User login
For MD-IQ on Family Practice News, but a regular topic for Rheumatology News
PCPs play a small part in low-value care spending
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.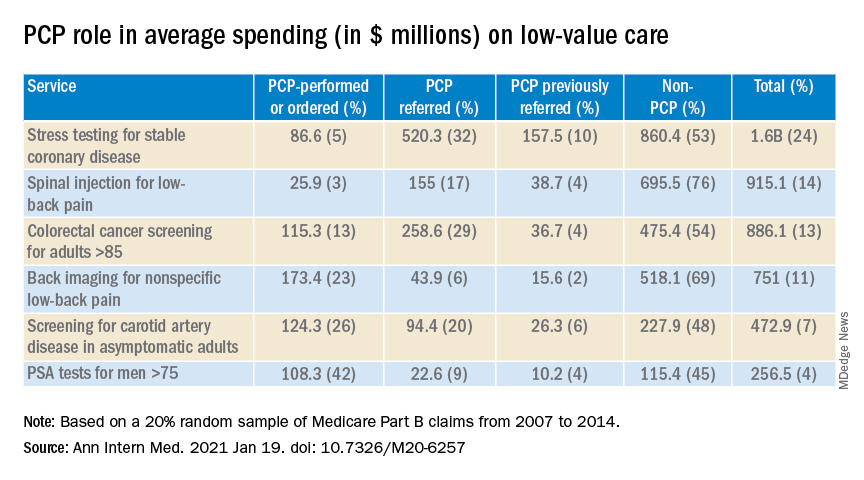
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Meta-analysis: No evidence that SNRIs relieve back pain
While some guidelines support serotonin norepinephrine reuptake inhibitors (SNRIs) as treatments for back pain, a new systematic review and meta-analysis of existing research found no firm evidence of a benefit. Adverse effects, however, are common.
“Our review shows that, although these medicines are effective, the effect is small and unlikely to be considered clinically important by most patients,” wrote the authors of the review, which appeared Jan. 20 in the BMJ. “Our review also showed that about two-thirds of patients using SNRIs experience adverse events.”
However, the report hinted that certain classes of antidepressants may provide significant relief in knee OA and sciatica.
According to a 2018 review, 10 of 15 clinical guidelines from around the world – including those of the American College of Physicians – recommended antidepressants as treatments for low back pain, and 2 advised against them. “Evidence supporting the use of antidepressants is, however, uncertain,” wrote the authors of the new review, led by Giovanni E. Ferreira, PhD, of the University of Sydney. “Systematic reviews of antidepressants for back pain and osteoarthritis have either not included several published trials, considered only one type of antidepressant (e.g., duloxetine), or failed to assess the certainty of evidence.”
For the new review, the authors analyzed 33 randomized, controlled trials with a total of 5,318 subjects. Both published data and unpublished data from clinical trial registries were included.
Back pain trials
A total of 19 trials examined back pain, mostly lower back pain (16 trials), and none lasted more than 1 year. Fifteen examined SNRIs while others looked at other kinds of antidepressants.
The researchers found that “the effect of SNRIs was small [on back pain] and below this review’s predetermined threshold of clinical importance. ... Evidence ranging from low to very low certainty showed no benefit of a range of antidepressant classes, including SSRIs [selective serotonin reuptake inhibitors], tetracyclic antidepressants, SARIs [serotonin antagonist and reuptake inhibitors], and NDRIs [norepinephrine and dopamine reuptake inhibitors] for pain and disability across follow-ups of 2 weeks or less, 3-13 weeks, and 3-12 months.”
Sciatica trials
Six trials examined antidepressants as treatments for sciatica. Very-low-certainty evidence suggested that SNRIs reduced pain at up to 2 weeks (1 trial, n = 50) but not at 3-13 weeks (3 trials, n = 96). The results of trials of tricyclic antidepressants (TCAs) were the opposite: low- to very-low-certainty evidence suggested the drugs didn’t reduce pain at up to 2 weeks (2 trials, n = 94) but did at 3-13 weeks (2 trials, n = 114) and 3-12 months (1 trial, n = 60).
“All sciatica trials were small, had imprecise estimates, and were at high risk of bias, which reduced the certainty of evidence to low and very low,” the authors cautioned. “This level of uncertainty indicates that the true estimate of effect of TCAs and SNRIs for sciatica is likely to be substantially different from what we estimated in our review.”
Knee OA trials
Eight trials examined SNRIs in knee OA. Moderate-certainty evidence linked the drugs to less pain at up to 2 weeks (four trials, n = 1,328) and low-certainty evidence linked them to less pain at 3-13 weeks (eight trials, n = 1,941). Low-certainty evidence also linked the drugs to less disability at 2 weeks or less (one trial, n = 353) and 3-13 weeks (seven trials, n = 1,810).
In knee OA, “the effect of SNRIs was small and below this review’s predetermined threshold of clinical importance,” the researchers wrote. “However, the lower limit of the confidence interval did contain clinically important effects for pain, but not for disability.”
Antidepressant side effects in trials
A total of 21 trials (n = 4,107) looked at side effects when antidepressants were studied as treatments for back pain and OA. Low-certainty evidence in 13 SNRI trials (n = 3,447) suggested a higher risk of any adverse events in antidepressant versus placebo (62.5% vs. 49.7%; relative risk, 1.23, 95% confidence interval, 1.16-1.30), but there was no significantly higher risk of serious adverse events in 10 SNRI trials with 3,309 subjects (1.6% vs. 1.3%; RR, 1.12, 95% CI, 0.61-2.07).
As for adverse effects of non-SNRIs, “the number of studies evaluating the safety of other antidepressant classes was small, trials were underpowered to detect harm, and the certainty of evidence ranged from low to very low,” the researchers wrote.
Going forward, the authors said that “large, definitive randomized trials that are free of industry ties are urgently needed to resolve uncertainties about the efficacy of antidepressants for sciatica and osteoarthritis highlighted by this review.”
‘Largely ineffective’ drug treatments
In an accompanying commentary, Martin Underwood, of the University of Warwick in Coventry, England, and Colin Tysall, of the University Hospitals of Coventry and Warwickshire, also in Coventry, noted that “drug treatments are largely ineffective for back pain and osteoarthritis and have the potential for serious harm. We need to work harder to help people with these disorders to live better with their pain without recourse to the prescription pad.”
However, they noted that SNRIs may still be helpful for patients with back pain or OA. “Absolute effect sizes for physical treatments for low-back pain are of similar magnitudes to those reported here and translate into numbers needed to treat of between five and nine. If the same were true for SNRIs, some people might choose to a try that option for a 1 in 10 chance of a worthwhile reduction in pain after 3 months. They can easily stop if treatment is ineffective or does not suit them.”
The research received no specific funding. The review authors disclosed relationships with GlaxoSmithKline (postgraduate scholarship), Pfizer (investigational product for two trials), and Flexeze (provision of heat wraps for a trial). Mr. Underwood reported being a director and shareholder of Clinvivo. Mr. Tysall reported no disclosures.
While some guidelines support serotonin norepinephrine reuptake inhibitors (SNRIs) as treatments for back pain, a new systematic review and meta-analysis of existing research found no firm evidence of a benefit. Adverse effects, however, are common.
“Our review shows that, although these medicines are effective, the effect is small and unlikely to be considered clinically important by most patients,” wrote the authors of the review, which appeared Jan. 20 in the BMJ. “Our review also showed that about two-thirds of patients using SNRIs experience adverse events.”
However, the report hinted that certain classes of antidepressants may provide significant relief in knee OA and sciatica.
According to a 2018 review, 10 of 15 clinical guidelines from around the world – including those of the American College of Physicians – recommended antidepressants as treatments for low back pain, and 2 advised against them. “Evidence supporting the use of antidepressants is, however, uncertain,” wrote the authors of the new review, led by Giovanni E. Ferreira, PhD, of the University of Sydney. “Systematic reviews of antidepressants for back pain and osteoarthritis have either not included several published trials, considered only one type of antidepressant (e.g., duloxetine), or failed to assess the certainty of evidence.”
For the new review, the authors analyzed 33 randomized, controlled trials with a total of 5,318 subjects. Both published data and unpublished data from clinical trial registries were included.
Back pain trials
A total of 19 trials examined back pain, mostly lower back pain (16 trials), and none lasted more than 1 year. Fifteen examined SNRIs while others looked at other kinds of antidepressants.
The researchers found that “the effect of SNRIs was small [on back pain] and below this review’s predetermined threshold of clinical importance. ... Evidence ranging from low to very low certainty showed no benefit of a range of antidepressant classes, including SSRIs [selective serotonin reuptake inhibitors], tetracyclic antidepressants, SARIs [serotonin antagonist and reuptake inhibitors], and NDRIs [norepinephrine and dopamine reuptake inhibitors] for pain and disability across follow-ups of 2 weeks or less, 3-13 weeks, and 3-12 months.”
Sciatica trials
Six trials examined antidepressants as treatments for sciatica. Very-low-certainty evidence suggested that SNRIs reduced pain at up to 2 weeks (1 trial, n = 50) but not at 3-13 weeks (3 trials, n = 96). The results of trials of tricyclic antidepressants (TCAs) were the opposite: low- to very-low-certainty evidence suggested the drugs didn’t reduce pain at up to 2 weeks (2 trials, n = 94) but did at 3-13 weeks (2 trials, n = 114) and 3-12 months (1 trial, n = 60).
“All sciatica trials were small, had imprecise estimates, and were at high risk of bias, which reduced the certainty of evidence to low and very low,” the authors cautioned. “This level of uncertainty indicates that the true estimate of effect of TCAs and SNRIs for sciatica is likely to be substantially different from what we estimated in our review.”
Knee OA trials
Eight trials examined SNRIs in knee OA. Moderate-certainty evidence linked the drugs to less pain at up to 2 weeks (four trials, n = 1,328) and low-certainty evidence linked them to less pain at 3-13 weeks (eight trials, n = 1,941). Low-certainty evidence also linked the drugs to less disability at 2 weeks or less (one trial, n = 353) and 3-13 weeks (seven trials, n = 1,810).
In knee OA, “the effect of SNRIs was small and below this review’s predetermined threshold of clinical importance,” the researchers wrote. “However, the lower limit of the confidence interval did contain clinically important effects for pain, but not for disability.”
Antidepressant side effects in trials
A total of 21 trials (n = 4,107) looked at side effects when antidepressants were studied as treatments for back pain and OA. Low-certainty evidence in 13 SNRI trials (n = 3,447) suggested a higher risk of any adverse events in antidepressant versus placebo (62.5% vs. 49.7%; relative risk, 1.23, 95% confidence interval, 1.16-1.30), but there was no significantly higher risk of serious adverse events in 10 SNRI trials with 3,309 subjects (1.6% vs. 1.3%; RR, 1.12, 95% CI, 0.61-2.07).
As for adverse effects of non-SNRIs, “the number of studies evaluating the safety of other antidepressant classes was small, trials were underpowered to detect harm, and the certainty of evidence ranged from low to very low,” the researchers wrote.
Going forward, the authors said that “large, definitive randomized trials that are free of industry ties are urgently needed to resolve uncertainties about the efficacy of antidepressants for sciatica and osteoarthritis highlighted by this review.”
‘Largely ineffective’ drug treatments
In an accompanying commentary, Martin Underwood, of the University of Warwick in Coventry, England, and Colin Tysall, of the University Hospitals of Coventry and Warwickshire, also in Coventry, noted that “drug treatments are largely ineffective for back pain and osteoarthritis and have the potential for serious harm. We need to work harder to help people with these disorders to live better with their pain without recourse to the prescription pad.”
However, they noted that SNRIs may still be helpful for patients with back pain or OA. “Absolute effect sizes for physical treatments for low-back pain are of similar magnitudes to those reported here and translate into numbers needed to treat of between five and nine. If the same were true for SNRIs, some people might choose to a try that option for a 1 in 10 chance of a worthwhile reduction in pain after 3 months. They can easily stop if treatment is ineffective or does not suit them.”
The research received no specific funding. The review authors disclosed relationships with GlaxoSmithKline (postgraduate scholarship), Pfizer (investigational product for two trials), and Flexeze (provision of heat wraps for a trial). Mr. Underwood reported being a director and shareholder of Clinvivo. Mr. Tysall reported no disclosures.
While some guidelines support serotonin norepinephrine reuptake inhibitors (SNRIs) as treatments for back pain, a new systematic review and meta-analysis of existing research found no firm evidence of a benefit. Adverse effects, however, are common.
“Our review shows that, although these medicines are effective, the effect is small and unlikely to be considered clinically important by most patients,” wrote the authors of the review, which appeared Jan. 20 in the BMJ. “Our review also showed that about two-thirds of patients using SNRIs experience adverse events.”
However, the report hinted that certain classes of antidepressants may provide significant relief in knee OA and sciatica.
According to a 2018 review, 10 of 15 clinical guidelines from around the world – including those of the American College of Physicians – recommended antidepressants as treatments for low back pain, and 2 advised against them. “Evidence supporting the use of antidepressants is, however, uncertain,” wrote the authors of the new review, led by Giovanni E. Ferreira, PhD, of the University of Sydney. “Systematic reviews of antidepressants for back pain and osteoarthritis have either not included several published trials, considered only one type of antidepressant (e.g., duloxetine), or failed to assess the certainty of evidence.”
For the new review, the authors analyzed 33 randomized, controlled trials with a total of 5,318 subjects. Both published data and unpublished data from clinical trial registries were included.
Back pain trials
A total of 19 trials examined back pain, mostly lower back pain (16 trials), and none lasted more than 1 year. Fifteen examined SNRIs while others looked at other kinds of antidepressants.
