Edwin R. Raffi, MD, MPH Instructor in Psychiatry Harvard Medical School Center for Women’s Mental Health Massachusetts General Hospital Boston, Massachusetts
Marlene P. Freeman, MD Associate Professor in Psychiatry Harvard Medical School Associate Director Center for Women’s Mental Health Massachusetts General Hospital Boston, Massachusetts
Disclosures Dr. Raffi reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products. Dr. Freeman has received research support from JayMac, Sage, and Takeda; and has served on advisory boards for Janssen, JDS Therapeutics, and Sage. Dr. Freeman is an employee of Massachusetts General Hospital (MGH) and works with the MGH Pregnancy Registry; this registry is sponsored by Alkermes, Forest/Actavis, Otsuka, and Sunovion. As an employee of MGH, Dr. Freeman works with the MGH Clinical Trials Network and Institute, which has received research funding from multiple pharmaceutical companies and the National Institute of Mental Health.
A better understanding of the causes of PMDD can lead to improved diagnosis and treatment
In an age when psychiatry strives to identify the biologic causes of disease, studying endocrine-related mood disorders is particularly intriguing. DSM-5 defines premenstrual dysphoric disorder (PMDD) as a depressive disorder, with a 12-month prevalence ranging from 1.8% to 5.8% among women who menstruate.1-3 Factors that differentiate PMDD from other affective disorders include etiology, duration, and temporal relationship with the menstrual cycle.
PMDD is a disorder of consistent yet intermittent change in mental health and functionality. Therefore, it may be underdiagnosed and consequently undertreated if a psychiatric evaluation does not coincide with symptom occurrence or if patients do not understand that intermittent symptoms are treatable.
This article summarizes what is known about the etiology of PMDD.Although there are several treatments for PMDD, many women experience adverse effects or incomplete effectiveness. Further understanding of this disorder may lead to more efficacious treatments. Additionally, understanding the pathophysiology of PMDD might shed a light on the etiology of other disorders that are temporally related to reproductive life changes, such as pregnancy-, postpartum-, or menopause-related affective dysregulation.
Making the diagnosis
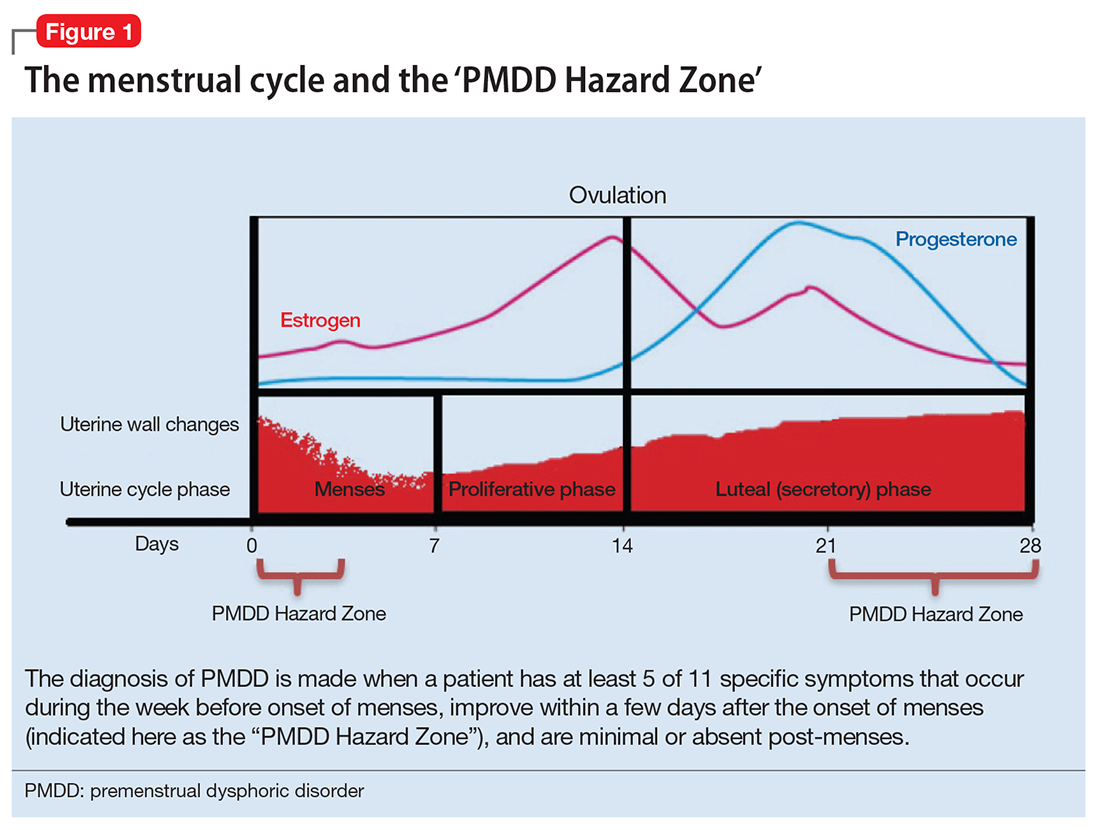
The diagnosis of PMDD is made when a patient has at least 5 of 11 specific symptoms that occur during the week before onset of menses, improve within a few days after the onset of menses (shown as the “PMDD Hazard Zone”in Figure 1), and are minimal or absent post-menses.3 Symptoms should be tracked prospectively for at least 2 menstrual cycles in order to confirm the diagnosis (one must be an affective symptom and another must be a behavioral/cognitive symptom).3
The affective symptoms are:
lability of affect (eg, sudden sadness, tearfulness, or sensitivity to rejection)
irritability, anger, or increased interpersonal conflicts
depressed mood, hopelessness, or self- deprecating thoughts
anxiety or tension, feeling “keyed up” or “on edge.”
