Accessed June 17, 2011.
Offer tranexamic acid to patients with heavy menstrual bleeding. The extended-release formulation is effective and well tolerated.1
STRENGTH OF RECOMMENDATION
A: Based on 1 good-quality randomized controlled trial (RCT).
Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116:865-875.
ILLUSTRATIVE CASE
A 32-year-old woman comes to your office complaining of heavy, but regular, menstrual bleeding, accompanied by clots and heavy cramping that often leave her drained and unable to work. She has taken oral contraceptives in the past, but they caused nausea, and nonsteroidal anti-inflammatory drugs (NSAIDs) did not provide adequate symptom relief.
A pelvic ultrasound shows that the patient has normal endometrial thickness and no fibroids. Aside from surgical intervention or the placement of a hormonal intrauterine device (IUD), what can you offer her?
Heavy menstrual bleeding is a frequent problem, common enough to cause an estimated 10% to 30% of women of reproductive age to seek treatment.2-4 Often the bleeding is severe enough to adversely affect the patient’s social, physical, and emotional well-being.
Adverse effects, variable efficacy limit use of other treatments
Quantitatively defined as blood loss ≥80 mL per cycle, heavy menstrual bleeding can also be diagnosed based on a patient’s perception of menstrual blood loss and its effect on her daily life.5,6 NSAIDs, hormonal medications, the placement of a hormonal IUD, and surgical procedures are all treatment options, but potential adverse effects, contraindications, personal preference, and variable efficacy can limit their use.7
The fibrinolysis-blood loss link
Fibrinolytic activity in menstrual blood, leading to increasing blood loss, has prompted the evaluation of hemostatic agents as potential therapeutic options.8 Oral tranexamic acid decreases fibrinolysis, thereby reducing menstrual blood loss;9 however, gastrointestinal (GI) side effects limit the usefulness of immediate-release tranexamic acid.9,10
This formulation of tranexamic acid has been used in Europe for heavy menstrual bleeding. A Cochrane review published in 2000 included 4 studies that compared immediate-release tranexamic acid therapy with placebo. The meta-analysis found a significant reduction in mean blood loss compared with placebo (weighted mean difference [WMD]=-94.0 mL; 95% confidence interval [CI], -151.4 to -36.5) and a significant change in mean reduction of blood loss (WMD=-110.2 mL; 95% CI, -146.5 to -73.8) compared with baseline in the treatment group. However, only one of the studies measured perceived improvement in monthly menstrual blood loss, and its sample size was inadequate to provide a precise estimate of the effect (relative risk [RR] 2.5; 95% CI, 0.9-7.3).11
An extended-release option. Oral extended-release (ER) tranexamic acid (Lysteda), approved by the US Food and Drug Administration in 2009,12 reduces blood loss with fewer GI effects than immediate-release tranexamic acid. In the RCT detailed below, Lukes et al assessed the efficacy and safety of this new formulation.
STUDY SUMMARY: ER formulation reduces blood loss, boosts quality of life
The researchers conducted a multicenter, randomized, double-blind placebo-controlled study comparing the effect of ER tranexamic acid on reduction of menstrual blood flow compared with placebo.1 Reduction in menstrual blood loss >50 mL and a reduction in menstrual blood loss ≥36 mL (an amount previously established to be perceived as meaningful to women) were related primary outcomes. Improvements in limitations in social or leisure and physical activities and in self-perceived menstrual blood loss were secondary outcomes.
Study participants were women ages 18 to 49 years who had heavy menstrual bleeding, a normal pelvic exam, and a normal transvaginal ultrasound; current use of a nonhormonal birth control method was also required. Women with fibroids were not excluded unless surgery was planned. Exclusion criteria included significant coagulation issues, endocrinopathy, ocular disease, pregnancy or lactation, endometrial abnormalities, cervical cancer, anovulatory dysfunctional uterine bleeding, metrorrhagia, menometrorrhagia, and polymenorrhea.
Participants were randomized to receive either tranexamic acid 1.3 g by mouth 3 times a day for 5 days per menstrual cycle, beginning with the onset of heavy bleeding, or a matched placebo. The use of anticoagulants or NSAIDs during the menstrual period was not permitted.
Heavy bleeding was defined as ≥60 mL of blood loss in one measured cycle and an average ≥80 mL of blood loss over 2 measured cycles.
Mean reduction in blood loss per cycle over 6 cycles was 70 mL (a 40.4% reduction) in the active treatment group vs 13 mL (an 8.2% reduction) in the placebo group (P<.001). The proportion of women with a ≥50% reduction from baseline in blood loss was greater in the tranexamic acid group compared with the placebo group (35% vs 7%; P<.001), yielding a number needed to treat of 4. The mean reduction in perceived blood loss was also greater in the treatment group, but the difference was not statistically significant.
The researchers used a validated menstrual quality-of-life scale that measured social and physical quality of life using a 5-point Likert scale. Women treated with tranexamic acid had a mean reduction of 0.89 points from baseline on the social and leisure activity question, compared with a mean reduction of 0.38 points for those in the placebo group. On the physical activity question, those in the tranexamic acid group had a mean reduction of 0.90 points from baseline, vs a mean decline of 0.35 points in the placebo group.
These findings indicate that the women who received tranexamic acid experienced significantly fewer limitations in social and physical activities. Responses to a question about limitations in work activities showed that the treatment group had significant improvements there, as well. The ER form of tranexamic acid used in the study was well tolerated, with no significant differences in adverse effects between the intervention and control groups.
WHAT’S NEW: Women with heavy menstrual bleeding have a new option
The ER formulation of tranexamic acid used in the study does not appear to have the GI side effects associated with the immediate-release formula.
Tranexamic acid is taken only during the menstrual cycle and does not interfere with ovulation. Thus, it can be used by women who desire fertility but are troubled by heavy bleeding.
CAVEATS: Questions about related conditions, use with hormones remain
The study included women with regular heavy menstrual periods (menorrhagia) and therefore may not be applicable to those with irregular heavy periods or anovulatory, dysfunctional uterine bleeding. In clinical practice, these conditions may overlap, but the safety and efficacy of tranexamic acid in such cases is unclear.
Another caveat, at least theoretically, is that research to date has neither identified nor excluded the possibility that tranexamic acid with concomitant use of hormonal agents might increase the risk of thrombotic events.13 This risk is low based on evidence to date, but the theoretical uncertainty leads us to be cautious about the combination of tranexamic acid and hormonal therapy for long-term use.
Xanodyne Pharmaceuticals (which manufactured Lysteda) and Ferring Pharmaceuticals (its current owner) were major sponsors of this study. While we cannot recognize any source of bias as a result of sponsorship, the independence of the investigators in publishing the findings was not clearly stated, so it is possible that future independent studies would contradict these findings.
CHALLENGES TO IMPLEMENTATION: The treatment is costly
Lysteda is expensive, costing about $170 for 30 tablets of 650 mg each.14 Cost aside, ER tranexamic acid appears to be safe, with no major barriers to its use.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Offer tranexamic acid to patients with heavy menstrual bleeding. The extended-release formulation is effective and well tolerated.1
STRENGTH OF RECOMMENDATION
A: Based on 1 good-quality randomized controlled trial (RCT).
Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116:865-875.
ILLUSTRATIVE CASE
A 32-year-old woman comes to your office complaining of heavy, but regular, menstrual bleeding, accompanied by clots and heavy cramping that often leave her drained and unable to work. She has taken oral contraceptives in the past, but they caused nausea, and nonsteroidal anti-inflammatory drugs (NSAIDs) did not provide adequate symptom relief.
A pelvic ultrasound shows that the patient has normal endometrial thickness and no fibroids. Aside from surgical intervention or the placement of a hormonal intrauterine device (IUD), what can you offer her?
Heavy menstrual bleeding is a frequent problem, common enough to cause an estimated 10% to 30% of women of reproductive age to seek treatment.2-4 Often the bleeding is severe enough to adversely affect the patient’s social, physical, and emotional well-being.
Adverse effects, variable efficacy limit use of other treatments
Quantitatively defined as blood loss ≥80 mL per cycle, heavy menstrual bleeding can also be diagnosed based on a patient’s perception of menstrual blood loss and its effect on her daily life.5,6 NSAIDs, hormonal medications, the placement of a hormonal IUD, and surgical procedures are all treatment options, but potential adverse effects, contraindications, personal preference, and variable efficacy can limit their use.7
The fibrinolysis-blood loss link
Fibrinolytic activity in menstrual blood, leading to increasing blood loss, has prompted the evaluation of hemostatic agents as potential therapeutic options.8 Oral tranexamic acid decreases fibrinolysis, thereby reducing menstrual blood loss;9 however, gastrointestinal (GI) side effects limit the usefulness of immediate-release tranexamic acid.9,10
This formulation of tranexamic acid has been used in Europe for heavy menstrual bleeding. A Cochrane review published in 2000 included 4 studies that compared immediate-release tranexamic acid therapy with placebo. The meta-analysis found a significant reduction in mean blood loss compared with placebo (weighted mean difference [WMD]=-94.0 mL; 95% confidence interval [CI], -151.4 to -36.5) and a significant change in mean reduction of blood loss (WMD=-110.2 mL; 95% CI, -146.5 to -73.8) compared with baseline in the treatment group. However, only one of the studies measured perceived improvement in monthly menstrual blood loss, and its sample size was inadequate to provide a precise estimate of the effect (relative risk [RR] 2.5; 95% CI, 0.9-7.3).11
An extended-release option. Oral extended-release (ER) tranexamic acid (Lysteda), approved by the US Food and Drug Administration in 2009,12 reduces blood loss with fewer GI effects than immediate-release tranexamic acid. In the RCT detailed below, Lukes et al assessed the efficacy and safety of this new formulation.
STUDY SUMMARY: ER formulation reduces blood loss, boosts quality of life
The researchers conducted a multicenter, randomized, double-blind placebo-controlled study comparing the effect of ER tranexamic acid on reduction of menstrual blood flow compared with placebo.1 Reduction in menstrual blood loss >50 mL and a reduction in menstrual blood loss ≥36 mL (an amount previously established to be perceived as meaningful to women) were related primary outcomes. Improvements in limitations in social or leisure and physical activities and in self-perceived menstrual blood loss were secondary outcomes.
Study participants were women ages 18 to 49 years who had heavy menstrual bleeding, a normal pelvic exam, and a normal transvaginal ultrasound; current use of a nonhormonal birth control method was also required. Women with fibroids were not excluded unless surgery was planned. Exclusion criteria included significant coagulation issues, endocrinopathy, ocular disease, pregnancy or lactation, endometrial abnormalities, cervical cancer, anovulatory dysfunctional uterine bleeding, metrorrhagia, menometrorrhagia, and polymenorrhea.
Participants were randomized to receive either tranexamic acid 1.3 g by mouth 3 times a day for 5 days per menstrual cycle, beginning with the onset of heavy bleeding, or a matched placebo. The use of anticoagulants or NSAIDs during the menstrual period was not permitted.
Heavy bleeding was defined as ≥60 mL of blood loss in one measured cycle and an average ≥80 mL of blood loss over 2 measured cycles.
Mean reduction in blood loss per cycle over 6 cycles was 70 mL (a 40.4% reduction) in the active treatment group vs 13 mL (an 8.2% reduction) in the placebo group (P<.001). The proportion of women with a ≥50% reduction from baseline in blood loss was greater in the tranexamic acid group compared with the placebo group (35% vs 7%; P<.001), yielding a number needed to treat of 4. The mean reduction in perceived blood loss was also greater in the treatment group, but the difference was not statistically significant.
The researchers used a validated menstrual quality-of-life scale that measured social and physical quality of life using a 5-point Likert scale. Women treated with tranexamic acid had a mean reduction of 0.89 points from baseline on the social and leisure activity question, compared with a mean reduction of 0.38 points for those in the placebo group. On the physical activity question, those in the tranexamic acid group had a mean reduction of 0.90 points from baseline, vs a mean decline of 0.35 points in the placebo group.
These findings indicate that the women who received tranexamic acid experienced significantly fewer limitations in social and physical activities. Responses to a question about limitations in work activities showed that the treatment group had significant improvements there, as well. The ER form of tranexamic acid used in the study was well tolerated, with no significant differences in adverse effects between the intervention and control groups.
WHAT’S NEW: Women with heavy menstrual bleeding have a new option
The ER formulation of tranexamic acid used in the study does not appear to have the GI side effects associated with the immediate-release formula.
Tranexamic acid is taken only during the menstrual cycle and does not interfere with ovulation. Thus, it can be used by women who desire fertility but are troubled by heavy bleeding.
CAVEATS: Questions about related conditions, use with hormones remain
The study included women with regular heavy menstrual periods (menorrhagia) and therefore may not be applicable to those with irregular heavy periods or anovulatory, dysfunctional uterine bleeding. In clinical practice, these conditions may overlap, but the safety and efficacy of tranexamic acid in such cases is unclear.
Another caveat, at least theoretically, is that research to date has neither identified nor excluded the possibility that tranexamic acid with concomitant use of hormonal agents might increase the risk of thrombotic events.13 This risk is low based on evidence to date, but the theoretical uncertainty leads us to be cautious about the combination of tranexamic acid and hormonal therapy for long-term use.
Xanodyne Pharmaceuticals (which manufactured Lysteda) and Ferring Pharmaceuticals (its current owner) were major sponsors of this study. While we cannot recognize any source of bias as a result of sponsorship, the independence of the investigators in publishing the findings was not clearly stated, so it is possible that future independent studies would contradict these findings.
CHALLENGES TO IMPLEMENTATION: The treatment is costly
Lysteda is expensive, costing about $170 for 30 tablets of 650 mg each.14 Cost aside, ER tranexamic acid appears to be safe, with no major barriers to its use.
Acknowledgement
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116:865-875.
2. Coulter A, Peto V, Jenkinson C. Quality of life and patient satisfaction following treatment for menorrhagia. Fam Pract. 1994;11:394-401.
3. Liu Z, Doan QV, Blumenthal P, et al. A systematic review evaluating health-related quality of life, work impairment, and health-care costs and utilization in abnormal uterine bleeding. Value Health. 2007;10:183-194.
4. Shapley M, Jordan K, Croft PR. Increased vaginal bleeding: the reasons women give for consulting primary care. J Obstet Gynaecol. 2003;23:48-50.
5. Rees M. Menorrhagia. BMJ Clin Res Ed. 1987;294:759-762.
6. Wyatt KM, Dimmock PW, Walker TJ, et al. Determination of total menstrual blood loss. Fertil Steril. 2001;76:125-131.
7. Hurskainen R, Grenman S, Komi I, et al. Diagnosis and treatment of menorrhagia. Acta Obstet Gynecol Scand. 2007;86:749-757.
8. Dockeray CJ, Sheppard BL, Daly L, et al. The fibrinolytic enzyme system in normal menstruation and excessive uterine bleeding and the effect of tranexamic acid. Eur J Obstet Gynecol Reprod Biol. 1987;24:309-318.
9. Wellington K, Wagstaff AJ. Tranexamic acid: a review of its use in the management of menorrhagia. Drugs. 2003;63:1417-1433.
10. Winkler UH. The effect of tranexamic acid on the quality of life of women with heavy menstrual bleeding. Eur J Obstet Gynecol Reprod Biol. 2001;99:238-243.
11. Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy menstrual bleeding. Cochrane Database Syst Rev. 2000;(4):CD000249.-
12. US Food and Drug Administration. FDA approves Lysteda to treat heavy menstrual bleeding. November 13, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/Press Announcements/2009/ucm190551.htm. Accessed June 14, 2011.
13. Berntorp E, Floorud C, Lethagen S. No increased risk of venous thrombosis in women taking tranexamic acid. Thromb Haemost. 2001;86:714-715.
14. Lysteda Drugstore.com. Available at: http://www.drugstore.com/lysteda/650mg-tablets/qxn66479065001. Accessed June 17, 2011.
1. Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116:865-875.
2. Coulter A, Peto V, Jenkinson C. Quality of life and patient satisfaction following treatment for menorrhagia. Fam Pract. 1994;11:394-401.
3. Liu Z, Doan QV, Blumenthal P, et al. A systematic review evaluating health-related quality of life, work impairment, and health-care costs and utilization in abnormal uterine bleeding. Value Health. 2007;10:183-194.
4. Shapley M, Jordan K, Croft PR. Increased vaginal bleeding: the reasons women give for consulting primary care. J Obstet Gynaecol. 2003;23:48-50.
5. Rees M. Menorrhagia. BMJ Clin Res Ed. 1987;294:759-762.
6. Wyatt KM, Dimmock PW, Walker TJ, et al. Determination of total menstrual blood loss. Fertil Steril. 2001;76:125-131.
7. Hurskainen R, Grenman S, Komi I, et al. Diagnosis and treatment of menorrhagia. Acta Obstet Gynecol Scand. 2007;86:749-757.
8. Dockeray CJ, Sheppard BL, Daly L, et al. The fibrinolytic enzyme system in normal menstruation and excessive uterine bleeding and the effect of tranexamic acid. Eur J Obstet Gynecol Reprod Biol. 1987;24:309-318.
9. Wellington K, Wagstaff AJ. Tranexamic acid: a review of its use in the management of menorrhagia. Drugs. 2003;63:1417-1433.
10. Winkler UH. The effect of tranexamic acid on the quality of life of women with heavy menstrual bleeding. Eur J Obstet Gynecol Reprod Biol. 2001;99:238-243.
11. Lethaby A, Farquhar C, Cooke I. Antifibrinolytics for heavy menstrual bleeding. Cochrane Database Syst Rev. 2000;(4):CD000249.-
12. US Food and Drug Administration. FDA approves Lysteda to treat heavy menstrual bleeding. November 13, 2009. Available at: http://www.fda.gov/NewsEvents/Newsroom/Press Announcements/2009/ucm190551.htm. Accessed June 14, 2011.
13. Berntorp E, Floorud C, Lethagen S. No increased risk of venous thrombosis in women taking tranexamic acid. Thromb Haemost. 2001;86:714-715.
14. Lysteda Drugstore.com. Available at: http://www.drugstore.com/lysteda/650mg-tablets/qxn66479065001. Accessed June 17, 2011.
Copyright © 2011 The Family Physicians Inquiries Network.
All rights reserved.
Treating UTIs in reproductive-age women—Proceed with caution
Nitrofurantoin and sulfonamides may cause major birth defects and should be used with caution—if at all—in women of reproductive age.1
Strength of Recommendation
B: Population-based case-control study
1. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch Pediatr Adolesc Med. 2009;163:978-985.
Illustrative case
A 24-year-old woman comes to your clinic because of frequent urination for the past 2 to 3 days. She is not taking any medication, but does take a daily prenatal vitamin because she and her husband are trying to conceive. After your examination, you order a urinalysis and perform a urine pregnancy test. The urinalysis shows bacteriuria ≥100,000 cfu/ml, and the pregnancy test is positive.
What will you prescribe to treat her urinary tract infection?
Antibacterial agents are among the most commonly used medications during pregnancy because treatment of infections is critical to both maternal and fetal well-being.1 Urinary tract infections (UTIs) are the most common medical complication during pregnancy, with Escherichia coli contributing to roughly 90% of the infections.2 Screening for and treating asymptomatic bacteriuria is also recommended during pregnancy to prevent pyelonephritis and increased maternal and fetal morbidity.3 In addition, UTIs are common in reproductive-age women who may not know they are pregnant or who become pregnant during treatment with antibiotics. And nitrofurantoin and sulfonamides are commonly prescribed antibiotics for the treatment of UTIs, both in pregnant women and women of reproductive age.
Prior warnings only address near-term pregnancy
Prior to the study detailed in this PURL, no clinical trials had reported a teratogenic risk associated with either nitrofurantoin (current pregnancy category B) or sulfonamide (current pregnancy category C).4 It is recommended, however, that both of these antibacterials be avoided in pregnant women who are near term because of the risk of hemolytic disease in patients with glucose-6-phosphate dehydrogenase deficiency associated with nitrofurantoin and the risk of kernicterus in neonates exposed to sulfamethoxazole.5
But a rise in E coli resistance to penicillins (resistance to amoxicillin, for example, can be as high as 30-40%6) has led to greater use of nitrofurantoin. The drug has been viewed as a safe and effective alternative treatment for UTIs associated with E coli.7 Indeed, nitrofurantoin has been considered to be the preferred antibiotic for bacteriuria suppression, as both ampicillin and cephalosporins can interfere with the normal gastrointestinal flora. Thus, nitrofurantoin is used extensively in pregnant women. Sulfonamides are also prescribed for pregnant women, although not as frequently.7,8
STUDY SUMMARY: First trimester use linked to many defects
The study by Crider et al1 was based on the National Birth Defects Prevention Study, an ongoing, population-based case control study of an estimated annual birth population of roughly 482,000, including cases identified by birth defects surveillance registries in 10 states.9 The researchers identified pregnancies affected by any of 30 types of birth defects from 1997 to 2003 (n=13,155). The controls (n=4941) were randomly selected from similar geographic locations, and matched for race/ethnicity, age, and prepregnancy body mass index. Exposure to antibacterials from 1 month prepregnancy through the end of the first trimester was recorded.