The researchers found that “the effect of SNRIs was small [on back pain] and below this review’s predetermined threshold of clinical importance. ... Evidence ranging from low to very low certainty showed no benefit of a range of antidepressant classes, including SSRIs [selective serotonin reuptake inhibitors], tetracyclic antidepressants, SARIs [serotonin antagonist and reuptake inhibitors], and NDRIs [norepinephrine and dopamine reuptake inhibitors] for pain and disability across follow-ups of 2 weeks or less, 3-13 weeks, and 3-12 months.”
Sciatica trials
Six trials examined antidepressants as treatments for sciatica. Very-low-certainty evidence suggested that SNRIs reduced pain at up to 2 weeks (1 trial, n = 50) but not at 3-13 weeks (3 trials, n = 96). The results of trials of tricyclic antidepressants (TCAs) were the opposite: low- to very-low-certainty evidence suggested the drugs didn’t reduce pain at up to 2 weeks (2 trials, n = 94) but did at 3-13 weeks (2 trials, n = 114) and 3-12 months (1 trial, n = 60).
“All sciatica trials were small, had imprecise estimates, and were at high risk of bias, which reduced the certainty of evidence to low and very low,” the authors cautioned. “This level of uncertainty indicates that the true estimate of effect of TCAs and SNRIs for sciatica is likely to be substantially different from what we estimated in our review.”
Knee OA trials
Eight trials examined SNRIs in knee OA. Moderate-certainty evidence linked the drugs to less pain at up to 2 weeks (four trials, n = 1,328) and low-certainty evidence linked them to less pain at 3-13 weeks (eight trials, n = 1,941). Low-certainty evidence also linked the drugs to less disability at 2 weeks or less (one trial, n = 353) and 3-13 weeks (seven trials, n = 1,810).
In knee OA, “the effect of SNRIs was small and below this review’s predetermined threshold of clinical importance,” the researchers wrote. “However, the lower limit of the confidence interval did contain clinically important effects for pain, but not for disability.”
Antidepressant side effects in trials
A total of 21 trials (n = 4,107) looked at side effects when antidepressants were studied as treatments for back pain and OA. Low-certainty evidence in 13 SNRI trials (n = 3,447) suggested a higher risk of any adverse events in antidepressant versus placebo (62.5% vs. 49.7%; relative risk, 1.23, 95% confidence interval, 1.16-1.30), but there was no significantly higher risk of serious adverse events in 10 SNRI trials with 3,309 subjects (1.6% vs. 1.3%; RR, 1.12, 95% CI, 0.61-2.07).
As for adverse effects of non-SNRIs, “the number of studies evaluating the safety of other antidepressant classes was small, trials were underpowered to detect harm, and the certainty of evidence ranged from low to very low,” the researchers wrote.
Going forward, the authors said that “large, definitive randomized trials that are free of industry ties are urgently needed to resolve uncertainties about the efficacy of antidepressants for sciatica and osteoarthritis highlighted by this review.”
‘Largely ineffective’ drug treatments
In an accompanying commentary, Martin Underwood, of the University of Warwick in Coventry, England, and Colin Tysall, of the University Hospitals of Coventry and Warwickshire, also in Coventry, noted that “drug treatments are largely ineffective for back pain and osteoarthritis and have the potential for serious harm. We need to work harder to help people with these disorders to live better with their pain without recourse to the prescription pad.”
However, they noted that SNRIs may still be helpful for patients with back pain or OA. “Absolute effect sizes for physical treatments for low-back pain are of similar magnitudes to those reported here and translate into numbers needed to treat of between five and nine. If the same were true for SNRIs, some people might choose to a try that option for a 1 in 10 chance of a worthwhile reduction in pain after 3 months. They can easily stop if treatment is ineffective or does not suit them.”
The research received no specific funding. The review authors disclosed relationships with GlaxoSmithKline (postgraduate scholarship), Pfizer (investigational product for two trials), and Flexeze (provision of heat wraps for a trial). Mr. Underwood reported being a director and shareholder of Clinvivo. Mr. Tysall reported no disclosures.
FROM THE BMJ
Greater reductions in knee OA pain seen with supportive rather than flexible shoes
according to a randomized trial that included more than 160 patients.

“Contrary to our hypothesis, flat flexible shoes were not superior to stable supportive shoes,” reported Kade L. Paterson, PhD, of the University of Melbourne, and colleagues. Their study was published Jan. 12 in Annals of Internal Medicine.
Research gap
Abnormal knee joint loading has been implicated in the pathogenesis of knee OA. Guidelines recommend that patients wear appropriate footwear, but research has not established which shoes are best.
The 2019 American College of Rheumatology clinical guidelines note that “optimal footwear is likely to be of considerable importance for those with knee and/or hip OA,” but “the available studies do not define the best type of footwear to improve specific outcomes for knee or hip OA.”
Some doctors call for thick, shock-absorbing soles and arch supports, based on expert opinion. On the other hand, studies have found that knee loading is lower with flat flexible shoes, and preliminary evidence has suggested that flat flexible shoes may improve OA symptoms, the investigators said.
To study this question, they enrolled in their trial 164 patients aged 50 years and older who had radiographic medial knee OA. Participants had knee pain on most days of the previous month, tibiofemoral osteophytes, and moderate to severe tibiofemoral OA.
The researchers randomly assigned 82 participants to flat flexible shoes and 82 participants to stable supportive shoes, worn for at least 6 hours a day for 6 months.
In the trial, flat flexible shoes included Merrell Bare Access (men’s and women’s), Vivobarefoot Primus Lite (men’s and women’s), Vivobarefoot Mata Canvas (men’s), Converse Dainty Low (women’s), and Lacoste Marice (men’s).
Stable supportive shoes included ASICS Kayano (men’s and women’s), Merrell Jungle Moc (men’s), Nike Air Max 90 Ultra (women’s), Rockport Edge Hill (men’s), and New Balance 624 (women’s).
After participants were randomly assigned to a group, they chose two different pairs of shoes from their assigned footwear group.
“Participants were not told that the purpose of the study was to compare flat flexible with stable supportive shoes,” the researchers noted. “Instead, they were informed only that the trial was comparing the effects of ‘different shoes’ on knee OA symptoms.”
The primary outcomes were changes in walking pain on a 0-10 scale and physical function as assessed by the Western Ontario and McMaster Universities Osteoarthritis Index subscale at 6 months. The researchers also assessed other measures of pain and function, physical activity, and quality of life.
In all, 161 participants reported 6-month primary outcomes. The between-group difference in change in pain favored stable supportive shoes (mean difference, 1.1 units). In the flat flexible shoe group, overall average knee pain while walking decreased from 6.3 at baseline to 5.2 at 6 months. In the stable supportive shoe group, knee pain while walking decreased from 6.1 to 4.
In addition, improvements in knee-related quality of life and ipsilateral hip pain favored stable supportive shoes.
Participants who wore stable supportive shoes also were less likely to report adverse events, compared with those who wore flat flexible shoes (15% vs. 32%). Knee pain, ankle or foot pain, and shin or calf pain were among the adverse events reported.
‘Important work’
“This study suggests that more supportive shoes may help some patients with knee osteoarthritis feel better,” Constance R. Chu, MD, professor of orthopedic surgery at Stanford (Calif.) University, said in an interview. “Shoes, insoles, wedges, and high heels have been shown to change loading of the knee related to knee pain and osteoarthritis ... This is important work toward providing more specific information on the optimum shoes for people with different patterns and types of arthritis to reduce pain and disability from early knee OA.”

The reported changes in pain may be clinically meaningful for many but not all patients, the authors wrote. “Despite biomechanical evidence showing that flat flexible shoes reduce medial knee load compared with stable supportive shoes, our findings show that this does not translate to improved knee osteoarthritis symptoms,” they said. “This may be because relationships between knee loading and symptoms are not as strong as previously thought, or because the small reductions in medial knee load with flat flexible shoes are insufficient to substantively improve pain and function.”
The trial did not include a control group of patients who wore their usual shoes, and it focused on a select subgroup of patients with knee OA, which may limit the study’s generalizability, the authors noted. The study excluded people with lateral joint space narrowing greater than or equal to medial, those with recent or planned knee surgery, and those who were using shoe orthoses or customized shoes.
The study was supported by grants from the National Health and Medical Research Council. Dr. Chu had no relevant disclosures.
according to a randomized trial that included more than 160 patients.
“Contrary to our hypothesis, flat flexible shoes were not superior to stable supportive shoes,” reported Kade L. Paterson, PhD, of the University of Melbourne, and colleagues. Their study was published Jan. 12 in Annals of Internal Medicine.
Research gap
Abnormal knee joint loading has been implicated in the pathogenesis of knee OA. Guidelines recommend that patients wear appropriate footwear, but research has not established which shoes are best.
The 2019 American College of Rheumatology clinical guidelines note that “optimal footwear is likely to be of considerable importance for those with knee and/or hip OA,” but “the available studies do not define the best type of footwear to improve specific outcomes for knee or hip OA.”
Some doctors call for thick, shock-absorbing soles and arch supports, based on expert opinion. On the other hand, studies have found that knee loading is lower with flat flexible shoes, and preliminary evidence has suggested that flat flexible shoes may improve OA symptoms, the investigators said.
To study this question, they enrolled in their trial 164 patients aged 50 years and older who had radiographic medial knee OA. Participants had knee pain on most days of the previous month, tibiofemoral osteophytes, and moderate to severe tibiofemoral OA.
The researchers randomly assigned 82 participants to flat flexible shoes and 82 participants to stable supportive shoes, worn for at least 6 hours a day for 6 months.
In the trial, flat flexible shoes included Merrell Bare Access (men’s and women’s), Vivobarefoot Primus Lite (men’s and women’s), Vivobarefoot Mata Canvas (men’s), Converse Dainty Low (women’s), and Lacoste Marice (men’s).
Stable supportive shoes included ASICS Kayano (men’s and women’s), Merrell Jungle Moc (men’s), Nike Air Max 90 Ultra (women’s), Rockport Edge Hill (men’s), and New Balance 624 (women’s).
After participants were randomly assigned to a group, they chose two different pairs of shoes from their assigned footwear group.
“Participants were not told that the purpose of the study was to compare flat flexible with stable supportive shoes,” the researchers noted. “Instead, they were informed only that the trial was comparing the effects of ‘different shoes’ on knee OA symptoms.”
The primary outcomes were changes in walking pain on a 0-10 scale and physical function as assessed by the Western Ontario and McMaster Universities Osteoarthritis Index subscale at 6 months. The researchers also assessed other measures of pain and function, physical activity, and quality of life.
In all, 161 participants reported 6-month primary outcomes. The between-group difference in change in pain favored stable supportive shoes (mean difference, 1.1 units). In the flat flexible shoe group, overall average knee pain while walking decreased from 6.3 at baseline to 5.2 at 6 months. In the stable supportive shoe group, knee pain while walking decreased from 6.1 to 4.
In addition, improvements in knee-related quality of life and ipsilateral hip pain favored stable supportive shoes.
Participants who wore stable supportive shoes also were less likely to report adverse events, compared with those who wore flat flexible shoes (15% vs. 32%). Knee pain, ankle or foot pain, and shin or calf pain were among the adverse events reported.
‘Important work’
“This study suggests that more supportive shoes may help some patients with knee osteoarthritis feel better,” Constance R. Chu, MD, professor of orthopedic surgery at Stanford (Calif.) University, said in an interview. “Shoes, insoles, wedges, and high heels have been shown to change loading of the knee related to knee pain and osteoarthritis ... This is important work toward providing more specific information on the optimum shoes for people with different patterns and types of arthritis to reduce pain and disability from early knee OA.”
The reported changes in pain may be clinically meaningful for many but not all patients, the authors wrote. “Despite biomechanical evidence showing that flat flexible shoes reduce medial knee load compared with stable supportive shoes, our findings show that this does not translate to improved knee osteoarthritis symptoms,” they said. “This may be because relationships between knee loading and symptoms are not as strong as previously thought, or because the small reductions in medial knee load with flat flexible shoes are insufficient to substantively improve pain and function.”
The trial did not include a control group of patients who wore their usual shoes, and it focused on a select subgroup of patients with knee OA, which may limit the study’s generalizability, the authors noted. The study excluded people with lateral joint space narrowing greater than or equal to medial, those with recent or planned knee surgery, and those who were using shoe orthoses or customized shoes.
The study was supported by grants from the National Health and Medical Research Council. Dr. Chu had no relevant disclosures.
according to a randomized trial that included more than 160 patients.
“Contrary to our hypothesis, flat flexible shoes were not superior to stable supportive shoes,” reported Kade L. Paterson, PhD, of the University of Melbourne, and colleagues. Their study was published Jan. 12 in Annals of Internal Medicine.
Research gap
Abnormal knee joint loading has been implicated in the pathogenesis of knee OA. Guidelines recommend that patients wear appropriate footwear, but research has not established which shoes are best.
The 2019 American College of Rheumatology clinical guidelines note that “optimal footwear is likely to be of considerable importance for those with knee and/or hip OA,” but “the available studies do not define the best type of footwear to improve specific outcomes for knee or hip OA.”
Some doctors call for thick, shock-absorbing soles and arch supports, based on expert opinion. On the other hand, studies have found that knee loading is lower with flat flexible shoes, and preliminary evidence has suggested that flat flexible shoes may improve OA symptoms, the investigators said.
To study this question, they enrolled in their trial 164 patients aged 50 years and older who had radiographic medial knee OA. Participants had knee pain on most days of the previous month, tibiofemoral osteophytes, and moderate to severe tibiofemoral OA.
The researchers randomly assigned 82 participants to flat flexible shoes and 82 participants to stable supportive shoes, worn for at least 6 hours a day for 6 months.