The behavioral/cognitive symptoms are:
decreased interest in usual activities (eg, work, hobbies, friends, school)
difficulty concentrating
lethargy, low energy, easy fatigability
change in appetite, overeating, food cravings
hypersomnia or insomnia
feeling overwhelmed or out of control
physical symptoms (breast tenderness or swelling, headache, joint or muscle pain, bloating, weight gain).
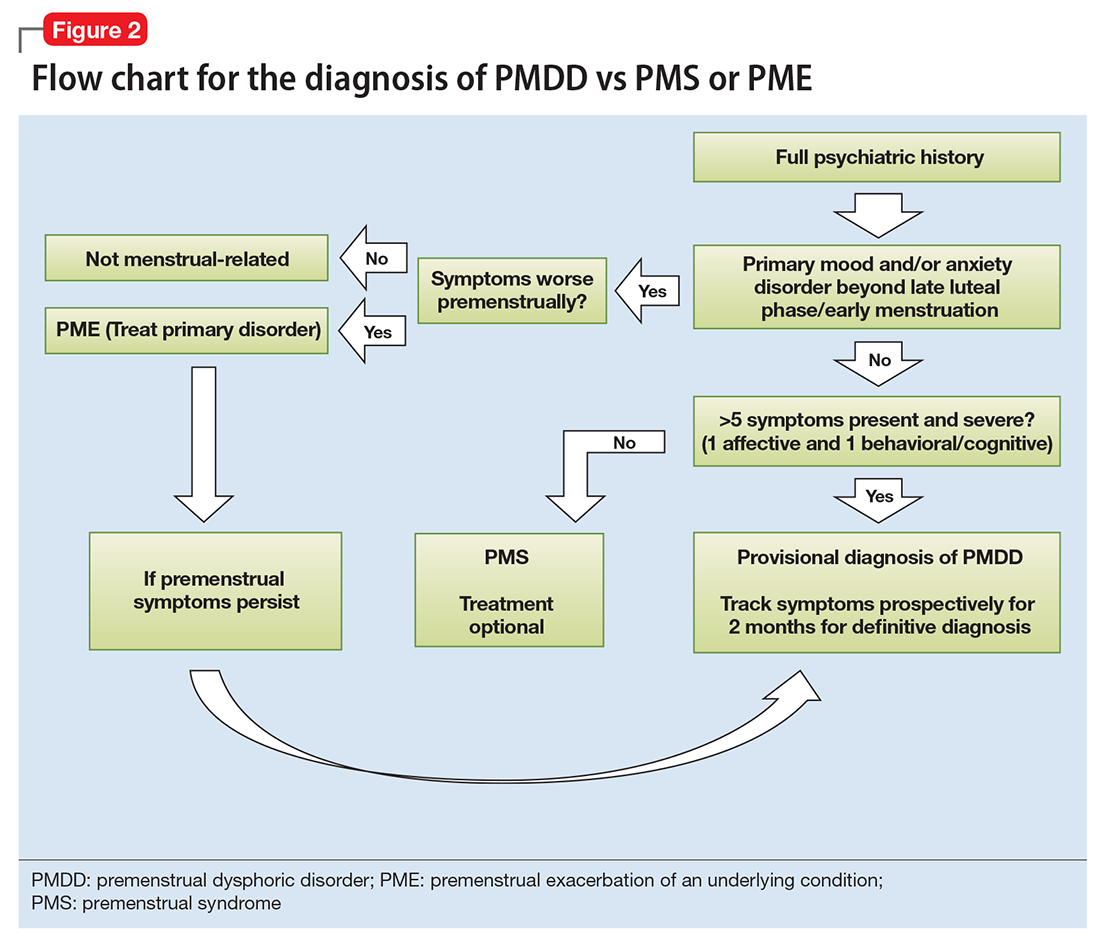
Ruling out premenstrual exacerbation (PME). Perhaps the most common cause for misdiagnosis of PMDD is failing to rule out PME of another underlying or comorbid condition (Figure 2). In many women who have a primary mood or anxiety disorder, the late luteal phase is a vulnerable time. A patient might be coping with untreated anxiety, for example, but the symptoms become unbearable the week before menstruation begins, which is likely when she seeks help. At this stage, a diagnosis of PMDD should be provisional at best. Often, PME is treated by treating the underlying condition. Therefore, a full diagnostic psychiatric interview is important to first rule out other underlying psychiatric disorders. PMDD is diagnosed if the premenstrual symptoms persist for 2 consecutive months after treating the suspected mood or anxiety disorder. Patients can use one of many PMDD daily symptom charts available online. Alternatively, they can use a cycle-tracking mobile phone application to correlate their symptoms with their cycle and share this information with their providers.