User login
Patients with epilepsy may underreport seizures, survey finds
according to survey results presented online as part of the 2020 American Academy of Neurology Science Highlights.
Clinicians, for their part, may underestimate the number of seizures that go unreported. This disconnect may contribute to complacency about epilepsy treatment regimens among patients, caregivers, and health care professionals (HCPs), despite continuations in seizures. “Improved reporting of all seizure occurrences and more frequent discussion of potential treatment changes, initiated by all groups, may be needed to optimize treatment outcomes,” said Patricia E. Penovich, MD, a neurologist at Minnesota Epilepsy Group in St. Paul, and colleagues.

To evaluate treatment complacency among adult patients with epilepsy, caregivers, and HCPs, Dr. Penovich and collaborators analyzed data from the STEP survey (Seize the Truth about Epilepsy Perceptions), which was conducted between February and March 2019. In all, 400 adults with epilepsy, 201 caregivers, and 258 HCPs completed the survey. The HCPs included 96 epileptologists, 112 general neurologists, and 50 nurse practitioners or physician assistants.
Patients had an average epilepsy duration of 16 years, and 58% were on at least their third antiepileptic drug (AED). In the past year, 52% of patients had 1-9 seizures, and 31% had 10 or more seizures. “Patients estimated reporting 45% of their seizures to their HCPs, and for the seizures not reported, 57% provided reasoning that they were not serious enough to mention,” reported Dr. Penovich and colleagues. “Alternatively, HCPs estimated that patients report 73% of seizures.”
Survey participants most frequently selected HCPs as the ones to initiate conversations about changing AEDs or increasing dosage. “Patient-initiated discussions were reported by 39% of patients for changing AEDs and 27% of patients for increasing AED dosage; 25% of patients reported they were likely to ask their HCP about changing treatments in the next 12 months,” the authors said. Discussion of vagus nerve stimulation was reported by 21% of HCPs, and 10% reported discussion of responsive neurostimulation. HCPs also discussed surgical options such as hemispherectomy (3%), corpus callosotomy and multiple subpial transection (4%), lobe resection (8%), and lesionectomy (11%).
Among patients with 13 or more seizures per year, 27% reported referral to an epilepsy center. Most survey participants – 61% of patients and HCPs and 68% of caregivers – “reported a desire for a treatment map that tells patients to see an epileptologist/specialist as soon as they have symptoms,” the researchers said.
“What we would like to think is that we are getting the whole scoop and the honest scoop” about seizure activity, Dr. Penovich said in an interview. “What this shows us is that that’s probably not always true. Some health care providers understand that the patients do not tell them everything,” but the degree of seizure underreporting may be surprising.
Dr. Penovich has seen this phenomenon in practice. In some cases, caregivers return to the office to explain that a patient did not report all of their seizures. Other patients may omit entire days of seizures in their diaries as an oversight. In addition, patients may not report seizures to avoid having a driver’s license revoked. In some instances, clinicians may not take the time to discuss seizure activity in detail.
Having an accurate picture of seizure activity is an “important part of working with our patients, particularly when we are trying to get them to the point of being seizure free,” said Dr. Penovich.
Failing a first or second AED indicates a greater likelihood that medication will not stop a patient’s seizures, “but it does not mean that you will not be controlled,” Dr. Penovich said. More medications, surgical options, and investigative treatments have become available. Still, AED trials should not prevent a timely referral to an epilepsy center. “You don’t need to go through 10 or 15 before you get referred” to an epilepsy center, she said.
The STEP survey was conducted by Kantar Health on behalf of SK Life Science. Dr. Penovich has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from SK Life Science, Neurelis, GW Pharmaceuticals, Engage Therapeutics, and UCB Pharma. A coauthor was employed by Kantar Health. Other coauthors disclosed compensation from SK Life Science and various pharmaceutical companies.
SOURCE: Penovich PE et al. AAN 2020, Abstract S59.007.
according to survey results presented online as part of the 2020 American Academy of Neurology Science Highlights.
Clinicians, for their part, may underestimate the number of seizures that go unreported. This disconnect may contribute to complacency about epilepsy treatment regimens among patients, caregivers, and health care professionals (HCPs), despite continuations in seizures. “Improved reporting of all seizure occurrences and more frequent discussion of potential treatment changes, initiated by all groups, may be needed to optimize treatment outcomes,” said Patricia E. Penovich, MD, a neurologist at Minnesota Epilepsy Group in St. Paul, and colleagues.
To evaluate treatment complacency among adult patients with epilepsy, caregivers, and HCPs, Dr. Penovich and collaborators analyzed data from the STEP survey (Seize the Truth about Epilepsy Perceptions), which was conducted between February and March 2019. In all, 400 adults with epilepsy, 201 caregivers, and 258 HCPs completed the survey. The HCPs included 96 epileptologists, 112 general neurologists, and 50 nurse practitioners or physician assistants.
Patients had an average epilepsy duration of 16 years, and 58% were on at least their third antiepileptic drug (AED). In the past year, 52% of patients had 1-9 seizures, and 31% had 10 or more seizures. “Patients estimated reporting 45% of their seizures to their HCPs, and for the seizures not reported, 57% provided reasoning that they were not serious enough to mention,” reported Dr. Penovich and colleagues. “Alternatively, HCPs estimated that patients report 73% of seizures.”
Survey participants most frequently selected HCPs as the ones to initiate conversations about changing AEDs or increasing dosage. “Patient-initiated discussions were reported by 39% of patients for changing AEDs and 27% of patients for increasing AED dosage; 25% of patients reported they were likely to ask their HCP about changing treatments in the next 12 months,” the authors said. Discussion of vagus nerve stimulation was reported by 21% of HCPs, and 10% reported discussion of responsive neurostimulation. HCPs also discussed surgical options such as hemispherectomy (3%), corpus callosotomy and multiple subpial transection (4%), lobe resection (8%), and lesionectomy (11%).
Among patients with 13 or more seizures per year, 27% reported referral to an epilepsy center. Most survey participants – 61% of patients and HCPs and 68% of caregivers – “reported a desire for a treatment map that tells patients to see an epileptologist/specialist as soon as they have symptoms,” the researchers said.
“What we would like to think is that we are getting the whole scoop and the honest scoop” about seizure activity, Dr. Penovich said in an interview. “What this shows us is that that’s probably not always true. Some health care providers understand that the patients do not tell them everything,” but the degree of seizure underreporting may be surprising.
Dr. Penovich has seen this phenomenon in practice. In some cases, caregivers return to the office to explain that a patient did not report all of their seizures. Other patients may omit entire days of seizures in their diaries as an oversight. In addition, patients may not report seizures to avoid having a driver’s license revoked. In some instances, clinicians may not take the time to discuss seizure activity in detail.
Having an accurate picture of seizure activity is an “important part of working with our patients, particularly when we are trying to get them to the point of being seizure free,” said Dr. Penovich.
Failing a first or second AED indicates a greater likelihood that medication will not stop a patient’s seizures, “but it does not mean that you will not be controlled,” Dr. Penovich said. More medications, surgical options, and investigative treatments have become available. Still, AED trials should not prevent a timely referral to an epilepsy center. “You don’t need to go through 10 or 15 before you get referred” to an epilepsy center, she said.
The STEP survey was conducted by Kantar Health on behalf of SK Life Science. Dr. Penovich has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from SK Life Science, Neurelis, GW Pharmaceuticals, Engage Therapeutics, and UCB Pharma. A coauthor was employed by Kantar Health. Other coauthors disclosed compensation from SK Life Science and various pharmaceutical companies.
SOURCE: Penovich PE et al. AAN 2020, Abstract S59.007.
according to survey results presented online as part of the 2020 American Academy of Neurology Science Highlights.
Clinicians, for their part, may underestimate the number of seizures that go unreported. This disconnect may contribute to complacency about epilepsy treatment regimens among patients, caregivers, and health care professionals (HCPs), despite continuations in seizures. “Improved reporting of all seizure occurrences and more frequent discussion of potential treatment changes, initiated by all groups, may be needed to optimize treatment outcomes,” said Patricia E. Penovich, MD, a neurologist at Minnesota Epilepsy Group in St. Paul, and colleagues.
To evaluate treatment complacency among adult patients with epilepsy, caregivers, and HCPs, Dr. Penovich and collaborators analyzed data from the STEP survey (Seize the Truth about Epilepsy Perceptions), which was conducted between February and March 2019. In all, 400 adults with epilepsy, 201 caregivers, and 258 HCPs completed the survey. The HCPs included 96 epileptologists, 112 general neurologists, and 50 nurse practitioners or physician assistants.
Patients had an average epilepsy duration of 16 years, and 58% were on at least their third antiepileptic drug (AED). In the past year, 52% of patients had 1-9 seizures, and 31% had 10 or more seizures. “Patients estimated reporting 45% of their seizures to their HCPs, and for the seizures not reported, 57% provided reasoning that they were not serious enough to mention,” reported Dr. Penovich and colleagues. “Alternatively, HCPs estimated that patients report 73% of seizures.”
Survey participants most frequently selected HCPs as the ones to initiate conversations about changing AEDs or increasing dosage. “Patient-initiated discussions were reported by 39% of patients for changing AEDs and 27% of patients for increasing AED dosage; 25% of patients reported they were likely to ask their HCP about changing treatments in the next 12 months,” the authors said. Discussion of vagus nerve stimulation was reported by 21% of HCPs, and 10% reported discussion of responsive neurostimulation. HCPs also discussed surgical options such as hemispherectomy (3%), corpus callosotomy and multiple subpial transection (4%), lobe resection (8%), and lesionectomy (11%).
Among patients with 13 or more seizures per year, 27% reported referral to an epilepsy center. Most survey participants – 61% of patients and HCPs and 68% of caregivers – “reported a desire for a treatment map that tells patients to see an epileptologist/specialist as soon as they have symptoms,” the researchers said.
“What we would like to think is that we are getting the whole scoop and the honest scoop” about seizure activity, Dr. Penovich said in an interview. “What this shows us is that that’s probably not always true. Some health care providers understand that the patients do not tell them everything,” but the degree of seizure underreporting may be surprising.
Dr. Penovich has seen this phenomenon in practice. In some cases, caregivers return to the office to explain that a patient did not report all of their seizures. Other patients may omit entire days of seizures in their diaries as an oversight. In addition, patients may not report seizures to avoid having a driver’s license revoked. In some instances, clinicians may not take the time to discuss seizure activity in detail.
Having an accurate picture of seizure activity is an “important part of working with our patients, particularly when we are trying to get them to the point of being seizure free,” said Dr. Penovich.
Failing a first or second AED indicates a greater likelihood that medication will not stop a patient’s seizures, “but it does not mean that you will not be controlled,” Dr. Penovich said. More medications, surgical options, and investigative treatments have become available. Still, AED trials should not prevent a timely referral to an epilepsy center. “You don’t need to go through 10 or 15 before you get referred” to an epilepsy center, she said.
The STEP survey was conducted by Kantar Health on behalf of SK Life Science. Dr. Penovich has received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities from SK Life Science, Neurelis, GW Pharmaceuticals, Engage Therapeutics, and UCB Pharma. A coauthor was employed by Kantar Health. Other coauthors disclosed compensation from SK Life Science and various pharmaceutical companies.
SOURCE: Penovich PE et al. AAN 2020, Abstract S59.007.
FROM AAN 2020
Statins and ICH: new meta-analysis
The meta-analysis was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Coauthor Abhi Pandhi, MD, the University of Tennessee Health Science Center, Memphis, explained that some previous studies have suggested that statin therapy may be associated with an increased risk for ICH, especially at higher doses. Other studies, however, have failed to confirm this and have shown an increase in cardiovascular events if statins are stopped.
To look further into this issue, Dr. Pandhi and colleagues conducted a meta-analysis of 19 clinical studies involving patients who had a history of cardiovascular or cerebrovascular events and who had been treated with statins. A total of 35,842 patients were included.
Results showed that statin use was not significantly associated with the risk for combined primary and secondary ICH (relative risk, 1.03; 95% confidence interval, 0.85–1.08). But the risk for cerebral ischemia (stroke and transient ischemic attack) was significantly lower in those who received statins (RR, 0.79; 95% CI, 0.61–0.87).
“Overall, we found no effect of statins on the risk of ICH, and benefits on reducing ischemic events are clear,” Dr. Pandhi said.
Increased secondary ICH?
However, a sensitivity analysis showed a trend toward a higher risk for secondary ICH among those who were assigned to statin treatment (odds ratio, 1.87; 95% CI, 0.91–3.86).
“While this may suggest an increased risk of secondary ICH, when we look at the big picture, putting all the data together, and given that ischemic events are far more common than ICH, the risk of stopping statins and losing the protection against ischemic events is probably greater than any harm even in patients with underlying risk factors for ICH,” Dr. Pandhi concluded.
Commenting on the study, Michael Szarek, PhD, who has also conducted research in this field, said: “The results of this meta-analysis appear to be consistent with individual randomized trials of statins in patients with cerebrovascular disease that have shown clear benefit in terms of ischemic stroke or TIA and potential harm in terms of hemorrhagic stroke.”
Dr. Szarek is chair and professor in the Department of Epidemiology and Biostatistics at the SUNY Downstate Health Sciences University, New York City.
“However, the much greater frequency of ischemic events, coupled with benefits in coronary and peripheral vascular territories, suggest the risk/benefit of statin treatment remains favorable in this patient population, with the possible exception of patients with a history of hemorrhagic stroke,” he added.
Also commenting on this latest meta-analysis, Pamela Rist, ScD, associate epidemiologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston, who has also authored studies in this area, said the results of this study seem similar to prior results from meta-analyses of clinical trials.
“It will be interesting to see the full manuscript to learn more about the sensitivity analyses they conducted and why they may have observed a nonsignificant increased risk of secondary ICH among some individuals using statins,” Dr. Rist added.
“Based on prior published meta-analyses of statin use and ICH, any potential increase in risk of hemorrhagic stroke is probably outweighed by the reduction in ischemic stroke and other cardiovascular events,” she concluded.
Dr. Pandhi has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Ishfaq A et al. AAN 2020. Abstract S9.010.
The meta-analysis was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Coauthor Abhi Pandhi, MD, the University of Tennessee Health Science Center, Memphis, explained that some previous studies have suggested that statin therapy may be associated with an increased risk for ICH, especially at higher doses. Other studies, however, have failed to confirm this and have shown an increase in cardiovascular events if statins are stopped.
To look further into this issue, Dr. Pandhi and colleagues conducted a meta-analysis of 19 clinical studies involving patients who had a history of cardiovascular or cerebrovascular events and who had been treated with statins. A total of 35,842 patients were included.