In the trial, flat flexible shoes included Merrell Bare Access (men’s and women’s), Vivobarefoot Primus Lite (men’s and women’s), Vivobarefoot Mata Canvas (men’s), Converse Dainty Low (women’s), and Lacoste Marice (men’s).
Stable supportive shoes included ASICS Kayano (men’s and women’s), Merrell Jungle Moc (men’s), Nike Air Max 90 Ultra (women’s), Rockport Edge Hill (men’s), and New Balance 624 (women’s).
After participants were randomly assigned to a group, they chose two different pairs of shoes from their assigned footwear group.
“Participants were not told that the purpose of the study was to compare flat flexible with stable supportive shoes,” the researchers noted. “Instead, they were informed only that the trial was comparing the effects of ‘different shoes’ on knee OA symptoms.”
The primary outcomes were changes in walking pain on a 0-10 scale and physical function as assessed by the Western Ontario and McMaster Universities Osteoarthritis Index subscale at 6 months. The researchers also assessed other measures of pain and function, physical activity, and quality of life.
In all, 161 participants reported 6-month primary outcomes. The between-group difference in change in pain favored stable supportive shoes (mean difference, 1.1 units). In the flat flexible shoe group, overall average knee pain while walking decreased from 6.3 at baseline to 5.2 at 6 months. In the stable supportive shoe group, knee pain while walking decreased from 6.1 to 4.
In addition, improvements in knee-related quality of life and ipsilateral hip pain favored stable supportive shoes.
Participants who wore stable supportive shoes also were less likely to report adverse events, compared with those who wore flat flexible shoes (15% vs. 32%). Knee pain, ankle or foot pain, and shin or calf pain were among the adverse events reported.
‘Important work’
“This study suggests that more supportive shoes may help some patients with knee osteoarthritis feel better,” Constance R. Chu, MD, professor of orthopedic surgery at Stanford (Calif.) University, said in an interview. “Shoes, insoles, wedges, and high heels have been shown to change loading of the knee related to knee pain and osteoarthritis ... This is important work toward providing more specific information on the optimum shoes for people with different patterns and types of arthritis to reduce pain and disability from early knee OA.”
The reported changes in pain may be clinically meaningful for many but not all patients, the authors wrote. “Despite biomechanical evidence showing that flat flexible shoes reduce medial knee load compared with stable supportive shoes, our findings show that this does not translate to improved knee osteoarthritis symptoms,” they said. “This may be because relationships between knee loading and symptoms are not as strong as previously thought, or because the small reductions in medial knee load with flat flexible shoes are insufficient to substantively improve pain and function.”
The trial did not include a control group of patients who wore their usual shoes, and it focused on a select subgroup of patients with knee OA, which may limit the study’s generalizability, the authors noted. The study excluded people with lateral joint space narrowing greater than or equal to medial, those with recent or planned knee surgery, and those who were using shoe orthoses or customized shoes.
The study was supported by grants from the National Health and Medical Research Council. Dr. Chu had no relevant disclosures.
FROM ANNALS OF INTERNAL MEDICINE
EULAR recommendations define strategies to improve adherence in RMDs
Clinicians who care for patients with rheumatic and musculoskeletal diseases (RMDs) can now refer to a new set of strategies and points to consider from a European League Against Rheumatism (EULAR) task force in building a patient-centered approach to improve adherence to treatments.

Nonadherence to treatments is concerning given that 30%-80% of patients who have RMDs are thought to not follow a recommended treatment plan according to their physicians’ instructions, according to first author Valentin Ritschl of the Medical University of Vienna and colleagues.
“The problem of poor adherence is addressed in some EULAR recommendations/points to consider on the management of specific health conditions or on the role of professionals,” Mr. Ritschl said in an interview. “However, all these recommendations focus on limited aspects of nonadherence and do not cover the multifaceted nature of this phenomenon.”
Mr. Ritschl and colleagues conducted an extensive systematic literature review, the results of which they presented to a task force consisting of a panel of international experts hailing from 12 different countries. The task force included rheumatologists and other health professionals in rheumatology, as well as patient representatives.
The collaboration resulted in investigators crafting a definition of adherence in addition to drafting four overarching principles and nine points to consider, which were published Dec. 18 in Annals of the Rheumatic Diseases.
They defined adherence as “the extent to which a person’s behavior corresponds with the agreed prescription, of pharmacological or nonpharmacological treatments, by a health care provider.”
The four overarching principles emphasize the following concepts: that adherence affects outcomes in people who have RMDs; the importance of shared decision-making, with the understanding that the adherence describes the patient’s behavior “following an agreed prescription”; that numerous factors can affect adherence; and the notion of adherence being a dynamic process that, consequently, requires continuous evaluation.
Among the nine points to consider, Mr. Ritschl and coauthors encouraged all health care providers involved in caring for RMD patients to assume responsibility for promoting adherence. Practitioners should also strive to create an ongoing, open dialogue to discuss adherence, especially in cases in which the patient’s RMD is not well controlled. The patient-centered recommendations include taking into account the patient’s goals and preferences because these greatly contribute to the patient’s ability to adhere to any medication regimen. Another arm of that exploration also requires the medical professional to evaluate any circumstances that could bear a negative effect on the patient’s adherence – whether it be medication access issues related to cost or availability, or functional challenges such as memory, motivation, or complexity of the medication regimen.
Mr. Ritschl believed the task force’s recommendations will add value and help improve overall outcomes in RMD population management.
“Until today, there are no recommendations or points to consider developed in order to support our patients to be adherent to the agreed treatment plan,” he said. “In our project/initiative, we therefore developed for the first time points to consider to detect, assess, and manage nonadherence in people with RMDs.”
Additionally, the recommendations offer some strategic insights to help improve clinical trials because the deleterious effects of nonadherence also affect study results.
Looking ahead, Mr. Ritschl said randomized, controlled trials are necessary to test strategies that might improve adherence. He strongly emphasized the importance of designing future research studies that are heavily patient centered and effective for shared decision-making.
The project was funded by EULAR. Mr. Ritschl reported having no disclosures, but many of his coauthors reported financial relationships with pharmaceutical companies.
SOURCE: Ritschl V et al. Ann Rheum Dis. 2020 Dec 18. doi: 10.1136/annrheumdis-2020-218986.
Clinicians who care for patients with rheumatic and musculoskeletal diseases (RMDs) can now refer to a new set of strategies and points to consider from a European League Against Rheumatism (EULAR) task force in building a patient-centered approach to improve adherence to treatments.
Nonadherence to treatments is concerning given that 30%-80% of patients who have RMDs are thought to not follow a recommended treatment plan according to their physicians’ instructions, according to first author Valentin Ritschl of the Medical University of Vienna and colleagues.
“The problem of poor adherence is addressed in some EULAR recommendations/points to consider on the management of specific health conditions or on the role of professionals,” Mr. Ritschl said in an interview. “However, all these recommendations focus on limited aspects of nonadherence and do not cover the multifaceted nature of this phenomenon.”
Mr. Ritschl and colleagues conducted an extensive systematic literature review, the results of which they presented to a task force consisting of a panel of international experts hailing from 12 different countries. The task force included rheumatologists and other health professionals in rheumatology, as well as patient representatives.
The collaboration resulted in investigators crafting a definition of adherence in addition to drafting four overarching principles and nine points to consider, which were published Dec. 18 in Annals of the Rheumatic Diseases.
They defined adherence as “the extent to which a person’s behavior corresponds with the agreed prescription, of pharmacological or nonpharmacological treatments, by a health care provider.”
The four overarching principles emphasize the following concepts: that adherence affects outcomes in people who have RMDs; the importance of shared decision-making, with the understanding that the adherence describes the patient’s behavior “following an agreed prescription”; that numerous factors can affect adherence; and the notion of adherence being a dynamic process that, consequently, requires continuous evaluation.
Among the nine points to consider, Mr. Ritschl and coauthors encouraged all health care providers involved in caring for RMD patients to assume responsibility for promoting adherence. Practitioners should also strive to create an ongoing, open dialogue to discuss adherence, especially in cases in which the patient’s RMD is not well controlled. The patient-centered recommendations include taking into account the patient’s goals and preferences because these greatly contribute to the patient’s ability to adhere to any medication regimen. Another arm of that exploration also requires the medical professional to evaluate any circumstances that could bear a negative effect on the patient’s adherence – whether it be medication access issues related to cost or availability, or functional challenges such as memory, motivation, or complexity of the medication regimen.
Mr. Ritschl believed the task force’s recommendations will add value and help improve overall outcomes in RMD population management.
“Until today, there are no recommendations or points to consider developed in order to support our patients to be adherent to the agreed treatment plan,” he said. “In our project/initiative, we therefore developed for the first time points to consider to detect, assess, and manage nonadherence in people with RMDs.”
Additionally, the recommendations offer some strategic insights to help improve clinical trials because the deleterious effects of nonadherence also affect study results.
Looking ahead, Mr. Ritschl said randomized, controlled trials are necessary to test strategies that might improve adherence. He strongly emphasized the importance of designing future research studies that are heavily patient centered and effective for shared decision-making.
The project was funded by EULAR. Mr. Ritschl reported having no disclosures, but many of his coauthors reported financial relationships with pharmaceutical companies.
SOURCE: Ritschl V et al. Ann Rheum Dis. 2020 Dec 18. doi: 10.1136/annrheumdis-2020-218986.
Clinicians who care for patients with rheumatic and musculoskeletal diseases (RMDs) can now refer to a new set of strategies and points to consider from a European League Against Rheumatism (EULAR) task force in building a patient-centered approach to improve adherence to treatments.
Nonadherence to treatments is concerning given that 30%-80% of patients who have RMDs are thought to not follow a recommended treatment plan according to their physicians’ instructions, according to first author Valentin Ritschl of the Medical University of Vienna and colleagues.
“The problem of poor adherence is addressed in some EULAR recommendations/points to consider on the management of specific health conditions or on the role of professionals,” Mr. Ritschl said in an interview. “However, all these recommendations focus on limited aspects of nonadherence and do not cover the multifaceted nature of this phenomenon.”
Mr. Ritschl and colleagues conducted an extensive systematic literature review, the results of which they presented to a task force consisting of a panel of international experts hailing from 12 different countries. The task force included rheumatologists and other health professionals in rheumatology, as well as patient representatives.
The collaboration resulted in investigators crafting a definition of adherence in addition to drafting four overarching principles and nine points to consider, which were published Dec. 18 in Annals of the Rheumatic Diseases.
They defined adherence as “the extent to which a person’s behavior corresponds with the agreed prescription, of pharmacological or nonpharmacological treatments, by a health care provider.”
The four overarching principles emphasize the following concepts: that adherence affects outcomes in people who have RMDs; the importance of shared decision-making, with the understanding that the adherence describes the patient’s behavior “following an agreed prescription”; that numerous factors can affect adherence; and the notion of adherence being a dynamic process that, consequently, requires continuous evaluation.
Among the nine points to consider, Mr. Ritschl and coauthors encouraged all health care providers involved in caring for RMD patients to assume responsibility for promoting adherence. Practitioners should also strive to create an ongoing, open dialogue to discuss adherence, especially in cases in which the patient’s RMD is not well controlled. The patient-centered recommendations include taking into account the patient’s goals and preferences because these greatly contribute to the patient’s ability to adhere to any medication regimen. Another arm of that exploration also requires the medical professional to evaluate any circumstances that could bear a negative effect on the patient’s adherence – whether it be medication access issues related to cost or availability, or functional challenges such as memory, motivation, or complexity of the medication regimen.
Mr. Ritschl believed the task force’s recommendations will add value and help improve overall outcomes in RMD population management.
“Until today, there are no recommendations or points to consider developed in order to support our patients to be adherent to the agreed treatment plan,” he said. “In our project/initiative, we therefore developed for the first time points to consider to detect, assess, and manage nonadherence in people with RMDs.”
Additionally, the recommendations offer some strategic insights to help improve clinical trials because the deleterious effects of nonadherence also affect study results.
Looking ahead, Mr. Ritschl said randomized, controlled trials are necessary to test strategies that might improve adherence. He strongly emphasized the importance of designing future research studies that are heavily patient centered and effective for shared decision-making.
The project was funded by EULAR. Mr. Ritschl reported having no disclosures, but many of his coauthors reported financial relationships with pharmaceutical companies.
SOURCE: Ritschl V et al. Ann Rheum Dis. 2020 Dec 18. doi: 10.1136/annrheumdis-2020-218986.
FROM ANNALS OF THE RHEUMATIC DISEASES
Radiofrequency ablation blocks hip, shoulder arthritis pain
Osteoarthritis patients report significant pain relief after treatment with cooled radiofrequency ablation, a new technique that “stuns” sensory nerves in shoulder and hip joints to reduce – and sometimes eliminate – pain.

“We send a small current to the sensory nerve to heat up the tissue and disrupt the fibers,” study lead author Felix Gonzalez, MD, of Emory University, Atlanta, said in an interview. “The effect is that the transmission of pain is significantly slowed or halted altogether.
“We damage something to fix something,” Dr. Gonzalez continued. “We target only the problematic nerve and get a very localized effect.”
Two-phase treatment
The treatment is performed in two phases. First, patients with shoulder pain are given an anesthetic to block their suprascapular, lateral pectoral, and axillary sensory articular nerves. Patients with hip pain have their obturator and femoral sensory articular nerves blocked.
A week or two later, the same nerves are treated with cooled radiofrequency ablation. Guided by x-ray imaging, a clinician heats up the affected nerve tissue using the tip of a needle, which is pointed at the nerve. “It’s a 22-gauge needle, slightly thicker than an acupuncture needle,” Dr. Gonzalez explained. “We heat up the nerve for about 2 minutes to about 60 degrees Celsius – it stuns the nerve,” he said.
