User login
Infections within first year of life predicted IBD
according to the findings of a large population-based study.
It remains unclear whether the risk reflects infections in themselves or the use of antibiotic therapy, wrote Charles N. Bernstein, MD, of the University of Manitoba, Winnipeg, and associates. Infections did not appear to be a proxy for immunodeficiency disorders, which were similarly infrequent among cases and controls, they noted. Limiting antibiotic usage, while desirable, would be difficult to do for infections as serious as many in the study. Hence, they suggested research to determine “exactly what antibiotic intake does to infant gut microflora or intestinal or systemic immune responses,” and whether giving probiotics or prebiotics after antibiotic therapy helps attenuate the risk of inflammatory bowel disease (IBD) and other autoimmune disorders. The findings were published in Gastroenterology.
IBD is probably multifactorial, but specific causal factors remain unclear. Based on mounting evidence for the role of gut dysbiosis, the researchers explored whether IBD is associated with higher rates of infections and other critical events during the neonatal period and the first year of life by comparing 825 patients with IBD and 5,999 controls matched by age, sex, and area of residence. The data source was the University of Manitoba IBD Epidemiology Database, which includes all Manitobans diagnosed with IBD from 1984 to 2010. The researchers also compared patients with 1,740 unaffected siblings.
Gastrointestinal infections, gastrointestinal disease, and abdominal pain during the first year of life did not predict subsequent IBD. Maternal IBD was the strongest risk factor (odds ratio, 4.5; 95% confidence interval, 3.1-6.7). Among neonatal events, the only significant risk factor was being in the highest versus the lowest socioeconomic quintile (OR, 1.35; 95% CI, 1.01-1.79). This association persisted during the first year of life.
Infections during the first year of life were a significant risk factor for IBD before age 10 (OR, 3.1; 95% CI, 1.1-8.8) and age 20 years (OR, 1.6; 95% CI, 1.2-2.2) in the population-based analysis. In contrast, patients and their unaffected siblings had similar rates of infection during early life. The study may have missed differences in exposures between these groups, or perhaps patients lack certain protective genes possessed by healthy siblings, the researchers wrote.
Numbers of antibiotic prescriptions during the first year and the first decade of life did not significantly differ between 33 cases and 270 controls with available data. However, there was a trend toward more antibiotics prescribed to patients versus controls.
“Together with our past reports that neither cesarean section birth nor antenatal or perinatal maternal use of antibiotics predict ultimate development of IBD, it seems that neonatal changes to the microbiome are subsumed by those occurring in the first year of life,” the investigators concluded. They recommended studying the infant gut microbiome before and for several months after infections and antibiotic exposure to determine which shifts in microbiota predict IBD onset.
The Manitoba Centre for Health Policy provided access to the Population Health Research Data Repository. Dr. Bernstein is supported by the Bingham Chair in Gastroenterology. He reported ties to AbbVie Canada, Ferring Canada, Janssen Canada, Shire Canada, Takeda Canada, Pfizer Canada, Napo Pharmaceuticals, 4D Pharma, and Mylan.
SOURCE: Bernstein CN et al. Gastroenterology. 2019 Feb 14. doi: 10.1053/j.gastro.2019.02.004.
Understanding and exploring factors that could impact inflammatory bowel disease (IBD) development is imperative. This study by Bernstein et al. evaluated whether environmental factors in the first year of life may impact subsequent diagnosis of IBD using population-based cohort data with robust and detailed health information. Maternal history of IBD was the most predictive factor in development of IBD, further evidence of a genetic component to disease pathogenesis. However, environmental factors such as high socioeconomic status within the first year of life were predictive of diagnosis of IBD later in life, possibly lending further support to the “hygiene hypothesis.”
Also, significant infections identified in the clinical setting or requiring hospitalization were predictive of subsequent IBD diagnosis. This is particularly interesting as gut microbiome perturbations increasingly take the stage as a possible pathway of significance in IBD. Could infection within the first year of life or the subsequent antibiotic use required affect the gut microbiome so significantly and perhaps permanently to affect development of later childhood or adult IBD?
Sara Horst, MD, MPH, is an associate professor of medicine in the department of gastroenterology, hepatology, and medicine at Vanderbilt University, Nashville, Tenn. She has consulted for Janssen, UCB, and Boehringer Ingelheim.
Understanding and exploring factors that could impact inflammatory bowel disease (IBD) development is imperative. This study by Bernstein et al. evaluated whether environmental factors in the first year of life may impact subsequent diagnosis of IBD using population-based cohort data with robust and detailed health information. Maternal history of IBD was the most predictive factor in development of IBD, further evidence of a genetic component to disease pathogenesis. However, environmental factors such as high socioeconomic status within the first year of life were predictive of diagnosis of IBD later in life, possibly lending further support to the “hygiene hypothesis.”
Also, significant infections identified in the clinical setting or requiring hospitalization were predictive of subsequent IBD diagnosis. This is particularly interesting as gut microbiome perturbations increasingly take the stage as a possible pathway of significance in IBD. Could infection within the first year of life or the subsequent antibiotic use required affect the gut microbiome so significantly and perhaps permanently to affect development of later childhood or adult IBD?
Sara Horst, MD, MPH, is an associate professor of medicine in the department of gastroenterology, hepatology, and medicine at Vanderbilt University, Nashville, Tenn. She has consulted for Janssen, UCB, and Boehringer Ingelheim.
Understanding and exploring factors that could impact inflammatory bowel disease (IBD) development is imperative. This study by Bernstein et al. evaluated whether environmental factors in the first year of life may impact subsequent diagnosis of IBD using population-based cohort data with robust and detailed health information. Maternal history of IBD was the most predictive factor in development of IBD, further evidence of a genetic component to disease pathogenesis. However, environmental factors such as high socioeconomic status within the first year of life were predictive of diagnosis of IBD later in life, possibly lending further support to the “hygiene hypothesis.”
Also, significant infections identified in the clinical setting or requiring hospitalization were predictive of subsequent IBD diagnosis. This is particularly interesting as gut microbiome perturbations increasingly take the stage as a possible pathway of significance in IBD. Could infection within the first year of life or the subsequent antibiotic use required affect the gut microbiome so significantly and perhaps permanently to affect development of later childhood or adult IBD?
Sara Horst, MD, MPH, is an associate professor of medicine in the department of gastroenterology, hepatology, and medicine at Vanderbilt University, Nashville, Tenn. She has consulted for Janssen, UCB, and Boehringer Ingelheim.
according to the findings of a large population-based study.
It remains unclear whether the risk reflects infections in themselves or the use of antibiotic therapy, wrote Charles N. Bernstein, MD, of the University of Manitoba, Winnipeg, and associates. Infections did not appear to be a proxy for immunodeficiency disorders, which were similarly infrequent among cases and controls, they noted. Limiting antibiotic usage, while desirable, would be difficult to do for infections as serious as many in the study. Hence, they suggested research to determine “exactly what antibiotic intake does to infant gut microflora or intestinal or systemic immune responses,” and whether giving probiotics or prebiotics after antibiotic therapy helps attenuate the risk of inflammatory bowel disease (IBD) and other autoimmune disorders. The findings were published in Gastroenterology.
IBD is probably multifactorial, but specific causal factors remain unclear. Based on mounting evidence for the role of gut dysbiosis, the researchers explored whether IBD is associated with higher rates of infections and other critical events during the neonatal period and the first year of life by comparing 825 patients with IBD and 5,999 controls matched by age, sex, and area of residence. The data source was the University of Manitoba IBD Epidemiology Database, which includes all Manitobans diagnosed with IBD from 1984 to 2010. The researchers also compared patients with 1,740 unaffected siblings.
Gastrointestinal infections, gastrointestinal disease, and abdominal pain during the first year of life did not predict subsequent IBD. Maternal IBD was the strongest risk factor (odds ratio, 4.5; 95% confidence interval, 3.1-6.7). Among neonatal events, the only significant risk factor was being in the highest versus the lowest socioeconomic quintile (OR, 1.35; 95% CI, 1.01-1.79). This association persisted during the first year of life.
Infections during the first year of life were a significant risk factor for IBD before age 10 (OR, 3.1; 95% CI, 1.1-8.8) and age 20 years (OR, 1.6; 95% CI, 1.2-2.2) in the population-based analysis. In contrast, patients and their unaffected siblings had similar rates of infection during early life. The study may have missed differences in exposures between these groups, or perhaps patients lack certain protective genes possessed by healthy siblings, the researchers wrote.
Numbers of antibiotic prescriptions during the first year and the first decade of life did not significantly differ between 33 cases and 270 controls with available data. However, there was a trend toward more antibiotics prescribed to patients versus controls.
“Together with our past reports that neither cesarean section birth nor antenatal or perinatal maternal use of antibiotics predict ultimate development of IBD, it seems that neonatal changes to the microbiome are subsumed by those occurring in the first year of life,” the investigators concluded. They recommended studying the infant gut microbiome before and for several months after infections and antibiotic exposure to determine which shifts in microbiota predict IBD onset.
The Manitoba Centre for Health Policy provided access to the Population Health Research Data Repository. Dr. Bernstein is supported by the Bingham Chair in Gastroenterology. He reported ties to AbbVie Canada, Ferring Canada, Janssen Canada, Shire Canada, Takeda Canada, Pfizer Canada, Napo Pharmaceuticals, 4D Pharma, and Mylan.
SOURCE: Bernstein CN et al. Gastroenterology. 2019 Feb 14. doi: 10.1053/j.gastro.2019.02.004.
according to the findings of a large population-based study.
It remains unclear whether the risk reflects infections in themselves or the use of antibiotic therapy, wrote Charles N. Bernstein, MD, of the University of Manitoba, Winnipeg, and associates. Infections did not appear to be a proxy for immunodeficiency disorders, which were similarly infrequent among cases and controls, they noted. Limiting antibiotic usage, while desirable, would be difficult to do for infections as serious as many in the study. Hence, they suggested research to determine “exactly what antibiotic intake does to infant gut microflora or intestinal or systemic immune responses,” and whether giving probiotics or prebiotics after antibiotic therapy helps attenuate the risk of inflammatory bowel disease (IBD) and other autoimmune disorders. The findings were published in Gastroenterology.
IBD is probably multifactorial, but specific causal factors remain unclear. Based on mounting evidence for the role of gut dysbiosis, the researchers explored whether IBD is associated with higher rates of infections and other critical events during the neonatal period and the first year of life by comparing 825 patients with IBD and 5,999 controls matched by age, sex, and area of residence. The data source was the University of Manitoba IBD Epidemiology Database, which includes all Manitobans diagnosed with IBD from 1984 to 2010. The researchers also compared patients with 1,740 unaffected siblings.
Gastrointestinal infections, gastrointestinal disease, and abdominal pain during the first year of life did not predict subsequent IBD. Maternal IBD was the strongest risk factor (odds ratio, 4.5; 95% confidence interval, 3.1-6.7). Among neonatal events, the only significant risk factor was being in the highest versus the lowest socioeconomic quintile (OR, 1.35; 95% CI, 1.01-1.79). This association persisted during the first year of life.
Infections during the first year of life were a significant risk factor for IBD before age 10 (OR, 3.1; 95% CI, 1.1-8.8) and age 20 years (OR, 1.6; 95% CI, 1.2-2.2) in the population-based analysis. In contrast, patients and their unaffected siblings had similar rates of infection during early life. The study may have missed differences in exposures between these groups, or perhaps patients lack certain protective genes possessed by healthy siblings, the researchers wrote.
Numbers of antibiotic prescriptions during the first year and the first decade of life did not significantly differ between 33 cases and 270 controls with available data. However, there was a trend toward more antibiotics prescribed to patients versus controls.
“Together with our past reports that neither cesarean section birth nor antenatal or perinatal maternal use of antibiotics predict ultimate development of IBD, it seems that neonatal changes to the microbiome are subsumed by those occurring in the first year of life,” the investigators concluded. They recommended studying the infant gut microbiome before and for several months after infections and antibiotic exposure to determine which shifts in microbiota predict IBD onset.
The Manitoba Centre for Health Policy provided access to the Population Health Research Data Repository. Dr. Bernstein is supported by the Bingham Chair in Gastroenterology. He reported ties to AbbVie Canada, Ferring Canada, Janssen Canada, Shire Canada, Takeda Canada, Pfizer Canada, Napo Pharmaceuticals, 4D Pharma, and Mylan.
SOURCE: Bernstein CN et al. Gastroenterology. 2019 Feb 14. doi: 10.1053/j.gastro.2019.02.004.
