User login
How is Acute Pericarditis Diagnosed and Treated?
Case
A 32-year-old female with no significant past medical history is evaluated for sharp, left-sided chest pain for five days. Her pain is intermittent, worse with deep inspiration and in the supine position. She denies any shortness of breath. Her temperature is 100.8ºF, but otherwise her vital signs are normal. The physical exam and chest radiograph are unremarkable, but an electrocardiogram shows diffuse ST-segment elevations. The initial troponin is mildly elevated at 0.35 ng/ml.
Could this patient have acute pericarditis? If so, how should she be managed?
Background
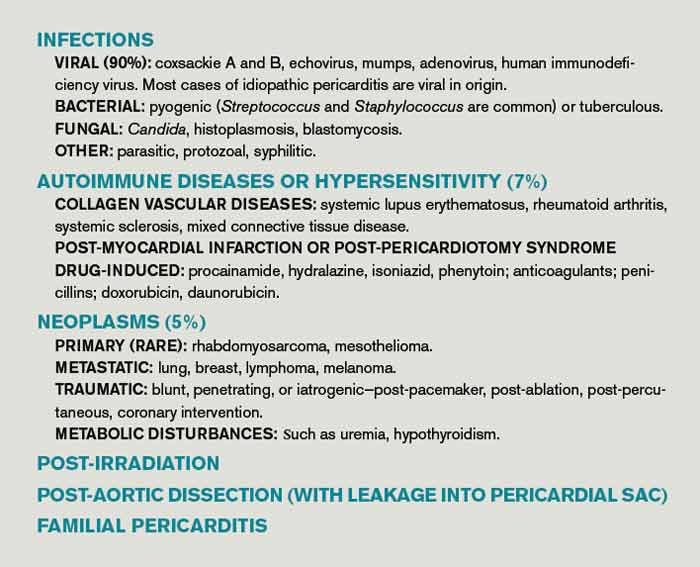
Pericarditis is the most common pericardial disease encountered by hospitalists. As many as 5% of chest pain cases unattributable to myocardial infarction (MI) are diagnosed with pericarditis.1 In immunocompetent individuals, as many as 90% of acute pericarditis cases are viral or idiopathic in etiology.1,2 Human immunodeficiency virus (HIV) and tuberculosis are common culprits in developing countries and immunocompromised hosts.3 Other specific etiologies of acute pericarditis include autoimmune diseases, neoplasms, chest irradiation, trauma, and metabolic disturbances (e.g. uremia). An etiologic classification of acute pericarditis is shown in Table 2 (p. 16).
Pericarditis primarily is a clinical diagnosis. Most patients present with chest pain.4 A pericardial friction rub may or may not be heard (sensitivity 16% to 85%), but when present is nearly 100% specific for pericarditis.2,5 Diffuse ST-segment elevation on electrocardiogram (EKG) is present in 60% to 90% of cases, but it can be difficult to differentiate from ST-segment elevations in acute MI.4,6
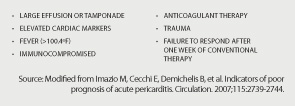
Uncomplicated acute pericarditis often is treated successfully as an outpatient.4 However, patients with high-risk features (see Table 1, right) should be hospitalized for identification and treatment of specific underlying etiology and for monitoring of complications, such as tamponade.7
Our patient has features consistent with pericarditis. In the following sections, we will review the diagnosis and treatment of acute pericarditis.
Review of the Data
How is acute pericarditis diagnosed?
Acute pericarditis is a clinical diagnosis supported by EKG and echocardiogram. At least two of the following four criteria must be present for the diagnosis: pleuritic chest pain, pericardial rub, diffuse ST-segment elevation on EKG, and pericardial effusion.8
History. Patients may report fever (46% in one small study of 69 patients) or a recent history of respiratory or gastrointestinal infection (40%).5 Most patients will report pleuritic chest pain. Typically, the pain is improved when sitting up and leaning forward, and gets worse when lying supine.4 Pain might radiate to the trapezius muscle ridge due to the common phrenic nerve innervation of pericardium and trapezius.9 However, pain might be minimal or absent in patients with uremic, neoplastic, tuberculous, or post-irradiation pericarditis.
Physical exam. A pericardial friction rub is nearly 100% specific for a pericarditis diagnosis, but sensitivity can vary (16% to 85%) depending on the frequency of auscultation and underlying etiology.2,5 It is thought to be caused by friction between the parietal and visceral layers of inflamed pericardium. A pericardial rub classically is described as a superficial, high-pitched, scratchy, or squeaking sound best heard with the diaphragm of the stethoscope at the lower left sternal border with the patient leaning forward.
Laboratory data. A complete blood count, metabolic panel, and cardiac enzymes should be checked in all patients with suspected acute pericarditis. Troponin values are elevated in up to one-third of patients, indicating cardiac muscle injury or myopericarditis, but have not been shown to adversely impact hospital length of stay, readmission, or complication rates.5,10 Markers of inflammation (e.g. erythrocyte sedimentation rate or C-reactive protein) are frequently elevated but do not point to a specific underlying etiology. Routine viral cultures and antibody titers are not useful.11
Most cases of pericarditis are presumed idiopathic (viral); however, finding a specific etiology should be considered in patients who do not respond after one week of therapy. Anti-nuclear antibody, complement levels, and rheumatoid factor can serve as screening tests for autoimmune disease. Purified protein derivative or quantiferon testing and HIV testing might be indicated in patients with appropriate risk factors. In cases of suspected tuberculous or neoplastic pericarditis, pericardial fluid analysis and biopsy could be warranted.
Electrocardiography. The EKG is the most useful test in diagnosing acute pericarditis. EKG changes in acute pericarditis can progress over four stages:
- Stage 1: diffuse ST elevations with or without PR depressions, initially;
- Stage 2: normalization of ST and PR segments, typically after several days;
- Stage 3: diffuse T-wave inversions; and
- Stage 4: normalization of T-waves, typically after weeks or months.
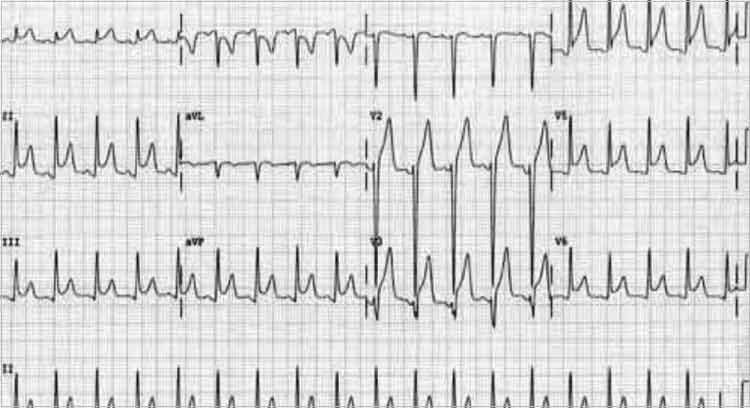
While all four stages are unlikely to be present in a given case, 80% of patients with pericarditis will demonstrate diffuse ST-segment elevations and PR-segment depression (see Figure 2, above).12
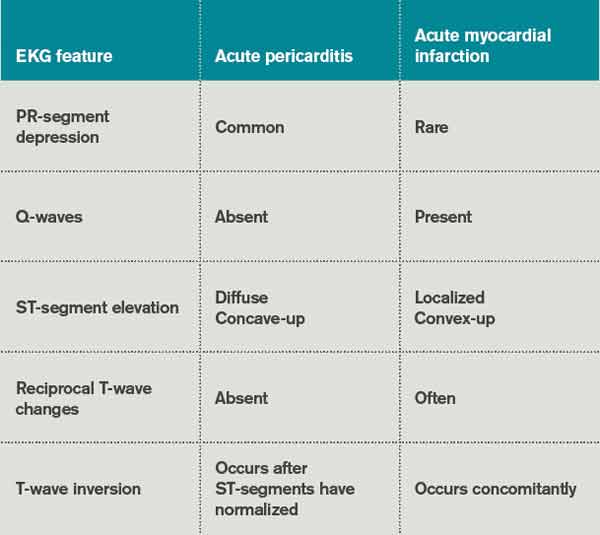
Table 3 lists EKG features helpful in differentiating acute pericarditis from acute myocardial infarction.
Chest radiography. Because a pericardial effusion often accompanies pericarditis, a chest radiograph (CXR) should be performed in all suspected cases. The CXR might show enlargement of the cardiac silhouette if more than 250 ml of pericardial fluid is present.3 A CXR also is helpful to diagnose concomitant pulmonary infection, pleural effusion, or mediastinal mass—all findings that could point to an underlying specific etiology of pericarditis and/or pericardial effusion.
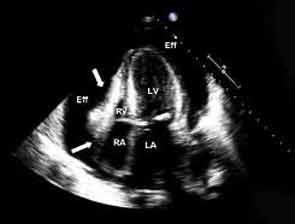
Echocardiography. An echocardiogram should be performed in all patients with suspected pericarditis to detect effusion, associated myocardial, or paracardial disease.13 The echocardiogram frequently is normal but could show an effusion in 60%, and tamponade (see Figure 1, p. 15) in 5%, of cases.4
Computed tomography (CT) and cardiac magnetic resonance imaging (CMR).CT or CMR are the imaging modalities of choice when an echocardiogram is inconclusive or in cases of pericarditis complicated by a hemorrhagic or localized effusion, pericardial thickening, or pericardial mass.14 They also help in precise imaging of neighboring structures, such as lungs or mediastinum.
Pericardial fluid analysis and pericardial biopsy. In cases of refractory pericarditis with effusion, pericardial fluid analysis might provide clues to the underlying etiology. Routine chemistry, cell count, gram and acid fast staining, culture, and cytology should be sent. In addition, acid-fast bacillus staining and culture, adenosine deaminase, and interferon-gamma testing should be ordered when tuberculous pericarditis is suspected. A pericardial biopsy may show granulomas or neoplastic cells. Overall, pericardial fluid analysis and biopsy reveal a diagnosis in roughly 20% of cases.11
How is acute pericarditis treated?
Most cases of uncomplicated acute pericarditis are viral and respond well to NSAID plus colchicine therapy.2,4 Failure to respond to NSAIDs plus colchicine—evidenced by persistent fever, pericardial chest pain, new pericardial effusion, or worsening of general illness—within a week of treatment should prompt a search for an underlying systemic illness. If found, treatment should be aimed at the causative illness.