“The result disrupts or slows down pain transmission while leaving the nerve intact.”
To test the efficacy of the technique, researchers treated 12 shoulders in patients with an average age of 61 years, and 11 hips in patients with an average age of 62 years.
Three months after treatment, patients with hip pain reported improvement in Hip Disability and Osteoarthritis Outcome Score (HOOS) from a baseline of 17.0 to 52.9 (P < .0001).
Shoulder pain was also reduced significantly. Using the American Shoulder and Elbow Surgeons (ASES) score, researchers reported an improvement from 17.2 (±6.6) at baseline to 65.7 (±5.9) at 3 months (P < .0001).
“We are targeting a subset of patients for this that don’t qualify for surgery,” Dr. Gonzalez noted. For patients with a body mass index above 35, or a history of hypertension, heart disease, or multiple strokes, opioids are the most common treatment, he said.
These patients “fall through the cracks,” he explained. Those who have mild to moderate pain are managed with physical therapy and injections, and those with severe pain go into surgery. “But what about the ones in the middle ... who are not eligible for surgery? They are at risk for opioid overuse,” he said. “So this treatment is a good option for them.”
Treats the symptoms, not the cause
“This study shows the efficacy of this method in taking care of shoulder and hip pain,” Luca Maria Sconfienza, MD, PhD, of Galeazzi Orthopedic Hospital in Milan, said in an interview. Dr. Sconfienza was not involved in Dr. Gonzalez’s study.
However, like corticosteroid injections, “the drawback of radiofrequency ablation is the fact that it only treats the symptoms and not the cause, and efficacy is usually limited over time,” she said.
Dr. Sconfienza said this study leaves her with three pertinent questions. “First, whether pain control extends beyond the 3-month follow-up reported by authors in the abstract; second, [what] is the efficacy of this method compared to other interventions (e.g., physical therapy, injections) or to doing nothing; and last, radiofrequency ablation is usually not a cheap treatment, thus a cost-efficacy analysis would be desirable, especially in comparison to other procedures.”
Dr. Gonzalez and Dr. Sconfienza have nothing relevant to disclose.
A version of this article originally appeared on Medscape.com.
Osteoarthritis patients report significant pain relief after treatment with cooled radiofrequency ablation, a new technique that “stuns” sensory nerves in shoulder and hip joints to reduce – and sometimes eliminate – pain.
“We send a small current to the sensory nerve to heat up the tissue and disrupt the fibers,” study lead author Felix Gonzalez, MD, of Emory University, Atlanta, said in an interview. “The effect is that the transmission of pain is significantly slowed or halted altogether.
“We damage something to fix something,” Dr. Gonzalez continued. “We target only the problematic nerve and get a very localized effect.”
Two-phase treatment
The treatment is performed in two phases. First, patients with shoulder pain are given an anesthetic to block their suprascapular, lateral pectoral, and axillary sensory articular nerves. Patients with hip pain have their obturator and femoral sensory articular nerves blocked.
A week or two later, the same nerves are treated with cooled radiofrequency ablation. Guided by x-ray imaging, a clinician heats up the affected nerve tissue using the tip of a needle, which is pointed at the nerve. “It’s a 22-gauge needle, slightly thicker than an acupuncture needle,” Dr. Gonzalez explained. “We heat up the nerve for about 2 minutes to about 60 degrees Celsius – it stuns the nerve,” he said.
“The result disrupts or slows down pain transmission while leaving the nerve intact.”
To test the efficacy of the technique, researchers treated 12 shoulders in patients with an average age of 61 years, and 11 hips in patients with an average age of 62 years.
Three months after treatment, patients with hip pain reported improvement in Hip Disability and Osteoarthritis Outcome Score (HOOS) from a baseline of 17.0 to 52.9 (P < .0001).
Shoulder pain was also reduced significantly. Using the American Shoulder and Elbow Surgeons (ASES) score, researchers reported an improvement from 17.2 (±6.6) at baseline to 65.7 (±5.9) at 3 months (P < .0001).
“We are targeting a subset of patients for this that don’t qualify for surgery,” Dr. Gonzalez noted. For patients with a body mass index above 35, or a history of hypertension, heart disease, or multiple strokes, opioids are the most common treatment, he said.
These patients “fall through the cracks,” he explained. Those who have mild to moderate pain are managed with physical therapy and injections, and those with severe pain go into surgery. “But what about the ones in the middle ... who are not eligible for surgery? They are at risk for opioid overuse,” he said. “So this treatment is a good option for them.”
Treats the symptoms, not the cause
“This study shows the efficacy of this method in taking care of shoulder and hip pain,” Luca Maria Sconfienza, MD, PhD, of Galeazzi Orthopedic Hospital in Milan, said in an interview. Dr. Sconfienza was not involved in Dr. Gonzalez’s study.
However, like corticosteroid injections, “the drawback of radiofrequency ablation is the fact that it only treats the symptoms and not the cause, and efficacy is usually limited over time,” she said.
Dr. Sconfienza said this study leaves her with three pertinent questions. “First, whether pain control extends beyond the 3-month follow-up reported by authors in the abstract; second, [what] is the efficacy of this method compared to other interventions (e.g., physical therapy, injections) or to doing nothing; and last, radiofrequency ablation is usually not a cheap treatment, thus a cost-efficacy analysis would be desirable, especially in comparison to other procedures.”
Dr. Gonzalez and Dr. Sconfienza have nothing relevant to disclose.
A version of this article originally appeared on Medscape.com.
Osteoarthritis patients report significant pain relief after treatment with cooled radiofrequency ablation, a new technique that “stuns” sensory nerves in shoulder and hip joints to reduce – and sometimes eliminate – pain.
“We send a small current to the sensory nerve to heat up the tissue and disrupt the fibers,” study lead author Felix Gonzalez, MD, of Emory University, Atlanta, said in an interview. “The effect is that the transmission of pain is significantly slowed or halted altogether.
“We damage something to fix something,” Dr. Gonzalez continued. “We target only the problematic nerve and get a very localized effect.”
Two-phase treatment
The treatment is performed in two phases. First, patients with shoulder pain are given an anesthetic to block their suprascapular, lateral pectoral, and axillary sensory articular nerves. Patients with hip pain have their obturator and femoral sensory articular nerves blocked.
A week or two later, the same nerves are treated with cooled radiofrequency ablation. Guided by x-ray imaging, a clinician heats up the affected nerve tissue using the tip of a needle, which is pointed at the nerve. “It’s a 22-gauge needle, slightly thicker than an acupuncture needle,” Dr. Gonzalez explained. “We heat up the nerve for about 2 minutes to about 60 degrees Celsius – it stuns the nerve,” he said.
“The result disrupts or slows down pain transmission while leaving the nerve intact.”
To test the efficacy of the technique, researchers treated 12 shoulders in patients with an average age of 61 years, and 11 hips in patients with an average age of 62 years.
Three months after treatment, patients with hip pain reported improvement in Hip Disability and Osteoarthritis Outcome Score (HOOS) from a baseline of 17.0 to 52.9 (P < .0001).
Shoulder pain was also reduced significantly. Using the American Shoulder and Elbow Surgeons (ASES) score, researchers reported an improvement from 17.2 (±6.6) at baseline to 65.7 (±5.9) at 3 months (P < .0001).
“We are targeting a subset of patients for this that don’t qualify for surgery,” Dr. Gonzalez noted. For patients with a body mass index above 35, or a history of hypertension, heart disease, or multiple strokes, opioids are the most common treatment, he said.
These patients “fall through the cracks,” he explained. Those who have mild to moderate pain are managed with physical therapy and injections, and those with severe pain go into surgery. “But what about the ones in the middle ... who are not eligible for surgery? They are at risk for opioid overuse,” he said. “So this treatment is a good option for them.”
Treats the symptoms, not the cause
“This study shows the efficacy of this method in taking care of shoulder and hip pain,” Luca Maria Sconfienza, MD, PhD, of Galeazzi Orthopedic Hospital in Milan, said in an interview. Dr. Sconfienza was not involved in Dr. Gonzalez’s study.
However, like corticosteroid injections, “the drawback of radiofrequency ablation is the fact that it only treats the symptoms and not the cause, and efficacy is usually limited over time,” she said.
Dr. Sconfienza said this study leaves her with three pertinent questions. “First, whether pain control extends beyond the 3-month follow-up reported by authors in the abstract; second, [what] is the efficacy of this method compared to other interventions (e.g., physical therapy, injections) or to doing nothing; and last, radiofrequency ablation is usually not a cheap treatment, thus a cost-efficacy analysis would be desirable, especially in comparison to other procedures.”
Dr. Gonzalez and Dr. Sconfienza have nothing relevant to disclose.
A version of this article originally appeared on Medscape.com.
To D or not to D? Vitamin D doesn’t reduce falls in older adults
Higher doses of vitamin D supplementation not only show no benefit in the prevention of falls in older adults at increased risk of falling, compared with the lowest doses, but they appear to increase the risk, new research shows.

Based on the findings, supplemental vitamin D above the minimum dose of 200 IU/day likely has little benefit, lead author Lawrence J. Appel, MD, MPH, told this news organization.
“In the absence of any benefit of 1,000 IU/day versus 2,000 IU/day [of vitamin D supplementation] on falls, along with the potential for harm from doses above 1,000 IU/day, it is hard to recommend a dose above 200 IU/day in older-aged persons, unless there is a compelling reason,” asserted Dr. Appel, director of the Welch Center for Prevention, Epidemiology, and Clinical Research at Johns Hopkins Bloomberg School of Public Health in Baltimore.
“More is not always better – and it may even be worse,” when it comes to vitamin D’s role in the prevention of falls, he said.
The research, published in Annals of Internal Medicine, adds important evidence in the ongoing struggle to prevent falls, says Bruce R. Troen, MD, in an accompanying editorial.
“Falls and their deleterious consequences remain a substantial risk for older adults and a huge challenge for health care teams,” writes Dr. Troen, a physician-investigator with the Veterans Affairs Western New York Healthcare System.
However, commenting in an interview, Dr. Troen cautions: “There are many epidemiological studies that are correlative, not causative, that do show a likelihood for benefit [with vitamin D supplementation]. … Therefore, there’s no reason for clinicians to discontinue vitamin D in individuals because of this study.”
“If you’re monitoring an older adult who is frail and has multiple comorbidities, you want to know what their vitamin D level is [and] provide them an appropriate supplement if needed,” he emphasized.
Some guidelines already reflect the lack of evidence of any role of vitamin D supplementation in the prevention of falls, including those of the 2018 U.S. Preventive Services Task Force, which, in a reversal of its 2012 recommendation, now does not recommend vitamin D supplementation for fall prevention in older persons without osteoporosis or vitamin D deficiency, Dr. Appel and colleagues note.
No prevention of falls regardless of baseline vitamin D
As part of STURDY (Study to understand fall reduction and vitamin D in you), Dr. Appel and colleagues enrolled 688 community-dwelling participants who had an elevated risk of falling, defined as a serum 25-hydroxyvitamin D [25(OH)D] level of 25 to 72.5 nmol/L (10-29 ng/dL).
Participants were a mean age of 77.2 years and had a mean total 25(OH)D level of 55.3 nmol/L at enrollment.
They were randomized to one of four doses of vitamin D3, including 200 IU/day (the control group), or 1,000, 2,000, or 4,000 IU/day.
The highest doses were found to be associated with worse – not better – outcomes including a shorter time to hospitalization or death, compared with the 1,000-IU/day group. The higher-dose groups were therefore switched to a dose of 1,000 IU/day or lower, and all participants were followed for up to 2 years.
Overall, 63% experienced falls over the course of the study, which, though high, was consistent with the study’s criteria of participants having an elevated fall risk.
Of the 667 participants who completed the trial, no benefit in prevention of falling was seen across any of the doses, compared with the control group dose of 200 IU/day, regardless of participants’ baseline vitamin D levels.
Safety analyses showed that even in the 1,000-IU/day group, a higher risk of first serious fall and first fall with hospitalization was seen compared with the 200-IU/day group.
A limitation is that the study did not have a placebo group, however, “200 IU/day is a very small dose, probably homeopathic,” Dr. Appel said. “It was likely close to a placebo,” he said.
Caveats: comorbidities, subgroups
In his editorial, Dr. Troen notes other studies, including VITAL (Vitamin D and Omega-3 Trial) also found no reduction in falls with higher vitamin D doses; however, that study did not show any significant risks with the higher doses.
He adds that the current study lacks information on subsets of participants.
“We don’t have enough information about the existing comorbidities and medications that these people are on to be able to pull back the layers. Maybe there is a subgroup that should not be getting 4,000 IU, whereas another subgroup may not be harmed and you may decide that patient can benefit,” he said.
Furthermore, the trial doesn’t address groups such as nursing home residents.
“I have, for instance, 85-year-olds with vitamin D levels of maybe 20 nmol/L with multiple medical issues, but levels that low were not included in the study, so this is a tricky business, but the bottom line is first, do no harm,” he said.
“We really need trials that factor in the multiple different aspects so we can come up, hopefully, with a holistic and interdisciplinary approach, which is usually the best way to optimize care for frail older adults,” he concluded.
The study received funding from the National Institute of Aging.
A version of this article originally appeared on Medscape.com.
Higher doses of vitamin D supplementation not only show no benefit in the prevention of falls in older adults at increased risk of falling, compared with the lowest doses, but they appear to increase the risk, new research shows.
Based on the findings, supplemental vitamin D above the minimum dose of 200 IU/day likely has little benefit, lead author Lawrence J. Appel, MD, MPH, told this news organization.