FROM GASTROENTEROLOGY
Induction trough levels predicted ustekinumab response in Crohn’s disease
For patients with Crohn’s disease, therapeutic drug monitoring helped identify early primary nonresponders to induction with ustekinumab, according to researchers. The report is in Clinical Gastroenterology and Hepatology.
At week 8, median trough levels of ustekinumab were 6.0 mcg per mL (interquartile range, 3.1-8.0) among patients who achieved a primary response to induction at week 16, versus 1.3 mcg/mL (IQR, 0.9-5.6 ) among primary nonresponders (P = .03). An 8-week ustekinumab trough level cutoff of 2.0 mcg/mL distinguished week 16 responders from nonresponders with an area under the receiver operating curve (AUROC) of 0.75, wrote Ninon Soufflet of University Claude Bernard Lyon 1 in France, and associates. The researchers recommended “dedicated studies” to assess whether escalating the dose of ustekinumab can benefit patients with lower trough levels at week 8.
Few studies have explored biomarkers for response to ustekinumab induction therapy. Hence, the researchers assessed the relative utility of ustekinumab trough levels, C-reactive protein (CRP) levels, and fecal calprotectin levels for predicting early primary nonresponse. All 51 study participants had active luminal Crohn’s disease and received body weight–based intravenous infusions of ustekinumab at baseline, followed by subcutaneous injections of 90 mg. Primary nonresponders did not achieve steroid-free clinical and biochemical remission at week 16, defined as a Harvey-Bradshaw Index (HBI) of 4 points or less, a CRP level under 5 mg/L, and a fecal calprotectin level under 250 mcg/g. Week 16 was chosen to account for any delayed responders, the researchers noted.
A total of 32 patients (63%) achieved remission to ustekinumab induction therapy by week 16. An 8-week trough level of 2.0 mcg/mL was found to be optimal and distinguished primary nonresponders from responders with a sensitivity of 87%, a specificity of 66%, a positive predictive value of 82%, and a negative predictive value of 75%. In prior studies, optimal thresholds exceeded 3.3 mcg/mL for achieving remission and 4.5 mcg/mL at week 26 for achieving endoscopic response, the researchers noted. They said that this discrepancy might reflect different time points for evaluation, assays for measuring ustekinumab, patient populations, and a lack of endoscopic data in their study. “The relatively small sample size and the short period of follow-up evaluation [were] substantial limitations” they acknowledged.
In this study, levels of CRP did not change significantly between weeks 0 and 16 among either responders or nonresponders. In contrast, fecal calprotectin levels dropped rapidly and significantly over time only in responders. Median fecal calprotectin levels were 1,612 mcg/g of stools at week 0 versus 374 mcg/g at week 4 and 339 mcg/g at week 8. The finding “confirms the value of this biomarker, as previously shown in inflammatory bowel disease with anti–tumor necrosis factor,” the researchers wrote.
The investigators did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
Learn more about therapeutic drug monitoring in IBD by reviewing the AGA Institute guideline at http://www.gastrojournal.org/article/S0016-5085(17)35963-2/fulltext.
SOURCE: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042. https://www.cghjournal.org/article/S1542-3565(19)30248-4/abstract
For patients with Crohn’s disease, therapeutic drug monitoring helped identify early primary nonresponders to induction with ustekinumab, according to researchers. The report is in Clinical Gastroenterology and Hepatology.
At week 8, median trough levels of ustekinumab were 6.0 mcg per mL (interquartile range, 3.1-8.0) among patients who achieved a primary response to induction at week 16, versus 1.3 mcg/mL (IQR, 0.9-5.6 ) among primary nonresponders (P = .03). An 8-week ustekinumab trough level cutoff of 2.0 mcg/mL distinguished week 16 responders from nonresponders with an area under the receiver operating curve (AUROC) of 0.75, wrote Ninon Soufflet of University Claude Bernard Lyon 1 in France, and associates. The researchers recommended “dedicated studies” to assess whether escalating the dose of ustekinumab can benefit patients with lower trough levels at week 8.
Few studies have explored biomarkers for response to ustekinumab induction therapy. Hence, the researchers assessed the relative utility of ustekinumab trough levels, C-reactive protein (CRP) levels, and fecal calprotectin levels for predicting early primary nonresponse. All 51 study participants had active luminal Crohn’s disease and received body weight–based intravenous infusions of ustekinumab at baseline, followed by subcutaneous injections of 90 mg. Primary nonresponders did not achieve steroid-free clinical and biochemical remission at week 16, defined as a Harvey-Bradshaw Index (HBI) of 4 points or less, a CRP level under 5 mg/L, and a fecal calprotectin level under 250 mcg/g. Week 16 was chosen to account for any delayed responders, the researchers noted.
A total of 32 patients (63%) achieved remission to ustekinumab induction therapy by week 16. An 8-week trough level of 2.0 mcg/mL was found to be optimal and distinguished primary nonresponders from responders with a sensitivity of 87%, a specificity of 66%, a positive predictive value of 82%, and a negative predictive value of 75%. In prior studies, optimal thresholds exceeded 3.3 mcg/mL for achieving remission and 4.5 mcg/mL at week 26 for achieving endoscopic response, the researchers noted. They said that this discrepancy might reflect different time points for evaluation, assays for measuring ustekinumab, patient populations, and a lack of endoscopic data in their study. “The relatively small sample size and the short period of follow-up evaluation [were] substantial limitations” they acknowledged.
In this study, levels of CRP did not change significantly between weeks 0 and 16 among either responders or nonresponders. In contrast, fecal calprotectin levels dropped rapidly and significantly over time only in responders. Median fecal calprotectin levels were 1,612 mcg/g of stools at week 0 versus 374 mcg/g at week 4 and 339 mcg/g at week 8. The finding “confirms the value of this biomarker, as previously shown in inflammatory bowel disease with anti–tumor necrosis factor,” the researchers wrote.
The investigators did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
Learn more about therapeutic drug monitoring in IBD by reviewing the AGA Institute guideline at http://www.gastrojournal.org/article/S0016-5085(17)35963-2/fulltext.
SOURCE: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042. https://www.cghjournal.org/article/S1542-3565(19)30248-4/abstract
For patients with Crohn’s disease, therapeutic drug monitoring helped identify early primary nonresponders to induction with ustekinumab, according to researchers. The report is in Clinical Gastroenterology and Hepatology.
At week 8, median trough levels of ustekinumab were 6.0 mcg per mL (interquartile range, 3.1-8.0) among patients who achieved a primary response to induction at week 16, versus 1.3 mcg/mL (IQR, 0.9-5.6 ) among primary nonresponders (P = .03). An 8-week ustekinumab trough level cutoff of 2.0 mcg/mL distinguished week 16 responders from nonresponders with an area under the receiver operating curve (AUROC) of 0.75, wrote Ninon Soufflet of University Claude Bernard Lyon 1 in France, and associates. The researchers recommended “dedicated studies” to assess whether escalating the dose of ustekinumab can benefit patients with lower trough levels at week 8.
Few studies have explored biomarkers for response to ustekinumab induction therapy. Hence, the researchers assessed the relative utility of ustekinumab trough levels, C-reactive protein (CRP) levels, and fecal calprotectin levels for predicting early primary nonresponse. All 51 study participants had active luminal Crohn’s disease and received body weight–based intravenous infusions of ustekinumab at baseline, followed by subcutaneous injections of 90 mg. Primary nonresponders did not achieve steroid-free clinical and biochemical remission at week 16, defined as a Harvey-Bradshaw Index (HBI) of 4 points or less, a CRP level under 5 mg/L, and a fecal calprotectin level under 250 mcg/g. Week 16 was chosen to account for any delayed responders, the researchers noted.
A total of 32 patients (63%) achieved remission to ustekinumab induction therapy by week 16. An 8-week trough level of 2.0 mcg/mL was found to be optimal and distinguished primary nonresponders from responders with a sensitivity of 87%, a specificity of 66%, a positive predictive value of 82%, and a negative predictive value of 75%. In prior studies, optimal thresholds exceeded 3.3 mcg/mL for achieving remission and 4.5 mcg/mL at week 26 for achieving endoscopic response, the researchers noted. They said that this discrepancy might reflect different time points for evaluation, assays for measuring ustekinumab, patient populations, and a lack of endoscopic data in their study. “The relatively small sample size and the short period of follow-up evaluation [were] substantial limitations” they acknowledged.
In this study, levels of CRP did not change significantly between weeks 0 and 16 among either responders or nonresponders. In contrast, fecal calprotectin levels dropped rapidly and significantly over time only in responders. Median fecal calprotectin levels were 1,612 mcg/g of stools at week 0 versus 374 mcg/g at week 4 and 339 mcg/g at week 8. The finding “confirms the value of this biomarker, as previously shown in inflammatory bowel disease with anti–tumor necrosis factor,” the researchers wrote.
The investigators did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
Learn more about therapeutic drug monitoring in IBD by reviewing the AGA Institute guideline at http://www.gastrojournal.org/article/S0016-5085(17)35963-2/fulltext.
SOURCE: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042. https://www.cghjournal.org/article/S1542-3565(19)30248-4/abstract
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Key clinical point: For patients with Crohn’s disease, therapeutic drug monitoring helped identify early nonresponse to ustekinumab induction.
Major finding: At week 8, median trough ustekinumab levels were 6 mcg/mL in week 16 responders and 1.3 mcg/mL in week 16 nonresponders (P = .03). An ustekinumab trough level of 2.0 mcg/mL or higher distinguished responders from nonresponders with an area under the receiver operating curve of 0.75.
Study details: Prospective study of 51 patients with active luminal Crohn’s disease.
Disclosures: The researchers did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
Source: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042.
Clock gene disruption might underlie IBD
Clock gene disruption may contribute to inflammatory bowel disease (IBD), and medical therapy might improve both gene expression and disease activity, suggest the results of a first-in-kind study.
Expression levels of five clock genes were significantly lower in inflamed intestinal mucosa from young, newly diagnosed, untreated patients with IBD, compared with intestinal mucosa from controls (P less than .05), wrote Yael Weintraub, MD, of Sourasky Tel-Aviv (Israel) Medical Center and associates in Clinical Gastroenterology and Hepatology. Uninflamed intestinal mucosa and peripheral white blood cells from patients also had significantly less clock gene mRNA, compared with corresponding samples from controls (P less than .05), which suggests that circadian clock disruption factors into the pathogenesis of IBD, the investigators said.
Sleep disturbances and shift work are significant risk factors for IBD and for disease flare. This prospective, 32-participant study assessed sleep patterns and mRNA expression levels for six genes associated with the circadian clock. Validated questionnaires found no significant differences in sleep timing, duration, tendency to snore, and “morningness” versus “eveningness” between patients and controls. However, patients tended to go to bed later and to rise later on weeknights than did controls (P = .08 and .06, respectively). This difference was more pronounced in patients with ulcerative colitis, compared with those with Crohn’s disease, the researchers noted.
In an adjusted analysis, five clock genes (CLOCK, BMAL1, CRY1, CRY2, and PER1) showed 3- to 66-fold lower expression in samples of inflamed intestinal mucosa from patients, compared with intestinal mucosa from controls. Expression of a sixth clock gene (PER2) also was lower but did not reach statistical significance. “Interestingly, noninflamed tissue obtained from IBD patients showed a similar significant reduction in clock gene expression, except for PER2, which showed threefold induction (P less than .001) compared to controls,” the researchers said.
Clock genes were expressed at lower levels in peripheral white blood cells from patients versus controls, and this disparity correlated with higher fecal calprotectin (but not C-reactive protein) levels. “The reduction in clock gene expression was more pronounced in ulcerative colitis compared to Crohn’s disease patients,” the researchers noted. Patients with ulcerative colitis had significantly reduced expression of all six clock genes, compared with controls, whereas patients with Crohn’s disease only had significantly reduced expression of CLOCK.
All 14 patients in the study had newly diagnosed, treatment-naive, endoscopically confirmed IBD. Most were in their early to mid-teens, and eight had Crohn’s disease, five had ulcerative colitis, and one had unclassified IBD. Endoscopic severity was usually mild or moderate. The 18 controls had negative endoscopy and histopathology findings but otherwise resembled patients in terms of age, body mass index, and sex distribution. Both patients and controls were recruited from the same tertiary care center.
“Importantly, a follow-up of a cohort of the IBD patients treated with 5-aminosalicylic acid (5-ASA) or anti-tumor necrosis factor (anti-TNF) revealed that their clinical score improved as well as their clock gene expression,” the investigators wrote. They called for “further research, clarifying the association between the circadian clock and IBD at the genetic and molecular levels, as well as interventional studies investigating the effect of circadian alterations on IBD therapy and course.”