Bacterial pericarditis usually requires surgical drainage in addition to treatment with appropriate antibiotics.11 Tuberculous pericarditis is treated with multidrug therapy; when underlying HIV is present, patients should receive highly active anti-retroviral therapy as well. Steroids and immunosuppressants should be considered in addition to NSAIDs and colchicine in autoimmune pericarditis.10 Neoplastic pericarditis may resolve with chemotherapy but it has a high recurrence rate.13 Uremic pericarditis requires intensified dialysis.
Treatment options for uncomplicated idiopathic or viral pericarditis include:
NSAIDs. It is important to adequately dose NSAIDs when treating acute pericarditis. Initial treatment options include ibuprofen (1,600 to 3,200 mg daily), indomethacin (75 to 150 mg daily) or aspirin (2 to 4 gm daily) for one week.11,15 Aspirin is preferred in patients with ischemic heart disease. For patients with symptoms that persist longer than a week, NSAIDS may be continued, but investigation for an underlying etiology is indicated. Concomitant proton-pump-inhibitor therapy should be considered in patients at high risk for peptic ulcer disease to minimize gastric side effects.
Colchicine. Colchicine has a favorable risk-benefit profile as an adjunct treatment for acute and recurrent pericarditis. Patients experience better symptom relief when treated with both colchicine and an NSAID, compared with NSAIDs alone (88% versus 63%). Recurrence rates are lower with combined therapy (11% versus 32%).16 Colchicine treatment (0.6 mg twice daily after a loading dose of up to 2 mg) is recommended for several months to greater than one year.13,16,17
Glucocorticoids. Routine glucocorticoid use should be avoided in the treatment of acute pericarditis, as it has been associated with an increased risk for recurrence (OR 4.3).16,18 Glucocorticoid use should be considered in cases of pericarditis refractory to NSAIDs and colchicine, cases in which NSAIDs and or colchicine are contraindicated, and in autoimmune or connective-tissue-disease-related pericarditis. Prednisone should be dosed up to 1 mg/kg/day for at least one month, depending on symptom resolution, then tapered after either NSAIDs or colchicine have been started.13 Smaller prednisone doses of up to 0.5 mg/kg/day could be as effective, with the added benefit of reduced side effects and recurrences.19
Invasive treatment. Pericardiocentesis and/or pericardiectomy should be considered when pericarditis is complicated by a large effusion or tamponade, constrictive physiology, or recurrent effusion.11 Pericardiocentesis is the least invasive option and helps provide immediate relief in cases of tamponade or large symptomatic effusions. It is the preferred modality for obtaining pericardial fluid for diagnostic analysis. However, effusions can recur and in those cases pericardial window is preferred, as it provides continued outflow of pericardial fluid. Pericardiectomy is recommended in cases of symptomatic constrictive pericarditis unresponsive to medical therapy.15
Back to the Case
The patient’s presentation—prodrome followed by fever and pleuritic chest pain—is characteristic of acute idiopathic pericarditis. No pericardial rub was heard, but EKG findings were typical. Troponin I elevation suggested underlying myopericarditis. An echocardiogram was unremarkable. Given the likely viral or idiopathic etiology, no further diagnostic tests were ordered to explore the possibility of an underlying systemic illness.
The patient was started on ibuprofen 600 mg every eight hours. She had significant relief of her symptoms within two days. A routine fever workup was negative. She was discharged the following day.
The patient was readmitted three months later with recurrent pleuritic chest pain, which did not improve with resumption of NSAID therapy. Initial troponin I was 0.22 ng/ml, electrocardiogram was unchanged, and an echocardiogram showed small effusion. She was started on ibuprofen 800 mg every eight hours, as well as colchicine 0.6 mg twice daily. Her symptoms resolved the next day and she was discharged with prescriptions for ibuprofen and colchicine. She was instructed to follow up with a primary-care doctor in one week.
At the clinic visit, ibuprofen was tapered but colchicine was continued for another six months. She remained asymptomatic at her six-month clinic follow-up.
Bottom Line
Acute pericarditis is a clinical diagnosis supported by EKG findings. Most cases are idiopathic or viral, and can be treated successfully with NSAIDs and colchicine. For cases that do not respond to initial therapy, or cases that present with high-risk features, a specific etiology should be sought.
Dr. Southern is chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y. Dr. Galhorta is an instructor and Drs. Martin, Korcak, and Stehlihova are assistant professors in the department of medicine at Albert Einstein.
References
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
- Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
- Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:717-727.
- Imazio M, Demichelis B, Parrini I, et al. Day-hospital treatment of acute pericarditis: a management program for outpatient therapy. J Am Coll Cardiol. 2004;43:1042-1046.
- Bonnefoy E, Godon P, Kirkorian G, et al. Serum cardiac troponin I and ST-segment elevation in patients with acute pericarditis. Eur Heart J. 2000;21:832-836.
- Salisbury AC, Olalla-Gomez C, Rihal CS, et al. Frequency and predictors of urgent coronary angiography in patients with acute pericarditis. Mayo Clin Proc. 2009;84(1):11-15.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744.
- Imazio M, Spodick DH, Brucato A, et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010;64(10):1384-1392.
- Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
- Imazio M, Demichelis B, Cecchi E. Cardiac troponin I in acute pericarditis. J Am Coll Cardiol. 2003;42(12):2144-2148.
- Sagristà Sauleda J, Permanyer Miralda G, Soler Soler J. Diagnosis and management of pericardial syndromes. Rev Esp Cardiol. 2005;58(7):830-841.
- Bruce MA, Spodick DH. Atypical electrocardiogram in acute pericarditis: characteristics and prevalence. J Electrocardiol. 1980;13:61-66.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J. 2004; 25(7):587-610.
- Verhaert D, Gabriel RS, Johnston D, et al. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333-343.
- Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the colchicine for acute pericarditis (COPE) trial. Circulation. 2005;112(13):2012-2016.
- Adler Y, Finkelstein Y, Guindo J, et al. Colchicine treatment for recurrent pericarditis: a decade of experience. Circulation. 1998;97:2183-185.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the colchicine for recurrent pericarditis (CORE) trial. Arch Intern Med. 2005;165:1987-1991.
- Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118:667-771.
Case
A 32-year-old female with no significant past medical history is evaluated for sharp, left-sided chest pain for five days. Her pain is intermittent, worse with deep inspiration and in the supine position. She denies any shortness of breath. Her temperature is 100.8ºF, but otherwise her vital signs are normal. The physical exam and chest radiograph are unremarkable, but an electrocardiogram shows diffuse ST-segment elevations. The initial troponin is mildly elevated at 0.35 ng/ml.
Could this patient have acute pericarditis? If so, how should she be managed?
Background
Pericarditis is the most common pericardial disease encountered by hospitalists. As many as 5% of chest pain cases unattributable to myocardial infarction (MI) are diagnosed with pericarditis.1 In immunocompetent individuals, as many as 90% of acute pericarditis cases are viral or idiopathic in etiology.1,2 Human immunodeficiency virus (HIV) and tuberculosis are common culprits in developing countries and immunocompromised hosts.3 Other specific etiologies of acute pericarditis include autoimmune diseases, neoplasms, chest irradiation, trauma, and metabolic disturbances (e.g. uremia). An etiologic classification of acute pericarditis is shown in Table 2 (p. 16).
Pericarditis primarily is a clinical diagnosis. Most patients present with chest pain.4 A pericardial friction rub may or may not be heard (sensitivity 16% to 85%), but when present is nearly 100% specific for pericarditis.2,5 Diffuse ST-segment elevation on electrocardiogram (EKG) is present in 60% to 90% of cases, but it can be difficult to differentiate from ST-segment elevations in acute MI.4,6
Uncomplicated acute pericarditis often is treated successfully as an outpatient.4 However, patients with high-risk features (see Table 1, right) should be hospitalized for identification and treatment of specific underlying etiology and for monitoring of complications, such as tamponade.7
Our patient has features consistent with pericarditis. In the following sections, we will review the diagnosis and treatment of acute pericarditis.
Review of the Data
How is acute pericarditis diagnosed?
Acute pericarditis is a clinical diagnosis supported by EKG and echocardiogram. At least two of the following four criteria must be present for the diagnosis: pleuritic chest pain, pericardial rub, diffuse ST-segment elevation on EKG, and pericardial effusion.8
History. Patients may report fever (46% in one small study of 69 patients) or a recent history of respiratory or gastrointestinal infection (40%).5 Most patients will report pleuritic chest pain. Typically, the pain is improved when sitting up and leaning forward, and gets worse when lying supine.4 Pain might radiate to the trapezius muscle ridge due to the common phrenic nerve innervation of pericardium and trapezius.9 However, pain might be minimal or absent in patients with uremic, neoplastic, tuberculous, or post-irradiation pericarditis.
Physical exam. A pericardial friction rub is nearly 100% specific for a pericarditis diagnosis, but sensitivity can vary (16% to 85%) depending on the frequency of auscultation and underlying etiology.2,5 It is thought to be caused by friction between the parietal and visceral layers of inflamed pericardium. A pericardial rub classically is described as a superficial, high-pitched, scratchy, or squeaking sound best heard with the diaphragm of the stethoscope at the lower left sternal border with the patient leaning forward.
Laboratory data. A complete blood count, metabolic panel, and cardiac enzymes should be checked in all patients with suspected acute pericarditis. Troponin values are elevated in up to one-third of patients, indicating cardiac muscle injury or myopericarditis, but have not been shown to adversely impact hospital length of stay, readmission, or complication rates.5,10 Markers of inflammation (e.g. erythrocyte sedimentation rate or C-reactive protein) are frequently elevated but do not point to a specific underlying etiology. Routine viral cultures and antibody titers are not useful.11
Most cases of pericarditis are presumed idiopathic (viral); however, finding a specific etiology should be considered in patients who do not respond after one week of therapy. Anti-nuclear antibody, complement levels, and rheumatoid factor can serve as screening tests for autoimmune disease. Purified protein derivative or quantiferon testing and HIV testing might be indicated in patients with appropriate risk factors. In cases of suspected tuberculous or neoplastic pericarditis, pericardial fluid analysis and biopsy could be warranted.