Results showed that statin use was not significantly associated with the risk for combined primary and secondary ICH (relative risk, 1.03; 95% confidence interval, 0.85–1.08). But the risk for cerebral ischemia (stroke and transient ischemic attack) was significantly lower in those who received statins (RR, 0.79; 95% CI, 0.61–0.87).
“Overall, we found no effect of statins on the risk of ICH, and benefits on reducing ischemic events are clear,” Dr. Pandhi said.
Increased secondary ICH?
However, a sensitivity analysis showed a trend toward a higher risk for secondary ICH among those who were assigned to statin treatment (odds ratio, 1.87; 95% CI, 0.91–3.86).
“While this may suggest an increased risk of secondary ICH, when we look at the big picture, putting all the data together, and given that ischemic events are far more common than ICH, the risk of stopping statins and losing the protection against ischemic events is probably greater than any harm even in patients with underlying risk factors for ICH,” Dr. Pandhi concluded.
Commenting on the study, Michael Szarek, PhD, who has also conducted research in this field, said: “The results of this meta-analysis appear to be consistent with individual randomized trials of statins in patients with cerebrovascular disease that have shown clear benefit in terms of ischemic stroke or TIA and potential harm in terms of hemorrhagic stroke.”
Dr. Szarek is chair and professor in the Department of Epidemiology and Biostatistics at the SUNY Downstate Health Sciences University, New York City.
“However, the much greater frequency of ischemic events, coupled with benefits in coronary and peripheral vascular territories, suggest the risk/benefit of statin treatment remains favorable in this patient population, with the possible exception of patients with a history of hemorrhagic stroke,” he added.
Also commenting on this latest meta-analysis, Pamela Rist, ScD, associate epidemiologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston, who has also authored studies in this area, said the results of this study seem similar to prior results from meta-analyses of clinical trials.
“It will be interesting to see the full manuscript to learn more about the sensitivity analyses they conducted and why they may have observed a nonsignificant increased risk of secondary ICH among some individuals using statins,” Dr. Rist added.
“Based on prior published meta-analyses of statin use and ICH, any potential increase in risk of hemorrhagic stroke is probably outweighed by the reduction in ischemic stroke and other cardiovascular events,” she concluded.
Dr. Pandhi has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Ishfaq A et al. AAN 2020. Abstract S9.010.
The meta-analysis was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Coauthor Abhi Pandhi, MD, the University of Tennessee Health Science Center, Memphis, explained that some previous studies have suggested that statin therapy may be associated with an increased risk for ICH, especially at higher doses. Other studies, however, have failed to confirm this and have shown an increase in cardiovascular events if statins are stopped.
To look further into this issue, Dr. Pandhi and colleagues conducted a meta-analysis of 19 clinical studies involving patients who had a history of cardiovascular or cerebrovascular events and who had been treated with statins. A total of 35,842 patients were included.
Results showed that statin use was not significantly associated with the risk for combined primary and secondary ICH (relative risk, 1.03; 95% confidence interval, 0.85–1.08). But the risk for cerebral ischemia (stroke and transient ischemic attack) was significantly lower in those who received statins (RR, 0.79; 95% CI, 0.61–0.87).
“Overall, we found no effect of statins on the risk of ICH, and benefits on reducing ischemic events are clear,” Dr. Pandhi said.
Increased secondary ICH?
However, a sensitivity analysis showed a trend toward a higher risk for secondary ICH among those who were assigned to statin treatment (odds ratio, 1.87; 95% CI, 0.91–3.86).
“While this may suggest an increased risk of secondary ICH, when we look at the big picture, putting all the data together, and given that ischemic events are far more common than ICH, the risk of stopping statins and losing the protection against ischemic events is probably greater than any harm even in patients with underlying risk factors for ICH,” Dr. Pandhi concluded.
Commenting on the study, Michael Szarek, PhD, who has also conducted research in this field, said: “The results of this meta-analysis appear to be consistent with individual randomized trials of statins in patients with cerebrovascular disease that have shown clear benefit in terms of ischemic stroke or TIA and potential harm in terms of hemorrhagic stroke.”
Dr. Szarek is chair and professor in the Department of Epidemiology and Biostatistics at the SUNY Downstate Health Sciences University, New York City.
“However, the much greater frequency of ischemic events, coupled with benefits in coronary and peripheral vascular territories, suggest the risk/benefit of statin treatment remains favorable in this patient population, with the possible exception of patients with a history of hemorrhagic stroke,” he added.
Also commenting on this latest meta-analysis, Pamela Rist, ScD, associate epidemiologist at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, Boston, who has also authored studies in this area, said the results of this study seem similar to prior results from meta-analyses of clinical trials.
“It will be interesting to see the full manuscript to learn more about the sensitivity analyses they conducted and why they may have observed a nonsignificant increased risk of secondary ICH among some individuals using statins,” Dr. Rist added.
“Based on prior published meta-analyses of statin use and ICH, any potential increase in risk of hemorrhagic stroke is probably outweighed by the reduction in ischemic stroke and other cardiovascular events,” she concluded.
Dr. Pandhi has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Ishfaq A et al. AAN 2020. Abstract S9.010.
AAN 2020
GI symptoms in Parkinson’s disease correlate with less microbial diversity
according to research presented online as part of the 2020 American Academy of Neurology Science Highlights.
Jade E. Kenna, a PhD candidate and research assistant at the Perron Institute of Neurological and Translational Science in Perth, Australia, described findings from a multicenter assessment of 167 patients with Parkinson’s disease and 100 controls from movement disorders clinics in Australia. Participants completed the self-report Gastrointestinal Symptom Rating Scale (GSRS), which rates the frequency and severity of 15 GI symptoms. In addition, stool samples were analyzed using targeted sequencing to characterize gut microbiome composition.
Although Parkinson’s disease is recognized primarily as a motor disorder, GI dysfunction may be one of the first symptoms. “This is hypothesized to result from a change in microbiota towards an inflammatory, dysbiotic composition,” Ms. Kenna said. A limited number of studies have reported an association between altered microbiota composition, GI symptoms, and Parkinson’s disease, but not in Australian cohorts.
Total GSRS score was significantly higher in patients with Parkinson’s disease, compared with controls. Eight of the symptoms – heartburn, acid reflux, nausea or vomiting, borborygmus, increased flatus, decreased passage of stools, feeling of incomplete evacuation, and passing hard stools – were significantly increased in patients with Parkinson’s disease. GSRS symptoms can be categorized as upper, lower, general, hypoactive, or hyperactive, and patients with Parkinson’s disease had significantly increased ratings in the upper, lower, and hypoactive GI symptom domains.
“This is quite a novel finding as not only has this not been assessed in an Australian cohort of individuals before, but the majority of existing literature focuses on the presence of constipation only,” Ms. Kenna said. “The treatment and understanding of nonmotor symptoms of Parkinson’s disease, in particular GI symptoms, remain as one of the top unmet needs reported by patients with Parkinson’s disease themselves. Therefore, a better, more thorough understanding of these symptoms is clearly needed, and research into this area has such value in terms of improving current therapeutic approaches, management strategies, and patient education.”
Microbial analyses found that Firmicutes and Proteobacteria were significantly increased and Verrucomicrobia trended toward an increase in patients with Parkinson’s disease. Fusobacteria was increased in controls. “Proteobacteria and Verrucomicrobia are known to promote inflammation, which can lead to GI symptoms. Furthermore, Faecalibacterium and Ruminococcus, which are reduced in [Parkinson’s disease], can metabolize various substrates to produce [short-chain fatty acids] like butyrate, which are known to aid against intestinal barrier dysfunction and inflammation,” she said.
Individuals with Parkinson’s disease had significantly less microbial diversity. As Parkinson’s disease severity and GI symptom severity increased, microbiome diversity decreased, Ms. Kenna said. “As reduced diversity is associated with increased intestinal inflammation, this indicates that the altered microbiome we saw in [individuals with Parkinson’s disease] may be instigating the increase in incidence and severity of GI symptoms.”
Ms. Kenna reported that she had no disclosures.
SOURCE: Kenna JE. AAN 2020, Abstract S17.006.
according to research presented online as part of the 2020 American Academy of Neurology Science Highlights.
Jade E. Kenna, a PhD candidate and research assistant at the Perron Institute of Neurological and Translational Science in Perth, Australia, described findings from a multicenter assessment of 167 patients with Parkinson’s disease and 100 controls from movement disorders clinics in Australia. Participants completed the self-report Gastrointestinal Symptom Rating Scale (GSRS), which rates the frequency and severity of 15 GI symptoms. In addition, stool samples were analyzed using targeted sequencing to characterize gut microbiome composition.
Although Parkinson’s disease is recognized primarily as a motor disorder, GI dysfunction may be one of the first symptoms. “This is hypothesized to result from a change in microbiota towards an inflammatory, dysbiotic composition,” Ms. Kenna said. A limited number of studies have reported an association between altered microbiota composition, GI symptoms, and Parkinson’s disease, but not in Australian cohorts.
Total GSRS score was significantly higher in patients with Parkinson’s disease, compared with controls. Eight of the symptoms – heartburn, acid reflux, nausea or vomiting, borborygmus, increased flatus, decreased passage of stools, feeling of incomplete evacuation, and passing hard stools – were significantly increased in patients with Parkinson’s disease. GSRS symptoms can be categorized as upper, lower, general, hypoactive, or hyperactive, and patients with Parkinson’s disease had significantly increased ratings in the upper, lower, and hypoactive GI symptom domains.
“This is quite a novel finding as not only has this not been assessed in an Australian cohort of individuals before, but the majority of existing literature focuses on the presence of constipation only,” Ms. Kenna said. “The treatment and understanding of nonmotor symptoms of Parkinson’s disease, in particular GI symptoms, remain as one of the top unmet needs reported by patients with Parkinson’s disease themselves. Therefore, a better, more thorough understanding of these symptoms is clearly needed, and research into this area has such value in terms of improving current therapeutic approaches, management strategies, and patient education.”
Microbial analyses found that Firmicutes and Proteobacteria were significantly increased and Verrucomicrobia trended toward an increase in patients with Parkinson’s disease. Fusobacteria was increased in controls. “Proteobacteria and Verrucomicrobia are known to promote inflammation, which can lead to GI symptoms. Furthermore, Faecalibacterium and Ruminococcus, which are reduced in [Parkinson’s disease], can metabolize various substrates to produce [short-chain fatty acids] like butyrate, which are known to aid against intestinal barrier dysfunction and inflammation,” she said.
Individuals with Parkinson’s disease had significantly less microbial diversity. As Parkinson’s disease severity and GI symptom severity increased, microbiome diversity decreased, Ms. Kenna said. “As reduced diversity is associated with increased intestinal inflammation, this indicates that the altered microbiome we saw in [individuals with Parkinson’s disease] may be instigating the increase in incidence and severity of GI symptoms.”
Ms. Kenna reported that she had no disclosures.
SOURCE: Kenna JE. AAN 2020, Abstract S17.006.
according to research presented online as part of the 2020 American Academy of Neurology Science Highlights.
Jade E. Kenna, a PhD candidate and research assistant at the Perron Institute of Neurological and Translational Science in Perth, Australia, described findings from a multicenter assessment of 167 patients with Parkinson’s disease and 100 controls from movement disorders clinics in Australia. Participants completed the self-report Gastrointestinal Symptom Rating Scale (GSRS), which rates the frequency and severity of 15 GI symptoms. In addition, stool samples were analyzed using targeted sequencing to characterize gut microbiome composition.
Although Parkinson’s disease is recognized primarily as a motor disorder, GI dysfunction may be one of the first symptoms. “This is hypothesized to result from a change in microbiota towards an inflammatory, dysbiotic composition,” Ms. Kenna said. A limited number of studies have reported an association between altered microbiota composition, GI symptoms, and Parkinson’s disease, but not in Australian cohorts.
Total GSRS score was significantly higher in patients with Parkinson’s disease, compared with controls. Eight of the symptoms – heartburn, acid reflux, nausea or vomiting, borborygmus, increased flatus, decreased passage of stools, feeling of incomplete evacuation, and passing hard stools – were significantly increased in patients with Parkinson’s disease. GSRS symptoms can be categorized as upper, lower, general, hypoactive, or hyperactive, and patients with Parkinson’s disease had significantly increased ratings in the upper, lower, and hypoactive GI symptom domains.
“This is quite a novel finding as not only has this not been assessed in an Australian cohort of individuals before, but the majority of existing literature focuses on the presence of constipation only,” Ms. Kenna said. “The treatment and understanding of nonmotor symptoms of Parkinson’s disease, in particular GI symptoms, remain as one of the top unmet needs reported by patients with Parkinson’s disease themselves. Therefore, a better, more thorough understanding of these symptoms is clearly needed, and research into this area has such value in terms of improving current therapeutic approaches, management strategies, and patient education.”
Microbial analyses found that Firmicutes and Proteobacteria were significantly increased and Verrucomicrobia trended toward an increase in patients with Parkinson’s disease. Fusobacteria was increased in controls. “Proteobacteria and Verrucomicrobia are known to promote inflammation, which can lead to GI symptoms. Furthermore, Faecalibacterium and Ruminococcus, which are reduced in [Parkinson’s disease], can metabolize various substrates to produce [short-chain fatty acids] like butyrate, which are known to aid against intestinal barrier dysfunction and inflammation,” she said.
Individuals with Parkinson’s disease had significantly less microbial diversity. As Parkinson’s disease severity and GI symptom severity increased, microbiome diversity decreased, Ms. Kenna said. “As reduced diversity is associated with increased intestinal inflammation, this indicates that the altered microbiome we saw in [individuals with Parkinson’s disease] may be instigating the increase in incidence and severity of GI symptoms.”
Ms. Kenna reported that she had no disclosures.
SOURCE: Kenna JE. AAN 2020, Abstract S17.006.
FROM AAN 2020
Initial high-efficacy MS therapy tied to less disability later
new research suggests. However, there is a trade-off: In this study of nearly 300 patients, those treated with initial HET experienced more disease activity in the first 2 years than other participants.
The HET benefit emerged between 2 and 10 years into the study. For example, the mean Expanded Disability Status Scale (EDSS) scores were significantly lower at 6 years in the early, aggressive treatment group than in the later HET group (2.4 vs 3.3, respectively).
“Treatment decisions made around the time of diagnosis will affect long-term outcomes,” said lead author Anna He, MBBS, currently with the Department of Clinical Neuroscience, Karolinska Institute, Stockholm, and the UCL Queen Square Institute of Neurology in London.
Using the most efficacious disease-modifying therapies from the start minimizes disability, “whereas those patients escalating to high-efficacy disease-modifying therapies later do not seem to catch up to those who commenced earlier,” Dr. He said.
“Patients and clinicians should be aware of this when choosing treatment in early MS,” she added.