The researchers did not report external funding sources. They reported having no conflicts of interest.
SOURCE: Weintraub Y et al. Clin Gastroenterol Hepatol. 2019 April 10. doi: 10.1016/j.cgh.2019.04.013.
Clock gene disruption may contribute to inflammatory bowel disease (IBD), and medical therapy might improve both gene expression and disease activity, suggest the results of a first-in-kind study.
Expression levels of five clock genes were significantly lower in inflamed intestinal mucosa from young, newly diagnosed, untreated patients with IBD, compared with intestinal mucosa from controls (P less than .05), wrote Yael Weintraub, MD, of Sourasky Tel-Aviv (Israel) Medical Center and associates in Clinical Gastroenterology and Hepatology. Uninflamed intestinal mucosa and peripheral white blood cells from patients also had significantly less clock gene mRNA, compared with corresponding samples from controls (P less than .05), which suggests that circadian clock disruption factors into the pathogenesis of IBD, the investigators said.
Sleep disturbances and shift work are significant risk factors for IBD and for disease flare. This prospective, 32-participant study assessed sleep patterns and mRNA expression levels for six genes associated with the circadian clock. Validated questionnaires found no significant differences in sleep timing, duration, tendency to snore, and “morningness” versus “eveningness” between patients and controls. However, patients tended to go to bed later and to rise later on weeknights than did controls (P = .08 and .06, respectively). This difference was more pronounced in patients with ulcerative colitis, compared with those with Crohn’s disease, the researchers noted.
In an adjusted analysis, five clock genes (CLOCK, BMAL1, CRY1, CRY2, and PER1) showed 3- to 66-fold lower expression in samples of inflamed intestinal mucosa from patients, compared with intestinal mucosa from controls. Expression of a sixth clock gene (PER2) also was lower but did not reach statistical significance. “Interestingly, noninflamed tissue obtained from IBD patients showed a similar significant reduction in clock gene expression, except for PER2, which showed threefold induction (P less than .001) compared to controls,” the researchers said.
Clock genes were expressed at lower levels in peripheral white blood cells from patients versus controls, and this disparity correlated with higher fecal calprotectin (but not C-reactive protein) levels. “The reduction in clock gene expression was more pronounced in ulcerative colitis compared to Crohn’s disease patients,” the researchers noted. Patients with ulcerative colitis had significantly reduced expression of all six clock genes, compared with controls, whereas patients with Crohn’s disease only had significantly reduced expression of CLOCK.
All 14 patients in the study had newly diagnosed, treatment-naive, endoscopically confirmed IBD. Most were in their early to mid-teens, and eight had Crohn’s disease, five had ulcerative colitis, and one had unclassified IBD. Endoscopic severity was usually mild or moderate. The 18 controls had negative endoscopy and histopathology findings but otherwise resembled patients in terms of age, body mass index, and sex distribution. Both patients and controls were recruited from the same tertiary care center.
“Importantly, a follow-up of a cohort of the IBD patients treated with 5-aminosalicylic acid (5-ASA) or anti-tumor necrosis factor (anti-TNF) revealed that their clinical score improved as well as their clock gene expression,” the investigators wrote. They called for “further research, clarifying the association between the circadian clock and IBD at the genetic and molecular levels, as well as interventional studies investigating the effect of circadian alterations on IBD therapy and course.”
The researchers did not report external funding sources. They reported having no conflicts of interest.
SOURCE: Weintraub Y et al. Clin Gastroenterol Hepatol. 2019 April 10. doi: 10.1016/j.cgh.2019.04.013.
Clock gene disruption may contribute to inflammatory bowel disease (IBD), and medical therapy might improve both gene expression and disease activity, suggest the results of a first-in-kind study.
Expression levels of five clock genes were significantly lower in inflamed intestinal mucosa from young, newly diagnosed, untreated patients with IBD, compared with intestinal mucosa from controls (P less than .05), wrote Yael Weintraub, MD, of Sourasky Tel-Aviv (Israel) Medical Center and associates in Clinical Gastroenterology and Hepatology. Uninflamed intestinal mucosa and peripheral white blood cells from patients also had significantly less clock gene mRNA, compared with corresponding samples from controls (P less than .05), which suggests that circadian clock disruption factors into the pathogenesis of IBD, the investigators said.
Sleep disturbances and shift work are significant risk factors for IBD and for disease flare. This prospective, 32-participant study assessed sleep patterns and mRNA expression levels for six genes associated with the circadian clock. Validated questionnaires found no significant differences in sleep timing, duration, tendency to snore, and “morningness” versus “eveningness” between patients and controls. However, patients tended to go to bed later and to rise later on weeknights than did controls (P = .08 and .06, respectively). This difference was more pronounced in patients with ulcerative colitis, compared with those with Crohn’s disease, the researchers noted.
In an adjusted analysis, five clock genes (CLOCK, BMAL1, CRY1, CRY2, and PER1) showed 3- to 66-fold lower expression in samples of inflamed intestinal mucosa from patients, compared with intestinal mucosa from controls. Expression of a sixth clock gene (PER2) also was lower but did not reach statistical significance. “Interestingly, noninflamed tissue obtained from IBD patients showed a similar significant reduction in clock gene expression, except for PER2, which showed threefold induction (P less than .001) compared to controls,” the researchers said.
Clock genes were expressed at lower levels in peripheral white blood cells from patients versus controls, and this disparity correlated with higher fecal calprotectin (but not C-reactive protein) levels. “The reduction in clock gene expression was more pronounced in ulcerative colitis compared to Crohn’s disease patients,” the researchers noted. Patients with ulcerative colitis had significantly reduced expression of all six clock genes, compared with controls, whereas patients with Crohn’s disease only had significantly reduced expression of CLOCK.
All 14 patients in the study had newly diagnosed, treatment-naive, endoscopically confirmed IBD. Most were in their early to mid-teens, and eight had Crohn’s disease, five had ulcerative colitis, and one had unclassified IBD. Endoscopic severity was usually mild or moderate. The 18 controls had negative endoscopy and histopathology findings but otherwise resembled patients in terms of age, body mass index, and sex distribution. Both patients and controls were recruited from the same tertiary care center.
“Importantly, a follow-up of a cohort of the IBD patients treated with 5-aminosalicylic acid (5-ASA) or anti-tumor necrosis factor (anti-TNF) revealed that their clinical score improved as well as their clock gene expression,” the investigators wrote. They called for “further research, clarifying the association between the circadian clock and IBD at the genetic and molecular levels, as well as interventional studies investigating the effect of circadian alterations on IBD therapy and course.”
The researchers did not report external funding sources. They reported having no conflicts of interest.
SOURCE: Weintraub Y et al. Clin Gastroenterol Hepatol. 2019 April 10. doi: 10.1016/j.cgh.2019.04.013.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
AGA Clinical Practice Update: Direct-acting antivirals and hepatocellular carcinoma
Achieving sustained virologic response to direct-acting antiviral therapy for chronic hepatitis C virus infection cuts lifetime hepatocellular carcinoma risk by approximately 70%, even when patients have baseline cirrhosis, experts wrote in Gastroenterology.

When used after curative-intent treatment for hepatocellular carcinoma, direct-acting antiviral (DAA) therapy also does not appear to make recurrent cancer more probable or more aggressive, wrote Amit G. Singal, MD, and associates in an American Gastroenterological Association clinical practice update. Studies that compared DAA therapy with either interferon-based therapy or no treatment have found “similar if not lower recurrence than the comparator groups,” they wrote. Rather, hepatocellular carcinoma is in itself highly recurrent: “While surgical resection and local ablative therapies are considered curative, [probability of] recurrence approaches 25%-35% within the first year, and 50%-60% within 2 years.”
Direct-acting antiviral therapy for chronic hepatitis C infection improves several aspects of liver health, but experts have debated whether and how these benefits affect the risk and behavior of hepatocellular carcinoma. To explore the issue, Dr. Singal, medical director of the liver tumor program and clinical chief of hepatology at UT Southwestern Medical Center in Dallas and associates reviewed published clinical trials, observational studies, and systematic reviews. Among 11 studies of more than 3,000 patients in five countries, sustained virologic response (SVR) to DAA therapy was associated with about a 70% reduction in the risk of liver cancer, even after adjustment for clinical and demographic variables. “The relative reduction is similar in patients with and without cirrhosis,” the experts wrote.
Since patients with fibrosis (F3) or cirrhosis are at highest risk for hepatocellular carcinoma, they should undergo baseline imaging and remain under indefinite post-SVR surveillance as long as they are eligible for potentially curative treatment, the practice update states. The experts recommended twice-yearly ultrasound, with or without serum alpha-fetoprotein, noting that current evidence supports neither shorter surveillance intervals nor alternative imaging modalities.
“The presence of active hepatocellular carcinoma is associated with a small but statistically significant decrease in SVR with DAA therapy,” the experts confirmed, based on the results of three studies. They recommended that, when possible, patients with hepatocellular carcinoma first receive curative-intent treatment, such as with liver resection or ablation. Direct-acting antiviral therapy can begin 4-6 months later, once there has been time to confirm response to hepatocellular carcinoma treatment.
For patients who are listed for liver transplantation, timing of DAA therapy “should be determined on a case-by-case basis with consideration of median wait times for the region, availability of HCV-positive organs, and degree of liver dysfunction,” they added. “For example, DAA therapy may be beneficial pretransplant for patients in regions with long wait times or limited hepatitis C virus–positive donor organ availability, whereas therapy may be delayed until posttransplant in regions with shorter wait times or a high proportion of hepatitis C virus–positive donor organs that would otherwise go unused.”
For patients with active intermediate or advanced liver cancer, it remains unclear whether DAA therapy is usually worth the costs and risks, they noted. This is because the likelihood of complete response is lower and the competing risk of death is higher than in patients with earlier-stage hepatocellular carcinoma. Pending further data, they recommend basing the decision on patients’ preferences, tumor burden, degree of liver dysfunction, and life expectancy. At their institutions, the researchers do not treat patients with DAA therapy unless their life expectancy exceeds 2 years.
The experts disclosed research funding from the National Cancer Institute, U.S. Veterans Administration, and the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Singal reported personal fees or research funding from AbbVie, Bayer, Bristol-Myers Squibb, Eisai, Exact Sciences, Exelixis, Gilead, Glycotest, Roche, and Wako Diagnostics. His coauthors disclosed ties to AbbVie, Allergan, Bristol-Myers Squibb, Conatus, Genfit, Gilead, Intercept, and Merck.
SOURCE: Singal AG et al. Gastroenterology. 2019 Mar 13. doi: 10.1053/j.gastro.2019.02.046.
Achieving sustained virologic response to direct-acting antiviral therapy for chronic hepatitis C virus infection cuts lifetime hepatocellular carcinoma risk by approximately 70%, even when patients have baseline cirrhosis, experts wrote in Gastroenterology.
When used after curative-intent treatment for hepatocellular carcinoma, direct-acting antiviral (DAA) therapy also does not appear to make recurrent cancer more probable or more aggressive, wrote Amit G. Singal, MD, and associates in an American Gastroenterological Association clinical practice update. Studies that compared DAA therapy with either interferon-based therapy or no treatment have found “similar if not lower recurrence than the comparator groups,” they wrote. Rather, hepatocellular carcinoma is in itself highly recurrent: “While surgical resection and local ablative therapies are considered curative, [probability of] recurrence approaches 25%-35% within the first year, and 50%-60% within 2 years.”
Direct-acting antiviral therapy for chronic hepatitis C infection improves several aspects of liver health, but experts have debated whether and how these benefits affect the risk and behavior of hepatocellular carcinoma. To explore the issue, Dr. Singal, medical director of the liver tumor program and clinical chief of hepatology at UT Southwestern Medical Center in Dallas and associates reviewed published clinical trials, observational studies, and systematic reviews. Among 11 studies of more than 3,000 patients in five countries, sustained virologic response (SVR) to DAA therapy was associated with about a 70% reduction in the risk of liver cancer, even after adjustment for clinical and demographic variables. “The relative reduction is similar in patients with and without cirrhosis,” the experts wrote.
Since patients with fibrosis (F3) or cirrhosis are at highest risk for hepatocellular carcinoma, they should undergo baseline imaging and remain under indefinite post-SVR surveillance as long as they are eligible for potentially curative treatment, the practice update states. The experts recommended twice-yearly ultrasound, with or without serum alpha-fetoprotein, noting that current evidence supports neither shorter surveillance intervals nor alternative imaging modalities.
