User login
Glucose self-monitoring: Think twice for type 2 patients
ILLUSTRATIVE CASE
Two weeks ago, you informed your patient—a 53-year-old man with a body mass index of 28.4—that he has type 2 diabetes. Since then, he has seen a nutritionist and begun exercising regularly. His hemoglobin A1c (HbA1c) is 7.7%. You recommend that he begin taking metformin. The patient is worried about the potential for oral antidiabetic agents to cause hypoglycemia. He’s aware that many patients with diabetes monitor their blood sugar levels at home and wants to know if he should, too. You wonder whether it’s necessary, or even advisable, to initiate self-monitoring at this time.
For patients with type 2 diabetes, self-monitoring of blood glucose makes intuitive sense. Theoretically, it reinforces self-management behaviors, promotes adherence to the prescribed medication regimen, and leads to better glucose control. It seems obvious, too, that patients taking medications intended to lower blood sugar need to be aware of their glucose levels so they can take action to reduce the risk of complications.
But things that make sense intuitively do not always stand up to scrutiny. New high-quality evidence suggests that for those with newly diagnosed diabetes, self-monitoring of blood glucose may do more harm than good.
More questions than answers
While it is generally accepted that glucose self-monitoring is useful for those with insulin-treated type 2 diabetes,2-4 evidence supporting the practice for patients with diabetes who do not require insulin is limited. Two recent meta-analyses of RCTs5,6 found that self-monitoring of blood glucose achieves a statistically significant reduction of 0.4% in HbA1c; the quality of the studies, however, was limited. A well-designed RCT was needed, the researchers concluded, to settle questions about the value of self-monitoring.
The most recent Cochrane review7 of self-monitoring reached a similar conclusion: The reviewers called for additional research into the benefits of self-monitoring for patients with diabetes who do not need insulin. The reviewers also emphasized the need for information on patient-related outcomes such as quality of life, well-being, and satisfaction.
Are recommendations out of step?
Despite the lack of definitive evidence, the Department of Health and Human Services calls on us to increase the proportion of patients with diabetes who monitor their blood sugar at least once daily to 60% as part of its Healthy People 2010 initiative.8 The American Diabetes Association states that self-monitoring of blood glucose may help patients taking oral antidiabetic agents achieve glycemic goals.9 And the International Diabetes Federation recommends that self-monitoring of blood glucose be offered to all people with type 2 diabetes taking insulin or oral agents—and be part of the patient education that is given to all those who are newly diagnosed.10
But all of these groups may need to rethink their recommendations in light of the latest findings from the O’Kane RCT.
STUDY SUMMARY: Self-monitoring has little effect on glycemic control
O’Kane and colleagues conducted a prospective RCT comparing self-monitoring versus no monitoring among 184 people with newly diagnosed type 2 diabetes.1 Patients were randomized to the self-monitoring or control group for 1 year, with clinic visits at 3-month intervals. Those who were already taking insulin or had engaged in self-monitoring of blood glucose were excluded.
At baseline, there was no significant difference in HbA1c, age, or sex between the 2 groups. Participants in both groups underwent identical diabetes education programs throughout the study period and received dietary and medical management based on the same treatment algorithm. Patients whose baseline HbA1c was >7.5% received metformin, followed by the sulfonylurea gliclazide if they did not reach target at the maximum dose of metformin. There was no significant difference in medication use at baseline or at 12 months.
Patients in the self-monitoring group were given glucose monitors and asked to record 4 fasting and 4 postprandial capillary blood glucose measurements per week. They were also taught to monitor and interpret blood glucose readings, and to respond appropriately to high or low readings.
At each follow-up visit, patients underwent blood tests for HbA1c, lipids, and electrolyte levels and completed questionnaires about treatment satisfaction, attitudes about diabetes, and levels of depression, anxiety, and well-being. Adherence to self-monitoring was verified by downloading meter readings. The dropout rate was low (2.2%), and adherence in the self-monitoring group was high. Study results were assessed using intent-to-treat analysis.
HbA1c fell in both the self-monitoring and control groups, with no significant differences at any point. The mean (standard deviation) value at 12 months was 6.9% (0.8%) in the self-monitoring group, compared to 6.9% (1.2%) in the control group, with a 95% confidence interval for the change in HbA1c of –0.25% to 0.38%. Throughout the study period, there was no difference in use of oral hypoglycemic medications or reported hypoglycemia.
Self-monitoring linked to depression
Measures of depression and anxiety were scored on a 100-point scale and compared to baseline measurements. At 12 months, participants in the self-monitoring group were more depressed, scoring 6% higher, on average, on the depression subscale of the well-being questionnaire (P=.01) than those in the control group. There was a trend toward increased anxiety in the self-monitoring group, but no significant differences in well-being, energy, or any of the other diabetes attitude subscales.
WHAT’S NEW: Less may be better
Because we emphasize self-management skills when we counsel patients about diabetes, it is surprising to learn that knowledge about glycemic control and blood sugar levels does not lead to better glycemic control. This RCT provides strong evidence that more information is not necessarily desirable, at least for patients with newly diagnosed type 2 diabetes who do not need insulin.
Depression is a known complication of diabetes. It affects an estimated 10% to 30% of patients with diabetes, who have double the odds of depression compared to people without diabetes.11,12 Patients with depression and diabetes have poorer glycemic control,13,14 an increased risk of complications,15-17 a decreased quality of life,18 an increased disability burden,19,20 and increased health care use and costs.18,21,22 In addition, they face a significantly higher risk of death from all causes, beyond the risks associated with depression or diabetes alone.23
CAVEATS: Patients on sulfonylureas may be an exception
This study used metformin as the initial oral medication, with sulfonylureas reserved for those who did not reach target glycemic control with maximum metformin therapy. The number of patients taking sulfonylureas was 11 in the self-monitoring group and 6 in the control group. Because hypoglycemia is a concern in patients taking sulfonylureas, there may be a role for self-monitoring of blood glucose in these patients.
Also of note: This study does not provide definitive evidence that self-monitoring of blood glucose causes harm. Although self-monitoring was associated with a 6% higher score on a depression subscale and a trend toward increased anxiety, overall satisfaction with treatment was similar in both groups. Additional studies are needed to better understand the relationship between self-monitoring and depression.
Self-monitoring may still be a good idea for certain patients, regardless of their diabetic medication regimen. When evaluating the potential benefits of self-monitoring of blood glucose, physicians should consider the individual’s predisposition to depression, among other concerns.
CHALLENGES TO IMPLEMENTATION: Hard to forego a practice that everyone expects
Self-monitoring serves different purposes for different populations. Blood glucose levels, along with HbA1c, can guide clinicians in making treatment decisions. Knowing blood sugar levels may be educational or empowering to patients, and provides critical information if hypoglycemia is a concern. These considerations lead us to conclude that while self-monitoring is not indicated for all newly diagnosed diabetic patients, it should be considered in selected circumstances.
Because of the prevalence of self-monitoring of blood glucose, patients may see it as a key component of an optimal self-management regimen. It may be hard to convince patients with newly diagnosed diabetes otherwise—and to convince some clinicians that there is little benefit in recommending it. Again, clinical judgment is required. We suspect, however, that with the proper explanation, many patients will be relieved to learn that they will not have to prick their fingers regularly or record their blood glucose.
Acknowledgements
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. O’Kane MJ, Bunting B, Copeland M, Coates VE. ESMON study group Efficacy of self monitoring of blood glucose in patients with newly diagnosed type 2 diabetes (ESMON study): randomised controlled trial. BMJ. 2008;336:1174-1177.
2. McIntosh A, Hutchinson A, Home PD, et al. Clinical guidelines and evidence review for Type 2 diabetes: management of blood glucose. 2002. Scharr, University of Sheffield. Available at: . Accessed July 29, 2008.
3. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee Canadian Diabetes Association 2003 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes. 2003;27(suppl 2):S18-S23.
4. Karter AJ, Ackerson LM, Darbinian JA, et al. Self-monitoring of blood glucose levels and glycemic control: the Northern California Kaiser Permanente Diabetes Registry. Am J Med. 2001;111:1-9.
5. Sarol JN Jr, Nicodemus NA Jr, Tan KM, Grava MB. Self-monitoring of blood glucose as part of a multi-component therapy among non-insulin requiring type 2 diabetes patients: a meta-analysis (1966-2004). Curr Med Res Opin. 2005;21:173-184.
6. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring of blood glucose in patients with type 2 diabetes who are not using insulin: a systematic review. Diabetes Care. 2005;28:1510-1517.
7. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2005;18(2):CD005060.-
8. US Department of Health and Human Services Healthy People 2010. Increase the proportion of adults with diabetes who perform self-blood-glucose-monitoring at least once daily. Available at: http://www.healthypeople.gov/document/html/objectives/05-17.htm. Accessed July 29, 2008
9. American Diabetes Association Executive summary: standards of medical care in diabetes—2008. Diabetes Care. 2008;31(suppl 1):S5-S11.Available at: http://care.diabetesjournals.org/cgi/content/full/31/Supplement_1/S5. Accessed July 29, 2008.
10. International Diabetes Federation Clinical Guidelines Taskforce Global guidelines for type 2 diabetes: recommendations for standard, comprehensive and minimal care. Diabetes Med. 2006;23:579-593.
11. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care. 2001;24:1069-1078.
12. Egede LE, Zheng D. Independent factors associated with major depressive disorder in a national sample of individuals with diabetes. Diabetes Care. 2003;26:104-111.
13. De Groot M, Jacobson AM, Samson JA, Welch G. Glycemic control and major depression in patients with type 1 and type 2 diabetes mellitus. J Psychosom Res. 1999;46:425-435.
14. Ciechanowski PS, Katon WJ, Russo JE, Hirsch IB. The relationship of depressive symptoms to symptom reporting, self-care and glucose control in diabetes. Gen Hosp Psychiatry. 2003;25:246-252.
15. De Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. 2001;63:619-630.
16. Black SA, Markides KS, Ray LA. Depression predicts increased incidence of adverse health outcomes in older Mexican Americans with type 2 diabetes. Diabetes Care. 2003;26:2822-2828.
17. Kinder LS, Kamarck TW, Baum A, Orchard TJ. Depressive symptomatology and coronary heart disease in type I diabetes mellitus: a study of possible mechanisms. Health Psychol. 2002;21:542-552.
18. Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med. 2000;160:3278-3285.
19. Egede LE. Diabetes, major depression, and functional disability among U.S. adults. Diabetes Care. 2004;27:421-428.
20. Egede LE. Effects of depression on work loss and disability bed days in individuals with diabetes. Diabetes Care. 2004;27:1751-1753.
21. Egede LE, Zheng D, Simpson K. Comorbid depression is associated with increased health care use and expenditures in individuals with diabetes. Diabetes Care. 2002;25:464-470.
22. Finkelstein EA, Bray JW, Chen H. Prevalence and costs of major depression among elderly claimants with diabetes. Diabetes Care. 2003;26:415-420.
23. Egede LE, Nietert PJ, Zheng D. Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care. 2005;28:1339-1345.
ILLUSTRATIVE CASE
Two weeks ago, you informed your patient—a 53-year-old man with a body mass index of 28.4—that he has type 2 diabetes. Since then, he has seen a nutritionist and begun exercising regularly. His hemoglobin A1c (HbA1c) is 7.7%. You recommend that he begin taking metformin. The patient is worried about the potential for oral antidiabetic agents to cause hypoglycemia. He’s aware that many patients with diabetes monitor their blood sugar levels at home and wants to know if he should, too. You wonder whether it’s necessary, or even advisable, to initiate self-monitoring at this time.
For patients with type 2 diabetes, self-monitoring of blood glucose makes intuitive sense. Theoretically, it reinforces self-management behaviors, promotes adherence to the prescribed medication regimen, and leads to better glucose control. It seems obvious, too, that patients taking medications intended to lower blood sugar need to be aware of their glucose levels so they can take action to reduce the risk of complications.
But things that make sense intuitively do not always stand up to scrutiny. New high-quality evidence suggests that for those with newly diagnosed diabetes, self-monitoring of blood glucose may do more harm than good.
More questions than answers
While it is generally accepted that glucose self-monitoring is useful for those with insulin-treated type 2 diabetes,2-4 evidence supporting the practice for patients with diabetes who do not require insulin is limited. Two recent meta-analyses of RCTs5,6 found that self-monitoring of blood glucose achieves a statistically significant reduction of 0.4% in HbA1c; the quality of the studies, however, was limited. A well-designed RCT was needed, the researchers concluded, to settle questions about the value of self-monitoring.
The most recent Cochrane review7 of self-monitoring reached a similar conclusion: The reviewers called for additional research into the benefits of self-monitoring for patients with diabetes who do not need insulin. The reviewers also emphasized the need for information on patient-related outcomes such as quality of life, well-being, and satisfaction.
Are recommendations out of step?
Despite the lack of definitive evidence, the Department of Health and Human Services calls on us to increase the proportion of patients with diabetes who monitor their blood sugar at least once daily to 60% as part of its Healthy People 2010 initiative.8 The American Diabetes Association states that self-monitoring of blood glucose may help patients taking oral antidiabetic agents achieve glycemic goals.9 And the International Diabetes Federation recommends that self-monitoring of blood glucose be offered to all people with type 2 diabetes taking insulin or oral agents—and be part of the patient education that is given to all those who are newly diagnosed.10
But all of these groups may need to rethink their recommendations in light of the latest findings from the O’Kane RCT.
STUDY SUMMARY: Self-monitoring has little effect on glycemic control
O’Kane and colleagues conducted a prospective RCT comparing self-monitoring versus no monitoring among 184 people with newly diagnosed type 2 diabetes.1 Patients were randomized to the self-monitoring or control group for 1 year, with clinic visits at 3-month intervals. Those who were already taking insulin or had engaged in self-monitoring of blood glucose were excluded.
At baseline, there was no significant difference in HbA1c, age, or sex between the 2 groups. Participants in both groups underwent identical diabetes education programs throughout the study period and received dietary and medical management based on the same treatment algorithm. Patients whose baseline HbA1c was >7.5% received metformin, followed by the sulfonylurea gliclazide if they did not reach target at the maximum dose of metformin. There was no significant difference in medication use at baseline or at 12 months.
Patients in the self-monitoring group were given glucose monitors and asked to record 4 fasting and 4 postprandial capillary blood glucose measurements per week. They were also taught to monitor and interpret blood glucose readings, and to respond appropriately to high or low readings.
At each follow-up visit, patients underwent blood tests for HbA1c, lipids, and electrolyte levels and completed questionnaires about treatment satisfaction, attitudes about diabetes, and levels of depression, anxiety, and well-being. Adherence to self-monitoring was verified by downloading meter readings. The dropout rate was low (2.2%), and adherence in the self-monitoring group was high. Study results were assessed using intent-to-treat analysis.
HbA1c fell in both the self-monitoring and control groups, with no significant differences at any point. The mean (standard deviation) value at 12 months was 6.9% (0.8%) in the self-monitoring group, compared to 6.9% (1.2%) in the control group, with a 95% confidence interval for the change in HbA1c of –0.25% to 0.38%. Throughout the study period, there was no difference in use of oral hypoglycemic medications or reported hypoglycemia.
Self-monitoring linked to depression
Measures of depression and anxiety were scored on a 100-point scale and compared to baseline measurements. At 12 months, participants in the self-monitoring group were more depressed, scoring 6% higher, on average, on the depression subscale of the well-being questionnaire (P=.01) than those in the control group. There was a trend toward increased anxiety in the self-monitoring group, but no significant differences in well-being, energy, or any of the other diabetes attitude subscales.
WHAT’S NEW: Less may be better
Because we emphasize self-management skills when we counsel patients about diabetes, it is surprising to learn that knowledge about glycemic control and blood sugar levels does not lead to better glycemic control. This RCT provides strong evidence that more information is not necessarily desirable, at least for patients with newly diagnosed type 2 diabetes who do not need insulin.
Depression is a known complication of diabetes. It affects an estimated 10% to 30% of patients with diabetes, who have double the odds of depression compared to people without diabetes.11,12 Patients with depression and diabetes have poorer glycemic control,13,14 an increased risk of complications,15-17 a decreased quality of life,18 an increased disability burden,19,20 and increased health care use and costs.18,21,22 In addition, they face a significantly higher risk of death from all causes, beyond the risks associated with depression or diabetes alone.23
CAVEATS: Patients on sulfonylureas may be an exception
This study used metformin as the initial oral medication, with sulfonylureas reserved for those who did not reach target glycemic control with maximum metformin therapy. The number of patients taking sulfonylureas was 11 in the self-monitoring group and 6 in the control group. Because hypoglycemia is a concern in patients taking sulfonylureas, there may be a role for self-monitoring of blood glucose in these patients.
Also of note: This study does not provide definitive evidence that self-monitoring of blood glucose causes harm. Although self-monitoring was associated with a 6% higher score on a depression subscale and a trend toward increased anxiety, overall satisfaction with treatment was similar in both groups. Additional studies are needed to better understand the relationship between self-monitoring and depression.
Self-monitoring may still be a good idea for certain patients, regardless of their diabetic medication regimen. When evaluating the potential benefits of self-monitoring of blood glucose, physicians should consider the individual’s predisposition to depression, among other concerns.
CHALLENGES TO IMPLEMENTATION: Hard to forego a practice that everyone expects
Self-monitoring serves different purposes for different populations. Blood glucose levels, along with HbA1c, can guide clinicians in making treatment decisions. Knowing blood sugar levels may be educational or empowering to patients, and provides critical information if hypoglycemia is a concern. These considerations lead us to conclude that while self-monitoring is not indicated for all newly diagnosed diabetic patients, it should be considered in selected circumstances.
Because of the prevalence of self-monitoring of blood glucose, patients may see it as a key component of an optimal self-management regimen. It may be hard to convince patients with newly diagnosed diabetes otherwise—and to convince some clinicians that there is little benefit in recommending it. Again, clinical judgment is required. We suspect, however, that with the proper explanation, many patients will be relieved to learn that they will not have to prick their fingers regularly or record their blood glucose.
Acknowledgements
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
ILLUSTRATIVE CASE
Two weeks ago, you informed your patient—a 53-year-old man with a body mass index of 28.4—that he has type 2 diabetes. Since then, he has seen a nutritionist and begun exercising regularly. His hemoglobin A1c (HbA1c) is 7.7%. You recommend that he begin taking metformin. The patient is worried about the potential for oral antidiabetic agents to cause hypoglycemia. He’s aware that many patients with diabetes monitor their blood sugar levels at home and wants to know if he should, too. You wonder whether it’s necessary, or even advisable, to initiate self-monitoring at this time.
For patients with type 2 diabetes, self-monitoring of blood glucose makes intuitive sense. Theoretically, it reinforces self-management behaviors, promotes adherence to the prescribed medication regimen, and leads to better glucose control. It seems obvious, too, that patients taking medications intended to lower blood sugar need to be aware of their glucose levels so they can take action to reduce the risk of complications.
But things that make sense intuitively do not always stand up to scrutiny. New high-quality evidence suggests that for those with newly diagnosed diabetes, self-monitoring of blood glucose may do more harm than good.
More questions than answers
While it is generally accepted that glucose self-monitoring is useful for those with insulin-treated type 2 diabetes,2-4 evidence supporting the practice for patients with diabetes who do not require insulin is limited. Two recent meta-analyses of RCTs5,6 found that self-monitoring of blood glucose achieves a statistically significant reduction of 0.4% in HbA1c; the quality of the studies, however, was limited. A well-designed RCT was needed, the researchers concluded, to settle questions about the value of self-monitoring.
The most recent Cochrane review7 of self-monitoring reached a similar conclusion: The reviewers called for additional research into the benefits of self-monitoring for patients with diabetes who do not need insulin. The reviewers also emphasized the need for information on patient-related outcomes such as quality of life, well-being, and satisfaction.
Are recommendations out of step?
Despite the lack of definitive evidence, the Department of Health and Human Services calls on us to increase the proportion of patients with diabetes who monitor their blood sugar at least once daily to 60% as part of its Healthy People 2010 initiative.8 The American Diabetes Association states that self-monitoring of blood glucose may help patients taking oral antidiabetic agents achieve glycemic goals.9 And the International Diabetes Federation recommends that self-monitoring of blood glucose be offered to all people with type 2 diabetes taking insulin or oral agents—and be part of the patient education that is given to all those who are newly diagnosed.10
But all of these groups may need to rethink their recommendations in light of the latest findings from the O’Kane RCT.
STUDY SUMMARY: Self-monitoring has little effect on glycemic control
O’Kane and colleagues conducted a prospective RCT comparing self-monitoring versus no monitoring among 184 people with newly diagnosed type 2 diabetes.1 Patients were randomized to the self-monitoring or control group for 1 year, with clinic visits at 3-month intervals. Those who were already taking insulin or had engaged in self-monitoring of blood glucose were excluded.
At baseline, there was no significant difference in HbA1c, age, or sex between the 2 groups. Participants in both groups underwent identical diabetes education programs throughout the study period and received dietary and medical management based on the same treatment algorithm. Patients whose baseline HbA1c was >7.5% received metformin, followed by the sulfonylurea gliclazide if they did not reach target at the maximum dose of metformin. There was no significant difference in medication use at baseline or at 12 months.
Patients in the self-monitoring group were given glucose monitors and asked to record 4 fasting and 4 postprandial capillary blood glucose measurements per week. They were also taught to monitor and interpret blood glucose readings, and to respond appropriately to high or low readings.
At each follow-up visit, patients underwent blood tests for HbA1c, lipids, and electrolyte levels and completed questionnaires about treatment satisfaction, attitudes about diabetes, and levels of depression, anxiety, and well-being. Adherence to self-monitoring was verified by downloading meter readings. The dropout rate was low (2.2%), and adherence in the self-monitoring group was high. Study results were assessed using intent-to-treat analysis.
HbA1c fell in both the self-monitoring and control groups, with no significant differences at any point. The mean (standard deviation) value at 12 months was 6.9% (0.8%) in the self-monitoring group, compared to 6.9% (1.2%) in the control group, with a 95% confidence interval for the change in HbA1c of –0.25% to 0.38%. Throughout the study period, there was no difference in use of oral hypoglycemic medications or reported hypoglycemia.
Self-monitoring linked to depression
Measures of depression and anxiety were scored on a 100-point scale and compared to baseline measurements. At 12 months, participants in the self-monitoring group were more depressed, scoring 6% higher, on average, on the depression subscale of the well-being questionnaire (P=.01) than those in the control group. There was a trend toward increased anxiety in the self-monitoring group, but no significant differences in well-being, energy, or any of the other diabetes attitude subscales.
WHAT’S NEW: Less may be better
Because we emphasize self-management skills when we counsel patients about diabetes, it is surprising to learn that knowledge about glycemic control and blood sugar levels does not lead to better glycemic control. This RCT provides strong evidence that more information is not necessarily desirable, at least for patients with newly diagnosed type 2 diabetes who do not need insulin.
Depression is a known complication of diabetes. It affects an estimated 10% to 30% of patients with diabetes, who have double the odds of depression compared to people without diabetes.11,12 Patients with depression and diabetes have poorer glycemic control,13,14 an increased risk of complications,15-17 a decreased quality of life,18 an increased disability burden,19,20 and increased health care use and costs.18,21,22 In addition, they face a significantly higher risk of death from all causes, beyond the risks associated with depression or diabetes alone.23
CAVEATS: Patients on sulfonylureas may be an exception
This study used metformin as the initial oral medication, with sulfonylureas reserved for those who did not reach target glycemic control with maximum metformin therapy. The number of patients taking sulfonylureas was 11 in the self-monitoring group and 6 in the control group. Because hypoglycemia is a concern in patients taking sulfonylureas, there may be a role for self-monitoring of blood glucose in these patients.
Also of note: This study does not provide definitive evidence that self-monitoring of blood glucose causes harm. Although self-monitoring was associated with a 6% higher score on a depression subscale and a trend toward increased anxiety, overall satisfaction with treatment was similar in both groups. Additional studies are needed to better understand the relationship between self-monitoring and depression.
Self-monitoring may still be a good idea for certain patients, regardless of their diabetic medication regimen. When evaluating the potential benefits of self-monitoring of blood glucose, physicians should consider the individual’s predisposition to depression, among other concerns.
CHALLENGES TO IMPLEMENTATION: Hard to forego a practice that everyone expects
Self-monitoring serves different purposes for different populations. Blood glucose levels, along with HbA1c, can guide clinicians in making treatment decisions. Knowing blood sugar levels may be educational or empowering to patients, and provides critical information if hypoglycemia is a concern. These considerations lead us to conclude that while self-monitoring is not indicated for all newly diagnosed diabetic patients, it should be considered in selected circumstances.
Because of the prevalence of self-monitoring of blood glucose, patients may see it as a key component of an optimal self-management regimen. It may be hard to convince patients with newly diagnosed diabetes otherwise—and to convince some clinicians that there is little benefit in recommending it. Again, clinical judgment is required. We suspect, however, that with the proper explanation, many patients will be relieved to learn that they will not have to prick their fingers regularly or record their blood glucose.
Acknowledgements
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center for Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. O’Kane MJ, Bunting B, Copeland M, Coates VE. ESMON study group Efficacy of self monitoring of blood glucose in patients with newly diagnosed type 2 diabetes (ESMON study): randomised controlled trial. BMJ. 2008;336:1174-1177.
2. McIntosh A, Hutchinson A, Home PD, et al. Clinical guidelines and evidence review for Type 2 diabetes: management of blood glucose. 2002. Scharr, University of Sheffield. Available at: . Accessed July 29, 2008.
3. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee Canadian Diabetes Association 2003 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes. 2003;27(suppl 2):S18-S23.
4. Karter AJ, Ackerson LM, Darbinian JA, et al. Self-monitoring of blood glucose levels and glycemic control: the Northern California Kaiser Permanente Diabetes Registry. Am J Med. 2001;111:1-9.
5. Sarol JN Jr, Nicodemus NA Jr, Tan KM, Grava MB. Self-monitoring of blood glucose as part of a multi-component therapy among non-insulin requiring type 2 diabetes patients: a meta-analysis (1966-2004). Curr Med Res Opin. 2005;21:173-184.
6. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring of blood glucose in patients with type 2 diabetes who are not using insulin: a systematic review. Diabetes Care. 2005;28:1510-1517.
7. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2005;18(2):CD005060.-
8. US Department of Health and Human Services Healthy People 2010. Increase the proportion of adults with diabetes who perform self-blood-glucose-monitoring at least once daily. Available at: http://www.healthypeople.gov/document/html/objectives/05-17.htm. Accessed July 29, 2008
9. American Diabetes Association Executive summary: standards of medical care in diabetes—2008. Diabetes Care. 2008;31(suppl 1):S5-S11.Available at: http://care.diabetesjournals.org/cgi/content/full/31/Supplement_1/S5. Accessed July 29, 2008.
10. International Diabetes Federation Clinical Guidelines Taskforce Global guidelines for type 2 diabetes: recommendations for standard, comprehensive and minimal care. Diabetes Med. 2006;23:579-593.
11. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care. 2001;24:1069-1078.
12. Egede LE, Zheng D. Independent factors associated with major depressive disorder in a national sample of individuals with diabetes. Diabetes Care. 2003;26:104-111.
13. De Groot M, Jacobson AM, Samson JA, Welch G. Glycemic control and major depression in patients with type 1 and type 2 diabetes mellitus. J Psychosom Res. 1999;46:425-435.
14. Ciechanowski PS, Katon WJ, Russo JE, Hirsch IB. The relationship of depressive symptoms to symptom reporting, self-care and glucose control in diabetes. Gen Hosp Psychiatry. 2003;25:246-252.
15. De Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. 2001;63:619-630.
16. Black SA, Markides KS, Ray LA. Depression predicts increased incidence of adverse health outcomes in older Mexican Americans with type 2 diabetes. Diabetes Care. 2003;26:2822-2828.
17. Kinder LS, Kamarck TW, Baum A, Orchard TJ. Depressive symptomatology and coronary heart disease in type I diabetes mellitus: a study of possible mechanisms. Health Psychol. 2002;21:542-552.
18. Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med. 2000;160:3278-3285.
19. Egede LE. Diabetes, major depression, and functional disability among U.S. adults. Diabetes Care. 2004;27:421-428.
20. Egede LE. Effects of depression on work loss and disability bed days in individuals with diabetes. Diabetes Care. 2004;27:1751-1753.
21. Egede LE, Zheng D, Simpson K. Comorbid depression is associated with increased health care use and expenditures in individuals with diabetes. Diabetes Care. 2002;25:464-470.
22. Finkelstein EA, Bray JW, Chen H. Prevalence and costs of major depression among elderly claimants with diabetes. Diabetes Care. 2003;26:415-420.
23. Egede LE, Nietert PJ, Zheng D. Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care. 2005;28:1339-1345.
1. O’Kane MJ, Bunting B, Copeland M, Coates VE. ESMON study group Efficacy of self monitoring of blood glucose in patients with newly diagnosed type 2 diabetes (ESMON study): randomised controlled trial. BMJ. 2008;336:1174-1177.
2. McIntosh A, Hutchinson A, Home PD, et al. Clinical guidelines and evidence review for Type 2 diabetes: management of blood glucose. 2002. Scharr, University of Sheffield. Available at: . Accessed July 29, 2008.
3. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee Canadian Diabetes Association 2003 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes. 2003;27(suppl 2):S18-S23.
4. Karter AJ, Ackerson LM, Darbinian JA, et al. Self-monitoring of blood glucose levels and glycemic control: the Northern California Kaiser Permanente Diabetes Registry. Am J Med. 2001;111:1-9.
5. Sarol JN Jr, Nicodemus NA Jr, Tan KM, Grava MB. Self-monitoring of blood glucose as part of a multi-component therapy among non-insulin requiring type 2 diabetes patients: a meta-analysis (1966-2004). Curr Med Res Opin. 2005;21:173-184.
6. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring of blood glucose in patients with type 2 diabetes who are not using insulin: a systematic review. Diabetes Care. 2005;28:1510-1517.
7. Welschen LM, Bloemendal E, Nijpels G, et al. Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin. Cochrane Database Syst Rev. 2005;18(2):CD005060.-
8. US Department of Health and Human Services Healthy People 2010. Increase the proportion of adults with diabetes who perform self-blood-glucose-monitoring at least once daily. Available at: http://www.healthypeople.gov/document/html/objectives/05-17.htm. Accessed July 29, 2008
9. American Diabetes Association Executive summary: standards of medical care in diabetes—2008. Diabetes Care. 2008;31(suppl 1):S5-S11.Available at: http://care.diabetesjournals.org/cgi/content/full/31/Supplement_1/S5. Accessed July 29, 2008.
10. International Diabetes Federation Clinical Guidelines Taskforce Global guidelines for type 2 diabetes: recommendations for standard, comprehensive and minimal care. Diabetes Med. 2006;23:579-593.
11. Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care. 2001;24:1069-1078.
12. Egede LE, Zheng D. Independent factors associated with major depressive disorder in a national sample of individuals with diabetes. Diabetes Care. 2003;26:104-111.
13. De Groot M, Jacobson AM, Samson JA, Welch G. Glycemic control and major depression in patients with type 1 and type 2 diabetes mellitus. J Psychosom Res. 1999;46:425-435.
14. Ciechanowski PS, Katon WJ, Russo JE, Hirsch IB. The relationship of depressive symptoms to symptom reporting, self-care and glucose control in diabetes. Gen Hosp Psychiatry. 2003;25:246-252.
15. De Groot M, Anderson R, Freedland KE, Clouse RE, Lustman PJ. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. 2001;63:619-630.
16. Black SA, Markides KS, Ray LA. Depression predicts increased incidence of adverse health outcomes in older Mexican Americans with type 2 diabetes. Diabetes Care. 2003;26:2822-2828.
17. Kinder LS, Kamarck TW, Baum A, Orchard TJ. Depressive symptomatology and coronary heart disease in type I diabetes mellitus: a study of possible mechanisms. Health Psychol. 2002;21:542-552.
18. Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med. 2000;160:3278-3285.
19. Egede LE. Diabetes, major depression, and functional disability among U.S. adults. Diabetes Care. 2004;27:421-428.
20. Egede LE. Effects of depression on work loss and disability bed days in individuals with diabetes. Diabetes Care. 2004;27:1751-1753.
21. Egede LE, Zheng D, Simpson K. Comorbid depression is associated with increased health care use and expenditures in individuals with diabetes. Diabetes Care. 2002;25:464-470.
22. Finkelstein EA, Bray JW, Chen H. Prevalence and costs of major depression among elderly claimants with diabetes. Diabetes Care. 2003;26:415-420.
23. Egede LE, Nietert PJ, Zheng D. Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care. 2005;28:1339-1345.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Acute gout: Oral steroids work as well as NSAIDs
Use a short course of oral steroids (prednisone 30-40 mg/d for 5 days) for treatment of acute gout when nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated. Steroids are also a reasonable choice as first-line treatment.1,2
Strength of recommendation
B: 2 good-quality, randomized controlled trials (RCTs)
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomized equivalence trial. Lancet. 2008;371:1854-1860.
Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
ILLUSTRATIVE CASE
A 68-year-old man with a history of ulcer disease and mild renal insufficiency comes to your office complaining of severe pain in his right foot. You note swelling and redness around the base of the big toe and diagnose acute gout. Wishing to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine because of the patient’s medical history, you wonder what you can safely prescribe for pain relief.
NSAIDs have become the mainstay of treatment for acute gout,3,4 replacing colchicine—widely used for gout pain relief since the early 19th century.5 Colchicine fell out of favor because it routinely causes diarrhea and requires caution in patients with renal insufficiency.6 Now, however, there is growing concern about the adverse effects of NSAIDs.
Comorbidities, age, mean fewer options
NSAIDs increase the risk of gastrointestinal (GI) bleeding, especially in the first week of use.7 Cyclooxygenase-2 (COX-2) inhibitors, considered as effective as NSAIDs in treating acute gout pain,8 are also associated with GI bleeds.9 In addition, NSAIDs and COX-2 inhibitors increase cardiovascular risks, prompting the American Heart Association to recommend restricted use of both.10 NSAIDs’ effect on renal function, fluid retention, and interactions with anticoagulants are additional concerns, because gout patients are generally older and often have comorbid renal and cardiovascular diseases.3,11-13
In the United States, nearly 70% of patients who develop acute gout seek treatment from primary care physicians.12 Family physicians need a safe alternative to NSAIDs to relieve the severe pain associated with this condition. Will oral corticosteroids fit the bill?
STUDY SUMMARIES: Oral steroids: A safe and effective alternative
Janssens et al1 conducted a double-blind, randomized equivalence trial of 118 patients to compare the efficacy of prednisolone and naproxen for the treatment of monoarticular gout, confirmed by crystal analysis of synovial fluid. The study was conducted in the eastern Netherlands at a trial center patients were referred to by their family physicians. Those with major comorbidities, including a history of GI bleed or peptic ulcer, were excluded.
Participants were randomized to receive either prednisolone 35 mg* or naproxen 500 mg twice a day, with look-alike placebo tablets of the alternate drug, for 5 days. Pain, the primary outcome, was scored on a validated visual analog scale from 0 mm (no pain) to 100 mm (worst pain experienced).15 The reduction in the pain score at 90 hours was similar in both groups. Only a few minor side effects were reported in both groups, and all completely resolved in 3 weeks.
The study by Man et al2 was a randomized trial that compared indomethacin with oral prednisolone in 90 patients presenting to an emergency department in Hong Kong. Diagnosis of gout was made by clinical impression. Participants in the indomethacin group also received an intramuscular (IM) injection of diclofenac 75 mg, and those in both groups were monitored for acetaminophen use as a secondary endpoint.
Pain reduction, the primary endpoint, was assessed with a 10-point visual analog score, and was slightly better statistically in the oral steroid group. The study was not designed to evaluate for safety, but the authors noted that patients in the indomethacin group experienced more adverse effects (number needed to harm [NNH] for any adverse event: 3; NNH for serious events: 6).

Short-term steroids have few side effects
In both studies, patients receiving oral steroids experienced no significant side effects. This finding is consistent with other studies that have investigated short-term oral steroid use in the treatment of both rheumatoid arthritis and asthma.16,17
WHAT’S NEW?: Evidence supports use of steroids for acute gout
In the United States, prednisone is prescribed as treatment for acute gout only about 9% of the time.12 These 2 studies—the first randomized trials comparing oral steroids with NSAIDs, the usual gout treatment—may lead to greater use of steroids for this painful condition.
Both studies were well designed and conducted in an outpatient (or emergency) setting. Both showed that a short course of oral steroids is as effective as NSAIDs, and without significant side effects.
Previous studies have compared IM steroids with NSAIDs, and IM steroids with IM adrenocorticotropic hormone (ACTH).18,19 However, these studies were not blinded—just one of their methodological problems.4
CAVEATS: Joint aspiration is not the norm
In the Janssens study, participants were diagnosed with gout after monosodium urate crystals were found in joint aspirate.1 This may not be the usual practice in primary care settings, where a clinical diagnosis of gout is typically made. The authors indicate that the failure to perform joint aspiration will lead to occasional cases of septic arthritis being treated with oral steroids. We recommend joint aspiration or a referral for such a procedure when clinical evidence (eg, fever and leukocytosis) is suggestive of septic arthritis.
Possible impact of acetaminophen
In the study by Man et al, acetaminophen was used by both groups as an adjunct for pain relief, and the amount used was higher (mean 10.3 g vs 6.4 g over 14 days) in the oral steroid group. It is possible that some of the pain relief experienced by those in the steroid group may have been from acetaminophen; however, a difference of 4 g over a 14-day period makes that unlikely. Even if additional acetaminophen is required, the advantages of oral steroids rather than NSAIDs or colchicine for patients with contraindications remain.
Also of note: These trials examined short-term treatment of acute gout. These findings cannot be extrapolated to the treatment of intercurrent gout or chronic gouty arthritis, since long-term steroid use has severe adverse effects.
CHALLENGES TO IMPLEMENTATION: No significant barriers
We found little to prevent physicians from adopting this practice changer. Oral steroids are readily available and inexpensive, and most primary care clinicians regularly prescribe them for other conditions. This practice change recommendation should be readily implemented.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
* Prednisone is the precursor of prednisolone and is activated in the liver. The activity of both drugs is comparable, and prednisone and prednisolone can be converted milligram to milligram. However, prednisolone may be preferred for patients with severe liver disease.14 (In the United States, prednisolone is available as a liquid and prednisone as a tablet.)
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860.
2. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
3. Sutaria S, Katbamna R, Underwood M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout—a systematic review. Rheumatology. 2006;45:1422-1431.
4. Janssens HJ, Lucassen PL, Van de Laar FA, Janssen M, Van de Lisdonk EH. Systemic corticosteroids for acute gout. Cochrane Database Syst Rev. 2008;(2):CD005521.-
5. Weinberger A, Pinkhas J. The history of colchicine. Korot. 1980;7:760-763.
6. Ahern MJ, Reid C, Gordon TP, McCredie M, Brooks PM, Jones M. Does colchicine work? The results of the first controlled study in acute gout. ANZ J Med. 1987;17:301-304.
7. Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320-326.