This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Patient-centered outcome
Instead of measures of brain volume, lesion count, serum neurofilament, or other biomarkers that are mainly of interest to clinicians and scientists, “the main outcome of interest to our patients is their disability,” Dr. He said. “The first question they ask at diagnosis is usually along the lines of: ‘What will my disability be in 10 years?’ ”
“This is what matters to patients and is fundamentally what motivated this study,” Dr. He added.
The investigators searched international MS registries for patients with relapsing-remitting MS starting HET, which included rituximab, ocrelizumab, mitoxantrone, alemtuzumab, or natalizumab.
They compared 117 participants who started HET within the first 2 years of clinical disease onset (the early group) with 181 participants who started HET after more than 4 years (the late group). All were followed for a median of 7.4 years (range, 6.4 to 8.6 years).
Difference in EDSS scores from baseline was the primary outcome. Both cohorts began the study with a mean EDSS score of 2.4, but between-group differences were significant at 10 years.
The secondary outcome of cumulative hazard of disability progression was higher in the early-treatment group from baseline to 2 years. Between the period of 2 and 10 years, the inverse was true.
In patients with highly active MS, “early exposure to high efficacy therapies is recommended,” Dr. He noted.
“We can already affect our patients’ lives enormously by utilizing our current toolbox in the most optimal way. It is our task to optimize this in a data-driven manner.”
Going forward, Dr. He plans to look at other outcomes, including patient-reported quality of life and health economic measures, and to take a different approach to future research.
Rather than assess MS outcomes from a disease-biology perspective, “I will be looking at MS outcomes from the perspective of its key stakeholders—the individual and society,” and the factors that influence them, Dr. He said.
Confirmatory evidence?
Commenting on the findings, Robert Gross, MD, a neurologist at the Rocky Mountain MS Center at the University of Colorado Denver in Aurora, said it is “hard to believe we are still having this debate” about earlier versus later HET.
There are now “numerous studies, including head-to-head trials and large cohort studies, showing superiority of highly efficacious agents to older disease-modifying therapies of more limited efficacy, as well as better outcomes with early versus delayed use of high-efficacy therapy,” said Dr. Gross, who was not involved with the current research.
“This study further adds to the evidence that we should be preferentially starting folks with relapsing-remitting MS right away on high-efficacy therapy, rather than waiting for relapses and disease progression to occur,” he added.
Drs. He and Gross have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
new research suggests. However, there is a trade-off: In this study of nearly 300 patients, those treated with initial HET experienced more disease activity in the first 2 years than other participants.
The HET benefit emerged between 2 and 10 years into the study. For example, the mean Expanded Disability Status Scale (EDSS) scores were significantly lower at 6 years in the early, aggressive treatment group than in the later HET group (2.4 vs 3.3, respectively).
“Treatment decisions made around the time of diagnosis will affect long-term outcomes,” said lead author Anna He, MBBS, currently with the Department of Clinical Neuroscience, Karolinska Institute, Stockholm, and the UCL Queen Square Institute of Neurology in London.
Using the most efficacious disease-modifying therapies from the start minimizes disability, “whereas those patients escalating to high-efficacy disease-modifying therapies later do not seem to catch up to those who commenced earlier,” Dr. He said.
“Patients and clinicians should be aware of this when choosing treatment in early MS,” she added.
This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Patient-centered outcome
Instead of measures of brain volume, lesion count, serum neurofilament, or other biomarkers that are mainly of interest to clinicians and scientists, “the main outcome of interest to our patients is their disability,” Dr. He said. “The first question they ask at diagnosis is usually along the lines of: ‘What will my disability be in 10 years?’ ”
“This is what matters to patients and is fundamentally what motivated this study,” Dr. He added.
The investigators searched international MS registries for patients with relapsing-remitting MS starting HET, which included rituximab, ocrelizumab, mitoxantrone, alemtuzumab, or natalizumab.
They compared 117 participants who started HET within the first 2 years of clinical disease onset (the early group) with 181 participants who started HET after more than 4 years (the late group). All were followed for a median of 7.4 years (range, 6.4 to 8.6 years).
Difference in EDSS scores from baseline was the primary outcome. Both cohorts began the study with a mean EDSS score of 2.4, but between-group differences were significant at 10 years.
The secondary outcome of cumulative hazard of disability progression was higher in the early-treatment group from baseline to 2 years. Between the period of 2 and 10 years, the inverse was true.
In patients with highly active MS, “early exposure to high efficacy therapies is recommended,” Dr. He noted.
“We can already affect our patients’ lives enormously by utilizing our current toolbox in the most optimal way. It is our task to optimize this in a data-driven manner.”
Going forward, Dr. He plans to look at other outcomes, including patient-reported quality of life and health economic measures, and to take a different approach to future research.
Rather than assess MS outcomes from a disease-biology perspective, “I will be looking at MS outcomes from the perspective of its key stakeholders—the individual and society,” and the factors that influence them, Dr. He said.
Confirmatory evidence?
Commenting on the findings, Robert Gross, MD, a neurologist at the Rocky Mountain MS Center at the University of Colorado Denver in Aurora, said it is “hard to believe we are still having this debate” about earlier versus later HET.
There are now “numerous studies, including head-to-head trials and large cohort studies, showing superiority of highly efficacious agents to older disease-modifying therapies of more limited efficacy, as well as better outcomes with early versus delayed use of high-efficacy therapy,” said Dr. Gross, who was not involved with the current research.
“This study further adds to the evidence that we should be preferentially starting folks with relapsing-remitting MS right away on high-efficacy therapy, rather than waiting for relapses and disease progression to occur,” he added.
Drs. He and Gross have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
new research suggests. However, there is a trade-off: In this study of nearly 300 patients, those treated with initial HET experienced more disease activity in the first 2 years than other participants.
The HET benefit emerged between 2 and 10 years into the study. For example, the mean Expanded Disability Status Scale (EDSS) scores were significantly lower at 6 years in the early, aggressive treatment group than in the later HET group (2.4 vs 3.3, respectively).
“Treatment decisions made around the time of diagnosis will affect long-term outcomes,” said lead author Anna He, MBBS, currently with the Department of Clinical Neuroscience, Karolinska Institute, Stockholm, and the UCL Queen Square Institute of Neurology in London.
Using the most efficacious disease-modifying therapies from the start minimizes disability, “whereas those patients escalating to high-efficacy disease-modifying therapies later do not seem to catch up to those who commenced earlier,” Dr. He said.
“Patients and clinicians should be aware of this when choosing treatment in early MS,” she added.
This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Patient-centered outcome
Instead of measures of brain volume, lesion count, serum neurofilament, or other biomarkers that are mainly of interest to clinicians and scientists, “the main outcome of interest to our patients is their disability,” Dr. He said. “The first question they ask at diagnosis is usually along the lines of: ‘What will my disability be in 10 years?’ ”
“This is what matters to patients and is fundamentally what motivated this study,” Dr. He added.
The investigators searched international MS registries for patients with relapsing-remitting MS starting HET, which included rituximab, ocrelizumab, mitoxantrone, alemtuzumab, or natalizumab.
They compared 117 participants who started HET within the first 2 years of clinical disease onset (the early group) with 181 participants who started HET after more than 4 years (the late group). All were followed for a median of 7.4 years (range, 6.4 to 8.6 years).
Difference in EDSS scores from baseline was the primary outcome. Both cohorts began the study with a mean EDSS score of 2.4, but between-group differences were significant at 10 years.
The secondary outcome of cumulative hazard of disability progression was higher in the early-treatment group from baseline to 2 years. Between the period of 2 and 10 years, the inverse was true.
In patients with highly active MS, “early exposure to high efficacy therapies is recommended,” Dr. He noted.
“We can already affect our patients’ lives enormously by utilizing our current toolbox in the most optimal way. It is our task to optimize this in a data-driven manner.”
Going forward, Dr. He plans to look at other outcomes, including patient-reported quality of life and health economic measures, and to take a different approach to future research.
Rather than assess MS outcomes from a disease-biology perspective, “I will be looking at MS outcomes from the perspective of its key stakeholders—the individual and society,” and the factors that influence them, Dr. He said.
Confirmatory evidence?
Commenting on the findings, Robert Gross, MD, a neurologist at the Rocky Mountain MS Center at the University of Colorado Denver in Aurora, said it is “hard to believe we are still having this debate” about earlier versus later HET.
There are now “numerous studies, including head-to-head trials and large cohort studies, showing superiority of highly efficacious agents to older disease-modifying therapies of more limited efficacy, as well as better outcomes with early versus delayed use of high-efficacy therapy,” said Dr. Gross, who was not involved with the current research.
“This study further adds to the evidence that we should be preferentially starting folks with relapsing-remitting MS right away on high-efficacy therapy, rather than waiting for relapses and disease progression to occur,” he added.
Drs. He and Gross have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Diastolic dysfunction is a common risk factor for cognitive decline
a new study suggests. “We found people with worsening diastolic dysfunction have more white matter hyperintensities on brain imaging and greater difficulty with executive functioning, suggesting that diastolic dysfunction is a common modifiable risk factor for cognitive impairment,” said lead author Alicia S. Parker, MD. Dr. Parker is assistant professor of cognitive and behavioral neurology at the Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases, University of Texas Health, San Antonio.
“This is an entirely new finding. While there have been some small studies suggesting a link between diastolic dysfunction and a reduction in working memory, this is by far the largest dataset on this topic and the first study that has included brain imaging and neuropsychological measures,” she said.
“Diastolic dysfunction is very common in the older population, and we need to do more to find it and treat it to help prevent or reduce cognitive decline,” Dr. Parker added.
This research is being presented online as part of the 2020 American Academy of Neurology Science Highlights.
Dr. Parker explained that systolic dysfunction is known to have a major effect on cardiovascular outcomes and has been found to be associated with cognitive decline. Proposed mechanisms for cognitive decline in patients with systolic dysfunction include low cardiac output, embolic infarctions, and hypoxic changes, among others.
“There is increasing interest in analyzing the influence of diastolic dysfunction on cardiovascular outcomes, and the effects of diastolic dysfunction on cognition are not currently well delineated, which this study seeks to address,” she added.
“While these results are new, they are not surprising. In general, we are finding more and more that heart health is connected to brain health,” she commented.
Dr. Parker and her colleagues started the current research after noticing in clinic that among patients with significant diastolic dysfunction, there were often changes on brain MRI imaging, and the patients often had trouble with executive function. “The effect of diastolic dysfunction on cognition has not been well characterized, so we wanted to look at this,” she said.
The investigators analyzed data from the Framingham Heart Study Offspring Cohort at examination 8, collected between 2005 and 2008. The study sample included 1,438 individuals older than 55 years who had undergone neuropsychological assessment and echocardiographic diastolic measurement. Systolic measurements were normal for the participants, and they did not currently have dementia, stroke, or other neurologic illness.
Results showed that increasing E/E’ ratio (the ratio of mitral peak velocity of early filling to early diastolic mitral annular velocity) indicated increasing diastolic dysfunction and was associated with an increase in the incidence of mild cognitive impairment (hazard ratio, 1.29; 95% confidence interval, 1.01-1.66; P < .043).
An increased E/E’ ratio was associated with increased executive function impairment in the “similarities” (beta, –0.29; P < .002) and “phonemic fluency” (–1.28; P < .001) tasks.
Participants with moderate to severe diastolic dysfunction were more impaired with respect to both similarities (–0.62; P < .046) and phonemic fluency (–2.60; P < .023).
Data from 1,217 participants showed that among those with mild diastolic dysfunction, there was a trend toward an increase in white matter hyperintensities (0.11; P < .105). For participants with moderate to severe diastolic dysfunction, white matter hyperintensities were increased (0.30; P < 0.001).
The results were unchanged after the researchers adjusted for many other predictors of cognitive decline affecting diastolic function.
The researchers conclude: “As cerebral small vessel disease clinically presents with executive dysfunction, these results align well.” They add that replication in additional cohorts and analyses of cognition in treatment trials of diastolic dysfunction are warranted.
Earlier interventions
Commenting on the study, Marco R. Di Tullio, MD, professor of medicine and Columbia University Medical Center, New York City, who is also studying the relationship between subclinical cardiac abnormalities and cognition, said: “This is a promising area of research, as it might allow us to uncover novel risk factors for cognitive decline at an early stage, before the development of clinically manifest cardiac disease, which might allow earlier interventions to decrease or delay the onset of cognitive decline.”
Dr. Di Tullio added that he would like to know more about the interaction between diastolic dysfunction, MRI abnormalities, and cognitive impairment risk. “In this study, MRI abnormalities and cognitive impairment are treated as separate outcomes, with diastolic dysfunction being the exposure for each of them. An additional analysis of the association between diastolic dysfunction and cognitive impairment stratified by presence or absence of brain MRI findings would have been interesting.”
Dr. Parker responded that this is an area of investigation. “We suspect that our cognitive findings would not be explained by any one MRI measure, though a comprehensive examination of MRI findings would be of benefit. The thought that there may be a reversible cardiac abnormality that does not have a structural brain imaging correlate on MRI is an interesting possibility,” she said.
Dr. Di Tullio also pointed out that at present, there is no specific treatment for diastolic dysfunction other than to address some the conditions that predispose to it, such as hypertension and atrial fibrillation.
“We completely agree that specific treatments are an area of investigation and that treatment is therefore targeted at associated modifiable conditions,” Dr. Parker replied.
With regard to more specific estimates of the prevalence of diastolic dysfunction, Dr. Parker cites another Framingham analysis that involved 2,355 persons without any prevalent cardiovascular conditions. That study found that diastolic dysfunction was rare until 50 years of age and then gradually increased with age.
About 5% of people in their 50s had mild diastolic dysfunction, and about 3% had moderate to severe diastolic dysfunction. Among persons in their 60s, about 18% had mild and 5% had severe diastolic dysfunction. Among persons in their 70s, mild diastolic dysfunction occurred in 35%, and moderate to severe disease was present in 18%; and in persons older than 80 years, nearly half had mild and about 20% had moderate to severe diastolic dysfunction.
Dr. Parker has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
a new study suggests. “We found people with worsening diastolic dysfunction have more white matter hyperintensities on brain imaging and greater difficulty with executive functioning, suggesting that diastolic dysfunction is a common modifiable risk factor for cognitive impairment,” said lead author Alicia S. Parker, MD. Dr. Parker is assistant professor of cognitive and behavioral neurology at the Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases, University of Texas Health, San Antonio.
“This is an entirely new finding. While there have been some small studies suggesting a link between diastolic dysfunction and a reduction in working memory, this is by far the largest dataset on this topic and the first study that has included brain imaging and neuropsychological measures,” she said.
“Diastolic dysfunction is very common in the older population, and we need to do more to find it and treat it to help prevent or reduce cognitive decline,” Dr. Parker added.