Electrocardiography. The EKG is the most useful test in diagnosing acute pericarditis. EKG changes in acute pericarditis can progress over four stages:
- Stage 1: diffuse ST elevations with or without PR depressions, initially;
- Stage 2: normalization of ST and PR segments, typically after several days;
- Stage 3: diffuse T-wave inversions; and
- Stage 4: normalization of T-waves, typically after weeks or months.
While all four stages are unlikely to be present in a given case, 80% of patients with pericarditis will demonstrate diffuse ST-segment elevations and PR-segment depression (see Figure 2, above).12
Table 3 lists EKG features helpful in differentiating acute pericarditis from acute myocardial infarction.
Chest radiography. Because a pericardial effusion often accompanies pericarditis, a chest radiograph (CXR) should be performed in all suspected cases. The CXR might show enlargement of the cardiac silhouette if more than 250 ml of pericardial fluid is present.3 A CXR also is helpful to diagnose concomitant pulmonary infection, pleural effusion, or mediastinal mass—all findings that could point to an underlying specific etiology of pericarditis and/or pericardial effusion.
Echocardiography. An echocardiogram should be performed in all patients with suspected pericarditis to detect effusion, associated myocardial, or paracardial disease.13 The echocardiogram frequently is normal but could show an effusion in 60%, and tamponade (see Figure 1, p. 15) in 5%, of cases.4
Computed tomography (CT) and cardiac magnetic resonance imaging (CMR).CT or CMR are the imaging modalities of choice when an echocardiogram is inconclusive or in cases of pericarditis complicated by a hemorrhagic or localized effusion, pericardial thickening, or pericardial mass.14 They also help in precise imaging of neighboring structures, such as lungs or mediastinum.
Pericardial fluid analysis and pericardial biopsy. In cases of refractory pericarditis with effusion, pericardial fluid analysis might provide clues to the underlying etiology. Routine chemistry, cell count, gram and acid fast staining, culture, and cytology should be sent. In addition, acid-fast bacillus staining and culture, adenosine deaminase, and interferon-gamma testing should be ordered when tuberculous pericarditis is suspected. A pericardial biopsy may show granulomas or neoplastic cells. Overall, pericardial fluid analysis and biopsy reveal a diagnosis in roughly 20% of cases.11
How is acute pericarditis treated?
Most cases of uncomplicated acute pericarditis are viral and respond well to NSAID plus colchicine therapy.2,4 Failure to respond to NSAIDs plus colchicine—evidenced by persistent fever, pericardial chest pain, new pericardial effusion, or worsening of general illness—within a week of treatment should prompt a search for an underlying systemic illness. If found, treatment should be aimed at the causative illness.
Bacterial pericarditis usually requires surgical drainage in addition to treatment with appropriate antibiotics.11 Tuberculous pericarditis is treated with multidrug therapy; when underlying HIV is present, patients should receive highly active anti-retroviral therapy as well. Steroids and immunosuppressants should be considered in addition to NSAIDs and colchicine in autoimmune pericarditis.10 Neoplastic pericarditis may resolve with chemotherapy but it has a high recurrence rate.13 Uremic pericarditis requires intensified dialysis.
Treatment options for uncomplicated idiopathic or viral pericarditis include:
NSAIDs. It is important to adequately dose NSAIDs when treating acute pericarditis. Initial treatment options include ibuprofen (1,600 to 3,200 mg daily), indomethacin (75 to 150 mg daily) or aspirin (2 to 4 gm daily) for one week.11,15 Aspirin is preferred in patients with ischemic heart disease. For patients with symptoms that persist longer than a week, NSAIDS may be continued, but investigation for an underlying etiology is indicated. Concomitant proton-pump-inhibitor therapy should be considered in patients at high risk for peptic ulcer disease to minimize gastric side effects.
Colchicine. Colchicine has a favorable risk-benefit profile as an adjunct treatment for acute and recurrent pericarditis. Patients experience better symptom relief when treated with both colchicine and an NSAID, compared with NSAIDs alone (88% versus 63%). Recurrence rates are lower with combined therapy (11% versus 32%).16 Colchicine treatment (0.6 mg twice daily after a loading dose of up to 2 mg) is recommended for several months to greater than one year.13,16,17
Glucocorticoids. Routine glucocorticoid use should be avoided in the treatment of acute pericarditis, as it has been associated with an increased risk for recurrence (OR 4.3).16,18 Glucocorticoid use should be considered in cases of pericarditis refractory to NSAIDs and colchicine, cases in which NSAIDs and or colchicine are contraindicated, and in autoimmune or connective-tissue-disease-related pericarditis. Prednisone should be dosed up to 1 mg/kg/day for at least one month, depending on symptom resolution, then tapered after either NSAIDs or colchicine have been started.13 Smaller prednisone doses of up to 0.5 mg/kg/day could be as effective, with the added benefit of reduced side effects and recurrences.19
Invasive treatment. Pericardiocentesis and/or pericardiectomy should be considered when pericarditis is complicated by a large effusion or tamponade, constrictive physiology, or recurrent effusion.11 Pericardiocentesis is the least invasive option and helps provide immediate relief in cases of tamponade or large symptomatic effusions. It is the preferred modality for obtaining pericardial fluid for diagnostic analysis. However, effusions can recur and in those cases pericardial window is preferred, as it provides continued outflow of pericardial fluid. Pericardiectomy is recommended in cases of symptomatic constrictive pericarditis unresponsive to medical therapy.15
Back to the Case
The patient’s presentation—prodrome followed by fever and pleuritic chest pain—is characteristic of acute idiopathic pericarditis. No pericardial rub was heard, but EKG findings were typical. Troponin I elevation suggested underlying myopericarditis. An echocardiogram was unremarkable. Given the likely viral or idiopathic etiology, no further diagnostic tests were ordered to explore the possibility of an underlying systemic illness.
The patient was started on ibuprofen 600 mg every eight hours. She had significant relief of her symptoms within two days. A routine fever workup was negative. She was discharged the following day.
The patient was readmitted three months later with recurrent pleuritic chest pain, which did not improve with resumption of NSAID therapy. Initial troponin I was 0.22 ng/ml, electrocardiogram was unchanged, and an echocardiogram showed small effusion. She was started on ibuprofen 800 mg every eight hours, as well as colchicine 0.6 mg twice daily. Her symptoms resolved the next day and she was discharged with prescriptions for ibuprofen and colchicine. She was instructed to follow up with a primary-care doctor in one week.
At the clinic visit, ibuprofen was tapered but colchicine was continued for another six months. She remained asymptomatic at her six-month clinic follow-up.
Bottom Line
Acute pericarditis is a clinical diagnosis supported by EKG findings. Most cases are idiopathic or viral, and can be treated successfully with NSAIDs and colchicine. For cases that do not respond to initial therapy, or cases that present with high-risk features, a specific etiology should be sought.
Dr. Southern is chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y. Dr. Galhorta is an instructor and Drs. Martin, Korcak, and Stehlihova are assistant professors in the department of medicine at Albert Einstein.
References
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
- Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
- Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:717-727.
- Imazio M, Demichelis B, Parrini I, et al. Day-hospital treatment of acute pericarditis: a management program for outpatient therapy. J Am Coll Cardiol. 2004;43:1042-1046.
- Bonnefoy E, Godon P, Kirkorian G, et al. Serum cardiac troponin I and ST-segment elevation in patients with acute pericarditis. Eur Heart J. 2000;21:832-836.
- Salisbury AC, Olalla-Gomez C, Rihal CS, et al. Frequency and predictors of urgent coronary angiography in patients with acute pericarditis. Mayo Clin Proc. 2009;84(1):11-15.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744.
- Imazio M, Spodick DH, Brucato A, et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010;64(10):1384-1392.
- Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
- Imazio M, Demichelis B, Cecchi E. Cardiac troponin I in acute pericarditis. J Am Coll Cardiol. 2003;42(12):2144-2148.
- Sagristà Sauleda J, Permanyer Miralda G, Soler Soler J. Diagnosis and management of pericardial syndromes. Rev Esp Cardiol. 2005;58(7):830-841.
- Bruce MA, Spodick DH. Atypical electrocardiogram in acute pericarditis: characteristics and prevalence. J Electrocardiol. 1980;13:61-66.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J. 2004; 25(7):587-610.
- Verhaert D, Gabriel RS, Johnston D, et al. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333-343.
- Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the colchicine for acute pericarditis (COPE) trial. Circulation. 2005;112(13):2012-2016.
- Adler Y, Finkelstein Y, Guindo J, et al. Colchicine treatment for recurrent pericarditis: a decade of experience. Circulation. 1998;97:2183-185.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the colchicine for recurrent pericarditis (CORE) trial. Arch Intern Med. 2005;165:1987-1991.
- Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118:667-771.
Case
A 32-year-old female with no significant past medical history is evaluated for sharp, left-sided chest pain for five days. Her pain is intermittent, worse with deep inspiration and in the supine position. She denies any shortness of breath. Her temperature is 100.8ºF, but otherwise her vital signs are normal. The physical exam and chest radiograph are unremarkable, but an electrocardiogram shows diffuse ST-segment elevations. The initial troponin is mildly elevated at 0.35 ng/ml.
Could this patient have acute pericarditis? If so, how should she be managed?
Background
Pericarditis is the most common pericardial disease encountered by hospitalists. As many as 5% of chest pain cases unattributable to myocardial infarction (MI) are diagnosed with pericarditis.1 In immunocompetent individuals, as many as 90% of acute pericarditis cases are viral or idiopathic in etiology.1,2 Human immunodeficiency virus (HIV) and tuberculosis are common culprits in developing countries and immunocompromised hosts.3 Other specific etiologies of acute pericarditis include autoimmune diseases, neoplasms, chest irradiation, trauma, and metabolic disturbances (e.g. uremia). An etiologic classification of acute pericarditis is shown in Table 2 (p. 16).
Pericarditis primarily is a clinical diagnosis. Most patients present with chest pain.4 A pericardial friction rub may or may not be heard (sensitivity 16% to 85%), but when present is nearly 100% specific for pericarditis.2,5 Diffuse ST-segment elevation on electrocardiogram (EKG) is present in 60% to 90% of cases, but it can be difficult to differentiate from ST-segment elevations in acute MI.4,6
Uncomplicated acute pericarditis often is treated successfully as an outpatient.4 However, patients with high-risk features (see Table 1, right) should be hospitalized for identification and treatment of specific underlying etiology and for monitoring of complications, such as tamponade.7
Our patient has features consistent with pericarditis. In the following sections, we will review the diagnosis and treatment of acute pericarditis.
