User login
DDNA 2019 - Heartburn: Modern Diagnosis of GERD
AT DIGESTIVE DISEASES: NEW ADVANCES

Interactive online module improved detection of Barrett’s esophagus neoplasia
An online educational tool for endoscopists helped improve their detection of Barrett’s esophagus–related neoplasia (BORN), researchers reported in the April issue of Gastroenterology.
In tests administered before and after training, endoscopists increased their rates of BORN detection by a median of 30% (P less than .001), reported J.J. Bergman, MD, PhD, of the University of Amsterdam, together with his associates. “To our knowledge, this is the first validated online, interactive endoscopic training program in our field,” they wrote. “Widespread use of this tool might improve management of Barrett’s esophagus by general endoscopists.”
To develop the program, the investigators recorded high-definition videos of upper endoscopies of patients with either BORN or nondysplastic Barrett’s esophagus. They sent these videos to three experts, who used special tools to superimpose their delineations of lesions.
Next, 68 general endoscopists (fellows, early-career general gastroenterologists, and senior general gastroenterologists) watched four batches of 20 videos each. The researchers compared the assessors’ interpretations with the experts’ to identify the 25 videos with the most educational impact. These were then shown in four batches of five to 121 new assessors (five videos were reserved for pre- and post testing).
From the first to the fourth batch of training videos, assessors sequentially improved their scores for detection, delineation, agreement delineation, and relative delineation of BORN, the researchers said. Among the 121 assessors in the second phase of development, median rates of detection of BORN rose by 30% after training. Furthermore, from baseline to the end of the study, scores rose by 46% for detection, 129% for delineation, 105% for agreement delineation, and 106% for relative delineation (all P less than .001). These improvements did not depend on the country of origin of the assessors or their level of endoscopic experience.
This module requires the use of high-definition videos whose resolution is not lost during replay or when viewed on the web, the researchers emphasized. They noted that the module is active, not passive – learners select the video frame to position a biopsy mark and delineate the lesion, and the software then gives them tailored feedback on their choice. Learners also can add and remove the experts’ delineations as well as their own during feedback sessions at the end of each batch of videos. This enables them to “fully appreciate the subtle appearance of the lesion on the selected time frame,” the investigators wrote.
By completing the training module, “general endoscopists with a wide range of experience and from different countries of origin can substantially and conveniently increase their skills for detection and delineation of early BORN lesions,” they concluded. “Therefore, the module could provide training in an essential upper gastrointestinal endoscopic skill that is not otherwise readily available.”
The investigators disclosed no external funding sources. They reported having no conflicts of interest.
SOURCE: Bergman JJ et al. Gastroenterology. 2019 Jan 2. doi: 10.1053/j.gastro.2018.12.021.
Endoscopic mucosal resection and ablation strategies offer the potential for minimally invasive, curative treatment for patients with Barrett’s esophagus–associated intramucosal neoplasia. For the gastroenterologist interested in endoscopic prevention and management of esophageal cancer, however, achieving proficiency in performance of these endoscopic techniques represents only part of the requisite preparatory experience. Acquisition of cognitive skills in lesion recognition is a fundamental and underappreciated component to a successful endoscopic treatment paradigm.

General endoscopist assessors were grouped into three groups based on level of experience. Following completion of the training module, scores in lesion detection and delineation increased irrespective of level of endoscopist experience.
The module is free, CME-accredited, and available for online use. Any endoscopist who performs Barrett’s screening, surveillance, and therapy should be motivated and incentivized to engage with this important educational tool.
Patrick Yachimski, MD, MPH, AGAF, is associate professor of medicine, director of pancreatobiliary endoscopy, division of gastroenterology, hepatology & nutrition, Vanderbilt University Medical Center, Nashville, Tenn. He has no conflicts.
Endoscopic mucosal resection and ablation strategies offer the potential for minimally invasive, curative treatment for patients with Barrett’s esophagus–associated intramucosal neoplasia. For the gastroenterologist interested in endoscopic prevention and management of esophageal cancer, however, achieving proficiency in performance of these endoscopic techniques represents only part of the requisite preparatory experience. Acquisition of cognitive skills in lesion recognition is a fundamental and underappreciated component to a successful endoscopic treatment paradigm.
General endoscopist assessors were grouped into three groups based on level of experience. Following completion of the training module, scores in lesion detection and delineation increased irrespective of level of endoscopist experience.
The module is free, CME-accredited, and available for online use. Any endoscopist who performs Barrett’s screening, surveillance, and therapy should be motivated and incentivized to engage with this important educational tool.
Patrick Yachimski, MD, MPH, AGAF, is associate professor of medicine, director of pancreatobiliary endoscopy, division of gastroenterology, hepatology & nutrition, Vanderbilt University Medical Center, Nashville, Tenn. He has no conflicts.
Endoscopic mucosal resection and ablation strategies offer the potential for minimally invasive, curative treatment for patients with Barrett’s esophagus–associated intramucosal neoplasia. For the gastroenterologist interested in endoscopic prevention and management of esophageal cancer, however, achieving proficiency in performance of these endoscopic techniques represents only part of the requisite preparatory experience. Acquisition of cognitive skills in lesion recognition is a fundamental and underappreciated component to a successful endoscopic treatment paradigm.
General endoscopist assessors were grouped into three groups based on level of experience. Following completion of the training module, scores in lesion detection and delineation increased irrespective of level of endoscopist experience.
The module is free, CME-accredited, and available for online use. Any endoscopist who performs Barrett’s screening, surveillance, and therapy should be motivated and incentivized to engage with this important educational tool.
Patrick Yachimski, MD, MPH, AGAF, is associate professor of medicine, director of pancreatobiliary endoscopy, division of gastroenterology, hepatology & nutrition, Vanderbilt University Medical Center, Nashville, Tenn. He has no conflicts.
An online educational tool for endoscopists helped improve their detection of Barrett’s esophagus–related neoplasia (BORN), researchers reported in the April issue of Gastroenterology.
In tests administered before and after training, endoscopists increased their rates of BORN detection by a median of 30% (P less than .001), reported J.J. Bergman, MD, PhD, of the University of Amsterdam, together with his associates. “To our knowledge, this is the first validated online, interactive endoscopic training program in our field,” they wrote. “Widespread use of this tool might improve management of Barrett’s esophagus by general endoscopists.”
To develop the program, the investigators recorded high-definition videos of upper endoscopies of patients with either BORN or nondysplastic Barrett’s esophagus. They sent these videos to three experts, who used special tools to superimpose their delineations of lesions.
Next, 68 general endoscopists (fellows, early-career general gastroenterologists, and senior general gastroenterologists) watched four batches of 20 videos each. The researchers compared the assessors’ interpretations with the experts’ to identify the 25 videos with the most educational impact. These were then shown in four batches of five to 121 new assessors (five videos were reserved for pre- and post testing).
From the first to the fourth batch of training videos, assessors sequentially improved their scores for detection, delineation, agreement delineation, and relative delineation of BORN, the researchers said. Among the 121 assessors in the second phase of development, median rates of detection of BORN rose by 30% after training. Furthermore, from baseline to the end of the study, scores rose by 46% for detection, 129% for delineation, 105% for agreement delineation, and 106% for relative delineation (all P less than .001). These improvements did not depend on the country of origin of the assessors or their level of endoscopic experience.
This module requires the use of high-definition videos whose resolution is not lost during replay or when viewed on the web, the researchers emphasized. They noted that the module is active, not passive – learners select the video frame to position a biopsy mark and delineate the lesion, and the software then gives them tailored feedback on their choice. Learners also can add and remove the experts’ delineations as well as their own during feedback sessions at the end of each batch of videos. This enables them to “fully appreciate the subtle appearance of the lesion on the selected time frame,” the investigators wrote.
By completing the training module, “general endoscopists with a wide range of experience and from different countries of origin can substantially and conveniently increase their skills for detection and delineation of early BORN lesions,” they concluded. “Therefore, the module could provide training in an essential upper gastrointestinal endoscopic skill that is not otherwise readily available.”
The investigators disclosed no external funding sources. They reported having no conflicts of interest.
SOURCE: Bergman JJ et al. Gastroenterology. 2019 Jan 2. doi: 10.1053/j.gastro.2018.12.021.
An online educational tool for endoscopists helped improve their detection of Barrett’s esophagus–related neoplasia (BORN), researchers reported in the April issue of Gastroenterology.
In tests administered before and after training, endoscopists increased their rates of BORN detection by a median of 30% (P less than .001), reported J.J. Bergman, MD, PhD, of the University of Amsterdam, together with his associates. “To our knowledge, this is the first validated online, interactive endoscopic training program in our field,” they wrote. “Widespread use of this tool might improve management of Barrett’s esophagus by general endoscopists.”
To develop the program, the investigators recorded high-definition videos of upper endoscopies of patients with either BORN or nondysplastic Barrett’s esophagus. They sent these videos to three experts, who used special tools to superimpose their delineations of lesions.
Next, 68 general endoscopists (fellows, early-career general gastroenterologists, and senior general gastroenterologists) watched four batches of 20 videos each. The researchers compared the assessors’ interpretations with the experts’ to identify the 25 videos with the most educational impact. These were then shown in four batches of five to 121 new assessors (five videos were reserved for pre- and post testing).
From the first to the fourth batch of training videos, assessors sequentially improved their scores for detection, delineation, agreement delineation, and relative delineation of BORN, the researchers said. Among the 121 assessors in the second phase of development, median rates of detection of BORN rose by 30% after training. Furthermore, from baseline to the end of the study, scores rose by 46% for detection, 129% for delineation, 105% for agreement delineation, and 106% for relative delineation (all P less than .001). These improvements did not depend on the country of origin of the assessors or their level of endoscopic experience.
This module requires the use of high-definition videos whose resolution is not lost during replay or when viewed on the web, the researchers emphasized. They noted that the module is active, not passive – learners select the video frame to position a biopsy mark and delineate the lesion, and the software then gives them tailored feedback on their choice. Learners also can add and remove the experts’ delineations as well as their own during feedback sessions at the end of each batch of videos. This enables them to “fully appreciate the subtle appearance of the lesion on the selected time frame,” the investigators wrote.
By completing the training module, “general endoscopists with a wide range of experience and from different countries of origin can substantially and conveniently increase their skills for detection and delineation of early BORN lesions,” they concluded. “Therefore, the module could provide training in an essential upper gastrointestinal endoscopic skill that is not otherwise readily available.”
The investigators disclosed no external funding sources. They reported having no conflicts of interest.
SOURCE: Bergman JJ et al. Gastroenterology. 2019 Jan 2. doi: 10.1053/j.gastro.2018.12.021.
FROM GASTROENTEROLOGY
Barrett’s esophagus uncommon in patients with uncomplicated GERD
Uncomplicated gastroesophageal reflux disease (GERD) accounted for 13.5% of esophagogastroduodenoscopies, but 5.6% of these patients had suspected Barrett’s esophagus and only 1.4% had suspected long-segment Barrett’s esophagus, researchers reported. The study appears in the April issue of Clinical Gastroenterology and Hepatology.
“The prevalence of suspected Barrett’s esophagus is lower than in prior time periods. This raises questions about the utility of esophagogastroduodenoscopies to detect Barrett’s esophagus in patients with uncomplicated GERD,” wrote Emery C. Lin, MD, of Oregon Health and Science University, Portland, and his associates there and at Massachusetts General Hospital, Boston.
Symptoms of GERD affect more than one in four U.S. adults and are a risk factor for Barrett’s esophagus. However, the prevalence of Barrett’s esophagus is unclear in patients with dysphagia and in the era of proton pump inhibitors, the researchers said. The American Gastroenterological Association strongly discourages reflexively screening patients with GERD for Barrett’s esophagus, but “weakly recommends” screening GERD patients with multiple risk factors for Barrett’s esophagus, including chronic GERD, hiatal hernia, older age (50 years and up), white race, male sex, increased body mass index, and intra-abdominal adiposity.
To understand the prevalence and findings of esophagogastroduodenoscopy in patients with GERD without alarm symptoms (including weight loss, dysphagia, and bleeding), the investigators studied 543,103 of these procedures performed at 82 sites in the United States between 2003 and 2013. The data came from the National Endoscopic Database, which generates endoscopy reports using a structured computer form.
A total of 73,535 esophagogastroduodenoscopies (13.5%) were performed for GERD without alarm symptoms. Among these patients, 4,122 (5.6%) had suspected Barrett’s esophagus, of which 24.2% had suspected long-segment Barrett’s esophagus (3 cm or longer). Among patients with uncomplicated GERD, the prevalence of suspected Barrett’s esophagus was 5.6%, and the prevalence of long-segment disease was 1.4%.
Although male sex, older age, and white race were significant risk factors for suspected Barrett’s esophagus and suspected long-segment disease, 23.6% of esophagogastroduodenoscopies were performed in white men older than 50 years. “We find that low-risk populations with uncomplicated GERD make up a significant number of esophagogastroduodenoscopies done for uncomplicated GERD,” the investigators wrote. “If esophagogastroduodenoscopies were limited to patients that met the AGA criteria of being male, white, and age over 50, we would have detected 34 of 47 (72.3%) of esophageal tumors and found suspected Barrett’s esophagus in nearly 10%, while reducing the burden of endoscopy by more than 75%.”
Hiatal hernia was a significant correlate of suspected Barrett’s esophagus (odds ratio, 1.6), the researchers noted. Esophagitis was not associated with suspected Barrett’s esophagus overall but did correlate with long-segment disease. Esophagitis might mask underlying short-segment Barrett’s esophagus, and short-segment Barrett’s esophagus might be milder in nature and more responsive to antisecretory therapy, the researchers said. They noted that severe (grade C/D) esophagitis was strongly linked with both short-segment and long-segment Barrett’s esophagus.
The National Institute of Diabetes and Digestive and Kidney Diseases provided funding. The researchers reported having no conflicts of interest.
SOURCE: Lin EC et al. Clin Gastroenterol Hepatol. 2019 Apr. doi: 10.1016/j.cgh.2018.08.066.
The utility and cost-effectiveness of screening for Barrett’s esophagus with esophagogastroduodenoscopy (EGD) remain contentious issues. National GI societies currently recommend screening in only a limited high-risk population, mainly white men aged 50 or older with chronic GERD and one or more additional risk factors. It is unclear to what degree those guidelines are adhered to in clinical practice. This study by Lin et al. sheds further light on this issue. The investigators showed that a significant proportion (more than 10%) of EGDs were performed for uncomplicated GERD, with less than one-quarter of those patients meeting the minimal criteria for screening for Barrett’s esophagus. Among this group, the prevalence of Barrett’s esophagus was found to be lower than previously reported. The data offer compelling evidence that screening low-risk patients with uncomplicated GERD by using upper endoscopy is not cost effective, and is at best marginally cost effective if limited to the high-risk group identified by national GI societies. The question arises whether we should abandon screening for Barrett’s esophagus altogether.