“The presence of active hepatocellular carcinoma is associated with a small but statistically significant decrease in SVR with DAA therapy,” the experts confirmed, based on the results of three studies. They recommended that, when possible, patients with hepatocellular carcinoma first receive curative-intent treatment, such as with liver resection or ablation. Direct-acting antiviral therapy can begin 4-6 months later, once there has been time to confirm response to hepatocellular carcinoma treatment.
For patients who are listed for liver transplantation, timing of DAA therapy “should be determined on a case-by-case basis with consideration of median wait times for the region, availability of HCV-positive organs, and degree of liver dysfunction,” they added. “For example, DAA therapy may be beneficial pretransplant for patients in regions with long wait times or limited hepatitis C virus–positive donor organ availability, whereas therapy may be delayed until posttransplant in regions with shorter wait times or a high proportion of hepatitis C virus–positive donor organs that would otherwise go unused.”
For patients with active intermediate or advanced liver cancer, it remains unclear whether DAA therapy is usually worth the costs and risks, they noted. This is because the likelihood of complete response is lower and the competing risk of death is higher than in patients with earlier-stage hepatocellular carcinoma. Pending further data, they recommend basing the decision on patients’ preferences, tumor burden, degree of liver dysfunction, and life expectancy. At their institutions, the researchers do not treat patients with DAA therapy unless their life expectancy exceeds 2 years.
The experts disclosed research funding from the National Cancer Institute, U.S. Veterans Administration, and the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Singal reported personal fees or research funding from AbbVie, Bayer, Bristol-Myers Squibb, Eisai, Exact Sciences, Exelixis, Gilead, Glycotest, Roche, and Wako Diagnostics. His coauthors disclosed ties to AbbVie, Allergan, Bristol-Myers Squibb, Conatus, Genfit, Gilead, Intercept, and Merck.
SOURCE: Singal AG et al. Gastroenterology. 2019 Mar 13. doi: 10.1053/j.gastro.2019.02.046.
Achieving sustained virologic response to direct-acting antiviral therapy for chronic hepatitis C virus infection cuts lifetime hepatocellular carcinoma risk by approximately 70%, even when patients have baseline cirrhosis, experts wrote in Gastroenterology.
When used after curative-intent treatment for hepatocellular carcinoma, direct-acting antiviral (DAA) therapy also does not appear to make recurrent cancer more probable or more aggressive, wrote Amit G. Singal, MD, and associates in an American Gastroenterological Association clinical practice update. Studies that compared DAA therapy with either interferon-based therapy or no treatment have found “similar if not lower recurrence than the comparator groups,” they wrote. Rather, hepatocellular carcinoma is in itself highly recurrent: “While surgical resection and local ablative therapies are considered curative, [probability of] recurrence approaches 25%-35% within the first year, and 50%-60% within 2 years.”
Direct-acting antiviral therapy for chronic hepatitis C infection improves several aspects of liver health, but experts have debated whether and how these benefits affect the risk and behavior of hepatocellular carcinoma. To explore the issue, Dr. Singal, medical director of the liver tumor program and clinical chief of hepatology at UT Southwestern Medical Center in Dallas and associates reviewed published clinical trials, observational studies, and systematic reviews. Among 11 studies of more than 3,000 patients in five countries, sustained virologic response (SVR) to DAA therapy was associated with about a 70% reduction in the risk of liver cancer, even after adjustment for clinical and demographic variables. “The relative reduction is similar in patients with and without cirrhosis,” the experts wrote.
Since patients with fibrosis (F3) or cirrhosis are at highest risk for hepatocellular carcinoma, they should undergo baseline imaging and remain under indefinite post-SVR surveillance as long as they are eligible for potentially curative treatment, the practice update states. The experts recommended twice-yearly ultrasound, with or without serum alpha-fetoprotein, noting that current evidence supports neither shorter surveillance intervals nor alternative imaging modalities.
“The presence of active hepatocellular carcinoma is associated with a small but statistically significant decrease in SVR with DAA therapy,” the experts confirmed, based on the results of three studies. They recommended that, when possible, patients with hepatocellular carcinoma first receive curative-intent treatment, such as with liver resection or ablation. Direct-acting antiviral therapy can begin 4-6 months later, once there has been time to confirm response to hepatocellular carcinoma treatment.
For patients who are listed for liver transplantation, timing of DAA therapy “should be determined on a case-by-case basis with consideration of median wait times for the region, availability of HCV-positive organs, and degree of liver dysfunction,” they added. “For example, DAA therapy may be beneficial pretransplant for patients in regions with long wait times or limited hepatitis C virus–positive donor organ availability, whereas therapy may be delayed until posttransplant in regions with shorter wait times or a high proportion of hepatitis C virus–positive donor organs that would otherwise go unused.”
For patients with active intermediate or advanced liver cancer, it remains unclear whether DAA therapy is usually worth the costs and risks, they noted. This is because the likelihood of complete response is lower and the competing risk of death is higher than in patients with earlier-stage hepatocellular carcinoma. Pending further data, they recommend basing the decision on patients’ preferences, tumor burden, degree of liver dysfunction, and life expectancy. At their institutions, the researchers do not treat patients with DAA therapy unless their life expectancy exceeds 2 years.
The experts disclosed research funding from the National Cancer Institute, U.S. Veterans Administration, and the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Singal reported personal fees or research funding from AbbVie, Bayer, Bristol-Myers Squibb, Eisai, Exact Sciences, Exelixis, Gilead, Glycotest, Roche, and Wako Diagnostics. His coauthors disclosed ties to AbbVie, Allergan, Bristol-Myers Squibb, Conatus, Genfit, Gilead, Intercept, and Merck.
SOURCE: Singal AG et al. Gastroenterology. 2019 Mar 13. doi: 10.1053/j.gastro.2019.02.046.
FROM GASTROENTEROLOGY
Ulipristal acetate tops placebo for uterine leiomyomas
according to a study of the intention-to-treat populations of the randomized, double-blind, phase III VENUS I and VENUS II trials.
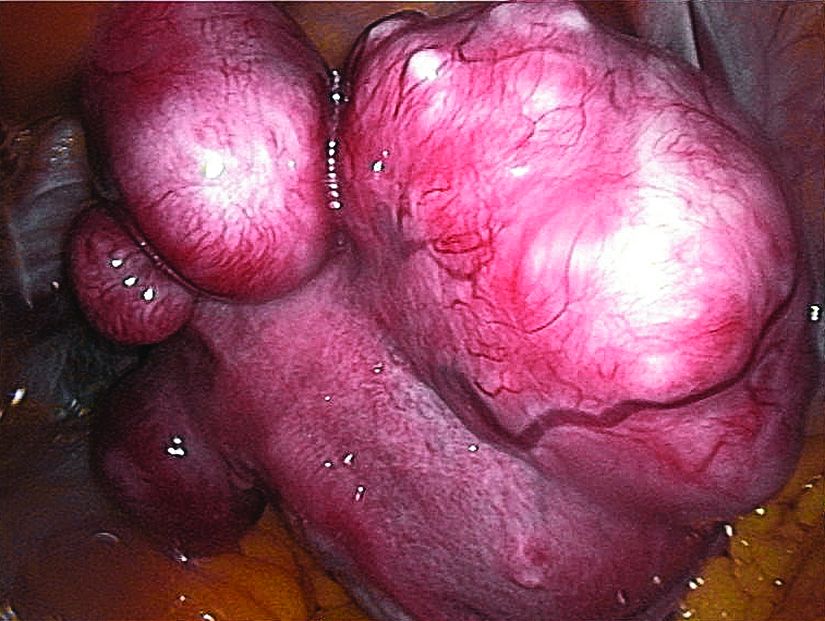
In these pivotal studies, ulipristal (Ella) at either 5 mg or 10 mg significantly improved both rate of and time to amenorrhea, noted Andrea S. Lukes, MD, of Carolina Women’s Research and Wellness Center in Durham, N.C. To assess effects on quality of life, she and her associates analyzed baseline and 12-week responses to the widely validated Uterine Fibroid Symptom Health-Related Quality of Life (UFS-QOL) questionnaire, which examined factors such as symptom severity, energy and mood, physical and social activities, self-consciousness, and sexual functioning.
Among 589 patients in the analysis, 169 received placebo, 215 received 5 mg ulipristal, and 205 received 10 mg ulipristal. At baseline, average total quality of life scores on UFS-QOL were 33 (standard deviation, 220), 32 (SD, 21), and 36 (SD, 23), respectively, the researchers wrote in Obstetrics & Gynecology.
After 12 weeks of treatment, both doses of ulipristal were associated with significantly greater improvements on all UFS-QOL scales, compared with placebo (P less than .001). For example, on a scale of 0-100, symptom severity improved by a mean of 23 with ulipristal 5 mg and by a mean of 30 with ulipristal 10 mg (both P less than .001 versus placebo).
“Although a small proportion of patients experienced no change or some worsening in these outcomes, the majority of women reported clear improvements; for example, more than 70% of patients in the ulipristal treatment arms achieved a meaningful improvement of 30 or more points on the Revised Activities subscale,” the researchers wrote.
Additionally, significantly greater improvements in physical and social activities were seen for both ulipristal doses, compared with placebo, from baseline to the end of treatment.
The VENUS II trial included two 12-week treatment courses. In this trial, women who switched from ulipristal to placebo experienced some worsening in quality of life, while those who switched from placebo to ulipristal improved their UFS-QOL scores, the investigators said. Patients who stayed on ulipristal throughout continued to benefit from one treatment course to the next.
The researchers concluded that the findings, “taken together with the significant improvements in amenorrhea, suggest that ulipristal is a promising, noninvasive treatment option for women suffering from symptomatic uterine leiomyomas.”
Allergan provided funding. Dr. Lukes disclosed ties to Allergan, AbbVie, Myovant, Merck, and several other companies. Four of the coauthors are employees of Allergan, and the two remaining coauthors had links to a number of pharmaceutical companies.
SOURCE: Lukes AS et al. Obstet Gynecol 2019;133 (5):869-78.
In this study, 77%-87% of women who received ulipristal acetate reported more than a 20-point improvement in health-related quality of life, compared with only 36% of placebo recipients, Joanna L. Hatfield, MD, wrote in an accompanying editorial.
“However, women with leiomyomas report a 51-point mean improvement after hysterectomy,” she noted. “Clinicians need to keep this difference in mind when counseling women with leiomyomas.”
Ulipristal can cause fatigue and weight gain leading to treatment discontinuation, she noted. Very rare cases of liver failure also have been reported, and there is no evidence that liver enzyme screening identifies patients at risk.
Nonetheless, for the approximately half of women with symptomatic leiomyomas who desire uterine-sparing treatment, selective progesterone receptor modulators like ulipristal offer “a noninvasive way to manage bleeding and bulk symptoms,” Dr. Hatfield said.
She advocated for long-term safety studies and a large pregnancy registry, calling ulipristal “neither a panacea nor a Pandora’s box,” but a choice that “lies somewhere in the middle, just [like] nearly all options that present themselves in a woman’s life.”
Dr. Hatfield is director of the fibroid program at Oregon Health & Science University in Portland. She did not report having conflicts of interest. She wrote an editorial accompanying the article by AS Lukes et al. (Obstet Gynecol. 2019 May;133[5]:867-8).
In this study, 77%-87% of women who received ulipristal acetate reported more than a 20-point improvement in health-related quality of life, compared with only 36% of placebo recipients, Joanna L. Hatfield, MD, wrote in an accompanying editorial.
“However, women with leiomyomas report a 51-point mean improvement after hysterectomy,” she noted. “Clinicians need to keep this difference in mind when counseling women with leiomyomas.”
Ulipristal can cause fatigue and weight gain leading to treatment discontinuation, she noted. Very rare cases of liver failure also have been reported, and there is no evidence that liver enzyme screening identifies patients at risk.
Nonetheless, for the approximately half of women with symptomatic leiomyomas who desire uterine-sparing treatment, selective progesterone receptor modulators like ulipristal offer “a noninvasive way to manage bleeding and bulk symptoms,” Dr. Hatfield said.
She advocated for long-term safety studies and a large pregnancy registry, calling ulipristal “neither a panacea nor a Pandora’s box,” but a choice that “lies somewhere in the middle, just [like] nearly all options that present themselves in a woman’s life.”
Dr. Hatfield is director of the fibroid program at Oregon Health & Science University in Portland. She did not report having conflicts of interest. She wrote an editorial accompanying the article by AS Lukes et al. (Obstet Gynecol. 2019 May;133[5]:867-8).
