User login
What’s new in non-STEMI management
SNOWMASS, COLO. – An early invasive strategy is particularly beneficial in octogenarians with non–ST-segment elevation myocardial infarction, according to a recent study involving close to 1 million NSTEMI patients aged 80 years or older.
The very eldest are an understudied segment of the NSTEMI population, for whom an initial conservative strategy has been the dominant approach in daily practice.
"This is an important study. We can see that as you get older and older, by virtue of the fact that you have more and more coronary disease, probably you’re going to be better off with an invasive strategy, all other things being equal," Dr. David R. Holmes Jr. commented in highlighting the study at the Annual Cardiovascular Conference at Snowmass.
The study included 968,542 octogenarians hospitalized with NSTEMI during 2003-2010 and entered into the Nationwide Inpatient Sample. Eighty-three percent were managed via an initial conservative approach, with coronary angiography performed only in the event of hemodynamic or electrical instability, refractory angina despite optimal medical therapy, or a test result indicative of high risk. The other 17% underwent an early invasive approach, with angiography within 48 hours of presentation.
Octogenarians managed via an early invasive strategy were more often younger, obese, smokers, dyslipidemic, hypertensive, white, and male, and more likely to have known vascular disease. In a multivariate analysis adjusted for potential confounders, the early invasive strategy group had a 34% reduction in in-hospital mortality compared with the conservatively managed group. They also had a 37% lower rate of acute ischemic stroke, a 40% reduction in intracranial hemorrhage, a 37% lower risk of gastrointestinal bleeding, and a shorter length of stay by an average of half a day. On the other side of the ledger, they had a 2.1-fold increased rate of cardiogenic shock (Am. J. Med. 2013;126:1076-83).
Does time to cath lab matter?
Another recent study looked at the optimal time frame for taking an NSTEMI patient to the cardiac catheterization laboratory as part of an invasive strategy. This was a meta-analysis of seven randomized controlled trials totaling 5,370 NSTEMI patients, along with four observational studies with more than 77,000 NSTEMI patients. The conclusion: There is as yet no persuasive evidence that the time interval makes a difference in outcomes (Ann. Intern. Med. 2013;158:261-70).
"That’s the data that’s available. It doesn’t matter how quickly you get the patient to the cath lab within that first period of time. You just need to take them, whether it’s in 2 hours, 6 hours, or 18 hours," Dr. Holmes said.
This has important implications as we think about systems of care. If somebody comes into the hospital late on a Friday night, do you have to take them to the cath lab Friday night, or can you wait electively and take them tomorrow or potentially even Monday morning when everybody’s there?" commented Dr. Holmes, professor of medicine at the Mayo Clinic in Rochester, Minn.
GRACE and CRUSADE
The cornerstone of decision making as to whether to opt for an invasive versus a conservative strategy in a given NSTEMI patient involves application of a formal risk score. A plethora of these risk scoring systems are in use today. Which is the best choice for a cardiologist as an aid to decision making? A meta-analysis involving 36 studies with nearly 117,000 NSTEMI patients has concluded that the GRACE (Global Registry of Acute Cardiac Events) risk score (JAMA 2004;291:2727-33) is the best of the pack. It significantly outperformed the TIMI score, which is the other widely used scoring system, as well as others less widely known (Contemp. Clin. Trials 2012:33:507-14).
"GRACE looks like it performs better. We’ll need better ones in the future, of course. But at the present time, select GRACE for risk stratification," advised the cardiologist, adding that a Grace score app is available.
Despite the fact that physicians are diagnosing and treating NSTEMI earlier in its course, in large part because of the widespread use of troponin assays in the emergency department, NSTEMI is still associated with substantial long-term morbidity and mortality, particularly in the elderly. This was underscored in a recent analysis of 19,336 NSTEMI patients aged 65 years or older who underwent early catheterization and were included in the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines) registry.
Twenty-one percent of patients received medical management alone, 60.8% underwent percutaneous coronary intervention, and 18.2% had coronary artery bypass graft surgery. The 5-year unadjusted all-cause mortality rate was 50% in the medically managed group, 33.5% in older patients who underwent PCI, and 24.2% in those who underwent CABG surgery. The unadjusted 5-year rate of a composite of death, readmission for MI, or readmission for stroke was 62.4% with medical management, 44.9% with PCI, and 33% with CABG. The investigators concluded that long-term outcomes in elderly NSTEMI patients appear to be better in this large registry when revascularization is accomplished via CABG than with PCI. This sets the stage for future confirmatory trials (Circ. Cardiovasc. Qual. Outcomes 2013;6:323-32).
Dr. Holmes noted that the incidence of NSTEMI has climbed steadily while that of STEMI has declined over the past couple of decades, not just in the United States but worldwide. In Australia, for example, during 1993-2010 the adjusted incidence of NSTEMI increased by a whopping 315%, from 67 to 182 cases per 100,000 person-years, while the adjusted incidence of STEMI fell by 30% (Am. J. Cardiol. 2013;112:169-73).
"NSTEMI is clearly an annuity for all of cardiology," Dr. Holmes said. "The growth rate is increasing and it will continue to increase as we get older."
He reported having no conflicts of interest.
These studies collectively offer guidance in key management decisions for an invasive strategy for our NSTEMI patients, namely, the factor of age, the impact of timing, and risk stratification scores. Currently, the "less is more" approach is often taken for octogenarians, but a large sample size from this registry shows better results across a spectrum of outcomes even while adjusting for cofounders. This should prompt a reevaluation of current practice. Although the timing of an invasive approach in STEMI is defined in prior studies, this large meta-analysis tells us that timing in NSTEMI does not correlate with outcomes as long as angiography is pursued at some point in time, a very important conclusion.
Finally, although TIMI scoring systems are used at most institutions, the GRACE score performed even better, a surprising finding.
Taken in sum, these key studies should be followed up by randomized controlled trials to definitively answer these important questions for our NSTEMI patients.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital. He is on the advisory board of Hospitalist News.
These studies collectively offer guidance in key management decisions for an invasive strategy for our NSTEMI patients, namely, the factor of age, the impact of timing, and risk stratification scores. Currently, the "less is more" approach is often taken for octogenarians, but a large sample size from this registry shows better results across a spectrum of outcomes even while adjusting for cofounders. This should prompt a reevaluation of current practice. Although the timing of an invasive approach in STEMI is defined in prior studies, this large meta-analysis tells us that timing in NSTEMI does not correlate with outcomes as long as angiography is pursued at some point in time, a very important conclusion.
Finally, although TIMI scoring systems are used at most institutions, the GRACE score performed even better, a surprising finding.
Taken in sum, these key studies should be followed up by randomized controlled trials to definitively answer these important questions for our NSTEMI patients.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital. He is on the advisory board of Hospitalist News.
These studies collectively offer guidance in key management decisions for an invasive strategy for our NSTEMI patients, namely, the factor of age, the impact of timing, and risk stratification scores. Currently, the "less is more" approach is often taken for octogenarians, but a large sample size from this registry shows better results across a spectrum of outcomes even while adjusting for cofounders. This should prompt a reevaluation of current practice. Although the timing of an invasive approach in STEMI is defined in prior studies, this large meta-analysis tells us that timing in NSTEMI does not correlate with outcomes as long as angiography is pursued at some point in time, a very important conclusion.
Finally, although TIMI scoring systems are used at most institutions, the GRACE score performed even better, a surprising finding.
Taken in sum, these key studies should be followed up by randomized controlled trials to definitively answer these important questions for our NSTEMI patients.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital. He is on the advisory board of Hospitalist News.
SNOWMASS, COLO. – An early invasive strategy is particularly beneficial in octogenarians with non–ST-segment elevation myocardial infarction, according to a recent study involving close to 1 million NSTEMI patients aged 80 years or older.
The very eldest are an understudied segment of the NSTEMI population, for whom an initial conservative strategy has been the dominant approach in daily practice.
"This is an important study. We can see that as you get older and older, by virtue of the fact that you have more and more coronary disease, probably you’re going to be better off with an invasive strategy, all other things being equal," Dr. David R. Holmes Jr. commented in highlighting the study at the Annual Cardiovascular Conference at Snowmass.
The study included 968,542 octogenarians hospitalized with NSTEMI during 2003-2010 and entered into the Nationwide Inpatient Sample. Eighty-three percent were managed via an initial conservative approach, with coronary angiography performed only in the event of hemodynamic or electrical instability, refractory angina despite optimal medical therapy, or a test result indicative of high risk. The other 17% underwent an early invasive approach, with angiography within 48 hours of presentation.
Octogenarians managed via an early invasive strategy were more often younger, obese, smokers, dyslipidemic, hypertensive, white, and male, and more likely to have known vascular disease. In a multivariate analysis adjusted for potential confounders, the early invasive strategy group had a 34% reduction in in-hospital mortality compared with the conservatively managed group. They also had a 37% lower rate of acute ischemic stroke, a 40% reduction in intracranial hemorrhage, a 37% lower risk of gastrointestinal bleeding, and a shorter length of stay by an average of half a day. On the other side of the ledger, they had a 2.1-fold increased rate of cardiogenic shock (Am. J. Med. 2013;126:1076-83).
Does time to cath lab matter?
Another recent study looked at the optimal time frame for taking an NSTEMI patient to the cardiac catheterization laboratory as part of an invasive strategy. This was a meta-analysis of seven randomized controlled trials totaling 5,370 NSTEMI patients, along with four observational studies with more than 77,000 NSTEMI patients. The conclusion: There is as yet no persuasive evidence that the time interval makes a difference in outcomes (Ann. Intern. Med. 2013;158:261-70).
"That’s the data that’s available. It doesn’t matter how quickly you get the patient to the cath lab within that first period of time. You just need to take them, whether it’s in 2 hours, 6 hours, or 18 hours," Dr. Holmes said.
This has important implications as we think about systems of care. If somebody comes into the hospital late on a Friday night, do you have to take them to the cath lab Friday night, or can you wait electively and take them tomorrow or potentially even Monday morning when everybody’s there?" commented Dr. Holmes, professor of medicine at the Mayo Clinic in Rochester, Minn.
GRACE and CRUSADE
The cornerstone of decision making as to whether to opt for an invasive versus a conservative strategy in a given NSTEMI patient involves application of a formal risk score. A plethora of these risk scoring systems are in use today. Which is the best choice for a cardiologist as an aid to decision making? A meta-analysis involving 36 studies with nearly 117,000 NSTEMI patients has concluded that the GRACE (Global Registry of Acute Cardiac Events) risk score (JAMA 2004;291:2727-33) is the best of the pack. It significantly outperformed the TIMI score, which is the other widely used scoring system, as well as others less widely known (Contemp. Clin. Trials 2012:33:507-14).
"GRACE looks like it performs better. We’ll need better ones in the future, of course. But at the present time, select GRACE for risk stratification," advised the cardiologist, adding that a Grace score app is available.
Despite the fact that physicians are diagnosing and treating NSTEMI earlier in its course, in large part because of the widespread use of troponin assays in the emergency department, NSTEMI is still associated with substantial long-term morbidity and mortality, particularly in the elderly. This was underscored in a recent analysis of 19,336 NSTEMI patients aged 65 years or older who underwent early catheterization and were included in the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines) registry.
Twenty-one percent of patients received medical management alone, 60.8% underwent percutaneous coronary intervention, and 18.2% had coronary artery bypass graft surgery. The 5-year unadjusted all-cause mortality rate was 50% in the medically managed group, 33.5% in older patients who underwent PCI, and 24.2% in those who underwent CABG surgery. The unadjusted 5-year rate of a composite of death, readmission for MI, or readmission for stroke was 62.4% with medical management, 44.9% with PCI, and 33% with CABG. The investigators concluded that long-term outcomes in elderly NSTEMI patients appear to be better in this large registry when revascularization is accomplished via CABG than with PCI. This sets the stage for future confirmatory trials (Circ. Cardiovasc. Qual. Outcomes 2013;6:323-32).
Dr. Holmes noted that the incidence of NSTEMI has climbed steadily while that of STEMI has declined over the past couple of decades, not just in the United States but worldwide. In Australia, for example, during 1993-2010 the adjusted incidence of NSTEMI increased by a whopping 315%, from 67 to 182 cases per 100,000 person-years, while the adjusted incidence of STEMI fell by 30% (Am. J. Cardiol. 2013;112:169-73).
"NSTEMI is clearly an annuity for all of cardiology," Dr. Holmes said. "The growth rate is increasing and it will continue to increase as we get older."
He reported having no conflicts of interest.
SNOWMASS, COLO. – An early invasive strategy is particularly beneficial in octogenarians with non–ST-segment elevation myocardial infarction, according to a recent study involving close to 1 million NSTEMI patients aged 80 years or older.
The very eldest are an understudied segment of the NSTEMI population, for whom an initial conservative strategy has been the dominant approach in daily practice.
"This is an important study. We can see that as you get older and older, by virtue of the fact that you have more and more coronary disease, probably you’re going to be better off with an invasive strategy, all other things being equal," Dr. David R. Holmes Jr. commented in highlighting the study at the Annual Cardiovascular Conference at Snowmass.
The study included 968,542 octogenarians hospitalized with NSTEMI during 2003-2010 and entered into the Nationwide Inpatient Sample. Eighty-three percent were managed via an initial conservative approach, with coronary angiography performed only in the event of hemodynamic or electrical instability, refractory angina despite optimal medical therapy, or a test result indicative of high risk. The other 17% underwent an early invasive approach, with angiography within 48 hours of presentation.
Octogenarians managed via an early invasive strategy were more often younger, obese, smokers, dyslipidemic, hypertensive, white, and male, and more likely to have known vascular disease. In a multivariate analysis adjusted for potential confounders, the early invasive strategy group had a 34% reduction in in-hospital mortality compared with the conservatively managed group. They also had a 37% lower rate of acute ischemic stroke, a 40% reduction in intracranial hemorrhage, a 37% lower risk of gastrointestinal bleeding, and a shorter length of stay by an average of half a day. On the other side of the ledger, they had a 2.1-fold increased rate of cardiogenic shock (Am. J. Med. 2013;126:1076-83).
Does time to cath lab matter?
Another recent study looked at the optimal time frame for taking an NSTEMI patient to the cardiac catheterization laboratory as part of an invasive strategy. This was a meta-analysis of seven randomized controlled trials totaling 5,370 NSTEMI patients, along with four observational studies with more than 77,000 NSTEMI patients. The conclusion: There is as yet no persuasive evidence that the time interval makes a difference in outcomes (Ann. Intern. Med. 2013;158:261-70).
"That’s the data that’s available. It doesn’t matter how quickly you get the patient to the cath lab within that first period of time. You just need to take them, whether it’s in 2 hours, 6 hours, or 18 hours," Dr. Holmes said.
This has important implications as we think about systems of care. If somebody comes into the hospital late on a Friday night, do you have to take them to the cath lab Friday night, or can you wait electively and take them tomorrow or potentially even Monday morning when everybody’s there?" commented Dr. Holmes, professor of medicine at the Mayo Clinic in Rochester, Minn.
GRACE and CRUSADE
The cornerstone of decision making as to whether to opt for an invasive versus a conservative strategy in a given NSTEMI patient involves application of a formal risk score. A plethora of these risk scoring systems are in use today. Which is the best choice for a cardiologist as an aid to decision making? A meta-analysis involving 36 studies with nearly 117,000 NSTEMI patients has concluded that the GRACE (Global Registry of Acute Cardiac Events) risk score (JAMA 2004;291:2727-33) is the best of the pack. It significantly outperformed the TIMI score, which is the other widely used scoring system, as well as others less widely known (Contemp. Clin. Trials 2012:33:507-14).
"GRACE looks like it performs better. We’ll need better ones in the future, of course. But at the present time, select GRACE for risk stratification," advised the cardiologist, adding that a Grace score app is available.
Despite the fact that physicians are diagnosing and treating NSTEMI earlier in its course, in large part because of the widespread use of troponin assays in the emergency department, NSTEMI is still associated with substantial long-term morbidity and mortality, particularly in the elderly. This was underscored in a recent analysis of 19,336 NSTEMI patients aged 65 years or older who underwent early catheterization and were included in the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines) registry.
Twenty-one percent of patients received medical management alone, 60.8% underwent percutaneous coronary intervention, and 18.2% had coronary artery bypass graft surgery. The 5-year unadjusted all-cause mortality rate was 50% in the medically managed group, 33.5% in older patients who underwent PCI, and 24.2% in those who underwent CABG surgery. The unadjusted 5-year rate of a composite of death, readmission for MI, or readmission for stroke was 62.4% with medical management, 44.9% with PCI, and 33% with CABG. The investigators concluded that long-term outcomes in elderly NSTEMI patients appear to be better in this large registry when revascularization is accomplished via CABG than with PCI. This sets the stage for future confirmatory trials (Circ. Cardiovasc. Qual. Outcomes 2013;6:323-32).
Dr. Holmes noted that the incidence of NSTEMI has climbed steadily while that of STEMI has declined over the past couple of decades, not just in the United States but worldwide. In Australia, for example, during 1993-2010 the adjusted incidence of NSTEMI increased by a whopping 315%, from 67 to 182 cases per 100,000 person-years, while the adjusted incidence of STEMI fell by 30% (Am. J. Cardiol. 2013;112:169-73).
"NSTEMI is clearly an annuity for all of cardiology," Dr. Holmes said. "The growth rate is increasing and it will continue to increase as we get older."
He reported having no conflicts of interest.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Higher MAP target fails to improve sepsis survival
Use of a high mean arterial pressure during initial resuscitation in patients with septic shock did not improve mortality at 28 or 90 days in the multicenter, open-label SEPSISPAM trial.
The Surviving Sepsis Campaign guidelines recommend targeting a mean arterial pressure (MAP) of at least 65 mm Hg, but suggest a higher target may be better for patients with atherosclerosis or previous hypertension. Retrospective data also suggest a MAP of more than 75 mm Hg may be needed to maintain kidney function during early sepsis.
For the current trial, investigators at 29 centers in France evenly randomized 776 patients to vasopressor treatment adjusted to maintain a MAP of 80-85 mm Hg (high-target group) or 65-70 mm Hg (low-target group).
The study’s primary endpoint of all-cause mortality at 28 days was 36.5% in the high-target group and 34% in the low-target group (nonsignificant hazard ratio in the high-target group, 1.07), according to data presented at the International Symposium on Intensive Care and Emergency Medicine and simultaneously published online (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMoa1312173]).
In addition, there were no significant differences between the high- and low-target groups in the secondary outcomes of 90-day mortality (43.7% vs. 42.3%; HR, 1.04), need for mechanical ventilation, ICU length of stay, or Sequential Organ Failure Assessment score at day 7.
Atrial fibrillation, however, was significantly more common in the high-target group than in the low-target group, at 6.7%, compared with 2.8%. This could be related to the high-target group receiving significantly higher doses of vasopressor catecholamines over a significantly longer time period, although other confounding factors cannot be ruled out, lead author Dr. Pierre Asfar of University Hospital of Angers (France), reported on behalf of SEPSISPAM investigators.
Among patients with chronic arterial hypertension, who comprised more than 40% of the study population, use of the high MAP target significantly reduced both the incidence of doubling of plasma creatinine (39% vs. 52%) and the rate of renal-replacement therapy (31.7% vs. 42.2%).
The authors noted that, although investigators were asked to treat patients to a MAP of 65-70 mm Hg in the low-target group, the observed pressures were for the most part between 70 and 75 mm Hg. The high-target group was likewise off goal, at a mean of 70 mm Hg. They also acknowledged that the lower-than-expected death rate, albeit in line with more recent trials, led to an underpowered study.
The French Ministry of Health funded the trial. Dr. Asfar reported lecture fees from LFB Biomedicaments.
Use of a high mean arterial pressure during initial resuscitation in patients with septic shock did not improve mortality at 28 or 90 days in the multicenter, open-label SEPSISPAM trial.
The Surviving Sepsis Campaign guidelines recommend targeting a mean arterial pressure (MAP) of at least 65 mm Hg, but suggest a higher target may be better for patients with atherosclerosis or previous hypertension. Retrospective data also suggest a MAP of more than 75 mm Hg may be needed to maintain kidney function during early sepsis.
For the current trial, investigators at 29 centers in France evenly randomized 776 patients to vasopressor treatment adjusted to maintain a MAP of 80-85 mm Hg (high-target group) or 65-70 mm Hg (low-target group).
The study’s primary endpoint of all-cause mortality at 28 days was 36.5% in the high-target group and 34% in the low-target group (nonsignificant hazard ratio in the high-target group, 1.07), according to data presented at the International Symposium on Intensive Care and Emergency Medicine and simultaneously published online (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMoa1312173]).
In addition, there were no significant differences between the high- and low-target groups in the secondary outcomes of 90-day mortality (43.7% vs. 42.3%; HR, 1.04), need for mechanical ventilation, ICU length of stay, or Sequential Organ Failure Assessment score at day 7.
Atrial fibrillation, however, was significantly more common in the high-target group than in the low-target group, at 6.7%, compared with 2.8%. This could be related to the high-target group receiving significantly higher doses of vasopressor catecholamines over a significantly longer time period, although other confounding factors cannot be ruled out, lead author Dr. Pierre Asfar of University Hospital of Angers (France), reported on behalf of SEPSISPAM investigators.
Among patients with chronic arterial hypertension, who comprised more than 40% of the study population, use of the high MAP target significantly reduced both the incidence of doubling of plasma creatinine (39% vs. 52%) and the rate of renal-replacement therapy (31.7% vs. 42.2%).
The authors noted that, although investigators were asked to treat patients to a MAP of 65-70 mm Hg in the low-target group, the observed pressures were for the most part between 70 and 75 mm Hg. The high-target group was likewise off goal, at a mean of 70 mm Hg. They also acknowledged that the lower-than-expected death rate, albeit in line with more recent trials, led to an underpowered study.
The French Ministry of Health funded the trial. Dr. Asfar reported lecture fees from LFB Biomedicaments.
Use of a high mean arterial pressure during initial resuscitation in patients with septic shock did not improve mortality at 28 or 90 days in the multicenter, open-label SEPSISPAM trial.
The Surviving Sepsis Campaign guidelines recommend targeting a mean arterial pressure (MAP) of at least 65 mm Hg, but suggest a higher target may be better for patients with atherosclerosis or previous hypertension. Retrospective data also suggest a MAP of more than 75 mm Hg may be needed to maintain kidney function during early sepsis.
For the current trial, investigators at 29 centers in France evenly randomized 776 patients to vasopressor treatment adjusted to maintain a MAP of 80-85 mm Hg (high-target group) or 65-70 mm Hg (low-target group).
The study’s primary endpoint of all-cause mortality at 28 days was 36.5% in the high-target group and 34% in the low-target group (nonsignificant hazard ratio in the high-target group, 1.07), according to data presented at the International Symposium on Intensive Care and Emergency Medicine and simultaneously published online (N. Engl. J. Med. 2014 March 18 [doi:10.1056/NEJMoa1312173]).
In addition, there were no significant differences between the high- and low-target groups in the secondary outcomes of 90-day mortality (43.7% vs. 42.3%; HR, 1.04), need for mechanical ventilation, ICU length of stay, or Sequential Organ Failure Assessment score at day 7.
Atrial fibrillation, however, was significantly more common in the high-target group than in the low-target group, at 6.7%, compared with 2.8%. This could be related to the high-target group receiving significantly higher doses of vasopressor catecholamines over a significantly longer time period, although other confounding factors cannot be ruled out, lead author Dr. Pierre Asfar of University Hospital of Angers (France), reported on behalf of SEPSISPAM investigators.
Among patients with chronic arterial hypertension, who comprised more than 40% of the study population, use of the high MAP target significantly reduced both the incidence of doubling of plasma creatinine (39% vs. 52%) and the rate of renal-replacement therapy (31.7% vs. 42.2%).
The authors noted that, although investigators were asked to treat patients to a MAP of 65-70 mm Hg in the low-target group, the observed pressures were for the most part between 70 and 75 mm Hg. The high-target group was likewise off goal, at a mean of 70 mm Hg. They also acknowledged that the lower-than-expected death rate, albeit in line with more recent trials, led to an underpowered study.
The French Ministry of Health funded the trial. Dr. Asfar reported lecture fees from LFB Biomedicaments.
FROM ISICEM 2014
Major finding: The 28-day mortality was 36.5% in the high-target group and 34% in the low-target group (P = .57).
Data source: A multicenter, open-label trial of 776 patients with septic shock who were treated to a low (60-65 mm Hg) or high (80-85 mm Hg) target mean arterial pressure.
Disclosures: The French Ministry of Health funded the trial. Dr. Asfar reported lecture fees from LFB Biomedicaments.
MicroRNA MIR-25 found to play key role in heart failure
A microRNA called MIR-25 is a key mediator of poor cardiac contractility in heart failure, according to a report published online March 12 in Nature.
The findings "suggest that inhibition of MIR-25 may be a novel therapeutic strategy for the treatment of heart failure," wrote Dr. Mark Mercola at Sanford-Burnham Medical Research Institute and the University of California, San Diego, and his associates (Nature 2014 March 12 [doi:10.1038/nature13073]).
The researchers developed a robotic high-throughput screening tool that they used to test 875 human microRNAs. They found that the microRNA MIR-25 markedly delayed calcium update kinetics in cardiomyocytes in vitro and was unregulated in myocardial samples from both mice and humans with severe heart failure.
Researchers also observed a significant decrease in left ventricular contractile function in mice when they used adeno-associated virus 9 (AAV9) to increase MIR-25 levels by about 50%.
Furthermore, the progression of heart failure in mice halted when the investigators injected them with an antisense oligonucleotide (antagomiR) against MIR-25. Furthermore, both cardiac function and survival improved significantly compared with mice injected with a control antagomiR.
The microRNA MIR-25 suppresses messenger RNA encoding a calcium-transporting ATPase called SERCA2a, which is the main mechanism for calcium uptake by cardiomyocytes during excitation-contraction coupling, the researchers said. Decreased SERCA2a activity is a major cause of poor contractility and cardiomyopathy, they noted.
The findings "identified MIR-25 as a critical repressor of SERCA2a and cardiac function during heart failure," the investigators said, adding that delayed calcium uptake kinetics in advanced heart failure are also mediated by changes in potassium channel density, sodium-calcium exchanger expression, and myofilament sensitivity to calcium.
The study was supported by the California Institute for Regenerative Medicine, the National Institutes of Health, Fondation Leducq, and the Sanford-Burnham Medical Research Institute. The authors declared no conflicts of interest.
A microRNA called MIR-25 is a key mediator of poor cardiac contractility in heart failure, according to a report published online March 12 in Nature.
The findings "suggest that inhibition of MIR-25 may be a novel therapeutic strategy for the treatment of heart failure," wrote Dr. Mark Mercola at Sanford-Burnham Medical Research Institute and the University of California, San Diego, and his associates (Nature 2014 March 12 [doi:10.1038/nature13073]).
The researchers developed a robotic high-throughput screening tool that they used to test 875 human microRNAs. They found that the microRNA MIR-25 markedly delayed calcium update kinetics in cardiomyocytes in vitro and was unregulated in myocardial samples from both mice and humans with severe heart failure.
Researchers also observed a significant decrease in left ventricular contractile function in mice when they used adeno-associated virus 9 (AAV9) to increase MIR-25 levels by about 50%.
Furthermore, the progression of heart failure in mice halted when the investigators injected them with an antisense oligonucleotide (antagomiR) against MIR-25. Furthermore, both cardiac function and survival improved significantly compared with mice injected with a control antagomiR.
The microRNA MIR-25 suppresses messenger RNA encoding a calcium-transporting ATPase called SERCA2a, which is the main mechanism for calcium uptake by cardiomyocytes during excitation-contraction coupling, the researchers said. Decreased SERCA2a activity is a major cause of poor contractility and cardiomyopathy, they noted.
The findings "identified MIR-25 as a critical repressor of SERCA2a and cardiac function during heart failure," the investigators said, adding that delayed calcium uptake kinetics in advanced heart failure are also mediated by changes in potassium channel density, sodium-calcium exchanger expression, and myofilament sensitivity to calcium.
The study was supported by the California Institute for Regenerative Medicine, the National Institutes of Health, Fondation Leducq, and the Sanford-Burnham Medical Research Institute. The authors declared no conflicts of interest.
A microRNA called MIR-25 is a key mediator of poor cardiac contractility in heart failure, according to a report published online March 12 in Nature.
The findings "suggest that inhibition of MIR-25 may be a novel therapeutic strategy for the treatment of heart failure," wrote Dr. Mark Mercola at Sanford-Burnham Medical Research Institute and the University of California, San Diego, and his associates (Nature 2014 March 12 [doi:10.1038/nature13073]).
The researchers developed a robotic high-throughput screening tool that they used to test 875 human microRNAs. They found that the microRNA MIR-25 markedly delayed calcium update kinetics in cardiomyocytes in vitro and was unregulated in myocardial samples from both mice and humans with severe heart failure.
Researchers also observed a significant decrease in left ventricular contractile function in mice when they used adeno-associated virus 9 (AAV9) to increase MIR-25 levels by about 50%.
Furthermore, the progression of heart failure in mice halted when the investigators injected them with an antisense oligonucleotide (antagomiR) against MIR-25. Furthermore, both cardiac function and survival improved significantly compared with mice injected with a control antagomiR.
The microRNA MIR-25 suppresses messenger RNA encoding a calcium-transporting ATPase called SERCA2a, which is the main mechanism for calcium uptake by cardiomyocytes during excitation-contraction coupling, the researchers said. Decreased SERCA2a activity is a major cause of poor contractility and cardiomyopathy, they noted.
The findings "identified MIR-25 as a critical repressor of SERCA2a and cardiac function during heart failure," the investigators said, adding that delayed calcium uptake kinetics in advanced heart failure are also mediated by changes in potassium channel density, sodium-calcium exchanger expression, and myofilament sensitivity to calcium.
The study was supported by the California Institute for Regenerative Medicine, the National Institutes of Health, Fondation Leducq, and the Sanford-Burnham Medical Research Institute. The authors declared no conflicts of interest.
FROM NATURE
Major finding: The microRNA MIR-25 markedly delayed calcium update by cardiomyocytes in vitro and was unregulated in mice and humans with heart failure. Overexpression of MIR-25 was associated with decreased heart muscle contractility, while inhibiting MIR-25 stopped the progression of heart failure in mice.
Data source: High-throughput functional screening of the human microRNAome.
Disclosures: The California Institute for Regenerative Medicine, the National Institutes of Health, Fondation Leducq, and the Sanford-Burnham Medical Research Institute supported the research. The authors declared no conflicts of interest.
First guidelines on pulmonary hypertension in sickle cell disease released
UPDATED 3/17/14*
The first treatment guidelines for pulmonary hypertension in sickle cell disease are now available from the American Thoracic Society.
Because more effective treatments has extended the lives of patients with the disease, their risk of mortality from pulmonary hypertension and elevated tricuspid regurgitant jet velocity has increased. Until now, however, there has been no standardized approach for identifying and managing these conditions.
The guidelines are published in the March 15 issue of the American Journal of Respiratory Critical Care Medicine.
The multidisciplinary committee that wrote the guidelines defined mortality risk as a tricuspid regurgitant velocity (TRV) of at least 2.5 m/second; an N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level of at least 160 pg/mL; or pulmonary hypertension (PH) confirmed by a right heart catheterization (RHC).
Patients with elevated mortality risk should be treated with hydroxyurea as first-line therapy. Chronic transfusion therapy for patients who are not candidates for or responsive to hydroxyurea is noted as a "weak recommendation."
For those with RHC-confirmed pulmonary hypertension, venous thromboembolism, and no additional risk factors for hemorrhage, indefinite – not limited – anticoagulant therapy is recommended.
For patients with either an elevated TRV or an elevated NT-pro-BNP level, the guidelines strongly recommend against pulmonary hypertensive–specific therapies such as prostanoid, endothelin-receptor antagonist, and phosphodiesterase-5 inhibitor therapy. The same guidance was given for patients who have RHC-confirmed PH.
While the guidelines recommend against targeted therapies for RHC-confirmed PH, a trial of either a prostanoid or an endothelin-receptor antagonist is recommended for patients with confirmed PH and elevated pulmonary vascular resistance, normal pulmonary capillary wedge pressure, and related symptoms. These patients should not be given phosphodiesterase-5 inhibitor therapy as first-line treatment.
The lack of both large-scale clinical trials in this population and integrated standards of care limit the guidelines’ effect, Dr. Elizabeth S. Klings, who chaired the guidelines committee, noted in a written statement. "Management of [these patients] will ultimately be a collaborative effort including adult and pediatric pulmonologists, cardiologists, and hematologists," added Dr. Klings of the department of medicine at Boston University.
Dr. Klings receives support from NIH grant R21HL107993.
Commentary – ‘Guidelines are a breath of fresh air’
Dr. Susan Millard comments: "I think the guidelines are a breath of fresh air. I feel they are very well thought out. More research needs to be done on the therapies for pulmonary hypertension, but the authors of these guidelines admit that there is a paucity of data in this area.

