Epidermal nevus syndrome (ENS), also known as Solomon syndrome, is a rare neurocutaneous disorder defined by mosaicism. Epidermal nevus syndrome may be associated with a variety of systemic findings, several of which have been described in the literature, including but not limited to central nervous system abnormalities and internal malignancies. There is a paucity of reports of patients with both epidermal nevi and papillary transitional cell bladder carcinoma in the literature. We present a rare case of systematized epidermal nevi associated with development of papillary transitional cell bladder carcinoma in a young woman. Patients diagnosed with generalized epidermal nevi should have workup for possible associated central nervous system, musculoskeletal, genitourinary abnormalities, and internal malignancies. The association of epidermal nevi and transitional cell bladder carcinoma may be linked to a mutation in the fibroblast growth factor receptor 3 gene, FGFR3, but a clear link has yet to be substantiated and additional molecular studies are needed.
Epidermal nevi are common benign cutaneous neoplasms.
Extensive systematized epidermal nevi can be a sign of internal disease.
References
Epidermal nevi can occur in isolation or in association with internal abnormalities. Epidermal nevus syndrome (ENS) is a heterogeneous group of neurocutaneous disorders characterized by mosaicism and epidermal nevi found in association with various systemic abnormalities.1-4 There are many possible associated systemic findings, including abnormalities of the central nervous, musculoskeletal, renal, and hematologic systems. Epidermal nevi have been associated with internal malignancies. We present the case of a patient with epidermal nevi associated with papillary transitional cell bladder carcinoma. According to a PubMed search of articles indexed for MEDLINE using the search terms transitional cell bladder carcinoma and epidermal nevus, there have only been 4 other cases of transitional cell bladder carcinoma and ENS reported in the literature,5-8 2 of which were reports of papillary transitional cell bladder carcinoma.5,6
Case Report
A 29-year-old woman presented to our clinic with a rash that had been present since 3 years of age. The emergency department consulted dermatology for evaluation of what was believed to be contact dermatitis; however, upon questioning the patient, it was revealed that the rash was chronic and persistent.