The challenge, however, is that the incidence of esophageal adenocarcinoma continues to rise (albeit at a slower pace in recent years), and 5-year survival of patients diagnosed with esophageal adenocarcinoma remains extremely poor. Therefore, prevention remains the optimal strategy. The solution may lie in adopting a lower-cost screening modality that can replace endoscopy for this purpose, and while many such techniques are under investigation, further studies are required to find a widely applicable alternative to EGD.
Nabil M. Mansour, MD, is an assistant professor, department of medicine, section of gastroenterology and hepatology, Baylor College of Medicine, Houston. He has no conflicts of interest.
The utility and cost-effectiveness of screening for Barrett’s esophagus with esophagogastroduodenoscopy (EGD) remain contentious issues. National GI societies currently recommend screening in only a limited high-risk population, mainly white men aged 50 or older with chronic GERD and one or more additional risk factors. It is unclear to what degree those guidelines are adhered to in clinical practice. This study by Lin et al. sheds further light on this issue. The investigators showed that a significant proportion (more than 10%) of EGDs were performed for uncomplicated GERD, with less than one-quarter of those patients meeting the minimal criteria for screening for Barrett’s esophagus. Among this group, the prevalence of Barrett’s esophagus was found to be lower than previously reported. The data offer compelling evidence that screening low-risk patients with uncomplicated GERD by using upper endoscopy is not cost effective, and is at best marginally cost effective if limited to the high-risk group identified by national GI societies. The question arises whether we should abandon screening for Barrett’s esophagus altogether.
The challenge, however, is that the incidence of esophageal adenocarcinoma continues to rise (albeit at a slower pace in recent years), and 5-year survival of patients diagnosed with esophageal adenocarcinoma remains extremely poor. Therefore, prevention remains the optimal strategy. The solution may lie in adopting a lower-cost screening modality that can replace endoscopy for this purpose, and while many such techniques are under investigation, further studies are required to find a widely applicable alternative to EGD.
Nabil M. Mansour, MD, is an assistant professor, department of medicine, section of gastroenterology and hepatology, Baylor College of Medicine, Houston. He has no conflicts of interest.
The utility and cost-effectiveness of screening for Barrett’s esophagus with esophagogastroduodenoscopy (EGD) remain contentious issues. National GI societies currently recommend screening in only a limited high-risk population, mainly white men aged 50 or older with chronic GERD and one or more additional risk factors. It is unclear to what degree those guidelines are adhered to in clinical practice. This study by Lin et al. sheds further light on this issue. The investigators showed that a significant proportion (more than 10%) of EGDs were performed for uncomplicated GERD, with less than one-quarter of those patients meeting the minimal criteria for screening for Barrett’s esophagus. Among this group, the prevalence of Barrett’s esophagus was found to be lower than previously reported. The data offer compelling evidence that screening low-risk patients with uncomplicated GERD by using upper endoscopy is not cost effective, and is at best marginally cost effective if limited to the high-risk group identified by national GI societies. The question arises whether we should abandon screening for Barrett’s esophagus altogether.
The challenge, however, is that the incidence of esophageal adenocarcinoma continues to rise (albeit at a slower pace in recent years), and 5-year survival of patients diagnosed with esophageal adenocarcinoma remains extremely poor. Therefore, prevention remains the optimal strategy. The solution may lie in adopting a lower-cost screening modality that can replace endoscopy for this purpose, and while many such techniques are under investigation, further studies are required to find a widely applicable alternative to EGD.
Nabil M. Mansour, MD, is an assistant professor, department of medicine, section of gastroenterology and hepatology, Baylor College of Medicine, Houston. He has no conflicts of interest.
Uncomplicated gastroesophageal reflux disease (GERD) accounted for 13.5% of esophagogastroduodenoscopies, but 5.6% of these patients had suspected Barrett’s esophagus and only 1.4% had suspected long-segment Barrett’s esophagus, researchers reported. The study appears in the April issue of Clinical Gastroenterology and Hepatology.
“The prevalence of suspected Barrett’s esophagus is lower than in prior time periods. This raises questions about the utility of esophagogastroduodenoscopies to detect Barrett’s esophagus in patients with uncomplicated GERD,” wrote Emery C. Lin, MD, of Oregon Health and Science University, Portland, and his associates there and at Massachusetts General Hospital, Boston.
Symptoms of GERD affect more than one in four U.S. adults and are a risk factor for Barrett’s esophagus. However, the prevalence of Barrett’s esophagus is unclear in patients with dysphagia and in the era of proton pump inhibitors, the researchers said. The American Gastroenterological Association strongly discourages reflexively screening patients with GERD for Barrett’s esophagus, but “weakly recommends” screening GERD patients with multiple risk factors for Barrett’s esophagus, including chronic GERD, hiatal hernia, older age (50 years and up), white race, male sex, increased body mass index, and intra-abdominal adiposity.
To understand the prevalence and findings of esophagogastroduodenoscopy in patients with GERD without alarm symptoms (including weight loss, dysphagia, and bleeding), the investigators studied 543,103 of these procedures performed at 82 sites in the United States between 2003 and 2013. The data came from the National Endoscopic Database, which generates endoscopy reports using a structured computer form.
A total of 73,535 esophagogastroduodenoscopies (13.5%) were performed for GERD without alarm symptoms. Among these patients, 4,122 (5.6%) had suspected Barrett’s esophagus, of which 24.2% had suspected long-segment Barrett’s esophagus (3 cm or longer). Among patients with uncomplicated GERD, the prevalence of suspected Barrett’s esophagus was 5.6%, and the prevalence of long-segment disease was 1.4%.
Although male sex, older age, and white race were significant risk factors for suspected Barrett’s esophagus and suspected long-segment disease, 23.6% of esophagogastroduodenoscopies were performed in white men older than 50 years. “We find that low-risk populations with uncomplicated GERD make up a significant number of esophagogastroduodenoscopies done for uncomplicated GERD,” the investigators wrote. “If esophagogastroduodenoscopies were limited to patients that met the AGA criteria of being male, white, and age over 50, we would have detected 34 of 47 (72.3%) of esophageal tumors and found suspected Barrett’s esophagus in nearly 10%, while reducing the burden of endoscopy by more than 75%.”
Hiatal hernia was a significant correlate of suspected Barrett’s esophagus (odds ratio, 1.6), the researchers noted. Esophagitis was not associated with suspected Barrett’s esophagus overall but did correlate with long-segment disease. Esophagitis might mask underlying short-segment Barrett’s esophagus, and short-segment Barrett’s esophagus might be milder in nature and more responsive to antisecretory therapy, the researchers said. They noted that severe (grade C/D) esophagitis was strongly linked with both short-segment and long-segment Barrett’s esophagus.
The National Institute of Diabetes and Digestive and Kidney Diseases provided funding. The researchers reported having no conflicts of interest.
SOURCE: Lin EC et al. Clin Gastroenterol Hepatol. 2019 Apr. doi: 10.1016/j.cgh.2018.08.066.
Uncomplicated gastroesophageal reflux disease (GERD) accounted for 13.5% of esophagogastroduodenoscopies, but 5.6% of these patients had suspected Barrett’s esophagus and only 1.4% had suspected long-segment Barrett’s esophagus, researchers reported. The study appears in the April issue of Clinical Gastroenterology and Hepatology.
“The prevalence of suspected Barrett’s esophagus is lower than in prior time periods. This raises questions about the utility of esophagogastroduodenoscopies to detect Barrett’s esophagus in patients with uncomplicated GERD,” wrote Emery C. Lin, MD, of Oregon Health and Science University, Portland, and his associates there and at Massachusetts General Hospital, Boston.
Symptoms of GERD affect more than one in four U.S. adults and are a risk factor for Barrett’s esophagus. However, the prevalence of Barrett’s esophagus is unclear in patients with dysphagia and in the era of proton pump inhibitors, the researchers said. The American Gastroenterological Association strongly discourages reflexively screening patients with GERD for Barrett’s esophagus, but “weakly recommends” screening GERD patients with multiple risk factors for Barrett’s esophagus, including chronic GERD, hiatal hernia, older age (50 years and up), white race, male sex, increased body mass index, and intra-abdominal adiposity.
To understand the prevalence and findings of esophagogastroduodenoscopy in patients with GERD without alarm symptoms (including weight loss, dysphagia, and bleeding), the investigators studied 543,103 of these procedures performed at 82 sites in the United States between 2003 and 2013. The data came from the National Endoscopic Database, which generates endoscopy reports using a structured computer form.
A total of 73,535 esophagogastroduodenoscopies (13.5%) were performed for GERD without alarm symptoms. Among these patients, 4,122 (5.6%) had suspected Barrett’s esophagus, of which 24.2% had suspected long-segment Barrett’s esophagus (3 cm or longer). Among patients with uncomplicated GERD, the prevalence of suspected Barrett’s esophagus was 5.6%, and the prevalence of long-segment disease was 1.4%.
Although male sex, older age, and white race were significant risk factors for suspected Barrett’s esophagus and suspected long-segment disease, 23.6% of esophagogastroduodenoscopies were performed in white men older than 50 years. “We find that low-risk populations with uncomplicated GERD make up a significant number of esophagogastroduodenoscopies done for uncomplicated GERD,” the investigators wrote. “If esophagogastroduodenoscopies were limited to patients that met the AGA criteria of being male, white, and age over 50, we would have detected 34 of 47 (72.3%) of esophageal tumors and found suspected Barrett’s esophagus in nearly 10%, while reducing the burden of endoscopy by more than 75%.”
Hiatal hernia was a significant correlate of suspected Barrett’s esophagus (odds ratio, 1.6), the researchers noted. Esophagitis was not associated with suspected Barrett’s esophagus overall but did correlate with long-segment disease. Esophagitis might mask underlying short-segment Barrett’s esophagus, and short-segment Barrett’s esophagus might be milder in nature and more responsive to antisecretory therapy, the researchers said. They noted that severe (grade C/D) esophagitis was strongly linked with both short-segment and long-segment Barrett’s esophagus.
The National Institute of Diabetes and Digestive and Kidney Diseases provided funding. The researchers reported having no conflicts of interest.
SOURCE: Lin EC et al. Clin Gastroenterol Hepatol. 2019 Apr. doi: 10.1016/j.cgh.2018.08.066.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Long-term budesonide oral suspension well tolerated in EoE
Treatment with budesonide oral suspension (BOS) was generally well tolerated and maintained a histologic response in some patients with eosinophilic esophagitis (EoE), according to the results of the 24-week, open-label extension phase of a multicenter, randomized, placebo-controlled, industry-sponsored trial.
Rates of histologic response (up to 6 eosinophils per high-power field) were “modest” – 23% among patients who stayed on BOS throughout the study and 48.5% among patients who initiated BOS after 12 weeks on placebo, reported Evan S. Dellon, MD, MPH, of the University of North Carolina in Chapel Hill and his associates. However, these rates “need to be viewed in the context of a highly symptomatic and histologically severe population with eosinophilic esophagitis,” they contended. A total of 11% of budesonide initiators developed esophageal candidiasis, they reported in Clinical Gastroenterology and Hepatology.
Budesonide oral suspension is a mucoadherent formulation of topical corticosteroid that has recently been developed to treat EoE. Previously, during the randomized, double-blind component of this phase 2 trial, 93 patients aged 11-40 years with active EoE and dysphagia received either BOS (2 mg) or placebo twice daily (Gastroenterology. 2017 Mar;157[4]:776-86). After 12 weeks, rates of histologic response were 39% for BOS versus 3% for placebo, and BOS significantly improved patients’ mean peak eosinophil count and scores on the Dysphagia Symptom Questionnaire, compared with baseline and compared with the response in the placebo group. During the open-label extension phase, 45 BOS continuers and 37 BOS initiators received 2 mg once daily for 12 weeks and then had the option to increase the BOS dose to 1.5-2.0 mg twice daily.
The rate of drug-related adverse events was 19% among BOS initiators and 4% among BOS continuers. One patient in each group developed oral candidiasis, while four BOS initiators (11%) developed esophageal candidiasis. Three BOS continuers had subnormal morning cortisol levels; while these were subclinical cases, they merit attention since long-term corticosteroids for EoE have been linked with possible hypothalamic–pituitary–adrenal axis suppression, the researchers noted.
In addition, while BOS initiators tended to maintain their endoscopic response, only 42% of those with an initial histologic response maintained a histologic response after 36 weeks of treatment or when leaving the study. Post hoc analyses confirmed that prolonged BOS treatment does not increase the chances of histologic or endoscopic response. Prior studies have suggested that EoE can become steroid-refractory over time and that certain molecular and histologic markers might predict resistance, the investigators noted.
Meritage Pharma (now part of Shire) was involved in the study design and conduct, data collection and management, and manuscript review. Dr. Dellon disclosed research funding from Meritage and Shire and a consulting relationship with Shire, along with ties to several other pharmaceutical companies. All six coinvestigators also disclosed ties to Meritage, Shire, or both, and two are Shire employees and stockholders.
*This story was updated on Feb. 7, 2019.
SOURCE: Dellon ES et al. Clin Gastroenterol Hepatol. 2018 Jun 11. doi: 10.1016/j.cgh.2018.05.051.
Guidelines regarding the management of eosinophilic esophagitis (EoE) with topical steroids are still unclear with regard to dosing and duration. Here, Dellon et al. present evidence that long-term budesonide oral suspension (BOS) therapy is safe and efficacious. Both the BOS and placebo cohorts of the initial, 12-week trial demonstrated clinical and histologic improvement on BOS over this 24-week period, with few adverse events. Maintenance of histologic response was only seen in 42% in initial BOS responders, suggesting steroid tolerance or resistance may develop. Another important observation was that peak eosinphil count decreased steroid dosing.

Finally, these data support the notion that initial responders are unlikely to gain response with continued therapy and may be better served with early transition to alternatives. Further research is needed to clarify these issues and which patients may be predisposed to nonresponse or loss of response.
Reena V. Chokshi, MD , is assistant professor of medicine in the department of gastroenterology at Baylor College of Medicine, Houston.