Review of the Data
How is acute pericarditis diagnosed?
Acute pericarditis is a clinical diagnosis supported by EKG and echocardiogram. At least two of the following four criteria must be present for the diagnosis: pleuritic chest pain, pericardial rub, diffuse ST-segment elevation on EKG, and pericardial effusion.8
History. Patients may report fever (46% in one small study of 69 patients) or a recent history of respiratory or gastrointestinal infection (40%).5 Most patients will report pleuritic chest pain. Typically, the pain is improved when sitting up and leaning forward, and gets worse when lying supine.4 Pain might radiate to the trapezius muscle ridge due to the common phrenic nerve innervation of pericardium and trapezius.9 However, pain might be minimal or absent in patients with uremic, neoplastic, tuberculous, or post-irradiation pericarditis.
Physical exam. A pericardial friction rub is nearly 100% specific for a pericarditis diagnosis, but sensitivity can vary (16% to 85%) depending on the frequency of auscultation and underlying etiology.2,5 It is thought to be caused by friction between the parietal and visceral layers of inflamed pericardium. A pericardial rub classically is described as a superficial, high-pitched, scratchy, or squeaking sound best heard with the diaphragm of the stethoscope at the lower left sternal border with the patient leaning forward.
Laboratory data. A complete blood count, metabolic panel, and cardiac enzymes should be checked in all patients with suspected acute pericarditis. Troponin values are elevated in up to one-third of patients, indicating cardiac muscle injury or myopericarditis, but have not been shown to adversely impact hospital length of stay, readmission, or complication rates.5,10 Markers of inflammation (e.g. erythrocyte sedimentation rate or C-reactive protein) are frequently elevated but do not point to a specific underlying etiology. Routine viral cultures and antibody titers are not useful.11
Most cases of pericarditis are presumed idiopathic (viral); however, finding a specific etiology should be considered in patients who do not respond after one week of therapy. Anti-nuclear antibody, complement levels, and rheumatoid factor can serve as screening tests for autoimmune disease. Purified protein derivative or quantiferon testing and HIV testing might be indicated in patients with appropriate risk factors. In cases of suspected tuberculous or neoplastic pericarditis, pericardial fluid analysis and biopsy could be warranted.
Electrocardiography. The EKG is the most useful test in diagnosing acute pericarditis. EKG changes in acute pericarditis can progress over four stages:
- Stage 1: diffuse ST elevations with or without PR depressions, initially;
- Stage 2: normalization of ST and PR segments, typically after several days;
- Stage 3: diffuse T-wave inversions; and
- Stage 4: normalization of T-waves, typically after weeks or months.
While all four stages are unlikely to be present in a given case, 80% of patients with pericarditis will demonstrate diffuse ST-segment elevations and PR-segment depression (see Figure 2, above).12
Table 3 lists EKG features helpful in differentiating acute pericarditis from acute myocardial infarction.
Chest radiography. Because a pericardial effusion often accompanies pericarditis, a chest radiograph (CXR) should be performed in all suspected cases. The CXR might show enlargement of the cardiac silhouette if more than 250 ml of pericardial fluid is present.3 A CXR also is helpful to diagnose concomitant pulmonary infection, pleural effusion, or mediastinal mass—all findings that could point to an underlying specific etiology of pericarditis and/or pericardial effusion.
Echocardiography. An echocardiogram should be performed in all patients with suspected pericarditis to detect effusion, associated myocardial, or paracardial disease.13 The echocardiogram frequently is normal but could show an effusion in 60%, and tamponade (see Figure 1, p. 15) in 5%, of cases.4
Computed tomography (CT) and cardiac magnetic resonance imaging (CMR).CT or CMR are the imaging modalities of choice when an echocardiogram is inconclusive or in cases of pericarditis complicated by a hemorrhagic or localized effusion, pericardial thickening, or pericardial mass.14 They also help in precise imaging of neighboring structures, such as lungs or mediastinum.
Pericardial fluid analysis and pericardial biopsy. In cases of refractory pericarditis with effusion, pericardial fluid analysis might provide clues to the underlying etiology. Routine chemistry, cell count, gram and acid fast staining, culture, and cytology should be sent. In addition, acid-fast bacillus staining and culture, adenosine deaminase, and interferon-gamma testing should be ordered when tuberculous pericarditis is suspected. A pericardial biopsy may show granulomas or neoplastic cells. Overall, pericardial fluid analysis and biopsy reveal a diagnosis in roughly 20% of cases.11
How is acute pericarditis treated?
Most cases of uncomplicated acute pericarditis are viral and respond well to NSAID plus colchicine therapy.2,4 Failure to respond to NSAIDs plus colchicine—evidenced by persistent fever, pericardial chest pain, new pericardial effusion, or worsening of general illness—within a week of treatment should prompt a search for an underlying systemic illness. If found, treatment should be aimed at the causative illness.
Bacterial pericarditis usually requires surgical drainage in addition to treatment with appropriate antibiotics.11 Tuberculous pericarditis is treated with multidrug therapy; when underlying HIV is present, patients should receive highly active anti-retroviral therapy as well. Steroids and immunosuppressants should be considered in addition to NSAIDs and colchicine in autoimmune pericarditis.10 Neoplastic pericarditis may resolve with chemotherapy but it has a high recurrence rate.13 Uremic pericarditis requires intensified dialysis.
Treatment options for uncomplicated idiopathic or viral pericarditis include:
NSAIDs. It is important to adequately dose NSAIDs when treating acute pericarditis. Initial treatment options include ibuprofen (1,600 to 3,200 mg daily), indomethacin (75 to 150 mg daily) or aspirin (2 to 4 gm daily) for one week.11,15 Aspirin is preferred in patients with ischemic heart disease. For patients with symptoms that persist longer than a week, NSAIDS may be continued, but investigation for an underlying etiology is indicated. Concomitant proton-pump-inhibitor therapy should be considered in patients at high risk for peptic ulcer disease to minimize gastric side effects.
Colchicine. Colchicine has a favorable risk-benefit profile as an adjunct treatment for acute and recurrent pericarditis. Patients experience better symptom relief when treated with both colchicine and an NSAID, compared with NSAIDs alone (88% versus 63%). Recurrence rates are lower with combined therapy (11% versus 32%).16 Colchicine treatment (0.6 mg twice daily after a loading dose of up to 2 mg) is recommended for several months to greater than one year.13,16,17
Glucocorticoids. Routine glucocorticoid use should be avoided in the treatment of acute pericarditis, as it has been associated with an increased risk for recurrence (OR 4.3).16,18 Glucocorticoid use should be considered in cases of pericarditis refractory to NSAIDs and colchicine, cases in which NSAIDs and or colchicine are contraindicated, and in autoimmune or connective-tissue-disease-related pericarditis. Prednisone should be dosed up to 1 mg/kg/day for at least one month, depending on symptom resolution, then tapered after either NSAIDs or colchicine have been started.13 Smaller prednisone doses of up to 0.5 mg/kg/day could be as effective, with the added benefit of reduced side effects and recurrences.19
Invasive treatment. Pericardiocentesis and/or pericardiectomy should be considered when pericarditis is complicated by a large effusion or tamponade, constrictive physiology, or recurrent effusion.11 Pericardiocentesis is the least invasive option and helps provide immediate relief in cases of tamponade or large symptomatic effusions. It is the preferred modality for obtaining pericardial fluid for diagnostic analysis. However, effusions can recur and in those cases pericardial window is preferred, as it provides continued outflow of pericardial fluid. Pericardiectomy is recommended in cases of symptomatic constrictive pericarditis unresponsive to medical therapy.15
Back to the Case
The patient’s presentation—prodrome followed by fever and pleuritic chest pain—is characteristic of acute idiopathic pericarditis. No pericardial rub was heard, but EKG findings were typical. Troponin I elevation suggested underlying myopericarditis. An echocardiogram was unremarkable. Given the likely viral or idiopathic etiology, no further diagnostic tests were ordered to explore the possibility of an underlying systemic illness.
The patient was started on ibuprofen 600 mg every eight hours. She had significant relief of her symptoms within two days. A routine fever workup was negative. She was discharged the following day.
The patient was readmitted three months later with recurrent pleuritic chest pain, which did not improve with resumption of NSAID therapy. Initial troponin I was 0.22 ng/ml, electrocardiogram was unchanged, and an echocardiogram showed small effusion. She was started on ibuprofen 800 mg every eight hours, as well as colchicine 0.6 mg twice daily. Her symptoms resolved the next day and she was discharged with prescriptions for ibuprofen and colchicine. She was instructed to follow up with a primary-care doctor in one week.
At the clinic visit, ibuprofen was tapered but colchicine was continued for another six months. She remained asymptomatic at her six-month clinic follow-up.
Bottom Line
Acute pericarditis is a clinical diagnosis supported by EKG findings. Most cases are idiopathic or viral, and can be treated successfully with NSAIDs and colchicine. For cases that do not respond to initial therapy, or cases that present with high-risk features, a specific etiology should be sought.
Dr. Southern is chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y. Dr. Galhorta is an instructor and Drs. Martin, Korcak, and Stehlihova are assistant professors in the department of medicine at Albert Einstein.
References
- Lange RA, Hillis LD. Clinical practice. Acute pericarditis. N Engl J Med. 2004;351:2195-2202.
- Zayas R, Anguita M, Torres F, et al. Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis. Am J Cardiol. 1995;75:378-382.
- Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet. 2004;363:717-727.
- Imazio M, Demichelis B, Parrini I, et al. Day-hospital treatment of acute pericarditis: a management program for outpatient therapy. J Am Coll Cardiol. 2004;43:1042-1046.
- Bonnefoy E, Godon P, Kirkorian G, et al. Serum cardiac troponin I and ST-segment elevation in patients with acute pericarditis. Eur Heart J. 2000;21:832-836.
- Salisbury AC, Olalla-Gomez C, Rihal CS, et al. Frequency and predictors of urgent coronary angiography in patients with acute pericarditis. Mayo Clin Proc. 2009;84(1):11-15.
- Imazio M, Cecchi E, Demichelis B, et al. Indicators of poor prognosis of acute pericarditis. Circulation. 2007;115:2739-2744.
