User login
Hospitalists ‘in exactly the right place’ to move to value-based care
Hospitalists are uniquely positioned to be agents of change in the health care system, helping to care for very sick patients as well as identifying cost-efficient ways to keep them well, Marc Harrison, MD, said in his keynote presentation Monday at HM19.

“You’re in exactly the right place in exactly the right specialty to make an enormous difference for our country, which desperately needs an upgrade in terms of how we approach keeping people well and then taking care of people when they’re sick in a superefficient as well as independent fashion,” said Dr. Harrison, president and CEO of Intermountain Healthcare, based in Salt Lake City.
Hospital medicine, hospitalists, and the health care system in general are at an inflection point, and leading change in a positive fashion is the “single core competency” attendees need as health care transitions toward value-based care. This means moving away from a volume-based care model and asking hard questions about whether providers are doing the right things for patients, said Dr. Harrison at the Annual Conference of the Society of Hospital Medicine.
“It’s going to require humility, risk taking, and a desire to truly serve others if we’re going to change the paradigm for health care delivery,” he added.
About one-third of health care that providers deliver is redundant, which costs the United States approximately $1 trillion per year, Dr. Harrison noted. “There’s plenty of money in American health care; it’s just being misspent.”
Health care is “expensive, not consumer centric, and provides uneven quality,” which has spurred businesses like Google and Amazon to try to change the model. Other trends in the health care industry are an increased focus on mergers and acquisitions, negative growth outlook for hospitals, rural hospitals facing closure, and consumers increasingly demanding transparency in health care in such places as their hospital bills.
“We need to be on our front foot” to adapt to these changes, said Dr. Harrison, which means changing how money is spent in U.S. health care. There is currently a disparity: 10% of a person’s health care comes from hospitals and clinics, while 90% of money spent in U.S. health care is on that 10%. Spending should instead be inverted, focused on population-based health initiatives such as addressing social issues surrounding housing, transportation, and food security.
A crisis is coming for providers and health systems that continue to focus on volume-based care models instead of making hard changes to value-based care, said Dr. Harrison. Population-based health initiatives that should be implemented include lowering the cost of care by shifting to outpatient care models and lowering insurance premiums.
“It doesn’t matter how technically good you are if people can’t afford what you’re doing,” he said.
Population-based health initiatives also should be modernized to care upstream, fixing the cause of health problems rather than treating the symptoms. The goal, said Dr. Harrison, is a system with end-to-end seamless care, in which providers understand patients’ goals, are intentional about keeping their patients well, and can “ensure seamless handoff” to other caregivers.
Dr. Harrison said the future of hospital medicine is providing acute care in this way, and attendees are uniquely suited to take care of patients not only in the hospital but also at home, as well as providing consultations with colleagues in care environments without hospitalist programs.
“You’re in the absolute perfect place to keep patients in the least-restrictive, least-expensive environment where they can receive superb care,” he said.
Hospitalists are uniquely positioned to be agents of change in the health care system, helping to care for very sick patients as well as identifying cost-efficient ways to keep them well, Marc Harrison, MD, said in his keynote presentation Monday at HM19.
“You’re in exactly the right place in exactly the right specialty to make an enormous difference for our country, which desperately needs an upgrade in terms of how we approach keeping people well and then taking care of people when they’re sick in a superefficient as well as independent fashion,” said Dr. Harrison, president and CEO of Intermountain Healthcare, based in Salt Lake City.
Hospital medicine, hospitalists, and the health care system in general are at an inflection point, and leading change in a positive fashion is the “single core competency” attendees need as health care transitions toward value-based care. This means moving away from a volume-based care model and asking hard questions about whether providers are doing the right things for patients, said Dr. Harrison at the Annual Conference of the Society of Hospital Medicine.
“It’s going to require humility, risk taking, and a desire to truly serve others if we’re going to change the paradigm for health care delivery,” he added.
About one-third of health care that providers deliver is redundant, which costs the United States approximately $1 trillion per year, Dr. Harrison noted. “There’s plenty of money in American health care; it’s just being misspent.”
Health care is “expensive, not consumer centric, and provides uneven quality,” which has spurred businesses like Google and Amazon to try to change the model. Other trends in the health care industry are an increased focus on mergers and acquisitions, negative growth outlook for hospitals, rural hospitals facing closure, and consumers increasingly demanding transparency in health care in such places as their hospital bills.
“We need to be on our front foot” to adapt to these changes, said Dr. Harrison, which means changing how money is spent in U.S. health care. There is currently a disparity: 10% of a person’s health care comes from hospitals and clinics, while 90% of money spent in U.S. health care is on that 10%. Spending should instead be inverted, focused on population-based health initiatives such as addressing social issues surrounding housing, transportation, and food security.
A crisis is coming for providers and health systems that continue to focus on volume-based care models instead of making hard changes to value-based care, said Dr. Harrison. Population-based health initiatives that should be implemented include lowering the cost of care by shifting to outpatient care models and lowering insurance premiums.
“It doesn’t matter how technically good you are if people can’t afford what you’re doing,” he said.
Population-based health initiatives also should be modernized to care upstream, fixing the cause of health problems rather than treating the symptoms. The goal, said Dr. Harrison, is a system with end-to-end seamless care, in which providers understand patients’ goals, are intentional about keeping their patients well, and can “ensure seamless handoff” to other caregivers.
Dr. Harrison said the future of hospital medicine is providing acute care in this way, and attendees are uniquely suited to take care of patients not only in the hospital but also at home, as well as providing consultations with colleagues in care environments without hospitalist programs.
“You’re in the absolute perfect place to keep patients in the least-restrictive, least-expensive environment where they can receive superb care,” he said.
Hospitalists are uniquely positioned to be agents of change in the health care system, helping to care for very sick patients as well as identifying cost-efficient ways to keep them well, Marc Harrison, MD, said in his keynote presentation Monday at HM19.
“You’re in exactly the right place in exactly the right specialty to make an enormous difference for our country, which desperately needs an upgrade in terms of how we approach keeping people well and then taking care of people when they’re sick in a superefficient as well as independent fashion,” said Dr. Harrison, president and CEO of Intermountain Healthcare, based in Salt Lake City.
Hospital medicine, hospitalists, and the health care system in general are at an inflection point, and leading change in a positive fashion is the “single core competency” attendees need as health care transitions toward value-based care. This means moving away from a volume-based care model and asking hard questions about whether providers are doing the right things for patients, said Dr. Harrison at the Annual Conference of the Society of Hospital Medicine.
“It’s going to require humility, risk taking, and a desire to truly serve others if we’re going to change the paradigm for health care delivery,” he added.
About one-third of health care that providers deliver is redundant, which costs the United States approximately $1 trillion per year, Dr. Harrison noted. “There’s plenty of money in American health care; it’s just being misspent.”
Health care is “expensive, not consumer centric, and provides uneven quality,” which has spurred businesses like Google and Amazon to try to change the model. Other trends in the health care industry are an increased focus on mergers and acquisitions, negative growth outlook for hospitals, rural hospitals facing closure, and consumers increasingly demanding transparency in health care in such places as their hospital bills.
“We need to be on our front foot” to adapt to these changes, said Dr. Harrison, which means changing how money is spent in U.S. health care. There is currently a disparity: 10% of a person’s health care comes from hospitals and clinics, while 90% of money spent in U.S. health care is on that 10%. Spending should instead be inverted, focused on population-based health initiatives such as addressing social issues surrounding housing, transportation, and food security.
A crisis is coming for providers and health systems that continue to focus on volume-based care models instead of making hard changes to value-based care, said Dr. Harrison. Population-based health initiatives that should be implemented include lowering the cost of care by shifting to outpatient care models and lowering insurance premiums.
“It doesn’t matter how technically good you are if people can’t afford what you’re doing,” he said.
Population-based health initiatives also should be modernized to care upstream, fixing the cause of health problems rather than treating the symptoms. The goal, said Dr. Harrison, is a system with end-to-end seamless care, in which providers understand patients’ goals, are intentional about keeping their patients well, and can “ensure seamless handoff” to other caregivers.
Dr. Harrison said the future of hospital medicine is providing acute care in this way, and attendees are uniquely suited to take care of patients not only in the hospital but also at home, as well as providing consultations with colleagues in care environments without hospitalist programs.
“You’re in the absolute perfect place to keep patients in the least-restrictive, least-expensive environment where they can receive superb care,” he said.
Hospital medicine grows globally
Hospital medicine is growing in popularity in some foreign countries, speakers said during Monday afternoon’s session, “International Hospital Medicine in the United Arab Emirates, Brazil and Holland.” The presenters discussed some of the history of hospital medicine in each of those countries as well as some current challenges.

Hospital medicine in the Netherlands started in about 2012, said Marjolein de Boom, MD, a hospitalist at Haaglanden Medical Centre. The country has its own 3-year training program for hospitalists, who first started to work in hospitals in the country in 2015. “It’s a relatively new and young specialty,” said Dr. de Boom, with 39 hospitalists in the country working in 8 of the 80 Dutch hospitals. Another 25 or so hospitalists are in training, “so it’s a growing profession,” she said. A Dutch chapter of SHM has been in place since 2017.
Hospitals in the Netherlands permit physicians to serve as hospitalists in different specialties depending on their needs. For example, Dr. de Boom works in the oncology department, as well as the surgical and trauma surgery units. One challenge has been to get more physicians interested in the hospitalist program because it’s newer and not as well-known, she said.