Crider et al interviewed all the participants up to 24 months after delivery to obtain their exposure history to penicillins, erythromycins, nitrofurantoin, sulfonamides, cephalosporins, quinolones, tetracyclines, other miscellaneous beta-lactams, aminoglycosides, antimycobacterial agents, and other antibiotics. (Exposure to antivirals, antifungals, and antiparasitic agents was not addressed.) Women who didn’t know whether they had been exposed to these agents or could not remember the timing of exposure were excluded.
Overall, antibacterial use ranged from 2% to 5.8%, and peaked in the third month of pregnancy. Penicillins were the most commonly used antibiotics. Odds ratios obtained for birth defects were adjusted for confounders such as maternal age, race, education level, prepregnancy body mass index, time from estimated date of delivery to the interview, use of folic acid or multivitamins from 1 month prior to pregnancy through the first month, and periconceptional smoking and/or alcohol use.
Nitrofurantoin was associated with anophthalmia or microphthalmos (adjusted odds ratio [AOR]=3.7; 95% confidence interval [CI], 1.1-12.2), hypoplastic left heart syndrome (AOR=4.2; 95% CI, 1.9-9.1), atrial septal defects (AOR=1.9; 95% CI, 1.1-3.4), and cleft lip with cleft palate (AOR=2.1; 95% CI, 1.2-3.9).
Sulfonamides were associated with anencephaly (AOR=3.4; 95% CI, 1.3-8.8), hypoplastic left heart syndrome (AOR=3.2; 95% CI, 1.3-7.6), coarctation of the aorta (AOR=2.7; 95% CI, 1.3-5.6), choanal atresia (AOR=8.0; 95% CI, 2.7-23.5), transverse limb deficiency (AOR=2.5; 95% CI, 1.0-5.9), and diaphragmatic hernia (AOR=2.4; 95% CI, 1.1-5.4).
Some links between other antibiotics and birth defects were also found. For example, erythromycins were associated with anencephaly and transverse limb deficiency, penicillins with intercalary limb deficiency, and cephalosporins with atrial septal defects. The authors noted, however, that these agents, which are commonly prescribed for pregnant women, were not associated with many birth defects—and that because of limited sample sizes for these drug classes, the associations may be spurious.
WHAT'S NEW: A large-scale study provides evidence of risk
Previous case studies and meta-analysis have shown no link between the use of nitrofurantoin and congenital abnormalities.8 Similarly, sulfonamides have not appeared to pose significant teratogenic risk. This is the first large-scale study evaluating the risk of birth defects associated with antibiotic use during pregnancy, and therefore provides evidence of risk not previously available.
CAVEATS: Study design raises questions of recall bias
The retrospective case-control methodology used in this study leaves open the possibility of recall bias, misclassification bias, and confounding bias. The length of time from actual exposure to data collection could affect the accuracy of participants’ memories. The data gathered were not cross-verified against medical records, and other issues, such as the possible effect of medications for other infections (eg, antivirals and antifungals), could not be measured. However, women who did not know or were unsure of their medication exposure history were excluded from the analysis, which should reduce the risk of this potential bias.
The investigators also controlled for several important sources of potential confounding bias, and the reporting rates were similar among participants in both the case and control groups. These measures provide some assurance that the outcomes are valid.
It would be unethical (and extraordinarily expensive) to conduct a prospective randomized controlled trial to confirm these findings. Case-control methodology is the most practical way to assess for the risk of birth defects, and our literature review suggests that this is the most rigorous study to date. In our view, the potential harm from continuing to use these antibiotics for pregnant women and women who may become pregnant far outweighs the risk that these findings may be erroneous.
That said, a final caveat is the fact that even a several-fold increase in the risk of a rare major birth defect such as those reported in this study is still a rare risk. There may be clinical situations in which the benefits of using nitrofurantoin or sulfonamides in women who are or may become pregnant outweigh the potential risks.
CHALLENGES TO IMPLEMENTATION: Finding an alternative treatment
The main challenge to implementing this new recommendation lies in choosing alternative antibiotics with which to treat UTIs in reproductive-age women and bacteriuria in pregnancy. Obtaining a pregnancy test in sexually active patients of reproductive age who are not using a reliable form of contraception seems like a prudent first step.
If the pregnancy test is positive, cephalexin should be a good initial choice until the results of culture and sensitivities are available. In the event of Enterococcus infection (for which cephalosporins are not active) or other organisms resistant to cephalosporins, the sensitivity results should provide guidance.3
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources; the grant was a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch Pediatr Adolesc Med. 2009;163:978-985.
2. Gilstrap LC, 3rd, Ramin SM. Urinary tract infections during pregnancy. Obstet Gynecol. 2001;28:581-591.
3. Macejko AM, Schaeffer AJ. Asymptomatic bacteriuria and symptomatic urinary tract infections during pregnancy. Urol Clin North Am. 2007;34:35-42.
4. Thomson Reuters (Healthcare). Micromedex® Healthcare Series Intranet. 5.1.
5. Czeizel AE, Rockenbauer M, Olsen J. Use of antibiotics during pregnancy. Eur J Obstet Gynecol Reprod Biol. 1998;81:1-8.
6. ABXguide. Urinary tract infections in pregnancy. Available at: http://prod.hopkins-abxguide.org/diagnosis/genitourinary/urinary_tract_infections_in_pregnancy.html?contentInstanceId=255490. Accessed February 15, 2010.
7. Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2002;162:41-47.
8. Shrim A, Garcia-Bournissen F, Koren G. Pharmaceutical agents and pregnancy in urology practice. Urol Clin North Am. 2007;34:27-33.
9. Yoon PW, Rasmussen SA, Lynberg MC, et al. The National Birth Defects Prevention Study. Public Health Rep. 2001;116(suppl 1):32-40.
Nitrofurantoin and sulfonamides may cause major birth defects and should be used with caution—if at all—in women of reproductive age.1
Strength of Recommendation
B: Population-based case-control study
1. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch Pediatr Adolesc Med. 2009;163:978-985.
Illustrative case
A 24-year-old woman comes to your clinic because of frequent urination for the past 2 to 3 days. She is not taking any medication, but does take a daily prenatal vitamin because she and her husband are trying to conceive. After your examination, you order a urinalysis and perform a urine pregnancy test. The urinalysis shows bacteriuria ≥100,000 cfu/ml, and the pregnancy test is positive.
What will you prescribe to treat her urinary tract infection?
Antibacterial agents are among the most commonly used medications during pregnancy because treatment of infections is critical to both maternal and fetal well-being.1 Urinary tract infections (UTIs) are the most common medical complication during pregnancy, with Escherichia coli contributing to roughly 90% of the infections.2 Screening for and treating asymptomatic bacteriuria is also recommended during pregnancy to prevent pyelonephritis and increased maternal and fetal morbidity.3 In addition, UTIs are common in reproductive-age women who may not know they are pregnant or who become pregnant during treatment with antibiotics. And nitrofurantoin and sulfonamides are commonly prescribed antibiotics for the treatment of UTIs, both in pregnant women and women of reproductive age.
Prior warnings only address near-term pregnancy
Prior to the study detailed in this PURL, no clinical trials had reported a teratogenic risk associated with either nitrofurantoin (current pregnancy category B) or sulfonamide (current pregnancy category C).4 It is recommended, however, that both of these antibacterials be avoided in pregnant women who are near term because of the risk of hemolytic disease in patients with glucose-6-phosphate dehydrogenase deficiency associated with nitrofurantoin and the risk of kernicterus in neonates exposed to sulfamethoxazole.5
But a rise in E coli resistance to penicillins (resistance to amoxicillin, for example, can be as high as 30-40%6) has led to greater use of nitrofurantoin. The drug has been viewed as a safe and effective alternative treatment for UTIs associated with E coli.7 Indeed, nitrofurantoin has been considered to be the preferred antibiotic for bacteriuria suppression, as both ampicillin and cephalosporins can interfere with the normal gastrointestinal flora. Thus, nitrofurantoin is used extensively in pregnant women. Sulfonamides are also prescribed for pregnant women, although not as frequently.7,8
STUDY SUMMARY: First trimester use linked to many defects
The study by Crider et al1 was based on the National Birth Defects Prevention Study, an ongoing, population-based case control study of an estimated annual birth population of roughly 482,000, including cases identified by birth defects surveillance registries in 10 states.9 The researchers identified pregnancies affected by any of 30 types of birth defects from 1997 to 2003 (n=13,155). The controls (n=4941) were randomly selected from similar geographic locations, and matched for race/ethnicity, age, and prepregnancy body mass index. Exposure to antibacterials from 1 month prepregnancy through the end of the first trimester was recorded.
Crider et al interviewed all the participants up to 24 months after delivery to obtain their exposure history to penicillins, erythromycins, nitrofurantoin, sulfonamides, cephalosporins, quinolones, tetracyclines, other miscellaneous beta-lactams, aminoglycosides, antimycobacterial agents, and other antibiotics. (Exposure to antivirals, antifungals, and antiparasitic agents was not addressed.) Women who didn’t know whether they had been exposed to these agents or could not remember the timing of exposure were excluded.
Overall, antibacterial use ranged from 2% to 5.8%, and peaked in the third month of pregnancy. Penicillins were the most commonly used antibiotics. Odds ratios obtained for birth defects were adjusted for confounders such as maternal age, race, education level, prepregnancy body mass index, time from estimated date of delivery to the interview, use of folic acid or multivitamins from 1 month prior to pregnancy through the first month, and periconceptional smoking and/or alcohol use.
Nitrofurantoin was associated with anophthalmia or microphthalmos (adjusted odds ratio [AOR]=3.7; 95% confidence interval [CI], 1.1-12.2), hypoplastic left heart syndrome (AOR=4.2; 95% CI, 1.9-9.1), atrial septal defects (AOR=1.9; 95% CI, 1.1-3.4), and cleft lip with cleft palate (AOR=2.1; 95% CI, 1.2-3.9).
Sulfonamides were associated with anencephaly (AOR=3.4; 95% CI, 1.3-8.8), hypoplastic left heart syndrome (AOR=3.2; 95% CI, 1.3-7.6), coarctation of the aorta (AOR=2.7; 95% CI, 1.3-5.6), choanal atresia (AOR=8.0; 95% CI, 2.7-23.5), transverse limb deficiency (AOR=2.5; 95% CI, 1.0-5.9), and diaphragmatic hernia (AOR=2.4; 95% CI, 1.1-5.4).
Some links between other antibiotics and birth defects were also found. For example, erythromycins were associated with anencephaly and transverse limb deficiency, penicillins with intercalary limb deficiency, and cephalosporins with atrial septal defects. The authors noted, however, that these agents, which are commonly prescribed for pregnant women, were not associated with many birth defects—and that because of limited sample sizes for these drug classes, the associations may be spurious.
WHAT'S NEW: A large-scale study provides evidence of risk
Previous case studies and meta-analysis have shown no link between the use of nitrofurantoin and congenital abnormalities.8 Similarly, sulfonamides have not appeared to pose significant teratogenic risk. This is the first large-scale study evaluating the risk of birth defects associated with antibiotic use during pregnancy, and therefore provides evidence of risk not previously available.
CAVEATS: Study design raises questions of recall bias
The retrospective case-control methodology used in this study leaves open the possibility of recall bias, misclassification bias, and confounding bias. The length of time from actual exposure to data collection could affect the accuracy of participants’ memories. The data gathered were not cross-verified against medical records, and other issues, such as the possible effect of medications for other infections (eg, antivirals and antifungals), could not be measured. However, women who did not know or were unsure of their medication exposure history were excluded from the analysis, which should reduce the risk of this potential bias.
The investigators also controlled for several important sources of potential confounding bias, and the reporting rates were similar among participants in both the case and control groups. These measures provide some assurance that the outcomes are valid.
It would be unethical (and extraordinarily expensive) to conduct a prospective randomized controlled trial to confirm these findings. Case-control methodology is the most practical way to assess for the risk of birth defects, and our literature review suggests that this is the most rigorous study to date. In our view, the potential harm from continuing to use these antibiotics for pregnant women and women who may become pregnant far outweighs the risk that these findings may be erroneous.
That said, a final caveat is the fact that even a several-fold increase in the risk of a rare major birth defect such as those reported in this study is still a rare risk. There may be clinical situations in which the benefits of using nitrofurantoin or sulfonamides in women who are or may become pregnant outweigh the potential risks.
CHALLENGES TO IMPLEMENTATION: Finding an alternative treatment
The main challenge to implementing this new recommendation lies in choosing alternative antibiotics with which to treat UTIs in reproductive-age women and bacteriuria in pregnancy. Obtaining a pregnancy test in sexually active patients of reproductive age who are not using a reliable form of contraception seems like a prudent first step.
If the pregnancy test is positive, cephalexin should be a good initial choice until the results of culture and sensitivities are available. In the event of Enterococcus infection (for which cephalosporins are not active) or other organisms resistant to cephalosporins, the sensitivity results should provide guidance.3
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources; the grant was a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Nitrofurantoin and sulfonamides may cause major birth defects and should be used with caution—if at all—in women of reproductive age.1
Strength of Recommendation
B: Population-based case-control study
1. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch Pediatr Adolesc Med. 2009;163:978-985.
Illustrative case
A 24-year-old woman comes to your clinic because of frequent urination for the past 2 to 3 days. She is not taking any medication, but does take a daily prenatal vitamin because she and her husband are trying to conceive. After your examination, you order a urinalysis and perform a urine pregnancy test. The urinalysis shows bacteriuria ≥100,000 cfu/ml, and the pregnancy test is positive.
What will you prescribe to treat her urinary tract infection?
Antibacterial agents are among the most commonly used medications during pregnancy because treatment of infections is critical to both maternal and fetal well-being.1 Urinary tract infections (UTIs) are the most common medical complication during pregnancy, with Escherichia coli contributing to roughly 90% of the infections.2 Screening for and treating asymptomatic bacteriuria is also recommended during pregnancy to prevent pyelonephritis and increased maternal and fetal morbidity.3 In addition, UTIs are common in reproductive-age women who may not know they are pregnant or who become pregnant during treatment with antibiotics. And nitrofurantoin and sulfonamides are commonly prescribed antibiotics for the treatment of UTIs, both in pregnant women and women of reproductive age.
Prior warnings only address near-term pregnancy
Prior to the study detailed in this PURL, no clinical trials had reported a teratogenic risk associated with either nitrofurantoin (current pregnancy category B) or sulfonamide (current pregnancy category C).4 It is recommended, however, that both of these antibacterials be avoided in pregnant women who are near term because of the risk of hemolytic disease in patients with glucose-6-phosphate dehydrogenase deficiency associated with nitrofurantoin and the risk of kernicterus in neonates exposed to sulfamethoxazole.5
But a rise in E coli resistance to penicillins (resistance to amoxicillin, for example, can be as high as 30-40%6) has led to greater use of nitrofurantoin. The drug has been viewed as a safe and effective alternative treatment for UTIs associated with E coli.7 Indeed, nitrofurantoin has been considered to be the preferred antibiotic for bacteriuria suppression, as both ampicillin and cephalosporins can interfere with the normal gastrointestinal flora. Thus, nitrofurantoin is used extensively in pregnant women. Sulfonamides are also prescribed for pregnant women, although not as frequently.7,8
STUDY SUMMARY: First trimester use linked to many defects
The study by Crider et al1 was based on the National Birth Defects Prevention Study, an ongoing, population-based case control study of an estimated annual birth population of roughly 482,000, including cases identified by birth defects surveillance registries in 10 states.9 The researchers identified pregnancies affected by any of 30 types of birth defects from 1997 to 2003 (n=13,155). The controls (n=4941) were randomly selected from similar geographic locations, and matched for race/ethnicity, age, and prepregnancy body mass index. Exposure to antibacterials from 1 month prepregnancy through the end of the first trimester was recorded.
Crider et al interviewed all the participants up to 24 months after delivery to obtain their exposure history to penicillins, erythromycins, nitrofurantoin, sulfonamides, cephalosporins, quinolones, tetracyclines, other miscellaneous beta-lactams, aminoglycosides, antimycobacterial agents, and other antibiotics. (Exposure to antivirals, antifungals, and antiparasitic agents was not addressed.) Women who didn’t know whether they had been exposed to these agents or could not remember the timing of exposure were excluded.
Overall, antibacterial use ranged from 2% to 5.8%, and peaked in the third month of pregnancy. Penicillins were the most commonly used antibiotics. Odds ratios obtained for birth defects were adjusted for confounders such as maternal age, race, education level, prepregnancy body mass index, time from estimated date of delivery to the interview, use of folic acid or multivitamins from 1 month prior to pregnancy through the first month, and periconceptional smoking and/or alcohol use.
Nitrofurantoin was associated with anophthalmia or microphthalmos (adjusted odds ratio [AOR]=3.7; 95% confidence interval [CI], 1.1-12.2), hypoplastic left heart syndrome (AOR=4.2; 95% CI, 1.9-9.1), atrial septal defects (AOR=1.9; 95% CI, 1.1-3.4), and cleft lip with cleft palate (AOR=2.1; 95% CI, 1.2-3.9).
Sulfonamides were associated with anencephaly (AOR=3.4; 95% CI, 1.3-8.8), hypoplastic left heart syndrome (AOR=3.2; 95% CI, 1.3-7.6), coarctation of the aorta (AOR=2.7; 95% CI, 1.3-5.6), choanal atresia (AOR=8.0; 95% CI, 2.7-23.5), transverse limb deficiency (AOR=2.5; 95% CI, 1.0-5.9), and diaphragmatic hernia (AOR=2.4; 95% CI, 1.1-5.4).
Some links between other antibiotics and birth defects were also found. For example, erythromycins were associated with anencephaly and transverse limb deficiency, penicillins with intercalary limb deficiency, and cephalosporins with atrial septal defects. The authors noted, however, that these agents, which are commonly prescribed for pregnant women, were not associated with many birth defects—and that because of limited sample sizes for these drug classes, the associations may be spurious.
WHAT'S NEW: A large-scale study provides evidence of risk
Previous case studies and meta-analysis have shown no link between the use of nitrofurantoin and congenital abnormalities.8 Similarly, sulfonamides have not appeared to pose significant teratogenic risk. This is the first large-scale study evaluating the risk of birth defects associated with antibiotic use during pregnancy, and therefore provides evidence of risk not previously available.
CAVEATS: Study design raises questions of recall bias
The retrospective case-control methodology used in this study leaves open the possibility of recall bias, misclassification bias, and confounding bias. The length of time from actual exposure to data collection could affect the accuracy of participants’ memories. The data gathered were not cross-verified against medical records, and other issues, such as the possible effect of medications for other infections (eg, antivirals and antifungals), could not be measured. However, women who did not know or were unsure of their medication exposure history were excluded from the analysis, which should reduce the risk of this potential bias.
The investigators also controlled for several important sources of potential confounding bias, and the reporting rates were similar among participants in both the case and control groups. These measures provide some assurance that the outcomes are valid.
It would be unethical (and extraordinarily expensive) to conduct a prospective randomized controlled trial to confirm these findings. Case-control methodology is the most practical way to assess for the risk of birth defects, and our literature review suggests that this is the most rigorous study to date. In our view, the potential harm from continuing to use these antibiotics for pregnant women and women who may become pregnant far outweighs the risk that these findings may be erroneous.
That said, a final caveat is the fact that even a several-fold increase in the risk of a rare major birth defect such as those reported in this study is still a rare risk. There may be clinical situations in which the benefits of using nitrofurantoin or sulfonamides in women who are or may become pregnant outweigh the potential risks.
CHALLENGES TO IMPLEMENTATION: Finding an alternative treatment
The main challenge to implementing this new recommendation lies in choosing alternative antibiotics with which to treat UTIs in reproductive-age women and bacteriuria in pregnancy. Obtaining a pregnancy test in sexually active patients of reproductive age who are not using a reliable form of contraception seems like a prudent first step.
If the pregnancy test is positive, cephalexin should be a good initial choice until the results of culture and sensitivities are available. In the event of Enterococcus infection (for which cephalosporins are not active) or other organisms resistant to cephalosporins, the sensitivity results should provide guidance.3
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources; the grant was a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch Pediatr Adolesc Med. 2009;163:978-985.