“In the absence of any benefit of 1,000 IU/day versus 2,000 IU/day [of vitamin D supplementation] on falls, along with the potential for harm from doses above 1,000 IU/day, it is hard to recommend a dose above 200 IU/day in older-aged persons, unless there is a compelling reason,” asserted Dr. Appel, director of the Welch Center for Prevention, Epidemiology, and Clinical Research at Johns Hopkins Bloomberg School of Public Health in Baltimore.
“More is not always better – and it may even be worse,” when it comes to vitamin D’s role in the prevention of falls, he said.
The research, published in Annals of Internal Medicine, adds important evidence in the ongoing struggle to prevent falls, says Bruce R. Troen, MD, in an accompanying editorial.
“Falls and their deleterious consequences remain a substantial risk for older adults and a huge challenge for health care teams,” writes Dr. Troen, a physician-investigator with the Veterans Affairs Western New York Healthcare System.
However, commenting in an interview, Dr. Troen cautions: “There are many epidemiological studies that are correlative, not causative, that do show a likelihood for benefit [with vitamin D supplementation]. … Therefore, there’s no reason for clinicians to discontinue vitamin D in individuals because of this study.”
“If you’re monitoring an older adult who is frail and has multiple comorbidities, you want to know what their vitamin D level is [and] provide them an appropriate supplement if needed,” he emphasized.
Some guidelines already reflect the lack of evidence of any role of vitamin D supplementation in the prevention of falls, including those of the 2018 U.S. Preventive Services Task Force, which, in a reversal of its 2012 recommendation, now does not recommend vitamin D supplementation for fall prevention in older persons without osteoporosis or vitamin D deficiency, Dr. Appel and colleagues note.
No prevention of falls regardless of baseline vitamin D
As part of STURDY (Study to understand fall reduction and vitamin D in you), Dr. Appel and colleagues enrolled 688 community-dwelling participants who had an elevated risk of falling, defined as a serum 25-hydroxyvitamin D [25(OH)D] level of 25 to 72.5 nmol/L (10-29 ng/dL).
Participants were a mean age of 77.2 years and had a mean total 25(OH)D level of 55.3 nmol/L at enrollment.
They were randomized to one of four doses of vitamin D3, including 200 IU/day (the control group), or 1,000, 2,000, or 4,000 IU/day.
The highest doses were found to be associated with worse – not better – outcomes including a shorter time to hospitalization or death, compared with the 1,000-IU/day group. The higher-dose groups were therefore switched to a dose of 1,000 IU/day or lower, and all participants were followed for up to 2 years.
Overall, 63% experienced falls over the course of the study, which, though high, was consistent with the study’s criteria of participants having an elevated fall risk.
Of the 667 participants who completed the trial, no benefit in prevention of falling was seen across any of the doses, compared with the control group dose of 200 IU/day, regardless of participants’ baseline vitamin D levels.
Safety analyses showed that even in the 1,000-IU/day group, a higher risk of first serious fall and first fall with hospitalization was seen compared with the 200-IU/day group.
A limitation is that the study did not have a placebo group, however, “200 IU/day is a very small dose, probably homeopathic,” Dr. Appel said. “It was likely close to a placebo,” he said.
Caveats: comorbidities, subgroups
In his editorial, Dr. Troen notes other studies, including VITAL (Vitamin D and Omega-3 Trial) also found no reduction in falls with higher vitamin D doses; however, that study did not show any significant risks with the higher doses.
He adds that the current study lacks information on subsets of participants.
“We don’t have enough information about the existing comorbidities and medications that these people are on to be able to pull back the layers. Maybe there is a subgroup that should not be getting 4,000 IU, whereas another subgroup may not be harmed and you may decide that patient can benefit,” he said.
Furthermore, the trial doesn’t address groups such as nursing home residents.
“I have, for instance, 85-year-olds with vitamin D levels of maybe 20 nmol/L with multiple medical issues, but levels that low were not included in the study, so this is a tricky business, but the bottom line is first, do no harm,” he said.
“We really need trials that factor in the multiple different aspects so we can come up, hopefully, with a holistic and interdisciplinary approach, which is usually the best way to optimize care for frail older adults,” he concluded.
The study received funding from the National Institute of Aging.
A version of this article originally appeared on Medscape.com.
Higher doses of vitamin D supplementation not only show no benefit in the prevention of falls in older adults at increased risk of falling, compared with the lowest doses, but they appear to increase the risk, new research shows.
Based on the findings, supplemental vitamin D above the minimum dose of 200 IU/day likely has little benefit, lead author Lawrence J. Appel, MD, MPH, told this news organization.
“In the absence of any benefit of 1,000 IU/day versus 2,000 IU/day [of vitamin D supplementation] on falls, along with the potential for harm from doses above 1,000 IU/day, it is hard to recommend a dose above 200 IU/day in older-aged persons, unless there is a compelling reason,” asserted Dr. Appel, director of the Welch Center for Prevention, Epidemiology, and Clinical Research at Johns Hopkins Bloomberg School of Public Health in Baltimore.
“More is not always better – and it may even be worse,” when it comes to vitamin D’s role in the prevention of falls, he said.
The research, published in Annals of Internal Medicine, adds important evidence in the ongoing struggle to prevent falls, says Bruce R. Troen, MD, in an accompanying editorial.
“Falls and their deleterious consequences remain a substantial risk for older adults and a huge challenge for health care teams,” writes Dr. Troen, a physician-investigator with the Veterans Affairs Western New York Healthcare System.
However, commenting in an interview, Dr. Troen cautions: “There are many epidemiological studies that are correlative, not causative, that do show a likelihood for benefit [with vitamin D supplementation]. … Therefore, there’s no reason for clinicians to discontinue vitamin D in individuals because of this study.”
“If you’re monitoring an older adult who is frail and has multiple comorbidities, you want to know what their vitamin D level is [and] provide them an appropriate supplement if needed,” he emphasized.
Some guidelines already reflect the lack of evidence of any role of vitamin D supplementation in the prevention of falls, including those of the 2018 U.S. Preventive Services Task Force, which, in a reversal of its 2012 recommendation, now does not recommend vitamin D supplementation for fall prevention in older persons without osteoporosis or vitamin D deficiency, Dr. Appel and colleagues note.
No prevention of falls regardless of baseline vitamin D
As part of STURDY (Study to understand fall reduction and vitamin D in you), Dr. Appel and colleagues enrolled 688 community-dwelling participants who had an elevated risk of falling, defined as a serum 25-hydroxyvitamin D [25(OH)D] level of 25 to 72.5 nmol/L (10-29 ng/dL).
Participants were a mean age of 77.2 years and had a mean total 25(OH)D level of 55.3 nmol/L at enrollment.
They were randomized to one of four doses of vitamin D3, including 200 IU/day (the control group), or 1,000, 2,000, or 4,000 IU/day.
The highest doses were found to be associated with worse – not better – outcomes including a shorter time to hospitalization or death, compared with the 1,000-IU/day group. The higher-dose groups were therefore switched to a dose of 1,000 IU/day or lower, and all participants were followed for up to 2 years.
Overall, 63% experienced falls over the course of the study, which, though high, was consistent with the study’s criteria of participants having an elevated fall risk.
Of the 667 participants who completed the trial, no benefit in prevention of falling was seen across any of the doses, compared with the control group dose of 200 IU/day, regardless of participants’ baseline vitamin D levels.
Safety analyses showed that even in the 1,000-IU/day group, a higher risk of first serious fall and first fall with hospitalization was seen compared with the 200-IU/day group.
A limitation is that the study did not have a placebo group, however, “200 IU/day is a very small dose, probably homeopathic,” Dr. Appel said. “It was likely close to a placebo,” he said.
Caveats: comorbidities, subgroups
In his editorial, Dr. Troen notes other studies, including VITAL (Vitamin D and Omega-3 Trial) also found no reduction in falls with higher vitamin D doses; however, that study did not show any significant risks with the higher doses.
He adds that the current study lacks information on subsets of participants.
“We don’t have enough information about the existing comorbidities and medications that these people are on to be able to pull back the layers. Maybe there is a subgroup that should not be getting 4,000 IU, whereas another subgroup may not be harmed and you may decide that patient can benefit,” he said.
Furthermore, the trial doesn’t address groups such as nursing home residents.
“I have, for instance, 85-year-olds with vitamin D levels of maybe 20 nmol/L with multiple medical issues, but levels that low were not included in the study, so this is a tricky business, but the bottom line is first, do no harm,” he said.
“We really need trials that factor in the multiple different aspects so we can come up, hopefully, with a holistic and interdisciplinary approach, which is usually the best way to optimize care for frail older adults,” he concluded.
The study received funding from the National Institute of Aging.
A version of this article originally appeared on Medscape.com.
Real acupuncture beat sham for osteoarthritis knee pain
Electro-acupuncture resulted in significant improvement in pain and function, compared with sham acupuncture, in a randomized trial of more than 400 adults with knee OA.
The socioeconomic burden of knee OA (KOA) remains high, and will likely increase with the aging population and rising rates of obesity, wrote first author Jian-Feng Tu, MD, PhD, of Beijing University of Chinese Medicine and colleagues. “Since no disease-modifying pharmaceutical agents have been approved, current KOA treatments are mainly symptomatic,” and identifying new therapies in addition to pharmacological agents or surgery is a research priority, they added. The research on acupuncture as a treatment for KOA has increased, but remains controversial as researchers attempt to determine the number of sessions needed for effectiveness.
In a study published in Arthritis & Rheumatology, the researchers recruited 480 adults aged 45-75 years with confirmed KOA who reported knee pain for longer than 6 months. Participants were randomized to three groups: electroacupuncture (EA), manual acupuncture (MA), or sham acupuncture (SA). Each group received three treatment sessions per week. In all groups, electrodes were attached to selected acupuncture needles, but the current was turned on only in the EA treatment group.
The primary outcome was the response rate after 8 weeks of treatment, defined as patients who achieved the minimal clinically important improvement (MCII) on both the Numeric Rating Scale and the Western Ontario and McMaster Universities Osteoarthritis Index function subscale.
Overall, response rates at 8 weeks were 60.3%, 58.6%, and 47.3% for the EA, MA, and SA groups, respectively.
Between-group differences were statistically significant for EA versus SA (13%, P = .0234) but not for MA versus SA (11.3%, P = .0507) at 8 weeks; however, both EA and MA groups showed significantly higher response rates, compared with the SA group at 16 and 26 weeks. “Although a clinically meaningful response rate for KOA is not available in the literature, the difference of 11.3%, which indicates the number needed to treat of 9, is acceptable in clinical practices,” the researchers noted.
Adverse events occurred in 11.5% of the EA group, 14.2% of the MA group, and 10.8% of the SA group, and included subcutaneous hematoma, post-needling pain, and pantalgia. All adverse events related to acupuncture resolved within a week and none were serious, the researchers wrote.
The study findings were limited by several factors, including the potential burden on patients of three sessions per week, the limited study population of patients with radiologic grades of II or III only, the use of self-reports, and the lack of blinding for outcome assessors, the researchers noted.
However, the results show persistent effects in reducing pain and improving function with EA or MA, compared with SA, the researchers wrote. The findings were strengthened by “adequate dosage of acupuncture, the use of the primary outcome at an individual level, and the rigorous methodology.” The use of the MCII in the primary outcome “can provide patients and policy makers with more straightforward information to decide whether a treatment should be used.”
Optimal dosing questions remain
Current options for managing KOA are limited by factors that include low efficacy and unwanted side effects, while joint replacements increase the burden on health care systems, wrote David J. Hunter, MBBS, PhD, of the University of Sydney, and Richard E. Harris, PhD, of the University of Michigan, Ann Arbor, in an accompanying editorial. “In this context, development of new treatments or identification of efficacy of existing therapies to address the huge unmet need of pain are strongly desired.” Acupuncture continues to gain popularity in North and South America, but its efficacy for pain and KOA remain controversial.
The question of dose is challenging when assessing acupuncture because the optimal dose and how to classify it remains unknown. “In this study, the authors used three treatments a week, which is more frequent than typical studies done in the West and potentially may not be feasible in some health care settings. A recent systematic review suggests that treatment frequency matters and a dose of three sessions per week may be superior to less frequent treatment,” they emphasized. Acupuncture is generally considered to be safe, but many health systems do not reimburse for it. Patients may have large out-of-pocket expenses because of the number of visits required, which may be a barrier to further implementation in practice.
“Acupuncture is already widely practiced and readily available in many countries and health care systems,” the editorialists said. However, “more research is needed in the areas of dose-response relationships, effects of blinding the acupuncturist, feasibility of three times weekly regimens, and clarifying the mechanism of effect, particularly given the persistence of benefit.”
The study was funded by Beijing Municipal Science & Technology Commission and Beijing Municipal Administration of Hospitals. The researchers had no financial conflicts to disclose. Dr. Hunter disclosed support from a National Health and Medical Research Council Investigator Grant and providing consulting advice for Merck Serono, TLC Bio, Tissuegene, Lilly, and Pfizer.
SOURCE: Tu J-F et al. Arthritis Rheumatol. 2020 Nov 10. doi: 10.1002/art.41584.
Electro-acupuncture resulted in significant improvement in pain and function, compared with sham acupuncture, in a randomized trial of more than 400 adults with knee OA.
The socioeconomic burden of knee OA (KOA) remains high, and will likely increase with the aging population and rising rates of obesity, wrote first author Jian-Feng Tu, MD, PhD, of Beijing University of Chinese Medicine and colleagues. “Since no disease-modifying pharmaceutical agents have been approved, current KOA treatments are mainly symptomatic,” and identifying new therapies in addition to pharmacological agents or surgery is a research priority, they added. The research on acupuncture as a treatment for KOA has increased, but remains controversial as researchers attempt to determine the number of sessions needed for effectiveness.