In this study, 77%-87% of women who received ulipristal acetate reported more than a 20-point improvement in health-related quality of life, compared with only 36% of placebo recipients, Joanna L. Hatfield, MD, wrote in an accompanying editorial.
“However, women with leiomyomas report a 51-point mean improvement after hysterectomy,” she noted. “Clinicians need to keep this difference in mind when counseling women with leiomyomas.”
Ulipristal can cause fatigue and weight gain leading to treatment discontinuation, she noted. Very rare cases of liver failure also have been reported, and there is no evidence that liver enzyme screening identifies patients at risk.
Nonetheless, for the approximately half of women with symptomatic leiomyomas who desire uterine-sparing treatment, selective progesterone receptor modulators like ulipristal offer “a noninvasive way to manage bleeding and bulk symptoms,” Dr. Hatfield said.
She advocated for long-term safety studies and a large pregnancy registry, calling ulipristal “neither a panacea nor a Pandora’s box,” but a choice that “lies somewhere in the middle, just [like] nearly all options that present themselves in a woman’s life.”
Dr. Hatfield is director of the fibroid program at Oregon Health & Science University in Portland. She did not report having conflicts of interest. She wrote an editorial accompanying the article by AS Lukes et al. (Obstet Gynecol. 2019 May;133[5]:867-8).
according to a study of the intention-to-treat populations of the randomized, double-blind, phase III VENUS I and VENUS II trials.
In these pivotal studies, ulipristal (Ella) at either 5 mg or 10 mg significantly improved both rate of and time to amenorrhea, noted Andrea S. Lukes, MD, of Carolina Women’s Research and Wellness Center in Durham, N.C. To assess effects on quality of life, she and her associates analyzed baseline and 12-week responses to the widely validated Uterine Fibroid Symptom Health-Related Quality of Life (UFS-QOL) questionnaire, which examined factors such as symptom severity, energy and mood, physical and social activities, self-consciousness, and sexual functioning.
Among 589 patients in the analysis, 169 received placebo, 215 received 5 mg ulipristal, and 205 received 10 mg ulipristal. At baseline, average total quality of life scores on UFS-QOL were 33 (standard deviation, 220), 32 (SD, 21), and 36 (SD, 23), respectively, the researchers wrote in Obstetrics & Gynecology.
After 12 weeks of treatment, both doses of ulipristal were associated with significantly greater improvements on all UFS-QOL scales, compared with placebo (P less than .001). For example, on a scale of 0-100, symptom severity improved by a mean of 23 with ulipristal 5 mg and by a mean of 30 with ulipristal 10 mg (both P less than .001 versus placebo).
“Although a small proportion of patients experienced no change or some worsening in these outcomes, the majority of women reported clear improvements; for example, more than 70% of patients in the ulipristal treatment arms achieved a meaningful improvement of 30 or more points on the Revised Activities subscale,” the researchers wrote.
Additionally, significantly greater improvements in physical and social activities were seen for both ulipristal doses, compared with placebo, from baseline to the end of treatment.
The VENUS II trial included two 12-week treatment courses. In this trial, women who switched from ulipristal to placebo experienced some worsening in quality of life, while those who switched from placebo to ulipristal improved their UFS-QOL scores, the investigators said. Patients who stayed on ulipristal throughout continued to benefit from one treatment course to the next.
The researchers concluded that the findings, “taken together with the significant improvements in amenorrhea, suggest that ulipristal is a promising, noninvasive treatment option for women suffering from symptomatic uterine leiomyomas.”
Allergan provided funding. Dr. Lukes disclosed ties to Allergan, AbbVie, Myovant, Merck, and several other companies. Four of the coauthors are employees of Allergan, and the two remaining coauthors had links to a number of pharmaceutical companies.
SOURCE: Lukes AS et al. Obstet Gynecol 2019;133 (5):869-78.
according to a study of the intention-to-treat populations of the randomized, double-blind, phase III VENUS I and VENUS II trials.
In these pivotal studies, ulipristal (Ella) at either 5 mg or 10 mg significantly improved both rate of and time to amenorrhea, noted Andrea S. Lukes, MD, of Carolina Women’s Research and Wellness Center in Durham, N.C. To assess effects on quality of life, she and her associates analyzed baseline and 12-week responses to the widely validated Uterine Fibroid Symptom Health-Related Quality of Life (UFS-QOL) questionnaire, which examined factors such as symptom severity, energy and mood, physical and social activities, self-consciousness, and sexual functioning.
Among 589 patients in the analysis, 169 received placebo, 215 received 5 mg ulipristal, and 205 received 10 mg ulipristal. At baseline, average total quality of life scores on UFS-QOL were 33 (standard deviation, 220), 32 (SD, 21), and 36 (SD, 23), respectively, the researchers wrote in Obstetrics & Gynecology.
After 12 weeks of treatment, both doses of ulipristal were associated with significantly greater improvements on all UFS-QOL scales, compared with placebo (P less than .001). For example, on a scale of 0-100, symptom severity improved by a mean of 23 with ulipristal 5 mg and by a mean of 30 with ulipristal 10 mg (both P less than .001 versus placebo).
“Although a small proportion of patients experienced no change or some worsening in these outcomes, the majority of women reported clear improvements; for example, more than 70% of patients in the ulipristal treatment arms achieved a meaningful improvement of 30 or more points on the Revised Activities subscale,” the researchers wrote.
Additionally, significantly greater improvements in physical and social activities were seen for both ulipristal doses, compared with placebo, from baseline to the end of treatment.
The VENUS II trial included two 12-week treatment courses. In this trial, women who switched from ulipristal to placebo experienced some worsening in quality of life, while those who switched from placebo to ulipristal improved their UFS-QOL scores, the investigators said. Patients who stayed on ulipristal throughout continued to benefit from one treatment course to the next.
The researchers concluded that the findings, “taken together with the significant improvements in amenorrhea, suggest that ulipristal is a promising, noninvasive treatment option for women suffering from symptomatic uterine leiomyomas.”
Allergan provided funding. Dr. Lukes disclosed ties to Allergan, AbbVie, Myovant, Merck, and several other companies. Four of the coauthors are employees of Allergan, and the two remaining coauthors had links to a number of pharmaceutical companies.
SOURCE: Lukes AS et al. Obstet Gynecol 2019;133 (5):869-78.
FROM OBSTETRICS & GYNECOLOGY
Key clinical point: For women with symptomatic uterine leiomyomas, ulipristal at either 5 mg or 10 mg significantly improved both the rate of and time to amenorrhea, compared with placebo.
Major finding: Patients who received 5 or 10 mg ulipristal showed significant improvements in Uterine Fibroid Symptom Health-Related Quality of Life scales, compared with those who received placebo (P less than .001).
Study details: VENUS I and II, 12-week randomized controlled trials of ulipristal acetate or placebo in 589 women with symptomatic uterine leiomyomas and abnormal uterine bleeding.
Disclosures: Allergan provided funding. Dr. Lukes disclosed ties to Allergan, AbbVie, Myovant, Merck, and several other companies. Four of the coauthors are employees of Allergan, and the two remaining coauthors had links to a number of pharmaceutical companies.
Source: Lukes AS et al. Obstet Gynecol. 2019 May;133(5):869-78.
Study compares tapering strategies in rheumatoid arthritis
Patients whose rheumatoid arthritis was in sustained remission had similar rates of flare for the first 9 months after they tapered off either their conventional synthetic disease-modifying antirheumatic drug (DMARD), or their tumor necrosis factor (TNF) inhibitor, researchers reported.

After the first year, first author Elise van Mulligen of Erasmus University Medical Center in Rotterdam, the Netherlands, and her associates found that flares rates were 10% lower among patients who first tapered conventional synthetic DMARDs, a difference that was not statistically significant. Because secondary endpoints also were similar between groups, patients should consider first tapering off their TNF inhibitor to save costs and reduce side effects, the researchers wrote in Annals of the Rheumatic Diseases.
Over the past decade, better drugs, treat-to-target approaches, and earlier disease detection have vastly improved outcomes in rheumatoid arthritis. As more patients achieve sustained remission, they are tapering off therapy in accordance with current guidelines. This multicenter, single-blinded, randomized trial (Tapering Strategies in Rheumatoid Arthritis [TARA]) is one of the first to compare tapering strategies, rather than looking at only whether tapering is feasible.
The study included 189 patients from the Netherlands whose rheumatoid arthritis was in sustained remission (Disease Activity Score [DAS] less than 2.4 and swollen joint count less than 1 for at least 3 months) on a conventional synthetic DMARD plus a TNF inhibitor. Patients were randomly assigned to either halve the conventional synthetic DMARD dose, or to double the TNF-inhibitor dosing interval. After 3 months, they cut the dose of their assigned taper medication to 25% of baseline. If they stayed in remission, they stopped the medication 3 months later. They avoided glucocorticoids throughout.
There were no serious adverse events related to tapering. Cumulative rates of flare at 1 year (DAS greater than 2.4 or swollen joint count greater than 1) were 33% for conventional synthetic DMARD taper (95% confidence interval, 24%-43%) and 43% (95% CI, 33%-53%) for TNF-inhibitor taper (P = .17). The two groups also had similar scores at 1 year on the DAS, Health Assessment Questionnaire-Disability Index, and European Quality of Life-5 Dimensions index.
The suggestion to first taper off TNF inhibitors reflects current European League Against Rheumatism guidelines, which advise first tapering glucocorticoids, then biologic DMARDS, and finally conventional synthetic DMARDs. “Our results and the fact that TNF blockers are more expensive than conventional synthetic DMARDs support the aforementioned tapering order,” the researchers concluded.
An unrestricted grant from ZonMW supported the work. The investigators reported having no conflicts of interest.
SOURCE: Mulligen E et al. Ann Rheum Dis. 2019 Apr 6. doi: 10.1136/annrheumdis-2018-214970.
Patients whose rheumatoid arthritis was in sustained remission had similar rates of flare for the first 9 months after they tapered off either their conventional synthetic disease-modifying antirheumatic drug (DMARD), or their tumor necrosis factor (TNF) inhibitor, researchers reported.
After the first year, first author Elise van Mulligen of Erasmus University Medical Center in Rotterdam, the Netherlands, and her associates found that flares rates were 10% lower among patients who first tapered conventional synthetic DMARDs, a difference that was not statistically significant. Because secondary endpoints also were similar between groups, patients should consider first tapering off their TNF inhibitor to save costs and reduce side effects, the researchers wrote in Annals of the Rheumatic Diseases.
Over the past decade, better drugs, treat-to-target approaches, and earlier disease detection have vastly improved outcomes in rheumatoid arthritis. As more patients achieve sustained remission, they are tapering off therapy in accordance with current guidelines. This multicenter, single-blinded, randomized trial (Tapering Strategies in Rheumatoid Arthritis [TARA]) is one of the first to compare tapering strategies, rather than looking at only whether tapering is feasible.
The study included 189 patients from the Netherlands whose rheumatoid arthritis was in sustained remission (Disease Activity Score [DAS] less than 2.4 and swollen joint count less than 1 for at least 3 months) on a conventional synthetic DMARD plus a TNF inhibitor. Patients were randomly assigned to either halve the conventional synthetic DMARD dose, or to double the TNF-inhibitor dosing interval. After 3 months, they cut the dose of their assigned taper medication to 25% of baseline. If they stayed in remission, they stopped the medication 3 months later. They avoided glucocorticoids throughout.
There were no serious adverse events related to tapering. Cumulative rates of flare at 1 year (DAS greater than 2.4 or swollen joint count greater than 1) were 33% for conventional synthetic DMARD taper (95% confidence interval, 24%-43%) and 43% (95% CI, 33%-53%) for TNF-inhibitor taper (P = .17). The two groups also had similar scores at 1 year on the DAS, Health Assessment Questionnaire-Disability Index, and European Quality of Life-5 Dimensions index.
The suggestion to first taper off TNF inhibitors reflects current European League Against Rheumatism guidelines, which advise first tapering glucocorticoids, then biologic DMARDS, and finally conventional synthetic DMARDs. “Our results and the fact that TNF blockers are more expensive than conventional synthetic DMARDs support the aforementioned tapering order,” the researchers concluded.
An unrestricted grant from ZonMW supported the work. The investigators reported having no conflicts of interest.
SOURCE: Mulligen E et al. Ann Rheum Dis. 2019 Apr 6. doi: 10.1136/annrheumdis-2018-214970.