Guidelines regarding the management of eosinophilic esophagitis (EoE) with topical steroids are still unclear with regard to dosing and duration. Here, Dellon et al. present evidence that long-term budesonide oral suspension (BOS) therapy is safe and efficacious. Both the BOS and placebo cohorts of the initial, 12-week trial demonstrated clinical and histologic improvement on BOS over this 24-week period, with few adverse events. Maintenance of histologic response was only seen in 42% in initial BOS responders, suggesting steroid tolerance or resistance may develop. Another important observation was that peak eosinphil count decreased steroid dosing.
Finally, these data support the notion that initial responders are unlikely to gain response with continued therapy and may be better served with early transition to alternatives. Further research is needed to clarify these issues and which patients may be predisposed to nonresponse or loss of response.
Reena V. Chokshi, MD , is assistant professor of medicine in the department of gastroenterology at Baylor College of Medicine, Houston.
Guidelines regarding the management of eosinophilic esophagitis (EoE) with topical steroids are still unclear with regard to dosing and duration. Here, Dellon et al. present evidence that long-term budesonide oral suspension (BOS) therapy is safe and efficacious. Both the BOS and placebo cohorts of the initial, 12-week trial demonstrated clinical and histologic improvement on BOS over this 24-week period, with few adverse events. Maintenance of histologic response was only seen in 42% in initial BOS responders, suggesting steroid tolerance or resistance may develop. Another important observation was that peak eosinphil count decreased steroid dosing.
Finally, these data support the notion that initial responders are unlikely to gain response with continued therapy and may be better served with early transition to alternatives. Further research is needed to clarify these issues and which patients may be predisposed to nonresponse or loss of response.
Reena V. Chokshi, MD , is assistant professor of medicine in the department of gastroenterology at Baylor College of Medicine, Houston.
Treatment with budesonide oral suspension (BOS) was generally well tolerated and maintained a histologic response in some patients with eosinophilic esophagitis (EoE), according to the results of the 24-week, open-label extension phase of a multicenter, randomized, placebo-controlled, industry-sponsored trial.
Rates of histologic response (up to 6 eosinophils per high-power field) were “modest” – 23% among patients who stayed on BOS throughout the study and 48.5% among patients who initiated BOS after 12 weeks on placebo, reported Evan S. Dellon, MD, MPH, of the University of North Carolina in Chapel Hill and his associates. However, these rates “need to be viewed in the context of a highly symptomatic and histologically severe population with eosinophilic esophagitis,” they contended. A total of 11% of budesonide initiators developed esophageal candidiasis, they reported in Clinical Gastroenterology and Hepatology.
Budesonide oral suspension is a mucoadherent formulation of topical corticosteroid that has recently been developed to treat EoE. Previously, during the randomized, double-blind component of this phase 2 trial, 93 patients aged 11-40 years with active EoE and dysphagia received either BOS (2 mg) or placebo twice daily (Gastroenterology. 2017 Mar;157[4]:776-86). After 12 weeks, rates of histologic response were 39% for BOS versus 3% for placebo, and BOS significantly improved patients’ mean peak eosinophil count and scores on the Dysphagia Symptom Questionnaire, compared with baseline and compared with the response in the placebo group. During the open-label extension phase, 45 BOS continuers and 37 BOS initiators received 2 mg once daily for 12 weeks and then had the option to increase the BOS dose to 1.5-2.0 mg twice daily.
The rate of drug-related adverse events was 19% among BOS initiators and 4% among BOS continuers. One patient in each group developed oral candidiasis, while four BOS initiators (11%) developed esophageal candidiasis. Three BOS continuers had subnormal morning cortisol levels; while these were subclinical cases, they merit attention since long-term corticosteroids for EoE have been linked with possible hypothalamic–pituitary–adrenal axis suppression, the researchers noted.
In addition, while BOS initiators tended to maintain their endoscopic response, only 42% of those with an initial histologic response maintained a histologic response after 36 weeks of treatment or when leaving the study. Post hoc analyses confirmed that prolonged BOS treatment does not increase the chances of histologic or endoscopic response. Prior studies have suggested that EoE can become steroid-refractory over time and that certain molecular and histologic markers might predict resistance, the investigators noted.
Meritage Pharma (now part of Shire) was involved in the study design and conduct, data collection and management, and manuscript review. Dr. Dellon disclosed research funding from Meritage and Shire and a consulting relationship with Shire, along with ties to several other pharmaceutical companies. All six coinvestigators also disclosed ties to Meritage, Shire, or both, and two are Shire employees and stockholders.
*This story was updated on Feb. 7, 2019.
SOURCE: Dellon ES et al. Clin Gastroenterol Hepatol. 2018 Jun 11. doi: 10.1016/j.cgh.2018.05.051.
Treatment with budesonide oral suspension (BOS) was generally well tolerated and maintained a histologic response in some patients with eosinophilic esophagitis (EoE), according to the results of the 24-week, open-label extension phase of a multicenter, randomized, placebo-controlled, industry-sponsored trial.
Rates of histologic response (up to 6 eosinophils per high-power field) were “modest” – 23% among patients who stayed on BOS throughout the study and 48.5% among patients who initiated BOS after 12 weeks on placebo, reported Evan S. Dellon, MD, MPH, of the University of North Carolina in Chapel Hill and his associates. However, these rates “need to be viewed in the context of a highly symptomatic and histologically severe population with eosinophilic esophagitis,” they contended. A total of 11% of budesonide initiators developed esophageal candidiasis, they reported in Clinical Gastroenterology and Hepatology.
Budesonide oral suspension is a mucoadherent formulation of topical corticosteroid that has recently been developed to treat EoE. Previously, during the randomized, double-blind component of this phase 2 trial, 93 patients aged 11-40 years with active EoE and dysphagia received either BOS (2 mg) or placebo twice daily (Gastroenterology. 2017 Mar;157[4]:776-86). After 12 weeks, rates of histologic response were 39% for BOS versus 3% for placebo, and BOS significantly improved patients’ mean peak eosinophil count and scores on the Dysphagia Symptom Questionnaire, compared with baseline and compared with the response in the placebo group. During the open-label extension phase, 45 BOS continuers and 37 BOS initiators received 2 mg once daily for 12 weeks and then had the option to increase the BOS dose to 1.5-2.0 mg twice daily.
The rate of drug-related adverse events was 19% among BOS initiators and 4% among BOS continuers. One patient in each group developed oral candidiasis, while four BOS initiators (11%) developed esophageal candidiasis. Three BOS continuers had subnormal morning cortisol levels; while these were subclinical cases, they merit attention since long-term corticosteroids for EoE have been linked with possible hypothalamic–pituitary–adrenal axis suppression, the researchers noted.
In addition, while BOS initiators tended to maintain their endoscopic response, only 42% of those with an initial histologic response maintained a histologic response after 36 weeks of treatment or when leaving the study. Post hoc analyses confirmed that prolonged BOS treatment does not increase the chances of histologic or endoscopic response. Prior studies have suggested that EoE can become steroid-refractory over time and that certain molecular and histologic markers might predict resistance, the investigators noted.
Meritage Pharma (now part of Shire) was involved in the study design and conduct, data collection and management, and manuscript review. Dr. Dellon disclosed research funding from Meritage and Shire and a consulting relationship with Shire, along with ties to several other pharmaceutical companies. All six coinvestigators also disclosed ties to Meritage, Shire, or both, and two are Shire employees and stockholders.
*This story was updated on Feb. 7, 2019.
SOURCE: Dellon ES et al. Clin Gastroenterol Hepatol. 2018 Jun 11. doi: 10.1016/j.cgh.2018.05.051.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Budesonide oral suspension was well tolerated and maintained a histologic response in some patients with eosinophilic esophagitis.
Major finding: A total of 42% of initial histologic responders maintained a histologic response (less than 6 eosinophils per high-power field) after 24 weeks. Treatment was generally well tolerated, but 11% of initiators developed esophageal candidiasis.
Study details: Open-label extension study of a 12-week, multicenter, randomized, double-blind, placebo-controlled trial.
Disclosures: Meritage Pharma (now part of Shire) was involved in the study design and conduct, data collection and management, and manuscript review. Dr. Dellon disclosed research funding from Meritage and Shire and a consulting relationship with Shire, along with ties to several other pharmaceutical companies. All six coinvestigators also disclosed ties to Meritage, Shire, or both, and two are Shire employees and stockholders.
Source: Dellon ES et al. Clin Gastroenterol Hepatol. 2018 Jun 11. https://doi.org/10.1016/j.cgh.2018.05.051
Study supports swallowed topical steroids as maintenance for eosinophilic esophagitis
For adults with eosinophilic esophagitis, maintenance treatment with swallowed topical steroids was associated with significantly higher remission rates when compared with “steroid holidays” in a single-center retrospective observational study presented in the February issue of Clinical Gastroenterology and Hepatology.
At a median follow-up time of 5 years, the rate of complete (including clinical, endoscopic, and histologic) remission was 16.1% when patients were receiving swallowed topical steroids but only 1.3% when they were not on these or other maintenance therapies (that is, on “drug holidays”), reported Thomas Greuter, MD, of University Hospital Zürich and the Mayo Clinic in Rochester, Minn., and his associates. Swallowed topical steroids also were associated with significantly higher rates of each individual endpoint (P less than .001). Swallowed topical steroid therapy did not appear to cause dysplasia or mucosal atrophy, although esophageal candidiasis was confirmed in 2.7% of visits when patients were on treatment. “Given the good safety profile of low-dose swallowed topical steroid therapy, we advocate for prolonged treatment. Dose-finding trials are needed to achieve higher remission rates,” the investigators wrote in Clinical Gastroenterology and Hepatology.
Several studies have confirmed the efficacy of short-term swallowed topical steroids for treating eosinophilic esophagitis, but only one small randomized trial has evaluated longer-term treatment, and participants were followed for only 1 year. Dr. Greuter and his associates therefore analyzed retrospective data from 229 adults in Switzerland who received swallowed topical steroids for eosinophilic esophagitis between 2000 and 2014. Induction therapy consisted of 1 mg swallowed topical steroids twice daily, allowing 2-4 weeks for a clinical response. Patients then received infinite maintenance therapy with 0.25 mg swallowed topical steroids twice daily. Patients tended to be male and diagnosed in their late 30s. Endoscopy commonly showed corrugated rings, white exudates, edema, and furrows, and 35% of patients had strictures. Peak eosinophil count typically was 25 cells per high-power frame.
Among 819 follow-up visits, 336 (41%) occurred when patients were on maintenance swallowed topical steroid therapy. The median duration of maintenance therapy prior to a follow-up visit was 347 days (interquartile range, 90-750 days) or 677 doses (IQR, 280-1413 doses). The rate of clinical remission was 31% when patients were on maintenance treatment but only 4.5% when they were not (P less than .001). Respective rates of endoscopic and histologic remission were 48.8% versus 17.8% (P less than .001) and 44.8% versus 10.1% (P less than .001). After accounting for numerous demographic and clinical variables, the only significant predictors of clinical remission were treatment with swallowed topical steroids (odds ratio, 16.98; 95% confidence interval, 6.69-43.09) and a negative family history of esophageal eosinophilia (OR, 4.02; 95% CI, 1.41-11.47).
This study excluded patients whose eosinophilic esophagitis had responded to proton pump inhibitor therapy. Also, the maintenance dose of swallowed topical steroid dose (0.25 mg twice daily) probably was too low to achieve efficacious drug levels in the esophageal mucosa, which could explain the high proportion of treatment-refractory cases, according to the researchers. Evaluating a higher maintenance dose “would be of particular interest in the future,” they added.
The Swiss National Science Foundation provided partial funding. Dr. Greuter disclosed a travel grant from Falk Pharma GmbH and Vifor and an unrestricted research grant from Novartis.
SOURCE: Greuter T et al. Clin Gastroenterol Hepatol. 2018 Jun 11.
For adults with eosinophilic esophagitis, maintenance treatment with swallowed topical steroids was associated with significantly higher remission rates when compared with “steroid holidays” in a single-center retrospective observational study presented in the February issue of Clinical Gastroenterology and Hepatology.
At a median follow-up time of 5 years, the rate of complete (including clinical, endoscopic, and histologic) remission was 16.1% when patients were receiving swallowed topical steroids but only 1.3% when they were not on these or other maintenance therapies (that is, on “drug holidays”), reported Thomas Greuter, MD, of University Hospital Zürich and the Mayo Clinic in Rochester, Minn., and his associates. Swallowed topical steroids also were associated with significantly higher rates of each individual endpoint (P less than .001). Swallowed topical steroid therapy did not appear to cause dysplasia or mucosal atrophy, although esophageal candidiasis was confirmed in 2.7% of visits when patients were on treatment. “Given the good safety profile of low-dose swallowed topical steroid therapy, we advocate for prolonged treatment. Dose-finding trials are needed to achieve higher remission rates,” the investigators wrote in Clinical Gastroenterology and Hepatology.
Several studies have confirmed the efficacy of short-term swallowed topical steroids for treating eosinophilic esophagitis, but only one small randomized trial has evaluated longer-term treatment, and participants were followed for only 1 year. Dr. Greuter and his associates therefore analyzed retrospective data from 229 adults in Switzerland who received swallowed topical steroids for eosinophilic esophagitis between 2000 and 2014. Induction therapy consisted of 1 mg swallowed topical steroids twice daily, allowing 2-4 weeks for a clinical response. Patients then received infinite maintenance therapy with 0.25 mg swallowed topical steroids twice daily. Patients tended to be male and diagnosed in their late 30s. Endoscopy commonly showed corrugated rings, white exudates, edema, and furrows, and 35% of patients had strictures. Peak eosinophil count typically was 25 cells per high-power frame.
Among 819 follow-up visits, 336 (41%) occurred when patients were on maintenance swallowed topical steroid therapy. The median duration of maintenance therapy prior to a follow-up visit was 347 days (interquartile range, 90-750 days) or 677 doses (IQR, 280-1413 doses). The rate of clinical remission was 31% when patients were on maintenance treatment but only 4.5% when they were not (P less than .001). Respective rates of endoscopic and histologic remission were 48.8% versus 17.8% (P less than .001) and 44.8% versus 10.1% (P less than .001). After accounting for numerous demographic and clinical variables, the only significant predictors of clinical remission were treatment with swallowed topical steroids (odds ratio, 16.98; 95% confidence interval, 6.69-43.09) and a negative family history of esophageal eosinophilia (OR, 4.02; 95% CI, 1.41-11.47).
This study excluded patients whose eosinophilic esophagitis had responded to proton pump inhibitor therapy. Also, the maintenance dose of swallowed topical steroid dose (0.25 mg twice daily) probably was too low to achieve efficacious drug levels in the esophageal mucosa, which could explain the high proportion of treatment-refractory cases, according to the researchers. Evaluating a higher maintenance dose “would be of particular interest in the future,” they added.