2. Gilstrap LC, 3rd, Ramin SM. Urinary tract infections during pregnancy. Obstet Gynecol. 2001;28:581-591.
3. Macejko AM, Schaeffer AJ. Asymptomatic bacteriuria and symptomatic urinary tract infections during pregnancy. Urol Clin North Am. 2007;34:35-42.
4. Thomson Reuters (Healthcare). Micromedex® Healthcare Series Intranet. 5.1.
5. Czeizel AE, Rockenbauer M, Olsen J. Use of antibiotics during pregnancy. Eur J Obstet Gynecol Reprod Biol. 1998;81:1-8.
6. ABXguide. Urinary tract infections in pregnancy. Available at: http://prod.hopkins-abxguide.org/diagnosis/genitourinary/urinary_tract_infections_in_pregnancy.html?contentInstanceId=255490. Accessed February 15, 2010.
7. Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2002;162:41-47.
8. Shrim A, Garcia-Bournissen F, Koren G. Pharmaceutical agents and pregnancy in urology practice. Urol Clin North Am. 2007;34:27-33.
9. Yoon PW, Rasmussen SA, Lynberg MC, et al. The National Birth Defects Prevention Study. Public Health Rep. 2001;116(suppl 1):32-40.
1. Crider KS, Cleves MA, Reefhuis J, et al. Antibacterial medication use during pregnancy and risk of birth defects: National Birth Defects Prevention Study. Arch Pediatr Adolesc Med. 2009;163:978-985.
2. Gilstrap LC, 3rd, Ramin SM. Urinary tract infections during pregnancy. Obstet Gynecol. 2001;28:581-591.
3. Macejko AM, Schaeffer AJ. Asymptomatic bacteriuria and symptomatic urinary tract infections during pregnancy. Urol Clin North Am. 2007;34:35-42.
4. Thomson Reuters (Healthcare). Micromedex® Healthcare Series Intranet. 5.1.
5. Czeizel AE, Rockenbauer M, Olsen J. Use of antibiotics during pregnancy. Eur J Obstet Gynecol Reprod Biol. 1998;81:1-8.
6. ABXguide. Urinary tract infections in pregnancy. Available at: http://prod.hopkins-abxguide.org/diagnosis/genitourinary/urinary_tract_infections_in_pregnancy.html?contentInstanceId=255490. Accessed February 15, 2010.
7. Huang ES, Stafford RS. National patterns in the treatment of urinary tract infections in women by ambulatory care physicians. Arch Intern Med. 2002;162:41-47.
8. Shrim A, Garcia-Bournissen F, Koren G. Pharmaceutical agents and pregnancy in urology practice. Urol Clin North Am. 2007;34:27-33.
9. Yoon PW, Rasmussen SA, Lynberg MC, et al. The National Birth Defects Prevention Study. Public Health Rep. 2001;116(suppl 1):32-40.
Copyright © 2010 The Family Physicians Inquiries Network.
All rights reserved.
Help patients prevent repeat ankle injury
Advise patients being treated for ankle sprain that reinjury—which is especially common during the first year—can result in chronic pain or disability, and that a home-based proprioceptive training program has been shown to significantly reduce the risk of recurrent sprain.1
STRENGTH OF RECOMMENDATION
A: Based on a high-quality randomized controlled trial (RCT).
Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ. 2009;339:b2684.
ILLUSTRATIVE CASE
A 35-year-old man comes to see you 1 day after injuring his left ankle, which he inverted while playing racquetball in a semicompetitive league. After a clinical exam, you diagnose an ankle sprain. You advise him to wrap the ankle for protection and recommend rest, ice, compression, and elevation. Besides treatment for the current sprain, however, he asks what he can do after recovery to prevent ankle reinjury.
What can you tell him?
An estimated 23,000 ankle sprains occur every day in the United States, which amounts to approximately 1 in every 10,000 people.2 In many sports, ankle sprain is the most common injury,3 partly because an athlete who incurs a first ankle sprain is at increased risk of another.4-6 The risk of reinjury is highest in the year immediately following the initial sprain.6-8
Long-term effects of repeat sprains
About half of recurrent ankle sprains result in chronic pain or disability, so preventing repeat sprains is an important patient-oriented treatment goal. Various modalities, including bracing, taping, and warm-up and strengthening exercises, have been used to prevent recurrence of ankle sprain. Proprioceptive training has also been suggested.5,9 A Cochrane review in 2001 found limited evidence for reduction of ankle sprain recurrence after proprioceptive exercises.10 Until the study reviewed in this PURL, its effectiveness remained uncertain.
STUDY SUMMARY: Exercise program reduces risk
Hupperets et al1 investigated the effectiveness of a home-based proprioceptive training program to prevent ankle sprain recurrence. Enrollees (N=522) in this well-done RCT were active sports participants ranging in age from 12 to 70 years, all of whom had incurred ankle sprains in the preceding 2 months. They were recruited throughout The Netherlands using a variety of medical channels—emergency departments, general practices, and physical therapy offices—and advertisements in newspapers and sports magazines, at sports tournaments, and on the Internet.
The athletes were randomized to the intervention or control group, with stratification for sex, type of enrollment, and type of care they initially received for the ankle sprain—which the participants in both groups received without interference from the authors. (Among the enrollees were 181 people who did not receive any medical care for their sprains.)
Participants in the intervention group were given an instructional DVD, a balance board, and an exercise sheet, with further instructions available on a Web site. They were told to engage in 3 self-guided treatment sessions per week for 8 weeks, with a maximum duration of 30 minutes per session. The regimen included a series of exercises such as the 1-legged stance, in which the patient slightly flexes the weight-bearing leg at the knee, hip, and ankle while the foot of the other leg is off the floor, then switches legs after a minute. The exercises involved increasing levels of difficulty—performed on an even surface, on an even surface with the eyes closed, or on a balance board.
The primary outcome was a self-reported new sprain of the previously injured ankle during 1000 hours of exposure to sports in a year of follow-up. Severe sprain—defined as a sprain leading to loss of sports time or resulting in health care costs or lost productivity—was a secondary outcome. Cox regression analysis was used to compare risk of a recurrent ankle sprain between the intervention and control groups, using an intention-to-treat analysis.
At the 1-year point, 56 of the 256 participants in the intervention group (22%) and 89 of the 266 participants in the control group (33%) reported recurrent ankle sprains. The risk of recurrence per 1000 hours of exposure for the intervention group was significantly lower (relative risk [RR]=0.63; 95% confidence interval [CI], 0.45–0.88) compared with the control group. Nine people would need to be treated to prevent 1 recurrent ankle sprain.
Similarly, significantly lower risks for severe sprains were found for the intervention group, as indicated by loss of sports time (RR=0.53; 95% CI, 0.32–0.88) and health care costs (RR=0.25; 95% CI, 0.12–0.50).
WHAT’S NEW?: High-quality study supports self-guided training program
This is the first RCT to assess the effect of a nonsupervised home-based proprioceptive training program, in addition to usual care, on the recurrence of ankle sprain. Two earlier studies had evaluated balance board exercises to prevent initial ankle injuries in young athletes, and both found these exercises to be effective.8,11 But prior studies evaluating prevention of recurrent ankle sprain have had methodology weaknesses or small sample sizes.12-14
One other RCT had studied the effect of an exercise program that included balance boards on the risk of ankle sprain recurrence and found a significant difference in favor or the intervention group (absolute risk reduction=22%).15 But the exercise program in that study was supervised by professionals rather than self-guided by patients. The study was also marred by significant loss to follow-up (27%), and the information on reinjury was collected retrospectively a year after the acute ankle sprain.
By comparison, the study done by Hupperets et al had a large sample size, minimal loss to follow-up (14%), and monthly check-in with patients to assess reinjury. The results show an absolute reduction of 11% in the risk of recurrence of ankle sprain. The evidence brought forth by this high-quality RCT supports adding a home-based proprioceptive training program for every patient with an acute ankle sprain to reduce the incidence of sprain recurrence.
CAVEATS: Will patients do their exercises?
One concern highlighted by this study is compliance with the treatment regimen. Only 23% of those in the intervention group fully complied with the 8-week program, 29% were partially compliant, 35% were not compliant, and 13% were of unknown compliance.
We think these findings reflect the compliance seen in the real world, so it is encouraging to know that the intervention was nonetheless effective. Clearly, some proprioceptive training is better than none; the optimal amount is not known.
Generalizability is another concern, since this study focused on athletes. However, the investigators included a wide spectrum of patients (ages 12-70 years, male and female, and those engaged in all levels of sports activity). Furthermore, since the mechanism of injury for lateral ankle sprain is generally the same, we think it is reasonable to assume that ankle sprains not related to sports would benefit from a proprioceptive program, as well.
CHALLENGES TO IMPLEMENTATION: No significant barriers exist
The treatment does not have any significant adverse effects and should be easy to recommend. Balance boards can be obtained from a sporting goods supplier or online, at a cost of $13 to $35. Some busy physician practices may not have the time or staff to teach patients how to carry out these exercises. In that case, a 1-time referral to a physical therapist should be sufficient.
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ. 2009;339:b2684.
2. Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle. Operation, cast, or early controlled mobilization. J Bone Joint Surg Am. 1991;73:305-312.
3. Fong DT, Hong Y, Chan LK, et al. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37:73-94.
4. Meeuwisse WH, Tyreman H, Hagel B, et al. A dynamic model of etiology in sport injury: the recursive nature of risk and causation. Clin J Sport Med. 2007;17:215-219.
5. Kaminski TW, Buckley BD, Powers ME, et al. Effect of strength and proprioception training on eversion to inversion strength ratios in subjects with unilateral functional ankle instability. Br J Sports Med. 2003;37:410-415.
6. Bahr R, Bahr IA. Incidence of acute volleyball injuries: a prospective cohort study of injury mechanisms and risk factors. Scand J Med Sci Sports. 1997;7:166-171.
7. Milgrom C, Shlamkovitch N, Finestone A, et al. Risk factors for lateral ankle sprain: a prospective study among military recruits. Foot Ankle. 1991;12:26-30.
8. Wedderkopp N, Kaltoft M, Holm R, et al. Comparison of two intervention programmes in young female players in European handball—with and without ankle disc. Scand J Med Sci Sports. 2003;13:371-375.
9. Hupperets MD, Verhagen EA, van Mechelen W. Effect of sensorimotor training on morphological, neurophysiological and functional characteristics of the ankle: a critical review. Sports Med. 2009;39:591-605.
10. Handoll HH, Rowe BH, Quinn KM, et al. Interventions for preventing ankle ligament injuries. Cochrane Database Syst Rev. 2001;(3):CD000018.-
11. Verhagen EA, Van der Beek AJ, Bouter LM, et al. A one season prospective cohort study of volleyball injuries. Br J Sports Med. 2004;38:477-481.
12. Tropp H, Askling C, Gillquist J. Prevention of ankle sprains. Am J Sports Med. 1985;13:259-262.
13. Wedderkopp N, Kaltoft M, Lundgaard B, et al. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sports. 1999;9:41-47.
14. Wester JU, Jespersen SM, Nielsen KD, et al. Wobble board training after partial sprains of the lateral ligaments of the ankle: A prospective randomized study. J Orthop Sports Phys Ther. 1996;23:332-336.
15. Holme E, Magnusson SP, Becher K, et al. The effect of supervised rehabilitation on strength, postural sway, position sense and re-injury risk after acute ankle ligament sprain. Scand J Med Sci Sports. 1999;9:104-109.
Advise patients being treated for ankle sprain that reinjury—which is especially common during the first year—can result in chronic pain or disability, and that a home-based proprioceptive training program has been shown to significantly reduce the risk of recurrent sprain.1
STRENGTH OF RECOMMENDATION
A: Based on a high-quality randomized controlled trial (RCT).
Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ. 2009;339:b2684.
ILLUSTRATIVE CASE
A 35-year-old man comes to see you 1 day after injuring his left ankle, which he inverted while playing racquetball in a semicompetitive league. After a clinical exam, you diagnose an ankle sprain. You advise him to wrap the ankle for protection and recommend rest, ice, compression, and elevation. Besides treatment for the current sprain, however, he asks what he can do after recovery to prevent ankle reinjury.
What can you tell him?
An estimated 23,000 ankle sprains occur every day in the United States, which amounts to approximately 1 in every 10,000 people.2 In many sports, ankle sprain is the most common injury,3 partly because an athlete who incurs a first ankle sprain is at increased risk of another.4-6 The risk of reinjury is highest in the year immediately following the initial sprain.6-8
Long-term effects of repeat sprains
About half of recurrent ankle sprains result in chronic pain or disability, so preventing repeat sprains is an important patient-oriented treatment goal. Various modalities, including bracing, taping, and warm-up and strengthening exercises, have been used to prevent recurrence of ankle sprain. Proprioceptive training has also been suggested.5,9 A Cochrane review in 2001 found limited evidence for reduction of ankle sprain recurrence after proprioceptive exercises.10 Until the study reviewed in this PURL, its effectiveness remained uncertain.
STUDY SUMMARY: Exercise program reduces risk
Hupperets et al1 investigated the effectiveness of a home-based proprioceptive training program to prevent ankle sprain recurrence. Enrollees (N=522) in this well-done RCT were active sports participants ranging in age from 12 to 70 years, all of whom had incurred ankle sprains in the preceding 2 months. They were recruited throughout The Netherlands using a variety of medical channels—emergency departments, general practices, and physical therapy offices—and advertisements in newspapers and sports magazines, at sports tournaments, and on the Internet.
The athletes were randomized to the intervention or control group, with stratification for sex, type of enrollment, and type of care they initially received for the ankle sprain—which the participants in both groups received without interference from the authors. (Among the enrollees were 181 people who did not receive any medical care for their sprains.)
Participants in the intervention group were given an instructional DVD, a balance board, and an exercise sheet, with further instructions available on a Web site. They were told to engage in 3 self-guided treatment sessions per week for 8 weeks, with a maximum duration of 30 minutes per session. The regimen included a series of exercises such as the 1-legged stance, in which the patient slightly flexes the weight-bearing leg at the knee, hip, and ankle while the foot of the other leg is off the floor, then switches legs after a minute. The exercises involved increasing levels of difficulty—performed on an even surface, on an even surface with the eyes closed, or on a balance board.
The primary outcome was a self-reported new sprain of the previously injured ankle during 1000 hours of exposure to sports in a year of follow-up. Severe sprain—defined as a sprain leading to loss of sports time or resulting in health care costs or lost productivity—was a secondary outcome. Cox regression analysis was used to compare risk of a recurrent ankle sprain between the intervention and control groups, using an intention-to-treat analysis.
At the 1-year point, 56 of the 256 participants in the intervention group (22%) and 89 of the 266 participants in the control group (33%) reported recurrent ankle sprains. The risk of recurrence per 1000 hours of exposure for the intervention group was significantly lower (relative risk [RR]=0.63; 95% confidence interval [CI], 0.45–0.88) compared with the control group. Nine people would need to be treated to prevent 1 recurrent ankle sprain.
Similarly, significantly lower risks for severe sprains were found for the intervention group, as indicated by loss of sports time (RR=0.53; 95% CI, 0.32–0.88) and health care costs (RR=0.25; 95% CI, 0.12–0.50).
WHAT’S NEW?: High-quality study supports self-guided training program
This is the first RCT to assess the effect of a nonsupervised home-based proprioceptive training program, in addition to usual care, on the recurrence of ankle sprain. Two earlier studies had evaluated balance board exercises to prevent initial ankle injuries in young athletes, and both found these exercises to be effective.8,11 But prior studies evaluating prevention of recurrent ankle sprain have had methodology weaknesses or small sample sizes.12-14
One other RCT had studied the effect of an exercise program that included balance boards on the risk of ankle sprain recurrence and found a significant difference in favor or the intervention group (absolute risk reduction=22%).15 But the exercise program in that study was supervised by professionals rather than self-guided by patients. The study was also marred by significant loss to follow-up (27%), and the information on reinjury was collected retrospectively a year after the acute ankle sprain.
By comparison, the study done by Hupperets et al had a large sample size, minimal loss to follow-up (14%), and monthly check-in with patients to assess reinjury. The results show an absolute reduction of 11% in the risk of recurrence of ankle sprain. The evidence brought forth by this high-quality RCT supports adding a home-based proprioceptive training program for every patient with an acute ankle sprain to reduce the incidence of sprain recurrence.
CAVEATS: Will patients do their exercises?
One concern highlighted by this study is compliance with the treatment regimen. Only 23% of those in the intervention group fully complied with the 8-week program, 29% were partially compliant, 35% were not compliant, and 13% were of unknown compliance.
We think these findings reflect the compliance seen in the real world, so it is encouraging to know that the intervention was nonetheless effective. Clearly, some proprioceptive training is better than none; the optimal amount is not known.
Generalizability is another concern, since this study focused on athletes. However, the investigators included a wide spectrum of patients (ages 12-70 years, male and female, and those engaged in all levels of sports activity). Furthermore, since the mechanism of injury for lateral ankle sprain is generally the same, we think it is reasonable to assume that ankle sprains not related to sports would benefit from a proprioceptive program, as well.
CHALLENGES TO IMPLEMENTATION: No significant barriers exist
The treatment does not have any significant adverse effects and should be easy to recommend. Balance boards can be obtained from a sporting goods supplier or online, at a cost of $13 to $35. Some busy physician practices may not have the time or staff to teach patients how to carry out these exercises. In that case, a 1-time referral to a physical therapist should be sufficient.
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
Advise patients being treated for ankle sprain that reinjury—which is especially common during the first year—can result in chronic pain or disability, and that a home-based proprioceptive training program has been shown to significantly reduce the risk of recurrent sprain.1
STRENGTH OF RECOMMENDATION
A: Based on a high-quality randomized controlled trial (RCT).
Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ. 2009;339:b2684.
ILLUSTRATIVE CASE
A 35-year-old man comes to see you 1 day after injuring his left ankle, which he inverted while playing racquetball in a semicompetitive league. After a clinical exam, you diagnose an ankle sprain. You advise him to wrap the ankle for protection and recommend rest, ice, compression, and elevation. Besides treatment for the current sprain, however, he asks what he can do after recovery to prevent ankle reinjury.
What can you tell him?
An estimated 23,000 ankle sprains occur every day in the United States, which amounts to approximately 1 in every 10,000 people.2 In many sports, ankle sprain is the most common injury,3 partly because an athlete who incurs a first ankle sprain is at increased risk of another.4-6 The risk of reinjury is highest in the year immediately following the initial sprain.6-8
Long-term effects of repeat sprains
About half of recurrent ankle sprains result in chronic pain or disability, so preventing repeat sprains is an important patient-oriented treatment goal. Various modalities, including bracing, taping, and warm-up and strengthening exercises, have been used to prevent recurrence of ankle sprain. Proprioceptive training has also been suggested.5,9 A Cochrane review in 2001 found limited evidence for reduction of ankle sprain recurrence after proprioceptive exercises.10 Until the study reviewed in this PURL, its effectiveness remained uncertain.
STUDY SUMMARY: Exercise program reduces risk
Hupperets et al1 investigated the effectiveness of a home-based proprioceptive training program to prevent ankle sprain recurrence. Enrollees (N=522) in this well-done RCT were active sports participants ranging in age from 12 to 70 years, all of whom had incurred ankle sprains in the preceding 2 months. They were recruited throughout The Netherlands using a variety of medical channels—emergency departments, general practices, and physical therapy offices—and advertisements in newspapers and sports magazines, at sports tournaments, and on the Internet.
The athletes were randomized to the intervention or control group, with stratification for sex, type of enrollment, and type of care they initially received for the ankle sprain—which the participants in both groups received without interference from the authors. (Among the enrollees were 181 people who did not receive any medical care for their sprains.)
Participants in the intervention group were given an instructional DVD, a balance board, and an exercise sheet, with further instructions available on a Web site. They were told to engage in 3 self-guided treatment sessions per week for 8 weeks, with a maximum duration of 30 minutes per session. The regimen included a series of exercises such as the 1-legged stance, in which the patient slightly flexes the weight-bearing leg at the knee, hip, and ankle while the foot of the other leg is off the floor, then switches legs after a minute. The exercises involved increasing levels of difficulty—performed on an even surface, on an even surface with the eyes closed, or on a balance board.
The primary outcome was a self-reported new sprain of the previously injured ankle during 1000 hours of exposure to sports in a year of follow-up. Severe sprain—defined as a sprain leading to loss of sports time or resulting in health care costs or lost productivity—was a secondary outcome. Cox regression analysis was used to compare risk of a recurrent ankle sprain between the intervention and control groups, using an intention-to-treat analysis.