This research is being presented online as part of the 2020 American Academy of Neurology Science Highlights.
Dr. Parker explained that systolic dysfunction is known to have a major effect on cardiovascular outcomes and has been found to be associated with cognitive decline. Proposed mechanisms for cognitive decline in patients with systolic dysfunction include low cardiac output, embolic infarctions, and hypoxic changes, among others.
“There is increasing interest in analyzing the influence of diastolic dysfunction on cardiovascular outcomes, and the effects of diastolic dysfunction on cognition are not currently well delineated, which this study seeks to address,” she added.
“While these results are new, they are not surprising. In general, we are finding more and more that heart health is connected to brain health,” she commented.
Dr. Parker and her colleagues started the current research after noticing in clinic that among patients with significant diastolic dysfunction, there were often changes on brain MRI imaging, and the patients often had trouble with executive function. “The effect of diastolic dysfunction on cognition has not been well characterized, so we wanted to look at this,” she said.
The investigators analyzed data from the Framingham Heart Study Offspring Cohort at examination 8, collected between 2005 and 2008. The study sample included 1,438 individuals older than 55 years who had undergone neuropsychological assessment and echocardiographic diastolic measurement. Systolic measurements were normal for the participants, and they did not currently have dementia, stroke, or other neurologic illness.
Results showed that increasing E/E’ ratio (the ratio of mitral peak velocity of early filling to early diastolic mitral annular velocity) indicated increasing diastolic dysfunction and was associated with an increase in the incidence of mild cognitive impairment (hazard ratio, 1.29; 95% confidence interval, 1.01-1.66; P < .043).
An increased E/E’ ratio was associated with increased executive function impairment in the “similarities” (beta, –0.29; P < .002) and “phonemic fluency” (–1.28; P < .001) tasks.
Participants with moderate to severe diastolic dysfunction were more impaired with respect to both similarities (–0.62; P < .046) and phonemic fluency (–2.60; P < .023).
Data from 1,217 participants showed that among those with mild diastolic dysfunction, there was a trend toward an increase in white matter hyperintensities (0.11; P < .105). For participants with moderate to severe diastolic dysfunction, white matter hyperintensities were increased (0.30; P < 0.001).
The results were unchanged after the researchers adjusted for many other predictors of cognitive decline affecting diastolic function.
The researchers conclude: “As cerebral small vessel disease clinically presents with executive dysfunction, these results align well.” They add that replication in additional cohorts and analyses of cognition in treatment trials of diastolic dysfunction are warranted.
Earlier interventions
Commenting on the study, Marco R. Di Tullio, MD, professor of medicine and Columbia University Medical Center, New York City, who is also studying the relationship between subclinical cardiac abnormalities and cognition, said: “This is a promising area of research, as it might allow us to uncover novel risk factors for cognitive decline at an early stage, before the development of clinically manifest cardiac disease, which might allow earlier interventions to decrease or delay the onset of cognitive decline.”
Dr. Di Tullio added that he would like to know more about the interaction between diastolic dysfunction, MRI abnormalities, and cognitive impairment risk. “In this study, MRI abnormalities and cognitive impairment are treated as separate outcomes, with diastolic dysfunction being the exposure for each of them. An additional analysis of the association between diastolic dysfunction and cognitive impairment stratified by presence or absence of brain MRI findings would have been interesting.”
Dr. Parker responded that this is an area of investigation. “We suspect that our cognitive findings would not be explained by any one MRI measure, though a comprehensive examination of MRI findings would be of benefit. The thought that there may be a reversible cardiac abnormality that does not have a structural brain imaging correlate on MRI is an interesting possibility,” she said.
Dr. Di Tullio also pointed out that at present, there is no specific treatment for diastolic dysfunction other than to address some the conditions that predispose to it, such as hypertension and atrial fibrillation.
“We completely agree that specific treatments are an area of investigation and that treatment is therefore targeted at associated modifiable conditions,” Dr. Parker replied.
With regard to more specific estimates of the prevalence of diastolic dysfunction, Dr. Parker cites another Framingham analysis that involved 2,355 persons without any prevalent cardiovascular conditions. That study found that diastolic dysfunction was rare until 50 years of age and then gradually increased with age.
About 5% of people in their 50s had mild diastolic dysfunction, and about 3% had moderate to severe diastolic dysfunction. Among persons in their 60s, about 18% had mild and 5% had severe diastolic dysfunction. Among persons in their 70s, mild diastolic dysfunction occurred in 35%, and moderate to severe disease was present in 18%; and in persons older than 80 years, nearly half had mild and about 20% had moderate to severe diastolic dysfunction.
Dr. Parker has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
a new study suggests. “We found people with worsening diastolic dysfunction have more white matter hyperintensities on brain imaging and greater difficulty with executive functioning, suggesting that diastolic dysfunction is a common modifiable risk factor for cognitive impairment,” said lead author Alicia S. Parker, MD. Dr. Parker is assistant professor of cognitive and behavioral neurology at the Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases, University of Texas Health, San Antonio.
“This is an entirely new finding. While there have been some small studies suggesting a link between diastolic dysfunction and a reduction in working memory, this is by far the largest dataset on this topic and the first study that has included brain imaging and neuropsychological measures,” she said.
“Diastolic dysfunction is very common in the older population, and we need to do more to find it and treat it to help prevent or reduce cognitive decline,” Dr. Parker added.
This research is being presented online as part of the 2020 American Academy of Neurology Science Highlights.
Dr. Parker explained that systolic dysfunction is known to have a major effect on cardiovascular outcomes and has been found to be associated with cognitive decline. Proposed mechanisms for cognitive decline in patients with systolic dysfunction include low cardiac output, embolic infarctions, and hypoxic changes, among others.
“There is increasing interest in analyzing the influence of diastolic dysfunction on cardiovascular outcomes, and the effects of diastolic dysfunction on cognition are not currently well delineated, which this study seeks to address,” she added.
“While these results are new, they are not surprising. In general, we are finding more and more that heart health is connected to brain health,” she commented.
Dr. Parker and her colleagues started the current research after noticing in clinic that among patients with significant diastolic dysfunction, there were often changes on brain MRI imaging, and the patients often had trouble with executive function. “The effect of diastolic dysfunction on cognition has not been well characterized, so we wanted to look at this,” she said.
The investigators analyzed data from the Framingham Heart Study Offspring Cohort at examination 8, collected between 2005 and 2008. The study sample included 1,438 individuals older than 55 years who had undergone neuropsychological assessment and echocardiographic diastolic measurement. Systolic measurements were normal for the participants, and they did not currently have dementia, stroke, or other neurologic illness.
Results showed that increasing E/E’ ratio (the ratio of mitral peak velocity of early filling to early diastolic mitral annular velocity) indicated increasing diastolic dysfunction and was associated with an increase in the incidence of mild cognitive impairment (hazard ratio, 1.29; 95% confidence interval, 1.01-1.66; P < .043).
An increased E/E’ ratio was associated with increased executive function impairment in the “similarities” (beta, –0.29; P < .002) and “phonemic fluency” (–1.28; P < .001) tasks.
Participants with moderate to severe diastolic dysfunction were more impaired with respect to both similarities (–0.62; P < .046) and phonemic fluency (–2.60; P < .023).
Data from 1,217 participants showed that among those with mild diastolic dysfunction, there was a trend toward an increase in white matter hyperintensities (0.11; P < .105). For participants with moderate to severe diastolic dysfunction, white matter hyperintensities were increased (0.30; P < 0.001).
The results were unchanged after the researchers adjusted for many other predictors of cognitive decline affecting diastolic function.
The researchers conclude: “As cerebral small vessel disease clinically presents with executive dysfunction, these results align well.” They add that replication in additional cohorts and analyses of cognition in treatment trials of diastolic dysfunction are warranted.
Earlier interventions
Commenting on the study, Marco R. Di Tullio, MD, professor of medicine and Columbia University Medical Center, New York City, who is also studying the relationship between subclinical cardiac abnormalities and cognition, said: “This is a promising area of research, as it might allow us to uncover novel risk factors for cognitive decline at an early stage, before the development of clinically manifest cardiac disease, which might allow earlier interventions to decrease or delay the onset of cognitive decline.”
Dr. Di Tullio added that he would like to know more about the interaction between diastolic dysfunction, MRI abnormalities, and cognitive impairment risk. “In this study, MRI abnormalities and cognitive impairment are treated as separate outcomes, with diastolic dysfunction being the exposure for each of them. An additional analysis of the association between diastolic dysfunction and cognitive impairment stratified by presence or absence of brain MRI findings would have been interesting.”
Dr. Parker responded that this is an area of investigation. “We suspect that our cognitive findings would not be explained by any one MRI measure, though a comprehensive examination of MRI findings would be of benefit. The thought that there may be a reversible cardiac abnormality that does not have a structural brain imaging correlate on MRI is an interesting possibility,” she said.
Dr. Di Tullio also pointed out that at present, there is no specific treatment for diastolic dysfunction other than to address some the conditions that predispose to it, such as hypertension and atrial fibrillation.
“We completely agree that specific treatments are an area of investigation and that treatment is therefore targeted at associated modifiable conditions,” Dr. Parker replied.
With regard to more specific estimates of the prevalence of diastolic dysfunction, Dr. Parker cites another Framingham analysis that involved 2,355 persons without any prevalent cardiovascular conditions. That study found that diastolic dysfunction was rare until 50 years of age and then gradually increased with age.
About 5% of people in their 50s had mild diastolic dysfunction, and about 3% had moderate to severe diastolic dysfunction. Among persons in their 60s, about 18% had mild and 5% had severe diastolic dysfunction. Among persons in their 70s, mild diastolic dysfunction occurred in 35%, and moderate to severe disease was present in 18%; and in persons older than 80 years, nearly half had mild and about 20% had moderate to severe diastolic dysfunction.
Dr. Parker has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Cautionary findings on acquired immunodeficiency from anti-CD20 MS therapy
, Brandi L. Vollmer, MPH, reported online as part of the 2020 American Academy of Neurology Science Highlights.
The hypogammaglobulinemia was preceded by an IgM of 40 mg/dL or less in 35% of cases and was accompanied by concurrent development of low IgM in another 39%, added Ms. Vollmer, a professional research assistant at the Rocky Mountain Multiple Sclerosis Center at Anschutz Medical Campus, University of Colorado, Denver.
She presented a retrospective study of 527 randomly selected MS patients and another 17 with neuromyelitis optica spectrum disorder who averaged 44 years of age and a 9.2-year disease duration upon commencing rituximab (Rituxan) with close laboratory monitoring. Their mean cumulative rituximab dose during a mean 30.2 months of therapy was 3,312 mg. Ninety-six MS patients eventually switched to ocrelizumab (Ocrevus), accumulating a total dose of 1,175 mg of that anti-CD20 humanized monoclonal antibody.
Absolute lymphocyte count dropped to 500 cells/mm3 or lower in 10.4% of patients at a mean of 11.3 months into anti-CD20 therapy. Low immunoglobulins came later: The mean time to onset of low IgM in affected patients was 19.7 months, and hypogammaglobulinemia, as defined by an IgG of 500 mg/dL or less, occurred at a mean of 36.1 months. Higher cumulative doses of anti-CD20 agents were associated with increased likelihood of hypogammaglobulinemia.
Asked to comment on the research findings, neurologist Nida Laurin, MD, said the Colorado study provides helpful insights into the timing of onset of acquired immunodeficiency in patients on B-cell-targeted therapy.
“This paper informs us that we should monitor our patients much closer for signs of hypogammaglobulinemia and lymphopenia starting with year 2 on therapy, and switch treatment when the threshold is reached. I do expect production of gamma globulins and lymphocytes to recover with discontinuation of anti-CD20 therapy, maybe over a period of 6-10 months. It might also recover with lower-dose therapy because the effect on B cells is dose-dependent,” observed Dr. Laurin, an MS specialist at the Banner Health–University Medicine Neuroscience Institute in Phoenix and the University of Arizona in Tucson.
Her colleague Barry Hendin, MD, noted that there is no consensus regarding the best response to all these changes.
“Some clinicians add IVIG, some change therapies, and some observe only,” said Dr. Hendin, a neurologist at Banner Health–University Medical Center, Phoenix, and clinical professor of neurology at the University of Arizona in Tucson.
However, Dr. Laurin asserted that it would be a mistake for physicians and patients to shrug off anti-CD20 therapy–induced lymphopenia in light of studies demonstrating that lymphopenia and older age are two main risk factors for progressive multifocal leukoencephalopathy in patients on disease-modifying therapies.
“More cases of PML can be expected with continuous use of anti-CD20 therapies if lymphopenia is ignored,” she cautioned.
Depressed levels of IgM and IgG have been associated with increased risk of serious infections. In light of the COVID-19 pandemic and the eventual prospect of a vaccine, it is especially important to avoid putting patients with MS in harm’s way via treatment-induced acquired immunodeficiency, Dr. Laurin said.
Ms. Vollmer reported having no financial conflicts regarding her study. Dr. Laurin reported serving as a speaker or consultant for Alexion, Allergan, Biogen, Bristol-Myers Squibb, EMD Serono, Genentech, Lundbeck, and Sanofi Genzyme. Dr. Hendin serves as a consultant to Biogen, Genentech, Genzyme, EMD Serono, Novartis, and Bristol-Myers Squibb.
SOURCE: Vollmer BL et al. AAN 2020. Abstract S29.002.
, Brandi L. Vollmer, MPH, reported online as part of the 2020 American Academy of Neurology Science Highlights.
The hypogammaglobulinemia was preceded by an IgM of 40 mg/dL or less in 35% of cases and was accompanied by concurrent development of low IgM in another 39%, added Ms. Vollmer, a professional research assistant at the Rocky Mountain Multiple Sclerosis Center at Anschutz Medical Campus, University of Colorado, Denver.
She presented a retrospective study of 527 randomly selected MS patients and another 17 with neuromyelitis optica spectrum disorder who averaged 44 years of age and a 9.2-year disease duration upon commencing rituximab (Rituxan) with close laboratory monitoring. Their mean cumulative rituximab dose during a mean 30.2 months of therapy was 3,312 mg. Ninety-six MS patients eventually switched to ocrelizumab (Ocrevus), accumulating a total dose of 1,175 mg of that anti-CD20 humanized monoclonal antibody.
Absolute lymphocyte count dropped to 500 cells/mm3 or lower in 10.4% of patients at a mean of 11.3 months into anti-CD20 therapy. Low immunoglobulins came later: The mean time to onset of low IgM in affected patients was 19.7 months, and hypogammaglobulinemia, as defined by an IgG of 500 mg/dL or less, occurred at a mean of 36.1 months. Higher cumulative doses of anti-CD20 agents were associated with increased likelihood of hypogammaglobulinemia.