Hospital medicine in the United Arab Emirates also is a newer concept. The American model of hospital medicine was first introduced to the region in 2014 by the Cleveland Clinic in Abu Dhabi, said Mahmoud Al-Hawamdeh, MD, MBA, SFHM, FACP, chair of hospital medicine at the medical center. “Before that, inpatient hospital care was done by traditional family and internal medicine physicians, general practitioners, and residents,” he said.
There are 43 hospitalists at Cleveland Clinic, Abu Dhabi, said Dr. Al-Hawamdeh. They cover about 50%-60% of inpatient services, as well as handle admissions for vascular surgery, ophthalmology, and some general services; they also comanage postcardiac surgery care, he said. “It has been a tremendous success to implement hospital medicine in the care for the inpatient with improved quality metrics, reduced length of stay, and improved patient satisfaction.”
However, there are some challenges, such as educating patients and families about the role of hospitalists, cultural barriers, and the lack of a postdischarge follow-up network and institutions such as skilled nursing facilities. Dr. Al-Hawamdeh worked with physicians from Johns Hopkins Aramco Healthcare and Hamad Medical Corporation to establish an SHM Middle East chapter in 2016.
In Brazil, hospital medicine started to take hold in 2004, said Guilherme Barcellos, MD, SFHM. At that time, just a few doctors were true hospitalists. Dr. Barcellos helped create two hospitalist societies in the country. Hospitalists balancing multiple jobs is still very common, but decreasing, he said, while hospital employment and medical group participation is increasing.
“It was a high-pressure environment, crying out for efficiency, that drove forward Brazilian hospital medicine,” Dr. Barcellos said, “together with new reimbursement models, surgical redesigns, primary care recognition and structure.”
Some challenges remain in Brazil as well, he said. Fancy private hospitals announce they have hospitalists when they may not. In addition, the role of generalists and subspecialists, and the role of certifications, is not always clear. But hospitalists are gaining a foothold, participating in a Choosing Wisely initiative in the country and organizing several conferences.
Hospital medicine is growing in popularity in some foreign countries, speakers said during Monday afternoon’s session, “International Hospital Medicine in the United Arab Emirates, Brazil and Holland.” The presenters discussed some of the history of hospital medicine in each of those countries as well as some current challenges.
Hospital medicine in the Netherlands started in about 2012, said Marjolein de Boom, MD, a hospitalist at Haaglanden Medical Centre. The country has its own 3-year training program for hospitalists, who first started to work in hospitals in the country in 2015. “It’s a relatively new and young specialty,” said Dr. de Boom, with 39 hospitalists in the country working in 8 of the 80 Dutch hospitals. Another 25 or so hospitalists are in training, “so it’s a growing profession,” she said. A Dutch chapter of SHM has been in place since 2017.
Hospitals in the Netherlands permit physicians to serve as hospitalists in different specialties depending on their needs. For example, Dr. de Boom works in the oncology department, as well as the surgical and trauma surgery units. One challenge has been to get more physicians interested in the hospitalist program because it’s newer and not as well-known, she said.
Hospital medicine in the United Arab Emirates also is a newer concept. The American model of hospital medicine was first introduced to the region in 2014 by the Cleveland Clinic in Abu Dhabi, said Mahmoud Al-Hawamdeh, MD, MBA, SFHM, FACP, chair of hospital medicine at the medical center. “Before that, inpatient hospital care was done by traditional family and internal medicine physicians, general practitioners, and residents,” he said.
There are 43 hospitalists at Cleveland Clinic, Abu Dhabi, said Dr. Al-Hawamdeh. They cover about 50%-60% of inpatient services, as well as handle admissions for vascular surgery, ophthalmology, and some general services; they also comanage postcardiac surgery care, he said. “It has been a tremendous success to implement hospital medicine in the care for the inpatient with improved quality metrics, reduced length of stay, and improved patient satisfaction.”
However, there are some challenges, such as educating patients and families about the role of hospitalists, cultural barriers, and the lack of a postdischarge follow-up network and institutions such as skilled nursing facilities. Dr. Al-Hawamdeh worked with physicians from Johns Hopkins Aramco Healthcare and Hamad Medical Corporation to establish an SHM Middle East chapter in 2016.
In Brazil, hospital medicine started to take hold in 2004, said Guilherme Barcellos, MD, SFHM. At that time, just a few doctors were true hospitalists. Dr. Barcellos helped create two hospitalist societies in the country. Hospitalists balancing multiple jobs is still very common, but decreasing, he said, while hospital employment and medical group participation is increasing.
“It was a high-pressure environment, crying out for efficiency, that drove forward Brazilian hospital medicine,” Dr. Barcellos said, “together with new reimbursement models, surgical redesigns, primary care recognition and structure.”
Some challenges remain in Brazil as well, he said. Fancy private hospitals announce they have hospitalists when they may not. In addition, the role of generalists and subspecialists, and the role of certifications, is not always clear. But hospitalists are gaining a foothold, participating in a Choosing Wisely initiative in the country and organizing several conferences.
Hospital medicine is growing in popularity in some foreign countries, speakers said during Monday afternoon’s session, “International Hospital Medicine in the United Arab Emirates, Brazil and Holland.” The presenters discussed some of the history of hospital medicine in each of those countries as well as some current challenges.
Hospital medicine in the Netherlands started in about 2012, said Marjolein de Boom, MD, a hospitalist at Haaglanden Medical Centre. The country has its own 3-year training program for hospitalists, who first started to work in hospitals in the country in 2015. “It’s a relatively new and young specialty,” said Dr. de Boom, with 39 hospitalists in the country working in 8 of the 80 Dutch hospitals. Another 25 or so hospitalists are in training, “so it’s a growing profession,” she said. A Dutch chapter of SHM has been in place since 2017.
Hospitals in the Netherlands permit physicians to serve as hospitalists in different specialties depending on their needs. For example, Dr. de Boom works in the oncology department, as well as the surgical and trauma surgery units. One challenge has been to get more physicians interested in the hospitalist program because it’s newer and not as well-known, she said.
Hospital medicine in the United Arab Emirates also is a newer concept. The American model of hospital medicine was first introduced to the region in 2014 by the Cleveland Clinic in Abu Dhabi, said Mahmoud Al-Hawamdeh, MD, MBA, SFHM, FACP, chair of hospital medicine at the medical center. “Before that, inpatient hospital care was done by traditional family and internal medicine physicians, general practitioners, and residents,” he said.
There are 43 hospitalists at Cleveland Clinic, Abu Dhabi, said Dr. Al-Hawamdeh. They cover about 50%-60% of inpatient services, as well as handle admissions for vascular surgery, ophthalmology, and some general services; they also comanage postcardiac surgery care, he said. “It has been a tremendous success to implement hospital medicine in the care for the inpatient with improved quality metrics, reduced length of stay, and improved patient satisfaction.”
However, there are some challenges, such as educating patients and families about the role of hospitalists, cultural barriers, and the lack of a postdischarge follow-up network and institutions such as skilled nursing facilities. Dr. Al-Hawamdeh worked with physicians from Johns Hopkins Aramco Healthcare and Hamad Medical Corporation to establish an SHM Middle East chapter in 2016.
In Brazil, hospital medicine started to take hold in 2004, said Guilherme Barcellos, MD, SFHM. At that time, just a few doctors were true hospitalists. Dr. Barcellos helped create two hospitalist societies in the country. Hospitalists balancing multiple jobs is still very common, but decreasing, he said, while hospital employment and medical group participation is increasing.
“It was a high-pressure environment, crying out for efficiency, that drove forward Brazilian hospital medicine,” Dr. Barcellos said, “together with new reimbursement models, surgical redesigns, primary care recognition and structure.”
Some challenges remain in Brazil as well, he said. Fancy private hospitals announce they have hospitalists when they may not. In addition, the role of generalists and subspecialists, and the role of certifications, is not always clear. But hospitalists are gaining a foothold, participating in a Choosing Wisely initiative in the country and organizing several conferences.

In transgender care, questions are the answer
New York OBGYN Zoe I. Rodriguez, MD, a pioneer in the care of transgender people, has witnessed a remarkable evolution in medicine.

Years ago, providers knew little to nothing about the unique needs of transgender patients. Now, Dr. Rodriguez said, “there’s tremendous interest in being able to competently treat and address transgender individuals.”
But increased awareness has come with a dose of worry. Providers are often afraid they’ll say or do the wrong thing.
Dr. Rodriguez, who is an assistant professor at the Icahn School of Medicine at Mount Sinai, New York, will help hospitalists gain confidence in treating transgender patients at an HM19 session on Tuesday. “I hope to eliminate this element of fear,” she said. “It’s just really about treating people with respect and dignity and having the knowledge to care for them appropriately.”
The United States is home to an estimated 1.4 million transgender people, and every one has a preferred name and preferred pronouns. It’s crucial for physicians to understand name and pronoun preferences and use them, Dr. Rodriguez said.
At her practice, an intake form asks patients how they wish to be addressed. “I know this information by the time I walk into the exam room,” she said.
For hospitalists, she said, getting this information beforehand may not be possible. In that case, she said, ask questions of the patient and don’t be afraid to get it wrong.
“Mistakes happen all the time,” Dr. Rodriguez said. “People will correct you if you misgender them or call them other than their preferred name. As long as the mistakes are not willful, apologize and move on.”