At the 1-year point, 56 of the 256 participants in the intervention group (22%) and 89 of the 266 participants in the control group (33%) reported recurrent ankle sprains. The risk of recurrence per 1000 hours of exposure for the intervention group was significantly lower (relative risk [RR]=0.63; 95% confidence interval [CI], 0.45–0.88) compared with the control group. Nine people would need to be treated to prevent 1 recurrent ankle sprain.
Similarly, significantly lower risks for severe sprains were found for the intervention group, as indicated by loss of sports time (RR=0.53; 95% CI, 0.32–0.88) and health care costs (RR=0.25; 95% CI, 0.12–0.50).
WHAT’S NEW?: High-quality study supports self-guided training program
This is the first RCT to assess the effect of a nonsupervised home-based proprioceptive training program, in addition to usual care, on the recurrence of ankle sprain. Two earlier studies had evaluated balance board exercises to prevent initial ankle injuries in young athletes, and both found these exercises to be effective.8,11 But prior studies evaluating prevention of recurrent ankle sprain have had methodology weaknesses or small sample sizes.12-14
One other RCT had studied the effect of an exercise program that included balance boards on the risk of ankle sprain recurrence and found a significant difference in favor or the intervention group (absolute risk reduction=22%).15 But the exercise program in that study was supervised by professionals rather than self-guided by patients. The study was also marred by significant loss to follow-up (27%), and the information on reinjury was collected retrospectively a year after the acute ankle sprain.
By comparison, the study done by Hupperets et al had a large sample size, minimal loss to follow-up (14%), and monthly check-in with patients to assess reinjury. The results show an absolute reduction of 11% in the risk of recurrence of ankle sprain. The evidence brought forth by this high-quality RCT supports adding a home-based proprioceptive training program for every patient with an acute ankle sprain to reduce the incidence of sprain recurrence.
CAVEATS: Will patients do their exercises?
One concern highlighted by this study is compliance with the treatment regimen. Only 23% of those in the intervention group fully complied with the 8-week program, 29% were partially compliant, 35% were not compliant, and 13% were of unknown compliance.
We think these findings reflect the compliance seen in the real world, so it is encouraging to know that the intervention was nonetheless effective. Clearly, some proprioceptive training is better than none; the optimal amount is not known.
Generalizability is another concern, since this study focused on athletes. However, the investigators included a wide spectrum of patients (ages 12-70 years, male and female, and those engaged in all levels of sports activity). Furthermore, since the mechanism of injury for lateral ankle sprain is generally the same, we think it is reasonable to assume that ankle sprains not related to sports would benefit from a proprioceptive program, as well.
CHALLENGES TO IMPLEMENTATION: No significant barriers exist
The treatment does not have any significant adverse effects and should be easy to recommend. Balance boards can be obtained from a sporting goods supplier or online, at a cost of $13 to $35. Some busy physician practices may not have the time or staff to teach patients how to carry out these exercises. In that case, a 1-time referral to a physical therapist should be sufficient.
Acknowledgment
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
Click here to view PURL METHODOLOGY
1. Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ. 2009;339:b2684.
2. Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle. Operation, cast, or early controlled mobilization. J Bone Joint Surg Am. 1991;73:305-312.
3. Fong DT, Hong Y, Chan LK, et al. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37:73-94.
4. Meeuwisse WH, Tyreman H, Hagel B, et al. A dynamic model of etiology in sport injury: the recursive nature of risk and causation. Clin J Sport Med. 2007;17:215-219.
5. Kaminski TW, Buckley BD, Powers ME, et al. Effect of strength and proprioception training on eversion to inversion strength ratios in subjects with unilateral functional ankle instability. Br J Sports Med. 2003;37:410-415.
6. Bahr R, Bahr IA. Incidence of acute volleyball injuries: a prospective cohort study of injury mechanisms and risk factors. Scand J Med Sci Sports. 1997;7:166-171.
7. Milgrom C, Shlamkovitch N, Finestone A, et al. Risk factors for lateral ankle sprain: a prospective study among military recruits. Foot Ankle. 1991;12:26-30.
8. Wedderkopp N, Kaltoft M, Holm R, et al. Comparison of two intervention programmes in young female players in European handball—with and without ankle disc. Scand J Med Sci Sports. 2003;13:371-375.
9. Hupperets MD, Verhagen EA, van Mechelen W. Effect of sensorimotor training on morphological, neurophysiological and functional characteristics of the ankle: a critical review. Sports Med. 2009;39:591-605.
10. Handoll HH, Rowe BH, Quinn KM, et al. Interventions for preventing ankle ligament injuries. Cochrane Database Syst Rev. 2001;(3):CD000018.-
11. Verhagen EA, Van der Beek AJ, Bouter LM, et al. A one season prospective cohort study of volleyball injuries. Br J Sports Med. 2004;38:477-481.
12. Tropp H, Askling C, Gillquist J. Prevention of ankle sprains. Am J Sports Med. 1985;13:259-262.
13. Wedderkopp N, Kaltoft M, Lundgaard B, et al. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sports. 1999;9:41-47.
14. Wester JU, Jespersen SM, Nielsen KD, et al. Wobble board training after partial sprains of the lateral ligaments of the ankle: A prospective randomized study. J Orthop Sports Phys Ther. 1996;23:332-336.
15. Holme E, Magnusson SP, Becher K, et al. The effect of supervised rehabilitation on strength, postural sway, position sense and re-injury risk after acute ankle ligament sprain. Scand J Med Sci Sports. 1999;9:104-109.
1. Hupperets MD, Verhagen EA, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised controlled trial. BMJ. 2009;339:b2684.
2. Kannus P, Renstrom P. Treatment for acute tears of the lateral ligaments of the ankle. Operation, cast, or early controlled mobilization. J Bone Joint Surg Am. 1991;73:305-312.
3. Fong DT, Hong Y, Chan LK, et al. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37:73-94.
4. Meeuwisse WH, Tyreman H, Hagel B, et al. A dynamic model of etiology in sport injury: the recursive nature of risk and causation. Clin J Sport Med. 2007;17:215-219.
5. Kaminski TW, Buckley BD, Powers ME, et al. Effect of strength and proprioception training on eversion to inversion strength ratios in subjects with unilateral functional ankle instability. Br J Sports Med. 2003;37:410-415.
6. Bahr R, Bahr IA. Incidence of acute volleyball injuries: a prospective cohort study of injury mechanisms and risk factors. Scand J Med Sci Sports. 1997;7:166-171.
7. Milgrom C, Shlamkovitch N, Finestone A, et al. Risk factors for lateral ankle sprain: a prospective study among military recruits. Foot Ankle. 1991;12:26-30.
8. Wedderkopp N, Kaltoft M, Holm R, et al. Comparison of two intervention programmes in young female players in European handball—with and without ankle disc. Scand J Med Sci Sports. 2003;13:371-375.
9. Hupperets MD, Verhagen EA, van Mechelen W. Effect of sensorimotor training on morphological, neurophysiological and functional characteristics of the ankle: a critical review. Sports Med. 2009;39:591-605.
10. Handoll HH, Rowe BH, Quinn KM, et al. Interventions for preventing ankle ligament injuries. Cochrane Database Syst Rev. 2001;(3):CD000018.-
11. Verhagen EA, Van der Beek AJ, Bouter LM, et al. A one season prospective cohort study of volleyball injuries. Br J Sports Med. 2004;38:477-481.
12. Tropp H, Askling C, Gillquist J. Prevention of ankle sprains. Am J Sports Med. 1985;13:259-262.
13. Wedderkopp N, Kaltoft M, Lundgaard B, et al. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sports. 1999;9:41-47.
14. Wester JU, Jespersen SM, Nielsen KD, et al. Wobble board training after partial sprains of the lateral ligaments of the ankle: A prospective randomized study. J Orthop Sports Phys Ther. 1996;23:332-336.
15. Holme E, Magnusson SP, Becher K, et al. The effect of supervised rehabilitation on strength, postural sway, position sense and re-injury risk after acute ankle ligament sprain. Scand J Med Sci Sports. 1999;9:104-109.
Copyright © 2010 The Family Physicians Inquiries Network.
All rights reserved.
What to do when warfarin therapy goes too far
- For patients with an elevated international normalized ratio (INR) with mild or no bleeding, withhold the warfarin and recheck INR in 1 to 2 days; if INR >5, add oral vitamin K supplementation (C).
- For major bleeding and elevated INR, hospital admission, vitamin K, fresh frozen plasma, and frequent monitoring are needed (B).
- Emergent situations call for hospitalization, clotting factor replacement, and vitamin K administered by slow intravenous infusion (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
I feel weak,” reports Mary Jo, a 67-year-old patient who scheduled today’s appointment when she began noticing black, tarry stools 2 days ago. Her chart reveals that she’s on warfarin therapy for chronic atrial fibrillation, and today’s labs show a hematocrit of 18 and an international normalized ratio (INR) of 6.
If Mary Jo were your patient, what would you do?
With some 30.6 million outpatient prescriptions dispensed in the United States in a single year,1 warfarin is among the nation’s most commonly prescribed medications. It is also a dangerous drug. Warfarin’s anticoagulant and antithrombotic effects occur through its ability to inhibit the enzymes responsible for the reduction of vitamin K—an essential cofactor in the normal production of vitamin K-dependent clotting factors II, VII, XI, and X and anticoagulant factors protein C and S. In the presence of warfarin, these clotting factors are produced in a partially carboxylated state with reduced or absent biological activity. The result is a hypocoagulability that can be life-threatening.
Given the sheer number of patients receiving warfarin therapy and the potential for hemorrhage and other adverse effects, primary care physicians need to be familiar with evidence-based recommendations for managing warfarin-induced hypocoagulation. This review will help ensure that when you see patients like Mary Jo, you’ll be prepared to take the best approach to reversing their hypocoagulable state.
Which patients face the highest risk?
The reported incidence of bleeding in patients taking warfarin varies significantly, but is generally in the range of 1% annually.2 Among those who develop warfarin-related major bleeds, however, the fatality rate may be as high as 13.4%.3
The risk of bleeding is highest in the first 30 days of warfarin therapy,3 and increases exponentially once the INR exceeds 5.4 Other risk factors include:
- age (the risk increases to about 5% per year for patients >75 years)5
- hypertension
- cerebrovascular disease
- ischemic stroke
- a history of bleeds.6-8
Multiple medications and herbal substances can interfere with warfarin therapy. Some agents work by augmenting warfarin’s effect; others, such as antiplatelet agents, directly increase the risk of bleeding through unrelated mechanisms; still others may counteract warfarin therapy by enhancing coagulation. Ask patients on warfarin therapy to tell you everything they’re taking, including all over-the-counter medications, supplements, and prescription drugs. TABLE 1 lists herbal substances with the potential to increase or decrease INR. A comprehensive list of drugs that can interact with warfarin is available at http://www.drugs.com/drug-interactions/coumadin_d00022.html.
TABLE 1
Herbal substances that may affect INR38-40
| INCREASE INR | DECREASE INR | |
|---|---|---|
| Angelica root Anise Arnica flower Asafoetida Bogbean Boldo-fenugreek Borage seed oil Bromelain Capsicum Celery Chamomile Clove Dashen Devil’s claw Dong quai Feverfew Fish oil Garlic Ginger Ginkgo | Goldenseal Horse chestnut Licorice root Lovage root Lycium barbarum (wolfberry) Meadowsweet Onion Papain Parsley Passionflower Poplar Quassia Quilinggao Red clover Rue Sweet clover Turmeric Vitamin E Willow bark | Coenzyme Q10 Ginseng Green tea St. John’s wort |
When reversal is needed, how best to achieve it?
The options for reversing warfarin-induced anticoagulation include withholding 1 or more doses of warfarin and providing vitamin K supplementation and clotting factor replacement, as needed. The decision of which combination to use is based on both the urgency ( TABLE 2 ) and completeness of reversal required (target INR range) and the risk of thrombosis when the anticoagulation is reversed.9
Vitamin K is actually a group of lipid-soluble chemicals that are necessary for the production of functional carboxylated clotting factors II, VII, IX, and X. Vitamin K1 (phytonadione), which is available in food and as a supplement, is the particular chemical that competes with warfarin. When it is used as a reversal agent, phytonadione is generally referred to simply as vitamin K.
The oral route of vitamin K is preferred, but its effect is delayed because of the time required for absorption and production of factors. Thus, a slow (15-30 min) infusion of intravenous (IV) vitamin K should be used if reversal is needed within 6 hours—or oral therapy is unavailable. Avoid subcutaneous administration; it is not reliable and may take up to 72 hours to reverse the INR.10-12 Intramuscular (IM) administration of vitamin K should also be avoided in patients taking warfarin because of concerns about hematoma formation, although a 2003 study of patients in teaching hospitals found that the IM route is used about 10% of the time.13
The optimal dose of vitamin K varies, based on patient-specific factors such as comorbidities, metabolic and genetic variation, weight, age, and liver function. Doses as low as 0.5 mg IV or 1 mg oral vitamin K have been effective in reversing an elevated INR to a therapeutic range in nonlife-threatening situations.11,14,15 The American College of Chest Physicians (ACCP), which issued new guidelines in 2008, recommends doses of <5 mg for an INR >5 but <9 if there is a high risk of bleeding; 5 to 10 mg is the recommended dose for all patients with an INR ≥9. In cases of significant bleeding, a dose of 10 mg IV is recommended.16 Excessive vitamin K supplementation may lead to warfarin resistance, making it necessary to use much higher doses of warfarin down the road to achieve therapeutic INR levels.
Fresh frozen plasma (FFP) replaces functional vitamin K-dependent clotting factors that are decreased in patients taking warfarin. The suggested dose is 15 mL/kg,17,18 but patients must be monitored with coagulation laboratory values to assess the amount needed. One unit of FFP is roughly 250 mL, which corresponds to roughly 250 units of clotting factors.
FFP works to offset coagulopathy quickly. But because the plasma is frozen, it has to be thawed and blood type-matched, which is time-consuming. FFP transfusion also may be associated with infections, although the risk is generally believed to be minimal.17 Other limitations in using FFP include the large volume of fluid that must be administered—with the attendant risk of fluid overload—and the possibility of significant infusion reactions that may require slowing the infusion rate.19
Prothrombin complex concentrate (PCC) is pooled from donor plasma and lyophilized to a powder. It is then reconstituted for clotting factor replacement, and is available through the pharmacy rather than the blood bank.20 PCC is dosed in international units of factor IX, although it includes proportional amounts of factors II, VII, and X and proteins C and S. The typical recommended dose is 30 to 50 U/kg.20,21
Although PCC contains human coagulation factors, it does not involve the same risks of fluid overload or infectious transmission as FFP. It can be given IV over 5 to 10 minutes. The risk of thrombogenicity has been reported in patients with hemophilia who receive PCC,22 but studies of PCC use in warfarin reversal have not shown this adverse effect.23,24 Data from the use of PCC for the treatment of hemophilia suggest that the risk of thromboembolic events begins with daily doses >200 U/kg. There is limited information about the safety of giving PCC to patients with mechanical valve replacement, pregnant women, and those in other high-risk situations.
Recombinant activated factor VII (rFVIIa) is also effective in reversing elevated INR.25,26 It replaces 1 of the clotting factors that is decreased in anticoagulated patients (factor VII), but the significance of not replacing factors II, IX, and X is unknown.27 The recommended quantity of rFVIIa ranges from a single dose of 1200 mcg to weight-based dosing (10-160 mcg/kg).25,28-30 (IV vitamin K and FFP are also given in emergent situations in which rFVIIa is administered.) Thrombogenicity is a possible complication with the use of rFVIIa, but data are scarce regarding the incidence of adverse effects.
Neither PCC nor rFVIIa has US Food and Drug Administration approval for use in reversing warfarin-induced anticoagulation. Their use for this purpose may be warranted only in situations that threaten life or limb, and must be guided by clinical judgment.
TABLE 2
How fast? Reversal agents and time of action32
| SPEED/TYPE OF REVERSAL REQUIRED | WHAT TO USE |
|---|---|
| Rapid (complete; within 10-15 minutes) | PCC or rFVIIa + vitamin K IV |
| Fast (partial) | FFP + vitamin K IV |
| Prompt (4-6 hours) | Vitamin K IV |
| Slow (within 24 hours) | Oral vitamin K |
| Ultra-slow (over a period of days) | Omit warfarin dose (no vitamin K) |
| FFP, fresh frozen plasma; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. | |
Severity of bleeding as a treatment guide
Studies of methods used to reverse warfarin’s anticoagulation effect are difficult to compare because of a lack of a standardized approach to the classification of bleeds.18,31,32 We’ve used the following classification system, modified from that of Fihn et al,31 to avoid confusion and inform treatment decisions:
- Minor bleed: Reported, not requiring additional testing
- Major bleed: Requiring medical evaluation and inpatient treatment and/or blood transfusion
- Life-threatening bleed: Leading to cardiac arrest, surgical/angiographic intervention, or irreversible sequelae (loss of limb/sight).
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 ( FIGURE )—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE
Reversal of warfarin-induced anticoagulation
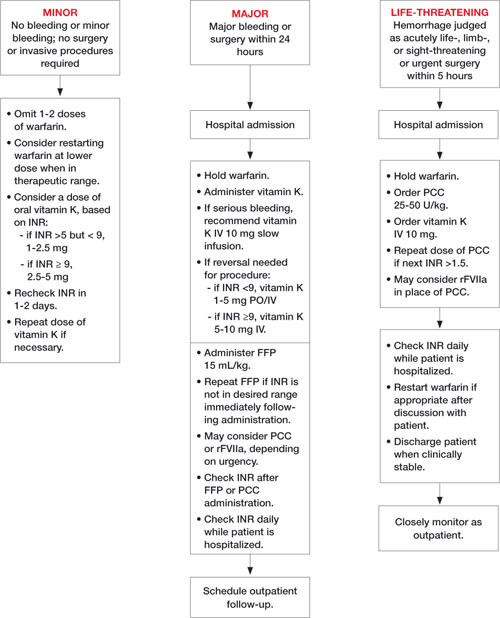
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII.
Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.
CORRESPONDENCE
Shailendra Prasad, MBBS, MPH, 1020 W. Broadway, Minneapolis, MN 55411; pras0054@umn.edu
1. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167:1414-1419.
2. Beyth RJ. Hemorrhagic complications of oral anticoagulant therapy. Clin Geriatr Med. 2001;17:49-56.
3. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139:893-900.
4. Levine MN, Raskob G, Beyth RJ, et al. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S287-S310.
5. Pengo V, Legnani C, Noventa F, et al. ISCOAT Study Group. (Italian Study on Complications of Oral Anticoagulant Therapy). Oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding. A multicenter inception cohort study. Thromb Haemost. 2001;85:418-422.
6. White RH, McKittrick T, Takakuwa J, et al. Management and prognosis of life-threatening bleeding during warfarin therapy. National Consortium of Anticoagulation Clinics. Arch Intern Med. 1996;156:1197-1201.
7. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91-99.
8. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993;342:1255-1262.
9. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S204-S233.
10. Crowther MA, Douketis JD, Schnurr T, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137:251-254.
11. Whitling AM, Bussey HI, Lyons RM. Comparing different routes and doses of phytonadione for reversing excessive anticoagulation. Arch Intern Med. 1998;158:2136-2140.
12. Nee R, Doppenschmidt D, Donovan DJ, et al. Intravenous versus subcutaneous vitamin K1 in reversing excessive oral anticoagulation. Am J Cardiol. 1999;83:286-288.
13. Fan J, Armitstead JA, Adams AG, et al. A retrospective evaluation of vitamin K1 therapy to reverse the anticoagulant effect of warfarin. Pharmacotherapy. 2003;23:1245-1250.
14. Lubetsky A, Yonath H, Olchovsky D, et al. Comparison of oral vs intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: a prospective randomized controlled study. Arch Intern Med. 2003;163:2469-2473.
15. Hung A, Singh S, Tait RC. A prospective randomized study to determine the optimal dose of intravenous vitamin K in reversal of over-warfarinization. Br J Haematol. 2000;109:537-539.
16. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(suppl):160S-198S.
17. Dentali F, Ageno W, Crowther M. Treatment of coumarin-associated coagulopathy: a systematic review and proposed algorithms. J Thromb Haemost. 2006;4:1853-1863.
18. Makris M, Watson HG. The management of coumarin-induced over-anticoagulation Annotation [see comment]. Br J Haematol. 2001;114:271-280.
19. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126:11-28.
20. Makris M. Optimisation of the prothrombin complex concentrate dose for warfarin reversal. Thromb Res. 2005;115:451-453.
21. Vigue B, Ract C, Tremey B, et al. Ultra-rapid management of oral anticoagulant therapy-related surgical intracranial hemorrhage. Intensive Care Med. 2007;33:721-725.