The rash was nonpruritic and was located on the face, hands (Figure 1), chest, buttocks, thighs, legs, and back (Figure 2). Although asymptomatic, the appearance of the skin caused the patient some emotional distress. As a child she had been evaluated by a dermatologist and a biopsy was performed, but she did not recall the results or have any records. She had been prescribed an oral medication by the dermatologist, but treatment was terminated early due to nausea. The skin lesions did not improve with the short course of treatment.
Figure 1. Hyperpigmented to flesh-colored patches in a blaschkoid distribution on the dorsal aspect of the right hand, along with hyperpigmented to flesh-colored verrucous plaques located on the second and third digits.
Figure 2. Blaschkoid distribution of macular hyperpigmentation on the back.
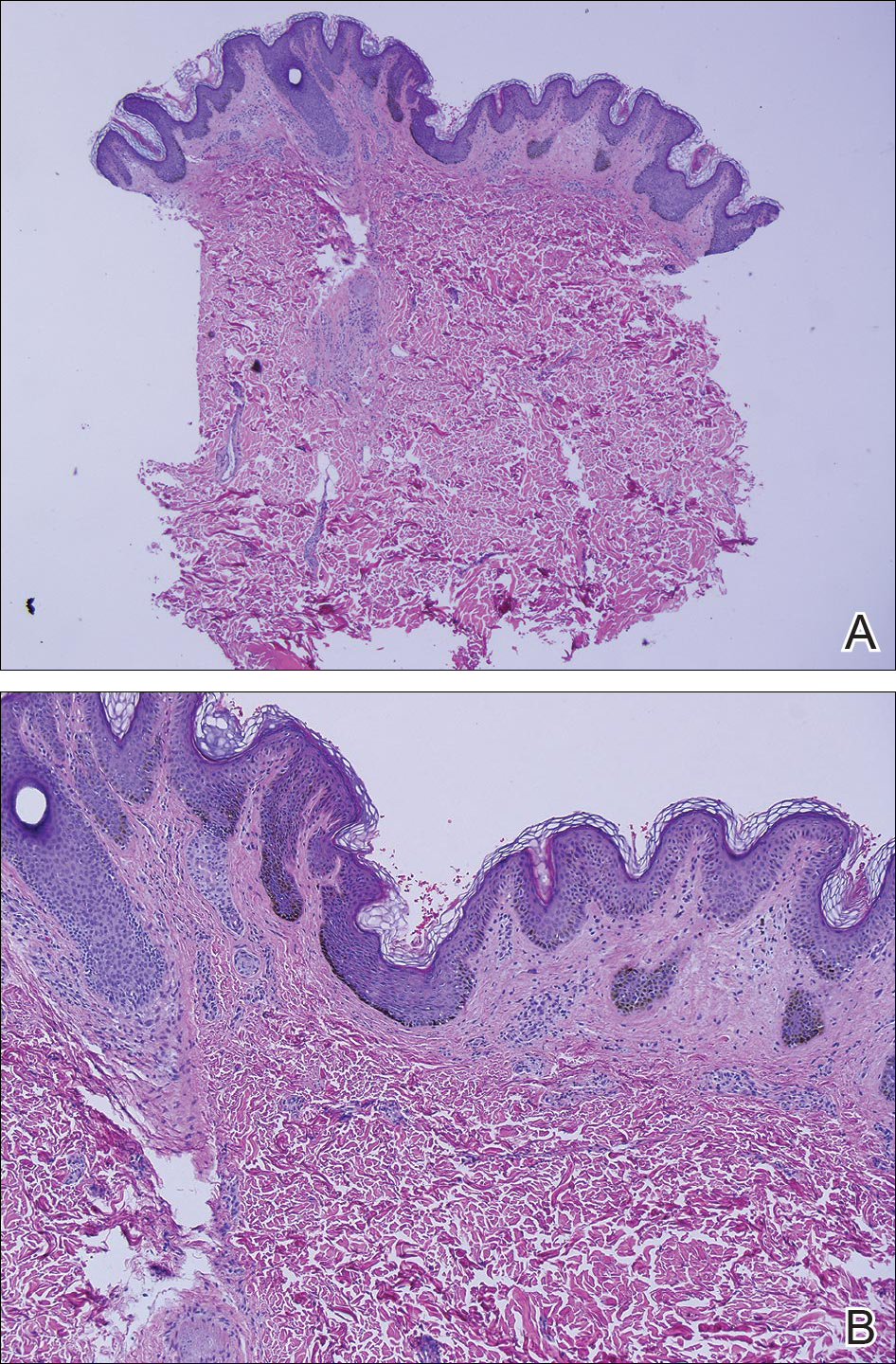
Eighteen months prior to presentation to our clinic, the patient was discovered to have hematuria on routine examination by her primary care physician. At that time, the patient underwent a workup for hematuria and a mass was discovered in the bladder via cystoscopy. A diagnosis of low-grade papillary transitional cell bladder carcinoma was made, and she underwent a partial cystectomy. No radiation or chemotherapy was required. The remainder of her medical history was only remarkable for asthma, which was well controlled with albuterol. On examination, generalized, hyperpigmented, reticulated patches, macules, and hyperpigmented verrucous plaques were distributed along the Blaschko lines, sparing the face. No limb abnormalities or dental or nail abnormalities were noted. Examination of the axillary and cervical lymph nodes was unremarkable, and no neurological abnormalities were noted. A 3-mm punch biopsy of the mid upper back was performed. Histopathology revealed papillomatous, nonorganoid, nonepidermolytic hyperplasia of the epidermis with elongated rete ridges (Figure 3), which was diagnosed as a nonorganoid nonepidermolytic epidermal nevus.
Figure 3. A 3-mm punch biopsy of the mid upper back showed epidermal papillations and nonepidermolytic hyperkeratosis on low power (A)(H&E, original magnification ×10) and higher power (B)(H&E, original magnification ×40).