In a study published in Arthritis & Rheumatology, the researchers recruited 480 adults aged 45-75 years with confirmed KOA who reported knee pain for longer than 6 months. Participants were randomized to three groups: electroacupuncture (EA), manual acupuncture (MA), or sham acupuncture (SA). Each group received three treatment sessions per week. In all groups, electrodes were attached to selected acupuncture needles, but the current was turned on only in the EA treatment group.
The primary outcome was the response rate after 8 weeks of treatment, defined as patients who achieved the minimal clinically important improvement (MCII) on both the Numeric Rating Scale and the Western Ontario and McMaster Universities Osteoarthritis Index function subscale.
Overall, response rates at 8 weeks were 60.3%, 58.6%, and 47.3% for the EA, MA, and SA groups, respectively.
Between-group differences were statistically significant for EA versus SA (13%, P = .0234) but not for MA versus SA (11.3%, P = .0507) at 8 weeks; however, both EA and MA groups showed significantly higher response rates, compared with the SA group at 16 and 26 weeks. “Although a clinically meaningful response rate for KOA is not available in the literature, the difference of 11.3%, which indicates the number needed to treat of 9, is acceptable in clinical practices,” the researchers noted.
Adverse events occurred in 11.5% of the EA group, 14.2% of the MA group, and 10.8% of the SA group, and included subcutaneous hematoma, post-needling pain, and pantalgia. All adverse events related to acupuncture resolved within a week and none were serious, the researchers wrote.
The study findings were limited by several factors, including the potential burden on patients of three sessions per week, the limited study population of patients with radiologic grades of II or III only, the use of self-reports, and the lack of blinding for outcome assessors, the researchers noted.
However, the results show persistent effects in reducing pain and improving function with EA or MA, compared with SA, the researchers wrote. The findings were strengthened by “adequate dosage of acupuncture, the use of the primary outcome at an individual level, and the rigorous methodology.” The use of the MCII in the primary outcome “can provide patients and policy makers with more straightforward information to decide whether a treatment should be used.”
Optimal dosing questions remain
Current options for managing KOA are limited by factors that include low efficacy and unwanted side effects, while joint replacements increase the burden on health care systems, wrote David J. Hunter, MBBS, PhD, of the University of Sydney, and Richard E. Harris, PhD, of the University of Michigan, Ann Arbor, in an accompanying editorial. “In this context, development of new treatments or identification of efficacy of existing therapies to address the huge unmet need of pain are strongly desired.” Acupuncture continues to gain popularity in North and South America, but its efficacy for pain and KOA remain controversial.
The question of dose is challenging when assessing acupuncture because the optimal dose and how to classify it remains unknown. “In this study, the authors used three treatments a week, which is more frequent than typical studies done in the West and potentially may not be feasible in some health care settings. A recent systematic review suggests that treatment frequency matters and a dose of three sessions per week may be superior to less frequent treatment,” they emphasized. Acupuncture is generally considered to be safe, but many health systems do not reimburse for it. Patients may have large out-of-pocket expenses because of the number of visits required, which may be a barrier to further implementation in practice.
“Acupuncture is already widely practiced and readily available in many countries and health care systems,” the editorialists said. However, “more research is needed in the areas of dose-response relationships, effects of blinding the acupuncturist, feasibility of three times weekly regimens, and clarifying the mechanism of effect, particularly given the persistence of benefit.”
The study was funded by Beijing Municipal Science & Technology Commission and Beijing Municipal Administration of Hospitals. The researchers had no financial conflicts to disclose. Dr. Hunter disclosed support from a National Health and Medical Research Council Investigator Grant and providing consulting advice for Merck Serono, TLC Bio, Tissuegene, Lilly, and Pfizer.
SOURCE: Tu J-F et al. Arthritis Rheumatol. 2020 Nov 10. doi: 10.1002/art.41584.
Electro-acupuncture resulted in significant improvement in pain and function, compared with sham acupuncture, in a randomized trial of more than 400 adults with knee OA.
The socioeconomic burden of knee OA (KOA) remains high, and will likely increase with the aging population and rising rates of obesity, wrote first author Jian-Feng Tu, MD, PhD, of Beijing University of Chinese Medicine and colleagues. “Since no disease-modifying pharmaceutical agents have been approved, current KOA treatments are mainly symptomatic,” and identifying new therapies in addition to pharmacological agents or surgery is a research priority, they added. The research on acupuncture as a treatment for KOA has increased, but remains controversial as researchers attempt to determine the number of sessions needed for effectiveness.
In a study published in Arthritis & Rheumatology, the researchers recruited 480 adults aged 45-75 years with confirmed KOA who reported knee pain for longer than 6 months. Participants were randomized to three groups: electroacupuncture (EA), manual acupuncture (MA), or sham acupuncture (SA). Each group received three treatment sessions per week. In all groups, electrodes were attached to selected acupuncture needles, but the current was turned on only in the EA treatment group.
The primary outcome was the response rate after 8 weeks of treatment, defined as patients who achieved the minimal clinically important improvement (MCII) on both the Numeric Rating Scale and the Western Ontario and McMaster Universities Osteoarthritis Index function subscale.
Overall, response rates at 8 weeks were 60.3%, 58.6%, and 47.3% for the EA, MA, and SA groups, respectively.
Between-group differences were statistically significant for EA versus SA (13%, P = .0234) but not for MA versus SA (11.3%, P = .0507) at 8 weeks; however, both EA and MA groups showed significantly higher response rates, compared with the SA group at 16 and 26 weeks. “Although a clinically meaningful response rate for KOA is not available in the literature, the difference of 11.3%, which indicates the number needed to treat of 9, is acceptable in clinical practices,” the researchers noted.
Adverse events occurred in 11.5% of the EA group, 14.2% of the MA group, and 10.8% of the SA group, and included subcutaneous hematoma, post-needling pain, and pantalgia. All adverse events related to acupuncture resolved within a week and none were serious, the researchers wrote.
The study findings were limited by several factors, including the potential burden on patients of three sessions per week, the limited study population of patients with radiologic grades of II or III only, the use of self-reports, and the lack of blinding for outcome assessors, the researchers noted.
However, the results show persistent effects in reducing pain and improving function with EA or MA, compared with SA, the researchers wrote. The findings were strengthened by “adequate dosage of acupuncture, the use of the primary outcome at an individual level, and the rigorous methodology.” The use of the MCII in the primary outcome “can provide patients and policy makers with more straightforward information to decide whether a treatment should be used.”
Optimal dosing questions remain
Current options for managing KOA are limited by factors that include low efficacy and unwanted side effects, while joint replacements increase the burden on health care systems, wrote David J. Hunter, MBBS, PhD, of the University of Sydney, and Richard E. Harris, PhD, of the University of Michigan, Ann Arbor, in an accompanying editorial. “In this context, development of new treatments or identification of efficacy of existing therapies to address the huge unmet need of pain are strongly desired.” Acupuncture continues to gain popularity in North and South America, but its efficacy for pain and KOA remain controversial.
The question of dose is challenging when assessing acupuncture because the optimal dose and how to classify it remains unknown. “In this study, the authors used three treatments a week, which is more frequent than typical studies done in the West and potentially may not be feasible in some health care settings. A recent systematic review suggests that treatment frequency matters and a dose of three sessions per week may be superior to less frequent treatment,” they emphasized. Acupuncture is generally considered to be safe, but many health systems do not reimburse for it. Patients may have large out-of-pocket expenses because of the number of visits required, which may be a barrier to further implementation in practice.
“Acupuncture is already widely practiced and readily available in many countries and health care systems,” the editorialists said. However, “more research is needed in the areas of dose-response relationships, effects of blinding the acupuncturist, feasibility of three times weekly regimens, and clarifying the mechanism of effect, particularly given the persistence of benefit.”
The study was funded by Beijing Municipal Science & Technology Commission and Beijing Municipal Administration of Hospitals. The researchers had no financial conflicts to disclose. Dr. Hunter disclosed support from a National Health and Medical Research Council Investigator Grant and providing consulting advice for Merck Serono, TLC Bio, Tissuegene, Lilly, and Pfizer.
SOURCE: Tu J-F et al. Arthritis Rheumatol. 2020 Nov 10. doi: 10.1002/art.41584.
FROM ARTHRITIS & RHEUMATOLOGY
Warfarin use linked to knee and hip replacement in osteoarthritis patients
Patients who take the vitamin K antagonist warfarin to prevent thromboembolic events are significantly more likely to require knee or hip replacement surgery – a surrogate endpoint for end-stage osteoarthritis – than are patients who take direct oral anticoagulants (DOACs), results of a U.K.-based study showed.
In a nested case-control study, warfarin use was associated with a 1.5-fold risk for knee and hip replacement, compared with use of DOACs.
The findings provide additional evidence for the role of vitamin K and vitamin K–dependent proteins for limiting osteoarthritis progression, said lead author Priyanka Ballal, MD, a rheumatology fellow at Boston University.
“Given the prevalence and impact of osteoarthritis, our data, along with the existing literature, support the need for a well-powered, randomized, controlled trial for evaluating vitamin K supplementation in osteoarthritis. Our study also raises the consideration of using DOACs over warfarin when indicated in people with or at risk of osteoarthritis,“ she said in a plenary session at the virtual annual meeting of the American College of Rheumatology.
Warfarin targets vitamin K for its role in coagulation, but vitamin K is also an essential co-factor for vitamin K-dependent proteins in bone and cartilage, Dr. Ballal said,
Inadequate vitamin K levels are associated with abnormal joint tissue mineralization, and with increased incidence and prevalence of osteoarthritis. In a randomized, controlled trial, vitamin K supplementation was associated with trends toward less osteoarthritis progression among patients with vitamin K deficiency, she said.
To see whether warfarin therapy has biologic effects similar to that seen in patients with vitamin K deficiency, Dr. Ballal and colleagues conducted a nested, case-control study using data from The Health Improvement Network (THIN), an electronic medical record database of patients enrolled with general practitioners in the United Kingdom.
The sample included adults aged 40-80 years with atrial fibrillation who had received one or more prescriptions for warfarin or a DOAC beginning in 2009, a year after DOACs were first marketed in the United Kingdom, and within 1 year of the index date (date of joint replacement surgery). The researchers excluded patients with knee or hip replacements before 2014, severe comorbidities that would limit joint replacement, or who had used either warfarin or a DOAC prior to study entry. Each case was matched by age, gender, and index date with up to four control patients (those who did not have surgery).
A total of 913 cases and 3,652 controls were included. The groups had similar characteristics (sex, age, cancer, renal disease, chronic lung disease, hypertension, and incidence of venous thromboembolism [VTE]), except for somewhat higher rates of diabetes and heart failure among controls, and a higher rate of obesity among cases.
The investigators first looked at warfarin use among all knee and/or hip replacement cases and controls and calculated an odds ratio of 1.57 (95% confidence interval [CI], 1.30-1.89) for knee and hip replacement with warfarin after adjustment for body mass index, factors influencing choice of anticoagulant, comorbidities, other medications, general practitioner visits, and hospitalizations.
The association between warfarin and joint replacement held up in an analysis restricted to knee replacement only, with an adjusted OR of 1.48 (95% CI, 1.16-1.89).
There was also a clear association between duration of warfarin use and risk of knee and hip replacement.
“This abstract suggests the role of adequate vitamin K may be important in decreasing progression of osteoarthritis, which would then favor patients with OA who are on warfarin to consider changing to a DOAC; however, further studies are needed to confirm this finding and consider its impact on VTE and wound healing postop,” said Minna Kohler, MD, director of the rheumatology musculoskeletal ultrasound program at Massachusetts General Hospital in Boston. Dr. Kohler, who was not involved in the study, replied to an email request for comment.
The study was supported by grants from the National Institutes of Health. Dr. Ballal and Dr. Kohler reported having no conflicts of interest to disclose.
SOURCE: Ballal P et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0934.
Patients who take the vitamin K antagonist warfarin to prevent thromboembolic events are significantly more likely to require knee or hip replacement surgery – a surrogate endpoint for end-stage osteoarthritis – than are patients who take direct oral anticoagulants (DOACs), results of a U.K.-based study showed.
In a nested case-control study, warfarin use was associated with a 1.5-fold risk for knee and hip replacement, compared with use of DOACs.
The findings provide additional evidence for the role of vitamin K and vitamin K–dependent proteins for limiting osteoarthritis progression, said lead author Priyanka Ballal, MD, a rheumatology fellow at Boston University.
“Given the prevalence and impact of osteoarthritis, our data, along with the existing literature, support the need for a well-powered, randomized, controlled trial for evaluating vitamin K supplementation in osteoarthritis. Our study also raises the consideration of using DOACs over warfarin when indicated in people with or at risk of osteoarthritis,“ she said in a plenary session at the virtual annual meeting of the American College of Rheumatology.
Warfarin targets vitamin K for its role in coagulation, but vitamin K is also an essential co-factor for vitamin K-dependent proteins in bone and cartilage, Dr. Ballal said,
Inadequate vitamin K levels are associated with abnormal joint tissue mineralization, and with increased incidence and prevalence of osteoarthritis. In a randomized, controlled trial, vitamin K supplementation was associated with trends toward less osteoarthritis progression among patients with vitamin K deficiency, she said.
To see whether warfarin therapy has biologic effects similar to that seen in patients with vitamin K deficiency, Dr. Ballal and colleagues conducted a nested, case-control study using data from The Health Improvement Network (THIN), an electronic medical record database of patients enrolled with general practitioners in the United Kingdom.
The sample included adults aged 40-80 years with atrial fibrillation who had received one or more prescriptions for warfarin or a DOAC beginning in 2009, a year after DOACs were first marketed in the United Kingdom, and within 1 year of the index date (date of joint replacement surgery). The researchers excluded patients with knee or hip replacements before 2014, severe comorbidities that would limit joint replacement, or who had used either warfarin or a DOAC prior to study entry. Each case was matched by age, gender, and index date with up to four control patients (those who did not have surgery).
