Tumors
Back or bone pain can be a subtle early presenting symptom of cancer or tumors of the bone or bone marrow. The most common malignant bone tumors in children are osteosarcoma and Ewing sarcoma.6 Both types may present with intermittent pain or pain that worsens over weeks to months. Fever also may be present, which can lead to a misdiagnosis of osteomyelitis. Acute leukemia presenting with bone/back pain and a history of nighttime pain combined with low WBC, platelets, or hemoglobin is highly suggestive of this diagnosis. Physical examination should identify lymphadenopathy, hepatomegaly, or splenomegaly. The child with back pain in whom there is concern for mass should have laboratory evaluation, including a complete blood cell count, erythrocyte sedimentation rate, C-reactive protein, alkaline phosphatase, and lactate dehydrogenase. Plain radiographs may demonstrate “onion skinning” or the “sunburst” pattern, indicating periosteal reaction, and is highly suggestive of malignancy (Figure 4). Benign tumors of childhood may present initially as back pain as well. Osteoid osteoma is a common benign tumor which presents with pain that becomes worse at night and may respond to nonsteroidal anti-inflammatory drugs.7
Spondylolysis
Spondylolysis, also known as “pars defect,” is a unilateral or bilateral fracture of the vertebral pars interarticularis—typically of the lower lumbar vertebrae, most commonly L5. Spondylolysis occurs after repetitive microtrauma. Spondylolisthesis is the slipping of one vertebra over another one. These diagnoses should be suspected in adolescents, especially athletic patients presenting with acute low-back pain. The pain associated with these conditions often extends into the posterior thigh and is relieved by rest. Examination findings include lumbosacral tenderness, particularly with extension or lateral bending. Radiographs should include AP, lateral, and oblique views and may demonstrate fracture, displacement of the vertebrae, or the classic “Scotty dog” sign with the crack (collar) on the neck of dog (Figure 5). Treatment consists of immobilization, activity restriction, and physiotherapy. Referral to orthopedics is advised for follow-up X-rays and monitoring. If conservative treatment fails to relieve pain or if slippage progressively worsens, spinal fusion is necessary.8Pediatric Cervical Spine Clearance
Thankfully, cervical spine injuries are rare, occurring in approximately 1% of children after blunt trauma.9 Left unrecognized, however, these injuries may result in permanent neurological disability. Children younger than 8 years of age are more likely to injure the upper cervical spine (C1 to C3) than older children and adults. This is because children have relatively larger heads than bodies and weaker cervical muscles and ligaments, making the upper cervical spine more mobile. The Emergency X-Radiography Utilization Study (NEXUS) criteria have been validated in adults; however, criteria for clearing the pediatric cervical spine are poorly studied. Because of limited data, there are few evidence-based guidelines for the clearance of the pediatric cervical spine. A study in 2001 found that the NEXUS guidelines where helpful in reducing imaging in 20% of children, but due to the low numbers of infants in this study, caution is advised when applying the NEXUS criteria to children under 2 years of age.9
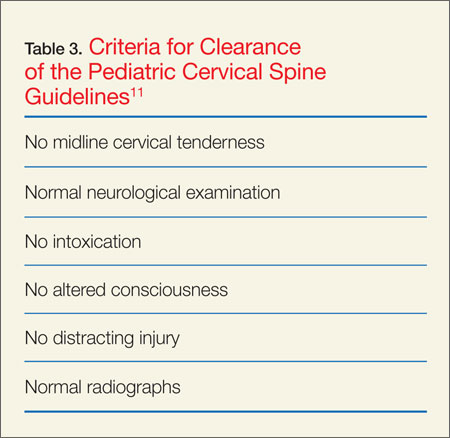
Midline posterior cervical tenderness, evidence of intoxication, altered level of consciousness, abnormal neurological examination, or distracting painful injury are indications for AP, lateral, and odontoid X-rays. After blunt trauma, if a patient is receiving an urgent computed tomography (CT) scan for another area of injury such as the head or abdomen, he or she should also receive a CT scan of the cervical spine. Additionally, those with significant mechanism of injury, focal neurological findings, significant altered level of consciousness, and/or significant posterior midline neck pain should also have a cervical spine CT scan.10 Neurosurgical service consultation is necessary in cases of abnormal cervical spine radiographs (plain films and/or CT scan), abnormal neurological examination (focal neurological findings or altered level of consciousness), or continued significant posterior midline cervical spine pain/tenderness, history, and resolution of focal neurological findings despite normal radiographs. Clearance of the cervical spine is possible if the patient has no posterior midline cervical tenderness; has a normal neurological examination; is not intoxicated; has no altered level of consciousness; has no painful distracting injury and normal radiographs; and has resolution of significant midline tenderness and/or altered level of consciousness when either one of these was the criteria that necessitated the radiographs (Table 3).11
Nonaccidental Trauma: Abuse
Orthopedic injury due to nonaccidental trauma (NAT) can be difficult to distinguish from normal childhood injuries. Identification of high-risk presentations is key in diagnosing these injuries and hopefully preventing further abuse. Femur fractures in children younger than age 1 year have a high likelihood of being nonaccidental, with between 60% to 80% of femoral shaft fractures resulting from abuse. No particular pattern of fracture is pathognomonic for NAT. The American Academy of Orthopaedic Surgeons recommends that children younger than age 36 months with a diaphyseal femur fracture be evaluated for child abuse.12