The Swiss National Science Foundation provided partial funding. Dr. Greuter disclosed a travel grant from Falk Pharma GmbH and Vifor and an unrestricted research grant from Novartis.
SOURCE: Greuter T et al. Clin Gastroenterol Hepatol. 2018 Jun 11.
For adults with eosinophilic esophagitis, maintenance treatment with swallowed topical steroids was associated with significantly higher remission rates when compared with “steroid holidays” in a single-center retrospective observational study presented in the February issue of Clinical Gastroenterology and Hepatology.
At a median follow-up time of 5 years, the rate of complete (including clinical, endoscopic, and histologic) remission was 16.1% when patients were receiving swallowed topical steroids but only 1.3% when they were not on these or other maintenance therapies (that is, on “drug holidays”), reported Thomas Greuter, MD, of University Hospital Zürich and the Mayo Clinic in Rochester, Minn., and his associates. Swallowed topical steroids also were associated with significantly higher rates of each individual endpoint (P less than .001). Swallowed topical steroid therapy did not appear to cause dysplasia or mucosal atrophy, although esophageal candidiasis was confirmed in 2.7% of visits when patients were on treatment. “Given the good safety profile of low-dose swallowed topical steroid therapy, we advocate for prolonged treatment. Dose-finding trials are needed to achieve higher remission rates,” the investigators wrote in Clinical Gastroenterology and Hepatology.
Several studies have confirmed the efficacy of short-term swallowed topical steroids for treating eosinophilic esophagitis, but only one small randomized trial has evaluated longer-term treatment, and participants were followed for only 1 year. Dr. Greuter and his associates therefore analyzed retrospective data from 229 adults in Switzerland who received swallowed topical steroids for eosinophilic esophagitis between 2000 and 2014. Induction therapy consisted of 1 mg swallowed topical steroids twice daily, allowing 2-4 weeks for a clinical response. Patients then received infinite maintenance therapy with 0.25 mg swallowed topical steroids twice daily. Patients tended to be male and diagnosed in their late 30s. Endoscopy commonly showed corrugated rings, white exudates, edema, and furrows, and 35% of patients had strictures. Peak eosinophil count typically was 25 cells per high-power frame.
Among 819 follow-up visits, 336 (41%) occurred when patients were on maintenance swallowed topical steroid therapy. The median duration of maintenance therapy prior to a follow-up visit was 347 days (interquartile range, 90-750 days) or 677 doses (IQR, 280-1413 doses). The rate of clinical remission was 31% when patients were on maintenance treatment but only 4.5% when they were not (P less than .001). Respective rates of endoscopic and histologic remission were 48.8% versus 17.8% (P less than .001) and 44.8% versus 10.1% (P less than .001). After accounting for numerous demographic and clinical variables, the only significant predictors of clinical remission were treatment with swallowed topical steroids (odds ratio, 16.98; 95% confidence interval, 6.69-43.09) and a negative family history of esophageal eosinophilia (OR, 4.02; 95% CI, 1.41-11.47).
This study excluded patients whose eosinophilic esophagitis had responded to proton pump inhibitor therapy. Also, the maintenance dose of swallowed topical steroid dose (0.25 mg twice daily) probably was too low to achieve efficacious drug levels in the esophageal mucosa, which could explain the high proportion of treatment-refractory cases, according to the researchers. Evaluating a higher maintenance dose “would be of particular interest in the future,” they added.
The Swiss National Science Foundation provided partial funding. Dr. Greuter disclosed a travel grant from Falk Pharma GmbH and Vifor and an unrestricted research grant from Novartis.
SOURCE: Greuter T et al. Clin Gastroenterol Hepatol. 2018 Jun 11.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Swallowed topical steroids appear to increase remission rates among adults with eosinophilic esophagitis.
Major finding: After a median of 5 years of follow-up, rates of clinical remission were 16.1% and 1.3%, respectively (P less than .001).
Study details: Retrospective cohort study of 229 adults with eosinophilic esophagitis.
Disclosures: The Swiss National Science Foundation provided partial funding. Dr. Greuter disclosed a travel grant from Falk Pharma GmbH and Vifor and an unrestricted research grant from Novartis.
Source: Greuter T et al. Clin Gastroenterol Hepatol. 2018 Jun 11.
No difference between PPI prophylaxis, placebo for GI bleeding
There was no significant difference in mortality between critically ill patients who received pantoprazole prophylaxis for gastrointestinal bleeding, and those who received placebo, new findings suggest.
In a multicenter, randomized trial of 3,298 adult patients at risk for gastrointestinal bleeding, 510 patients (31.1%) in the pantoprazole group and 499 (30.4%) in the placebo group had died at 90 days (relative risk, 1.02; 95% confidence interval, 0.91-1.13; P = .76). The results were published in the New England Journal of Medicine.
Patients were aged 18 years or older; had been admitted to the ICU for an acute condition in one of six international centers; and had at least one risk factor for gastrointestinal bleeding including shock, use of anticoagulant agents, renal replacement therapy, mechanical ventilation (expected to last more than 24 hours), any history of liver disease, or any history of or ongoing coagulopathy. A total of 1,645 patients were randomly assigned to receive 40 mg of intravenous pantoprazole once daily and 1,653 received placebo, reported Mette Krag, MD, of the department of intensive care at Rigshospitalet in Copenhagen, and her coauthors.
The primary outcome was 90-day mortality. Secondary outcomes were clinically important events in the ICU, clinically important gastrointestinal bleeding in the ICU, infectious adverse events in the ICU, and days alive without the use of life support within the 90-day period.
One or more clinically important events occurred in 21.9% of patients in the pantoprazole group and in 22.6% in the placebo group (RR, 0.96; 95% CI, 0.83-1.11). In the pantoprazole group, 2.5% of patients had clinically important gastrointestinal bleeding, compared with 4.2% in the placebo group, Dr. Krag and her coauthors wrote.
The findings are similar to other recently published results, which showed “no significant differences ... in the rates of death or infectious complications between patients receiving placebo or no prophylaxis and those receiving proton pump inhibitors,” the authors wrote.
Dr. Krag reported financial support from Innovation Fund Denmark, Ehrenreich’s Foundation, and several other organizations.
SOURCE: Krag M et al. N Engl J Med. 2018 Dec 6. doi: 10.1056/NEJMoa1714919.
This article was updated 12/6/18.
“The take-home message from this trial is that, given the low incidence of clinically important upper gastrointestinal bleeding in the ICU, prophylaxis with a PPI [proton pump inhibitor], if initiated, should be reserved for seriously ill patients who are at high risk for this complication,” wrote Alan Barkun, MD, CM, of McGill University, Montreal, and Marc Bardou, MD, PhD, of the Centre Hospitalier Universitaire Dijon–Bourgogne (France), in an editorial published with the study.
Though 90-day mortality was similar between groups in this trial, “the between-group difference in the rate of important upper gastrointestinal bleeding may still support the recommendation of using a prophylactic PPI” given the absence of a difference in the rate of adverse events between the two groups, they added.
Dr. Barkun reported no disclosures; Dr. Bardou reported support from the French Medicines Agency.
“The take-home message from this trial is that, given the low incidence of clinically important upper gastrointestinal bleeding in the ICU, prophylaxis with a PPI [proton pump inhibitor], if initiated, should be reserved for seriously ill patients who are at high risk for this complication,” wrote Alan Barkun, MD, CM, of McGill University, Montreal, and Marc Bardou, MD, PhD, of the Centre Hospitalier Universitaire Dijon–Bourgogne (France), in an editorial published with the study.
Though 90-day mortality was similar between groups in this trial, “the between-group difference in the rate of important upper gastrointestinal bleeding may still support the recommendation of using a prophylactic PPI” given the absence of a difference in the rate of adverse events between the two groups, they added.
Dr. Barkun reported no disclosures; Dr. Bardou reported support from the French Medicines Agency.
“The take-home message from this trial is that, given the low incidence of clinically important upper gastrointestinal bleeding in the ICU, prophylaxis with a PPI [proton pump inhibitor], if initiated, should be reserved for seriously ill patients who are at high risk for this complication,” wrote Alan Barkun, MD, CM, of McGill University, Montreal, and Marc Bardou, MD, PhD, of the Centre Hospitalier Universitaire Dijon–Bourgogne (France), in an editorial published with the study.
Though 90-day mortality was similar between groups in this trial, “the between-group difference in the rate of important upper gastrointestinal bleeding may still support the recommendation of using a prophylactic PPI” given the absence of a difference in the rate of adverse events between the two groups, they added.
Dr. Barkun reported no disclosures; Dr. Bardou reported support from the French Medicines Agency.
There was no significant difference in mortality between critically ill patients who received pantoprazole prophylaxis for gastrointestinal bleeding, and those who received placebo, new findings suggest.
In a multicenter, randomized trial of 3,298 adult patients at risk for gastrointestinal bleeding, 510 patients (31.1%) in the pantoprazole group and 499 (30.4%) in the placebo group had died at 90 days (relative risk, 1.02; 95% confidence interval, 0.91-1.13; P = .76). The results were published in the New England Journal of Medicine.
Patients were aged 18 years or older; had been admitted to the ICU for an acute condition in one of six international centers; and had at least one risk factor for gastrointestinal bleeding including shock, use of anticoagulant agents, renal replacement therapy, mechanical ventilation (expected to last more than 24 hours), any history of liver disease, or any history of or ongoing coagulopathy. A total of 1,645 patients were randomly assigned to receive 40 mg of intravenous pantoprazole once daily and 1,653 received placebo, reported Mette Krag, MD, of the department of intensive care at Rigshospitalet in Copenhagen, and her coauthors.
The primary outcome was 90-day mortality. Secondary outcomes were clinically important events in the ICU, clinically important gastrointestinal bleeding in the ICU, infectious adverse events in the ICU, and days alive without the use of life support within the 90-day period.
One or more clinically important events occurred in 21.9% of patients in the pantoprazole group and in 22.6% in the placebo group (RR, 0.96; 95% CI, 0.83-1.11). In the pantoprazole group, 2.5% of patients had clinically important gastrointestinal bleeding, compared with 4.2% in the placebo group, Dr. Krag and her coauthors wrote.
The findings are similar to other recently published results, which showed “no significant differences ... in the rates of death or infectious complications between patients receiving placebo or no prophylaxis and those receiving proton pump inhibitors,” the authors wrote.
Dr. Krag reported financial support from Innovation Fund Denmark, Ehrenreich’s Foundation, and several other organizations.
SOURCE: Krag M et al. N Engl J Med. 2018 Dec 6. doi: 10.1056/NEJMoa1714919.
This article was updated 12/6/18.
There was no significant difference in mortality between critically ill patients who received pantoprazole prophylaxis for gastrointestinal bleeding, and those who received placebo, new findings suggest.
In a multicenter, randomized trial of 3,298 adult patients at risk for gastrointestinal bleeding, 510 patients (31.1%) in the pantoprazole group and 499 (30.4%) in the placebo group had died at 90 days (relative risk, 1.02; 95% confidence interval, 0.91-1.13; P = .76). The results were published in the New England Journal of Medicine.
Patients were aged 18 years or older; had been admitted to the ICU for an acute condition in one of six international centers; and had at least one risk factor for gastrointestinal bleeding including shock, use of anticoagulant agents, renal replacement therapy, mechanical ventilation (expected to last more than 24 hours), any history of liver disease, or any history of or ongoing coagulopathy. A total of 1,645 patients were randomly assigned to receive 40 mg of intravenous pantoprazole once daily and 1,653 received placebo, reported Mette Krag, MD, of the department of intensive care at Rigshospitalet in Copenhagen, and her coauthors.
The primary outcome was 90-day mortality. Secondary outcomes were clinically important events in the ICU, clinically important gastrointestinal bleeding in the ICU, infectious adverse events in the ICU, and days alive without the use of life support within the 90-day period.
One or more clinically important events occurred in 21.9% of patients in the pantoprazole group and in 22.6% in the placebo group (RR, 0.96; 95% CI, 0.83-1.11). In the pantoprazole group, 2.5% of patients had clinically important gastrointestinal bleeding, compared with 4.2% in the placebo group, Dr. Krag and her coauthors wrote.
The findings are similar to other recently published results, which showed “no significant differences ... in the rates of death or infectious complications between patients receiving placebo or no prophylaxis and those receiving proton pump inhibitors,” the authors wrote.
Dr. Krag reported financial support from Innovation Fund Denmark, Ehrenreich’s Foundation, and several other organizations.
SOURCE: Krag M et al. N Engl J Med. 2018 Dec 6. doi: 10.1056/NEJMoa1714919.
This article was updated 12/6/18.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: There was no significant difference in mortality between patients who received pantoprazole prophylaxis for gastrointestinal bleeding, and those who received placebo.
Major finding: Just over 31% of patients in the pantoprazole group and 30.4% in the placebo group had died at 90 days (relative risk, 1.02; 95% confidence interval, 0.91-1.13; P = .76).
Study details: A multicenter, randomized trial of 3,298 adult ICU patients at risk for gastrointestinal bleeding.
Disclosures: Dr. Krag reported financial support from Innovation Fund Denmark, Ehrenreich’s Foundation, and several other organizations.
Source: Krag M et al. N Engl J Med. 2018 Dec 6. doi: 10.1056/NEJMoa1714919.
Anticoagulant choice, PPI cotherapy impact risk of upper GI bleeding
Patients receiving oral anticoagulant treatment had the lowest risk of gastrointestinal bleeding when taking apixaban, compared with rivaroxaban, dabigatran, and warfarin, according to a recent study.
Further, patients who received proton pump inhibitor (PPI) cotherapy had a lower overall risk of gastrointestinal bleeding, according to Wayne A. Ray, PhD, from the department of health policy at Vanderbilt University, Nashville, Tenn., and his colleagues.
“These findings indicate the potential benefits of a gastrointestinal bleeding risk assessment before initiating anticoagulant treatment,” Dr. Ray and his colleagues wrote in their study, which was published in JAMA.
Dr. Ray and his colleagues performed a retrospective, population-based study of 1,643,123 Medicare beneficiaries (mean age, 76.4 years) who received 1,713,183 new episodes of oral anticoagulant treatment between January 2011 and September 2015. They analyzed how patients reacted to apixaban, dabigatran, rivaroxaban, or warfarin both with and without PPI cotherapy.