It’s also important to understand the special needs that transgender patients may – or may not – have. For example, not every transgender patient takes hormones. Even if a patient does, the hormones may not affect as many body processes as you might assume, Dr. Rodriguez said.
Also, not every transgender person has had surgery. However, it can be helpful to understand what surgery entails. “If they get their surgery done in Thailand, a popular destination, and they need treatment in Topeka for an issue related to their surgery, it would be good for the hospitalist to understand what’s done during the surgery.”
In her session, Dr. Rodriguez will also talk about creating an LGBT-friendly environment. “These patients are already feeling very vulnerable and marginalized within these vast health systems,” she said. “It makes a big difference to know that someone is there and gets it.”
Dr. Rodriguez also plans to emphasize the importance of staying aware and up to date about transgender issues. “It’s a continuum,” she said. “There will be more evolution as people come up with new terminologies and words to describe their gender expression and identity. It will be crucially important for physicians to be aware and respectful.”
What Hospitalists Need to Know About Caring for Transgender Patients
Tuesday, 3:50 - 4:30 p.m.
Maryland A/1-3
New York OBGYN Zoe I. Rodriguez, MD, a pioneer in the care of transgender people, has witnessed a remarkable evolution in medicine.
Years ago, providers knew little to nothing about the unique needs of transgender patients. Now, Dr. Rodriguez said, “there’s tremendous interest in being able to competently treat and address transgender individuals.”
But increased awareness has come with a dose of worry. Providers are often afraid they’ll say or do the wrong thing.
Dr. Rodriguez, who is an assistant professor at the Icahn School of Medicine at Mount Sinai, New York, will help hospitalists gain confidence in treating transgender patients at an HM19 session on Tuesday. “I hope to eliminate this element of fear,” she said. “It’s just really about treating people with respect and dignity and having the knowledge to care for them appropriately.”
The United States is home to an estimated 1.4 million transgender people, and every one has a preferred name and preferred pronouns. It’s crucial for physicians to understand name and pronoun preferences and use them, Dr. Rodriguez said.
At her practice, an intake form asks patients how they wish to be addressed. “I know this information by the time I walk into the exam room,” she said.
For hospitalists, she said, getting this information beforehand may not be possible. In that case, she said, ask questions of the patient and don’t be afraid to get it wrong.
“Mistakes happen all the time,” Dr. Rodriguez said. “People will correct you if you misgender them or call them other than their preferred name. As long as the mistakes are not willful, apologize and move on.”
It’s also important to understand the special needs that transgender patients may – or may not – have. For example, not every transgender patient takes hormones. Even if a patient does, the hormones may not affect as many body processes as you might assume, Dr. Rodriguez said.
Also, not every transgender person has had surgery. However, it can be helpful to understand what surgery entails. “If they get their surgery done in Thailand, a popular destination, and they need treatment in Topeka for an issue related to their surgery, it would be good for the hospitalist to understand what’s done during the surgery.”
In her session, Dr. Rodriguez will also talk about creating an LGBT-friendly environment. “These patients are already feeling very vulnerable and marginalized within these vast health systems,” she said. “It makes a big difference to know that someone is there and gets it.”
Dr. Rodriguez also plans to emphasize the importance of staying aware and up to date about transgender issues. “It’s a continuum,” she said. “There will be more evolution as people come up with new terminologies and words to describe their gender expression and identity. It will be crucially important for physicians to be aware and respectful.”
What Hospitalists Need to Know About Caring for Transgender Patients
Tuesday, 3:50 - 4:30 p.m.
Maryland A/1-3
New York OBGYN Zoe I. Rodriguez, MD, a pioneer in the care of transgender people, has witnessed a remarkable evolution in medicine.
Years ago, providers knew little to nothing about the unique needs of transgender patients. Now, Dr. Rodriguez said, “there’s tremendous interest in being able to competently treat and address transgender individuals.”
But increased awareness has come with a dose of worry. Providers are often afraid they’ll say or do the wrong thing.
Dr. Rodriguez, who is an assistant professor at the Icahn School of Medicine at Mount Sinai, New York, will help hospitalists gain confidence in treating transgender patients at an HM19 session on Tuesday. “I hope to eliminate this element of fear,” she said. “It’s just really about treating people with respect and dignity and having the knowledge to care for them appropriately.”
The United States is home to an estimated 1.4 million transgender people, and every one has a preferred name and preferred pronouns. It’s crucial for physicians to understand name and pronoun preferences and use them, Dr. Rodriguez said.
At her practice, an intake form asks patients how they wish to be addressed. “I know this information by the time I walk into the exam room,” she said.
For hospitalists, she said, getting this information beforehand may not be possible. In that case, she said, ask questions of the patient and don’t be afraid to get it wrong.
“Mistakes happen all the time,” Dr. Rodriguez said. “People will correct you if you misgender them or call them other than their preferred name. As long as the mistakes are not willful, apologize and move on.”
It’s also important to understand the special needs that transgender patients may – or may not – have. For example, not every transgender patient takes hormones. Even if a patient does, the hormones may not affect as many body processes as you might assume, Dr. Rodriguez said.
Also, not every transgender person has had surgery. However, it can be helpful to understand what surgery entails. “If they get their surgery done in Thailand, a popular destination, and they need treatment in Topeka for an issue related to their surgery, it would be good for the hospitalist to understand what’s done during the surgery.”
In her session, Dr. Rodriguez will also talk about creating an LGBT-friendly environment. “These patients are already feeling very vulnerable and marginalized within these vast health systems,” she said. “It makes a big difference to know that someone is there and gets it.”
Dr. Rodriguez also plans to emphasize the importance of staying aware and up to date about transgender issues. “It’s a continuum,” she said. “There will be more evolution as people come up with new terminologies and words to describe their gender expression and identity. It will be crucially important for physicians to be aware and respectful.”
What Hospitalists Need to Know About Caring for Transgender Patients
Tuesday, 3:50 - 4:30 p.m.
Maryland A/1-3
‘Update in HM’ highlights top research
When Christopher Moriates, MD, SFHM, and Carrie Herzke, MD, SFHM, accepted the opportunity to present the “Update in Hospital Medicine” session at HM19, it was a big moment for both of them.
Not only will they headline one of the most popular sessions at the Annual Conference, but they also will be giving a talk on stage together for the first time. The possibility that it could all go wrong in front of more than 5,000 attendees at HM19 certainly crossed their minds.
“No matter what, it’ll be fun,” said Dr. Moriates, assistant dean for health care value at the University of Texas at Austin.
The aim of Tuesday afternoon’s session is to inform busy hospitalists of what they might have missed over the past year by highlighting the most important papers, from multiple specialties, that affect hospital medicine.
The two presenters may be familiar to hospitalists: Dr. Herzke, associate vice chair for clinical affairs in the department of medicine at Johns Hopkins Medicine in Baltimore, is a member of the SHM Academic Committee, the SHM Mentoring Subcommittee, and the Annual Conference Committee. Dr. Moriates is a regular contributor to The Hospital Leader, the official blog of SHM, and also has a personal connection to the “Update in Hospital Medicine” session.
“I watched with awe as my mentor, Michelle Mourad, MD, presented ‘Update in Hospital Medicine’ on the big stage at National Harbor in 2013,” Dr. Moriates said. “It is hard to imagine that I will be following her footsteps onto that same stage this year.”
Dr. Moriates and Dr. Herzke have spent months preparing for their presentation: Together, they have pored through a year’s worth of literature, narrowing down hundreds of studies to bring attendees the Top 20 papers with an impact on hospital medicine for the session. They each collected articles throughout the year, checking in regularly to outline the themes and rank papers for the session. In January, Dr. Moriates and Dr. Herzke reviewed all the articles they had collected, finalizing the major themes and highlights for the Update.
“The harder part was dropping a few of the articles we had selected in order to make it under an hour,” he said. “We tried to come up with the highlights that all hospitalists should know about, which are most likely to inform their practices over the coming year. And so, if you haven’t picked up a journal in a year, hopefully within an hour, Carrie and I can give you a quick download.”
Attendees familiar with “Update in Hospital Medicine” also will know that the exact details of what is being presented are secret. It is one of the few sessions at HM19 where slides are not published beforehand on the official Annual Conference app. The only way to know the details of the top studies is to attend the session.
“You have to be there to find out,” Dr. Moriates said.
But curiosity should not be the only reason for hospitalists to attend. Dr. Herzke said this year’s “Update in Hospital Medicine” session holds some practice pearls that may surprise attendees.
“We picked out some studies that we think should make people question common practices and consider making changes to how they practice medicine at their home institution, or their home hospital,” she said.
“It’s fair to say there were a number of studies this year that questioned conventional practices or put forth clear evidence that suggests we should be doing things differently in the hospital than the way we currently are doing them, across a number of scenarios,” Dr. Moriates said.
Attendees can expect studies in the fields of infectious disease, cardiology, and hematology to make the Top 20 list of best papers for the session. However, the challenge is always to present clinical pearls that apply to all hospitalists, regardless of where they practice.
“I think one thing about hospitalists is that our practices are very broad based, and we have to be up to date in lots of different fields,” Dr. Moriates said. “And so, we will cover the top literature across an array of fields matching the breadth and diversity of the patients that we take care of as hospitalists.”