- Imazio M, Spodick DH, Brucato A, et al. Diagnostic issues in the clinical management of pericarditis. Int J Clin Pract. 2010;64(10):1384-1392.
- Spodick DH. Acute pericarditis: current concepts and practice. JAMA. 2003;289:1150-1153.
- Imazio M, Demichelis B, Cecchi E. Cardiac troponin I in acute pericarditis. J Am Coll Cardiol. 2003;42(12):2144-2148.
- Sagristà Sauleda J, Permanyer Miralda G, Soler Soler J. Diagnosis and management of pericardial syndromes. Rev Esp Cardiol. 2005;58(7):830-841.
- Bruce MA, Spodick DH. Atypical electrocardiogram in acute pericarditis: characteristics and prevalence. J Electrocardiol. 1980;13:61-66.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary; the task force on the diagnosis and management of pericardial diseases of the European Society of Cardiology. Eur Heart J. 2004; 25(7):587-610.
- Verhaert D, Gabriel RS, Johnston D, et al. The role of multimodality imaging in the management of pericardial disease. Circ Cardiovasc Imaging. 2010;3:333-343.
- Imazio M, Spodick DH, Brucato A, et al. Controversial issues in the management of pericardial diseases. Circulation. 2010;121:916-928.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine in addition to conventional therapy for acute pericarditis: results of the colchicine for acute pericarditis (COPE) trial. Circulation. 2005;112(13):2012-2016.
- Adler Y, Finkelstein Y, Guindo J, et al. Colchicine treatment for recurrent pericarditis: a decade of experience. Circulation. 1998;97:2183-185.
- Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the colchicine for recurrent pericarditis (CORE) trial. Arch Intern Med. 2005;165:1987-1991.
- Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation. 2008;118:667-771.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Nearly all CDIs Related to Exposure in Healthcare Setting
- In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
- Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
- Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
- Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
- Rivaroxaban for the Treatment of Acute Pulmonary Embolism
- Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
- Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Nearly all CDIs Related to Exposure in Healthcare Setting
Clinical question: What is the contribution of non-hospital healthcare exposures to the burden of Clostridium difficile infection (CDI)?
Background: CDI is common among hospitalized patients and is associated with high rates of morbidity. Most CDI prevention programs are aimed at hospital-based risk factors. However, non-hospital healthcare exposures might contribute significantly to the burden of CDI, and hospital-based prevention programs might not address these risks.
Study design: Retrospective analysis of three population-based data sets.
Setting: Three population data sets tracking infections on a national and state level in the U.S.
Synopsis: This study analyzed two data sets to determine the contribution of non-hospital healthcare exposure to CDIs, and examined a third to determine whether a program addressing hospital-based exposures reduced the rate of CDI.Using data from the CDC’s Emerging Infections Program, 10,342 CDI cases from 111 hospitals were examined. Each case was classified as hospital onset (i.e. occurring three days after admission), nursing home onset, or community onset. A total of 94% of cases were associated with recent exposure to healthcare, 75% were classified as non-hospital onset, and 20% of hospital-onset cases were in patients who had recently been in a nursing home, suggesting that non-hospital-based healthcare exposures play a significant role. The second analysis used data from the National Healthcare Safety Network to examine 42,157 CDIs in 711 hospitals.
The authors found that 52% of CDIs were present on admission. The pooled rate of hospital-onset CDI was low (7.4 per 10,000 patient-days). The final analysis examined hospital-onset CDI rates across three hospital-based prevention programs over a period of nearly two years. The interventions were associated with a 20% decrease in CDI rates (to 7.5 from 9.3 per 10,000 patient days).
Bottom line: Nearly all CDIs are related to exposure in healthcare settings. Exposure to nursing home and ambulatory care seem to play a major role, and infection-control measures in addition to hospital-based strategies need to target these areas. Hospital-based interventions moderately decreased overall rates of CDI.
Citation: Centers for Disease Control and Prevention. Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157-162.
In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
Clinical question: Is a strategy utilizing CT angiography safe to allow discharge from the emergency department low- to intermediate-risk patients with possible acute coronary syndrome (ACS)?
Background: Admission rates for patients with possible acute coronary syndrome are high, but the majority of patients will not have cardiac causes of the symptoms. Coronary computed tomographic angiography (CCTA) has a high negative predictive value for the detection of coronary artery disease, but its utility in determining if a patient can be safely discharged from the emergency department has not been established.
Study design: Prospective, randomized, controlled, multicenter trial.
Setting: Five EDs in the U.S.; three included observation units.
Synopsis: The study enrolled 1,392 patients in a 2:1 ratio, with two-thirds undergoing CCTA and the other third treated with usual care (those admitted for possible ACS with a TIMI score of 0 to 2). Of 908 patients assigned to CCTA, 640 had a negative test, and none of them died or had a myocardial infarction within 30 days. Patients in the CCTA group were more likely than the group undergoing usual care to be discharged from the ED (49.6% vs. 22.7%), have a shorter length of stay (18 hours vs. 24.8 hours, P<.0001), and receive a coronary disease diagnosis.
Bottom line: In a randomized controlled trial, the use of CCTA to evaluate low- to intermediate-risk emergency department patients with possible ACS appears to be safe and effective, and leads to more discharges from the ED.
Citation: Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393-1403.
Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
Clinical question: Can impending physiological deterioration be predicted in medical-surgical ward patients using data from a comprehensive electronic health record (EHR)?
Background: Unplanned ICU transfer is associated with increased mortality and morbidity. Previous studies have examined physiological variables and track-and-trigger systems that might help in the identification of ward patients who are at risk for deterioration and transfer to a higher level of care. More hospitals across the U.S. are using EHRs, and eventually all hospitals are expected to be using one. However, it is unclear if an EHR-based model can accurately predict patients’ clinical deterioration.
Study design: Retrospective case-control study; the unit of analysis was the “patient shift,” each defined by a particular 12-hour period and patient. A complex model to predict patient deterioration and transfer to the ICU was developed and validated using EHR data that was available prior to the deterioration shift.
Setting: Fourteen hospitals of the Northern California Kaiser Permanente Medical Care Program (an integrated healthcare delivery system) that have used an operational EHR for at least three months.
Synopsis: The study identified 4,036 patient-shifts during which a transfer to the ICU occurred, and compared these with 39,782 patient-shifts during which no transfer occurred. Variables in the model included patient demographic data, diagnoses, comorbidities, lab results, and vital signs. The EHR-based predictive model performed well at predicting clinical deterioration and transfer to the ICU (derivation c-statistic 0.84, validation c-statistic 0.77). The model performed best among patients with gastrointestinal diseases (c-statistic 0.84) and worst in patients with acute myocardial infarction (c-statistic 0.57).
Bottom line: Impending physiologic deterioration can be predicted using EHR-based models.
Citation: Escobar GJ, Laguardia JC, Turk BJ, et al. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012:doi:10.1002/jhm.1929 [Epub ahead of print].
Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
Clinical question: How accurate are rapid influenza diagnostic tests, and can they be used to guide further management?
Background: Three million to 5 million people a year develop influenza, which has a high mortality rate and potential global implications. The gold-standard diagnostic tests, PCR and viral culture, have a long turnaround time and are expensive. There have been limited systematic reviews addressing the accuracy of various rapid influenza diagnostic tests (RIDTs), especially in adults.
Study design: Systematic review and meta-analysis.
Setting: Varied.
Synopsis: Studies that compared commercial rapid influenza tests versus reference standards of PCR or viral culture were included. The 159 rapid tests were evaluated in 119 studies representing 26 different brands of commercial tests. Sixty-two of 119 studies included both adults and children, and 41 studies included children only. Overall, rapid influenza tests had a sensitivity of 62.3% and a specificity of 98.2%. There was a higher sensitivity for children than adults (67% vs. 54%) and a higher sensitivity for influenza A than influenza B (65% vs. 52%). The brand of rapid test made little difference. Most articles reviewed did not include a direct comparison between individual brands of RIDTs.
Bottom line: Rapid influenza diagnostic tests have low sensitivity and high specificity. A positive rapid test indicates likely influenza, but a negative test does not rule it out.
Citation: Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156:500-511.
Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
Clinical question: Does a multipronged approach to QI interventions improve the adherence to evidence-based therapies in acute coronary syndromes?
Background: Despite evidence-based recommendations for the use of antiplatelet medication, anticoagulants, beta-blockers, and statins in the setting of an acute coronary syndrome, adherence to these recommendations is poor, especially in low- to middle-income patients.
Study design: Cluster-randomized, prospective, blinded trial.
Setting: Thirty-six urban, public hospitals in Brazil.
Synopsis: Hospitals were randomly allocated to a multifaceted QI strategy versus routine practice. At each hospital, patients were enrolled in a consecutive manner when they presented to the emergency department with an acute coronary syndrome. The QI intervention included multiple modalities, including checklists in the ED, reminders, case management (by a trained RN) to ensure compliance, and educational materials to the staff (pocket algorithms and interactive web programs).
The primary endpoint was adherence to all available evidence-based therapies in the first 24 hours of management. Patients were more likely to receive all evidence-based therapies in hospitals that received the intervention (67.9% vs. 49.5%, P=0.01). The secondary endpoint (adherence at 24 hours and at discharge) was also significantly in favor of the intervention group (50.9% vs. 31.9%, P=0.03).
The findings might not be applicable to institutions with high adherence rates to evidence-based therapy.
Bottom line: A multifaceted QI intervention improves adherence to evidence-based therapies in urban hospitals in medium-income countries.
Citation: Berwanger O, Guimaraes HP, Lanranjeira LN, et al. Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012 [Epub ahead of print].
Rivaroxaban for the Treatment of Acute Pulmonary Embolism
Clinical question: How does the efficacy and safety of rivaroxaban compare with low-molecular-weight heparin (LMWH) plus vitamin K antagonist (VKA) for treatment of acute pulmonary embolism (PE)?
Background: Data support the use of rivaroxaban for stroke prevention in atrial fibrillation, for VTE prophylaxis after orthopedic surgery, and for the treatment of acute coronary syndromes and acute deep vein thromboses. The EINSTEIN-PE investigators now study rivaroxaban for the treatment of acute symptomatic PE.
Study design: Randomized, open-label, noninferiority trial.
Setting: Two hundred sixty-three sites in 38 countries.
