Evaluation and Management of Pancreatic Cystic Lesions
Journal of Clinical Outcomes Management. 2015 December;22(12)
References
The second iteration of guidelines put forth by an international panel of experts is perhaps the most widely accepted among pancreatologists. Published in 2012, the panel narrowed the criteria from their first guidelines (2006) regarding surgical resection of a pancreatic cyst [6,17]. Patients with a pancreatic cyst who have any of the following 3 features (or “high-risk stigmata”) warrant immediate consideration of surgical resection. These features are (1) obstructive jaundice in the setting of a head cyst, (2) presence of an enhancing solid component within the cyst, and (3) main pancreatic ductal dilation of 10 or more mm [6]. The presence of other “worrisome” features should prompt further investigation with endoscopic ultrasound (EUS) and these include (1) presentation of a cyst with pancreatitis, (2) cysts 3 cm or greater in size, (3) thickened or enhancing cyst walls, (4) nonenhancing mural nodules, and (5) tapering of the pancreatic duct with distal pancreatic atrophy ( Table 2 )[6].
The American Gastroenterological Association (AGA) recently produced guidelines in 2015 [14]. In comparison to the international consensus guidelines, there are a few key differences, which have now become a point of vigorous debate and disagreement among pancreatologists and confusion among general gastroenterologists and surgeons in the community. Where the international consensus guidelines have stricter criteria to define the appropriateness of surgery, the AGA guidelines are more liberal. AGA defined cysts appropriate for surgery as having 2 out of 3 of the following features: (1) cyst size ≥ 3 cm, (2) presence of a solid component in the cyst, and (3) dilation of the main pancreatic duct. Those having 1 out of 3 criteria were defined as needing further investigation with EUS [14]. These criteria are more relaxed and will likely lead to more surgical resections.
Another difference involves surveillance recommendations. The international consensus guidelines do not define a period when surveillance can be safely stopped. The AGA guidelines define 5 years as the period where if there is no significant change in the cyst from surveillance MRIs performed every 1 to 2 years, then surveillance can be stopped [14]. As the natural history of these cysts remain substantially uncertain, with evidence that malignant transformation occurs after 5 years, this particular recommendation by the AGA remains highly controversial [18,19]. Other differences between these 2 guidelines are summarized in Table 2 [6,14].
Until the surveillance recommendations by the AGA are validated with further studies, we generally follow the 2012 international consensus guidelines. We generally prefer MRI for initial and surveillance evaluations of pancreatic cysts. Besides the lack of radiation exposure, some studies show MRI to have better inter-reader variability [20], better resolution to show cyst communication with the main pancreatic duct [21], and better characterization of peripheral pancreatic cysts [22]. At our center, when a solid mass is suspected, a CT pancreas protocol is preferred in lieu of an MRI by our surgical team.
Case 1 Continued
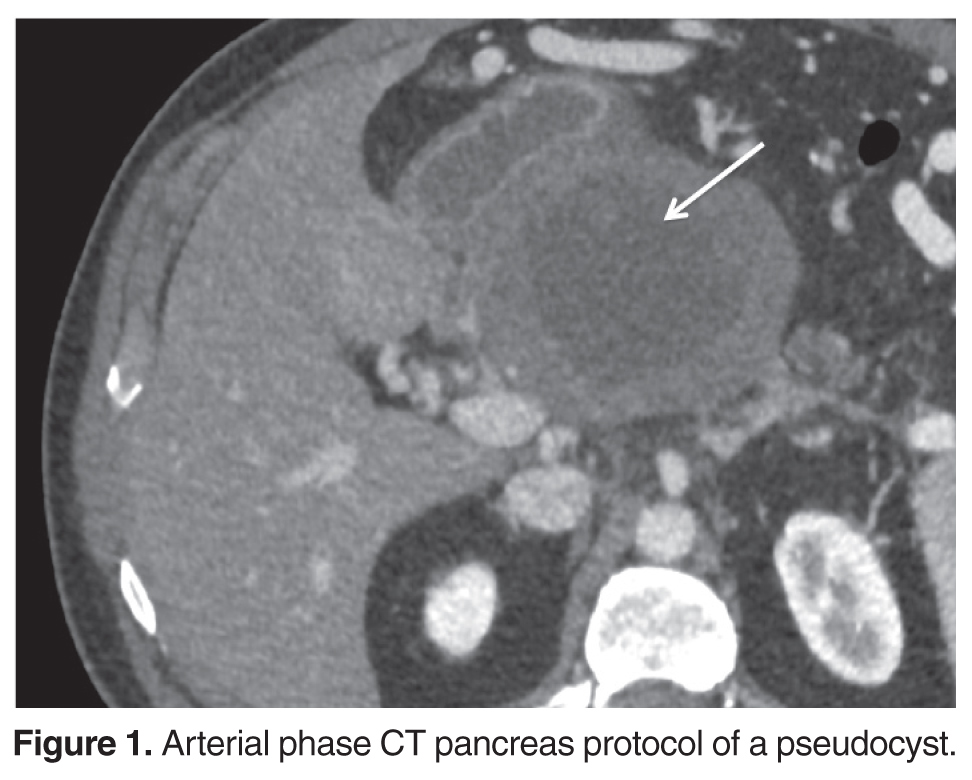
Given the smaller size and absence of high-risk stigmata or worrisome features, surveillance of his cyst was recommnded. He unfortunately did not follow up and presented 7 years later with several months of abdominal pain and esophageal reflux symptoms. A CT scan was repeated which showed that the cyst had grown to 10.7 x 8.8 x 8.9 cm with an adjacent smaller cyst ( Figure 1