22. Kohler M. Thrombogenicity of prothrombin complex concentrates. Thromb Res. 1999;95(suppl 1):S13-S17.
23. Lorenz R, Kienast J, Otto U, et al. Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study. Blood Coagul Fibrinolysis. 2007;18:565-570.
24. Pabinger I, Brenner B, Kalina U, et al. Beriplex P/N Anticoagulation Reversal Study Group. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008;6:622-631.
25. Sorensen B, Johansen P, Nielsen GL, et al. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469-477.
26. Brody DL, Aiyagari V, Shackleford AM, et al. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
27. Tanaka KA, Szlam F, Dickneite G, et al. Effects of prothrombin complex concentrate and recombinant activated factor VII on vitamin K antagonist induced anticoagulation. Thromb Res. 2008;122:117-123.
28. Lin J, Hanigan WC, Tarantino M, et al. The use of recombinant activated factor VII to reverse warfarin-induced anticoagulation in patients with hemorrhages in the central nervous system: preliminary findings. J Neurosurg. 2003;98:737-740.
29. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
30. Dager WE, King JH, Regalia RC, et al. Reversal of elevated international normalized ratio and bleeding with low-dose recombinant factor VII in patients receiving warfarin. Pharmacotherapy. 2006;26:1091-1098.
31. Fihn SD, McDonell M, Martin D, et al. Risk factors for complications of chronic anticoagulation. A multicenter study. Warfarin Optimized Outpatient Follow-up Study Group. Ann Intern Med. 1993;118:511-520.
32. Hanley JP. Warfarin reversal. J Clin Pathol. 2004;57:1132-1139.
33. Yasaka M, Sakata T, Minematsu K, et al. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
34. Evans G, Luddington R, Baglin T. Beriplex P/N reverses severe warfarin-induced anticoagulation immediately and completely in patients presenting with major bleeding. Br J Haematol. 2001;115:998-1001.
35. Lubetsky A, Hoffman R, Zimlichman R, et al. Efficacy and safety of complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004;113:371-378.
36. Cartmill M, Dolan G, Byrne JL, et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
37. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
38. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165:1095-1106.
39. Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiological Approach. 6th ed. New York: McGraw-Hill Companies, Inc.; 2005:373-413.
40. Micromedex Healthcare Series. Drug-REAX System. New York: Thomson Reuters; 2008.
- For patients with an elevated international normalized ratio (INR) with mild or no bleeding, withhold the warfarin and recheck INR in 1 to 2 days; if INR >5, add oral vitamin K supplementation (C).
- For major bleeding and elevated INR, hospital admission, vitamin K, fresh frozen plasma, and frequent monitoring are needed (B).
- Emergent situations call for hospitalization, clotting factor replacement, and vitamin K administered by slow intravenous infusion (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
I feel weak,” reports Mary Jo, a 67-year-old patient who scheduled today’s appointment when she began noticing black, tarry stools 2 days ago. Her chart reveals that she’s on warfarin therapy for chronic atrial fibrillation, and today’s labs show a hematocrit of 18 and an international normalized ratio (INR) of 6.
If Mary Jo were your patient, what would you do?
With some 30.6 million outpatient prescriptions dispensed in the United States in a single year,1 warfarin is among the nation’s most commonly prescribed medications. It is also a dangerous drug. Warfarin’s anticoagulant and antithrombotic effects occur through its ability to inhibit the enzymes responsible for the reduction of vitamin K—an essential cofactor in the normal production of vitamin K-dependent clotting factors II, VII, XI, and X and anticoagulant factors protein C and S. In the presence of warfarin, these clotting factors are produced in a partially carboxylated state with reduced or absent biological activity. The result is a hypocoagulability that can be life-threatening.
Given the sheer number of patients receiving warfarin therapy and the potential for hemorrhage and other adverse effects, primary care physicians need to be familiar with evidence-based recommendations for managing warfarin-induced hypocoagulation. This review will help ensure that when you see patients like Mary Jo, you’ll be prepared to take the best approach to reversing their hypocoagulable state.
Which patients face the highest risk?
The reported incidence of bleeding in patients taking warfarin varies significantly, but is generally in the range of 1% annually.2 Among those who develop warfarin-related major bleeds, however, the fatality rate may be as high as 13.4%.3
The risk of bleeding is highest in the first 30 days of warfarin therapy,3 and increases exponentially once the INR exceeds 5.4 Other risk factors include:
- age (the risk increases to about 5% per year for patients >75 years)5
- hypertension
- cerebrovascular disease
- ischemic stroke
- a history of bleeds.6-8
Multiple medications and herbal substances can interfere with warfarin therapy. Some agents work by augmenting warfarin’s effect; others, such as antiplatelet agents, directly increase the risk of bleeding through unrelated mechanisms; still others may counteract warfarin therapy by enhancing coagulation. Ask patients on warfarin therapy to tell you everything they’re taking, including all over-the-counter medications, supplements, and prescription drugs. TABLE 1 lists herbal substances with the potential to increase or decrease INR. A comprehensive list of drugs that can interact with warfarin is available at http://www.drugs.com/drug-interactions/coumadin_d00022.html.
TABLE 1
Herbal substances that may affect INR38-40
| INCREASE INR | DECREASE INR | |
|---|---|---|
| Angelica root Anise Arnica flower Asafoetida Bogbean Boldo-fenugreek Borage seed oil Bromelain Capsicum Celery Chamomile Clove Dashen Devil’s claw Dong quai Feverfew Fish oil Garlic Ginger Ginkgo | Goldenseal Horse chestnut Licorice root Lovage root Lycium barbarum (wolfberry) Meadowsweet Onion Papain Parsley Passionflower Poplar Quassia Quilinggao Red clover Rue Sweet clover Turmeric Vitamin E Willow bark | Coenzyme Q10 Ginseng Green tea St. John’s wort |
When reversal is needed, how best to achieve it?
The options for reversing warfarin-induced anticoagulation include withholding 1 or more doses of warfarin and providing vitamin K supplementation and clotting factor replacement, as needed. The decision of which combination to use is based on both the urgency ( TABLE 2 ) and completeness of reversal required (target INR range) and the risk of thrombosis when the anticoagulation is reversed.9
Vitamin K is actually a group of lipid-soluble chemicals that are necessary for the production of functional carboxylated clotting factors II, VII, IX, and X. Vitamin K1 (phytonadione), which is available in food and as a supplement, is the particular chemical that competes with warfarin. When it is used as a reversal agent, phytonadione is generally referred to simply as vitamin K.
The oral route of vitamin K is preferred, but its effect is delayed because of the time required for absorption and production of factors. Thus, a slow (15-30 min) infusion of intravenous (IV) vitamin K should be used if reversal is needed within 6 hours—or oral therapy is unavailable. Avoid subcutaneous administration; it is not reliable and may take up to 72 hours to reverse the INR.10-12 Intramuscular (IM) administration of vitamin K should also be avoided in patients taking warfarin because of concerns about hematoma formation, although a 2003 study of patients in teaching hospitals found that the IM route is used about 10% of the time.13
The optimal dose of vitamin K varies, based on patient-specific factors such as comorbidities, metabolic and genetic variation, weight, age, and liver function. Doses as low as 0.5 mg IV or 1 mg oral vitamin K have been effective in reversing an elevated INR to a therapeutic range in nonlife-threatening situations.11,14,15 The American College of Chest Physicians (ACCP), which issued new guidelines in 2008, recommends doses of <5 mg for an INR >5 but <9 if there is a high risk of bleeding; 5 to 10 mg is the recommended dose for all patients with an INR ≥9. In cases of significant bleeding, a dose of 10 mg IV is recommended.16 Excessive vitamin K supplementation may lead to warfarin resistance, making it necessary to use much higher doses of warfarin down the road to achieve therapeutic INR levels.
Fresh frozen plasma (FFP) replaces functional vitamin K-dependent clotting factors that are decreased in patients taking warfarin. The suggested dose is 15 mL/kg,17,18 but patients must be monitored with coagulation laboratory values to assess the amount needed. One unit of FFP is roughly 250 mL, which corresponds to roughly 250 units of clotting factors.
FFP works to offset coagulopathy quickly. But because the plasma is frozen, it has to be thawed and blood type-matched, which is time-consuming. FFP transfusion also may be associated with infections, although the risk is generally believed to be minimal.17 Other limitations in using FFP include the large volume of fluid that must be administered—with the attendant risk of fluid overload—and the possibility of significant infusion reactions that may require slowing the infusion rate.19
Prothrombin complex concentrate (PCC) is pooled from donor plasma and lyophilized to a powder. It is then reconstituted for clotting factor replacement, and is available through the pharmacy rather than the blood bank.20 PCC is dosed in international units of factor IX, although it includes proportional amounts of factors II, VII, and X and proteins C and S. The typical recommended dose is 30 to 50 U/kg.20,21
Although PCC contains human coagulation factors, it does not involve the same risks of fluid overload or infectious transmission as FFP. It can be given IV over 5 to 10 minutes. The risk of thrombogenicity has been reported in patients with hemophilia who receive PCC,22 but studies of PCC use in warfarin reversal have not shown this adverse effect.23,24 Data from the use of PCC for the treatment of hemophilia suggest that the risk of thromboembolic events begins with daily doses >200 U/kg. There is limited information about the safety of giving PCC to patients with mechanical valve replacement, pregnant women, and those in other high-risk situations.
Recombinant activated factor VII (rFVIIa) is also effective in reversing elevated INR.25,26 It replaces 1 of the clotting factors that is decreased in anticoagulated patients (factor VII), but the significance of not replacing factors II, IX, and X is unknown.27 The recommended quantity of rFVIIa ranges from a single dose of 1200 mcg to weight-based dosing (10-160 mcg/kg).25,28-30 (IV vitamin K and FFP are also given in emergent situations in which rFVIIa is administered.) Thrombogenicity is a possible complication with the use of rFVIIa, but data are scarce regarding the incidence of adverse effects.
Neither PCC nor rFVIIa has US Food and Drug Administration approval for use in reversing warfarin-induced anticoagulation. Their use for this purpose may be warranted only in situations that threaten life or limb, and must be guided by clinical judgment.
TABLE 2
How fast? Reversal agents and time of action32
| SPEED/TYPE OF REVERSAL REQUIRED | WHAT TO USE |
|---|---|
| Rapid (complete; within 10-15 minutes) | PCC or rFVIIa + vitamin K IV |
| Fast (partial) | FFP + vitamin K IV |
| Prompt (4-6 hours) | Vitamin K IV |
| Slow (within 24 hours) | Oral vitamin K |
| Ultra-slow (over a period of days) | Omit warfarin dose (no vitamin K) |
| FFP, fresh frozen plasma; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. | |
Severity of bleeding as a treatment guide
Studies of methods used to reverse warfarin’s anticoagulation effect are difficult to compare because of a lack of a standardized approach to the classification of bleeds.18,31,32 We’ve used the following classification system, modified from that of Fihn et al,31 to avoid confusion and inform treatment decisions:
- Minor bleed: Reported, not requiring additional testing
- Major bleed: Requiring medical evaluation and inpatient treatment and/or blood transfusion
- Life-threatening bleed: Leading to cardiac arrest, surgical/angiographic intervention, or irreversible sequelae (loss of limb/sight).
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 ( FIGURE )—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE
Reversal of warfarin-induced anticoagulation
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII.
Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.
CORRESPONDENCE
Shailendra Prasad, MBBS, MPH, 1020 W. Broadway, Minneapolis, MN 55411; pras0054@umn.edu
- For patients with an elevated international normalized ratio (INR) with mild or no bleeding, withhold the warfarin and recheck INR in 1 to 2 days; if INR >5, add oral vitamin K supplementation (C).
- For major bleeding and elevated INR, hospital admission, vitamin K, fresh frozen plasma, and frequent monitoring are needed (B).
- Emergent situations call for hospitalization, clotting factor replacement, and vitamin K administered by slow intravenous infusion (A).
Strength of recommendation (SOR)
- Good-quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
I feel weak,” reports Mary Jo, a 67-year-old patient who scheduled today’s appointment when she began noticing black, tarry stools 2 days ago. Her chart reveals that she’s on warfarin therapy for chronic atrial fibrillation, and today’s labs show a hematocrit of 18 and an international normalized ratio (INR) of 6.
If Mary Jo were your patient, what would you do?
With some 30.6 million outpatient prescriptions dispensed in the United States in a single year,1 warfarin is among the nation’s most commonly prescribed medications. It is also a dangerous drug. Warfarin’s anticoagulant and antithrombotic effects occur through its ability to inhibit the enzymes responsible for the reduction of vitamin K—an essential cofactor in the normal production of vitamin K-dependent clotting factors II, VII, XI, and X and anticoagulant factors protein C and S. In the presence of warfarin, these clotting factors are produced in a partially carboxylated state with reduced or absent biological activity. The result is a hypocoagulability that can be life-threatening.
Given the sheer number of patients receiving warfarin therapy and the potential for hemorrhage and other adverse effects, primary care physicians need to be familiar with evidence-based recommendations for managing warfarin-induced hypocoagulation. This review will help ensure that when you see patients like Mary Jo, you’ll be prepared to take the best approach to reversing their hypocoagulable state.
Which patients face the highest risk?
The reported incidence of bleeding in patients taking warfarin varies significantly, but is generally in the range of 1% annually.2 Among those who develop warfarin-related major bleeds, however, the fatality rate may be as high as 13.4%.3
The risk of bleeding is highest in the first 30 days of warfarin therapy,3 and increases exponentially once the INR exceeds 5.4 Other risk factors include:
- age (the risk increases to about 5% per year for patients >75 years)5
- hypertension
- cerebrovascular disease
- ischemic stroke
- a history of bleeds.6-8
Multiple medications and herbal substances can interfere with warfarin therapy. Some agents work by augmenting warfarin’s effect; others, such as antiplatelet agents, directly increase the risk of bleeding through unrelated mechanisms; still others may counteract warfarin therapy by enhancing coagulation. Ask patients on warfarin therapy to tell you everything they’re taking, including all over-the-counter medications, supplements, and prescription drugs. TABLE 1 lists herbal substances with the potential to increase or decrease INR. A comprehensive list of drugs that can interact with warfarin is available at http://www.drugs.com/drug-interactions/coumadin_d00022.html.
TABLE 1
Herbal substances that may affect INR38-40
| INCREASE INR | DECREASE INR | |
|---|---|---|
| Angelica root Anise Arnica flower Asafoetida Bogbean Boldo-fenugreek Borage seed oil Bromelain Capsicum Celery Chamomile Clove Dashen Devil’s claw Dong quai Feverfew Fish oil Garlic Ginger Ginkgo | Goldenseal Horse chestnut Licorice root Lovage root Lycium barbarum (wolfberry) Meadowsweet Onion Papain Parsley Passionflower Poplar Quassia Quilinggao Red clover Rue Sweet clover Turmeric Vitamin E Willow bark | Coenzyme Q10 Ginseng Green tea St. John’s wort |
When reversal is needed, how best to achieve it?
The options for reversing warfarin-induced anticoagulation include withholding 1 or more doses of warfarin and providing vitamin K supplementation and clotting factor replacement, as needed. The decision of which combination to use is based on both the urgency ( TABLE 2 ) and completeness of reversal required (target INR range) and the risk of thrombosis when the anticoagulation is reversed.9
Vitamin K is actually a group of lipid-soluble chemicals that are necessary for the production of functional carboxylated clotting factors II, VII, IX, and X. Vitamin K1 (phytonadione), which is available in food and as a supplement, is the particular chemical that competes with warfarin. When it is used as a reversal agent, phytonadione is generally referred to simply as vitamin K.
The oral route of vitamin K is preferred, but its effect is delayed because of the time required for absorption and production of factors. Thus, a slow (15-30 min) infusion of intravenous (IV) vitamin K should be used if reversal is needed within 6 hours—or oral therapy is unavailable. Avoid subcutaneous administration; it is not reliable and may take up to 72 hours to reverse the INR.10-12 Intramuscular (IM) administration of vitamin K should also be avoided in patients taking warfarin because of concerns about hematoma formation, although a 2003 study of patients in teaching hospitals found that the IM route is used about 10% of the time.13
The optimal dose of vitamin K varies, based on patient-specific factors such as comorbidities, metabolic and genetic variation, weight, age, and liver function. Doses as low as 0.5 mg IV or 1 mg oral vitamin K have been effective in reversing an elevated INR to a therapeutic range in nonlife-threatening situations.11,14,15 The American College of Chest Physicians (ACCP), which issued new guidelines in 2008, recommends doses of <5 mg for an INR >5 but <9 if there is a high risk of bleeding; 5 to 10 mg is the recommended dose for all patients with an INR ≥9. In cases of significant bleeding, a dose of 10 mg IV is recommended.16 Excessive vitamin K supplementation may lead to warfarin resistance, making it necessary to use much higher doses of warfarin down the road to achieve therapeutic INR levels.
Fresh frozen plasma (FFP) replaces functional vitamin K-dependent clotting factors that are decreased in patients taking warfarin. The suggested dose is 15 mL/kg,17,18 but patients must be monitored with coagulation laboratory values to assess the amount needed. One unit of FFP is roughly 250 mL, which corresponds to roughly 250 units of clotting factors.
FFP works to offset coagulopathy quickly. But because the plasma is frozen, it has to be thawed and blood type-matched, which is time-consuming. FFP transfusion also may be associated with infections, although the risk is generally believed to be minimal.17 Other limitations in using FFP include the large volume of fluid that must be administered—with the attendant risk of fluid overload—and the possibility of significant infusion reactions that may require slowing the infusion rate.19
Prothrombin complex concentrate (PCC) is pooled from donor plasma and lyophilized to a powder. It is then reconstituted for clotting factor replacement, and is available through the pharmacy rather than the blood bank.20 PCC is dosed in international units of factor IX, although it includes proportional amounts of factors II, VII, and X and proteins C and S. The typical recommended dose is 30 to 50 U/kg.20,21
Although PCC contains human coagulation factors, it does not involve the same risks of fluid overload or infectious transmission as FFP. It can be given IV over 5 to 10 minutes. The risk of thrombogenicity has been reported in patients with hemophilia who receive PCC,22 but studies of PCC use in warfarin reversal have not shown this adverse effect.23,24 Data from the use of PCC for the treatment of hemophilia suggest that the risk of thromboembolic events begins with daily doses >200 U/kg. There is limited information about the safety of giving PCC to patients with mechanical valve replacement, pregnant women, and those in other high-risk situations.
Recombinant activated factor VII (rFVIIa) is also effective in reversing elevated INR.25,26 It replaces 1 of the clotting factors that is decreased in anticoagulated patients (factor VII), but the significance of not replacing factors II, IX, and X is unknown.27 The recommended quantity of rFVIIa ranges from a single dose of 1200 mcg to weight-based dosing (10-160 mcg/kg).25,28-30 (IV vitamin K and FFP are also given in emergent situations in which rFVIIa is administered.) Thrombogenicity is a possible complication with the use of rFVIIa, but data are scarce regarding the incidence of adverse effects.
Neither PCC nor rFVIIa has US Food and Drug Administration approval for use in reversing warfarin-induced anticoagulation. Their use for this purpose may be warranted only in situations that threaten life or limb, and must be guided by clinical judgment.
TABLE 2
How fast? Reversal agents and time of action32
| SPEED/TYPE OF REVERSAL REQUIRED | WHAT TO USE |
|---|---|
| Rapid (complete; within 10-15 minutes) | PCC or rFVIIa + vitamin K IV |
| Fast (partial) | FFP + vitamin K IV |
| Prompt (4-6 hours) | Vitamin K IV |
| Slow (within 24 hours) | Oral vitamin K |
| Ultra-slow (over a period of days) | Omit warfarin dose (no vitamin K) |
| FFP, fresh frozen plasma; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII. | |
Severity of bleeding as a treatment guide
Studies of methods used to reverse warfarin’s anticoagulation effect are difficult to compare because of a lack of a standardized approach to the classification of bleeds.18,31,32 We’ve used the following classification system, modified from that of Fihn et al,31 to avoid confusion and inform treatment decisions:
- Minor bleed: Reported, not requiring additional testing
- Major bleed: Requiring medical evaluation and inpatient treatment and/or blood transfusion
- Life-threatening bleed: Leading to cardiac arrest, surgical/angiographic intervention, or irreversible sequelae (loss of limb/sight).
Here’s how to put this classification system—and the ACCP’s 2008 guidelines for managing patients with elevated INR16 ( FIGURE )—into action:
In the case of minor bleeding and elevated INR, withhold the next 1 to 2 doses of warfarin.16 If the patient is considered high risk, give oral vitamin K in small amounts (1-2.5 mg). Keep in mind that excessive amounts of vitamin K will promote warfarin resistance.