Asked to comment on the research findings, neurologist Nida Laurin, MD, said the Colorado study provides helpful insights into the timing of onset of acquired immunodeficiency in patients on B-cell-targeted therapy.
“This paper informs us that we should monitor our patients much closer for signs of hypogammaglobulinemia and lymphopenia starting with year 2 on therapy, and switch treatment when the threshold is reached. I do expect production of gamma globulins and lymphocytes to recover with discontinuation of anti-CD20 therapy, maybe over a period of 6-10 months. It might also recover with lower-dose therapy because the effect on B cells is dose-dependent,” observed Dr. Laurin, an MS specialist at the Banner Health–University Medicine Neuroscience Institute in Phoenix and the University of Arizona in Tucson.
Her colleague Barry Hendin, MD, noted that there is no consensus regarding the best response to all these changes.
“Some clinicians add IVIG, some change therapies, and some observe only,” said Dr. Hendin, a neurologist at Banner Health–University Medical Center, Phoenix, and clinical professor of neurology at the University of Arizona in Tucson.
However, Dr. Laurin asserted that it would be a mistake for physicians and patients to shrug off anti-CD20 therapy–induced lymphopenia in light of studies demonstrating that lymphopenia and older age are two main risk factors for progressive multifocal leukoencephalopathy in patients on disease-modifying therapies.
“More cases of PML can be expected with continuous use of anti-CD20 therapies if lymphopenia is ignored,” she cautioned.
Depressed levels of IgM and IgG have been associated with increased risk of serious infections. In light of the COVID-19 pandemic and the eventual prospect of a vaccine, it is especially important to avoid putting patients with MS in harm’s way via treatment-induced acquired immunodeficiency, Dr. Laurin said.
Ms. Vollmer reported having no financial conflicts regarding her study. Dr. Laurin reported serving as a speaker or consultant for Alexion, Allergan, Biogen, Bristol-Myers Squibb, EMD Serono, Genentech, Lundbeck, and Sanofi Genzyme. Dr. Hendin serves as a consultant to Biogen, Genentech, Genzyme, EMD Serono, Novartis, and Bristol-Myers Squibb.
SOURCE: Vollmer BL et al. AAN 2020. Abstract S29.002.
, Brandi L. Vollmer, MPH, reported online as part of the 2020 American Academy of Neurology Science Highlights.
The hypogammaglobulinemia was preceded by an IgM of 40 mg/dL or less in 35% of cases and was accompanied by concurrent development of low IgM in another 39%, added Ms. Vollmer, a professional research assistant at the Rocky Mountain Multiple Sclerosis Center at Anschutz Medical Campus, University of Colorado, Denver.
She presented a retrospective study of 527 randomly selected MS patients and another 17 with neuromyelitis optica spectrum disorder who averaged 44 years of age and a 9.2-year disease duration upon commencing rituximab (Rituxan) with close laboratory monitoring. Their mean cumulative rituximab dose during a mean 30.2 months of therapy was 3,312 mg. Ninety-six MS patients eventually switched to ocrelizumab (Ocrevus), accumulating a total dose of 1,175 mg of that anti-CD20 humanized monoclonal antibody.
Absolute lymphocyte count dropped to 500 cells/mm3 or lower in 10.4% of patients at a mean of 11.3 months into anti-CD20 therapy. Low immunoglobulins came later: The mean time to onset of low IgM in affected patients was 19.7 months, and hypogammaglobulinemia, as defined by an IgG of 500 mg/dL or less, occurred at a mean of 36.1 months. Higher cumulative doses of anti-CD20 agents were associated with increased likelihood of hypogammaglobulinemia.
Asked to comment on the research findings, neurologist Nida Laurin, MD, said the Colorado study provides helpful insights into the timing of onset of acquired immunodeficiency in patients on B-cell-targeted therapy.
“This paper informs us that we should monitor our patients much closer for signs of hypogammaglobulinemia and lymphopenia starting with year 2 on therapy, and switch treatment when the threshold is reached. I do expect production of gamma globulins and lymphocytes to recover with discontinuation of anti-CD20 therapy, maybe over a period of 6-10 months. It might also recover with lower-dose therapy because the effect on B cells is dose-dependent,” observed Dr. Laurin, an MS specialist at the Banner Health–University Medicine Neuroscience Institute in Phoenix and the University of Arizona in Tucson.
Her colleague Barry Hendin, MD, noted that there is no consensus regarding the best response to all these changes.
“Some clinicians add IVIG, some change therapies, and some observe only,” said Dr. Hendin, a neurologist at Banner Health–University Medical Center, Phoenix, and clinical professor of neurology at the University of Arizona in Tucson.
However, Dr. Laurin asserted that it would be a mistake for physicians and patients to shrug off anti-CD20 therapy–induced lymphopenia in light of studies demonstrating that lymphopenia and older age are two main risk factors for progressive multifocal leukoencephalopathy in patients on disease-modifying therapies.
“More cases of PML can be expected with continuous use of anti-CD20 therapies if lymphopenia is ignored,” she cautioned.
Depressed levels of IgM and IgG have been associated with increased risk of serious infections. In light of the COVID-19 pandemic and the eventual prospect of a vaccine, it is especially important to avoid putting patients with MS in harm’s way via treatment-induced acquired immunodeficiency, Dr. Laurin said.
Ms. Vollmer reported having no financial conflicts regarding her study. Dr. Laurin reported serving as a speaker or consultant for Alexion, Allergan, Biogen, Bristol-Myers Squibb, EMD Serono, Genentech, Lundbeck, and Sanofi Genzyme. Dr. Hendin serves as a consultant to Biogen, Genentech, Genzyme, EMD Serono, Novartis, and Bristol-Myers Squibb.
SOURCE: Vollmer BL et al. AAN 2020. Abstract S29.002.
REPORTING FROM AAN 2020
Five-year siponimod data support early MS treatment
Among and had a lower annualized relapse rate up to 5 years later, compared with patients who initially received placebo and switched to siponimod. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.

Benefits of siponimod gained during the controlled period were “sustained for up to 5 years, suggesting a continuous effect of siponimod and underlining the advantages of early treatment initiation with siponimod,” the researchers said. Incidence rates of adverse events during the extension study were consistent with those during the controlled treatment period.
The results “highlight the critical importance of early treatment intervention ... to ensure the best possible long-term outcomes for patients with MS who are experiencing progression,” study investigator Bruce Cree, MD, PhD, said in a news release.
“It’s never too early to stay ahead of progression in MS, since the early identification of physical and cognitive changes – even subtle ones – can indicate MS disease progression and therefore allow for timely intervention.” said Dr. Cree, who is clinical research director and George A. Zimmermann Endowed Professor in Multiple Sclerosis at the University of California, San Francisco.
Siponimod, marketed as Mayzent, is a sphingosine 1-phosphate receptor modulator that selectively binds to S1P1 and S1P5 receptors. The oral drug was approved by the Food and Drug Administration in 2019 for the treatment of relapsing forms of MS, including clinically isolated syndrome, relapsing remitting disease, and active secondary progressive disease in adults.
To assess the long-term efficacy and safety of siponimod in patients with secondary progressive MS, Dr. Cree and colleagues analyzed data from patients in the controlled and extension parts of the EXPAND trial. Patients could have had been in the study for as long as 5 years at the data cutoff in April 2019. Efficacy analyses included time to 3-month confirmed disability progression on the Expanded Disability Status Scale (EDSS), time to 6-month confirmed disability progression, time to 6-month confirmed worsening of 4 or more points on the Symbol Digit Modalities Test (SDMT), and annualized relapse rate. In EXPAND, the researchers defined confirmed disability progression as a 1-point increase in EDSS if the baseline score was 3.0-5.0, or a 0.5-point increase if the baseline score was 5.5-6.5.
“Of the 1,224 (74% of 1,651 randomized) patients entering the extension, 878 (72%) were ongoing,” the researchers reported. Patients who received siponimod continuously were less likely to experience 3-month confirmed disability progression and 6-month confirmed disability progression, relative to patients who switched from placebo. In addition, patients who received continuous siponimod treatment had a prolonged time to 6-month confirmed disability progression, compared with patients who switched from placebo. For the 25th percentile of patients, continuous siponimod treatment corresponded to a delay of 54% (21 months vs. 13.6 months). Risk of worsening on the SDMT was reduced by 23% in the continuous siponimod–treatment group. For the 25th percentile of patients, this reduced risk corresponded to a delay of 62% (29.6 months vs. 18.3 months). ARR was 0.054 in the continuous-siponimod group, compared with 0.097 in the group that switched to siponimod from placebo, a reduction of 52%.
Dr. Cree has received personal compensation from Novartis, which markets siponimod, as well as Akili, Alexion, Atara, Biogen, EMD Serono, and TG Therapeutics. His coauthors reported receiving research support and personal compensation from Novartis and other pharmaceutical companies. Several coauthors were Novartis employees.
SOURCE: Kappos L et al. AAN 2020, Abstract S40.003.
Among and had a lower annualized relapse rate up to 5 years later, compared with patients who initially received placebo and switched to siponimod. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Benefits of siponimod gained during the controlled period were “sustained for up to 5 years, suggesting a continuous effect of siponimod and underlining the advantages of early treatment initiation with siponimod,” the researchers said. Incidence rates of adverse events during the extension study were consistent with those during the controlled treatment period.
The results “highlight the critical importance of early treatment intervention ... to ensure the best possible long-term outcomes for patients with MS who are experiencing progression,” study investigator Bruce Cree, MD, PhD, said in a news release.
“It’s never too early to stay ahead of progression in MS, since the early identification of physical and cognitive changes – even subtle ones – can indicate MS disease progression and therefore allow for timely intervention.” said Dr. Cree, who is clinical research director and George A. Zimmermann Endowed Professor in Multiple Sclerosis at the University of California, San Francisco.
Siponimod, marketed as Mayzent, is a sphingosine 1-phosphate receptor modulator that selectively binds to S1P1 and S1P5 receptors. The oral drug was approved by the Food and Drug Administration in 2019 for the treatment of relapsing forms of MS, including clinically isolated syndrome, relapsing remitting disease, and active secondary progressive disease in adults.
To assess the long-term efficacy and safety of siponimod in patients with secondary progressive MS, Dr. Cree and colleagues analyzed data from patients in the controlled and extension parts of the EXPAND trial. Patients could have had been in the study for as long as 5 years at the data cutoff in April 2019. Efficacy analyses included time to 3-month confirmed disability progression on the Expanded Disability Status Scale (EDSS), time to 6-month confirmed disability progression, time to 6-month confirmed worsening of 4 or more points on the Symbol Digit Modalities Test (SDMT), and annualized relapse rate. In EXPAND, the researchers defined confirmed disability progression as a 1-point increase in EDSS if the baseline score was 3.0-5.0, or a 0.5-point increase if the baseline score was 5.5-6.5.
“Of the 1,224 (74% of 1,651 randomized) patients entering the extension, 878 (72%) were ongoing,” the researchers reported. Patients who received siponimod continuously were less likely to experience 3-month confirmed disability progression and 6-month confirmed disability progression, relative to patients who switched from placebo. In addition, patients who received continuous siponimod treatment had a prolonged time to 6-month confirmed disability progression, compared with patients who switched from placebo. For the 25th percentile of patients, continuous siponimod treatment corresponded to a delay of 54% (21 months vs. 13.6 months). Risk of worsening on the SDMT was reduced by 23% in the continuous siponimod–treatment group. For the 25th percentile of patients, this reduced risk corresponded to a delay of 62% (29.6 months vs. 18.3 months). ARR was 0.054 in the continuous-siponimod group, compared with 0.097 in the group that switched to siponimod from placebo, a reduction of 52%.
Dr. Cree has received personal compensation from Novartis, which markets siponimod, as well as Akili, Alexion, Atara, Biogen, EMD Serono, and TG Therapeutics. His coauthors reported receiving research support and personal compensation from Novartis and other pharmaceutical companies. Several coauthors were Novartis employees.
SOURCE: Kappos L et al. AAN 2020, Abstract S40.003.
Among and had a lower annualized relapse rate up to 5 years later, compared with patients who initially received placebo and switched to siponimod. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Benefits of siponimod gained during the controlled period were “sustained for up to 5 years, suggesting a continuous effect of siponimod and underlining the advantages of early treatment initiation with siponimod,” the researchers said. Incidence rates of adverse events during the extension study were consistent with those during the controlled treatment period.
The results “highlight the critical importance of early treatment intervention ... to ensure the best possible long-term outcomes for patients with MS who are experiencing progression,” study investigator Bruce Cree, MD, PhD, said in a news release.
“It’s never too early to stay ahead of progression in MS, since the early identification of physical and cognitive changes – even subtle ones – can indicate MS disease progression and therefore allow for timely intervention.” said Dr. Cree, who is clinical research director and George A. Zimmermann Endowed Professor in Multiple Sclerosis at the University of California, San Francisco.
Siponimod, marketed as Mayzent, is a sphingosine 1-phosphate receptor modulator that selectively binds to S1P1 and S1P5 receptors. The oral drug was approved by the Food and Drug Administration in 2019 for the treatment of relapsing forms of MS, including clinically isolated syndrome, relapsing remitting disease, and active secondary progressive disease in adults.
To assess the long-term efficacy and safety of siponimod in patients with secondary progressive MS, Dr. Cree and colleagues analyzed data from patients in the controlled and extension parts of the EXPAND trial. Patients could have had been in the study for as long as 5 years at the data cutoff in April 2019. Efficacy analyses included time to 3-month confirmed disability progression on the Expanded Disability Status Scale (EDSS), time to 6-month confirmed disability progression, time to 6-month confirmed worsening of 4 or more points on the Symbol Digit Modalities Test (SDMT), and annualized relapse rate. In EXPAND, the researchers defined confirmed disability progression as a 1-point increase in EDSS if the baseline score was 3.0-5.0, or a 0.5-point increase if the baseline score was 5.5-6.5.
“Of the 1,224 (74% of 1,651 randomized) patients entering the extension, 878 (72%) were ongoing,” the researchers reported. Patients who received siponimod continuously were less likely to experience 3-month confirmed disability progression and 6-month confirmed disability progression, relative to patients who switched from placebo. In addition, patients who received continuous siponimod treatment had a prolonged time to 6-month confirmed disability progression, compared with patients who switched from placebo. For the 25th percentile of patients, continuous siponimod treatment corresponded to a delay of 54% (21 months vs. 13.6 months). Risk of worsening on the SDMT was reduced by 23% in the continuous siponimod–treatment group. For the 25th percentile of patients, this reduced risk corresponded to a delay of 62% (29.6 months vs. 18.3 months). ARR was 0.054 in the continuous-siponimod group, compared with 0.097 in the group that switched to siponimod from placebo, a reduction of 52%.