In addition, more collaboration is needed between our pulmonary, hematology, oncology, and cardiology specialties. Pulmonologists do not perform right heart catheterizations, but when we ask cardiologists about pulmonary hypertension concerns, we regularly get shot down by the ones who feel that echocardiograms are sufficient to look for this problem. Yet when we want help managing these patients, they don’t want to do that either because it is pulmonary hypertension. You need a dedicated group of people locally to work-up these patients.
There are not many experienced pulmonary hypertension centers easily accessible for both adult and pediatric patient referrals. It is difficult, for example, to refer patients out of state and get it approved by insurance companies.
Dr. Millard is a pediatric pulmonologist at Helen DeVos Children’s Hospital, Grand Rapids, Mich., and a CHEST board member.
*Dr. David Langleben responds: Cardiology input is essential [for patients with sickle cell disease being evaluated for pulmonary hypertension]. A multidisciplinary approach always benefits the patient. The patients may have high output cardiac failure, diastolic dysfunction, cardiomyopathies and myocardial ischemia. Heart catheterization is indispensable, as is echocardiography. They are complementary.
Dr. Langleben is professor of medicine at McGill University and director of cardiology and of the Centre for Pulmonary Vascular Disease at Jewish General Hospital, both in Montreal.
UPDATED 3/17/14*
The first treatment guidelines for pulmonary hypertension in sickle cell disease are now available from the American Thoracic Society.
Because more effective treatments has extended the lives of patients with the disease, their risk of mortality from pulmonary hypertension and elevated tricuspid regurgitant jet velocity has increased. Until now, however, there has been no standardized approach for identifying and managing these conditions.
The guidelines are published in the March 15 issue of the American Journal of Respiratory Critical Care Medicine.
The multidisciplinary committee that wrote the guidelines defined mortality risk as a tricuspid regurgitant velocity (TRV) of at least 2.5 m/second; an N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level of at least 160 pg/mL; or pulmonary hypertension (PH) confirmed by a right heart catheterization (RHC).
Patients with elevated mortality risk should be treated with hydroxyurea as first-line therapy. Chronic transfusion therapy for patients who are not candidates for or responsive to hydroxyurea is noted as a "weak recommendation."
For those with RHC-confirmed pulmonary hypertension, venous thromboembolism, and no additional risk factors for hemorrhage, indefinite – not limited – anticoagulant therapy is recommended.
For patients with either an elevated TRV or an elevated NT-pro-BNP level, the guidelines strongly recommend against pulmonary hypertensive–specific therapies such as prostanoid, endothelin-receptor antagonist, and phosphodiesterase-5 inhibitor therapy. The same guidance was given for patients who have RHC-confirmed PH.
While the guidelines recommend against targeted therapies for RHC-confirmed PH, a trial of either a prostanoid or an endothelin-receptor antagonist is recommended for patients with confirmed PH and elevated pulmonary vascular resistance, normal pulmonary capillary wedge pressure, and related symptoms. These patients should not be given phosphodiesterase-5 inhibitor therapy as first-line treatment.
The lack of both large-scale clinical trials in this population and integrated standards of care limit the guidelines’ effect, Dr. Elizabeth S. Klings, who chaired the guidelines committee, noted in a written statement. "Management of [these patients] will ultimately be a collaborative effort including adult and pediatric pulmonologists, cardiologists, and hematologists," added Dr. Klings of the department of medicine at Boston University.
Dr. Klings receives support from NIH grant R21HL107993.
Commentary – ‘Guidelines are a breath of fresh air’
Dr. Susan Millard comments: "I think the guidelines are a breath of fresh air. I feel they are very well thought out. More research needs to be done on the therapies for pulmonary hypertension, but the authors of these guidelines admit that there is a paucity of data in this area.
In addition, more collaboration is needed between our pulmonary, hematology, oncology, and cardiology specialties. Pulmonologists do not perform right heart catheterizations, but when we ask cardiologists about pulmonary hypertension concerns, we regularly get shot down by the ones who feel that echocardiograms are sufficient to look for this problem. Yet when we want help managing these patients, they don’t want to do that either because it is pulmonary hypertension. You need a dedicated group of people locally to work-up these patients.
There are not many experienced pulmonary hypertension centers easily accessible for both adult and pediatric patient referrals. It is difficult, for example, to refer patients out of state and get it approved by insurance companies.
Dr. Millard is a pediatric pulmonologist at Helen DeVos Children’s Hospital, Grand Rapids, Mich., and a CHEST board member.
*Dr. David Langleben responds: Cardiology input is essential [for patients with sickle cell disease being evaluated for pulmonary hypertension]. A multidisciplinary approach always benefits the patient. The patients may have high output cardiac failure, diastolic dysfunction, cardiomyopathies and myocardial ischemia. Heart catheterization is indispensable, as is echocardiography. They are complementary.
Dr. Langleben is professor of medicine at McGill University and director of cardiology and of the Centre for Pulmonary Vascular Disease at Jewish General Hospital, both in Montreal.
UPDATED 3/17/14*
The first treatment guidelines for pulmonary hypertension in sickle cell disease are now available from the American Thoracic Society.
Because more effective treatments has extended the lives of patients with the disease, their risk of mortality from pulmonary hypertension and elevated tricuspid regurgitant jet velocity has increased. Until now, however, there has been no standardized approach for identifying and managing these conditions.
The guidelines are published in the March 15 issue of the American Journal of Respiratory Critical Care Medicine.
The multidisciplinary committee that wrote the guidelines defined mortality risk as a tricuspid regurgitant velocity (TRV) of at least 2.5 m/second; an N-terminal pro-brain natriuretic peptide (NT-pro-BNP) level of at least 160 pg/mL; or pulmonary hypertension (PH) confirmed by a right heart catheterization (RHC).
Patients with elevated mortality risk should be treated with hydroxyurea as first-line therapy. Chronic transfusion therapy for patients who are not candidates for or responsive to hydroxyurea is noted as a "weak recommendation."
For those with RHC-confirmed pulmonary hypertension, venous thromboembolism, and no additional risk factors for hemorrhage, indefinite – not limited – anticoagulant therapy is recommended.
For patients with either an elevated TRV or an elevated NT-pro-BNP level, the guidelines strongly recommend against pulmonary hypertensive–specific therapies such as prostanoid, endothelin-receptor antagonist, and phosphodiesterase-5 inhibitor therapy. The same guidance was given for patients who have RHC-confirmed PH.
While the guidelines recommend against targeted therapies for RHC-confirmed PH, a trial of either a prostanoid or an endothelin-receptor antagonist is recommended for patients with confirmed PH and elevated pulmonary vascular resistance, normal pulmonary capillary wedge pressure, and related symptoms. These patients should not be given phosphodiesterase-5 inhibitor therapy as first-line treatment.
The lack of both large-scale clinical trials in this population and integrated standards of care limit the guidelines’ effect, Dr. Elizabeth S. Klings, who chaired the guidelines committee, noted in a written statement. "Management of [these patients] will ultimately be a collaborative effort including adult and pediatric pulmonologists, cardiologists, and hematologists," added Dr. Klings of the department of medicine at Boston University.
Dr. Klings receives support from NIH grant R21HL107993.
Commentary – ‘Guidelines are a breath of fresh air’
Dr. Susan Millard comments: "I think the guidelines are a breath of fresh air. I feel they are very well thought out. More research needs to be done on the therapies for pulmonary hypertension, but the authors of these guidelines admit that there is a paucity of data in this area.
In addition, more collaboration is needed between our pulmonary, hematology, oncology, and cardiology specialties. Pulmonologists do not perform right heart catheterizations, but when we ask cardiologists about pulmonary hypertension concerns, we regularly get shot down by the ones who feel that echocardiograms are sufficient to look for this problem. Yet when we want help managing these patients, they don’t want to do that either because it is pulmonary hypertension. You need a dedicated group of people locally to work-up these patients.
There are not many experienced pulmonary hypertension centers easily accessible for both adult and pediatric patient referrals. It is difficult, for example, to refer patients out of state and get it approved by insurance companies.
Dr. Millard is a pediatric pulmonologist at Helen DeVos Children’s Hospital, Grand Rapids, Mich., and a CHEST board member.
*Dr. David Langleben responds: Cardiology input is essential [for patients with sickle cell disease being evaluated for pulmonary hypertension]. A multidisciplinary approach always benefits the patient. The patients may have high output cardiac failure, diastolic dysfunction, cardiomyopathies and myocardial ischemia. Heart catheterization is indispensable, as is echocardiography. They are complementary.
Dr. Langleben is professor of medicine at McGill University and director of cardiology and of the Centre for Pulmonary Vascular Disease at Jewish General Hospital, both in Montreal.
FROM AMERICAN JOURNAL OF RESPIRATORY CRITICAL CARE MEDICINE