Dr. Moriates and Dr. Herzke had no relevant financial conflicts.
Update in Hospital Medicine
Tuesday, 1:00 – 2:00 p.m.
Potomac ABCD
When Christopher Moriates, MD, SFHM, and Carrie Herzke, MD, SFHM, accepted the opportunity to present the “Update in Hospital Medicine” session at HM19, it was a big moment for both of them.
Not only will they headline one of the most popular sessions at the Annual Conference, but they also will be giving a talk on stage together for the first time. The possibility that it could all go wrong in front of more than 5,000 attendees at HM19 certainly crossed their minds.
“No matter what, it’ll be fun,” said Dr. Moriates, assistant dean for health care value at the University of Texas at Austin.
The aim of Tuesday afternoon’s session is to inform busy hospitalists of what they might have missed over the past year by highlighting the most important papers, from multiple specialties, that affect hospital medicine.
The two presenters may be familiar to hospitalists: Dr. Herzke, associate vice chair for clinical affairs in the department of medicine at Johns Hopkins Medicine in Baltimore, is a member of the SHM Academic Committee, the SHM Mentoring Subcommittee, and the Annual Conference Committee. Dr. Moriates is a regular contributor to The Hospital Leader, the official blog of SHM, and also has a personal connection to the “Update in Hospital Medicine” session.
“I watched with awe as my mentor, Michelle Mourad, MD, presented ‘Update in Hospital Medicine’ on the big stage at National Harbor in 2013,” Dr. Moriates said. “It is hard to imagine that I will be following her footsteps onto that same stage this year.”
Dr. Moriates and Dr. Herzke have spent months preparing for their presentation: Together, they have pored through a year’s worth of literature, narrowing down hundreds of studies to bring attendees the Top 20 papers with an impact on hospital medicine for the session. They each collected articles throughout the year, checking in regularly to outline the themes and rank papers for the session. In January, Dr. Moriates and Dr. Herzke reviewed all the articles they had collected, finalizing the major themes and highlights for the Update.
“The harder part was dropping a few of the articles we had selected in order to make it under an hour,” he said. “We tried to come up with the highlights that all hospitalists should know about, which are most likely to inform their practices over the coming year. And so, if you haven’t picked up a journal in a year, hopefully within an hour, Carrie and I can give you a quick download.”
Attendees familiar with “Update in Hospital Medicine” also will know that the exact details of what is being presented are secret. It is one of the few sessions at HM19 where slides are not published beforehand on the official Annual Conference app. The only way to know the details of the top studies is to attend the session.
“You have to be there to find out,” Dr. Moriates said.
But curiosity should not be the only reason for hospitalists to attend. Dr. Herzke said this year’s “Update in Hospital Medicine” session holds some practice pearls that may surprise attendees.
“We picked out some studies that we think should make people question common practices and consider making changes to how they practice medicine at their home institution, or their home hospital,” she said.
“It’s fair to say there were a number of studies this year that questioned conventional practices or put forth clear evidence that suggests we should be doing things differently in the hospital than the way we currently are doing them, across a number of scenarios,” Dr. Moriates said.
Attendees can expect studies in the fields of infectious disease, cardiology, and hematology to make the Top 20 list of best papers for the session. However, the challenge is always to present clinical pearls that apply to all hospitalists, regardless of where they practice.
“I think one thing about hospitalists is that our practices are very broad based, and we have to be up to date in lots of different fields,” Dr. Moriates said. “And so, we will cover the top literature across an array of fields matching the breadth and diversity of the patients that we take care of as hospitalists.”
Dr. Moriates and Dr. Herzke had no relevant financial conflicts.
Update in Hospital Medicine
Tuesday, 1:00 – 2:00 p.m.
Potomac ABCD
When Christopher Moriates, MD, SFHM, and Carrie Herzke, MD, SFHM, accepted the opportunity to present the “Update in Hospital Medicine” session at HM19, it was a big moment for both of them.
Not only will they headline one of the most popular sessions at the Annual Conference, but they also will be giving a talk on stage together for the first time. The possibility that it could all go wrong in front of more than 5,000 attendees at HM19 certainly crossed their minds.
“No matter what, it’ll be fun,” said Dr. Moriates, assistant dean for health care value at the University of Texas at Austin.
The aim of Tuesday afternoon’s session is to inform busy hospitalists of what they might have missed over the past year by highlighting the most important papers, from multiple specialties, that affect hospital medicine.
The two presenters may be familiar to hospitalists: Dr. Herzke, associate vice chair for clinical affairs in the department of medicine at Johns Hopkins Medicine in Baltimore, is a member of the SHM Academic Committee, the SHM Mentoring Subcommittee, and the Annual Conference Committee. Dr. Moriates is a regular contributor to The Hospital Leader, the official blog of SHM, and also has a personal connection to the “Update in Hospital Medicine” session.
“I watched with awe as my mentor, Michelle Mourad, MD, presented ‘Update in Hospital Medicine’ on the big stage at National Harbor in 2013,” Dr. Moriates said. “It is hard to imagine that I will be following her footsteps onto that same stage this year.”
Dr. Moriates and Dr. Herzke have spent months preparing for their presentation: Together, they have pored through a year’s worth of literature, narrowing down hundreds of studies to bring attendees the Top 20 papers with an impact on hospital medicine for the session. They each collected articles throughout the year, checking in regularly to outline the themes and rank papers for the session. In January, Dr. Moriates and Dr. Herzke reviewed all the articles they had collected, finalizing the major themes and highlights for the Update.
“The harder part was dropping a few of the articles we had selected in order to make it under an hour,” he said. “We tried to come up with the highlights that all hospitalists should know about, which are most likely to inform their practices over the coming year. And so, if you haven’t picked up a journal in a year, hopefully within an hour, Carrie and I can give you a quick download.”
Attendees familiar with “Update in Hospital Medicine” also will know that the exact details of what is being presented are secret. It is one of the few sessions at HM19 where slides are not published beforehand on the official Annual Conference app. The only way to know the details of the top studies is to attend the session.
“You have to be there to find out,” Dr. Moriates said.
But curiosity should not be the only reason for hospitalists to attend. Dr. Herzke said this year’s “Update in Hospital Medicine” session holds some practice pearls that may surprise attendees.
“We picked out some studies that we think should make people question common practices and consider making changes to how they practice medicine at their home institution, or their home hospital,” she said.
“It’s fair to say there were a number of studies this year that questioned conventional practices or put forth clear evidence that suggests we should be doing things differently in the hospital than the way we currently are doing them, across a number of scenarios,” Dr. Moriates said.
Attendees can expect studies in the fields of infectious disease, cardiology, and hematology to make the Top 20 list of best papers for the session. However, the challenge is always to present clinical pearls that apply to all hospitalists, regardless of where they practice.
“I think one thing about hospitalists is that our practices are very broad based, and we have to be up to date in lots of different fields,” Dr. Moriates said. “And so, we will cover the top literature across an array of fields matching the breadth and diversity of the patients that we take care of as hospitalists.”
Dr. Moriates and Dr. Herzke had no relevant financial conflicts.
Update in Hospital Medicine
Tuesday, 1:00 – 2:00 p.m.
Potomac ABCD

What’s your favorite aspect of HM19?
Attendees explain what they enjoy about the Annual Conference.

Attendees explain what they enjoy about the Annual Conference.
Attendees explain what they enjoy about the Annual Conference.

How has hospital medicine changed since you started?

HM19 attendees relay their perspectives on how the practice of hospital medicine has evolved over the course of their careers.
HM19 attendees relay their perspectives on how the practice of hospital medicine has evolved over the course of their careers.
HM19 attendees relay their perspectives on how the practice of hospital medicine has evolved over the course of their careers.
Hands-on critical care lessons provided at HM19
As the hospitalist tried to position the portable video laryngoscope properly in the airway of the critically ill “patient,” HM19 faculty moderator Brian Kaufman, MD, professor of medicine, anesthesiology, and neurology at New York University (NYU) School of Medicine, issued a word of caution: Rotating it into position should be done gently or there’s a risk of tearing tissue.