Overall, the risk of gastrointestinal bleeding across 754,389 person-years without PPI therapy was 115 per 10,000 person-years (95% confidence interval, 112-118) in 7,119 patients. The researchers found the risk of gastrointestinal bleeding was highest in patients taking rivaroxaban (1,278 patients; 144 per 10,000 person-years; 95% CI, 136-152) and lowest when taking apixaban (279 patients; 120 per 10,000 person-years; incidence rate ratio, 1,97; 95% CI, 1.73-2.25), compared with dabigatran (629 patients; 120 per 10,000 person-years; IRR, 1.19; 95% CI, 1.08-1.32) and warfarin (4,933 patients; 113 per 10,000 person-years; IRR, 1.27; 95% CI, 1.19-1.35). There was a significantly lower incidence of gastrointestinal bleeding for apixaban, compared with warfarin (IRR, 0.64; 95% CI, 0.57-0.73) and dabigatran (IRR, 0.61; 95% CI, 0.52-0.70).
There was a lower overall incidence of gastrointestinal bleeding when receiving PPI cotherapy (264,447 person-years; 76 per 10,000 person-years), compared with patients who received anticoagulant treatment without PPI cotherapy (IRR, 0.66; 95% CI, 0.62-0.69). This reduced incidence of gastrointestinal bleeding was also seen in patients receiving PPI cotherapy and taking apixaban (IRR, 0.66; 95% CI, 0.52-0.85), dabigatran (IRR, 0.49; 95% CI, 0.41-0.59), rivaroxaban (IRR, 0.75; 95% CI, 0.68-0.84), and warfarin (IRR, 0.65; 95% CI, 0.62-0.69).
The researchers noted that limitations in this study included potential misclassification of anticoagulant treatment, PPI cotherapy, and NSAIDs because of a reliance on filled prescription data; confounding by unmeasured factors such as aspirin exposure or Helicobacter pylori infection; and gastrointestinal bleeding being measured using a disease risk score.
This study was supported by a grant from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
SOURCE: Ray WA et al. JAMA. 2018 Dec 4. doi: 10.1001/jama.2018.17242.
Patients receiving oral anticoagulant treatment had the lowest risk of gastrointestinal bleeding when taking apixaban, compared with rivaroxaban, dabigatran, and warfarin, according to a recent study.
Further, patients who received proton pump inhibitor (PPI) cotherapy had a lower overall risk of gastrointestinal bleeding, according to Wayne A. Ray, PhD, from the department of health policy at Vanderbilt University, Nashville, Tenn., and his colleagues.
“These findings indicate the potential benefits of a gastrointestinal bleeding risk assessment before initiating anticoagulant treatment,” Dr. Ray and his colleagues wrote in their study, which was published in JAMA.
Dr. Ray and his colleagues performed a retrospective, population-based study of 1,643,123 Medicare beneficiaries (mean age, 76.4 years) who received 1,713,183 new episodes of oral anticoagulant treatment between January 2011 and September 2015. They analyzed how patients reacted to apixaban, dabigatran, rivaroxaban, or warfarin both with and without PPI cotherapy.
Overall, the risk of gastrointestinal bleeding across 754,389 person-years without PPI therapy was 115 per 10,000 person-years (95% confidence interval, 112-118) in 7,119 patients. The researchers found the risk of gastrointestinal bleeding was highest in patients taking rivaroxaban (1,278 patients; 144 per 10,000 person-years; 95% CI, 136-152) and lowest when taking apixaban (279 patients; 120 per 10,000 person-years; incidence rate ratio, 1,97; 95% CI, 1.73-2.25), compared with dabigatran (629 patients; 120 per 10,000 person-years; IRR, 1.19; 95% CI, 1.08-1.32) and warfarin (4,933 patients; 113 per 10,000 person-years; IRR, 1.27; 95% CI, 1.19-1.35). There was a significantly lower incidence of gastrointestinal bleeding for apixaban, compared with warfarin (IRR, 0.64; 95% CI, 0.57-0.73) and dabigatran (IRR, 0.61; 95% CI, 0.52-0.70).
There was a lower overall incidence of gastrointestinal bleeding when receiving PPI cotherapy (264,447 person-years; 76 per 10,000 person-years), compared with patients who received anticoagulant treatment without PPI cotherapy (IRR, 0.66; 95% CI, 0.62-0.69). This reduced incidence of gastrointestinal bleeding was also seen in patients receiving PPI cotherapy and taking apixaban (IRR, 0.66; 95% CI, 0.52-0.85), dabigatran (IRR, 0.49; 95% CI, 0.41-0.59), rivaroxaban (IRR, 0.75; 95% CI, 0.68-0.84), and warfarin (IRR, 0.65; 95% CI, 0.62-0.69).
The researchers noted that limitations in this study included potential misclassification of anticoagulant treatment, PPI cotherapy, and NSAIDs because of a reliance on filled prescription data; confounding by unmeasured factors such as aspirin exposure or Helicobacter pylori infection; and gastrointestinal bleeding being measured using a disease risk score.
This study was supported by a grant from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
SOURCE: Ray WA et al. JAMA. 2018 Dec 4. doi: 10.1001/jama.2018.17242.
Patients receiving oral anticoagulant treatment had the lowest risk of gastrointestinal bleeding when taking apixaban, compared with rivaroxaban, dabigatran, and warfarin, according to a recent study.
Further, patients who received proton pump inhibitor (PPI) cotherapy had a lower overall risk of gastrointestinal bleeding, according to Wayne A. Ray, PhD, from the department of health policy at Vanderbilt University, Nashville, Tenn., and his colleagues.
“These findings indicate the potential benefits of a gastrointestinal bleeding risk assessment before initiating anticoagulant treatment,” Dr. Ray and his colleagues wrote in their study, which was published in JAMA.
Dr. Ray and his colleagues performed a retrospective, population-based study of 1,643,123 Medicare beneficiaries (mean age, 76.4 years) who received 1,713,183 new episodes of oral anticoagulant treatment between January 2011 and September 2015. They analyzed how patients reacted to apixaban, dabigatran, rivaroxaban, or warfarin both with and without PPI cotherapy.
Overall, the risk of gastrointestinal bleeding across 754,389 person-years without PPI therapy was 115 per 10,000 person-years (95% confidence interval, 112-118) in 7,119 patients. The researchers found the risk of gastrointestinal bleeding was highest in patients taking rivaroxaban (1,278 patients; 144 per 10,000 person-years; 95% CI, 136-152) and lowest when taking apixaban (279 patients; 120 per 10,000 person-years; incidence rate ratio, 1,97; 95% CI, 1.73-2.25), compared with dabigatran (629 patients; 120 per 10,000 person-years; IRR, 1.19; 95% CI, 1.08-1.32) and warfarin (4,933 patients; 113 per 10,000 person-years; IRR, 1.27; 95% CI, 1.19-1.35). There was a significantly lower incidence of gastrointestinal bleeding for apixaban, compared with warfarin (IRR, 0.64; 95% CI, 0.57-0.73) and dabigatran (IRR, 0.61; 95% CI, 0.52-0.70).
There was a lower overall incidence of gastrointestinal bleeding when receiving PPI cotherapy (264,447 person-years; 76 per 10,000 person-years), compared with patients who received anticoagulant treatment without PPI cotherapy (IRR, 0.66; 95% CI, 0.62-0.69). This reduced incidence of gastrointestinal bleeding was also seen in patients receiving PPI cotherapy and taking apixaban (IRR, 0.66; 95% CI, 0.52-0.85), dabigatran (IRR, 0.49; 95% CI, 0.41-0.59), rivaroxaban (IRR, 0.75; 95% CI, 0.68-0.84), and warfarin (IRR, 0.65; 95% CI, 0.62-0.69).
The researchers noted that limitations in this study included potential misclassification of anticoagulant treatment, PPI cotherapy, and NSAIDs because of a reliance on filled prescription data; confounding by unmeasured factors such as aspirin exposure or Helicobacter pylori infection; and gastrointestinal bleeding being measured using a disease risk score.
This study was supported by a grant from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
SOURCE: Ray WA et al. JAMA. 2018 Dec 4. doi: 10.1001/jama.2018.17242.
FROM JAMA
Key clinical point: In patients receiving oral anticoagulant treatment, risk of gastrointestinal bleeding was highest in patients taking rivaroxaban, lowest when taking apixaban, and there was a lower overall incidence of gastrointestinal bleeding when receiving proton pump inhibitor cotherapy.
Major finding: Per 10,000 person-years, the incidence rate of gastrointestinal bleeding was 144 for rivaroxaban, 73 for apixaban, 120 for dabigatran, and 113 for warfarin; there was a gastrointestinal bleeding incidence rate ratio of 0.66 for patients using protein pump inhibitor cotherapy.
Study details: A retrospective, population-based study of 1,643,123 Medicare beneficiaries who received oral anticoagulant treatment between January 2011 and September 2015.
Disclosures: This study was supported by a grant from the National Heart, Lung, and Blood Institute. The authors reported no relevant conflicts of interest.
Source: Ray WA et al. JAMA. 2018 Dec 4. doi: 10.1001/jama.2018.17242.
Surgical model to study reflux esophagitis after esophagojejunostomy
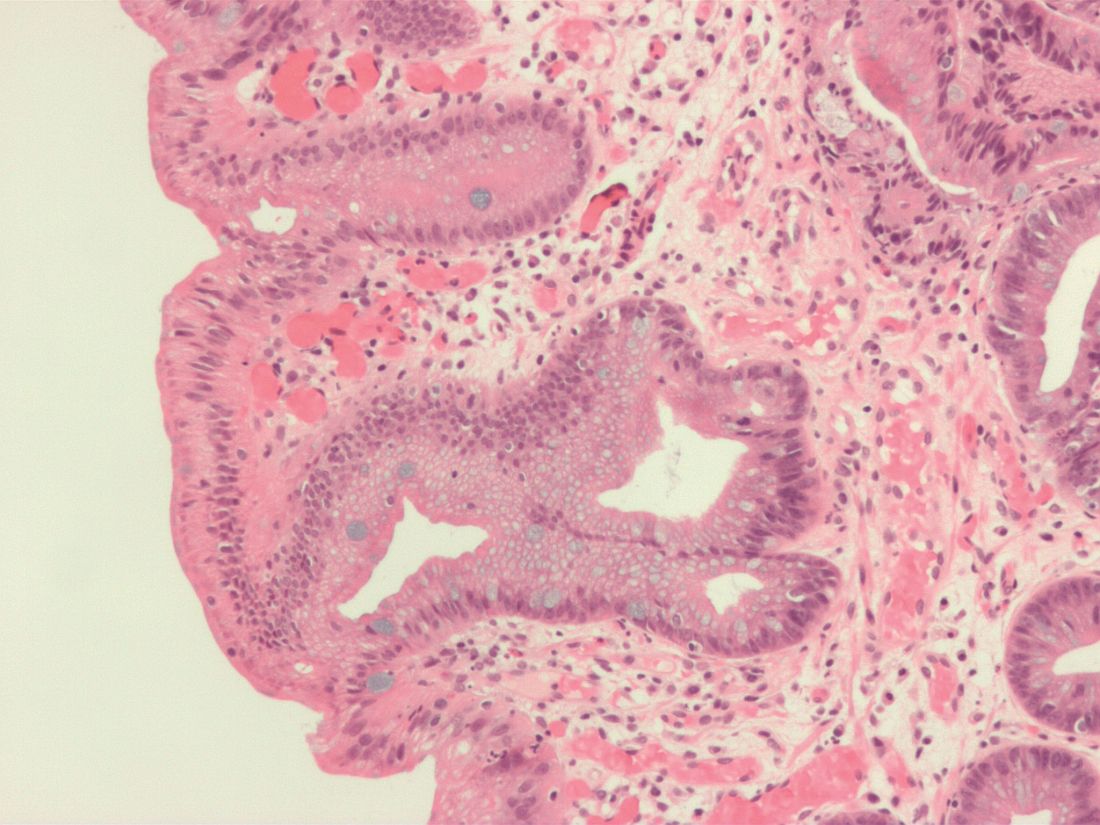
During a wound repair process in rats, metaplastic columnar-lined esophagus was produced and increased in length following esophagojejunostomy, which may be independent of stem cell reprogramming, according to results from an anastomosed rodent study.
The investigators studied esophageal and tissue sections of 52 rats at different time points after esophagojejunostomy and samples were analyzed for length, type, and location of columnar lining. In addition, the sections were examined immunophenotypically to elucidate the molecular changes that occur during ulceration. Agoston T. Agoston, MD, PhD, of Brigham and Women’s Hospital and the department of pathology at Harvard Medical School, Boston, and colleagues reported the findings in Cellular and Molecular Gastroenterology and Hepatology.
“This rodent columnar-lined esophagus has been proposed to develop from cellular reprogramming of progenitor cells, but studies on early columnar-lined esophagus development are lacking,” the researchers wrote.
In the model, ulceration was seen 2 weeks after surgery, which began distally at the esophagojejunal anastomosis. Representative of wound healing, reepithelialization of the ulcer region took place through formation of immature glands, which were found to bud directly from jejunal crypts.
After immunophenotypic analysis, the researchers reported that “immunohistochemical characterization of neoglandular epithelium located immediately proximal to the anastomosis showed features similar to those of the native nonproliferating jejunal epithelium located immediately distal to the anastomosis.” They further reported that “the columnar-lined esophagus’s immunoprofile was similar to jejunal crypt epithelium.”
Upon further examination of the ulcer segment, Dr. Agoston and colleagues found that columnar-lined esophagus elongated from 0.15 mm (standard error of the mean, ± 0.1) to 5.22 mm (SEM, ± 0.37) at 2 and 32 weeks post esophagojejunostomy, respectively.
“There was a highly significant linear relationship between the length of the neoglandular epithelium in the distal esophagus and the number of weeks after surgery (correlation coefficient, 0.94; P less than .0001),” the investigators stated.
Locational analysis revealed epithelial-mesenchymal transition markers being expressed by spindle-shaped cells at the leading edge of the columnar-lined esophagus. In addition, neoglands were identified within esophageal ulcer beds and actively dividing squamous epithelium was seen exclusively at the proximal ulcer border.
Following the systematic analysis, the authors noted that the columnar-lined esophagus was most likely the result of jejunal cell migration into the esophagus. They suggested that if compared, jejunal cells may competitively dominate squamous cells in the context of chronic gastroesophageal reflux disease. Furthermore, they observed that the region of ulceration following esophagojejunostomy in their model was more expansive than that reported in other comparable rodent models of reflux esophagitis.