8. Rubin BR, Burton R, Navarra S, et al. Efficacy and safety profile of treatment with etoricoxib 120 mg once daily compared with indomethacin 50 mg three times daily in acute gout: a randomized controlled trial. Arthritis Rheum. 2004;50:598-606.
9. Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf. 2004;27:411-420.
10. Antman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115:1634-1642.
11. Petersel D, Schlesinger N. Treatment of acute gout in hospitalized patients. J Rheumatol. 2007;34:1566-1568.
12. Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498-501.
13. Krishnan E, Svendsen K, Neaton JD, Grandits G, Kuller LH. MRFIT Research Group. Long-term cardiovascular mortality among middle-aged men with gout. Arch Intern Med. 2008;168:1104-1110.
14. Davis M, Williams R, Chakraborty J, et al. Prednisone or prednisolone for the treatment of chronic active hepatitis? A comparison of plasma availability. Br J Clin Pharmacol. 1978;5:501-505.
15. Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23:285-295.
16. Gotzsche PC, Johansen HK. Short-term low-dose corticosteroids vs placebo and nonsteroidal antiinflammatory drugs in rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD000189.-
17. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002308.-
18. Alloway JA, Moriarty MJ, Hoogland YT, Nashel DJ. Comparison of triamcinolone acetonide with indomethacin in the treatment of acute gouty arthritis. J Rheumatol. 1993;20:111-113.
19. Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and triamcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol. 1994;21:1325-1327.
Use a short course of oral steroids (prednisone 30-40 mg/d for 5 days) for treatment of acute gout when nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated. Steroids are also a reasonable choice as first-line treatment.1,2
Strength of recommendation
B: 2 good-quality, randomized controlled trials (RCTs)
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomized equivalence trial. Lancet. 2008;371:1854-1860.
Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
ILLUSTRATIVE CASE
A 68-year-old man with a history of ulcer disease and mild renal insufficiency comes to your office complaining of severe pain in his right foot. You note swelling and redness around the base of the big toe and diagnose acute gout. Wishing to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine because of the patient’s medical history, you wonder what you can safely prescribe for pain relief.
NSAIDs have become the mainstay of treatment for acute gout,3,4 replacing colchicine—widely used for gout pain relief since the early 19th century.5 Colchicine fell out of favor because it routinely causes diarrhea and requires caution in patients with renal insufficiency.6 Now, however, there is growing concern about the adverse effects of NSAIDs.
Comorbidities, age, mean fewer options
NSAIDs increase the risk of gastrointestinal (GI) bleeding, especially in the first week of use.7 Cyclooxygenase-2 (COX-2) inhibitors, considered as effective as NSAIDs in treating acute gout pain,8 are also associated with GI bleeds.9 In addition, NSAIDs and COX-2 inhibitors increase cardiovascular risks, prompting the American Heart Association to recommend restricted use of both.10 NSAIDs’ effect on renal function, fluid retention, and interactions with anticoagulants are additional concerns, because gout patients are generally older and often have comorbid renal and cardiovascular diseases.3,11-13
In the United States, nearly 70% of patients who develop acute gout seek treatment from primary care physicians.12 Family physicians need a safe alternative to NSAIDs to relieve the severe pain associated with this condition. Will oral corticosteroids fit the bill?
STUDY SUMMARIES: Oral steroids: A safe and effective alternative
Janssens et al1 conducted a double-blind, randomized equivalence trial of 118 patients to compare the efficacy of prednisolone and naproxen for the treatment of monoarticular gout, confirmed by crystal analysis of synovial fluid. The study was conducted in the eastern Netherlands at a trial center patients were referred to by their family physicians. Those with major comorbidities, including a history of GI bleed or peptic ulcer, were excluded.
Participants were randomized to receive either prednisolone 35 mg* or naproxen 500 mg twice a day, with look-alike placebo tablets of the alternate drug, for 5 days. Pain, the primary outcome, was scored on a validated visual analog scale from 0 mm (no pain) to 100 mm (worst pain experienced).15 The reduction in the pain score at 90 hours was similar in both groups. Only a few minor side effects were reported in both groups, and all completely resolved in 3 weeks.
The study by Man et al2 was a randomized trial that compared indomethacin with oral prednisolone in 90 patients presenting to an emergency department in Hong Kong. Diagnosis of gout was made by clinical impression. Participants in the indomethacin group also received an intramuscular (IM) injection of diclofenac 75 mg, and those in both groups were monitored for acetaminophen use as a secondary endpoint.
Pain reduction, the primary endpoint, was assessed with a 10-point visual analog score, and was slightly better statistically in the oral steroid group. The study was not designed to evaluate for safety, but the authors noted that patients in the indomethacin group experienced more adverse effects (number needed to harm [NNH] for any adverse event: 3; NNH for serious events: 6).
Short-term steroids have few side effects
In both studies, patients receiving oral steroids experienced no significant side effects. This finding is consistent with other studies that have investigated short-term oral steroid use in the treatment of both rheumatoid arthritis and asthma.16,17
WHAT’S NEW?: Evidence supports use of steroids for acute gout
In the United States, prednisone is prescribed as treatment for acute gout only about 9% of the time.12 These 2 studies—the first randomized trials comparing oral steroids with NSAIDs, the usual gout treatment—may lead to greater use of steroids for this painful condition.
Both studies were well designed and conducted in an outpatient (or emergency) setting. Both showed that a short course of oral steroids is as effective as NSAIDs, and without significant side effects.
Previous studies have compared IM steroids with NSAIDs, and IM steroids with IM adrenocorticotropic hormone (ACTH).18,19 However, these studies were not blinded—just one of their methodological problems.4
CAVEATS: Joint aspiration is not the norm
In the Janssens study, participants were diagnosed with gout after monosodium urate crystals were found in joint aspirate.1 This may not be the usual practice in primary care settings, where a clinical diagnosis of gout is typically made. The authors indicate that the failure to perform joint aspiration will lead to occasional cases of septic arthritis being treated with oral steroids. We recommend joint aspiration or a referral for such a procedure when clinical evidence (eg, fever and leukocytosis) is suggestive of septic arthritis.
Possible impact of acetaminophen
In the study by Man et al, acetaminophen was used by both groups as an adjunct for pain relief, and the amount used was higher (mean 10.3 g vs 6.4 g over 14 days) in the oral steroid group. It is possible that some of the pain relief experienced by those in the steroid group may have been from acetaminophen; however, a difference of 4 g over a 14-day period makes that unlikely. Even if additional acetaminophen is required, the advantages of oral steroids rather than NSAIDs or colchicine for patients with contraindications remain.
Also of note: These trials examined short-term treatment of acute gout. These findings cannot be extrapolated to the treatment of intercurrent gout or chronic gouty arthritis, since long-term steroid use has severe adverse effects.
CHALLENGES TO IMPLEMENTATION: No significant barriers
We found little to prevent physicians from adopting this practice changer. Oral steroids are readily available and inexpensive, and most primary care clinicians regularly prescribe them for other conditions. This practice change recommendation should be readily implemented.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
* Prednisone is the precursor of prednisolone and is activated in the liver. The activity of both drugs is comparable, and prednisone and prednisolone can be converted milligram to milligram. However, prednisolone may be preferred for patients with severe liver disease.14 (In the United States, prednisolone is available as a liquid and prednisone as a tablet.)
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Use a short course of oral steroids (prednisone 30-40 mg/d for 5 days) for treatment of acute gout when nonsteroidal anti-inflammatory drugs (NSAIDs) are contraindicated. Steroids are also a reasonable choice as first-line treatment.1,2
Strength of recommendation
B: 2 good-quality, randomized controlled trials (RCTs)
Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomized equivalence trial. Lancet. 2008;371:1854-1860.
Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
ILLUSTRATIVE CASE
A 68-year-old man with a history of ulcer disease and mild renal insufficiency comes to your office complaining of severe pain in his right foot. You note swelling and redness around the base of the big toe and diagnose acute gout. Wishing to avoid nonsteroidal anti-inflammatory drugs (NSAIDs) and colchicine because of the patient’s medical history, you wonder what you can safely prescribe for pain relief.
NSAIDs have become the mainstay of treatment for acute gout,3,4 replacing colchicine—widely used for gout pain relief since the early 19th century.5 Colchicine fell out of favor because it routinely causes diarrhea and requires caution in patients with renal insufficiency.6 Now, however, there is growing concern about the adverse effects of NSAIDs.
Comorbidities, age, mean fewer options
NSAIDs increase the risk of gastrointestinal (GI) bleeding, especially in the first week of use.7 Cyclooxygenase-2 (COX-2) inhibitors, considered as effective as NSAIDs in treating acute gout pain,8 are also associated with GI bleeds.9 In addition, NSAIDs and COX-2 inhibitors increase cardiovascular risks, prompting the American Heart Association to recommend restricted use of both.10 NSAIDs’ effect on renal function, fluid retention, and interactions with anticoagulants are additional concerns, because gout patients are generally older and often have comorbid renal and cardiovascular diseases.3,11-13
In the United States, nearly 70% of patients who develop acute gout seek treatment from primary care physicians.12 Family physicians need a safe alternative to NSAIDs to relieve the severe pain associated with this condition. Will oral corticosteroids fit the bill?
STUDY SUMMARIES: Oral steroids: A safe and effective alternative
Janssens et al1 conducted a double-blind, randomized equivalence trial of 118 patients to compare the efficacy of prednisolone and naproxen for the treatment of monoarticular gout, confirmed by crystal analysis of synovial fluid. The study was conducted in the eastern Netherlands at a trial center patients were referred to by their family physicians. Those with major comorbidities, including a history of GI bleed or peptic ulcer, were excluded.
Participants were randomized to receive either prednisolone 35 mg* or naproxen 500 mg twice a day, with look-alike placebo tablets of the alternate drug, for 5 days. Pain, the primary outcome, was scored on a validated visual analog scale from 0 mm (no pain) to 100 mm (worst pain experienced).15 The reduction in the pain score at 90 hours was similar in both groups. Only a few minor side effects were reported in both groups, and all completely resolved in 3 weeks.
The study by Man et al2 was a randomized trial that compared indomethacin with oral prednisolone in 90 patients presenting to an emergency department in Hong Kong. Diagnosis of gout was made by clinical impression. Participants in the indomethacin group also received an intramuscular (IM) injection of diclofenac 75 mg, and those in both groups were monitored for acetaminophen use as a secondary endpoint.
Pain reduction, the primary endpoint, was assessed with a 10-point visual analog score, and was slightly better statistically in the oral steroid group. The study was not designed to evaluate for safety, but the authors noted that patients in the indomethacin group experienced more adverse effects (number needed to harm [NNH] for any adverse event: 3; NNH for serious events: 6).
Short-term steroids have few side effects
In both studies, patients receiving oral steroids experienced no significant side effects. This finding is consistent with other studies that have investigated short-term oral steroid use in the treatment of both rheumatoid arthritis and asthma.16,17
WHAT’S NEW?: Evidence supports use of steroids for acute gout
In the United States, prednisone is prescribed as treatment for acute gout only about 9% of the time.12 These 2 studies—the first randomized trials comparing oral steroids with NSAIDs, the usual gout treatment—may lead to greater use of steroids for this painful condition.
Both studies were well designed and conducted in an outpatient (or emergency) setting. Both showed that a short course of oral steroids is as effective as NSAIDs, and without significant side effects.
Previous studies have compared IM steroids with NSAIDs, and IM steroids with IM adrenocorticotropic hormone (ACTH).18,19 However, these studies were not blinded—just one of their methodological problems.4
CAVEATS: Joint aspiration is not the norm
In the Janssens study, participants were diagnosed with gout after monosodium urate crystals were found in joint aspirate.1 This may not be the usual practice in primary care settings, where a clinical diagnosis of gout is typically made. The authors indicate that the failure to perform joint aspiration will lead to occasional cases of septic arthritis being treated with oral steroids. We recommend joint aspiration or a referral for such a procedure when clinical evidence (eg, fever and leukocytosis) is suggestive of septic arthritis.
Possible impact of acetaminophen
In the study by Man et al, acetaminophen was used by both groups as an adjunct for pain relief, and the amount used was higher (mean 10.3 g vs 6.4 g over 14 days) in the oral steroid group. It is possible that some of the pain relief experienced by those in the steroid group may have been from acetaminophen; however, a difference of 4 g over a 14-day period makes that unlikely. Even if additional acetaminophen is required, the advantages of oral steroids rather than NSAIDs or colchicine for patients with contraindications remain.
Also of note: These trials examined short-term treatment of acute gout. These findings cannot be extrapolated to the treatment of intercurrent gout or chronic gouty arthritis, since long-term steroid use has severe adverse effects.
CHALLENGES TO IMPLEMENTATION: No significant barriers
We found little to prevent physicians from adopting this practice changer. Oral steroids are readily available and inexpensive, and most primary care clinicians regularly prescribe them for other conditions. This practice change recommendation should be readily implemented.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
* Prednisone is the precursor of prednisolone and is activated in the liver. The activity of both drugs is comparable, and prednisone and prednisolone can be converted milligram to milligram. However, prednisolone may be preferred for patients with severe liver disease.14 (In the United States, prednisolone is available as a liquid and prednisone as a tablet.)
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860.
2. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
3. Sutaria S, Katbamna R, Underwood M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout—a systematic review. Rheumatology. 2006;45:1422-1431.
4. Janssens HJ, Lucassen PL, Van de Laar FA, Janssen M, Van de Lisdonk EH. Systemic corticosteroids for acute gout. Cochrane Database Syst Rev. 2008;(2):CD005521.-
5. Weinberger A, Pinkhas J. The history of colchicine. Korot. 1980;7:760-763.
6. Ahern MJ, Reid C, Gordon TP, McCredie M, Brooks PM, Jones M. Does colchicine work? The results of the first controlled study in acute gout. ANZ J Med. 1987;17:301-304.
7. Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320-326.
8. Rubin BR, Burton R, Navarra S, et al. Efficacy and safety profile of treatment with etoricoxib 120 mg once daily compared with indomethacin 50 mg three times daily in acute gout: a randomized controlled trial. Arthritis Rheum. 2004;50:598-606.
9. Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf. 2004;27:411-420.
10. Antman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115:1634-1642.
11. Petersel D, Schlesinger N. Treatment of acute gout in hospitalized patients. J Rheumatol. 2007;34:1566-1568.
12. Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498-501.
13. Krishnan E, Svendsen K, Neaton JD, Grandits G, Kuller LH. MRFIT Research Group. Long-term cardiovascular mortality among middle-aged men with gout. Arch Intern Med. 2008;168:1104-1110.
14. Davis M, Williams R, Chakraborty J, et al. Prednisone or prednisolone for the treatment of chronic active hepatitis? A comparison of plasma availability. Br J Clin Pharmacol. 1978;5:501-505.
15. Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23:285-295.
16. Gotzsche PC, Johansen HK. Short-term low-dose corticosteroids vs placebo and nonsteroidal antiinflammatory drugs in rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD000189.-
17. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002308.-
18. Alloway JA, Moriarty MJ, Hoogland YT, Nashel DJ. Comparison of triamcinolone acetonide with indomethacin in the treatment of acute gouty arthritis. J Rheumatol. 1993;20:111-113.
19. Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and triamcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol. 1994;21:1325-1327.
1. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371:1854-1860.
2. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49:670-677.
3. Sutaria S, Katbamna R, Underwood M. Effectiveness of interventions for the treatment of acute and prevention of recurrent gout—a systematic review. Rheumatology. 2006;45:1422-1431.
4. Janssens HJ, Lucassen PL, Van de Laar FA, Janssen M, Van de Lisdonk EH. Systemic corticosteroids for acute gout. Cochrane Database Syst Rev. 2008;(2):CD005521.-
5. Weinberger A, Pinkhas J. The history of colchicine. Korot. 1980;7:760-763.
6. Ahern MJ, Reid C, Gordon TP, McCredie M, Brooks PM, Jones M. Does colchicine work? The results of the first controlled study in acute gout. ANZ J Med. 1987;17:301-304.
7. Lewis SC, Langman MJ, Laporte JR, Matthews JN, Rawlins MD, Wiholm BE. Dose-response relationships between individual nonaspirin nonsteroidal anti-inflammatory drugs (NANSAIDs) and serious upper gastrointestinal bleeding: a meta-analysis based on individual patient data. Br J Clin Pharmacol. 2002;54:320-326.
8. Rubin BR, Burton R, Navarra S, et al. Efficacy and safety profile of treatment with etoricoxib 120 mg once daily compared with indomethacin 50 mg three times daily in acute gout: a randomized controlled trial. Arthritis Rheum. 2004;50:598-606.
9. Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R. Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf. 2004;27:411-420.
10. Antman EM, Bennett JS, Daugherty A, et al. Use of nonsteroidal antiinflammatory drugs: an update for clinicians: a scientific statement from the American Heart Association. Circulation. 2007;115:1634-1642.
11. Petersel D, Schlesinger N. Treatment of acute gout in hospitalized patients. J Rheumatol. 2007;34:1566-1568.
12. Krishnan E, Lienesch D, Kwoh CK. Gout in ambulatory care settings in the United States. J Rheumatol. 2008;35:498-501.
13. Krishnan E, Svendsen K, Neaton JD, Grandits G, Kuller LH. MRFIT Research Group. Long-term cardiovascular mortality among middle-aged men with gout. Arch Intern Med. 2008;168:1104-1110.
14. Davis M, Williams R, Chakraborty J, et al. Prednisone or prednisolone for the treatment of chronic active hepatitis? A comparison of plasma availability. Br J Clin Pharmacol. 1978;5:501-505.
15. Todd KH. Pain assessment instruments for use in the emergency department. Emerg Med Clin North Am. 2005;23:285-295.
16. Gotzsche PC, Johansen HK. Short-term low-dose corticosteroids vs placebo and nonsteroidal antiinflammatory drugs in rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(3):CD000189.-
17. Rowe BH, Spooner C, Ducharme FM, Bretzlaff JA, Bota GW. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev. 2001;(1):CD002308.-
18. Alloway JA, Moriarty MJ, Hoogland YT, Nashel DJ. Comparison of triamcinolone acetonide with indomethacin in the treatment of acute gouty arthritis. J Rheumatol. 1993;20:111-113.
19. Siegel LB, Alloway JA, Nashel DJ. Comparison of adrenocorticotropic hormone and triamcinolone acetonide in the treatment of acute gouty arthritis. J Rheumatol. 1994;21:1325-1327.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Sequential therapy boosts H pylori eradication rates
Prescribe sequential therapy rather than the standard (concurrent) therapy to improve H pylori eradication rates, particularly in treatment-naïve patients.1
Strength of recommendation
B: Based on a well-done meta-analysis with disease-oriented outcomes
Jafri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Ann Intern Med. 2008;148:923-931.
ILLUSTRATIVE CASE
A 40-year-old woman with a peptic ulcer has been diagnosed with Helicobacter pylori infection, and schedules a visit to discuss treatment. You’re aware of the declining eradication rates associated with standard therapy, and have heard that sequential therapy may be a more effective option. Should you offer it to this patient?
An estimated 30% to 40% of the US population is infected with H pylori,2 a bacterium that plays a crucial role in the pathogenesis of peptic ulcer disease, chronic gastritis, and gastric cancer.1 The triple-drug regimen (a proton-pump inhibitor [PPI] and clarithromycin with amoxicillin, tinidazole, or another imidazole) is commonly used to treat H pylori in Europe and in the United States.3 Yet the eradication rate associated with this standard 3-drug regimen in this country is <80%, and appears to be on the decline. The likely problem: the increase in antibiotic-resistant strains of H pylori.2
Put amoxicillin first
In Italy, eradication rates of >90% have been reported with a sequential therapy: a PPI and amoxicillin for 5 days, followed by the PPI, clarithromycin, and tinidazole for an additional 5 days (FIGURE).4 (Because tinidazole is a relatively new drug in the United States and physicians may use other drugs in its class instead, we refer to the drug class—imidazoles—rather than a specific medication in the FIGURE and much of the text that follows.) Using amoxicillin before the other antibiotics weakens bacterial cell walls, preventing the formation of drug efflux channels that can inhibit clarithromycin and other antibiotics, according to 1 theory.1 Thus, clarithromycin and an imidazole are more effective in the second phase of treatment.1
Should US physicians adopt the Italian protocol and prescribe tinidazole? Would metronidazole or other imidazoles be equally effective?
FIGURE
Sequential vs standard therapy: A comparison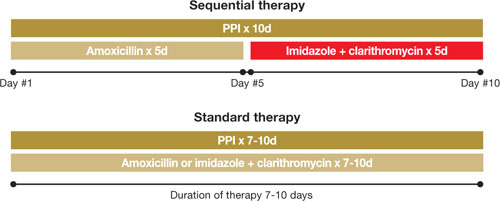
STUDY SUMMARY: Sequential therapy is better on all counts
This meta-analysis found 9 randomized controlled trials (RCTs) that compared H pylori eradication rates with standard 7- to 10-day triple-drug therapy to 10-day sequential therapy; an additional small study used a 5-day triple-drug comparison group. The authors performed a thorough search and used standard meta-analysis methods for data synthesis and analysis. The patients were all H pylori treatment naïve and had not used PPIs, histamine-2 receptor antagonists, or antibiotics in the month preceding the study. All patients (n=2747) had documented H pylori infection based on fecal antigen test, histologic evaluation, biopsy urease test, or urea breath test.
All the trials were conducted in Italy, although 2 of the studies included patients from the United States. Nine RCTs compared a triple-therapy regimen with PPI to sequential therapy, 1 RCT compared a triple-drug regimen with ranitidine to sequential therapy, and 1 included only pediatric patients. Pooled eradication rates were 93.4% (95% confidence interval [CI,] 91.3%-95.5%) for sequential therapy and 76.9% (CI, 71.0%-82.8%) for standard therapy, with a relative risk reduction of 71% (CI, 64%-77%).1 The authors estimated that for every 6.3 patients (95% CI, 5.2-7.1) treated with sequential therapy, there would be 1 additional cure compared to standard therapy. Standard 7- to 10-day triple therapy remained inferior to sequential therapy in all subgroup analyses, including patients with risk factors for eradication failure.
Adherence rates were similar in both groups. Sequential therapy resulted in a median adherence rate of 97.4% (range, 90.0%-98.9%), with standard therapy at 96.8% (range, 93.0%-100%).1 Reported side effects were also similar in both treatment groups.1
WHAT’S NEW?: This meta-analysis reduces doubt
The latest American College of Gastroenterology guidelines on the management of H pylori infection acknowledge that sequential therapy has shown promise in Europe, but the organization has not supported a change from the standard regimen to sequential therapy as first-line treatment. The standard triple-therapy regimen is approved by the US Food and Drug Administration, and is the most commonly used H pylori treatment in the United States.1 This is the first meta-analysis based solely on RCTs, and it clearly demonstrates that sequential therapy increased eradication rates.
Helicobacter pylori (called H pylori for short) is a type of bacteria that can cause an ulcer (sore) to develop within the lining of your stomach and intestines. Ulcers can cause pain and bleeding, so it is important to get rid of this bacteria. To do this, you will need to take 4 different medicines over the next 10 days. They must be taken in a certain order, exactly as your doctor has prescribed.
One of the drugs you will be taking (for the entire 10-day period) is a proton pump inhibitor (called a PPI), a medicine that helps reduce the amount of acid in your stomach. ______________ is the name of the PPI your doctor has ordered. Take it twice a day, once in the morning and once in the evening, for 10 days.
You will also take 3 different kinds of antibiotics to eliminate the H pylori bacteria. For the first 5 days, you will take amoxicillin twice a day (2 pills in the morning and 2 in the evening), along with the PPI.
After 5 days, all the amoxicillin pills should be gone, and you will switch to 2 other antibiotics: clarithromycin AND ______________. For the next 5 days, you will take 1 PPI plus 1 clarithromycin and 1 ______________ every morning AND every night.
These medications may cause nausea, diarrhea, and a bad taste in your mouth. These side effects are usually not serious, but if they bother you so much that you cannot continue to take the medicine, it is important to call our office right away.
To remember to take each of the medicines in the morning AND evening on the correct day, use this chart to follow along. Put a check mark in the morning box or the evening box every time you take your medicine.
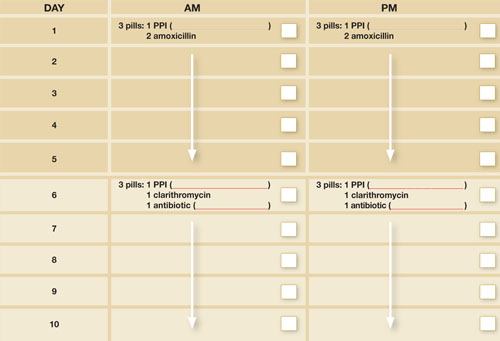
CAVEATS: Drug resistance, previous Tx could skew results
This meta-analysis only included studies performed in Italy, although 2 of the trials did include US recruits. Drug resistance patterns may be different in this country, which could alter sequential therapy’s eradication rates.
Because 3 antibiotics are used in sequential therapy, we may have fewer remaining options for patients who do not respond to this regimen, and we do not have information about patients with previous treatment failures. In addition, this meta-analysis only evaluated H pylori eradication rates in treatment-naïve patients, so we have no information about the effectiveness of this regimen in patients with previous treatment failures.
Would other sequential regimens—or drugs—work?
Patients who are allergic to amoxicillin would not be candidates for this sequential therapy protocol. While sequential therapy was compared with 7- to 10-day standard triple therapy, this study did not compare it with other regimens—eg, quadruple therapy or a 14-day course of standard triple-drug therapy.
Other drugs may also affect outcomes. The sequential therapy studies all used tinidazole, a relatively new agent in the United States; we don’t know whether metronidazole or other imidazoles are as effective.
The authors of this meta-analysis also noted the possibility of publication bias, but we doubt that there are enough unpublished data to invalidate the findings. Also, the selected RCTs only addressed eradication rates and not patient-oriented outcomes. However, most patient-oriented outcomes, including cancer and ulcers, can take years, even decades, to develop.
CHALLENGES TO IMPLEMENTATION: Sequential therapy may be confusing
While adherence rates were similar in the standard and sequential treatment groups in the meta-analysis, sequential therapy—which requires switching medications midway through treatment—might be more confusing for patients in actual practice. This has the potential to negatively affect adherence to the sequential regimen.
It will be important for physicians who prescribe sequential therapy to counsel patients on the importance of completing the treatment regimen exactly as prescribed and to provide clear instructions for doing so, ideally in the form of a patient handout like the one on page 653. Cost is not a problem; the price of sequential therapy is about equal to, or possibly less than, that of standard therapy.5
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Jafri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Ann Intern Med. 2008;148:923-931.
2. Chey WD, Wong BC. American College of Gastroenterology guideline on the management of Helicobacter pylori infection. Am J Gastroenterol. 2007;102:1808-1825.
3. Malfertheiner P, Megraud F, O’Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 2007;56:772-781.
4. Zullo A, De FV, Hassan C, Morini S, Vaira D. The sequential therapy regimen for Helicobacter pylori eradication: a pooled-data analysis. Gut. 2007;56:1353-1357.
5. Vaira D, Zullo A, Vakil N, et al. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: a randomized trial. Ann Intern Med. 2007;146:556-563.
PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Prescribe sequential therapy rather than the standard (concurrent) therapy to improve H pylori eradication rates, particularly in treatment-naïve patients.1
Strength of recommendation
B: Based on a well-done meta-analysis with disease-oriented outcomes
Jafri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Ann Intern Med. 2008;148:923-931.
ILLUSTRATIVE CASE
A 40-year-old woman with a peptic ulcer has been diagnosed with Helicobacter pylori infection, and schedules a visit to discuss treatment. You’re aware of the declining eradication rates associated with standard therapy, and have heard that sequential therapy may be a more effective option. Should you offer it to this patient?
An estimated 30% to 40% of the US population is infected with H pylori,2 a bacterium that plays a crucial role in the pathogenesis of peptic ulcer disease, chronic gastritis, and gastric cancer.1 The triple-drug regimen (a proton-pump inhibitor [PPI] and clarithromycin with amoxicillin, tinidazole, or another imidazole) is commonly used to treat H pylori in Europe and in the United States.3 Yet the eradication rate associated with this standard 3-drug regimen in this country is <80%, and appears to be on the decline. The likely problem: the increase in antibiotic-resistant strains of H pylori.2
Put amoxicillin first
In Italy, eradication rates of >90% have been reported with a sequential therapy: a PPI and amoxicillin for 5 days, followed by the PPI, clarithromycin, and tinidazole for an additional 5 days (FIGURE).4 (Because tinidazole is a relatively new drug in the United States and physicians may use other drugs in its class instead, we refer to the drug class—imidazoles—rather than a specific medication in the FIGURE and much of the text that follows.) Using amoxicillin before the other antibiotics weakens bacterial cell walls, preventing the formation of drug efflux channels that can inhibit clarithromycin and other antibiotics, according to 1 theory.1 Thus, clarithromycin and an imidazole are more effective in the second phase of treatment.1
Should US physicians adopt the Italian protocol and prescribe tinidazole? Would metronidazole or other imidazoles be equally effective?
FIGURE
Sequential vs standard therapy: A comparison
STUDY SUMMARY: Sequential therapy is better on all counts
This meta-analysis found 9 randomized controlled trials (RCTs) that compared H pylori eradication rates with standard 7- to 10-day triple-drug therapy to 10-day sequential therapy; an additional small study used a 5-day triple-drug comparison group. The authors performed a thorough search and used standard meta-analysis methods for data synthesis and analysis. The patients were all H pylori treatment naïve and had not used PPIs, histamine-2 receptor antagonists, or antibiotics in the month preceding the study. All patients (n=2747) had documented H pylori infection based on fecal antigen test, histologic evaluation, biopsy urease test, or urea breath test.
All the trials were conducted in Italy, although 2 of the studies included patients from the United States. Nine RCTs compared a triple-therapy regimen with PPI to sequential therapy, 1 RCT compared a triple-drug regimen with ranitidine to sequential therapy, and 1 included only pediatric patients. Pooled eradication rates were 93.4% (95% confidence interval [CI,] 91.3%-95.5%) for sequential therapy and 76.9% (CI, 71.0%-82.8%) for standard therapy, with a relative risk reduction of 71% (CI, 64%-77%).1 The authors estimated that for every 6.3 patients (95% CI, 5.2-7.1) treated with sequential therapy, there would be 1 additional cure compared to standard therapy. Standard 7- to 10-day triple therapy remained inferior to sequential therapy in all subgroup analyses, including patients with risk factors for eradication failure.
Adherence rates were similar in both groups. Sequential therapy resulted in a median adherence rate of 97.4% (range, 90.0%-98.9%), with standard therapy at 96.8% (range, 93.0%-100%).1 Reported side effects were also similar in both treatment groups.1
WHAT’S NEW?: This meta-analysis reduces doubt
The latest American College of Gastroenterology guidelines on the management of H pylori infection acknowledge that sequential therapy has shown promise in Europe, but the organization has not supported a change from the standard regimen to sequential therapy as first-line treatment. The standard triple-therapy regimen is approved by the US Food and Drug Administration, and is the most commonly used H pylori treatment in the United States.1 This is the first meta-analysis based solely on RCTs, and it clearly demonstrates that sequential therapy increased eradication rates.
Helicobacter pylori (called H pylori for short) is a type of bacteria that can cause an ulcer (sore) to develop within the lining of your stomach and intestines. Ulcers can cause pain and bleeding, so it is important to get rid of this bacteria. To do this, you will need to take 4 different medicines over the next 10 days. They must be taken in a certain order, exactly as your doctor has prescribed.
One of the drugs you will be taking (for the entire 10-day period) is a proton pump inhibitor (called a PPI), a medicine that helps reduce the amount of acid in your stomach. ______________ is the name of the PPI your doctor has ordered. Take it twice a day, once in the morning and once in the evening, for 10 days.
You will also take 3 different kinds of antibiotics to eliminate the H pylori bacteria. For the first 5 days, you will take amoxicillin twice a day (2 pills in the morning and 2 in the evening), along with the PPI.
After 5 days, all the amoxicillin pills should be gone, and you will switch to 2 other antibiotics: clarithromycin AND ______________. For the next 5 days, you will take 1 PPI plus 1 clarithromycin and 1 ______________ every morning AND every night.
These medications may cause nausea, diarrhea, and a bad taste in your mouth. These side effects are usually not serious, but if they bother you so much that you cannot continue to take the medicine, it is important to call our office right away.
To remember to take each of the medicines in the morning AND evening on the correct day, use this chart to follow along. Put a check mark in the morning box or the evening box every time you take your medicine.
CAVEATS: Drug resistance, previous Tx could skew results
This meta-analysis only included studies performed in Italy, although 2 of the trials did include US recruits. Drug resistance patterns may be different in this country, which could alter sequential therapy’s eradication rates.
Because 3 antibiotics are used in sequential therapy, we may have fewer remaining options for patients who do not respond to this regimen, and we do not have information about patients with previous treatment failures. In addition, this meta-analysis only evaluated H pylori eradication rates in treatment-naïve patients, so we have no information about the effectiveness of this regimen in patients with previous treatment failures.
Would other sequential regimens—or drugs—work?
Patients who are allergic to amoxicillin would not be candidates for this sequential therapy protocol. While sequential therapy was compared with 7- to 10-day standard triple therapy, this study did not compare it with other regimens—eg, quadruple therapy or a 14-day course of standard triple-drug therapy.
Other drugs may also affect outcomes. The sequential therapy studies all used tinidazole, a relatively new agent in the United States; we don’t know whether metronidazole or other imidazoles are as effective.
The authors of this meta-analysis also noted the possibility of publication bias, but we doubt that there are enough unpublished data to invalidate the findings. Also, the selected RCTs only addressed eradication rates and not patient-oriented outcomes. However, most patient-oriented outcomes, including cancer and ulcers, can take years, even decades, to develop.
CHALLENGES TO IMPLEMENTATION: Sequential therapy may be confusing
While adherence rates were similar in the standard and sequential treatment groups in the meta-analysis, sequential therapy—which requires switching medications midway through treatment—might be more confusing for patients in actual practice. This has the potential to negatively affect adherence to the sequential regimen.
It will be important for physicians who prescribe sequential therapy to counsel patients on the importance of completing the treatment regimen exactly as prescribed and to provide clear instructions for doing so, ideally in the form of a patient handout like the one on page 653. Cost is not a problem; the price of sequential therapy is about equal to, or possibly less than, that of standard therapy.5
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Prescribe sequential therapy rather than the standard (concurrent) therapy to improve H pylori eradication rates, particularly in treatment-naïve patients.1
Strength of recommendation
B: Based on a well-done meta-analysis with disease-oriented outcomes
Jafri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Ann Intern Med. 2008;148:923-931.
ILLUSTRATIVE CASE
A 40-year-old woman with a peptic ulcer has been diagnosed with Helicobacter pylori infection, and schedules a visit to discuss treatment. You’re aware of the declining eradication rates associated with standard therapy, and have heard that sequential therapy may be a more effective option. Should you offer it to this patient?
An estimated 30% to 40% of the US population is infected with H pylori,2 a bacterium that plays a crucial role in the pathogenesis of peptic ulcer disease, chronic gastritis, and gastric cancer.1 The triple-drug regimen (a proton-pump inhibitor [PPI] and clarithromycin with amoxicillin, tinidazole, or another imidazole) is commonly used to treat H pylori in Europe and in the United States.3 Yet the eradication rate associated with this standard 3-drug regimen in this country is <80%, and appears to be on the decline. The likely problem: the increase in antibiotic-resistant strains of H pylori.2
Put amoxicillin first
In Italy, eradication rates of >90% have been reported with a sequential therapy: a PPI and amoxicillin for 5 days, followed by the PPI, clarithromycin, and tinidazole for an additional 5 days (FIGURE).4 (Because tinidazole is a relatively new drug in the United States and physicians may use other drugs in its class instead, we refer to the drug class—imidazoles—rather than a specific medication in the FIGURE and much of the text that follows.) Using amoxicillin before the other antibiotics weakens bacterial cell walls, preventing the formation of drug efflux channels that can inhibit clarithromycin and other antibiotics, according to 1 theory.1 Thus, clarithromycin and an imidazole are more effective in the second phase of treatment.1
Should US physicians adopt the Italian protocol and prescribe tinidazole? Would metronidazole or other imidazoles be equally effective?
FIGURE
Sequential vs standard therapy: A comparison
STUDY SUMMARY: Sequential therapy is better on all counts
This meta-analysis found 9 randomized controlled trials (RCTs) that compared H pylori eradication rates with standard 7- to 10-day triple-drug therapy to 10-day sequential therapy; an additional small study used a 5-day triple-drug comparison group. The authors performed a thorough search and used standard meta-analysis methods for data synthesis and analysis. The patients were all H pylori treatment naïve and had not used PPIs, histamine-2 receptor antagonists, or antibiotics in the month preceding the study. All patients (n=2747) had documented H pylori infection based on fecal antigen test, histologic evaluation, biopsy urease test, or urea breath test.
All the trials were conducted in Italy, although 2 of the studies included patients from the United States. Nine RCTs compared a triple-therapy regimen with PPI to sequential therapy, 1 RCT compared a triple-drug regimen with ranitidine to sequential therapy, and 1 included only pediatric patients. Pooled eradication rates were 93.4% (95% confidence interval [CI,] 91.3%-95.5%) for sequential therapy and 76.9% (CI, 71.0%-82.8%) for standard therapy, with a relative risk reduction of 71% (CI, 64%-77%).1 The authors estimated that for every 6.3 patients (95% CI, 5.2-7.1) treated with sequential therapy, there would be 1 additional cure compared to standard therapy. Standard 7- to 10-day triple therapy remained inferior to sequential therapy in all subgroup analyses, including patients with risk factors for eradication failure.
Adherence rates were similar in both groups. Sequential therapy resulted in a median adherence rate of 97.4% (range, 90.0%-98.9%), with standard therapy at 96.8% (range, 93.0%-100%).1 Reported side effects were also similar in both treatment groups.1
WHAT’S NEW?: This meta-analysis reduces doubt
The latest American College of Gastroenterology guidelines on the management of H pylori infection acknowledge that sequential therapy has shown promise in Europe, but the organization has not supported a change from the standard regimen to sequential therapy as first-line treatment. The standard triple-therapy regimen is approved by the US Food and Drug Administration, and is the most commonly used H pylori treatment in the United States.1 This is the first meta-analysis based solely on RCTs, and it clearly demonstrates that sequential therapy increased eradication rates.
Helicobacter pylori (called H pylori for short) is a type of bacteria that can cause an ulcer (sore) to develop within the lining of your stomach and intestines. Ulcers can cause pain and bleeding, so it is important to get rid of this bacteria. To do this, you will need to take 4 different medicines over the next 10 days. They must be taken in a certain order, exactly as your doctor has prescribed.
One of the drugs you will be taking (for the entire 10-day period) is a proton pump inhibitor (called a PPI), a medicine that helps reduce the amount of acid in your stomach. ______________ is the name of the PPI your doctor has ordered. Take it twice a day, once in the morning and once in the evening, for 10 days.
You will also take 3 different kinds of antibiotics to eliminate the H pylori bacteria. For the first 5 days, you will take amoxicillin twice a day (2 pills in the morning and 2 in the evening), along with the PPI.