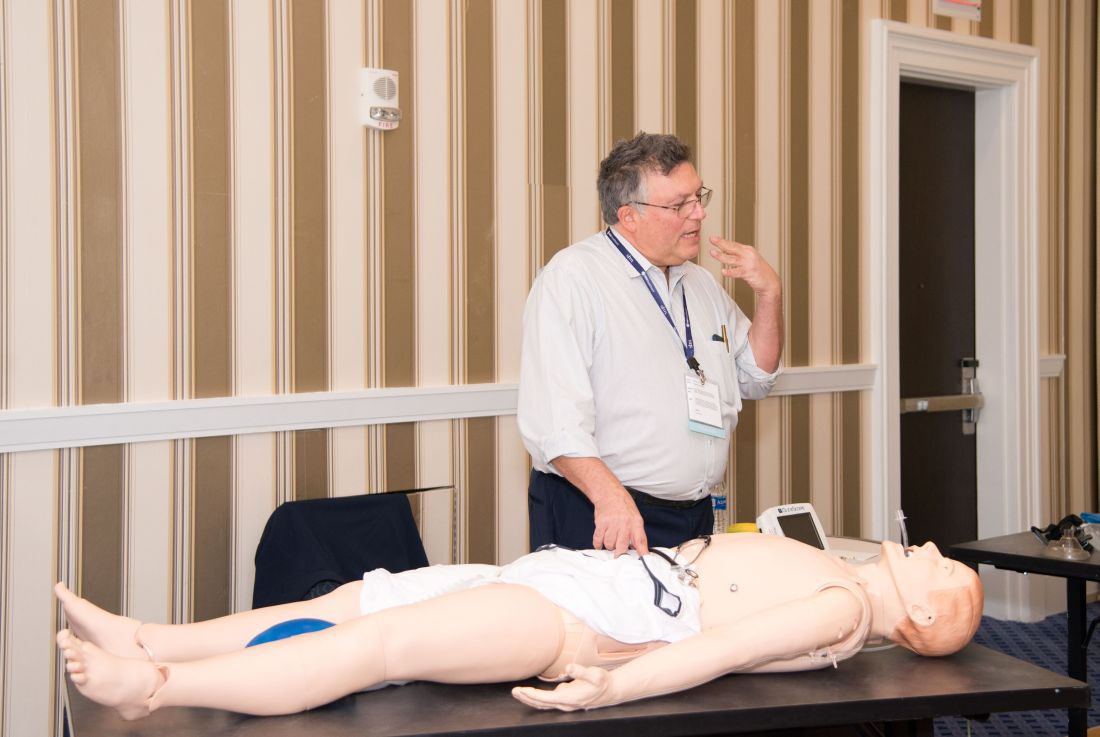
One step at a time, hospitalists attending the session grew more confident and knowledgeable in handling urgent matters involving patients who are critically ill, including cases of shock, mechanical ventilation, overdoses, and ultrasound.
Kevin Felner, MD, associate professor of medicine at NYU School of Medicine, said there’s a growing need for more exposure to caring for the critically ill, including intubation.
“There are a lot of hospitalists who are intubating, and they’re not formally trained in it because medicine residencies don’t typically train people to manage airways,” he said. “We’ve met hospitalists who’ve said, ‘I was hired and was told I had to manage an airway.’”
“It might massage some of the things you’re doing, make you afraid of things you should be afraid of, make you think about something that’s easy to do that you’re not doing, and make things safer,” Dr. Felner said.
In a simulation room, James Horowitz, MD, clinical assistant professor and cardiologist at NYU School of Medicine, demonstrated how to use a laryngeal mask airway (LMA), a simpler alternative to intubating the trachea for keeping an airway open. Dr. Kaufman, standing next to him, clarified how important a skill this is, especially when someone needs air in the next minute or is at risk of death.
“Knowing how to put an LMA in can be life-saving,” Dr. Kaufman said.
In a lecture on shock in the critically ill, Dr. Felner said it’s important to be nimble in handling this common problem –quickly identifying the cause, whether it’s a cardiogenic issue, a low-volume circulation problem, a question of vasodilation, or an obstructive problem. He said guidelines – such as aiming for a mean arterial pressure of 65 mm Hg –are helpful generally, but individuals routinely call for making exceptions to guidelines.
Anthony Andriotis, MD, a pulmonologist at NYU who specializes in critical care, offered an array of key points when managing patients with a ventilator. For instance, when you need to prolong a patient’s expiratory time so they can exhale air more effectively to get rid of entrapped air in their lungs, lowering their respiratory rate is far more effective than decreasing the time it takes them to breathe in or increasing the flow rate of the air they’re breathing.
Some basic points – such as remembering that it’s important to be aware of the pressure when volume control has been imposed and to be aware of volume control when the pressure has been set – are crucial, he said.
The idea behind the pre-course, Dr. Felner said, was to give hospitalists a chance to enter tricky situations with everything to gain, but nothing to lose. He described it as giving students “learning scars” – those times you made a serious error that left you with a lesson you’ll never forget.
“We’re trying to create learning scars, but in a safe scenario.”
As the hospitalist tried to position the portable video laryngoscope properly in the airway of the critically ill “patient,” HM19 faculty moderator Brian Kaufman, MD, professor of medicine, anesthesiology, and neurology at New York University (NYU) School of Medicine, issued a word of caution: Rotating it into position should be done gently or there’s a risk of tearing tissue.
One step at a time, hospitalists attending the session grew more confident and knowledgeable in handling urgent matters involving patients who are critically ill, including cases of shock, mechanical ventilation, overdoses, and ultrasound.
Kevin Felner, MD, associate professor of medicine at NYU School of Medicine, said there’s a growing need for more exposure to caring for the critically ill, including intubation.
“There are a lot of hospitalists who are intubating, and they’re not formally trained in it because medicine residencies don’t typically train people to manage airways,” he said. “We’ve met hospitalists who’ve said, ‘I was hired and was told I had to manage an airway.’”
“It might massage some of the things you’re doing, make you afraid of things you should be afraid of, make you think about something that’s easy to do that you’re not doing, and make things safer,” Dr. Felner said.
In a simulation room, James Horowitz, MD, clinical assistant professor and cardiologist at NYU School of Medicine, demonstrated how to use a laryngeal mask airway (LMA), a simpler alternative to intubating the trachea for keeping an airway open. Dr. Kaufman, standing next to him, clarified how important a skill this is, especially when someone needs air in the next minute or is at risk of death.
“Knowing how to put an LMA in can be life-saving,” Dr. Kaufman said.
In a lecture on shock in the critically ill, Dr. Felner said it’s important to be nimble in handling this common problem –quickly identifying the cause, whether it’s a cardiogenic issue, a low-volume circulation problem, a question of vasodilation, or an obstructive problem. He said guidelines – such as aiming for a mean arterial pressure of 65 mm Hg –are helpful generally, but individuals routinely call for making exceptions to guidelines.
Anthony Andriotis, MD, a pulmonologist at NYU who specializes in critical care, offered an array of key points when managing patients with a ventilator. For instance, when you need to prolong a patient’s expiratory time so they can exhale air more effectively to get rid of entrapped air in their lungs, lowering their respiratory rate is far more effective than decreasing the time it takes them to breathe in or increasing the flow rate of the air they’re breathing.
Some basic points – such as remembering that it’s important to be aware of the pressure when volume control has been imposed and to be aware of volume control when the pressure has been set – are crucial, he said.
The idea behind the pre-course, Dr. Felner said, was to give hospitalists a chance to enter tricky situations with everything to gain, but nothing to lose. He described it as giving students “learning scars” – those times you made a serious error that left you with a lesson you’ll never forget.
“We’re trying to create learning scars, but in a safe scenario.”
As the hospitalist tried to position the portable video laryngoscope properly in the airway of the critically ill “patient,” HM19 faculty moderator Brian Kaufman, MD, professor of medicine, anesthesiology, and neurology at New York University (NYU) School of Medicine, issued a word of caution: Rotating it into position should be done gently or there’s a risk of tearing tissue.
One step at a time, hospitalists attending the session grew more confident and knowledgeable in handling urgent matters involving patients who are critically ill, including cases of shock, mechanical ventilation, overdoses, and ultrasound.
Kevin Felner, MD, associate professor of medicine at NYU School of Medicine, said there’s a growing need for more exposure to caring for the critically ill, including intubation.
“There are a lot of hospitalists who are intubating, and they’re not formally trained in it because medicine residencies don’t typically train people to manage airways,” he said. “We’ve met hospitalists who’ve said, ‘I was hired and was told I had to manage an airway.’”
“It might massage some of the things you’re doing, make you afraid of things you should be afraid of, make you think about something that’s easy to do that you’re not doing, and make things safer,” Dr. Felner said.
In a simulation room, James Horowitz, MD, clinical assistant professor and cardiologist at NYU School of Medicine, demonstrated how to use a laryngeal mask airway (LMA), a simpler alternative to intubating the trachea for keeping an airway open. Dr. Kaufman, standing next to him, clarified how important a skill this is, especially when someone needs air in the next minute or is at risk of death.
“Knowing how to put an LMA in can be life-saving,” Dr. Kaufman said.
In a lecture on shock in the critically ill, Dr. Felner said it’s important to be nimble in handling this common problem –quickly identifying the cause, whether it’s a cardiogenic issue, a low-volume circulation problem, a question of vasodilation, or an obstructive problem. He said guidelines – such as aiming for a mean arterial pressure of 65 mm Hg –are helpful generally, but individuals routinely call for making exceptions to guidelines.
Anthony Andriotis, MD, a pulmonologist at NYU who specializes in critical care, offered an array of key points when managing patients with a ventilator. For instance, when you need to prolong a patient’s expiratory time so they can exhale air more effectively to get rid of entrapped air in their lungs, lowering their respiratory rate is far more effective than decreasing the time it takes them to breathe in or increasing the flow rate of the air they’re breathing.
Some basic points – such as remembering that it’s important to be aware of the pressure when volume control has been imposed and to be aware of volume control when the pressure has been set – are crucial, he said.
The idea behind the pre-course, Dr. Felner said, was to give hospitalists a chance to enter tricky situations with everything to gain, but nothing to lose. He described it as giving students “learning scars” – those times you made a serious error that left you with a lesson you’ll never forget.
“We’re trying to create learning scars, but in a safe scenario.”
Planning for change in hospitalist practice management
At Sunday’s HM19 pre-course “Oh, the Places We’ll Go! Practice Management Tools for Navigating the Changing Role of Your Hospital Medicine Group,” the theme was how to anticipate and embrace changing roles as hospital medicine groups are being asked to take on more responsibility.

