Overview
Candidates for noninvasive ventilation (NIV) most commonly present to the ED with acute respiratory failure (ARF) secondary to chronic obstructive pulmonary disease (COPD) or congestive heart-failure (CHF) exacerbations. The emergency physician (EP) must select patients appropriately, recognizing which would benefit most from NIV, as well as those with contraindications to this therapy. When indicated, early application confers benefit to the patient and can help avoid endotracheal intubation. Once therapy is initiated, clinical deterioration is still possible, and close monitoring and troubleshooting are imperative. Frequently, the clinician must make adjustments in ventilatory parameters to support the patient.
In this article, the author discusses the evidence supporting the use of NIV in appropriately selected patients with ARF, as well as review the types of NIV commonly used in the ED, the physiologic effects of positive-pressure ventilation (PPV), and how to identify and avoid common pitfalls.
Case Presentation Examples
Case 1

A 72-year-old man with a past medical history of COPD was brought to the ED by emergency medical services for evaluation of shortness of breath and wheezing. The patient’s initial oxygen (O2) saturation was 84%, which responded to bronchodilators and supplemental O2. At the time of arrival, he was somewhat somnolent, but aroused to verbal stimuli. A nonrebreather mask was placed delivering 15 L/minute of O2 with a saturation of 96%. His vital signs were: blood pressure (BP), 142/76 mm Hg, heart rate, 108 beats/minute; and respiratory rate (RR), 13 breaths/minute. A cardiac monitor revealed sinus tachycardia, and a portable chest X-ray was obtained (Figure 1). On lung examination, the patient’s breath sounds were diminished in the bases with suboptimal respiratory effort and expiratory wheezes in all lung fields. Venous blood gas measurement revealed a pH of 7.25; end-tidal carbon dioxide (CO2) was 77.
After the initial assessment, the EP considered NIV as an adjunct to improve ventilation as he suspected the patient was experiencing significant respiratory acidosis secondary to CO2 retention. The respiratory therapist suggested NIV at 12/5 before titrating down the fraction of inspired O2 (FiO2) and sought approval from the EP.
Discussion Questions: Is the above recommendation from the respiratory therapist the most appropriate therapy for this patient? What are the contraindications to this treatment and how should he be monitored to measure improvement?
Case 2

A 54-year-old woman presented to the ED for shortness of breath. On examination, she was diaphoretic and in severe distress with one- to two-word dyspnea and gasping respirations with pink-tinged sputum. Her BP was 236/158 mm Hg. A portable chest X-ray was obtained (Figure 2); rales were present with significant jugular venous distension. An electrocardiogram revealed a left-ventricular hypertrophy strain pattern but no evidence of ST-segment elevation.
During the assessment, the EP considered hypertensive emergency with resulting flash pulmonary edema as the cause of the patient’s condition; as such, he contemplated NIV to decrease the work of breathing and improve oxygenation. However, the EP had concerns regarding the preload and afterload ramifications. Although there was no respiratory therapist in the ED, the EP was able to set up the machine, but was not certain which mode of NIV or initial settings would be appropriate.
Discussion Questions: What is the protocol for proper set up to ensure a good mask fit? Once therapy is initiated, how should the EP monitor the patient? How should the EP explain this therapy to the patient and instruct her on how to work with the ventilator?
Acute-Care Application
Noninvasive ventilation refers to PPV delivered through a device such as a facemask, nasal mask, nasal plugs, or helmet. This modality was first used in the 1940s to treat respiratory failure, and its use has since grown to parallel that of mechanical ventilation.1-3 Although the application of NIV does not represent definitive airway management, this therapy has dramatically changed the care and treatment of both chronic and ARF. It serves as a significant intervention to prevent further respiratory compromise; to reverse either existing physiologic, hemodynamic, or ventilatory derangements; and to avoid endotracheal intubation.
Modes of Delivery
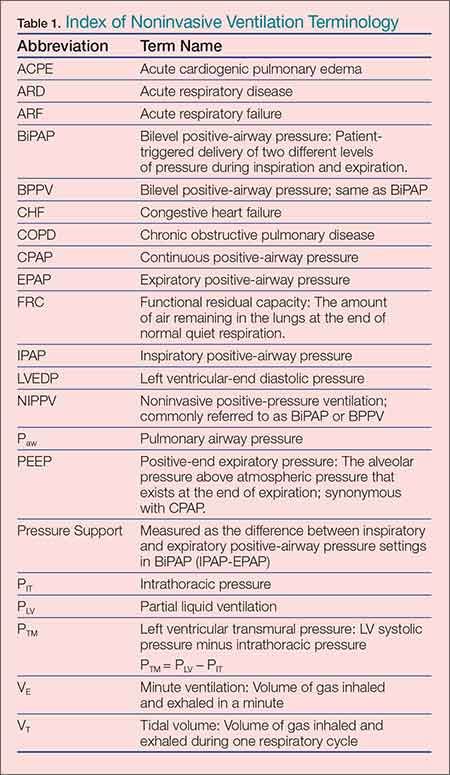
In the acute setting, NIV is typically delivered via two modes. Continuous positive-airway pressure (CPAP) is delivered regardless of the phase of respiration, and noninvasive positive-pressure ventilation (NIPPV; typically referred to as bi-level positive-airway pressure [BiPAP] or BPPV) is delivered in the inspiratory and expiratory phases of the respiratory cycle. Inspiratory positive-airway pressure (IPAP) refers to an inspiratory boost that is triggered by the negative airway pressure on inspiration in a synchronous fashion. This inspiratory pressure is fixed, but the volume delivered fluctuates based on the patient’s inspiratory effort. Expiratory positive-airway pressure (EPAP) is the delivery of constant pressure during exhalation. The difference between the IPAP and EPAP is referred to as pressure support, which serves to decrease the work of breathing and improve ventilation. (A list of commonly used abbreviations, terms, and definitions are outlined in Table 1.)