After 5 days, all the amoxicillin pills should be gone, and you will switch to 2 other antibiotics: clarithromycin AND ______________. For the next 5 days, you will take 1 PPI plus 1 clarithromycin and 1 ______________ every morning AND every night.
These medications may cause nausea, diarrhea, and a bad taste in your mouth. These side effects are usually not serious, but if they bother you so much that you cannot continue to take the medicine, it is important to call our office right away.
To remember to take each of the medicines in the morning AND evening on the correct day, use this chart to follow along. Put a check mark in the morning box or the evening box every time you take your medicine.
CAVEATS: Drug resistance, previous Tx could skew results
This meta-analysis only included studies performed in Italy, although 2 of the trials did include US recruits. Drug resistance patterns may be different in this country, which could alter sequential therapy’s eradication rates.
Because 3 antibiotics are used in sequential therapy, we may have fewer remaining options for patients who do not respond to this regimen, and we do not have information about patients with previous treatment failures. In addition, this meta-analysis only evaluated H pylori eradication rates in treatment-naïve patients, so we have no information about the effectiveness of this regimen in patients with previous treatment failures.
Would other sequential regimens—or drugs—work?
Patients who are allergic to amoxicillin would not be candidates for this sequential therapy protocol. While sequential therapy was compared with 7- to 10-day standard triple therapy, this study did not compare it with other regimens—eg, quadruple therapy or a 14-day course of standard triple-drug therapy.
Other drugs may also affect outcomes. The sequential therapy studies all used tinidazole, a relatively new agent in the United States; we don’t know whether metronidazole or other imidazoles are as effective.
The authors of this meta-analysis also noted the possibility of publication bias, but we doubt that there are enough unpublished data to invalidate the findings. Also, the selected RCTs only addressed eradication rates and not patient-oriented outcomes. However, most patient-oriented outcomes, including cancer and ulcers, can take years, even decades, to develop.
CHALLENGES TO IMPLEMENTATION: Sequential therapy may be confusing
While adherence rates were similar in the standard and sequential treatment groups in the meta-analysis, sequential therapy—which requires switching medications midway through treatment—might be more confusing for patients in actual practice. This has the potential to negatively affect adherence to the sequential regimen.
It will be important for physicians who prescribe sequential therapy to counsel patients on the importance of completing the treatment regimen exactly as prescribed and to provide clear instructions for doing so, ideally in the form of a patient handout like the one on page 653. Cost is not a problem; the price of sequential therapy is about equal to, or possibly less than, that of standard therapy.5
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Jafri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Ann Intern Med. 2008;148:923-931.
2. Chey WD, Wong BC. American College of Gastroenterology guideline on the management of Helicobacter pylori infection. Am J Gastroenterol. 2007;102:1808-1825.
3. Malfertheiner P, Megraud F, O’Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 2007;56:772-781.
4. Zullo A, De FV, Hassan C, Morini S, Vaira D. The sequential therapy regimen for Helicobacter pylori eradication: a pooled-data analysis. Gut. 2007;56:1353-1357.
5. Vaira D, Zullo A, Vakil N, et al. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: a randomized trial. Ann Intern Med. 2007;146:556-563.
PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Jafri NS, Hornung CA, Howden CW. Meta-analysis: sequential therapy appears superior to standard therapy for Helicobacter pylori infection in patients naive to treatment. Ann Intern Med. 2008;148:923-931.
2. Chey WD, Wong BC. American College of Gastroenterology guideline on the management of Helicobacter pylori infection. Am J Gastroenterol. 2007;102:1808-1825.
3. Malfertheiner P, Megraud F, O’Morain C, et al. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut. 2007;56:772-781.
4. Zullo A, De FV, Hassan C, Morini S, Vaira D. The sequential therapy regimen for Helicobacter pylori eradication: a pooled-data analysis. Gut. 2007;56:1353-1357.
5. Vaira D, Zullo A, Vakil N, et al. Sequential therapy versus standard triple-drug therapy for Helicobacter pylori eradication: a randomized trial. Ann Intern Med. 2007;146:556-563.
PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Help smokers quit: Tell them their “lung age”
ILLUSTRATIVE CASE
A 48-year-old man comes to your office for a routine physical. He has a 30 pack-year smoking history. When you talk to him about smoking cessation, he tells you he’s tried to stop more than once, but he can’t seem to stay motivated. You find no evidence of chronic lung disease and do not perform spirometry screening. (The US Preventive Services Task Force does not recommend spirometry for asymptomatic patients.) But could spirometry have therapeutic value in this case?
Smoking is the leading modifiable risk factor for mortality in the United States,2 and smoking cessation is the most effective intervention. Nortriptyline, bupropion, nicotine replacement agents, and varenicline are effective pharmacological treatments.3 Adding counseling to medication significantly improves quit rates (estimated odds ratio [OR]=1.4; 95% confidence interval [CI], 1.2-1.6).3 Nonetheless, physicians’ efforts to help patients stop smoking frequently fail.
But another option has caught—and held—the attention of researchers.
The promise of biomarkers
It has long been suspected that presenting smokers with evidence of tobacco’s harmful effect on their bodies—biomarkers—might encourage them to stop. Biomarkers that have been tested in randomized controlled trials (RCTs) include spirometry, exhaled carbon monoxide measurement, ultrasonography of carotid and femoral arteries, and genetic susceptibility to lung cancer, as well as combinations of these markers. But the results of most biomarker studies have been disappointing. A 2005 Cochrane Database review found insufficient evidence of the effectiveness of these markers in boosting quit rates.4
Lung age, a biomarker that’s easily understood
Lung age, a clever presentation of spirometry results, had not been tested in an RCT prior to the study we summarize below. Defined in 1985, lung age refers to the average age of a nonsmoker with a forced expiratory volume at 1 second (FEV1) equal to that of the person being tested ( FIGURE 1 ). The primary purpose was to make spirometry results easier for patients to understand, but researchers also envisioned it as a way to demonstrate the premature lung damage suffered as a consequence of smoking.5
FIGURE 1
Translating FEV1 into lung age1
![]()
STUDY SUMMARY: Graphic display more effective than FEV1 results
This study was a well-done, multicenter RCT evaluating the effect on tobacco quit rates of informing adult smokers of their lung age.1 Smokers ages 35 and older from 5 general practices in England were invited to participate. The authors excluded patients using oxygen and those with a history of tuberculosis, lung cancer, asbestosis, bronchiectasis, silicosis, or pneumonectomy. The study included 561 participants with an average of 33 pack-years of smoking, who underwent spirometry before being divided into an intervention or a control group. The researchers used standardized instruments to confirm the baseline comparability of the 2 groups.
Subjects in both groups were given information about local smoking cessation clinics and strongly encouraged to quit. All were told that their lung function would be retested in 12 months.
The controls received letters with their spirometry results presented as FEV1. In contrast, participants in the intervention group received the results in the form of a computer-generated graphic display of lung age ( FIGURE 2 ), which was further explained by a health care worker. They also received a letter within 1 month containing the same data. Participants were evaluated for smoking cessation at 12 months, and those who reported quitting received confirmatory carbon monoxide breath testing and salivary cotinine testing. Eleven percent of the subjects were lost to follow-up.
FIGURE 2
Lung age helps spirometry pack a bigger punch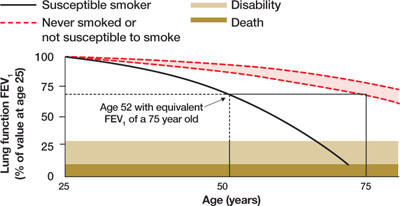
Drawing a vertical line from the patient’s age (on the horizontal axis) to reach the solid curve representing the lung function of the “susceptible smoker” and extending the line horizontally to reach the curve with the broken lines representing “never smokers” graphically shows the patient’s lung age and the accelerated decline in lung function associated with smoking. The patient shown here is a 52-year-old smoker with FEV1 equivalent to a 75-year-old nonsmoker.
Source: Parkes G et al. BMJ. 2008;336:598-600. Reproduced with permission from the BMJ Publishing Group.
Quit rates higher when patients know lung age
At 1 year, verified quit rates were 13.6% in the intervention group and 6.4% in the control group (a difference of 7.2%, 95% CI, 2.2%-12.1%; P=.005). This means that for every 14 smokers who are told their lung age and shown a graphic display of this biomarker, 1 additional smoker will quit after 1 year.
Contrary to what might be expected, the investigators found that quitting did not depend on the degree of lung damage. Patients with both normal and abnormal lung age quit smoking at similar rates.
WHAT’S NEW: Lung age resonates more than spirometry alone
This is the first RCT demonstrating that informing smokers of their lung age can help them quit, and the first well-designed study to demonstrate improved cessation rates using a physiological biomarker. The research also suggests that successful quitting may have less to do with spirometry results—the level of severity of lung damage it shows—than with the way the results are presented. Giving patients information about their lung function in an easily understandable format, the authors observe, appears to result in higher quit rates.
CAVEATS: Young smokers weren’t studied
The study did not test to see if this intervention would work in younger adults, as only those 35 years of age and older were enrolled. This is a single study, and it is possible that the findings cannot be generalized to other groups or are due to unmeasured confounding factors. However, the intervention is unlikely to cause any significant harm, so we see no risks associated with it other than the cost of spirometry.
CHALLENGES TO IMPLEMENTATION: Time and expense of spirometry
We suspect the biggest challenges to implementing this recommendation in clinical practice are the expense of obtaining a spirometer ( TABLE ), staff training for those practices without one, and the time needed for the intervention. The average time to perform spirometry on study participants was 30 minutes; a health care worker spent, on average, another 15 minutes reviewing results with each member of the intervention group.
Another challenge: Not all spirometers calculate lung age or can create a graphic similar to FIGURE 2 . However, any FEV1 measurement, whether it is generated by formal pulmonary function testing or by an inexpensive hand-held meter, can easily be converted to lung age using the formula shown in FIGURE 1 . If desired, the same elements—the patient’s age, height, and gender as well as FEV1—could also be used to create a computer-generated graphic display.
TABLE
Spirometry: equipment costs
| The initial cost of a spirometer varies widely, depending on the sophistication of the equipment and the available options and features. Additional costs—for disposable mouthpieces, line filters, nose clips, and hoses, for example—are low. A sampling of reasonably priced models well suited for office use is shown below. All of these models meet American Thoracic Society criteria for spirometry, and all calculate lung age. | ||
|---|---|---|
| SPIROMETER MANUFACTURER/MODEL | PRICE | SUPPLIER |
| Futuremed Discovery-2 | $2,125 | medsupplier.com |
| Micro Medical MicroLoop | $1,780 | Miami-med.com |
| Micro Medical SpiroUSB | $1,580 | Miami-med.com |
| NDD EasyOne Frontline | $1,000 | medsupplier.com |
| SDI Diagnostics Spirolab II | $2,600 | med-electronics.com |
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336:598-600.
2. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291:1238-1245.
3. Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical practice guideline. Rockville, MD: US Department of Health and Human Services, Public Health Service; May 2008. Available at: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use08.pdf. Accessed July 6, 2008.
4. Bize R, Burnand B, Mueller Y, Cornuz J. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2005;(4):CD004705.-
5. Morris JF, Temple W. Spirometric “lung age” estimation for motivating smoking cessation. Prev Med. 1985;14:655-662.
ILLUSTRATIVE CASE
A 48-year-old man comes to your office for a routine physical. He has a 30 pack-year smoking history. When you talk to him about smoking cessation, he tells you he’s tried to stop more than once, but he can’t seem to stay motivated. You find no evidence of chronic lung disease and do not perform spirometry screening. (The US Preventive Services Task Force does not recommend spirometry for asymptomatic patients.) But could spirometry have therapeutic value in this case?
Smoking is the leading modifiable risk factor for mortality in the United States,2 and smoking cessation is the most effective intervention. Nortriptyline, bupropion, nicotine replacement agents, and varenicline are effective pharmacological treatments.3 Adding counseling to medication significantly improves quit rates (estimated odds ratio [OR]=1.4; 95% confidence interval [CI], 1.2-1.6).3 Nonetheless, physicians’ efforts to help patients stop smoking frequently fail.
But another option has caught—and held—the attention of researchers.
The promise of biomarkers
It has long been suspected that presenting smokers with evidence of tobacco’s harmful effect on their bodies—biomarkers—might encourage them to stop. Biomarkers that have been tested in randomized controlled trials (RCTs) include spirometry, exhaled carbon monoxide measurement, ultrasonography of carotid and femoral arteries, and genetic susceptibility to lung cancer, as well as combinations of these markers. But the results of most biomarker studies have been disappointing. A 2005 Cochrane Database review found insufficient evidence of the effectiveness of these markers in boosting quit rates.4
Lung age, a biomarker that’s easily understood
Lung age, a clever presentation of spirometry results, had not been tested in an RCT prior to the study we summarize below. Defined in 1985, lung age refers to the average age of a nonsmoker with a forced expiratory volume at 1 second (FEV1) equal to that of the person being tested ( FIGURE 1 ). The primary purpose was to make spirometry results easier for patients to understand, but researchers also envisioned it as a way to demonstrate the premature lung damage suffered as a consequence of smoking.5
FIGURE 1
Translating FEV1 into lung age1
![]()
STUDY SUMMARY: Graphic display more effective than FEV1 results
This study was a well-done, multicenter RCT evaluating the effect on tobacco quit rates of informing adult smokers of their lung age.1 Smokers ages 35 and older from 5 general practices in England were invited to participate. The authors excluded patients using oxygen and those with a history of tuberculosis, lung cancer, asbestosis, bronchiectasis, silicosis, or pneumonectomy. The study included 561 participants with an average of 33 pack-years of smoking, who underwent spirometry before being divided into an intervention or a control group. The researchers used standardized instruments to confirm the baseline comparability of the 2 groups.
Subjects in both groups were given information about local smoking cessation clinics and strongly encouraged to quit. All were told that their lung function would be retested in 12 months.
The controls received letters with their spirometry results presented as FEV1. In contrast, participants in the intervention group received the results in the form of a computer-generated graphic display of lung age ( FIGURE 2 ), which was further explained by a health care worker. They also received a letter within 1 month containing the same data. Participants were evaluated for smoking cessation at 12 months, and those who reported quitting received confirmatory carbon monoxide breath testing and salivary cotinine testing. Eleven percent of the subjects were lost to follow-up.
FIGURE 2
Lung age helps spirometry pack a bigger punch
Drawing a vertical line from the patient’s age (on the horizontal axis) to reach the solid curve representing the lung function of the “susceptible smoker” and extending the line horizontally to reach the curve with the broken lines representing “never smokers” graphically shows the patient’s lung age and the accelerated decline in lung function associated with smoking. The patient shown here is a 52-year-old smoker with FEV1 equivalent to a 75-year-old nonsmoker.
Source: Parkes G et al. BMJ. 2008;336:598-600. Reproduced with permission from the BMJ Publishing Group.
Quit rates higher when patients know lung age
At 1 year, verified quit rates were 13.6% in the intervention group and 6.4% in the control group (a difference of 7.2%, 95% CI, 2.2%-12.1%; P=.005). This means that for every 14 smokers who are told their lung age and shown a graphic display of this biomarker, 1 additional smoker will quit after 1 year.
Contrary to what might be expected, the investigators found that quitting did not depend on the degree of lung damage. Patients with both normal and abnormal lung age quit smoking at similar rates.
WHAT’S NEW: Lung age resonates more than spirometry alone
This is the first RCT demonstrating that informing smokers of their lung age can help them quit, and the first well-designed study to demonstrate improved cessation rates using a physiological biomarker. The research also suggests that successful quitting may have less to do with spirometry results—the level of severity of lung damage it shows—than with the way the results are presented. Giving patients information about their lung function in an easily understandable format, the authors observe, appears to result in higher quit rates.
CAVEATS: Young smokers weren’t studied
The study did not test to see if this intervention would work in younger adults, as only those 35 years of age and older were enrolled. This is a single study, and it is possible that the findings cannot be generalized to other groups or are due to unmeasured confounding factors. However, the intervention is unlikely to cause any significant harm, so we see no risks associated with it other than the cost of spirometry.
CHALLENGES TO IMPLEMENTATION: Time and expense of spirometry
We suspect the biggest challenges to implementing this recommendation in clinical practice are the expense of obtaining a spirometer ( TABLE ), staff training for those practices without one, and the time needed for the intervention. The average time to perform spirometry on study participants was 30 minutes; a health care worker spent, on average, another 15 minutes reviewing results with each member of the intervention group.
Another challenge: Not all spirometers calculate lung age or can create a graphic similar to FIGURE 2 . However, any FEV1 measurement, whether it is generated by formal pulmonary function testing or by an inexpensive hand-held meter, can easily be converted to lung age using the formula shown in FIGURE 1 . If desired, the same elements—the patient’s age, height, and gender as well as FEV1—could also be used to create a computer-generated graphic display.
TABLE
Spirometry: equipment costs
| The initial cost of a spirometer varies widely, depending on the sophistication of the equipment and the available options and features. Additional costs—for disposable mouthpieces, line filters, nose clips, and hoses, for example—are low. A sampling of reasonably priced models well suited for office use is shown below. All of these models meet American Thoracic Society criteria for spirometry, and all calculate lung age. | ||
|---|---|---|
| SPIROMETER MANUFACTURER/MODEL | PRICE | SUPPLIER |
| Futuremed Discovery-2 | $2,125 | medsupplier.com |
| Micro Medical MicroLoop | $1,780 | Miami-med.com |
| Micro Medical SpiroUSB | $1,580 | Miami-med.com |
| NDD EasyOne Frontline | $1,000 | medsupplier.com |
| SDI Diagnostics Spirolab II | $2,600 | med-electronics.com |
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
ILLUSTRATIVE CASE
A 48-year-old man comes to your office for a routine physical. He has a 30 pack-year smoking history. When you talk to him about smoking cessation, he tells you he’s tried to stop more than once, but he can’t seem to stay motivated. You find no evidence of chronic lung disease and do not perform spirometry screening. (The US Preventive Services Task Force does not recommend spirometry for asymptomatic patients.) But could spirometry have therapeutic value in this case?
Smoking is the leading modifiable risk factor for mortality in the United States,2 and smoking cessation is the most effective intervention. Nortriptyline, bupropion, nicotine replacement agents, and varenicline are effective pharmacological treatments.3 Adding counseling to medication significantly improves quit rates (estimated odds ratio [OR]=1.4; 95% confidence interval [CI], 1.2-1.6).3 Nonetheless, physicians’ efforts to help patients stop smoking frequently fail.
But another option has caught—and held—the attention of researchers.
The promise of biomarkers
It has long been suspected that presenting smokers with evidence of tobacco’s harmful effect on their bodies—biomarkers—might encourage them to stop. Biomarkers that have been tested in randomized controlled trials (RCTs) include spirometry, exhaled carbon monoxide measurement, ultrasonography of carotid and femoral arteries, and genetic susceptibility to lung cancer, as well as combinations of these markers. But the results of most biomarker studies have been disappointing. A 2005 Cochrane Database review found insufficient evidence of the effectiveness of these markers in boosting quit rates.4
Lung age, a biomarker that’s easily understood
Lung age, a clever presentation of spirometry results, had not been tested in an RCT prior to the study we summarize below. Defined in 1985, lung age refers to the average age of a nonsmoker with a forced expiratory volume at 1 second (FEV1) equal to that of the person being tested ( FIGURE 1 ). The primary purpose was to make spirometry results easier for patients to understand, but researchers also envisioned it as a way to demonstrate the premature lung damage suffered as a consequence of smoking.5
FIGURE 1
Translating FEV1 into lung age1
![]()
STUDY SUMMARY: Graphic display more effective than FEV1 results
This study was a well-done, multicenter RCT evaluating the effect on tobacco quit rates of informing adult smokers of their lung age.1 Smokers ages 35 and older from 5 general practices in England were invited to participate. The authors excluded patients using oxygen and those with a history of tuberculosis, lung cancer, asbestosis, bronchiectasis, silicosis, or pneumonectomy. The study included 561 participants with an average of 33 pack-years of smoking, who underwent spirometry before being divided into an intervention or a control group. The researchers used standardized instruments to confirm the baseline comparability of the 2 groups.
Subjects in both groups were given information about local smoking cessation clinics and strongly encouraged to quit. All were told that their lung function would be retested in 12 months.
The controls received letters with their spirometry results presented as FEV1. In contrast, participants in the intervention group received the results in the form of a computer-generated graphic display of lung age ( FIGURE 2 ), which was further explained by a health care worker. They also received a letter within 1 month containing the same data. Participants were evaluated for smoking cessation at 12 months, and those who reported quitting received confirmatory carbon monoxide breath testing and salivary cotinine testing. Eleven percent of the subjects were lost to follow-up.
FIGURE 2
Lung age helps spirometry pack a bigger punch
Drawing a vertical line from the patient’s age (on the horizontal axis) to reach the solid curve representing the lung function of the “susceptible smoker” and extending the line horizontally to reach the curve with the broken lines representing “never smokers” graphically shows the patient’s lung age and the accelerated decline in lung function associated with smoking. The patient shown here is a 52-year-old smoker with FEV1 equivalent to a 75-year-old nonsmoker.
Source: Parkes G et al. BMJ. 2008;336:598-600. Reproduced with permission from the BMJ Publishing Group.
Quit rates higher when patients know lung age
At 1 year, verified quit rates were 13.6% in the intervention group and 6.4% in the control group (a difference of 7.2%, 95% CI, 2.2%-12.1%; P=.005). This means that for every 14 smokers who are told their lung age and shown a graphic display of this biomarker, 1 additional smoker will quit after 1 year.
Contrary to what might be expected, the investigators found that quitting did not depend on the degree of lung damage. Patients with both normal and abnormal lung age quit smoking at similar rates.
WHAT’S NEW: Lung age resonates more than spirometry alone
This is the first RCT demonstrating that informing smokers of their lung age can help them quit, and the first well-designed study to demonstrate improved cessation rates using a physiological biomarker. The research also suggests that successful quitting may have less to do with spirometry results—the level of severity of lung damage it shows—than with the way the results are presented. Giving patients information about their lung function in an easily understandable format, the authors observe, appears to result in higher quit rates.
CAVEATS: Young smokers weren’t studied
The study did not test to see if this intervention would work in younger adults, as only those 35 years of age and older were enrolled. This is a single study, and it is possible that the findings cannot be generalized to other groups or are due to unmeasured confounding factors. However, the intervention is unlikely to cause any significant harm, so we see no risks associated with it other than the cost of spirometry.
CHALLENGES TO IMPLEMENTATION: Time and expense of spirometry
We suspect the biggest challenges to implementing this recommendation in clinical practice are the expense of obtaining a spirometer ( TABLE ), staff training for those practices without one, and the time needed for the intervention. The average time to perform spirometry on study participants was 30 minutes; a health care worker spent, on average, another 15 minutes reviewing results with each member of the intervention group.
Another challenge: Not all spirometers calculate lung age or can create a graphic similar to FIGURE 2 . However, any FEV1 measurement, whether it is generated by formal pulmonary function testing or by an inexpensive hand-held meter, can easily be converted to lung age using the formula shown in FIGURE 1 . If desired, the same elements—the patient’s age, height, and gender as well as FEV1—could also be used to create a computer-generated graphic display.
TABLE
Spirometry: equipment costs
| The initial cost of a spirometer varies widely, depending on the sophistication of the equipment and the available options and features. Additional costs—for disposable mouthpieces, line filters, nose clips, and hoses, for example—are low. A sampling of reasonably priced models well suited for office use is shown below. All of these models meet American Thoracic Society criteria for spirometry, and all calculate lung age. | ||
|---|---|---|
| SPIROMETER MANUFACTURER/MODEL | PRICE | SUPPLIER |
| Futuremed Discovery-2 | $2,125 | medsupplier.com |
| Micro Medical MicroLoop | $1,780 | Miami-med.com |
| Micro Medical SpiroUSB | $1,580 | Miami-med.com |
| NDD EasyOne Frontline | $1,000 | medsupplier.com |
| SDI Diagnostics Spirolab II | $2,600 | med-electronics.com |
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
PURL METHODOLOGY
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336:598-600.
2. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291:1238-1245.
3. Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical practice guideline. Rockville, MD: US Department of Health and Human Services, Public Health Service; May 2008. Available at: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use08.pdf. Accessed July 6, 2008.
4. Bize R, Burnand B, Mueller Y, Cornuz J. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2005;(4):CD004705.-
5. Morris JF, Temple W. Spirometric “lung age” estimation for motivating smoking cessation. Prev Med. 1985;14:655-662.
1. Parkes G, Greenhalgh T, Griffin M, Dent R. Effect on smoking quit rate of telling patients their lung age: the Step2quit randomised controlled trial. BMJ. 2008;336:598-600.
2. Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004;291:1238-1245.
3. Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical practice guideline. Rockville, MD: US Department of Health and Human Services, Public Health Service; May 2008. Available at: http://www.surgeongeneral.gov/tobacco/treating_tobacco_use08.pdf. Accessed July 6, 2008.
4. Bize R, Burnand B, Mueller Y, Cornuz J. Biomedical risk assessment as an aid for smoking cessation. Cochrane Database Syst Rev. 2005;(4):CD004705.-
5. Morris JF, Temple W. Spirometric “lung age” estimation for motivating smoking cessation. Prev Med. 1985;14:655-662.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Can metformin undo weight gain induced by antipsychotics?
Lack of evidence for weight loss drugs
The most recent guideline on this topic does not recommend any medication, citing a lack of evidence. In its 2003 consensus statement, a panel representing the American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and the North American Association for the Study of Obesity3 recommends:
- That patients taking second-generation antipsychotics have the following assessments at baseline and regular intervals: weight, height, waist circumference, blood pressure, fasting plasma glucose, and fasting lipids.
- Providing nutrition and exercise counseling to all patients who are over-weight or obese at baseline.
- Initiating treatment with one of the second-generation antipsychotics with a lower risk of weight gain for patients at high risk of diabetes (ie, family history) and for patients who gain 5% or more of their initial weight or develop worsening hyperglycemia or dyslipidemia during treatment.
This guideline does not recommend metformin to reduce weight gain.
A 2007 Cochrane review of interventions to reduce weight gain in patients with schizophrenia included 23 randomized controlled trials of a variety of weight loss interventions, including cognitive/behavioral interventions and a variety of medications, including sibutramine, orlistat, fluoxetine, topiramate, and metformin. The authors highlighted the limited number of studies of short duration and with small sample sizes and concluded that the evidence was insufficient for the use of pharmacologic interventions to prevent or treat weight gain.5
STUDY SUMMARY: Lifestyle changes and metformin compared
This randomized controlled trial was conducted in China and included 128 adults aged 18 to 45 with a first psychotic episode of schizophrenia. All patients had to have gained more than 10% of their pretreatment body weight during the first year of treatment with an antipsychotic medication (clozapine, olanzapine, risperidone, or sulpiride [not approved for use in the United States]). All study participants had to be under the care of an adult caregiver who monitored and recorded food intake, exercise, and medication intake. Patients with diabetes, cardiovascular disease, liver or renal dysfunction, substance abuse, or psychiatric diagnoses other than schizophrenia were excluded.
Patients were randomized to 1 of 4 groups for the 12 weeks of the study:
- Metformin alone, 250 mg 3 times daily
- Placebo alone
- Lifestyle intervention plus metformin
- Lifestyle intervention plus placebo
The lifestyle intervention included 3 components: (1) education: monthly programs on nutrition and physical activity; (2) diet: the American Heart Association step 2 diet (<30% calories from fat, 55% carbohydrates, >15% protein, with at least 15 g fiber per 1000 kcal); and (3) exercise: 1 week of sessions with an exercise physiologist followed by an individualized home-based exercise program.
Primary outcomes included changes in weight, body mass index (BMI), waist circumference, and fasting glucose ( TABLE 2 ). Ten of the 128 randomized patients either discontinued the study or were lost to follow up, but all 128 patients were included in the analysis.
TABLE 2
Mean difference between baseline and endpoint (week 12) of treatment outcomes (95% confidence intervals)1
| LIFESTYLE + METFORMIN | METFORMIN | LIFESTYLE | PLACEBO | |
|---|---|---|---|---|
| Weight, kg | -4.7 (-5.7 to -3.4) | -3.2 (-3.9 to -2.5) | -1.4 (-2.0 to -0.7) | 3.1 (2.4 to 3.8) |
| BMI, kg/m2 | -1.8 (-2.3 to -1.3) | -1.2 (-1.5 to -0.9) | -0.5 (-0.8 to -0.3) | 1.2 (0.9 to 1.5) |
| Waist circumference, cm | -2.0 (-2.4 to -1.5) | -1.3 (-1.5 to -1.1) | 0.1 (-0.5 to 0.7) | 2.2 (1.7 to 2.8) |
| Fasting glucose, mg/dL | -7.2 (-10.8 to -5.4) | -10.8 (-16.2 to -7.2) | -7.2 (-9.0 to -3.6) | 1.8 (-1.8 to 3.6) |
Best result: Lifestyle changes plus metformin
Compared with baseline, weight decreased by 7.3% in the lifestyle plus metformin group, by 4.9% in the metformin-only group, and by 2.2% in the lifestyle-only group; in the placebo group, weight increased by 4.8%.
Participants in all 3 intervention groups also showed significant decreases in the mean fasting glucose, insulin levels, and insulin resistance index (IRI). The insulin levels and the IRI increased in the placebo group.
No significant differences in adverse effects were noted among the 4 treatment groups.1
WHAT’S NEW: Convincing evidence
This is the first randomized controlled trial to show convincingly that metformin alone or in combination with lifestyle changes is superior to lifestyle changes alone or placebo for reducing weight gain and other adverse metabolic outcomes induced by second-generation antipsychotics.
Intensive lifestyle interventions
Prior studies found that intensive lifestyle interventions can help reduce antipsychotic-related weight gain. A 3-month randomized controlled trial compared an early behavioral intervention (dietary counseling, an exercise program, and behavior therapy) with routine care in 61 patients with first-episode psychosis who were taking risperidone, olanzapine, or haloperidol;6 significantly fewer patients assigned to behavioral intervention had an increased initial body weight of more than 7%: 39% in the behavioral intervention group vs 79% in the routine care group (P<.002).
Small samples, small effect sizes
Past studies of metformin for antipsychotic-associated weight gain have generally shown a small benefit, though small sample sizes and small effect sizes prohibited definitive conclusions. Unlike the study by Wu and colleagues,1 none of these past studies were designed to compare the combination of metformin and lifestyle intervention with metformin alone, lifestyle intervention alone, or placebo alone.
Klein et al conducted a randomized placebo-controlled trial of metformin in 39 children ages 10 to 17 whose weight had increased more than 10% on atypical antipsychotic therapy.7 The children treated with placebo gained a mean of 4 kg and increased their mean BMI by 1.12 kg/m2 during 16 weeks of treatment, while those in the metformin group did not gain weight and decreased their mean BMI by 0.43 kg/m2.
Baptista et al randomized 40 in-patients with schizophrenia, who were being switched from conventional antipsychotics to olanzapine, to either metformin (850-1750 mg/d) or placebo. Both groups gained a similar amount of weight after the 14-week study (5.5 vs 6.3 kg, metformin vs placebo). Three patients who started with high fasting glucose had decreases while taking metformin, and 3 patients given placebo developed elevated fasting glucose during the study.8
In another randomized controlled trial of metformin vs placebo in 80 patients who had been taking olanzapine for at least 4 months, Baptista et al found only a small, insignificant difference in weight loss after 12 weeks of treatment (metformin group lost 1.4 kg, placebo group lost 0.18 kg, P=.09). They reported that both groups were highly motivated to lose weight and were compliant with the healthy lifestyle recommendations.9
An adequately powered study
The trial1 highlighted in this PURL had an adequate sample size to compare metformin plus a lifestyle intervention with either treatment alone or placebo. It showed a clinically important effect of metformin both by itself and in conjunction with the lifestyle intervention.
CAVEATS: Consider switching drugs
Before adding metformin to help with weight loss, primary care clinicians should contact the patient’s psychiatrist to discuss the option of switching antipsychotic medications. Switching from a medication with a higher risk for weight gain, such as olanzapine, to one with a lower risk, such as aripiprazole or ziprasidone, can lead to significant weight loss.10
Not an option for some
However, some patients, especially those taking clozapine, may have already tried multiple antipsychotic agents without success, and switching is not an option for them.
Prescribing metformin
CHALLENGES TO IMPLEMENTATION: Adherence
These study participants were under the care of an adult caregiver who monitored and recorded food and medication intake and exercise level. The lifestyle intervention was thorough and structured and this kind of program is often not available to us for our patients. As a consequence, we may not obtain the same results as in this study. However, even the metformin-alone group showed improvements, and if our patients can reliably take their second-generation antipsychotic, they should also be able to take metformin reliably.
Patient resistance
Some patients may resist taking an additional medication to treat the side effects of their antipsychotic medication. Taking the time to educate them about the increased risk of diabetes and cardiovascular disease related to weight gain may help convince them to do so. Warn them about possible gastrointestinal adverse effects of metformin, which tend to lessen or disappear with time.
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Wu R-R, Zhao J-P, Jin H, et al. Lifestyle intervention and metformin for treatment of antipsychotic-induced weight gain: a randomized controlled trial. JAMA. 2008;299:185-193.
2. Rowland K, Schumann SA. Have pedometer, will travel. J Fam Pract. 2008;57:90-93.
3. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
4. Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;68(suppl 1):20-27.
5. Faulkner G, Cohn T, Remington G. Interventions to reduce weight gain in schizophrenia. Cochrane Database Syst Rev. 2007;(1):CD005148.-
6. Alvarez-Jiménez M, González-Blanch C, Vázquez-Barquero JL, et al. Attenuation of antipsychotic-induced weight gain with early behavioral intervention in drug-naïve first-episode psychosis patients: a randomized controlled trial. J Clin Psychiatry. 2006;67:1253-1260.
7. Klein DJ, Cottingham EM, Sorter M, Barton BA, Morrison JA. A randomized, double-blind, placebo-controlled trial of metformin treatment of weight gain associated with initiation of atypical antipsychotic therapy in children and adolescents. Am J Psychiatry. 2006;163:2072-2079.
8. Baptista T, Martínez J, Lacruz A, et al. Metformin for prevention of weight gain and insulin resistance with olanzapine: a double-blind placebo-controlled trial. Can J Psychiatry. 2006;51:192-196.
9. Baptista T, Rangel N, Fernández V, et al. Metformin as an adjunctive treatment to control body weight and metabolic dysfunction during olanzapine administration: a multicentric, double-blind, placebo-controlled trial. Schizophrenia Res. 2007;93:99-108.
10. Weiden PJ. Switching antipsychotics as a treatment strategy for antipsychotic-induced weight gain and dyslipidemia. J Clin Psychiatry. 2007;68(suppl 4):34-39.
Lack of evidence for weight loss drugs
The most recent guideline on this topic does not recommend any medication, citing a lack of evidence. In its 2003 consensus statement, a panel representing the American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and the North American Association for the Study of Obesity3 recommends:
- That patients taking second-generation antipsychotics have the following assessments at baseline and regular intervals: weight, height, waist circumference, blood pressure, fasting plasma glucose, and fasting lipids.
- Providing nutrition and exercise counseling to all patients who are over-weight or obese at baseline.
- Initiating treatment with one of the second-generation antipsychotics with a lower risk of weight gain for patients at high risk of diabetes (ie, family history) and for patients who gain 5% or more of their initial weight or develop worsening hyperglycemia or dyslipidemia during treatment.
This guideline does not recommend metformin to reduce weight gain.
A 2007 Cochrane review of interventions to reduce weight gain in patients with schizophrenia included 23 randomized controlled trials of a variety of weight loss interventions, including cognitive/behavioral interventions and a variety of medications, including sibutramine, orlistat, fluoxetine, topiramate, and metformin. The authors highlighted the limited number of studies of short duration and with small sample sizes and concluded that the evidence was insufficient for the use of pharmacologic interventions to prevent or treat weight gain.5
STUDY SUMMARY: Lifestyle changes and metformin compared
This randomized controlled trial was conducted in China and included 128 adults aged 18 to 45 with a first psychotic episode of schizophrenia. All patients had to have gained more than 10% of their pretreatment body weight during the first year of treatment with an antipsychotic medication (clozapine, olanzapine, risperidone, or sulpiride [not approved for use in the United States]). All study participants had to be under the care of an adult caregiver who monitored and recorded food intake, exercise, and medication intake. Patients with diabetes, cardiovascular disease, liver or renal dysfunction, substance abuse, or psychiatric diagnoses other than schizophrenia were excluded.
Patients were randomized to 1 of 4 groups for the 12 weeks of the study:
- Metformin alone, 250 mg 3 times daily
- Placebo alone
- Lifestyle intervention plus metformin
- Lifestyle intervention plus placebo
The lifestyle intervention included 3 components: (1) education: monthly programs on nutrition and physical activity; (2) diet: the American Heart Association step 2 diet (<30% calories from fat, 55% carbohydrates, >15% protein, with at least 15 g fiber per 1000 kcal); and (3) exercise: 1 week of sessions with an exercise physiologist followed by an individualized home-based exercise program.
Primary outcomes included changes in weight, body mass index (BMI), waist circumference, and fasting glucose ( TABLE 2 ). Ten of the 128 randomized patients either discontinued the study or were lost to follow up, but all 128 patients were included in the analysis.
TABLE 2
Mean difference between baseline and endpoint (week 12) of treatment outcomes (95% confidence intervals)1
| LIFESTYLE + METFORMIN | METFORMIN | LIFESTYLE | PLACEBO | |
|---|---|---|---|---|
| Weight, kg | -4.7 (-5.7 to -3.4) | -3.2 (-3.9 to -2.5) | -1.4 (-2.0 to -0.7) | 3.1 (2.4 to 3.8) |
| BMI, kg/m2 | -1.8 (-2.3 to -1.3) | -1.2 (-1.5 to -0.9) | -0.5 (-0.8 to -0.3) | 1.2 (0.9 to 1.5) |
| Waist circumference, cm | -2.0 (-2.4 to -1.5) | -1.3 (-1.5 to -1.1) | 0.1 (-0.5 to 0.7) | 2.2 (1.7 to 2.8) |
| Fasting glucose, mg/dL | -7.2 (-10.8 to -5.4) | -10.8 (-16.2 to -7.2) | -7.2 (-9.0 to -3.6) | 1.8 (-1.8 to 3.6) |
Best result: Lifestyle changes plus metformin
Compared with baseline, weight decreased by 7.3% in the lifestyle plus metformin group, by 4.9% in the metformin-only group, and by 2.2% in the lifestyle-only group; in the placebo group, weight increased by 4.8%.
Participants in all 3 intervention groups also showed significant decreases in the mean fasting glucose, insulin levels, and insulin resistance index (IRI). The insulin levels and the IRI increased in the placebo group.
No significant differences in adverse effects were noted among the 4 treatment groups.1
WHAT’S NEW: Convincing evidence
This is the first randomized controlled trial to show convincingly that metformin alone or in combination with lifestyle changes is superior to lifestyle changes alone or placebo for reducing weight gain and other adverse metabolic outcomes induced by second-generation antipsychotics.