Synopsis: The investigators enrolled 4,832 patients with acute symptomatic PE (with or without DVT). Rivaroxaban alone was compared with standard therapy (enoxaparin followed by VKA to an international normalized ratio [INR] of 2 to 3) for three, six, or 12 months. The mean study duration was nine months. INR was in the therapeutic range 62.7% of the time.
The combined primary endpoint of fatal or nonfatal PE, or DVT, occurred in 2.1% in the rivaroxaban group and 1.8% in the standard-therapy group, meeting the pre-specified criteria for non-inferiority (HR 1.12; 95% CI: 0.75-1.68). There were no significant differences in the primary safety outcome of bleeding (HR, 0.90; 95% CI: 0.76-1.07). However, major bleeding events favored rivaroxaban, with events in 1.1% vs. 2.2% of those on VKA (HR 0.49, CI 0.31-0.79, P=0.003). Efficacy and safety of fixed-dose rivaroxaban did not vary by age, sex, weight, glomerular filtration rate, or extent of initial PE.
Bottom line: In patients with symptomatic acute PE, rivaroxaban is noninferior to standard treatment with LMWH plus VKA and might have a safety benefit of less major bleeding. Rivaroxaban and other new oral anticoagulants are likely to be used more frequently as more data is accumulated, but at this time, the guidelines continue to recommend VKA and LMWH as first-line agents.
Citation: The EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287-1297.
Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
Clinical question: Does stent implantation lead to better outcomes when compared to medical therapy in patients with stable coronary artery disease (CAD)?
Background: It is unclear whether stent implantation improves outcomes any more than medical therapy in patients with stable CAD. This is a meta-analysis of trials comparing outcomes of coronary stent implantation with optimal medical therapy.
Study design: Meta-analysis of eight prospective randomized nonblinded trials comparing stent implantation plus medical therapy to medical therapy alone in patients with stable CAD. Outcomes of death, nonfatal myocardial infarction, unplanned revascularization, and persistent angina were compared between the two groups.
Setting: Varied.
Synopsis: Eight trials with 7,229 patients were included with an average follow-up of 4.3 years. In a pooled analysis, coronary stenting versus medical therapy was associated with similar risk of death (8.9% vs. 9.1% P=0.83); nonfatal myocardial infarction (8.9% vs. 8.1%, P=0.22); and persistent angina (29% vs. 33%, P=0.10). Coronary stenting was associated with decreased risk of unplanned revascularization, but the difference was not significant (21.4% vs. 30.7%, P=0.11).
Bottom line: In stable CAD, coronary stent implantation provides no additional benefit when compared to medical therapy.
Citation: Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs. medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312-319.
Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Clinical question: Should patients with hip or knee surgery receive venous thromboprophylaxis (VTE) prophylaxis for seven to 10 days post-operatively or for 21 days or more?
Background: Venous thromboembolism is the most frequent medical complication of knee and hip surgeries. Routine prophylaxis is recommended for minimum of seven to 10 days, but a longer duration might be more beneficial.
Study design: Systemic review and meta-analysis of eight randomized, controlled trials comparing different duration of VTE prophylaxis after hip fracture surgery and total hip or knee replacement.
Setting: Varied.
Synopsis: Eight trials with 2,917 patients met inclusion criteria. Pharmacological agents used for VTE prophylaxis in these trials were coumadin, enoxaparin, dalteparin, and fondaparinux. In patients with hip replacement, undergoing VTE prophylaxis for ≥21 days (compared with seven to 10 days) was associated with a decreased risk of pulmonary embolism (odds ratio [OR] 0.14, 95% CI 0.04-0.47), symptomatic DVTs (OR 0.36, 95% CI 0.16-0.81), asymptomatic DVTs (OR 0.48, 95% CI 0.31-0.75), and proximal DVTs (RR 0.29, CI 0.16-0.52). Prophylaxis for ≥21 days was also associated with an increased risk of minor bleeding (OR 7.55, 95% CI 1.51-37.64).
Data were not sufficient for evaluation of prolonged prophylaxis for total knee replacement and hip fracture surgery.
Bottom line: Prolonged prophylaxis is associated with fewer VTE events in patients with hip replacement but also carries increased risk of minor bleeding.
Citation: Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012 May 15 [Epub ahead of print].
In This Edition
Literature At A Glance
A guide to this month’s studies
- Nearly all CDIs Related to Exposure in Healthcare Setting
- In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
- Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
- Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
- Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
- Rivaroxaban for the Treatment of Acute Pulmonary Embolism
- Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
- Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Nearly all CDIs Related to Exposure in Healthcare Setting
Clinical question: What is the contribution of non-hospital healthcare exposures to the burden of Clostridium difficile infection (CDI)?
Background: CDI is common among hospitalized patients and is associated with high rates of morbidity. Most CDI prevention programs are aimed at hospital-based risk factors. However, non-hospital healthcare exposures might contribute significantly to the burden of CDI, and hospital-based prevention programs might not address these risks.
Study design: Retrospective analysis of three population-based data sets.
Setting: Three population data sets tracking infections on a national and state level in the U.S.
Synopsis: This study analyzed two data sets to determine the contribution of non-hospital healthcare exposure to CDIs, and examined a third to determine whether a program addressing hospital-based exposures reduced the rate of CDI.Using data from the CDC’s Emerging Infections Program, 10,342 CDI cases from 111 hospitals were examined. Each case was classified as hospital onset (i.e. occurring three days after admission), nursing home onset, or community onset. A total of 94% of cases were associated with recent exposure to healthcare, 75% were classified as non-hospital onset, and 20% of hospital-onset cases were in patients who had recently been in a nursing home, suggesting that non-hospital-based healthcare exposures play a significant role. The second analysis used data from the National Healthcare Safety Network to examine 42,157 CDIs in 711 hospitals.
The authors found that 52% of CDIs were present on admission. The pooled rate of hospital-onset CDI was low (7.4 per 10,000 patient-days). The final analysis examined hospital-onset CDI rates across three hospital-based prevention programs over a period of nearly two years. The interventions were associated with a 20% decrease in CDI rates (to 7.5 from 9.3 per 10,000 patient days).
Bottom line: Nearly all CDIs are related to exposure in healthcare settings. Exposure to nursing home and ambulatory care seem to play a major role, and infection-control measures in addition to hospital-based strategies need to target these areas. Hospital-based interventions moderately decreased overall rates of CDI.
Citation: Centers for Disease Control and Prevention. Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157-162.
In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
Clinical question: Is a strategy utilizing CT angiography safe to allow discharge from the emergency department low- to intermediate-risk patients with possible acute coronary syndrome (ACS)?
Background: Admission rates for patients with possible acute coronary syndrome are high, but the majority of patients will not have cardiac causes of the symptoms. Coronary computed tomographic angiography (CCTA) has a high negative predictive value for the detection of coronary artery disease, but its utility in determining if a patient can be safely discharged from the emergency department has not been established.
Study design: Prospective, randomized, controlled, multicenter trial.
Setting: Five EDs in the U.S.; three included observation units.
Synopsis: The study enrolled 1,392 patients in a 2:1 ratio, with two-thirds undergoing CCTA and the other third treated with usual care (those admitted for possible ACS with a TIMI score of 0 to 2). Of 908 patients assigned to CCTA, 640 had a negative test, and none of them died or had a myocardial infarction within 30 days. Patients in the CCTA group were more likely than the group undergoing usual care to be discharged from the ED (49.6% vs. 22.7%), have a shorter length of stay (18 hours vs. 24.8 hours, P<.0001), and receive a coronary disease diagnosis.
Bottom line: In a randomized controlled trial, the use of CCTA to evaluate low- to intermediate-risk emergency department patients with possible ACS appears to be safe and effective, and leads to more discharges from the ED.
Citation: Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393-1403.
Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
Clinical question: Can impending physiological deterioration be predicted in medical-surgical ward patients using data from a comprehensive electronic health record (EHR)?
Background: Unplanned ICU transfer is associated with increased mortality and morbidity. Previous studies have examined physiological variables and track-and-trigger systems that might help in the identification of ward patients who are at risk for deterioration and transfer to a higher level of care. More hospitals across the U.S. are using EHRs, and eventually all hospitals are expected to be using one. However, it is unclear if an EHR-based model can accurately predict patients’ clinical deterioration.
Study design: Retrospective case-control study; the unit of analysis was the “patient shift,” each defined by a particular 12-hour period and patient. A complex model to predict patient deterioration and transfer to the ICU was developed and validated using EHR data that was available prior to the deterioration shift.
Setting: Fourteen hospitals of the Northern California Kaiser Permanente Medical Care Program (an integrated healthcare delivery system) that have used an operational EHR for at least three months.
Synopsis: The study identified 4,036 patient-shifts during which a transfer to the ICU occurred, and compared these with 39,782 patient-shifts during which no transfer occurred. Variables in the model included patient demographic data, diagnoses, comorbidities, lab results, and vital signs. The EHR-based predictive model performed well at predicting clinical deterioration and transfer to the ICU (derivation c-statistic 0.84, validation c-statistic 0.77). The model performed best among patients with gastrointestinal diseases (c-statistic 0.84) and worst in patients with acute myocardial infarction (c-statistic 0.57).
Bottom line: Impending physiologic deterioration can be predicted using EHR-based models.
Citation: Escobar GJ, Laguardia JC, Turk BJ, et al. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012:doi:10.1002/jhm.1929 [Epub ahead of print].
Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
Clinical question: How accurate are rapid influenza diagnostic tests, and can they be used to guide further management?
Background: Three million to 5 million people a year develop influenza, which has a high mortality rate and potential global implications. The gold-standard diagnostic tests, PCR and viral culture, have a long turnaround time and are expensive. There have been limited systematic reviews addressing the accuracy of various rapid influenza diagnostic tests (RIDTs), especially in adults.
Study design: Systematic review and meta-analysis.
Setting: Varied.
Synopsis: Studies that compared commercial rapid influenza tests versus reference standards of PCR or viral culture were included. The 159 rapid tests were evaluated in 119 studies representing 26 different brands of commercial tests. Sixty-two of 119 studies included both adults and children, and 41 studies included children only. Overall, rapid influenza tests had a sensitivity of 62.3% and a specificity of 98.2%. There was a higher sensitivity for children than adults (67% vs. 54%) and a higher sensitivity for influenza A than influenza B (65% vs. 52%). The brand of rapid test made little difference. Most articles reviewed did not include a direct comparison between individual brands of RIDTs.
