Therese Borden is the editor of CHEST Physician. After 20 years of research, writing, and editing in the field of international development and economics, she began working in the field of medical editing and has held a variety of editorial positions with the company. She holds a PhD in International Economics from American University, Washington, and a BA in history from the University of Washington, Seattle.
News

Sleepless in the pandemic
Overexposure to media COVID-19 content may contribute to emotional distress and sleeplessness.
News
‘Collateral damage’: COVID-19 threatens patients with COPD
Patients presenting at the ED with acute exacerbations of COPD could experience diagnostic and treatment delays.

News
Second U.S. coronavirus patient confirmed
A Chicago resident returning from Wuhan, China, on Jan. 13, 2020, developed symptoms of the disease and contacted her health care provider.
News
Two new cases of coronavirus pneumonia in Thailand, Japan
The new cases of 2019-nCoV were identified in travelers from the affected province in China.
News
Mystery pneumonia in China has health officials on alert
There are no reports of person-to-person transmission or health care worker infection of this pneumonia.
News
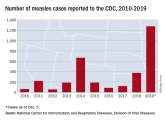
The measles comeback of 2019
Three-quarters of these cases in 2019 were linked to recent outbreaks in New York.

News
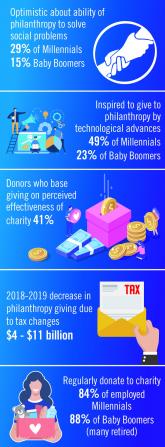
Environmental Scan: Drivers of philanthropy
Charitable giving, foundation support, and grants touch the lives of millions of patients and have an impact across all fields of practice of...
News

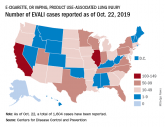
Vaping-linked lung injury: 2,172 cases, 42 deaths
Forty-two deaths from EVALI have been confirmed in 24 states and the District of Columbia.
News
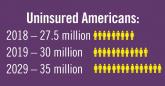
Environmental Scan: Drivers of social, political and environmental change
Spiraling costs of medical care, consumer activism around health care delivery, an aging population, and growing evidence of climate change are...
News

CDC identifies probable culprit in vaping lung injuries
In addition, obtaining vaping devices from informal sources, such as from a dealer, off the street, or from a friend, was more likely to be linked...
News
Vaping-linked lung injury cases near 1,900
Thirty-seven deaths from vaping-associated lung injuries have been reported in 24 states and the District of Columbia.