Drs. Charest, Chandra, and Hamann are from HonorHealth Dermatology Residency, Scottsdale, Arizona. Dr. Hamann also is from The Contact Dermatitis Institute, Phoenix, Arizona. Dr. Hamann also is from and Dr. Salem is from the Department of Dermatology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire. Dr. LeBlanc is from the Department of Pathology and Laboratory Medicine, Dartmouth-Hitchcock Medical Center.
The authors report no conflict of interest.
Correspondence: Guy Charest, DO, HonorHealth Dermatology Residency, 7400 E Thompson Peak Pkwy, Scottsdale, AZ 85255 (gucharest@honorhealth.com).
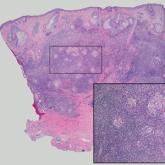
A 62-year-old man with a history of cylindromas presented to our clinic with multiple asymptomatic, 3- to 4-mm, nonmobile, dome-shaped, telangiectatic, pink papules over the parietal and vertex scalp that had been present for more than 10 years without change. Several family members had similar lesions that had not been evaluated by a physician, and there had been no genetic evaluation. Shave biopsies of several lesions were performed.
H&E, original magnifications ×40 and ×100, respectively.
The Diagnosis: Spiradenocylindroma
Shave biopsies of our patient’s lesions showed wellcircumscribed dermal nodules resembling a spiradenoma with 3 cell populations: those with lighter nuclei, darker nuclei, and scattered lymphocytes. However, the conspicuous globules of basement membrane material were reminiscent of a cylindroma. These overlapping features and the patient’s history of cylindroma were suggestive of a diagnosis of spiradenocylindroma.
Spiradenocylindroma is an uncommon dermal tumor with features that overlap with spiradenoma and cylindroma.1 It may manifest as a solitary lesion or multiple lesions and can occur sporadically or in the context of a family history. Histologically, it must be distinguished from other intradermal basaloid neoplasms including conventional cylindroma and spiradenoma, dermal duct tumor, hidradenoma, and trichoblastoma.
When patients present with multiple cylindromas, spiradenomas, or spiradenocylindromas, physicians should consider genetic testing and review of the family history to assess for cylindromatosis gene mutations or Brooke-Spiegler syndrome. Biopsy and histologic examination are important because malignant tumors can evolve from pre-existing spiradenocylindromas, cylindromas, and spiradenomas,2 with an increased risk in patients with Brooke-Spiegler syndrome.1 Our patient declined further genetic workup but continues to follow up with dermatology for monitoring of lesions.
Dermal duct tumors are morphologic variants of poromas that are derived from sweat gland lineage and usually manifest as solitary dome-shaped papules, plaques, or nodules most often seen on acral surfaces as well as the head and neck.3 Clinically, they may be indistinguishable from spiradenocylindromas and require biopsy for histologic evaluation. They can be distinguished from spiradenocylindroma by the presence of small dermal nodules composed of cuboidal cells with ample pink cytoplasm and cuticle-lined ducts (Figure 1).
FIGURE 1. Dermal duct tumors have a relatively eosinophilic appearance due to their cuboidal poroid cells that resemble epidermal keratinocytes punctuated by cuticle-lined ducts (H&E, original magnification ×100).
Trichoblastomas typically are deep-seated basaloid follicular neoplasms on the scalp with papillary mesenchyme resembling the normal fibrous sheath of the hair follicle, often replete with papillary mesenchymal bodies (Figure 2). There generally are no retraction spaces between its basaloid nests and the surrounding stroma, which is unlikely to contain mucin relative to basal cell carcinoma (BCC).4,5
FIGURE 2. Trichoblastomas have germinative follicular basaloid cells that closely resemble those of basal cell carcinoma but are deepseated tumors with papillary mesenchyme and less stromal mucin (H&E, original magnification ×100; inset, original magnification ×40).
Adenoid cystic carcinoma is a rare salivary gland tumor that can metastasize to the skin and rarely arises as a primary skin adnexal tumor. It manifests as a slowgrowing mass that can be tender to palpation.6 Histologic examination shows dermal islands with cribriform blue and pink spaces. Compared to BCC, adenoid cystic carcinoma cells are enlarged and epithelioid with relatively scarce cytoplasm (Figure 3).6,7 Adenoid cystic carcinoma can show variable growth patterns including infiltrative nests and trabeculae. Perineural invasion is common, and there is a high risk for local recurrence.7 First-line therapy usually is surgical, and postoperative radiotherapy may be required.6,7
FIGURE 3. Adenoid cystic carcinoma is composed of cribriform nests and irregular infiltrative trabeculae. Its two constituent cell populations have large ovoid nuclei with variable hyperchromasia. No papillary mesenchyme, mucinous stroma, palisading, or clefting is present at the perimeter of infiltrative nests (H&E, original magnification ×100).
Nodular BCC commonly manifests as an enlarging nonhealing lesion on sun-exposed skin and has many subtypes, typically with arborizing telangiectases on dermoscopy. Histopathologic examination of nodular BCC reveals a nest of basaloid follicular germinative cells in the dermis with peripheral palisading and a fibromyxoid stroma (Figure 4).8 Patients with Brooke-Spiegler syndrome are at increased risk for nodular BCC, which may be clinically indistinguishable from spiradenoma, cylindroma, and spiradenocylindroma, necessitating histologic assessment.
FIGURE 4. Basal cell carcinoma with nodular morphology is composed of germinative follicular basaloid cells with peripheral palisading and clefts filled with mucin (H&E, original magnification ×100).