Intensive lifestyle interventions
Prior studies found that intensive lifestyle interventions can help reduce antipsychotic-related weight gain. A 3-month randomized controlled trial compared an early behavioral intervention (dietary counseling, an exercise program, and behavior therapy) with routine care in 61 patients with first-episode psychosis who were taking risperidone, olanzapine, or haloperidol;6 significantly fewer patients assigned to behavioral intervention had an increased initial body weight of more than 7%: 39% in the behavioral intervention group vs 79% in the routine care group (P<.002).
Small samples, small effect sizes
Past studies of metformin for antipsychotic-associated weight gain have generally shown a small benefit, though small sample sizes and small effect sizes prohibited definitive conclusions. Unlike the study by Wu and colleagues,1 none of these past studies were designed to compare the combination of metformin and lifestyle intervention with metformin alone, lifestyle intervention alone, or placebo alone.
Klein et al conducted a randomized placebo-controlled trial of metformin in 39 children ages 10 to 17 whose weight had increased more than 10% on atypical antipsychotic therapy.7 The children treated with placebo gained a mean of 4 kg and increased their mean BMI by 1.12 kg/m2 during 16 weeks of treatment, while those in the metformin group did not gain weight and decreased their mean BMI by 0.43 kg/m2.
Baptista et al randomized 40 in-patients with schizophrenia, who were being switched from conventional antipsychotics to olanzapine, to either metformin (850-1750 mg/d) or placebo. Both groups gained a similar amount of weight after the 14-week study (5.5 vs 6.3 kg, metformin vs placebo). Three patients who started with high fasting glucose had decreases while taking metformin, and 3 patients given placebo developed elevated fasting glucose during the study.8
In another randomized controlled trial of metformin vs placebo in 80 patients who had been taking olanzapine for at least 4 months, Baptista et al found only a small, insignificant difference in weight loss after 12 weeks of treatment (metformin group lost 1.4 kg, placebo group lost 0.18 kg, P=.09). They reported that both groups were highly motivated to lose weight and were compliant with the healthy lifestyle recommendations.9
An adequately powered study
The trial1 highlighted in this PURL had an adequate sample size to compare metformin plus a lifestyle intervention with either treatment alone or placebo. It showed a clinically important effect of metformin both by itself and in conjunction with the lifestyle intervention.
CAVEATS: Consider switching drugs
Before adding metformin to help with weight loss, primary care clinicians should contact the patient’s psychiatrist to discuss the option of switching antipsychotic medications. Switching from a medication with a higher risk for weight gain, such as olanzapine, to one with a lower risk, such as aripiprazole or ziprasidone, can lead to significant weight loss.10
Not an option for some
However, some patients, especially those taking clozapine, may have already tried multiple antipsychotic agents without success, and switching is not an option for them.
Prescribing metformin
CHALLENGES TO IMPLEMENTATION: Adherence
These study participants were under the care of an adult caregiver who monitored and recorded food and medication intake and exercise level. The lifestyle intervention was thorough and structured and this kind of program is often not available to us for our patients. As a consequence, we may not obtain the same results as in this study. However, even the metformin-alone group showed improvements, and if our patients can reliably take their second-generation antipsychotic, they should also be able to take metformin reliably.
Patient resistance
Some patients may resist taking an additional medication to treat the side effects of their antipsychotic medication. Taking the time to educate them about the increased risk of diabetes and cardiovascular disease related to weight gain may help convince them to do so. Warn them about possible gastrointestinal adverse effects of metformin, which tend to lessen or disappear with time.
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Lack of evidence for weight loss drugs
The most recent guideline on this topic does not recommend any medication, citing a lack of evidence. In its 2003 consensus statement, a panel representing the American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and the North American Association for the Study of Obesity3 recommends:
- That patients taking second-generation antipsychotics have the following assessments at baseline and regular intervals: weight, height, waist circumference, blood pressure, fasting plasma glucose, and fasting lipids.
- Providing nutrition and exercise counseling to all patients who are over-weight or obese at baseline.
- Initiating treatment with one of the second-generation antipsychotics with a lower risk of weight gain for patients at high risk of diabetes (ie, family history) and for patients who gain 5% or more of their initial weight or develop worsening hyperglycemia or dyslipidemia during treatment.
This guideline does not recommend metformin to reduce weight gain.
A 2007 Cochrane review of interventions to reduce weight gain in patients with schizophrenia included 23 randomized controlled trials of a variety of weight loss interventions, including cognitive/behavioral interventions and a variety of medications, including sibutramine, orlistat, fluoxetine, topiramate, and metformin. The authors highlighted the limited number of studies of short duration and with small sample sizes and concluded that the evidence was insufficient for the use of pharmacologic interventions to prevent or treat weight gain.5
STUDY SUMMARY: Lifestyle changes and metformin compared
This randomized controlled trial was conducted in China and included 128 adults aged 18 to 45 with a first psychotic episode of schizophrenia. All patients had to have gained more than 10% of their pretreatment body weight during the first year of treatment with an antipsychotic medication (clozapine, olanzapine, risperidone, or sulpiride [not approved for use in the United States]). All study participants had to be under the care of an adult caregiver who monitored and recorded food intake, exercise, and medication intake. Patients with diabetes, cardiovascular disease, liver or renal dysfunction, substance abuse, or psychiatric diagnoses other than schizophrenia were excluded.
Patients were randomized to 1 of 4 groups for the 12 weeks of the study:
- Metformin alone, 250 mg 3 times daily
- Placebo alone
- Lifestyle intervention plus metformin
- Lifestyle intervention plus placebo
The lifestyle intervention included 3 components: (1) education: monthly programs on nutrition and physical activity; (2) diet: the American Heart Association step 2 diet (<30% calories from fat, 55% carbohydrates, >15% protein, with at least 15 g fiber per 1000 kcal); and (3) exercise: 1 week of sessions with an exercise physiologist followed by an individualized home-based exercise program.
Primary outcomes included changes in weight, body mass index (BMI), waist circumference, and fasting glucose ( TABLE 2 ). Ten of the 128 randomized patients either discontinued the study or were lost to follow up, but all 128 patients were included in the analysis.
TABLE 2
Mean difference between baseline and endpoint (week 12) of treatment outcomes (95% confidence intervals)1
| LIFESTYLE + METFORMIN | METFORMIN | LIFESTYLE | PLACEBO | |
|---|---|---|---|---|
| Weight, kg | -4.7 (-5.7 to -3.4) | -3.2 (-3.9 to -2.5) | -1.4 (-2.0 to -0.7) | 3.1 (2.4 to 3.8) |
| BMI, kg/m2 | -1.8 (-2.3 to -1.3) | -1.2 (-1.5 to -0.9) | -0.5 (-0.8 to -0.3) | 1.2 (0.9 to 1.5) |
| Waist circumference, cm | -2.0 (-2.4 to -1.5) | -1.3 (-1.5 to -1.1) | 0.1 (-0.5 to 0.7) | 2.2 (1.7 to 2.8) |
| Fasting glucose, mg/dL | -7.2 (-10.8 to -5.4) | -10.8 (-16.2 to -7.2) | -7.2 (-9.0 to -3.6) | 1.8 (-1.8 to 3.6) |
Best result: Lifestyle changes plus metformin
Compared with baseline, weight decreased by 7.3% in the lifestyle plus metformin group, by 4.9% in the metformin-only group, and by 2.2% in the lifestyle-only group; in the placebo group, weight increased by 4.8%.
Participants in all 3 intervention groups also showed significant decreases in the mean fasting glucose, insulin levels, and insulin resistance index (IRI). The insulin levels and the IRI increased in the placebo group.
No significant differences in adverse effects were noted among the 4 treatment groups.1
WHAT’S NEW: Convincing evidence
This is the first randomized controlled trial to show convincingly that metformin alone or in combination with lifestyle changes is superior to lifestyle changes alone or placebo for reducing weight gain and other adverse metabolic outcomes induced by second-generation antipsychotics.
Intensive lifestyle interventions
Prior studies found that intensive lifestyle interventions can help reduce antipsychotic-related weight gain. A 3-month randomized controlled trial compared an early behavioral intervention (dietary counseling, an exercise program, and behavior therapy) with routine care in 61 patients with first-episode psychosis who were taking risperidone, olanzapine, or haloperidol;6 significantly fewer patients assigned to behavioral intervention had an increased initial body weight of more than 7%: 39% in the behavioral intervention group vs 79% in the routine care group (P<.002).
Small samples, small effect sizes
Past studies of metformin for antipsychotic-associated weight gain have generally shown a small benefit, though small sample sizes and small effect sizes prohibited definitive conclusions. Unlike the study by Wu and colleagues,1 none of these past studies were designed to compare the combination of metformin and lifestyle intervention with metformin alone, lifestyle intervention alone, or placebo alone.
Klein et al conducted a randomized placebo-controlled trial of metformin in 39 children ages 10 to 17 whose weight had increased more than 10% on atypical antipsychotic therapy.7 The children treated with placebo gained a mean of 4 kg and increased their mean BMI by 1.12 kg/m2 during 16 weeks of treatment, while those in the metformin group did not gain weight and decreased their mean BMI by 0.43 kg/m2.
Baptista et al randomized 40 in-patients with schizophrenia, who were being switched from conventional antipsychotics to olanzapine, to either metformin (850-1750 mg/d) or placebo. Both groups gained a similar amount of weight after the 14-week study (5.5 vs 6.3 kg, metformin vs placebo). Three patients who started with high fasting glucose had decreases while taking metformin, and 3 patients given placebo developed elevated fasting glucose during the study.8
In another randomized controlled trial of metformin vs placebo in 80 patients who had been taking olanzapine for at least 4 months, Baptista et al found only a small, insignificant difference in weight loss after 12 weeks of treatment (metformin group lost 1.4 kg, placebo group lost 0.18 kg, P=.09). They reported that both groups were highly motivated to lose weight and were compliant with the healthy lifestyle recommendations.9
An adequately powered study
The trial1 highlighted in this PURL had an adequate sample size to compare metformin plus a lifestyle intervention with either treatment alone or placebo. It showed a clinically important effect of metformin both by itself and in conjunction with the lifestyle intervention.
CAVEATS: Consider switching drugs
Before adding metformin to help with weight loss, primary care clinicians should contact the patient’s psychiatrist to discuss the option of switching antipsychotic medications. Switching from a medication with a higher risk for weight gain, such as olanzapine, to one with a lower risk, such as aripiprazole or ziprasidone, can lead to significant weight loss.10
Not an option for some
However, some patients, especially those taking clozapine, may have already tried multiple antipsychotic agents without success, and switching is not an option for them.
Prescribing metformin
CHALLENGES TO IMPLEMENTATION: Adherence
These study participants were under the care of an adult caregiver who monitored and recorded food and medication intake and exercise level. The lifestyle intervention was thorough and structured and this kind of program is often not available to us for our patients. As a consequence, we may not obtain the same results as in this study. However, even the metformin-alone group showed improvements, and if our patients can reliably take their second-generation antipsychotic, they should also be able to take metformin reliably.
Patient resistance
Some patients may resist taking an additional medication to treat the side effects of their antipsychotic medication. Taking the time to educate them about the increased risk of diabetes and cardiovascular disease related to weight gain may help convince them to do so. Warn them about possible gastrointestinal adverse effects of metformin, which tend to lessen or disappear with time.
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Wu R-R, Zhao J-P, Jin H, et al. Lifestyle intervention and metformin for treatment of antipsychotic-induced weight gain: a randomized controlled trial. JAMA. 2008;299:185-193.
2. Rowland K, Schumann SA. Have pedometer, will travel. J Fam Pract. 2008;57:90-93.
3. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
4. Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;68(suppl 1):20-27.
5. Faulkner G, Cohn T, Remington G. Interventions to reduce weight gain in schizophrenia. Cochrane Database Syst Rev. 2007;(1):CD005148.-
6. Alvarez-Jiménez M, González-Blanch C, Vázquez-Barquero JL, et al. Attenuation of antipsychotic-induced weight gain with early behavioral intervention in drug-naïve first-episode psychosis patients: a randomized controlled trial. J Clin Psychiatry. 2006;67:1253-1260.
7. Klein DJ, Cottingham EM, Sorter M, Barton BA, Morrison JA. A randomized, double-blind, placebo-controlled trial of metformin treatment of weight gain associated with initiation of atypical antipsychotic therapy in children and adolescents. Am J Psychiatry. 2006;163:2072-2079.
8. Baptista T, Martínez J, Lacruz A, et al. Metformin for prevention of weight gain and insulin resistance with olanzapine: a double-blind placebo-controlled trial. Can J Psychiatry. 2006;51:192-196.
9. Baptista T, Rangel N, Fernández V, et al. Metformin as an adjunctive treatment to control body weight and metabolic dysfunction during olanzapine administration: a multicentric, double-blind, placebo-controlled trial. Schizophrenia Res. 2007;93:99-108.
10. Weiden PJ. Switching antipsychotics as a treatment strategy for antipsychotic-induced weight gain and dyslipidemia. J Clin Psychiatry. 2007;68(suppl 4):34-39.
1. Wu R-R, Zhao J-P, Jin H, et al. Lifestyle intervention and metformin for treatment of antipsychotic-induced weight gain: a randomized controlled trial. JAMA. 2008;299:185-193.
2. Rowland K, Schumann SA. Have pedometer, will travel. J Fam Pract. 2008;57:90-93.
3. American Diabetes Association; American Psychiatric Association; American Association of Clinical Endocrinologists; North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
4. Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;68(suppl 1):20-27.
5. Faulkner G, Cohn T, Remington G. Interventions to reduce weight gain in schizophrenia. Cochrane Database Syst Rev. 2007;(1):CD005148.-
6. Alvarez-Jiménez M, González-Blanch C, Vázquez-Barquero JL, et al. Attenuation of antipsychotic-induced weight gain with early behavioral intervention in drug-naïve first-episode psychosis patients: a randomized controlled trial. J Clin Psychiatry. 2006;67:1253-1260.
7. Klein DJ, Cottingham EM, Sorter M, Barton BA, Morrison JA. A randomized, double-blind, placebo-controlled trial of metformin treatment of weight gain associated with initiation of atypical antipsychotic therapy in children and adolescents. Am J Psychiatry. 2006;163:2072-2079.
8. Baptista T, Martínez J, Lacruz A, et al. Metformin for prevention of weight gain and insulin resistance with olanzapine: a double-blind placebo-controlled trial. Can J Psychiatry. 2006;51:192-196.
9. Baptista T, Rangel N, Fernández V, et al. Metformin as an adjunctive treatment to control body weight and metabolic dysfunction during olanzapine administration: a multicentric, double-blind, placebo-controlled trial. Schizophrenia Res. 2007;93:99-108.
10. Weiden PJ. Switching antipsychotics as a treatment strategy for antipsychotic-induced weight gain and dyslipidemia. J Clin Psychiatry. 2007;68(suppl 4):34-39.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Patients insist on antibiotics for sinusitis? Here is a good reason to say “no”
ILLUSTRATIVE CASE
A 23-year-old woman presents to your office with a 1-week history of cough, purulent nasal discharge, and unilateral facial pain. You diagnose acute sinusitis.
Should you prescribe an antibiotic?
No. Yet it’s no wonder that most adults treated for acute sinusitis leave the doctor’s office with a prescription for antibiotics. Until the publication of the meta-analysis by Young and colleagues1 featured in this PURL, we have lacked A-level evidence from studies conducted in realistic settings—like your practice and ours.
Review of serial data from the National Ambulatory Medical Care Surveys (NAMCS) from 1999 through 2005 does show a slight downward trend in antibiotic prescribing for acute sinusitis: 1999-2002 data showed that 83% of cases of acute sinusitis were treated with an antibiotic.2 Data from the 2004 and 2005 NAMCS reveal that family physicians prescribed antibiotics for 80% of patients with acute sinusitis in 2004 and 76% of patients in 2005 (S. Medvedev, unpublished data, NAMCS database, March 2008).
Is this continued high rate of antibiotic prescribing justified?
Do antibiotics improve symptoms and shorten the duration of illness or not?
These questions are important, obviously, not only because of the high rate of prescribing but also because sinusitis is one of the most common diagnoses: approximately 20 million cases annually in the United States, or about 21% of all outpatient antibiotic prescriptions for adults.2
Which patients might benefit from antibiotics?
Common clinical signs and symptoms cannot identify patients with rhinosinusitis for whom treatment is clearly justified, given the cost, adverse events, and bacterial resistance associated with antibiotic use
- Severity of symptoms is important only in that signs suggestive of a serious complication are the sole reason for immediate antibiotic treatment
- Purulent discharge noted in the pharynx on exam was associated with a higher likelihood of benefit from antibiotics, but NNT was 8
- Antibiotics are not justified even if a patient reports having symptoms for longer than 7-10 days
Source: Young et al.1
A diagnostic dilemma
Before we discuss the evidence that is summarized in the excellent meta-analysis by Young and colleagues,1 let’s acknowledge that acute sinusitis is undeniably a diagnostic dilemma. Distinguishing bacterial from viral infection is nearly impossible on clinical grounds because the symptoms are so similar. A litany of identical upper respiratory symptoms accompanies both viral and bacterial sinus infections. Purulent nasal secretions, maxillary facial pain (especially with unilateral predominance), maxillary tooth pain (which is uncommon with sinus infection), altered sense of smell, and worsening illness after improvement constitute the short list of signs and symptoms that has some predictive value, but even the presence of all of these is not a terrific predictor of bacterial sinus infection. Plain x-rays have low accuracy in distinguishing viral from bacterial infection. Computed tomography (CT) sinus scans are better but far from perfect, are not readily available in practice, and are expensive.
Sinusitis in the real world
How effective are antibiotics for patients diagnosed not by sinus x-rays or CTs, but by signs and symptoms—as we typically do in daily practice?
A meta-analysis3 of 13 randomized controlled trials (RCTs) found that sinusitis improved without antibiotics, but it included trials in which patients were recruited based on results of imaging studies and cultures, which are not normally used in primary care clinical practice. That study compared antibiotic treatment to placebo for acute uncomplicated sinusitis; 35% of placebo-treated patients were clinically cured by 7 to 12 days and 73% were improved after 7 days. Antibiotic therapy increased cure rates by 15% and improvement rates by 14%, yielding a number needed to treat of 7 to achieve 1 additional positive outcome at 7 days.
STUDY SUMMARY: Meta-analysis of primary care trials
Young and colleagues1 aggregated and analyzed individual patient-level data from all known placebo-controlled, randomized, antibiotic treatment trials of adults with clinical symptoms of acute sinusitis that were conducted in primary care settings. They excluded trials that used imaging or bacterial culture as part of patient recruitment.
Studies were included that allowed the use of concomitant medication such as nonsteroidal anti-inflammatory drugs, decongestants, or nasal steroids, as long as patients in both groups had access to the same medications. All trials excluded patients with severe symptoms such as high fever, periorbital swelling or erythema, or intense facial pain, important exclusions that we will discuss below.
They identified 10 such studies and completed an intent-to-treat analysis of the 9 double-blind trials for which patient level data were available. Using individual data from 2547 patients, the odds ratio for an overall antibiotic treatment effect was 1.37 (95% confidence interval, 1.13-1.66), with a number needed to treat (NNT) of 15.
This finding means that 15 patients needed to be given an antibiotic for 1 additional patient to be cured at 8 to 15 days after treatment commenced. Using statistical modeling, they determined that 64% of patients treated with placebo were cured at 14 days compared with 70% given an antibiotic. One patient out of 1381 treated with placebo experienced a serious complication, a brain abscess.
Do antibiotics benefit any subgroups?
The investigators also analyzed the prognostic value of specific signs and symptoms to answer the question: Is there any subgroup of patients who might benefit more from antibiotic treatment?
Duration. Patients with a longer duration of symptoms, more severe symptoms, or increased age took longer to cure, but were no more likely to benefit from antibiotic treatment than other patients.
Symptoms, such as a previous common cold, pain on bending, unilateral facial pain, tooth pain, and purulent nasal discharge did not have any prognostic value.
Only one sign—purulent discharge noted in the pharynx on examination—was associated with a higher likelihood of benefit from treatment with antibiotics, but the NNT was still 8 in this group. Patients with symptoms for 7 days or longer were no more likely to respond to antibiotics than those with symptoms for fewer than 7 days.1
WHAT’S NEW: Realistic evidence from realistic settings
We believe this meta-analysis provides a high level of evidence against routine treatment of sinusitis with antibiotics in primary care practice. Treating 15 patients with an antibiotic to possibly benefit 1 patient 2 weeks after treatment commences does not seem like a good idea when one considers the cost and complications of antibiotic use. Diarrhea and other adverse outcomes are 80% more common among patients with sinusitis who are treated with an antibiotic compared with placebo.3 As noted above, prior meta-analyses of antibiotic treatment for acute sinusitis have been more encouraging than this meta-analysis, with a number needed to treat of 7, but those meta-analyses are clearly overly optimistic for the results one will achieve in primary care practice using clinical signs and symptoms to diagnose acute sinusitis.3,4 Unlike the Young study, they included trials in specialty clinics with CT scans and sinus puncture and culture used for the diagnostic standard.
Symptoms >1 week are not a reason to prescribe
One very important new finding in this meta-analysis that should change practice is that the duration of illness did not predict a positive response to antibiotics.
Current national recommendations are to use an antibiotic for patients with a duration of illness longer than 1 week, as these patients are presumably more likely to have a bacterial infection.5-7 However, that recommendation had been based on expert opinion, not on data from clinical trials. A longer duration of symptoms should not be a reason to prescribe an antibiotic for sinusitis symptoms.
How can you help your patient?
What to do, then, for patients with acute sinusitis? Treat the symptoms, which means recommending pain medication for facial pain or headache and saline nasal spray for the nasal discharge, not antibiotics or nasal corticosteroids. Side effects will be fewer and costs will be lower.
- Saline irrigation. A 2007 Cochrane review of 8 chronic and recurrent sinusitis trials showed that nasal saline irrigation is effective for reducing symptoms of chronic and recurrent sinusitis.8 Although we do not have high-quality RCT data on saline nasal irrigation for treatment of acute sinusitis, nasal saline irrigation is harmless and inexpensive.
- What about nasal steroids? The evidence is equivocal, and the most recent high-quality RCT of nasal steroids showed no effect.9
CAVEATS: Refer seriously ill patients and complicated cases
A very important caveat to our recommendation is that seriously ill patients must be managed differently. Very infrequently a patient develops a serious complication of acute sinusitis such as brain abscess, periorbital cellulitis, or meningitis. Therefore, seriously ill patients with signs and symptoms of acute bacterial sinusitis, such as high fever, periorbital erythema or edema, severe headache, or intense facial pain must be carefully evaluated and treated with great caution and close follow-up. These patients should be referred immediately for consultation with an otolaryngologist.
Of course, mildly ill patients today may become quite ill tomorrow, so always provide advice to patients to return if they are getting worse, a good clinical practice for any condition that is usually benign but occasionally serious.
Patients who have prolonged or recurrent sinusitis symptoms need further evaluation for other diagnoses such as allergies, cystic fibrosis, fungal sinus infection, and other illnesses associated with immune compromise. These complicated patients benefit from consultation with an otolaryngologist who has a specific interest in chronic and recurrent sinusitis, and perhaps consultation from an infectious disease specialist as well.
CHALLENGES TO IMPLEMENTATION: The patient who wants a pill
Some patients may be accustomed to receiving an antibiotic prescription for their “sinus infections” and may resist conservative management. It may be difficult to convince them that antibiotics won’t make a difference when they attribute past resolution of symptoms to antibiotics.
Take enough time to educate your patients on the natural course of illness, the positive benefits of nasal saline, and the reasons not to use unnecessary antibiotics (eg, they are not effective, have potential adverse effects, and can contribute to future antibiotic resistance); this effort will save you time in future visits.10 A “just in case you don’t get better” prescription to be filled only if the patient is not improving in the next few days is about 50% effective in reducing antibiotic usage for upper respiratory infections.11
Acknowledgement
We acknowledge Sofia Medvedev of the University HealthSystem Consortium (UHC) in Oak Brook, IL for analysis of the National Ambulatory Medical Care Survey data.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
2. Sharp HJ, Denman D, Puumala S, Leopold DA. Treatment of acute and chronic rhinosinusitis in the United States, 1999-2002. Arch Otolaryngol Head Neck Surg. 2007;133:260-265.
3. Rosenfeld RM, Singer M, Jones S. Systematic review of antimicrobial therapy in patients with acute rhinosinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S32-S45.
4. Williams JW, Jr, Aguilar C, Cornell J, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2003;(2):CD000243.-
5. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. For the American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine; Centers for Disease Control; Infectious Diseases Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med. 2001;134:498-505.
6. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guidelines: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1-S31.
7. Anon JB, Jacobs MR, Poole MD, et al. For the Sinus and Allergy Health Partnership. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130(1 suppl):S1-S45.
8. Harvey R, Hannan SA, Badia L, Scadding G. Nasal saline irrigations for the symptoms of chronic rhinosinusitis. Cochrane Database Syst Rev. 2007;(3):CD006394.-
9. Williamson IG, Rumsby K, Benge S, et al. Antibiotics and topical nasal steroid for treatment of acute maxillary sinusitis: a randomized controlled trial. JAMA. 2007;298:2487-2496.
10. Little P, Gould C, Williamson I, Warner G, Gantley M, Kinmonth AL. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. BMJ. 1997;315:350-352.
11. Arroll B, Kenealy T, Kerse N. Do delayed prescriptions reduce antibiotic use in respiratory tract infections? A systematic review. Br J Gen Pract. 2003;53:871-877.
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
ILLUSTRATIVE CASE
A 23-year-old woman presents to your office with a 1-week history of cough, purulent nasal discharge, and unilateral facial pain. You diagnose acute sinusitis.
Should you prescribe an antibiotic?
No. Yet it’s no wonder that most adults treated for acute sinusitis leave the doctor’s office with a prescription for antibiotics. Until the publication of the meta-analysis by Young and colleagues1 featured in this PURL, we have lacked A-level evidence from studies conducted in realistic settings—like your practice and ours.
Review of serial data from the National Ambulatory Medical Care Surveys (NAMCS) from 1999 through 2005 does show a slight downward trend in antibiotic prescribing for acute sinusitis: 1999-2002 data showed that 83% of cases of acute sinusitis were treated with an antibiotic.2 Data from the 2004 and 2005 NAMCS reveal that family physicians prescribed antibiotics for 80% of patients with acute sinusitis in 2004 and 76% of patients in 2005 (S. Medvedev, unpublished data, NAMCS database, March 2008).
Is this continued high rate of antibiotic prescribing justified?
Do antibiotics improve symptoms and shorten the duration of illness or not?
These questions are important, obviously, not only because of the high rate of prescribing but also because sinusitis is one of the most common diagnoses: approximately 20 million cases annually in the United States, or about 21% of all outpatient antibiotic prescriptions for adults.2
Which patients might benefit from antibiotics?
Common clinical signs and symptoms cannot identify patients with rhinosinusitis for whom treatment is clearly justified, given the cost, adverse events, and bacterial resistance associated with antibiotic use
- Severity of symptoms is important only in that signs suggestive of a serious complication are the sole reason for immediate antibiotic treatment
- Purulent discharge noted in the pharynx on exam was associated with a higher likelihood of benefit from antibiotics, but NNT was 8
- Antibiotics are not justified even if a patient reports having symptoms for longer than 7-10 days
Source: Young et al.1
A diagnostic dilemma
Before we discuss the evidence that is summarized in the excellent meta-analysis by Young and colleagues,1 let’s acknowledge that acute sinusitis is undeniably a diagnostic dilemma. Distinguishing bacterial from viral infection is nearly impossible on clinical grounds because the symptoms are so similar. A litany of identical upper respiratory symptoms accompanies both viral and bacterial sinus infections. Purulent nasal secretions, maxillary facial pain (especially with unilateral predominance), maxillary tooth pain (which is uncommon with sinus infection), altered sense of smell, and worsening illness after improvement constitute the short list of signs and symptoms that has some predictive value, but even the presence of all of these is not a terrific predictor of bacterial sinus infection. Plain x-rays have low accuracy in distinguishing viral from bacterial infection. Computed tomography (CT) sinus scans are better but far from perfect, are not readily available in practice, and are expensive.
Sinusitis in the real world
How effective are antibiotics for patients diagnosed not by sinus x-rays or CTs, but by signs and symptoms—as we typically do in daily practice?
A meta-analysis3 of 13 randomized controlled trials (RCTs) found that sinusitis improved without antibiotics, but it included trials in which patients were recruited based on results of imaging studies and cultures, which are not normally used in primary care clinical practice. That study compared antibiotic treatment to placebo for acute uncomplicated sinusitis; 35% of placebo-treated patients were clinically cured by 7 to 12 days and 73% were improved after 7 days. Antibiotic therapy increased cure rates by 15% and improvement rates by 14%, yielding a number needed to treat of 7 to achieve 1 additional positive outcome at 7 days.
STUDY SUMMARY: Meta-analysis of primary care trials
Young and colleagues1 aggregated and analyzed individual patient-level data from all known placebo-controlled, randomized, antibiotic treatment trials of adults with clinical symptoms of acute sinusitis that were conducted in primary care settings. They excluded trials that used imaging or bacterial culture as part of patient recruitment.
Studies were included that allowed the use of concomitant medication such as nonsteroidal anti-inflammatory drugs, decongestants, or nasal steroids, as long as patients in both groups had access to the same medications. All trials excluded patients with severe symptoms such as high fever, periorbital swelling or erythema, or intense facial pain, important exclusions that we will discuss below.
They identified 10 such studies and completed an intent-to-treat analysis of the 9 double-blind trials for which patient level data were available. Using individual data from 2547 patients, the odds ratio for an overall antibiotic treatment effect was 1.37 (95% confidence interval, 1.13-1.66), with a number needed to treat (NNT) of 15.
This finding means that 15 patients needed to be given an antibiotic for 1 additional patient to be cured at 8 to 15 days after treatment commenced. Using statistical modeling, they determined that 64% of patients treated with placebo were cured at 14 days compared with 70% given an antibiotic. One patient out of 1381 treated with placebo experienced a serious complication, a brain abscess.
Do antibiotics benefit any subgroups?
The investigators also analyzed the prognostic value of specific signs and symptoms to answer the question: Is there any subgroup of patients who might benefit more from antibiotic treatment?
Duration. Patients with a longer duration of symptoms, more severe symptoms, or increased age took longer to cure, but were no more likely to benefit from antibiotic treatment than other patients.
Symptoms, such as a previous common cold, pain on bending, unilateral facial pain, tooth pain, and purulent nasal discharge did not have any prognostic value.
Only one sign—purulent discharge noted in the pharynx on examination—was associated with a higher likelihood of benefit from treatment with antibiotics, but the NNT was still 8 in this group. Patients with symptoms for 7 days or longer were no more likely to respond to antibiotics than those with symptoms for fewer than 7 days.1
WHAT’S NEW: Realistic evidence from realistic settings
We believe this meta-analysis provides a high level of evidence against routine treatment of sinusitis with antibiotics in primary care practice. Treating 15 patients with an antibiotic to possibly benefit 1 patient 2 weeks after treatment commences does not seem like a good idea when one considers the cost and complications of antibiotic use. Diarrhea and other adverse outcomes are 80% more common among patients with sinusitis who are treated with an antibiotic compared with placebo.3 As noted above, prior meta-analyses of antibiotic treatment for acute sinusitis have been more encouraging than this meta-analysis, with a number needed to treat of 7, but those meta-analyses are clearly overly optimistic for the results one will achieve in primary care practice using clinical signs and symptoms to diagnose acute sinusitis.3,4 Unlike the Young study, they included trials in specialty clinics with CT scans and sinus puncture and culture used for the diagnostic standard.
Symptoms >1 week are not a reason to prescribe
One very important new finding in this meta-analysis that should change practice is that the duration of illness did not predict a positive response to antibiotics.
Current national recommendations are to use an antibiotic for patients with a duration of illness longer than 1 week, as these patients are presumably more likely to have a bacterial infection.5-7 However, that recommendation had been based on expert opinion, not on data from clinical trials. A longer duration of symptoms should not be a reason to prescribe an antibiotic for sinusitis symptoms.
How can you help your patient?
What to do, then, for patients with acute sinusitis? Treat the symptoms, which means recommending pain medication for facial pain or headache and saline nasal spray for the nasal discharge, not antibiotics or nasal corticosteroids. Side effects will be fewer and costs will be lower.
- Saline irrigation. A 2007 Cochrane review of 8 chronic and recurrent sinusitis trials showed that nasal saline irrigation is effective for reducing symptoms of chronic and recurrent sinusitis.8 Although we do not have high-quality RCT data on saline nasal irrigation for treatment of acute sinusitis, nasal saline irrigation is harmless and inexpensive.
- What about nasal steroids? The evidence is equivocal, and the most recent high-quality RCT of nasal steroids showed no effect.9
CAVEATS: Refer seriously ill patients and complicated cases
A very important caveat to our recommendation is that seriously ill patients must be managed differently. Very infrequently a patient develops a serious complication of acute sinusitis such as brain abscess, periorbital cellulitis, or meningitis. Therefore, seriously ill patients with signs and symptoms of acute bacterial sinusitis, such as high fever, periorbital erythema or edema, severe headache, or intense facial pain must be carefully evaluated and treated with great caution and close follow-up. These patients should be referred immediately for consultation with an otolaryngologist.
Of course, mildly ill patients today may become quite ill tomorrow, so always provide advice to patients to return if they are getting worse, a good clinical practice for any condition that is usually benign but occasionally serious.
Patients who have prolonged or recurrent sinusitis symptoms need further evaluation for other diagnoses such as allergies, cystic fibrosis, fungal sinus infection, and other illnesses associated with immune compromise. These complicated patients benefit from consultation with an otolaryngologist who has a specific interest in chronic and recurrent sinusitis, and perhaps consultation from an infectious disease specialist as well.
CHALLENGES TO IMPLEMENTATION: The patient who wants a pill
Some patients may be accustomed to receiving an antibiotic prescription for their “sinus infections” and may resist conservative management. It may be difficult to convince them that antibiotics won’t make a difference when they attribute past resolution of symptoms to antibiotics.
Take enough time to educate your patients on the natural course of illness, the positive benefits of nasal saline, and the reasons not to use unnecessary antibiotics (eg, they are not effective, have potential adverse effects, and can contribute to future antibiotic resistance); this effort will save you time in future visits.10 A “just in case you don’t get better” prescription to be filled only if the patient is not improving in the next few days is about 50% effective in reducing antibiotic usage for upper respiratory infections.11
Acknowledgement
We acknowledge Sofia Medvedev of the University HealthSystem Consortium (UHC) in Oak Brook, IL for analysis of the National Ambulatory Medical Care Survey data.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
ILLUSTRATIVE CASE
A 23-year-old woman presents to your office with a 1-week history of cough, purulent nasal discharge, and unilateral facial pain. You diagnose acute sinusitis.
Should you prescribe an antibiotic?
No. Yet it’s no wonder that most adults treated for acute sinusitis leave the doctor’s office with a prescription for antibiotics. Until the publication of the meta-analysis by Young and colleagues1 featured in this PURL, we have lacked A-level evidence from studies conducted in realistic settings—like your practice and ours.
Review of serial data from the National Ambulatory Medical Care Surveys (NAMCS) from 1999 through 2005 does show a slight downward trend in antibiotic prescribing for acute sinusitis: 1999-2002 data showed that 83% of cases of acute sinusitis were treated with an antibiotic.2 Data from the 2004 and 2005 NAMCS reveal that family physicians prescribed antibiotics for 80% of patients with acute sinusitis in 2004 and 76% of patients in 2005 (S. Medvedev, unpublished data, NAMCS database, March 2008).
Is this continued high rate of antibiotic prescribing justified?
Do antibiotics improve symptoms and shorten the duration of illness or not?
These questions are important, obviously, not only because of the high rate of prescribing but also because sinusitis is one of the most common diagnoses: approximately 20 million cases annually in the United States, or about 21% of all outpatient antibiotic prescriptions for adults.2
Which patients might benefit from antibiotics?
Common clinical signs and symptoms cannot identify patients with rhinosinusitis for whom treatment is clearly justified, given the cost, adverse events, and bacterial resistance associated with antibiotic use
- Severity of symptoms is important only in that signs suggestive of a serious complication are the sole reason for immediate antibiotic treatment
- Purulent discharge noted in the pharynx on exam was associated with a higher likelihood of benefit from antibiotics, but NNT was 8
- Antibiotics are not justified even if a patient reports having symptoms for longer than 7-10 days
Source: Young et al.1
A diagnostic dilemma
Before we discuss the evidence that is summarized in the excellent meta-analysis by Young and colleagues,1 let’s acknowledge that acute sinusitis is undeniably a diagnostic dilemma. Distinguishing bacterial from viral infection is nearly impossible on clinical grounds because the symptoms are so similar. A litany of identical upper respiratory symptoms accompanies both viral and bacterial sinus infections. Purulent nasal secretions, maxillary facial pain (especially with unilateral predominance), maxillary tooth pain (which is uncommon with sinus infection), altered sense of smell, and worsening illness after improvement constitute the short list of signs and symptoms that has some predictive value, but even the presence of all of these is not a terrific predictor of bacterial sinus infection. Plain x-rays have low accuracy in distinguishing viral from bacterial infection. Computed tomography (CT) sinus scans are better but far from perfect, are not readily available in practice, and are expensive.
Sinusitis in the real world
How effective are antibiotics for patients diagnosed not by sinus x-rays or CTs, but by signs and symptoms—as we typically do in daily practice?
A meta-analysis3 of 13 randomized controlled trials (RCTs) found that sinusitis improved without antibiotics, but it included trials in which patients were recruited based on results of imaging studies and cultures, which are not normally used in primary care clinical practice. That study compared antibiotic treatment to placebo for acute uncomplicated sinusitis; 35% of placebo-treated patients were clinically cured by 7 to 12 days and 73% were improved after 7 days. Antibiotic therapy increased cure rates by 15% and improvement rates by 14%, yielding a number needed to treat of 7 to achieve 1 additional positive outcome at 7 days.
STUDY SUMMARY: Meta-analysis of primary care trials
Young and colleagues1 aggregated and analyzed individual patient-level data from all known placebo-controlled, randomized, antibiotic treatment trials of adults with clinical symptoms of acute sinusitis that were conducted in primary care settings. They excluded trials that used imaging or bacterial culture as part of patient recruitment.
Studies were included that allowed the use of concomitant medication such as nonsteroidal anti-inflammatory drugs, decongestants, or nasal steroids, as long as patients in both groups had access to the same medications. All trials excluded patients with severe symptoms such as high fever, periorbital swelling or erythema, or intense facial pain, important exclusions that we will discuss below.
They identified 10 such studies and completed an intent-to-treat analysis of the 9 double-blind trials for which patient level data were available. Using individual data from 2547 patients, the odds ratio for an overall antibiotic treatment effect was 1.37 (95% confidence interval, 1.13-1.66), with a number needed to treat (NNT) of 15.