HFPEF’s diverse features pose management and trial challenges
When the highly-anticipated results from the TOPCAT trial reported last November failed to show a statistically significant efficacy benefit from spironolactone treatment in patients with heart failure and preserved left ventricular ejection fraction for the study’s primary endpoint of death or heart failure hospitalization, the neutral result represented more than another failed treatment trial in this rapidly expanding patient population that remains bereft of treatments with proven efficacy.
TOPCAT’s results also underscored the heterogeneity of patients diagnosed with heart failure with preserved ejection fraction (HFPEF), a signature feature of the syndrome. Heterogeneity is believed to have played a large role in the lack of success in TOPCAT as well as in several other major HFPEF trials.

Although HFPEF is defined as patients who exhibit clear clinical symptoms of heart failure but with a LVEF of at least 45%, and more recently at least 50%, what’s become increasingly clear as neutral trial results accumulate is that HFPEF is a syndrome. Far from a single pathologic entity, it can have different etiologies and present as different subtypes in a spectrum of abnormalities and severities.
HFPEF "is not just a simple disease of diastolic function and a stiff ventricle. It’s a very complicated, highly integrated, multisystem failure of cardiovascular and peripheral reserve," said Dr. Barry A. Borlaug, a cardiologist at the Mayo Clinic in Rochester, Minn. "A lot of us are coming to the conclusion that there are different subphenotypes of HFPEF, each with unique mechanisms and clinical trajectories that probably need unique treatment," he said in an interview.
"This is a very heterogeneous syndrome with no one etiology and a wide range of patients, some with marked ventricular hypertrophy, some with diastolic dysfunction, some who are fairly asymptomatic but become symptomatic with exercise, some who are compensated and stable, and others who are uncompensated. The spectrum of disease is very broad, and it may be many diseases," said Dr. Scott D. Solomon, professor of medicine at Harvard Medical School and director of noninvasive cardiology at Brigham and Women’s Hospital, Boston.
Last year, the heart failure literature featured two editorials spelling out proposed visions of the HFPEF spectrum. One of these proposed three characteristic types of HFPEF patients (J. Am. Coll. Cardiol. 2013;62:1339-42): those with exercise-induced diastolic dysfunction with no symptoms at rest, minimal fluid retention, and never hospitalized for heart failure but with long-standing hypertension and exercise intolerance; patients with volume overload and edema, recently hospitalized heart failure with dyspnea on exertion, and moderately severe heart failure symptoms; and the worst form, patients who have developed pulmonary hypertension and right ventricular failure as a consequence of their HFPEF and now have frequent heart failure hospitalizations. But patients do not necessarily progress from one severity stage to the next, noted Dr. Sanjiv J. Shah, a cardiologist at Northwestern University, Chicago, who wrote the editorial.

"Patients can progress back and forth across the spectrum" or remain in one stage, he said in an interview. "The syndrome is quite heterogeneous, not only in clinical presentation, but in etiology, and pathophysiology. There is still much to learn about the natural history of HFPEF , how it develops, and the trajectory of patients."
The second editorial described several relatively common HFPEF phenotypes that can appear individually or in combination, including filling limitation, ejection limitation, cardioacceleration, and vasoregulation (Eur. Heart J. 2013;34:1393-5). "Patients with heart failure caused by severe mitral insufficiency or aortic stenosis will clearly behave differently and respond to treatments differently from patients with hypertropic cardiomyopathy, constrictive pericarditis, or high-output heart failure. However, despite this heterogeneity these entities continue currently to be lumped together into the category of HFPEF," Dr. Borlaug wrote in this editorial.
The perils of heterogeneity
In addition to providing a better framework for understanding the causes and consequences of HFPEF, the paradigm of HFPEF as a heterogeneous syndrome also helps explain why the major intervention trials that focused on HFPEF patients, starting a decade ago with studies such as CHARM Preserved (Lancet 2003;362:777-81) and I-PRESERVE (N. Engl. J. Med. 2008;359:2456-67), and continuing through to the recent TOPCAT, have all failed to produce a statistically significant benefit for their primary endpoints.
"Heterogeneity confounds our ability to identify effective treatments. It’s the most likely single explanation" for the neutral HFPEF trials, Dr. Borlaug said. "I don’t think it’s as simple as one thing, but my speculation is that it’s the dominant reason."

"Many trials such as CHARM Preserved and TOPCAT seemed to enroll some patients who in retrospect did not have HFPEF," noted Dr. Gregg C. Fonarow, professor of medicine and associate chief of cardiology at UCLA in Los Angeles. "The key to future clinical trials will be better classification of HFPEF" and better matching of HFPEF patients to their treatment, said Dr. Shah.
"In the neutral megatrials some of the patients did not have HFPEF but had other disorders such as deconditioning and obesity – things that cannot be helped by treatments directed at the heart. We need to identify the patients who will respond to the treatment," said Dr. Burkert M. Pieske, professor and director of cardiology at the Medical University of Graz, Austria.
The TOPCAT (Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist) results reported last November exemplified the problem of patient heterogeneity. The study enrolled more than 3,400 patients in six countries: Argentina, Brazil, Canada, Russia, the Republic of Georgia, and the United States. Retrospective analysis showed that among patients in the placebo group, the primary endpoint of death or heart failure hospitalization during follow-up occurred at a rate of 12.6 events/100 patient-years among the 881 patients treated in the four Western Hemisphere countries, and at a rate of 2.3 events/100 patient-years among the 842 patients treated in Russia or Georgia, a greater than fivefold difference between the two subgroups.
"As a whole, the patients in Russia and Georgia had a lower event rate and were certainly less severely ill than the other patients, but they supposedly still had heart failure. Defining this disorder is difficult, and when a patient has signs and symptoms of heart failure and preserved ejection fraction you may not be certain that heart failure is causing the symptoms. That’s why many people think that we should use another criterion" to define HFPEF in trials, such as elevated serum level of some form of natriuretic peptide, said Dr. Solomon, a TOPCAT coinvestigator. By design, patients could enter TOPCAT either because of a recent heart failure hospitalization, which is how 72% of patients got in, or by having a threshold level of natriuretic peptide, the way the remaining 28% entered the study. Within the subgroup enrolled by natriuretic peptide level, spironolactone treatment had a statistically significant effect in reducing the primary endpoint, while in the other 72% the drug produced no discernable benefit over placebo.

"TOPCAT had funding problems, recruitment problems, and monitoring problems. There was not enough money for good monitoring," said Dr. Pieske, who did not participate in TOPCAT. The patients enrolled in Russia and Georgia were "unbelievably stable," with their 2.3/100 patient-years event rate. "Even if the drug works, it can’t exert an effect if there are no events."
Dr. Pieske ran a much smaller study of spironolactone involving 422 patients with HFPEF, the Aldosterone Receptor Blockade in Diastolic Heart Failure (Aldo-DHF) trial, which showed efficacy for the endpoint of improved diastolic function but not for the co-endpoint of improved exercise capacity (JAMA 2013;309:781-91).
"If you look at TOPCAT and Aldo-DHF together and ask, does spironolactone work, the answer is yes if you select the right patients, those with clear evidence of cardiac functional abnormalities and increased natriuretic peptide levels or documented hospitalization for heart failure. The drug clearly works in these patients, but there were enough inconsistencies in these trials so that this will not get into the treatment guidelines," Dr. Pieske said in an interview.
"Spironolactone provides most benefit in patients who are volume overloaded, have right-heart failure, or both. These are also the patients most likely to have elevated natriuretic peptide. Spironolactone does not seem to benefit as much early-stage HFPEF," noted Dr. Shah.