FIGURE
Reversal of warfarin-induced anticoagulation
FFP, fresh frozen plasma; INR, international normalized ratio; IV, intravenous; PCC, prothrombin complex concentrate; rFVIIa, recombinant activated factor VII.
Adapted from: Ansell J et al. Chest. 2008.16 Ask the patient to return to your office in 1 or 2 days for a recheck of INR. If it remains elevated, give another dose of vitamin K. Warfarin may need to be restarted at a lower dose depending on the clinical situation.17,32
In cases of major bleeding and elevated INR, stop the warfarin, give vitamin K (the administration route will be based on clinical presentation and the urgency of reversal), and arrange for factor replacement and hospital admission.16 Use FFP, if possible, because more is known about its safety than the safety of PCC or rFVIIa. That said, the choice of factor replacement should be based on the urgency of reversal and on clinical condition.16,33,34
INR should be rechecked immediately after factor replacement. Because coagulation factors have varied half-lives, INR should be checked daily for the next 4 days to confirm that it remains at a therapeutic level.16
In cases of life-threatening bleeding, stop the warfarin, give 10 mg vitamin K IV, and replace clotting factors.16 PCC should be considered because it will reverse the anticoagulation in the shortest amount of time, without limitations associated with fluid status, blood type-matching, or infusion reaction.35,36 While the risk of thrombosis needs to be evaluated in each high-risk circumstance, the use of either PCC or rFVIIa, depending on availability, is appropriate for a life-threatening bleed.29,37
Classifying—and treating—our patient
Based on our classification system, we determined that Mary Jo had major bleeding: She needed inpatient monitoring, with the possibility of a blood transfusion, but her condition was not life-threatening. She was hospitalized immediately. Her warfarin was withheld and she was given vitamin K IV and FFP to reverse her hypocoagulable state.
Once Mary Jo’s hypocoagulable state was reversed, which took about 4 hours, she was evaluated and found to have a small bleeding ulcer. The ulcer was cauterized, and her condition remained stable. A detailed investigation of possible reasons for the patient’s elevated INR did not reveal any causes. Three days after the cauterization, Mary Jo was started back on a lower dosing schedule of warfarin. She was discharged after a 5-day stay, with instructions to return to the clinic in 5 days for continued monitoring.
CORRESPONDENCE
Shailendra Prasad, MBBS, MPH, 1020 W. Broadway, Minneapolis, MN 55411; pras0054@umn.edu
1. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167:1414-1419.
2. Beyth RJ. Hemorrhagic complications of oral anticoagulant therapy. Clin Geriatr Med. 2001;17:49-56.
3. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139:893-900.
4. Levine MN, Raskob G, Beyth RJ, et al. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S287-S310.
5. Pengo V, Legnani C, Noventa F, et al. ISCOAT Study Group. (Italian Study on Complications of Oral Anticoagulant Therapy). Oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding. A multicenter inception cohort study. Thromb Haemost. 2001;85:418-422.
6. White RH, McKittrick T, Takakuwa J, et al. Management and prognosis of life-threatening bleeding during warfarin therapy. National Consortium of Anticoagulation Clinics. Arch Intern Med. 1996;156:1197-1201.
7. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91-99.
8. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993;342:1255-1262.
9. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S204-S233.
10. Crowther MA, Douketis JD, Schnurr T, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137:251-254.
11. Whitling AM, Bussey HI, Lyons RM. Comparing different routes and doses of phytonadione for reversing excessive anticoagulation. Arch Intern Med. 1998;158:2136-2140.
12. Nee R, Doppenschmidt D, Donovan DJ, et al. Intravenous versus subcutaneous vitamin K1 in reversing excessive oral anticoagulation. Am J Cardiol. 1999;83:286-288.
13. Fan J, Armitstead JA, Adams AG, et al. A retrospective evaluation of vitamin K1 therapy to reverse the anticoagulant effect of warfarin. Pharmacotherapy. 2003;23:1245-1250.
14. Lubetsky A, Yonath H, Olchovsky D, et al. Comparison of oral vs intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: a prospective randomized controlled study. Arch Intern Med. 2003;163:2469-2473.
15. Hung A, Singh S, Tait RC. A prospective randomized study to determine the optimal dose of intravenous vitamin K in reversal of over-warfarinization. Br J Haematol. 2000;109:537-539.
16. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(suppl):160S-198S.
17. Dentali F, Ageno W, Crowther M. Treatment of coumarin-associated coagulopathy: a systematic review and proposed algorithms. J Thromb Haemost. 2006;4:1853-1863.
18. Makris M, Watson HG. The management of coumarin-induced over-anticoagulation Annotation [see comment]. Br J Haematol. 2001;114:271-280.
19. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126:11-28.
20. Makris M. Optimisation of the prothrombin complex concentrate dose for warfarin reversal. Thromb Res. 2005;115:451-453.
21. Vigue B, Ract C, Tremey B, et al. Ultra-rapid management of oral anticoagulant therapy-related surgical intracranial hemorrhage. Intensive Care Med. 2007;33:721-725.
22. Kohler M. Thrombogenicity of prothrombin complex concentrates. Thromb Res. 1999;95(suppl 1):S13-S17.
23. Lorenz R, Kienast J, Otto U, et al. Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study. Blood Coagul Fibrinolysis. 2007;18:565-570.
24. Pabinger I, Brenner B, Kalina U, et al. Beriplex P/N Anticoagulation Reversal Study Group. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008;6:622-631.
25. Sorensen B, Johansen P, Nielsen GL, et al. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469-477.
26. Brody DL, Aiyagari V, Shackleford AM, et al. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
27. Tanaka KA, Szlam F, Dickneite G, et al. Effects of prothrombin complex concentrate and recombinant activated factor VII on vitamin K antagonist induced anticoagulation. Thromb Res. 2008;122:117-123.
28. Lin J, Hanigan WC, Tarantino M, et al. The use of recombinant activated factor VII to reverse warfarin-induced anticoagulation in patients with hemorrhages in the central nervous system: preliminary findings. J Neurosurg. 2003;98:737-740.
29. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
30. Dager WE, King JH, Regalia RC, et al. Reversal of elevated international normalized ratio and bleeding with low-dose recombinant factor VII in patients receiving warfarin. Pharmacotherapy. 2006;26:1091-1098.
31. Fihn SD, McDonell M, Martin D, et al. Risk factors for complications of chronic anticoagulation. A multicenter study. Warfarin Optimized Outpatient Follow-up Study Group. Ann Intern Med. 1993;118:511-520.
32. Hanley JP. Warfarin reversal. J Clin Pathol. 2004;57:1132-1139.
33. Yasaka M, Sakata T, Minematsu K, et al. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
34. Evans G, Luddington R, Baglin T. Beriplex P/N reverses severe warfarin-induced anticoagulation immediately and completely in patients presenting with major bleeding. Br J Haematol. 2001;115:998-1001.
35. Lubetsky A, Hoffman R, Zimlichman R, et al. Efficacy and safety of complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004;113:371-378.
36. Cartmill M, Dolan G, Byrne JL, et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
37. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
38. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165:1095-1106.
39. Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiological Approach. 6th ed. New York: McGraw-Hill Companies, Inc.; 2005:373-413.
40. Micromedex Healthcare Series. Drug-REAX System. New York: Thomson Reuters; 2008.
1. Wysowski DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch Intern Med. 2007;167:1414-1419.
2. Beyth RJ. Hemorrhagic complications of oral anticoagulant therapy. Clin Geriatr Med. 2001;17:49-56.
3. Linkins LA, Choi PT, Douketis JD. Clinical impact of bleeding in patients taking oral anticoagulant therapy for venous thromboembolism: a meta-analysis. Ann Intern Med. 2003;139:893-900.
4. Levine MN, Raskob G, Beyth RJ, et al. Hemorrhagic complications of anticoagulant treatment: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S287-S310.
5. Pengo V, Legnani C, Noventa F, et al. ISCOAT Study Group. (Italian Study on Complications of Oral Anticoagulant Therapy). Oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and risk of bleeding. A multicenter inception cohort study. Thromb Haemost. 2001;85:418-422.
6. White RH, McKittrick T, Takakuwa J, et al. Management and prognosis of life-threatening bleeding during warfarin therapy. National Consortium of Anticoagulation Clinics. Arch Intern Med. 1996;156:1197-1201.
7. Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91-99.
8. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European Atrial Fibrillation Trial) Study Group. Lancet. 1993;342:1255-1262.
9. Ansell J, Hirsh J, Poller L, et al. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(suppl 3):S204-S233.
10. Crowther MA, Douketis JD, Schnurr T, et al. Oral vitamin K lowers the international normalized ratio more rapidly than subcutaneous vitamin K in the treatment of warfarin-associated coagulopathy. A randomized, controlled trial. Ann Intern Med. 2002;137:251-254.
11. Whitling AM, Bussey HI, Lyons RM. Comparing different routes and doses of phytonadione for reversing excessive anticoagulation. Arch Intern Med. 1998;158:2136-2140.
12. Nee R, Doppenschmidt D, Donovan DJ, et al. Intravenous versus subcutaneous vitamin K1 in reversing excessive oral anticoagulation. Am J Cardiol. 1999;83:286-288.
13. Fan J, Armitstead JA, Adams AG, et al. A retrospective evaluation of vitamin K1 therapy to reverse the anticoagulant effect of warfarin. Pharmacotherapy. 2003;23:1245-1250.
14. Lubetsky A, Yonath H, Olchovsky D, et al. Comparison of oral vs intravenous phytonadione (vitamin K1) in patients with excessive anticoagulation: a prospective randomized controlled study. Arch Intern Med. 2003;163:2469-2473.
15. Hung A, Singh S, Tait RC. A prospective randomized study to determine the optimal dose of intravenous vitamin K in reversal of over-warfarinization. Br J Haematol. 2000;109:537-539.
16. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists. Chest. 2008;133(suppl):160S-198S.
17. Dentali F, Ageno W, Crowther M. Treatment of coumarin-associated coagulopathy: a systematic review and proposed algorithms. J Thromb Haemost. 2006;4:1853-1863.
18. Makris M, Watson HG. The management of coumarin-induced over-anticoagulation Annotation [see comment]. Br J Haematol. 2001;114:271-280.
19. O’Shaughnessy DF, Atterbury C, Bolton Maggs P, et al. British Committee for Standards in Haematology, Blood Transfusion Task Force. Guidelines for the use of fresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol. 2004;126:11-28.
20. Makris M. Optimisation of the prothrombin complex concentrate dose for warfarin reversal. Thromb Res. 2005;115:451-453.
21. Vigue B, Ract C, Tremey B, et al. Ultra-rapid management of oral anticoagulant therapy-related surgical intracranial hemorrhage. Intensive Care Med. 2007;33:721-725.
22. Kohler M. Thrombogenicity of prothrombin complex concentrates. Thromb Res. 1999;95(suppl 1):S13-S17.
23. Lorenz R, Kienast J, Otto U, et al. Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study. Blood Coagul Fibrinolysis. 2007;18:565-570.
24. Pabinger I, Brenner B, Kalina U, et al. Beriplex P/N Anticoagulation Reversal Study Group. Prothrombin complex concentrate (Beriplex P/N) for emergency anticoagulation reversal: a prospective multinational clinical trial. J Thromb Haemost. 2008;6:622-631.
25. Sorensen B, Johansen P, Nielsen GL, et al. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469-477.
26. Brody DL, Aiyagari V, Shackleford AM, et al. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care. 2005;2:263-267.
27. Tanaka KA, Szlam F, Dickneite G, et al. Effects of prothrombin complex concentrate and recombinant activated factor VII on vitamin K antagonist induced anticoagulation. Thromb Res. 2008;122:117-123.
28. Lin J, Hanigan WC, Tarantino M, et al. The use of recombinant activated factor VII to reverse warfarin-induced anticoagulation in patients with hemorrhages in the central nervous system: preliminary findings. J Neurosurg. 2003;98:737-740.
29. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777-785.
30. Dager WE, King JH, Regalia RC, et al. Reversal of elevated international normalized ratio and bleeding with low-dose recombinant factor VII in patients receiving warfarin. Pharmacotherapy. 2006;26:1091-1098.
31. Fihn SD, McDonell M, Martin D, et al. Risk factors for complications of chronic anticoagulation. A multicenter study. Warfarin Optimized Outpatient Follow-up Study Group. Ann Intern Med. 1993;118:511-520.
32. Hanley JP. Warfarin reversal. J Clin Pathol. 2004;57:1132-1139.
33. Yasaka M, Sakata T, Minematsu K, et al. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25-30.
34. Evans G, Luddington R, Baglin T. Beriplex P/N reverses severe warfarin-induced anticoagulation immediately and completely in patients presenting with major bleeding. Br J Haematol. 2001;115:998-1001.
35. Lubetsky A, Hoffman R, Zimlichman R, et al. Efficacy and safety of complex concentrate (Octaplex) for rapid reversal of oral anticoagulation. Thromb Res. 2004;113:371-378.
36. Cartmill M, Dolan G, Byrne JL, et al. Prothrombin complex concentrate for oral anticoagulant reversal in neurosurgical emergencies. Br J Neurosurg. 2000;14:458-461.
37. Deveras RA, Kessler CM. Reversal of warfarin-induced excessive anticoagulation with recombinant human factor VIIa concentrate. Ann Intern Med. 2002;137:884-888.
38. Holbrook AM, Pereira JA, Labiris R, et al. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med. 2005;165:1095-1106.
39. Haines ST, Zeolla M, Witt DM. Venous Thromboembolism. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiological Approach. 6th ed. New York: McGraw-Hill Companies, Inc.; 2005:373-413.
40. Micromedex Healthcare Series. Drug-REAX System. New York: Thomson Reuters; 2008.
Let them eat nuts—this snack is safe for diverticulosis patients
ILLUSTRATIVE CASE
John M, a 50-year-old patient, recently had a routine colonoscopy and was diagnosed with diverticulosis. Concerned because a friend has had multiple bouts of diverticulitis and a partial colectomy, John schedules an appointment to discuss management of diverticulosis. His friend has told John he’ll have to follow a strict diet and avoid nuts, corn, and popcorn altogether. Anxious to avoid the complications his friend has experienced, John turns to you for dietary advice. Would you know what dietary advice is best?
Diverticulosis affects one-third of the US population by age 60; by the age of 85, two-thirds are affected.2,3 This common digestive disorder has been associated with a diet high in refined carbohydrates, and is less prevalent among people who follow a vegetarian diet.4-6 Up to 35% of patients with diverticulosis develop complications, including diverticulitis and diverticular bleeding, that frequently require hospitalization and invasive procedures.7,8
Nuts or no nuts? In search of evidence
Biological mechanisms responsible for the development of diverticular complications are poorly understood.1,4 But luminal trauma has been suggested as a contributory factor and nuts, corn, popcorn, and seeds have long been viewed as likely culprits.8 Thus, physicians have historically advised patients with diverticular disease to avoid these foods.8-12
That recommendation, however, had little evidence to support it. Until the study by Strate et al that we report on here, no studies had assessed the consumption of nuts, corn, popcorn, or seeds as a risk factor for diverticulitis or diverticular complications.1,13 Conversely, there was a growing body of evidence that a diet rich in nuts may provide protection against many common disorders, including coronary heart disease, diabetes, colon and prostate cancers, and gall bladder disease.14-19 The research by Strate et al settles the matter, but it also provides an interesting twist.
STUDY SUMMARY: Nuts and popcorn linked to lower risk
The Strate trial is part of the Health Professionals Follow-up Study, a prospective cohort study that followed male health professionals in the United States from 1986 to 2004.20 A counterpart to the all-female Nurses’ Health Study, this long-running study allowed investigators to evaluate the relationship between nutritional factors and the incidence of serious illnesses such as cancer, heart disease, and other vascular diseases. The study population was comprised of 47,228 men between the ages of 40 and 75 years who completed periodic self-administered medical and dietary questionnaires.
At baseline, all the men were free of diverticulosis or related complications, as well as cancer and inflammatory bowel disease. During the 18 years of follow-up, 801 incident cases of diverticulitis and 383 cases of diverticular bleeding occurred. After analyzing the data, the researchers reported that, not only was the consumption of nuts and/or popcorn not associated with an increased risk of diverticulitis, it had a protective effect. The hazard ratios for men with the highest intake of nuts and/or popcorn (at least twice a week) compared with men with the lowest intake (less than once a month) were 0.80 (95% confidence interval [CI], 0.63-1.01) for nuts and 0.72 (95% CI, 0.56-0.92) for popcorn. The researchers found no association, positive or negative, between corn consumption and diverticulitis, nor between nut, corn, or popcorn consumption and diverticular bleeding or the development of uncomplicated diverticulosis.1
FIGURE
Colonoscopy reveals diverticular disease
This colonoscopic image shows the presence of a diverticulum.
WHAT’S NEW?: A long-standing belief gets debunked
This study—the first to examine the relationship between a diet rich in nuts, corn, or popcorn and diverticular disease—showed that these foods did not increase the risk of developing diverticulosis, diverticulitis, or diverticular bleeding. Moreover, it found an association between a diet rich in nuts or popcorn and a decreased risk of diverticulitis. Although we can’t characterize this as a cause-and-effect relationship based on this study, the evidence convinces us that, at the least, nuts, corn, and popcorn do not increase the risk of diverticular disease. We think we can confidently tell patients to enjoy these foods.
CAVEATS: Protective effect of nuts is tough to explain
As with all cohort studies, there is a possibility of unmeasured confounding variables which, in this case, could account for the protective effect of nuts and popcorn suggested by the decreased risk of diverticulitis. Although this was a large and carefully conducted prospective cohort study involving health professionals, we are not aware of any proven pathophysiologic mechanism by which nuts, corn, and popcorn may either increase or decrease the risk of diverticular disease or its complications.
A randomized controlled trial addressing this dietary issue is unlikely—and probably unnecessary. This study provides the strongest evidence on this topic by far. We think many patients have been unnecessarily deprived of these foods.
The study did not enroll young patients or women. However, diverticulosis is rare before the age of 40.2,9 And, because no clear sex difference has been observed in diverticular disease, we see no reason why this evidence should not apply equally to female patients.2,13
Also of note: This study did not assess total seed intake, per se. Rather, it assessed the consumption of strawberries and blueberries, the source of the seeds. The researchers found no association between strawberries and blueberries and diverticular complications, and we see no reason to tell patients to avoid them.
CHALLENGES TO IMPLEMENTATION: There are no obstacles to implementation
Dietary advice is an integral part of primary care practice. We see no challenges to implementing this practice changer, which should come as welcome news to patients at risk of diverticular disease or its complications.
Acknowledgements
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Strate LL, Liu YL, Syngal S, et al. Nut, corn, and popcorn consumption and the incidence of diverticular disease. JAMA. 2008;300:907-914.
2. Hughes LE. Postmortem survey of diverticular disease of the colon. II. The muscular abnormality of the sigmoid colon. Gut. 1969;10:344-351.
3. Bogardus ST, Jr. What do we know about diverticular disease? A brief overview. J Clin Gastroenterol. 2006;40(suppl 3):S108-S111.
4. Floch MH, Bina I. The natural history of diverticulitis: fact and theory. J Clin Gastroenterol. 2004;38(5 suppl):S2-S7.
5. Nair P, Mayberry JF. Vegetarianism, dietary fibre and gastro-intestinal disease. Dig Dis. 1994;12:177-185.
6. Painter NS, Burkitt DP. Diverticular disease of the colon: a deficiency disease of Western civilization. Br Med J. 1971;2:450-454.
7. McGuire HH, Jr. Bleeding colonic diverticula. A reappraisal of natural history and management. Ann Surg. 1994;220:653-656.
8. Horner JL. Natural history of diverticulosis of the colon. Am J Dig Dis. 1958;3:343-350.
9. Jacobs DO. Clinical practice. Diverticulitis. N Engl J Med. 2007;357:2057-2066.
10. Schechter S, Mulvey J, Eisenstat TE. Management of uncomplicated acute diverticulitis: results of a survey. Dis Colon Rectum. 1999;42:470-475.
11. National Digestive Diseases Information Clearing-house. Diverticulosis and diverticulitis. Bethesda, Md: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; July 2008. NIH publication 08-1163. Available at: http://digestive.niddk.nih.gov/ddiseases/pubs/diverticulosis/. Accessed December 17, 2008.
12. Gearhart SL. Diverticular disease and common anorectal disorders. In: Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw-Hill; 2008:chap 291.