Dr. Cree has received personal compensation from Novartis, which markets siponimod, as well as Akili, Alexion, Atara, Biogen, EMD Serono, and TG Therapeutics. His coauthors reported receiving research support and personal compensation from Novartis and other pharmaceutical companies. Several coauthors were Novartis employees.
SOURCE: Kappos L et al. AAN 2020, Abstract S40.003.
FROM AAN 2020

Economic burden of migraine increases with the number of treatment failures
, researchers wrote. Utilization of health care resources and associated costs are greater among patients with three or more treatment failures, compared with patients with fewer treatment failures. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.

Migraine entails a significant economic burden, including direct costs (e.g., medical costs) and indirect costs (e.g., lost productivity). Information about the burden associated with failed preventive treatments among migraineurs is limited, however. Lawrence C. Newman, MD, director of the division of headache at NYU Langone Health in New York, and colleagues conducted a study to characterize health care resource utilization (HCRU) and its associated costs among migraineurs, stratified by the number of preventive treatment failures.
About one quarter of patients had two treatment failures
Using data from the IBM MarketScan Commercial and Medicare Supplemental database, Dr. Newman and colleagues identified patients who received a new diagnosis of migraine between Jan. 1, 2011, and June 30, 2015. Next, they identified the number of treatment failures during the 2 years following the initial migraine diagnosis. They assessed HCRU and associated costs during the 12 months following an index event. The index was the date of initiation of the second preventive treatment for patients with one treatment failure, the date of initiation of the third treatment for patients with two treatment failures, and the date of initiation of the fourth treatment for patients with three or more treatment failures.
Dr. Newman’s group identified 44,181 patients with incident migraine who had failed preventive treatments. Of this population, 27,112 patients (61.4%) had one treatment failure, 10,583 (24%) had two treatment failures, and 6,486 (14.7%) had three or more treatment failures.
The total medical cost per patient, including emergency room (ER), inpatient (IP), and outpatient (OP) care, increased with increasing number of treatment failures ($10,329 for one, $13,774 for two, and $35,392 for three or more). When the investigators added prescription drug costs, the total health care costs also increased with number of treatment failures ($13,946 for one, $18,685 for two, and $41,864 for three or more).
Similarly, the per-patient annual health care provider visits increased with increasing numbers of treatment failures. The number of ER visits per year was 0.54, 0.69, and 1.02 for patients with one, two, and three or more treatment failures, respectively. The annual number of IP visits was 0.46, 0.59, and 0.97, for patients with one, two, and three or more treatment failures, respectively. OP visits showed a similar trend. The annual number of office visits was 9.47 for patients with one, 11.24 for patients with two, and 14.26 for patients with three or more treatment failures. The annual number of other visits was 13.15 for patients with one, 15.73 for patients with two, and 19.96 for patients with three or more treatment failures.
Guidelines could enable appropriate treatment
Reasons for treatment failure include misdiagnosis of the headache disorder, failure to identify and account for comorbidities, overlooking concurrent acute medication overuse, and inappropriate dose or formulation, said Dr. Newman. “Common pitfalls in prevention that lead to treatment failure include not using evidence-based treatments, starting at too low of a dose and not increasing, starting too high or increasing the dose too quickly, discontinuing the medication before an effect can be seen (before 8 weeks), patient nonadherence, and not establishing realistic expectations.”
Available resources could help clinicians treat migraine effectively. “The American Headache Society (AHS)/AAN preventive guidelines have been retired, yet they offered several levels of effectiveness of pharmacologic treatments that were evidence-based,” said Dr. Newman. “Furthermore, in 2019, the AHS published a consensus statement on integrating new migraine treatments into clinical practice. This statement offered advice about the new anti-CGRP agents, onabotulinum toxin, and neuromodulation devices. I think this is a good starting point for neurologists to be familiar with to choose appropriate therapeutic options for people living with migraine.”
Earlier treatment may reduce patients’ economic burden
The study’s weaknesses included its observational design and its reliance on diagnostic codes, which raised the possibility that comorbidities were inadequately recognized, said Dr. Newman. The reasons that patients changed medications are unknown, and the results are not generalizable to patients aged 65 years or older, he added.
Major strengths of Dr. Newman’s study are its large sample size and wealth of available data, said Alan M. Rapoport, MD, clinical professor of neurology at the University of California, Los Angeles. “The multiple subcategories suggest that this was a carefully organized and implemented study,” he added. If any diagnoses of migraine were provided by general practitioners with little knowledge of migraine, this would weaken the study, said Dr. Rapoport, editor-in-chief of Neurology Reviews.
“We can ease the economic burden of migraineurs by improving acute care therapy with better selection and earlier starting of effective preventive therapy,” he continued. “Going for migraine-specific acute care therapy is better than pain medications or other nonspecific therapies. If you do not stop a migraine attack with effective therapy, you increase the odds that the patient will go on to chronic migraine. It is always important to effectively teach doctors and nurses to improve their diagnostic skills and use the optimal acute and preventive therapy.” For their next trial, maximizing an accurate diagnosis and performing a prospective study measuring treatment outcomes will be particularly valuable, Dr. Rapoport concluded.
Dr. Newman’s study was supported by Novartis Pharma in Basel, Switzerland. Together with Amgen, Novartis developed erenumab. Dr. Newman has received compensation from Allergan, Alder, Amgen, Biohaven, Novartis, Teva, Supernus, and Theranica for consulting, serving on a scientific advisory board, speaking, or other activities. He has received compensation from Springer Scientific for editorial services.
SOURCE: Newman L et al. AAN 2020, Abstract S47.009.
, researchers wrote. Utilization of health care resources and associated costs are greater among patients with three or more treatment failures, compared with patients with fewer treatment failures. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Migraine entails a significant economic burden, including direct costs (e.g., medical costs) and indirect costs (e.g., lost productivity). Information about the burden associated with failed preventive treatments among migraineurs is limited, however. Lawrence C. Newman, MD, director of the division of headache at NYU Langone Health in New York, and colleagues conducted a study to characterize health care resource utilization (HCRU) and its associated costs among migraineurs, stratified by the number of preventive treatment failures.
About one quarter of patients had two treatment failures
Using data from the IBM MarketScan Commercial and Medicare Supplemental database, Dr. Newman and colleagues identified patients who received a new diagnosis of migraine between Jan. 1, 2011, and June 30, 2015. Next, they identified the number of treatment failures during the 2 years following the initial migraine diagnosis. They assessed HCRU and associated costs during the 12 months following an index event. The index was the date of initiation of the second preventive treatment for patients with one treatment failure, the date of initiation of the third treatment for patients with two treatment failures, and the date of initiation of the fourth treatment for patients with three or more treatment failures.
Dr. Newman’s group identified 44,181 patients with incident migraine who had failed preventive treatments. Of this population, 27,112 patients (61.4%) had one treatment failure, 10,583 (24%) had two treatment failures, and 6,486 (14.7%) had three or more treatment failures.
The total medical cost per patient, including emergency room (ER), inpatient (IP), and outpatient (OP) care, increased with increasing number of treatment failures ($10,329 for one, $13,774 for two, and $35,392 for three or more). When the investigators added prescription drug costs, the total health care costs also increased with number of treatment failures ($13,946 for one, $18,685 for two, and $41,864 for three or more).
Similarly, the per-patient annual health care provider visits increased with increasing numbers of treatment failures. The number of ER visits per year was 0.54, 0.69, and 1.02 for patients with one, two, and three or more treatment failures, respectively. The annual number of IP visits was 0.46, 0.59, and 0.97, for patients with one, two, and three or more treatment failures, respectively. OP visits showed a similar trend. The annual number of office visits was 9.47 for patients with one, 11.24 for patients with two, and 14.26 for patients with three or more treatment failures. The annual number of other visits was 13.15 for patients with one, 15.73 for patients with two, and 19.96 for patients with three or more treatment failures.
Guidelines could enable appropriate treatment
Reasons for treatment failure include misdiagnosis of the headache disorder, failure to identify and account for comorbidities, overlooking concurrent acute medication overuse, and inappropriate dose or formulation, said Dr. Newman. “Common pitfalls in prevention that lead to treatment failure include not using evidence-based treatments, starting at too low of a dose and not increasing, starting too high or increasing the dose too quickly, discontinuing the medication before an effect can be seen (before 8 weeks), patient nonadherence, and not establishing realistic expectations.”
Available resources could help clinicians treat migraine effectively. “The American Headache Society (AHS)/AAN preventive guidelines have been retired, yet they offered several levels of effectiveness of pharmacologic treatments that were evidence-based,” said Dr. Newman. “Furthermore, in 2019, the AHS published a consensus statement on integrating new migraine treatments into clinical practice. This statement offered advice about the new anti-CGRP agents, onabotulinum toxin, and neuromodulation devices. I think this is a good starting point for neurologists to be familiar with to choose appropriate therapeutic options for people living with migraine.”
Earlier treatment may reduce patients’ economic burden
The study’s weaknesses included its observational design and its reliance on diagnostic codes, which raised the possibility that comorbidities were inadequately recognized, said Dr. Newman. The reasons that patients changed medications are unknown, and the results are not generalizable to patients aged 65 years or older, he added.
Major strengths of Dr. Newman’s study are its large sample size and wealth of available data, said Alan M. Rapoport, MD, clinical professor of neurology at the University of California, Los Angeles. “The multiple subcategories suggest that this was a carefully organized and implemented study,” he added. If any diagnoses of migraine were provided by general practitioners with little knowledge of migraine, this would weaken the study, said Dr. Rapoport, editor-in-chief of Neurology Reviews.
“We can ease the economic burden of migraineurs by improving acute care therapy with better selection and earlier starting of effective preventive therapy,” he continued. “Going for migraine-specific acute care therapy is better than pain medications or other nonspecific therapies. If you do not stop a migraine attack with effective therapy, you increase the odds that the patient will go on to chronic migraine. It is always important to effectively teach doctors and nurses to improve their diagnostic skills and use the optimal acute and preventive therapy.” For their next trial, maximizing an accurate diagnosis and performing a prospective study measuring treatment outcomes will be particularly valuable, Dr. Rapoport concluded.
Dr. Newman’s study was supported by Novartis Pharma in Basel, Switzerland. Together with Amgen, Novartis developed erenumab. Dr. Newman has received compensation from Allergan, Alder, Amgen, Biohaven, Novartis, Teva, Supernus, and Theranica for consulting, serving on a scientific advisory board, speaking, or other activities. He has received compensation from Springer Scientific for editorial services.
SOURCE: Newman L et al. AAN 2020, Abstract S47.009.
, researchers wrote. Utilization of health care resources and associated costs are greater among patients with three or more treatment failures, compared with patients with fewer treatment failures. This research was presented online as part of the 2020 American Academy of Neurology Science Highlights.
Migraine entails a significant economic burden, including direct costs (e.g., medical costs) and indirect costs (e.g., lost productivity). Information about the burden associated with failed preventive treatments among migraineurs is limited, however. Lawrence C. Newman, MD, director of the division of headache at NYU Langone Health in New York, and colleagues conducted a study to characterize health care resource utilization (HCRU) and its associated costs among migraineurs, stratified by the number of preventive treatment failures.
About one quarter of patients had two treatment failures
Using data from the IBM MarketScan Commercial and Medicare Supplemental database, Dr. Newman and colleagues identified patients who received a new diagnosis of migraine between Jan. 1, 2011, and June 30, 2015. Next, they identified the number of treatment failures during the 2 years following the initial migraine diagnosis. They assessed HCRU and associated costs during the 12 months following an index event. The index was the date of initiation of the second preventive treatment for patients with one treatment failure, the date of initiation of the third treatment for patients with two treatment failures, and the date of initiation of the fourth treatment for patients with three or more treatment failures.
Dr. Newman’s group identified 44,181 patients with incident migraine who had failed preventive treatments. Of this population, 27,112 patients (61.4%) had one treatment failure, 10,583 (24%) had two treatment failures, and 6,486 (14.7%) had three or more treatment failures.
The total medical cost per patient, including emergency room (ER), inpatient (IP), and outpatient (OP) care, increased with increasing number of treatment failures ($10,329 for one, $13,774 for two, and $35,392 for three or more). When the investigators added prescription drug costs, the total health care costs also increased with number of treatment failures ($13,946 for one, $18,685 for two, and $41,864 for three or more).
Similarly, the per-patient annual health care provider visits increased with increasing numbers of treatment failures. The number of ER visits per year was 0.54, 0.69, and 1.02 for patients with one, two, and three or more treatment failures, respectively. The annual number of IP visits was 0.46, 0.59, and 0.97, for patients with one, two, and three or more treatment failures, respectively. OP visits showed a similar trend. The annual number of office visits was 9.47 for patients with one, 11.24 for patients with two, and 14.26 for patients with three or more treatment failures. The annual number of other visits was 13.15 for patients with one, 15.73 for patients with two, and 19.96 for patients with three or more treatment failures.
Guidelines could enable appropriate treatment
Reasons for treatment failure include misdiagnosis of the headache disorder, failure to identify and account for comorbidities, overlooking concurrent acute medication overuse, and inappropriate dose or formulation, said Dr. Newman. “Common pitfalls in prevention that lead to treatment failure include not using evidence-based treatments, starting at too low of a dose and not increasing, starting too high or increasing the dose too quickly, discontinuing the medication before an effect can be seen (before 8 weeks), patient nonadherence, and not establishing realistic expectations.”
Available resources could help clinicians treat migraine effectively. “The American Headache Society (AHS)/AAN preventive guidelines have been retired, yet they offered several levels of effectiveness of pharmacologic treatments that were evidence-based,” said Dr. Newman. “Furthermore, in 2019, the AHS published a consensus statement on integrating new migraine treatments into clinical practice. This statement offered advice about the new anti-CGRP agents, onabotulinum toxin, and neuromodulation devices. I think this is a good starting point for neurologists to be familiar with to choose appropriate therapeutic options for people living with migraine.”
Earlier treatment may reduce patients’ economic burden
The study’s weaknesses included its observational design and its reliance on diagnostic codes, which raised the possibility that comorbidities were inadequately recognized, said Dr. Newman. The reasons that patients changed medications are unknown, and the results are not generalizable to patients aged 65 years or older, he added.
Major strengths of Dr. Newman’s study are its large sample size and wealth of available data, said Alan M. Rapoport, MD, clinical professor of neurology at the University of California, Los Angeles. “The multiple subcategories suggest that this was a carefully organized and implemented study,” he added. If any diagnoses of migraine were provided by general practitioners with little knowledge of migraine, this would weaken the study, said Dr. Rapoport, editor-in-chief of Neurology Reviews.