Several experts cautioned that because the TOPCAT results failed to produce a statistically significant benefit for the study’s primary endpoint, any other conclusions from the results must be made very cautiously, and several also said that they wanted to see the full, published results which had not appeared as of late February. They also noted that many patients with HFPEF, most likely a majority, do not have elevated blood levels of natriuretic peptide.
Where HFPEF management stands now
Evidence-based guidelines for the specific treatment of HFPEF are simple. There aren’t any.
The American Heart Association/American College of Cardiology heart failure management guidelines released last October made no disease-specific treatment recommendations (J. Amer. Coll. Cardiol. 2013;62:e147-e239). They call for controlling hypertension in patients who need intervention by prevailing standards, treatment with a diuretic in patients with volume overload, coronary revascularization if coronary disease is present, and management of atrial fibrillation if that’s present. The European Society of Cardiology’s guidelines issued in 2012 say pretty much the same (Eur. J. Cardiol. 2012;33:1787-1847), except they add this statement: "No treatment has yet been shown, convincingly, to reduce morbidity and mortality in patients with HFPEF."
If nothing else, TOPCAT’s results further solidified spironolactone’s role as a reasonably safe drug for blood pressure lowering in HFPEF patients who are also hypertensive. Hypertension control is a must for patients with HFPEF as it’s believed to significantly contribute to HFPEF in most patients. "Hypertension is the most common underlying cause of HFPEF," said Dr. John R. Teerlink, professor of medicine and director of the heart failure program at the San Francisco Veterans Affairs Medical Center.

When it comes to treating hypertension in HFPEF patients, "unless there is a contraindication, spironolactone should be one of the first drugs to try, but I’m not sure you can say it’s the first choice" based on current evidence, Dr. Borlaug said.
A diuretic is an obvious antihypertensive for HFPEF patients with fluid overload. And there were suggestions of benefit from the ACE inhibitor perindopril in elderly patients in the PEP-CHF trial (Eur. Heart J. 2006;27:2338-45), another large HFPEF-treatment trial that failed to show significant benefit for the primary endpoint with perindopril treatment but had positive results in some secondary endpoints.
Patients "get these drugs to treat their hypertension, but we believe they may also help their heart failure. It’s a belief system. My colleagues and I already use a lot of spironolactone to treat hypertension, and the TOPCAT results won’t change my practice. I’m not comfortable telling people that you should use an aldosterone antagonist because of TOPCAT," Dr. Teerlink said in an interview.
"An angiotensin-converting enzyme inhibitor will probably work; spironolactone probably works if you get the diagnosis right; we don’t know about beta-blockers; and there is some evidence for using digoxin," said Dr. John G.F. Cleland, professor of cardiology at the University of Hull, Kingston-upon-Hull, England. "There must also be good treatment of hypertension, and judicious use of diuretics."
"I’m careful with beta-blockers; I’ve had some patients who felt miserable on them," said Dr. Borlaug. "Some HFPEF patients don’t have a stroke volume, they don’t have diastole, all they have is heart rate, and if you take that away they are left with no cardiac output."
Aside from controlling blood pressure, experts advise good management of other comorbidities such as coronary disease, atrial fibrillation, diabetes, sleep disordered breathing, and renal disease. "Clinicians should make sure that they are not missing severe coronary artery disease, infiltrative cardiomyopathy, constrictive pericarditis, or other causes of HFPEF that have specific treatments," said Dr. Shah. Some drugs have shown promise in early-phase studies – such as ivabradine and neprilysin – but phase III trials are needed. "My advice on how to manage patients with HFPEF is to make every effort to enroll them in a randomized clinical trial," said Dr. Fonarow.

Another key is making the diagnosis, ideally to prevent development of irreversible cardiovascular damage. "HFPEF is difficult to diagnose with certainty unless you do a cardiac catheterization to measure filling pressures, but in patients with early-stage HFPEF, even their invasive hemodynamics look pretty normal," said Dr. Borlaug. Another approach is an exercise echo, which is noninvasive and can identify stress-induced diastolic dysfunction, but the sensitivity and specificity of this approach remains uncertain, he said. And an elevated natriuretic peptide level can help nail the HFPEF diagnosis in some patients but many other patients have levels within the normal range.
To find HFPEF patients, apply a low index of suspicion and look for breathlessness, loss of functional capacity, signs of congestion, lung crackles, echocardiographic signs, pulmonary artery hypertension, and an enlarged left atrium, he suggested.
"Finding patients is a big challenge," said Dr. Pieske. HFPEF patients tend to be elderly, women, and people who are obese who have hypertension and perhaps diabetes. "They complain of dyspnea and fatigue and many physicians think this is just how it is. They will not consider that there is a true diagnosis behind these symptoms and complaints," especially if the patient has preserved left ventricular ejection fraction and a normal natriuretic peptide level." A diastolic stress test using exercise and an echo exam may identify stable patients with early-stage diastolic dysfunction but this requires confirmation, he said.
HFPEF dominates heart failure, lacks good treatment
Experts say the onus on physicians to diagnose and manage HFPEF will grow substantially, since HFPEF is not only highly prevalent but also increasing faster than heart failure with reduced ejection fraction (HFREF). Results from 13 community-based studies published during 1997-2006 showed that HFPEF represented an average of 55% of all heart failure cases, Dr. Carolyn S.P. Lam said last November during a talk at the American Heart Association’s scientific sessions.