“The scope of hospitalist practice is evolving rapidly, both clinically and in terms of all of the other things that hospitalists are being asked to do,” said Leslie Flores, MHA, SFHM, a partner at Nelson Flores Hospital Medicine Consultants, La Quinta, Calif., and course co-director, in an interview before the pre-course. “Our goals with this program are to help leaders position their hospitalist groups for success with this changing environment that they’re living in and the changing roles of hospitalists.”
In an audience poll at the beginning of the pre-course, attendees – a majority of whom were practicing hospitalists and managers of hospitalist groups – said their biggest challenge areas were related to compensation or workflows that have not evolved to match their changing role, and disagreements over who should admit patients.
One of the goals of the session was to give hospitalist leaders ideas to address these issues, which included information on how to implement better team-based care and interdisciplinary care models within their groups, as well as how to adjust their compensation, scheduling, and staffing models to prepare for this “new world of hospitalist medicine,” said Ms. Flores.
“One of the biggest sources of contention and stress that we see in hospitalist groups is that there’s just so much change, and it’s happening so rapidly, and people are having a hard time really figuring out how to deal with all of that,” she said.
The day began with John Nelson, MD, MHM, outlining the “Trends in Scope of Practice Evolution.” Dr. Nelson, a partner at Nelson Flores Hospital Medicine Consultants, medical director of Overlake Medical Center in Bellevue, Wash., and course co-director, said hospitalists are increasingly working more in outpatient care, post-acute care, and other specialty facilities. In addition, as group size increases, the likelihood a hospitalist group will be responsible for an observation or short stay unit increases, while a larger group is less likely to have a clinical responsibility for a code blue, cardiac arrest, or rapid response team.
Other topics in the pre-course focused on how to change the culture in a group to an environment where team members are empowered to ask questions or voice concerns, improve patient flow by removing reasons for delays in discharge, recruit the right team members to a group, handle transitions of care, and anticipate change in a group. In addition, the speakers participated in discussions where they shared their biggest successes and failures in practice as leaders and participated in a lightning round where they provided “off-the-cuff” responses to questions from Ms. Flores.
Although hospitalists did not create the current environment that is expanding their role in the health care system, they can position themselves to decide what the scope of their role is, said Dr. Nelson.
“What we should do is navigate our group through these changes in the way that’s going to be most effective for ourselves, the providers in our group, and our organization,” he said. “Those groups that try to dig their heels in or resist all change, they fail. . . and they frustrate themselves. So instead, if you engage in planning for changes in the scope of your practice, you have a chance to make it go the way you’d like it to go, and you’re going to be more satisfied.”
At Sunday’s HM19 pre-course “Oh, the Places We’ll Go! Practice Management Tools for Navigating the Changing Role of Your Hospital Medicine Group,” the theme was how to anticipate and embrace changing roles as hospital medicine groups are being asked to take on more responsibility.
“The scope of hospitalist practice is evolving rapidly, both clinically and in terms of all of the other things that hospitalists are being asked to do,” said Leslie Flores, MHA, SFHM, a partner at Nelson Flores Hospital Medicine Consultants, La Quinta, Calif., and course co-director, in an interview before the pre-course. “Our goals with this program are to help leaders position their hospitalist groups for success with this changing environment that they’re living in and the changing roles of hospitalists.”
In an audience poll at the beginning of the pre-course, attendees – a majority of whom were practicing hospitalists and managers of hospitalist groups – said their biggest challenge areas were related to compensation or workflows that have not evolved to match their changing role, and disagreements over who should admit patients.
One of the goals of the session was to give hospitalist leaders ideas to address these issues, which included information on how to implement better team-based care and interdisciplinary care models within their groups, as well as how to adjust their compensation, scheduling, and staffing models to prepare for this “new world of hospitalist medicine,” said Ms. Flores.
“One of the biggest sources of contention and stress that we see in hospitalist groups is that there’s just so much change, and it’s happening so rapidly, and people are having a hard time really figuring out how to deal with all of that,” she said.
The day began with John Nelson, MD, MHM, outlining the “Trends in Scope of Practice Evolution.” Dr. Nelson, a partner at Nelson Flores Hospital Medicine Consultants, medical director of Overlake Medical Center in Bellevue, Wash., and course co-director, said hospitalists are increasingly working more in outpatient care, post-acute care, and other specialty facilities. In addition, as group size increases, the likelihood a hospitalist group will be responsible for an observation or short stay unit increases, while a larger group is less likely to have a clinical responsibility for a code blue, cardiac arrest, or rapid response team.
Other topics in the pre-course focused on how to change the culture in a group to an environment where team members are empowered to ask questions or voice concerns, improve patient flow by removing reasons for delays in discharge, recruit the right team members to a group, handle transitions of care, and anticipate change in a group. In addition, the speakers participated in discussions where they shared their biggest successes and failures in practice as leaders and participated in a lightning round where they provided “off-the-cuff” responses to questions from Ms. Flores.
Although hospitalists did not create the current environment that is expanding their role in the health care system, they can position themselves to decide what the scope of their role is, said Dr. Nelson.
“What we should do is navigate our group through these changes in the way that’s going to be most effective for ourselves, the providers in our group, and our organization,” he said. “Those groups that try to dig their heels in or resist all change, they fail. . . and they frustrate themselves. So instead, if you engage in planning for changes in the scope of your practice, you have a chance to make it go the way you’d like it to go, and you’re going to be more satisfied.”
At Sunday’s HM19 pre-course “Oh, the Places We’ll Go! Practice Management Tools for Navigating the Changing Role of Your Hospital Medicine Group,” the theme was how to anticipate and embrace changing roles as hospital medicine groups are being asked to take on more responsibility.
“The scope of hospitalist practice is evolving rapidly, both clinically and in terms of all of the other things that hospitalists are being asked to do,” said Leslie Flores, MHA, SFHM, a partner at Nelson Flores Hospital Medicine Consultants, La Quinta, Calif., and course co-director, in an interview before the pre-course. “Our goals with this program are to help leaders position their hospitalist groups for success with this changing environment that they’re living in and the changing roles of hospitalists.”
In an audience poll at the beginning of the pre-course, attendees – a majority of whom were practicing hospitalists and managers of hospitalist groups – said their biggest challenge areas were related to compensation or workflows that have not evolved to match their changing role, and disagreements over who should admit patients.
One of the goals of the session was to give hospitalist leaders ideas to address these issues, which included information on how to implement better team-based care and interdisciplinary care models within their groups, as well as how to adjust their compensation, scheduling, and staffing models to prepare for this “new world of hospitalist medicine,” said Ms. Flores.
“One of the biggest sources of contention and stress that we see in hospitalist groups is that there’s just so much change, and it’s happening so rapidly, and people are having a hard time really figuring out how to deal with all of that,” she said.
The day began with John Nelson, MD, MHM, outlining the “Trends in Scope of Practice Evolution.” Dr. Nelson, a partner at Nelson Flores Hospital Medicine Consultants, medical director of Overlake Medical Center in Bellevue, Wash., and course co-director, said hospitalists are increasingly working more in outpatient care, post-acute care, and other specialty facilities. In addition, as group size increases, the likelihood a hospitalist group will be responsible for an observation or short stay unit increases, while a larger group is less likely to have a clinical responsibility for a code blue, cardiac arrest, or rapid response team.
Other topics in the pre-course focused on how to change the culture in a group to an environment where team members are empowered to ask questions or voice concerns, improve patient flow by removing reasons for delays in discharge, recruit the right team members to a group, handle transitions of care, and anticipate change in a group. In addition, the speakers participated in discussions where they shared their biggest successes and failures in practice as leaders and participated in a lightning round where they provided “off-the-cuff” responses to questions from Ms. Flores.
Although hospitalists did not create the current environment that is expanding their role in the health care system, they can position themselves to decide what the scope of their role is, said Dr. Nelson.
“What we should do is navigate our group through these changes in the way that’s going to be most effective for ourselves, the providers in our group, and our organization,” he said. “Those groups that try to dig their heels in or resist all change, they fail. . . and they frustrate themselves. So instead, if you engage in planning for changes in the scope of your practice, you have a chance to make it go the way you’d like it to go, and you’re going to be more satisfied.”
Syncope session showcases latest research and guidance for practice
Syncope is a common problem, but an area in which practice likely varies by region and provider, according to Carrie Herzke, MD, SFHM, of Johns Hopkins University in Baltimore.
The variation in practice also suggests opportunities to safely cut costs, Dr. Herzke said in an interview.
Dr. Herzke will review the recent literature and summarize the current guidelines related to the treatment of syncope in her session, “SyncopE – Effective, Efficient and Economic Evaluations,” on Monday, March 25, at HM19.
“At the end of this session I am hopeful attendees will have a better understanding of the current guidelines, as well as which tests are most likely to be high value in the evaluation of syncope,” Dr. Herzke said. But before testing, clinicians should keep in mind that a history and physical examination are key components to evaluating syncope, she noted.
The European Society of Cardiology Guidelines for Syncope, published in 2018, feature several new concepts for evaluating and managing syncope in clinical settings and testing, including tilt testing, a greater role for prolonged ECG monitoring, use of video recording for suspected syncope, consideration of adenosine sensitive syncope, and consideration of neurological causes of syncope.
The ESC guidelines include using algorithms to determine the appropriate therapy for reflex syncope based on age, severity, and clinical forms. The guidelines also address diagnostic tests, monitoring in and out of the hospital, and treatment options including lifestyle changes and education as well as pharmacotherapy.
