Evaluation and Management of Pancreatic Cystic Lesions
Journal of Clinical Outcomes Management. 2015 December;22(12)
References
Management of pancreatic fluid collections is largely based on surgical series. Drainage procedures for pancreatic fluid collections are often undertaken for intractable symptoms or concerns of infection [8,24,25,26]. Asymptomatic pseudocysts can be safely followed. Specific techniques used for pancreatic fluid collection management vary by institutional expertise. Endoscopic drainage can be done by transpapillary stenting if main duct communication is present, or transgastric/transduodenal stenting if the cyst wall is mature and accessible by these approaches [32]. If necrosis is present this can be debrided endoscopically [33]. Laparoscopic surgical options are preferred to open approaches, and can be performed in 1 procedure where endoscopic approaches may require multiple procedures. The most common approach is to drain the cyst by creating a cyst-gastrostomy, or when not feasible a cyst-duodenostomy or cyst-jejunostomy [26,34]. Percutaneous drainage is less commonly performed and used for unstable patients as it can lead to cutaneous fistulas [34]. The best technique for intervention should be decided in the context of a multidisciplinary team. The option for conservative management should be considered as well because about 60% of those managed conservatively will have resolution in 1 year [35].
Case 2
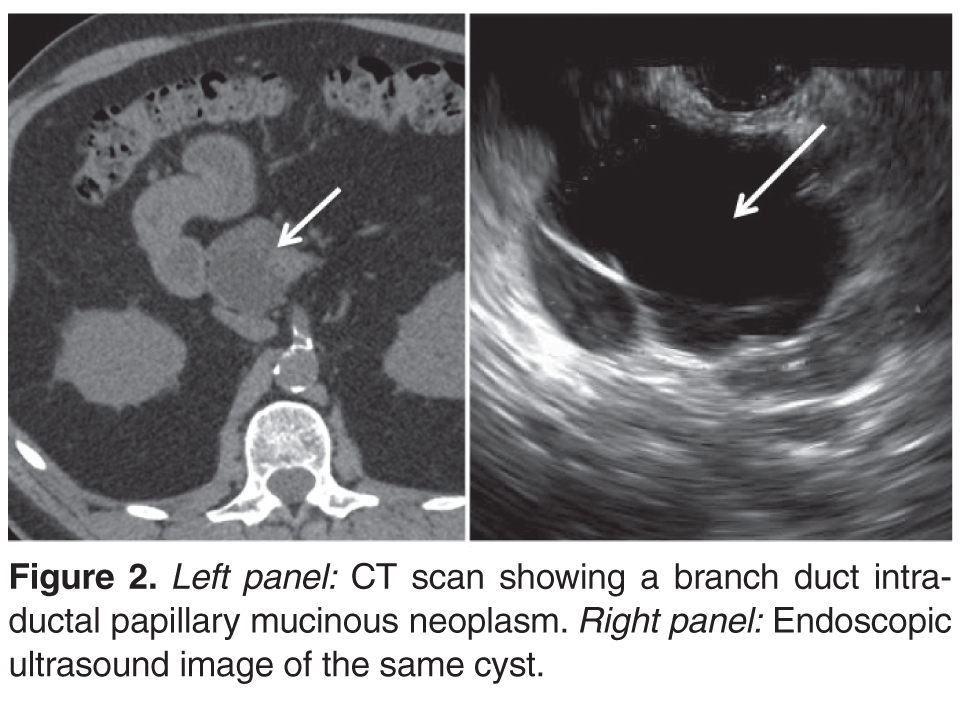
A 65-year-old male had a CT scan of the abdomen and pelvis for hematuria. While no clear source of hematuria was identified, a pancreatic cyst was described prompting a dedicated CT pancreas protocol scan. This showed a 3.4 x 4.0 x 5.5 cm multicystic lesion in the head of the pancreas with mural nodules but no dilation of the main pancreatic duct or biliary ducts ( Figure 2 ). He had no correlating symptoms and lab test results were normal.
• What is the role of endoscopic ultrasound with FNA in the diagnosis of pancreatic cysts?
While more invasive than CT or MRI, EUS provides detailed imaging to characterize relevant clinical features and allows fine needle aspiration of the cyst fluid and tissue of intra-cystic masses (Table 2) [6,14]. While MRI imaging resolution is continuing to improve [22,36,37], EUS is generally considered superior [38] for diagnosing high-risk lesions. A limitation of EUS, however, is significant inter-observer variability when compared with MRI [37,39,40].
EUS enables FNA of the cyst, which offers unique oppor-tunities for diagnosis. Cyst fluid cytology unfortunately has limited diagnostic yield, with a recent meta-analysis showing sensitivity 63%, specificity 88%, and AUC of 0.89 in differentiating mucinous from nonmucinous cysts [41]. The low sensitivity is likely because cyst fluid is paucicellular. Techniques that include targeting the cyst wall are under investigation and may improve the diagnostic yield of cytological analysis [42]. Tumor markers such as CEA have been widely used in the cyst fluid, with a value > 192 ng/mL having 63% sensitivity and 88% specificity (AUC of 0.79) for mucinous pancreatic cysts [43]. Other cyst fluid markers have been or are being developed including mutated KRAS DNA [44], mutated GNAS DNA [45,46], micro RNA [47,48], glucose [49], proteomic analysis [50], and multiple other molecules [51]. At this time, many of these markers are under investigation.
Case 2 Continued
An endoscopic ultrasound was performed and showed normal main pancreatic and common bile ducts. No intra-cystic mural nodules were observed. FNA was performed. Cytology showed “paucicellular fluid” and the cyst fluid CEA was 319 ng/mL. Having met the original consensus criteria for surgical resection [17] based on size, the presence of mural nodules, and due to suspicion for a mucinous cyst based on the CEA level, the patient underwent a Whipple procedure. The final pathology was a branch-duct IPMN with moderate dysplasia.