Two recent reports of U.S. data documented that the increasing prevalence of HFPEF is outpacing that of HFREF by 1% per year, driven by the aging of the American population (older age is a risk factor for HFPEF) and by the increasing prevalence of comorbidities that contribute to HFPEF. One of the reports, based on U.S. national data collected by the Get With the Guidelines Program, extrapolated that by the end of this decade about 65% of all patients hospitalized for heart failure will have a left ventricular ejection fraction of 40% or greater, the vast majority with HFPEF (Curr. Heart Fail. Rep. 2013;10:401-10). What’s coming is a HFPEF "epidemic," said Dr. Lam, a cardiologist at the National University Heart Centre in Singapore.
The fact that HFPEF is now at least as prevalent as HFREF, that it is about as lethal independent of what comorbidities might contribute, and that it is growing more prevalent than HFREF sharply contrasts with the absence of treatments with proven efficacy. How did that happen?
"Research into HFPEF is decades behind research into HFREF," said Dr. Fonarow. "HFPEF was largely ignored because the prevailing wisdom [20 or so years ago] was that it represented only a small proportion of cases and that outcomes were much better compared with HFREF." Only with registry data and community-based studies run more recently did cardiologists realize that outcomes from HFPEF were as bad as from HFREF. Progress was further hampered by enrollment of patients who did not have HFPEF or a broad spectrum of patients unable to respond equally well to the treatment under study.
"There are large gaps in knowledge of the pathophysiology of HFPEF and little investment has been made to identify potential therapeutic targets. This creates cascading levels of challenges for developing effective treatments despite the massive unmet need," said Dr. Fonarow.
"We don’t know what to treat yet," was Dr. Teerlink’s summation of the HFPEF dilemma.
Dr. Borlaug said that he has been a consultant to GlaxoSmithKline, Merck, Amgen, CardioKinetix, and DC Devices and has received research support from Atcor. Dr. Solomon said he has been a consultant to and received research support from Novartis and more than 10 other drug and device companies. Dr. Pieske said that he has received honoraria from Bayer, Boehringer Ingelheim, Servier, Medtronic, Bristol-Myers Squibb, Menarini, and Novartis and received research support from Bayer and Medtronic. Dr. Shah said that he has been a consultant to Novartis, Bayer Schering, and the Pulmonary Hypertension Association. Dr. Fonarow said that he has been a consultant to Medtronic, Novartis, and Pfizer. Dr. Teerlink said that he has been an adviser to and received research support from Novartis. Dr. Cleland said that he has received honoraria from Novartis and research funding from Pfizer. Dr. Lam said that she has been a consultant to Bayer, Novartis, and DC Devices and has received research support from Boston Scientific, Medtronic, and Vifor Pharma.
On Twitter @mitchelzoler
When the highly-anticipated results from the TOPCAT trial reported last November failed to show a statistically significant efficacy benefit from spironolactone treatment in patients with heart failure and preserved left ventricular ejection fraction for the study’s primary endpoint of death or heart failure hospitalization, the neutral result represented more than another failed treatment trial in this rapidly expanding patient population that remains bereft of treatments with proven efficacy.
TOPCAT’s results also underscored the heterogeneity of patients diagnosed with heart failure with preserved ejection fraction (HFPEF), a signature feature of the syndrome. Heterogeneity is believed to have played a large role in the lack of success in TOPCAT as well as in several other major HFPEF trials.
Although HFPEF is defined as patients who exhibit clear clinical symptoms of heart failure but with a LVEF of at least 45%, and more recently at least 50%, what’s become increasingly clear as neutral trial results accumulate is that HFPEF is a syndrome. Far from a single pathologic entity, it can have different etiologies and present as different subtypes in a spectrum of abnormalities and severities.
HFPEF "is not just a simple disease of diastolic function and a stiff ventricle. It’s a very complicated, highly integrated, multisystem failure of cardiovascular and peripheral reserve," said Dr. Barry A. Borlaug, a cardiologist at the Mayo Clinic in Rochester, Minn. "A lot of us are coming to the conclusion that there are different subphenotypes of HFPEF, each with unique mechanisms and clinical trajectories that probably need unique treatment," he said in an interview.
"This is a very heterogeneous syndrome with no one etiology and a wide range of patients, some with marked ventricular hypertrophy, some with diastolic dysfunction, some who are fairly asymptomatic but become symptomatic with exercise, some who are compensated and stable, and others who are uncompensated. The spectrum of disease is very broad, and it may be many diseases," said Dr. Scott D. Solomon, professor of medicine at Harvard Medical School and director of noninvasive cardiology at Brigham and Women’s Hospital, Boston.
Last year, the heart failure literature featured two editorials spelling out proposed visions of the HFPEF spectrum. One of these proposed three characteristic types of HFPEF patients (J. Am. Coll. Cardiol. 2013;62:1339-42): those with exercise-induced diastolic dysfunction with no symptoms at rest, minimal fluid retention, and never hospitalized for heart failure but with long-standing hypertension and exercise intolerance; patients with volume overload and edema, recently hospitalized heart failure with dyspnea on exertion, and moderately severe heart failure symptoms; and the worst form, patients who have developed pulmonary hypertension and right ventricular failure as a consequence of their HFPEF and now have frequent heart failure hospitalizations. But patients do not necessarily progress from one severity stage to the next, noted Dr. Sanjiv J. Shah, a cardiologist at Northwestern University, Chicago, who wrote the editorial.
"Patients can progress back and forth across the spectrum" or remain in one stage, he said in an interview. "The syndrome is quite heterogeneous, not only in clinical presentation, but in etiology, and pathophysiology. There is still much to learn about the natural history of HFPEF , how it develops, and the trajectory of patients."
The second editorial described several relatively common HFPEF phenotypes that can appear individually or in combination, including filling limitation, ejection limitation, cardioacceleration, and vasoregulation (Eur. Heart J. 2013;34:1393-5). "Patients with heart failure caused by severe mitral insufficiency or aortic stenosis will clearly behave differently and respond to treatments differently from patients with hypertropic cardiomyopathy, constrictive pericarditis, or high-output heart failure. However, despite this heterogeneity these entities continue currently to be lumped together into the category of HFPEF," Dr. Borlaug wrote in this editorial.
The perils of heterogeneity
In addition to providing a better framework for understanding the causes and consequences of HFPEF, the paradigm of HFPEF as a heterogeneous syndrome also helps explain why the major intervention trials that focused on HFPEF patients, starting a decade ago with studies such as CHARM Preserved (Lancet 2003;362:777-81) and I-PRESERVE (N. Engl. J. Med. 2008;359:2456-67), and continuing through to the recent TOPCAT, have all failed to produce a statistically significant benefit for their primary endpoints.
"Heterogeneity confounds our ability to identify effective treatments. It’s the most likely single explanation" for the neutral HFPEF trials, Dr. Borlaug said. "I don’t think it’s as simple as one thing, but my speculation is that it’s the dominant reason."
"Many trials such as CHARM Preserved and TOPCAT seemed to enroll some patients who in retrospect did not have HFPEF," noted Dr. Gregg C. Fonarow, professor of medicine and associate chief of cardiology at UCLA in Los Angeles. "The key to future clinical trials will be better classification of HFPEF" and better matching of HFPEF patients to their treatment, said Dr. Shah.
"In the neutral megatrials some of the patients did not have HFPEF but had other disorders such as deconditioning and obesity – things that cannot be helped by treatments directed at the heart. We need to identify the patients who will respond to the treatment," said Dr. Burkert M. Pieske, professor and director of cardiology at the Medical University of Graz, Austria.
The TOPCAT (Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist) results reported last November exemplified the problem of patient heterogeneity. The study enrolled more than 3,400 patients in six countries: Argentina, Brazil, Canada, Russia, the Republic of Georgia, and the United States. Retrospective analysis showed that among patients in the placebo group, the primary endpoint of death or heart failure hospitalization during follow-up occurred at a rate of 12.6 events/100 patient-years among the 881 patients treated in the four Western Hemisphere countries, and at a rate of 2.3 events/100 patient-years among the 842 patients treated in Russia or Georgia, a greater than fivefold difference between the two subgroups.
"As a whole, the patients in Russia and Georgia had a lower event rate and were certainly less severely ill than the other patients, but they supposedly still had heart failure. Defining this disorder is difficult, and when a patient has signs and symptoms of heart failure and preserved ejection fraction you may not be certain that heart failure is causing the symptoms. That’s why many people think that we should use another criterion" to define HFPEF in trials, such as elevated serum level of some form of natriuretic peptide, said Dr. Solomon, a TOPCAT coinvestigator. By design, patients could enter TOPCAT either because of a recent heart failure hospitalization, which is how 72% of patients got in, or by having a threshold level of natriuretic peptide, the way the remaining 28% entered the study. Within the subgroup enrolled by natriuretic peptide level, spironolactone treatment had a statistically significant effect in reducing the primary endpoint, while in the other 72% the drug produced no discernable benefit over placebo.
"TOPCAT had funding problems, recruitment problems, and monitoring problems. There was not enough money for good monitoring," said Dr. Pieske, who did not participate in TOPCAT. The patients enrolled in Russia and Georgia were "unbelievably stable," with their 2.3/100 patient-years event rate. "Even if the drug works, it can’t exert an effect if there are no events."
Dr. Pieske ran a much smaller study of spironolactone involving 422 patients with HFPEF, the Aldosterone Receptor Blockade in Diastolic Heart Failure (Aldo-DHF) trial, which showed efficacy for the endpoint of improved diastolic function but not for the co-endpoint of improved exercise capacity (JAMA 2013;309:781-91).
"If you look at TOPCAT and Aldo-DHF together and ask, does spironolactone work, the answer is yes if you select the right patients, those with clear evidence of cardiac functional abnormalities and increased natriuretic peptide levels or documented hospitalization for heart failure. The drug clearly works in these patients, but there were enough inconsistencies in these trials so that this will not get into the treatment guidelines," Dr. Pieske said in an interview.
"Spironolactone provides most benefit in patients who are volume overloaded, have right-heart failure, or both. These are also the patients most likely to have elevated natriuretic peptide. Spironolactone does not seem to benefit as much early-stage HFPEF," noted Dr. Shah.
Several experts cautioned that because the TOPCAT results failed to produce a statistically significant benefit for the study’s primary endpoint, any other conclusions from the results must be made very cautiously, and several also said that they wanted to see the full, published results which had not appeared as of late February. They also noted that many patients with HFPEF, most likely a majority, do not have elevated blood levels of natriuretic peptide.
Where HFPEF management stands now
Evidence-based guidelines for the specific treatment of HFPEF are simple. There aren’t any.
The American Heart Association/American College of Cardiology heart failure management guidelines released last October made no disease-specific treatment recommendations (J. Amer. Coll. Cardiol. 2013;62:e147-e239). They call for controlling hypertension in patients who need intervention by prevailing standards, treatment with a diuretic in patients with volume overload, coronary revascularization if coronary disease is present, and management of atrial fibrillation if that’s present. The European Society of Cardiology’s guidelines issued in 2012 say pretty much the same (Eur. J. Cardiol. 2012;33:1787-1847), except they add this statement: "No treatment has yet been shown, convincingly, to reduce morbidity and mortality in patients with HFPEF."
If nothing else, TOPCAT’s results further solidified spironolactone’s role as a reasonably safe drug for blood pressure lowering in HFPEF patients who are also hypertensive. Hypertension control is a must for patients with HFPEF as it’s believed to significantly contribute to HFPEF in most patients. "Hypertension is the most common underlying cause of HFPEF," said Dr. John R. Teerlink, professor of medicine and director of the heart failure program at the San Francisco Veterans Affairs Medical Center.
When it comes to treating hypertension in HFPEF patients, "unless there is a contraindication, spironolactone should be one of the first drugs to try, but I’m not sure you can say it’s the first choice" based on current evidence, Dr. Borlaug said.
A diuretic is an obvious antihypertensive for HFPEF patients with fluid overload. And there were suggestions of benefit from the ACE inhibitor perindopril in elderly patients in the PEP-CHF trial (Eur. Heart J. 2006;27:2338-45), another large HFPEF-treatment trial that failed to show significant benefit for the primary endpoint with perindopril treatment but had positive results in some secondary endpoints.
Patients "get these drugs to treat their hypertension, but we believe they may also help their heart failure. It’s a belief system. My colleagues and I already use a lot of spironolactone to treat hypertension, and the TOPCAT results won’t change my practice. I’m not comfortable telling people that you should use an aldosterone antagonist because of TOPCAT," Dr. Teerlink said in an interview.
"An angiotensin-converting enzyme inhibitor will probably work; spironolactone probably works if you get the diagnosis right; we don’t know about beta-blockers; and there is some evidence for using digoxin," said Dr. John G.F. Cleland, professor of cardiology at the University of Hull, Kingston-upon-Hull, England. "There must also be good treatment of hypertension, and judicious use of diuretics."
"I’m careful with beta-blockers; I’ve had some patients who felt miserable on them," said Dr. Borlaug. "Some HFPEF patients don’t have a stroke volume, they don’t have diastole, all they have is heart rate, and if you take that away they are left with no cardiac output."
Aside from controlling blood pressure, experts advise good management of other comorbidities such as coronary disease, atrial fibrillation, diabetes, sleep disordered breathing, and renal disease. "Clinicians should make sure that they are not missing severe coronary artery disease, infiltrative cardiomyopathy, constrictive pericarditis, or other causes of HFPEF that have specific treatments," said Dr. Shah. Some drugs have shown promise in early-phase studies – such as ivabradine and neprilysin – but phase III trials are needed. "My advice on how to manage patients with HFPEF is to make every effort to enroll them in a randomized clinical trial," said Dr. Fonarow.
Another key is making the diagnosis, ideally to prevent development of irreversible cardiovascular damage. "HFPEF is difficult to diagnose with certainty unless you do a cardiac catheterization to measure filling pressures, but in patients with early-stage HFPEF, even their invasive hemodynamics look pretty normal," said Dr. Borlaug. Another approach is an exercise echo, which is noninvasive and can identify stress-induced diastolic dysfunction, but the sensitivity and specificity of this approach remains uncertain, he said. And an elevated natriuretic peptide level can help nail the HFPEF diagnosis in some patients but many other patients have levels within the normal range.
To find HFPEF patients, apply a low index of suspicion and look for breathlessness, loss of functional capacity, signs of congestion, lung crackles, echocardiographic signs, pulmonary artery hypertension, and an enlarged left atrium, he suggested.
"Finding patients is a big challenge," said Dr. Pieske. HFPEF patients tend to be elderly, women, and people who are obese who have hypertension and perhaps diabetes. "They complain of dyspnea and fatigue and many physicians think this is just how it is. They will not consider that there is a true diagnosis behind these symptoms and complaints," especially if the patient has preserved left ventricular ejection fraction and a normal natriuretic peptide level." A diastolic stress test using exercise and an echo exam may identify stable patients with early-stage diastolic dysfunction but this requires confirmation, he said.
HFPEF dominates heart failure, lacks good treatment
Experts say the onus on physicians to diagnose and manage HFPEF will grow substantially, since HFPEF is not only highly prevalent but also increasing faster than heart failure with reduced ejection fraction (HFREF). Results from 13 community-based studies published during 1997-2006 showed that HFPEF represented an average of 55% of all heart failure cases, Dr. Carolyn S.P. Lam said last November during a talk at the American Heart Association’s scientific sessions.
Two recent reports of U.S. data documented that the increasing prevalence of HFPEF is outpacing that of HFREF by 1% per year, driven by the aging of the American population (older age is a risk factor for HFPEF) and by the increasing prevalence of comorbidities that contribute to HFPEF. One of the reports, based on U.S. national data collected by the Get With the Guidelines Program, extrapolated that by the end of this decade about 65% of all patients hospitalized for heart failure will have a left ventricular ejection fraction of 40% or greater, the vast majority with HFPEF (Curr. Heart Fail. Rep. 2013;10:401-10). What’s coming is a HFPEF "epidemic," said Dr. Lam, a cardiologist at the National University Heart Centre in Singapore.
The fact that HFPEF is now at least as prevalent as HFREF, that it is about as lethal independent of what comorbidities might contribute, and that it is growing more prevalent than HFREF sharply contrasts with the absence of treatments with proven efficacy. How did that happen?
"Research into HFPEF is decades behind research into HFREF," said Dr. Fonarow. "HFPEF was largely ignored because the prevailing wisdom [20 or so years ago] was that it represented only a small proportion of cases and that outcomes were much better compared with HFREF." Only with registry data and community-based studies run more recently did cardiologists realize that outcomes from HFPEF were as bad as from HFREF. Progress was further hampered by enrollment of patients who did not have HFPEF or a broad spectrum of patients unable to respond equally well to the treatment under study.
"There are large gaps in knowledge of the pathophysiology of HFPEF and little investment has been made to identify potential therapeutic targets. This creates cascading levels of challenges for developing effective treatments despite the massive unmet need," said Dr. Fonarow.
"We don’t know what to treat yet," was Dr. Teerlink’s summation of the HFPEF dilemma.
Dr. Borlaug said that he has been a consultant to GlaxoSmithKline, Merck, Amgen, CardioKinetix, and DC Devices and has received research support from Atcor. Dr. Solomon said he has been a consultant to and received research support from Novartis and more than 10 other drug and device companies. Dr. Pieske said that he has received honoraria from Bayer, Boehringer Ingelheim, Servier, Medtronic, Bristol-Myers Squibb, Menarini, and Novartis and received research support from Bayer and Medtronic. Dr. Shah said that he has been a consultant to Novartis, Bayer Schering, and the Pulmonary Hypertension Association. Dr. Fonarow said that he has been a consultant to Medtronic, Novartis, and Pfizer. Dr. Teerlink said that he has been an adviser to and received research support from Novartis. Dr. Cleland said that he has received honoraria from Novartis and research funding from Pfizer. Dr. Lam said that she has been a consultant to Bayer, Novartis, and DC Devices and has received research support from Boston Scientific, Medtronic, and Vifor Pharma.
On Twitter @mitchelzoler
When the highly-anticipated results from the TOPCAT trial reported last November failed to show a statistically significant efficacy benefit from spironolactone treatment in patients with heart failure and preserved left ventricular ejection fraction for the study’s primary endpoint of death or heart failure hospitalization, the neutral result represented more than another failed treatment trial in this rapidly expanding patient population that remains bereft of treatments with proven efficacy.
TOPCAT’s results also underscored the heterogeneity of patients diagnosed with heart failure with preserved ejection fraction (HFPEF), a signature feature of the syndrome. Heterogeneity is believed to have played a large role in the lack of success in TOPCAT as well as in several other major HFPEF trials.
Although HFPEF is defined as patients who exhibit clear clinical symptoms of heart failure but with a LVEF of at least 45%, and more recently at least 50%, what’s become increasingly clear as neutral trial results accumulate is that HFPEF is a syndrome. Far from a single pathologic entity, it can have different etiologies and present as different subtypes in a spectrum of abnormalities and severities.
HFPEF "is not just a simple disease of diastolic function and a stiff ventricle. It’s a very complicated, highly integrated, multisystem failure of cardiovascular and peripheral reserve," said Dr. Barry A. Borlaug, a cardiologist at the Mayo Clinic in Rochester, Minn. "A lot of us are coming to the conclusion that there are different subphenotypes of HFPEF, each with unique mechanisms and clinical trajectories that probably need unique treatment," he said in an interview.
"This is a very heterogeneous syndrome with no one etiology and a wide range of patients, some with marked ventricular hypertrophy, some with diastolic dysfunction, some who are fairly asymptomatic but become symptomatic with exercise, some who are compensated and stable, and others who are uncompensated. The spectrum of disease is very broad, and it may be many diseases," said Dr. Scott D. Solomon, professor of medicine at Harvard Medical School and director of noninvasive cardiology at Brigham and Women’s Hospital, Boston.
Last year, the heart failure literature featured two editorials spelling out proposed visions of the HFPEF spectrum. One of these proposed three characteristic types of HFPEF patients (J. Am. Coll. Cardiol. 2013;62:1339-42): those with exercise-induced diastolic dysfunction with no symptoms at rest, minimal fluid retention, and never hospitalized for heart failure but with long-standing hypertension and exercise intolerance; patients with volume overload and edema, recently hospitalized heart failure with dyspnea on exertion, and moderately severe heart failure symptoms; and the worst form, patients who have developed pulmonary hypertension and right ventricular failure as a consequence of their HFPEF and now have frequent heart failure hospitalizations. But patients do not necessarily progress from one severity stage to the next, noted Dr. Sanjiv J. Shah, a cardiologist at Northwestern University, Chicago, who wrote the editorial.
"Patients can progress back and forth across the spectrum" or remain in one stage, he said in an interview. "The syndrome is quite heterogeneous, not only in clinical presentation, but in etiology, and pathophysiology. There is still much to learn about the natural history of HFPEF , how it develops, and the trajectory of patients."
The second editorial described several relatively common HFPEF phenotypes that can appear individually or in combination, including filling limitation, ejection limitation, cardioacceleration, and vasoregulation (Eur. Heart J. 2013;34:1393-5). "Patients with heart failure caused by severe mitral insufficiency or aortic stenosis will clearly behave differently and respond to treatments differently from patients with hypertropic cardiomyopathy, constrictive pericarditis, or high-output heart failure. However, despite this heterogeneity these entities continue currently to be lumped together into the category of HFPEF," Dr. Borlaug wrote in this editorial.
The perils of heterogeneity
In addition to providing a better framework for understanding the causes and consequences of HFPEF, the paradigm of HFPEF as a heterogeneous syndrome also helps explain why the major intervention trials that focused on HFPEF patients, starting a decade ago with studies such as CHARM Preserved (Lancet 2003;362:777-81) and I-PRESERVE (N. Engl. J. Med. 2008;359:2456-67), and continuing through to the recent TOPCAT, have all failed to produce a statistically significant benefit for their primary endpoints.
"Heterogeneity confounds our ability to identify effective treatments. It’s the most likely single explanation" for the neutral HFPEF trials, Dr. Borlaug said. "I don’t think it’s as simple as one thing, but my speculation is that it’s the dominant reason."
"Many trials such as CHARM Preserved and TOPCAT seemed to enroll some patients who in retrospect did not have HFPEF," noted Dr. Gregg C. Fonarow, professor of medicine and associate chief of cardiology at UCLA in Los Angeles. "The key to future clinical trials will be better classification of HFPEF" and better matching of HFPEF patients to their treatment, said Dr. Shah.
"In the neutral megatrials some of the patients did not have HFPEF but had other disorders such as deconditioning and obesity – things that cannot be helped by treatments directed at the heart. We need to identify the patients who will respond to the treatment," said Dr. Burkert M. Pieske, professor and director of cardiology at the Medical University of Graz, Austria.
The TOPCAT (Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist) results reported last November exemplified the problem of patient heterogeneity. The study enrolled more than 3,400 patients in six countries: Argentina, Brazil, Canada, Russia, the Republic of Georgia, and the United States. Retrospective analysis showed that among patients in the placebo group, the primary endpoint of death or heart failure hospitalization during follow-up occurred at a rate of 12.6 events/100 patient-years among the 881 patients treated in the four Western Hemisphere countries, and at a rate of 2.3 events/100 patient-years among the 842 patients treated in Russia or Georgia, a greater than fivefold difference between the two subgroups.
"As a whole, the patients in Russia and Georgia had a lower event rate and were certainly less severely ill than the other patients, but they supposedly still had heart failure. Defining this disorder is difficult, and when a patient has signs and symptoms of heart failure and preserved ejection fraction you may not be certain that heart failure is causing the symptoms. That’s why many people think that we should use another criterion" to define HFPEF in trials, such as elevated serum level of some form of natriuretic peptide, said Dr. Solomon, a TOPCAT coinvestigator. By design, patients could enter TOPCAT either because of a recent heart failure hospitalization, which is how 72% of patients got in, or by having a threshold level of natriuretic peptide, the way the remaining 28% entered the study. Within the subgroup enrolled by natriuretic peptide level, spironolactone treatment had a statistically significant effect in reducing the primary endpoint, while in the other 72% the drug produced no discernable benefit over placebo.
"TOPCAT had funding problems, recruitment problems, and monitoring problems. There was not enough money for good monitoring," said Dr. Pieske, who did not participate in TOPCAT. The patients enrolled in Russia and Georgia were "unbelievably stable," with their 2.3/100 patient-years event rate. "Even if the drug works, it can’t exert an effect if there are no events."
Dr. Pieske ran a much smaller study of spironolactone involving 422 patients with HFPEF, the Aldosterone Receptor Blockade in Diastolic Heart Failure (Aldo-DHF) trial, which showed efficacy for the endpoint of improved diastolic function but not for the co-endpoint of improved exercise capacity (JAMA 2013;309:781-91).
"If you look at TOPCAT and Aldo-DHF together and ask, does spironolactone work, the answer is yes if you select the right patients, those with clear evidence of cardiac functional abnormalities and increased natriuretic peptide levels or documented hospitalization for heart failure. The drug clearly works in these patients, but there were enough inconsistencies in these trials so that this will not get into the treatment guidelines," Dr. Pieske said in an interview.
"Spironolactone provides most benefit in patients who are volume overloaded, have right-heart failure, or both. These are also the patients most likely to have elevated natriuretic peptide. Spironolactone does not seem to benefit as much early-stage HFPEF," noted Dr. Shah.
Several experts cautioned that because the TOPCAT results failed to produce a statistically significant benefit for the study’s primary endpoint, any other conclusions from the results must be made very cautiously, and several also said that they wanted to see the full, published results which had not appeared as of late February. They also noted that many patients with HFPEF, most likely a majority, do not have elevated blood levels of natriuretic peptide.
Where HFPEF management stands now
Evidence-based guidelines for the specific treatment of HFPEF are simple. There aren’t any.
The American Heart Association/American College of Cardiology heart failure management guidelines released last October made no disease-specific treatment recommendations (J. Amer. Coll. Cardiol. 2013;62:e147-e239). They call for controlling hypertension in patients who need intervention by prevailing standards, treatment with a diuretic in patients with volume overload, coronary revascularization if coronary disease is present, and management of atrial fibrillation if that’s present. The European Society of Cardiology’s guidelines issued in 2012 say pretty much the same (Eur. J. Cardiol. 2012;33:1787-1847), except they add this statement: "No treatment has yet been shown, convincingly, to reduce morbidity and mortality in patients with HFPEF."
If nothing else, TOPCAT’s results further solidified spironolactone’s role as a reasonably safe drug for blood pressure lowering in HFPEF patients who are also hypertensive. Hypertension control is a must for patients with HFPEF as it’s believed to significantly contribute to HFPEF in most patients. "Hypertension is the most common underlying cause of HFPEF," said Dr. John R. Teerlink, professor of medicine and director of the heart failure program at the San Francisco Veterans Affairs Medical Center.
When it comes to treating hypertension in HFPEF patients, "unless there is a contraindication, spironolactone should be one of the first drugs to try, but I’m not sure you can say it’s the first choice" based on current evidence, Dr. Borlaug said.
A diuretic is an obvious antihypertensive for HFPEF patients with fluid overload. And there were suggestions of benefit from the ACE inhibitor perindopril in elderly patients in the PEP-CHF trial (Eur. Heart J. 2006;27:2338-45), another large HFPEF-treatment trial that failed to show significant benefit for the primary endpoint with perindopril treatment but had positive results in some secondary endpoints.
Patients "get these drugs to treat their hypertension, but we believe they may also help their heart failure. It’s a belief system. My colleagues and I already use a lot of spironolactone to treat hypertension, and the TOPCAT results won’t change my practice. I’m not comfortable telling people that you should use an aldosterone antagonist because of TOPCAT," Dr. Teerlink said in an interview.
"An angiotensin-converting enzyme inhibitor will probably work; spironolactone probably works if you get the diagnosis right; we don’t know about beta-blockers; and there is some evidence for using digoxin," said Dr. John G.F. Cleland, professor of cardiology at the University of Hull, Kingston-upon-Hull, England. "There must also be good treatment of hypertension, and judicious use of diuretics."
"I’m careful with beta-blockers; I’ve had some patients who felt miserable on them," said Dr. Borlaug. "Some HFPEF patients don’t have a stroke volume, they don’t have diastole, all they have is heart rate, and if you take that away they are left with no cardiac output."
Aside from controlling blood pressure, experts advise good management of other comorbidities such as coronary disease, atrial fibrillation, diabetes, sleep disordered breathing, and renal disease. "Clinicians should make sure that they are not missing severe coronary artery disease, infiltrative cardiomyopathy, constrictive pericarditis, or other causes of HFPEF that have specific treatments," said Dr. Shah. Some drugs have shown promise in early-phase studies – such as ivabradine and neprilysin – but phase III trials are needed. "My advice on how to manage patients with HFPEF is to make every effort to enroll them in a randomized clinical trial," said Dr. Fonarow.
Another key is making the diagnosis, ideally to prevent development of irreversible cardiovascular damage. "HFPEF is difficult to diagnose with certainty unless you do a cardiac catheterization to measure filling pressures, but in patients with early-stage HFPEF, even their invasive hemodynamics look pretty normal," said Dr. Borlaug. Another approach is an exercise echo, which is noninvasive and can identify stress-induced diastolic dysfunction, but the sensitivity and specificity of this approach remains uncertain, he said. And an elevated natriuretic peptide level can help nail the HFPEF diagnosis in some patients but many other patients have levels within the normal range.
To find HFPEF patients, apply a low index of suspicion and look for breathlessness, loss of functional capacity, signs of congestion, lung crackles, echocardiographic signs, pulmonary artery hypertension, and an enlarged left atrium, he suggested.
"Finding patients is a big challenge," said Dr. Pieske. HFPEF patients tend to be elderly, women, and people who are obese who have hypertension and perhaps diabetes. "They complain of dyspnea and fatigue and many physicians think this is just how it is. They will not consider that there is a true diagnosis behind these symptoms and complaints," especially if the patient has preserved left ventricular ejection fraction and a normal natriuretic peptide level." A diastolic stress test using exercise and an echo exam may identify stable patients with early-stage diastolic dysfunction but this requires confirmation, he said.
HFPEF dominates heart failure, lacks good treatment
Experts say the onus on physicians to diagnose and manage HFPEF will grow substantially, since HFPEF is not only highly prevalent but also increasing faster than heart failure with reduced ejection fraction (HFREF). Results from 13 community-based studies published during 1997-2006 showed that HFPEF represented an average of 55% of all heart failure cases, Dr. Carolyn S.P. Lam said last November during a talk at the American Heart Association’s scientific sessions.
Two recent reports of U.S. data documented that the increasing prevalence of HFPEF is outpacing that of HFREF by 1% per year, driven by the aging of the American population (older age is a risk factor for HFPEF) and by the increasing prevalence of comorbidities that contribute to HFPEF. One of the reports, based on U.S. national data collected by the Get With the Guidelines Program, extrapolated that by the end of this decade about 65% of all patients hospitalized for heart failure will have a left ventricular ejection fraction of 40% or greater, the vast majority with HFPEF (Curr. Heart Fail. Rep. 2013;10:401-10). What’s coming is a HFPEF "epidemic," said Dr. Lam, a cardiologist at the National University Heart Centre in Singapore.
The fact that HFPEF is now at least as prevalent as HFREF, that it is about as lethal independent of what comorbidities might contribute, and that it is growing more prevalent than HFREF sharply contrasts with the absence of treatments with proven efficacy. How did that happen?
"Research into HFPEF is decades behind research into HFREF," said Dr. Fonarow. "HFPEF was largely ignored because the prevailing wisdom [20 or so years ago] was that it represented only a small proportion of cases and that outcomes were much better compared with HFREF." Only with registry data and community-based studies run more recently did cardiologists realize that outcomes from HFPEF were as bad as from HFREF. Progress was further hampered by enrollment of patients who did not have HFPEF or a broad spectrum of patients unable to respond equally well to the treatment under study.
"There are large gaps in knowledge of the pathophysiology of HFPEF and little investment has been made to identify potential therapeutic targets. This creates cascading levels of challenges for developing effective treatments despite the massive unmet need," said Dr. Fonarow.
"We don’t know what to treat yet," was Dr. Teerlink’s summation of the HFPEF dilemma.
Dr. Borlaug said that he has been a consultant to GlaxoSmithKline, Merck, Amgen, CardioKinetix, and DC Devices and has received research support from Atcor. Dr. Solomon said he has been a consultant to and received research support from Novartis and more than 10 other drug and device companies. Dr. Pieske said that he has received honoraria from Bayer, Boehringer Ingelheim, Servier, Medtronic, Bristol-Myers Squibb, Menarini, and Novartis and received research support from Bayer and Medtronic. Dr. Shah said that he has been a consultant to Novartis, Bayer Schering, and the Pulmonary Hypertension Association. Dr. Fonarow said that he has been a consultant to Medtronic, Novartis, and Pfizer. Dr. Teerlink said that he has been an adviser to and received research support from Novartis. Dr. Cleland said that he has received honoraria from Novartis and research funding from Pfizer. Dr. Lam said that she has been a consultant to Bayer, Novartis, and DC Devices and has received research support from Boston Scientific, Medtronic, and Vifor Pharma.
On Twitter @mitchelzoler