Dr. Herzke also will review the 2017 ACC/AHA/HRS Guideline for Patients With Syncope, published in 2017 in the journal Circulation. This guideline has an algorithm for initial evaluation of patients with syncope that includes a history, physical, and ECG. If the cause is known, patients should be assessed for risk and treated; syncope of unknown cause requires further evaluation, and the guideline presents recommendations for additional assessment through means including cardiac imaging, stress testing, blood testing, neurological testing, and tilt table testing.
“The selection of a given diagnostic test, after the initial history, physical examination, and baseline ECG, is a clinical decision based on the patient’s clinical presentation, risk stratification, and a clear understanding of diagnostic and prognostic value of any further testing,” according to the guideline authors.
The 2017 ACC/AHA/HRS Guideline for Patients With Syncope also provides recommendations for the management of cardiovascular conditions, including arrhythmic and structural conditions.
Dr. Herzke said she thinks that the topic of pulmonary embolism and syncope may prompt the liveliest discussion, and she will include several recent articles on this topic in her literature review.
“There has been some debate about how often PE is present in patients presenting after a syncopal episode,” she said. A recent study published in JAMA Internal Medicine found a prevalence of PE from 0.06% to 0.55% among all adults presenting to an ED with syncope and a prevalence of PE from 0.14% to 0.83%.
SyncopE – Effective, Efficient and Economic Evaluations
Monday 1:10 pm
Maryland BD/4-6
Syncope is a common problem, but an area in which practice likely varies by region and provider, according to Carrie Herzke, MD, SFHM, of Johns Hopkins University in Baltimore.
The variation in practice also suggests opportunities to safely cut costs, Dr. Herzke said in an interview.
Dr. Herzke will review the recent literature and summarize the current guidelines related to the treatment of syncope in her session, “SyncopE – Effective, Efficient and Economic Evaluations,” on Monday, March 25, at HM19.
“At the end of this session I am hopeful attendees will have a better understanding of the current guidelines, as well as which tests are most likely to be high value in the evaluation of syncope,” Dr. Herzke said. But before testing, clinicians should keep in mind that a history and physical examination are key components to evaluating syncope, she noted.
The European Society of Cardiology Guidelines for Syncope, published in 2018, feature several new concepts for evaluating and managing syncope in clinical settings and testing, including tilt testing, a greater role for prolonged ECG monitoring, use of video recording for suspected syncope, consideration of adenosine sensitive syncope, and consideration of neurological causes of syncope.
The ESC guidelines include using algorithms to determine the appropriate therapy for reflex syncope based on age, severity, and clinical forms. The guidelines also address diagnostic tests, monitoring in and out of the hospital, and treatment options including lifestyle changes and education as well as pharmacotherapy.
Dr. Herzke also will review the 2017 ACC/AHA/HRS Guideline for Patients With Syncope, published in 2017 in the journal Circulation. This guideline has an algorithm for initial evaluation of patients with syncope that includes a history, physical, and ECG. If the cause is known, patients should be assessed for risk and treated; syncope of unknown cause requires further evaluation, and the guideline presents recommendations for additional assessment through means including cardiac imaging, stress testing, blood testing, neurological testing, and tilt table testing.
“The selection of a given diagnostic test, after the initial history, physical examination, and baseline ECG, is a clinical decision based on the patient’s clinical presentation, risk stratification, and a clear understanding of diagnostic and prognostic value of any further testing,” according to the guideline authors.
The 2017 ACC/AHA/HRS Guideline for Patients With Syncope also provides recommendations for the management of cardiovascular conditions, including arrhythmic and structural conditions.
Dr. Herzke said she thinks that the topic of pulmonary embolism and syncope may prompt the liveliest discussion, and she will include several recent articles on this topic in her literature review.
“There has been some debate about how often PE is present in patients presenting after a syncopal episode,” she said. A recent study published in JAMA Internal Medicine found a prevalence of PE from 0.06% to 0.55% among all adults presenting to an ED with syncope and a prevalence of PE from 0.14% to 0.83%.
SyncopE – Effective, Efficient and Economic Evaluations
Monday 1:10 pm
Maryland BD/4-6
Syncope is a common problem, but an area in which practice likely varies by region and provider, according to Carrie Herzke, MD, SFHM, of Johns Hopkins University in Baltimore.
The variation in practice also suggests opportunities to safely cut costs, Dr. Herzke said in an interview.
Dr. Herzke will review the recent literature and summarize the current guidelines related to the treatment of syncope in her session, “SyncopE – Effective, Efficient and Economic Evaluations,” on Monday, March 25, at HM19.
“At the end of this session I am hopeful attendees will have a better understanding of the current guidelines, as well as which tests are most likely to be high value in the evaluation of syncope,” Dr. Herzke said. But before testing, clinicians should keep in mind that a history and physical examination are key components to evaluating syncope, she noted.
The European Society of Cardiology Guidelines for Syncope, published in 2018, feature several new concepts for evaluating and managing syncope in clinical settings and testing, including tilt testing, a greater role for prolonged ECG monitoring, use of video recording for suspected syncope, consideration of adenosine sensitive syncope, and consideration of neurological causes of syncope.
The ESC guidelines include using algorithms to determine the appropriate therapy for reflex syncope based on age, severity, and clinical forms. The guidelines also address diagnostic tests, monitoring in and out of the hospital, and treatment options including lifestyle changes and education as well as pharmacotherapy.
Dr. Herzke also will review the 2017 ACC/AHA/HRS Guideline for Patients With Syncope, published in 2017 in the journal Circulation. This guideline has an algorithm for initial evaluation of patients with syncope that includes a history, physical, and ECG. If the cause is known, patients should be assessed for risk and treated; syncope of unknown cause requires further evaluation, and the guideline presents recommendations for additional assessment through means including cardiac imaging, stress testing, blood testing, neurological testing, and tilt table testing.
“The selection of a given diagnostic test, after the initial history, physical examination, and baseline ECG, is a clinical decision based on the patient’s clinical presentation, risk stratification, and a clear understanding of diagnostic and prognostic value of any further testing,” according to the guideline authors.
The 2017 ACC/AHA/HRS Guideline for Patients With Syncope also provides recommendations for the management of cardiovascular conditions, including arrhythmic and structural conditions.
Dr. Herzke said she thinks that the topic of pulmonary embolism and syncope may prompt the liveliest discussion, and she will include several recent articles on this topic in her literature review.
“There has been some debate about how often PE is present in patients presenting after a syncopal episode,” she said. A recent study published in JAMA Internal Medicine found a prevalence of PE from 0.06% to 0.55% among all adults presenting to an ED with syncope and a prevalence of PE from 0.14% to 0.83%.
SyncopE – Effective, Efficient and Economic Evaluations
Monday 1:10 pm
Maryland BD/4-6
The power of policy at HM19
Mini-track features CMS insights
Due to the steadily growing interest of SHM members in health care policy and advocacy issues, the 2019 Annual Conference will include a mini-track dedicated to policy issues.
To be held on Monday, March 25th at HM19 in Orlando, the health care policy mini-track will update conference attendees on some of the Washington developments that affect hospitalists, said Josh Boswell, director of government relations at SHM.
“Many of the policy developments in D.C. are directly impacting our members’ practices,” he said. “A couple of years ago, it was decided to add a specific track at the annual conference to cover some of these policy issues, and we’ve generally had positive feedback on the sessions.”
This year, the mini-track will consist of two separate sessions, held back to back. “Both sessions are designed to give attendees an entrée into health policy and explain developments that are happening right now in Washington that impact their practice,” said Joshua Lapps, government relations manager at SHM.
The first session – “CMS Policy Update: An Overview of Meaningful Measures and the Quality Payment Program” – will take place from 2:00 to 3:30 p.m., and will feature Reena Duseja, MD, MS, the acting director for Quality Measurement and Value-Based Incentives Group in the Centers for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services. Dr. Duseja oversees the development of measures and analyses for a variety of CMS quality reporting and value-based purchasing programs. She is also an emergency medicine physician and was an associate professor at the University of California, San Francisco, in the department of emergency medicine, where she led quality improvement activities.
“The session with Dr. Duseja will be an inside look into the approach that CMS is taking for quality measurement and pay-for-performance programs, specifically looking at the quality payment program which came out of the Medicare Access and Chip Reauthorization Act,” Mr. Lapps said. “It will be a high-level discussion about how the programs affect hospitalists, and how hospitalists participate in the programs. It’s also a chance for attendees to hear some of the thinking inside CMS.”
Dr. Duseja is also hoping to get feedback from HM19 attendees. “She wants the session to be educational for our members, as well as an opportunity for her to learn from hospitalists,” Mr. Lapps said.
According to Dr. Duseja, her presentation will provide attendees with an overview of the Quality Payment Program under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), specifically highlighting policy changes from 2018 to 2019 to the Merit-based Incentive Payment System (MIPS) and Meaningful Measures Initiative. Attendees will learn more about CMS’s approach to quality and quality measurement, as well as the future of quality reporting programs.
Following Dr. Duseja’s presentation, the second mini-track session will take place from 3:40 to 4:25 p.m. It will focus more intently on the processes around health care policy making.
“We heard from our members who attended this mini-track at the past two annual conferences that they would like us to explain how policy making works: the play-by-play in D.C. on how we get to where we are,” Mr. Boswell said.