Patients whose rheumatoid arthritis was in sustained remission had similar rates of flare for the first 9 months after they tapered off either their conventional synthetic disease-modifying antirheumatic drug (DMARD), or their tumor necrosis factor (TNF) inhibitor, researchers reported.
After the first year, first author Elise van Mulligen of Erasmus University Medical Center in Rotterdam, the Netherlands, and her associates found that flares rates were 10% lower among patients who first tapered conventional synthetic DMARDs, a difference that was not statistically significant. Because secondary endpoints also were similar between groups, patients should consider first tapering off their TNF inhibitor to save costs and reduce side effects, the researchers wrote in Annals of the Rheumatic Diseases.
Over the past decade, better drugs, treat-to-target approaches, and earlier disease detection have vastly improved outcomes in rheumatoid arthritis. As more patients achieve sustained remission, they are tapering off therapy in accordance with current guidelines. This multicenter, single-blinded, randomized trial (Tapering Strategies in Rheumatoid Arthritis [TARA]) is one of the first to compare tapering strategies, rather than looking at only whether tapering is feasible.
The study included 189 patients from the Netherlands whose rheumatoid arthritis was in sustained remission (Disease Activity Score [DAS] less than 2.4 and swollen joint count less than 1 for at least 3 months) on a conventional synthetic DMARD plus a TNF inhibitor. Patients were randomly assigned to either halve the conventional synthetic DMARD dose, or to double the TNF-inhibitor dosing interval. After 3 months, they cut the dose of their assigned taper medication to 25% of baseline. If they stayed in remission, they stopped the medication 3 months later. They avoided glucocorticoids throughout.
There were no serious adverse events related to tapering. Cumulative rates of flare at 1 year (DAS greater than 2.4 or swollen joint count greater than 1) were 33% for conventional synthetic DMARD taper (95% confidence interval, 24%-43%) and 43% (95% CI, 33%-53%) for TNF-inhibitor taper (P = .17). The two groups also had similar scores at 1 year on the DAS, Health Assessment Questionnaire-Disability Index, and European Quality of Life-5 Dimensions index.
The suggestion to first taper off TNF inhibitors reflects current European League Against Rheumatism guidelines, which advise first tapering glucocorticoids, then biologic DMARDS, and finally conventional synthetic DMARDs. “Our results and the fact that TNF blockers are more expensive than conventional synthetic DMARDs support the aforementioned tapering order,” the researchers concluded.
An unrestricted grant from ZonMW supported the work. The investigators reported having no conflicts of interest.
SOURCE: Mulligen E et al. Ann Rheum Dis. 2019 Apr 6. doi: 10.1136/annrheumdis-2018-214970.
FROM ANNALS OF THE RHEUMATIC DISEASES
Induction trough levels predicted ustekinumab response in Crohn’s disease
For patients with Crohn’s disease, therapeutic drug monitoring helped identify early primary nonresponders to induction with ustekinumab, according to researchers. The report is in Clinical Gastroenterology and Hepatology.
At week 8, median trough levels of ustekinumab were 6.0 mcg per mL (interquartile range, 3.1-8.0) among patients who achieved a primary response to induction at week 16, versus 1.3 mcg/mL (IQR, 0.9-5.6 ) among primary nonresponders (P = .03). An 8-week ustekinumab trough level cutoff of 2.0 mcg/mL distinguished week 16 responders from nonresponders with an area under the receiver operating curve (AUROC) of 0.75, wrote Ninon Soufflet of University Claude Bernard Lyon 1 in France, and associates. The researchers recommended “dedicated studies” to assess whether escalating the dose of ustekinumab can benefit patients with lower trough levels at week 8.
Few studies have explored biomarkers for response to ustekinumab induction therapy. Hence, the researchers assessed the relative utility of ustekinumab trough levels, C-reactive protein (CRP) levels, and fecal calprotectin levels for predicting early primary nonresponse. All 51 study participants had active luminal Crohn’s disease and received body weight–based intravenous infusions of ustekinumab at baseline, followed by subcutaneous injections of 90 mg. Primary nonresponders did not achieve steroid-free clinical and biochemical remission at week 16, defined as a Harvey-Bradshaw Index (HBI) of 4 points or less, a CRP level under 5 mg/L, and a fecal calprotectin level under 250 mcg/g. Week 16 was chosen to account for any delayed responders, the researchers noted.
A total of 32 patients (63%) achieved remission to ustekinumab induction therapy by week 16. An 8-week trough level of 2.0 mcg/mL was found to be optimal and distinguished primary nonresponders from responders with a sensitivity of 87%, a specificity of 66%, a positive predictive value of 82%, and a negative predictive value of 75%. In prior studies, optimal thresholds exceeded 3.3 mcg/mL for achieving remission and 4.5 mcg/mL at week 26 for achieving endoscopic response, the researchers noted. They said that this discrepancy might reflect different time points for evaluation, assays for measuring ustekinumab, patient populations, and a lack of endoscopic data in their study. “The relatively small sample size and the short period of follow-up evaluation [were] substantial limitations” they acknowledged.
In this study, levels of CRP did not change significantly between weeks 0 and 16 among either responders or nonresponders. In contrast, fecal calprotectin levels dropped rapidly and significantly over time only in responders. Median fecal calprotectin levels were 1,612 mcg/g of stools at week 0 versus 374 mcg/g at week 4 and 339 mcg/g at week 8. The finding “confirms the value of this biomarker, as previously shown in inflammatory bowel disease with anti–tumor necrosis factor,” the researchers wrote.
The investigators did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
SOURCE: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042. https://www.cghjournal.org/article/S1542-3565(19)30248-4/abstract
For patients with Crohn’s disease, therapeutic drug monitoring helped identify early primary nonresponders to induction with ustekinumab, according to researchers. The report is in Clinical Gastroenterology and Hepatology.
At week 8, median trough levels of ustekinumab were 6.0 mcg per mL (interquartile range, 3.1-8.0) among patients who achieved a primary response to induction at week 16, versus 1.3 mcg/mL (IQR, 0.9-5.6 ) among primary nonresponders (P = .03). An 8-week ustekinumab trough level cutoff of 2.0 mcg/mL distinguished week 16 responders from nonresponders with an area under the receiver operating curve (AUROC) of 0.75, wrote Ninon Soufflet of University Claude Bernard Lyon 1 in France, and associates. The researchers recommended “dedicated studies” to assess whether escalating the dose of ustekinumab can benefit patients with lower trough levels at week 8.
Few studies have explored biomarkers for response to ustekinumab induction therapy. Hence, the researchers assessed the relative utility of ustekinumab trough levels, C-reactive protein (CRP) levels, and fecal calprotectin levels for predicting early primary nonresponse. All 51 study participants had active luminal Crohn’s disease and received body weight–based intravenous infusions of ustekinumab at baseline, followed by subcutaneous injections of 90 mg. Primary nonresponders did not achieve steroid-free clinical and biochemical remission at week 16, defined as a Harvey-Bradshaw Index (HBI) of 4 points or less, a CRP level under 5 mg/L, and a fecal calprotectin level under 250 mcg/g. Week 16 was chosen to account for any delayed responders, the researchers noted.
A total of 32 patients (63%) achieved remission to ustekinumab induction therapy by week 16. An 8-week trough level of 2.0 mcg/mL was found to be optimal and distinguished primary nonresponders from responders with a sensitivity of 87%, a specificity of 66%, a positive predictive value of 82%, and a negative predictive value of 75%. In prior studies, optimal thresholds exceeded 3.3 mcg/mL for achieving remission and 4.5 mcg/mL at week 26 for achieving endoscopic response, the researchers noted. They said that this discrepancy might reflect different time points for evaluation, assays for measuring ustekinumab, patient populations, and a lack of endoscopic data in their study. “The relatively small sample size and the short period of follow-up evaluation [were] substantial limitations” they acknowledged.
In this study, levels of CRP did not change significantly between weeks 0 and 16 among either responders or nonresponders. In contrast, fecal calprotectin levels dropped rapidly and significantly over time only in responders. Median fecal calprotectin levels were 1,612 mcg/g of stools at week 0 versus 374 mcg/g at week 4 and 339 mcg/g at week 8. The finding “confirms the value of this biomarker, as previously shown in inflammatory bowel disease with anti–tumor necrosis factor,” the researchers wrote.
The investigators did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
SOURCE: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042. https://www.cghjournal.org/article/S1542-3565(19)30248-4/abstract
For patients with Crohn’s disease, therapeutic drug monitoring helped identify early primary nonresponders to induction with ustekinumab, according to researchers. The report is in Clinical Gastroenterology and Hepatology.
At week 8, median trough levels of ustekinumab were 6.0 mcg per mL (interquartile range, 3.1-8.0) among patients who achieved a primary response to induction at week 16, versus 1.3 mcg/mL (IQR, 0.9-5.6 ) among primary nonresponders (P = .03). An 8-week ustekinumab trough level cutoff of 2.0 mcg/mL distinguished week 16 responders from nonresponders with an area under the receiver operating curve (AUROC) of 0.75, wrote Ninon Soufflet of University Claude Bernard Lyon 1 in France, and associates. The researchers recommended “dedicated studies” to assess whether escalating the dose of ustekinumab can benefit patients with lower trough levels at week 8.
Few studies have explored biomarkers for response to ustekinumab induction therapy. Hence, the researchers assessed the relative utility of ustekinumab trough levels, C-reactive protein (CRP) levels, and fecal calprotectin levels for predicting early primary nonresponse. All 51 study participants had active luminal Crohn’s disease and received body weight–based intravenous infusions of ustekinumab at baseline, followed by subcutaneous injections of 90 mg. Primary nonresponders did not achieve steroid-free clinical and biochemical remission at week 16, defined as a Harvey-Bradshaw Index (HBI) of 4 points or less, a CRP level under 5 mg/L, and a fecal calprotectin level under 250 mcg/g. Week 16 was chosen to account for any delayed responders, the researchers noted.
A total of 32 patients (63%) achieved remission to ustekinumab induction therapy by week 16. An 8-week trough level of 2.0 mcg/mL was found to be optimal and distinguished primary nonresponders from responders with a sensitivity of 87%, a specificity of 66%, a positive predictive value of 82%, and a negative predictive value of 75%. In prior studies, optimal thresholds exceeded 3.3 mcg/mL for achieving remission and 4.5 mcg/mL at week 26 for achieving endoscopic response, the researchers noted. They said that this discrepancy might reflect different time points for evaluation, assays for measuring ustekinumab, patient populations, and a lack of endoscopic data in their study. “The relatively small sample size and the short period of follow-up evaluation [were] substantial limitations” they acknowledged.
In this study, levels of CRP did not change significantly between weeks 0 and 16 among either responders or nonresponders. In contrast, fecal calprotectin levels dropped rapidly and significantly over time only in responders. Median fecal calprotectin levels were 1,612 mcg/g of stools at week 0 versus 374 mcg/g at week 4 and 339 mcg/g at week 8. The finding “confirms the value of this biomarker, as previously shown in inflammatory bowel disease with anti–tumor necrosis factor,” the researchers wrote.
The investigators did not acknowledge external funding sources. Dr. Soufflet reported having no conflicts of interest. The senior author and three coinvestigators disclosed ties to MSD, AbbVie, Tillots, and several other pharmaceutical companies.
SOURCE: Soufflet N et al. Clin Gastroenterol Hepatol. 2019 Mar 6. doi: 10.1016/j.cgh.2019.02.042. https://www.cghjournal.org/article/S1542-3565(19)30248-4/abstract
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Tailoring the Mediterranean diet for NAFLD
Adults with nonalcoholic fatty liver disease (NAFLD) were more likely to implement the Mediterranean diet when they had greater nutritional knowledge and skills, family support, nutritional care, and positive reinforcement in the media, according to an in-depth study of 19 patients.

Barriers to adopting the diet included “an obesogenic environment, life stressors, and demand for convenience. Poor understanding of the causes and significance of NAFLD adversely affected readiness to change dietary habits,” wrote Laura Haigh of Newcastle University in Newcastle Upon Tyne, England, and associates. The study, which included both standard quantitative methods and semistructured interviews, was published in Clinical Gastroenterology and Hepatology.
The Mediterranean diet emphasizes vegetables, legumes, fish, fruits, whole grains, nuts, and olive oil in lieu of processed foods, sweets, saturated fats, and red meat. This diet has been definitively shown to improve insulin sensitivity and steatosis, even when patients do not lose weight. This has sparked interest in its use for NAFLD disease, but keys to its successful adoption in Northern Europe are not well understood.
