As with US adults, infants and children appear to be at increased risk for gastroesophageal reflux disease (GERD). Lacking a cardinal symptom in children and often linked with confounding extra-esophageal symptoms, pediatric GERD challenges the primary care clinician to make an early diagnosis, preventing progressive damage and possible complications. Management begins with conservative lifestyle changes; pharmacologic and surgical options are reserved for specific pediatric patients.
Traditionally, gastroesophageal reflux disease (GERD) has been viewed as an adult disease, but it is now recognized as a disorder that also occurs in children. A teenager with heartburn, a child with complaints of chest pain, and a coughing infant refusing to feed may all be experiencing it. Review of the literature reveals an increased incidence of GERD in both adults and children, making it one of the five most common gastrointestinal (GI) conditions in the United States.1
US pediatric hospitalization rates associated with GERD significantly increased from 1995 to 2000, accounting for 4% of these admissions.1 In a 2009 review of ICD-9 codes in a large claims database, GERD was diagnosed in 12.3% of North American infants and in 1% of other pediatric age-groups.2,3 In another recent study in which pediatric endoscopy data from 1999 to 2002 were analyzed, 9.5% of children age 1 year and 7.6% of children age 2 had erosive esophagitis.4
It is unclear whether the increased frequency in diagnosis of GERD should be attributed to improved diagnostic strategies or to an actual increase in disease prevalence.1 In any event, a timely diagnosis of GERD is essential to allow for appropriate intervention and early symptom management to reduce the risk for complications.
Overall, GERD is primarily a Western disease, affecting an estimated 10% to 15% of this geographic population. It is associated with obesity, recent dietary trends, and other causes.5 Prevalence of GERD in the general population has been shown to vary across ethnic groups. In the US, persons of Hispanic descent are more likely to be affected than whites, with symptoms of GERD least common among Asian-Americans.5
Since pediatric GERD is seen in primary care settings in the same rising numbers as associated hospital admissions, clinicians who provide primary care must be aware of its contributing factors, treatment modalities that are most effective in reducing symptoms, and strategies to prevent this disease. Treatment choices vary according to patient age-groups: infants (younger than 1 year), children ages 1 to 11 years, and adolescents, 12 to 18.
DISTINGUISHING GERD FROM GER
Gastroesophageal reflux (GER) is the term used to describe the passage of gastric contents, including stomach acid, fluids, and food, into the esophagus, with or without regurgitation or vomiting.6 GER is a normal, common physiologic process among infants, in whom frequent feedings, small stomach size, and predominance of the recumbent position allow reflux to occur during transient relaxation of the lower esophageal sphincter.6-9
Healthy infants and children may have asymptomatic episodes of GER; or episodes may be short, lasting less than three minutes, and occurring postprandially.6 Only when GER involves blood loss, esophagitis, strictures, nutritional deficits, and/or apnea should GERD be considered.9
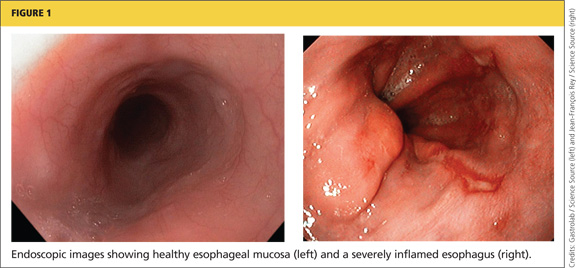
The pathologic process known as GERD involves persistent, troublesome symptoms resulting from continued mucosal exposure to stomach acid, damaging the lining of the esophagus and possibly leading to erosive esophagitis.6,10,11 Endoscopic findings indicating GERD-associated esophageal damage include visible tears in the esophageal mucosa near the gastroesophageal junction6 (see Figure 1). In one single-center US study, almost 30% of patients with pediatric GERD who underwent endoscopy had erosive esophagitis.4
Continued on next page >>