13. Stollman NH, Raskin JB. Diagnosis and management of diverticular disease of the colon in adults. Ad Hoc Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol. 1999;94:3110-3121.
14. Hu FB, Stampfer MJ, Manson JE, et al. Frequent nut consumption and risk of coronary heart disease in women: prospective cohort study. BMJ. 1998;317:1341-1345.
15. Blomhoff R, Carlsen MH, Andersen LF, et al. Health benefits of nuts: potential role of antioxidants. Br J Nutr. 2006;96(suppl 2):S52-S60.
16. Jenab M, Ferrari P, Slimani N, et al. Association of nut and seed intake with colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol Biomarkers Prev. 2004;13:1595-1603.
17. Jiang R, Manson JE, Stampfer MJ, et al. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA. 2002;288:2554-2560.
18. Tsai CJ, Leitzmann MF, Hu FB, et al. Frequent nut consumption and decreased risk of cholecystectomy in women. Am J Clin Nutr. 2004;80:76-81.
19. Albert CM, Gaziano JM, Willett WC, et al. Nut consumption and decreased risk of sudden cardiac death in the Physicians’ Health Study. Arch Intern Med. 2002;162:1382-1387.
20. Harvard School of Public Health. Health professionals follow-up study. Available at: http://www.hsph.harvard.edu/hpfs/. Accessed December 17, 2008.
ILLUSTRATIVE CASE
John M, a 50-year-old patient, recently had a routine colonoscopy and was diagnosed with diverticulosis. Concerned because a friend has had multiple bouts of diverticulitis and a partial colectomy, John schedules an appointment to discuss management of diverticulosis. His friend has told John he’ll have to follow a strict diet and avoid nuts, corn, and popcorn altogether. Anxious to avoid the complications his friend has experienced, John turns to you for dietary advice. Would you know what dietary advice is best?
Diverticulosis affects one-third of the US population by age 60; by the age of 85, two-thirds are affected.2,3 This common digestive disorder has been associated with a diet high in refined carbohydrates, and is less prevalent among people who follow a vegetarian diet.4-6 Up to 35% of patients with diverticulosis develop complications, including diverticulitis and diverticular bleeding, that frequently require hospitalization and invasive procedures.7,8
Nuts or no nuts? In search of evidence
Biological mechanisms responsible for the development of diverticular complications are poorly understood.1,4 But luminal trauma has been suggested as a contributory factor and nuts, corn, popcorn, and seeds have long been viewed as likely culprits.8 Thus, physicians have historically advised patients with diverticular disease to avoid these foods.8-12
That recommendation, however, had little evidence to support it. Until the study by Strate et al that we report on here, no studies had assessed the consumption of nuts, corn, popcorn, or seeds as a risk factor for diverticulitis or diverticular complications.1,13 Conversely, there was a growing body of evidence that a diet rich in nuts may provide protection against many common disorders, including coronary heart disease, diabetes, colon and prostate cancers, and gall bladder disease.14-19 The research by Strate et al settles the matter, but it also provides an interesting twist.
STUDY SUMMARY: Nuts and popcorn linked to lower risk
The Strate trial is part of the Health Professionals Follow-up Study, a prospective cohort study that followed male health professionals in the United States from 1986 to 2004.20 A counterpart to the all-female Nurses’ Health Study, this long-running study allowed investigators to evaluate the relationship between nutritional factors and the incidence of serious illnesses such as cancer, heart disease, and other vascular diseases. The study population was comprised of 47,228 men between the ages of 40 and 75 years who completed periodic self-administered medical and dietary questionnaires.
At baseline, all the men were free of diverticulosis or related complications, as well as cancer and inflammatory bowel disease. During the 18 years of follow-up, 801 incident cases of diverticulitis and 383 cases of diverticular bleeding occurred. After analyzing the data, the researchers reported that, not only was the consumption of nuts and/or popcorn not associated with an increased risk of diverticulitis, it had a protective effect. The hazard ratios for men with the highest intake of nuts and/or popcorn (at least twice a week) compared with men with the lowest intake (less than once a month) were 0.80 (95% confidence interval [CI], 0.63-1.01) for nuts and 0.72 (95% CI, 0.56-0.92) for popcorn. The researchers found no association, positive or negative, between corn consumption and diverticulitis, nor between nut, corn, or popcorn consumption and diverticular bleeding or the development of uncomplicated diverticulosis.1
FIGURE
Colonoscopy reveals diverticular disease
This colonoscopic image shows the presence of a diverticulum.
WHAT’S NEW?: A long-standing belief gets debunked
This study—the first to examine the relationship between a diet rich in nuts, corn, or popcorn and diverticular disease—showed that these foods did not increase the risk of developing diverticulosis, diverticulitis, or diverticular bleeding. Moreover, it found an association between a diet rich in nuts or popcorn and a decreased risk of diverticulitis. Although we can’t characterize this as a cause-and-effect relationship based on this study, the evidence convinces us that, at the least, nuts, corn, and popcorn do not increase the risk of diverticular disease. We think we can confidently tell patients to enjoy these foods.
CAVEATS: Protective effect of nuts is tough to explain
As with all cohort studies, there is a possibility of unmeasured confounding variables which, in this case, could account for the protective effect of nuts and popcorn suggested by the decreased risk of diverticulitis. Although this was a large and carefully conducted prospective cohort study involving health professionals, we are not aware of any proven pathophysiologic mechanism by which nuts, corn, and popcorn may either increase or decrease the risk of diverticular disease or its complications.
A randomized controlled trial addressing this dietary issue is unlikely—and probably unnecessary. This study provides the strongest evidence on this topic by far. We think many patients have been unnecessarily deprived of these foods.
The study did not enroll young patients or women. However, diverticulosis is rare before the age of 40.2,9 And, because no clear sex difference has been observed in diverticular disease, we see no reason why this evidence should not apply equally to female patients.2,13
Also of note: This study did not assess total seed intake, per se. Rather, it assessed the consumption of strawberries and blueberries, the source of the seeds. The researchers found no association between strawberries and blueberries and diverticular complications, and we see no reason to tell patients to avoid them.
CHALLENGES TO IMPLEMENTATION: There are no obstacles to implementation
Dietary advice is an integral part of primary care practice. We see no challenges to implementing this practice changer, which should come as welcome news to patients at risk of diverticular disease or its complications.
Acknowledgements
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
ILLUSTRATIVE CASE
John M, a 50-year-old patient, recently had a routine colonoscopy and was diagnosed with diverticulosis. Concerned because a friend has had multiple bouts of diverticulitis and a partial colectomy, John schedules an appointment to discuss management of diverticulosis. His friend has told John he’ll have to follow a strict diet and avoid nuts, corn, and popcorn altogether. Anxious to avoid the complications his friend has experienced, John turns to you for dietary advice. Would you know what dietary advice is best?
Diverticulosis affects one-third of the US population by age 60; by the age of 85, two-thirds are affected.2,3 This common digestive disorder has been associated with a diet high in refined carbohydrates, and is less prevalent among people who follow a vegetarian diet.4-6 Up to 35% of patients with diverticulosis develop complications, including diverticulitis and diverticular bleeding, that frequently require hospitalization and invasive procedures.7,8
Nuts or no nuts? In search of evidence
Biological mechanisms responsible for the development of diverticular complications are poorly understood.1,4 But luminal trauma has been suggested as a contributory factor and nuts, corn, popcorn, and seeds have long been viewed as likely culprits.8 Thus, physicians have historically advised patients with diverticular disease to avoid these foods.8-12
That recommendation, however, had little evidence to support it. Until the study by Strate et al that we report on here, no studies had assessed the consumption of nuts, corn, popcorn, or seeds as a risk factor for diverticulitis or diverticular complications.1,13 Conversely, there was a growing body of evidence that a diet rich in nuts may provide protection against many common disorders, including coronary heart disease, diabetes, colon and prostate cancers, and gall bladder disease.14-19 The research by Strate et al settles the matter, but it also provides an interesting twist.
STUDY SUMMARY: Nuts and popcorn linked to lower risk
The Strate trial is part of the Health Professionals Follow-up Study, a prospective cohort study that followed male health professionals in the United States from 1986 to 2004.20 A counterpart to the all-female Nurses’ Health Study, this long-running study allowed investigators to evaluate the relationship between nutritional factors and the incidence of serious illnesses such as cancer, heart disease, and other vascular diseases. The study population was comprised of 47,228 men between the ages of 40 and 75 years who completed periodic self-administered medical and dietary questionnaires.
At baseline, all the men were free of diverticulosis or related complications, as well as cancer and inflammatory bowel disease. During the 18 years of follow-up, 801 incident cases of diverticulitis and 383 cases of diverticular bleeding occurred. After analyzing the data, the researchers reported that, not only was the consumption of nuts and/or popcorn not associated with an increased risk of diverticulitis, it had a protective effect. The hazard ratios for men with the highest intake of nuts and/or popcorn (at least twice a week) compared with men with the lowest intake (less than once a month) were 0.80 (95% confidence interval [CI], 0.63-1.01) for nuts and 0.72 (95% CI, 0.56-0.92) for popcorn. The researchers found no association, positive or negative, between corn consumption and diverticulitis, nor between nut, corn, or popcorn consumption and diverticular bleeding or the development of uncomplicated diverticulosis.1
FIGURE
Colonoscopy reveals diverticular disease
This colonoscopic image shows the presence of a diverticulum.
WHAT’S NEW?: A long-standing belief gets debunked
This study—the first to examine the relationship between a diet rich in nuts, corn, or popcorn and diverticular disease—showed that these foods did not increase the risk of developing diverticulosis, diverticulitis, or diverticular bleeding. Moreover, it found an association between a diet rich in nuts or popcorn and a decreased risk of diverticulitis. Although we can’t characterize this as a cause-and-effect relationship based on this study, the evidence convinces us that, at the least, nuts, corn, and popcorn do not increase the risk of diverticular disease. We think we can confidently tell patients to enjoy these foods.
CAVEATS: Protective effect of nuts is tough to explain
As with all cohort studies, there is a possibility of unmeasured confounding variables which, in this case, could account for the protective effect of nuts and popcorn suggested by the decreased risk of diverticulitis. Although this was a large and carefully conducted prospective cohort study involving health professionals, we are not aware of any proven pathophysiologic mechanism by which nuts, corn, and popcorn may either increase or decrease the risk of diverticular disease or its complications.
A randomized controlled trial addressing this dietary issue is unlikely—and probably unnecessary. This study provides the strongest evidence on this topic by far. We think many patients have been unnecessarily deprived of these foods.
The study did not enroll young patients or women. However, diverticulosis is rare before the age of 40.2,9 And, because no clear sex difference has been observed in diverticular disease, we see no reason why this evidence should not apply equally to female patients.2,13
Also of note: This study did not assess total seed intake, per se. Rather, it assessed the consumption of strawberries and blueberries, the source of the seeds. The researchers found no association between strawberries and blueberries and diverticular complications, and we see no reason to tell patients to avoid them.
CHALLENGES TO IMPLEMENTATION: There are no obstacles to implementation
Dietary advice is an integral part of primary care practice. We see no challenges to implementing this practice changer, which should come as welcome news to patients at risk of diverticular disease or its complications.
Acknowledgements
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Strate LL, Liu YL, Syngal S, et al. Nut, corn, and popcorn consumption and the incidence of diverticular disease. JAMA. 2008;300:907-914.
2. Hughes LE. Postmortem survey of diverticular disease of the colon. II. The muscular abnormality of the sigmoid colon. Gut. 1969;10:344-351.
3. Bogardus ST, Jr. What do we know about diverticular disease? A brief overview. J Clin Gastroenterol. 2006;40(suppl 3):S108-S111.
4. Floch MH, Bina I. The natural history of diverticulitis: fact and theory. J Clin Gastroenterol. 2004;38(5 suppl):S2-S7.
5. Nair P, Mayberry JF. Vegetarianism, dietary fibre and gastro-intestinal disease. Dig Dis. 1994;12:177-185.
6. Painter NS, Burkitt DP. Diverticular disease of the colon: a deficiency disease of Western civilization. Br Med J. 1971;2:450-454.
7. McGuire HH, Jr. Bleeding colonic diverticula. A reappraisal of natural history and management. Ann Surg. 1994;220:653-656.
8. Horner JL. Natural history of diverticulosis of the colon. Am J Dig Dis. 1958;3:343-350.
9. Jacobs DO. Clinical practice. Diverticulitis. N Engl J Med. 2007;357:2057-2066.
10. Schechter S, Mulvey J, Eisenstat TE. Management of uncomplicated acute diverticulitis: results of a survey. Dis Colon Rectum. 1999;42:470-475.
11. National Digestive Diseases Information Clearing-house. Diverticulosis and diverticulitis. Bethesda, Md: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; July 2008. NIH publication 08-1163. Available at: http://digestive.niddk.nih.gov/ddiseases/pubs/diverticulosis/. Accessed December 17, 2008.
12. Gearhart SL. Diverticular disease and common anorectal disorders. In: Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw-Hill; 2008:chap 291.
13. Stollman NH, Raskin JB. Diagnosis and management of diverticular disease of the colon in adults. Ad Hoc Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol. 1999;94:3110-3121.
14. Hu FB, Stampfer MJ, Manson JE, et al. Frequent nut consumption and risk of coronary heart disease in women: prospective cohort study. BMJ. 1998;317:1341-1345.
15. Blomhoff R, Carlsen MH, Andersen LF, et al. Health benefits of nuts: potential role of antioxidants. Br J Nutr. 2006;96(suppl 2):S52-S60.
16. Jenab M, Ferrari P, Slimani N, et al. Association of nut and seed intake with colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol Biomarkers Prev. 2004;13:1595-1603.
17. Jiang R, Manson JE, Stampfer MJ, et al. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA. 2002;288:2554-2560.
18. Tsai CJ, Leitzmann MF, Hu FB, et al. Frequent nut consumption and decreased risk of cholecystectomy in women. Am J Clin Nutr. 2004;80:76-81.
19. Albert CM, Gaziano JM, Willett WC, et al. Nut consumption and decreased risk of sudden cardiac death in the Physicians’ Health Study. Arch Intern Med. 2002;162:1382-1387.
20. Harvard School of Public Health. Health professionals follow-up study. Available at: http://www.hsph.harvard.edu/hpfs/. Accessed December 17, 2008.
1. Strate LL, Liu YL, Syngal S, et al. Nut, corn, and popcorn consumption and the incidence of diverticular disease. JAMA. 2008;300:907-914.
2. Hughes LE. Postmortem survey of diverticular disease of the colon. II. The muscular abnormality of the sigmoid colon. Gut. 1969;10:344-351.
3. Bogardus ST, Jr. What do we know about diverticular disease? A brief overview. J Clin Gastroenterol. 2006;40(suppl 3):S108-S111.
4. Floch MH, Bina I. The natural history of diverticulitis: fact and theory. J Clin Gastroenterol. 2004;38(5 suppl):S2-S7.
5. Nair P, Mayberry JF. Vegetarianism, dietary fibre and gastro-intestinal disease. Dig Dis. 1994;12:177-185.
6. Painter NS, Burkitt DP. Diverticular disease of the colon: a deficiency disease of Western civilization. Br Med J. 1971;2:450-454.
7. McGuire HH, Jr. Bleeding colonic diverticula. A reappraisal of natural history and management. Ann Surg. 1994;220:653-656.
8. Horner JL. Natural history of diverticulosis of the colon. Am J Dig Dis. 1958;3:343-350.
9. Jacobs DO. Clinical practice. Diverticulitis. N Engl J Med. 2007;357:2057-2066.
10. Schechter S, Mulvey J, Eisenstat TE. Management of uncomplicated acute diverticulitis: results of a survey. Dis Colon Rectum. 1999;42:470-475.
11. National Digestive Diseases Information Clearing-house. Diverticulosis and diverticulitis. Bethesda, Md: National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health; July 2008. NIH publication 08-1163. Available at: http://digestive.niddk.nih.gov/ddiseases/pubs/diverticulosis/. Accessed December 17, 2008.
12. Gearhart SL. Diverticular disease and common anorectal disorders. In: Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw-Hill; 2008:chap 291.
13. Stollman NH, Raskin JB. Diagnosis and management of diverticular disease of the colon in adults. Ad Hoc Practice Parameters Committee of the American College of Gastroenterology. Am J Gastroenterol. 1999;94:3110-3121.
14. Hu FB, Stampfer MJ, Manson JE, et al. Frequent nut consumption and risk of coronary heart disease in women: prospective cohort study. BMJ. 1998;317:1341-1345.
15. Blomhoff R, Carlsen MH, Andersen LF, et al. Health benefits of nuts: potential role of antioxidants. Br J Nutr. 2006;96(suppl 2):S52-S60.
16. Jenab M, Ferrari P, Slimani N, et al. Association of nut and seed intake with colorectal cancer risk in the European Prospective Investigation into Cancer and Nutrition. Cancer Epidemiol Biomarkers Prev. 2004;13:1595-1603.
17. Jiang R, Manson JE, Stampfer MJ, et al. Nut and peanut butter consumption and risk of type 2 diabetes in women. JAMA. 2002;288:2554-2560.
18. Tsai CJ, Leitzmann MF, Hu FB, et al. Frequent nut consumption and decreased risk of cholecystectomy in women. Am J Clin Nutr. 2004;80:76-81.
19. Albert CM, Gaziano JM, Willett WC, et al. Nut consumption and decreased risk of sudden cardiac death in the Physicians’ Health Study. Arch Intern Med. 2002;162:1382-1387.
20. Harvard School of Public Health. Health professionals follow-up study. Available at: http://www.hsph.harvard.edu/hpfs/. Accessed December 17, 2008.
Copyright © 2009 The Family Physicians Inquiries Network.
All rights reserved.
Acute gout: Oral steroids work as well as NSAIDs
Use a short course of oral steroids (prednisone 30-40 mg/d for 5 days) for treatment of acute gout when nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated. Steroids are also a reasonable choice as first-line treatment.1,2
Strength of recommendation
B: 2 good-quality, randomized controlled trials (RCTs)
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomized equivalence trial. Lancet. 2008;371:1854-1860.
Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
ILLUSTRATIVE CASE
A 68-year-old man with a history of ulcer disease and mild renal insufficiency comes to your office complaining of severe pain in his right foot. You note swelling and redness around the base of the big toe and diagnose acute gout. Wishing to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine because of the patient’s medical history, you wonder what you can safely prescribe for pain relief.
NSAIDs have become the mainstay of treatment for acute gout,3,4 replacing colchicine—widely used for gout pain relief since the early 19th century.5 Colchicine fell out of favor because it routinely causes diarrhea and requires caution in patients with renal insufficiency.6 Now, however, there is growing concern about the adverse effects of NSAIDs.
Comorbidities, age, mean fewer options
NSAIDs increase the risk of gastrointestinal (GI) bleeding, especially in the first week of use.7 Cyclooxygenase-2 (COX-2) inhibitors, considered as effective as NSAIDs in treating acute gout pain,8 are also associated with GI bleeds.9 In addition, NSAIDs and COX-2 inhibitors increase cardiovascular risks, prompting the American Heart Association to recommend restricted use of both.10 NSAIDs’ effect on renal function, fluid retention, and interactions with anticoagulants are additional concerns, because gout patients are generally older and often have comorbid renal and cardiovascular diseases.3,11-13
In the United States, nearly 70% of patients who develop acute gout seek treatment from primary care physicians.12 Family physicians need a safe alternative to NSAIDs to relieve the severe pain associated with this condition. Will oral corticosteroids fit the bill?
STUDY SUMMARIES: Oral steroids: A safe and effective alternative
Janssens et al1 conducted a double-blind, randomized equivalence trial of 118 patients to compare the efficacy of prednisolone and naproxen for the treatment of monoarticular gout, confirmed by crystal analysis of synovial fluid. The study was conducted in the eastern Netherlands at a trial center patients were referred to by their family physicians. Those with major comorbidities, including a history of GI bleed or peptic ulcer, were excluded.
Participants were randomized to receive either prednisolone 35 mg* or naproxen 500 mg twice a day, with look-alike placebo tablets of the alternate drug, for 5 days. Pain, the primary outcome, was scored on a validated visual analog scale from 0 mm (no pain) to 100 mm (worst pain experienced).15 The reduction in the pain score at 90 hours was similar in both groups. Only a few minor side effects were reported in both groups, and all completely resolved in 3 weeks.
The study by Man et al2 was a randomized trial that compared indomethacin with oral prednisolone in 90 patients presenting to an emergency department in Hong Kong. Diagnosis of gout was made by clinical impression. Participants in the indomethacin group also received an intramuscular (IM) injection of diclofenac 75 mg, and those in both groups were monitored for acetaminophen use as a secondary endpoint.