This finding means that 15 patients needed to be given an antibiotic for 1 additional patient to be cured at 8 to 15 days after treatment commenced. Using statistical modeling, they determined that 64% of patients treated with placebo were cured at 14 days compared with 70% given an antibiotic. One patient out of 1381 treated with placebo experienced a serious complication, a brain abscess.
Do antibiotics benefit any subgroups?
The investigators also analyzed the prognostic value of specific signs and symptoms to answer the question: Is there any subgroup of patients who might benefit more from antibiotic treatment?
Duration. Patients with a longer duration of symptoms, more severe symptoms, or increased age took longer to cure, but were no more likely to benefit from antibiotic treatment than other patients.
Symptoms, such as a previous common cold, pain on bending, unilateral facial pain, tooth pain, and purulent nasal discharge did not have any prognostic value.
Only one sign—purulent discharge noted in the pharynx on examination—was associated with a higher likelihood of benefit from treatment with antibiotics, but the NNT was still 8 in this group. Patients with symptoms for 7 days or longer were no more likely to respond to antibiotics than those with symptoms for fewer than 7 days.1
WHAT’S NEW: Realistic evidence from realistic settings
We believe this meta-analysis provides a high level of evidence against routine treatment of sinusitis with antibiotics in primary care practice. Treating 15 patients with an antibiotic to possibly benefit 1 patient 2 weeks after treatment commences does not seem like a good idea when one considers the cost and complications of antibiotic use. Diarrhea and other adverse outcomes are 80% more common among patients with sinusitis who are treated with an antibiotic compared with placebo.3 As noted above, prior meta-analyses of antibiotic treatment for acute sinusitis have been more encouraging than this meta-analysis, with a number needed to treat of 7, but those meta-analyses are clearly overly optimistic for the results one will achieve in primary care practice using clinical signs and symptoms to diagnose acute sinusitis.3,4 Unlike the Young study, they included trials in specialty clinics with CT scans and sinus puncture and culture used for the diagnostic standard.
Symptoms >1 week are not a reason to prescribe
One very important new finding in this meta-analysis that should change practice is that the duration of illness did not predict a positive response to antibiotics.
Current national recommendations are to use an antibiotic for patients with a duration of illness longer than 1 week, as these patients are presumably more likely to have a bacterial infection.5-7 However, that recommendation had been based on expert opinion, not on data from clinical trials. A longer duration of symptoms should not be a reason to prescribe an antibiotic for sinusitis symptoms.
How can you help your patient?
What to do, then, for patients with acute sinusitis? Treat the symptoms, which means recommending pain medication for facial pain or headache and saline nasal spray for the nasal discharge, not antibiotics or nasal corticosteroids. Side effects will be fewer and costs will be lower.
- Saline irrigation. A 2007 Cochrane review of 8 chronic and recurrent sinusitis trials showed that nasal saline irrigation is effective for reducing symptoms of chronic and recurrent sinusitis.8 Although we do not have high-quality RCT data on saline nasal irrigation for treatment of acute sinusitis, nasal saline irrigation is harmless and inexpensive.
- What about nasal steroids? The evidence is equivocal, and the most recent high-quality RCT of nasal steroids showed no effect.9
CAVEATS: Refer seriously ill patients and complicated cases
A very important caveat to our recommendation is that seriously ill patients must be managed differently. Very infrequently a patient develops a serious complication of acute sinusitis such as brain abscess, periorbital cellulitis, or meningitis. Therefore, seriously ill patients with signs and symptoms of acute bacterial sinusitis, such as high fever, periorbital erythema or edema, severe headache, or intense facial pain must be carefully evaluated and treated with great caution and close follow-up. These patients should be referred immediately for consultation with an otolaryngologist.
Of course, mildly ill patients today may become quite ill tomorrow, so always provide advice to patients to return if they are getting worse, a good clinical practice for any condition that is usually benign but occasionally serious.
Patients who have prolonged or recurrent sinusitis symptoms need further evaluation for other diagnoses such as allergies, cystic fibrosis, fungal sinus infection, and other illnesses associated with immune compromise. These complicated patients benefit from consultation with an otolaryngologist who has a specific interest in chronic and recurrent sinusitis, and perhaps consultation from an infectious disease specialist as well.
CHALLENGES TO IMPLEMENTATION: The patient who wants a pill
Some patients may be accustomed to receiving an antibiotic prescription for their “sinus infections” and may resist conservative management. It may be difficult to convince them that antibiotics won’t make a difference when they attribute past resolution of symptoms to antibiotics.
Take enough time to educate your patients on the natural course of illness, the positive benefits of nasal saline, and the reasons not to use unnecessary antibiotics (eg, they are not effective, have potential adverse effects, and can contribute to future antibiotic resistance); this effort will save you time in future visits.10 A “just in case you don’t get better” prescription to be filled only if the patient is not improving in the next few days is about 50% effective in reducing antibiotic usage for upper respiratory infections.11
Acknowledgement
We acknowledge Sofia Medvedev of the University HealthSystem Consortium (UHC) in Oak Brook, IL for analysis of the National Ambulatory Medical Care Survey data.
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
2. Sharp HJ, Denman D, Puumala S, Leopold DA. Treatment of acute and chronic rhinosinusitis in the United States, 1999-2002. Arch Otolaryngol Head Neck Surg. 2007;133:260-265.
3. Rosenfeld RM, Singer M, Jones S. Systematic review of antimicrobial therapy in patients with acute rhinosinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S32-S45.
4. Williams JW, Jr, Aguilar C, Cornell J, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2003;(2):CD000243.-
5. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. For the American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine; Centers for Disease Control; Infectious Diseases Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med. 2001;134:498-505.
6. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guidelines: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1-S31.
7. Anon JB, Jacobs MR, Poole MD, et al. For the Sinus and Allergy Health Partnership. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130(1 suppl):S1-S45.
8. Harvey R, Hannan SA, Badia L, Scadding G. Nasal saline irrigations for the symptoms of chronic rhinosinusitis. Cochrane Database Syst Rev. 2007;(3):CD006394.-
9. Williamson IG, Rumsby K, Benge S, et al. Antibiotics and topical nasal steroid for treatment of acute maxillary sinusitis: a randomized controlled trial. JAMA. 2007;298:2487-2496.
10. Little P, Gould C, Williamson I, Warner G, Gantley M, Kinmonth AL. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. BMJ. 1997;315:350-352.
11. Arroll B, Kenealy T, Kerse N. Do delayed prescriptions reduce antibiotic use in respiratory tract infections? A systematic review. Br J Gen Pract. 2003;53:871-877.
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet. 2008;371:908-914.
2. Sharp HJ, Denman D, Puumala S, Leopold DA. Treatment of acute and chronic rhinosinusitis in the United States, 1999-2002. Arch Otolaryngol Head Neck Surg. 2007;133:260-265.
3. Rosenfeld RM, Singer M, Jones S. Systematic review of antimicrobial therapy in patients with acute rhinosinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S32-S45.
4. Williams JW, Jr, Aguilar C, Cornell J, et al. Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev. 2003;(2):CD000243.-
5. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA. For the American Academy of Family Physicians; American College of Physicians-American Society of Internal Medicine; Centers for Disease Control; Infectious Diseases Society of America. Principles of appropriate antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med. 2001;134:498-505.
6. Rosenfeld RM, Andes D, Bhattacharyya N, et al. Clinical practice guidelines: adult sinusitis. Otolaryngol Head Neck Surg. 2007;137(3 suppl):S1-S31.
7. Anon JB, Jacobs MR, Poole MD, et al. For the Sinus and Allergy Health Partnership. Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg. 2004;130(1 suppl):S1-S45.
8. Harvey R, Hannan SA, Badia L, Scadding G. Nasal saline irrigations for the symptoms of chronic rhinosinusitis. Cochrane Database Syst Rev. 2007;(3):CD006394.-
9. Williamson IG, Rumsby K, Benge S, et al. Antibiotics and topical nasal steroid for treatment of acute maxillary sinusitis: a randomized controlled trial. JAMA. 2007;298:2487-2496.
10. Little P, Gould C, Williamson I, Warner G, Gantley M, Kinmonth AL. Reattendance and complications in a randomised trial of prescribing strategies for sore throat: the medicalising effect of prescribing antibiotics. BMJ. 1997;315:350-352.
11. Arroll B, Kenealy T, Kerse N. Do delayed prescriptions reduce antibiotic use in respiratory tract infections? A systematic review. Br J Gen Pract. 2003;53:871-877.
The PURLs Surveillance System is supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Use anesthetic drops to relieve acute otitis media pain
ILLUSTRATIVE CASE
A mother brings her 3-year-old son to your office first thing in the morning. The boy has fever and right ear pain. You see that the tympanic membrane is dull, red, and bulging. The mother has been up most of the night with her child. She implores you to “do something.” She is exhausted and her son is crying and holding his right ear. You know that antibiotics will not provide immediate pain relief and oral analgesics will take a while to help. What can you offer that will help right away?
Until this study, we’ve had only 1 placebo-controlled trial to guide how we manage a big problem. Big in terms of distress to parents and children, and in sheer numbers—acute otitis media (AOM) is extremely common in children.2,3
Routine antibiotics: Woeful lack of evidence
Even when antibiotics are indicated, pain relief is minimal and takes several days.4-8 Despite “a woeful lack of substantial evidence on the question of antibiotic therapy” for AOM, it is the most common reason for the prescription of antibiotics in children.4,6 A Cochrane review showed that antibiotics have no effect on recurrence of AOM or complications, including hearing impairment.5 The same review showed no pain reduction in 24 hours and only 30% pain reduction in 2 to 7 days with antibiotic use.5 Antibiotics clearly have a minimal role in providing pain relief for AOM.
Oral analgesics too slow
Oral analgesic use in AOM has been studied and has shown good results. We calculated the number needed to treat (1.0 divided by the absolute risk reduction) for both ibuprofen (number needed to treat [NNT]=5) and acetaminophen (NNT=6) from data in the 1996 trial by Bertin et al.9
It is a common practice in the United States to treat AOM with oral analgesics. However, the onset of pain relief with oral medications can be slow and the relief is generally not complete, so oral medications are not immediately helpful to meet the needs of our crying 3-year-old patient and his exhausted mother.
Topical anesthetics
To our knowledge, prior evidence on the efficacy of topical anesthetics is limited to 1 placebo-controlled trial. A randomized trial by Hoberman et al,10 with 54 subjects, showed a statistically significant 25% reduction in pain with the analgesic drops Auralgan (containing antipyrine, benzocaine, and glycerine) at 30 minutes when compared with olive oil. A 2006 Cochrane review11 did not include the Bolt et al trial1 described in this PURL, but did include the Hoberman trial10 and 3 trials that compared a topical anesthetic with naturopathic herbal ear drops for AOM pain, and the review concluded that evidence was insufficient.
Topical anesthetic plus oraI analgesia for earache relief
Bolt P et al.1
STUDY SUMMARY: Pain measured by visual analogue, Bieri faces scales
This double-blind, randomized, placebo-controlled trial1 compared aqueous lidocaine 2% drops with saline drops in the ear, for reducing pain due to AOM in patients 3 to 17 years of age. The trial was conducted at an Australian children’s hospital emergency room. The study evaluated “lignocaine,” the name for lidocaine in Australia.
Emergency physicians instilled 3 drops of either lidocaine or saline into the affected ear in the 2 groups (n=31 in the study group and n=32 in the placebo group). Patients, parents, treating physicians, and staff administering ear drops and assessing pain were blinded to group assignment. Doctors measured pain at baseline and after 30 minutes and patients measured pain at baseline, 10, 20, and 30 minutes after the drops were instilled, using the Bieri faces pain scale and a visual analogue scale.12
Lidocaine reduced pain scores by 50% from baseline at 10 and 30 minutes compared with saline. No serious side effects were noted at 30 minutes, although 3 patients in the lidocaine group complained of mild dizziness the next day. The treating physician prescribed paracetamol (equivalent to acetaminophen) for participants in both the lidocaine and the placebo group at their discretion. The proportion given paracetamol was similar in both groups.
WHAT’S NEW: Pain relief is immediate
Family physicians have used topical anethestics for otitis externa for decades. This RCT adds evidence that topical anesthetics are useful for providing immediate pain relief from AOM, as well. The 2004 guidelines from the American Academy of Pediatrics and the American Academy of Family Physicians indicate that management of AOM should include the assessment and treatment of pain.
We think that topical agents such as lidocaine and benzocaine are useful adjuncts to oral analgesics in providing immediate pain relief, especially in the face of evidence showing that antibiotics do not offer significant pain relief.
Previous studies have shown that aqueous lidocaine is ineffective on uninflamed tympanic membrane.13 The results of this study are consistent with increased uptake of the drug through the inflamed tympanic membrane.
CAVEATS: Children >3 years studied
This trial included only children older than 3 years, so the results may not apply to younger children and infants.
This essentially was a study of ear pain treatment, which, in our view, does not detract from the clinical usefulness of the findings. Topical anesthetics seem to be useful for ear pain in general.
Concurrent analgesics
Some variability existed in the oral analgesics the children received, as these agents were given at the discretion of the parents and treating physicians. We think that this does not detract from the study findings, as it represents a practical, real-world setting, which is desirable in an effectiveness RCT. Moreover, the extent of pain reduction was over and above that conferred by analgesic administration.
CHALLENGES TO IMPLEMENTATION: Lidocaine is not sold in a dropper
Aqueous lidocaine is not sold in a bottle with a dropper: our search on www.drugstore.com and www.drugs.com did not yield an otic preparation with only aqueous lidocaine. However, 2% injectable lidocaine, which is readily available, can be used with a dropper. Aqueous lidocaine can be compounded at a compounding pharmacy and placed in a bottle with a dropper.
Benzocaine might be a suitable substitute
In preparing this PURL, we learned from several colleagues that they always keep a bottle of benzocaine in their pocket and they apply the drops to the ears of their pediatric patients with AOM when they see them in their offices or in the emergency department.
Benzocaine is available in various brand names (eg, Auralgan, Americaine, A/B otic drops, among others). These are oil suspensions and not an aqueous solution as used in this study, so it would be important not to use these preparations in the presence of a ruptured tympanic membrane because the oil suspension may not be absorbed. The aqueous solution will be absorbed so it can be used even if a ruptured tympanic membrane is suspected.
In most situations rupture of the tympanic membrane gives immediate pain relief. However, in some, the pain persists and it may be difficult to tell if the tympanic membrane has ruptured or the debris and pus is from otitis externa. In those situations, the aqueous lidocaine solution might be preferred.
Should parents give drops at home?
This study does not address home use of these drops. However, benzocaine preparations have been used safely for many years for otitis externa at home, and we cannot think of any reason why drops could not be prescribed for home use in acute otitis media.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Bolt P, Barnett P, Babl FE, Sharwood LN. Topical lignocaine for pain relief in acute otitis media: results of a double-blind placebo-controlled randomised trial. Arch Dis Child. 2008;93:40-44.
2. Teele DW, Klein JO, Rosner B. Epidemiology of otitis media during the first seven years of life in children in greater Boston: a prospective, cohort study. J Infect Dis. 1989;160:83-94.
3. Arnold J. Otitis media and its complications. In: Nelson W, Behrman R, Kliegman R, Arvin A, eds. Nelson Textbook of Pediatrics. 15th ed. Philadelphia: Saunders; 1996:1814-1824.
4. Chan LS, Takata GS, Shekelle P, Morton SC, Mason W, Marcy SM. Evidence assessment of management of acute otitis media: II. Research gaps and priorities for future research. Pediatrics. 2001;108:248-254.
5. Glasziou PP, Del Mar CB, Sanders SL, Hayem M. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2004;(1):CD000219.
6. Hendley JO. Clinical practice. Otitis media. N Engl J Med. 2002;347:1169-1174.
7. Rovers MM, Glasziou P, Appelman CL, et al. Antibiotics for acute otitis media: a meta-analysis with individual patient data. Lancet. 2006;368:1429-1435.
8. Gasper K, St Anna L, Montgomery L. Clinical inquiries. Are antibiotics effective for otitis media with effusion? J Fam Pract. 2003;52:321-323.
9. Bertin L, Pons G, d’Athis P, et al. A randomized, double-blind, multicentre controlled trial of ibuprofen versus acetaminophen and placebo for symptoms of acute otitis media in children. Fundam Clin Pharmacol. 1996;10:387-392.
10. Hoberman A, Paradise JL, Reynolds EA, Urkin J. Efficacy of Auralgan for treating ear pain in children with acute otitis media. Arch Pediatr Adolesc Med. 1997;151:675-678.
11. Cochrane Database Syst Rev 2006 Jul 19;3: CD005657.
12. Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The Faces Pain Scale-Revised: toward a common metric in pediatric pain measurement. Pain. 2001;93:173-183.
13. Moller A, Grontved A. Topical anaesthesia of the normal tympanic membrane: a controlled clinical trial of different suspensions of lidocaine. ORL J Otorhinolaryngol Relat Spec. 1990;52:168-173.
ILLUSTRATIVE CASE
A mother brings her 3-year-old son to your office first thing in the morning. The boy has fever and right ear pain. You see that the tympanic membrane is dull, red, and bulging. The mother has been up most of the night with her child. She implores you to “do something.” She is exhausted and her son is crying and holding his right ear. You know that antibiotics will not provide immediate pain relief and oral analgesics will take a while to help. What can you offer that will help right away?
Until this study, we’ve had only 1 placebo-controlled trial to guide how we manage a big problem. Big in terms of distress to parents and children, and in sheer numbers—acute otitis media (AOM) is extremely common in children.2,3
Routine antibiotics: Woeful lack of evidence
Even when antibiotics are indicated, pain relief is minimal and takes several days.4-8 Despite “a woeful lack of substantial evidence on the question of antibiotic therapy” for AOM, it is the most common reason for the prescription of antibiotics in children.4,6 A Cochrane review showed that antibiotics have no effect on recurrence of AOM or complications, including hearing impairment.5 The same review showed no pain reduction in 24 hours and only 30% pain reduction in 2 to 7 days with antibiotic use.5 Antibiotics clearly have a minimal role in providing pain relief for AOM.
Oral analgesics too slow
Oral analgesic use in AOM has been studied and has shown good results. We calculated the number needed to treat (1.0 divided by the absolute risk reduction) for both ibuprofen (number needed to treat [NNT]=5) and acetaminophen (NNT=6) from data in the 1996 trial by Bertin et al.9
It is a common practice in the United States to treat AOM with oral analgesics. However, the onset of pain relief with oral medications can be slow and the relief is generally not complete, so oral medications are not immediately helpful to meet the needs of our crying 3-year-old patient and his exhausted mother.
Topical anesthetics
To our knowledge, prior evidence on the efficacy of topical anesthetics is limited to 1 placebo-controlled trial. A randomized trial by Hoberman et al,10 with 54 subjects, showed a statistically significant 25% reduction in pain with the analgesic drops Auralgan (containing antipyrine, benzocaine, and glycerine) at 30 minutes when compared with olive oil. A 2006 Cochrane review11 did not include the Bolt et al trial1 described in this PURL, but did include the Hoberman trial10 and 3 trials that compared a topical anesthetic with naturopathic herbal ear drops for AOM pain, and the review concluded that evidence was insufficient.
Topical anesthetic plus oraI analgesia for earache relief
Bolt P et al.1
STUDY SUMMARY: Pain measured by visual analogue, Bieri faces scales
This double-blind, randomized, placebo-controlled trial1 compared aqueous lidocaine 2% drops with saline drops in the ear, for reducing pain due to AOM in patients 3 to 17 years of age. The trial was conducted at an Australian children’s hospital emergency room. The study evaluated “lignocaine,” the name for lidocaine in Australia.
Emergency physicians instilled 3 drops of either lidocaine or saline into the affected ear in the 2 groups (n=31 in the study group and n=32 in the placebo group). Patients, parents, treating physicians, and staff administering ear drops and assessing pain were blinded to group assignment. Doctors measured pain at baseline and after 30 minutes and patients measured pain at baseline, 10, 20, and 30 minutes after the drops were instilled, using the Bieri faces pain scale and a visual analogue scale.12
Lidocaine reduced pain scores by 50% from baseline at 10 and 30 minutes compared with saline. No serious side effects were noted at 30 minutes, although 3 patients in the lidocaine group complained of mild dizziness the next day. The treating physician prescribed paracetamol (equivalent to acetaminophen) for participants in both the lidocaine and the placebo group at their discretion. The proportion given paracetamol was similar in both groups.
WHAT’S NEW: Pain relief is immediate
Family physicians have used topical anethestics for otitis externa for decades. This RCT adds evidence that topical anesthetics are useful for providing immediate pain relief from AOM, as well. The 2004 guidelines from the American Academy of Pediatrics and the American Academy of Family Physicians indicate that management of AOM should include the assessment and treatment of pain.
We think that topical agents such as lidocaine and benzocaine are useful adjuncts to oral analgesics in providing immediate pain relief, especially in the face of evidence showing that antibiotics do not offer significant pain relief.
Previous studies have shown that aqueous lidocaine is ineffective on uninflamed tympanic membrane.13 The results of this study are consistent with increased uptake of the drug through the inflamed tympanic membrane.
CAVEATS: Children >3 years studied
This trial included only children older than 3 years, so the results may not apply to younger children and infants.
This essentially was a study of ear pain treatment, which, in our view, does not detract from the clinical usefulness of the findings. Topical anesthetics seem to be useful for ear pain in general.
Concurrent analgesics
Some variability existed in the oral analgesics the children received, as these agents were given at the discretion of the parents and treating physicians. We think that this does not detract from the study findings, as it represents a practical, real-world setting, which is desirable in an effectiveness RCT. Moreover, the extent of pain reduction was over and above that conferred by analgesic administration.
CHALLENGES TO IMPLEMENTATION: Lidocaine is not sold in a dropper
Aqueous lidocaine is not sold in a bottle with a dropper: our search on www.drugstore.com and www.drugs.com did not yield an otic preparation with only aqueous lidocaine. However, 2% injectable lidocaine, which is readily available, can be used with a dropper. Aqueous lidocaine can be compounded at a compounding pharmacy and placed in a bottle with a dropper.
Benzocaine might be a suitable substitute
In preparing this PURL, we learned from several colleagues that they always keep a bottle of benzocaine in their pocket and they apply the drops to the ears of their pediatric patients with AOM when they see them in their offices or in the emergency department.
Benzocaine is available in various brand names (eg, Auralgan, Americaine, A/B otic drops, among others). These are oil suspensions and not an aqueous solution as used in this study, so it would be important not to use these preparations in the presence of a ruptured tympanic membrane because the oil suspension may not be absorbed. The aqueous solution will be absorbed so it can be used even if a ruptured tympanic membrane is suspected.
In most situations rupture of the tympanic membrane gives immediate pain relief. However, in some, the pain persists and it may be difficult to tell if the tympanic membrane has ruptured or the debris and pus is from otitis externa. In those situations, the aqueous lidocaine solution might be preferred.
Should parents give drops at home?
This study does not address home use of these drops. However, benzocaine preparations have been used safely for many years for otitis externa at home, and we cannot think of any reason why drops could not be prescribed for home use in acute otitis media.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
ILLUSTRATIVE CASE
A mother brings her 3-year-old son to your office first thing in the morning. The boy has fever and right ear pain. You see that the tympanic membrane is dull, red, and bulging. The mother has been up most of the night with her child. She implores you to “do something.” She is exhausted and her son is crying and holding his right ear. You know that antibiotics will not provide immediate pain relief and oral analgesics will take a while to help. What can you offer that will help right away?
Until this study, we’ve had only 1 placebo-controlled trial to guide how we manage a big problem. Big in terms of distress to parents and children, and in sheer numbers—acute otitis media (AOM) is extremely common in children.2,3
Routine antibiotics: Woeful lack of evidence
Even when antibiotics are indicated, pain relief is minimal and takes several days.4-8 Despite “a woeful lack of substantial evidence on the question of antibiotic therapy” for AOM, it is the most common reason for the prescription of antibiotics in children.4,6 A Cochrane review showed that antibiotics have no effect on recurrence of AOM or complications, including hearing impairment.5 The same review showed no pain reduction in 24 hours and only 30% pain reduction in 2 to 7 days with antibiotic use.5 Antibiotics clearly have a minimal role in providing pain relief for AOM.
Oral analgesics too slow
Oral analgesic use in AOM has been studied and has shown good results. We calculated the number needed to treat (1.0 divided by the absolute risk reduction) for both ibuprofen (number needed to treat [NNT]=5) and acetaminophen (NNT=6) from data in the 1996 trial by Bertin et al.9
It is a common practice in the United States to treat AOM with oral analgesics. However, the onset of pain relief with oral medications can be slow and the relief is generally not complete, so oral medications are not immediately helpful to meet the needs of our crying 3-year-old patient and his exhausted mother.
Topical anesthetics
To our knowledge, prior evidence on the efficacy of topical anesthetics is limited to 1 placebo-controlled trial. A randomized trial by Hoberman et al,10 with 54 subjects, showed a statistically significant 25% reduction in pain with the analgesic drops Auralgan (containing antipyrine, benzocaine, and glycerine) at 30 minutes when compared with olive oil. A 2006 Cochrane review11 did not include the Bolt et al trial1 described in this PURL, but did include the Hoberman trial10 and 3 trials that compared a topical anesthetic with naturopathic herbal ear drops for AOM pain, and the review concluded that evidence was insufficient.
Topical anesthetic plus oraI analgesia for earache relief
Bolt P et al.1
STUDY SUMMARY: Pain measured by visual analogue, Bieri faces scales
This double-blind, randomized, placebo-controlled trial1 compared aqueous lidocaine 2% drops with saline drops in the ear, for reducing pain due to AOM in patients 3 to 17 years of age. The trial was conducted at an Australian children’s hospital emergency room. The study evaluated “lignocaine,” the name for lidocaine in Australia.
Emergency physicians instilled 3 drops of either lidocaine or saline into the affected ear in the 2 groups (n=31 in the study group and n=32 in the placebo group). Patients, parents, treating physicians, and staff administering ear drops and assessing pain were blinded to group assignment. Doctors measured pain at baseline and after 30 minutes and patients measured pain at baseline, 10, 20, and 30 minutes after the drops were instilled, using the Bieri faces pain scale and a visual analogue scale.12
Lidocaine reduced pain scores by 50% from baseline at 10 and 30 minutes compared with saline. No serious side effects were noted at 30 minutes, although 3 patients in the lidocaine group complained of mild dizziness the next day. The treating physician prescribed paracetamol (equivalent to acetaminophen) for participants in both the lidocaine and the placebo group at their discretion. The proportion given paracetamol was similar in both groups.
WHAT’S NEW: Pain relief is immediate
Family physicians have used topical anethestics for otitis externa for decades. This RCT adds evidence that topical anesthetics are useful for providing immediate pain relief from AOM, as well. The 2004 guidelines from the American Academy of Pediatrics and the American Academy of Family Physicians indicate that management of AOM should include the assessment and treatment of pain.
We think that topical agents such as lidocaine and benzocaine are useful adjuncts to oral analgesics in providing immediate pain relief, especially in the face of evidence showing that antibiotics do not offer significant pain relief.
Previous studies have shown that aqueous lidocaine is ineffective on uninflamed tympanic membrane.13 The results of this study are consistent with increased uptake of the drug through the inflamed tympanic membrane.
CAVEATS: Children >3 years studied
This trial included only children older than 3 years, so the results may not apply to younger children and infants.
This essentially was a study of ear pain treatment, which, in our view, does not detract from the clinical usefulness of the findings. Topical anesthetics seem to be useful for ear pain in general.
Concurrent analgesics
Some variability existed in the oral analgesics the children received, as these agents were given at the discretion of the parents and treating physicians. We think that this does not detract from the study findings, as it represents a practical, real-world setting, which is desirable in an effectiveness RCT. Moreover, the extent of pain reduction was over and above that conferred by analgesic administration.
CHALLENGES TO IMPLEMENTATION: Lidocaine is not sold in a dropper
Aqueous lidocaine is not sold in a bottle with a dropper: our search on www.drugstore.com and www.drugs.com did not yield an otic preparation with only aqueous lidocaine. However, 2% injectable lidocaine, which is readily available, can be used with a dropper. Aqueous lidocaine can be compounded at a compounding pharmacy and placed in a bottle with a dropper.
Benzocaine might be a suitable substitute
In preparing this PURL, we learned from several colleagues that they always keep a bottle of benzocaine in their pocket and they apply the drops to the ears of their pediatric patients with AOM when they see them in their offices or in the emergency department.
Benzocaine is available in various brand names (eg, Auralgan, Americaine, A/B otic drops, among others). These are oil suspensions and not an aqueous solution as used in this study, so it would be important not to use these preparations in the presence of a ruptured tympanic membrane because the oil suspension may not be absorbed. The aqueous solution will be absorbed so it can be used even if a ruptured tympanic membrane is suspected.
In most situations rupture of the tympanic membrane gives immediate pain relief. However, in some, the pain persists and it may be difficult to tell if the tympanic membrane has ruptured or the debris and pus is from otitis externa. In those situations, the aqueous lidocaine solution might be preferred.
Should parents give drops at home?
This study does not address home use of these drops. However, benzocaine preparations have been used safely for many years for otitis externa at home, and we cannot think of any reason why drops could not be prescribed for home use in acute otitis media.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Bolt P, Barnett P, Babl FE, Sharwood LN. Topical lignocaine for pain relief in acute otitis media: results of a double-blind placebo-controlled randomised trial. Arch Dis Child. 2008;93:40-44.
2. Teele DW, Klein JO, Rosner B. Epidemiology of otitis media during the first seven years of life in children in greater Boston: a prospective, cohort study. J Infect Dis. 1989;160:83-94.
3. Arnold J. Otitis media and its complications. In: Nelson W, Behrman R, Kliegman R, Arvin A, eds. Nelson Textbook of Pediatrics. 15th ed. Philadelphia: Saunders; 1996:1814-1824.
4. Chan LS, Takata GS, Shekelle P, Morton SC, Mason W, Marcy SM. Evidence assessment of management of acute otitis media: II. Research gaps and priorities for future research. Pediatrics. 2001;108:248-254.
5. Glasziou PP, Del Mar CB, Sanders SL, Hayem M. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2004;(1):CD000219.
6. Hendley JO. Clinical practice. Otitis media. N Engl J Med. 2002;347:1169-1174.
7. Rovers MM, Glasziou P, Appelman CL, et al. Antibiotics for acute otitis media: a meta-analysis with individual patient data. Lancet. 2006;368:1429-1435.
8. Gasper K, St Anna L, Montgomery L. Clinical inquiries. Are antibiotics effective for otitis media with effusion? J Fam Pract. 2003;52:321-323.
9. Bertin L, Pons G, d’Athis P, et al. A randomized, double-blind, multicentre controlled trial of ibuprofen versus acetaminophen and placebo for symptoms of acute otitis media in children. Fundam Clin Pharmacol. 1996;10:387-392.
10. Hoberman A, Paradise JL, Reynolds EA, Urkin J. Efficacy of Auralgan for treating ear pain in children with acute otitis media. Arch Pediatr Adolesc Med. 1997;151:675-678.
11. Cochrane Database Syst Rev 2006 Jul 19;3: CD005657.
12. Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The Faces Pain Scale-Revised: toward a common metric in pediatric pain measurement. Pain. 2001;93:173-183.
13. Moller A, Grontved A. Topical anaesthesia of the normal tympanic membrane: a controlled clinical trial of different suspensions of lidocaine. ORL J Otorhinolaryngol Relat Spec. 1990;52:168-173.
1. Bolt P, Barnett P, Babl FE, Sharwood LN. Topical lignocaine for pain relief in acute otitis media: results of a double-blind placebo-controlled randomised trial. Arch Dis Child. 2008;93:40-44.
2. Teele DW, Klein JO, Rosner B. Epidemiology of otitis media during the first seven years of life in children in greater Boston: a prospective, cohort study. J Infect Dis. 1989;160:83-94.
3. Arnold J. Otitis media and its complications. In: Nelson W, Behrman R, Kliegman R, Arvin A, eds. Nelson Textbook of Pediatrics. 15th ed. Philadelphia: Saunders; 1996:1814-1824.
4. Chan LS, Takata GS, Shekelle P, Morton SC, Mason W, Marcy SM. Evidence assessment of management of acute otitis media: II. Research gaps and priorities for future research. Pediatrics. 2001;108:248-254.
5. Glasziou PP, Del Mar CB, Sanders SL, Hayem M. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev. 2004;(1):CD000219.
6. Hendley JO. Clinical practice. Otitis media. N Engl J Med. 2002;347:1169-1174.
7. Rovers MM, Glasziou P, Appelman CL, et al. Antibiotics for acute otitis media: a meta-analysis with individual patient data. Lancet. 2006;368:1429-1435.
8. Gasper K, St Anna L, Montgomery L. Clinical inquiries. Are antibiotics effective for otitis media with effusion? J Fam Pract. 2003;52:321-323.
9. Bertin L, Pons G, d’Athis P, et al. A randomized, double-blind, multicentre controlled trial of ibuprofen versus acetaminophen and placebo for symptoms of acute otitis media in children. Fundam Clin Pharmacol. 1996;10:387-392.
10. Hoberman A, Paradise JL, Reynolds EA, Urkin J. Efficacy of Auralgan for treating ear pain in children with acute otitis media. Arch Pediatr Adolesc Med. 1997;151:675-678.
11. Cochrane Database Syst Rev 2006 Jul 19;3: CD005657.
12. Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I, Goodenough B. The Faces Pain Scale-Revised: toward a common metric in pediatric pain measurement. Pain. 2001;93:173-183.
13. Moller A, Grontved A. Topical anaesthesia of the normal tympanic membrane: a controlled clinical trial of different suspensions of lidocaine. ORL J Otorhinolaryngol Relat Spec. 1990;52:168-173.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Hypertension with metabolic syndrome: Think thiazides are old hat? ALLHAT says think again
ILLUSTRATIVE CASE
Your new patient is a 57-year-old African American man. His blood pressure is 150/95 mm Hg, fasting glucose 115 mg/dL, body mass index 32, and triglycerides 155 mg/dL; he is on no prior medications. During the course of his care you diagnose hypertension with metabolic syndrome and decide to recommend an antihypertensive. Thiazide-type diuretics are your standard initial therapy, but this patient has metabolic syndrome, and you know that certain antihypertensive agents have a more favorable metabolic profile than thiazide diuretics. Furthermore, metabolic differences among races have been touted as reason to use other agents in black patients. Should you recommend a thiazide diuretic, or another agent?
Until now, we’ve had no simple approach to treating hypertension in patients with metabolic syndrome—and half or more of our hypertensive patients over the age of 55 have this disorder.
Now, however, we can base decisions on clinical outcomes data from a subgroup analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT).1 This new subgroup analysis supports use of thiazide-type diuretics in these patients—particularly in black patients—despite the more favorable metabolic profile of calcium channel blockers, alpha-blockers, and angiotensin-converting enzyme (ACE) inhibitors.
Cost is no longer as big a factor as it once was, now that ACE inhibitors and alpha-blockers, as well as thiazide diuretics, are available generically.
Does a better metabolic profile improve outcomes?
We have had reason to be concerned about the metabolic adverse effects of thiazide-type diuretics in the past. Studies published before this ALLHAT subgroup analysis showed that hydrochlorothiazide for essential hypertension had adverse effects on potassium, glucose, and lipid metabolism. Some speculated that these changes aggravate the metabolic changes in early diabetes2-4 and may contribute to increased coronary heart disease risk.5,6
FIGURE
Outcomes favor thiazides
We know many physicians who have adopted thiazide-type diuretics as the first-line treatment for hypertension in metabolic syndrome, but until now, data have been inadequate to support this decision.
A subgroup analysis from the ALLHAT1 concludes: “The ALLHAT findings fail to support the preference for calcium channel blockers, alpha-blockers, or angiotensin-converting enzyme inhibitors compared with thiazide-type diuretics in patients with the metabolic syndrome, despite their more favorable metabolic profiles. This was particularly true for black participants.”
| Hypertension Blood pressure target for patients enrolled in the ALLHAT was <140/90 mm Hg | Metabolic syndrome, in the subgroup analysis, was defined as hypertension plus 2 of the following risk factors for coronary heart disease: | ||
| 1. Obesity Body mass index at least 30 | 2. Lipid disorder Fasting triglyceride level >150 mg/dL and high-density lipoprotein cholesterol level <40 mg/dL in men, or <50 mg/dL in women | 3. Glycemic disorder Fasting glucose level >100 mg/dL, or nonfasting glucose level >200 mg/dL, or history of diabetes | |
ACE inhibitors and ARBs
The metabolic benefits of ACE inhibitors and angiotensin-receptor blockers (ARBs) are widely known. In comparative studies prior to this ALLHAT subgroup analysis, ACE inhibitors were thought to be preferable to thiazide diuretics and beta-blockers for patients with obesity7 or the metabolic syndrome.8 These agents also protect against diabetic nephropathy.9 Other studies attribute additional vascular benefits to ACE inhibitors,10 beyond that of lowering blood pressure.
A 2005 meta-analysis by Abuissa et al11 showed that ACE inhibitors and ARBs were associated with significant reductions in the incidence of newly diagnosed diabetes, which, in turn, might lead to reduced heart disease. That report concluded that use of ACE inhibitors or ARBs should be considered in patients with prediabetic conditions such as metabolic syndrome, hypertension, impaired fasting glucose, family history of diabetes, obesity, congestive heart failure, or coronary heart disease.
Calcium-channel blockers and alpha-blockers
Calcium-channel blockers and alpha-blockers also do not appear to have the adverse metabolic effects of thiazides, and have also been advocated over beta-blockers and thiazides for hypertensive patients with metabolic syndrome.12-15
Racial differences
In a consensus statement developed before the findings from the ALLHAT subgroup analysis were available, it was noted that racial differences in metabolic syndrome may make the selection of antihypertensive agents particularly important in African American patients.16
ALLHAT and JNC7 recommendations
The 2002 ALLHAT demonstrated that chlorthalidone (a thiazide-type diuretic) is superior to lisinopril, amlodipine, and doxazosin in preventing 1 or more major forms of cardiovascular disease. No difference was observed, however, for fatal coronary heart disease, nonfatal myocardial infarction, or all-cause mortality.17 These findings persisted in sub-group analyses stratified by race, diabetic status, and level of renal function, but ALLHAT did not identify patients with metabolic syndrome a priori.
The ALLHAT influenced the 2003 Joint National Commission VII (JNC7) Report, which recommends thiazide diuretics for first-line treatment of hypertension in the absence of compelling indications to begin an alternative antihypertensive agent.18
Special consideration, but no recommendation. The JNC7 Report mentions the metabolic syndrome as a special consideration, but does not explicitly recommend a first-line therapy other than thiazides.
Anecdotally, we know many physicians who have adopted thiazide-type diuretics as the first-line treatment for hypertension in metabolic syndrome, but until now, data have been inadequate to support this decision.
It is unclear to us how this conflicting information has played out in current practice. We know that many physicians already choose thiazides as their first-line agent for hypertensive patients with metabolic syndrome. And we suspect that many choose other agents.