Physician/patient communication on ICDs deemed problematic
SNOWMASS, COLO. – Cardiologist-patient discussions at the time of decision making about implantable cardioverter-defibrillator therapy are fraught with a disturbing degree of misrepresentation and omission, according to a recent study involving patient focus groups and formal scrutiny of observed physician-patient interactions.
"Our study demonstrates that patient-physician communication about ICDs is characterized by patient misinformation and a lack of attention to psychosocial and long-term risks by the prescribing physicians. ... Training of cardiologists on information exchange with patients may promote informed decision making and preempt threats to patient quality of life," concluded Dr. Paul J. Hauptman and his coinvestigators at St. Louis University.

At the Annual Cardiovascular Conference at Snowmass, Dr. Clyde W. Yancy highlighted the Hauptman study for shining a spotlight on an area in which the quality of communication with patients apparently leaves much to be desired. The study has drawn interest at the federally funded Patient-Centered Outcomes Research Institute (PCORI), where Dr. Yancy, a former president of the American Heart Association, is part of the leadership. Dr. Joe V. Selby, PCORI executive director, recently announced plans to spend roughly $1 billion on patient-centered comparative effectiveness research projects over the next 2 years.
The Hauptman study involved eight focus groups with a total of 41 ICD recipients in three different metropolitan areas as well as observation of 11 cardiologists as they each conducted two discussions about ICDs with individual device candidates.
Trained observers faulted 18 of the 22 cardiologist-patient interviews because the cardiologists didn’t address, minimized, or outright denied quality of life issues and the long-term consequences of ICD therapy, including increased risks for anxiety and depression as well as for inappropriate shocks.
Among the actual statements by cardiologists extracted from the physician-patient discussions were these: "The ICD will only go off if you are in VT/VF," "Inadvertent shock is not detrimental," "Inappropriate shock ... almost never happens," and "These devices are well tested and rarely have problems, so don’t worry about it." Cardiologists frequently compared the ICD to a seat belt, a safety net, or "an ambulance that follows you around." The first mention of a quality of life issue occurred on average halfway through the preimplantation discussions, which averaged 24 minutes in length. Although an increased prevalence of depression secondary to inappropriate ICD discharge or change in body image has been well documented in multiple studies, this possibility was discussed in only 1 of the 22 physician-patient interactions.

"No cardiologist discussed the epidemiological or clinical data on the prevalence of actual lifesaving ICD shocks, the prevalence of patients who ever require a shock, or the risk for death, despite ICD shock," the investigators noted (JAMA Intern. Med. 2013;173:571-7).
In the 2-hour-long patient focus groups, which were conducted with a different population than in the observed cardiologist-patient discussions, only 2 of 41 patients with ICDs could recall preimplantation mention of the possibility of depression or other emotional consequences of having an ICD. Only 5 of 41 patients could recall having a preimplantation discussion about inappropriate shocks. Two remembered mention of the possibility of device recalls.
The small sample size is a limitation of this study. Nevertheless, these rather disheartening data constitute some of the little evidence available on the information exchange between patients and cardiologists surrounding decision-making about ICDs, noted Dr. Yancy, professor of medicine and of medical social sciences as well as chief of cardiology at Northwestern University, Chicago.
"It just continues to be very startling that when you sit down with patients and understand what prism they’re using to see the data, you see information like this," he commented.
Another speaker, Dr. Bernard J. Gersh, was less circumspect. He was left shaking his head following Dr. Yancy’s overview of the Hauptman study findings.
"I was absolutely flabbergasted by the ICD patient information data. I was amazed and disappointed," said Dr. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
Dr. Yancy reported having no financial conflicts. Dr. Gersh is on the advisory boards of St. Jude Medical and Boston Scientific.
SNOWMASS, COLO. – Cardiologist-patient discussions at the time of decision making about implantable cardioverter-defibrillator therapy are fraught with a disturbing degree of misrepresentation and omission, according to a recent study involving patient focus groups and formal scrutiny of observed physician-patient interactions.
"Our study demonstrates that patient-physician communication about ICDs is characterized by patient misinformation and a lack of attention to psychosocial and long-term risks by the prescribing physicians. ... Training of cardiologists on information exchange with patients may promote informed decision making and preempt threats to patient quality of life," concluded Dr. Paul J. Hauptman and his coinvestigators at St. Louis University.
At the Annual Cardiovascular Conference at Snowmass, Dr. Clyde W. Yancy highlighted the Hauptman study for shining a spotlight on an area in which the quality of communication with patients apparently leaves much to be desired. The study has drawn interest at the federally funded Patient-Centered Outcomes Research Institute (PCORI), where Dr. Yancy, a former president of the American Heart Association, is part of the leadership. Dr. Joe V. Selby, PCORI executive director, recently announced plans to spend roughly $1 billion on patient-centered comparative effectiveness research projects over the next 2 years.
The Hauptman study involved eight focus groups with a total of 41 ICD recipients in three different metropolitan areas as well as observation of 11 cardiologists as they each conducted two discussions about ICDs with individual device candidates.
Trained observers faulted 18 of the 22 cardiologist-patient interviews because the cardiologists didn’t address, minimized, or outright denied quality of life issues and the long-term consequences of ICD therapy, including increased risks for anxiety and depression as well as for inappropriate shocks.
Among the actual statements by cardiologists extracted from the physician-patient discussions were these: "The ICD will only go off if you are in VT/VF," "Inadvertent shock is not detrimental," "Inappropriate shock ... almost never happens," and "These devices are well tested and rarely have problems, so don’t worry about it." Cardiologists frequently compared the ICD to a seat belt, a safety net, or "an ambulance that follows you around." The first mention of a quality of life issue occurred on average halfway through the preimplantation discussions, which averaged 24 minutes in length. Although an increased prevalence of depression secondary to inappropriate ICD discharge or change in body image has been well documented in multiple studies, this possibility was discussed in only 1 of the 22 physician-patient interactions.
"No cardiologist discussed the epidemiological or clinical data on the prevalence of actual lifesaving ICD shocks, the prevalence of patients who ever require a shock, or the risk for death, despite ICD shock," the investigators noted (JAMA Intern. Med. 2013;173:571-7).
In the 2-hour-long patient focus groups, which were conducted with a different population than in the observed cardiologist-patient discussions, only 2 of 41 patients with ICDs could recall preimplantation mention of the possibility of depression or other emotional consequences of having an ICD. Only 5 of 41 patients could recall having a preimplantation discussion about inappropriate shocks. Two remembered mention of the possibility of device recalls.
The small sample size is a limitation of this study. Nevertheless, these rather disheartening data constitute some of the little evidence available on the information exchange between patients and cardiologists surrounding decision-making about ICDs, noted Dr. Yancy, professor of medicine and of medical social sciences as well as chief of cardiology at Northwestern University, Chicago.
"It just continues to be very startling that when you sit down with patients and understand what prism they’re using to see the data, you see information like this," he commented.
Another speaker, Dr. Bernard J. Gersh, was less circumspect. He was left shaking his head following Dr. Yancy’s overview of the Hauptman study findings.
"I was absolutely flabbergasted by the ICD patient information data. I was amazed and disappointed," said Dr. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
Dr. Yancy reported having no financial conflicts. Dr. Gersh is on the advisory boards of St. Jude Medical and Boston Scientific.
SNOWMASS, COLO. – Cardiologist-patient discussions at the time of decision making about implantable cardioverter-defibrillator therapy are fraught with a disturbing degree of misrepresentation and omission, according to a recent study involving patient focus groups and formal scrutiny of observed physician-patient interactions.
"Our study demonstrates that patient-physician communication about ICDs is characterized by patient misinformation and a lack of attention to psychosocial and long-term risks by the prescribing physicians. ... Training of cardiologists on information exchange with patients may promote informed decision making and preempt threats to patient quality of life," concluded Dr. Paul J. Hauptman and his coinvestigators at St. Louis University.
At the Annual Cardiovascular Conference at Snowmass, Dr. Clyde W. Yancy highlighted the Hauptman study for shining a spotlight on an area in which the quality of communication with patients apparently leaves much to be desired. The study has drawn interest at the federally funded Patient-Centered Outcomes Research Institute (PCORI), where Dr. Yancy, a former president of the American Heart Association, is part of the leadership. Dr. Joe V. Selby, PCORI executive director, recently announced plans to spend roughly $1 billion on patient-centered comparative effectiveness research projects over the next 2 years.
The Hauptman study involved eight focus groups with a total of 41 ICD recipients in three different metropolitan areas as well as observation of 11 cardiologists as they each conducted two discussions about ICDs with individual device candidates.
Trained observers faulted 18 of the 22 cardiologist-patient interviews because the cardiologists didn’t address, minimized, or outright denied quality of life issues and the long-term consequences of ICD therapy, including increased risks for anxiety and depression as well as for inappropriate shocks.
Among the actual statements by cardiologists extracted from the physician-patient discussions were these: "The ICD will only go off if you are in VT/VF," "Inadvertent shock is not detrimental," "Inappropriate shock ... almost never happens," and "These devices are well tested and rarely have problems, so don’t worry about it." Cardiologists frequently compared the ICD to a seat belt, a safety net, or "an ambulance that follows you around." The first mention of a quality of life issue occurred on average halfway through the preimplantation discussions, which averaged 24 minutes in length. Although an increased prevalence of depression secondary to inappropriate ICD discharge or change in body image has been well documented in multiple studies, this possibility was discussed in only 1 of the 22 physician-patient interactions.
"No cardiologist discussed the epidemiological or clinical data on the prevalence of actual lifesaving ICD shocks, the prevalence of patients who ever require a shock, or the risk for death, despite ICD shock," the investigators noted (JAMA Intern. Med. 2013;173:571-7).
In the 2-hour-long patient focus groups, which were conducted with a different population than in the observed cardiologist-patient discussions, only 2 of 41 patients with ICDs could recall preimplantation mention of the possibility of depression or other emotional consequences of having an ICD. Only 5 of 41 patients could recall having a preimplantation discussion about inappropriate shocks. Two remembered mention of the possibility of device recalls.
The small sample size is a limitation of this study. Nevertheless, these rather disheartening data constitute some of the little evidence available on the information exchange between patients and cardiologists surrounding decision-making about ICDs, noted Dr. Yancy, professor of medicine and of medical social sciences as well as chief of cardiology at Northwestern University, Chicago.
"It just continues to be very startling that when you sit down with patients and understand what prism they’re using to see the data, you see information like this," he commented.
Another speaker, Dr. Bernard J. Gersh, was less circumspect. He was left shaking his head following Dr. Yancy’s overview of the Hauptman study findings.
"I was absolutely flabbergasted by the ICD patient information data. I was amazed and disappointed," said Dr. Gersh, professor of medicine at the Mayo Clinic in Rochester, Minn.
Dr. Yancy reported having no financial conflicts. Dr. Gersh is on the advisory boards of St. Jude Medical and Boston Scientific.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
Post-LVAD acute kidney injury is predictor of all-cause mortality
Acute kidney injury is not only common after implantation of a left ventricular assist device, it is also an independent predictor of 30-day and 1-year all-cause mortality, according to a retrospective, single-institution study.
In addition, multivariate analysis showed that only diabetes was a significant predictor of post-LVAD implantation acute kidney injury (AKI), the investigators stated in the report published online Feb. 15 in the American Journal of Nephrology.
Dr. Abhijit Naik and Dr. Jay L. Koyner of the section of nephrology at the University of Chicago and their colleagues identified 168 patients who underwent LVAD implantation at the university. They excluded 11 patients because of previous end-stage renal disease and intraoperative mortality. The remaining cohort of 157 patients served as their study population, which was 78% men and 58% white and had a mean age of around 57 years (Am. J. Nephrol. 2014 Feb. 15 [doi:10.1159/000358495]).