Therefore, the researchers recruited 19 NAFLD patients from a tertiary care center in the United Kingdom for a 12-week Mediterranean diet intervention. Most were female, white, in their late 50s, obese, and had type 2 diabetes. “Participants were taught behavioral strategies through the provision of shopping lists, meal planners, and recipes. No advice was given on calorie allowances or physical activities,” the investigators noted.
By using a 14-point assessment tool, they found that dietary adherence rose significantly at 12 weeks, compared with baseline (P = .006). In all, 79% of patients lost weight (mean, 2.4 kg; P = .001 versus baseline), and 72% significantly increased their serum level of HDL cholesterol. Interviews linked successful adoption of the diet with diverse factors, such as believing that NAFLD is lifestyle associated, realizing that healthier nutrition can improve health outcomes, and having access to transportation and budget grocery stories. Patients generally saw the Mediterranean diet as flexible and affordable, but they struggled to adopt it if they worked irregular hours, experienced substantial life stress or were very busy, or tended to eat for self-reward or self-comfort.
Other cited barriers included “diet saboteurs” (including spouses), the plethora of unhealthy foods available in patients’ environments, low nutritional or medical knowledge, and cultural, social, or taste incompatibility, the researchers reported. Taken together, the findings underscore “the futility of a one-size-fits-all approach” when implementing the Mediterranean diet in this population, they concluded. Instead, their patients valued a collaborative, tailored approach – ideally one that incorporated in-person and group-based treatment, as well as online support.
Funders included the North East of England hub of the Allied Health Professions Research Network, the Elucidating Pathways of Steatohepatitis consortium, the Horizon 2020 Framework Program of the European Union, and the Newcastle NIHR Biomedical Research Centre. The researchers reported having no conflicts of interest.
SOURCE: Haigh L et al. Clin Gastroenterol Hepatol. 2018 Oct 31. doi: 10.1016/j.cgh.2018.10.044.
Adults with nonalcoholic fatty liver disease (NAFLD) were more likely to implement the Mediterranean diet when they had greater nutritional knowledge and skills, family support, nutritional care, and positive reinforcement in the media, according to an in-depth study of 19 patients.
Barriers to adopting the diet included “an obesogenic environment, life stressors, and demand for convenience. Poor understanding of the causes and significance of NAFLD adversely affected readiness to change dietary habits,” wrote Laura Haigh of Newcastle University in Newcastle Upon Tyne, England, and associates. The study, which included both standard quantitative methods and semistructured interviews, was published in Clinical Gastroenterology and Hepatology.
The Mediterranean diet emphasizes vegetables, legumes, fish, fruits, whole grains, nuts, and olive oil in lieu of processed foods, sweets, saturated fats, and red meat. This diet has been definitively shown to improve insulin sensitivity and steatosis, even when patients do not lose weight. This has sparked interest in its use for NAFLD disease, but keys to its successful adoption in Northern Europe are not well understood.
Therefore, the researchers recruited 19 NAFLD patients from a tertiary care center in the United Kingdom for a 12-week Mediterranean diet intervention. Most were female, white, in their late 50s, obese, and had type 2 diabetes. “Participants were taught behavioral strategies through the provision of shopping lists, meal planners, and recipes. No advice was given on calorie allowances or physical activities,” the investigators noted.
By using a 14-point assessment tool, they found that dietary adherence rose significantly at 12 weeks, compared with baseline (P = .006). In all, 79% of patients lost weight (mean, 2.4 kg; P = .001 versus baseline), and 72% significantly increased their serum level of HDL cholesterol. Interviews linked successful adoption of the diet with diverse factors, such as believing that NAFLD is lifestyle associated, realizing that healthier nutrition can improve health outcomes, and having access to transportation and budget grocery stories. Patients generally saw the Mediterranean diet as flexible and affordable, but they struggled to adopt it if they worked irregular hours, experienced substantial life stress or were very busy, or tended to eat for self-reward or self-comfort.
Other cited barriers included “diet saboteurs” (including spouses), the plethora of unhealthy foods available in patients’ environments, low nutritional or medical knowledge, and cultural, social, or taste incompatibility, the researchers reported. Taken together, the findings underscore “the futility of a one-size-fits-all approach” when implementing the Mediterranean diet in this population, they concluded. Instead, their patients valued a collaborative, tailored approach – ideally one that incorporated in-person and group-based treatment, as well as online support.
Funders included the North East of England hub of the Allied Health Professions Research Network, the Elucidating Pathways of Steatohepatitis consortium, the Horizon 2020 Framework Program of the European Union, and the Newcastle NIHR Biomedical Research Centre. The researchers reported having no conflicts of interest.
SOURCE: Haigh L et al. Clin Gastroenterol Hepatol. 2018 Oct 31. doi: 10.1016/j.cgh.2018.10.044.
Adults with nonalcoholic fatty liver disease (NAFLD) were more likely to implement the Mediterranean diet when they had greater nutritional knowledge and skills, family support, nutritional care, and positive reinforcement in the media, according to an in-depth study of 19 patients.
Barriers to adopting the diet included “an obesogenic environment, life stressors, and demand for convenience. Poor understanding of the causes and significance of NAFLD adversely affected readiness to change dietary habits,” wrote Laura Haigh of Newcastle University in Newcastle Upon Tyne, England, and associates. The study, which included both standard quantitative methods and semistructured interviews, was published in Clinical Gastroenterology and Hepatology.
The Mediterranean diet emphasizes vegetables, legumes, fish, fruits, whole grains, nuts, and olive oil in lieu of processed foods, sweets, saturated fats, and red meat. This diet has been definitively shown to improve insulin sensitivity and steatosis, even when patients do not lose weight. This has sparked interest in its use for NAFLD disease, but keys to its successful adoption in Northern Europe are not well understood.
Therefore, the researchers recruited 19 NAFLD patients from a tertiary care center in the United Kingdom for a 12-week Mediterranean diet intervention. Most were female, white, in their late 50s, obese, and had type 2 diabetes. “Participants were taught behavioral strategies through the provision of shopping lists, meal planners, and recipes. No advice was given on calorie allowances or physical activities,” the investigators noted.
By using a 14-point assessment tool, they found that dietary adherence rose significantly at 12 weeks, compared with baseline (P = .006). In all, 79% of patients lost weight (mean, 2.4 kg; P = .001 versus baseline), and 72% significantly increased their serum level of HDL cholesterol. Interviews linked successful adoption of the diet with diverse factors, such as believing that NAFLD is lifestyle associated, realizing that healthier nutrition can improve health outcomes, and having access to transportation and budget grocery stories. Patients generally saw the Mediterranean diet as flexible and affordable, but they struggled to adopt it if they worked irregular hours, experienced substantial life stress or were very busy, or tended to eat for self-reward or self-comfort.
Other cited barriers included “diet saboteurs” (including spouses), the plethora of unhealthy foods available in patients’ environments, low nutritional or medical knowledge, and cultural, social, or taste incompatibility, the researchers reported. Taken together, the findings underscore “the futility of a one-size-fits-all approach” when implementing the Mediterranean diet in this population, they concluded. Instead, their patients valued a collaborative, tailored approach – ideally one that incorporated in-person and group-based treatment, as well as online support.
Funders included the North East of England hub of the Allied Health Professions Research Network, the Elucidating Pathways of Steatohepatitis consortium, the Horizon 2020 Framework Program of the European Union, and the Newcastle NIHR Biomedical Research Centre. The researchers reported having no conflicts of interest.
SOURCE: Haigh L et al. Clin Gastroenterol Hepatol. 2018 Oct 31. doi: 10.1016/j.cgh.2018.10.044.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Positive psoriatic arthritis screens occur often in psoriasis patients
One out of eight patients with psoriasis had a positive screen for possibly undiagnosed psoriatic arthritis, according to an analysis of data from a prospective registry.

The finding highlights the need for better psoriatic arthritis screening among patients with psoriasis, said Philip J. Mease, MD, of the University of Washington, Seattle, and associates. The simple, five-question Psoriasis Epidemiology Screening Tool (PEST) used in this study could be deployed in general or dermatology practices to identify psoriasis patients who might need a rheumatology referral, they wrote. The report is in the Journal of the European Academy of Dermatology and Venereology.
Up to 30% of patients with psoriasis have comorbid psoriatic arthritis, but many such cases go undiagnosed, and even a 6-month diagnostic delay can worsen peripheral joint erosion and physical disability.
This study included 1,516 patients with psoriasis seen at 114 private and academic practices in 34 states that participate in the independent, prospective Corrona Psoriasis Registry. A total of 904 patients without dermatologist-reported psoriatic arthritis responded to the validated PEST, which assesses risk of psoriatic arthritis by asking whether the test taker has been told by a doctor that he or she has arthritis and whether they have experienced swollen joints, heel pain, pronounced and unexplained swelling of a finger or toe, and pitting of the fingernails or toenails. Each “yes” response is worth 1 point, and total scores of 3 or higher indicate risk of psoriatic arthritis. A total of 112 (12.4%) had a score of 3 or higher.
The average age of patients who met this threshold was 53 years, 4 years older than those who did not (P = .02). Patients with PEST scores of 3 or more also had a significantly longer duration of psoriasis and were significantly more likely to have nail disease and a family history of psoriasis. Demographically, they were more likely to be white, female, and unemployed. They had significantly higher rates of several comorbidities, including depression and anxiety, cardiovascular disease, obesity, and serious infections. Finally, they reported having significantly more pain and fatigue and significantly worse health-related quality of life.
The study did not account for possible confounding. “Further research is needed to characterize patients by individual PEST score and to assess outcomes over time,” the researchers wrote. “The use of screening tools can be beneficial in the detection of psoriatic arthritis, and comprehensive efforts to validate them in multiple clinical settings must continue, along with collection of critical feedback from patients and clinicians.”
Corrona and Novartis designed and helped conduct the study. Novartis, the chief funder, participated in data analysis and manuscript review. Dr. Mease disclosed research funding from Novartis and several other pharmaceutical companies. He also disclosed consulting and speakers bureau fees from Novartis, Corrona, and several other companies.
SOURCE: Mease PJ et al. J Eur Acad Dermatol Venereol. 2019 Mar 5. doi: 10.1111/jdv.15443.
One out of eight patients with psoriasis had a positive screen for possibly undiagnosed psoriatic arthritis, according to an analysis of data from a prospective registry.
The finding highlights the need for better psoriatic arthritis screening among patients with psoriasis, said Philip J. Mease, MD, of the University of Washington, Seattle, and associates. The simple, five-question Psoriasis Epidemiology Screening Tool (PEST) used in this study could be deployed in general or dermatology practices to identify psoriasis patients who might need a rheumatology referral, they wrote. The report is in the Journal of the European Academy of Dermatology and Venereology.
Up to 30% of patients with psoriasis have comorbid psoriatic arthritis, but many such cases go undiagnosed, and even a 6-month diagnostic delay can worsen peripheral joint erosion and physical disability.
This study included 1,516 patients with psoriasis seen at 114 private and academic practices in 34 states that participate in the independent, prospective Corrona Psoriasis Registry. A total of 904 patients without dermatologist-reported psoriatic arthritis responded to the validated PEST, which assesses risk of psoriatic arthritis by asking whether the test taker has been told by a doctor that he or she has arthritis and whether they have experienced swollen joints, heel pain, pronounced and unexplained swelling of a finger or toe, and pitting of the fingernails or toenails. Each “yes” response is worth 1 point, and total scores of 3 or higher indicate risk of psoriatic arthritis. A total of 112 (12.4%) had a score of 3 or higher.
The average age of patients who met this threshold was 53 years, 4 years older than those who did not (P = .02). Patients with PEST scores of 3 or more also had a significantly longer duration of psoriasis and were significantly more likely to have nail disease and a family history of psoriasis. Demographically, they were more likely to be white, female, and unemployed. They had significantly higher rates of several comorbidities, including depression and anxiety, cardiovascular disease, obesity, and serious infections. Finally, they reported having significantly more pain and fatigue and significantly worse health-related quality of life.
The study did not account for possible confounding. “Further research is needed to characterize patients by individual PEST score and to assess outcomes over time,” the researchers wrote. “The use of screening tools can be beneficial in the detection of psoriatic arthritis, and comprehensive efforts to validate them in multiple clinical settings must continue, along with collection of critical feedback from patients and clinicians.”
Corrona and Novartis designed and helped conduct the study. Novartis, the chief funder, participated in data analysis and manuscript review. Dr. Mease disclosed research funding from Novartis and several other pharmaceutical companies. He also disclosed consulting and speakers bureau fees from Novartis, Corrona, and several other companies.