Bottom line: Rapid influenza diagnostic tests have low sensitivity and high specificity. A positive rapid test indicates likely influenza, but a negative test does not rule it out.
Citation: Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156:500-511.
Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
Clinical question: Does a multipronged approach to QI interventions improve the adherence to evidence-based therapies in acute coronary syndromes?
Background: Despite evidence-based recommendations for the use of antiplatelet medication, anticoagulants, beta-blockers, and statins in the setting of an acute coronary syndrome, adherence to these recommendations is poor, especially in low- to middle-income patients.
Study design: Cluster-randomized, prospective, blinded trial.
Setting: Thirty-six urban, public hospitals in Brazil.
Synopsis: Hospitals were randomly allocated to a multifaceted QI strategy versus routine practice. At each hospital, patients were enrolled in a consecutive manner when they presented to the emergency department with an acute coronary syndrome. The QI intervention included multiple modalities, including checklists in the ED, reminders, case management (by a trained RN) to ensure compliance, and educational materials to the staff (pocket algorithms and interactive web programs).
The primary endpoint was adherence to all available evidence-based therapies in the first 24 hours of management. Patients were more likely to receive all evidence-based therapies in hospitals that received the intervention (67.9% vs. 49.5%, P=0.01). The secondary endpoint (adherence at 24 hours and at discharge) was also significantly in favor of the intervention group (50.9% vs. 31.9%, P=0.03).
The findings might not be applicable to institutions with high adherence rates to evidence-based therapy.
Bottom line: A multifaceted QI intervention improves adherence to evidence-based therapies in urban hospitals in medium-income countries.
Citation: Berwanger O, Guimaraes HP, Lanranjeira LN, et al. Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012 [Epub ahead of print].
Rivaroxaban for the Treatment of Acute Pulmonary Embolism
Clinical question: How does the efficacy and safety of rivaroxaban compare with low-molecular-weight heparin (LMWH) plus vitamin K antagonist (VKA) for treatment of acute pulmonary embolism (PE)?
Background: Data support the use of rivaroxaban for stroke prevention in atrial fibrillation, for VTE prophylaxis after orthopedic surgery, and for the treatment of acute coronary syndromes and acute deep vein thromboses. The EINSTEIN-PE investigators now study rivaroxaban for the treatment of acute symptomatic PE.
Study design: Randomized, open-label, noninferiority trial.
Setting: Two hundred sixty-three sites in 38 countries.
Synopsis: The investigators enrolled 4,832 patients with acute symptomatic PE (with or without DVT). Rivaroxaban alone was compared with standard therapy (enoxaparin followed by VKA to an international normalized ratio [INR] of 2 to 3) for three, six, or 12 months. The mean study duration was nine months. INR was in the therapeutic range 62.7% of the time.
The combined primary endpoint of fatal or nonfatal PE, or DVT, occurred in 2.1% in the rivaroxaban group and 1.8% in the standard-therapy group, meeting the pre-specified criteria for non-inferiority (HR 1.12; 95% CI: 0.75-1.68). There were no significant differences in the primary safety outcome of bleeding (HR, 0.90; 95% CI: 0.76-1.07). However, major bleeding events favored rivaroxaban, with events in 1.1% vs. 2.2% of those on VKA (HR 0.49, CI 0.31-0.79, P=0.003). Efficacy and safety of fixed-dose rivaroxaban did not vary by age, sex, weight, glomerular filtration rate, or extent of initial PE.
Bottom line: In patients with symptomatic acute PE, rivaroxaban is noninferior to standard treatment with LMWH plus VKA and might have a safety benefit of less major bleeding. Rivaroxaban and other new oral anticoagulants are likely to be used more frequently as more data is accumulated, but at this time, the guidelines continue to recommend VKA and LMWH as first-line agents.
Citation: The EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287-1297.
Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
Clinical question: Does stent implantation lead to better outcomes when compared to medical therapy in patients with stable coronary artery disease (CAD)?
Background: It is unclear whether stent implantation improves outcomes any more than medical therapy in patients with stable CAD. This is a meta-analysis of trials comparing outcomes of coronary stent implantation with optimal medical therapy.
Study design: Meta-analysis of eight prospective randomized nonblinded trials comparing stent implantation plus medical therapy to medical therapy alone in patients with stable CAD. Outcomes of death, nonfatal myocardial infarction, unplanned revascularization, and persistent angina were compared between the two groups.
Setting: Varied.
Synopsis: Eight trials with 7,229 patients were included with an average follow-up of 4.3 years. In a pooled analysis, coronary stenting versus medical therapy was associated with similar risk of death (8.9% vs. 9.1% P=0.83); nonfatal myocardial infarction (8.9% vs. 8.1%, P=0.22); and persistent angina (29% vs. 33%, P=0.10). Coronary stenting was associated with decreased risk of unplanned revascularization, but the difference was not significant (21.4% vs. 30.7%, P=0.11).
Bottom line: In stable CAD, coronary stent implantation provides no additional benefit when compared to medical therapy.
Citation: Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs. medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312-319.
Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Clinical question: Should patients with hip or knee surgery receive venous thromboprophylaxis (VTE) prophylaxis for seven to 10 days post-operatively or for 21 days or more?
Background: Venous thromboembolism is the most frequent medical complication of knee and hip surgeries. Routine prophylaxis is recommended for minimum of seven to 10 days, but a longer duration might be more beneficial.
Study design: Systemic review and meta-analysis of eight randomized, controlled trials comparing different duration of VTE prophylaxis after hip fracture surgery and total hip or knee replacement.
Setting: Varied.
Synopsis: Eight trials with 2,917 patients met inclusion criteria. Pharmacological agents used for VTE prophylaxis in these trials were coumadin, enoxaparin, dalteparin, and fondaparinux. In patients with hip replacement, undergoing VTE prophylaxis for ≥21 days (compared with seven to 10 days) was associated with a decreased risk of pulmonary embolism (odds ratio [OR] 0.14, 95% CI 0.04-0.47), symptomatic DVTs (OR 0.36, 95% CI 0.16-0.81), asymptomatic DVTs (OR 0.48, 95% CI 0.31-0.75), and proximal DVTs (RR 0.29, CI 0.16-0.52). Prophylaxis for ≥21 days was also associated with an increased risk of minor bleeding (OR 7.55, 95% CI 1.51-37.64).
Data were not sufficient for evaluation of prolonged prophylaxis for total knee replacement and hip fracture surgery.
Bottom line: Prolonged prophylaxis is associated with fewer VTE events in patients with hip replacement but also carries increased risk of minor bleeding.
Citation: Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012 May 15 [Epub ahead of print].
In This Edition
Literature At A Glance
A guide to this month’s studies
- Nearly all CDIs Related to Exposure in Healthcare Setting
- In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
- Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
- Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
- Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
- Rivaroxaban for the Treatment of Acute Pulmonary Embolism
- Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
- Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Nearly all CDIs Related to Exposure in Healthcare Setting
Clinical question: What is the contribution of non-hospital healthcare exposures to the burden of Clostridium difficile infection (CDI)?
Background: CDI is common among hospitalized patients and is associated with high rates of morbidity. Most CDI prevention programs are aimed at hospital-based risk factors. However, non-hospital healthcare exposures might contribute significantly to the burden of CDI, and hospital-based prevention programs might not address these risks.
Study design: Retrospective analysis of three population-based data sets.
Setting: Three population data sets tracking infections on a national and state level in the U.S.
Synopsis: This study analyzed two data sets to determine the contribution of non-hospital healthcare exposure to CDIs, and examined a third to determine whether a program addressing hospital-based exposures reduced the rate of CDI.Using data from the CDC’s Emerging Infections Program, 10,342 CDI cases from 111 hospitals were examined. Each case was classified as hospital onset (i.e. occurring three days after admission), nursing home onset, or community onset. A total of 94% of cases were associated with recent exposure to healthcare, 75% were classified as non-hospital onset, and 20% of hospital-onset cases were in patients who had recently been in a nursing home, suggesting that non-hospital-based healthcare exposures play a significant role. The second analysis used data from the National Healthcare Safety Network to examine 42,157 CDIs in 711 hospitals.
The authors found that 52% of CDIs were present on admission. The pooled rate of hospital-onset CDI was low (7.4 per 10,000 patient-days). The final analysis examined hospital-onset CDI rates across three hospital-based prevention programs over a period of nearly two years. The interventions were associated with a 20% decrease in CDI rates (to 7.5 from 9.3 per 10,000 patient days).
Bottom line: Nearly all CDIs are related to exposure in healthcare settings. Exposure to nursing home and ambulatory care seem to play a major role, and infection-control measures in addition to hospital-based strategies need to target these areas. Hospital-based interventions moderately decreased overall rates of CDI.
Citation: Centers for Disease Control and Prevention. Vital signs: preventing Clostridium difficile infections. MMWR Morb Mortal Wkly Rep. 2012;61:157-162.
In Suspected Acute Coronary Syndrome, CT Angiography Identifies Patients Safe for Discharge
Clinical question: Is a strategy utilizing CT angiography safe to allow discharge from the emergency department low- to intermediate-risk patients with possible acute coronary syndrome (ACS)?
Background: Admission rates for patients with possible acute coronary syndrome are high, but the majority of patients will not have cardiac causes of the symptoms. Coronary computed tomographic angiography (CCTA) has a high negative predictive value for the detection of coronary artery disease, but its utility in determining if a patient can be safely discharged from the emergency department has not been established.
Study design: Prospective, randomized, controlled, multicenter trial.
Setting: Five EDs in the U.S.; three included observation units.
Synopsis: The study enrolled 1,392 patients in a 2:1 ratio, with two-thirds undergoing CCTA and the other third treated with usual care (those admitted for possible ACS with a TIMI score of 0 to 2). Of 908 patients assigned to CCTA, 640 had a negative test, and none of them died or had a myocardial infarction within 30 days. Patients in the CCTA group were more likely than the group undergoing usual care to be discharged from the ED (49.6% vs. 22.7%), have a shorter length of stay (18 hours vs. 24.8 hours, P<.0001), and receive a coronary disease diagnosis.
Bottom line: In a randomized controlled trial, the use of CCTA to evaluate low- to intermediate-risk emergency department patients with possible ACS appears to be safe and effective, and leads to more discharges from the ED.
Citation: Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes. N Engl J Med. 2012;366:1393-1403.