The obtained demographic, biochemical, and clinical profiles from the national Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), the Society of Thoracic Surgeons (STS) database, and the University of Chicago medical record (EMR). Baseline creatinine was defined as the listing of creatinine data obtained from the INTERMACS registry, or failing that, the last serum creatinine in the EMR prior to device implantation.
They defined the primary outcome of AKI as a 50% rise in serum creatinine over the preoperative baseline during the first 7 postoperative days. All-cause mortality was monitored over 1 year after implantation, with data reported at 30 and 365 days.
A total of 44 of 157 (28%) of patients developed AKI based on the study criteria. The only significant baseline differences between the patients with and without AKI were the presence of diabetes and cerebrovascular disease (CVD), each significantly higher in the patients who developed AKI.
Univariate analysis showed CVD and diabetes as significant predictors of developing AKI, but upon multivariate analysis, only diabetes retained significance (odds ratio, 2.27; P = .04).
As for mortality, only AKI (hazard ratio, 3.01; P = .03) and cardiopulmonary bypass time (HR, 1.01; P = .02) were significant predictors of 30-day mortality. Preoperative diabetes mellitus (HR, 1.9; P = .03) or postimplantation AKI (HR, 1.85; P = .03) were significant independent predictors of 1-year mortality. Higher preoperative body mass index was significantly and slightly protective (HR, 0.95; P = .03).
The authors stated that the strength of their study was that it is the largest cohort study of LVAD patients to employ a consensus definition of AKI; limitations were its single-center and retrospective nature and the use of database reviews.
As AKI is a common adverse outcome following traditional cardiac surgery, including coronary artery bypass grafting and/or valve replacement, more research is needed to tease out any differences unique to LVAD implantation, the investigators said.
"Given the high AKI rates and the mounting evidence linking AKI to mortality following VAD implantation, the use of biomarkers to identify patients at risk may have a role. Large prospective multicenter trials are needed to develop a risk stratification system to identify patients at risk for developing post-VAD implantation AKI," the researchers concluded.
Dr. Koyner was supported by a K23 grant from the National Institutes of Health. One of the coauthors reported research funding from Thoratec and another reported consulting fees from Thoratec and HeartWare. The other authors reported no disclosures.
Acute kidney injury is not only common after implantation of a left ventricular assist device, it is also an independent predictor of 30-day and 1-year all-cause mortality, according to a retrospective, single-institution study.
In addition, multivariate analysis showed that only diabetes was a significant predictor of post-LVAD implantation acute kidney injury (AKI), the investigators stated in the report published online Feb. 15 in the American Journal of Nephrology.
Dr. Abhijit Naik and Dr. Jay L. Koyner of the section of nephrology at the University of Chicago and their colleagues identified 168 patients who underwent LVAD implantation at the university. They excluded 11 patients because of previous end-stage renal disease and intraoperative mortality. The remaining cohort of 157 patients served as their study population, which was 78% men and 58% white and had a mean age of around 57 years (Am. J. Nephrol. 2014 Feb. 15 [doi:10.1159/000358495]).
The obtained demographic, biochemical, and clinical profiles from the national Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), the Society of Thoracic Surgeons (STS) database, and the University of Chicago medical record (EMR). Baseline creatinine was defined as the listing of creatinine data obtained from the INTERMACS registry, or failing that, the last serum creatinine in the EMR prior to device implantation.
They defined the primary outcome of AKI as a 50% rise in serum creatinine over the preoperative baseline during the first 7 postoperative days. All-cause mortality was monitored over 1 year after implantation, with data reported at 30 and 365 days.
A total of 44 of 157 (28%) of patients developed AKI based on the study criteria. The only significant baseline differences between the patients with and without AKI were the presence of diabetes and cerebrovascular disease (CVD), each significantly higher in the patients who developed AKI.
Univariate analysis showed CVD and diabetes as significant predictors of developing AKI, but upon multivariate analysis, only diabetes retained significance (odds ratio, 2.27; P = .04).
As for mortality, only AKI (hazard ratio, 3.01; P = .03) and cardiopulmonary bypass time (HR, 1.01; P = .02) were significant predictors of 30-day mortality. Preoperative diabetes mellitus (HR, 1.9; P = .03) or postimplantation AKI (HR, 1.85; P = .03) were significant independent predictors of 1-year mortality. Higher preoperative body mass index was significantly and slightly protective (HR, 0.95; P = .03).
The authors stated that the strength of their study was that it is the largest cohort study of LVAD patients to employ a consensus definition of AKI; limitations were its single-center and retrospective nature and the use of database reviews.
As AKI is a common adverse outcome following traditional cardiac surgery, including coronary artery bypass grafting and/or valve replacement, more research is needed to tease out any differences unique to LVAD implantation, the investigators said.
"Given the high AKI rates and the mounting evidence linking AKI to mortality following VAD implantation, the use of biomarkers to identify patients at risk may have a role. Large prospective multicenter trials are needed to develop a risk stratification system to identify patients at risk for developing post-VAD implantation AKI," the researchers concluded.
Dr. Koyner was supported by a K23 grant from the National Institutes of Health. One of the coauthors reported research funding from Thoratec and another reported consulting fees from Thoratec and HeartWare. The other authors reported no disclosures.
Acute kidney injury is not only common after implantation of a left ventricular assist device, it is also an independent predictor of 30-day and 1-year all-cause mortality, according to a retrospective, single-institution study.
In addition, multivariate analysis showed that only diabetes was a significant predictor of post-LVAD implantation acute kidney injury (AKI), the investigators stated in the report published online Feb. 15 in the American Journal of Nephrology.
Dr. Abhijit Naik and Dr. Jay L. Koyner of the section of nephrology at the University of Chicago and their colleagues identified 168 patients who underwent LVAD implantation at the university. They excluded 11 patients because of previous end-stage renal disease and intraoperative mortality. The remaining cohort of 157 patients served as their study population, which was 78% men and 58% white and had a mean age of around 57 years (Am. J. Nephrol. 2014 Feb. 15 [doi:10.1159/000358495]).
The obtained demographic, biochemical, and clinical profiles from the national Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), the Society of Thoracic Surgeons (STS) database, and the University of Chicago medical record (EMR). Baseline creatinine was defined as the listing of creatinine data obtained from the INTERMACS registry, or failing that, the last serum creatinine in the EMR prior to device implantation.
They defined the primary outcome of AKI as a 50% rise in serum creatinine over the preoperative baseline during the first 7 postoperative days. All-cause mortality was monitored over 1 year after implantation, with data reported at 30 and 365 days.
A total of 44 of 157 (28%) of patients developed AKI based on the study criteria. The only significant baseline differences between the patients with and without AKI were the presence of diabetes and cerebrovascular disease (CVD), each significantly higher in the patients who developed AKI.
Univariate analysis showed CVD and diabetes as significant predictors of developing AKI, but upon multivariate analysis, only diabetes retained significance (odds ratio, 2.27; P = .04).
As for mortality, only AKI (hazard ratio, 3.01; P = .03) and cardiopulmonary bypass time (HR, 1.01; P = .02) were significant predictors of 30-day mortality. Preoperative diabetes mellitus (HR, 1.9; P = .03) or postimplantation AKI (HR, 1.85; P = .03) were significant independent predictors of 1-year mortality. Higher preoperative body mass index was significantly and slightly protective (HR, 0.95; P = .03).
The authors stated that the strength of their study was that it is the largest cohort study of LVAD patients to employ a consensus definition of AKI; limitations were its single-center and retrospective nature and the use of database reviews.
As AKI is a common adverse outcome following traditional cardiac surgery, including coronary artery bypass grafting and/or valve replacement, more research is needed to tease out any differences unique to LVAD implantation, the investigators said.
"Given the high AKI rates and the mounting evidence linking AKI to mortality following VAD implantation, the use of biomarkers to identify patients at risk may have a role. Large prospective multicenter trials are needed to develop a risk stratification system to identify patients at risk for developing post-VAD implantation AKI," the researchers concluded.
Dr. Koyner was supported by a K23 grant from the National Institutes of Health. One of the coauthors reported research funding from Thoratec and another reported consulting fees from Thoratec and HeartWare. The other authors reported no disclosures.
FROM THE AMERICAN JOURNAL OF NEPHROLOGY
Major finding: Acute kidney injury was a significant predictor of 30-day mortality (hazard ratio, 3.01; P = .03) in patients who had implantation of a left ventricular assist device.
Data source: A retrospective, single-institution study using INTERMACS and STS databases with a sample of 168 patients who had undergone LVAD implantation.
Disclosures: Dr. Koyner was supported by a K23 grant from the National Institutes of Health. One of the coauthors reported research funding from Thoratec and another reported consulting fees from Thoratec and HeartWare. The other authors reported no disclosures.

Latest heart failure guidelines break new ground
SNOWMASS, COLO. – The latest heart failure guidelines from the American College of Cardiology/American Heart Association place a new emphasis on aldosterone antagonists as a central aspect of the management of symptomatic or previously symptomatic heart failure with reduced ejection fraction – while underscoring important caveats to their use.
Aldosterone antagonist therapy earns the strongest possible designation in the guidelines: a Class I/Level of Evidence A recommendation. This is based on data from multiple randomized trials showing that, used appropriately, these agents result in a 30% relative risk reduction in mortality and a 35% reduction in the relative risk of heart failure hospitalization, with a number needed to treat for 36 months of just six patients to prevent one additional death. Those figures place the aldosterone antagonists on a par with the other Class I/A heart failure medications – beta-blockers, ACE inhibitors or angiotensin receptor blockers, and hydralazine/isosorbide dinitrate in African Americans – in terms of benefits (see chart).

"These data are quite striking," Dr. Clyde W. Yancy observed in presenting highlights of the 2013 ACC/AHA guidelines at the Annual Cardiovascular Conference at Snowmass.
"For many years, we’ve functioned in a space where we thought there’s not that much we can do for heart failure, and I would now argue stridently against that. You can see the incredibly low numbers needed to treat here. Only a handful of patients need to be exposed to these therapies to derive a significant benefit on mortality. These are data we should incorporate in our clinical practice without exclusion," declared Dr. Yancy, who chaired the heart failure guideline-writing committee.
The important caveat regarding the aldosterone antagonists is that they should be used only in patients with an estimated glomerular filtration rate greater than 30 mL/min per 1.73 m2 and a serum potassium level below 5.0 mEq/dL. Otherwise that Class I/A recommendation plummets to III/B, meaning the treatment is inappropriate and potentially harmful, continued Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
The guidelines emphasize the imperative to implement what has come to be termed guideline-directed medical therapy, known by the acronym GDMT. The panel found persuasive an analysis showing that heart failure patients with reduced ejection fraction who were on two of seven evidence-based, guideline-directed management interventions had an adjusted 38% reduction in 2-year mortality risk compared with those on none or one, while those on three interventions had a 62% decrease in the odds of mortality and patients on four or more had mortality reductions of about 70% (J. Am. Heart Assoc. 2012;1:16-26).
The seven interventions are beta-blockers, ACE inhibitors or ARBs, aldosterone antagonists, anticoagulation for atrial fibrillation, cardiac resynchronization therapy, implantable cardioverter-defibrillators, and heart failure education for eligible patients.
The guidelines advise strongly against the combined use of an ACE inhibitor and ARB. It’s an either/or treatment strategy. Studies indicate there is no additive benefit with the combination, only an increased risk of side effects.
An important innovation in the guidelines is the new prominence afforded to heart failure with preserved ejection fraction, known as HFpEF (pronounced heff-peff).