We analyzed the National Ambulatory Medical Care Survey data (http://www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm) from 2004 and 2005 and found that only 3% to 5% of outpatients with diabetes and hypertension were taking thiazides at all (unpublished data). Metabolic syndrome is not a variable in this dataset, so we could not determine the use of thiazides in hypertension and metabolic syndrome.
Our informal polling of colleagues suggested that large numbers of hypertensive patients with metabolic syndrome are not currently receiving the more beneficial thiazides.
STUDY SUMMARY: Chlorthalidone outcomes were equivalent or better
Wright and colleagues analyzed a sub-group1 of the ALLHAT cohort, which consisted of 42,418 participants, aged ≥55, with hypertension and at least 1 other cardiovascular risk factor ( FIGURE ).
Patients were randomly assigned to therapy with chlorthalidone, amlodipine, lisinopril, or doxazosin. After randomization, if patients failed to reach the target blood pressure (<140/90 mm Hg) with their assigned therapy, they were started on atenolol, clonidine, or reserpine. If they required a third agent, they received hydralazine. The doxazosin arm was stopped early due to increased stroke and heart failure risk.
The ALLHAT was well done and designed for adequate power to evaluate clinical outcomes in racial subgroups, as well as the general population.
Outcomes were compared by race in hypertensive patients with and without metabolic syndrome.
A total of 23,077 (54%) patients met all criteria; 12,818 were black, 7327 (57%) of whom had metabolic syndrome.
Not surprisingly in a study of this size, the expected metabolic effects of all 4 antihypertensive agents were detected. Patients taking chlorthalidone had higher glucose levels (1–4 mg/dL) and higher levels of cholesterol, although these higher glucose and cholesterol levels were not statistically significant for all comparisons over time and between different drugs.
Outcomes in the chlorthalidone group were equivalent or superior to the 3 other therapies, generally. This pattern held true regardless of race ( TABLE ):
Heart failure rates were significantly higher in patients with metabolic syndrome across all treatments compared with chlorthalidone.
Combined cardiovascular disease rates were higher with lisinopril and doxazosin compared with chlorthalidone.
Stroke rates were higher among black participants only in the lisinopril group.
TABLE
Number needed to treat to prevent blood pressure-related adverse outcomes in patients with hypertension and metabolic syndrome
| NUMBER NEEDED TO TREAT (NNT)= number of patients that would need to take chlorthalidone to prevent 1 outcome, compared with the alternate drug (4.9 years of chlorthalidone instead of lisinopril or amlodipine or 3.2 years of chlorthalidone instead of doxazosin). Smaller numbers indicate a bigger effect. | ||||||
|---|---|---|---|---|---|---|
| OUTCOME | CHLORTHALIDONE VS AMLODIPINE | CHLORTHALIDONE VS LISINOPRIL | CHLORTHALIDONE VS DOXAZOSIN | |||
| Black | Non-black | Black | Non-black | Black | Non-black | |
| Combined cardiovascular disease | 22 | NS | 18 | 53 | 14 | 34 |
| Stroke | NS | -111 | 59 | NS | 37 | NS |
| Heart failure | 29 | 48 | 28 | 143 | 28 | 25 |
| All-cause mortality | NS | NS | NS | NS | NS | NS |
| NS=not significant. | ||||||
| Source: The authors calculated the NNTs from the event rates reported.1 | ||||||
WHAT’S NEW: Most effective, least expensive
First-line use of thiazide diuretics for hypertension gained major support from the findings of the first ALLHAT report, published in 2002. A year later, JNC7 supported the practice. Yet questions have persisted about whether the choice of initial antihypertensive agent in patients with metabolic syndrome warrants special consideration.
The difference for one patient is small, but when you consider the high prevalence of hypertension, the cumulative benefit at a population level is significant. This subgroup analysis confirms that there is no harm, and potentially a small benefit, in using chlorthalidone as a first-line agent for treating hypertension in patients with metabolic syndrome, regardless of race—despite the measurable and presumably adverse effects of diuretic agents on metabolic measurements.
How large is the benefit of first-line thiazides, overall?
Although, statistically, the relative risks (RR) are not large, the sheer number of patients means that there is significant benefit to the selection of thiazides as first-line treatment in most patients.
CAVEATS: Is stroke a concern? Was follow-up sufficient?
In this study, the only finding of harm in the diuretic group was an increased risk for stroke compared with amlodipine among non-black patients with metabolic syndrome. While this finding does raise some uncertainty, we still think that, on balance, thiazides are the most beneficial, even in this subgroup, as there was a larger benefit in preventing heart failure.
Another theoretical possibility is that follow-up was too short to demonstrate harm from the metabolic effects of thiazides. However, the metabolic effects of thiazides are very small and we believe that the evidence of benefit shown during this study period easily outweighs any such theoretical harms.
We also assume that hydrochlorothiazide, a commonly prescribed thiazide, has the same benefits as chlorthalidone, the medication studied.
Most ALLHAT participants with metabolic syndrome already had diabetes: 67.6% of black participants and 51.8% of non-black participants. Another sub-group analysis of the ALLHAT studied patients with metabolic syndrome without diabetes, and found similar results.19
Of note, lisinopril reduced the onset of diabetes over 5 years (number needed to treat [NNT]=22.2), at the cost of increased heart failure (RR=1.31; 95% confidence interval [CI], 1.04-1.64) and combined cardiovascular disease (RR=1.19; 95% CI, 1.07-1.32). This potentially confounds the claim that thiazides are effective in preventing diabetes, since so many people had it to begin with.
The criteria for metabolic syndrome did not include waist circumference, which is the National Cholesterol Education Program definition. The World Health Organization definition, however, does allow substitution of BMI. Purists would have you believe waist circumference is necessary. In practice, we have come to use BMI as an adequate surrogate. Some say it has, in fact, replaced waist circumference.
CHALLENGES TO IMPLEMENTATION: Inertia
Few interventions are as simple as this. Thiazide diuretics are well tolerated, need to be taken only once daily, and are inexpensive. Because generics are available, little to no pharmaceutical marketing is done to promote their use. The major barriers to implementing this practice may be overcoming clinical inertia, and the message of pharmaceutical marketing on behalf of the more expensive alternatives.
Acknowledgement
We acknowledge Sofia Medvedev, PhD, University HealthSystem Consortium, Oak Brook, IL for analysis of the National Ambulatory Medical Care Survey data.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at here.
1. Wright JT, Jr, Harris-Haywood S, Pressel S, et al. Clinical outcomes by race in hypertensive patients with and without the metabolic syndrome: Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Arch Intern Med. 2008;168:207-217.
2. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326:1427.-
3. Eberly LE, Cohen JD, Prineas R, Yang L. Intervention Trial Research group. Impact of incident diabetes and incident nonfatal cardiovascular disease on 18-year mortality: the Multiple Risk Factor Intervention Trial experience. Diabetes Care. 2003;26:848-854.
4. Pollare T, Lithell H, Berne C. A comparison of the effects of hydrochlorothiazide and captopril on glucose and lipid metabolism in patients with hyper-tension. N Engl J Med. 1989;321:868-873.
5. Mancia G, Grassi G, Zanchetti A. New-onset diabetes and antihypertensive drugs. J Hypertens. 2006;24:3-10.
6. Skarfors ET, Lithell HO, Selinus I, Aberg H. Do antihypertensive drugs precipitate diabetes? BMJ. 1989;298:1147-1152
7. Scholze J, Grimm E, Herrmann D, Unger T, Kintscher U. Optimal treatment of obesity-related hypertension: the Hypertension-Obesity-Sibutra-mine (HOS) study. Circulation. 2007;115:1991-1998.
8. Bakris G, Molitch M, Hewkin A, et al. STAR Investigators. Differences in glucose tolerance between fixed-dose antihypertensive drug combinations in people with metabolic syndrome. Diabetes Care. 2006;29:2592-2597.
9. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med. 1993;329:1456-1462.
10. Gianni M, Bosch J, Pogue J, et al. Effect of long-term ACE-inhibitor therapy in elderly vascular disease patients. Eur Heart J. 2007;28:1382-1388.
11. Abuissa H, Jones PG, Marso SP, O’Keefe JH Jr. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers for prevention of type 2 diabetes: a meta-analysis of randomized clinical trials. J Am Coll Cardiol. 2005;46:821-826.
12. Mykkänen L, Kuusisto J, Pyörälä K, Laakso M, Haffner SM. Increased risk of non-insulin-dependent diabetes mellitus in elderly hypertensive subjects. J Hypertens. 1994;12:1425-1432.
13. Giles TD, Sander GE. Pathophysiologic, diagnostic, and therapeutic aspects of the metabolic syndrome. J Clin Hypertens (Greenwich). 2005;7:669-678.
14. Mancia G. The association of hypertension and diabetes: prevalence, cardiovascular risk and protection by blood pressure reduction. Acta Diabetol. 2005;42(suppl 1):S17-S25.
15. Wagh A, Stone NJ. Treatment of metabolic syndrome. Expert Rev Cardiovasc Ther. 2004;2:213-228.
16. Hall WD, Clark LT, Wenger NK, et al. African-American Lipid and Cardiovascular Council. The metabolic syndrome in African Americans: a review. Ethn Dis. 2003;13:414-428.
17. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group, Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981-2997.
18. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Bethesda, MD: US Department of Health and Human Services, National Heart, Lung, and Blood Institute; December 2003. Available at: http://www.nhlbi.nih.gov/guidelines/hypertension. Accessed March 31, 2008.
19. Black HR, Davis B, Barzilay J, et al. Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Metabolic and clinical outcomes in nondiabetic individuals with the metabolic syndrome assigned to chlorthalidone, amlodipine, or lisinopril as initial treatment for hypertension: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Diabetes Care. 2008;31:353-360.
ILLUSTRATIVE CASE
Your new patient is a 57-year-old African American man. His blood pressure is 150/95 mm Hg, fasting glucose 115 mg/dL, body mass index 32, and triglycerides 155 mg/dL; he is on no prior medications. During the course of his care you diagnose hypertension with metabolic syndrome and decide to recommend an antihypertensive. Thiazide-type diuretics are your standard initial therapy, but this patient has metabolic syndrome, and you know that certain antihypertensive agents have a more favorable metabolic profile than thiazide diuretics. Furthermore, metabolic differences among races have been touted as reason to use other agents in black patients. Should you recommend a thiazide diuretic, or another agent?
Until now, we’ve had no simple approach to treating hypertension in patients with metabolic syndrome—and half or more of our hypertensive patients over the age of 55 have this disorder.
Now, however, we can base decisions on clinical outcomes data from a subgroup analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT).1 This new subgroup analysis supports use of thiazide-type diuretics in these patients—particularly in black patients—despite the more favorable metabolic profile of calcium channel blockers, alpha-blockers, and angiotensin-converting enzyme (ACE) inhibitors.
Cost is no longer as big a factor as it once was, now that ACE inhibitors and alpha-blockers, as well as thiazide diuretics, are available generically.
Does a better metabolic profile improve outcomes?
We have had reason to be concerned about the metabolic adverse effects of thiazide-type diuretics in the past. Studies published before this ALLHAT subgroup analysis showed that hydrochlorothiazide for essential hypertension had adverse effects on potassium, glucose, and lipid metabolism. Some speculated that these changes aggravate the metabolic changes in early diabetes2-4 and may contribute to increased coronary heart disease risk.5,6
FIGURE
Outcomes favor thiazides
We know many physicians who have adopted thiazide-type diuretics as the first-line treatment for hypertension in metabolic syndrome, but until now, data have been inadequate to support this decision.
A subgroup analysis from the ALLHAT1 concludes: “The ALLHAT findings fail to support the preference for calcium channel blockers, alpha-blockers, or angiotensin-converting enzyme inhibitors compared with thiazide-type diuretics in patients with the metabolic syndrome, despite their more favorable metabolic profiles. This was particularly true for black participants.”
| Hypertension Blood pressure target for patients enrolled in the ALLHAT was <140/90 mm Hg | Metabolic syndrome, in the subgroup analysis, was defined as hypertension plus 2 of the following risk factors for coronary heart disease: | ||
| 1. Obesity Body mass index at least 30 | 2. Lipid disorder Fasting triglyceride level >150 mg/dL and high-density lipoprotein cholesterol level <40 mg/dL in men, or <50 mg/dL in women | 3. Glycemic disorder Fasting glucose level >100 mg/dL, or nonfasting glucose level >200 mg/dL, or history of diabetes | |
ACE inhibitors and ARBs
The metabolic benefits of ACE inhibitors and angiotensin-receptor blockers (ARBs) are widely known. In comparative studies prior to this ALLHAT subgroup analysis, ACE inhibitors were thought to be preferable to thiazide diuretics and beta-blockers for patients with obesity7 or the metabolic syndrome.8 These agents also protect against diabetic nephropathy.9 Other studies attribute additional vascular benefits to ACE inhibitors,10 beyond that of lowering blood pressure.
A 2005 meta-analysis by Abuissa et al11 showed that ACE inhibitors and ARBs were associated with significant reductions in the incidence of newly diagnosed diabetes, which, in turn, might lead to reduced heart disease. That report concluded that use of ACE inhibitors or ARBs should be considered in patients with prediabetic conditions such as metabolic syndrome, hypertension, impaired fasting glucose, family history of diabetes, obesity, congestive heart failure, or coronary heart disease.
Calcium-channel blockers and alpha-blockers
Calcium-channel blockers and alpha-blockers also do not appear to have the adverse metabolic effects of thiazides, and have also been advocated over beta-blockers and thiazides for hypertensive patients with metabolic syndrome.12-15
Racial differences
In a consensus statement developed before the findings from the ALLHAT subgroup analysis were available, it was noted that racial differences in metabolic syndrome may make the selection of antihypertensive agents particularly important in African American patients.16
ALLHAT and JNC7 recommendations
The 2002 ALLHAT demonstrated that chlorthalidone (a thiazide-type diuretic) is superior to lisinopril, amlodipine, and doxazosin in preventing 1 or more major forms of cardiovascular disease. No difference was observed, however, for fatal coronary heart disease, nonfatal myocardial infarction, or all-cause mortality.17 These findings persisted in sub-group analyses stratified by race, diabetic status, and level of renal function, but ALLHAT did not identify patients with metabolic syndrome a priori.
The ALLHAT influenced the 2003 Joint National Commission VII (JNC7) Report, which recommends thiazide diuretics for first-line treatment of hypertension in the absence of compelling indications to begin an alternative antihypertensive agent.18
Special consideration, but no recommendation. The JNC7 Report mentions the metabolic syndrome as a special consideration, but does not explicitly recommend a first-line therapy other than thiazides.
Anecdotally, we know many physicians who have adopted thiazide-type diuretics as the first-line treatment for hypertension in metabolic syndrome, but until now, data have been inadequate to support this decision.
It is unclear to us how this conflicting information has played out in current practice. We know that many physicians already choose thiazides as their first-line agent for hypertensive patients with metabolic syndrome. And we suspect that many choose other agents.
We analyzed the National Ambulatory Medical Care Survey data (http://www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm) from 2004 and 2005 and found that only 3% to 5% of outpatients with diabetes and hypertension were taking thiazides at all (unpublished data). Metabolic syndrome is not a variable in this dataset, so we could not determine the use of thiazides in hypertension and metabolic syndrome.
Our informal polling of colleagues suggested that large numbers of hypertensive patients with metabolic syndrome are not currently receiving the more beneficial thiazides.
STUDY SUMMARY: Chlorthalidone outcomes were equivalent or better
Wright and colleagues analyzed a sub-group1 of the ALLHAT cohort, which consisted of 42,418 participants, aged ≥55, with hypertension and at least 1 other cardiovascular risk factor ( FIGURE ).
Patients were randomly assigned to therapy with chlorthalidone, amlodipine, lisinopril, or doxazosin. After randomization, if patients failed to reach the target blood pressure (<140/90 mm Hg) with their assigned therapy, they were started on atenolol, clonidine, or reserpine. If they required a third agent, they received hydralazine. The doxazosin arm was stopped early due to increased stroke and heart failure risk.
The ALLHAT was well done and designed for adequate power to evaluate clinical outcomes in racial subgroups, as well as the general population.
Outcomes were compared by race in hypertensive patients with and without metabolic syndrome.
A total of 23,077 (54%) patients met all criteria; 12,818 were black, 7327 (57%) of whom had metabolic syndrome.
Not surprisingly in a study of this size, the expected metabolic effects of all 4 antihypertensive agents were detected. Patients taking chlorthalidone had higher glucose levels (1–4 mg/dL) and higher levels of cholesterol, although these higher glucose and cholesterol levels were not statistically significant for all comparisons over time and between different drugs.
Outcomes in the chlorthalidone group were equivalent or superior to the 3 other therapies, generally. This pattern held true regardless of race ( TABLE ):
Heart failure rates were significantly higher in patients with metabolic syndrome across all treatments compared with chlorthalidone.
Combined cardiovascular disease rates were higher with lisinopril and doxazosin compared with chlorthalidone.
Stroke rates were higher among black participants only in the lisinopril group.
TABLE
Number needed to treat to prevent blood pressure-related adverse outcomes in patients with hypertension and metabolic syndrome
| NUMBER NEEDED TO TREAT (NNT)= number of patients that would need to take chlorthalidone to prevent 1 outcome, compared with the alternate drug (4.9 years of chlorthalidone instead of lisinopril or amlodipine or 3.2 years of chlorthalidone instead of doxazosin). Smaller numbers indicate a bigger effect. | ||||||
|---|---|---|---|---|---|---|
| OUTCOME | CHLORTHALIDONE VS AMLODIPINE | CHLORTHALIDONE VS LISINOPRIL | CHLORTHALIDONE VS DOXAZOSIN | |||
| Black | Non-black | Black | Non-black | Black | Non-black | |
| Combined cardiovascular disease | 22 | NS | 18 | 53 | 14 | 34 |
| Stroke | NS | -111 | 59 | NS | 37 | NS |
| Heart failure | 29 | 48 | 28 | 143 | 28 | 25 |
| All-cause mortality | NS | NS | NS | NS | NS | NS |
| NS=not significant. | ||||||
| Source: The authors calculated the NNTs from the event rates reported.1 | ||||||
WHAT’S NEW: Most effective, least expensive
First-line use of thiazide diuretics for hypertension gained major support from the findings of the first ALLHAT report, published in 2002. A year later, JNC7 supported the practice. Yet questions have persisted about whether the choice of initial antihypertensive agent in patients with metabolic syndrome warrants special consideration.
The difference for one patient is small, but when you consider the high prevalence of hypertension, the cumulative benefit at a population level is significant. This subgroup analysis confirms that there is no harm, and potentially a small benefit, in using chlorthalidone as a first-line agent for treating hypertension in patients with metabolic syndrome, regardless of race—despite the measurable and presumably adverse effects of diuretic agents on metabolic measurements.
How large is the benefit of first-line thiazides, overall?
Although, statistically, the relative risks (RR) are not large, the sheer number of patients means that there is significant benefit to the selection of thiazides as first-line treatment in most patients.
CAVEATS: Is stroke a concern? Was follow-up sufficient?
In this study, the only finding of harm in the diuretic group was an increased risk for stroke compared with amlodipine among non-black patients with metabolic syndrome. While this finding does raise some uncertainty, we still think that, on balance, thiazides are the most beneficial, even in this subgroup, as there was a larger benefit in preventing heart failure.
Another theoretical possibility is that follow-up was too short to demonstrate harm from the metabolic effects of thiazides. However, the metabolic effects of thiazides are very small and we believe that the evidence of benefit shown during this study period easily outweighs any such theoretical harms.
We also assume that hydrochlorothiazide, a commonly prescribed thiazide, has the same benefits as chlorthalidone, the medication studied.
Most ALLHAT participants with metabolic syndrome already had diabetes: 67.6% of black participants and 51.8% of non-black participants. Another sub-group analysis of the ALLHAT studied patients with metabolic syndrome without diabetes, and found similar results.19
Of note, lisinopril reduced the onset of diabetes over 5 years (number needed to treat [NNT]=22.2), at the cost of increased heart failure (RR=1.31; 95% confidence interval [CI], 1.04-1.64) and combined cardiovascular disease (RR=1.19; 95% CI, 1.07-1.32). This potentially confounds the claim that thiazides are effective in preventing diabetes, since so many people had it to begin with.
The criteria for metabolic syndrome did not include waist circumference, which is the National Cholesterol Education Program definition. The World Health Organization definition, however, does allow substitution of BMI. Purists would have you believe waist circumference is necessary. In practice, we have come to use BMI as an adequate surrogate. Some say it has, in fact, replaced waist circumference.
CHALLENGES TO IMPLEMENTATION: Inertia
Few interventions are as simple as this. Thiazide diuretics are well tolerated, need to be taken only once daily, and are inexpensive. Because generics are available, little to no pharmaceutical marketing is done to promote their use. The major barriers to implementing this practice may be overcoming clinical inertia, and the message of pharmaceutical marketing on behalf of the more expensive alternatives.
Acknowledgement
We acknowledge Sofia Medvedev, PhD, University HealthSystem Consortium, Oak Brook, IL for analysis of the National Ambulatory Medical Care Survey data.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at here.
ILLUSTRATIVE CASE
Your new patient is a 57-year-old African American man. His blood pressure is 150/95 mm Hg, fasting glucose 115 mg/dL, body mass index 32, and triglycerides 155 mg/dL; he is on no prior medications. During the course of his care you diagnose hypertension with metabolic syndrome and decide to recommend an antihypertensive. Thiazide-type diuretics are your standard initial therapy, but this patient has metabolic syndrome, and you know that certain antihypertensive agents have a more favorable metabolic profile than thiazide diuretics. Furthermore, metabolic differences among races have been touted as reason to use other agents in black patients. Should you recommend a thiazide diuretic, or another agent?
Until now, we’ve had no simple approach to treating hypertension in patients with metabolic syndrome—and half or more of our hypertensive patients over the age of 55 have this disorder.
Now, however, we can base decisions on clinical outcomes data from a subgroup analysis of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT).1 This new subgroup analysis supports use of thiazide-type diuretics in these patients—particularly in black patients—despite the more favorable metabolic profile of calcium channel blockers, alpha-blockers, and angiotensin-converting enzyme (ACE) inhibitors.
Cost is no longer as big a factor as it once was, now that ACE inhibitors and alpha-blockers, as well as thiazide diuretics, are available generically.
Does a better metabolic profile improve outcomes?
We have had reason to be concerned about the metabolic adverse effects of thiazide-type diuretics in the past. Studies published before this ALLHAT subgroup analysis showed that hydrochlorothiazide for essential hypertension had adverse effects on potassium, glucose, and lipid metabolism. Some speculated that these changes aggravate the metabolic changes in early diabetes2-4 and may contribute to increased coronary heart disease risk.5,6
FIGURE
Outcomes favor thiazides
We know many physicians who have adopted thiazide-type diuretics as the first-line treatment for hypertension in metabolic syndrome, but until now, data have been inadequate to support this decision.
A subgroup analysis from the ALLHAT1 concludes: “The ALLHAT findings fail to support the preference for calcium channel blockers, alpha-blockers, or angiotensin-converting enzyme inhibitors compared with thiazide-type diuretics in patients with the metabolic syndrome, despite their more favorable metabolic profiles. This was particularly true for black participants.”
| Hypertension Blood pressure target for patients enrolled in the ALLHAT was <140/90 mm Hg | Metabolic syndrome, in the subgroup analysis, was defined as hypertension plus 2 of the following risk factors for coronary heart disease: | ||
| 1. Obesity Body mass index at least 30 | 2. Lipid disorder Fasting triglyceride level >150 mg/dL and high-density lipoprotein cholesterol level <40 mg/dL in men, or <50 mg/dL in women | 3. Glycemic disorder Fasting glucose level >100 mg/dL, or nonfasting glucose level >200 mg/dL, or history of diabetes | |
ACE inhibitors and ARBs
The metabolic benefits of ACE inhibitors and angiotensin-receptor blockers (ARBs) are widely known. In comparative studies prior to this ALLHAT subgroup analysis, ACE inhibitors were thought to be preferable to thiazide diuretics and beta-blockers for patients with obesity7 or the metabolic syndrome.8 These agents also protect against diabetic nephropathy.9 Other studies attribute additional vascular benefits to ACE inhibitors,10 beyond that of lowering blood pressure.
A 2005 meta-analysis by Abuissa et al11 showed that ACE inhibitors and ARBs were associated with significant reductions in the incidence of newly diagnosed diabetes, which, in turn, might lead to reduced heart disease. That report concluded that use of ACE inhibitors or ARBs should be considered in patients with prediabetic conditions such as metabolic syndrome, hypertension, impaired fasting glucose, family history of diabetes, obesity, congestive heart failure, or coronary heart disease.
Calcium-channel blockers and alpha-blockers
Calcium-channel blockers and alpha-blockers also do not appear to have the adverse metabolic effects of thiazides, and have also been advocated over beta-blockers and thiazides for hypertensive patients with metabolic syndrome.12-15
Racial differences
In a consensus statement developed before the findings from the ALLHAT subgroup analysis were available, it was noted that racial differences in metabolic syndrome may make the selection of antihypertensive agents particularly important in African American patients.16
ALLHAT and JNC7 recommendations
The 2002 ALLHAT demonstrated that chlorthalidone (a thiazide-type diuretic) is superior to lisinopril, amlodipine, and doxazosin in preventing 1 or more major forms of cardiovascular disease. No difference was observed, however, for fatal coronary heart disease, nonfatal myocardial infarction, or all-cause mortality.17 These findings persisted in sub-group analyses stratified by race, diabetic status, and level of renal function, but ALLHAT did not identify patients with metabolic syndrome a priori.
The ALLHAT influenced the 2003 Joint National Commission VII (JNC7) Report, which recommends thiazide diuretics for first-line treatment of hypertension in the absence of compelling indications to begin an alternative antihypertensive agent.18
Special consideration, but no recommendation. The JNC7 Report mentions the metabolic syndrome as a special consideration, but does not explicitly recommend a first-line therapy other than thiazides.
Anecdotally, we know many physicians who have adopted thiazide-type diuretics as the first-line treatment for hypertension in metabolic syndrome, but until now, data have been inadequate to support this decision.
It is unclear to us how this conflicting information has played out in current practice. We know that many physicians already choose thiazides as their first-line agent for hypertensive patients with metabolic syndrome. And we suspect that many choose other agents.
We analyzed the National Ambulatory Medical Care Survey data (http://www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm) from 2004 and 2005 and found that only 3% to 5% of outpatients with diabetes and hypertension were taking thiazides at all (unpublished data). Metabolic syndrome is not a variable in this dataset, so we could not determine the use of thiazides in hypertension and metabolic syndrome.
Our informal polling of colleagues suggested that large numbers of hypertensive patients with metabolic syndrome are not currently receiving the more beneficial thiazides.
STUDY SUMMARY: Chlorthalidone outcomes were equivalent or better
Wright and colleagues analyzed a sub-group1 of the ALLHAT cohort, which consisted of 42,418 participants, aged ≥55, with hypertension and at least 1 other cardiovascular risk factor ( FIGURE ).
Patients were randomly assigned to therapy with chlorthalidone, amlodipine, lisinopril, or doxazosin. After randomization, if patients failed to reach the target blood pressure (<140/90 mm Hg) with their assigned therapy, they were started on atenolol, clonidine, or reserpine. If they required a third agent, they received hydralazine. The doxazosin arm was stopped early due to increased stroke and heart failure risk.
The ALLHAT was well done and designed for adequate power to evaluate clinical outcomes in racial subgroups, as well as the general population.
Outcomes were compared by race in hypertensive patients with and without metabolic syndrome.
A total of 23,077 (54%) patients met all criteria; 12,818 were black, 7327 (57%) of whom had metabolic syndrome.
Not surprisingly in a study of this size, the expected metabolic effects of all 4 antihypertensive agents were detected. Patients taking chlorthalidone had higher glucose levels (1–4 mg/dL) and higher levels of cholesterol, although these higher glucose and cholesterol levels were not statistically significant for all comparisons over time and between different drugs.
Outcomes in the chlorthalidone group were equivalent or superior to the 3 other therapies, generally. This pattern held true regardless of race ( TABLE ):
Heart failure rates were significantly higher in patients with metabolic syndrome across all treatments compared with chlorthalidone.
Combined cardiovascular disease rates were higher with lisinopril and doxazosin compared with chlorthalidone.
Stroke rates were higher among black participants only in the lisinopril group.
TABLE
Number needed to treat to prevent blood pressure-related adverse outcomes in patients with hypertension and metabolic syndrome
| NUMBER NEEDED TO TREAT (NNT)= number of patients that would need to take chlorthalidone to prevent 1 outcome, compared with the alternate drug (4.9 years of chlorthalidone instead of lisinopril or amlodipine or 3.2 years of chlorthalidone instead of doxazosin). Smaller numbers indicate a bigger effect. | ||||||
|---|---|---|---|---|---|---|
| OUTCOME | CHLORTHALIDONE VS AMLODIPINE | CHLORTHALIDONE VS LISINOPRIL | CHLORTHALIDONE VS DOXAZOSIN | |||
| Black | Non-black | Black | Non-black | Black | Non-black | |
| Combined cardiovascular disease | 22 | NS | 18 | 53 | 14 | 34 |
| Stroke | NS | -111 | 59 | NS | 37 | NS |
| Heart failure | 29 | 48 | 28 | 143 | 28 | 25 |
| All-cause mortality | NS | NS | NS | NS | NS | NS |
| NS=not significant. | ||||||
| Source: The authors calculated the NNTs from the event rates reported.1 | ||||||
WHAT’S NEW: Most effective, least expensive
First-line use of thiazide diuretics for hypertension gained major support from the findings of the first ALLHAT report, published in 2002. A year later, JNC7 supported the practice. Yet questions have persisted about whether the choice of initial antihypertensive agent in patients with metabolic syndrome warrants special consideration.
The difference for one patient is small, but when you consider the high prevalence of hypertension, the cumulative benefit at a population level is significant. This subgroup analysis confirms that there is no harm, and potentially a small benefit, in using chlorthalidone as a first-line agent for treating hypertension in patients with metabolic syndrome, regardless of race—despite the measurable and presumably adverse effects of diuretic agents on metabolic measurements.
How large is the benefit of first-line thiazides, overall?
Although, statistically, the relative risks (RR) are not large, the sheer number of patients means that there is significant benefit to the selection of thiazides as first-line treatment in most patients.
CAVEATS: Is stroke a concern? Was follow-up sufficient?
In this study, the only finding of harm in the diuretic group was an increased risk for stroke compared with amlodipine among non-black patients with metabolic syndrome. While this finding does raise some uncertainty, we still think that, on balance, thiazides are the most beneficial, even in this subgroup, as there was a larger benefit in preventing heart failure.
Another theoretical possibility is that follow-up was too short to demonstrate harm from the metabolic effects of thiazides. However, the metabolic effects of thiazides are very small and we believe that the evidence of benefit shown during this study period easily outweighs any such theoretical harms.
We also assume that hydrochlorothiazide, a commonly prescribed thiazide, has the same benefits as chlorthalidone, the medication studied.
Most ALLHAT participants with metabolic syndrome already had diabetes: 67.6% of black participants and 51.8% of non-black participants. Another sub-group analysis of the ALLHAT studied patients with metabolic syndrome without diabetes, and found similar results.19
Of note, lisinopril reduced the onset of diabetes over 5 years (number needed to treat [NNT]=22.2), at the cost of increased heart failure (RR=1.31; 95% confidence interval [CI], 1.04-1.64) and combined cardiovascular disease (RR=1.19; 95% CI, 1.07-1.32). This potentially confounds the claim that thiazides are effective in preventing diabetes, since so many people had it to begin with.
The criteria for metabolic syndrome did not include waist circumference, which is the National Cholesterol Education Program definition. The World Health Organization definition, however, does allow substitution of BMI. Purists would have you believe waist circumference is necessary. In practice, we have come to use BMI as an adequate surrogate. Some say it has, in fact, replaced waist circumference.
CHALLENGES TO IMPLEMENTATION: Inertia
Few interventions are as simple as this. Thiazide diuretics are well tolerated, need to be taken only once daily, and are inexpensive. Because generics are available, little to no pharmaceutical marketing is done to promote their use. The major barriers to implementing this practice may be overcoming clinical inertia, and the message of pharmaceutical marketing on behalf of the more expensive alternatives.
Acknowledgement
We acknowledge Sofia Medvedev, PhD, University HealthSystem Consortium, Oak Brook, IL for analysis of the National Ambulatory Medical Care Survey data.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at here.
1. Wright JT, Jr, Harris-Haywood S, Pressel S, et al. Clinical outcomes by race in hypertensive patients with and without the metabolic syndrome: Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Arch Intern Med. 2008;168:207-217.
2. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326:1427.-
3. Eberly LE, Cohen JD, Prineas R, Yang L. Intervention Trial Research group. Impact of incident diabetes and incident nonfatal cardiovascular disease on 18-year mortality: the Multiple Risk Factor Intervention Trial experience. Diabetes Care. 2003;26:848-854.
4. Pollare T, Lithell H, Berne C. A comparison of the effects of hydrochlorothiazide and captopril on glucose and lipid metabolism in patients with hyper-tension. N Engl J Med. 1989;321:868-873.
5. Mancia G, Grassi G, Zanchetti A. New-onset diabetes and antihypertensive drugs. J Hypertens. 2006;24:3-10.
6. Skarfors ET, Lithell HO, Selinus I, Aberg H. Do antihypertensive drugs precipitate diabetes? BMJ. 1989;298:1147-1152
7. Scholze J, Grimm E, Herrmann D, Unger T, Kintscher U. Optimal treatment of obesity-related hypertension: the Hypertension-Obesity-Sibutra-mine (HOS) study. Circulation. 2007;115:1991-1998.
8. Bakris G, Molitch M, Hewkin A, et al. STAR Investigators. Differences in glucose tolerance between fixed-dose antihypertensive drug combinations in people with metabolic syndrome. Diabetes Care. 2006;29:2592-2597.
9. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med. 1993;329:1456-1462.
10. Gianni M, Bosch J, Pogue J, et al. Effect of long-term ACE-inhibitor therapy in elderly vascular disease patients. Eur Heart J. 2007;28:1382-1388.
11. Abuissa H, Jones PG, Marso SP, O’Keefe JH Jr. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers for prevention of type 2 diabetes: a meta-analysis of randomized clinical trials. J Am Coll Cardiol. 2005;46:821-826.
12. Mykkänen L, Kuusisto J, Pyörälä K, Laakso M, Haffner SM. Increased risk of non-insulin-dependent diabetes mellitus in elderly hypertensive subjects. J Hypertens. 1994;12:1425-1432.
13. Giles TD, Sander GE. Pathophysiologic, diagnostic, and therapeutic aspects of the metabolic syndrome. J Clin Hypertens (Greenwich). 2005;7:669-678.
14. Mancia G. The association of hypertension and diabetes: prevalence, cardiovascular risk and protection by blood pressure reduction. Acta Diabetol. 2005;42(suppl 1):S17-S25.
15. Wagh A, Stone NJ. Treatment of metabolic syndrome. Expert Rev Cardiovasc Ther. 2004;2:213-228.
16. Hall WD, Clark LT, Wenger NK, et al. African-American Lipid and Cardiovascular Council. The metabolic syndrome in African Americans: a review. Ethn Dis. 2003;13:414-428.
17. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group, Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981-2997.
18. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Bethesda, MD: US Department of Health and Human Services, National Heart, Lung, and Blood Institute; December 2003. Available at: http://www.nhlbi.nih.gov/guidelines/hypertension. Accessed March 31, 2008.
19. Black HR, Davis B, Barzilay J, et al. Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Metabolic and clinical outcomes in nondiabetic individuals with the metabolic syndrome assigned to chlorthalidone, amlodipine, or lisinopril as initial treatment for hypertension: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Diabetes Care. 2008;31:353-360.
1. Wright JT, Jr, Harris-Haywood S, Pressel S, et al. Clinical outcomes by race in hypertensive patients with and without the metabolic syndrome: Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Arch Intern Med. 2008;168:207-217.
2. Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326:1427.-
3. Eberly LE, Cohen JD, Prineas R, Yang L. Intervention Trial Research group. Impact of incident diabetes and incident nonfatal cardiovascular disease on 18-year mortality: the Multiple Risk Factor Intervention Trial experience. Diabetes Care. 2003;26:848-854.
4. Pollare T, Lithell H, Berne C. A comparison of the effects of hydrochlorothiazide and captopril on glucose and lipid metabolism in patients with hyper-tension. N Engl J Med. 1989;321:868-873.
5. Mancia G, Grassi G, Zanchetti A. New-onset diabetes and antihypertensive drugs. J Hypertens. 2006;24:3-10.
6. Skarfors ET, Lithell HO, Selinus I, Aberg H. Do antihypertensive drugs precipitate diabetes? BMJ. 1989;298:1147-1152
7. Scholze J, Grimm E, Herrmann D, Unger T, Kintscher U. Optimal treatment of obesity-related hypertension: the Hypertension-Obesity-Sibutra-mine (HOS) study. Circulation. 2007;115:1991-1998.
8. Bakris G, Molitch M, Hewkin A, et al. STAR Investigators. Differences in glucose tolerance between fixed-dose antihypertensive drug combinations in people with metabolic syndrome. Diabetes Care. 2006;29:2592-2597.
9. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med. 1993;329:1456-1462.
10. Gianni M, Bosch J, Pogue J, et al. Effect of long-term ACE-inhibitor therapy in elderly vascular disease patients. Eur Heart J. 2007;28:1382-1388.
11. Abuissa H, Jones PG, Marso SP, O’Keefe JH Jr. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers for prevention of type 2 diabetes: a meta-analysis of randomized clinical trials. J Am Coll Cardiol. 2005;46:821-826.
12. Mykkänen L, Kuusisto J, Pyörälä K, Laakso M, Haffner SM. Increased risk of non-insulin-dependent diabetes mellitus in elderly hypertensive subjects. J Hypertens. 1994;12:1425-1432.
13. Giles TD, Sander GE. Pathophysiologic, diagnostic, and therapeutic aspects of the metabolic syndrome. J Clin Hypertens (Greenwich). 2005;7:669-678.
14. Mancia G. The association of hypertension and diabetes: prevalence, cardiovascular risk and protection by blood pressure reduction. Acta Diabetol. 2005;42(suppl 1):S17-S25.
15. Wagh A, Stone NJ. Treatment of metabolic syndrome. Expert Rev Cardiovasc Ther. 2004;2:213-228.
16. Hall WD, Clark LT, Wenger NK, et al. African-American Lipid and Cardiovascular Council. The metabolic syndrome in African Americans: a review. Ethn Dis. 2003;13:414-428.
17. ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group, Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981-2997.
18. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7). Bethesda, MD: US Department of Health and Human Services, National Heart, Lung, and Blood Institute; December 2003. Available at: http://www.nhlbi.nih.gov/guidelines/hypertension. Accessed March 31, 2008.