“We can ease the economic burden of migraineurs by improving acute care therapy with better selection and earlier starting of effective preventive therapy,” he continued. “Going for migraine-specific acute care therapy is better than pain medications or other nonspecific therapies. If you do not stop a migraine attack with effective therapy, you increase the odds that the patient will go on to chronic migraine. It is always important to effectively teach doctors and nurses to improve their diagnostic skills and use the optimal acute and preventive therapy.” For their next trial, maximizing an accurate diagnosis and performing a prospective study measuring treatment outcomes will be particularly valuable, Dr. Rapoport concluded.
Dr. Newman’s study was supported by Novartis Pharma in Basel, Switzerland. Together with Amgen, Novartis developed erenumab. Dr. Newman has received compensation from Allergan, Alder, Amgen, Biohaven, Novartis, Teva, Supernus, and Theranica for consulting, serving on a scientific advisory board, speaking, or other activities. He has received compensation from Springer Scientific for editorial services.
SOURCE: Newman L et al. AAN 2020, Abstract S47.009.
From AAN 2020

Prior head injury is associated with severe Parkinson’s disease phenotype
according to research presented online as part of the 2020 American Academy of Neurology Science Highlights.

Neurologists have identified various phenotypes among patients with Parkinson’s disease; however, the factors that determine these phenotypes, which may include genetic and environmental variables, are poorly understood. Ethan G. Brown, MD, assistant professor of neurology at the University of California, San Francisco, and colleagues hypothesized that head injury, which is a risk factor for Parkinson’s disease, would be associated with a more severe phenotype.
“Head injury is a risk factor for other conditions that involve cognitive impairment,” said Dr. Brown. “The mechanisms of how head injury contributes to neurodegenerative disease are not clear, but may be related to the initiation of an inflammatory cascade that can have a long-term, chronic effect. We hypothesized that these long-term sequelae may contribute to symptoms in Parkinson’s disease.”
An analysis of data from two cohorts
The researchers examined the relationship between head injury and clinical features by analyzing data for two cohorts of patients with Parkinson’s disease. Through an online survey, the investigators elicited information about head injury and other exposures from participants in the Parkinson’s Progression Markers Initiative (PPMI) and the Fox Insight (FI) study. Dr. Brown and colleagues determined disease phenotypes for participants in PPMI using baseline Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) score and 5-year change in Montreal Cognitive Assessment score. For participants in FI, the researchers determined phenotypes using baseline self-reported MDS-UPDRS-II score and self-reported cognitive impairment. They used parametric and nonparametric tests as appropriate and adjusted the results for age, sex, and smoking history.
In all, 267 participants with Parkinson’s disease in PPMI and 25,308 in FI submitted information about head injury. In the PPMI cohort, head injury before Parkinson’s disease diagnosis was associated with greater nonmotor symptom burden at enrollment. The mean MDS-UPDRS-I score was 7.73 among participants with any injury, compared with 6.19 among participants with no injury. Similarly, the mean MDS-UPDRS-I score was 8.29 among participants with severe head injury, compared with 6.19 among participants with no injury. Motor symptoms were worse among participants with severe injury (MDS-UPDRS-II score, 8.35). Among 110 participants who were followed for 5 years, patients who reported severe head injury before diagnosis had a decline in cognitive function. The mean change in Montreal Cognitive Assessment score was –0.60 for patients with severe head injury and 0.76 in those with no head injury.
“The improvement from baseline in the participants with Parkinson’s disease but without head injury was small and not statistically significant,” said Dr. Brown. The increase could have resulted from practice effect, although it is not certain, he added. “We are continuing to evaluate other, more sensitive tests of cognitive impairment to try to understand these results more completely in this population.”
In the FI cohort, participants who reported a prior head injury had more motor symptoms (MDS-UPDRS-II, 14.4), compared with those without head injury (MDS-UPDRS-II, 12.1). Also, the risk of self-reported cognitive impairment was elevated in participants who reported head injury (odds ratio, 1.58).
“The results most affected by the self-reported nature of [the] FI [data] are the cognitive impairment results,” said Dr. Brown. “Subjective cognitive impairment ... is very different from objective cognitive impairment, which could be measured through in-person testing in the PPMI cohort. Many factors may contribute to noticing cognitive decline, some of which can be measured and controlled for, but some cannot. There may be a correlation between subjective cognitive decline and true cognitive impairment, but this has not been fully studied in Parkinson’s disease.”
The search for the underlying mechanism
Clarifying whether the relationship between head injury and Parkinson’s disease phenotype is causal or whether falling is an early indication of worse symptoms will require more longitudinal data. “We would like to further characterize the differences between people with Parkinson’s disease with and without a history of head injury,” said Dr. Brown. “More detailed understanding of these phenotypic differences could point to an underlying mechanism, or whether or not other comorbid conditions are involved. We would also like to understand whether genetics plays a role.”
The PPMI and FI studies are funded by the Michael J. Fox Foundation. Dr. Brown has received compensation from HiOscar, NEJM Knowledge Plus, and Rune Labs and has received research support from Gateway Institute for Brain Research.
SOURCE: Brown EG et al. AAN 2020, Abstract S17.002.
according to research presented online as part of the 2020 American Academy of Neurology Science Highlights.
Neurologists have identified various phenotypes among patients with Parkinson’s disease; however, the factors that determine these phenotypes, which may include genetic and environmental variables, are poorly understood. Ethan G. Brown, MD, assistant professor of neurology at the University of California, San Francisco, and colleagues hypothesized that head injury, which is a risk factor for Parkinson’s disease, would be associated with a more severe phenotype.
“Head injury is a risk factor for other conditions that involve cognitive impairment,” said Dr. Brown. “The mechanisms of how head injury contributes to neurodegenerative disease are not clear, but may be related to the initiation of an inflammatory cascade that can have a long-term, chronic effect. We hypothesized that these long-term sequelae may contribute to symptoms in Parkinson’s disease.”
An analysis of data from two cohorts
The researchers examined the relationship between head injury and clinical features by analyzing data for two cohorts of patients with Parkinson’s disease. Through an online survey, the investigators elicited information about head injury and other exposures from participants in the Parkinson’s Progression Markers Initiative (PPMI) and the Fox Insight (FI) study. Dr. Brown and colleagues determined disease phenotypes for participants in PPMI using baseline Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) score and 5-year change in Montreal Cognitive Assessment score. For participants in FI, the researchers determined phenotypes using baseline self-reported MDS-UPDRS-II score and self-reported cognitive impairment. They used parametric and nonparametric tests as appropriate and adjusted the results for age, sex, and smoking history.
In all, 267 participants with Parkinson’s disease in PPMI and 25,308 in FI submitted information about head injury. In the PPMI cohort, head injury before Parkinson’s disease diagnosis was associated with greater nonmotor symptom burden at enrollment. The mean MDS-UPDRS-I score was 7.73 among participants with any injury, compared with 6.19 among participants with no injury. Similarly, the mean MDS-UPDRS-I score was 8.29 among participants with severe head injury, compared with 6.19 among participants with no injury. Motor symptoms were worse among participants with severe injury (MDS-UPDRS-II score, 8.35). Among 110 participants who were followed for 5 years, patients who reported severe head injury before diagnosis had a decline in cognitive function. The mean change in Montreal Cognitive Assessment score was –0.60 for patients with severe head injury and 0.76 in those with no head injury.
“The improvement from baseline in the participants with Parkinson’s disease but without head injury was small and not statistically significant,” said Dr. Brown. The increase could have resulted from practice effect, although it is not certain, he added. “We are continuing to evaluate other, more sensitive tests of cognitive impairment to try to understand these results more completely in this population.”
In the FI cohort, participants who reported a prior head injury had more motor symptoms (MDS-UPDRS-II, 14.4), compared with those without head injury (MDS-UPDRS-II, 12.1). Also, the risk of self-reported cognitive impairment was elevated in participants who reported head injury (odds ratio, 1.58).
“The results most affected by the self-reported nature of [the] FI [data] are the cognitive impairment results,” said Dr. Brown. “Subjective cognitive impairment ... is very different from objective cognitive impairment, which could be measured through in-person testing in the PPMI cohort. Many factors may contribute to noticing cognitive decline, some of which can be measured and controlled for, but some cannot. There may be a correlation between subjective cognitive decline and true cognitive impairment, but this has not been fully studied in Parkinson’s disease.”
The search for the underlying mechanism
Clarifying whether the relationship between head injury and Parkinson’s disease phenotype is causal or whether falling is an early indication of worse symptoms will require more longitudinal data. “We would like to further characterize the differences between people with Parkinson’s disease with and without a history of head injury,” said Dr. Brown. “More detailed understanding of these phenotypic differences could point to an underlying mechanism, or whether or not other comorbid conditions are involved. We would also like to understand whether genetics plays a role.”
The PPMI and FI studies are funded by the Michael J. Fox Foundation. Dr. Brown has received compensation from HiOscar, NEJM Knowledge Plus, and Rune Labs and has received research support from Gateway Institute for Brain Research.
SOURCE: Brown EG et al. AAN 2020, Abstract S17.002.
according to research presented online as part of the 2020 American Academy of Neurology Science Highlights.
Neurologists have identified various phenotypes among patients with Parkinson’s disease; however, the factors that determine these phenotypes, which may include genetic and environmental variables, are poorly understood. Ethan G. Brown, MD, assistant professor of neurology at the University of California, San Francisco, and colleagues hypothesized that head injury, which is a risk factor for Parkinson’s disease, would be associated with a more severe phenotype.
“Head injury is a risk factor for other conditions that involve cognitive impairment,” said Dr. Brown. “The mechanisms of how head injury contributes to neurodegenerative disease are not clear, but may be related to the initiation of an inflammatory cascade that can have a long-term, chronic effect. We hypothesized that these long-term sequelae may contribute to symptoms in Parkinson’s disease.”
An analysis of data from two cohorts
The researchers examined the relationship between head injury and clinical features by analyzing data for two cohorts of patients with Parkinson’s disease. Through an online survey, the investigators elicited information about head injury and other exposures from participants in the Parkinson’s Progression Markers Initiative (PPMI) and the Fox Insight (FI) study. Dr. Brown and colleagues determined disease phenotypes for participants in PPMI using baseline Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) score and 5-year change in Montreal Cognitive Assessment score. For participants in FI, the researchers determined phenotypes using baseline self-reported MDS-UPDRS-II score and self-reported cognitive impairment. They used parametric and nonparametric tests as appropriate and adjusted the results for age, sex, and smoking history.
In all, 267 participants with Parkinson’s disease in PPMI and 25,308 in FI submitted information about head injury. In the PPMI cohort, head injury before Parkinson’s disease diagnosis was associated with greater nonmotor symptom burden at enrollment. The mean MDS-UPDRS-I score was 7.73 among participants with any injury, compared with 6.19 among participants with no injury. Similarly, the mean MDS-UPDRS-I score was 8.29 among participants with severe head injury, compared with 6.19 among participants with no injury. Motor symptoms were worse among participants with severe injury (MDS-UPDRS-II score, 8.35). Among 110 participants who were followed for 5 years, patients who reported severe head injury before diagnosis had a decline in cognitive function. The mean change in Montreal Cognitive Assessment score was –0.60 for patients with severe head injury and 0.76 in those with no head injury.
“The improvement from baseline in the participants with Parkinson’s disease but without head injury was small and not statistically significant,” said Dr. Brown. The increase could have resulted from practice effect, although it is not certain, he added. “We are continuing to evaluate other, more sensitive tests of cognitive impairment to try to understand these results more completely in this population.”
In the FI cohort, participants who reported a prior head injury had more motor symptoms (MDS-UPDRS-II, 14.4), compared with those without head injury (MDS-UPDRS-II, 12.1). Also, the risk of self-reported cognitive impairment was elevated in participants who reported head injury (odds ratio, 1.58).
“The results most affected by the self-reported nature of [the] FI [data] are the cognitive impairment results,” said Dr. Brown. “Subjective cognitive impairment ... is very different from objective cognitive impairment, which could be measured through in-person testing in the PPMI cohort. Many factors may contribute to noticing cognitive decline, some of which can be measured and controlled for, but some cannot. There may be a correlation between subjective cognitive decline and true cognitive impairment, but this has not been fully studied in Parkinson’s disease.”
The search for the underlying mechanism
Clarifying whether the relationship between head injury and Parkinson’s disease phenotype is causal or whether falling is an early indication of worse symptoms will require more longitudinal data. “We would like to further characterize the differences between people with Parkinson’s disease with and without a history of head injury,” said Dr. Brown. “More detailed understanding of these phenotypic differences could point to an underlying mechanism, or whether or not other comorbid conditions are involved. We would also like to understand whether genetics plays a role.”
The PPMI and FI studies are funded by the Michael J. Fox Foundation. Dr. Brown has received compensation from HiOscar, NEJM Knowledge Plus, and Rune Labs and has received research support from Gateway Institute for Brain Research.
SOURCE: Brown EG et al. AAN 2020, Abstract S17.002.
FROM AAN 2020
Predictors of ICH after thrombectomy identified
(ICH), new research suggests. In a study of nearly 600 patients undergoing thrombectomy, investigators combined a modified Thrombolysis in Cerebral Ischemia (TICI) score, an Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and glucose levels (the “TAG score”) to predict risk. Results showed that each unit increase in the combination score was associated with a significant, nearly twofold greater likelihood of symptomatic ICH.

“It is very easy” to calculate the new score in a clinical setting, lead author Mayra Johana Montalvo Perero, MD, Department of Neurology, Brown University and Rhode Island Hospital, Providence, said. “You just need three variables.”
The findings were presented online as part of the 2020 American Academy of Neurology Science Highlights.
Limited data
High TAG scores are associated with symptomatic ICH in patients receiving mechanical thrombectomy, Dr. Montalvo Perero and colleagues said.
Although clinical predictors of symptomatic ICH are well established, “there is limited data in patients who underwent mechanical thrombectomy,” the researchers noted.
To learn more, they assessed 578 patients (52% women; mean age, 73 years) who had mechanical thrombectomy for acute ischemic stroke at a comprehensive stroke center. Within this cohort, 19 patients (3.3%) developed symptomatic ICH.
The investigators compared clinical and radiographic findings between patients who experienced symptomatic ICH and those who did not.
The TICI score emerged as a predictor when each unit decrease in this score was associated with greater risk for symptomatic ICH (odds ratio, 5.13; 95% confidence interval, 1.84-14.29; P = .002).
Each one-point decrease in the ASPECTS score also predicted increased risk (OR, 1.52; 95% CI, 1.1-2.0; P = .003).
“The main driver is the size of the stroke core, which is correlated with the ASPECTS score,” Dr. Montalvo Perero said.
Each 10 mg/dL increase in glucose level also correlated with increased risk (OR, 1.07; 95% CI, 1.01-1.13; P = .018).