"What’s most different in the new heart failure guidelines is that we have uploaded HFpEF to the front page," said Dr. Yancy. "We want you to appreciate how important it is. We recognize that there’s no evidence-based intervention that changes its natural history; rather, the focus is on identification and treatment of the comorbidities. It’s important to emphasize that this is a novel way of thinking about heart failure for a very important iteration of that disease."
Among the other highlights of the guidelines is a clarification of the current role for biomarker-guided heart failure therapy. B-type natriuretic peptide (BNP) or N-terminal pro-BNP measurements are deemed useful in making the diagnosis of heart failure as well as in establishing prognosis. Serial measurements can be used to titrate GDMT to optimal doses. But there are as yet no data to show that using the biomarkers to titrate GDMT to higher doses improves mortality.
The 2013 ACC/AHA Guideline for the Management of Heart Failure was developed in collaboration with the American Academy of Family Physicians, the American College of Chest Physicians, the Heart Rhythm Society, and the International Society for Heart and Lung Transplantation (J. Am. Coll. Cardiol. 2013;62:e147-e239).
Dr. Yancy reported having no financial conflicts.
SNOWMASS, COLO. – The latest heart failure guidelines from the American College of Cardiology/American Heart Association place a new emphasis on aldosterone antagonists as a central aspect of the management of symptomatic or previously symptomatic heart failure with reduced ejection fraction – while underscoring important caveats to their use.
Aldosterone antagonist therapy earns the strongest possible designation in the guidelines: a Class I/Level of Evidence A recommendation. This is based on data from multiple randomized trials showing that, used appropriately, these agents result in a 30% relative risk reduction in mortality and a 35% reduction in the relative risk of heart failure hospitalization, with a number needed to treat for 36 months of just six patients to prevent one additional death. Those figures place the aldosterone antagonists on a par with the other Class I/A heart failure medications – beta-blockers, ACE inhibitors or angiotensin receptor blockers, and hydralazine/isosorbide dinitrate in African Americans – in terms of benefits (see chart).
"These data are quite striking," Dr. Clyde W. Yancy observed in presenting highlights of the 2013 ACC/AHA guidelines at the Annual Cardiovascular Conference at Snowmass.
"For many years, we’ve functioned in a space where we thought there’s not that much we can do for heart failure, and I would now argue stridently against that. You can see the incredibly low numbers needed to treat here. Only a handful of patients need to be exposed to these therapies to derive a significant benefit on mortality. These are data we should incorporate in our clinical practice without exclusion," declared Dr. Yancy, who chaired the heart failure guideline-writing committee.
The important caveat regarding the aldosterone antagonists is that they should be used only in patients with an estimated glomerular filtration rate greater than 30 mL/min per 1.73 m2 and a serum potassium level below 5.0 mEq/dL. Otherwise that Class I/A recommendation plummets to III/B, meaning the treatment is inappropriate and potentially harmful, continued Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
The guidelines emphasize the imperative to implement what has come to be termed guideline-directed medical therapy, known by the acronym GDMT. The panel found persuasive an analysis showing that heart failure patients with reduced ejection fraction who were on two of seven evidence-based, guideline-directed management interventions had an adjusted 38% reduction in 2-year mortality risk compared with those on none or one, while those on three interventions had a 62% decrease in the odds of mortality and patients on four or more had mortality reductions of about 70% (J. Am. Heart Assoc. 2012;1:16-26).
The seven interventions are beta-blockers, ACE inhibitors or ARBs, aldosterone antagonists, anticoagulation for atrial fibrillation, cardiac resynchronization therapy, implantable cardioverter-defibrillators, and heart failure education for eligible patients.
The guidelines advise strongly against the combined use of an ACE inhibitor and ARB. It’s an either/or treatment strategy. Studies indicate there is no additive benefit with the combination, only an increased risk of side effects.
An important innovation in the guidelines is the new prominence afforded to heart failure with preserved ejection fraction, known as HFpEF (pronounced heff-peff).
"What’s most different in the new heart failure guidelines is that we have uploaded HFpEF to the front page," said Dr. Yancy. "We want you to appreciate how important it is. We recognize that there’s no evidence-based intervention that changes its natural history; rather, the focus is on identification and treatment of the comorbidities. It’s important to emphasize that this is a novel way of thinking about heart failure for a very important iteration of that disease."
Among the other highlights of the guidelines is a clarification of the current role for biomarker-guided heart failure therapy. B-type natriuretic peptide (BNP) or N-terminal pro-BNP measurements are deemed useful in making the diagnosis of heart failure as well as in establishing prognosis. Serial measurements can be used to titrate GDMT to optimal doses. But there are as yet no data to show that using the biomarkers to titrate GDMT to higher doses improves mortality.
The 2013 ACC/AHA Guideline for the Management of Heart Failure was developed in collaboration with the American Academy of Family Physicians, the American College of Chest Physicians, the Heart Rhythm Society, and the International Society for Heart and Lung Transplantation (J. Am. Coll. Cardiol. 2013;62:e147-e239).
Dr. Yancy reported having no financial conflicts.
SNOWMASS, COLO. – The latest heart failure guidelines from the American College of Cardiology/American Heart Association place a new emphasis on aldosterone antagonists as a central aspect of the management of symptomatic or previously symptomatic heart failure with reduced ejection fraction – while underscoring important caveats to their use.
Aldosterone antagonist therapy earns the strongest possible designation in the guidelines: a Class I/Level of Evidence A recommendation. This is based on data from multiple randomized trials showing that, used appropriately, these agents result in a 30% relative risk reduction in mortality and a 35% reduction in the relative risk of heart failure hospitalization, with a number needed to treat for 36 months of just six patients to prevent one additional death. Those figures place the aldosterone antagonists on a par with the other Class I/A heart failure medications – beta-blockers, ACE inhibitors or angiotensin receptor blockers, and hydralazine/isosorbide dinitrate in African Americans – in terms of benefits (see chart).
"These data are quite striking," Dr. Clyde W. Yancy observed in presenting highlights of the 2013 ACC/AHA guidelines at the Annual Cardiovascular Conference at Snowmass.
"For many years, we’ve functioned in a space where we thought there’s not that much we can do for heart failure, and I would now argue stridently against that. You can see the incredibly low numbers needed to treat here. Only a handful of patients need to be exposed to these therapies to derive a significant benefit on mortality. These are data we should incorporate in our clinical practice without exclusion," declared Dr. Yancy, who chaired the heart failure guideline-writing committee.
The important caveat regarding the aldosterone antagonists is that they should be used only in patients with an estimated glomerular filtration rate greater than 30 mL/min per 1.73 m2 and a serum potassium level below 5.0 mEq/dL. Otherwise that Class I/A recommendation plummets to III/B, meaning the treatment is inappropriate and potentially harmful, continued Dr. Yancy, professor of medicine and of medical social sciences and chief of cardiology at Northwestern University, Chicago.
The guidelines emphasize the imperative to implement what has come to be termed guideline-directed medical therapy, known by the acronym GDMT. The panel found persuasive an analysis showing that heart failure patients with reduced ejection fraction who were on two of seven evidence-based, guideline-directed management interventions had an adjusted 38% reduction in 2-year mortality risk compared with those on none or one, while those on three interventions had a 62% decrease in the odds of mortality and patients on four or more had mortality reductions of about 70% (J. Am. Heart Assoc. 2012;1:16-26).
The seven interventions are beta-blockers, ACE inhibitors or ARBs, aldosterone antagonists, anticoagulation for atrial fibrillation, cardiac resynchronization therapy, implantable cardioverter-defibrillators, and heart failure education for eligible patients.
The guidelines advise strongly against the combined use of an ACE inhibitor and ARB. It’s an either/or treatment strategy. Studies indicate there is no additive benefit with the combination, only an increased risk of side effects.
An important innovation in the guidelines is the new prominence afforded to heart failure with preserved ejection fraction, known as HFpEF (pronounced heff-peff).
"What’s most different in the new heart failure guidelines is that we have uploaded HFpEF to the front page," said Dr. Yancy. "We want you to appreciate how important it is. We recognize that there’s no evidence-based intervention that changes its natural history; rather, the focus is on identification and treatment of the comorbidities. It’s important to emphasize that this is a novel way of thinking about heart failure for a very important iteration of that disease."
Among the other highlights of the guidelines is a clarification of the current role for biomarker-guided heart failure therapy. B-type natriuretic peptide (BNP) or N-terminal pro-BNP measurements are deemed useful in making the diagnosis of heart failure as well as in establishing prognosis. Serial measurements can be used to titrate GDMT to optimal doses. But there are as yet no data to show that using the biomarkers to titrate GDMT to higher doses improves mortality.
The 2013 ACC/AHA Guideline for the Management of Heart Failure was developed in collaboration with the American Academy of Family Physicians, the American College of Chest Physicians, the Heart Rhythm Society, and the International Society for Heart and Lung Transplantation (J. Am. Coll. Cardiol. 2013;62:e147-e239).
Dr. Yancy reported having no financial conflicts.
EXPERT ANALYSIS FROM THE CARDIOVASCULAR CONFERENCE AT SNOWMASS
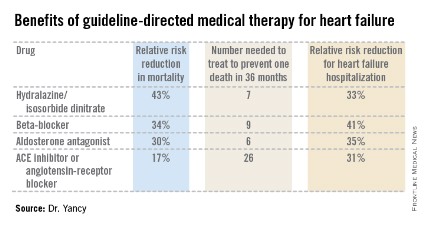
Medicare to cover cardiac rehab for some HF patients
Medicare will begin covering cardiac rehabilitation for patients with stable, chronic heart failure with a left ventricular ejection fraction of 35% or less.
The Centers for Medicare & Medicaid Services announced the new policy on Feb. 18.
About 5 million Americans have heart failure, but only half have an ejection fraction of less than 35%, Dr. Joseph A. Hill, chief of cardiology at the University of Texas Southwestern Medical Center, Dallas, said in an interview. Dr. Hill is chairman of the Heart Failure Society of America’s advocacy committee.
The HFSA, along with the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR), the American College of Cardiology (ACC), and the American Heart Association (AHA), submitted a formal request to the CMS to add heart failure to the list of approved indications for coverage for cardiac rehabilitation. The agency began its analysis process in June 2013.
At that time, cardiac rehab was covered only for acute myocardial infarction within the preceding 12 months, coronary artery bypass surgery, current stable angina pectoris, heart valve repair or replacement, percutaneous transluminal coronary angioplasty or coronary stenting, and a heart or heart-lung transplant. Cardiac rehab includes physician prescribed exercise; risk factor modification, including education, counseling, and behavioral intervention; psychosocial assessment; and outcomes assessment.
Physician supervision is required for coverage.
The CMS said it had reconsidered coverage for some heart failure patients as a result of the HF-Action study, published in 2009 (JAMA 2009;301:1439-50). That study "provided the best evidence of benefit" in the HF patient group, but in particular for patients with an ejection fraction of 35% or less and New York Heart Association (NYHA) class II-IV symptoms.
Specifically, the coverage is extended to "beneficiaries with stable, chronic heart failure defined as patients with left ventricular ejection fraction of 35% or less and [NYHA] class II to IV symptoms despite being on optimal heart failure therapy for at least six weeks." The decision defines stable patients as those who have not had recent (within the past 6 weeks) or planned (within the past 6 months) major cardiovascular hospitalizations or procedures.
"We conclude that the evidence that supports the clinical benefits of the individual components of CR programs is sufficient to determine that participation in these programs improves health outcomes for Medicare beneficiaries with chronic HF," the CMS noted in its analysis.
"We’re very pleased," with the CMS decision, said Dr. Hill.
The ACC said it was still evaluating the decision. But Dr. M. Eugene Sherman, chairman of the ACC’s Advocacy Steering Committee, added that "we are pleased to see Medicare expand coverage of cardiac rehabilitation services, as the ACC requested, to a new patient population where medical and scientific literature demonstrates a medical benefit."
Dr. Hill said that the HFSA and others were hopeful that the CMS would eventually expand coverage of rehab to the remainder of HF patients.
On Twitter @aliciaault
Medicare will begin covering cardiac rehabilitation for patients with stable, chronic heart failure with a left ventricular ejection fraction of 35% or less.
The Centers for Medicare & Medicaid Services announced the new policy on Feb. 18.
About 5 million Americans have heart failure, but only half have an ejection fraction of less than 35%, Dr. Joseph A. Hill, chief of cardiology at the University of Texas Southwestern Medical Center, Dallas, said in an interview. Dr. Hill is chairman of the Heart Failure Society of America’s advocacy committee.
The HFSA, along with the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR), the American College of Cardiology (ACC), and the American Heart Association (AHA), submitted a formal request to the CMS to add heart failure to the list of approved indications for coverage for cardiac rehabilitation. The agency began its analysis process in June 2013.
At that time, cardiac rehab was covered only for acute myocardial infarction within the preceding 12 months, coronary artery bypass surgery, current stable angina pectoris, heart valve repair or replacement, percutaneous transluminal coronary angioplasty or coronary stenting, and a heart or heart-lung transplant. Cardiac rehab includes physician prescribed exercise; risk factor modification, including education, counseling, and behavioral intervention; psychosocial assessment; and outcomes assessment.
Physician supervision is required for coverage.
The CMS said it had reconsidered coverage for some heart failure patients as a result of the HF-Action study, published in 2009 (JAMA 2009;301:1439-50). That study "provided the best evidence of benefit" in the HF patient group, but in particular for patients with an ejection fraction of 35% or less and New York Heart Association (NYHA) class II-IV symptoms.
Specifically, the coverage is extended to "beneficiaries with stable, chronic heart failure defined as patients with left ventricular ejection fraction of 35% or less and [NYHA] class II to IV symptoms despite being on optimal heart failure therapy for at least six weeks." The decision defines stable patients as those who have not had recent (within the past 6 weeks) or planned (within the past 6 months) major cardiovascular hospitalizations or procedures.
"We conclude that the evidence that supports the clinical benefits of the individual components of CR programs is sufficient to determine that participation in these programs improves health outcomes for Medicare beneficiaries with chronic HF," the CMS noted in its analysis.
"We’re very pleased," with the CMS decision, said Dr. Hill.
The ACC said it was still evaluating the decision. But Dr. M. Eugene Sherman, chairman of the ACC’s Advocacy Steering Committee, added that "we are pleased to see Medicare expand coverage of cardiac rehabilitation services, as the ACC requested, to a new patient population where medical and scientific literature demonstrates a medical benefit."
Dr. Hill said that the HFSA and others were hopeful that the CMS would eventually expand coverage of rehab to the remainder of HF patients.
On Twitter @aliciaault
Medicare will begin covering cardiac rehabilitation for patients with stable, chronic heart failure with a left ventricular ejection fraction of 35% or less.
The Centers for Medicare & Medicaid Services announced the new policy on Feb. 18.
About 5 million Americans have heart failure, but only half have an ejection fraction of less than 35%, Dr. Joseph A. Hill, chief of cardiology at the University of Texas Southwestern Medical Center, Dallas, said in an interview. Dr. Hill is chairman of the Heart Failure Society of America’s advocacy committee.
The HFSA, along with the American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR), the American College of Cardiology (ACC), and the American Heart Association (AHA), submitted a formal request to the CMS to add heart failure to the list of approved indications for coverage for cardiac rehabilitation. The agency began its analysis process in June 2013.
At that time, cardiac rehab was covered only for acute myocardial infarction within the preceding 12 months, coronary artery bypass surgery, current stable angina pectoris, heart valve repair or replacement, percutaneous transluminal coronary angioplasty or coronary stenting, and a heart or heart-lung transplant. Cardiac rehab includes physician prescribed exercise; risk factor modification, including education, counseling, and behavioral intervention; psychosocial assessment; and outcomes assessment.
Physician supervision is required for coverage.
The CMS said it had reconsidered coverage for some heart failure patients as a result of the HF-Action study, published in 2009 (JAMA 2009;301:1439-50). That study "provided the best evidence of benefit" in the HF patient group, but in particular for patients with an ejection fraction of 35% or less and New York Heart Association (NYHA) class II-IV symptoms.
Specifically, the coverage is extended to "beneficiaries with stable, chronic heart failure defined as patients with left ventricular ejection fraction of 35% or less and [NYHA] class II to IV symptoms despite being on optimal heart failure therapy for at least six weeks." The decision defines stable patients as those who have not had recent (within the past 6 weeks) or planned (within the past 6 months) major cardiovascular hospitalizations or procedures.
"We conclude that the evidence that supports the clinical benefits of the individual components of CR programs is sufficient to determine that participation in these programs improves health outcomes for Medicare beneficiaries with chronic HF," the CMS noted in its analysis.
"We’re very pleased," with the CMS decision, said Dr. Hill.
The ACC said it was still evaluating the decision. But Dr. M. Eugene Sherman, chairman of the ACC’s Advocacy Steering Committee, added that "we are pleased to see Medicare expand coverage of cardiac rehabilitation services, as the ACC requested, to a new patient population where medical and scientific literature demonstrates a medical benefit."
Dr. Hill said that the HFSA and others were hopeful that the CMS would eventually expand coverage of rehab to the remainder of HF patients.
On Twitter @aliciaault
PITCH is called for a balk
Just as spring training has begun, the National Institutes of Health has withdrawn funding for an important clinical trial, "Phosphodiesterase Type 5 Inhibition With Tadalafil Changes Outcomes in Heart Failure," or PITCH.
The role of PDE-5 inhibition in heart failure should be fully explored; the fact that the trial will not move forward now is a blow to the heart failure community and most importantly, patients. Although the details are not fully known, it appears that enrollment was slower than anticipated, a common phenomenon when clinical trials are initiated. (Full disclosure: I was in the process of submission of the regulatory paperwork and contracting to participate as a local principal investigator in PITCH when the trial was terminated.)

PITCH is an example of translational medicine on steroids. A wealth of basic and preclinical data suggested that nitric oxide–induced vasodilation may impact outcomes in human heart failure. A lot of effort, much of it supported by the National Heart, Lung, and Blood Institute, was expended over the last two decades in this area. Indeed, just ask the Nobel Prize winners of 1998.
Is there any way for the investigators to get back "on the mound" to test the hypothesis? With patents expiring, don’t expect industry support to materialize. This leaves us with an important unanswered question. Quite unfortunate, when you think about how much we have examined inhibition of the renin-angiotensin system from every conceivable angle. PITCH needs a reliever. Who will it be?
Dr. Paul Hauptman is professor of internal medicine and assistant dean of clinical-translational research at Saint Louis University, and director of heart failure at Saint Louis University Hospital. He serves as an associate editor for Circulation: Heart Failure and blogs while staring out his office window at the Arch.
Just as spring training has begun, the National Institutes of Health has withdrawn funding for an important clinical trial, "Phosphodiesterase Type 5 Inhibition With Tadalafil Changes Outcomes in Heart Failure," or PITCH.
The role of PDE-5 inhibition in heart failure should be fully explored; the fact that the trial will not move forward now is a blow to the heart failure community and most importantly, patients. Although the details are not fully known, it appears that enrollment was slower than anticipated, a common phenomenon when clinical trials are initiated. (Full disclosure: I was in the process of submission of the regulatory paperwork and contracting to participate as a local principal investigator in PITCH when the trial was terminated.)
PITCH is an example of translational medicine on steroids. A wealth of basic and preclinical data suggested that nitric oxide–induced vasodilation may impact outcomes in human heart failure. A lot of effort, much of it supported by the National Heart, Lung, and Blood Institute, was expended over the last two decades in this area. Indeed, just ask the Nobel Prize winners of 1998.
Is there any way for the investigators to get back "on the mound" to test the hypothesis? With patents expiring, don’t expect industry support to materialize. This leaves us with an important unanswered question. Quite unfortunate, when you think about how much we have examined inhibition of the renin-angiotensin system from every conceivable angle. PITCH needs a reliever. Who will it be?
Dr. Paul Hauptman is professor of internal medicine and assistant dean of clinical-translational research at Saint Louis University, and director of heart failure at Saint Louis University Hospital. He serves as an associate editor for Circulation: Heart Failure and blogs while staring out his office window at the Arch.
Just as spring training has begun, the National Institutes of Health has withdrawn funding for an important clinical trial, "Phosphodiesterase Type 5 Inhibition With Tadalafil Changes Outcomes in Heart Failure," or PITCH.
The role of PDE-5 inhibition in heart failure should be fully explored; the fact that the trial will not move forward now is a blow to the heart failure community and most importantly, patients. Although the details are not fully known, it appears that enrollment was slower than anticipated, a common phenomenon when clinical trials are initiated. (Full disclosure: I was in the process of submission of the regulatory paperwork and contracting to participate as a local principal investigator in PITCH when the trial was terminated.)
PITCH is an example of translational medicine on steroids. A wealth of basic and preclinical data suggested that nitric oxide–induced vasodilation may impact outcomes in human heart failure. A lot of effort, much of it supported by the National Heart, Lung, and Blood Institute, was expended over the last two decades in this area. Indeed, just ask the Nobel Prize winners of 1998.
Is there any way for the investigators to get back "on the mound" to test the hypothesis? With patents expiring, don’t expect industry support to materialize. This leaves us with an important unanswered question. Quite unfortunate, when you think about how much we have examined inhibition of the renin-angiotensin system from every conceivable angle. PITCH needs a reliever. Who will it be?
Dr. Paul Hauptman is professor of internal medicine and assistant dean of clinical-translational research at Saint Louis University, and director of heart failure at Saint Louis University Hospital. He serves as an associate editor for Circulation: Heart Failure and blogs while staring out his office window at the Arch.