19. Black HR, Davis B, Barzilay J, et al. Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Metabolic and clinical outcomes in nondiabetic individuals with the metabolic syndrome assigned to chlorthalidone, amlodipine, or lisinopril as initial treatment for hypertension: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Diabetes Care. 2008;31:353-360.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
Drugs help pass more ureteral stones
Prescribe tamsulosin (typically 0.4 mg daily) or nifedipine (typically 30 mg daily) for patients with lower ureteral calculi, to speed stone passage and to avoid surgical intervention
Strength of recommendation
A: Meta-analysis of randomized controlled trials
Singh A, Alter HJ, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Ann Emerg Med. 2007; 50:552-563.1
ILLUSTRATIVE CASE
A 52-year-old man presents to your office for follow-up 2 days after he was seen in the ED and diagnosed with a distal ureteral calculus, his first. His pain is reasonably well controlled, but he has not yet passed the stone. Is there anything you can do to help him pass the stone?
Yes. Patients who are candidates for observation should be offered a trial of “medical expulsive therapy” using an α-antagonist or a calcium channel blocker. Until now, medical therapy for kidney stones consisted of pain relief only.
The ordeal of a first stone is all too common—the lifetime prevalence of kidney stones is 5.2%—and the probability of recurrence is about 50%.2,3
NHANES data show increasing prevalence between the periods 1976-1980 and 1988-1996.3 One fifth to one third of kidney stones require surgical intervention.4 In a cohort of 245 patients presenting to an ED in Canada, 50 (20%) required further procedures, including lithotripsy. Stones ≥ 6 mm in size were much less likely to pass (OR=10.7, 95% CI 4.6-24.8).5 The burden on the healthcare system is significant; there are approximately 2 million out-patient visits annually for this problem, and diagnosis and treatment costs about $2 billion annually.6
Watch and wait
The standard approach is a period of watchful waiting and pain control, with urgent urological referral for patients with evidence of upper urinary tract infection, high grade obstruction, inadequate pain or nausea control, or insufficient renal reserve.2,4 Most patients treated with watchful waiting pass their stone within 4 weeks. Any stones that don’t pass within 8 weeks are unlikely to pass spontaneously.2,7
Medical therapy has been proposed for decades
Medications that relax ureteral smooth muscle to help pass ureteral stones have been proposed for decades.8 Prior to 2000, however, only 1 randomized controlled trial (RCT) of medical therapy for ureteral stones had been published.9 A subsequent meta-analysis found 9 studies and showed that medical therapy did increase the chances that a stone would pass.10 The Singh meta-analysis found 13 subsequently published studies and nearly tripled the number of patients evaluated.
STUDY SUMMARY: A well-done meta-analysis
This meta-analysis is based on 16 studies of α-antagonists (most used tamsulosin) and 9 studies of nifedipine, a calcium channel blocker.1 The studies were identified by a comprehensive search strategy that included Medline, EMBASE, and the Cochrane Controlled Trials Register from January 1980 to January 2007. The authors included all randomized trials or controlled clinical trials of medical therapy for adults with acute ureteral colic.
The authors assessed the studies for quality using the Jadad scale, a validated scale of study quality. Higher scores represent better quality, including better documentation of randomization, blinding, and follow-up. The authors specified their planned sensitivity analyses, and used the random effects model to synthesize the results, which tends to provide a more conservative estimate of the effect.
In other words, this was a very well done meta-analysis.
Twenty-two studies met the inclusion criteria: 13 of α-antagonists, 6 of nifedipine, and 3 of both. In 13 of the 16 studies of α-antagonists, tamsulosin (Flomax) was the study drug. The results from the terazosin (Hytrin) and doxazosin (Cardura) studies were included with the tamsulosin studies. The Jadad quality scores of the 22 studies were fairly low, with a median of 2 (range of 0 to 3) on the 5-point scale. The most common deduction was because the study was not double-blinded.
Medical therapy makes sense
“Therapy using either α-antagonists or calcium channel blockers augments the stone expulsion rate compared to standard therapy for moderately sized distal ureteral stones.” 1 CT showing distal ureteral stone
α-Antagonist studies
These 16 studies enrolled 1235 patients with distal ureteral stones. Mean stone size ranged from 4.3 to 7.8 mm. α-Antagonists improved the stone expulsion rate (RR= 1.59, 95% CI 1.44-1.75; NNT=3.3).
The mean time to expulsion of the stone ranged from 2.7 to 14.2 days and duration of therapy ranged from 1 to 7 weeks. In the 9 trials that reported the time to stone expulsion, the stone came out between 2 and 6 days earlier than the control groups.
Adverse effects were reported in 4% of patients receiving the active medication; most were mild.
Nifedipine studies
There were 686 patients in the 9 trials of nifedipine. The mean stone size was 3.9 to 12.8 mm. Some studies included stones in the more proximal as well as the distal ureter.
Nifedipine treatment increased the rate of stone expulsion (RR=1.5, 95% CI 1.34-1.68; NNT=3.9). Time to stone expulsion was shorter in 7 of the 9 studies.
Adverse effects were reported in 15% of the patients. Most of these were mild— nausea, vomiting, asthenia, and dyspepsia.
WHAT’S NEW: Strong evidence for use of medical therapy
The new findings from the Singh meta-analysis reviewed in this PURL supports physicians who have already adopted this practice and should encourage usage by those who have not yet done so.
Inpatients in academic medical centers
There is a growing trend to use tamsulosin to facilitate passage of ureteral stones. The University Health System Consortium (www.uhc.org) has complete clinical data on inpatients with ureteral stones, from 64 academic medical centers and teaching hospitals, between 2003 and 2007. We used this database to analyze trends in the use of tamsulosin in 4300 inpatients with ureteral stones (ICD 9 code 5921).
In 2003, only 3.3% of patients with a discharge diagnosis of ureteral stone received tamsulosin. In 2007, 34.1% of patients with ureteral stones discharged from these hospitals received tamsulosin, with similar rates of use when stratified by the specialty of the attending physician at discharge (family medicine, emergency medicine, internal medicine, urology) (FIGURE 1). We noted a wide range in the rate of adoption of this practice among academic medical centers: 48% in the centers with the highest rate of usage and 4.4% in the centers with the lowest rate.
FIGURE 1
% of inpatients in academic medical centers who received tamsulosin for ureteral stones, by year
Source: Unpublished data from the University Health System Consortium
Outpatients from a sample of US practices
The use of tamsulosin or nifedipine in outpatient practice was infrequent even 2 or 3 years ago. We used the National Ambulatory Medical Care Survey data (www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm) from 2004 and 2005 (the most recent available), which provides a sample of all US outpatient practices. Only 7% of an estimated 1,345,000 patients diagnosed with ureteral stones were prescribed either tamsulosin or nifedipine, and urologists cared for most of those.
These unpublished data show that physicians in academic medical centers are increasingly adopting the practice of using tamsulosin or nifedipine for expulsion of ureteral stones, that urologists appear to be the first to begin using these medications in outpatients several years ago, and that this practice is being adopted actively in selected academic medical centers.
CAVEATS: Is either drug better? Too little data to tell
Our conclusion is that the strengths of this meta-analysis outweigh the weaknesses, the findings across studies are consistent, and the use of smooth-muscle relaxants for this indication makes sense from a mechanistic point of view.
The quality of a meta-analysis is only as good as the quality of the included studies, and, in this case, the overall quality of studies was not uniformly high. Median Jadad score, a summary measure of study quality, was 2, and the highest score was 3 (of a maximum of 5). The most common problem was lack of blinding, which can be critical in studies with subjective outcomes such as pain. We doubt that the lack of blinding led to any significant misclassification of outcome in this study, however.
Patients either passed the stone or they didn’t, or had a surgical intervention or not. It is reassuring that, when the best quality studies (Jadad score= 3) were analyzed separately, the results were equally good.
There have not been sufficient head-to-head trials to know if one is better than the other. We prefer α-antagonists because of the lower apparent side-effect profile. Our analysis of the UHC data shows that most of the physicians who are using medical therapy are using tamsulosin primarily for this diagnosis.
The majority of the patients in the studies included in the meta-analysis had been referred to a urologist. This raises the possibility that this treatment may not be as effective in patients with less severe symptoms for whom urological consultation is not necessary.
CHALLENGES TO IMPLEMENTATION: This change should be easy to put into practice
Tamsulosin is the best studied of the drugs, but also the most expensive. Based on the estimated number need to treat (NNT) of between 3 and 4 to prevent a surgical intervention and an estimated cost of around $90 for 1 month (www. drugstore.com, February 16, 2008), tamsulosin seems like a good investment to avoid surgical intervention.
The evidence for the other α-antagonists is consistent with that of tamsulosin, but there are fewer data, so it is not clear that the other agents will work as well.
Many people with renal colic are diagnosed and treated in the emergency department; they may not see their family physician until some time after the stone is diagnosed. It is unclear what effect this delay might have on medication effectiveness.
Neither tamsulosin nor nifedipine have an FDA indication for ureterolithiasis. However, they are prescribed commonly, and most physicians are familiar with their use and adverse-effect profiles.
Drugs used in the meta-analysis studies
α-Antagonists
Tamsulosin (Flomax)
Terazosin (Hytrin)
Doxazosin (Cardura)
Calcium channel blockers
Nifedipine (Adalat, Nifedical, Procardia)
Acknowledgement
We acknowledge Sofia Medvedev, PhD of the University HealthSystem Consortium (UHC) in Oak Brook, IL for analysis of the UHC Clinical Database and the National Ambulatory Medical Care Survey data.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Singh A, Alter HJ, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Ann Emerg Med. 2007;50:552-563.
2. Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350:684-693.
3. Stamatelou KK, Francis ME, Jones CA, Nyberg LM. Curhan GC. Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney International. 2003;63:1817-1823.
4. American Urological Association. Clinical Guidelines: Ureteral Calculi. Last updated 2007. Available at: http://www.auanet.org/guidelines/uretcal07.cfm. Accessed February 11, 2008.
5. Papa L, Stiell IG, Wells GA, Ball I, Battram E, Mahoney JE. Predicting intervention in renal colic patients after emergency department evaluation. Can J Emerg Med. 2005;7:78-86.
6. Pearle MS, Calhoun EA, Curhan GC. Urologic Diseases of America Project. Urologic diseases in America project: urolithiasis. J Urol. 2005;173:848-857.
7. Morse RM, Resnick MI. Ureteral calculi: natural history and treatment in an era of advanced technology. J Urol. 1991;145:263-265.
8. Peters HJ, Eckstein W. Possible pharmacological means of treating renal colic. Urol Res. 1975;3:55-59.
9. Borghi L, Meschi T, Amato F, Novarini A, Giannini A, Quarantelli C, et al. Nifedipine and methylpredniso-lone in facilitating ureteral stone passage: a randomized, double-blind, placebo-controlled study. J Urol. 1994;152:1095-1098.
10. Hollingsworth JM, Rogers MA, Kaufman SR, Bradford TJ, Saint S, Wei JT, et al. Medical therapy to facilitate urinary stone passage: a meta-analysis. Lancet. 2006;368:1171-1179.
Prescribe tamsulosin (typically 0.4 mg daily) or nifedipine (typically 30 mg daily) for patients with lower ureteral calculi, to speed stone passage and to avoid surgical intervention
Strength of recommendation
A: Meta-analysis of randomized controlled trials
Singh A, Alter HJ, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Ann Emerg Med. 2007; 50:552-563.1
ILLUSTRATIVE CASE
A 52-year-old man presents to your office for follow-up 2 days after he was seen in the ED and diagnosed with a distal ureteral calculus, his first. His pain is reasonably well controlled, but he has not yet passed the stone. Is there anything you can do to help him pass the stone?
Yes. Patients who are candidates for observation should be offered a trial of “medical expulsive therapy” using an α-antagonist or a calcium channel blocker. Until now, medical therapy for kidney stones consisted of pain relief only.
The ordeal of a first stone is all too common—the lifetime prevalence of kidney stones is 5.2%—and the probability of recurrence is about 50%.2,3
NHANES data show increasing prevalence between the periods 1976-1980 and 1988-1996.3 One fifth to one third of kidney stones require surgical intervention.4 In a cohort of 245 patients presenting to an ED in Canada, 50 (20%) required further procedures, including lithotripsy. Stones ≥ 6 mm in size were much less likely to pass (OR=10.7, 95% CI 4.6-24.8).5 The burden on the healthcare system is significant; there are approximately 2 million out-patient visits annually for this problem, and diagnosis and treatment costs about $2 billion annually.6
Watch and wait
The standard approach is a period of watchful waiting and pain control, with urgent urological referral for patients with evidence of upper urinary tract infection, high grade obstruction, inadequate pain or nausea control, or insufficient renal reserve.2,4 Most patients treated with watchful waiting pass their stone within 4 weeks. Any stones that don’t pass within 8 weeks are unlikely to pass spontaneously.2,7
Medical therapy has been proposed for decades
Medications that relax ureteral smooth muscle to help pass ureteral stones have been proposed for decades.8 Prior to 2000, however, only 1 randomized controlled trial (RCT) of medical therapy for ureteral stones had been published.9 A subsequent meta-analysis found 9 studies and showed that medical therapy did increase the chances that a stone would pass.10 The Singh meta-analysis found 13 subsequently published studies and nearly tripled the number of patients evaluated.
STUDY SUMMARY: A well-done meta-analysis
This meta-analysis is based on 16 studies of α-antagonists (most used tamsulosin) and 9 studies of nifedipine, a calcium channel blocker.1 The studies were identified by a comprehensive search strategy that included Medline, EMBASE, and the Cochrane Controlled Trials Register from January 1980 to January 2007. The authors included all randomized trials or controlled clinical trials of medical therapy for adults with acute ureteral colic.
The authors assessed the studies for quality using the Jadad scale, a validated scale of study quality. Higher scores represent better quality, including better documentation of randomization, blinding, and follow-up. The authors specified their planned sensitivity analyses, and used the random effects model to synthesize the results, which tends to provide a more conservative estimate of the effect.
In other words, this was a very well done meta-analysis.
Twenty-two studies met the inclusion criteria: 13 of α-antagonists, 6 of nifedipine, and 3 of both. In 13 of the 16 studies of α-antagonists, tamsulosin (Flomax) was the study drug. The results from the terazosin (Hytrin) and doxazosin (Cardura) studies were included with the tamsulosin studies. The Jadad quality scores of the 22 studies were fairly low, with a median of 2 (range of 0 to 3) on the 5-point scale. The most common deduction was because the study was not double-blinded.
Medical therapy makes sense
“Therapy using either α-antagonists or calcium channel blockers augments the stone expulsion rate compared to standard therapy for moderately sized distal ureteral stones.” 1 CT showing distal ureteral stone
α-Antagonist studies
These 16 studies enrolled 1235 patients with distal ureteral stones. Mean stone size ranged from 4.3 to 7.8 mm. α-Antagonists improved the stone expulsion rate (RR= 1.59, 95% CI 1.44-1.75; NNT=3.3).
The mean time to expulsion of the stone ranged from 2.7 to 14.2 days and duration of therapy ranged from 1 to 7 weeks. In the 9 trials that reported the time to stone expulsion, the stone came out between 2 and 6 days earlier than the control groups.
Adverse effects were reported in 4% of patients receiving the active medication; most were mild.
Nifedipine studies
There were 686 patients in the 9 trials of nifedipine. The mean stone size was 3.9 to 12.8 mm. Some studies included stones in the more proximal as well as the distal ureter.
Nifedipine treatment increased the rate of stone expulsion (RR=1.5, 95% CI 1.34-1.68; NNT=3.9). Time to stone expulsion was shorter in 7 of the 9 studies.
Adverse effects were reported in 15% of the patients. Most of these were mild— nausea, vomiting, asthenia, and dyspepsia.
WHAT’S NEW: Strong evidence for use of medical therapy
The new findings from the Singh meta-analysis reviewed in this PURL supports physicians who have already adopted this practice and should encourage usage by those who have not yet done so.
Inpatients in academic medical centers
There is a growing trend to use tamsulosin to facilitate passage of ureteral stones. The University Health System Consortium (www.uhc.org) has complete clinical data on inpatients with ureteral stones, from 64 academic medical centers and teaching hospitals, between 2003 and 2007. We used this database to analyze trends in the use of tamsulosin in 4300 inpatients with ureteral stones (ICD 9 code 5921).
In 2003, only 3.3% of patients with a discharge diagnosis of ureteral stone received tamsulosin. In 2007, 34.1% of patients with ureteral stones discharged from these hospitals received tamsulosin, with similar rates of use when stratified by the specialty of the attending physician at discharge (family medicine, emergency medicine, internal medicine, urology) (FIGURE 1). We noted a wide range in the rate of adoption of this practice among academic medical centers: 48% in the centers with the highest rate of usage and 4.4% in the centers with the lowest rate.
FIGURE 1
% of inpatients in academic medical centers who received tamsulosin for ureteral stones, by year
Source: Unpublished data from the University Health System Consortium
Outpatients from a sample of US practices
The use of tamsulosin or nifedipine in outpatient practice was infrequent even 2 or 3 years ago. We used the National Ambulatory Medical Care Survey data (www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm) from 2004 and 2005 (the most recent available), which provides a sample of all US outpatient practices. Only 7% of an estimated 1,345,000 patients diagnosed with ureteral stones were prescribed either tamsulosin or nifedipine, and urologists cared for most of those.
These unpublished data show that physicians in academic medical centers are increasingly adopting the practice of using tamsulosin or nifedipine for expulsion of ureteral stones, that urologists appear to be the first to begin using these medications in outpatients several years ago, and that this practice is being adopted actively in selected academic medical centers.
CAVEATS: Is either drug better? Too little data to tell
Our conclusion is that the strengths of this meta-analysis outweigh the weaknesses, the findings across studies are consistent, and the use of smooth-muscle relaxants for this indication makes sense from a mechanistic point of view.
The quality of a meta-analysis is only as good as the quality of the included studies, and, in this case, the overall quality of studies was not uniformly high. Median Jadad score, a summary measure of study quality, was 2, and the highest score was 3 (of a maximum of 5). The most common problem was lack of blinding, which can be critical in studies with subjective outcomes such as pain. We doubt that the lack of blinding led to any significant misclassification of outcome in this study, however.
Patients either passed the stone or they didn’t, or had a surgical intervention or not. It is reassuring that, when the best quality studies (Jadad score= 3) were analyzed separately, the results were equally good.
There have not been sufficient head-to-head trials to know if one is better than the other. We prefer α-antagonists because of the lower apparent side-effect profile. Our analysis of the UHC data shows that most of the physicians who are using medical therapy are using tamsulosin primarily for this diagnosis.
The majority of the patients in the studies included in the meta-analysis had been referred to a urologist. This raises the possibility that this treatment may not be as effective in patients with less severe symptoms for whom urological consultation is not necessary.
CHALLENGES TO IMPLEMENTATION: This change should be easy to put into practice
Tamsulosin is the best studied of the drugs, but also the most expensive. Based on the estimated number need to treat (NNT) of between 3 and 4 to prevent a surgical intervention and an estimated cost of around $90 for 1 month (www. drugstore.com, February 16, 2008), tamsulosin seems like a good investment to avoid surgical intervention.
The evidence for the other α-antagonists is consistent with that of tamsulosin, but there are fewer data, so it is not clear that the other agents will work as well.
Many people with renal colic are diagnosed and treated in the emergency department; they may not see their family physician until some time after the stone is diagnosed. It is unclear what effect this delay might have on medication effectiveness.
Neither tamsulosin nor nifedipine have an FDA indication for ureterolithiasis. However, they are prescribed commonly, and most physicians are familiar with their use and adverse-effect profiles.
Drugs used in the meta-analysis studies
α-Antagonists
Tamsulosin (Flomax)
Terazosin (Hytrin)
Doxazosin (Cardura)
Calcium channel blockers
Nifedipine (Adalat, Nifedical, Procardia)
Acknowledgement
We acknowledge Sofia Medvedev, PhD of the University HealthSystem Consortium (UHC) in Oak Brook, IL for analysis of the UHC Clinical Database and the National Ambulatory Medical Care Survey data.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Prescribe tamsulosin (typically 0.4 mg daily) or nifedipine (typically 30 mg daily) for patients with lower ureteral calculi, to speed stone passage and to avoid surgical intervention
Strength of recommendation
A: Meta-analysis of randomized controlled trials
Singh A, Alter HJ, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Ann Emerg Med. 2007; 50:552-563.1
ILLUSTRATIVE CASE
A 52-year-old man presents to your office for follow-up 2 days after he was seen in the ED and diagnosed with a distal ureteral calculus, his first. His pain is reasonably well controlled, but he has not yet passed the stone. Is there anything you can do to help him pass the stone?
Yes. Patients who are candidates for observation should be offered a trial of “medical expulsive therapy” using an α-antagonist or a calcium channel blocker. Until now, medical therapy for kidney stones consisted of pain relief only.
The ordeal of a first stone is all too common—the lifetime prevalence of kidney stones is 5.2%—and the probability of recurrence is about 50%.2,3
NHANES data show increasing prevalence between the periods 1976-1980 and 1988-1996.3 One fifth to one third of kidney stones require surgical intervention.4 In a cohort of 245 patients presenting to an ED in Canada, 50 (20%) required further procedures, including lithotripsy. Stones ≥ 6 mm in size were much less likely to pass (OR=10.7, 95% CI 4.6-24.8).5 The burden on the healthcare system is significant; there are approximately 2 million out-patient visits annually for this problem, and diagnosis and treatment costs about $2 billion annually.6
Watch and wait
The standard approach is a period of watchful waiting and pain control, with urgent urological referral for patients with evidence of upper urinary tract infection, high grade obstruction, inadequate pain or nausea control, or insufficient renal reserve.2,4 Most patients treated with watchful waiting pass their stone within 4 weeks. Any stones that don’t pass within 8 weeks are unlikely to pass spontaneously.2,7
Medical therapy has been proposed for decades
Medications that relax ureteral smooth muscle to help pass ureteral stones have been proposed for decades.8 Prior to 2000, however, only 1 randomized controlled trial (RCT) of medical therapy for ureteral stones had been published.9 A subsequent meta-analysis found 9 studies and showed that medical therapy did increase the chances that a stone would pass.10 The Singh meta-analysis found 13 subsequently published studies and nearly tripled the number of patients evaluated.
STUDY SUMMARY: A well-done meta-analysis
This meta-analysis is based on 16 studies of α-antagonists (most used tamsulosin) and 9 studies of nifedipine, a calcium channel blocker.1 The studies were identified by a comprehensive search strategy that included Medline, EMBASE, and the Cochrane Controlled Trials Register from January 1980 to January 2007. The authors included all randomized trials or controlled clinical trials of medical therapy for adults with acute ureteral colic.
The authors assessed the studies for quality using the Jadad scale, a validated scale of study quality. Higher scores represent better quality, including better documentation of randomization, blinding, and follow-up. The authors specified their planned sensitivity analyses, and used the random effects model to synthesize the results, which tends to provide a more conservative estimate of the effect.
In other words, this was a very well done meta-analysis.
Twenty-two studies met the inclusion criteria: 13 of α-antagonists, 6 of nifedipine, and 3 of both. In 13 of the 16 studies of α-antagonists, tamsulosin (Flomax) was the study drug. The results from the terazosin (Hytrin) and doxazosin (Cardura) studies were included with the tamsulosin studies. The Jadad quality scores of the 22 studies were fairly low, with a median of 2 (range of 0 to 3) on the 5-point scale. The most common deduction was because the study was not double-blinded.
Medical therapy makes sense
“Therapy using either α-antagonists or calcium channel blockers augments the stone expulsion rate compared to standard therapy for moderately sized distal ureteral stones.” 1 CT showing distal ureteral stone
α-Antagonist studies
These 16 studies enrolled 1235 patients with distal ureteral stones. Mean stone size ranged from 4.3 to 7.8 mm. α-Antagonists improved the stone expulsion rate (RR= 1.59, 95% CI 1.44-1.75; NNT=3.3).
The mean time to expulsion of the stone ranged from 2.7 to 14.2 days and duration of therapy ranged from 1 to 7 weeks. In the 9 trials that reported the time to stone expulsion, the stone came out between 2 and 6 days earlier than the control groups.
Adverse effects were reported in 4% of patients receiving the active medication; most were mild.
Nifedipine studies
There were 686 patients in the 9 trials of nifedipine. The mean stone size was 3.9 to 12.8 mm. Some studies included stones in the more proximal as well as the distal ureter.
Nifedipine treatment increased the rate of stone expulsion (RR=1.5, 95% CI 1.34-1.68; NNT=3.9). Time to stone expulsion was shorter in 7 of the 9 studies.
Adverse effects were reported in 15% of the patients. Most of these were mild— nausea, vomiting, asthenia, and dyspepsia.
WHAT’S NEW: Strong evidence for use of medical therapy
The new findings from the Singh meta-analysis reviewed in this PURL supports physicians who have already adopted this practice and should encourage usage by those who have not yet done so.
Inpatients in academic medical centers
There is a growing trend to use tamsulosin to facilitate passage of ureteral stones. The University Health System Consortium (www.uhc.org) has complete clinical data on inpatients with ureteral stones, from 64 academic medical centers and teaching hospitals, between 2003 and 2007. We used this database to analyze trends in the use of tamsulosin in 4300 inpatients with ureteral stones (ICD 9 code 5921).
In 2003, only 3.3% of patients with a discharge diagnosis of ureteral stone received tamsulosin. In 2007, 34.1% of patients with ureteral stones discharged from these hospitals received tamsulosin, with similar rates of use when stratified by the specialty of the attending physician at discharge (family medicine, emergency medicine, internal medicine, urology) (FIGURE 1). We noted a wide range in the rate of adoption of this practice among academic medical centers: 48% in the centers with the highest rate of usage and 4.4% in the centers with the lowest rate.
FIGURE 1
% of inpatients in academic medical centers who received tamsulosin for ureteral stones, by year
Source: Unpublished data from the University Health System Consortium
Outpatients from a sample of US practices
The use of tamsulosin or nifedipine in outpatient practice was infrequent even 2 or 3 years ago. We used the National Ambulatory Medical Care Survey data (www.cdc.gov/nchs/about/major/ahcd/ahcd1.htm) from 2004 and 2005 (the most recent available), which provides a sample of all US outpatient practices. Only 7% of an estimated 1,345,000 patients diagnosed with ureteral stones were prescribed either tamsulosin or nifedipine, and urologists cared for most of those.
These unpublished data show that physicians in academic medical centers are increasingly adopting the practice of using tamsulosin or nifedipine for expulsion of ureteral stones, that urologists appear to be the first to begin using these medications in outpatients several years ago, and that this practice is being adopted actively in selected academic medical centers.
CAVEATS: Is either drug better? Too little data to tell
Our conclusion is that the strengths of this meta-analysis outweigh the weaknesses, the findings across studies are consistent, and the use of smooth-muscle relaxants for this indication makes sense from a mechanistic point of view.
The quality of a meta-analysis is only as good as the quality of the included studies, and, in this case, the overall quality of studies was not uniformly high. Median Jadad score, a summary measure of study quality, was 2, and the highest score was 3 (of a maximum of 5). The most common problem was lack of blinding, which can be critical in studies with subjective outcomes such as pain. We doubt that the lack of blinding led to any significant misclassification of outcome in this study, however.
Patients either passed the stone or they didn’t, or had a surgical intervention or not. It is reassuring that, when the best quality studies (Jadad score= 3) were analyzed separately, the results were equally good.
There have not been sufficient head-to-head trials to know if one is better than the other. We prefer α-antagonists because of the lower apparent side-effect profile. Our analysis of the UHC data shows that most of the physicians who are using medical therapy are using tamsulosin primarily for this diagnosis.
The majority of the patients in the studies included in the meta-analysis had been referred to a urologist. This raises the possibility that this treatment may not be as effective in patients with less severe symptoms for whom urological consultation is not necessary.
CHALLENGES TO IMPLEMENTATION: This change should be easy to put into practice
Tamsulosin is the best studied of the drugs, but also the most expensive. Based on the estimated number need to treat (NNT) of between 3 and 4 to prevent a surgical intervention and an estimated cost of around $90 for 1 month (www. drugstore.com, February 16, 2008), tamsulosin seems like a good investment to avoid surgical intervention.
The evidence for the other α-antagonists is consistent with that of tamsulosin, but there are fewer data, so it is not clear that the other agents will work as well.
Many people with renal colic are diagnosed and treated in the emergency department; they may not see their family physician until some time after the stone is diagnosed. It is unclear what effect this delay might have on medication effectiveness.
Neither tamsulosin nor nifedipine have an FDA indication for ureterolithiasis. However, they are prescribed commonly, and most physicians are familiar with their use and adverse-effect profiles.
Drugs used in the meta-analysis studies
α-Antagonists
Tamsulosin (Flomax)
Terazosin (Hytrin)
Doxazosin (Cardura)
Calcium channel blockers
Nifedipine (Adalat, Nifedical, Procardia)
Acknowledgement
We acknowledge Sofia Medvedev, PhD of the University HealthSystem Consortium (UHC) in Oak Brook, IL for analysis of the UHC Clinical Database and the National Ambulatory Medical Care Survey data.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Singh A, Alter HJ, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Ann Emerg Med. 2007;50:552-563.
2. Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350:684-693.
3. Stamatelou KK, Francis ME, Jones CA, Nyberg LM. Curhan GC. Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney International. 2003;63:1817-1823.
4. American Urological Association. Clinical Guidelines: Ureteral Calculi. Last updated 2007. Available at: http://www.auanet.org/guidelines/uretcal07.cfm. Accessed February 11, 2008.
5. Papa L, Stiell IG, Wells GA, Ball I, Battram E, Mahoney JE. Predicting intervention in renal colic patients after emergency department evaluation. Can J Emerg Med. 2005;7:78-86.
6. Pearle MS, Calhoun EA, Curhan GC. Urologic Diseases of America Project. Urologic diseases in America project: urolithiasis. J Urol. 2005;173:848-857.
7. Morse RM, Resnick MI. Ureteral calculi: natural history and treatment in an era of advanced technology. J Urol. 1991;145:263-265.
8. Peters HJ, Eckstein W. Possible pharmacological means of treating renal colic. Urol Res. 1975;3:55-59.
9. Borghi L, Meschi T, Amato F, Novarini A, Giannini A, Quarantelli C, et al. Nifedipine and methylpredniso-lone in facilitating ureteral stone passage: a randomized, double-blind, placebo-controlled study. J Urol. 1994;152:1095-1098.
10. Hollingsworth JM, Rogers MA, Kaufman SR, Bradford TJ, Saint S, Wei JT, et al. Medical therapy to facilitate urinary stone passage: a meta-analysis. Lancet. 2006;368:1171-1179.
1. Singh A, Alter HJ, Littlepage A. A systematic review of medical therapy to facilitate passage of ureteral calculi. Ann Emerg Med. 2007;50:552-563.
2. Teichman JM. Clinical practice. Acute renal colic from ureteral calculus. N Engl J Med. 2004;350:684-693.
3. Stamatelou KK, Francis ME, Jones CA, Nyberg LM. Curhan GC. Time trends in reported prevalence of kidney stones in the United States: 1976-1994. Kidney International. 2003;63:1817-1823.
4. American Urological Association. Clinical Guidelines: Ureteral Calculi. Last updated 2007. Available at: http://www.auanet.org/guidelines/uretcal07.cfm. Accessed February 11, 2008.
5. Papa L, Stiell IG, Wells GA, Ball I, Battram E, Mahoney JE. Predicting intervention in renal colic patients after emergency department evaluation. Can J Emerg Med. 2005;7:78-86.
6. Pearle MS, Calhoun EA, Curhan GC. Urologic Diseases of America Project. Urologic diseases in America project: urolithiasis. J Urol. 2005;173:848-857.
7. Morse RM, Resnick MI. Ureteral calculi: natural history and treatment in an era of advanced technology. J Urol. 1991;145:263-265.
8. Peters HJ, Eckstein W. Possible pharmacological means of treating renal colic. Urol Res. 1975;3:55-59.
9. Borghi L, Meschi T, Amato F, Novarini A, Giannini A, Quarantelli C, et al. Nifedipine and methylpredniso-lone in facilitating ureteral stone passage: a randomized, double-blind, placebo-controlled study. J Urol. 1994;152:1095-1098.
10. Hollingsworth JM, Rogers MA, Kaufman SR, Bradford TJ, Saint S, Wei JT, et al. Medical therapy to facilitate urinary stone passage: a meta-analysis. Lancet. 2006;368:1171-1179.
Copyright © 2008 The Family Physicians Inquiries Network.
All rights reserved.
This obscure herb works for the common cold
Offer patients Pelargonium sidoides (30 drops 3 times a day) to reduce the severity and duration of common cold symptoms and to get patients back to work sooner.1
Strength of recommendation
B: A single well-designed randomized controlled trial
Lizogub VG, Riley DS, Heger M. Efficacy of a Pelargonium sidoides preparation in patients with the common cold: A randomized, double blind, placebo-controlled clinical trial. Explore (NY) 2007; 3:573–584.
ILLUSTRATIVE CASE
A 39-year-old, otherwise healthy woman presents to your clinic with a sore throat, nasal congestion, and dry cough she’s had since yesterday. She wants an antibiotic, but your evaluation reveals an uncomplicated viral upper respiratory infection—a common cold. You would like to provide her with an alternative treatment, but you are aware of the lack of evidence for clear benefit of zinc lozenges, echinacea, and vitamin C. Is there any other medication that might benefit this patient?
Yes. Pelargonium sidoides, a species of South African geranium used for centuries in Zulu medicine,2 shows promise as an herbal remedy for respiratory infections. Two randomized trials show that extracts of P sidoides improve symptoms of acute bronchitis which, like the common cold, is usually caused by a virus.3-5
There is a plausible biological mechanism of action. In vitro studies show that Pelargonium extract induces the interferon system and up-regulates cytokines important in protecting host cells from viral infection.6
BACKGROUND: $17 billion dollar cold
Our patients want more relief from cold symptoms and are clearly willing to pay for it. Americans spend approximately $2.9 billion annually on over-the-counter (OTC) cold preparations and $1.1 billion on unnecessary antibiotics.7 The term “common cold” refers to a collection of symptoms, including sore throat, rhinorrhea, nasal congestion, cough, low-grade fever, and malaise, usually self-limited and lasting 10 to 14 days, caused by a number of viruses, most commonly by a rhinovirus.8 According to the 2005 National Ambulatory Medical Care Survey, the common cold is the third most common diagnosis in physicians’ offices behind only hypertension and well-infant/child visits.9 A 2001 US telephone survey determined that approximately 500 million episodes of non-influenza viral infection occur annually, resulting in direct costs of $17 billion for physician services and medications and approximately 200 million missed days of work.7
CLINICAL CONTEXT: Evidence proves most cold remedies don’t work
Although colds are common and result in annoying symptoms and missed work, much of the money spent on remedies is wasted. A truly effective treatment would be valuable to our patients.
Despite brisk sales, evidence for the efficacy of various cold remedies is inconclusive and contradictory. We found 6 Cochrane reviews of cold treatments, including antitussives, antihistamines, decongestants, vitamin C, echinacea, and zinc lozenges. With the exception of pseudoephedrine for nasal symptoms, the evidence that any product improves symptoms or decreases the duration of the cold is not encouraging.
Cough medications. The 2004 Cochrane Review of OTC medications for cough10 found no consistent evidence that any of them work. Codeine was no more effective than placebo for reducing cough symptoms. Three efficacy studies of dextromethorphan for cough showed either no difference or small but possibly clinically insignificant improvement in cough over placebo. One study of guaifenesin showed benefit over placebo in reducing cough frequency; another one showed no benefit over placebo.
Vitamin C, echinacea. Three Cochrane reviews found no conclusive evidence of benefit over placebo for either vitamin C11 or echinacea12 in treating the common cold.
Zinc. A new panel has been convened by the Cochrane group to reassess the effectiveness of zinc, but a 1999 Cochrane review13 found no benefit for zinc over placebo.
Antihistamines are not effective for relieving cold symptoms.14
Pseudoephedrine is the only medication with good-quality evidence for effectiveness, but only for reducing nasal symptoms.15 The authors concluded that patients may be encouraged to continue pseudoephedrine for up to 5 days if found to be effective with the first dose. Nasal congestion and discharge, however, are only 2 of the many irritating symptoms of a cold.

Bernard Ewigman, MD, MSPH
If you are in full-time clinical practice, a medical director of a practice, or otherwise directly involved in decision-making about adopting new practices, join our team of “reality checkers.”
Just email me at be.editor@gmail.com
STUDY SUMMARY: Duration and severity of symptoms are reduced
This was a multicenter, prospective, double-blind, placebo-controlled randomized trial to evaluate the effectiveness of a liquid herbal preparation from the roots of Pelargonium sidoides for decreasing the duration and severity of symptoms of the common cold.
Patient characteristics. Patients were recruited from 8 outpatient departments in Ukraine between December 2003 and May 2004. Two hundred and seven (207) patients were eligible. The number of ineligible and excluded patients was not stated. These 207 patients were randomized into 1 of 4 groups:
- 52 received 30 drops 3 times daily vs 51 patients who received placebo
- 52 patients received 60 drops 3 times daily vs 52 patients who received a higher-dose placebo.
The report gives the outcomes of the low-dose arm only. Two-thirds of the participants were women; all were Caucasian. Patients in the treatment and placebo groups were similar in terms of recurrent disease, prior use of medication for the common cold, smoking, and alcohol and caffeine consumption. All had a negative Group A beta-hemolytic strep test.
Inclusion criteria. Patients included men and women 18 to 55 years of age; able to provide written informed consent; with 2 major cold symptoms (nasal discharge, sore throat) and at least 1 minor cold symptom (nasal congestion, sneezing, scratchy throat, hoarseness, cough, headaches, muscle aches, or fever) or presence of 1 major cold symptom and at least 3 minor cold symptoms; duration of symptoms 24 to 48 hours.
Exclusion criteria were any acute ear, nose, throat and respiratory tract disease other than the common cold; positive rapid strep test; 6 or more episodes of recurrent tonsillitis, sinusitis, or otitis within the past 12 months or any chronic ear, nose, throat or respiratory tract disease; treatment with antibiotics, glucocorticoids, or antihistamine drugs during the 4 weeks prior to enrollment in the trial; treatment with cold medications that might impair the trial results (eg, decongestants, local anesthetics); and use of cough or pain relief medications, or any other treatment for the common cold within 7 days prior to enrollment in the trial.
Treatment regimen. Patients were assigned to take 30 drops of either the study herbal preparation or 30 drops of placebo 3 times daily, at least 30 minutes before or after a meal, from day 1 continuing to day 10. The investigational drug and placebo were supplied by Dr. Willmar Schwabe GmbH & Co. (Karlsruhe, Germany). The investigational medication is a preparation of the roots of P sidoides, extraction solution: ethanol 11% (1:8-10) (wt/wt). The placebo was matched for color, smell, taste, and viscosity. Paracetamol (acetaminophen) tablets were allowed for all patients for fever greater than 39°C.
Primary endpoint. Severity of cold symptoms was evaluated using the Cold Intensity Score (CIS), a validated scale derived from the sum of scores for 10 cold-related symptoms (nasal drainage, sore throat, nasal congestion, sneezing, scratchy throat, hoarseness, cough, headaches, muscle aches, and fever) on a scale of 0 to 4, where 0=not present and 4=very severe, to a maximum of 40 points. At baseline, the mean total CIS was comparable in both treatment and placebo groups (17.8±4.0 vs 16.9±3.4). From baseline to day 5, the mean total CIS decreased by 10.4±3.0 in the treatment group vs 5.6±4.3 in the placebo group (P<.0001).