A total of 913 cases and 3,652 controls were included. The groups had similar characteristics (sex, age, cancer, renal disease, chronic lung disease, hypertension, and incidence of venous thromboembolism [VTE]), except for somewhat higher rates of diabetes and heart failure among controls, and a higher rate of obesity among cases.
The investigators first looked at warfarin use among all knee and/or hip replacement cases and controls and calculated an odds ratio of 1.57 (95% confidence interval [CI], 1.30-1.89) for knee and hip replacement with warfarin after adjustment for body mass index, factors influencing choice of anticoagulant, comorbidities, other medications, general practitioner visits, and hospitalizations.
The association between warfarin and joint replacement held up in an analysis restricted to knee replacement only, with an adjusted OR of 1.48 (95% CI, 1.16-1.89).
There was also a clear association between duration of warfarin use and risk of knee and hip replacement.
“This abstract suggests the role of adequate vitamin K may be important in decreasing progression of osteoarthritis, which would then favor patients with OA who are on warfarin to consider changing to a DOAC; however, further studies are needed to confirm this finding and consider its impact on VTE and wound healing postop,” said Minna Kohler, MD, director of the rheumatology musculoskeletal ultrasound program at Massachusetts General Hospital in Boston. Dr. Kohler, who was not involved in the study, replied to an email request for comment.
The study was supported by grants from the National Institutes of Health. Dr. Ballal and Dr. Kohler reported having no conflicts of interest to disclose.
SOURCE: Ballal P et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0934.
Patients who take the vitamin K antagonist warfarin to prevent thromboembolic events are significantly more likely to require knee or hip replacement surgery – a surrogate endpoint for end-stage osteoarthritis – than are patients who take direct oral anticoagulants (DOACs), results of a U.K.-based study showed.
In a nested case-control study, warfarin use was associated with a 1.5-fold risk for knee and hip replacement, compared with use of DOACs.
The findings provide additional evidence for the role of vitamin K and vitamin K–dependent proteins for limiting osteoarthritis progression, said lead author Priyanka Ballal, MD, a rheumatology fellow at Boston University.
“Given the prevalence and impact of osteoarthritis, our data, along with the existing literature, support the need for a well-powered, randomized, controlled trial for evaluating vitamin K supplementation in osteoarthritis. Our study also raises the consideration of using DOACs over warfarin when indicated in people with or at risk of osteoarthritis,“ she said in a plenary session at the virtual annual meeting of the American College of Rheumatology.
Warfarin targets vitamin K for its role in coagulation, but vitamin K is also an essential co-factor for vitamin K-dependent proteins in bone and cartilage, Dr. Ballal said,
Inadequate vitamin K levels are associated with abnormal joint tissue mineralization, and with increased incidence and prevalence of osteoarthritis. In a randomized, controlled trial, vitamin K supplementation was associated with trends toward less osteoarthritis progression among patients with vitamin K deficiency, she said.
To see whether warfarin therapy has biologic effects similar to that seen in patients with vitamin K deficiency, Dr. Ballal and colleagues conducted a nested, case-control study using data from The Health Improvement Network (THIN), an electronic medical record database of patients enrolled with general practitioners in the United Kingdom.
The sample included adults aged 40-80 years with atrial fibrillation who had received one or more prescriptions for warfarin or a DOAC beginning in 2009, a year after DOACs were first marketed in the United Kingdom, and within 1 year of the index date (date of joint replacement surgery). The researchers excluded patients with knee or hip replacements before 2014, severe comorbidities that would limit joint replacement, or who had used either warfarin or a DOAC prior to study entry. Each case was matched by age, gender, and index date with up to four control patients (those who did not have surgery).
A total of 913 cases and 3,652 controls were included. The groups had similar characteristics (sex, age, cancer, renal disease, chronic lung disease, hypertension, and incidence of venous thromboembolism [VTE]), except for somewhat higher rates of diabetes and heart failure among controls, and a higher rate of obesity among cases.
The investigators first looked at warfarin use among all knee and/or hip replacement cases and controls and calculated an odds ratio of 1.57 (95% confidence interval [CI], 1.30-1.89) for knee and hip replacement with warfarin after adjustment for body mass index, factors influencing choice of anticoagulant, comorbidities, other medications, general practitioner visits, and hospitalizations.
The association between warfarin and joint replacement held up in an analysis restricted to knee replacement only, with an adjusted OR of 1.48 (95% CI, 1.16-1.89).
There was also a clear association between duration of warfarin use and risk of knee and hip replacement.
“This abstract suggests the role of adequate vitamin K may be important in decreasing progression of osteoarthritis, which would then favor patients with OA who are on warfarin to consider changing to a DOAC; however, further studies are needed to confirm this finding and consider its impact on VTE and wound healing postop,” said Minna Kohler, MD, director of the rheumatology musculoskeletal ultrasound program at Massachusetts General Hospital in Boston. Dr. Kohler, who was not involved in the study, replied to an email request for comment.
The study was supported by grants from the National Institutes of Health. Dr. Ballal and Dr. Kohler reported having no conflicts of interest to disclose.
SOURCE: Ballal P et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 0934.
FROM ACR 2020
FDA issues new NSAIDs warning for second half of pregnancy
The U.S. Food and Drug Administration released new warnings Oct. 15 that most nonsteroidal anti-inflammatory agents (NSAIDs) carry an elevated risk for kidney complications in unborn children when taken around weeks 20 or later in pregnancy.
Citing newly available research, the agency states the risk of low amniotic fluid (known as oligohydramnios) can occur, which in turn can cause rare but serious kidney problems in the offspring. Pregnancy complications also can result.
The FDA action expands on earlier warnings about agents in this drug class, which the FDA previously cautioned about taking after week 30 of pregnancy because of heart-related risks.
Manufacturers of both over-the-counter and prescription NSAIDs – including ibuprofen, naproxen, diclofenac, and celecoxib – will be required to update their labeling with the new warning.
Low-dose (81-mg) aspirin is excluded from this warning.
“Low-dose aspirin may be an important treatment for some women during pregnancy and should be taken under the direction of a healthcare professional,” the agency stated in a news release.
“It is important that women understand the benefits and risks of the medications they may take over the course of their pregnancy,” Patrizia Cavazzoni, MD, acting director of FDA’s Center for Drug Evaluation and Research, states in the release. “To this end, the agency is using its regulatory authority to inform women and their healthcare providers about the risks if NSAIDs are used after around 20 weeks of pregnancy and beyond.”
Oligohydramnios can arise quickly – in as little as 2 days – or weeks after starting regular NSAID use in this patient population. The condition usually resolves if a pregnant woman stops taking the NSAID, the agency notes.
If a health care provider believes NSAIDs are necessary between about 20 and 30 weeks of pregnancy, use should be limited to the lowest effective dose and shortest duration possible, the Drug Safety Communication notes.
As a reminder, health care professionals and patients should report side effects from NSAIDs to the FDA’s MedWatch program.
A version of this article originally appeared on Medscape.com.
The U.S. Food and Drug Administration released new warnings Oct. 15 that most nonsteroidal anti-inflammatory agents (NSAIDs) carry an elevated risk for kidney complications in unborn children when taken around weeks 20 or later in pregnancy.
Citing newly available research, the agency states the risk of low amniotic fluid (known as oligohydramnios) can occur, which in turn can cause rare but serious kidney problems in the offspring. Pregnancy complications also can result.
The FDA action expands on earlier warnings about agents in this drug class, which the FDA previously cautioned about taking after week 30 of pregnancy because of heart-related risks.
Manufacturers of both over-the-counter and prescription NSAIDs – including ibuprofen, naproxen, diclofenac, and celecoxib – will be required to update their labeling with the new warning.
Low-dose (81-mg) aspirin is excluded from this warning.
“Low-dose aspirin may be an important treatment for some women during pregnancy and should be taken under the direction of a healthcare professional,” the agency stated in a news release.
“It is important that women understand the benefits and risks of the medications they may take over the course of their pregnancy,” Patrizia Cavazzoni, MD, acting director of FDA’s Center for Drug Evaluation and Research, states in the release. “To this end, the agency is using its regulatory authority to inform women and their healthcare providers about the risks if NSAIDs are used after around 20 weeks of pregnancy and beyond.”
Oligohydramnios can arise quickly – in as little as 2 days – or weeks after starting regular NSAID use in this patient population. The condition usually resolves if a pregnant woman stops taking the NSAID, the agency notes.
If a health care provider believes NSAIDs are necessary between about 20 and 30 weeks of pregnancy, use should be limited to the lowest effective dose and shortest duration possible, the Drug Safety Communication notes.
As a reminder, health care professionals and patients should report side effects from NSAIDs to the FDA’s MedWatch program.
A version of this article originally appeared on Medscape.com.
The U.S. Food and Drug Administration released new warnings Oct. 15 that most nonsteroidal anti-inflammatory agents (NSAIDs) carry an elevated risk for kidney complications in unborn children when taken around weeks 20 or later in pregnancy.
Citing newly available research, the agency states the risk of low amniotic fluid (known as oligohydramnios) can occur, which in turn can cause rare but serious kidney problems in the offspring. Pregnancy complications also can result.
The FDA action expands on earlier warnings about agents in this drug class, which the FDA previously cautioned about taking after week 30 of pregnancy because of heart-related risks.
Manufacturers of both over-the-counter and prescription NSAIDs – including ibuprofen, naproxen, diclofenac, and celecoxib – will be required to update their labeling with the new warning.
Low-dose (81-mg) aspirin is excluded from this warning.
“Low-dose aspirin may be an important treatment for some women during pregnancy and should be taken under the direction of a healthcare professional,” the agency stated in a news release.
“It is important that women understand the benefits and risks of the medications they may take over the course of their pregnancy,” Patrizia Cavazzoni, MD, acting director of FDA’s Center for Drug Evaluation and Research, states in the release. “To this end, the agency is using its regulatory authority to inform women and their healthcare providers about the risks if NSAIDs are used after around 20 weeks of pregnancy and beyond.”
Oligohydramnios can arise quickly – in as little as 2 days – or weeks after starting regular NSAID use in this patient population. The condition usually resolves if a pregnant woman stops taking the NSAID, the agency notes.
If a health care provider believes NSAIDs are necessary between about 20 and 30 weeks of pregnancy, use should be limited to the lowest effective dose and shortest duration possible, the Drug Safety Communication notes.
As a reminder, health care professionals and patients should report side effects from NSAIDs to the FDA’s MedWatch program.
A version of this article originally appeared on Medscape.com.
Stress tests before knee, hip replacement surgeries down, with no ill effects
Cardiac stress testing before hip and knee replacements has dropped steadily since 2006, according to results from a new study that also showed major cardiac complications to be low in the absence of stress testing – even among people with established risk factors.

Routine stress testing before noncardiac surgeries has come under fire in recent decades as an overuse of resources and a burden on patients. Practice guidelines issued in 2007 and 2014 by the American College of Cardiology and the American Heart Association sought to limit the use of preoperative testing to patients with specific cardiovascular risk factors who might have their management changed by the test results.
For their study, published online in JAMA Cardiology, Daniel S. Rubin, MD, of the University of Chicago and colleagues looked at employee-based insurance data, which included Medicare Advantage claims, for more than 800,000 total hip or knee arthroplasties (28% hip and 72% knee replacements) conducted between 2004 and 2017.
While some 10% of the cohort (mean age 62, 58% women) received a stress test in the 2 months before surgery, the investigators found that the frequency of preoperative stress testing dropped annually starting in late 2006, when it peaked at about 14%, to about 7% in 2017. Older age, male sex and a Revised Cardiac Risk Index score of 1 or greater were all associated with a higher likelihood of being tested.
The overall frequency of myocardial infarction or cardiac arrest was 0.24%, occurring in 1,677 of 686,067 patients. While the rate was higher in patients with at least one RCRI condition, this did not differ significantly between those who received a preoperative stress test and those who did not (0.60%; 221 of 36,554 vs. 0.57%; 694 of 122,466 patients.
The 2007 and 2014 ACC/AHA guidelines make clear that patients with zero RCRI conditions – which comprise a history of ischemic heart disease, heart failure, insulin therapy for diabetes, cerebrovascular disease, or chronic kidney disease – should not receive a stress test before an intermediate-risk surgery such as a hip or knee replacement. But in this study, Dr. Rubin and his colleagues found that almost half of patients who had no RCRI risk factors were stress tested anyway. This means, Dr. Rubin said in an interview, that “there’s still room for improvement” in reducing testing.
“I never want to question how a physician chooses to practice, but I have to applaud physicians for reining in the use of this test. We’re using less of this test and yet the incidence of myocardial infarction and cardiac arrest is also going down, which also calls into question whether we’re getting better at choosing the right patients for the test; or the test doesn’t impact outcomes; or overall health of these patients is improving,” he said.
One surprise finding in the study, Dr. Rubin noted, was a higher rate of complications among people without RCRI conditions who were stress tested, compared with those who were not, with a mean complication rate of 0.27%, compared with 0.14% among those who did not receive a test (P < .001). “The RCRI doesn’t capture certain things,” Dr. Rubin said. “And we know that no risk stratification tool is going to capture everything.”
The RCRI, he noted, is based on a clinical history. “If you haven’t been diagnosed yet, it won’t appear as a risk factor, even if you’re clearly at risk. The question then becomes for a physician, do you do the test or not? On a day-to-day basis it’s hard to make that decision because you want what’s best for the individual patient – and it’s hard to generalize from a study of 800,000 people what’s right for that one patient. That said, it doesn’t appear that stress testing improves outcomes and a decrease in testing appears appropriate.”