Pain reduction, the primary endpoint, was assessed with a 10-point visual analog score, and was slightly better statistically in the oral steroid group. The study was not designed to evaluate for safety, but the authors noted that patients in the indomethacin group experienced more adverse effects (number needed to harm [NNH] for any adverse event: 3; NNH for serious events: 6).

Short-term steroids have few side effects
In both studies, patients receiving oral steroids experienced no significant side effects. This finding is consistent with other studies that have investigated short-term oral steroid use in the treatment of both rheumatoid arthritis and asthma.16,17
WHAT’S NEW?: Evidence supports use of steroids for acute gout
In the United States, prednisone is prescribed as treatment for acute gout only about 9% of the time.12 These 2 studies—the first randomized trials comparing oral steroids with NSAIDs, the usual gout treatment—may lead to greater use of steroids for this painful condition.
Both studies were well designed and conducted in an outpatient (or emergency) setting. Both showed that a short course of oral steroids is as effective as NSAIDs, and without significant side effects.
Previous studies have compared IM steroids with NSAIDs, and IM steroids with IM adrenocorticotropic hormone (ACTH).18,19 However, these studies were not blinded—just one of their methodological problems.4
CAVEATS: Joint aspiration is not the norm
In the Janssens study, participants were diagnosed with gout after monosodium urate crystals were found in joint aspirate.1 This may not be the usual practice in primary care settings, where a clinical diagnosis of gout is typically made. The authors indicate that the failure to perform joint aspiration will lead to occasional cases of septic arthritis being treated with oral steroids. We recommend joint aspiration or a referral for such a procedure when clinical evidence (eg, fever and leukocytosis) is suggestive of septic arthritis.
Possible impact of acetaminophen
In the study by Man et al, acetaminophen was used by both groups as an adjunct for pain relief, and the amount used was higher (mean 10.3 g vs 6.4 g over 14 days) in the oral steroid group. It is possible that some of the pain relief experienced by those in the steroid group may have been from acetaminophen; however, a difference of 4 g over a 14-day period makes that unlikely. Even if additional acetaminophen is required, the advantages of oral steroids rather than NSAIDs or colchicine for patients with contraindications remain.
Also of note: These trials examined short-term treatment of acute gout. These findings cannot be extrapolated to the treatment of intercurrent gout or chronic gouty arthritis, since long-term steroid use has severe adverse effects.
CHALLENGES TO IMPLEMENTATION: No significant barriers
We found little to prevent physicians from adopting this practice changer. Oral steroids are readily available and inexpensive, and most primary care clinicians regularly prescribe them for other conditions. This practice change recommendation should be readily implemented.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
* Prednisone is the precursor of prednisolone and is activated in the liver. The activity of both drugs is comparable, and prednisone and prednisolone can be converted milligram to milligram. However, prednisolone may be preferred for patients with severe liver disease.14 (In the United States, prednisolone is available as a liquid and prednisone as a tablet.)
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860.
2. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
3. Sutaria S, Katbamna R, Underwood M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout—a systematic review. Rheumatology. 2006;45:1422-1431.
4. Janssens HJ, Lucassen PL, Van de Laar FA, Janssen M, Van de Lisdonk EH. Systemic corticosteroids for acute gout. Cochrane Database Syst Rev. 2008;(2):CD005521.-
5. Weinberger A, Pinkhas J. The history of colchicine. Korot. 1980;7:760-763.
6. Ahern MJ, Reid C, Gordon TP, McCredie M, Brooks PM, Jones M. Does colchicine work? The results of the first controlled study in acute gout. ANZ J Med. 1987;17:301-304.
7. Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320-326.
8. Rubin BR, Burton R, Navarra S, et al. Efficacy and safety profile of treatment with etoricoxib 120 mg once daily compared with indomethacin 50 mg three times daily in acute gout: a randomized controlled trial. Arthritis Rheum. 2004;50:598-606.
9. Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf. 2004;27:411-420.
10. Antman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115:1634-1642.
11. Petersel D, Schlesinger N. Treatment of acute gout in hospitalized patients. J Rheumatol. 2007;34:1566-1568.
12. Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498-501.
13. Krishnan E, Svendsen K, Neaton JD, Grandits G, Kuller LH. MRFIT Research Group. Long-term cardiovascular mortality among middle-aged men with gout. Arch Intern Med. 2008;168:1104-1110.
14. Davis M, Williams R, Chakraborty J, et al. Prednisone or prednisolone for the treatment of chronic active hepatitis? A comparison of plasma availability. Br J Clin Pharmacol. 1978;5:501-505.
15. Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23:285-295.
16. Gotzsche PC, Johansen HK. Short-term low-dose corticosteroids vs placebo and nonsteroidal antiinflammatory drugs in rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD000189.-
17. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002308.-
18. Alloway JA, Moriarty MJ, Hoogland YT, Nashel DJ. Comparison of triamcinolone acetonide with indomethacin in the treatment of acute gouty arthritis. J Rheumatol. 1993;20:111-113.
19. Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and triamcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol. 1994;21:1325-1327.
Use a short course of oral steroids (prednisone 30-40 mg/d for 5 days) for treatment of acute gout when nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated. Steroids are also a reasonable choice as first-line treatment.1,2
Strength of recommendation
B: 2 good-quality, randomized controlled trials (RCTs)
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomized equivalence trial. Lancet. 2008;371:1854-1860.
Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
ILLUSTRATIVE CASE
A 68-year-old man with a history of ulcer disease and mild renal insufficiency comes to your office complaining of severe pain in his right foot. You note swelling and redness around the base of the big toe and diagnose acute gout. Wishing to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine because of the patient’s medical history, you wonder what you can safely prescribe for pain relief.
NSAIDs have become the mainstay of treatment for acute gout,3,4 replacing colchicine—widely used for gout pain relief since the early 19th century.5 Colchicine fell out of favor because it routinely causes diarrhea and requires caution in patients with renal insufficiency.6 Now, however, there is growing concern about the adverse effects of NSAIDs.
Comorbidities, age, mean fewer options
NSAIDs increase the risk of gastrointestinal (GI) bleeding, especially in the first week of use.7 Cyclooxygenase-2 (COX-2) inhibitors, considered as effective as NSAIDs in treating acute gout pain,8 are also associated with GI bleeds.9 In addition, NSAIDs and COX-2 inhibitors increase cardiovascular risks, prompting the American Heart Association to recommend restricted use of both.10 NSAIDs’ effect on renal function, fluid retention, and interactions with anticoagulants are additional concerns, because gout patients are generally older and often have comorbid renal and cardiovascular diseases.3,11-13
In the United States, nearly 70% of patients who develop acute gout seek treatment from primary care physicians.12 Family physicians need a safe alternative to NSAIDs to relieve the severe pain associated with this condition. Will oral corticosteroids fit the bill?
STUDY SUMMARIES: Oral steroids: A safe and effective alternative
Janssens et al1 conducted a double-blind, randomized equivalence trial of 118 patients to compare the efficacy of prednisolone and naproxen for the treatment of monoarticular gout, confirmed by crystal analysis of synovial fluid. The study was conducted in the eastern Netherlands at a trial center patients were referred to by their family physicians. Those with major comorbidities, including a history of GI bleed or peptic ulcer, were excluded.
Participants were randomized to receive either prednisolone 35 mg* or naproxen 500 mg twice a day, with look-alike placebo tablets of the alternate drug, for 5 days. Pain, the primary outcome, was scored on a validated visual analog scale from 0 mm (no pain) to 100 mm (worst pain experienced).15 The reduction in the pain score at 90 hours was similar in both groups. Only a few minor side effects were reported in both groups, and all completely resolved in 3 weeks.
The study by Man et al2 was a randomized trial that compared indomethacin with oral prednisolone in 90 patients presenting to an emergency department in Hong Kong. Diagnosis of gout was made by clinical impression. Participants in the indomethacin group also received an intramuscular (IM) injection of diclofenac 75 mg, and those in both groups were monitored for acetaminophen use as a secondary endpoint.
Pain reduction, the primary endpoint, was assessed with a 10-point visual analog score, and was slightly better statistically in the oral steroid group. The study was not designed to evaluate for safety, but the authors noted that patients in the indomethacin group experienced more adverse effects (number needed to harm [NNH] for any adverse event: 3; NNH for serious events: 6).
Short-term steroids have few side effects
In both studies, patients receiving oral steroids experienced no significant side effects. This finding is consistent with other studies that have investigated short-term oral steroid use in the treatment of both rheumatoid arthritis and asthma.16,17
WHAT’S NEW?: Evidence supports use of steroids for acute gout
In the United States, prednisone is prescribed as treatment for acute gout only about 9% of the time.12 These 2 studies—the first randomized trials comparing oral steroids with NSAIDs, the usual gout treatment—may lead to greater use of steroids for this painful condition.
Both studies were well designed and conducted in an outpatient (or emergency) setting. Both showed that a short course of oral steroids is as effective as NSAIDs, and without significant side effects.
Previous studies have compared IM steroids with NSAIDs, and IM steroids with IM adrenocorticotropic hormone (ACTH).18,19 However, these studies were not blinded—just one of their methodological problems.4
CAVEATS: Joint aspiration is not the norm
In the Janssens study, participants were diagnosed with gout after monosodium urate crystals were found in joint aspirate.1 This may not be the usual practice in primary care settings, where a clinical diagnosis of gout is typically made. The authors indicate that the failure to perform joint aspiration will lead to occasional cases of septic arthritis being treated with oral steroids. We recommend joint aspiration or a referral for such a procedure when clinical evidence (eg, fever and leukocytosis) is suggestive of septic arthritis.
Possible impact of acetaminophen
In the study by Man et al, acetaminophen was used by both groups as an adjunct for pain relief, and the amount used was higher (mean 10.3 g vs 6.4 g over 14 days) in the oral steroid group. It is possible that some of the pain relief experienced by those in the steroid group may have been from acetaminophen; however, a difference of 4 g over a 14-day period makes that unlikely. Even if additional acetaminophen is required, the advantages of oral steroids rather than NSAIDs or colchicine for patients with contraindications remain.
Also of note: These trials examined short-term treatment of acute gout. These findings cannot be extrapolated to the treatment of intercurrent gout or chronic gouty arthritis, since long-term steroid use has severe adverse effects.
CHALLENGES TO IMPLEMENTATION: No significant barriers
We found little to prevent physicians from adopting this practice changer. Oral steroids are readily available and inexpensive, and most primary care clinicians regularly prescribe them for other conditions. This practice change recommendation should be readily implemented.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
* Prednisone is the precursor of prednisolone and is activated in the liver. The activity of both drugs is comparable, and prednisone and prednisolone can be converted milligram to milligram. However, prednisolone may be preferred for patients with severe liver disease.14 (In the United States, prednisolone is available as a liquid and prednisone as a tablet.)
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Use a short course of oral steroids (prednisone 30-40 mg/d for 5 days) for treatment of acute gout when nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated. Steroids are also a reasonable choice as first-line treatment.1,2
Strength of recommendation
B: 2 good-quality, randomized controlled trials (RCTs)
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomized equivalence trial. Lancet. 2008;371:1854-1860.
Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
ILLUSTRATIVE CASE
A 68-year-old man with a history of ulcer disease and mild renal insufficiency comes to your office complaining of severe pain in his right foot. You note swelling and redness around the base of the big toe and diagnose acute gout. Wishing to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine because of the patient’s medical history, you wonder what you can safely prescribe for pain relief.
NSAIDs have become the mainstay of treatment for acute gout,3,4 replacing colchicine—widely used for gout pain relief since the early 19th century.5 Colchicine fell out of favor because it routinely causes diarrhea and requires caution in patients with renal insufficiency.6 Now, however, there is growing concern about the adverse effects of NSAIDs.
Comorbidities, age, mean fewer options
NSAIDs increase the risk of gastrointestinal (GI) bleeding, especially in the first week of use.7 Cyclooxygenase-2 (COX-2) inhibitors, considered as effective as NSAIDs in treating acute gout pain,8 are also associated with GI bleeds.9 In addition, NSAIDs and COX-2 inhibitors increase cardiovascular risks, prompting the American Heart Association to recommend restricted use of both.10 NSAIDs’ effect on renal function, fluid retention, and interactions with anticoagulants are additional concerns, because gout patients are generally older and often have comorbid renal and cardiovascular diseases.3,11-13
In the United States, nearly 70% of patients who develop acute gout seek treatment from primary care physicians.12 Family physicians need a safe alternative to NSAIDs to relieve the severe pain associated with this condition. Will oral corticosteroids fit the bill?
STUDY SUMMARIES: Oral steroids: A safe and effective alternative
Janssens et al1 conducted a double-blind, randomized equivalence trial of 118 patients to compare the efficacy of prednisolone and naproxen for the treatment of monoarticular gout, confirmed by crystal analysis of synovial fluid. The study was conducted in the eastern Netherlands at a trial center patients were referred to by their family physicians. Those with major comorbidities, including a history of GI bleed or peptic ulcer, were excluded.
Participants were randomized to receive either prednisolone 35 mg* or naproxen 500 mg twice a day, with look-alike placebo tablets of the alternate drug, for 5 days. Pain, the primary outcome, was scored on a validated visual analog scale from 0 mm (no pain) to 100 mm (worst pain experienced).15 The reduction in the pain score at 90 hours was similar in both groups. Only a few minor side effects were reported in both groups, and all completely resolved in 3 weeks.
The study by Man et al2 was a randomized trial that compared indomethacin with oral prednisolone in 90 patients presenting to an emergency department in Hong Kong. Diagnosis of gout was made by clinical impression. Participants in the indomethacin group also received an intramuscular (IM) injection of diclofenac 75 mg, and those in both groups were monitored for acetaminophen use as a secondary endpoint.
Pain reduction, the primary endpoint, was assessed with a 10-point visual analog score, and was slightly better statistically in the oral steroid group. The study was not designed to evaluate for safety, but the authors noted that patients in the indomethacin group experienced more adverse effects (number needed to harm [NNH] for any adverse event: 3; NNH for serious events: 6).
Short-term steroids have few side effects
In both studies, patients receiving oral steroids experienced no significant side effects. This finding is consistent with other studies that have investigated short-term oral steroid use in the treatment of both rheumatoid arthritis and asthma.16,17
WHAT’S NEW?: Evidence supports use of steroids for acute gout
In the United States, prednisone is prescribed as treatment for acute gout only about 9% of the time.12 These 2 studies—the first randomized trials comparing oral steroids with NSAIDs, the usual gout treatment—may lead to greater use of steroids for this painful condition.
Both studies were well designed and conducted in an outpatient (or emergency) setting. Both showed that a short course of oral steroids is as effective as NSAIDs, and without significant side effects.
Previous studies have compared IM steroids with NSAIDs, and IM steroids with IM adrenocorticotropic hormone (ACTH).18,19 However, these studies were not blinded—just one of their methodological problems.4
CAVEATS: Joint aspiration is not the norm
In the Janssens study, participants were diagnosed with gout after monosodium urate crystals were found in joint aspirate.1 This may not be the usual practice in primary care settings, where a clinical diagnosis of gout is typically made. The authors indicate that the failure to perform joint aspiration will lead to occasional cases of septic arthritis being treated with oral steroids. We recommend joint aspiration or a referral for such a procedure when clinical evidence (eg, fever and leukocytosis) is suggestive of septic arthritis.
Possible impact of acetaminophen
In the study by Man et al, acetaminophen was used by both groups as an adjunct for pain relief, and the amount used was higher (mean 10.3 g vs 6.4 g over 14 days) in the oral steroid group. It is possible that some of the pain relief experienced by those in the steroid group may have been from acetaminophen; however, a difference of 4 g over a 14-day period makes that unlikely. Even if additional acetaminophen is required, the advantages of oral steroids rather than NSAIDs or colchicine for patients with contraindications remain.
Also of note: These trials examined short-term treatment of acute gout. These findings cannot be extrapolated to the treatment of intercurrent gout or chronic gouty arthritis, since long-term steroid use has severe adverse effects.
CHALLENGES TO IMPLEMENTATION: No significant barriers
We found little to prevent physicians from adopting this practice changer. Oral steroids are readily available and inexpensive, and most primary care clinicians regularly prescribe them for other conditions. This practice change recommendation should be readily implemented.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
* Prednisone is the precursor of prednisolone and is activated in the liver. The activity of both drugs is comparable, and prednisone and prednisolone can be converted milligram to milligram. However, prednisolone may be preferred for patients with severe liver disease.14 (In the United States, prednisolone is available as a liquid and prednisone as a tablet.)
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860.
2. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
3. Sutaria S, Katbamna R, Underwood M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout—a systematic review. Rheumatology. 2006;45:1422-1431.
4. Janssens HJ, Lucassen PL, Van de Laar FA, Janssen M, Van de Lisdonk EH. Systemic corticosteroids for acute gout. Cochrane Database Syst Rev. 2008;(2):CD005521.-
5. Weinberger A, Pinkhas J. The history of colchicine. Korot. 1980;7:760-763.
6. Ahern MJ, Reid C, Gordon TP, McCredie M, Brooks PM, Jones M. Does colchicine work? The results of the first controlled study in acute gout. ANZ J Med. 1987;17:301-304.
7. Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320-326.
8. Rubin BR, Burton R, Navarra S, et al. Efficacy and safety profile of treatment with etoricoxib 120 mg once daily compared with indomethacin 50 mg three times daily in acute gout: a randomized controlled trial. Arthritis Rheum. 2004;50:598-606.
9. Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf. 2004;27:411-420.
10. Antman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115:1634-1642.
11. Petersel D, Schlesinger N. Treatment of acute gout in hospitalized patients. J Rheumatol. 2007;34:1566-1568.
12. Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498-501.
13. Krishnan E, Svendsen K, Neaton JD, Grandits G, Kuller LH. MRFIT Research Group. Long-term cardiovascular mortality among middle-aged men with gout. Arch Intern Med. 2008;168:1104-1110.
14. Davis M, Williams R, Chakraborty J, et al. Prednisone or prednisolone for the treatment of chronic active hepatitis? A comparison of plasma availability. Br J Clin Pharmacol. 1978;5:501-505.
15. Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23:285-295.
16. Gotzsche PC, Johansen HK. Short-term low-dose corticosteroids vs placebo and nonsteroidal antiinflammatory drugs in rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD000189.-
17. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002308.-
18. Alloway JA, Moriarty MJ, Hoogland YT, Nashel DJ. Comparison of triamcinolone acetonide with indomethacin in the treatment of acute gouty arthritis. J Rheumatol. 1993;20:111-113.
19. Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and triamcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol. 1994;21:1325-1327.
1. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860.
2. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
3. Sutaria S, Katbamna R, Underwood M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout—a systematic review. Rheumatology. 2006;45:1422-1431.
4. Janssens HJ, Lucassen PL, Van de Laar FA, Janssen M, Van de Lisdonk EH. Systemic corticosteroids for acute gout. Cochrane Database Syst Rev. 2008;(2):CD005521.-
5. Weinberger A, Pinkhas J. The history of colchicine. Korot. 1980;7:760-763.
6. Ahern MJ, Reid C, Gordon TP, McCredie M, Brooks PM, Jones M. Does colchicine work? The results of the first controlled study in acute gout. ANZ J Med. 1987;17:301-304.
7. Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320-326.
8. Rubin BR, Burton R, Navarra S, et al. Efficacy and safety profile of treatment with etoricoxib 120 mg once daily compared with indomethacin 50 mg three times daily in acute gout: a randomized controlled trial. Arthritis Rheum. 2004;50:598-606.
9. Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf. 2004;27:411-420.
10. Antman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115:1634-1642.
11. Petersel D, Schlesinger N. Treatment of acute gout in hospitalized patients. J Rheumatol. 2007;34:1566-1568.
12. Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498-501.
13. Krishnan E, Svendsen K, Neaton JD, Grandits G, Kuller LH. MRFIT Research Group. Long-term cardiovascular mortality among middle-aged men with gout. Arch Intern Med. 2008;168:1104-1110.
14. Davis M, Williams R, Chakraborty J, et al. Prednisone or prednisolone for the treatment of chronic active hepatitis? A comparison of plasma availability. Br J Clin Pharmacol. 1978;5:501-505.
15. Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23:285-295.
16. Gotzsche PC, Johansen HK. Short-term low-dose corticosteroids vs placebo and nonsteroidal antiinflammatory drugs in rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD000189.-
17. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002308.-
18. Alloway JA, Moriarty MJ, Hoogland YT, Nashel DJ. Comparison of triamcinolone acetonide with indomethacin in the treatment of acute gouty arthritis. J Rheumatol. 1993;20:111-113.
19. Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and triamcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol. 1994;21:1325-1327.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.