Secondary endpoints. The number of patients achieving clinical cure (defined by CIS ≤1) by day 10 was significantly higher in the treatment group (78.8% vs 31.4%, P<.0001). The mean duration of days absent from work was significantly lower in the treatment group (6.9±1.8 vs 8.2±2.1, P<.0003), as was number of days with less than 100% usual activity level (7.1±1.5 vs 8.7±1.3, P<.0001). Data for both the primary and secondary endpoints were evaluated according to an intention-to-treat analysis. Both the intervention and placebo sides each had 4 patients that became ineligible after initial randomization. No patients were lost to follow-up.
Safety and tolerability. Patients in the low-dose arm experienced 3 nonserious adverse events, and 1 experienced mild epistaxis. Two additional patients (1 in the treatment and 1 in the placebo group) experienced moderate to severe tracheitis, not attributable to the study medication. Tolerability was rated slightly better in the treatment than placebo group on day 5. Forty-nine of 52 patients (94%) in the treatment group rated the preparation as good or very good tolerability vs 42 of 51 patients (82%) in the placebo group.
WHAT’S NEW?: A first
This is the first study that demonstrates the efficacy and safety of P sidoides in the treatment of the common cold. More importantly, this degree of improvement in cold symptoms is dramatically better than other common OTC treatments, including vitamin C, echinacea, and zinc preparations.
CAVEATS: How is this different from other cold remedies?
Patients are already spending a lot on cold remedies; this study suggests money would be better spent on having a ready supply of Pelargonium in the medicine cabinet, and it appears to be safe.
Other initially promising complementary and alternative therapies, such as zinc, echinacea, and vitamin C, have not been shown to be effective with more vigorous evaluation. We recognize that this is only 1 clinical trial, and the results may not be replicated in future trials. However, we are impressed by the effect size—twice the size as that seen for placebo, with a reduction in half of total cold symptom severity over 5 days and a reduction of missed time from work by more than a full day on average over placebo.
In vitro studies suggest a physiologic mechanism that is consistent with the study outcomes.
Similar findings are reported for symptom reduction in acute bronchitis.
Safety
There were no significant adverse events in this study, which is consistent with the findings of the studies of acute bronchitis.12-14P sidoides has been widely used in Germany since the 1980s, with an annual sale value in 2002 of $55 million or 4.1 million packages.
The Uppsala Monitoring Centre, in conjunction with the World Health Organization international pharmacovigilance program, received 34 case reports between 2002 and 2006 of allergic reactions to ethanolic herbal extract of Pelargonium root, 2 of which involved life-threatening circulatory collapse requiring emergency medical attention. Given the extremely rare occurrence of these events we believe the minimal risk is acceptable. The others involved rash and pruritus.
Also of note: contact dermatitis to Pelargonium houseplants has been reported. As a result, product information will be added to product packaging, warning of common reactions of gastrointestinal complaints (gastric pain, heartburn, nausea, and diarrhea) as well as the potential for serious allergic reaction. In addition, since some of the active compounds are plant coumarins, there is a theoretical risk of interaction with warfarin and aspirin but no serious bleeding events have been reported.16
It is also recommended that individuals with renal or hepatic disease or women who are pregnant or breastfeeding avoid use of this preparation, as safety studies have not been performed.
Other study design issues
A few other issues struck us as important when assessing the validity of this study. For example, 1 of the authors appears to be an employee of the pharmaceutical company that manufactures the preparation, raising the conflict of interest issue.
We were also curious about why the results of the high-dose arm were not reported in this manuscript. Could there have been a higher rate of adverse events in the high-dose arm? Knowing how many patients were ineligible or excluded, and the efficacy or safety in the high-dose arm would give us more confidence in the findings, but we decided that these were not necessarily fatal flaws.
Bottom line
Despite the above caveats, this was a well-designed randomized controlled trial that suggests that P sidoides is impressively efficacious in decreasing the duration and severity of the common cold. In the final analysis, we think that these findings justify recommending this to our patients.
CHALLENGES TO IMPLEMENTATION: 2-day window
The medication was started within 48 hours of the onset of symptoms. We generally see patients seeking treatment for the common cold well after the first 2 days. The efficacy of Pelargonium is no doubt less when started later in the course of the illness. Colds resolve spontaneously, so to get the benefit of this treatment, it likely must be started early.
Our conclusion is that patients could be advised to purchase the medication to have on hand at home at the start of the cold season.
Availability of the drug
P sidoides is available in the US under the brand name Umcka Coldcare.
The preparation used in the study is marketed in Europe by ISO-Arzneimittel17 under the name Umckaloabo, which is a combination of the Zulu words for lung symptoms and breast pain.18
Our Internet search on the term “Pelargonium sidoides” failed to yield a distributor of the German preparation used in the study that would be available in the United States. However, a different manufacturer, Nature’s Way, distributes a number of similar preparations containing extract of the root of P sidoides under the name Umcka Coldcare. Umcka Cold-care appears to be readily available for purchase, both on-line and through local health food stores, for less than $20 per 4-oz (120-mL) bottle. A different retailer, African Red Tea, offers syrup, 1:10 ethanolic extract for $29.95 for 100-mL bottle.19 Like the German preparation, these formulations are delivered by dropper.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Lizogub VG, Riley DS, Heger M. Efficacy of a Pelargonium sidoides preparation in patients with the common cold: A randomized, double blind, placebo-controlled clinical trial. Explore (NY) 2007;3:573-584.
2. Bladt S, Wagner H. From Zulu medicine to the European phytomedicine Umckaloabo. Phytomedicine 2007;14 (suppl 1):2-4.
3. Matthys H, Eisebitt R, Seith B, Heger M. Efficacy and safety of an extract of Pelargonium sidoides (EPs 7630) in adults with acute bronchitis: A randomized, double-blind, placebo-controlled trial. Phytomedicine 2003;10(Suppl 4):7-17.
4. Chuchalin AG, Berman B, Lehmacher W. Treatment of acute bronchitis in adults with a Pelargonium sidoides preparation (EPs 7630): A randomized, double-blind, placebo-controlled trial. Explore (NY) 2005;1:437-445.
5. Matthys H, Heger M. Treatment of acute bronchitis with a liquid herbal drug preparation from Pelargonium sidoides (EPs 7630): A randomized, double-blind, placebo-controlled multicentre study. Curr Med Res Opinion 2007;23:323-331.
6. Kolodziej H, Kiderlen AF. In vitro evaluation of antibacterial and immunomodulatory activities of Pelargonium reniforme, Pelargonium sidoides and the related herbal drug preparation EPs 7630. Phytomedicine 2007;14 (suppl 1):18-26.
7. Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non-influenza related viral respiratory tract infection in the United States. Arch Intern Med 2003;163:487-494.
8. Heikkinen T, Jarvinen A. The common cold. Lancet 2003;361:51-59.
9. Cherry DK, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2005 Summary. Adv Data 2007;387:1-39.
10. Schroeder K, Fahey T. Over-the-counter medications for acute cough in children and adults in ambulatory settings. Cochrane Database Syst Rev 2004;(4):cD001831.-
11. Douglas RM, Hemila H, Chalker E, Treacy B. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev 2004;(4):cD000980.-
12. Linde K, Barrett B, Wolkart K, Bauer R, Melchart D. Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev 2006;(1):cD000530.-
13. Marshall I. Zinc for the common cold. Cochrane Database Syst Rev 1999;(2):cD001364.-(With-drawn 2006, Issue 3).
14. Sutter AI, Lemiengre M, Campbell H, Mackinnon HF. Anithistamines for the common cold. Cochrane Database Syst Rev 2003;(3):cD001267.-
15. Taverner D, Latte J, Draper M. Nasal decongestants for the common cold. Cochrane Database Syst Rev 2004;(3):cD001953.-
16. De Boer HJ, Hagemann U, Bate J, Meyboom RHB. Allergic reactions to medicines derived from Pelargonium species. Drug Saf 2007;30:677-680.
17. ISO-Arzneimittel. Distributor of Umckaloabo. Available at: umckaloabo.com. Accessed January 7, 2008.
18. Taylor PW, Maalim S, Coleman S. The strange story of umckaloabo. Pharm J 2005;275:790-792.
19. African Red Tea Imports. Available at: www.africanredtea.com/pelargonium-syrup.html. Accessed January 7, 2008.
Offer patients Pelargonium sidoides (30 drops 3 times a day) to reduce the severity and duration of common cold symptoms and to get patients back to work sooner.1
Strength of recommendation
B: A single well-designed randomized controlled trial
Lizogub VG, Riley DS, Heger M. Efficacy of a Pelargonium sidoides preparation in patients with the common cold: A randomized, double blind, placebo-controlled clinical trial. Explore (NY) 2007; 3:573–584.
ILLUSTRATIVE CASE
A 39-year-old, otherwise healthy woman presents to your clinic with a sore throat, nasal congestion, and dry cough she’s had since yesterday. She wants an antibiotic, but your evaluation reveals an uncomplicated viral upper respiratory infection—a common cold. You would like to provide her with an alternative treatment, but you are aware of the lack of evidence for clear benefit of zinc lozenges, echinacea, and vitamin C. Is there any other medication that might benefit this patient?
Yes. Pelargonium sidoides, a species of South African geranium used for centuries in Zulu medicine,2 shows promise as an herbal remedy for respiratory infections. Two randomized trials show that extracts of P sidoides improve symptoms of acute bronchitis which, like the common cold, is usually caused by a virus.3-5
There is a plausible biological mechanism of action. In vitro studies show that Pelargonium extract induces the interferon system and up-regulates cytokines important in protecting host cells from viral infection.6
BACKGROUND: $17 billion dollar cold
Our patients want more relief from cold symptoms and are clearly willing to pay for it. Americans spend approximately $2.9 billion annually on over-the-counter (OTC) cold preparations and $1.1 billion on unnecessary antibiotics.7 The term “common cold” refers to a collection of symptoms, including sore throat, rhinorrhea, nasal congestion, cough, low-grade fever, and malaise, usually self-limited and lasting 10 to 14 days, caused by a number of viruses, most commonly by a rhinovirus.8 According to the 2005 National Ambulatory Medical Care Survey, the common cold is the third most common diagnosis in physicians’ offices behind only hypertension and well-infant/child visits.9 A 2001 US telephone survey determined that approximately 500 million episodes of non-influenza viral infection occur annually, resulting in direct costs of $17 billion for physician services and medications and approximately 200 million missed days of work.7
CLINICAL CONTEXT: Evidence proves most cold remedies don’t work
Although colds are common and result in annoying symptoms and missed work, much of the money spent on remedies is wasted. A truly effective treatment would be valuable to our patients.
Despite brisk sales, evidence for the efficacy of various cold remedies is inconclusive and contradictory. We found 6 Cochrane reviews of cold treatments, including antitussives, antihistamines, decongestants, vitamin C, echinacea, and zinc lozenges. With the exception of pseudoephedrine for nasal symptoms, the evidence that any product improves symptoms or decreases the duration of the cold is not encouraging.
Cough medications. The 2004 Cochrane Review of OTC medications for cough10 found no consistent evidence that any of them work. Codeine was no more effective than placebo for reducing cough symptoms. Three efficacy studies of dextromethorphan for cough showed either no difference or small but possibly clinically insignificant improvement in cough over placebo. One study of guaifenesin showed benefit over placebo in reducing cough frequency; another one showed no benefit over placebo.
Vitamin C, echinacea. Three Cochrane reviews found no conclusive evidence of benefit over placebo for either vitamin C11 or echinacea12 in treating the common cold.
Zinc. A new panel has been convened by the Cochrane group to reassess the effectiveness of zinc, but a 1999 Cochrane review13 found no benefit for zinc over placebo.
Antihistamines are not effective for relieving cold symptoms.14
Pseudoephedrine is the only medication with good-quality evidence for effectiveness, but only for reducing nasal symptoms.15 The authors concluded that patients may be encouraged to continue pseudoephedrine for up to 5 days if found to be effective with the first dose. Nasal congestion and discharge, however, are only 2 of the many irritating symptoms of a cold.
Bernard Ewigman, MD, MSPH
If you are in full-time clinical practice, a medical director of a practice, or otherwise directly involved in decision-making about adopting new practices, join our team of “reality checkers.”
Just email me at be.editor@gmail.com
STUDY SUMMARY: Duration and severity of symptoms are reduced
This was a multicenter, prospective, double-blind, placebo-controlled randomized trial to evaluate the effectiveness of a liquid herbal preparation from the roots of Pelargonium sidoides for decreasing the duration and severity of symptoms of the common cold.
Patient characteristics. Patients were recruited from 8 outpatient departments in Ukraine between December 2003 and May 2004. Two hundred and seven (207) patients were eligible. The number of ineligible and excluded patients was not stated. These 207 patients were randomized into 1 of 4 groups:
- 52 received 30 drops 3 times daily vs 51 patients who received placebo
- 52 patients received 60 drops 3 times daily vs 52 patients who received a higher-dose placebo.
The report gives the outcomes of the low-dose arm only. Two-thirds of the participants were women; all were Caucasian. Patients in the treatment and placebo groups were similar in terms of recurrent disease, prior use of medication for the common cold, smoking, and alcohol and caffeine consumption. All had a negative Group A beta-hemolytic strep test.
Inclusion criteria. Patients included men and women 18 to 55 years of age; able to provide written informed consent; with 2 major cold symptoms (nasal discharge, sore throat) and at least 1 minor cold symptom (nasal congestion, sneezing, scratchy throat, hoarseness, cough, headaches, muscle aches, or fever) or presence of 1 major cold symptom and at least 3 minor cold symptoms; duration of symptoms 24 to 48 hours.
Exclusion criteria were any acute ear, nose, throat and respiratory tract disease other than the common cold; positive rapid strep test; 6 or more episodes of recurrent tonsillitis, sinusitis, or otitis within the past 12 months or any chronic ear, nose, throat or respiratory tract disease; treatment with antibiotics, glucocorticoids, or antihistamine drugs during the 4 weeks prior to enrollment in the trial; treatment with cold medications that might impair the trial results (eg, decongestants, local anesthetics); and use of cough or pain relief medications, or any other treatment for the common cold within 7 days prior to enrollment in the trial.
Treatment regimen. Patients were assigned to take 30 drops of either the study herbal preparation or 30 drops of placebo 3 times daily, at least 30 minutes before or after a meal, from day 1 continuing to day 10. The investigational drug and placebo were supplied by Dr. Willmar Schwabe GmbH & Co. (Karlsruhe, Germany). The investigational medication is a preparation of the roots of P sidoides, extraction solution: ethanol 11% (1:8-10) (wt/wt). The placebo was matched for color, smell, taste, and viscosity. Paracetamol (acetaminophen) tablets were allowed for all patients for fever greater than 39°C.
Primary endpoint. Severity of cold symptoms was evaluated using the Cold Intensity Score (CIS), a validated scale derived from the sum of scores for 10 cold-related symptoms (nasal drainage, sore throat, nasal congestion, sneezing, scratchy throat, hoarseness, cough, headaches, muscle aches, and fever) on a scale of 0 to 4, where 0=not present and 4=very severe, to a maximum of 40 points. At baseline, the mean total CIS was comparable in both treatment and placebo groups (17.8±4.0 vs 16.9±3.4). From baseline to day 5, the mean total CIS decreased by 10.4±3.0 in the treatment group vs 5.6±4.3 in the placebo group (P<.0001).
Secondary endpoints. The number of patients achieving clinical cure (defined by CIS ≤1) by day 10 was significantly higher in the treatment group (78.8% vs 31.4%, P<.0001). The mean duration of days absent from work was significantly lower in the treatment group (6.9±1.8 vs 8.2±2.1, P<.0003), as was number of days with less than 100% usual activity level (7.1±1.5 vs 8.7±1.3, P<.0001). Data for both the primary and secondary endpoints were evaluated according to an intention-to-treat analysis. Both the intervention and placebo sides each had 4 patients that became ineligible after initial randomization. No patients were lost to follow-up.
Safety and tolerability. Patients in the low-dose arm experienced 3 nonserious adverse events, and 1 experienced mild epistaxis. Two additional patients (1 in the treatment and 1 in the placebo group) experienced moderate to severe tracheitis, not attributable to the study medication. Tolerability was rated slightly better in the treatment than placebo group on day 5. Forty-nine of 52 patients (94%) in the treatment group rated the preparation as good or very good tolerability vs 42 of 51 patients (82%) in the placebo group.
WHAT’S NEW?: A first
This is the first study that demonstrates the efficacy and safety of P sidoides in the treatment of the common cold. More importantly, this degree of improvement in cold symptoms is dramatically better than other common OTC treatments, including vitamin C, echinacea, and zinc preparations.
CAVEATS: How is this different from other cold remedies?
Patients are already spending a lot on cold remedies; this study suggests money would be better spent on having a ready supply of Pelargonium in the medicine cabinet, and it appears to be safe.
Other initially promising complementary and alternative therapies, such as zinc, echinacea, and vitamin C, have not been shown to be effective with more vigorous evaluation. We recognize that this is only 1 clinical trial, and the results may not be replicated in future trials. However, we are impressed by the effect size—twice the size as that seen for placebo, with a reduction in half of total cold symptom severity over 5 days and a reduction of missed time from work by more than a full day on average over placebo.
In vitro studies suggest a physiologic mechanism that is consistent with the study outcomes.
Similar findings are reported for symptom reduction in acute bronchitis.
Safety
There were no significant adverse events in this study, which is consistent with the findings of the studies of acute bronchitis.12-14P sidoides has been widely used in Germany since the 1980s, with an annual sale value in 2002 of $55 million or 4.1 million packages.
The Uppsala Monitoring Centre, in conjunction with the World Health Organization international pharmacovigilance program, received 34 case reports between 2002 and 2006 of allergic reactions to ethanolic herbal extract of Pelargonium root, 2 of which involved life-threatening circulatory collapse requiring emergency medical attention. Given the extremely rare occurrence of these events we believe the minimal risk is acceptable. The others involved rash and pruritus.
Also of note: contact dermatitis to Pelargonium houseplants has been reported. As a result, product information will be added to product packaging, warning of common reactions of gastrointestinal complaints (gastric pain, heartburn, nausea, and diarrhea) as well as the potential for serious allergic reaction. In addition, since some of the active compounds are plant coumarins, there is a theoretical risk of interaction with warfarin and aspirin but no serious bleeding events have been reported.16
It is also recommended that individuals with renal or hepatic disease or women who are pregnant or breastfeeding avoid use of this preparation, as safety studies have not been performed.
Other study design issues
A few other issues struck us as important when assessing the validity of this study. For example, 1 of the authors appears to be an employee of the pharmaceutical company that manufactures the preparation, raising the conflict of interest issue.
We were also curious about why the results of the high-dose arm were not reported in this manuscript. Could there have been a higher rate of adverse events in the high-dose arm? Knowing how many patients were ineligible or excluded, and the efficacy or safety in the high-dose arm would give us more confidence in the findings, but we decided that these were not necessarily fatal flaws.
Bottom line
Despite the above caveats, this was a well-designed randomized controlled trial that suggests that P sidoides is impressively efficacious in decreasing the duration and severity of the common cold. In the final analysis, we think that these findings justify recommending this to our patients.
CHALLENGES TO IMPLEMENTATION: 2-day window
The medication was started within 48 hours of the onset of symptoms. We generally see patients seeking treatment for the common cold well after the first 2 days. The efficacy of Pelargonium is no doubt less when started later in the course of the illness. Colds resolve spontaneously, so to get the benefit of this treatment, it likely must be started early.
Our conclusion is that patients could be advised to purchase the medication to have on hand at home at the start of the cold season.
Availability of the drug
P sidoides is available in the US under the brand name Umcka Coldcare.
The preparation used in the study is marketed in Europe by ISO-Arzneimittel17 under the name Umckaloabo, which is a combination of the Zulu words for lung symptoms and breast pain.18
Our Internet search on the term “Pelargonium sidoides” failed to yield a distributor of the German preparation used in the study that would be available in the United States. However, a different manufacturer, Nature’s Way, distributes a number of similar preparations containing extract of the root of P sidoides under the name Umcka Coldcare. Umcka Cold-care appears to be readily available for purchase, both on-line and through local health food stores, for less than $20 per 4-oz (120-mL) bottle. A different retailer, African Red Tea, offers syrup, 1:10 ethanolic extract for $29.95 for 100-mL bottle.19 Like the German preparation, these formulations are delivered by dropper.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
Offer patients Pelargonium sidoides (30 drops 3 times a day) to reduce the severity and duration of common cold symptoms and to get patients back to work sooner.1
Strength of recommendation
B: A single well-designed randomized controlled trial
Lizogub VG, Riley DS, Heger M. Efficacy of a Pelargonium sidoides preparation in patients with the common cold: A randomized, double blind, placebo-controlled clinical trial. Explore (NY) 2007; 3:573–584.
ILLUSTRATIVE CASE
A 39-year-old, otherwise healthy woman presents to your clinic with a sore throat, nasal congestion, and dry cough she’s had since yesterday. She wants an antibiotic, but your evaluation reveals an uncomplicated viral upper respiratory infection—a common cold. You would like to provide her with an alternative treatment, but you are aware of the lack of evidence for clear benefit of zinc lozenges, echinacea, and vitamin C. Is there any other medication that might benefit this patient?
Yes. Pelargonium sidoides, a species of South African geranium used for centuries in Zulu medicine,2 shows promise as an herbal remedy for respiratory infections. Two randomized trials show that extracts of P sidoides improve symptoms of acute bronchitis which, like the common cold, is usually caused by a virus.3-5
There is a plausible biological mechanism of action. In vitro studies show that Pelargonium extract induces the interferon system and up-regulates cytokines important in protecting host cells from viral infection.6
BACKGROUND: $17 billion dollar cold
Our patients want more relief from cold symptoms and are clearly willing to pay for it. Americans spend approximately $2.9 billion annually on over-the-counter (OTC) cold preparations and $1.1 billion on unnecessary antibiotics.7 The term “common cold” refers to a collection of symptoms, including sore throat, rhinorrhea, nasal congestion, cough, low-grade fever, and malaise, usually self-limited and lasting 10 to 14 days, caused by a number of viruses, most commonly by a rhinovirus.8 According to the 2005 National Ambulatory Medical Care Survey, the common cold is the third most common diagnosis in physicians’ offices behind only hypertension and well-infant/child visits.9 A 2001 US telephone survey determined that approximately 500 million episodes of non-influenza viral infection occur annually, resulting in direct costs of $17 billion for physician services and medications and approximately 200 million missed days of work.7
CLINICAL CONTEXT: Evidence proves most cold remedies don’t work
Although colds are common and result in annoying symptoms and missed work, much of the money spent on remedies is wasted. A truly effective treatment would be valuable to our patients.
Despite brisk sales, evidence for the efficacy of various cold remedies is inconclusive and contradictory. We found 6 Cochrane reviews of cold treatments, including antitussives, antihistamines, decongestants, vitamin C, echinacea, and zinc lozenges. With the exception of pseudoephedrine for nasal symptoms, the evidence that any product improves symptoms or decreases the duration of the cold is not encouraging.
Cough medications. The 2004 Cochrane Review of OTC medications for cough10 found no consistent evidence that any of them work. Codeine was no more effective than placebo for reducing cough symptoms. Three efficacy studies of dextromethorphan for cough showed either no difference or small but possibly clinically insignificant improvement in cough over placebo. One study of guaifenesin showed benefit over placebo in reducing cough frequency; another one showed no benefit over placebo.
Vitamin C, echinacea. Three Cochrane reviews found no conclusive evidence of benefit over placebo for either vitamin C11 or echinacea12 in treating the common cold.
Zinc. A new panel has been convened by the Cochrane group to reassess the effectiveness of zinc, but a 1999 Cochrane review13 found no benefit for zinc over placebo.
Antihistamines are not effective for relieving cold symptoms.14
Pseudoephedrine is the only medication with good-quality evidence for effectiveness, but only for reducing nasal symptoms.15 The authors concluded that patients may be encouraged to continue pseudoephedrine for up to 5 days if found to be effective with the first dose. Nasal congestion and discharge, however, are only 2 of the many irritating symptoms of a cold.
Bernard Ewigman, MD, MSPH
If you are in full-time clinical practice, a medical director of a practice, or otherwise directly involved in decision-making about adopting new practices, join our team of “reality checkers.”
Just email me at be.editor@gmail.com
STUDY SUMMARY: Duration and severity of symptoms are reduced
This was a multicenter, prospective, double-blind, placebo-controlled randomized trial to evaluate the effectiveness of a liquid herbal preparation from the roots of Pelargonium sidoides for decreasing the duration and severity of symptoms of the common cold.
Patient characteristics. Patients were recruited from 8 outpatient departments in Ukraine between December 2003 and May 2004. Two hundred and seven (207) patients were eligible. The number of ineligible and excluded patients was not stated. These 207 patients were randomized into 1 of 4 groups:
- 52 received 30 drops 3 times daily vs 51 patients who received placebo
- 52 patients received 60 drops 3 times daily vs 52 patients who received a higher-dose placebo.
The report gives the outcomes of the low-dose arm only. Two-thirds of the participants were women; all were Caucasian. Patients in the treatment and placebo groups were similar in terms of recurrent disease, prior use of medication for the common cold, smoking, and alcohol and caffeine consumption. All had a negative Group A beta-hemolytic strep test.
Inclusion criteria. Patients included men and women 18 to 55 years of age; able to provide written informed consent; with 2 major cold symptoms (nasal discharge, sore throat) and at least 1 minor cold symptom (nasal congestion, sneezing, scratchy throat, hoarseness, cough, headaches, muscle aches, or fever) or presence of 1 major cold symptom and at least 3 minor cold symptoms; duration of symptoms 24 to 48 hours.
Exclusion criteria were any acute ear, nose, throat and respiratory tract disease other than the common cold; positive rapid strep test; 6 or more episodes of recurrent tonsillitis, sinusitis, or otitis within the past 12 months or any chronic ear, nose, throat or respiratory tract disease; treatment with antibiotics, glucocorticoids, or antihistamine drugs during the 4 weeks prior to enrollment in the trial; treatment with cold medications that might impair the trial results (eg, decongestants, local anesthetics); and use of cough or pain relief medications, or any other treatment for the common cold within 7 days prior to enrollment in the trial.
Treatment regimen. Patients were assigned to take 30 drops of either the study herbal preparation or 30 drops of placebo 3 times daily, at least 30 minutes before or after a meal, from day 1 continuing to day 10. The investigational drug and placebo were supplied by Dr. Willmar Schwabe GmbH & Co. (Karlsruhe, Germany). The investigational medication is a preparation of the roots of P sidoides, extraction solution: ethanol 11% (1:8-10) (wt/wt). The placebo was matched for color, smell, taste, and viscosity. Paracetamol (acetaminophen) tablets were allowed for all patients for fever greater than 39°C.
Primary endpoint. Severity of cold symptoms was evaluated using the Cold Intensity Score (CIS), a validated scale derived from the sum of scores for 10 cold-related symptoms (nasal drainage, sore throat, nasal congestion, sneezing, scratchy throat, hoarseness, cough, headaches, muscle aches, and fever) on a scale of 0 to 4, where 0=not present and 4=very severe, to a maximum of 40 points. At baseline, the mean total CIS was comparable in both treatment and placebo groups (17.8±4.0 vs 16.9±3.4). From baseline to day 5, the mean total CIS decreased by 10.4±3.0 in the treatment group vs 5.6±4.3 in the placebo group (P<.0001).
Secondary endpoints. The number of patients achieving clinical cure (defined by CIS ≤1) by day 10 was significantly higher in the treatment group (78.8% vs 31.4%, P<.0001). The mean duration of days absent from work was significantly lower in the treatment group (6.9±1.8 vs 8.2±2.1, P<.0003), as was number of days with less than 100% usual activity level (7.1±1.5 vs 8.7±1.3, P<.0001). Data for both the primary and secondary endpoints were evaluated according to an intention-to-treat analysis. Both the intervention and placebo sides each had 4 patients that became ineligible after initial randomization. No patients were lost to follow-up.
Safety and tolerability. Patients in the low-dose arm experienced 3 nonserious adverse events, and 1 experienced mild epistaxis. Two additional patients (1 in the treatment and 1 in the placebo group) experienced moderate to severe tracheitis, not attributable to the study medication. Tolerability was rated slightly better in the treatment than placebo group on day 5. Forty-nine of 52 patients (94%) in the treatment group rated the preparation as good or very good tolerability vs 42 of 51 patients (82%) in the placebo group.
WHAT’S NEW?: A first
This is the first study that demonstrates the efficacy and safety of P sidoides in the treatment of the common cold. More importantly, this degree of improvement in cold symptoms is dramatically better than other common OTC treatments, including vitamin C, echinacea, and zinc preparations.
CAVEATS: How is this different from other cold remedies?
Patients are already spending a lot on cold remedies; this study suggests money would be better spent on having a ready supply of Pelargonium in the medicine cabinet, and it appears to be safe.
Other initially promising complementary and alternative therapies, such as zinc, echinacea, and vitamin C, have not been shown to be effective with more vigorous evaluation. We recognize that this is only 1 clinical trial, and the results may not be replicated in future trials. However, we are impressed by the effect size—twice the size as that seen for placebo, with a reduction in half of total cold symptom severity over 5 days and a reduction of missed time from work by more than a full day on average over placebo.
In vitro studies suggest a physiologic mechanism that is consistent with the study outcomes.
Similar findings are reported for symptom reduction in acute bronchitis.
Safety
There were no significant adverse events in this study, which is consistent with the findings of the studies of acute bronchitis.12-14P sidoides has been widely used in Germany since the 1980s, with an annual sale value in 2002 of $55 million or 4.1 million packages.
The Uppsala Monitoring Centre, in conjunction with the World Health Organization international pharmacovigilance program, received 34 case reports between 2002 and 2006 of allergic reactions to ethanolic herbal extract of Pelargonium root, 2 of which involved life-threatening circulatory collapse requiring emergency medical attention. Given the extremely rare occurrence of these events we believe the minimal risk is acceptable. The others involved rash and pruritus.
Also of note: contact dermatitis to Pelargonium houseplants has been reported. As a result, product information will be added to product packaging, warning of common reactions of gastrointestinal complaints (gastric pain, heartburn, nausea, and diarrhea) as well as the potential for serious allergic reaction. In addition, since some of the active compounds are plant coumarins, there is a theoretical risk of interaction with warfarin and aspirin but no serious bleeding events have been reported.16
It is also recommended that individuals with renal or hepatic disease or women who are pregnant or breastfeeding avoid use of this preparation, as safety studies have not been performed.
Other study design issues
A few other issues struck us as important when assessing the validity of this study. For example, 1 of the authors appears to be an employee of the pharmaceutical company that manufactures the preparation, raising the conflict of interest issue.
We were also curious about why the results of the high-dose arm were not reported in this manuscript. Could there have been a higher rate of adverse events in the high-dose arm? Knowing how many patients were ineligible or excluded, and the efficacy or safety in the high-dose arm would give us more confidence in the findings, but we decided that these were not necessarily fatal flaws.
Bottom line
Despite the above caveats, this was a well-designed randomized controlled trial that suggests that P sidoides is impressively efficacious in decreasing the duration and severity of the common cold. In the final analysis, we think that these findings justify recommending this to our patients.
CHALLENGES TO IMPLEMENTATION: 2-day window
The medication was started within 48 hours of the onset of symptoms. We generally see patients seeking treatment for the common cold well after the first 2 days. The efficacy of Pelargonium is no doubt less when started later in the course of the illness. Colds resolve spontaneously, so to get the benefit of this treatment, it likely must be started early.
Our conclusion is that patients could be advised to purchase the medication to have on hand at home at the start of the cold season.
Availability of the drug
P sidoides is available in the US under the brand name Umcka Coldcare.
The preparation used in the study is marketed in Europe by ISO-Arzneimittel17 under the name Umckaloabo, which is a combination of the Zulu words for lung symptoms and breast pain.18
Our Internet search on the term “Pelargonium sidoides” failed to yield a distributor of the German preparation used in the study that would be available in the United States. However, a different manufacturer, Nature’s Way, distributes a number of similar preparations containing extract of the root of P sidoides under the name Umcka Coldcare. Umcka Cold-care appears to be readily available for purchase, both on-line and through local health food stores, for less than $20 per 4-oz (120-mL) bottle. A different retailer, African Red Tea, offers syrup, 1:10 ethanolic extract for $29.95 for 100-mL bottle.19 Like the German preparation, these formulations are delivered by dropper.
PURLs methodology
This study was selected and evaluated using FPIN’s Priority Updates from the Research Literature (PURL) Surveillance System methodology. The criteria and findings leading to the selection of this study as a PURL can be accessed at www.jfponline.com/purls.
1. Lizogub VG, Riley DS, Heger M. Efficacy of a Pelargonium sidoides preparation in patients with the common cold: A randomized, double blind, placebo-controlled clinical trial. Explore (NY) 2007;3:573-584.
2. Bladt S, Wagner H. From Zulu medicine to the European phytomedicine Umckaloabo. Phytomedicine 2007;14 (suppl 1):2-4.
3. Matthys H, Eisebitt R, Seith B, Heger M. Efficacy and safety of an extract of Pelargonium sidoides (EPs 7630) in adults with acute bronchitis: A randomized, double-blind, placebo-controlled trial. Phytomedicine 2003;10(Suppl 4):7-17.
4. Chuchalin AG, Berman B, Lehmacher W. Treatment of acute bronchitis in adults with a Pelargonium sidoides preparation (EPs 7630): A randomized, double-blind, placebo-controlled trial. Explore (NY) 2005;1:437-445.
5. Matthys H, Heger M. Treatment of acute bronchitis with a liquid herbal drug preparation from Pelargonium sidoides (EPs 7630): A randomized, double-blind, placebo-controlled multicentre study. Curr Med Res Opinion 2007;23:323-331.
6. Kolodziej H, Kiderlen AF. In vitro evaluation of antibacterial and immunomodulatory activities of Pelargonium reniforme, Pelargonium sidoides and the related herbal drug preparation EPs 7630. Phytomedicine 2007;14 (suppl 1):18-26.
7. Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non-influenza related viral respiratory tract infection in the United States. Arch Intern Med 2003;163:487-494.
8. Heikkinen T, Jarvinen A. The common cold. Lancet 2003;361:51-59.
9. Cherry DK, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2005 Summary. Adv Data 2007;387:1-39.
10. Schroeder K, Fahey T. Over-the-counter medications for acute cough in children and adults in ambulatory settings. Cochrane Database Syst Rev 2004;(4):cD001831.-
11. Douglas RM, Hemila H, Chalker E, Treacy B. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev 2004;(4):cD000980.-
12. Linde K, Barrett B, Wolkart K, Bauer R, Melchart D. Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev 2006;(1):cD000530.-
13. Marshall I. Zinc for the common cold. Cochrane Database Syst Rev 1999;(2):cD001364.-(With-drawn 2006, Issue 3).
14. Sutter AI, Lemiengre M, Campbell H, Mackinnon HF. Anithistamines for the common cold. Cochrane Database Syst Rev 2003;(3):cD001267.-
15. Taverner D, Latte J, Draper M. Nasal decongestants for the common cold. Cochrane Database Syst Rev 2004;(3):cD001953.-
16. De Boer HJ, Hagemann U, Bate J, Meyboom RHB. Allergic reactions to medicines derived from Pelargonium species. Drug Saf 2007;30:677-680.
17. ISO-Arzneimittel. Distributor of Umckaloabo. Available at: umckaloabo.com. Accessed January 7, 2008.
18. Taylor PW, Maalim S, Coleman S. The strange story of umckaloabo. Pharm J 2005;275:790-792.
19. African Red Tea Imports. Available at: www.africanredtea.com/pelargonium-syrup.html. Accessed January 7, 2008.
1. Lizogub VG, Riley DS, Heger M. Efficacy of a Pelargonium sidoides preparation in patients with the common cold: A randomized, double blind, placebo-controlled clinical trial. Explore (NY) 2007;3:573-584.
2. Bladt S, Wagner H. From Zulu medicine to the European phytomedicine Umckaloabo. Phytomedicine 2007;14 (suppl 1):2-4.
3. Matthys H, Eisebitt R, Seith B, Heger M. Efficacy and safety of an extract of Pelargonium sidoides (EPs 7630) in adults with acute bronchitis: A randomized, double-blind, placebo-controlled trial. Phytomedicine 2003;10(Suppl 4):7-17.
4. Chuchalin AG, Berman B, Lehmacher W. Treatment of acute bronchitis in adults with a Pelargonium sidoides preparation (EPs 7630): A randomized, double-blind, placebo-controlled trial. Explore (NY) 2005;1:437-445.
5. Matthys H, Heger M. Treatment of acute bronchitis with a liquid herbal drug preparation from Pelargonium sidoides (EPs 7630): A randomized, double-blind, placebo-controlled multicentre study. Curr Med Res Opinion 2007;23:323-331.
6. Kolodziej H, Kiderlen AF. In vitro evaluation of antibacterial and immunomodulatory activities of Pelargonium reniforme, Pelargonium sidoides and the related herbal drug preparation EPs 7630. Phytomedicine 2007;14 (suppl 1):18-26.
7. Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non-influenza related viral respiratory tract infection in the United States. Arch Intern Med 2003;163:487-494.
8. Heikkinen T, Jarvinen A. The common cold. Lancet 2003;361:51-59.
9. Cherry DK, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2005 Summary. Adv Data 2007;387:1-39.
10. Schroeder K, Fahey T. Over-the-counter medications for acute cough in children and adults in ambulatory settings. Cochrane Database Syst Rev 2004;(4):cD001831.-
11. Douglas RM, Hemila H, Chalker E, Treacy B. Vitamin C for preventing and treating the common cold. Cochrane Database Syst Rev 2004;(4):cD000980.-
12. Linde K, Barrett B, Wolkart K, Bauer R, Melchart D. Echinacea for preventing and treating the common cold. Cochrane Database Syst Rev 2006;(1):cD000530.-
13. Marshall I. Zinc for the common cold. Cochrane Database Syst Rev 1999;(2):cD001364.-(With-drawn 2006, Issue 3).
14. Sutter AI, Lemiengre M, Campbell H, Mackinnon HF. Anithistamines for the common cold. Cochrane Database Syst Rev 2003;(3):cD001267.-
15. Taverner D, Latte J, Draper M. Nasal decongestants for the common cold. Cochrane Database Syst Rev 2004;(3):cD001953.-
16. De Boer HJ, Hagemann U, Bate J, Meyboom RHB. Allergic reactions to medicines derived from Pelargonium species. Drug Saf 2007;30:677-680.
17. ISO-Arzneimittel. Distributor of Umckaloabo. Available at: umckaloabo.com. Accessed January 7, 2008.
18. Taylor PW, Maalim S, Coleman S. The strange story of umckaloabo. Pharm J 2005;275:790-792.
19. African Red Tea Imports. Available at: www.africanredtea.com/pelargonium-syrup.html. Accessed January 7, 2008.