“The reason for this difference is not clear, but we speculate that it is the result of technical aspects of our reflux-inducing surgery,” the researchers wrote. They further explained that “we intentionally fashioned a large anastomotic orifice between the esophagus and jejunum, perhaps larger than that fashioned by other investigators.” And they concluded, “we suspect that this larger orifice resulted in esophageal exposure to larger volumes of refluxate and, consequently, larger areas of ulceration.”
The authors acknowledged their results may not be fully applicable in the context of human Barrett’s esophagus, given the rodent model. However, they do believe the findings may provide a basis to help understand the wound repair process, particularly the distal edge of ulcers that border the columnar epithelium.
“Using a rat model of reflux esophagitis via surgical esophagojejunostomy, we have shown that a metaplastic, columnar-lined esophagus develops via a wound healing process, and not via genetic reprogramming of progenitor cells,” the researchers concluded.
The study was supported by grant funding from the National Institutes of Health and the Baylor Scott and White Research Institute. The authors reported no conflicts of interest.
SOURCE: Agoston AT et al. Cell Mol Gastroenterol Hepatol. 2018 Jun 26. doi: 10.1016/j.jcmgh.2018.06.007.
Agoston et al. reported that metaplastic columnar-lined esophagus develops in a wound-healing process on the distal edge of the ulcer, starting distally at the esophagojejunal anastomosis in the esophagojejunal anastomosed rat model. They also concluded that the columnar-lined esophagus was caused through migration of jejunal cells into the esophagus.
These new findings bring up a couple of issues. One is that metaplastic columnar-lined esophagus originates from jejunal crypt budding over the anastomosis. Some researchers may think this is not metaplasia, as there is no reprogramming of the stem cells. However, the definition of metaplasia is an endpoint such that a normal lineage is placed in an abnormal position, and it can be called metaplasia even it is from budding of jejunal crypt. This new finding is not denying metaplasia.
The second issue is whether these rodent models are really mimicking human metaplastic columnar-lined esophagus or not. In humans, metaplastic columnar-lined esophagus usually accompanies gastroesophageal reflux, but jejunum is not next to esophagus, and jejunal crypt budding is less likely. However, it is common to observe ulcerated lesions in the proximal front of long-segment Barrett’s esophagus in humans. In this process, the model of Agosto et al. is describing the human metaplastic columnar-lined esophagus elongation.
There would be more reprogramming happening in the body of animals under the effect of microenvironment. This is a kind of adaptation, and analyzing key factors for this reprogramming would be the path to clarifying carcinogenesis in the metaplastic field and also a way to advance regenerative medicine.
Sachiyo Nomura MD, PhD, AGAF, FACS, is an investigator in gastrointestinal carcinogenesis and epithelial biology, and a gastrointestinal surgeon, at University of Tokyo Hospital, department of stomach and esophageal surgery, as well as an associate professor, department of gastrointestinal surgery, graduate school of medicine, at the university. She has no conflicts.
Agoston et al. reported that metaplastic columnar-lined esophagus develops in a wound-healing process on the distal edge of the ulcer, starting distally at the esophagojejunal anastomosis in the esophagojejunal anastomosed rat model. They also concluded that the columnar-lined esophagus was caused through migration of jejunal cells into the esophagus.
These new findings bring up a couple of issues. One is that metaplastic columnar-lined esophagus originates from jejunal crypt budding over the anastomosis. Some researchers may think this is not metaplasia, as there is no reprogramming of the stem cells. However, the definition of metaplasia is an endpoint such that a normal lineage is placed in an abnormal position, and it can be called metaplasia even it is from budding of jejunal crypt. This new finding is not denying metaplasia.
The second issue is whether these rodent models are really mimicking human metaplastic columnar-lined esophagus or not. In humans, metaplastic columnar-lined esophagus usually accompanies gastroesophageal reflux, but jejunum is not next to esophagus, and jejunal crypt budding is less likely. However, it is common to observe ulcerated lesions in the proximal front of long-segment Barrett’s esophagus in humans. In this process, the model of Agosto et al. is describing the human metaplastic columnar-lined esophagus elongation.
There would be more reprogramming happening in the body of animals under the effect of microenvironment. This is a kind of adaptation, and analyzing key factors for this reprogramming would be the path to clarifying carcinogenesis in the metaplastic field and also a way to advance regenerative medicine.
Sachiyo Nomura MD, PhD, AGAF, FACS, is an investigator in gastrointestinal carcinogenesis and epithelial biology, and a gastrointestinal surgeon, at University of Tokyo Hospital, department of stomach and esophageal surgery, as well as an associate professor, department of gastrointestinal surgery, graduate school of medicine, at the university. She has no conflicts.
Agoston et al. reported that metaplastic columnar-lined esophagus develops in a wound-healing process on the distal edge of the ulcer, starting distally at the esophagojejunal anastomosis in the esophagojejunal anastomosed rat model. They also concluded that the columnar-lined esophagus was caused through migration of jejunal cells into the esophagus.
These new findings bring up a couple of issues. One is that metaplastic columnar-lined esophagus originates from jejunal crypt budding over the anastomosis. Some researchers may think this is not metaplasia, as there is no reprogramming of the stem cells. However, the definition of metaplasia is an endpoint such that a normal lineage is placed in an abnormal position, and it can be called metaplasia even it is from budding of jejunal crypt. This new finding is not denying metaplasia.
The second issue is whether these rodent models are really mimicking human metaplastic columnar-lined esophagus or not. In humans, metaplastic columnar-lined esophagus usually accompanies gastroesophageal reflux, but jejunum is not next to esophagus, and jejunal crypt budding is less likely. However, it is common to observe ulcerated lesions in the proximal front of long-segment Barrett’s esophagus in humans. In this process, the model of Agosto et al. is describing the human metaplastic columnar-lined esophagus elongation.
There would be more reprogramming happening in the body of animals under the effect of microenvironment. This is a kind of adaptation, and analyzing key factors for this reprogramming would be the path to clarifying carcinogenesis in the metaplastic field and also a way to advance regenerative medicine.
Sachiyo Nomura MD, PhD, AGAF, FACS, is an investigator in gastrointestinal carcinogenesis and epithelial biology, and a gastrointestinal surgeon, at University of Tokyo Hospital, department of stomach and esophageal surgery, as well as an associate professor, department of gastrointestinal surgery, graduate school of medicine, at the university. She has no conflicts.
During a wound repair process in rats, metaplastic columnar-lined esophagus was produced and increased in length following esophagojejunostomy, which may be independent of stem cell reprogramming, according to results from an anastomosed rodent study.
The investigators studied esophageal and tissue sections of 52 rats at different time points after esophagojejunostomy and samples were analyzed for length, type, and location of columnar lining. In addition, the sections were examined immunophenotypically to elucidate the molecular changes that occur during ulceration. Agoston T. Agoston, MD, PhD, of Brigham and Women’s Hospital and the department of pathology at Harvard Medical School, Boston, and colleagues reported the findings in Cellular and Molecular Gastroenterology and Hepatology.
“This rodent columnar-lined esophagus has been proposed to develop from cellular reprogramming of progenitor cells, but studies on early columnar-lined esophagus development are lacking,” the researchers wrote.
In the model, ulceration was seen 2 weeks after surgery, which began distally at the esophagojejunal anastomosis. Representative of wound healing, reepithelialization of the ulcer region took place through formation of immature glands, which were found to bud directly from jejunal crypts.
After immunophenotypic analysis, the researchers reported that “immunohistochemical characterization of neoglandular epithelium located immediately proximal to the anastomosis showed features similar to those of the native nonproliferating jejunal epithelium located immediately distal to the anastomosis.” They further reported that “the columnar-lined esophagus’s immunoprofile was similar to jejunal crypt epithelium.”
Upon further examination of the ulcer segment, Dr. Agoston and colleagues found that columnar-lined esophagus elongated from 0.15 mm (standard error of the mean, ± 0.1) to 5.22 mm (SEM, ± 0.37) at 2 and 32 weeks post esophagojejunostomy, respectively.
“There was a highly significant linear relationship between the length of the neoglandular epithelium in the distal esophagus and the number of weeks after surgery (correlation coefficient, 0.94; P less than .0001),” the investigators stated.
Locational analysis revealed epithelial-mesenchymal transition markers being expressed by spindle-shaped cells at the leading edge of the columnar-lined esophagus. In addition, neoglands were identified within esophageal ulcer beds and actively dividing squamous epithelium was seen exclusively at the proximal ulcer border.
Following the systematic analysis, the authors noted that the columnar-lined esophagus was most likely the result of jejunal cell migration into the esophagus. They suggested that if compared, jejunal cells may competitively dominate squamous cells in the context of chronic gastroesophageal reflux disease. Furthermore, they observed that the region of ulceration following esophagojejunostomy in their model was more expansive than that reported in other comparable rodent models of reflux esophagitis.
“The reason for this difference is not clear, but we speculate that it is the result of technical aspects of our reflux-inducing surgery,” the researchers wrote. They further explained that “we intentionally fashioned a large anastomotic orifice between the esophagus and jejunum, perhaps larger than that fashioned by other investigators.” And they concluded, “we suspect that this larger orifice resulted in esophageal exposure to larger volumes of refluxate and, consequently, larger areas of ulceration.”
The authors acknowledged their results may not be fully applicable in the context of human Barrett’s esophagus, given the rodent model. However, they do believe the findings may provide a basis to help understand the wound repair process, particularly the distal edge of ulcers that border the columnar epithelium.
“Using a rat model of reflux esophagitis via surgical esophagojejunostomy, we have shown that a metaplastic, columnar-lined esophagus develops via a wound healing process, and not via genetic reprogramming of progenitor cells,” the researchers concluded.
The study was supported by grant funding from the National Institutes of Health and the Baylor Scott and White Research Institute. The authors reported no conflicts of interest.
SOURCE: Agoston AT et al. Cell Mol Gastroenterol Hepatol. 2018 Jun 26. doi: 10.1016/j.jcmgh.2018.06.007.
During a wound repair process in rats, metaplastic columnar-lined esophagus was produced and increased in length following esophagojejunostomy, which may be independent of stem cell reprogramming, according to results from an anastomosed rodent study.
The investigators studied esophageal and tissue sections of 52 rats at different time points after esophagojejunostomy and samples were analyzed for length, type, and location of columnar lining. In addition, the sections were examined immunophenotypically to elucidate the molecular changes that occur during ulceration. Agoston T. Agoston, MD, PhD, of Brigham and Women’s Hospital and the department of pathology at Harvard Medical School, Boston, and colleagues reported the findings in Cellular and Molecular Gastroenterology and Hepatology.
“This rodent columnar-lined esophagus has been proposed to develop from cellular reprogramming of progenitor cells, but studies on early columnar-lined esophagus development are lacking,” the researchers wrote.
In the model, ulceration was seen 2 weeks after surgery, which began distally at the esophagojejunal anastomosis. Representative of wound healing, reepithelialization of the ulcer region took place through formation of immature glands, which were found to bud directly from jejunal crypts.
After immunophenotypic analysis, the researchers reported that “immunohistochemical characterization of neoglandular epithelium located immediately proximal to the anastomosis showed features similar to those of the native nonproliferating jejunal epithelium located immediately distal to the anastomosis.” They further reported that “the columnar-lined esophagus’s immunoprofile was similar to jejunal crypt epithelium.”
Upon further examination of the ulcer segment, Dr. Agoston and colleagues found that columnar-lined esophagus elongated from 0.15 mm (standard error of the mean, ± 0.1) to 5.22 mm (SEM, ± 0.37) at 2 and 32 weeks post esophagojejunostomy, respectively.
“There was a highly significant linear relationship between the length of the neoglandular epithelium in the distal esophagus and the number of weeks after surgery (correlation coefficient, 0.94; P less than .0001),” the investigators stated.
Locational analysis revealed epithelial-mesenchymal transition markers being expressed by spindle-shaped cells at the leading edge of the columnar-lined esophagus. In addition, neoglands were identified within esophageal ulcer beds and actively dividing squamous epithelium was seen exclusively at the proximal ulcer border.
Following the systematic analysis, the authors noted that the columnar-lined esophagus was most likely the result of jejunal cell migration into the esophagus. They suggested that if compared, jejunal cells may competitively dominate squamous cells in the context of chronic gastroesophageal reflux disease. Furthermore, they observed that the region of ulceration following esophagojejunostomy in their model was more expansive than that reported in other comparable rodent models of reflux esophagitis.
“The reason for this difference is not clear, but we speculate that it is the result of technical aspects of our reflux-inducing surgery,” the researchers wrote. They further explained that “we intentionally fashioned a large anastomotic orifice between the esophagus and jejunum, perhaps larger than that fashioned by other investigators.” And they concluded, “we suspect that this larger orifice resulted in esophageal exposure to larger volumes of refluxate and, consequently, larger areas of ulceration.”
The authors acknowledged their results may not be fully applicable in the context of human Barrett’s esophagus, given the rodent model. However, they do believe the findings may provide a basis to help understand the wound repair process, particularly the distal edge of ulcers that border the columnar epithelium.
“Using a rat model of reflux esophagitis via surgical esophagojejunostomy, we have shown that a metaplastic, columnar-lined esophagus develops via a wound healing process, and not via genetic reprogramming of progenitor cells,” the researchers concluded.
The study was supported by grant funding from the National Institutes of Health and the Baylor Scott and White Research Institute. The authors reported no conflicts of interest.
SOURCE: Agoston AT et al. Cell Mol Gastroenterol Hepatol. 2018 Jun 26. doi: 10.1016/j.jcmgh.2018.06.007.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: Post esophagojejunostomy in rats, a wound repair process produces metaplastic columnar-lined esophagus likely independent of progenitor cell reprogramming.
Major finding: In an esophageal tissue section, columnar-lined esophagus length was significantly elongated from 0.15 (±0.1) mm to 5.22 (±0.37) mm at 2 and 32 weeks, respectively, following esophagojejunostomy.
Study details: Histologic and immunophenotypic analysis of 52 rats investigating the molecular characteristics of columnar-lined esophagus, specific to ulceration and wound healing, following surgery in an anastomosed rodent model.
Disclosures: The study was supported by grant funding from the National Institutes of Health and the Baylor Scott and White Research Institute. The authors reported no conflicts of interest.
Source: Agoston AT et al. Cell Mol Gastroenterol Hepatol. 2018 Jun 26. doi: 10.1016/j.jcmgh.2018.06.007.
AGA Clinical Practice Update: Diagnosis of rumination syndrome
Additionally, promote diaphragmatic breathing to help manage the condition, advised authors of an expert review of clinical practice updates for rumination syndrome published in Clinical Gastroenterology and Hepatology.