Impending Physiological Deterioration Can Be Predicted Using Data from a Comprehensive EHR
Clinical question: Can impending physiological deterioration be predicted in medical-surgical ward patients using data from a comprehensive electronic health record (EHR)?
Background: Unplanned ICU transfer is associated with increased mortality and morbidity. Previous studies have examined physiological variables and track-and-trigger systems that might help in the identification of ward patients who are at risk for deterioration and transfer to a higher level of care. More hospitals across the U.S. are using EHRs, and eventually all hospitals are expected to be using one. However, it is unclear if an EHR-based model can accurately predict patients’ clinical deterioration.
Study design: Retrospective case-control study; the unit of analysis was the “patient shift,” each defined by a particular 12-hour period and patient. A complex model to predict patient deterioration and transfer to the ICU was developed and validated using EHR data that was available prior to the deterioration shift.
Setting: Fourteen hospitals of the Northern California Kaiser Permanente Medical Care Program (an integrated healthcare delivery system) that have used an operational EHR for at least three months.
Synopsis: The study identified 4,036 patient-shifts during which a transfer to the ICU occurred, and compared these with 39,782 patient-shifts during which no transfer occurred. Variables in the model included patient demographic data, diagnoses, comorbidities, lab results, and vital signs. The EHR-based predictive model performed well at predicting clinical deterioration and transfer to the ICU (derivation c-statistic 0.84, validation c-statistic 0.77). The model performed best among patients with gastrointestinal diseases (c-statistic 0.84) and worst in patients with acute myocardial infarction (c-statistic 0.57).
Bottom line: Impending physiologic deterioration can be predicted using EHR-based models.
Citation: Escobar GJ, Laguardia JC, Turk BJ, et al. Early detection of impending physiologic deterioration among patients who are not in intensive care: Development of predictive models using data from an automated electronic medical record. J Hosp Med. 2012:doi:10.1002/jhm.1929 [Epub ahead of print].
Rapid Influenza Diagnostic Tests Have Low Sensitivity and High Specificity
Clinical question: How accurate are rapid influenza diagnostic tests, and can they be used to guide further management?
Background: Three million to 5 million people a year develop influenza, which has a high mortality rate and potential global implications. The gold-standard diagnostic tests, PCR and viral culture, have a long turnaround time and are expensive. There have been limited systematic reviews addressing the accuracy of various rapid influenza diagnostic tests (RIDTs), especially in adults.
Study design: Systematic review and meta-analysis.
Setting: Varied.
Synopsis: Studies that compared commercial rapid influenza tests versus reference standards of PCR or viral culture were included. The 159 rapid tests were evaluated in 119 studies representing 26 different brands of commercial tests. Sixty-two of 119 studies included both adults and children, and 41 studies included children only. Overall, rapid influenza tests had a sensitivity of 62.3% and a specificity of 98.2%. There was a higher sensitivity for children than adults (67% vs. 54%) and a higher sensitivity for influenza A than influenza B (65% vs. 52%). The brand of rapid test made little difference. Most articles reviewed did not include a direct comparison between individual brands of RIDTs.
Bottom line: Rapid influenza diagnostic tests have low sensitivity and high specificity. A positive rapid test indicates likely influenza, but a negative test does not rule it out.
Citation: Chartrand C, Leeflang MM, Minion J, Brewer T, Pai M. Accuracy of rapid influenza diagnostic tests: a meta-analysis. Ann Intern Med. 2012;156:500-511.
Multifaceted QI Intervention Increases Adherence to Evidence-Based Therapy in Acute Coronary Syndrome
Clinical question: Does a multipronged approach to QI interventions improve the adherence to evidence-based therapies in acute coronary syndromes?
Background: Despite evidence-based recommendations for the use of antiplatelet medication, anticoagulants, beta-blockers, and statins in the setting of an acute coronary syndrome, adherence to these recommendations is poor, especially in low- to middle-income patients.
Study design: Cluster-randomized, prospective, blinded trial.
Setting: Thirty-six urban, public hospitals in Brazil.
Synopsis: Hospitals were randomly allocated to a multifaceted QI strategy versus routine practice. At each hospital, patients were enrolled in a consecutive manner when they presented to the emergency department with an acute coronary syndrome. The QI intervention included multiple modalities, including checklists in the ED, reminders, case management (by a trained RN) to ensure compliance, and educational materials to the staff (pocket algorithms and interactive web programs).
The primary endpoint was adherence to all available evidence-based therapies in the first 24 hours of management. Patients were more likely to receive all evidence-based therapies in hospitals that received the intervention (67.9% vs. 49.5%, P=0.01). The secondary endpoint (adherence at 24 hours and at discharge) was also significantly in favor of the intervention group (50.9% vs. 31.9%, P=0.03).
The findings might not be applicable to institutions with high adherence rates to evidence-based therapy.
Bottom line: A multifaceted QI intervention improves adherence to evidence-based therapies in urban hospitals in medium-income countries.
Citation: Berwanger O, Guimaraes HP, Lanranjeira LN, et al. Effect of a multifaceted intervention on use of evidence-based therapies in patients with acute coronary syndromes in Brazil: the BRIDGE-ACS randomized trial. JAMA. 2012 [Epub ahead of print].
Rivaroxaban for the Treatment of Acute Pulmonary Embolism
Clinical question: How does the efficacy and safety of rivaroxaban compare with low-molecular-weight heparin (LMWH) plus vitamin K antagonist (VKA) for treatment of acute pulmonary embolism (PE)?
Background: Data support the use of rivaroxaban for stroke prevention in atrial fibrillation, for VTE prophylaxis after orthopedic surgery, and for the treatment of acute coronary syndromes and acute deep vein thromboses. The EINSTEIN-PE investigators now study rivaroxaban for the treatment of acute symptomatic PE.
Study design: Randomized, open-label, noninferiority trial.
Setting: Two hundred sixty-three sites in 38 countries.
Synopsis: The investigators enrolled 4,832 patients with acute symptomatic PE (with or without DVT). Rivaroxaban alone was compared with standard therapy (enoxaparin followed by VKA to an international normalized ratio [INR] of 2 to 3) for three, six, or 12 months. The mean study duration was nine months. INR was in the therapeutic range 62.7% of the time.
The combined primary endpoint of fatal or nonfatal PE, or DVT, occurred in 2.1% in the rivaroxaban group and 1.8% in the standard-therapy group, meeting the pre-specified criteria for non-inferiority (HR 1.12; 95% CI: 0.75-1.68). There were no significant differences in the primary safety outcome of bleeding (HR, 0.90; 95% CI: 0.76-1.07). However, major bleeding events favored rivaroxaban, with events in 1.1% vs. 2.2% of those on VKA (HR 0.49, CI 0.31-0.79, P=0.003). Efficacy and safety of fixed-dose rivaroxaban did not vary by age, sex, weight, glomerular filtration rate, or extent of initial PE.
Bottom line: In patients with symptomatic acute PE, rivaroxaban is noninferior to standard treatment with LMWH plus VKA and might have a safety benefit of less major bleeding. Rivaroxaban and other new oral anticoagulants are likely to be used more frequently as more data is accumulated, but at this time, the guidelines continue to recommend VKA and LMWH as first-line agents.
Citation: The EINSTEIN-PE Investigators, Büller HR, Prins MH, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med. 2012;366:1287-1297.
Coronary Stent Implantation Provides No Additional Benefit when Compared with Medical Therapy Alone in Patients with Stable Coronary Artery Disease
Clinical question: Does stent implantation lead to better outcomes when compared to medical therapy in patients with stable coronary artery disease (CAD)?
Background: It is unclear whether stent implantation improves outcomes any more than medical therapy in patients with stable CAD. This is a meta-analysis of trials comparing outcomes of coronary stent implantation with optimal medical therapy.
Study design: Meta-analysis of eight prospective randomized nonblinded trials comparing stent implantation plus medical therapy to medical therapy alone in patients with stable CAD. Outcomes of death, nonfatal myocardial infarction, unplanned revascularization, and persistent angina were compared between the two groups.
Setting: Varied.
Synopsis: Eight trials with 7,229 patients were included with an average follow-up of 4.3 years. In a pooled analysis, coronary stenting versus medical therapy was associated with similar risk of death (8.9% vs. 9.1% P=0.83); nonfatal myocardial infarction (8.9% vs. 8.1%, P=0.22); and persistent angina (29% vs. 33%, P=0.10). Coronary stenting was associated with decreased risk of unplanned revascularization, but the difference was not significant (21.4% vs. 30.7%, P=0.11).
Bottom line: In stable CAD, coronary stent implantation provides no additional benefit when compared to medical therapy.
Citation: Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs. medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312-319.
Prolonged Versus Standard Duration Venous Thromboprophylaxis after Major Orthopedic Surgery
Clinical question: Should patients with hip or knee surgery receive venous thromboprophylaxis (VTE) prophylaxis for seven to 10 days post-operatively or for 21 days or more?
Background: Venous thromboembolism is the most frequent medical complication of knee and hip surgeries. Routine prophylaxis is recommended for minimum of seven to 10 days, but a longer duration might be more beneficial.
Study design: Systemic review and meta-analysis of eight randomized, controlled trials comparing different duration of VTE prophylaxis after hip fracture surgery and total hip or knee replacement.
Setting: Varied.
Synopsis: Eight trials with 2,917 patients met inclusion criteria. Pharmacological agents used for VTE prophylaxis in these trials were coumadin, enoxaparin, dalteparin, and fondaparinux. In patients with hip replacement, undergoing VTE prophylaxis for ≥21 days (compared with seven to 10 days) was associated with a decreased risk of pulmonary embolism (odds ratio [OR] 0.14, 95% CI 0.04-0.47), symptomatic DVTs (OR 0.36, 95% CI 0.16-0.81), asymptomatic DVTs (OR 0.48, 95% CI 0.31-0.75), and proximal DVTs (RR 0.29, CI 0.16-0.52). Prophylaxis for ≥21 days was also associated with an increased risk of minor bleeding (OR 7.55, 95% CI 1.51-37.64).
Data were not sufficient for evaluation of prolonged prophylaxis for total knee replacement and hip fracture surgery.
Bottom line: Prolonged prophylaxis is associated with fewer VTE events in patients with hip replacement but also carries increased risk of minor bleeding.
Citation: Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012 May 15 [Epub ahead of print].