The second session will feature a presentation by Jennifer Bell, founding partner at Chamber Hill Strategies, who represents SHM in Washington. “Jennifer will be discussing how Washington works, the policy process and the pressure points at which SHM and its members can exert influence,” Mr. Lapps said.
Attendees can expect to learn a lot from either session, Mr. Lapps said. “Attendees will learn about the basic contours of the Quality Payment Program that Medicare oversees, and some of the specific new elements of that program this year that were designed with hospitalists in mind. For example, Dr. Duseja will be talking about a facility-based reporting option under the Merit-Based Incentive Payment System. I think our members should gain a concrete understanding of some of the new directions that CMS is heading this year. Overall, they’ll have a better sense of the vision behind quality measures and quality measurement. This is a really exciting opportunity to hear from someone who is both a clinician and works on policy at CMS.”
The policy mini-track offers hospitalists a chance to get a look “behind the curtain” at policy making from someone who is helping to write the rules.
“Attendees will gain insight on where they fit in these programs – and also have the opportunity to tell Dr. Duseja if they don’t feel these programs are a good fit for them,” Mr. Boswell said. “Oftentimes these programs are not structured ideally for hospitalists. So, hearing directly from hospitalists who are experiencing problems would be extraordinarily helpful to a CMS official. I think attendees should view the policy track not only as an opportunity to learn from CMS, but as an opportunity to educate CMS about our issues.”
Mini-track features CMS insights
Mini-track features CMS insights
Due to the steadily growing interest of SHM members in health care policy and advocacy issues, the 2019 Annual Conference will include a mini-track dedicated to policy issues.
To be held on Monday, March 25th at HM19 in Orlando, the health care policy mini-track will update conference attendees on some of the Washington developments that affect hospitalists, said Josh Boswell, director of government relations at SHM.
“Many of the policy developments in D.C. are directly impacting our members’ practices,” he said. “A couple of years ago, it was decided to add a specific track at the annual conference to cover some of these policy issues, and we’ve generally had positive feedback on the sessions.”
This year, the mini-track will consist of two separate sessions, held back to back. “Both sessions are designed to give attendees an entrée into health policy and explain developments that are happening right now in Washington that impact their practice,” said Joshua Lapps, government relations manager at SHM.
The first session – “CMS Policy Update: An Overview of Meaningful Measures and the Quality Payment Program” – will take place from 2:00 to 3:30 p.m., and will feature Reena Duseja, MD, MS, the acting director for Quality Measurement and Value-Based Incentives Group in the Centers for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services. Dr. Duseja oversees the development of measures and analyses for a variety of CMS quality reporting and value-based purchasing programs. She is also an emergency medicine physician and was an associate professor at the University of California, San Francisco, in the department of emergency medicine, where she led quality improvement activities.
“The session with Dr. Duseja will be an inside look into the approach that CMS is taking for quality measurement and pay-for-performance programs, specifically looking at the quality payment program which came out of the Medicare Access and Chip Reauthorization Act,” Mr. Lapps said. “It will be a high-level discussion about how the programs affect hospitalists, and how hospitalists participate in the programs. It’s also a chance for attendees to hear some of the thinking inside CMS.”
Dr. Duseja is also hoping to get feedback from HM19 attendees. “She wants the session to be educational for our members, as well as an opportunity for her to learn from hospitalists,” Mr. Lapps said.
According to Dr. Duseja, her presentation will provide attendees with an overview of the Quality Payment Program under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), specifically highlighting policy changes from 2018 to 2019 to the Merit-based Incentive Payment System (MIPS) and Meaningful Measures Initiative. Attendees will learn more about CMS’s approach to quality and quality measurement, as well as the future of quality reporting programs.
Following Dr. Duseja’s presentation, the second mini-track session will take place from 3:40 to 4:25 p.m. It will focus more intently on the processes around health care policy making.
“We heard from our members who attended this mini-track at the past two annual conferences that they would like us to explain how policy making works: the play-by-play in D.C. on how we get to where we are,” Mr. Boswell said.
The second session will feature a presentation by Jennifer Bell, founding partner at Chamber Hill Strategies, who represents SHM in Washington. “Jennifer will be discussing how Washington works, the policy process and the pressure points at which SHM and its members can exert influence,” Mr. Lapps said.
Attendees can expect to learn a lot from either session, Mr. Lapps said. “Attendees will learn about the basic contours of the Quality Payment Program that Medicare oversees, and some of the specific new elements of that program this year that were designed with hospitalists in mind. For example, Dr. Duseja will be talking about a facility-based reporting option under the Merit-Based Incentive Payment System. I think our members should gain a concrete understanding of some of the new directions that CMS is heading this year. Overall, they’ll have a better sense of the vision behind quality measures and quality measurement. This is a really exciting opportunity to hear from someone who is both a clinician and works on policy at CMS.”
The policy mini-track offers hospitalists a chance to get a look “behind the curtain” at policy making from someone who is helping to write the rules.
“Attendees will gain insight on where they fit in these programs – and also have the opportunity to tell Dr. Duseja if they don’t feel these programs are a good fit for them,” Mr. Boswell said. “Oftentimes these programs are not structured ideally for hospitalists. So, hearing directly from hospitalists who are experiencing problems would be extraordinarily helpful to a CMS official. I think attendees should view the policy track not only as an opportunity to learn from CMS, but as an opportunity to educate CMS about our issues.”
Due to the steadily growing interest of SHM members in health care policy and advocacy issues, the 2019 Annual Conference will include a mini-track dedicated to policy issues.
To be held on Monday, March 25th at HM19 in Orlando, the health care policy mini-track will update conference attendees on some of the Washington developments that affect hospitalists, said Josh Boswell, director of government relations at SHM.
“Many of the policy developments in D.C. are directly impacting our members’ practices,” he said. “A couple of years ago, it was decided to add a specific track at the annual conference to cover some of these policy issues, and we’ve generally had positive feedback on the sessions.”
This year, the mini-track will consist of two separate sessions, held back to back. “Both sessions are designed to give attendees an entrée into health policy and explain developments that are happening right now in Washington that impact their practice,” said Joshua Lapps, government relations manager at SHM.
The first session – “CMS Policy Update: An Overview of Meaningful Measures and the Quality Payment Program” – will take place from 2:00 to 3:30 p.m., and will feature Reena Duseja, MD, MS, the acting director for Quality Measurement and Value-Based Incentives Group in the Centers for Clinical Standards and Quality at the Centers for Medicare & Medicaid Services. Dr. Duseja oversees the development of measures and analyses for a variety of CMS quality reporting and value-based purchasing programs. She is also an emergency medicine physician and was an associate professor at the University of California, San Francisco, in the department of emergency medicine, where she led quality improvement activities.
“The session with Dr. Duseja will be an inside look into the approach that CMS is taking for quality measurement and pay-for-performance programs, specifically looking at the quality payment program which came out of the Medicare Access and Chip Reauthorization Act,” Mr. Lapps said. “It will be a high-level discussion about how the programs affect hospitalists, and how hospitalists participate in the programs. It’s also a chance for attendees to hear some of the thinking inside CMS.”
Dr. Duseja is also hoping to get feedback from HM19 attendees. “She wants the session to be educational for our members, as well as an opportunity for her to learn from hospitalists,” Mr. Lapps said.
According to Dr. Duseja, her presentation will provide attendees with an overview of the Quality Payment Program under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), specifically highlighting policy changes from 2018 to 2019 to the Merit-based Incentive Payment System (MIPS) and Meaningful Measures Initiative. Attendees will learn more about CMS’s approach to quality and quality measurement, as well as the future of quality reporting programs.
Following Dr. Duseja’s presentation, the second mini-track session will take place from 3:40 to 4:25 p.m. It will focus more intently on the processes around health care policy making.
“We heard from our members who attended this mini-track at the past two annual conferences that they would like us to explain how policy making works: the play-by-play in D.C. on how we get to where we are,” Mr. Boswell said.
The second session will feature a presentation by Jennifer Bell, founding partner at Chamber Hill Strategies, who represents SHM in Washington. “Jennifer will be discussing how Washington works, the policy process and the pressure points at which SHM and its members can exert influence,” Mr. Lapps said.
Attendees can expect to learn a lot from either session, Mr. Lapps said. “Attendees will learn about the basic contours of the Quality Payment Program that Medicare oversees, and some of the specific new elements of that program this year that were designed with hospitalists in mind. For example, Dr. Duseja will be talking about a facility-based reporting option under the Merit-Based Incentive Payment System. I think our members should gain a concrete understanding of some of the new directions that CMS is heading this year. Overall, they’ll have a better sense of the vision behind quality measures and quality measurement. This is a really exciting opportunity to hear from someone who is both a clinician and works on policy at CMS.”
The policy mini-track offers hospitalists a chance to get a look “behind the curtain” at policy making from someone who is helping to write the rules.
“Attendees will gain insight on where they fit in these programs – and also have the opportunity to tell Dr. Duseja if they don’t feel these programs are a good fit for them,” Mr. Boswell said. “Oftentimes these programs are not structured ideally for hospitalists. So, hearing directly from hospitalists who are experiencing problems would be extraordinarily helpful to a CMS official. I think attendees should view the policy track not only as an opportunity to learn from CMS, but as an opportunity to educate CMS about our issues.”