“Patients, not unsurprisingly, typically use the word ‘vomiting’ to describe rumination events, and many patients are misdiagnosed as having refractory vomiting, gastroesophageal reflux disease, or gastroparesis,” Magnus Halland, MD, of the Mayo Clinic in Rochester, Minn., and colleagues wrote in the review. “A long delay in receiving a diagnosis is common and can lead to unnecessary testing, reduced quality of life, and even invasive procedures such as surgery or feeding tubes.”
Rumination syndrome differs from vomiting, the authors noted, because the retrograde flow of ingested gastric content does not have an acidic taste and may in fact taste like food or drink recently ingested. Rumination can occur without any preceding events, after a reflux episode or by the swallowing of air that causes gastric straining but typically happens within 1 hour to 2 hours after a meal. Patients can experience weight loss, dental erosions and caries, heartburn, nausea, bloating, diarrhea, abdominal pain, abdominal discomfort, and belching, among other symptoms, in the presence of rumination syndrome, the authors said.
Dr. Halland and his colleagues provided seven best practice recommendations for rumination syndrome in their updates, which include:
- Patients who show symptoms of consistent postprandial regurgitation, often misdiagnosed with refractory gastroesophageal reflux or vomiting, should be considered for rumination syndrome.
- Patients who have dysphagia, nausea, nocturnal regurgitation, or gastric symptoms outside of meals are less likely to have rumination syndrome, but those symptoms do not exclude the condition.
- Rome IV criteria are advised to diagnose rumination syndrome after medical work-up, which includes “persistent or recurrent regurgitation of recently ingested food into the mouth with subsequent spitting or remastication and swallowing” not preceded by retching where patients fulfill these symptom criteria for 3 months with a minimum of 6 months of symptoms before diagnosis.
- Patients should receive first-line therapy for rumination syndrome consisting of diaphragmatic breathing with or without biofeedback.
- Patients should be referred to a speech therapist, gastroenterologist, psychologist, or other knowledgeable health practitioners to learn effective diaphragmatic breathing.
- Current limitations in the diagnosis of rumination syndrome include need for expertise and lack of standardized protocols, but “testing for rumination syndrome with postprandial high-resolution esophageal impedance manometry can be used to support the diagnosis.”
- Bacloflen (10 mg) taken three times daily is a “reasonable next step” for patients who do not respond to treatment.
The authors acknowledged that many questions, such as the pathophysiology and initiating factors of rumination syndrome, are unknown and noted future studies are needed to address epidemiology, develop validated tools for measuring symptoms, and study diaphragmatic breathing’s effect on reducing symptoms of rumination syndrome as well as the condition’s impact on quality of life.
“Indeed, the basic question of how subconsciously one can learn to regurgitate still needs to be answered,” Dr. Halland and his colleagues wrote.
The authors report no relevant conflicts of interest.
SOURCE: Halland M et al. Clin Gastroenterol Hepatol. 2018 Jun 11. doi: 10.1016/j.cgh.2018.05.049.
Additionally, promote diaphragmatic breathing to help manage the condition, advised authors of an expert review of clinical practice updates for rumination syndrome published in Clinical Gastroenterology and Hepatology.
“Patients, not unsurprisingly, typically use the word ‘vomiting’ to describe rumination events, and many patients are misdiagnosed as having refractory vomiting, gastroesophageal reflux disease, or gastroparesis,” Magnus Halland, MD, of the Mayo Clinic in Rochester, Minn., and colleagues wrote in the review. “A long delay in receiving a diagnosis is common and can lead to unnecessary testing, reduced quality of life, and even invasive procedures such as surgery or feeding tubes.”
Rumination syndrome differs from vomiting, the authors noted, because the retrograde flow of ingested gastric content does not have an acidic taste and may in fact taste like food or drink recently ingested. Rumination can occur without any preceding events, after a reflux episode or by the swallowing of air that causes gastric straining but typically happens within 1 hour to 2 hours after a meal. Patients can experience weight loss, dental erosions and caries, heartburn, nausea, bloating, diarrhea, abdominal pain, abdominal discomfort, and belching, among other symptoms, in the presence of rumination syndrome, the authors said.
Dr. Halland and his colleagues provided seven best practice recommendations for rumination syndrome in their updates, which include:
- Patients who show symptoms of consistent postprandial regurgitation, often misdiagnosed with refractory gastroesophageal reflux or vomiting, should be considered for rumination syndrome.
- Patients who have dysphagia, nausea, nocturnal regurgitation, or gastric symptoms outside of meals are less likely to have rumination syndrome, but those symptoms do not exclude the condition.
- Rome IV criteria are advised to diagnose rumination syndrome after medical work-up, which includes “persistent or recurrent regurgitation of recently ingested food into the mouth with subsequent spitting or remastication and swallowing” not preceded by retching where patients fulfill these symptom criteria for 3 months with a minimum of 6 months of symptoms before diagnosis.
- Patients should receive first-line therapy for rumination syndrome consisting of diaphragmatic breathing with or without biofeedback.
- Patients should be referred to a speech therapist, gastroenterologist, psychologist, or other knowledgeable health practitioners to learn effective diaphragmatic breathing.
- Current limitations in the diagnosis of rumination syndrome include need for expertise and lack of standardized protocols, but “testing for rumination syndrome with postprandial high-resolution esophageal impedance manometry can be used to support the diagnosis.”
- Bacloflen (10 mg) taken three times daily is a “reasonable next step” for patients who do not respond to treatment.
The authors acknowledged that many questions, such as the pathophysiology and initiating factors of rumination syndrome, are unknown and noted future studies are needed to address epidemiology, develop validated tools for measuring symptoms, and study diaphragmatic breathing’s effect on reducing symptoms of rumination syndrome as well as the condition’s impact on quality of life.
“Indeed, the basic question of how subconsciously one can learn to regurgitate still needs to be answered,” Dr. Halland and his colleagues wrote.
The authors report no relevant conflicts of interest.
SOURCE: Halland M et al. Clin Gastroenterol Hepatol. 2018 Jun 11. doi: 10.1016/j.cgh.2018.05.049.
Additionally, promote diaphragmatic breathing to help manage the condition, advised authors of an expert review of clinical practice updates for rumination syndrome published in Clinical Gastroenterology and Hepatology.
“Patients, not unsurprisingly, typically use the word ‘vomiting’ to describe rumination events, and many patients are misdiagnosed as having refractory vomiting, gastroesophageal reflux disease, or gastroparesis,” Magnus Halland, MD, of the Mayo Clinic in Rochester, Minn., and colleagues wrote in the review. “A long delay in receiving a diagnosis is common and can lead to unnecessary testing, reduced quality of life, and even invasive procedures such as surgery or feeding tubes.”
Rumination syndrome differs from vomiting, the authors noted, because the retrograde flow of ingested gastric content does not have an acidic taste and may in fact taste like food or drink recently ingested. Rumination can occur without any preceding events, after a reflux episode or by the swallowing of air that causes gastric straining but typically happens within 1 hour to 2 hours after a meal. Patients can experience weight loss, dental erosions and caries, heartburn, nausea, bloating, diarrhea, abdominal pain, abdominal discomfort, and belching, among other symptoms, in the presence of rumination syndrome, the authors said.
Dr. Halland and his colleagues provided seven best practice recommendations for rumination syndrome in their updates, which include:
- Patients who show symptoms of consistent postprandial regurgitation, often misdiagnosed with refractory gastroesophageal reflux or vomiting, should be considered for rumination syndrome.
- Patients who have dysphagia, nausea, nocturnal regurgitation, or gastric symptoms outside of meals are less likely to have rumination syndrome, but those symptoms do not exclude the condition.
- Rome IV criteria are advised to diagnose rumination syndrome after medical work-up, which includes “persistent or recurrent regurgitation of recently ingested food into the mouth with subsequent spitting or remastication and swallowing” not preceded by retching where patients fulfill these symptom criteria for 3 months with a minimum of 6 months of symptoms before diagnosis.
- Patients should receive first-line therapy for rumination syndrome consisting of diaphragmatic breathing with or without biofeedback.
- Patients should be referred to a speech therapist, gastroenterologist, psychologist, or other knowledgeable health practitioners to learn effective diaphragmatic breathing.
- Current limitations in the diagnosis of rumination syndrome include need for expertise and lack of standardized protocols, but “testing for rumination syndrome with postprandial high-resolution esophageal impedance manometry can be used to support the diagnosis.”
- Bacloflen (10 mg) taken three times daily is a “reasonable next step” for patients who do not respond to treatment.
The authors acknowledged that many questions, such as the pathophysiology and initiating factors of rumination syndrome, are unknown and noted future studies are needed to address epidemiology, develop validated tools for measuring symptoms, and study diaphragmatic breathing’s effect on reducing symptoms of rumination syndrome as well as the condition’s impact on quality of life.
“Indeed, the basic question of how subconsciously one can learn to regurgitate still needs to be answered,” Dr. Halland and his colleagues wrote.
The authors report no relevant conflicts of interest.
SOURCE: Halland M et al. Clin Gastroenterol Hepatol. 2018 Jun 11. doi: 10.1016/j.cgh.2018.05.049.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Experts update diagnostic guidelines for eosinophilic esophagitis
The diagnosis of eosinophilic esophagitis no longer needs to include a trial of proton pump inhibitor (PPI) therapy, according to an updated international consensus statement published in the October issue of Gastroenterology.
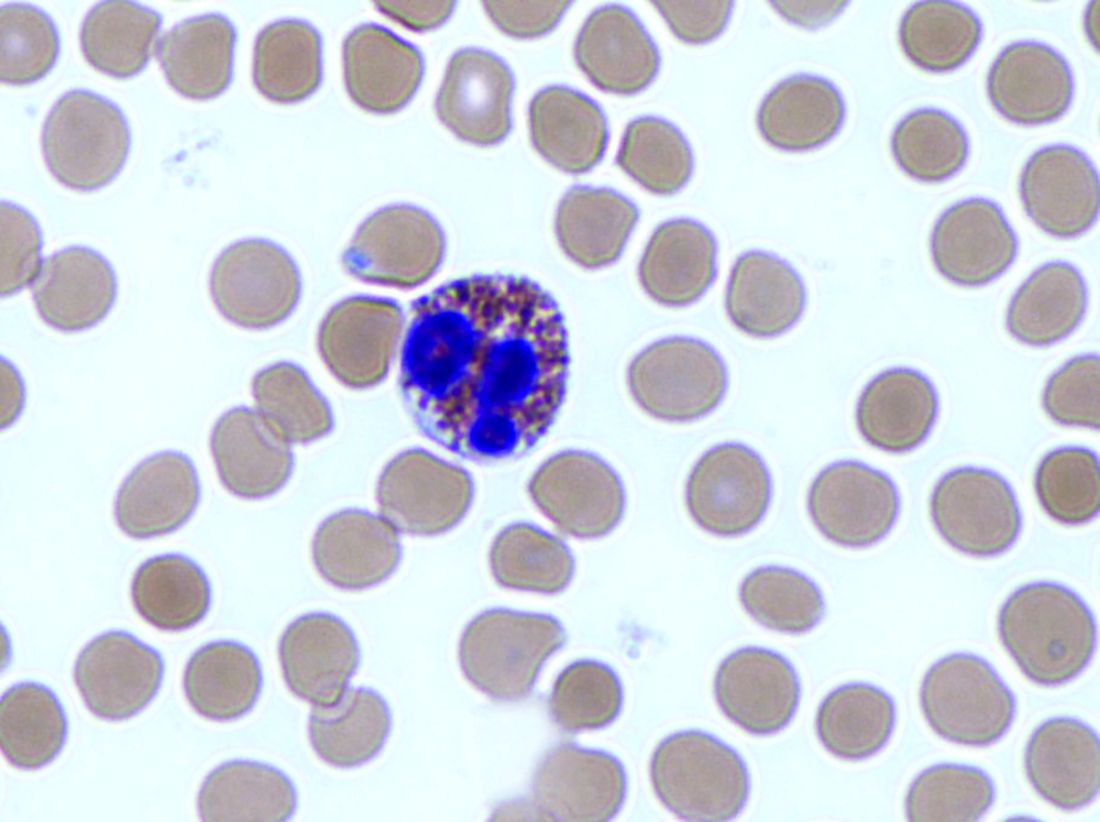
“An initial rationale for the PPI trial was to distinguish eosinophilic esophagitis from gastroesophageal reflux disease, but it is now known that these conditions have a complex relationship and are not necessarily mutually exclusive,” wrote Evan S. Dellon, MD, of the University of North Carolina at Chapel Hill, and his associates. According to current evidence, “PPIs are better classified as a treatment for esophageal eosinophilia that may be due to eosinophilic esophagitis than as a diagnostic criterion,” they said.
Diagnostic guidelines for eosinophilic esophagitis were published first in 2007 and were updated in 2011. The guideline authors recommended either pH monitoring or an 8-week trial of high-dose PPI therapy to rule out inflammation from gastroesophageal reflux disease (GERD).
But subsequent publications described patients with symptomatic esophageal eosinophilia who responded to PPIs and lacked classic GERD symptoms. Guidelines called this condition “PPI-responsive esophageal eosinophilia” and considered it a separate entity from GERD.
However, an “evolving body of research” shows that eosinophilic esophagitis can overlap with GERD, Dr. Dellon and his associates wrote. Furthermore, each of these conditions can trigger the other. Eosinophilic esophagitis can decrease esophageal compliance, leading to secondary reflux, while gastroesophageal reflux can erode the esophageal epithelium, triggering antigen exposure and eosinophilia.
Therefore, Dr. Dellon and his associates recommended defining eosinophilic esophagitis as signs and symptoms of esophageal dysfunction and an esophageal biopsy showing at least 15 eosinophils per high-power field, or approximately 60 eosinophils per millimeter, with infiltration limited to the esophagus. They stressed the importance of esophageal biopsy even if endoscopy shows normal mucosa. “As per prior guidelines, multiple biopsies from two or more esophageal levels, targeting areas of apparent inflammation, are recommended to increase the diagnostic yield,” they added. “Gastric and duodenal biopsies should be obtained as clinically indicated by symptoms, endoscopic findings in the stomach or duodenum, or high index of suspicion for a mucosal process.”
Physicians should increase their suspicion of eosinophilic esophagitis if patients have other types of atopy or endoscopic findings of “rings, furrows, exudates, edema, stricture, narrowing, and crepe-paper mucosa,” they added. In addition to GERD, they recommended looking carefully for other conditions that can trigger esophageal eosinophilia, such as pemphigus, drug hypersensitivity reactions, achalasia, and Crohn’s disease with esophageal involvement.