Dr. Rubin and his colleagues described as a weakness of their study that it did not capture the full scope of preoperative stress testing among Medicare patients, who are older and therefore more likely to be tested.
That the 2007 and 2014 practice guidelines bore on the drop in testing was not demonstrated by Dr. Rubin and colleagues’ study, which saw declines begin even before the guidelines were published. Nonetheless, the results appear to validate the approach advocated in the guidelines, said guideline coauthor Joshua Beckman, MD, of Vanderbilt University, whose recent research has focused on identifying risk factors for MI after noncardiac surgery.
“I hope that the guidelines have helped in changing the culture for the use of preoperative stress testing as a regular thing,” Dr. Beckman said in an interview. “In fact, the guidelines say you shouldn’t do anything before an operation that you wouldn’t do anyway. So these findings are certainly in agreement with what we’re suggesting and support the idea that unless you have something that is unstable or active, stress testing isn’t likely to help.”
Annemarie Thompson, MD, of Duke University in Durham, N.C., another coauthor on the 2014 guidelines, commented in an interview that Dr. Rubin and colleagues’ findings of a doubled rate of complications among people without RCRI conditions who were stress tested, compared with those who were not might mean something “other than just sheer overuse or overordering of tests inappropriately.”
Rather, she said, physicians might be seeing something in the clinic that cannot be captured by a screening tool reliant on existing diagnoses. “Maybe when they’re sitting in front of you in a clinic, they’re so immobile that you’re left wondering. Or maybe they haven’t been seen by a doctor in a long time,” Dr. Thompson said. “So they don’t have diagnoses if they haven’t been followed. I think what [this finding] shows is that clinicians are detecting something. They may not know what it is. But we have to give a little wiggle room to the clinician who is sitting there looking at a patient who looks like they may not make it through surgery.”
Dr. Thompson said it would be helpful, after a big-data study like this one, to go through the clinical histories of those patients – in this study fewer than 100 – who had no RCRI risk factors and yet were stress tested and ended up having complications. “Until then we’re not going to solve the mystery,” she said. “But it’s a very, very interesting study.”
Dr. Rubin is the president of DRDR Mobile Health, a company that creates mobile applications for health care and from which he has not received compensation. One of his coauthors on the study, Dr. Peter Nagele, reported fee income from Roche Diagnostics. Dr. Beckman disclosed personal fees from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, and other pharmaceutical manufacturers. Dr. Thompson has no disclosures.
SOURCE: Rubin et al. JAMA Cardiol. 2020 Sep 30. doi: 10.1001/jamacardio.2020.4311.
Cardiac stress testing before hip and knee replacements has dropped steadily since 2006, according to results from a new study that also showed major cardiac complications to be low in the absence of stress testing – even among people with established risk factors.
Routine stress testing before noncardiac surgeries has come under fire in recent decades as an overuse of resources and a burden on patients. Practice guidelines issued in 2007 and 2014 by the American College of Cardiology and the American Heart Association sought to limit the use of preoperative testing to patients with specific cardiovascular risk factors who might have their management changed by the test results.
For their study, published online in JAMA Cardiology, Daniel S. Rubin, MD, of the University of Chicago and colleagues looked at employee-based insurance data, which included Medicare Advantage claims, for more than 800,000 total hip or knee arthroplasties (28% hip and 72% knee replacements) conducted between 2004 and 2017.
While some 10% of the cohort (mean age 62, 58% women) received a stress test in the 2 months before surgery, the investigators found that the frequency of preoperative stress testing dropped annually starting in late 2006, when it peaked at about 14%, to about 7% in 2017. Older age, male sex and a Revised Cardiac Risk Index score of 1 or greater were all associated with a higher likelihood of being tested.
The overall frequency of myocardial infarction or cardiac arrest was 0.24%, occurring in 1,677 of 686,067 patients. While the rate was higher in patients with at least one RCRI condition, this did not differ significantly between those who received a preoperative stress test and those who did not (0.60%; 221 of 36,554 vs. 0.57%; 694 of 122,466 patients.
The 2007 and 2014 ACC/AHA guidelines make clear that patients with zero RCRI conditions – which comprise a history of ischemic heart disease, heart failure, insulin therapy for diabetes, cerebrovascular disease, or chronic kidney disease – should not receive a stress test before an intermediate-risk surgery such as a hip or knee replacement. But in this study, Dr. Rubin and his colleagues found that almost half of patients who had no RCRI risk factors were stress tested anyway. This means, Dr. Rubin said in an interview, that “there’s still room for improvement” in reducing testing.
“I never want to question how a physician chooses to practice, but I have to applaud physicians for reining in the use of this test. We’re using less of this test and yet the incidence of myocardial infarction and cardiac arrest is also going down, which also calls into question whether we’re getting better at choosing the right patients for the test; or the test doesn’t impact outcomes; or overall health of these patients is improving,” he said.
One surprise finding in the study, Dr. Rubin noted, was a higher rate of complications among people without RCRI conditions who were stress tested, compared with those who were not, with a mean complication rate of 0.27%, compared with 0.14% among those who did not receive a test (P < .001). “The RCRI doesn’t capture certain things,” Dr. Rubin said. “And we know that no risk stratification tool is going to capture everything.”
The RCRI, he noted, is based on a clinical history. “If you haven’t been diagnosed yet, it won’t appear as a risk factor, even if you’re clearly at risk. The question then becomes for a physician, do you do the test or not? On a day-to-day basis it’s hard to make that decision because you want what’s best for the individual patient – and it’s hard to generalize from a study of 800,000 people what’s right for that one patient. That said, it doesn’t appear that stress testing improves outcomes and a decrease in testing appears appropriate.”
Dr. Rubin and his colleagues described as a weakness of their study that it did not capture the full scope of preoperative stress testing among Medicare patients, who are older and therefore more likely to be tested.
That the 2007 and 2014 practice guidelines bore on the drop in testing was not demonstrated by Dr. Rubin and colleagues’ study, which saw declines begin even before the guidelines were published. Nonetheless, the results appear to validate the approach advocated in the guidelines, said guideline coauthor Joshua Beckman, MD, of Vanderbilt University, whose recent research has focused on identifying risk factors for MI after noncardiac surgery.
“I hope that the guidelines have helped in changing the culture for the use of preoperative stress testing as a regular thing,” Dr. Beckman said in an interview. “In fact, the guidelines say you shouldn’t do anything before an operation that you wouldn’t do anyway. So these findings are certainly in agreement with what we’re suggesting and support the idea that unless you have something that is unstable or active, stress testing isn’t likely to help.”
Annemarie Thompson, MD, of Duke University in Durham, N.C., another coauthor on the 2014 guidelines, commented in an interview that Dr. Rubin and colleagues’ findings of a doubled rate of complications among people without RCRI conditions who were stress tested, compared with those who were not might mean something “other than just sheer overuse or overordering of tests inappropriately.”
Rather, she said, physicians might be seeing something in the clinic that cannot be captured by a screening tool reliant on existing diagnoses. “Maybe when they’re sitting in front of you in a clinic, they’re so immobile that you’re left wondering. Or maybe they haven’t been seen by a doctor in a long time,” Dr. Thompson said. “So they don’t have diagnoses if they haven’t been followed. I think what [this finding] shows is that clinicians are detecting something. They may not know what it is. But we have to give a little wiggle room to the clinician who is sitting there looking at a patient who looks like they may not make it through surgery.”
Dr. Thompson said it would be helpful, after a big-data study like this one, to go through the clinical histories of those patients – in this study fewer than 100 – who had no RCRI risk factors and yet were stress tested and ended up having complications. “Until then we’re not going to solve the mystery,” she said. “But it’s a very, very interesting study.”
Dr. Rubin is the president of DRDR Mobile Health, a company that creates mobile applications for health care and from which he has not received compensation. One of his coauthors on the study, Dr. Peter Nagele, reported fee income from Roche Diagnostics. Dr. Beckman disclosed personal fees from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, and other pharmaceutical manufacturers. Dr. Thompson has no disclosures.
SOURCE: Rubin et al. JAMA Cardiol. 2020 Sep 30. doi: 10.1001/jamacardio.2020.4311.
Cardiac stress testing before hip and knee replacements has dropped steadily since 2006, according to results from a new study that also showed major cardiac complications to be low in the absence of stress testing – even among people with established risk factors.
Routine stress testing before noncardiac surgeries has come under fire in recent decades as an overuse of resources and a burden on patients. Practice guidelines issued in 2007 and 2014 by the American College of Cardiology and the American Heart Association sought to limit the use of preoperative testing to patients with specific cardiovascular risk factors who might have their management changed by the test results.
For their study, published online in JAMA Cardiology, Daniel S. Rubin, MD, of the University of Chicago and colleagues looked at employee-based insurance data, which included Medicare Advantage claims, for more than 800,000 total hip or knee arthroplasties (28% hip and 72% knee replacements) conducted between 2004 and 2017.
While some 10% of the cohort (mean age 62, 58% women) received a stress test in the 2 months before surgery, the investigators found that the frequency of preoperative stress testing dropped annually starting in late 2006, when it peaked at about 14%, to about 7% in 2017. Older age, male sex and a Revised Cardiac Risk Index score of 1 or greater were all associated with a higher likelihood of being tested.
The overall frequency of myocardial infarction or cardiac arrest was 0.24%, occurring in 1,677 of 686,067 patients. While the rate was higher in patients with at least one RCRI condition, this did not differ significantly between those who received a preoperative stress test and those who did not (0.60%; 221 of 36,554 vs. 0.57%; 694 of 122,466 patients.
The 2007 and 2014 ACC/AHA guidelines make clear that patients with zero RCRI conditions – which comprise a history of ischemic heart disease, heart failure, insulin therapy for diabetes, cerebrovascular disease, or chronic kidney disease – should not receive a stress test before an intermediate-risk surgery such as a hip or knee replacement. But in this study, Dr. Rubin and his colleagues found that almost half of patients who had no RCRI risk factors were stress tested anyway. This means, Dr. Rubin said in an interview, that “there’s still room for improvement” in reducing testing.
“I never want to question how a physician chooses to practice, but I have to applaud physicians for reining in the use of this test. We’re using less of this test and yet the incidence of myocardial infarction and cardiac arrest is also going down, which also calls into question whether we’re getting better at choosing the right patients for the test; or the test doesn’t impact outcomes; or overall health of these patients is improving,” he said.
One surprise finding in the study, Dr. Rubin noted, was a higher rate of complications among people without RCRI conditions who were stress tested, compared with those who were not, with a mean complication rate of 0.27%, compared with 0.14% among those who did not receive a test (P < .001). “The RCRI doesn’t capture certain things,” Dr. Rubin said. “And we know that no risk stratification tool is going to capture everything.”
The RCRI, he noted, is based on a clinical history. “If you haven’t been diagnosed yet, it won’t appear as a risk factor, even if you’re clearly at risk. The question then becomes for a physician, do you do the test or not? On a day-to-day basis it’s hard to make that decision because you want what’s best for the individual patient – and it’s hard to generalize from a study of 800,000 people what’s right for that one patient. That said, it doesn’t appear that stress testing improves outcomes and a decrease in testing appears appropriate.”
Dr. Rubin and his colleagues described as a weakness of their study that it did not capture the full scope of preoperative stress testing among Medicare patients, who are older and therefore more likely to be tested.
That the 2007 and 2014 practice guidelines bore on the drop in testing was not demonstrated by Dr. Rubin and colleagues’ study, which saw declines begin even before the guidelines were published. Nonetheless, the results appear to validate the approach advocated in the guidelines, said guideline coauthor Joshua Beckman, MD, of Vanderbilt University, whose recent research has focused on identifying risk factors for MI after noncardiac surgery.
“I hope that the guidelines have helped in changing the culture for the use of preoperative stress testing as a regular thing,” Dr. Beckman said in an interview. “In fact, the guidelines say you shouldn’t do anything before an operation that you wouldn’t do anyway. So these findings are certainly in agreement with what we’re suggesting and support the idea that unless you have something that is unstable or active, stress testing isn’t likely to help.”
Annemarie Thompson, MD, of Duke University in Durham, N.C., another coauthor on the 2014 guidelines, commented in an interview that Dr. Rubin and colleagues’ findings of a doubled rate of complications among people without RCRI conditions who were stress tested, compared with those who were not might mean something “other than just sheer overuse or overordering of tests inappropriately.”
Rather, she said, physicians might be seeing something in the clinic that cannot be captured by a screening tool reliant on existing diagnoses. “Maybe when they’re sitting in front of you in a clinic, they’re so immobile that you’re left wondering. Or maybe they haven’t been seen by a doctor in a long time,” Dr. Thompson said. “So they don’t have diagnoses if they haven’t been followed. I think what [this finding] shows is that clinicians are detecting something. They may not know what it is. But we have to give a little wiggle room to the clinician who is sitting there looking at a patient who looks like they may not make it through surgery.”
Dr. Thompson said it would be helpful, after a big-data study like this one, to go through the clinical histories of those patients – in this study fewer than 100 – who had no RCRI risk factors and yet were stress tested and ended up having complications. “Until then we’re not going to solve the mystery,” she said. “But it’s a very, very interesting study.”
Dr. Rubin is the president of DRDR Mobile Health, a company that creates mobile applications for health care and from which he has not received compensation. One of his coauthors on the study, Dr. Peter Nagele, reported fee income from Roche Diagnostics. Dr. Beckman disclosed personal fees from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, and other pharmaceutical manufacturers. Dr. Thompson has no disclosures.
SOURCE: Rubin et al. JAMA Cardiol. 2020 Sep 30. doi: 10.1001/jamacardio.2020.4311.
FROM JAMA CARDIOLOGY