Twice the risk
The investigators then combined these three independent variables into a weighted TAG score based on a multivariate analysis. Each unit increase in this composite score was associated with increased risk of symptomatic ICH (OR, 1.98; 95% CI, 1.48-2.66; P < .001).
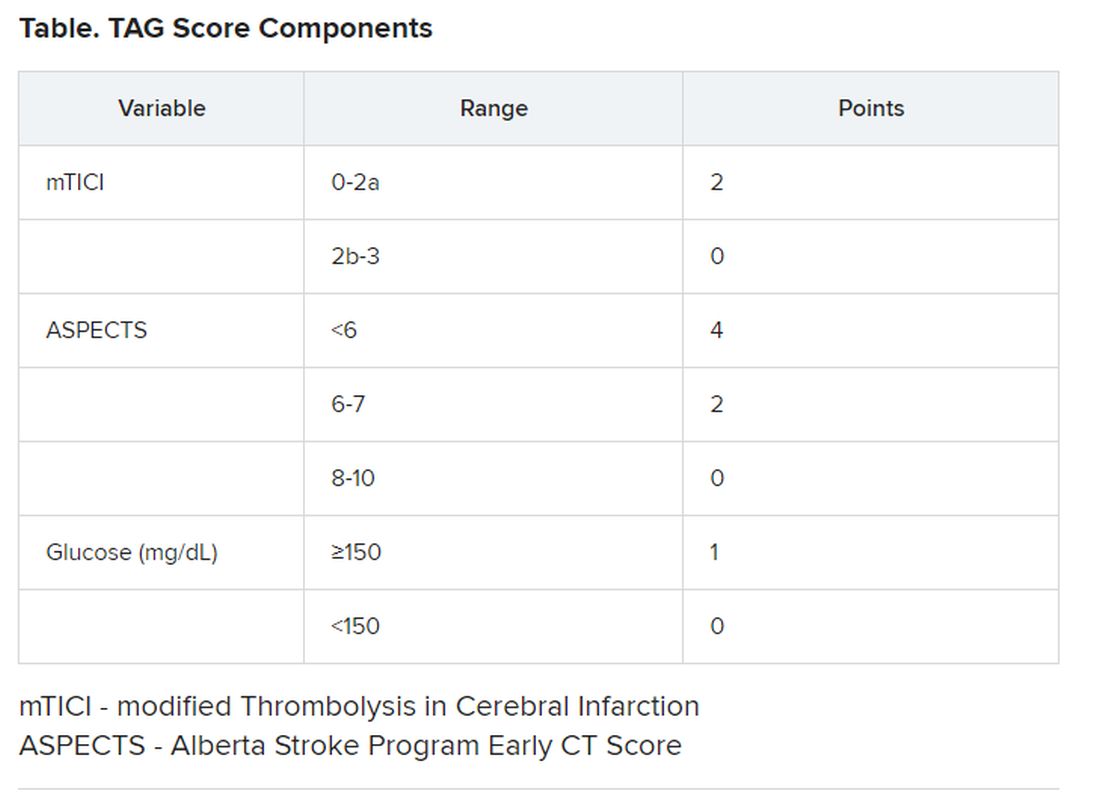
There was no association between patients who received tissue plasminogen activator (tPA) and risk of symptomatic ICH, which Dr. Montalvo Perero said was surprising.
However, “that may be due to a small number” of patients with symptomatic ICH included in the study, she said. “Therefore, that would be an interesting question to ask in future studies with bigger cohorts.”
Larger studies are also needed to validate this scoring system and to test strategies to reduce risk of symptomatic ICH and make thrombectomy safer in patients with elevated TAG scores, Dr. Montalvo Perero said.
A step in the right direction?
Commenting on the study, Jeremy Payne, MD, PhD, director of the Stroke Center at Banner Health’s University Medicine Neuroscience Institute in Phoenix, Arizona, noted the importance of predicting which patients might have secondary bleeding after interventional treatment of a large vessel occlusion stroke
“In aggregate, the role of endovascular thrombectomy is quite clear, but we still struggle to predict at the individual patient level who will benefit,” said Dr. Payne, who was not involved with the research.
Transfer and treatment of these patients also carries an economic cost. “Just getting patients to our center, where about 80% of the complex stroke patients come by helicopter, costs upwards of $30,000,” Dr. Payne said. “The financial argument isn’t one we like to talk much about, but we’re committing to spending probably $100,000-$200,000 on each person’s care.”
This study “attempts to address an important issue,” he said.
Predicting who is more likely to benefit leads to the assumption that if that were to happen, “we could skip all the rigamarole of helicopters and procedures, avoid the extra expense and particularly not make things worse than they already are,” explained Dr. Payne.
Potential limitations include that this is a single-center study and is based on an analysis of 19 patients out of 578. As a result, it is not clear that these findings will necessarily be generalizable to other centers, said Dr. Payne.
The TICI and ASPECTS “are pretty obvious markers of risk,” he noted. “The glucose levels, however, are more subtly interesting.”
He also pointed out that an association between diabetes and worse stroke outcomes is well established.
“The mechanisms are poorly understood, but the role of glucose keeps popping up as a potential marker of risk, and so it’s interesting that it bubbles up in their work too,” Dr. Payne said.
Furthermore, unlike TICI and ASPECTS, glucose levels are modifiable.
“Overall, then, we will continue to study this,” Dr. Payne said. “It’s very important to refine our ability to predict which patients may receive benefit versus harm from such procedures, and this is a step in the right direction.”
Some findings were also published December 2019 in the Journal of Neurology, Neurosurgery & Psychiatry.
Montalvo Perero and Payne have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Motalvo Perero MJ et al. AAN 2020, Abstract S20.001.
(ICH), new research suggests. In a study of nearly 600 patients undergoing thrombectomy, investigators combined a modified Thrombolysis in Cerebral Ischemia (TICI) score, an Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and glucose levels (the “TAG score”) to predict risk. Results showed that each unit increase in the combination score was associated with a significant, nearly twofold greater likelihood of symptomatic ICH.
“It is very easy” to calculate the new score in a clinical setting, lead author Mayra Johana Montalvo Perero, MD, Department of Neurology, Brown University and Rhode Island Hospital, Providence, said. “You just need three variables.”
The findings were presented online as part of the 2020 American Academy of Neurology Science Highlights.
Limited data
High TAG scores are associated with symptomatic ICH in patients receiving mechanical thrombectomy, Dr. Montalvo Perero and colleagues said.
Although clinical predictors of symptomatic ICH are well established, “there is limited data in patients who underwent mechanical thrombectomy,” the researchers noted.
To learn more, they assessed 578 patients (52% women; mean age, 73 years) who had mechanical thrombectomy for acute ischemic stroke at a comprehensive stroke center. Within this cohort, 19 patients (3.3%) developed symptomatic ICH.
The investigators compared clinical and radiographic findings between patients who experienced symptomatic ICH and those who did not.
The TICI score emerged as a predictor when each unit decrease in this score was associated with greater risk for symptomatic ICH (odds ratio, 5.13; 95% confidence interval, 1.84-14.29; P = .002).
Each one-point decrease in the ASPECTS score also predicted increased risk (OR, 1.52; 95% CI, 1.1-2.0; P = .003).
“The main driver is the size of the stroke core, which is correlated with the ASPECTS score,” Dr. Montalvo Perero said.
Each 10 mg/dL increase in glucose level also correlated with increased risk (OR, 1.07; 95% CI, 1.01-1.13; P = .018).
Twice the risk
The investigators then combined these three independent variables into a weighted TAG score based on a multivariate analysis. Each unit increase in this composite score was associated with increased risk of symptomatic ICH (OR, 1.98; 95% CI, 1.48-2.66; P < .001).
There was no association between patients who received tissue plasminogen activator (tPA) and risk of symptomatic ICH, which Dr. Montalvo Perero said was surprising.
However, “that may be due to a small number” of patients with symptomatic ICH included in the study, she said. “Therefore, that would be an interesting question to ask in future studies with bigger cohorts.”
Larger studies are also needed to validate this scoring system and to test strategies to reduce risk of symptomatic ICH and make thrombectomy safer in patients with elevated TAG scores, Dr. Montalvo Perero said.
A step in the right direction?
Commenting on the study, Jeremy Payne, MD, PhD, director of the Stroke Center at Banner Health’s University Medicine Neuroscience Institute in Phoenix, Arizona, noted the importance of predicting which patients might have secondary bleeding after interventional treatment of a large vessel occlusion stroke
“In aggregate, the role of endovascular thrombectomy is quite clear, but we still struggle to predict at the individual patient level who will benefit,” said Dr. Payne, who was not involved with the research.
Transfer and treatment of these patients also carries an economic cost. “Just getting patients to our center, where about 80% of the complex stroke patients come by helicopter, costs upwards of $30,000,” Dr. Payne said. “The financial argument isn’t one we like to talk much about, but we’re committing to spending probably $100,000-$200,000 on each person’s care.”
This study “attempts to address an important issue,” he said.
Predicting who is more likely to benefit leads to the assumption that if that were to happen, “we could skip all the rigamarole of helicopters and procedures, avoid the extra expense and particularly not make things worse than they already are,” explained Dr. Payne.
Potential limitations include that this is a single-center study and is based on an analysis of 19 patients out of 578. As a result, it is not clear that these findings will necessarily be generalizable to other centers, said Dr. Payne.
The TICI and ASPECTS “are pretty obvious markers of risk,” he noted. “The glucose levels, however, are more subtly interesting.”
He also pointed out that an association between diabetes and worse stroke outcomes is well established.
“The mechanisms are poorly understood, but the role of glucose keeps popping up as a potential marker of risk, and so it’s interesting that it bubbles up in their work too,” Dr. Payne said.
Furthermore, unlike TICI and ASPECTS, glucose levels are modifiable.
“Overall, then, we will continue to study this,” Dr. Payne said. “It’s very important to refine our ability to predict which patients may receive benefit versus harm from such procedures, and this is a step in the right direction.”
Some findings were also published December 2019 in the Journal of Neurology, Neurosurgery & Psychiatry.
Montalvo Perero and Payne have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Motalvo Perero MJ et al. AAN 2020, Abstract S20.001.
(ICH), new research suggests. In a study of nearly 600 patients undergoing thrombectomy, investigators combined a modified Thrombolysis in Cerebral Ischemia (TICI) score, an Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and glucose levels (the “TAG score”) to predict risk. Results showed that each unit increase in the combination score was associated with a significant, nearly twofold greater likelihood of symptomatic ICH.
“It is very easy” to calculate the new score in a clinical setting, lead author Mayra Johana Montalvo Perero, MD, Department of Neurology, Brown University and Rhode Island Hospital, Providence, said. “You just need three variables.”
The findings were presented online as part of the 2020 American Academy of Neurology Science Highlights.
Limited data
High TAG scores are associated with symptomatic ICH in patients receiving mechanical thrombectomy, Dr. Montalvo Perero and colleagues said.
Although clinical predictors of symptomatic ICH are well established, “there is limited data in patients who underwent mechanical thrombectomy,” the researchers noted.
To learn more, they assessed 578 patients (52% women; mean age, 73 years) who had mechanical thrombectomy for acute ischemic stroke at a comprehensive stroke center. Within this cohort, 19 patients (3.3%) developed symptomatic ICH.
The investigators compared clinical and radiographic findings between patients who experienced symptomatic ICH and those who did not.
The TICI score emerged as a predictor when each unit decrease in this score was associated with greater risk for symptomatic ICH (odds ratio, 5.13; 95% confidence interval, 1.84-14.29; P = .002).
Each one-point decrease in the ASPECTS score also predicted increased risk (OR, 1.52; 95% CI, 1.1-2.0; P = .003).
“The main driver is the size of the stroke core, which is correlated with the ASPECTS score,” Dr. Montalvo Perero said.
Each 10 mg/dL increase in glucose level also correlated with increased risk (OR, 1.07; 95% CI, 1.01-1.13; P = .018).
Twice the risk
The investigators then combined these three independent variables into a weighted TAG score based on a multivariate analysis. Each unit increase in this composite score was associated with increased risk of symptomatic ICH (OR, 1.98; 95% CI, 1.48-2.66; P < .001).
There was no association between patients who received tissue plasminogen activator (tPA) and risk of symptomatic ICH, which Dr. Montalvo Perero said was surprising.
However, “that may be due to a small number” of patients with symptomatic ICH included in the study, she said. “Therefore, that would be an interesting question to ask in future studies with bigger cohorts.”
Larger studies are also needed to validate this scoring system and to test strategies to reduce risk of symptomatic ICH and make thrombectomy safer in patients with elevated TAG scores, Dr. Montalvo Perero said.
A step in the right direction?
Commenting on the study, Jeremy Payne, MD, PhD, director of the Stroke Center at Banner Health’s University Medicine Neuroscience Institute in Phoenix, Arizona, noted the importance of predicting which patients might have secondary bleeding after interventional treatment of a large vessel occlusion stroke
“In aggregate, the role of endovascular thrombectomy is quite clear, but we still struggle to predict at the individual patient level who will benefit,” said Dr. Payne, who was not involved with the research.
Transfer and treatment of these patients also carries an economic cost. “Just getting patients to our center, where about 80% of the complex stroke patients come by helicopter, costs upwards of $30,000,” Dr. Payne said. “The financial argument isn’t one we like to talk much about, but we’re committing to spending probably $100,000-$200,000 on each person’s care.”
This study “attempts to address an important issue,” he said.
Predicting who is more likely to benefit leads to the assumption that if that were to happen, “we could skip all the rigamarole of helicopters and procedures, avoid the extra expense and particularly not make things worse than they already are,” explained Dr. Payne.
Potential limitations include that this is a single-center study and is based on an analysis of 19 patients out of 578. As a result, it is not clear that these findings will necessarily be generalizable to other centers, said Dr. Payne.
The TICI and ASPECTS “are pretty obvious markers of risk,” he noted. “The glucose levels, however, are more subtly interesting.”
He also pointed out that an association between diabetes and worse stroke outcomes is well established.
“The mechanisms are poorly understood, but the role of glucose keeps popping up as a potential marker of risk, and so it’s interesting that it bubbles up in their work too,” Dr. Payne said.
Furthermore, unlike TICI and ASPECTS, glucose levels are modifiable.
“Overall, then, we will continue to study this,” Dr. Payne said. “It’s very important to refine our ability to predict which patients may receive benefit versus harm from such procedures, and this is a step in the right direction.”
Some findings were also published December 2019 in the Journal of Neurology, Neurosurgery & Psychiatry.
Montalvo Perero and Payne have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
SOURCE: Motalvo Perero MJ et al. AAN 2020, Abstract S20.001.
AAN 2020