To create the guideline, Dr. Dellon and his associates searched PubMed for studies of all designs and sizes published from 1966 through December 2016. Teams of experts on specific topics then reviewed and discussed relevant literature. In May 2017, 43 reviewers met for 8 hours to present and discuss conclusions. There was 100% agreement to remove the PPI trial from the diagnostic criteria, the experts noted.
The authors disclosed financial support from the International Gastrointestinal Eosinophilic Diseases Researchers (TIGERS), The David and Denise Bunning Family, and the Rare Disease Clinical Research Network. Dr. Dellon disclosed consulting relationships and receiving research funding from Adare, Celgene/Receptos, Regeneron, and Shire among others. The majority of his coauthors also disclosed relationships with numerous medical companies.
SOURCE: Dellon ES et al. Gastroenterology. 2018 Jul 12. doi: 10.1053/j.gastro.2018.07.009.
Studies in the 1980s linked the presence of esophageal mucosal eosinophils with increased acid exposure on pH monitoring. For the next 2 decades, clinicians viewed eosinophils on esophageal biopsies as diagnostic for GERD such that the initial description of EoE by Attwood in 1993 distinguished EoE from GERD by the presence of esophageal eosinophilia in the absence of either reflux esophagitis or abnormal acid exposure on pH testing. Consequently, the initial diagnostic criteria for EoE in 2007 included a lack of response to PPI and/or normal pH testing to establish the diagnosis of EoE. Reflecting growing uncertainty regarding the ability of PPI therapy to differentiate acid-induced from allergic inflammatory mechanisms, an updated consensus in 2011 introduced the terminology “PPI responsive esophageal eosinophilia (PPIREE)” to describe an increasingly recognized subset of patients with suspected EoE that resolved with PPI. Now, supported by scientific evidence accumulated over the past decade, AGREE has taken a step back by removing the PPI trial from the diagnosis of EoE, thereby abandoning the PPIREE terminology. This step simplifies the diagnosis of EoE and acknowledges that a histologic response to PPI does not “rule in” GERD or “rule out” EoE. It is important to emphasize that the updated criteria still advocate careful consideration of secondary causes of esophageal eosinophilia prior to the diagnosis of EoE.
Ramifications of the updated diagnostic criteria include the opportunities for clinicians to consider use of topical corticosteroids and diet therapies, rather than mandate an up-front PPI trial, in patients with EoE. On a practical level, based on their effectiveness, safety, and ease of administration, PPIs remain positioned as a favorable initial intervention for EoE. Conceptually, however, the paradigm shift highlights the ability of research to improve our understanding of disease pathogenesis and thereby impact clinical management.
Ikuo Hirano, MD, AGAF, is in the division of gastroenterology, Northwestern University, Chicago. He has received grant support from the NIH Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR, U54 AI117804), which is part of the Rare Disease Clinical Research Network. He has received research funding and consulting fees from Celgene, Regeneron, Shire, and others.
Studies in the 1980s linked the presence of esophageal mucosal eosinophils with increased acid exposure on pH monitoring. For the next 2 decades, clinicians viewed eosinophils on esophageal biopsies as diagnostic for GERD such that the initial description of EoE by Attwood in 1993 distinguished EoE from GERD by the presence of esophageal eosinophilia in the absence of either reflux esophagitis or abnormal acid exposure on pH testing. Consequently, the initial diagnostic criteria for EoE in 2007 included a lack of response to PPI and/or normal pH testing to establish the diagnosis of EoE. Reflecting growing uncertainty regarding the ability of PPI therapy to differentiate acid-induced from allergic inflammatory mechanisms, an updated consensus in 2011 introduced the terminology “PPI responsive esophageal eosinophilia (PPIREE)” to describe an increasingly recognized subset of patients with suspected EoE that resolved with PPI. Now, supported by scientific evidence accumulated over the past decade, AGREE has taken a step back by removing the PPI trial from the diagnosis of EoE, thereby abandoning the PPIREE terminology. This step simplifies the diagnosis of EoE and acknowledges that a histologic response to PPI does not “rule in” GERD or “rule out” EoE. It is important to emphasize that the updated criteria still advocate careful consideration of secondary causes of esophageal eosinophilia prior to the diagnosis of EoE.
Ramifications of the updated diagnostic criteria include the opportunities for clinicians to consider use of topical corticosteroids and diet therapies, rather than mandate an up-front PPI trial, in patients with EoE. On a practical level, based on their effectiveness, safety, and ease of administration, PPIs remain positioned as a favorable initial intervention for EoE. Conceptually, however, the paradigm shift highlights the ability of research to improve our understanding of disease pathogenesis and thereby impact clinical management.
Ikuo Hirano, MD, AGAF, is in the division of gastroenterology, Northwestern University, Chicago. He has received grant support from the NIH Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR, U54 AI117804), which is part of the Rare Disease Clinical Research Network. He has received research funding and consulting fees from Celgene, Regeneron, Shire, and others.
Studies in the 1980s linked the presence of esophageal mucosal eosinophils with increased acid exposure on pH monitoring. For the next 2 decades, clinicians viewed eosinophils on esophageal biopsies as diagnostic for GERD such that the initial description of EoE by Attwood in 1993 distinguished EoE from GERD by the presence of esophageal eosinophilia in the absence of either reflux esophagitis or abnormal acid exposure on pH testing. Consequently, the initial diagnostic criteria for EoE in 2007 included a lack of response to PPI and/or normal pH testing to establish the diagnosis of EoE. Reflecting growing uncertainty regarding the ability of PPI therapy to differentiate acid-induced from allergic inflammatory mechanisms, an updated consensus in 2011 introduced the terminology “PPI responsive esophageal eosinophilia (PPIREE)” to describe an increasingly recognized subset of patients with suspected EoE that resolved with PPI. Now, supported by scientific evidence accumulated over the past decade, AGREE has taken a step back by removing the PPI trial from the diagnosis of EoE, thereby abandoning the PPIREE terminology. This step simplifies the diagnosis of EoE and acknowledges that a histologic response to PPI does not “rule in” GERD or “rule out” EoE. It is important to emphasize that the updated criteria still advocate careful consideration of secondary causes of esophageal eosinophilia prior to the diagnosis of EoE.
Ramifications of the updated diagnostic criteria include the opportunities for clinicians to consider use of topical corticosteroids and diet therapies, rather than mandate an up-front PPI trial, in patients with EoE. On a practical level, based on their effectiveness, safety, and ease of administration, PPIs remain positioned as a favorable initial intervention for EoE. Conceptually, however, the paradigm shift highlights the ability of research to improve our understanding of disease pathogenesis and thereby impact clinical management.
Ikuo Hirano, MD, AGAF, is in the division of gastroenterology, Northwestern University, Chicago. He has received grant support from the NIH Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR, U54 AI117804), which is part of the Rare Disease Clinical Research Network. He has received research funding and consulting fees from Celgene, Regeneron, Shire, and others.
The diagnosis of eosinophilic esophagitis no longer needs to include a trial of proton pump inhibitor (PPI) therapy, according to an updated international consensus statement published in the October issue of Gastroenterology.
“An initial rationale for the PPI trial was to distinguish eosinophilic esophagitis from gastroesophageal reflux disease, but it is now known that these conditions have a complex relationship and are not necessarily mutually exclusive,” wrote Evan S. Dellon, MD, of the University of North Carolina at Chapel Hill, and his associates. According to current evidence, “PPIs are better classified as a treatment for esophageal eosinophilia that may be due to eosinophilic esophagitis than as a diagnostic criterion,” they said.
Diagnostic guidelines for eosinophilic esophagitis were published first in 2007 and were updated in 2011. The guideline authors recommended either pH monitoring or an 8-week trial of high-dose PPI therapy to rule out inflammation from gastroesophageal reflux disease (GERD).
But subsequent publications described patients with symptomatic esophageal eosinophilia who responded to PPIs and lacked classic GERD symptoms. Guidelines called this condition “PPI-responsive esophageal eosinophilia” and considered it a separate entity from GERD.
However, an “evolving body of research” shows that eosinophilic esophagitis can overlap with GERD, Dr. Dellon and his associates wrote. Furthermore, each of these conditions can trigger the other. Eosinophilic esophagitis can decrease esophageal compliance, leading to secondary reflux, while gastroesophageal reflux can erode the esophageal epithelium, triggering antigen exposure and eosinophilia.
Therefore, Dr. Dellon and his associates recommended defining eosinophilic esophagitis as signs and symptoms of esophageal dysfunction and an esophageal biopsy showing at least 15 eosinophils per high-power field, or approximately 60 eosinophils per millimeter, with infiltration limited to the esophagus. They stressed the importance of esophageal biopsy even if endoscopy shows normal mucosa. “As per prior guidelines, multiple biopsies from two or more esophageal levels, targeting areas of apparent inflammation, are recommended to increase the diagnostic yield,” they added. “Gastric and duodenal biopsies should be obtained as clinically indicated by symptoms, endoscopic findings in the stomach or duodenum, or high index of suspicion for a mucosal process.”
Physicians should increase their suspicion of eosinophilic esophagitis if patients have other types of atopy or endoscopic findings of “rings, furrows, exudates, edema, stricture, narrowing, and crepe-paper mucosa,” they added. In addition to GERD, they recommended looking carefully for other conditions that can trigger esophageal eosinophilia, such as pemphigus, drug hypersensitivity reactions, achalasia, and Crohn’s disease with esophageal involvement.
To create the guideline, Dr. Dellon and his associates searched PubMed for studies of all designs and sizes published from 1966 through December 2016. Teams of experts on specific topics then reviewed and discussed relevant literature. In May 2017, 43 reviewers met for 8 hours to present and discuss conclusions. There was 100% agreement to remove the PPI trial from the diagnostic criteria, the experts noted.
The authors disclosed financial support from the International Gastrointestinal Eosinophilic Diseases Researchers (TIGERS), The David and Denise Bunning Family, and the Rare Disease Clinical Research Network. Dr. Dellon disclosed consulting relationships and receiving research funding from Adare, Celgene/Receptos, Regeneron, and Shire among others. The majority of his coauthors also disclosed relationships with numerous medical companies.
SOURCE: Dellon ES et al. Gastroenterology. 2018 Jul 12. doi: 10.1053/j.gastro.2018.07.009.
The diagnosis of eosinophilic esophagitis no longer needs to include a trial of proton pump inhibitor (PPI) therapy, according to an updated international consensus statement published in the October issue of Gastroenterology.
“An initial rationale for the PPI trial was to distinguish eosinophilic esophagitis from gastroesophageal reflux disease, but it is now known that these conditions have a complex relationship and are not necessarily mutually exclusive,” wrote Evan S. Dellon, MD, of the University of North Carolina at Chapel Hill, and his associates. According to current evidence, “PPIs are better classified as a treatment for esophageal eosinophilia that may be due to eosinophilic esophagitis than as a diagnostic criterion,” they said.
Diagnostic guidelines for eosinophilic esophagitis were published first in 2007 and were updated in 2011. The guideline authors recommended either pH monitoring or an 8-week trial of high-dose PPI therapy to rule out inflammation from gastroesophageal reflux disease (GERD).
But subsequent publications described patients with symptomatic esophageal eosinophilia who responded to PPIs and lacked classic GERD symptoms. Guidelines called this condition “PPI-responsive esophageal eosinophilia” and considered it a separate entity from GERD.
However, an “evolving body of research” shows that eosinophilic esophagitis can overlap with GERD, Dr. Dellon and his associates wrote. Furthermore, each of these conditions can trigger the other. Eosinophilic esophagitis can decrease esophageal compliance, leading to secondary reflux, while gastroesophageal reflux can erode the esophageal epithelium, triggering antigen exposure and eosinophilia.
Therefore, Dr. Dellon and his associates recommended defining eosinophilic esophagitis as signs and symptoms of esophageal dysfunction and an esophageal biopsy showing at least 15 eosinophils per high-power field, or approximately 60 eosinophils per millimeter, with infiltration limited to the esophagus. They stressed the importance of esophageal biopsy even if endoscopy shows normal mucosa. “As per prior guidelines, multiple biopsies from two or more esophageal levels, targeting areas of apparent inflammation, are recommended to increase the diagnostic yield,” they added. “Gastric and duodenal biopsies should be obtained as clinically indicated by symptoms, endoscopic findings in the stomach or duodenum, or high index of suspicion for a mucosal process.”
Physicians should increase their suspicion of eosinophilic esophagitis if patients have other types of atopy or endoscopic findings of “rings, furrows, exudates, edema, stricture, narrowing, and crepe-paper mucosa,” they added. In addition to GERD, they recommended looking carefully for other conditions that can trigger esophageal eosinophilia, such as pemphigus, drug hypersensitivity reactions, achalasia, and Crohn’s disease with esophageal involvement.
To create the guideline, Dr. Dellon and his associates searched PubMed for studies of all designs and sizes published from 1966 through December 2016. Teams of experts on specific topics then reviewed and discussed relevant literature. In May 2017, 43 reviewers met for 8 hours to present and discuss conclusions. There was 100% agreement to remove the PPI trial from the diagnostic criteria, the experts noted.
The authors disclosed financial support from the International Gastrointestinal Eosinophilic Diseases Researchers (TIGERS), The David and Denise Bunning Family, and the Rare Disease Clinical Research Network. Dr. Dellon disclosed consulting relationships and receiving research funding from Adare, Celgene/Receptos, Regeneron, and Shire among others. The majority of his coauthors also disclosed relationships with numerous medical companies.
SOURCE: Dellon ES et al. Gastroenterology. 2018 Jul 12. doi: 10.1053/j.gastro.2018.07.009.
FROM GASTROENTEROLOGY
Key clinical point: The diagnosis of eosinophilic esophagitis no longer needs to include a trial of proton pump inhibitor therapy.
Major finding: Eosinophilic esophagitis and gastroesophageal reflux disease are not mutually exclusive.
Study details: Review by an international consensus panel of studies published between 1966 and 2016.
Disclosures: The authors disclosed financial support from the International Gastrointestinal Eosinophilic Diseases Researchers (TIGERS), The David and Denise Bunning Family, the Rare Disease Clinical Research Network. Dr. Dellon disclosed consulting relationships with Adare, Allakos, Alivio, Banner, Celgene/Receptos, Enumeral, GSK, Regeneron, and Shire. He also reported receiving research funding from Adare, Celgene/Receptos, Miraca, Meritage, Nutricia, Regeneron, and Shire and educational grants from Banner and Holoclara. The majority of his coauthors disclosed relationships with numerous medical companies.
Source: Dellon ES et al. Gastroenterology. 2018 Jul 12. doi: 10.1053/j.gastro.2018.07.009.