SOURCE: Mease PJ et al. J Eur Acad Dermatol Venereol. 2019 Mar 5. doi: 10.1111/jdv.15443.
One out of eight patients with psoriasis had a positive screen for possibly undiagnosed psoriatic arthritis, according to an analysis of data from a prospective registry.
The finding highlights the need for better psoriatic arthritis screening among patients with psoriasis, said Philip J. Mease, MD, of the University of Washington, Seattle, and associates. The simple, five-question Psoriasis Epidemiology Screening Tool (PEST) used in this study could be deployed in general or dermatology practices to identify psoriasis patients who might need a rheumatology referral, they wrote. The report is in the Journal of the European Academy of Dermatology and Venereology.
Up to 30% of patients with psoriasis have comorbid psoriatic arthritis, but many such cases go undiagnosed, and even a 6-month diagnostic delay can worsen peripheral joint erosion and physical disability.
This study included 1,516 patients with psoriasis seen at 114 private and academic practices in 34 states that participate in the independent, prospective Corrona Psoriasis Registry. A total of 904 patients without dermatologist-reported psoriatic arthritis responded to the validated PEST, which assesses risk of psoriatic arthritis by asking whether the test taker has been told by a doctor that he or she has arthritis and whether they have experienced swollen joints, heel pain, pronounced and unexplained swelling of a finger or toe, and pitting of the fingernails or toenails. Each “yes” response is worth 1 point, and total scores of 3 or higher indicate risk of psoriatic arthritis. A total of 112 (12.4%) had a score of 3 or higher.
The average age of patients who met this threshold was 53 years, 4 years older than those who did not (P = .02). Patients with PEST scores of 3 or more also had a significantly longer duration of psoriasis and were significantly more likely to have nail disease and a family history of psoriasis. Demographically, they were more likely to be white, female, and unemployed. They had significantly higher rates of several comorbidities, including depression and anxiety, cardiovascular disease, obesity, and serious infections. Finally, they reported having significantly more pain and fatigue and significantly worse health-related quality of life.
The study did not account for possible confounding. “Further research is needed to characterize patients by individual PEST score and to assess outcomes over time,” the researchers wrote. “The use of screening tools can be beneficial in the detection of psoriatic arthritis, and comprehensive efforts to validate them in multiple clinical settings must continue, along with collection of critical feedback from patients and clinicians.”
Corrona and Novartis designed and helped conduct the study. Novartis, the chief funder, participated in data analysis and manuscript review. Dr. Mease disclosed research funding from Novartis and several other pharmaceutical companies. He also disclosed consulting and speakers bureau fees from Novartis, Corrona, and several other companies.
SOURCE: Mease PJ et al. J Eur Acad Dermatol Venereol. 2019 Mar 5. doi: 10.1111/jdv.15443.
FROM THE JOURNAL OF THE EUROPEAN ACADEMY OF DERMATOLOGY AND VENEREOLOGY
Gene therapy restored immunity in newly diagnosed SCID-X1
For infants with newly diagnosed X-linked severe combined immunodeficiency (SCID-X1), lentiviral gene therapy and targeted busulfan conditioning successfully induced multilineage engraftment of transduced cells, researchers reported.

By 3-4 months after infusion, seven of eight patients had normal numbers of CD3+, CD4+, and naive CD4+ T cells; normal counts of natural killer (NK) cells; and vector marking of T cells, B cells, NK cells, myeloid cells, and bone marrow progenitors, Ewelina Mamcarz, MD, of St. Jude Children’s Research Hospital in Memphis, and her associates reported in the New England Journal of Medicine.
The eighth infant at first lacked a sufficient T-cell response but responded to a boost of gene-corrected cells without busulfan conditioning.
By 6-12 months after infusion, IgM levels also had normalized in seven of the eight infants and showed polyclonal patterns without clonal dominance, according to the investigators. Among four infants who were able to stop intravenous immunoglobulin therapy, three responded to vaccinations with tetanus, diphtheria, pertussis, polio, and pneumococcal polysaccharide. Such restoration of humoral immunity “has not been achieved in previously reported trials of gene therapy for infants with newly diagnosed SCID-X1,” wrote the investigators of this dual-center, phase 1/2 study.
X-linked severe combined immunodeficiency – “bubble boy disease” – is characterized by a lack of T cells, NK cells, and B cells, and is caused by mutations in IL2RG. Some 80% of affected infants have no matched sibling donor for hematopoietic stem cell transplantation, and transplantation from other donors can produce an inadequate response and graft-versus-host disease. Prior attempts at gene therapy with gamma-retroviral vectors had led to vector-induced leukemia or had failed to induce humoral immunity or normal NK cell production.
“Our new lentiviral vector gene therapy combined with nonmyeloablative busulfan conditioning has been successful in restoring immunity in five patients 7-23 years of age in whom a previous allogeneic hematopoietic stem cell transplantation for SCID-X1 had failed,” the investigators wrote. “We hypothesized that the combination of this lentiviral vector and low-exposure busulfan administered by means of pharmacokinetic dose targeting would be safe and effective as the primary treatment in infants with newly diagnosed SCID-X1.”
Their protocol included one to two daily intravenous doses of busulfan, targeting a cumulative area under the curve of 22 mg per hr/L. They calculated the first dose by weight and age using a population-based pharmacokinetic model and adjusted the second dose based on first-dose pharmacokinetics.
After a median of 16.4 months, all infants continued to grow normally and cleared previous infections, and there were no unanticipated side effects from bone marrow harvest, busulfan conditioning, or cell infusion.
“It is hoped that durable, complete adaptive immunity will be achieved in the majority of the patients over time,” the researchers wrote.
They continue to follow the patients to assess therapeutic safety, immune durability, and persistence of the transferred gene in hematopoietic and immune cells.
Study funders included the American Lebanese Syrian Associated Charities, the National Institutes of Health, the California Institute of Regenerative Medicine, and the Assisi Foundation of Memphis. St. Jude Children’s Research Hospital has licensed the gene therapy and partnered with Mustang Bio to develop and commercialize it. Dr. Mamcarz reported receiving grant support from the study funders.
SOURCE: Mamcarz E et al. N Engl J Med. 2019; 380:1525-34.
For infants with newly diagnosed X-linked severe combined immunodeficiency (SCID-X1), lentiviral gene therapy and targeted busulfan conditioning successfully induced multilineage engraftment of transduced cells, researchers reported.
By 3-4 months after infusion, seven of eight patients had normal numbers of CD3+, CD4+, and naive CD4+ T cells; normal counts of natural killer (NK) cells; and vector marking of T cells, B cells, NK cells, myeloid cells, and bone marrow progenitors, Ewelina Mamcarz, MD, of St. Jude Children’s Research Hospital in Memphis, and her associates reported in the New England Journal of Medicine.
The eighth infant at first lacked a sufficient T-cell response but responded to a boost of gene-corrected cells without busulfan conditioning.
By 6-12 months after infusion, IgM levels also had normalized in seven of the eight infants and showed polyclonal patterns without clonal dominance, according to the investigators. Among four infants who were able to stop intravenous immunoglobulin therapy, three responded to vaccinations with tetanus, diphtheria, pertussis, polio, and pneumococcal polysaccharide. Such restoration of humoral immunity “has not been achieved in previously reported trials of gene therapy for infants with newly diagnosed SCID-X1,” wrote the investigators of this dual-center, phase 1/2 study.
X-linked severe combined immunodeficiency – “bubble boy disease” – is characterized by a lack of T cells, NK cells, and B cells, and is caused by mutations in IL2RG. Some 80% of affected infants have no matched sibling donor for hematopoietic stem cell transplantation, and transplantation from other donors can produce an inadequate response and graft-versus-host disease. Prior attempts at gene therapy with gamma-retroviral vectors had led to vector-induced leukemia or had failed to induce humoral immunity or normal NK cell production.
“Our new lentiviral vector gene therapy combined with nonmyeloablative busulfan conditioning has been successful in restoring immunity in five patients 7-23 years of age in whom a previous allogeneic hematopoietic stem cell transplantation for SCID-X1 had failed,” the investigators wrote. “We hypothesized that the combination of this lentiviral vector and low-exposure busulfan administered by means of pharmacokinetic dose targeting would be safe and effective as the primary treatment in infants with newly diagnosed SCID-X1.”
Their protocol included one to two daily intravenous doses of busulfan, targeting a cumulative area under the curve of 22 mg per hr/L. They calculated the first dose by weight and age using a population-based pharmacokinetic model and adjusted the second dose based on first-dose pharmacokinetics.
After a median of 16.4 months, all infants continued to grow normally and cleared previous infections, and there were no unanticipated side effects from bone marrow harvest, busulfan conditioning, or cell infusion.
“It is hoped that durable, complete adaptive immunity will be achieved in the majority of the patients over time,” the researchers wrote.
They continue to follow the patients to assess therapeutic safety, immune durability, and persistence of the transferred gene in hematopoietic and immune cells.
Study funders included the American Lebanese Syrian Associated Charities, the National Institutes of Health, the California Institute of Regenerative Medicine, and the Assisi Foundation of Memphis. St. Jude Children’s Research Hospital has licensed the gene therapy and partnered with Mustang Bio to develop and commercialize it. Dr. Mamcarz reported receiving grant support from the study funders.
SOURCE: Mamcarz E et al. N Engl J Med. 2019; 380:1525-34.
For infants with newly diagnosed X-linked severe combined immunodeficiency (SCID-X1), lentiviral gene therapy and targeted busulfan conditioning successfully induced multilineage engraftment of transduced cells, researchers reported.
By 3-4 months after infusion, seven of eight patients had normal numbers of CD3+, CD4+, and naive CD4+ T cells; normal counts of natural killer (NK) cells; and vector marking of T cells, B cells, NK cells, myeloid cells, and bone marrow progenitors, Ewelina Mamcarz, MD, of St. Jude Children’s Research Hospital in Memphis, and her associates reported in the New England Journal of Medicine.
The eighth infant at first lacked a sufficient T-cell response but responded to a boost of gene-corrected cells without busulfan conditioning.
By 6-12 months after infusion, IgM levels also had normalized in seven of the eight infants and showed polyclonal patterns without clonal dominance, according to the investigators. Among four infants who were able to stop intravenous immunoglobulin therapy, three responded to vaccinations with tetanus, diphtheria, pertussis, polio, and pneumococcal polysaccharide. Such restoration of humoral immunity “has not been achieved in previously reported trials of gene therapy for infants with newly diagnosed SCID-X1,” wrote the investigators of this dual-center, phase 1/2 study.
X-linked severe combined immunodeficiency – “bubble boy disease” – is characterized by a lack of T cells, NK cells, and B cells, and is caused by mutations in IL2RG. Some 80% of affected infants have no matched sibling donor for hematopoietic stem cell transplantation, and transplantation from other donors can produce an inadequate response and graft-versus-host disease. Prior attempts at gene therapy with gamma-retroviral vectors had led to vector-induced leukemia or had failed to induce humoral immunity or normal NK cell production.
“Our new lentiviral vector gene therapy combined with nonmyeloablative busulfan conditioning has been successful in restoring immunity in five patients 7-23 years of age in whom a previous allogeneic hematopoietic stem cell transplantation for SCID-X1 had failed,” the investigators wrote. “We hypothesized that the combination of this lentiviral vector and low-exposure busulfan administered by means of pharmacokinetic dose targeting would be safe and effective as the primary treatment in infants with newly diagnosed SCID-X1.”
Their protocol included one to two daily intravenous doses of busulfan, targeting a cumulative area under the curve of 22 mg per hr/L. They calculated the first dose by weight and age using a population-based pharmacokinetic model and adjusted the second dose based on first-dose pharmacokinetics.
After a median of 16.4 months, all infants continued to grow normally and cleared previous infections, and there were no unanticipated side effects from bone marrow harvest, busulfan conditioning, or cell infusion.
“It is hoped that durable, complete adaptive immunity will be achieved in the majority of the patients over time,” the researchers wrote.
They continue to follow the patients to assess therapeutic safety, immune durability, and persistence of the transferred gene in hematopoietic and immune cells.
Study funders included the American Lebanese Syrian Associated Charities, the National Institutes of Health, the California Institute of Regenerative Medicine, and the Assisi Foundation of Memphis. St. Jude Children’s Research Hospital has licensed the gene therapy and partnered with Mustang Bio to develop and commercialize it. Dr. Mamcarz reported receiving grant support from the study funders.
SOURCE: Mamcarz E et al. N Engl J Med. 2019; 380:1525-34.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE