User login
An Officer and a Physician
Imagine being transferred to a hospital where the temperature is 20 below outside, and 40 inches of snow fill the parking lot. Few physicians would sign on for such an assignment. For a brave few, it’s all in a day’s work.
Maj. Ramey Wilson, MD, is a U.S. Army physician who encountered such conditions during his 15-month experience in Afghanistan. “A couple of times, when we couldn’t get helicopters [for evacuation], we had to turn my aid station into a mini-hospital. There were no nurses, labs, or X-ray,” he says. “With only basic supplies and my combat medics, we had to provide all the patient care until the weather broke.”
Not quite the circumstances most hospitalists encounter in their daily practice.
Hospitalists in the military face daunting odds, and at the same time are blessed with some unexpected advantages. On the plus side, military physicians cite the camaraderie, teamwork, honor of caring for soldiers, and the opportunity to train other providers, both in traditional, U.S.-based residencies and while deployed. Among the minuses, they mention a lack of equipment and supplies when they are assigned to forward-deployed soldiers on foreign soil, the heartache of being separated from family, and lower compensation. Most military physicians, however, say that the lower compensation can be offset by generous government benefits and the absence of medical school debt.
All in all, hospitalists in the military have a unique—and sometimes adventurous—story to tell.
Challenges Met, Success Exemplified
Dr. Wilson is a hospitalist and Army physician assigned to Fort Bragg, N.C. Until this past summer, he was the chief of internal medicine at Womack Army Medical Center, one of eight full-service hospitals in the U.S. Army Medical Command. Because the Army is still familiarizing itself with the HM model and the role hospitalists play in the delivery of healthcare, resident house staff meet many of the operational needs, including night and weekend coverage. “The Army doesn’t have a good system for 24-hour continuous care at busy hospitals without residents,” Dr. Wilson says, “and we’ve worked hard to get hospitalists into our system.”
While other Army medical centers have internal-medicine residencies, Womack has only a family medicine residency program. Residents once provided extensive coverage for the hospital, but decreasing numbers (only four interns this year) and work-hour restrictions have shifted the inpatient responsibilities to the internal-medicine staff. “All of the military general internists have functionally become hospitalists to support the inpatient medicine and ICU services,” Dr. Wilson says. “Our family medicine house staff coverage has evaporated.”
The conditions he sees at Womack are similar to what he sees at FirstHealth Moore Regional Hospital, the civilian community hospital in Pinehurst, N.C., where he practices part time. Womack serves two major military populations: those on active duty and their family members, and those no longer on active duty or retired (and not a part of the Veterans Administration program).

—Col. Walt Franz, MD, U.S. Army Medical Corps, Amarah/Al Kut, Iraq
Dr. Wilson, who served in the Ghazni province in eastern Afghanistan, was the only American physician in an area of 8,800 square miles. He and his physician-assistant staff were tasked with keeping U.S. soldiers healthy, serving acute resuscitative trauma care and “basic sick call.” In addition to caring for U.S. and coalition soldiers, he partnered with the Ghazni Ministry of Health to improve the delivery of healthcare to residents of the province.
“Afghanistan has a great plan for medical care through its ‘basic’ package of health services and ‘essential’ package hospital services, developed with assistance from the U.S. Agency for International Development [USAID], and which we used as our road map for the Afghan public health service,” Dr. Wilson says. He and a nurse practitioner from the nearby provincial reconstruction team worked out of a forward operating base outside Ghazni’s provincial capital—the city of Ghazni—and the nearby provincial hospital. He says his hospitalist background was helpful when it came to working with and teaching the Afghan physicians and nurses at the hospital, which served as the referral center for several surrounding provinces.
“There was no infection-control program; their hospital and clinics were heated by wood stoves; and they were using the one endotracheal tube that had been left by the International Red Cross years earlier,” he says, noting that during his tour, the U.S. military dropped basic medical equipment and supplies—which were shared with the local hospital—into his forward operating base. “They were doing anesthesia without monitors. We trained them with an initial focus of making surgery safer. … To say that it was challenging is an understatement, and for many different reasons.”
Almost every other week, Dr. Wilson hosted a medical conference at his base for 10 to 20 Afghan physicians. Due to local customs, female providers were not allowed to travel without a male relative, so Dr. Wilson’s team videotaped the classes, had them translated into the Pashto language, and arranged with the hospital directors to distribute them to female physicians.
The needs in both army and civilian circumstances are huge in Afghanistan. Most Afghan hospitals and clinics are without Internet access, so decision support and telemedicine consultative service is out of the question. Textbooks are in short supply, too. Because the Taliban decreed that no image of a human being is allowed in print, they confiscated and destroyed all of the country’s anatomy books.
In terms of training, the key to success with locals is demonstrating what success can look like.
“Most of these providers have practiced in a system that they think is as good as it can be given the lack of advanced machinery and equipment,” Dr. Wilson says.
Physicians who visit U.S. military or Western hospitals and witness the successes possible in infection control, nursing care, medication administration, and medical documentation return to Afghanistan excited about the skills introduced to them. “They see that the provision of really good medical care is more dependent on having a clean space, a well-organized system, good communication, and solid basic medical care,” Dr. Wilson says.
Contrast to Care Continuity
Col. Walt Franz, MD, of U.S. Army Medical Corps headquartered in Amarah/Al Kut, Iraq, has just begun the work of partnering with Iraqi physicians and nurses for the first time since 2003. In 2004, as a public health team leader, his primary task was helping Iraqi providers with hospital and clinic projects. The projects ranged in cost from $40,000 (for securing an X-ray machine) to $5,000 for such smaller repairs and fix-ups as securing parts to make an elevator run. In fact, patients were being carried up several flights of stairs in the local, six-story hospital.
For about five months in 2008, Dr. Franz was deputy commander for clinical services for hospital and outpatient medical care at a combat support hospital. Since the beginning of 2009, he has been the commander of the 945th Forward Surgical Team at a small forward base in Amarah, near the Iraq-Iran border. “Our mission here is to provide urgent surgical resuscitation for the critically wounded and evac[uation] by helo [helicopter],” Dr. Franz says.
When he’s at home and working at the Mayo Clinic in Rochester, Minn., he practices primarily as a family physician. With nearly 30 years of clinical practice under his belt, Dr. Franz also puts in plenty of hours as a hospitalist. He has practiced during four deployments: three to Iraq and one to Germany.
“Active duty in a war zone presents experiences ranging from the inspiring to the absolutely tragic,” Dr. Franz says. “There is nothing worse than a casualty coming in on a medevac. It’s someone’s son or daughter or husband or wife, and nothing approaches the joy of helping a soldier. In fact, as a civilian, we scrupulously follow the Geneva Convention requirements.” (The treaty affords wounded and sick soldiers to be cared for and protected even though they may become prisoners of war.)
After you eliminate the dangers of enemy fire, there are still big differences between combat versus civilian medicine, he says. One is that combat medicine is usually acute care with little or no followup in the theater of operation, Dr. Franz says. Combat medicine has a strong foundation in echelons of care and evacuations away from the initial point of care. It runs concurrent to the civilian premise of continuity, and the limited number of specialists in theater usually means the Army relies on evacuation or electronic consults.
Maysan Province, where Dr. Franz is stationed, is the poorest part of Iraq. Because of its large Shia population, its citizens were devastated during the Iran-Iraq war and brutalized by Saddam Hussein. “The docs here are very street-smart; their work ethic is great and they have done without for a long time,” Dr. Franz says. Providers at the 540-bed hospital in Al Amarah see 200 patients per day in the ED; several hundred outpatients are triaged, and senior staff physicians see 75 or more cases daily. “One young doc told me it was not unusual to have 500 patients present to a regional ED in a 24-hour period, making triage and care almost overwhelming,” he says.
The biggest problem Dr. Franz witnesses in Iraqi hospitals is the lack of specialty nurses. His teams are teaching classes and training trainers in ED triage, basic ICU care, and the ultrasound FAST (Focused Assessment with Sonography in Trauma) exam skills Iraqi providers can use anywhere in the hospital.
Other issues include a lack of continuing medical education; poor infrastructure, which chokes the supply of pharmaceuticals and other medical equipment; and paucity of specialty nursing. Dr. Franz also cites critical staffing issues, such as the large number of physicians who have fled the country and the rising prominence of the private, fee-for-service care system, which can attract physicians and nurses away from the public system.
Care for Female Soldiers
With three other OB hospitalists, also known as laborists, Brook Thomson, MD, spent the summer organizing an OB/GYN hospital medicine program at Saint Alphonsus Regional Medical Center in Boise, Idaho. A veteran of military medicine, Dr. Thomson trained at Uniformed Services University of Health Sciences (USUHS) and completed an OB/GYN residency in 1997, then was stationed in Germany for four years. From 2001 to 2004, he served as chief of obstetrics at Madigan Army Medical Center in Tacoma, Wash., during which time he was deployed to Iraq for 10 months.
The OB/GYN expertise combined with the HM practice model that Dr. Thomson offers is a growing need in the military. “The number of women in the military is increasing, and there just aren’t a lot of people who understand female soldiers’ special needs,” he says.
Supporting women’s health has become an important aspect of battlefield medicine, namely the rooting out of potential sexual abuse. Dr. Thomson has published on the subject.1
In 2003, he was deployed as a general medical officer in Kuwait and assigned to the Basra area of Iraq, treating the gamut of patient needs. Recent Army policy changes, he says, ensure that OB/GYN military physicians now practice within their specialty.
A Canadian Perspective
Brendan James Hughes, MD, CCFP, returned from his military tour of duty and became a family practitioner in Lakefield, Ontario, a small community about 100 miles north of Toronto, and medical director of first-aid services for the Ontario Zone of the Canadian Red Cross.
In 2001, when Dr. Hughes was deployed as a hospitalist to Bosnia-Herzegovina for six months, the unrest from the civil war that involved Bosnians, Croatians, and Serbs (more than 100,000 were killed, and millions were injured or displaced), had settled, and his unit returned home without any loss of life. Upon his return, he transitioned from military life to become a full-time civilian hospitalist for six years in Ontario and Alberta. He now works as a part-time hospitalist.
Dr. Hughes says Canadian military practice is more acute and trauma-based now, as compared to his 2001 deployment in Eastern Europe. He notices many more deaths and major trauma cases in reports from Afghanistan, mostly blast injuries, limb amputations, and acute brain injuries, than there would be in a traditional, nonmilitary HM practice. He also notes that a lot of time and effort was placed on rehabilitation-focused practice that the patients required in the recovery phase.
Military practice differs from civilian hospitalist practice in other ways, he says. “In the military, every patient is essentially a workplace patient where the military is the employer,” Dr. Hughes says. Although clinicians maintain patient confidentiality, they are obliged to the chain of command to provide information on patient abilities. “We are careful not to relay a specific diagnosis without patient consent, but we have to dictate any needed restrictions on duty that are important in a combat situation, for themselves and for others,” he adds.
Such privacy and disclosure concerns are particularly difficult to navigate when it comes to diagnosis and treatment of alcohol and drug abuse, depression, post-traumatic stress, and suicide risk—issues that can lead soldiers to develop such long-term problems as substance abuse, marital discord, and marital abuse. TH
Andrea Sattinger is a freelance writer based in North Carolina.
Reference
- Thomson B, Nielsen P. Women’s healthcare in Operation Iraqi Freedom: a survey of camps with echelon one or two facilities. Mil Med. 2006;171:216-219.
The U.S. Army Medical Command
Each branch of the U.S. armed services—Army, Navy, Air Force, Marines and Coast Guard—has dedicated medical personnel and training programs.
The Army has the largest program, with more than 20,000 physicians, eight large medical centers, and 26 medical department activities; numerous clinics in the U.S., Europe, and Japan are grouped under six major subordinate commands called regional medical commands.
The Army offers training programs in six areas of medicine: dental, medical, medical service, medical specialist, nursing, and veterinary. The Army currently is offering $20,000 sign-on bonuses to medical and dental students, and offers free tuition and generous scholarship opportunities to qualified applicants.
For more information, visit www.armymedicine.army.mil/.
Darnall Army Medical Center

Darnall Army Medical Center is located 60 miles north of Austin and services more than 145,000 beneficiaries. The facility has five primary-care clinics, four troop medical clinics, 22 specialty clinics, and is home to the 1st Cavalry Division and the 4th Infantry Division (Mechanized).
Eisenhower Army Medical Center

The Dwight D. Eisenhower Army Medical Center hosts the Center for Total Access, which features lifelike electronic dummies that respond to stimuli and the effects of administering certain kinds of care and medication in a battlefield situation.
Landstuhl Regional Medical Center

Landstuhl Regional Medical Center is the only Army medical facility to house an Air Force Aero-medical Evacuation Unit. The hospital is also a primary evacuation point for injured soldiers who need further treatment before coming home to the U.S. or returning to their units in theater.
Madigan Army Medical Center

Madigan Army Medical Center is one of only three designated Level Two trauma centers within the U.S. Medical Command. Recently, the hospital's Andersen Simulation Center received a three-year accreditation from the American College of Surgeons, becoming the only Defense Department medical educational institution to attain that status.
San Antonio Military Medical Center

San Antonio Military Medical Center is located in San Antonio, Texas. It plays a critical role in patient care, graduate medical education and research, as well as taking care of wounded service members.
Tripler Army Medical Center

The Tripler Army Medical Center is the largest Army medical treatment facility in the Pacific Basin. The Center of Excellence in Disaster Management and Humanitarian Assistance is also located at the facility. The U.N. Department of Peacekeeping Operations has designated the CE as a Peace Operations Institute, the only United Nations-designated Peace Operations Institute currently in the United States.
Womack Army Medical Center

Womack Army Medial Center personnel use the latest technology to better serve its patients. From interventional radiology techniques to laser eye surgery, its physicians strive keep their fingers on the pulse of modern medicine.
William Beaumont Army Medical Center

The William Beaumont Army Medical Center is affiliated with such institutions as Texas Tech University School of Medicine, University of Texas at El Paso School of Nursing, and El Paso Community College Nursing School. It also provides opportunities for medical students throughout the nation to do rotations at the facility.
Walter Reed Army Medical Center

Walter Reed Army Medical Hospital generates the largest number of ongoing clinical research studies within the Department of Defense. It is often referred to as the flagship of DoD clinical research and is the largest and most diverse biomedical research laboratory in DoD.
Source: www.goarmy.com
Dr. Wilson’s photos from Afghanistan
Click images to enlarge
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
 |
PHOTOS COURTESY OF MAJ. RAMEY WILSON
Imagine being transferred to a hospital where the temperature is 20 below outside, and 40 inches of snow fill the parking lot. Few physicians would sign on for such an assignment. For a brave few, it’s all in a day’s work.
Maj. Ramey Wilson, MD, is a U.S. Army physician who encountered such conditions during his 15-month experience in Afghanistan. “A couple of times, when we couldn’t get helicopters [for evacuation], we had to turn my aid station into a mini-hospital. There were no nurses, labs, or X-ray,” he says. “With only basic supplies and my combat medics, we had to provide all the patient care until the weather broke.”
Not quite the circumstances most hospitalists encounter in their daily practice.
Hospitalists in the military face daunting odds, and at the same time are blessed with some unexpected advantages. On the plus side, military physicians cite the camaraderie, teamwork, honor of caring for soldiers, and the opportunity to train other providers, both in traditional, U.S.-based residencies and while deployed. Among the minuses, they mention a lack of equipment and supplies when they are assigned to forward-deployed soldiers on foreign soil, the heartache of being separated from family, and lower compensation. Most military physicians, however, say that the lower compensation can be offset by generous government benefits and the absence of medical school debt.
All in all, hospitalists in the military have a unique—and sometimes adventurous—story to tell.
Challenges Met, Success Exemplified
Dr. Wilson is a hospitalist and Army physician assigned to Fort Bragg, N.C. Until this past summer, he was the chief of internal medicine at Womack Army Medical Center, one of eight full-service hospitals in the U.S. Army Medical Command. Because the Army is still familiarizing itself with the HM model and the role hospitalists play in the delivery of healthcare, resident house staff meet many of the operational needs, including night and weekend coverage. “The Army doesn’t have a good system for 24-hour continuous care at busy hospitals without residents,” Dr. Wilson says, “and we’ve worked hard to get hospitalists into our system.”
While other Army medical centers have internal-medicine residencies, Womack has only a family medicine residency program. Residents once provided extensive coverage for the hospital, but decreasing numbers (only four interns this year) and work-hour restrictions have shifted the inpatient responsibilities to the internal-medicine staff. “All of the military general internists have functionally become hospitalists to support the inpatient medicine and ICU services,” Dr. Wilson says. “Our family medicine house staff coverage has evaporated.”
The conditions he sees at Womack are similar to what he sees at FirstHealth Moore Regional Hospital, the civilian community hospital in Pinehurst, N.C., where he practices part time. Womack serves two major military populations: those on active duty and their family members, and those no longer on active duty or retired (and not a part of the Veterans Administration program).
—Col. Walt Franz, MD, U.S. Army Medical Corps, Amarah/Al Kut, Iraq
Dr. Wilson, who served in the Ghazni province in eastern Afghanistan, was the only American physician in an area of 8,800 square miles. He and his physician-assistant staff were tasked with keeping U.S. soldiers healthy, serving acute resuscitative trauma care and “basic sick call.” In addition to caring for U.S. and coalition soldiers, he partnered with the Ghazni Ministry of Health to improve the delivery of healthcare to residents of the province.
“Afghanistan has a great plan for medical care through its ‘basic’ package of health services and ‘essential’ package hospital services, developed with assistance from the U.S. Agency for International Development [USAID], and which we used as our road map for the Afghan public health service,” Dr. Wilson says. He and a nurse practitioner from the nearby provincial reconstruction team worked out of a forward operating base outside Ghazni’s provincial capital—the city of Ghazni—and the nearby provincial hospital. He says his hospitalist background was helpful when it came to working with and teaching the Afghan physicians and nurses at the hospital, which served as the referral center for several surrounding provinces.
“There was no infection-control program; their hospital and clinics were heated by wood stoves; and they were using the one endotracheal tube that had been left by the International Red Cross years earlier,” he says, noting that during his tour, the U.S. military dropped basic medical equipment and supplies—which were shared with the local hospital—into his forward operating base. “They were doing anesthesia without monitors. We trained them with an initial focus of making surgery safer. … To say that it was challenging is an understatement, and for many different reasons.”
Almost every other week, Dr. Wilson hosted a medical conference at his base for 10 to 20 Afghan physicians. Due to local customs, female providers were not allowed to travel without a male relative, so Dr. Wilson’s team videotaped the classes, had them translated into the Pashto language, and arranged with the hospital directors to distribute them to female physicians.
The needs in both army and civilian circumstances are huge in Afghanistan. Most Afghan hospitals and clinics are without Internet access, so decision support and telemedicine consultative service is out of the question. Textbooks are in short supply, too. Because the Taliban decreed that no image of a human being is allowed in print, they confiscated and destroyed all of the country’s anatomy books.
In terms of training, the key to success with locals is demonstrating what success can look like.
“Most of these providers have practiced in a system that they think is as good as it can be given the lack of advanced machinery and equipment,” Dr. Wilson says.
Physicians who visit U.S. military or Western hospitals and witness the successes possible in infection control, nursing care, medication administration, and medical documentation return to Afghanistan excited about the skills introduced to them. “They see that the provision of really good medical care is more dependent on having a clean space, a well-organized system, good communication, and solid basic medical care,” Dr. Wilson says.
Contrast to Care Continuity
Col. Walt Franz, MD, of U.S. Army Medical Corps headquartered in Amarah/Al Kut, Iraq, has just begun the work of partnering with Iraqi physicians and nurses for the first time since 2003. In 2004, as a public health team leader, his primary task was helping Iraqi providers with hospital and clinic projects. The projects ranged in cost from $40,000 (for securing an X-ray machine) to $5,000 for such smaller repairs and fix-ups as securing parts to make an elevator run. In fact, patients were being carried up several flights of stairs in the local, six-story hospital.
For about five months in 2008, Dr. Franz was deputy commander for clinical services for hospital and outpatient medical care at a combat support hospital. Since the beginning of 2009, he has been the commander of the 945th Forward Surgical Team at a small forward base in Amarah, near the Iraq-Iran border. “Our mission here is to provide urgent surgical resuscitation for the critically wounded and evac[uation] by helo [helicopter],” Dr. Franz says.
When he’s at home and working at the Mayo Clinic in Rochester, Minn., he practices primarily as a family physician. With nearly 30 years of clinical practice under his belt, Dr. Franz also puts in plenty of hours as a hospitalist. He has practiced during four deployments: three to Iraq and one to Germany.
“Active duty in a war zone presents experiences ranging from the inspiring to the absolutely tragic,” Dr. Franz says. “There is nothing worse than a casualty coming in on a medevac. It’s someone’s son or daughter or husband or wife, and nothing approaches the joy of helping a soldier. In fact, as a civilian, we scrupulously follow the Geneva Convention requirements.” (The treaty affords wounded and sick soldiers to be cared for and protected even though they may become prisoners of war.)
After you eliminate the dangers of enemy fire, there are still big differences between combat versus civilian medicine, he says. One is that combat medicine is usually acute care with little or no followup in the theater of operation, Dr. Franz says. Combat medicine has a strong foundation in echelons of care and evacuations away from the initial point of care. It runs concurrent to the civilian premise of continuity, and the limited number of specialists in theater usually means the Army relies on evacuation or electronic consults.
Maysan Province, where Dr. Franz is stationed, is the poorest part of Iraq. Because of its large Shia population, its citizens were devastated during the Iran-Iraq war and brutalized by Saddam Hussein. “The docs here are very street-smart; their work ethic is great and they have done without for a long time,” Dr. Franz says. Providers at the 540-bed hospital in Al Amarah see 200 patients per day in the ED; several hundred outpatients are triaged, and senior staff physicians see 75 or more cases daily. “One young doc told me it was not unusual to have 500 patients present to a regional ED in a 24-hour period, making triage and care almost overwhelming,” he says.
The biggest problem Dr. Franz witnesses in Iraqi hospitals is the lack of specialty nurses. His teams are teaching classes and training trainers in ED triage, basic ICU care, and the ultrasound FAST (Focused Assessment with Sonography in Trauma) exam skills Iraqi providers can use anywhere in the hospital.
Other issues include a lack of continuing medical education; poor infrastructure, which chokes the supply of pharmaceuticals and other medical equipment; and paucity of specialty nursing. Dr. Franz also cites critical staffing issues, such as the large number of physicians who have fled the country and the rising prominence of the private, fee-for-service care system, which can attract physicians and nurses away from the public system.
Care for Female Soldiers
With three other OB hospitalists, also known as laborists, Brook Thomson, MD, spent the summer organizing an OB/GYN hospital medicine program at Saint Alphonsus Regional Medical Center in Boise, Idaho. A veteran of military medicine, Dr. Thomson trained at Uniformed Services University of Health Sciences (USUHS) and completed an OB/GYN residency in 1997, then was stationed in Germany for four years. From 2001 to 2004, he served as chief of obstetrics at Madigan Army Medical Center in Tacoma, Wash., during which time he was deployed to Iraq for 10 months.
The OB/GYN expertise combined with the HM practice model that Dr. Thomson offers is a growing need in the military. “The number of women in the military is increasing, and there just aren’t a lot of people who understand female soldiers’ special needs,” he says.
Supporting women’s health has become an important aspect of battlefield medicine, namely the rooting out of potential sexual abuse. Dr. Thomson has published on the subject.1
In 2003, he was deployed as a general medical officer in Kuwait and assigned to the Basra area of Iraq, treating the gamut of patient needs. Recent Army policy changes, he says, ensure that OB/GYN military physicians now practice within their specialty.
A Canadian Perspective
Brendan James Hughes, MD, CCFP, returned from his military tour of duty and became a family practitioner in Lakefield, Ontario, a small community about 100 miles north of Toronto, and medical director of first-aid services for the Ontario Zone of the Canadian Red Cross.
In 2001, when Dr. Hughes was deployed as a hospitalist to Bosnia-Herzegovina for six months, the unrest from the civil war that involved Bosnians, Croatians, and Serbs (more than 100,000 were killed, and millions were injured or displaced), had settled, and his unit returned home without any loss of life. Upon his return, he transitioned from military life to become a full-time civilian hospitalist for six years in Ontario and Alberta. He now works as a part-time hospitalist.
Dr. Hughes says Canadian military practice is more acute and trauma-based now, as compared to his 2001 deployment in Eastern Europe. He notices many more deaths and major trauma cases in reports from Afghanistan, mostly blast injuries, limb amputations, and acute brain injuries, than there would be in a traditional, nonmilitary HM practice. He also notes that a lot of time and effort was placed on rehabilitation-focused practice that the patients required in the recovery phase.
Military practice differs from civilian hospitalist practice in other ways, he says. “In the military, every patient is essentially a workplace patient where the military is the employer,” Dr. Hughes says. Although clinicians maintain patient confidentiality, they are obliged to the chain of command to provide information on patient abilities. “We are careful not to relay a specific diagnosis without patient consent, but we have to dictate any needed restrictions on duty that are important in a combat situation, for themselves and for others,” he adds.
Such privacy and disclosure concerns are particularly difficult to navigate when it comes to diagnosis and treatment of alcohol and drug abuse, depression, post-traumatic stress, and suicide risk—issues that can lead soldiers to develop such long-term problems as substance abuse, marital discord, and marital abuse. TH
Andrea Sattinger is a freelance writer based in North Carolina.
Reference
- Thomson B, Nielsen P. Women’s healthcare in Operation Iraqi Freedom: a survey of camps with echelon one or two facilities. Mil Med. 2006;171:216-219.
The U.S. Army Medical Command
Each branch of the U.S. armed services—Army, Navy, Air Force, Marines and Coast Guard—has dedicated medical personnel and training programs.
The Army has the largest program, with more than 20,000 physicians, eight large medical centers, and 26 medical department activities; numerous clinics in the U.S., Europe, and Japan are grouped under six major subordinate commands called regional medical commands.
The Army offers training programs in six areas of medicine: dental, medical, medical service, medical specialist, nursing, and veterinary. The Army currently is offering $20,000 sign-on bonuses to medical and dental students, and offers free tuition and generous scholarship opportunities to qualified applicants.
For more information, visit www.armymedicine.army.mil/.
Darnall Army Medical Center
Darnall Army Medical Center is located 60 miles north of Austin and services more than 145,000 beneficiaries. The facility has five primary-care clinics, four troop medical clinics, 22 specialty clinics, and is home to the 1st Cavalry Division and the 4th Infantry Division (Mechanized).
Eisenhower Army Medical Center
The Dwight D. Eisenhower Army Medical Center hosts the Center for Total Access, which features lifelike electronic dummies that respond to stimuli and the effects of administering certain kinds of care and medication in a battlefield situation.
Landstuhl Regional Medical Center
Landstuhl Regional Medical Center is the only Army medical facility to house an Air Force Aero-medical Evacuation Unit. The hospital is also a primary evacuation point for injured soldiers who need further treatment before coming home to the U.S. or returning to their units in theater.
Madigan Army Medical Center
Madigan Army Medical Center is one of only three designated Level Two trauma centers within the U.S. Medical Command. Recently, the hospital's Andersen Simulation Center received a three-year accreditation from the American College of Surgeons, becoming the only Defense Department medical educational institution to attain that status.
San Antonio Military Medical Center
San Antonio Military Medical Center is located in San Antonio, Texas. It plays a critical role in patient care, graduate medical education and research, as well as taking care of wounded service members.
Tripler Army Medical Center
The Tripler Army Medical Center is the largest Army medical treatment facility in the Pacific Basin. The Center of Excellence in Disaster Management and Humanitarian Assistance is also located at the facility. The U.N. Department of Peacekeeping Operations has designated the CE as a Peace Operations Institute, the only United Nations-designated Peace Operations Institute currently in the United States.
Womack Army Medical Center
Womack Army Medial Center personnel use the latest technology to better serve its patients. From interventional radiology techniques to laser eye surgery, its physicians strive keep their fingers on the pulse of modern medicine.
William Beaumont Army Medical Center
The William Beaumont Army Medical Center is affiliated with such institutions as Texas Tech University School of Medicine, University of Texas at El Paso School of Nursing, and El Paso Community College Nursing School. It also provides opportunities for medical students throughout the nation to do rotations at the facility.
Walter Reed Army Medical Center
Walter Reed Army Medical Hospital generates the largest number of ongoing clinical research studies within the Department of Defense. It is often referred to as the flagship of DoD clinical research and is the largest and most diverse biomedical research laboratory in DoD.
Source: www.goarmy.com
Dr. Wilson’s photos from Afghanistan
Click images to enlarge
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHOTOS COURTESY OF MAJ. RAMEY WILSON
Imagine being transferred to a hospital where the temperature is 20 below outside, and 40 inches of snow fill the parking lot. Few physicians would sign on for such an assignment. For a brave few, it’s all in a day’s work.
Maj. Ramey Wilson, MD, is a U.S. Army physician who encountered such conditions during his 15-month experience in Afghanistan. “A couple of times, when we couldn’t get helicopters [for evacuation], we had to turn my aid station into a mini-hospital. There were no nurses, labs, or X-ray,” he says. “With only basic supplies and my combat medics, we had to provide all the patient care until the weather broke.”
Not quite the circumstances most hospitalists encounter in their daily practice.
Hospitalists in the military face daunting odds, and at the same time are blessed with some unexpected advantages. On the plus side, military physicians cite the camaraderie, teamwork, honor of caring for soldiers, and the opportunity to train other providers, both in traditional, U.S.-based residencies and while deployed. Among the minuses, they mention a lack of equipment and supplies when they are assigned to forward-deployed soldiers on foreign soil, the heartache of being separated from family, and lower compensation. Most military physicians, however, say that the lower compensation can be offset by generous government benefits and the absence of medical school debt.
All in all, hospitalists in the military have a unique—and sometimes adventurous—story to tell.
Challenges Met, Success Exemplified
Dr. Wilson is a hospitalist and Army physician assigned to Fort Bragg, N.C. Until this past summer, he was the chief of internal medicine at Womack Army Medical Center, one of eight full-service hospitals in the U.S. Army Medical Command. Because the Army is still familiarizing itself with the HM model and the role hospitalists play in the delivery of healthcare, resident house staff meet many of the operational needs, including night and weekend coverage. “The Army doesn’t have a good system for 24-hour continuous care at busy hospitals without residents,” Dr. Wilson says, “and we’ve worked hard to get hospitalists into our system.”
While other Army medical centers have internal-medicine residencies, Womack has only a family medicine residency program. Residents once provided extensive coverage for the hospital, but decreasing numbers (only four interns this year) and work-hour restrictions have shifted the inpatient responsibilities to the internal-medicine staff. “All of the military general internists have functionally become hospitalists to support the inpatient medicine and ICU services,” Dr. Wilson says. “Our family medicine house staff coverage has evaporated.”
The conditions he sees at Womack are similar to what he sees at FirstHealth Moore Regional Hospital, the civilian community hospital in Pinehurst, N.C., where he practices part time. Womack serves two major military populations: those on active duty and their family members, and those no longer on active duty or retired (and not a part of the Veterans Administration program).
—Col. Walt Franz, MD, U.S. Army Medical Corps, Amarah/Al Kut, Iraq
Dr. Wilson, who served in the Ghazni province in eastern Afghanistan, was the only American physician in an area of 8,800 square miles. He and his physician-assistant staff were tasked with keeping U.S. soldiers healthy, serving acute resuscitative trauma care and “basic sick call.” In addition to caring for U.S. and coalition soldiers, he partnered with the Ghazni Ministry of Health to improve the delivery of healthcare to residents of the province.
“Afghanistan has a great plan for medical care through its ‘basic’ package of health services and ‘essential’ package hospital services, developed with assistance from the U.S. Agency for International Development [USAID], and which we used as our road map for the Afghan public health service,” Dr. Wilson says. He and a nurse practitioner from the nearby provincial reconstruction team worked out of a forward operating base outside Ghazni’s provincial capital—the city of Ghazni—and the nearby provincial hospital. He says his hospitalist background was helpful when it came to working with and teaching the Afghan physicians and nurses at the hospital, which served as the referral center for several surrounding provinces.
“There was no infection-control program; their hospital and clinics were heated by wood stoves; and they were using the one endotracheal tube that had been left by the International Red Cross years earlier,” he says, noting that during his tour, the U.S. military dropped basic medical equipment and supplies—which were shared with the local hospital—into his forward operating base. “They were doing anesthesia without monitors. We trained them with an initial focus of making surgery safer. … To say that it was challenging is an understatement, and for many different reasons.”
Almost every other week, Dr. Wilson hosted a medical conference at his base for 10 to 20 Afghan physicians. Due to local customs, female providers were not allowed to travel without a male relative, so Dr. Wilson’s team videotaped the classes, had them translated into the Pashto language, and arranged with the hospital directors to distribute them to female physicians.
The needs in both army and civilian circumstances are huge in Afghanistan. Most Afghan hospitals and clinics are without Internet access, so decision support and telemedicine consultative service is out of the question. Textbooks are in short supply, too. Because the Taliban decreed that no image of a human being is allowed in print, they confiscated and destroyed all of the country’s anatomy books.
In terms of training, the key to success with locals is demonstrating what success can look like.
“Most of these providers have practiced in a system that they think is as good as it can be given the lack of advanced machinery and equipment,” Dr. Wilson says.
Physicians who visit U.S. military or Western hospitals and witness the successes possible in infection control, nursing care, medication administration, and medical documentation return to Afghanistan excited about the skills introduced to them. “They see that the provision of really good medical care is more dependent on having a clean space, a well-organized system, good communication, and solid basic medical care,” Dr. Wilson says.
Contrast to Care Continuity
Col. Walt Franz, MD, of U.S. Army Medical Corps headquartered in Amarah/Al Kut, Iraq, has just begun the work of partnering with Iraqi physicians and nurses for the first time since 2003. In 2004, as a public health team leader, his primary task was helping Iraqi providers with hospital and clinic projects. The projects ranged in cost from $40,000 (for securing an X-ray machine) to $5,000 for such smaller repairs and fix-ups as securing parts to make an elevator run. In fact, patients were being carried up several flights of stairs in the local, six-story hospital.
For about five months in 2008, Dr. Franz was deputy commander for clinical services for hospital and outpatient medical care at a combat support hospital. Since the beginning of 2009, he has been the commander of the 945th Forward Surgical Team at a small forward base in Amarah, near the Iraq-Iran border. “Our mission here is to provide urgent surgical resuscitation for the critically wounded and evac[uation] by helo [helicopter],” Dr. Franz says.
When he’s at home and working at the Mayo Clinic in Rochester, Minn., he practices primarily as a family physician. With nearly 30 years of clinical practice under his belt, Dr. Franz also puts in plenty of hours as a hospitalist. He has practiced during four deployments: three to Iraq and one to Germany.
“Active duty in a war zone presents experiences ranging from the inspiring to the absolutely tragic,” Dr. Franz says. “There is nothing worse than a casualty coming in on a medevac. It’s someone’s son or daughter or husband or wife, and nothing approaches the joy of helping a soldier. In fact, as a civilian, we scrupulously follow the Geneva Convention requirements.” (The treaty affords wounded and sick soldiers to be cared for and protected even though they may become prisoners of war.)
After you eliminate the dangers of enemy fire, there are still big differences between combat versus civilian medicine, he says. One is that combat medicine is usually acute care with little or no followup in the theater of operation, Dr. Franz says. Combat medicine has a strong foundation in echelons of care and evacuations away from the initial point of care. It runs concurrent to the civilian premise of continuity, and the limited number of specialists in theater usually means the Army relies on evacuation or electronic consults.
Maysan Province, where Dr. Franz is stationed, is the poorest part of Iraq. Because of its large Shia population, its citizens were devastated during the Iran-Iraq war and brutalized by Saddam Hussein. “The docs here are very street-smart; their work ethic is great and they have done without for a long time,” Dr. Franz says. Providers at the 540-bed hospital in Al Amarah see 200 patients per day in the ED; several hundred outpatients are triaged, and senior staff physicians see 75 or more cases daily. “One young doc told me it was not unusual to have 500 patients present to a regional ED in a 24-hour period, making triage and care almost overwhelming,” he says.
The biggest problem Dr. Franz witnesses in Iraqi hospitals is the lack of specialty nurses. His teams are teaching classes and training trainers in ED triage, basic ICU care, and the ultrasound FAST (Focused Assessment with Sonography in Trauma) exam skills Iraqi providers can use anywhere in the hospital.
Other issues include a lack of continuing medical education; poor infrastructure, which chokes the supply of pharmaceuticals and other medical equipment; and paucity of specialty nursing. Dr. Franz also cites critical staffing issues, such as the large number of physicians who have fled the country and the rising prominence of the private, fee-for-service care system, which can attract physicians and nurses away from the public system.
Care for Female Soldiers
With three other OB hospitalists, also known as laborists, Brook Thomson, MD, spent the summer organizing an OB/GYN hospital medicine program at Saint Alphonsus Regional Medical Center in Boise, Idaho. A veteran of military medicine, Dr. Thomson trained at Uniformed Services University of Health Sciences (USUHS) and completed an OB/GYN residency in 1997, then was stationed in Germany for four years. From 2001 to 2004, he served as chief of obstetrics at Madigan Army Medical Center in Tacoma, Wash., during which time he was deployed to Iraq for 10 months.
The OB/GYN expertise combined with the HM practice model that Dr. Thomson offers is a growing need in the military. “The number of women in the military is increasing, and there just aren’t a lot of people who understand female soldiers’ special needs,” he says.
Supporting women’s health has become an important aspect of battlefield medicine, namely the rooting out of potential sexual abuse. Dr. Thomson has published on the subject.1
In 2003, he was deployed as a general medical officer in Kuwait and assigned to the Basra area of Iraq, treating the gamut of patient needs. Recent Army policy changes, he says, ensure that OB/GYN military physicians now practice within their specialty.
A Canadian Perspective
Brendan James Hughes, MD, CCFP, returned from his military tour of duty and became a family practitioner in Lakefield, Ontario, a small community about 100 miles north of Toronto, and medical director of first-aid services for the Ontario Zone of the Canadian Red Cross.
In 2001, when Dr. Hughes was deployed as a hospitalist to Bosnia-Herzegovina for six months, the unrest from the civil war that involved Bosnians, Croatians, and Serbs (more than 100,000 were killed, and millions were injured or displaced), had settled, and his unit returned home without any loss of life. Upon his return, he transitioned from military life to become a full-time civilian hospitalist for six years in Ontario and Alberta. He now works as a part-time hospitalist.
Dr. Hughes says Canadian military practice is more acute and trauma-based now, as compared to his 2001 deployment in Eastern Europe. He notices many more deaths and major trauma cases in reports from Afghanistan, mostly blast injuries, limb amputations, and acute brain injuries, than there would be in a traditional, nonmilitary HM practice. He also notes that a lot of time and effort was placed on rehabilitation-focused practice that the patients required in the recovery phase.
Military practice differs from civilian hospitalist practice in other ways, he says. “In the military, every patient is essentially a workplace patient where the military is the employer,” Dr. Hughes says. Although clinicians maintain patient confidentiality, they are obliged to the chain of command to provide information on patient abilities. “We are careful not to relay a specific diagnosis without patient consent, but we have to dictate any needed restrictions on duty that are important in a combat situation, for themselves and for others,” he adds.
Such privacy and disclosure concerns are particularly difficult to navigate when it comes to diagnosis and treatment of alcohol and drug abuse, depression, post-traumatic stress, and suicide risk—issues that can lead soldiers to develop such long-term problems as substance abuse, marital discord, and marital abuse. TH
Andrea Sattinger is a freelance writer based in North Carolina.
Reference
- Thomson B, Nielsen P. Women’s healthcare in Operation Iraqi Freedom: a survey of camps with echelon one or two facilities. Mil Med. 2006;171:216-219.
The U.S. Army Medical Command
Each branch of the U.S. armed services—Army, Navy, Air Force, Marines and Coast Guard—has dedicated medical personnel and training programs.
The Army has the largest program, with more than 20,000 physicians, eight large medical centers, and 26 medical department activities; numerous clinics in the U.S., Europe, and Japan are grouped under six major subordinate commands called regional medical commands.
The Army offers training programs in six areas of medicine: dental, medical, medical service, medical specialist, nursing, and veterinary. The Army currently is offering $20,000 sign-on bonuses to medical and dental students, and offers free tuition and generous scholarship opportunities to qualified applicants.
For more information, visit www.armymedicine.army.mil/.
Darnall Army Medical Center
Darnall Army Medical Center is located 60 miles north of Austin and services more than 145,000 beneficiaries. The facility has five primary-care clinics, four troop medical clinics, 22 specialty clinics, and is home to the 1st Cavalry Division and the 4th Infantry Division (Mechanized).
Eisenhower Army Medical Center
The Dwight D. Eisenhower Army Medical Center hosts the Center for Total Access, which features lifelike electronic dummies that respond to stimuli and the effects of administering certain kinds of care and medication in a battlefield situation.
Landstuhl Regional Medical Center
Landstuhl Regional Medical Center is the only Army medical facility to house an Air Force Aero-medical Evacuation Unit. The hospital is also a primary evacuation point for injured soldiers who need further treatment before coming home to the U.S. or returning to their units in theater.
Madigan Army Medical Center
Madigan Army Medical Center is one of only three designated Level Two trauma centers within the U.S. Medical Command. Recently, the hospital's Andersen Simulation Center received a three-year accreditation from the American College of Surgeons, becoming the only Defense Department medical educational institution to attain that status.
San Antonio Military Medical Center
San Antonio Military Medical Center is located in San Antonio, Texas. It plays a critical role in patient care, graduate medical education and research, as well as taking care of wounded service members.
Tripler Army Medical Center
The Tripler Army Medical Center is the largest Army medical treatment facility in the Pacific Basin. The Center of Excellence in Disaster Management and Humanitarian Assistance is also located at the facility. The U.N. Department of Peacekeeping Operations has designated the CE as a Peace Operations Institute, the only United Nations-designated Peace Operations Institute currently in the United States.
Womack Army Medical Center
Womack Army Medial Center personnel use the latest technology to better serve its patients. From interventional radiology techniques to laser eye surgery, its physicians strive keep their fingers on the pulse of modern medicine.
William Beaumont Army Medical Center
The William Beaumont Army Medical Center is affiliated with such institutions as Texas Tech University School of Medicine, University of Texas at El Paso School of Nursing, and El Paso Community College Nursing School. It also provides opportunities for medical students throughout the nation to do rotations at the facility.
Walter Reed Army Medical Center
Walter Reed Army Medical Hospital generates the largest number of ongoing clinical research studies within the Department of Defense. It is often referred to as the flagship of DoD clinical research and is the largest and most diverse biomedical research laboratory in DoD.
Source: www.goarmy.com
Dr. Wilson’s photos from Afghanistan
Click images to enlarge
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PHOTOS COURTESY OF MAJ. RAMEY WILSON
ONLINE EXCLUSIVE: Training in Two Cultures: Medicine and Soldiering
Undergrads who choose the military and attend USUHS receive free tuition, books and other supplies; hand-held devices and related subscriptions, and basic medical equipment such as stethoscopes. In addition, USUHS medical students are paid as an active-duty second lieutenant (the going rate for the U.S. Army is about $1,900 per month).
Once they graduate, military residents work in uniform at military facilities and are afforded housing allowances. The government also covers the cost of medical malpractice insurance and supports them in any litigation while they are on active service. If they complete 20 years in active service, military physicians receive a generous retirement package, including a retained 40% to 50% pension for the rest of their lives, and they can seek work in the civilian sector after their military career.
For those who choose the military from the outset, the Department of Defense offers sign-on bonuses of $20,000 and a Health Service Professional Scholarship (HPSP) program for qualified applicants. It covers all medical school costs at a civilian medical school of the student’s choice. (Recent studies show the typical medical school grad has $120,000 of school load debt; $160,000 if they attended a private school.) The caveat is that after graduation, whether from USUHS or a civilian medical school, the physician works in uniform as a military physician for a pre-determined payback period (e.g., the Army obligation is one year of service for every year of scholarship).
The military offers training programs in medical, dental, optometry, veterinary, psychiatric nurse practitioner, and clinical and counseling psychology. Training at USUHS or with an HPSP requires each student before matriculation to choose his or her preferred branch of military service for the payback period. Whichever route a student takes, USUHS or HPSP, the student will end up as a doctor and a trained service member knowledgeable about areas including rank structure, military administration, and personal physical fitness.
Undergrads who choose the military and attend USUHS receive free tuition, books and other supplies; hand-held devices and related subscriptions, and basic medical equipment such as stethoscopes. In addition, USUHS medical students are paid as an active-duty second lieutenant (the going rate for the U.S. Army is about $1,900 per month).
Once they graduate, military residents work in uniform at military facilities and are afforded housing allowances. The government also covers the cost of medical malpractice insurance and supports them in any litigation while they are on active service. If they complete 20 years in active service, military physicians receive a generous retirement package, including a retained 40% to 50% pension for the rest of their lives, and they can seek work in the civilian sector after their military career.
For those who choose the military from the outset, the Department of Defense offers sign-on bonuses of $20,000 and a Health Service Professional Scholarship (HPSP) program for qualified applicants. It covers all medical school costs at a civilian medical school of the student’s choice. (Recent studies show the typical medical school grad has $120,000 of school load debt; $160,000 if they attended a private school.) The caveat is that after graduation, whether from USUHS or a civilian medical school, the physician works in uniform as a military physician for a pre-determined payback period (e.g., the Army obligation is one year of service for every year of scholarship).
The military offers training programs in medical, dental, optometry, veterinary, psychiatric nurse practitioner, and clinical and counseling psychology. Training at USUHS or with an HPSP requires each student before matriculation to choose his or her preferred branch of military service for the payback period. Whichever route a student takes, USUHS or HPSP, the student will end up as a doctor and a trained service member knowledgeable about areas including rank structure, military administration, and personal physical fitness.
Undergrads who choose the military and attend USUHS receive free tuition, books and other supplies; hand-held devices and related subscriptions, and basic medical equipment such as stethoscopes. In addition, USUHS medical students are paid as an active-duty second lieutenant (the going rate for the U.S. Army is about $1,900 per month).
Once they graduate, military residents work in uniform at military facilities and are afforded housing allowances. The government also covers the cost of medical malpractice insurance and supports them in any litigation while they are on active service. If they complete 20 years in active service, military physicians receive a generous retirement package, including a retained 40% to 50% pension for the rest of their lives, and they can seek work in the civilian sector after their military career.
For those who choose the military from the outset, the Department of Defense offers sign-on bonuses of $20,000 and a Health Service Professional Scholarship (HPSP) program for qualified applicants. It covers all medical school costs at a civilian medical school of the student’s choice. (Recent studies show the typical medical school grad has $120,000 of school load debt; $160,000 if they attended a private school.) The caveat is that after graduation, whether from USUHS or a civilian medical school, the physician works in uniform as a military physician for a pre-determined payback period (e.g., the Army obligation is one year of service for every year of scholarship).
The military offers training programs in medical, dental, optometry, veterinary, psychiatric nurse practitioner, and clinical and counseling psychology. Training at USUHS or with an HPSP requires each student before matriculation to choose his or her preferred branch of military service for the payback period. Whichever route a student takes, USUHS or HPSP, the student will end up as a doctor and a trained service member knowledgeable about areas including rank structure, military administration, and personal physical fitness.
The Big One
In March 2005 the Agency for Healthcare Research and Quality and the HHS Office of Public Health Emergency Preparedness published a report of guidelines for officials on how to plan for delivering health and medical care in a mass casualty event.1
After federal, state, and local authorities’ failure to supply desperately needed assistance following Hurricane Katrina, that report of recommendations from a 39-member panel of experts in bioethics, emergency medicine, emergency management, health administration, health law, and policy is more crucial than ever. This report offers a framework for providing optimal medical care during a potential bioterrorist attack or other public health emergency.
How well do you know your institutions’ plans and protocols for these types of events? How personally prepared are you and your families? Overall, what should your highest concerns be in order to prepare yourself now and in the future?
Definitions
The term disaster is defined many ways, but typically all definitions involve some sort of impact on the community and interruption of services from business as usual beyond the point where outside assistance is needed. Defining what is meant by a mass casualty incident (MCI), on the other hand, is more relative to the location in which it is being declared.
“Typically a mass casualty event is thought of as one in which the number of patients exceeds the amount of resources that are routinely available,” says Andrew Garrett, MD, FAAP, the director of disaster response and pediatric preparedness programs at the National Center for Disaster Preparedness at Columbia University’s Joseph L. Mailman School of Public Health, New York. “But that is a dynamic definition because in Chicago a bus accident with 15 patients might not be a mass casualty incident, but in rural Cody, Wyoming, a car accident with four people might be. It’s where you exceed the resources that are available locally that is important.”
The difference between an emergency, a disaster, or an MCI revolves more around semantics, the environment in which you will work, and the short-term goals of patient care. “We’re not asking people to reinvent the way in which they practice medicine,” says Dr. Garrett “but a disaster or MCI changes the paradigm in which they do it—to do the most good for the most people.”
Who’s in Charge?
The Hospital Emergency Incident Command System (HEICS) was adapted from a plan to coordinate and improve the safety of the wildland firefighting system in California. It was transitioned to serve as a model in hospitals to meet the same goals of staff accountability and safety during a disaster response. HEICS places one “incident commander” at the top of the pyramid in charge of all the separate areas of responsibility, such as logistics, finance, operations, medical care, safety, and so on.
“The way the system works,” says Dr. Garrett, “is that everyone working in a hospital response is supervised by only one person who answers to the command staff. The goal is that there’s one incident commander who knows everything that’s going on at the incident to avoid the trap of multiple people making command decisions at the same time.”
Redundant command structure is a common problem in a large-scale response to disaster. That was certainly the case in Hurricane Katrina, he says, where multiple agencies—federal, state, and local—did not follow this model of disaster response.
“It’s a simple concept,” says Dr. Garrett, “but unless responders practice it, it is difficult to utilize in a real emergency.”
Every hospital should have a HEICS or similar structure set up and the key emergency response roles pre-identified by job title, he says. And while knowledge of weapons of mass destruction (WMD) and incident command is improving, says Stephen V. Cantrill, MD, FACEP, associate director, Department of Emergency Medicine at Denver Health Medical Center, “Some hospitals have taken it seriously; others wish the whole thing would go away.”
More than likely, in the event of a disaster, the HEICS organizational tree is outlined all the way to the top commander in your hospital’s plan. Your role, in general, may have already been determined in this plan, but the conventional wisdom in your hospital (as in most) may be: You’ll learn your roles and responsibilities when the time comes. In fact, depending on your setting, the hospitalist may hold the most senior position in-house overnight or on the weekend—especially if there is not an emergency department at the hospital.
“The thing is, at first people are going to look to the most senior clinician to be in charge during a crisis,” says Dr. Garrett. Perhaps the smaller the hospital, the more you need to know what to do and what is expected of you to fit into the larger picture in the community. “And even if it is a smaller hospital the system and the needs are the same.”
What Types of Care?
Although many types of events can be handled the same way, some involve additional concerns. “With WMD or a contagious disease outbreak, there is the added issue of ‘What’s the risk to me as a provider in the hospital?’” says Dr. Garrett. “And if it’s a community or statewide or national event, ‘What’s the risk to my family?’ Then you’re dealing with issues that aren’t business as usual.”
The hospitalist and the administration will then have to think about other complex issues such as how many people are not going to come to work. Added to that, with a smaller staff, you may need to ask, “What will the scope of my practice be if I’m called to the front of the hospital to help do triage? Roles and responsibilities can change very quickly,” he says.
“Hospitalists are invaluable resources in an institution and in fact [in disaster events] they will be pressed into service because of their location,” says Dr. Cantrill, who with colleagues has trained 15,000 healthcare providers throughout Colorado as one of 17 centers to receive a three-year grant from the Health Resources Services Administration (HRSA) to conduct WMD training. “Especially in the private sector when it hits the fan, the hospitalist is going to be one of the first people to be called.”
In most disasters, the hospitalist’s medical practice will be a departure from the details of daily practice. “Because the majority of hospitalists have internal medicine as their background … they tend to be very detail oriented, which is really their strength,” says Dr. Cantrill. “But in a case like this, they may not have that luxury.”
Another major consideration and “probably the stickiest one,” is altering your standards of care in terms of providing efficiency care or austere care as opposed to what you normally consider appropriate medical care.
What hospitalists will do in any disaster depends on the event—natural, biological, chemical, or use of weaponry—and how your metropolitan or rural area is set up. If it is a biological or bioterrorist event, the pathogen involved may make a difference. Although anthrax is not contagious, for instance, in the event of a large-scale airborne anthrax attack, the need for ventilators will quickly overwhelm resources.2 “That’s one of our largest areas of vulnerability,” says Dr. Cantrill, “whether we’re talking influenza or pneumonic plague, it still is an important factor: How many people can I support?”
The issue of limited ventilators may not be completely soluble, he explains. In ordinary circumstances hospitals can get, say, ventilators from a strategic national stockpile from which equipment can be flown out within 12 hours. Yet if an influenza pandemic breaks out, then the entire country may be involved, rendering that plan inoperable. And even if you have extra ventilators, do you have extra respiratory techs to administer them?
Dr. Cantrill’s institution, with a grant received from HRSA, offers a two-hour course to train people with some medical knowledge to be respiratory assistants who can manage ventilated patients in an emergency.
Injuries may increase exponentially in the case of a disaster. Other needs include vaccinations, treatment for dehydration, serious heat- and cold-related illness, or threats from floodwater (i.e., water laced with toxic chemicals, human waste, fire ants, rats, and snakes).3
Kate Rathbun, MD, MPH, family physician in Baton Rouge, La., is certified in disaster management and knows well the problems that can arise in providing medical care in such an event.4 When Hurricane Katrina hit in 2005, everyone in range of the winds, rain, and destruction, “hunkered down to weather the storm.” The day after the storm, Dr. Rathbun joined other providers and administrators, opened their clinic, and readied themselves to treat trauma and lacerations. It soon became obvious that their biggest health issue was the inability of the displaced to manage their chronic diseases. (Baton Rouge’s normal population of 600,000 exceeded a million within days.)
In cases of diabetes, cardiac disease, HIV infection, or tuberculosis, for example, being without medications might mean lethal disease exacerbations.3 In many cases, patients have no prior history documentation on presentation, and with computers often shut down the provider is faced with prescribing for or actually putting a stock of medications into patients’ hands.
Additional concerns pertain to those who cannot receive hemodialysis or seizure prophylaxis; or disrupted care for those with special needs such as hospice patients, the mentally and physically disabled, the elderly, and individuals in detox programs.
When Dr. Rathbun and her coworkers put a couple of nurses on the phones to handle incoming requests for drugs, she gave them some standards: If it’s for chronic disease medications, prescribe a 30-day supply and three refills (to ensure that 30 days later they would not once again be inundated with calls). When patients requested narcotics or scheduled drugs, they were told they would have to be seen by a provider.
Branching Points and Skill Sets
What will your community expect your institution to respond to and provide in the event of disaster? Here is where hospitalists can delineate what they can do when the time comes, says Erin Stucky, MD, a pediatric hospitalist at Children’s Hospital, San Diego.
“Most disaster preparedness algorithms have roles based on ‘hospital-based providers,’” she says, “but when it comes down to medical administration, many of them stop at the emergency department.”
From that point on they are likely to say “I don’t know”—that is, the rest of that decision tree is left in the hands of whoever is in the lead positions of physician, administrator, and nurse.
“That’s where the hospitalist can say, ‘Let me tell you my skill set,’” says Dr. Stucky, such as “I can triage patients; I can help to coordinate and disseminate information or help to outside providers who are calling; I can help to coordinate provider groups to go to different areas within our hospital to coordinate staffing … because I know operating rooms or I know this subset of patient types.”
At some institutions where hospitalists have been around for a longer time the disaster plan’s algorithm has branching points that don’t end in the emergency department. “Each [branch] has separate blocks that are horizontally equivalent,” says Dr. Stucky, “and the bleed-down [recognizes] the hospitalist as the major ward medical officer responsible for ensuring that floor 6, that’s neuro, and floor 5, hem-onc, and so on, have the correct staffing and are responsible for people reporting to them as well as dividing them as a labor pool into who’s available to go where.”
In general, however, regardless of setting, she says, a “hospitalist knows intimately the structure of the hospital, the flow between units, and can help other patients to get to different parts of the institution where care is still safe, such as observation areas.”
Communications: Up and Down, Out and In
Part of the global-facility thought process must include what communications will be for everything from the county medical system and EMS response to, within an institution, the communication between floors and between people on horizontal lines of authority. In addition, information in and out of the hospital from workers to their families is crucial so that workers can concentrate on the tasks at hand.
Questions must be considered ahead of time: How do I communicate to those people outside whom I need to have come in? How do I get response to the appropriate people who are calling in to find out how many patients we’re caring for? There may be other calls from someone who says, for example, that the ventilator has stopped working for her elderly mother.
And hospitalists must also be ready to support the urgent care or primary care satellite clinics and communicate what’s going on at the hospital, says Dr. Rathbun, “so that someone like me, who is a primary care practitioner in the community, can know that if I call this number or this person, I’m going to be able to say, ‘I’m down here at the [clinic] and here’s what I’ve got,’ or “I know things are terrible, but I have a diabetic you had in the hospital three weeks ago who’s crashed again, and you’ve got to find him a bed.’”
Communication plans might include the provision of satellite phones or two-way radios, says Dr. Stucky, and this will affect concrete issues, such as staffing and allowances for who can come and leave.
“In our institution we make this [communication] a unit-specific responsibility of the nurse team leader,” she says. “The nurses each have a phone and those nurse phones are freed up for any person available on that unit to be used to communicate with the outside world.”
Personal Disaster Plans
“I think another vitally important—and I mean vital importance in the same manner as vital signs—is for each hospitalist to have a personal disaster plan for their family/personal life,” says Mitchell Wilson, MD, medical director, FirstHealth of the Carolinas Hospitalist Services and section chief of Hospital Medicine in the Department of Medicine at the University of North Carolina at Chapel Hill. “As the front line ‘foot soldier,’ the potential to harm our families during a pandemic is enormous.”
Dr. Garrett agrees. “One of the things that we’re not so good at in this country is coming up with emergency plans for our own family—even those of us who are in the medical business and take care of others,” he says. “Taking this step just makes good sense—and serves to be able to maximize your own availability and also be confident that you have the ways and means to know that your family is safe and secure and given the best opportunity to survive in a disaster.”
According to Dr. Wilson, families with vulnerable members, such as the young, elderly, and infirm, must have a plan in place to minimize the risk to them. “The hospitalist who comes home sick [or] infected is a danger to the very safe place [to] which [hospitalists and their families] seek refuge,” he says.
Preparedness includes delineating in your family what your points of contact will be. “Part of the stress that’s involved in being a physician and being expected to report to work [may involve] worrying where your family is or whether they have a safe meeting place; who’s picking up the children from school; does the school for my children have a plan, etc.,” says Dr. Garrett.
If you know that your children’s school has an emergency plan, your spouse’s workplace has a plan, and any relative in a long-term care facility has a plan, you’ll be much more likely to stay on the job and care for patients.
“And if my child is on a school bus that needs to be evacuated somewhere out of town,” he says, “I want to know there’s a phone number that my whole family knows to reconnect somehow.”
No Assumptions
Losing utility power is always a concern in emergencies and disasters. “After 9/11 in New York City, lots of people flooded into emergency departments,” says Ann Waller, ScD, an associate professor in the Department of Emergency Medicine at the University of North Carolina at Chapel Hill and the UNC director for NC DETECT. (See “Disease Surveillance,” p. 20.)
“The emergency departments abandoned their electronic systems and went back to paper and pencil because it was faster to just do the bare minimum … and get them into each team than to enter all the information required,” she explains. “That was a real eye-opener for those of us who rely on electronic data.”
Preparing for crisis involves imagining the inaccessibility of all electronic communications and records, including data collection and surveillance, pharmacy, e-mail, and historical documentation and other medical records.
The general rule in disaster preparedness is to plan for 72-hour capacity: How and what do I need to exist for 72 hours? “And the standard is that you should try to do that for your average daily census plus 100 patients,” says Dr. Stucky.
Scheduling and staffing is another issue. “Be prepared to provide flex staffing and scheduling to provide surge capacity,” says Dr. Wilson.
Think on Your Feet: Training
If they are so inclined, hospitalists can become involved in disaster response, through disaster medical assistance teams, community emergency response teams, or through the Red Cross—to name a few. And there are plenty of ways to take advantage of free training, some of which provide CME.
Another important question to ask of your institution, says Dr. Stucky (who co-presented on the topic of disaster preparedness at this year’s SHM Annual Meeting) is whether they have run any mock disasters.
“You have to do that,” she says. “Half of disaster response is preparedness, but the other half is thinking on your feet. And there’s no way to do that without mocking a drill.”
While there can be value in computer-run mock-ups, “there’s nothing like doing it,” she says. “We learn at least 25 things every time we do it.” And though one drill does not a totally prepared institution make, “it does mean at least you have the right people in those strategic positions [and they] are people who can think on their feet.”
A valuable training resource from AHRQ is listed in the resources at the end of this article.5
Be Prepared
With the vast amount of information on disaster preparedness available, one clear goal is to narrow it to avoid feeling overwhelmed.
“I think that is a real challenge,” says Dr. Cantrill, “but the first step is the motivation to at least look.”
Take for example the motivation of a flu pandemic. “It’s going to happen sooner or later, one of these days, but we know it this time,” says Waller. “We have the ability to be more prepared. … This is a huge opportunity to see it coming and to do as much as we can [correctly]. Which is not to say we can avoid everything, but at least we can be as prepared as we’ve ever been able to be.”
Conclusion
For hospitalists, there are several key techniques for individuals to be able to increase their readiness for disaster in the workplace. The first is to avoid relying initially or entirely on external help to supply a response, says Dr. Garrett: “You are the medical response, and there may be a delay until outside assistance is available.”
A second key is to visualize—as well as possible—any circumstances you might face personally and professionally and to formulate questions, seek answers, and talk to colleagues and supervisors about what your role will be. A third factor is to participate in training in the form of drills and tabletop exercises for your hospital. An unpracticed disaster plan may be more dangerous than no plan at all. TH
Andrea Sattinger also writes the “Alliances” department in this issue.
References
- AHRQ. Altered Standards of Care in Mass Casualty Events. Rockville, MD: Agency for Healthcare Research and Quality; April 2005:Health Systems Research Inc. under Contract No. 290-04-0010.
- Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004 Sep;44(3):253-261.
- Greenough PG, Kirsch TD. Hurricane Katrina. Public health response—assessing needs. N Engl J Med. 2005 Oct 13;353(15):1544-1546.
- Rathbun KC, Cranmer H. Hurricane Katrina and disaster medical care. N Engl J Med. 2006 Feb 16;354:772-773.
- Hsu EB, Jenckes MW, Catlett CL, et al. Training of hospital staff to respond to a mass casualty incident. Evidence Report/Technology Assessment No. 95. Rockville, MD: Agency for Healthcare Research and Quality. Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018; June 2004: AHRQ Publication No. 04-E015-2. Accessible at: www.ahrq.gov/downloads/pub/evidence/pdf/hospmci/hospmci.pdf. Last accessed June 1, 2006.
Resources
National Links
- Centers for Disease Control, Emergency Preparedness and Response: www.bt.cdc.gov/
- The Hospital Emergency Incident Command System (HEICS) is an emergency management system that employs a logical management structure, defined responsibilities, clear reporting channels, and a common nomenclature to help unify hospitals with other emergency responders: www.emsa.cahwnet.gov/dms2/heics3.htm
- State, local, and tribal public health departments have their own public health preparedness and response plans.
- The National Center for Environmental Health (NCEH): www.cdc.gov/nceh/emergency.htm.
- Two other CDC resources contain materials to address public health preparedness needs: the Division of Emergency and Environmental Health Services (EEHS) and the Environmental Public Health Readiness Branch (EPHRB). See all-hazards public health emergency response guide): www.cdc.gov/nceh/eehs/
- U.S. Department of Homeland Security, for family preparedness: www.ready.gov/
- AHRQ bioterrorism link: www.ahrq.gov/news/pubcat/c_biot.htm#biot002
- George Washington University Institute for Crisis, Disaster, and Risk Management offers programs, including training, in the area of crisis, emergency and risk management: www.gwu.edu/~icdrm/
- North Carolina Links—North Carolina Office of Public Health Preparedness and Response (NC PHPR): www.epi.state.nc.us/epi/phpr/provides information and resources regarding the threat of bioterrorism and other emerging infectious diseases within the state and around the nation.
- The Health Alert Network (HAN) system is designed to immediately alert key health officials and care providers in North Carolina to acts of bioterrorism as well as other types of emerging disease threats: www.nchan.org/
- DPH Immunization branch: www.immunizenc.com/
- State Web sites, such as San Diego Country Office of Emergency Systems: www.co.sandiego.ca.us/oes/ or the County of San Diego Health and Human Services Terrorism Preparedness: www.co.san-diego.ca.us/terrorism/links.html
In March 2005 the Agency for Healthcare Research and Quality and the HHS Office of Public Health Emergency Preparedness published a report of guidelines for officials on how to plan for delivering health and medical care in a mass casualty event.1
After federal, state, and local authorities’ failure to supply desperately needed assistance following Hurricane Katrina, that report of recommendations from a 39-member panel of experts in bioethics, emergency medicine, emergency management, health administration, health law, and policy is more crucial than ever. This report offers a framework for providing optimal medical care during a potential bioterrorist attack or other public health emergency.
How well do you know your institutions’ plans and protocols for these types of events? How personally prepared are you and your families? Overall, what should your highest concerns be in order to prepare yourself now and in the future?
Definitions
The term disaster is defined many ways, but typically all definitions involve some sort of impact on the community and interruption of services from business as usual beyond the point where outside assistance is needed. Defining what is meant by a mass casualty incident (MCI), on the other hand, is more relative to the location in which it is being declared.
“Typically a mass casualty event is thought of as one in which the number of patients exceeds the amount of resources that are routinely available,” says Andrew Garrett, MD, FAAP, the director of disaster response and pediatric preparedness programs at the National Center for Disaster Preparedness at Columbia University’s Joseph L. Mailman School of Public Health, New York. “But that is a dynamic definition because in Chicago a bus accident with 15 patients might not be a mass casualty incident, but in rural Cody, Wyoming, a car accident with four people might be. It’s where you exceed the resources that are available locally that is important.”
The difference between an emergency, a disaster, or an MCI revolves more around semantics, the environment in which you will work, and the short-term goals of patient care. “We’re not asking people to reinvent the way in which they practice medicine,” says Dr. Garrett “but a disaster or MCI changes the paradigm in which they do it—to do the most good for the most people.”
Who’s in Charge?
The Hospital Emergency Incident Command System (HEICS) was adapted from a plan to coordinate and improve the safety of the wildland firefighting system in California. It was transitioned to serve as a model in hospitals to meet the same goals of staff accountability and safety during a disaster response. HEICS places one “incident commander” at the top of the pyramid in charge of all the separate areas of responsibility, such as logistics, finance, operations, medical care, safety, and so on.
“The way the system works,” says Dr. Garrett, “is that everyone working in a hospital response is supervised by only one person who answers to the command staff. The goal is that there’s one incident commander who knows everything that’s going on at the incident to avoid the trap of multiple people making command decisions at the same time.”
Redundant command structure is a common problem in a large-scale response to disaster. That was certainly the case in Hurricane Katrina, he says, where multiple agencies—federal, state, and local—did not follow this model of disaster response.
“It’s a simple concept,” says Dr. Garrett, “but unless responders practice it, it is difficult to utilize in a real emergency.”
Every hospital should have a HEICS or similar structure set up and the key emergency response roles pre-identified by job title, he says. And while knowledge of weapons of mass destruction (WMD) and incident command is improving, says Stephen V. Cantrill, MD, FACEP, associate director, Department of Emergency Medicine at Denver Health Medical Center, “Some hospitals have taken it seriously; others wish the whole thing would go away.”
More than likely, in the event of a disaster, the HEICS organizational tree is outlined all the way to the top commander in your hospital’s plan. Your role, in general, may have already been determined in this plan, but the conventional wisdom in your hospital (as in most) may be: You’ll learn your roles and responsibilities when the time comes. In fact, depending on your setting, the hospitalist may hold the most senior position in-house overnight or on the weekend—especially if there is not an emergency department at the hospital.
“The thing is, at first people are going to look to the most senior clinician to be in charge during a crisis,” says Dr. Garrett. Perhaps the smaller the hospital, the more you need to know what to do and what is expected of you to fit into the larger picture in the community. “And even if it is a smaller hospital the system and the needs are the same.”
What Types of Care?
Although many types of events can be handled the same way, some involve additional concerns. “With WMD or a contagious disease outbreak, there is the added issue of ‘What’s the risk to me as a provider in the hospital?’” says Dr. Garrett. “And if it’s a community or statewide or national event, ‘What’s the risk to my family?’ Then you’re dealing with issues that aren’t business as usual.”
The hospitalist and the administration will then have to think about other complex issues such as how many people are not going to come to work. Added to that, with a smaller staff, you may need to ask, “What will the scope of my practice be if I’m called to the front of the hospital to help do triage? Roles and responsibilities can change very quickly,” he says.
“Hospitalists are invaluable resources in an institution and in fact [in disaster events] they will be pressed into service because of their location,” says Dr. Cantrill, who with colleagues has trained 15,000 healthcare providers throughout Colorado as one of 17 centers to receive a three-year grant from the Health Resources Services Administration (HRSA) to conduct WMD training. “Especially in the private sector when it hits the fan, the hospitalist is going to be one of the first people to be called.”
In most disasters, the hospitalist’s medical practice will be a departure from the details of daily practice. “Because the majority of hospitalists have internal medicine as their background … they tend to be very detail oriented, which is really their strength,” says Dr. Cantrill. “But in a case like this, they may not have that luxury.”
Another major consideration and “probably the stickiest one,” is altering your standards of care in terms of providing efficiency care or austere care as opposed to what you normally consider appropriate medical care.
What hospitalists will do in any disaster depends on the event—natural, biological, chemical, or use of weaponry—and how your metropolitan or rural area is set up. If it is a biological or bioterrorist event, the pathogen involved may make a difference. Although anthrax is not contagious, for instance, in the event of a large-scale airborne anthrax attack, the need for ventilators will quickly overwhelm resources.2 “That’s one of our largest areas of vulnerability,” says Dr. Cantrill, “whether we’re talking influenza or pneumonic plague, it still is an important factor: How many people can I support?”
The issue of limited ventilators may not be completely soluble, he explains. In ordinary circumstances hospitals can get, say, ventilators from a strategic national stockpile from which equipment can be flown out within 12 hours. Yet if an influenza pandemic breaks out, then the entire country may be involved, rendering that plan inoperable. And even if you have extra ventilators, do you have extra respiratory techs to administer them?
Dr. Cantrill’s institution, with a grant received from HRSA, offers a two-hour course to train people with some medical knowledge to be respiratory assistants who can manage ventilated patients in an emergency.
Injuries may increase exponentially in the case of a disaster. Other needs include vaccinations, treatment for dehydration, serious heat- and cold-related illness, or threats from floodwater (i.e., water laced with toxic chemicals, human waste, fire ants, rats, and snakes).3
Kate Rathbun, MD, MPH, family physician in Baton Rouge, La., is certified in disaster management and knows well the problems that can arise in providing medical care in such an event.4 When Hurricane Katrina hit in 2005, everyone in range of the winds, rain, and destruction, “hunkered down to weather the storm.” The day after the storm, Dr. Rathbun joined other providers and administrators, opened their clinic, and readied themselves to treat trauma and lacerations. It soon became obvious that their biggest health issue was the inability of the displaced to manage their chronic diseases. (Baton Rouge’s normal population of 600,000 exceeded a million within days.)
In cases of diabetes, cardiac disease, HIV infection, or tuberculosis, for example, being without medications might mean lethal disease exacerbations.3 In many cases, patients have no prior history documentation on presentation, and with computers often shut down the provider is faced with prescribing for or actually putting a stock of medications into patients’ hands.
Additional concerns pertain to those who cannot receive hemodialysis or seizure prophylaxis; or disrupted care for those with special needs such as hospice patients, the mentally and physically disabled, the elderly, and individuals in detox programs.
When Dr. Rathbun and her coworkers put a couple of nurses on the phones to handle incoming requests for drugs, she gave them some standards: If it’s for chronic disease medications, prescribe a 30-day supply and three refills (to ensure that 30 days later they would not once again be inundated with calls). When patients requested narcotics or scheduled drugs, they were told they would have to be seen by a provider.
Branching Points and Skill Sets
What will your community expect your institution to respond to and provide in the event of disaster? Here is where hospitalists can delineate what they can do when the time comes, says Erin Stucky, MD, a pediatric hospitalist at Children’s Hospital, San Diego.
“Most disaster preparedness algorithms have roles based on ‘hospital-based providers,’” she says, “but when it comes down to medical administration, many of them stop at the emergency department.”
From that point on they are likely to say “I don’t know”—that is, the rest of that decision tree is left in the hands of whoever is in the lead positions of physician, administrator, and nurse.
“That’s where the hospitalist can say, ‘Let me tell you my skill set,’” says Dr. Stucky, such as “I can triage patients; I can help to coordinate and disseminate information or help to outside providers who are calling; I can help to coordinate provider groups to go to different areas within our hospital to coordinate staffing … because I know operating rooms or I know this subset of patient types.”
At some institutions where hospitalists have been around for a longer time the disaster plan’s algorithm has branching points that don’t end in the emergency department. “Each [branch] has separate blocks that are horizontally equivalent,” says Dr. Stucky, “and the bleed-down [recognizes] the hospitalist as the major ward medical officer responsible for ensuring that floor 6, that’s neuro, and floor 5, hem-onc, and so on, have the correct staffing and are responsible for people reporting to them as well as dividing them as a labor pool into who’s available to go where.”
In general, however, regardless of setting, she says, a “hospitalist knows intimately the structure of the hospital, the flow between units, and can help other patients to get to different parts of the institution where care is still safe, such as observation areas.”
Communications: Up and Down, Out and In
Part of the global-facility thought process must include what communications will be for everything from the county medical system and EMS response to, within an institution, the communication between floors and between people on horizontal lines of authority. In addition, information in and out of the hospital from workers to their families is crucial so that workers can concentrate on the tasks at hand.
Questions must be considered ahead of time: How do I communicate to those people outside whom I need to have come in? How do I get response to the appropriate people who are calling in to find out how many patients we’re caring for? There may be other calls from someone who says, for example, that the ventilator has stopped working for her elderly mother.
And hospitalists must also be ready to support the urgent care or primary care satellite clinics and communicate what’s going on at the hospital, says Dr. Rathbun, “so that someone like me, who is a primary care practitioner in the community, can know that if I call this number or this person, I’m going to be able to say, ‘I’m down here at the [clinic] and here’s what I’ve got,’ or “I know things are terrible, but I have a diabetic you had in the hospital three weeks ago who’s crashed again, and you’ve got to find him a bed.’”
Communication plans might include the provision of satellite phones or two-way radios, says Dr. Stucky, and this will affect concrete issues, such as staffing and allowances for who can come and leave.
“In our institution we make this [communication] a unit-specific responsibility of the nurse team leader,” she says. “The nurses each have a phone and those nurse phones are freed up for any person available on that unit to be used to communicate with the outside world.”
Personal Disaster Plans
“I think another vitally important—and I mean vital importance in the same manner as vital signs—is for each hospitalist to have a personal disaster plan for their family/personal life,” says Mitchell Wilson, MD, medical director, FirstHealth of the Carolinas Hospitalist Services and section chief of Hospital Medicine in the Department of Medicine at the University of North Carolina at Chapel Hill. “As the front line ‘foot soldier,’ the potential to harm our families during a pandemic is enormous.”
Dr. Garrett agrees. “One of the things that we’re not so good at in this country is coming up with emergency plans for our own family—even those of us who are in the medical business and take care of others,” he says. “Taking this step just makes good sense—and serves to be able to maximize your own availability and also be confident that you have the ways and means to know that your family is safe and secure and given the best opportunity to survive in a disaster.”
According to Dr. Wilson, families with vulnerable members, such as the young, elderly, and infirm, must have a plan in place to minimize the risk to them. “The hospitalist who comes home sick [or] infected is a danger to the very safe place [to] which [hospitalists and their families] seek refuge,” he says.
Preparedness includes delineating in your family what your points of contact will be. “Part of the stress that’s involved in being a physician and being expected to report to work [may involve] worrying where your family is or whether they have a safe meeting place; who’s picking up the children from school; does the school for my children have a plan, etc.,” says Dr. Garrett.
If you know that your children’s school has an emergency plan, your spouse’s workplace has a plan, and any relative in a long-term care facility has a plan, you’ll be much more likely to stay on the job and care for patients.
“And if my child is on a school bus that needs to be evacuated somewhere out of town,” he says, “I want to know there’s a phone number that my whole family knows to reconnect somehow.”
No Assumptions
Losing utility power is always a concern in emergencies and disasters. “After 9/11 in New York City, lots of people flooded into emergency departments,” says Ann Waller, ScD, an associate professor in the Department of Emergency Medicine at the University of North Carolina at Chapel Hill and the UNC director for NC DETECT. (See “Disease Surveillance,” p. 20.)
“The emergency departments abandoned their electronic systems and went back to paper and pencil because it was faster to just do the bare minimum … and get them into each team than to enter all the information required,” she explains. “That was a real eye-opener for those of us who rely on electronic data.”
Preparing for crisis involves imagining the inaccessibility of all electronic communications and records, including data collection and surveillance, pharmacy, e-mail, and historical documentation and other medical records.
The general rule in disaster preparedness is to plan for 72-hour capacity: How and what do I need to exist for 72 hours? “And the standard is that you should try to do that for your average daily census plus 100 patients,” says Dr. Stucky.
Scheduling and staffing is another issue. “Be prepared to provide flex staffing and scheduling to provide surge capacity,” says Dr. Wilson.
Think on Your Feet: Training
If they are so inclined, hospitalists can become involved in disaster response, through disaster medical assistance teams, community emergency response teams, or through the Red Cross—to name a few. And there are plenty of ways to take advantage of free training, some of which provide CME.
Another important question to ask of your institution, says Dr. Stucky (who co-presented on the topic of disaster preparedness at this year’s SHM Annual Meeting) is whether they have run any mock disasters.
“You have to do that,” she says. “Half of disaster response is preparedness, but the other half is thinking on your feet. And there’s no way to do that without mocking a drill.”
While there can be value in computer-run mock-ups, “there’s nothing like doing it,” she says. “We learn at least 25 things every time we do it.” And though one drill does not a totally prepared institution make, “it does mean at least you have the right people in those strategic positions [and they] are people who can think on their feet.”
A valuable training resource from AHRQ is listed in the resources at the end of this article.5
Be Prepared
With the vast amount of information on disaster preparedness available, one clear goal is to narrow it to avoid feeling overwhelmed.
“I think that is a real challenge,” says Dr. Cantrill, “but the first step is the motivation to at least look.”
Take for example the motivation of a flu pandemic. “It’s going to happen sooner or later, one of these days, but we know it this time,” says Waller. “We have the ability to be more prepared. … This is a huge opportunity to see it coming and to do as much as we can [correctly]. Which is not to say we can avoid everything, but at least we can be as prepared as we’ve ever been able to be.”
Conclusion
For hospitalists, there are several key techniques for individuals to be able to increase their readiness for disaster in the workplace. The first is to avoid relying initially or entirely on external help to supply a response, says Dr. Garrett: “You are the medical response, and there may be a delay until outside assistance is available.”
A second key is to visualize—as well as possible—any circumstances you might face personally and professionally and to formulate questions, seek answers, and talk to colleagues and supervisors about what your role will be. A third factor is to participate in training in the form of drills and tabletop exercises for your hospital. An unpracticed disaster plan may be more dangerous than no plan at all. TH
Andrea Sattinger also writes the “Alliances” department in this issue.
References
- AHRQ. Altered Standards of Care in Mass Casualty Events. Rockville, MD: Agency for Healthcare Research and Quality; April 2005:Health Systems Research Inc. under Contract No. 290-04-0010.
- Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004 Sep;44(3):253-261.
- Greenough PG, Kirsch TD. Hurricane Katrina. Public health response—assessing needs. N Engl J Med. 2005 Oct 13;353(15):1544-1546.
- Rathbun KC, Cranmer H. Hurricane Katrina and disaster medical care. N Engl J Med. 2006 Feb 16;354:772-773.
- Hsu EB, Jenckes MW, Catlett CL, et al. Training of hospital staff to respond to a mass casualty incident. Evidence Report/Technology Assessment No. 95. Rockville, MD: Agency for Healthcare Research and Quality. Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018; June 2004: AHRQ Publication No. 04-E015-2. Accessible at: www.ahrq.gov/downloads/pub/evidence/pdf/hospmci/hospmci.pdf. Last accessed June 1, 2006.
Resources
National Links
- Centers for Disease Control, Emergency Preparedness and Response: www.bt.cdc.gov/
- The Hospital Emergency Incident Command System (HEICS) is an emergency management system that employs a logical management structure, defined responsibilities, clear reporting channels, and a common nomenclature to help unify hospitals with other emergency responders: www.emsa.cahwnet.gov/dms2/heics3.htm
- State, local, and tribal public health departments have their own public health preparedness and response plans.
- The National Center for Environmental Health (NCEH): www.cdc.gov/nceh/emergency.htm.
- Two other CDC resources contain materials to address public health preparedness needs: the Division of Emergency and Environmental Health Services (EEHS) and the Environmental Public Health Readiness Branch (EPHRB). See all-hazards public health emergency response guide): www.cdc.gov/nceh/eehs/
- U.S. Department of Homeland Security, for family preparedness: www.ready.gov/
- AHRQ bioterrorism link: www.ahrq.gov/news/pubcat/c_biot.htm#biot002
- George Washington University Institute for Crisis, Disaster, and Risk Management offers programs, including training, in the area of crisis, emergency and risk management: www.gwu.edu/~icdrm/
- North Carolina Links—North Carolina Office of Public Health Preparedness and Response (NC PHPR): www.epi.state.nc.us/epi/phpr/provides information and resources regarding the threat of bioterrorism and other emerging infectious diseases within the state and around the nation.
- The Health Alert Network (HAN) system is designed to immediately alert key health officials and care providers in North Carolina to acts of bioterrorism as well as other types of emerging disease threats: www.nchan.org/
- DPH Immunization branch: www.immunizenc.com/
- State Web sites, such as San Diego Country Office of Emergency Systems: www.co.sandiego.ca.us/oes/ or the County of San Diego Health and Human Services Terrorism Preparedness: www.co.san-diego.ca.us/terrorism/links.html
In March 2005 the Agency for Healthcare Research and Quality and the HHS Office of Public Health Emergency Preparedness published a report of guidelines for officials on how to plan for delivering health and medical care in a mass casualty event.1
After federal, state, and local authorities’ failure to supply desperately needed assistance following Hurricane Katrina, that report of recommendations from a 39-member panel of experts in bioethics, emergency medicine, emergency management, health administration, health law, and policy is more crucial than ever. This report offers a framework for providing optimal medical care during a potential bioterrorist attack or other public health emergency.
How well do you know your institutions’ plans and protocols for these types of events? How personally prepared are you and your families? Overall, what should your highest concerns be in order to prepare yourself now and in the future?
Definitions
The term disaster is defined many ways, but typically all definitions involve some sort of impact on the community and interruption of services from business as usual beyond the point where outside assistance is needed. Defining what is meant by a mass casualty incident (MCI), on the other hand, is more relative to the location in which it is being declared.
“Typically a mass casualty event is thought of as one in which the number of patients exceeds the amount of resources that are routinely available,” says Andrew Garrett, MD, FAAP, the director of disaster response and pediatric preparedness programs at the National Center for Disaster Preparedness at Columbia University’s Joseph L. Mailman School of Public Health, New York. “But that is a dynamic definition because in Chicago a bus accident with 15 patients might not be a mass casualty incident, but in rural Cody, Wyoming, a car accident with four people might be. It’s where you exceed the resources that are available locally that is important.”
The difference between an emergency, a disaster, or an MCI revolves more around semantics, the environment in which you will work, and the short-term goals of patient care. “We’re not asking people to reinvent the way in which they practice medicine,” says Dr. Garrett “but a disaster or MCI changes the paradigm in which they do it—to do the most good for the most people.”
Who’s in Charge?
The Hospital Emergency Incident Command System (HEICS) was adapted from a plan to coordinate and improve the safety of the wildland firefighting system in California. It was transitioned to serve as a model in hospitals to meet the same goals of staff accountability and safety during a disaster response. HEICS places one “incident commander” at the top of the pyramid in charge of all the separate areas of responsibility, such as logistics, finance, operations, medical care, safety, and so on.
“The way the system works,” says Dr. Garrett, “is that everyone working in a hospital response is supervised by only one person who answers to the command staff. The goal is that there’s one incident commander who knows everything that’s going on at the incident to avoid the trap of multiple people making command decisions at the same time.”
Redundant command structure is a common problem in a large-scale response to disaster. That was certainly the case in Hurricane Katrina, he says, where multiple agencies—federal, state, and local—did not follow this model of disaster response.
“It’s a simple concept,” says Dr. Garrett, “but unless responders practice it, it is difficult to utilize in a real emergency.”
Every hospital should have a HEICS or similar structure set up and the key emergency response roles pre-identified by job title, he says. And while knowledge of weapons of mass destruction (WMD) and incident command is improving, says Stephen V. Cantrill, MD, FACEP, associate director, Department of Emergency Medicine at Denver Health Medical Center, “Some hospitals have taken it seriously; others wish the whole thing would go away.”
More than likely, in the event of a disaster, the HEICS organizational tree is outlined all the way to the top commander in your hospital’s plan. Your role, in general, may have already been determined in this plan, but the conventional wisdom in your hospital (as in most) may be: You’ll learn your roles and responsibilities when the time comes. In fact, depending on your setting, the hospitalist may hold the most senior position in-house overnight or on the weekend—especially if there is not an emergency department at the hospital.
“The thing is, at first people are going to look to the most senior clinician to be in charge during a crisis,” says Dr. Garrett. Perhaps the smaller the hospital, the more you need to know what to do and what is expected of you to fit into the larger picture in the community. “And even if it is a smaller hospital the system and the needs are the same.”
What Types of Care?
Although many types of events can be handled the same way, some involve additional concerns. “With WMD or a contagious disease outbreak, there is the added issue of ‘What’s the risk to me as a provider in the hospital?’” says Dr. Garrett. “And if it’s a community or statewide or national event, ‘What’s the risk to my family?’ Then you’re dealing with issues that aren’t business as usual.”
The hospitalist and the administration will then have to think about other complex issues such as how many people are not going to come to work. Added to that, with a smaller staff, you may need to ask, “What will the scope of my practice be if I’m called to the front of the hospital to help do triage? Roles and responsibilities can change very quickly,” he says.
“Hospitalists are invaluable resources in an institution and in fact [in disaster events] they will be pressed into service because of their location,” says Dr. Cantrill, who with colleagues has trained 15,000 healthcare providers throughout Colorado as one of 17 centers to receive a three-year grant from the Health Resources Services Administration (HRSA) to conduct WMD training. “Especially in the private sector when it hits the fan, the hospitalist is going to be one of the first people to be called.”
In most disasters, the hospitalist’s medical practice will be a departure from the details of daily practice. “Because the majority of hospitalists have internal medicine as their background … they tend to be very detail oriented, which is really their strength,” says Dr. Cantrill. “But in a case like this, they may not have that luxury.”
Another major consideration and “probably the stickiest one,” is altering your standards of care in terms of providing efficiency care or austere care as opposed to what you normally consider appropriate medical care.
What hospitalists will do in any disaster depends on the event—natural, biological, chemical, or use of weaponry—and how your metropolitan or rural area is set up. If it is a biological or bioterrorist event, the pathogen involved may make a difference. Although anthrax is not contagious, for instance, in the event of a large-scale airborne anthrax attack, the need for ventilators will quickly overwhelm resources.2 “That’s one of our largest areas of vulnerability,” says Dr. Cantrill, “whether we’re talking influenza or pneumonic plague, it still is an important factor: How many people can I support?”
The issue of limited ventilators may not be completely soluble, he explains. In ordinary circumstances hospitals can get, say, ventilators from a strategic national stockpile from which equipment can be flown out within 12 hours. Yet if an influenza pandemic breaks out, then the entire country may be involved, rendering that plan inoperable. And even if you have extra ventilators, do you have extra respiratory techs to administer them?
Dr. Cantrill’s institution, with a grant received from HRSA, offers a two-hour course to train people with some medical knowledge to be respiratory assistants who can manage ventilated patients in an emergency.
Injuries may increase exponentially in the case of a disaster. Other needs include vaccinations, treatment for dehydration, serious heat- and cold-related illness, or threats from floodwater (i.e., water laced with toxic chemicals, human waste, fire ants, rats, and snakes).3
Kate Rathbun, MD, MPH, family physician in Baton Rouge, La., is certified in disaster management and knows well the problems that can arise in providing medical care in such an event.4 When Hurricane Katrina hit in 2005, everyone in range of the winds, rain, and destruction, “hunkered down to weather the storm.” The day after the storm, Dr. Rathbun joined other providers and administrators, opened their clinic, and readied themselves to treat trauma and lacerations. It soon became obvious that their biggest health issue was the inability of the displaced to manage their chronic diseases. (Baton Rouge’s normal population of 600,000 exceeded a million within days.)
In cases of diabetes, cardiac disease, HIV infection, or tuberculosis, for example, being without medications might mean lethal disease exacerbations.3 In many cases, patients have no prior history documentation on presentation, and with computers often shut down the provider is faced with prescribing for or actually putting a stock of medications into patients’ hands.
Additional concerns pertain to those who cannot receive hemodialysis or seizure prophylaxis; or disrupted care for those with special needs such as hospice patients, the mentally and physically disabled, the elderly, and individuals in detox programs.
When Dr. Rathbun and her coworkers put a couple of nurses on the phones to handle incoming requests for drugs, she gave them some standards: If it’s for chronic disease medications, prescribe a 30-day supply and three refills (to ensure that 30 days later they would not once again be inundated with calls). When patients requested narcotics or scheduled drugs, they were told they would have to be seen by a provider.
Branching Points and Skill Sets
What will your community expect your institution to respond to and provide in the event of disaster? Here is where hospitalists can delineate what they can do when the time comes, says Erin Stucky, MD, a pediatric hospitalist at Children’s Hospital, San Diego.
“Most disaster preparedness algorithms have roles based on ‘hospital-based providers,’” she says, “but when it comes down to medical administration, many of them stop at the emergency department.”
From that point on they are likely to say “I don’t know”—that is, the rest of that decision tree is left in the hands of whoever is in the lead positions of physician, administrator, and nurse.
“That’s where the hospitalist can say, ‘Let me tell you my skill set,’” says Dr. Stucky, such as “I can triage patients; I can help to coordinate and disseminate information or help to outside providers who are calling; I can help to coordinate provider groups to go to different areas within our hospital to coordinate staffing … because I know operating rooms or I know this subset of patient types.”
At some institutions where hospitalists have been around for a longer time the disaster plan’s algorithm has branching points that don’t end in the emergency department. “Each [branch] has separate blocks that are horizontally equivalent,” says Dr. Stucky, “and the bleed-down [recognizes] the hospitalist as the major ward medical officer responsible for ensuring that floor 6, that’s neuro, and floor 5, hem-onc, and so on, have the correct staffing and are responsible for people reporting to them as well as dividing them as a labor pool into who’s available to go where.”
In general, however, regardless of setting, she says, a “hospitalist knows intimately the structure of the hospital, the flow between units, and can help other patients to get to different parts of the institution where care is still safe, such as observation areas.”
Communications: Up and Down, Out and In
Part of the global-facility thought process must include what communications will be for everything from the county medical system and EMS response to, within an institution, the communication between floors and between people on horizontal lines of authority. In addition, information in and out of the hospital from workers to their families is crucial so that workers can concentrate on the tasks at hand.
Questions must be considered ahead of time: How do I communicate to those people outside whom I need to have come in? How do I get response to the appropriate people who are calling in to find out how many patients we’re caring for? There may be other calls from someone who says, for example, that the ventilator has stopped working for her elderly mother.
And hospitalists must also be ready to support the urgent care or primary care satellite clinics and communicate what’s going on at the hospital, says Dr. Rathbun, “so that someone like me, who is a primary care practitioner in the community, can know that if I call this number or this person, I’m going to be able to say, ‘I’m down here at the [clinic] and here’s what I’ve got,’ or “I know things are terrible, but I have a diabetic you had in the hospital three weeks ago who’s crashed again, and you’ve got to find him a bed.’”
Communication plans might include the provision of satellite phones or two-way radios, says Dr. Stucky, and this will affect concrete issues, such as staffing and allowances for who can come and leave.
“In our institution we make this [communication] a unit-specific responsibility of the nurse team leader,” she says. “The nurses each have a phone and those nurse phones are freed up for any person available on that unit to be used to communicate with the outside world.”
Personal Disaster Plans
“I think another vitally important—and I mean vital importance in the same manner as vital signs—is for each hospitalist to have a personal disaster plan for their family/personal life,” says Mitchell Wilson, MD, medical director, FirstHealth of the Carolinas Hospitalist Services and section chief of Hospital Medicine in the Department of Medicine at the University of North Carolina at Chapel Hill. “As the front line ‘foot soldier,’ the potential to harm our families during a pandemic is enormous.”
Dr. Garrett agrees. “One of the things that we’re not so good at in this country is coming up with emergency plans for our own family—even those of us who are in the medical business and take care of others,” he says. “Taking this step just makes good sense—and serves to be able to maximize your own availability and also be confident that you have the ways and means to know that your family is safe and secure and given the best opportunity to survive in a disaster.”
According to Dr. Wilson, families with vulnerable members, such as the young, elderly, and infirm, must have a plan in place to minimize the risk to them. “The hospitalist who comes home sick [or] infected is a danger to the very safe place [to] which [hospitalists and their families] seek refuge,” he says.
Preparedness includes delineating in your family what your points of contact will be. “Part of the stress that’s involved in being a physician and being expected to report to work [may involve] worrying where your family is or whether they have a safe meeting place; who’s picking up the children from school; does the school for my children have a plan, etc.,” says Dr. Garrett.
If you know that your children’s school has an emergency plan, your spouse’s workplace has a plan, and any relative in a long-term care facility has a plan, you’ll be much more likely to stay on the job and care for patients.
“And if my child is on a school bus that needs to be evacuated somewhere out of town,” he says, “I want to know there’s a phone number that my whole family knows to reconnect somehow.”
No Assumptions
Losing utility power is always a concern in emergencies and disasters. “After 9/11 in New York City, lots of people flooded into emergency departments,” says Ann Waller, ScD, an associate professor in the Department of Emergency Medicine at the University of North Carolina at Chapel Hill and the UNC director for NC DETECT. (See “Disease Surveillance,” p. 20.)
“The emergency departments abandoned their electronic systems and went back to paper and pencil because it was faster to just do the bare minimum … and get them into each team than to enter all the information required,” she explains. “That was a real eye-opener for those of us who rely on electronic data.”
Preparing for crisis involves imagining the inaccessibility of all electronic communications and records, including data collection and surveillance, pharmacy, e-mail, and historical documentation and other medical records.
The general rule in disaster preparedness is to plan for 72-hour capacity: How and what do I need to exist for 72 hours? “And the standard is that you should try to do that for your average daily census plus 100 patients,” says Dr. Stucky.
Scheduling and staffing is another issue. “Be prepared to provide flex staffing and scheduling to provide surge capacity,” says Dr. Wilson.
Think on Your Feet: Training
If they are so inclined, hospitalists can become involved in disaster response, through disaster medical assistance teams, community emergency response teams, or through the Red Cross—to name a few. And there are plenty of ways to take advantage of free training, some of which provide CME.
Another important question to ask of your institution, says Dr. Stucky (who co-presented on the topic of disaster preparedness at this year’s SHM Annual Meeting) is whether they have run any mock disasters.
“You have to do that,” she says. “Half of disaster response is preparedness, but the other half is thinking on your feet. And there’s no way to do that without mocking a drill.”
While there can be value in computer-run mock-ups, “there’s nothing like doing it,” she says. “We learn at least 25 things every time we do it.” And though one drill does not a totally prepared institution make, “it does mean at least you have the right people in those strategic positions [and they] are people who can think on their feet.”
A valuable training resource from AHRQ is listed in the resources at the end of this article.5
Be Prepared
With the vast amount of information on disaster preparedness available, one clear goal is to narrow it to avoid feeling overwhelmed.
“I think that is a real challenge,” says Dr. Cantrill, “but the first step is the motivation to at least look.”
Take for example the motivation of a flu pandemic. “It’s going to happen sooner or later, one of these days, but we know it this time,” says Waller. “We have the ability to be more prepared. … This is a huge opportunity to see it coming and to do as much as we can [correctly]. Which is not to say we can avoid everything, but at least we can be as prepared as we’ve ever been able to be.”
Conclusion
For hospitalists, there are several key techniques for individuals to be able to increase their readiness for disaster in the workplace. The first is to avoid relying initially or entirely on external help to supply a response, says Dr. Garrett: “You are the medical response, and there may be a delay until outside assistance is available.”
A second key is to visualize—as well as possible—any circumstances you might face personally and professionally and to formulate questions, seek answers, and talk to colleagues and supervisors about what your role will be. A third factor is to participate in training in the form of drills and tabletop exercises for your hospital. An unpracticed disaster plan may be more dangerous than no plan at all. TH
Andrea Sattinger also writes the “Alliances” department in this issue.
References
- AHRQ. Altered Standards of Care in Mass Casualty Events. Rockville, MD: Agency for Healthcare Research and Quality; April 2005:Health Systems Research Inc. under Contract No. 290-04-0010.
- Hick JL, Hanfling D, Burstein JL, et al. Health care facility and community strategies for patient care surge capacity. Ann Emerg Med. 2004 Sep;44(3):253-261.
- Greenough PG, Kirsch TD. Hurricane Katrina. Public health response—assessing needs. N Engl J Med. 2005 Oct 13;353(15):1544-1546.
- Rathbun KC, Cranmer H. Hurricane Katrina and disaster medical care. N Engl J Med. 2006 Feb 16;354:772-773.
- Hsu EB, Jenckes MW, Catlett CL, et al. Training of hospital staff to respond to a mass casualty incident. Evidence Report/Technology Assessment No. 95. Rockville, MD: Agency for Healthcare Research and Quality. Prepared by the Johns Hopkins University Evidence-based Practice Center under Contract No. 290-02-0018; June 2004: AHRQ Publication No. 04-E015-2. Accessible at: www.ahrq.gov/downloads/pub/evidence/pdf/hospmci/hospmci.pdf. Last accessed June 1, 2006.
Resources
National Links
- Centers for Disease Control, Emergency Preparedness and Response: www.bt.cdc.gov/
- The Hospital Emergency Incident Command System (HEICS) is an emergency management system that employs a logical management structure, defined responsibilities, clear reporting channels, and a common nomenclature to help unify hospitals with other emergency responders: www.emsa.cahwnet.gov/dms2/heics3.htm
- State, local, and tribal public health departments have their own public health preparedness and response plans.
- The National Center for Environmental Health (NCEH): www.cdc.gov/nceh/emergency.htm.
- Two other CDC resources contain materials to address public health preparedness needs: the Division of Emergency and Environmental Health Services (EEHS) and the Environmental Public Health Readiness Branch (EPHRB). See all-hazards public health emergency response guide): www.cdc.gov/nceh/eehs/
- U.S. Department of Homeland Security, for family preparedness: www.ready.gov/
- AHRQ bioterrorism link: www.ahrq.gov/news/pubcat/c_biot.htm#biot002
- George Washington University Institute for Crisis, Disaster, and Risk Management offers programs, including training, in the area of crisis, emergency and risk management: www.gwu.edu/~icdrm/
- North Carolina Links—North Carolina Office of Public Health Preparedness and Response (NC PHPR): www.epi.state.nc.us/epi/phpr/provides information and resources regarding the threat of bioterrorism and other emerging infectious diseases within the state and around the nation.
- The Health Alert Network (HAN) system is designed to immediately alert key health officials and care providers in North Carolina to acts of bioterrorism as well as other types of emerging disease threats: www.nchan.org/
- DPH Immunization branch: www.immunizenc.com/
- State Web sites, such as San Diego Country Office of Emergency Systems: www.co.sandiego.ca.us/oes/ or the County of San Diego Health and Human Services Terrorism Preparedness: www.co.san-diego.ca.us/terrorism/links.html
Back in the Saddle
When Tait Shanafelt, MD, and his colleagues at the Mayo Clinic in Rochester, Minn., investigated whether medical residents who rated high on burnout also delivered lower quality care, they found an interesting correlation: Physicians who reported errors experienced more burnout, and burned-out physicians made more errors.1
“While the patient safety issue is paramount, there is also a pretty substantial personal cost to physicians when they perceive that they have made an error,” says Dr. Shanafelt, an assistant professor of medicine.
Whether or not a bad outcome stems from “errors,” hospitalists may experience a psychoemotional aftermath. They often suffer in silence, imagining that few other doctors make errors. This common experience has historically been covered by a veil of silence.2
Silent Struggle
Caregivers are largely hesitant to discuss their involvement in adverse events.
“Their reluctance to discuss this with their colleagues is a common barrier to work through this in constructive ways,” Dr. Shanafelt says.
Though clinical decisions have systems and individual components, when mistakes happen it’s the latter with which hospitalists struggle silently—and often dysfunctionally.
“Every serious adverse event has at least two victims: the patient and family; and the caregiver,” says Albert W. Wu, MD, a professor of health policy and management at Johns Hopkins University in Baltimore.3-5
Although there is merit in analyzing the mistake and learning from it, doing so without facing the personal consequences is insufficient.
“Even if there was a system factor that can be identified, physicians still feel personally responsible for their patients and they often carry a sense of guilt around with them,” Dr. Shanafelt says.
That feeling of responsibility is not necessarily a bad thing.
“It is important to recognize that everything is not a systems error,” says Lenny Feldman, MD, an assistant professor and hospitalist with the Division of General Internal Medicine at Johns Hopkins Hospital. “Individuals want to be able to take responsibility for the bad things that have happened, and there is a value to that.”
The medical profession has just begun to fully acknowledge the inevitability of errors and the need for clinicians to be trained to manage them. Emotional responses to bad outcomes or medical errors include fear, guilt, anger, embarrassment, humiliation, and depression, which can last days—or years.
“The cognoscenti of coping know that there are adaptive and maladaptive ways of coping,” says Dr. Wu. “Adaptive would be reframing and growing and learning from the incident, channeling the energy into trying to do better next time. Maladaptive strategies include denial, turning to alcohol, and becoming angry.”
—Albert W. Wu, MD, professor of health policy and management, Johns Hopkins University, Baltimore
What Hospitalists Can Do
Healthcare is changing its culture so reporting adverse events is easier, without an emphasis on assigning blame.
Support is available by phone, disclosure protocols have been created, and practitioners work with risk management personnel to involve patients and families in discussions and apologies. These processes can give physicians a healthy way to be transparent about what happened and also to know that their institutions support them.
Mixed emotions are common after a bad choice or outcome, but the stakes are particularly high in hospital-based specialties.
“Physicians who practice in hospitals are at particular risk for being involved in instances where patients are harmed, partly because of the acuity of patients and partly because they are repeatedly in this environment,” Dr. Wu says. “In a way, for some physicians and nurses, it is like working in a war zone. It is necessary for you to return to that zone to work, even after something bad happens. That, in itself, can be traumatic.”
Experts accentuate the importance of providing hospitalists, especially young ones, the tools to help them recognize and manage post-event emotional baggage. These tools can serve as a roadmap on how to work through their experience.
Periodic debriefing with peers helps hospitalists discuss what’s going on in their practice. But if a hospitalist has not established this trust and support beforehand, it may be difficult to locate the right support after an event occurs.
“There is a healing that goes on when you are able to share with your colleagues who can tell you about their own experiences with this,” says Dr. Shanafelt.
Dr. Feldman agrees. After a couple of bad patient outcomes this year, he needed to talk as much as possible in a few forums, including with his hospitalist group leader and his peers. As the associate program director at his institution, he also checked in with his residents.
“I know how I’m feeling, which is horrible,” Dr. Feldman says. “You know if you’re doing it, your residents are probably doing the same thing.”
Teaching hospitalists can help change the culture by making them willing to share their own experiences with trainees.
“For supervising physicians to say, in effect, to medical students and residents, ‘In my own career, these are things I have experienced and how I’ve worked through them,’ can help young physicians recognize that identifying and working though the consequences of errors on both a professional and personal level is an important part of being a mindful physician,” says Dr. Shanafelt.
Open and humble sharing means trainees can act similarly.
“When we were first presenting our data to the residents in one of our early studies, I often felt like a priest with physicians coming me to confess their mistakes,” Dr. Shanafelt says. “After having this experience repeat itself over and over, I recognized that sharing this was a cathartic event for them.”
The most helpful thing hospitalists can do for each other is listen without judgment.
“We need to realize it is going to happen to each and every one of us, and be prepared to offer a shoulder to cry on to help your colleague work through it,” says Dr. Feldman.
Dr. Wu believes clinicians need to examine their capacity to offer such support.
“We are not as reassuring as we could be,” Dr. Wu says. “I think we tend to hold back, maybe because we are so fearful of the whole idea. Really admitting that this is a normal, common event frightens us too much.”
What Hospitalist Groups Can Do
Cleo Hardin, MD, section chief of pediatric hospital medicine at the University of Arizona in Tucson, says her department deals with post-event distress several ways. Her doctors talk with her, share in their departmental morbidity and mortality conference, and don’t ignore errors and bad outcomes.
“Anytime there is a bad outcome,” Dr. Hardin says, “it is very important for the leader of the group to meet with the individual to ask, ‘What do we need to do to reduce the likelihood that you’re going to develop post-traumatic stress disorder and that you’re going to question everything you do in the future? You are a good doctor. How do we keep you being a good doctor?’ ”
A show of support by the whole team is of utmost importance.
“There is a tremendous amount of camaraderie in the group, and we all understand [that clinical practice] is not an exact science,” Dr. Hardin says. “There’s a lot of art in medicine.”
An expression of that art showed up several years ago in her hospital’s pediatrics unit when a child died on Christmas Day.
“On the day an event happens, I think the person is reeling and in shock and can’t hear anything,” Dr. Hardin says. “I called the hospitalist to ask whether he needed coverage. He declined, saying he was afraid if he got off the horse, he would never get back on.”
The following month they discussed the event at their mortality and morbidity conference; the entire hospitalist section was there.
“We sat together, and it was very clear to the hospitalist involved in the event that he was not there alone,” Dr. Hardin says. “We told him how much we appreciated him and respected him, and we were there to be his support.”
What Leaders Can Do
As the director of the hospitalist program at Johns Hopkins Hospital, Daniel J. Brotman, MD, FACP, understands that the level of upset after a bad outcome can be dramatic.
“Whether or not it was your fault, and independent of any medical-legal ramifications, although those certainly exist,” he says, “there’s a personal sense of just being a human being; of wanting to go back; questioning whether you made a right decision, a wrong decision; and facing whether you would change anything if you could do it again.”
Dr. Brotman believes in leading by example. “What you want is an open-door policy where faculty members can say, ‘Something bad happened, I need to get it off my chest, and I need to do it now,’” he says.
The group leader also needs to know what happened in case there’s a need for damage control beyond the hospitalist group. The leader should ultimately be the one who confers forgiveness.
“If somebody feels they are keeping a secret, it’s going to make matters worse,” Dr. Brotman says.
Research confirms the needs for “confession, restitution, and absolution,” and hospitalists need their competence validated.6
Even though I [have been] honest and said, ‘I don’t think I would have made that decision,’ I also have said, ‘I know that in terms of your thought process, you were acting in the best interest of the patient … and you’re one of the most compassionate physicians I know,” Dr. Brotman says.
As leaders gather information on an adverse event, they may also be in a better position to advocate for the hospitalist in subsequent conversations. In so doing, they can save that individual further embarrassment and humiliation.
“I hope that I’m able to process what I was experiencing in a way that doesn’t paralyze me,” Dr. Feldman says. “But I hope it informs me to the gravity of the situation.” TH
Andrea Sattinger is a medical writer based in North Carolina.
References
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071-1078.
- Goldberg RM, Kuhn G, Andrew LB, et al. Coping with medical mistakes and errors in judgment. Ann Emerg Med. 2002;39(3):287-292.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999;131(12):970-972.
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727.
- Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mistakes? JAMA. 1991;265(16):2089-2094.
- Wears RL, Wu AW. Dealing with failure: the aftermath of errors and adverse events. Ann Emerg Med. 2002;39(3):344-346.
When Tait Shanafelt, MD, and his colleagues at the Mayo Clinic in Rochester, Minn., investigated whether medical residents who rated high on burnout also delivered lower quality care, they found an interesting correlation: Physicians who reported errors experienced more burnout, and burned-out physicians made more errors.1
“While the patient safety issue is paramount, there is also a pretty substantial personal cost to physicians when they perceive that they have made an error,” says Dr. Shanafelt, an assistant professor of medicine.
Whether or not a bad outcome stems from “errors,” hospitalists may experience a psychoemotional aftermath. They often suffer in silence, imagining that few other doctors make errors. This common experience has historically been covered by a veil of silence.2
Silent Struggle
Caregivers are largely hesitant to discuss their involvement in adverse events.
“Their reluctance to discuss this with their colleagues is a common barrier to work through this in constructive ways,” Dr. Shanafelt says.
Though clinical decisions have systems and individual components, when mistakes happen it’s the latter with which hospitalists struggle silently—and often dysfunctionally.
“Every serious adverse event has at least two victims: the patient and family; and the caregiver,” says Albert W. Wu, MD, a professor of health policy and management at Johns Hopkins University in Baltimore.3-5
Although there is merit in analyzing the mistake and learning from it, doing so without facing the personal consequences is insufficient.
“Even if there was a system factor that can be identified, physicians still feel personally responsible for their patients and they often carry a sense of guilt around with them,” Dr. Shanafelt says.
That feeling of responsibility is not necessarily a bad thing.
“It is important to recognize that everything is not a systems error,” says Lenny Feldman, MD, an assistant professor and hospitalist with the Division of General Internal Medicine at Johns Hopkins Hospital. “Individuals want to be able to take responsibility for the bad things that have happened, and there is a value to that.”
The medical profession has just begun to fully acknowledge the inevitability of errors and the need for clinicians to be trained to manage them. Emotional responses to bad outcomes or medical errors include fear, guilt, anger, embarrassment, humiliation, and depression, which can last days—or years.
“The cognoscenti of coping know that there are adaptive and maladaptive ways of coping,” says Dr. Wu. “Adaptive would be reframing and growing and learning from the incident, channeling the energy into trying to do better next time. Maladaptive strategies include denial, turning to alcohol, and becoming angry.”
—Albert W. Wu, MD, professor of health policy and management, Johns Hopkins University, Baltimore
What Hospitalists Can Do
Healthcare is changing its culture so reporting adverse events is easier, without an emphasis on assigning blame.
Support is available by phone, disclosure protocols have been created, and practitioners work with risk management personnel to involve patients and families in discussions and apologies. These processes can give physicians a healthy way to be transparent about what happened and also to know that their institutions support them.
Mixed emotions are common after a bad choice or outcome, but the stakes are particularly high in hospital-based specialties.
“Physicians who practice in hospitals are at particular risk for being involved in instances where patients are harmed, partly because of the acuity of patients and partly because they are repeatedly in this environment,” Dr. Wu says. “In a way, for some physicians and nurses, it is like working in a war zone. It is necessary for you to return to that zone to work, even after something bad happens. That, in itself, can be traumatic.”
Experts accentuate the importance of providing hospitalists, especially young ones, the tools to help them recognize and manage post-event emotional baggage. These tools can serve as a roadmap on how to work through their experience.
Periodic debriefing with peers helps hospitalists discuss what’s going on in their practice. But if a hospitalist has not established this trust and support beforehand, it may be difficult to locate the right support after an event occurs.
“There is a healing that goes on when you are able to share with your colleagues who can tell you about their own experiences with this,” says Dr. Shanafelt.
Dr. Feldman agrees. After a couple of bad patient outcomes this year, he needed to talk as much as possible in a few forums, including with his hospitalist group leader and his peers. As the associate program director at his institution, he also checked in with his residents.
“I know how I’m feeling, which is horrible,” Dr. Feldman says. “You know if you’re doing it, your residents are probably doing the same thing.”
Teaching hospitalists can help change the culture by making them willing to share their own experiences with trainees.
“For supervising physicians to say, in effect, to medical students and residents, ‘In my own career, these are things I have experienced and how I’ve worked through them,’ can help young physicians recognize that identifying and working though the consequences of errors on both a professional and personal level is an important part of being a mindful physician,” says Dr. Shanafelt.
Open and humble sharing means trainees can act similarly.
“When we were first presenting our data to the residents in one of our early studies, I often felt like a priest with physicians coming me to confess their mistakes,” Dr. Shanafelt says. “After having this experience repeat itself over and over, I recognized that sharing this was a cathartic event for them.”
The most helpful thing hospitalists can do for each other is listen without judgment.
“We need to realize it is going to happen to each and every one of us, and be prepared to offer a shoulder to cry on to help your colleague work through it,” says Dr. Feldman.
Dr. Wu believes clinicians need to examine their capacity to offer such support.
“We are not as reassuring as we could be,” Dr. Wu says. “I think we tend to hold back, maybe because we are so fearful of the whole idea. Really admitting that this is a normal, common event frightens us too much.”
What Hospitalist Groups Can Do
Cleo Hardin, MD, section chief of pediatric hospital medicine at the University of Arizona in Tucson, says her department deals with post-event distress several ways. Her doctors talk with her, share in their departmental morbidity and mortality conference, and don’t ignore errors and bad outcomes.
“Anytime there is a bad outcome,” Dr. Hardin says, “it is very important for the leader of the group to meet with the individual to ask, ‘What do we need to do to reduce the likelihood that you’re going to develop post-traumatic stress disorder and that you’re going to question everything you do in the future? You are a good doctor. How do we keep you being a good doctor?’ ”
A show of support by the whole team is of utmost importance.
“There is a tremendous amount of camaraderie in the group, and we all understand [that clinical practice] is not an exact science,” Dr. Hardin says. “There’s a lot of art in medicine.”
An expression of that art showed up several years ago in her hospital’s pediatrics unit when a child died on Christmas Day.
“On the day an event happens, I think the person is reeling and in shock and can’t hear anything,” Dr. Hardin says. “I called the hospitalist to ask whether he needed coverage. He declined, saying he was afraid if he got off the horse, he would never get back on.”
The following month they discussed the event at their mortality and morbidity conference; the entire hospitalist section was there.
“We sat together, and it was very clear to the hospitalist involved in the event that he was not there alone,” Dr. Hardin says. “We told him how much we appreciated him and respected him, and we were there to be his support.”
What Leaders Can Do
As the director of the hospitalist program at Johns Hopkins Hospital, Daniel J. Brotman, MD, FACP, understands that the level of upset after a bad outcome can be dramatic.
“Whether or not it was your fault, and independent of any medical-legal ramifications, although those certainly exist,” he says, “there’s a personal sense of just being a human being; of wanting to go back; questioning whether you made a right decision, a wrong decision; and facing whether you would change anything if you could do it again.”
Dr. Brotman believes in leading by example. “What you want is an open-door policy where faculty members can say, ‘Something bad happened, I need to get it off my chest, and I need to do it now,’” he says.
The group leader also needs to know what happened in case there’s a need for damage control beyond the hospitalist group. The leader should ultimately be the one who confers forgiveness.
“If somebody feels they are keeping a secret, it’s going to make matters worse,” Dr. Brotman says.
Research confirms the needs for “confession, restitution, and absolution,” and hospitalists need their competence validated.6
Even though I [have been] honest and said, ‘I don’t think I would have made that decision,’ I also have said, ‘I know that in terms of your thought process, you were acting in the best interest of the patient … and you’re one of the most compassionate physicians I know,” Dr. Brotman says.
As leaders gather information on an adverse event, they may also be in a better position to advocate for the hospitalist in subsequent conversations. In so doing, they can save that individual further embarrassment and humiliation.
“I hope that I’m able to process what I was experiencing in a way that doesn’t paralyze me,” Dr. Feldman says. “But I hope it informs me to the gravity of the situation.” TH
Andrea Sattinger is a medical writer based in North Carolina.
References
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071-1078.
- Goldberg RM, Kuhn G, Andrew LB, et al. Coping with medical mistakes and errors in judgment. Ann Emerg Med. 2002;39(3):287-292.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999;131(12):970-972.
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727.
- Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mistakes? JAMA. 1991;265(16):2089-2094.
- Wears RL, Wu AW. Dealing with failure: the aftermath of errors and adverse events. Ann Emerg Med. 2002;39(3):344-346.
When Tait Shanafelt, MD, and his colleagues at the Mayo Clinic in Rochester, Minn., investigated whether medical residents who rated high on burnout also delivered lower quality care, they found an interesting correlation: Physicians who reported errors experienced more burnout, and burned-out physicians made more errors.1
“While the patient safety issue is paramount, there is also a pretty substantial personal cost to physicians when they perceive that they have made an error,” says Dr. Shanafelt, an assistant professor of medicine.
Whether or not a bad outcome stems from “errors,” hospitalists may experience a psychoemotional aftermath. They often suffer in silence, imagining that few other doctors make errors. This common experience has historically been covered by a veil of silence.2
Silent Struggle
Caregivers are largely hesitant to discuss their involvement in adverse events.
“Their reluctance to discuss this with their colleagues is a common barrier to work through this in constructive ways,” Dr. Shanafelt says.
Though clinical decisions have systems and individual components, when mistakes happen it’s the latter with which hospitalists struggle silently—and often dysfunctionally.
“Every serious adverse event has at least two victims: the patient and family; and the caregiver,” says Albert W. Wu, MD, a professor of health policy and management at Johns Hopkins University in Baltimore.3-5
Although there is merit in analyzing the mistake and learning from it, doing so without facing the personal consequences is insufficient.
“Even if there was a system factor that can be identified, physicians still feel personally responsible for their patients and they often carry a sense of guilt around with them,” Dr. Shanafelt says.
That feeling of responsibility is not necessarily a bad thing.
“It is important to recognize that everything is not a systems error,” says Lenny Feldman, MD, an assistant professor and hospitalist with the Division of General Internal Medicine at Johns Hopkins Hospital. “Individuals want to be able to take responsibility for the bad things that have happened, and there is a value to that.”
The medical profession has just begun to fully acknowledge the inevitability of errors and the need for clinicians to be trained to manage them. Emotional responses to bad outcomes or medical errors include fear, guilt, anger, embarrassment, humiliation, and depression, which can last days—or years.
“The cognoscenti of coping know that there are adaptive and maladaptive ways of coping,” says Dr. Wu. “Adaptive would be reframing and growing and learning from the incident, channeling the energy into trying to do better next time. Maladaptive strategies include denial, turning to alcohol, and becoming angry.”
—Albert W. Wu, MD, professor of health policy and management, Johns Hopkins University, Baltimore
What Hospitalists Can Do
Healthcare is changing its culture so reporting adverse events is easier, without an emphasis on assigning blame.
Support is available by phone, disclosure protocols have been created, and practitioners work with risk management personnel to involve patients and families in discussions and apologies. These processes can give physicians a healthy way to be transparent about what happened and also to know that their institutions support them.
Mixed emotions are common after a bad choice or outcome, but the stakes are particularly high in hospital-based specialties.
“Physicians who practice in hospitals are at particular risk for being involved in instances where patients are harmed, partly because of the acuity of patients and partly because they are repeatedly in this environment,” Dr. Wu says. “In a way, for some physicians and nurses, it is like working in a war zone. It is necessary for you to return to that zone to work, even after something bad happens. That, in itself, can be traumatic.”
Experts accentuate the importance of providing hospitalists, especially young ones, the tools to help them recognize and manage post-event emotional baggage. These tools can serve as a roadmap on how to work through their experience.
Periodic debriefing with peers helps hospitalists discuss what’s going on in their practice. But if a hospitalist has not established this trust and support beforehand, it may be difficult to locate the right support after an event occurs.
“There is a healing that goes on when you are able to share with your colleagues who can tell you about their own experiences with this,” says Dr. Shanafelt.
Dr. Feldman agrees. After a couple of bad patient outcomes this year, he needed to talk as much as possible in a few forums, including with his hospitalist group leader and his peers. As the associate program director at his institution, he also checked in with his residents.
“I know how I’m feeling, which is horrible,” Dr. Feldman says. “You know if you’re doing it, your residents are probably doing the same thing.”
Teaching hospitalists can help change the culture by making them willing to share their own experiences with trainees.
“For supervising physicians to say, in effect, to medical students and residents, ‘In my own career, these are things I have experienced and how I’ve worked through them,’ can help young physicians recognize that identifying and working though the consequences of errors on both a professional and personal level is an important part of being a mindful physician,” says Dr. Shanafelt.
Open and humble sharing means trainees can act similarly.
“When we were first presenting our data to the residents in one of our early studies, I often felt like a priest with physicians coming me to confess their mistakes,” Dr. Shanafelt says. “After having this experience repeat itself over and over, I recognized that sharing this was a cathartic event for them.”
The most helpful thing hospitalists can do for each other is listen without judgment.
“We need to realize it is going to happen to each and every one of us, and be prepared to offer a shoulder to cry on to help your colleague work through it,” says Dr. Feldman.
Dr. Wu believes clinicians need to examine their capacity to offer such support.
“We are not as reassuring as we could be,” Dr. Wu says. “I think we tend to hold back, maybe because we are so fearful of the whole idea. Really admitting that this is a normal, common event frightens us too much.”
What Hospitalist Groups Can Do
Cleo Hardin, MD, section chief of pediatric hospital medicine at the University of Arizona in Tucson, says her department deals with post-event distress several ways. Her doctors talk with her, share in their departmental morbidity and mortality conference, and don’t ignore errors and bad outcomes.
“Anytime there is a bad outcome,” Dr. Hardin says, “it is very important for the leader of the group to meet with the individual to ask, ‘What do we need to do to reduce the likelihood that you’re going to develop post-traumatic stress disorder and that you’re going to question everything you do in the future? You are a good doctor. How do we keep you being a good doctor?’ ”
A show of support by the whole team is of utmost importance.
“There is a tremendous amount of camaraderie in the group, and we all understand [that clinical practice] is not an exact science,” Dr. Hardin says. “There’s a lot of art in medicine.”
An expression of that art showed up several years ago in her hospital’s pediatrics unit when a child died on Christmas Day.
“On the day an event happens, I think the person is reeling and in shock and can’t hear anything,” Dr. Hardin says. “I called the hospitalist to ask whether he needed coverage. He declined, saying he was afraid if he got off the horse, he would never get back on.”
The following month they discussed the event at their mortality and morbidity conference; the entire hospitalist section was there.
“We sat together, and it was very clear to the hospitalist involved in the event that he was not there alone,” Dr. Hardin says. “We told him how much we appreciated him and respected him, and we were there to be his support.”
What Leaders Can Do
As the director of the hospitalist program at Johns Hopkins Hospital, Daniel J. Brotman, MD, FACP, understands that the level of upset after a bad outcome can be dramatic.
“Whether or not it was your fault, and independent of any medical-legal ramifications, although those certainly exist,” he says, “there’s a personal sense of just being a human being; of wanting to go back; questioning whether you made a right decision, a wrong decision; and facing whether you would change anything if you could do it again.”
Dr. Brotman believes in leading by example. “What you want is an open-door policy where faculty members can say, ‘Something bad happened, I need to get it off my chest, and I need to do it now,’” he says.
The group leader also needs to know what happened in case there’s a need for damage control beyond the hospitalist group. The leader should ultimately be the one who confers forgiveness.
“If somebody feels they are keeping a secret, it’s going to make matters worse,” Dr. Brotman says.
Research confirms the needs for “confession, restitution, and absolution,” and hospitalists need their competence validated.6
Even though I [have been] honest and said, ‘I don’t think I would have made that decision,’ I also have said, ‘I know that in terms of your thought process, you were acting in the best interest of the patient … and you’re one of the most compassionate physicians I know,” Dr. Brotman says.
As leaders gather information on an adverse event, they may also be in a better position to advocate for the hospitalist in subsequent conversations. In so doing, they can save that individual further embarrassment and humiliation.
“I hope that I’m able to process what I was experiencing in a way that doesn’t paralyze me,” Dr. Feldman says. “But I hope it informs me to the gravity of the situation.” TH
Andrea Sattinger is a medical writer based in North Carolina.
References
- West CP, Huschka MM, Novotny PJ, et al. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071-1078.
- Goldberg RM, Kuhn G, Andrew LB, et al. Coping with medical mistakes and errors in judgment. Ann Emerg Med. 2002;39(3):287-292.
- Wu AW. Handling hospital errors: is disclosure the best defense? Ann Intern Med. 1999;131(12):970-972.
- Wu AW. Medical error: the second victim. BMJ. 2000;320(7237):726-727.
- Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mistakes? JAMA. 1991;265(16):2089-2094.
- Wears RL, Wu AW. Dealing with failure: the aftermath of errors and adverse events. Ann Emerg Med. 2002;39(3):344-346.
Perilous Intersection
When Amsterdam Airport Schiphol in the Netherlands revamped its men’s restrooms, the architects installed small, Euro-style urinals: a surefire way to throw urine off target. To solve this problem, the black outline of a fly was etched in the porcelain near each urinal’s drain. Users’ aim improved and spillage was reduced by 80%. “They try to power blast it away,” says Sanjay Saint, MD, hospitalist and professor of internal medicine at the Ann Arbor VA Medical Center, University of Michigan. “By the time they might realize that the fly isn’t going anywhere, the men are done and walking away.”
It’s a guy thing, sure. It also is an example of a human factors intervention. “Science teaches us that implementing a design for a machine or device that elicits an instinctive reaction from someone using it is a clear-cut way to avoid error,” Dr. Saint explains.
What It Is and Why It’s Important
Human factors (HF), or human factors engineering (HFE), also sometimes called usability engineering or systems-based practice, refers to the study of human abilities and characteristics as they affect the design and smooth operation of equipment, systems, and jobs.1 HF is the basic science underlying much of patient safety practice. For instance, the current recommendation that hospitals standardize equipment, such as ventilators, programmable IV pumps, and defibrillators, is an example of making tasks human friendly. The use of cognitive psychology and biomechanics to develop and improve software and hand tools are another example of HF principles.
In general, HF examines the component tasks of an activity in terms of three factorial domains: physical and environmental factors, cognitive factors (skill demands and mental workload), and organizational factors. Each task is assessed in terms of necessary interactions of the individual and work environment, the device/system design, and associated team dynamics.
HF use in healthcare is not new; for roughly four decades HF researchers have emphasized the key role of HF in safe medical design, healthcare facility operations, and patient safety processes. HF helps organizations deepen analyses of adverse events and develop effective solutions.2 HF is used in the design of labeling, warnings or alarms, software programs, information displays, paper forms, process and activity flow, workplace design, cognitive aids, decision support systems, and policies and protocols.
For hospitalists, human factors knowledge is most useful in process improvement, says John Gosbee, MD, MS, a human factors engineering and healthcare specialist at the University of Michigan. Dr. Gosbee, who has worked with hospitalists in Ann Arbor and around the country, originally studied aerospace medicine, pursued a subspecialty in occupational medicine, and from 1988 to 1992 worked at NASA designing space hospitals. In the dozens of lectures and workshops he has conducted, he has learned numerous physicians resist learning about HF. At first they protest, claiming they “didn’t go to medical school to become engineers” or “weren’t hired to have you tell us we need to be some kind of designer or computer-science software evaluator.”
Dr. Gosbee couldn’t agree more, but after the a-ha! moment, usually in an interactive experience when the hospitalist sees a poor system design is an obstacle to safety and process flow, they open up to adopting the HF mindset. Once on board with HF, hospitalists are quick to translate the theories to their own practices, identifying potential vulnerabilities and risks.
Manufacturers of healthcare equipment and systems don’t want to hear from “safety geeks,” Dr. Gosbee says; the companies want to hear from front-line providers who regularly use the products. “Hospitalists are in great position to provide that input because they see what happens across a broad swath of hospital settings,” he says, “and they could amalgamate the fact that everyone across specialties is having some trouble with this computer screen or new infusion device.”
Dr. Gosbee’s first-hand knowledge and experience solving hospitalist issues with HF techniques evolved into a teaching career. He says the university administration supports his belief in the practicality of HF lessons, and he now works as the lead instructor for a majority of the university’s medical residents.
“Human factors engineering is an efficient way to flip people’s brains around 180 degrees toward systems thinking,” Dr. Gosbee explains, “which is required if the organization wants to become a high-reliability organization.”3
Examples in Medicine
Russ Cucina, MD, MS, hospitalist at the University of California San Francisco Medical Center, describes a practical example of human factors engineering in a simple, widely used design. When cars ran on leaded gasoline, the design of the leaded gas pump nozzle precluded it from being inserted into an unleaded gas tank. “Even though one was clearly labeled leaded and other unleaded, human beings are bad at catching those things, especially when they’re in a hurry and under stress,” says Dr. Cucina, whose research includes clinical human-computer interaction science with an emphasis on human factors and patient safety.
A similar concept is what is missing from the Swan Ganz catheter design. The three ports (proximal, middle, and distal) connecting the catheter to the ICU monitor all have the same shape, making it easy to errantly connect one or more to the wrong port. “You’d think the manufacturers would shape the connectors in a way that would preclude incorrect connections,” Dr. Cucina says, “but that has not been done. We leave it to the vigilance of the bedside nurse or intensivist or hospitalist to hook these up correctly, rather than redesigning them so that cannot be done incorrectly.”
One way to think about human factors engineering is to think about forcing “a round peg into a square hole.” In the hospital setting, round pegs into square holes equate to errors. HF tries to solve the issue (round peg into a round hole, and vice versa). “Were you to apply human factors to the Swan Ganz catheter port connectors,” Dr. Cucina says, “you’d have round into the round hole, square into the square, and triangular into the triangular. You’d have no choice but to do the right thing.”
Efforts to implement systems that anticipate and minimize the chances of human error, such as computer physician order entry and patient bar coding, are attempts to overcome by design those instances where it is possible to place round pegs into square holes.
HF Projects in Motion
A number of hospitalists around the country have or are using HF as part of projects and studies to reduce human errors.
Culture change: In the early 2000s, Janet Nagamine, MD, a hospitalist with Kaiser Permanente in Santa Clara, Calif., and her colleagues took human factors concepts to front-line ICU staff. The human factors training provided a framework to reinforce three basic concepts: all humans make errors; processes can be designed to reduce the possibility of error; and processes can be designed so errors are detected and corrected before causing injury.4 “My colleagues and I knew that the punitive, ‘shame-and-blame’ culture around mistakes and errors were preventing us from identifying problems and moving forward with solutions,” Dr. Nagamine says.
A former ICU nurse and current chair of SHM’s Hospital Quality and Patient Safety (HQPS) Committee, Dr. Nagamine first became involved in HF when she realized how many patients suffered adverse events stemming from poorly designed medical systems. “Some of my most respected mentors were involved in these kinds of cases, and I knew eventually that would be me,” she says. It was a disturbing reality. During her medical training it was drilled into her head smart, diligent doctors would be successful. “But bad things happen in medicine; it’s part of what we do,” she says. “Rather than deny that things will inevitably go wrong, I wanted to study safety science and reliable system design.” She asked herself, how can we prevent the same mistakes from happening to competent people who practice in poorly designed systems? “The patterns are there,” she says. “You can train your eyes to look for vulnerabilities and patterns, then find the solutions.”
After she started looking at adverse events as system failures, rather than solely personal failures, she engaged the staff to redesign systems. She introduced HF concepts and provided an infrastructure to make it safe to report and discuss problems. The project included a new medication error reporting system and the creation of departmental patient safety teams. A palpable culture change developed when front-line staff and managers became empowered to find solutions working side-by-side with the quality and risk management departments.
The result? A dramatic increase in medication errors and near-miss reports: from eight faulty problems per quarter in 2000 to 200 reports per quarter by 2001.
To sum up the essence of Dr. Nagamine’s project, she invokes her favorite quotation from systems expert James Reason: “We can’t change the human condition, but we can change the conditions under which humans work.”1,5
Bar coding workarounds: Hospitalist Tosha Wetterneck, MD, and her colleagues at the University of Wisconsin School of Medicine and Dentistry focused their HF-trained eyes on medication errors.5 The team applied HF concepts as part of a study of bar-coded medication administration systems (BCMAs). Ideally, BCMAs help confirm the five rights of medication administration: the right patient, drug, dose, route, and time. The study authors identified the hospitalist staff had developed 46 workarounds in place of proper use of the BCMA. With each workaround, the researchers identified six potential errors. Furthermore, nurses were overriding the BCMA alerts for 4.2% of patients charted, and for 10.3% of total medication.
By creating an exhaustive template, the study authors broke down the use of BCMA workarounds to the finest detail of task component. They learned many workarounds were engendered by difficulties with the technology and by interactions between BCMA technologies and environmental, technical, process, workload, training, and policy concerns. Data shows BCMAs still have an important role in preventing error; during one year, almost 24,000 BCMA alerts led users to change their action, instead of overriding an alert. “These causes (and related workarounds) are neither rare nor secret,” the authors write. “They are hiding in plain sight.”1,5
Dr. Wetterneck is part of the Systems Engineering Initiative for Patient Safety (SEIPS), an interdisciplinary research group located within the Center for Quality and Productivity Improvement in the College of Engineering at the University of Wisconsin-Madison.6,7 SEIPS uses HF principles to study the safety and quality of healthcare systems.
Congestive heart failure order sets: Researchers in another study incorporated HF science in their review of clinical practice guideline use and application for congestive heart failure (CHF). Reingold and Kulstad studied the impact of HF design elements on order set utilization and recommendations compliance.8
Using retrospective medical record review of adult patients admitted from the emergency department with CHF, the study measured acuity and clinical practice guideline (CPG) parameters before and after introducing new orders. In 87 adult patients before and 84 patients after beginning the new order set, attention to HF design elements significantly improved utilization of the orders and CPG compliance.
Infusion device programming: In another instance, a multidisciplinary research team applied HF design principles to common nursing procedures: programming an insulin infusion and programming a heparin infusion.9,10 An HF usability checklist was developed, and it revealed systematic error-provoking conditions in both tasks.
The good news is the pitfalls were remedied easily.
Not only did researchers subsequently commit to modify training procedures and redesign preprinted orders, they took the bigger step of providing feedback to the manufacturer and committing to incorporate usability testing in future procurement of medical devices. TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
References
1. Gosbee JW. Conclusion: you need human factors engineering expertise to see design hazards that are hiding in “plain sight!” Jt Comm J Qual Saf. 2004;30(12):696-700.
2. Gosbee J. Introduction to the human factors engineering series. Jt Comm J Qual Saf. 2004;30(4): 215-219.
3. Reason J. Human error: models and management. BMJ. 2000; 320(7237):768-770.
4. Etchells E, Juurlink D, Levinson W. Medication errors: the human factor. CMAJ. 2008;178(1):63-64.
5. Koppel R, Wetterneck T, Telles JL, Karsh BT. Workarounds to barcode medication administration systems: their occurrences, causes, and threats to patient safety. J Am Med Inform Assoc. 2008;15(4):408-423.
6. SEIPS model. http://cqpi.engr.wisc.edu/seips_ home/. Accessed Dec. 20, 2008.
7. Carayon P, Schoofs Hundt A, Karsh BT, et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15 Suppl 1:850-858.
8. Reingold S, Kulstad E. Impact of human factor design on the use of order sets in the treatment of congestive heart failure. Acad Emerg Med. 2007;14(11):1097-1105.
9. Etchells E, Bailey C, Biason R, et al. Human factors in action: getting “pumped” at a nursing usability laboratory. Healthc Q. 2006;9 Spec No:69-74.
10. Carayon P, Wetterneck T, Schoofs Hundt A, et al. Observing nurse interaction with infusion pump technologies. In: Henriksen K, Battles J, Lewin D, eds. Advances in Patient Safety: From Research to Implementation. Rockville, Md.: Agency for Healthcare Research and Quality; Feb. 2005, AHRQ Publication No. 05-0021-2.
When Amsterdam Airport Schiphol in the Netherlands revamped its men’s restrooms, the architects installed small, Euro-style urinals: a surefire way to throw urine off target. To solve this problem, the black outline of a fly was etched in the porcelain near each urinal’s drain. Users’ aim improved and spillage was reduced by 80%. “They try to power blast it away,” says Sanjay Saint, MD, hospitalist and professor of internal medicine at the Ann Arbor VA Medical Center, University of Michigan. “By the time they might realize that the fly isn’t going anywhere, the men are done and walking away.”
It’s a guy thing, sure. It also is an example of a human factors intervention. “Science teaches us that implementing a design for a machine or device that elicits an instinctive reaction from someone using it is a clear-cut way to avoid error,” Dr. Saint explains.
What It Is and Why It’s Important
Human factors (HF), or human factors engineering (HFE), also sometimes called usability engineering or systems-based practice, refers to the study of human abilities and characteristics as they affect the design and smooth operation of equipment, systems, and jobs.1 HF is the basic science underlying much of patient safety practice. For instance, the current recommendation that hospitals standardize equipment, such as ventilators, programmable IV pumps, and defibrillators, is an example of making tasks human friendly. The use of cognitive psychology and biomechanics to develop and improve software and hand tools are another example of HF principles.
In general, HF examines the component tasks of an activity in terms of three factorial domains: physical and environmental factors, cognitive factors (skill demands and mental workload), and organizational factors. Each task is assessed in terms of necessary interactions of the individual and work environment, the device/system design, and associated team dynamics.
HF use in healthcare is not new; for roughly four decades HF researchers have emphasized the key role of HF in safe medical design, healthcare facility operations, and patient safety processes. HF helps organizations deepen analyses of adverse events and develop effective solutions.2 HF is used in the design of labeling, warnings or alarms, software programs, information displays, paper forms, process and activity flow, workplace design, cognitive aids, decision support systems, and policies and protocols.
For hospitalists, human factors knowledge is most useful in process improvement, says John Gosbee, MD, MS, a human factors engineering and healthcare specialist at the University of Michigan. Dr. Gosbee, who has worked with hospitalists in Ann Arbor and around the country, originally studied aerospace medicine, pursued a subspecialty in occupational medicine, and from 1988 to 1992 worked at NASA designing space hospitals. In the dozens of lectures and workshops he has conducted, he has learned numerous physicians resist learning about HF. At first they protest, claiming they “didn’t go to medical school to become engineers” or “weren’t hired to have you tell us we need to be some kind of designer or computer-science software evaluator.”
Dr. Gosbee couldn’t agree more, but after the a-ha! moment, usually in an interactive experience when the hospitalist sees a poor system design is an obstacle to safety and process flow, they open up to adopting the HF mindset. Once on board with HF, hospitalists are quick to translate the theories to their own practices, identifying potential vulnerabilities and risks.
Manufacturers of healthcare equipment and systems don’t want to hear from “safety geeks,” Dr. Gosbee says; the companies want to hear from front-line providers who regularly use the products. “Hospitalists are in great position to provide that input because they see what happens across a broad swath of hospital settings,” he says, “and they could amalgamate the fact that everyone across specialties is having some trouble with this computer screen or new infusion device.”
Dr. Gosbee’s first-hand knowledge and experience solving hospitalist issues with HF techniques evolved into a teaching career. He says the university administration supports his belief in the practicality of HF lessons, and he now works as the lead instructor for a majority of the university’s medical residents.
“Human factors engineering is an efficient way to flip people’s brains around 180 degrees toward systems thinking,” Dr. Gosbee explains, “which is required if the organization wants to become a high-reliability organization.”3
Examples in Medicine
Russ Cucina, MD, MS, hospitalist at the University of California San Francisco Medical Center, describes a practical example of human factors engineering in a simple, widely used design. When cars ran on leaded gasoline, the design of the leaded gas pump nozzle precluded it from being inserted into an unleaded gas tank. “Even though one was clearly labeled leaded and other unleaded, human beings are bad at catching those things, especially when they’re in a hurry and under stress,” says Dr. Cucina, whose research includes clinical human-computer interaction science with an emphasis on human factors and patient safety.
A similar concept is what is missing from the Swan Ganz catheter design. The three ports (proximal, middle, and distal) connecting the catheter to the ICU monitor all have the same shape, making it easy to errantly connect one or more to the wrong port. “You’d think the manufacturers would shape the connectors in a way that would preclude incorrect connections,” Dr. Cucina says, “but that has not been done. We leave it to the vigilance of the bedside nurse or intensivist or hospitalist to hook these up correctly, rather than redesigning them so that cannot be done incorrectly.”
One way to think about human factors engineering is to think about forcing “a round peg into a square hole.” In the hospital setting, round pegs into square holes equate to errors. HF tries to solve the issue (round peg into a round hole, and vice versa). “Were you to apply human factors to the Swan Ganz catheter port connectors,” Dr. Cucina says, “you’d have round into the round hole, square into the square, and triangular into the triangular. You’d have no choice but to do the right thing.”
Efforts to implement systems that anticipate and minimize the chances of human error, such as computer physician order entry and patient bar coding, are attempts to overcome by design those instances where it is possible to place round pegs into square holes.
HF Projects in Motion
A number of hospitalists around the country have or are using HF as part of projects and studies to reduce human errors.
Culture change: In the early 2000s, Janet Nagamine, MD, a hospitalist with Kaiser Permanente in Santa Clara, Calif., and her colleagues took human factors concepts to front-line ICU staff. The human factors training provided a framework to reinforce three basic concepts: all humans make errors; processes can be designed to reduce the possibility of error; and processes can be designed so errors are detected and corrected before causing injury.4 “My colleagues and I knew that the punitive, ‘shame-and-blame’ culture around mistakes and errors were preventing us from identifying problems and moving forward with solutions,” Dr. Nagamine says.
A former ICU nurse and current chair of SHM’s Hospital Quality and Patient Safety (HQPS) Committee, Dr. Nagamine first became involved in HF when she realized how many patients suffered adverse events stemming from poorly designed medical systems. “Some of my most respected mentors were involved in these kinds of cases, and I knew eventually that would be me,” she says. It was a disturbing reality. During her medical training it was drilled into her head smart, diligent doctors would be successful. “But bad things happen in medicine; it’s part of what we do,” she says. “Rather than deny that things will inevitably go wrong, I wanted to study safety science and reliable system design.” She asked herself, how can we prevent the same mistakes from happening to competent people who practice in poorly designed systems? “The patterns are there,” she says. “You can train your eyes to look for vulnerabilities and patterns, then find the solutions.”
After she started looking at adverse events as system failures, rather than solely personal failures, she engaged the staff to redesign systems. She introduced HF concepts and provided an infrastructure to make it safe to report and discuss problems. The project included a new medication error reporting system and the creation of departmental patient safety teams. A palpable culture change developed when front-line staff and managers became empowered to find solutions working side-by-side with the quality and risk management departments.
The result? A dramatic increase in medication errors and near-miss reports: from eight faulty problems per quarter in 2000 to 200 reports per quarter by 2001.
To sum up the essence of Dr. Nagamine’s project, she invokes her favorite quotation from systems expert James Reason: “We can’t change the human condition, but we can change the conditions under which humans work.”1,5
Bar coding workarounds: Hospitalist Tosha Wetterneck, MD, and her colleagues at the University of Wisconsin School of Medicine and Dentistry focused their HF-trained eyes on medication errors.5 The team applied HF concepts as part of a study of bar-coded medication administration systems (BCMAs). Ideally, BCMAs help confirm the five rights of medication administration: the right patient, drug, dose, route, and time. The study authors identified the hospitalist staff had developed 46 workarounds in place of proper use of the BCMA. With each workaround, the researchers identified six potential errors. Furthermore, nurses were overriding the BCMA alerts for 4.2% of patients charted, and for 10.3% of total medication.
By creating an exhaustive template, the study authors broke down the use of BCMA workarounds to the finest detail of task component. They learned many workarounds were engendered by difficulties with the technology and by interactions between BCMA technologies and environmental, technical, process, workload, training, and policy concerns. Data shows BCMAs still have an important role in preventing error; during one year, almost 24,000 BCMA alerts led users to change their action, instead of overriding an alert. “These causes (and related workarounds) are neither rare nor secret,” the authors write. “They are hiding in plain sight.”1,5
Dr. Wetterneck is part of the Systems Engineering Initiative for Patient Safety (SEIPS), an interdisciplinary research group located within the Center for Quality and Productivity Improvement in the College of Engineering at the University of Wisconsin-Madison.6,7 SEIPS uses HF principles to study the safety and quality of healthcare systems.
Congestive heart failure order sets: Researchers in another study incorporated HF science in their review of clinical practice guideline use and application for congestive heart failure (CHF). Reingold and Kulstad studied the impact of HF design elements on order set utilization and recommendations compliance.8
Using retrospective medical record review of adult patients admitted from the emergency department with CHF, the study measured acuity and clinical practice guideline (CPG) parameters before and after introducing new orders. In 87 adult patients before and 84 patients after beginning the new order set, attention to HF design elements significantly improved utilization of the orders and CPG compliance.
Infusion device programming: In another instance, a multidisciplinary research team applied HF design principles to common nursing procedures: programming an insulin infusion and programming a heparin infusion.9,10 An HF usability checklist was developed, and it revealed systematic error-provoking conditions in both tasks.
The good news is the pitfalls were remedied easily.
Not only did researchers subsequently commit to modify training procedures and redesign preprinted orders, they took the bigger step of providing feedback to the manufacturer and committing to incorporate usability testing in future procurement of medical devices. TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
References
1. Gosbee JW. Conclusion: you need human factors engineering expertise to see design hazards that are hiding in “plain sight!” Jt Comm J Qual Saf. 2004;30(12):696-700.
2. Gosbee J. Introduction to the human factors engineering series. Jt Comm J Qual Saf. 2004;30(4): 215-219.
3. Reason J. Human error: models and management. BMJ. 2000; 320(7237):768-770.
4. Etchells E, Juurlink D, Levinson W. Medication errors: the human factor. CMAJ. 2008;178(1):63-64.
5. Koppel R, Wetterneck T, Telles JL, Karsh BT. Workarounds to barcode medication administration systems: their occurrences, causes, and threats to patient safety. J Am Med Inform Assoc. 2008;15(4):408-423.
6. SEIPS model. http://cqpi.engr.wisc.edu/seips_ home/. Accessed Dec. 20, 2008.
7. Carayon P, Schoofs Hundt A, Karsh BT, et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15 Suppl 1:850-858.
8. Reingold S, Kulstad E. Impact of human factor design on the use of order sets in the treatment of congestive heart failure. Acad Emerg Med. 2007;14(11):1097-1105.
9. Etchells E, Bailey C, Biason R, et al. Human factors in action: getting “pumped” at a nursing usability laboratory. Healthc Q. 2006;9 Spec No:69-74.
10. Carayon P, Wetterneck T, Schoofs Hundt A, et al. Observing nurse interaction with infusion pump technologies. In: Henriksen K, Battles J, Lewin D, eds. Advances in Patient Safety: From Research to Implementation. Rockville, Md.: Agency for Healthcare Research and Quality; Feb. 2005, AHRQ Publication No. 05-0021-2.
When Amsterdam Airport Schiphol in the Netherlands revamped its men’s restrooms, the architects installed small, Euro-style urinals: a surefire way to throw urine off target. To solve this problem, the black outline of a fly was etched in the porcelain near each urinal’s drain. Users’ aim improved and spillage was reduced by 80%. “They try to power blast it away,” says Sanjay Saint, MD, hospitalist and professor of internal medicine at the Ann Arbor VA Medical Center, University of Michigan. “By the time they might realize that the fly isn’t going anywhere, the men are done and walking away.”
It’s a guy thing, sure. It also is an example of a human factors intervention. “Science teaches us that implementing a design for a machine or device that elicits an instinctive reaction from someone using it is a clear-cut way to avoid error,” Dr. Saint explains.
What It Is and Why It’s Important
Human factors (HF), or human factors engineering (HFE), also sometimes called usability engineering or systems-based practice, refers to the study of human abilities and characteristics as they affect the design and smooth operation of equipment, systems, and jobs.1 HF is the basic science underlying much of patient safety practice. For instance, the current recommendation that hospitals standardize equipment, such as ventilators, programmable IV pumps, and defibrillators, is an example of making tasks human friendly. The use of cognitive psychology and biomechanics to develop and improve software and hand tools are another example of HF principles.
In general, HF examines the component tasks of an activity in terms of three factorial domains: physical and environmental factors, cognitive factors (skill demands and mental workload), and organizational factors. Each task is assessed in terms of necessary interactions of the individual and work environment, the device/system design, and associated team dynamics.
HF use in healthcare is not new; for roughly four decades HF researchers have emphasized the key role of HF in safe medical design, healthcare facility operations, and patient safety processes. HF helps organizations deepen analyses of adverse events and develop effective solutions.2 HF is used in the design of labeling, warnings or alarms, software programs, information displays, paper forms, process and activity flow, workplace design, cognitive aids, decision support systems, and policies and protocols.
For hospitalists, human factors knowledge is most useful in process improvement, says John Gosbee, MD, MS, a human factors engineering and healthcare specialist at the University of Michigan. Dr. Gosbee, who has worked with hospitalists in Ann Arbor and around the country, originally studied aerospace medicine, pursued a subspecialty in occupational medicine, and from 1988 to 1992 worked at NASA designing space hospitals. In the dozens of lectures and workshops he has conducted, he has learned numerous physicians resist learning about HF. At first they protest, claiming they “didn’t go to medical school to become engineers” or “weren’t hired to have you tell us we need to be some kind of designer or computer-science software evaluator.”
Dr. Gosbee couldn’t agree more, but after the a-ha! moment, usually in an interactive experience when the hospitalist sees a poor system design is an obstacle to safety and process flow, they open up to adopting the HF mindset. Once on board with HF, hospitalists are quick to translate the theories to their own practices, identifying potential vulnerabilities and risks.
Manufacturers of healthcare equipment and systems don’t want to hear from “safety geeks,” Dr. Gosbee says; the companies want to hear from front-line providers who regularly use the products. “Hospitalists are in great position to provide that input because they see what happens across a broad swath of hospital settings,” he says, “and they could amalgamate the fact that everyone across specialties is having some trouble with this computer screen or new infusion device.”
Dr. Gosbee’s first-hand knowledge and experience solving hospitalist issues with HF techniques evolved into a teaching career. He says the university administration supports his belief in the practicality of HF lessons, and he now works as the lead instructor for a majority of the university’s medical residents.
“Human factors engineering is an efficient way to flip people’s brains around 180 degrees toward systems thinking,” Dr. Gosbee explains, “which is required if the organization wants to become a high-reliability organization.”3
Examples in Medicine
Russ Cucina, MD, MS, hospitalist at the University of California San Francisco Medical Center, describes a practical example of human factors engineering in a simple, widely used design. When cars ran on leaded gasoline, the design of the leaded gas pump nozzle precluded it from being inserted into an unleaded gas tank. “Even though one was clearly labeled leaded and other unleaded, human beings are bad at catching those things, especially when they’re in a hurry and under stress,” says Dr. Cucina, whose research includes clinical human-computer interaction science with an emphasis on human factors and patient safety.
A similar concept is what is missing from the Swan Ganz catheter design. The three ports (proximal, middle, and distal) connecting the catheter to the ICU monitor all have the same shape, making it easy to errantly connect one or more to the wrong port. “You’d think the manufacturers would shape the connectors in a way that would preclude incorrect connections,” Dr. Cucina says, “but that has not been done. We leave it to the vigilance of the bedside nurse or intensivist or hospitalist to hook these up correctly, rather than redesigning them so that cannot be done incorrectly.”
One way to think about human factors engineering is to think about forcing “a round peg into a square hole.” In the hospital setting, round pegs into square holes equate to errors. HF tries to solve the issue (round peg into a round hole, and vice versa). “Were you to apply human factors to the Swan Ganz catheter port connectors,” Dr. Cucina says, “you’d have round into the round hole, square into the square, and triangular into the triangular. You’d have no choice but to do the right thing.”
Efforts to implement systems that anticipate and minimize the chances of human error, such as computer physician order entry and patient bar coding, are attempts to overcome by design those instances where it is possible to place round pegs into square holes.
HF Projects in Motion
A number of hospitalists around the country have or are using HF as part of projects and studies to reduce human errors.
Culture change: In the early 2000s, Janet Nagamine, MD, a hospitalist with Kaiser Permanente in Santa Clara, Calif., and her colleagues took human factors concepts to front-line ICU staff. The human factors training provided a framework to reinforce three basic concepts: all humans make errors; processes can be designed to reduce the possibility of error; and processes can be designed so errors are detected and corrected before causing injury.4 “My colleagues and I knew that the punitive, ‘shame-and-blame’ culture around mistakes and errors were preventing us from identifying problems and moving forward with solutions,” Dr. Nagamine says.
A former ICU nurse and current chair of SHM’s Hospital Quality and Patient Safety (HQPS) Committee, Dr. Nagamine first became involved in HF when she realized how many patients suffered adverse events stemming from poorly designed medical systems. “Some of my most respected mentors were involved in these kinds of cases, and I knew eventually that would be me,” she says. It was a disturbing reality. During her medical training it was drilled into her head smart, diligent doctors would be successful. “But bad things happen in medicine; it’s part of what we do,” she says. “Rather than deny that things will inevitably go wrong, I wanted to study safety science and reliable system design.” She asked herself, how can we prevent the same mistakes from happening to competent people who practice in poorly designed systems? “The patterns are there,” she says. “You can train your eyes to look for vulnerabilities and patterns, then find the solutions.”
After she started looking at adverse events as system failures, rather than solely personal failures, she engaged the staff to redesign systems. She introduced HF concepts and provided an infrastructure to make it safe to report and discuss problems. The project included a new medication error reporting system and the creation of departmental patient safety teams. A palpable culture change developed when front-line staff and managers became empowered to find solutions working side-by-side with the quality and risk management departments.
The result? A dramatic increase in medication errors and near-miss reports: from eight faulty problems per quarter in 2000 to 200 reports per quarter by 2001.
To sum up the essence of Dr. Nagamine’s project, she invokes her favorite quotation from systems expert James Reason: “We can’t change the human condition, but we can change the conditions under which humans work.”1,5
Bar coding workarounds: Hospitalist Tosha Wetterneck, MD, and her colleagues at the University of Wisconsin School of Medicine and Dentistry focused their HF-trained eyes on medication errors.5 The team applied HF concepts as part of a study of bar-coded medication administration systems (BCMAs). Ideally, BCMAs help confirm the five rights of medication administration: the right patient, drug, dose, route, and time. The study authors identified the hospitalist staff had developed 46 workarounds in place of proper use of the BCMA. With each workaround, the researchers identified six potential errors. Furthermore, nurses were overriding the BCMA alerts for 4.2% of patients charted, and for 10.3% of total medication.
By creating an exhaustive template, the study authors broke down the use of BCMA workarounds to the finest detail of task component. They learned many workarounds were engendered by difficulties with the technology and by interactions between BCMA technologies and environmental, technical, process, workload, training, and policy concerns. Data shows BCMAs still have an important role in preventing error; during one year, almost 24,000 BCMA alerts led users to change their action, instead of overriding an alert. “These causes (and related workarounds) are neither rare nor secret,” the authors write. “They are hiding in plain sight.”1,5
Dr. Wetterneck is part of the Systems Engineering Initiative for Patient Safety (SEIPS), an interdisciplinary research group located within the Center for Quality and Productivity Improvement in the College of Engineering at the University of Wisconsin-Madison.6,7 SEIPS uses HF principles to study the safety and quality of healthcare systems.
Congestive heart failure order sets: Researchers in another study incorporated HF science in their review of clinical practice guideline use and application for congestive heart failure (CHF). Reingold and Kulstad studied the impact of HF design elements on order set utilization and recommendations compliance.8
Using retrospective medical record review of adult patients admitted from the emergency department with CHF, the study measured acuity and clinical practice guideline (CPG) parameters before and after introducing new orders. In 87 adult patients before and 84 patients after beginning the new order set, attention to HF design elements significantly improved utilization of the orders and CPG compliance.
Infusion device programming: In another instance, a multidisciplinary research team applied HF design principles to common nursing procedures: programming an insulin infusion and programming a heparin infusion.9,10 An HF usability checklist was developed, and it revealed systematic error-provoking conditions in both tasks.
The good news is the pitfalls were remedied easily.
Not only did researchers subsequently commit to modify training procedures and redesign preprinted orders, they took the bigger step of providing feedback to the manufacturer and committing to incorporate usability testing in future procurement of medical devices. TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
References
1. Gosbee JW. Conclusion: you need human factors engineering expertise to see design hazards that are hiding in “plain sight!” Jt Comm J Qual Saf. 2004;30(12):696-700.
2. Gosbee J. Introduction to the human factors engineering series. Jt Comm J Qual Saf. 2004;30(4): 215-219.
3. Reason J. Human error: models and management. BMJ. 2000; 320(7237):768-770.
4. Etchells E, Juurlink D, Levinson W. Medication errors: the human factor. CMAJ. 2008;178(1):63-64.
5. Koppel R, Wetterneck T, Telles JL, Karsh BT. Workarounds to barcode medication administration systems: their occurrences, causes, and threats to patient safety. J Am Med Inform Assoc. 2008;15(4):408-423.
6. SEIPS model. http://cqpi.engr.wisc.edu/seips_ home/. Accessed Dec. 20, 2008.
7. Carayon P, Schoofs Hundt A, Karsh BT, et al. Work system design for patient safety: the SEIPS model. Qual Saf Health Care. 2006;15 Suppl 1:850-858.
8. Reingold S, Kulstad E. Impact of human factor design on the use of order sets in the treatment of congestive heart failure. Acad Emerg Med. 2007;14(11):1097-1105.
9. Etchells E, Bailey C, Biason R, et al. Human factors in action: getting “pumped” at a nursing usability laboratory. Healthc Q. 2006;9 Spec No:69-74.
10. Carayon P, Wetterneck T, Schoofs Hundt A, et al. Observing nurse interaction with infusion pump technologies. In: Henriksen K, Battles J, Lewin D, eds. Advances in Patient Safety: From Research to Implementation. Rockville, Md.: Agency for Healthcare Research and Quality; Feb. 2005, AHRQ Publication No. 05-0021-2.
Resident Restrictions
Effective July 1, the Accreditation Council for Graduate Medical Education (ACGME) is adopting rules changes to further restrict the number of patients internal medicine residents follow. The impact of this change may reach beyond academic institutions and teaching services. Non-teaching services and institutions may see some fallout, as hospital administration shuffles caseloads of residents and hospitalist attendings. The potential results likely will impact resident training, hospitalist training, and hospitalist practice management, namely recruitment and hospitalist job satisfaction.
Why the Change?
With the 2003 restrictions on resident work-hours duty and now the capping of patient caseloads, the ACGME is attempting to ensure residency programs are not viewed as a source of cheap labor and excessive stress. Also, “the Residency Review Committee (RRC) is cognizant too much service can be a barrier to education,” says Lenny Feldman, MD, a hospitalist and associate program director at Johns Hopkins Medical Center in Baltimore. But there is a danger in the reverse: too little service may undersupply residents with the depth and breadth of cases they need under their belts to competently enter practice. “Education should be the foremost mission for residency programs, but trying to find that exact balance between service and education is tough,” Dr. Feldman says.
In a Nutshell
As leader of the 70-hospitalist Health Partners Medical Group in Minneapolis-St. Paul, a University of Minnesota affiliate working with internal medicine residents, Burke T. Kealey, MD, views the ACGME rule change on a professional and personal level. In the big picture, Dr. Kealey observes three main effects:
- Hospitalists will be seeing more patients and probably more patients at night;
- The cost of hospital care will increase for hospitals and hospital medicine groups (HMGs); and
- The experience level of new graduates applying to be hospitalists will diminish.
In essence, there are few ways to handle the looming cap on residents’ patient caseloads. (see Practical Approaches, p. 24) Given the financial constraints imposed by this new, unfunded mandate, and taking into account the fact most residency programs depend on federal funding, it generally is believed increasing the number of residents cannot be considered an option. “Given the looming physician shortage, there is pressure on the federal government to increase the amount of GME support and the number of residency spots,” Dr. Feldman says. “Medical schools have increased enrollment pretty significantly, but the bottleneck is the number of GME-supported residency positions.”
HM Crossroads
Leslie Flores, MHA, principal with Nelson Flores Hospital Medicine Consultants, and the director of SHM’s Practice Management Institute, believes the new rule dramatically will impact teaching hospitals and HMGs. “I think it is likely to be harder for academic hospitalists, who are working on teaching services, to generate reasonable productivity, which will place an even greater financial burden on academic practices,” she says. “But the larger effect will be that non-teaching services in teaching hospitals will be expected to pick up the slack and, subsequently, grow in order to accommodate the patient numbers.”
Asking staff physicians to increase their patient load, even incrementally, is a poor solution, at best, Dr. Kealey says. And it may be tough for some places to recruit more hospitalists, a function of the hospitalist labor shortage.
William Rifkin, MD, a hospitalist and associate director of clinical medicine at Albert Einstein College of Medicine, and director of the residency program at Jacobi Medical Center, Bronx, N.Y., estimates hospitalist jobs in teaching institutions will increasingly morph into non-teaching positions. “Where currently the ratio of teaching to nonteaching jobs is 50-50,” Dr. Rifkin says, “by 2009, 80% of internal medicine training programs will have to build or expand a new, non-teaching service, and more than half of hospitalist duties will be non-teaching.”
A recent recommendation from the Institute of Mecidine (IOM) reinforces the national movement to restructure resident work hours and duties. Released Dec. 2, 2008, the “Resident Duty Hours: Enhancing Sleep, Supervision, and Safety” report calls for a maximum shift length of 30 hours with admission of patients for up to 16 hours, plus a five-hour, uninterrupted sleep period between 10 p.m. and 8 a.m., with the remaining hours for transitional and educational activity.
The consensus is the ACGME rules changes likely will alter the hospitalist job description and produce an even greater shortage of qualified, experienced physicians. Leora Horwitz, MD, MHS, an assistant professor in internal medicine at Yale University School of Medicine in New Haven, Conn., says “hospitalists are really an amalgamation of two very distinct types: the short-term hospitalist who takes the job for a year or two right after residency and before fellowship, and the longer-term hospitalist who takes on the job as at least an intermediate-term career. It could be that recruitment and retention differ for these types.”
Dr. Rifkin isn’t alone when he asks, “Can a hospitalist last that long doing patient care alone? There are only so many people who will move up to be leaders in HMGs. So while this will probably be good for recruitment in the short term, in the long term, we don’t know.”
Immediate Consequences
Some ramifications of hospital medicine as a whole taking on more patients and more hospitalists will parallel the growing pains of individual HMGs. For instance, hospitalist group’s social bonds may not be as tight, says Dr. Feldman. But where many obstacles are surmountable, “what is not surmountable is if hospitals don’t choose to increase the size of their hospitalist programs. The deathblow to most hospitalist programs is if you ask the group, and each individual, to do more work that is not commensurate with the original expectations. And with the market already tight, most hospitals can’t afford to have unhappy hospitalists.”
Financially, the new rules will place a heavy burden on HMGs and hospital administrators. With no additional reimbursement under the GME system, most hospitals will have to get creative with existing budgets. “Part of the concern is that patients that hospitalists see on a teaching service tend to be the lower socioeconomic population of patients―Medicaid and self-pay patients―where there is inadequate reimbursement anyway,” Flores says. The answer likely will be sending those patients to a non-teaching service, which in essence transfers the financial burden. “Hospitals will have to find money from somewhere.”
Teaching hospitals not part of large academic medical centers contribute to hospitalists’ compensation when they help train family medicine and internal medicine residents. “Because they are not technically academic hospitalists,” Flores says, “they need to be alerted about how these rule changes may influence the way they manage and run the finances of their practice.”
Some of the solutions to the problems inherent in this change depend on the practice and scheduling model. In the aftermath of the work-hour restriction, many hospitalist programs changed their scheduling method to day float/night float, or the “drip” method of admission (taking admissions every day), versus the “bolus” method (every fourth or fifth day), Dr. Feldman says. The bolus method likely leads to scenarios where the new ACGME cap will come into play.
There is the possibility the rule change could turn out to be a boon to HMGs, Dr. Feldman says. Programs without hospitalists may hire them; small groups may expand, increasing job opportunities. Additionally, teaching opportunities for hospitalist attendings may improve with the decreased number of patients on a service residents follow. “Hopefully, this will increase opportunities for teaching residents and increase the satisfaction of those involved in teaching,” he says. “Ultimately, it may result in improved resident education while creating more job opportunities for hospitalists―a win-win for both groups.”
Will Training Suffer?
Dr. Kealey has concerns about the long-term effects on the training residents who become hospitalists. “First, they won’t get enough experience to be competent hospitalists on graduation. Second, the number of patients is being capped, but the number of ACGME-required outpatient clinic sessions is rising, increasing from about 108 to 130 over a 30-month period,” he says. “Residency programs will to have to figure out how to fit these sessions into training, and that may squeeze out inpatient time.”
Third, with the work hours and caseload restrictions on residents, educators are concerned residents will not receive an adequate level of training.
Kenneth P. Patrick, MD, director of the hospitalist program at Chestnut Hill Hospital in Philadelphia, is worried, too, especially when it comes to the educational implications. As a former residency program director, one who shares concerns about residents’ large workloads, Dr. Patrick believes strongly in medical education and is wary of the path it seems to be taking. “What a hospital medicine group can provide to residents is the opportunity to learn from a smaller patient load,” Dr. Patrick says, “and regulatory agencies should carefully address that. Cutting back on the number of service hours and patients can have both a positive and negative effect. Most people are only adjusting the numbers of hours and patients, and not viewing the whole picture.”
Another likely result of the rules change is the mindset residents could be developing, an issue that rings true with most HMG directors. “I worry that our residents will be sheltered during training and will emerge into a real world where there won’t be caps,” Dr. Kealey says. “They will be in systems where people have to cooperate with each other in order to handle patient surges and large patient volumes. Though they may graduate, join a group, and become acculturated, it concerns me that their initial primary training, rather than encouraging them to think as part of a system, may be training them to think of ‘my restrictions, my needs, my limitation.’ ”
Prepare for Change
What is the answer? Two hospitalists echoed the same, simple solutions: “Give us more money” and “We need more bodies.”
Simplicity aside, residency and hospital medicine programs will need to prepare for the change. “Instead of happening gradually, suddenly every [residency] program in the country will lose 20% of its capacity,” Dr. Rikfin says.
Michael Pistoria, DO, FACP, associate general division of internal medicine chief at Lehigh Valley Hospital in Allentown, Pa., believes institutions with closely aligned hospitalist and residency programs will benefit from “enlightenment on both sides. Residency programs are increasingly alert to the vital role that HMGs play in supporting residency programs,” he says. “They are more aware of the impact these types of decisions have on the staffing of HMGs.”
Mid-level providers are one possible solution. “Programs will increasingly look to supplement their existing group with advanced practice clinicians—physician assistants and non-physician providers―a less-expensive alternative,” Dr. Pistoria says
Does hiring mid-level practitioners pose a risk for unintended adverse events and delays to diagnosis? “There may be an extended growth curve for these providers,” Dr. Pistoria says, “due to less clinical exposure and experience than a new physician hospitalist just out of residency.”
However, these advanced practice clinicians often are quick to adapt to the hospitalist setting, learning the skills required to be an effective hospitalist through on-the-job training. “On-the-job training for physician hospitalists can focus on education, quality improvement, safety―some of the value-added pieces,” Dr. Pistoria points out.
Without a doubt, ACGME’s new cap on residency caseloads will impact hospital medicine, both at the national level and the individual group level. HMG efforts to recruit, schedule, train and pay hospitalists will be affected, as will the level of experience patients receive from recent residency graduates.
“It is incumbent on us to get involved in committees and process and performance improvement projects,” Dr. Pistoria says, “so that when leadership approaches administrators regarding residency caseload cutbacks, we can make a strong case for recruiting more hospitalists.” TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
Effective July 1, the Accreditation Council for Graduate Medical Education (ACGME) is adopting rules changes to further restrict the number of patients internal medicine residents follow. The impact of this change may reach beyond academic institutions and teaching services. Non-teaching services and institutions may see some fallout, as hospital administration shuffles caseloads of residents and hospitalist attendings. The potential results likely will impact resident training, hospitalist training, and hospitalist practice management, namely recruitment and hospitalist job satisfaction.
Why the Change?
With the 2003 restrictions on resident work-hours duty and now the capping of patient caseloads, the ACGME is attempting to ensure residency programs are not viewed as a source of cheap labor and excessive stress. Also, “the Residency Review Committee (RRC) is cognizant too much service can be a barrier to education,” says Lenny Feldman, MD, a hospitalist and associate program director at Johns Hopkins Medical Center in Baltimore. But there is a danger in the reverse: too little service may undersupply residents with the depth and breadth of cases they need under their belts to competently enter practice. “Education should be the foremost mission for residency programs, but trying to find that exact balance between service and education is tough,” Dr. Feldman says.
In a Nutshell
As leader of the 70-hospitalist Health Partners Medical Group in Minneapolis-St. Paul, a University of Minnesota affiliate working with internal medicine residents, Burke T. Kealey, MD, views the ACGME rule change on a professional and personal level. In the big picture, Dr. Kealey observes three main effects:
- Hospitalists will be seeing more patients and probably more patients at night;
- The cost of hospital care will increase for hospitals and hospital medicine groups (HMGs); and
- The experience level of new graduates applying to be hospitalists will diminish.
In essence, there are few ways to handle the looming cap on residents’ patient caseloads. (see Practical Approaches, p. 24) Given the financial constraints imposed by this new, unfunded mandate, and taking into account the fact most residency programs depend on federal funding, it generally is believed increasing the number of residents cannot be considered an option. “Given the looming physician shortage, there is pressure on the federal government to increase the amount of GME support and the number of residency spots,” Dr. Feldman says. “Medical schools have increased enrollment pretty significantly, but the bottleneck is the number of GME-supported residency positions.”
HM Crossroads
Leslie Flores, MHA, principal with Nelson Flores Hospital Medicine Consultants, and the director of SHM’s Practice Management Institute, believes the new rule dramatically will impact teaching hospitals and HMGs. “I think it is likely to be harder for academic hospitalists, who are working on teaching services, to generate reasonable productivity, which will place an even greater financial burden on academic practices,” she says. “But the larger effect will be that non-teaching services in teaching hospitals will be expected to pick up the slack and, subsequently, grow in order to accommodate the patient numbers.”
Asking staff physicians to increase their patient load, even incrementally, is a poor solution, at best, Dr. Kealey says. And it may be tough for some places to recruit more hospitalists, a function of the hospitalist labor shortage.
William Rifkin, MD, a hospitalist and associate director of clinical medicine at Albert Einstein College of Medicine, and director of the residency program at Jacobi Medical Center, Bronx, N.Y., estimates hospitalist jobs in teaching institutions will increasingly morph into non-teaching positions. “Where currently the ratio of teaching to nonteaching jobs is 50-50,” Dr. Rifkin says, “by 2009, 80% of internal medicine training programs will have to build or expand a new, non-teaching service, and more than half of hospitalist duties will be non-teaching.”
A recent recommendation from the Institute of Mecidine (IOM) reinforces the national movement to restructure resident work hours and duties. Released Dec. 2, 2008, the “Resident Duty Hours: Enhancing Sleep, Supervision, and Safety” report calls for a maximum shift length of 30 hours with admission of patients for up to 16 hours, plus a five-hour, uninterrupted sleep period between 10 p.m. and 8 a.m., with the remaining hours for transitional and educational activity.
The consensus is the ACGME rules changes likely will alter the hospitalist job description and produce an even greater shortage of qualified, experienced physicians. Leora Horwitz, MD, MHS, an assistant professor in internal medicine at Yale University School of Medicine in New Haven, Conn., says “hospitalists are really an amalgamation of two very distinct types: the short-term hospitalist who takes the job for a year or two right after residency and before fellowship, and the longer-term hospitalist who takes on the job as at least an intermediate-term career. It could be that recruitment and retention differ for these types.”
Dr. Rifkin isn’t alone when he asks, “Can a hospitalist last that long doing patient care alone? There are only so many people who will move up to be leaders in HMGs. So while this will probably be good for recruitment in the short term, in the long term, we don’t know.”
Immediate Consequences
Some ramifications of hospital medicine as a whole taking on more patients and more hospitalists will parallel the growing pains of individual HMGs. For instance, hospitalist group’s social bonds may not be as tight, says Dr. Feldman. But where many obstacles are surmountable, “what is not surmountable is if hospitals don’t choose to increase the size of their hospitalist programs. The deathblow to most hospitalist programs is if you ask the group, and each individual, to do more work that is not commensurate with the original expectations. And with the market already tight, most hospitals can’t afford to have unhappy hospitalists.”
Financially, the new rules will place a heavy burden on HMGs and hospital administrators. With no additional reimbursement under the GME system, most hospitals will have to get creative with existing budgets. “Part of the concern is that patients that hospitalists see on a teaching service tend to be the lower socioeconomic population of patients―Medicaid and self-pay patients―where there is inadequate reimbursement anyway,” Flores says. The answer likely will be sending those patients to a non-teaching service, which in essence transfers the financial burden. “Hospitals will have to find money from somewhere.”
Teaching hospitals not part of large academic medical centers contribute to hospitalists’ compensation when they help train family medicine and internal medicine residents. “Because they are not technically academic hospitalists,” Flores says, “they need to be alerted about how these rule changes may influence the way they manage and run the finances of their practice.”
Some of the solutions to the problems inherent in this change depend on the practice and scheduling model. In the aftermath of the work-hour restriction, many hospitalist programs changed their scheduling method to day float/night float, or the “drip” method of admission (taking admissions every day), versus the “bolus” method (every fourth or fifth day), Dr. Feldman says. The bolus method likely leads to scenarios where the new ACGME cap will come into play.
There is the possibility the rule change could turn out to be a boon to HMGs, Dr. Feldman says. Programs without hospitalists may hire them; small groups may expand, increasing job opportunities. Additionally, teaching opportunities for hospitalist attendings may improve with the decreased number of patients on a service residents follow. “Hopefully, this will increase opportunities for teaching residents and increase the satisfaction of those involved in teaching,” he says. “Ultimately, it may result in improved resident education while creating more job opportunities for hospitalists―a win-win for both groups.”
Will Training Suffer?
Dr. Kealey has concerns about the long-term effects on the training residents who become hospitalists. “First, they won’t get enough experience to be competent hospitalists on graduation. Second, the number of patients is being capped, but the number of ACGME-required outpatient clinic sessions is rising, increasing from about 108 to 130 over a 30-month period,” he says. “Residency programs will to have to figure out how to fit these sessions into training, and that may squeeze out inpatient time.”
Third, with the work hours and caseload restrictions on residents, educators are concerned residents will not receive an adequate level of training.
Kenneth P. Patrick, MD, director of the hospitalist program at Chestnut Hill Hospital in Philadelphia, is worried, too, especially when it comes to the educational implications. As a former residency program director, one who shares concerns about residents’ large workloads, Dr. Patrick believes strongly in medical education and is wary of the path it seems to be taking. “What a hospital medicine group can provide to residents is the opportunity to learn from a smaller patient load,” Dr. Patrick says, “and regulatory agencies should carefully address that. Cutting back on the number of service hours and patients can have both a positive and negative effect. Most people are only adjusting the numbers of hours and patients, and not viewing the whole picture.”
Another likely result of the rules change is the mindset residents could be developing, an issue that rings true with most HMG directors. “I worry that our residents will be sheltered during training and will emerge into a real world where there won’t be caps,” Dr. Kealey says. “They will be in systems where people have to cooperate with each other in order to handle patient surges and large patient volumes. Though they may graduate, join a group, and become acculturated, it concerns me that their initial primary training, rather than encouraging them to think as part of a system, may be training them to think of ‘my restrictions, my needs, my limitation.’ ”
Prepare for Change
What is the answer? Two hospitalists echoed the same, simple solutions: “Give us more money” and “We need more bodies.”
Simplicity aside, residency and hospital medicine programs will need to prepare for the change. “Instead of happening gradually, suddenly every [residency] program in the country will lose 20% of its capacity,” Dr. Rikfin says.
Michael Pistoria, DO, FACP, associate general division of internal medicine chief at Lehigh Valley Hospital in Allentown, Pa., believes institutions with closely aligned hospitalist and residency programs will benefit from “enlightenment on both sides. Residency programs are increasingly alert to the vital role that HMGs play in supporting residency programs,” he says. “They are more aware of the impact these types of decisions have on the staffing of HMGs.”
Mid-level providers are one possible solution. “Programs will increasingly look to supplement their existing group with advanced practice clinicians—physician assistants and non-physician providers―a less-expensive alternative,” Dr. Pistoria says
Does hiring mid-level practitioners pose a risk for unintended adverse events and delays to diagnosis? “There may be an extended growth curve for these providers,” Dr. Pistoria says, “due to less clinical exposure and experience than a new physician hospitalist just out of residency.”
However, these advanced practice clinicians often are quick to adapt to the hospitalist setting, learning the skills required to be an effective hospitalist through on-the-job training. “On-the-job training for physician hospitalists can focus on education, quality improvement, safety―some of the value-added pieces,” Dr. Pistoria points out.
Without a doubt, ACGME’s new cap on residency caseloads will impact hospital medicine, both at the national level and the individual group level. HMG efforts to recruit, schedule, train and pay hospitalists will be affected, as will the level of experience patients receive from recent residency graduates.
“It is incumbent on us to get involved in committees and process and performance improvement projects,” Dr. Pistoria says, “so that when leadership approaches administrators regarding residency caseload cutbacks, we can make a strong case for recruiting more hospitalists.” TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
Effective July 1, the Accreditation Council for Graduate Medical Education (ACGME) is adopting rules changes to further restrict the number of patients internal medicine residents follow. The impact of this change may reach beyond academic institutions and teaching services. Non-teaching services and institutions may see some fallout, as hospital administration shuffles caseloads of residents and hospitalist attendings. The potential results likely will impact resident training, hospitalist training, and hospitalist practice management, namely recruitment and hospitalist job satisfaction.
Why the Change?
With the 2003 restrictions on resident work-hours duty and now the capping of patient caseloads, the ACGME is attempting to ensure residency programs are not viewed as a source of cheap labor and excessive stress. Also, “the Residency Review Committee (RRC) is cognizant too much service can be a barrier to education,” says Lenny Feldman, MD, a hospitalist and associate program director at Johns Hopkins Medical Center in Baltimore. But there is a danger in the reverse: too little service may undersupply residents with the depth and breadth of cases they need under their belts to competently enter practice. “Education should be the foremost mission for residency programs, but trying to find that exact balance between service and education is tough,” Dr. Feldman says.
In a Nutshell
As leader of the 70-hospitalist Health Partners Medical Group in Minneapolis-St. Paul, a University of Minnesota affiliate working with internal medicine residents, Burke T. Kealey, MD, views the ACGME rule change on a professional and personal level. In the big picture, Dr. Kealey observes three main effects:
- Hospitalists will be seeing more patients and probably more patients at night;
- The cost of hospital care will increase for hospitals and hospital medicine groups (HMGs); and
- The experience level of new graduates applying to be hospitalists will diminish.
In essence, there are few ways to handle the looming cap on residents’ patient caseloads. (see Practical Approaches, p. 24) Given the financial constraints imposed by this new, unfunded mandate, and taking into account the fact most residency programs depend on federal funding, it generally is believed increasing the number of residents cannot be considered an option. “Given the looming physician shortage, there is pressure on the federal government to increase the amount of GME support and the number of residency spots,” Dr. Feldman says. “Medical schools have increased enrollment pretty significantly, but the bottleneck is the number of GME-supported residency positions.”
HM Crossroads
Leslie Flores, MHA, principal with Nelson Flores Hospital Medicine Consultants, and the director of SHM’s Practice Management Institute, believes the new rule dramatically will impact teaching hospitals and HMGs. “I think it is likely to be harder for academic hospitalists, who are working on teaching services, to generate reasonable productivity, which will place an even greater financial burden on academic practices,” she says. “But the larger effect will be that non-teaching services in teaching hospitals will be expected to pick up the slack and, subsequently, grow in order to accommodate the patient numbers.”
Asking staff physicians to increase their patient load, even incrementally, is a poor solution, at best, Dr. Kealey says. And it may be tough for some places to recruit more hospitalists, a function of the hospitalist labor shortage.
William Rifkin, MD, a hospitalist and associate director of clinical medicine at Albert Einstein College of Medicine, and director of the residency program at Jacobi Medical Center, Bronx, N.Y., estimates hospitalist jobs in teaching institutions will increasingly morph into non-teaching positions. “Where currently the ratio of teaching to nonteaching jobs is 50-50,” Dr. Rifkin says, “by 2009, 80% of internal medicine training programs will have to build or expand a new, non-teaching service, and more than half of hospitalist duties will be non-teaching.”
A recent recommendation from the Institute of Mecidine (IOM) reinforces the national movement to restructure resident work hours and duties. Released Dec. 2, 2008, the “Resident Duty Hours: Enhancing Sleep, Supervision, and Safety” report calls for a maximum shift length of 30 hours with admission of patients for up to 16 hours, plus a five-hour, uninterrupted sleep period between 10 p.m. and 8 a.m., with the remaining hours for transitional and educational activity.
The consensus is the ACGME rules changes likely will alter the hospitalist job description and produce an even greater shortage of qualified, experienced physicians. Leora Horwitz, MD, MHS, an assistant professor in internal medicine at Yale University School of Medicine in New Haven, Conn., says “hospitalists are really an amalgamation of two very distinct types: the short-term hospitalist who takes the job for a year or two right after residency and before fellowship, and the longer-term hospitalist who takes on the job as at least an intermediate-term career. It could be that recruitment and retention differ for these types.”
Dr. Rifkin isn’t alone when he asks, “Can a hospitalist last that long doing patient care alone? There are only so many people who will move up to be leaders in HMGs. So while this will probably be good for recruitment in the short term, in the long term, we don’t know.”
Immediate Consequences
Some ramifications of hospital medicine as a whole taking on more patients and more hospitalists will parallel the growing pains of individual HMGs. For instance, hospitalist group’s social bonds may not be as tight, says Dr. Feldman. But where many obstacles are surmountable, “what is not surmountable is if hospitals don’t choose to increase the size of their hospitalist programs. The deathblow to most hospitalist programs is if you ask the group, and each individual, to do more work that is not commensurate with the original expectations. And with the market already tight, most hospitals can’t afford to have unhappy hospitalists.”
Financially, the new rules will place a heavy burden on HMGs and hospital administrators. With no additional reimbursement under the GME system, most hospitals will have to get creative with existing budgets. “Part of the concern is that patients that hospitalists see on a teaching service tend to be the lower socioeconomic population of patients―Medicaid and self-pay patients―where there is inadequate reimbursement anyway,” Flores says. The answer likely will be sending those patients to a non-teaching service, which in essence transfers the financial burden. “Hospitals will have to find money from somewhere.”
Teaching hospitals not part of large academic medical centers contribute to hospitalists’ compensation when they help train family medicine and internal medicine residents. “Because they are not technically academic hospitalists,” Flores says, “they need to be alerted about how these rule changes may influence the way they manage and run the finances of their practice.”
Some of the solutions to the problems inherent in this change depend on the practice and scheduling model. In the aftermath of the work-hour restriction, many hospitalist programs changed their scheduling method to day float/night float, or the “drip” method of admission (taking admissions every day), versus the “bolus” method (every fourth or fifth day), Dr. Feldman says. The bolus method likely leads to scenarios where the new ACGME cap will come into play.
There is the possibility the rule change could turn out to be a boon to HMGs, Dr. Feldman says. Programs without hospitalists may hire them; small groups may expand, increasing job opportunities. Additionally, teaching opportunities for hospitalist attendings may improve with the decreased number of patients on a service residents follow. “Hopefully, this will increase opportunities for teaching residents and increase the satisfaction of those involved in teaching,” he says. “Ultimately, it may result in improved resident education while creating more job opportunities for hospitalists―a win-win for both groups.”
Will Training Suffer?
Dr. Kealey has concerns about the long-term effects on the training residents who become hospitalists. “First, they won’t get enough experience to be competent hospitalists on graduation. Second, the number of patients is being capped, but the number of ACGME-required outpatient clinic sessions is rising, increasing from about 108 to 130 over a 30-month period,” he says. “Residency programs will to have to figure out how to fit these sessions into training, and that may squeeze out inpatient time.”
Third, with the work hours and caseload restrictions on residents, educators are concerned residents will not receive an adequate level of training.
Kenneth P. Patrick, MD, director of the hospitalist program at Chestnut Hill Hospital in Philadelphia, is worried, too, especially when it comes to the educational implications. As a former residency program director, one who shares concerns about residents’ large workloads, Dr. Patrick believes strongly in medical education and is wary of the path it seems to be taking. “What a hospital medicine group can provide to residents is the opportunity to learn from a smaller patient load,” Dr. Patrick says, “and regulatory agencies should carefully address that. Cutting back on the number of service hours and patients can have both a positive and negative effect. Most people are only adjusting the numbers of hours and patients, and not viewing the whole picture.”
Another likely result of the rules change is the mindset residents could be developing, an issue that rings true with most HMG directors. “I worry that our residents will be sheltered during training and will emerge into a real world where there won’t be caps,” Dr. Kealey says. “They will be in systems where people have to cooperate with each other in order to handle patient surges and large patient volumes. Though they may graduate, join a group, and become acculturated, it concerns me that their initial primary training, rather than encouraging them to think as part of a system, may be training them to think of ‘my restrictions, my needs, my limitation.’ ”
Prepare for Change
What is the answer? Two hospitalists echoed the same, simple solutions: “Give us more money” and “We need more bodies.”
Simplicity aside, residency and hospital medicine programs will need to prepare for the change. “Instead of happening gradually, suddenly every [residency] program in the country will lose 20% of its capacity,” Dr. Rikfin says.
Michael Pistoria, DO, FACP, associate general division of internal medicine chief at Lehigh Valley Hospital in Allentown, Pa., believes institutions with closely aligned hospitalist and residency programs will benefit from “enlightenment on both sides. Residency programs are increasingly alert to the vital role that HMGs play in supporting residency programs,” he says. “They are more aware of the impact these types of decisions have on the staffing of HMGs.”
Mid-level providers are one possible solution. “Programs will increasingly look to supplement their existing group with advanced practice clinicians—physician assistants and non-physician providers―a less-expensive alternative,” Dr. Pistoria says
Does hiring mid-level practitioners pose a risk for unintended adverse events and delays to diagnosis? “There may be an extended growth curve for these providers,” Dr. Pistoria says, “due to less clinical exposure and experience than a new physician hospitalist just out of residency.”
However, these advanced practice clinicians often are quick to adapt to the hospitalist setting, learning the skills required to be an effective hospitalist through on-the-job training. “On-the-job training for physician hospitalists can focus on education, quality improvement, safety―some of the value-added pieces,” Dr. Pistoria points out.
Without a doubt, ACGME’s new cap on residency caseloads will impact hospital medicine, both at the national level and the individual group level. HMG efforts to recruit, schedule, train and pay hospitalists will be affected, as will the level of experience patients receive from recent residency graduates.
“It is incumbent on us to get involved in committees and process and performance improvement projects,” Dr. Pistoria says, “so that when leadership approaches administrators regarding residency caseload cutbacks, we can make a strong case for recruiting more hospitalists.” TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
Deja Vu
We thought they were gone, but they’ve returned: diseases once considered “vintage bugs” that were common in as late as the mid-20th century. In the past these diseases killed one in three people younger than 20 who had survived an infancy during which many of their contemporaries died.1
“When you think about disease states, you think about some that are gone from the world,” says Erin Stucky, MD, a pediatric hospitalist at the University of California, San Diego, “but there are very few truly gone from the world.”
Some of the major infectious diseases that hospitalists may [still] see are pertussis (whooping cough), measles, and mumps, but scarlet fever and varicella (chicken pox) also endure—not to mention those occurrences of polio around the country that epidemiologists and infectious diseases specialists are monitoring closely. Rickets, a vitamin-D-deficiency-related disease also thought to be a relic of the 18th century, is showing up in certain patient populations—and not exclusively in infants and children.
This is a crossover clinical issue, our pediatric hospitalists say, and thus one to which their hospitalist partners who treat adult patients must also remain alert.


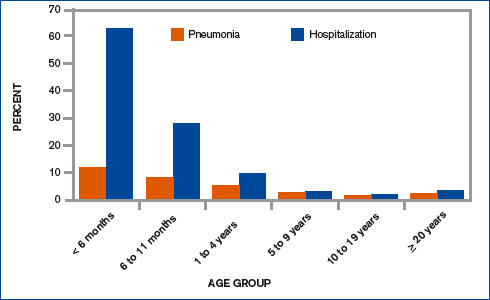
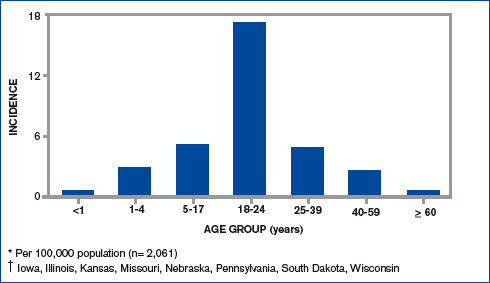
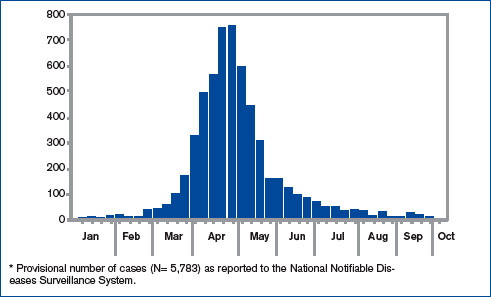
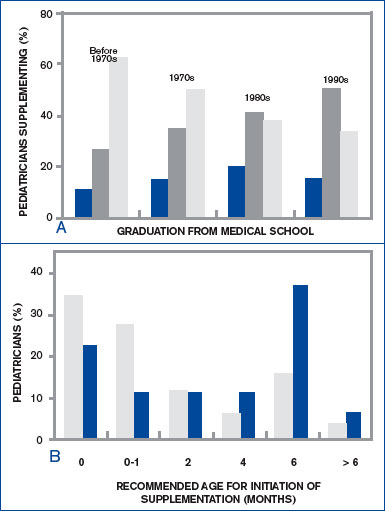
Pertussis (Whooping Cough)
Despite vaccination protocols, pediatric hospitalists continue to see whooping cough in young infants. (See Figure 1, p. 39.) Even with treatment, the damage can be severe, and the length of stay (LOS) is prolonged compared with those of most other patients with complex illnesses. “Vaccine fatigue” means that immunization lasts only until adolescence or early adulthood, at which time they need appropriate boosters. If the patient hasn’t receive boosters, the initial immunization loses its effectiveness; unprotected, they can be infected with the disease, though sometimes not badly enough for them to seek care. When they do, the diagnosis is often community-acquired mild pneumonia or a more traditional bronchitis. Either by accident or because the physician has given it thought, those illnesses are treated with a macrolide drug, which is also—coincidentally and serendipitously—the drug of choice for pertussis. But many remain carriers because they are not accurately diagnosed or never seek care.
“There is a huge reservoir of people carrying pertussis, particularly [in] the adolescent and adult population[s],” says Alison Holmes, MD, a pediatric hospitalist at Concord Hospital, N.H. “And the babies who get really sick from it are the under two- to three-month group who have not yet been immunized or have just been immunized. Because it is so rampant in the adolescent and adult community, those children can still get sick.”
“Unfortunately,” says Dr. Stucky, “what’s happening is that if physicians are not thinking pertussis, they don’t talk about pertussis to that adult patient who … is either around children or has children in the home. So they don’t know to tell that person to watch for these same signs and symptoms in that young infant, who then could have a much more severe outcome from getting [the infection].”
As with most patients who contract illnesses, these patients may never have heard of the disease and unless educated may not understand the implications of the diagnosis. They might realize their disease could spread to family members, “but most people don’t absorb that information and use that information thoughtfully,” says Dr. Stucky. The onus is, therefore, on the physician to warn adult patients specifically about the serious danger that exists for infants in the two- to three-month-old group, who may not have been vaccinated or whose single-vaccination immunity is not adequate protection against the disease.
While the numbers in babies appear to be what they have always been, the incidence has grown in the teen years and even later into adulthood. This is more likely the result of increased testing for pertussis, as opposed to being only due to a true resurgence. Data from studies of adults with prolonged cough revealed that 20% to 25% have serologic evidence of recent pertussis infection.2 Adults are the major reservoir of infection, and infection spreads quickly in a population in a closed environment where droplets spread easily person to person.5
For both teens and adults, testing and immunization with the newly recommended DTaP (diphtheria-tetanus-pertussis)—as opposed to the more limited Td—can help upgrade immunity. Although a patient can recover from pertussis on his or her own within one to two weeks following treatment, the intent of treatment is primarily to limit the spread of disease to others.4-7
The problem when adults get pertussis, says Dr. Holmes, who is also an assistant professor of community and family medicine at Dartmouth Medical School, Hanover, N.H., “is that they often don’t show up complaining about this horrible paroxysmal coughing until they’re about three or four weeks into the illness, and it hasn’t gone away. You go for hours and hours feeling completely fine and wonderful, and why would you bother going to the doctor?”
Babies are most at risk, however. “They often don’t have the energy or the muscle strength, so they just stop breathing instead,” she says.
Mark Dworkin, MD, MPH, TM, the state epidemiologist and team leader for the Rapid Response Team at the Illinois Department of Public Health, is active in outbreak investigation. He wrote a compelling argument for maintaining a high index of suspicion when physicians see adolescent and adult patients who have a cough that has lasted more than two weeks.4
It has been estimated that more than one million cases of pertussis occur in the United States each year; that number has continued to grow for 20 years. From 1990 to 2001, the incidence of pertussis in adults increased by 400%. But many physicians believe that pertussis is only a pediatric illness. A survey of internists in Washington state showed that only 38% of respondents knew about the risk of vaccine fatigue, and just 36% knew that the nasopharyngeal swab is the preferred method for sample collection. Public health professionals were also concerned with the finding that too many pediatricians and nonpediatricians (43% and 41%, respectively) were not able to define a reportable case.
The first challenge that faces internists, writes Dr. Dworkin, is recognizing pertussis, which in some cases presents with mild symptoms; some adults won’t even have a cough.4 But at the other end of the disease spectrum, symptoms may be as brutal as bilateral subconjunctival hemorrhage or rib fracture due to convulsive coughing. In any case, what goes unrecognized, undiagnosed, and untreated becomes a particularly serious risk for vulnerable infants. Once pertussis is identified, positive results on polymerase chain reaction or culture can help convince skeptical colleagues who may still believe pertussis is exclusively a childhood disease—and a vintage one at that.
“What we in pediatrics champion … is for [these immunizations] to help the young child; the less disease we have out there, the better off we’re going to eventually be,” says Dr. Stucky, who projects that, within just a few years, Tdap vaccinations for adolescents and adults up to age 64 might lead to a reduction of infection in the three-month-old group.6
Measles and Mumps
From January 1 to October 7, 2006, 45 states and the District of Columbia reported 5,783 confirmed or probable mumps cases to the Centers for Disease Control and Prevention (CDC). (See Figures 2 and 3, above.)8 The Advisory Committee on Immunization Practices (ACIP) announced that continuing data from surveillance reports meant that healthcare workers should remain alert to suspected cases, conduct appropriate laboratory testing, and use every opportunity to ensure adequate immunity, particularly among populations at high risk.7
In contrast to the circumstances with pertussis, with mumps “there have been pockets of people who have either chosen not to immunize their child[ren], or their child[ren] get exposed to it somehow,” says Dr. Stucky, “and although they might be immunized, they might not have had a good response.” In an environment such as a school, “where one child can cough on a few and then cough on a few [more],” there is an environment where the infection can spread rampantly.
With mumps and measles, these could be called true outbreaks, such as the classic example that occurred in Kansas 18 years ago or the epidemic that disseminated from a college campus in Iowa in the spring of 2006, which originated from only two airline passengers on nine different flights within one week.8
College dorms and cafeterias can be treacherous breeding grounds for pathogens, and this generation of college students is susceptible for a few reasons. For one, in the late 1980s, when they were infants, the vaccine schedule was changed; the measles/mumps/rubella vaccine was upgraded from one dose to two—and not all children received the two doses.
The unimmunized who are exposed to measles and mumps remain at highest risk for spreading the disease. Although in 2005, 76%-79% of children aged 19-35 months received the entire recommended series of shots against whooping cough, diphtheria, tetanus, polio, measles, mumps, rubella, chicken pox, hepatitis B, and Haemophilus influenza type B, that still means that 21%-24% of the children—or potentially one out of five kids—did not.9
Other factors causing low levels of immunization include parents’ Internet-fueled fears of links to autism; immigrants crossing U.S. borders from Mexico or other countries where immunization is not standardized; religious and philosophical reasons; and international travel.10
“When young adults travel internationally [to places] where they are exposed to young children and adults who have never been immunized,” that’s a big risk, says Dr. Stucky. “All it would take is one [infected] student coming into a dorm and passing it around [to others with lapsed coverage or no immunization for the disease].” And while providers may think of travelers being exposed to diseases such as malaria and typhoid fever in developing countries, “in reality, a lot of the common things we’re immunizing for in our country are not immunized for in other countries, and those can be brought back.”
Rickets
The incidence of rickets is increasing, especially in black and Hispanic children and particularly in the north.11,12 Epidemiologists trace the rise to an increase in breast-feeding (good for immunity, but breast milk lacks substantial vitamin D), overuse of sunscreen or lack of exposure to sunlight, and changes in physician recommendations for vitamin supplementation. The effects of rickets alone can be profound, but other long-term consequences of vitamin D deficiency may include type I diabetes, cancer (especially of the prostate), and osteoporosis.12
In the past few decades, physicians have been less likely to recommend vitamin D supplementation for babies, and an interesting study by Davenport and colleagues correlates the year of medical school completion to that decline as well as substantial variability as to the age at which supplement use is begun.12 (See Figures 4a and 4b, left.)
“Most of the cases I have run into have been in [recent] African immigrants, where the mothers stay covered and they are vitamin D deficient,” says Dr. Holmes. “It’s wonderful that they culturally breast-feed, but they come to the U.S., and they’re pretty afraid to go outside in a new society.”
Varicella (Chicken Pox)
Varicella was removed from the CDC’s national notifiable disease list in 1981, but in 1995 a varicella vaccine was recommended for routine childhood vaccination.13 Before the licensure of that vaccine, varicella was a universal childhood disease in the U.S., causing 4 million cases, 11,000 hospitalizations, and 100 deaths every year.14 In 2002, the Council of State and Territorial Epidemiologists recommended that varicella be included in the National Notifiable Surveillance System by 2003 and that case-based surveillance in all states be established by 2005.13 CDC’s ACIP recommended in 2006 that a routine second dose of varicella vaccine be given to children between the ages of four and six years old.
Contracting chicken pox as an adult is a much more morbid occurrence than catching it as a child. Although varicella is not life threatening (as are diphtheria, tetanus, and measles) or sterility-causing (as is mumps), when the vaccine was approved, some pediatricians, including Dr. Stucky, became concerned that “now we’re creating a population that has never seen the wild-type varicella virus, and what does that mean? Were we just delaying something into an age category where people will get sicker?” Recognizing varicella, therefore, is critical even for hospitalists who treat adults.
Conclusion
“I’ve seen mumps, measles, varicella, pertussis,” says Dr. Stucky, “but our adult [hospitalist] partners hadn’t.” She encourages her colleagues who treat adult populations “to read and be diligent. These diseases can exist in adults, or even in children who were once vaccinated, and all hospitalists need to know “what to do, how to treat them, and [that] the consequences in adults are hands down worse than in children.”
Dr. Stucky believes hospitalists who treat adults would do well to consult physicians who practiced in the 1950s because they understand the history as well as clinical signs and symptoms of these diseases; she says, “For the hospitalist who treats adults, these are the equivalent of emerging infectious diseases.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Carmichael M. 'Vintage' bugs return. Newsweek. May 1, 2006:Vol. 147, p. 38. Available at: www.msnbc.msn.com/id/12440796/site/newsweek/. Accessed on November 29, 2006.
- Herwaldt LA. Pertussis in adults. What physicians need to know. Arch Intern Med. 1991;151:1510-1512.
- Schafer S, Gillette H, Hedberg K, et al. A community-wide pertussis outbreak: an argument for universal booster vaccination. Arch Intern Med. 2006 Jun 26;166(12):1317-1321.
- Dworkin MS. Adults are whooping, but are internists listening? Ann Intern Med. 2005 May 17;142(10):832-835. Available at: www.annals.org/cgi/reprint/142/10/832.pdf. Accessed on November 19, 2006.
- Gregory DS. Pertussis: a disease affecting all ages. Am Fam Physician. 2006 Aug 1;74(3):420-426.
- Finger R, Shoemaker J. Preventing pertussis in infants by vaccinating adults. Am Fam Physician. 2006 Aug 1;74(3):382.
- Broder KR, Cortese MM, Iskander JK, et al. Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55:1-34.
- MMWR. Brief report: update: mumps activity—United States, January 1-October 7, 2006. MMWR. 2006 Oct 27;55(42):1152-1153.
- National Briefing: Science and health: race gap closes in vaccinations, U.S. says. New York Times. September 15, 2006.
- Calandrillo SP. Vanishing vaccinations: why are so many Americans opting out of vaccinating their children? Univ Mich J Law Reform. 2004 Winter;37(2):353-440.
- Kreiter SR, Schwartz RP, Kirkman HN Jr, et al. Nutritional rickets in African American breast-fed infants. J Pediatr. 2000 Aug;137(2):153-157.
- Davenport ML, Uckun A, Calikoglu AS. Pediatrician patterns of prescribing vitamin supplementation for infants: do they contribute to rickets? Pediatrics. 2004 Jan;113(1 Pt 1):179-180.
- MMWR. Varicella surveillance practices—United States, 2004. MMWR. 2006 Oct 19;55:1126-1129.
- Seward JF, Watson BM, Peterson CL, et al. Varicella disease after introduction of varicella vaccine in the United States, 1995-2000. JAMA. 2002 Feb 6;287(5):606-611.
We thought they were gone, but they’ve returned: diseases once considered “vintage bugs” that were common in as late as the mid-20th century. In the past these diseases killed one in three people younger than 20 who had survived an infancy during which many of their contemporaries died.1
“When you think about disease states, you think about some that are gone from the world,” says Erin Stucky, MD, a pediatric hospitalist at the University of California, San Diego, “but there are very few truly gone from the world.”
Some of the major infectious diseases that hospitalists may [still] see are pertussis (whooping cough), measles, and mumps, but scarlet fever and varicella (chicken pox) also endure—not to mention those occurrences of polio around the country that epidemiologists and infectious diseases specialists are monitoring closely. Rickets, a vitamin-D-deficiency-related disease also thought to be a relic of the 18th century, is showing up in certain patient populations—and not exclusively in infants and children.
This is a crossover clinical issue, our pediatric hospitalists say, and thus one to which their hospitalist partners who treat adult patients must also remain alert.
Pertussis (Whooping Cough)
Despite vaccination protocols, pediatric hospitalists continue to see whooping cough in young infants. (See Figure 1, p. 39.) Even with treatment, the damage can be severe, and the length of stay (LOS) is prolonged compared with those of most other patients with complex illnesses. “Vaccine fatigue” means that immunization lasts only until adolescence or early adulthood, at which time they need appropriate boosters. If the patient hasn’t receive boosters, the initial immunization loses its effectiveness; unprotected, they can be infected with the disease, though sometimes not badly enough for them to seek care. When they do, the diagnosis is often community-acquired mild pneumonia or a more traditional bronchitis. Either by accident or because the physician has given it thought, those illnesses are treated with a macrolide drug, which is also—coincidentally and serendipitously—the drug of choice for pertussis. But many remain carriers because they are not accurately diagnosed or never seek care.
“There is a huge reservoir of people carrying pertussis, particularly [in] the adolescent and adult population[s],” says Alison Holmes, MD, a pediatric hospitalist at Concord Hospital, N.H. “And the babies who get really sick from it are the under two- to three-month group who have not yet been immunized or have just been immunized. Because it is so rampant in the adolescent and adult community, those children can still get sick.”
“Unfortunately,” says Dr. Stucky, “what’s happening is that if physicians are not thinking pertussis, they don’t talk about pertussis to that adult patient who … is either around children or has children in the home. So they don’t know to tell that person to watch for these same signs and symptoms in that young infant, who then could have a much more severe outcome from getting [the infection].”
As with most patients who contract illnesses, these patients may never have heard of the disease and unless educated may not understand the implications of the diagnosis. They might realize their disease could spread to family members, “but most people don’t absorb that information and use that information thoughtfully,” says Dr. Stucky. The onus is, therefore, on the physician to warn adult patients specifically about the serious danger that exists for infants in the two- to three-month-old group, who may not have been vaccinated or whose single-vaccination immunity is not adequate protection against the disease.
While the numbers in babies appear to be what they have always been, the incidence has grown in the teen years and even later into adulthood. This is more likely the result of increased testing for pertussis, as opposed to being only due to a true resurgence. Data from studies of adults with prolonged cough revealed that 20% to 25% have serologic evidence of recent pertussis infection.2 Adults are the major reservoir of infection, and infection spreads quickly in a population in a closed environment where droplets spread easily person to person.5
For both teens and adults, testing and immunization with the newly recommended DTaP (diphtheria-tetanus-pertussis)—as opposed to the more limited Td—can help upgrade immunity. Although a patient can recover from pertussis on his or her own within one to two weeks following treatment, the intent of treatment is primarily to limit the spread of disease to others.4-7
The problem when adults get pertussis, says Dr. Holmes, who is also an assistant professor of community and family medicine at Dartmouth Medical School, Hanover, N.H., “is that they often don’t show up complaining about this horrible paroxysmal coughing until they’re about three or four weeks into the illness, and it hasn’t gone away. You go for hours and hours feeling completely fine and wonderful, and why would you bother going to the doctor?”
Babies are most at risk, however. “They often don’t have the energy or the muscle strength, so they just stop breathing instead,” she says.
Mark Dworkin, MD, MPH, TM, the state epidemiologist and team leader for the Rapid Response Team at the Illinois Department of Public Health, is active in outbreak investigation. He wrote a compelling argument for maintaining a high index of suspicion when physicians see adolescent and adult patients who have a cough that has lasted more than two weeks.4
It has been estimated that more than one million cases of pertussis occur in the United States each year; that number has continued to grow for 20 years. From 1990 to 2001, the incidence of pertussis in adults increased by 400%. But many physicians believe that pertussis is only a pediatric illness. A survey of internists in Washington state showed that only 38% of respondents knew about the risk of vaccine fatigue, and just 36% knew that the nasopharyngeal swab is the preferred method for sample collection. Public health professionals were also concerned with the finding that too many pediatricians and nonpediatricians (43% and 41%, respectively) were not able to define a reportable case.
The first challenge that faces internists, writes Dr. Dworkin, is recognizing pertussis, which in some cases presents with mild symptoms; some adults won’t even have a cough.4 But at the other end of the disease spectrum, symptoms may be as brutal as bilateral subconjunctival hemorrhage or rib fracture due to convulsive coughing. In any case, what goes unrecognized, undiagnosed, and untreated becomes a particularly serious risk for vulnerable infants. Once pertussis is identified, positive results on polymerase chain reaction or culture can help convince skeptical colleagues who may still believe pertussis is exclusively a childhood disease—and a vintage one at that.
“What we in pediatrics champion … is for [these immunizations] to help the young child; the less disease we have out there, the better off we’re going to eventually be,” says Dr. Stucky, who projects that, within just a few years, Tdap vaccinations for adolescents and adults up to age 64 might lead to a reduction of infection in the three-month-old group.6
Measles and Mumps
From January 1 to October 7, 2006, 45 states and the District of Columbia reported 5,783 confirmed or probable mumps cases to the Centers for Disease Control and Prevention (CDC). (See Figures 2 and 3, above.)8 The Advisory Committee on Immunization Practices (ACIP) announced that continuing data from surveillance reports meant that healthcare workers should remain alert to suspected cases, conduct appropriate laboratory testing, and use every opportunity to ensure adequate immunity, particularly among populations at high risk.7
In contrast to the circumstances with pertussis, with mumps “there have been pockets of people who have either chosen not to immunize their child[ren], or their child[ren] get exposed to it somehow,” says Dr. Stucky, “and although they might be immunized, they might not have had a good response.” In an environment such as a school, “where one child can cough on a few and then cough on a few [more],” there is an environment where the infection can spread rampantly.
With mumps and measles, these could be called true outbreaks, such as the classic example that occurred in Kansas 18 years ago or the epidemic that disseminated from a college campus in Iowa in the spring of 2006, which originated from only two airline passengers on nine different flights within one week.8
College dorms and cafeterias can be treacherous breeding grounds for pathogens, and this generation of college students is susceptible for a few reasons. For one, in the late 1980s, when they were infants, the vaccine schedule was changed; the measles/mumps/rubella vaccine was upgraded from one dose to two—and not all children received the two doses.
The unimmunized who are exposed to measles and mumps remain at highest risk for spreading the disease. Although in 2005, 76%-79% of children aged 19-35 months received the entire recommended series of shots against whooping cough, diphtheria, tetanus, polio, measles, mumps, rubella, chicken pox, hepatitis B, and Haemophilus influenza type B, that still means that 21%-24% of the children—or potentially one out of five kids—did not.9
Other factors causing low levels of immunization include parents’ Internet-fueled fears of links to autism; immigrants crossing U.S. borders from Mexico or other countries where immunization is not standardized; religious and philosophical reasons; and international travel.10
“When young adults travel internationally [to places] where they are exposed to young children and adults who have never been immunized,” that’s a big risk, says Dr. Stucky. “All it would take is one [infected] student coming into a dorm and passing it around [to others with lapsed coverage or no immunization for the disease].” And while providers may think of travelers being exposed to diseases such as malaria and typhoid fever in developing countries, “in reality, a lot of the common things we’re immunizing for in our country are not immunized for in other countries, and those can be brought back.”
Rickets
The incidence of rickets is increasing, especially in black and Hispanic children and particularly in the north.11,12 Epidemiologists trace the rise to an increase in breast-feeding (good for immunity, but breast milk lacks substantial vitamin D), overuse of sunscreen or lack of exposure to sunlight, and changes in physician recommendations for vitamin supplementation. The effects of rickets alone can be profound, but other long-term consequences of vitamin D deficiency may include type I diabetes, cancer (especially of the prostate), and osteoporosis.12
In the past few decades, physicians have been less likely to recommend vitamin D supplementation for babies, and an interesting study by Davenport and colleagues correlates the year of medical school completion to that decline as well as substantial variability as to the age at which supplement use is begun.12 (See Figures 4a and 4b, left.)
“Most of the cases I have run into have been in [recent] African immigrants, where the mothers stay covered and they are vitamin D deficient,” says Dr. Holmes. “It’s wonderful that they culturally breast-feed, but they come to the U.S., and they’re pretty afraid to go outside in a new society.”
Varicella (Chicken Pox)
Varicella was removed from the CDC’s national notifiable disease list in 1981, but in 1995 a varicella vaccine was recommended for routine childhood vaccination.13 Before the licensure of that vaccine, varicella was a universal childhood disease in the U.S., causing 4 million cases, 11,000 hospitalizations, and 100 deaths every year.14 In 2002, the Council of State and Territorial Epidemiologists recommended that varicella be included in the National Notifiable Surveillance System by 2003 and that case-based surveillance in all states be established by 2005.13 CDC’s ACIP recommended in 2006 that a routine second dose of varicella vaccine be given to children between the ages of four and six years old.
Contracting chicken pox as an adult is a much more morbid occurrence than catching it as a child. Although varicella is not life threatening (as are diphtheria, tetanus, and measles) or sterility-causing (as is mumps), when the vaccine was approved, some pediatricians, including Dr. Stucky, became concerned that “now we’re creating a population that has never seen the wild-type varicella virus, and what does that mean? Were we just delaying something into an age category where people will get sicker?” Recognizing varicella, therefore, is critical even for hospitalists who treat adults.
Conclusion
“I’ve seen mumps, measles, varicella, pertussis,” says Dr. Stucky, “but our adult [hospitalist] partners hadn’t.” She encourages her colleagues who treat adult populations “to read and be diligent. These diseases can exist in adults, or even in children who were once vaccinated, and all hospitalists need to know “what to do, how to treat them, and [that] the consequences in adults are hands down worse than in children.”
Dr. Stucky believes hospitalists who treat adults would do well to consult physicians who practiced in the 1950s because they understand the history as well as clinical signs and symptoms of these diseases; she says, “For the hospitalist who treats adults, these are the equivalent of emerging infectious diseases.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Carmichael M. 'Vintage' bugs return. Newsweek. May 1, 2006:Vol. 147, p. 38. Available at: www.msnbc.msn.com/id/12440796/site/newsweek/. Accessed on November 29, 2006.
- Herwaldt LA. Pertussis in adults. What physicians need to know. Arch Intern Med. 1991;151:1510-1512.
- Schafer S, Gillette H, Hedberg K, et al. A community-wide pertussis outbreak: an argument for universal booster vaccination. Arch Intern Med. 2006 Jun 26;166(12):1317-1321.
- Dworkin MS. Adults are whooping, but are internists listening? Ann Intern Med. 2005 May 17;142(10):832-835. Available at: www.annals.org/cgi/reprint/142/10/832.pdf. Accessed on November 19, 2006.
- Gregory DS. Pertussis: a disease affecting all ages. Am Fam Physician. 2006 Aug 1;74(3):420-426.
- Finger R, Shoemaker J. Preventing pertussis in infants by vaccinating adults. Am Fam Physician. 2006 Aug 1;74(3):382.
- Broder KR, Cortese MM, Iskander JK, et al. Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55:1-34.
- MMWR. Brief report: update: mumps activity—United States, January 1-October 7, 2006. MMWR. 2006 Oct 27;55(42):1152-1153.
- National Briefing: Science and health: race gap closes in vaccinations, U.S. says. New York Times. September 15, 2006.
- Calandrillo SP. Vanishing vaccinations: why are so many Americans opting out of vaccinating their children? Univ Mich J Law Reform. 2004 Winter;37(2):353-440.
- Kreiter SR, Schwartz RP, Kirkman HN Jr, et al. Nutritional rickets in African American breast-fed infants. J Pediatr. 2000 Aug;137(2):153-157.
- Davenport ML, Uckun A, Calikoglu AS. Pediatrician patterns of prescribing vitamin supplementation for infants: do they contribute to rickets? Pediatrics. 2004 Jan;113(1 Pt 1):179-180.
- MMWR. Varicella surveillance practices—United States, 2004. MMWR. 2006 Oct 19;55:1126-1129.
- Seward JF, Watson BM, Peterson CL, et al. Varicella disease after introduction of varicella vaccine in the United States, 1995-2000. JAMA. 2002 Feb 6;287(5):606-611.
We thought they were gone, but they’ve returned: diseases once considered “vintage bugs” that were common in as late as the mid-20th century. In the past these diseases killed one in three people younger than 20 who had survived an infancy during which many of their contemporaries died.1
“When you think about disease states, you think about some that are gone from the world,” says Erin Stucky, MD, a pediatric hospitalist at the University of California, San Diego, “but there are very few truly gone from the world.”
Some of the major infectious diseases that hospitalists may [still] see are pertussis (whooping cough), measles, and mumps, but scarlet fever and varicella (chicken pox) also endure—not to mention those occurrences of polio around the country that epidemiologists and infectious diseases specialists are monitoring closely. Rickets, a vitamin-D-deficiency-related disease also thought to be a relic of the 18th century, is showing up in certain patient populations—and not exclusively in infants and children.
This is a crossover clinical issue, our pediatric hospitalists say, and thus one to which their hospitalist partners who treat adult patients must also remain alert.
Pertussis (Whooping Cough)
Despite vaccination protocols, pediatric hospitalists continue to see whooping cough in young infants. (See Figure 1, p. 39.) Even with treatment, the damage can be severe, and the length of stay (LOS) is prolonged compared with those of most other patients with complex illnesses. “Vaccine fatigue” means that immunization lasts only until adolescence or early adulthood, at which time they need appropriate boosters. If the patient hasn’t receive boosters, the initial immunization loses its effectiveness; unprotected, they can be infected with the disease, though sometimes not badly enough for them to seek care. When they do, the diagnosis is often community-acquired mild pneumonia or a more traditional bronchitis. Either by accident or because the physician has given it thought, those illnesses are treated with a macrolide drug, which is also—coincidentally and serendipitously—the drug of choice for pertussis. But many remain carriers because they are not accurately diagnosed or never seek care.
“There is a huge reservoir of people carrying pertussis, particularly [in] the adolescent and adult population[s],” says Alison Holmes, MD, a pediatric hospitalist at Concord Hospital, N.H. “And the babies who get really sick from it are the under two- to three-month group who have not yet been immunized or have just been immunized. Because it is so rampant in the adolescent and adult community, those children can still get sick.”
“Unfortunately,” says Dr. Stucky, “what’s happening is that if physicians are not thinking pertussis, they don’t talk about pertussis to that adult patient who … is either around children or has children in the home. So they don’t know to tell that person to watch for these same signs and symptoms in that young infant, who then could have a much more severe outcome from getting [the infection].”
As with most patients who contract illnesses, these patients may never have heard of the disease and unless educated may not understand the implications of the diagnosis. They might realize their disease could spread to family members, “but most people don’t absorb that information and use that information thoughtfully,” says Dr. Stucky. The onus is, therefore, on the physician to warn adult patients specifically about the serious danger that exists for infants in the two- to three-month-old group, who may not have been vaccinated or whose single-vaccination immunity is not adequate protection against the disease.
While the numbers in babies appear to be what they have always been, the incidence has grown in the teen years and even later into adulthood. This is more likely the result of increased testing for pertussis, as opposed to being only due to a true resurgence. Data from studies of adults with prolonged cough revealed that 20% to 25% have serologic evidence of recent pertussis infection.2 Adults are the major reservoir of infection, and infection spreads quickly in a population in a closed environment where droplets spread easily person to person.5
For both teens and adults, testing and immunization with the newly recommended DTaP (diphtheria-tetanus-pertussis)—as opposed to the more limited Td—can help upgrade immunity. Although a patient can recover from pertussis on his or her own within one to two weeks following treatment, the intent of treatment is primarily to limit the spread of disease to others.4-7
The problem when adults get pertussis, says Dr. Holmes, who is also an assistant professor of community and family medicine at Dartmouth Medical School, Hanover, N.H., “is that they often don’t show up complaining about this horrible paroxysmal coughing until they’re about three or four weeks into the illness, and it hasn’t gone away. You go for hours and hours feeling completely fine and wonderful, and why would you bother going to the doctor?”
Babies are most at risk, however. “They often don’t have the energy or the muscle strength, so they just stop breathing instead,” she says.
Mark Dworkin, MD, MPH, TM, the state epidemiologist and team leader for the Rapid Response Team at the Illinois Department of Public Health, is active in outbreak investigation. He wrote a compelling argument for maintaining a high index of suspicion when physicians see adolescent and adult patients who have a cough that has lasted more than two weeks.4
It has been estimated that more than one million cases of pertussis occur in the United States each year; that number has continued to grow for 20 years. From 1990 to 2001, the incidence of pertussis in adults increased by 400%. But many physicians believe that pertussis is only a pediatric illness. A survey of internists in Washington state showed that only 38% of respondents knew about the risk of vaccine fatigue, and just 36% knew that the nasopharyngeal swab is the preferred method for sample collection. Public health professionals were also concerned with the finding that too many pediatricians and nonpediatricians (43% and 41%, respectively) were not able to define a reportable case.
The first challenge that faces internists, writes Dr. Dworkin, is recognizing pertussis, which in some cases presents with mild symptoms; some adults won’t even have a cough.4 But at the other end of the disease spectrum, symptoms may be as brutal as bilateral subconjunctival hemorrhage or rib fracture due to convulsive coughing. In any case, what goes unrecognized, undiagnosed, and untreated becomes a particularly serious risk for vulnerable infants. Once pertussis is identified, positive results on polymerase chain reaction or culture can help convince skeptical colleagues who may still believe pertussis is exclusively a childhood disease—and a vintage one at that.
“What we in pediatrics champion … is for [these immunizations] to help the young child; the less disease we have out there, the better off we’re going to eventually be,” says Dr. Stucky, who projects that, within just a few years, Tdap vaccinations for adolescents and adults up to age 64 might lead to a reduction of infection in the three-month-old group.6
Measles and Mumps
From January 1 to October 7, 2006, 45 states and the District of Columbia reported 5,783 confirmed or probable mumps cases to the Centers for Disease Control and Prevention (CDC). (See Figures 2 and 3, above.)8 The Advisory Committee on Immunization Practices (ACIP) announced that continuing data from surveillance reports meant that healthcare workers should remain alert to suspected cases, conduct appropriate laboratory testing, and use every opportunity to ensure adequate immunity, particularly among populations at high risk.7
In contrast to the circumstances with pertussis, with mumps “there have been pockets of people who have either chosen not to immunize their child[ren], or their child[ren] get exposed to it somehow,” says Dr. Stucky, “and although they might be immunized, they might not have had a good response.” In an environment such as a school, “where one child can cough on a few and then cough on a few [more],” there is an environment where the infection can spread rampantly.
With mumps and measles, these could be called true outbreaks, such as the classic example that occurred in Kansas 18 years ago or the epidemic that disseminated from a college campus in Iowa in the spring of 2006, which originated from only two airline passengers on nine different flights within one week.8
College dorms and cafeterias can be treacherous breeding grounds for pathogens, and this generation of college students is susceptible for a few reasons. For one, in the late 1980s, when they were infants, the vaccine schedule was changed; the measles/mumps/rubella vaccine was upgraded from one dose to two—and not all children received the two doses.
The unimmunized who are exposed to measles and mumps remain at highest risk for spreading the disease. Although in 2005, 76%-79% of children aged 19-35 months received the entire recommended series of shots against whooping cough, diphtheria, tetanus, polio, measles, mumps, rubella, chicken pox, hepatitis B, and Haemophilus influenza type B, that still means that 21%-24% of the children—or potentially one out of five kids—did not.9
Other factors causing low levels of immunization include parents’ Internet-fueled fears of links to autism; immigrants crossing U.S. borders from Mexico or other countries where immunization is not standardized; religious and philosophical reasons; and international travel.10
“When young adults travel internationally [to places] where they are exposed to young children and adults who have never been immunized,” that’s a big risk, says Dr. Stucky. “All it would take is one [infected] student coming into a dorm and passing it around [to others with lapsed coverage or no immunization for the disease].” And while providers may think of travelers being exposed to diseases such as malaria and typhoid fever in developing countries, “in reality, a lot of the common things we’re immunizing for in our country are not immunized for in other countries, and those can be brought back.”
Rickets
The incidence of rickets is increasing, especially in black and Hispanic children and particularly in the north.11,12 Epidemiologists trace the rise to an increase in breast-feeding (good for immunity, but breast milk lacks substantial vitamin D), overuse of sunscreen or lack of exposure to sunlight, and changes in physician recommendations for vitamin supplementation. The effects of rickets alone can be profound, but other long-term consequences of vitamin D deficiency may include type I diabetes, cancer (especially of the prostate), and osteoporosis.12
In the past few decades, physicians have been less likely to recommend vitamin D supplementation for babies, and an interesting study by Davenport and colleagues correlates the year of medical school completion to that decline as well as substantial variability as to the age at which supplement use is begun.12 (See Figures 4a and 4b, left.)
“Most of the cases I have run into have been in [recent] African immigrants, where the mothers stay covered and they are vitamin D deficient,” says Dr. Holmes. “It’s wonderful that they culturally breast-feed, but they come to the U.S., and they’re pretty afraid to go outside in a new society.”
Varicella (Chicken Pox)
Varicella was removed from the CDC’s national notifiable disease list in 1981, but in 1995 a varicella vaccine was recommended for routine childhood vaccination.13 Before the licensure of that vaccine, varicella was a universal childhood disease in the U.S., causing 4 million cases, 11,000 hospitalizations, and 100 deaths every year.14 In 2002, the Council of State and Territorial Epidemiologists recommended that varicella be included in the National Notifiable Surveillance System by 2003 and that case-based surveillance in all states be established by 2005.13 CDC’s ACIP recommended in 2006 that a routine second dose of varicella vaccine be given to children between the ages of four and six years old.
Contracting chicken pox as an adult is a much more morbid occurrence than catching it as a child. Although varicella is not life threatening (as are diphtheria, tetanus, and measles) or sterility-causing (as is mumps), when the vaccine was approved, some pediatricians, including Dr. Stucky, became concerned that “now we’re creating a population that has never seen the wild-type varicella virus, and what does that mean? Were we just delaying something into an age category where people will get sicker?” Recognizing varicella, therefore, is critical even for hospitalists who treat adults.
Conclusion
“I’ve seen mumps, measles, varicella, pertussis,” says Dr. Stucky, “but our adult [hospitalist] partners hadn’t.” She encourages her colleagues who treat adult populations “to read and be diligent. These diseases can exist in adults, or even in children who were once vaccinated, and all hospitalists need to know “what to do, how to treat them, and [that] the consequences in adults are hands down worse than in children.”
Dr. Stucky believes hospitalists who treat adults would do well to consult physicians who practiced in the 1950s because they understand the history as well as clinical signs and symptoms of these diseases; she says, “For the hospitalist who treats adults, these are the equivalent of emerging infectious diseases.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Carmichael M. 'Vintage' bugs return. Newsweek. May 1, 2006:Vol. 147, p. 38. Available at: www.msnbc.msn.com/id/12440796/site/newsweek/. Accessed on November 29, 2006.
- Herwaldt LA. Pertussis in adults. What physicians need to know. Arch Intern Med. 1991;151:1510-1512.
- Schafer S, Gillette H, Hedberg K, et al. A community-wide pertussis outbreak: an argument for universal booster vaccination. Arch Intern Med. 2006 Jun 26;166(12):1317-1321.
- Dworkin MS. Adults are whooping, but are internists listening? Ann Intern Med. 2005 May 17;142(10):832-835. Available at: www.annals.org/cgi/reprint/142/10/832.pdf. Accessed on November 19, 2006.
- Gregory DS. Pertussis: a disease affecting all ages. Am Fam Physician. 2006 Aug 1;74(3):420-426.
- Finger R, Shoemaker J. Preventing pertussis in infants by vaccinating adults. Am Fam Physician. 2006 Aug 1;74(3):382.
- Broder KR, Cortese MM, Iskander JK, et al. Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2006;55:1-34.
- MMWR. Brief report: update: mumps activity—United States, January 1-October 7, 2006. MMWR. 2006 Oct 27;55(42):1152-1153.
- National Briefing: Science and health: race gap closes in vaccinations, U.S. says. New York Times. September 15, 2006.
- Calandrillo SP. Vanishing vaccinations: why are so many Americans opting out of vaccinating their children? Univ Mich J Law Reform. 2004 Winter;37(2):353-440.
- Kreiter SR, Schwartz RP, Kirkman HN Jr, et al. Nutritional rickets in African American breast-fed infants. J Pediatr. 2000 Aug;137(2):153-157.
- Davenport ML, Uckun A, Calikoglu AS. Pediatrician patterns of prescribing vitamin supplementation for infants: do they contribute to rickets? Pediatrics. 2004 Jan;113(1 Pt 1):179-180.
- MMWR. Varicella surveillance practices—United States, 2004. MMWR. 2006 Oct 19;55:1126-1129.
- Seward JF, Watson BM, Peterson CL, et al. Varicella disease after introduction of varicella vaccine in the United States, 1995-2000. JAMA. 2002 Feb 6;287(5):606-611.
Report Card Reservations
When Rajeev Alexander, MD, lead hospitalist at Oregon Medical Group with PeaceHealth of Eugene, Ore., sought out an ophthalmologist, he didn’t go to provider Web sites or directory pages. He did what most healthcare patients do: He asked around.
Some of the nurses at work gave him suggestions. “‘This guy does a lot of LASIK and might push it.’ Or, ‘This guy has good relationships with patients.’ Or, ‘This is the guy I’d send my husband to,’” Dr. Alexander explains. “That helped.”
Were he to recommend a hospital, Dr. Alexander says he would base his selection on one major criterion: the collegiality of the facility’s doctors, pharmacists, and nurses. “If all the specialists in the hospital are talking to each other, and if they feel they can trust each other,” he says, “then I think you’re going to get good care.”
Dr. Alexander never mentions checking the performance of the physician or hospital he may use. It seems he’s not alone. In recent years, some famous cases have brought attention to how infrequently patients actually consult the available quality data when selecting a provider.
It’s unlikely, for example, that Sen. Ted Kennedy (D-Mass.) researched provider collegiality as a quality measure when he chose a neurosurgeon at Duke University Medical Center to remove his malignant glioma. In 2004, when President Clinton needed his quadruple coronary bypass operation, he used an average-rated New York cardiologist. Why? Because, according to Dr. Jha, he didn’t compare quality reports.
Physicians are just as guilty of ignoring the information. Audience feedback at a hospital medicine continuing medical education course demonstrated to Robert M. Wachter, MD, chief of the division of hospital medicine and chief of the medical service at the University of California San Francisco Medical Center, that even members of UCSF’s Epidemiology and Biostatistics Department do not consult quality data before making medical decisions for themselves or a loved one. “Patients won’t start using quality data until we do it ourselves,” Dr. Wachter writes in his blog, Wachter’s World (www.wachtersworld.com). “Best guess: three to five years.”
So how much progress have we really made in using publicly reported data to pick individual providers and hospitals? What should be measured in the future as it affects hospitalist practice? How can hospitalists influence the types of data collected?
Along the Continuum
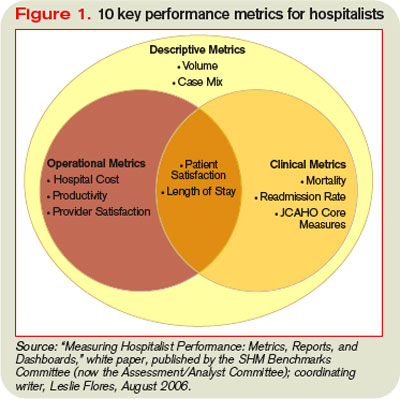
The problem isn’t because people don’t know about the data. More than one-quarter (26%) of consumers who participated in a 2002 Harris poll said they are aware of hospital report cards, Dr. Wachter writes in his book Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. However, only 3% considered changing their care based on those ratings, and only 1% actually made a change.1
Those who do consult the data seem to benefit—at least that is the case for users of New York state’s public reporting system for coronary artery bypass surgery. Dr. Jha and Arnold Epstein, MD, professor and chair of the department of Health Policy and Management at Harvard’s School of Public Health, found users who picked a top-performing hospital or surgeon had approximately half the mortality risk as did those who selected from the bottom quartile.2
But it is unusual for patients to choose a hospital based on publicly reported information alone, and Dr. Jha believes it’s largely due to mindset. “People are not used to approaching healthcare the way they would walk into a car dealership, for instance, ready to do battle,” he says.
Even if physicians and patients don’t consistently use the data, publishing it still has value. It helps physicians gauge their professional status, for example. “If someone is not looking good,” Dr. Jha says, “it is a huge impetus to improve, as long as you believe that what you are measuring is really associated with quality.”
Those who don’t believe it may have trouble, and sooner than they think. With 70 million beneficiaries, the Centers for Medicare and Medicaid Services (CMS) sets the tone for healthcare quality in the U.S. In fact, Medicare beneficiaries comprise about one-third of those in a typical hospitalist’s practice. Since March 2008, the CMS Web site www.hospitalcompare.hhs.gov/ has reported hospital service data and soon will post cost comparisons.
“CMS is a payer we have to pay attention to (them),” says Patrick Torcson, MD, chair of SHM’s Performance and Standards Committee. “The CMS performance and quality agenda is specified at the statutory level as part of the Congressional record, and is very political. Therefore, that agenda right now is part scientific, part policy, and part methodology. There is a little something in it for everybody.”
Increasingly, quality measures are gradually, and insidiously, changing healthcare. For instance, Dr. Jha’s study found outcomes data did not greatly influence hospital market share, however, the surgeons with the highest publicly reported mortality rates were much more likely to retire after the release of each report card.2
Obstacles to Utilization
If these data can help us make educated healthcare decisions, why aren’t more people consulting them? To start, current measures aren’t sufficient, says Peter K. Lindenauer, MD, MSc, FACP, a hospitalist and associate professor of medicine at Baystate Medical Center in Springfield, Mass.
“The number of measures and the strength of the evidence that current process measures are based on are still quite limited,” Dr. Lindenauer says. “Moreover, it is unclear how much the structural and process measures that have remained the focus of most public reporting contribute to patient outcomes.” It’s difficult to make statistically meaningful comparisons across hospitals or providers. Those efforts are “hampered by inadequate risk adjustment and tend to be underpowered to detect statistically significant differences.”
Another problem facing public reporting comparison initiatives is differences in healthcare utilization and spending across U.S. regions with similar levels of patient illness, says Stephanie Jackson, MD, a hospitalist with PeaceHealth and a member of SHM’s Public Policy Committee.3 The public cannot look at data it doesn’t have. For example, when Dr. Jackson asked researchers for data on coronary stroke rates, she was informed some physicians asked the data be held back because they didn’t like what it showed. “Why aren’t we demanding [that data]?” Dr. Jackson asks.
Essentially, then, quality data utilization is an evolving story. ”An ongoing debate exists between proponents of public reporting who believe that the best way to improve measures is to start using them,” Dr. Lindenauer says, “and those who advocate a more cautious approach and argue we should not rush to publicize data until we are clear about what the numbers signify and what to measure.”
Some hospitals use more than 10 criteria as the benchmark for core measures, and 10 additional dimensions hospitalists use to assess their own internal performance (see Figure 1, pg. 41). Beyond that, metrics vary from hospital to hospital.
What Hospitalists Can Do
“It is very challenging to find doctors who are well-versed in public reporting of quality data,” says Latha Sivaprasad, MD, medical director, quality management and patient safety at Beth Israel Medical Center in New York City. Dr. Jackson believes the more hospitalists know about quality data, the more they will want to use it. “Even though some hospitalists may be afraid to find out how they are doing,” she says, “in general, the better we get at measuring individual performance, the more hospitalists can examine their performance and how they can improve as individuals, as a group, and as an institution.”
Additionally, the era of value-based purchasing (pay for performance) is here—in the form of CMS’ Physician Quality Reporting Initiative. For the past year, physicians have reported on specific performance measures tied to a 1.5% bonus payout. Of the program’s 74 measures in 2007 and 119 measures in 2008, 11 have reporting specifications applicable to hospitalists.
“Three to 5% of the DRG [diagnosis-related group] reimbursement could be at stake for hospitals to achieve certain benchmarks,” Dr. Torcson says. “This will be a great opportunity for hospitalists to partner with their hospitals to develop synergy in achieving performance goals that are going to help maximize hospital quality initiatives and reimbursement.”
Hospitalists can get more involved with quality measures by:
- Joining the hospital quality improvement or patient safety teams;
- Creating toolkits to educate physicians in using quality data;
- Setting up unit-sponsored interdisciplinary teams on the floors to marry all lines of care; and
- Educating the public.
“The conventional wisdom is that the more procedures that an institution does, the better their performance,” Dr. Alexander says, giving as an example a specialized cardiac hospital. “But you really want your surgery in a hospital where they manage at least a moderately high number of procedures and have a very high” success rate treating complications.
Dr. Sivaprasad believes the public wants guidance on medical care quality, legal ramifications of care, physician-specific volume, and the significance of physician hospital privileges. “Maybe we should be more public about system outcomes changes that resulted from root-cause analyses performed,” she adds.
Whatever the level, hospitalists should get involved, Dr. Vidyarthi says. “Quality improvement is an area where you as hospitalists may be asked to engage—and you’re needed.” TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
References
1. Wachter R, Shojania K. Internal Bleeding: The Truth Behind America's Terrifying Epidemic of Medical Mistakes. New York. Rugged Land. 2004.
2. Jha AK, Epstein AM. The predictive accuracy of the New York state coronary artery bypass surgery report-card system. Health Aff. 2006;25(3):844-855.
3. Sirovich BE, Gottlieb DJ, Welch HG, Fisher ES. Regional variations in healthcare intensity and physician perceptions of quality of care. Ann Intern Med 2006;144(9):641-649.
When Rajeev Alexander, MD, lead hospitalist at Oregon Medical Group with PeaceHealth of Eugene, Ore., sought out an ophthalmologist, he didn’t go to provider Web sites or directory pages. He did what most healthcare patients do: He asked around.
Some of the nurses at work gave him suggestions. “‘This guy does a lot of LASIK and might push it.’ Or, ‘This guy has good relationships with patients.’ Or, ‘This is the guy I’d send my husband to,’” Dr. Alexander explains. “That helped.”
Were he to recommend a hospital, Dr. Alexander says he would base his selection on one major criterion: the collegiality of the facility’s doctors, pharmacists, and nurses. “If all the specialists in the hospital are talking to each other, and if they feel they can trust each other,” he says, “then I think you’re going to get good care.”
Dr. Alexander never mentions checking the performance of the physician or hospital he may use. It seems he’s not alone. In recent years, some famous cases have brought attention to how infrequently patients actually consult the available quality data when selecting a provider.
It’s unlikely, for example, that Sen. Ted Kennedy (D-Mass.) researched provider collegiality as a quality measure when he chose a neurosurgeon at Duke University Medical Center to remove his malignant glioma. In 2004, when President Clinton needed his quadruple coronary bypass operation, he used an average-rated New York cardiologist. Why? Because, according to Dr. Jha, he didn’t compare quality reports.
Physicians are just as guilty of ignoring the information. Audience feedback at a hospital medicine continuing medical education course demonstrated to Robert M. Wachter, MD, chief of the division of hospital medicine and chief of the medical service at the University of California San Francisco Medical Center, that even members of UCSF’s Epidemiology and Biostatistics Department do not consult quality data before making medical decisions for themselves or a loved one. “Patients won’t start using quality data until we do it ourselves,” Dr. Wachter writes in his blog, Wachter’s World (www.wachtersworld.com). “Best guess: three to five years.”
So how much progress have we really made in using publicly reported data to pick individual providers and hospitals? What should be measured in the future as it affects hospitalist practice? How can hospitalists influence the types of data collected?
Along the Continuum
The problem isn’t because people don’t know about the data. More than one-quarter (26%) of consumers who participated in a 2002 Harris poll said they are aware of hospital report cards, Dr. Wachter writes in his book Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. However, only 3% considered changing their care based on those ratings, and only 1% actually made a change.1
Those who do consult the data seem to benefit—at least that is the case for users of New York state’s public reporting system for coronary artery bypass surgery. Dr. Jha and Arnold Epstein, MD, professor and chair of the department of Health Policy and Management at Harvard’s School of Public Health, found users who picked a top-performing hospital or surgeon had approximately half the mortality risk as did those who selected from the bottom quartile.2
But it is unusual for patients to choose a hospital based on publicly reported information alone, and Dr. Jha believes it’s largely due to mindset. “People are not used to approaching healthcare the way they would walk into a car dealership, for instance, ready to do battle,” he says.
Even if physicians and patients don’t consistently use the data, publishing it still has value. It helps physicians gauge their professional status, for example. “If someone is not looking good,” Dr. Jha says, “it is a huge impetus to improve, as long as you believe that what you are measuring is really associated with quality.”
Those who don’t believe it may have trouble, and sooner than they think. With 70 million beneficiaries, the Centers for Medicare and Medicaid Services (CMS) sets the tone for healthcare quality in the U.S. In fact, Medicare beneficiaries comprise about one-third of those in a typical hospitalist’s practice. Since March 2008, the CMS Web site www.hospitalcompare.hhs.gov/ has reported hospital service data and soon will post cost comparisons.
“CMS is a payer we have to pay attention to (them),” says Patrick Torcson, MD, chair of SHM’s Performance and Standards Committee. “The CMS performance and quality agenda is specified at the statutory level as part of the Congressional record, and is very political. Therefore, that agenda right now is part scientific, part policy, and part methodology. There is a little something in it for everybody.”
Increasingly, quality measures are gradually, and insidiously, changing healthcare. For instance, Dr. Jha’s study found outcomes data did not greatly influence hospital market share, however, the surgeons with the highest publicly reported mortality rates were much more likely to retire after the release of each report card.2
Obstacles to Utilization
If these data can help us make educated healthcare decisions, why aren’t more people consulting them? To start, current measures aren’t sufficient, says Peter K. Lindenauer, MD, MSc, FACP, a hospitalist and associate professor of medicine at Baystate Medical Center in Springfield, Mass.
“The number of measures and the strength of the evidence that current process measures are based on are still quite limited,” Dr. Lindenauer says. “Moreover, it is unclear how much the structural and process measures that have remained the focus of most public reporting contribute to patient outcomes.” It’s difficult to make statistically meaningful comparisons across hospitals or providers. Those efforts are “hampered by inadequate risk adjustment and tend to be underpowered to detect statistically significant differences.”
Another problem facing public reporting comparison initiatives is differences in healthcare utilization and spending across U.S. regions with similar levels of patient illness, says Stephanie Jackson, MD, a hospitalist with PeaceHealth and a member of SHM’s Public Policy Committee.3 The public cannot look at data it doesn’t have. For example, when Dr. Jackson asked researchers for data on coronary stroke rates, she was informed some physicians asked the data be held back because they didn’t like what it showed. “Why aren’t we demanding [that data]?” Dr. Jackson asks.
Essentially, then, quality data utilization is an evolving story. ”An ongoing debate exists between proponents of public reporting who believe that the best way to improve measures is to start using them,” Dr. Lindenauer says, “and those who advocate a more cautious approach and argue we should not rush to publicize data until we are clear about what the numbers signify and what to measure.”
Some hospitals use more than 10 criteria as the benchmark for core measures, and 10 additional dimensions hospitalists use to assess their own internal performance (see Figure 1, pg. 41). Beyond that, metrics vary from hospital to hospital.
What Hospitalists Can Do
“It is very challenging to find doctors who are well-versed in public reporting of quality data,” says Latha Sivaprasad, MD, medical director, quality management and patient safety at Beth Israel Medical Center in New York City. Dr. Jackson believes the more hospitalists know about quality data, the more they will want to use it. “Even though some hospitalists may be afraid to find out how they are doing,” she says, “in general, the better we get at measuring individual performance, the more hospitalists can examine their performance and how they can improve as individuals, as a group, and as an institution.”
Additionally, the era of value-based purchasing (pay for performance) is here—in the form of CMS’ Physician Quality Reporting Initiative. For the past year, physicians have reported on specific performance measures tied to a 1.5% bonus payout. Of the program’s 74 measures in 2007 and 119 measures in 2008, 11 have reporting specifications applicable to hospitalists.
“Three to 5% of the DRG [diagnosis-related group] reimbursement could be at stake for hospitals to achieve certain benchmarks,” Dr. Torcson says. “This will be a great opportunity for hospitalists to partner with their hospitals to develop synergy in achieving performance goals that are going to help maximize hospital quality initiatives and reimbursement.”
Hospitalists can get more involved with quality measures by:
- Joining the hospital quality improvement or patient safety teams;
- Creating toolkits to educate physicians in using quality data;
- Setting up unit-sponsored interdisciplinary teams on the floors to marry all lines of care; and
- Educating the public.
“The conventional wisdom is that the more procedures that an institution does, the better their performance,” Dr. Alexander says, giving as an example a specialized cardiac hospital. “But you really want your surgery in a hospital where they manage at least a moderately high number of procedures and have a very high” success rate treating complications.
Dr. Sivaprasad believes the public wants guidance on medical care quality, legal ramifications of care, physician-specific volume, and the significance of physician hospital privileges. “Maybe we should be more public about system outcomes changes that resulted from root-cause analyses performed,” she adds.
Whatever the level, hospitalists should get involved, Dr. Vidyarthi says. “Quality improvement is an area where you as hospitalists may be asked to engage—and you’re needed.” TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
References
1. Wachter R, Shojania K. Internal Bleeding: The Truth Behind America's Terrifying Epidemic of Medical Mistakes. New York. Rugged Land. 2004.
2. Jha AK, Epstein AM. The predictive accuracy of the New York state coronary artery bypass surgery report-card system. Health Aff. 2006;25(3):844-855.
3. Sirovich BE, Gottlieb DJ, Welch HG, Fisher ES. Regional variations in healthcare intensity and physician perceptions of quality of care. Ann Intern Med 2006;144(9):641-649.
When Rajeev Alexander, MD, lead hospitalist at Oregon Medical Group with PeaceHealth of Eugene, Ore., sought out an ophthalmologist, he didn’t go to provider Web sites or directory pages. He did what most healthcare patients do: He asked around.
Some of the nurses at work gave him suggestions. “‘This guy does a lot of LASIK and might push it.’ Or, ‘This guy has good relationships with patients.’ Or, ‘This is the guy I’d send my husband to,’” Dr. Alexander explains. “That helped.”
Were he to recommend a hospital, Dr. Alexander says he would base his selection on one major criterion: the collegiality of the facility’s doctors, pharmacists, and nurses. “If all the specialists in the hospital are talking to each other, and if they feel they can trust each other,” he says, “then I think you’re going to get good care.”
Dr. Alexander never mentions checking the performance of the physician or hospital he may use. It seems he’s not alone. In recent years, some famous cases have brought attention to how infrequently patients actually consult the available quality data when selecting a provider.
It’s unlikely, for example, that Sen. Ted Kennedy (D-Mass.) researched provider collegiality as a quality measure when he chose a neurosurgeon at Duke University Medical Center to remove his malignant glioma. In 2004, when President Clinton needed his quadruple coronary bypass operation, he used an average-rated New York cardiologist. Why? Because, according to Dr. Jha, he didn’t compare quality reports.
Physicians are just as guilty of ignoring the information. Audience feedback at a hospital medicine continuing medical education course demonstrated to Robert M. Wachter, MD, chief of the division of hospital medicine and chief of the medical service at the University of California San Francisco Medical Center, that even members of UCSF’s Epidemiology and Biostatistics Department do not consult quality data before making medical decisions for themselves or a loved one. “Patients won’t start using quality data until we do it ourselves,” Dr. Wachter writes in his blog, Wachter’s World (www.wachtersworld.com). “Best guess: three to five years.”
So how much progress have we really made in using publicly reported data to pick individual providers and hospitals? What should be measured in the future as it affects hospitalist practice? How can hospitalists influence the types of data collected?
Along the Continuum
The problem isn’t because people don’t know about the data. More than one-quarter (26%) of consumers who participated in a 2002 Harris poll said they are aware of hospital report cards, Dr. Wachter writes in his book Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. However, only 3% considered changing their care based on those ratings, and only 1% actually made a change.1
Those who do consult the data seem to benefit—at least that is the case for users of New York state’s public reporting system for coronary artery bypass surgery. Dr. Jha and Arnold Epstein, MD, professor and chair of the department of Health Policy and Management at Harvard’s School of Public Health, found users who picked a top-performing hospital or surgeon had approximately half the mortality risk as did those who selected from the bottom quartile.2
But it is unusual for patients to choose a hospital based on publicly reported information alone, and Dr. Jha believes it’s largely due to mindset. “People are not used to approaching healthcare the way they would walk into a car dealership, for instance, ready to do battle,” he says.
Even if physicians and patients don’t consistently use the data, publishing it still has value. It helps physicians gauge their professional status, for example. “If someone is not looking good,” Dr. Jha says, “it is a huge impetus to improve, as long as you believe that what you are measuring is really associated with quality.”
Those who don’t believe it may have trouble, and sooner than they think. With 70 million beneficiaries, the Centers for Medicare and Medicaid Services (CMS) sets the tone for healthcare quality in the U.S. In fact, Medicare beneficiaries comprise about one-third of those in a typical hospitalist’s practice. Since March 2008, the CMS Web site www.hospitalcompare.hhs.gov/ has reported hospital service data and soon will post cost comparisons.
“CMS is a payer we have to pay attention to (them),” says Patrick Torcson, MD, chair of SHM’s Performance and Standards Committee. “The CMS performance and quality agenda is specified at the statutory level as part of the Congressional record, and is very political. Therefore, that agenda right now is part scientific, part policy, and part methodology. There is a little something in it for everybody.”
Increasingly, quality measures are gradually, and insidiously, changing healthcare. For instance, Dr. Jha’s study found outcomes data did not greatly influence hospital market share, however, the surgeons with the highest publicly reported mortality rates were much more likely to retire after the release of each report card.2
Obstacles to Utilization
If these data can help us make educated healthcare decisions, why aren’t more people consulting them? To start, current measures aren’t sufficient, says Peter K. Lindenauer, MD, MSc, FACP, a hospitalist and associate professor of medicine at Baystate Medical Center in Springfield, Mass.
“The number of measures and the strength of the evidence that current process measures are based on are still quite limited,” Dr. Lindenauer says. “Moreover, it is unclear how much the structural and process measures that have remained the focus of most public reporting contribute to patient outcomes.” It’s difficult to make statistically meaningful comparisons across hospitals or providers. Those efforts are “hampered by inadequate risk adjustment and tend to be underpowered to detect statistically significant differences.”
Another problem facing public reporting comparison initiatives is differences in healthcare utilization and spending across U.S. regions with similar levels of patient illness, says Stephanie Jackson, MD, a hospitalist with PeaceHealth and a member of SHM’s Public Policy Committee.3 The public cannot look at data it doesn’t have. For example, when Dr. Jackson asked researchers for data on coronary stroke rates, she was informed some physicians asked the data be held back because they didn’t like what it showed. “Why aren’t we demanding [that data]?” Dr. Jackson asks.
Essentially, then, quality data utilization is an evolving story. ”An ongoing debate exists between proponents of public reporting who believe that the best way to improve measures is to start using them,” Dr. Lindenauer says, “and those who advocate a more cautious approach and argue we should not rush to publicize data until we are clear about what the numbers signify and what to measure.”
Some hospitals use more than 10 criteria as the benchmark for core measures, and 10 additional dimensions hospitalists use to assess their own internal performance (see Figure 1, pg. 41). Beyond that, metrics vary from hospital to hospital.
What Hospitalists Can Do
“It is very challenging to find doctors who are well-versed in public reporting of quality data,” says Latha Sivaprasad, MD, medical director, quality management and patient safety at Beth Israel Medical Center in New York City. Dr. Jackson believes the more hospitalists know about quality data, the more they will want to use it. “Even though some hospitalists may be afraid to find out how they are doing,” she says, “in general, the better we get at measuring individual performance, the more hospitalists can examine their performance and how they can improve as individuals, as a group, and as an institution.”
Additionally, the era of value-based purchasing (pay for performance) is here—in the form of CMS’ Physician Quality Reporting Initiative. For the past year, physicians have reported on specific performance measures tied to a 1.5% bonus payout. Of the program’s 74 measures in 2007 and 119 measures in 2008, 11 have reporting specifications applicable to hospitalists.
“Three to 5% of the DRG [diagnosis-related group] reimbursement could be at stake for hospitals to achieve certain benchmarks,” Dr. Torcson says. “This will be a great opportunity for hospitalists to partner with their hospitals to develop synergy in achieving performance goals that are going to help maximize hospital quality initiatives and reimbursement.”
Hospitalists can get more involved with quality measures by:
- Joining the hospital quality improvement or patient safety teams;
- Creating toolkits to educate physicians in using quality data;
- Setting up unit-sponsored interdisciplinary teams on the floors to marry all lines of care; and
- Educating the public.
“The conventional wisdom is that the more procedures that an institution does, the better their performance,” Dr. Alexander says, giving as an example a specialized cardiac hospital. “But you really want your surgery in a hospital where they manage at least a moderately high number of procedures and have a very high” success rate treating complications.
Dr. Sivaprasad believes the public wants guidance on medical care quality, legal ramifications of care, physician-specific volume, and the significance of physician hospital privileges. “Maybe we should be more public about system outcomes changes that resulted from root-cause analyses performed,” she adds.
Whatever the level, hospitalists should get involved, Dr. Vidyarthi says. “Quality improvement is an area where you as hospitalists may be asked to engage—and you’re needed.” TH
Andrea M. Sattinger is a medical writer based in North Carolina and a frequent contributor to The Hospitalist.
References
1. Wachter R, Shojania K. Internal Bleeding: The Truth Behind America's Terrifying Epidemic of Medical Mistakes. New York. Rugged Land. 2004.
2. Jha AK, Epstein AM. The predictive accuracy of the New York state coronary artery bypass surgery report-card system. Health Aff. 2006;25(3):844-855.
3. Sirovich BE, Gottlieb DJ, Welch HG, Fisher ES. Regional variations in healthcare intensity and physician perceptions of quality of care. Ann Intern Med 2006;144(9):641-649.
One Size Does Not Fit All
When it comes to hospital medicine groups, size matters. Some physicians, like Jeffrey Hay, MD, senior vice president for medical operations and chief medical officer at Lakeside Comprehensive Healthcare in Glendale, Calif., say larger groups (i.e., those with 20 or more physicians) have the advantages of financial stability, better advancement opportunities and more support for physicians.
But Dr. Hay also sings the praises of smaller groups. A small hospital medicine group (HMG) can be a niche for those who seek particular geographic ties and a long-term commitment, he says.
Then again, a big hospital in an affluent coastal area of California, for example, has had a long-term relationship with its hospitalist group for more than 10 years. “The [hospitalists] made a decision,” Dr. Hay says. “They want to be there, they want to work and retire there. This is it; and it works for everybody.”
Which size works for you? The Hospitalist asked physicians who have experience with both large and small groups to comment about salary, shift coverage, advancement and research opportunities, and social networking. Perhaps their answers can help you decide.
Salary Expectation
Working at a smaller institution doesn’t necessarily mean receiving lower compensation, says Joe D. Metcalf II, MD, director of the five-physician HMG at Faith Regional Health Services in Norfolk, Neb. “Because recruiting hospitalists to any location is competitive, most recruiters understand they must offer a competitive salary and benefit package to their applicants.”
Salary discrepancies could, however, stem from geographic location of the group, differing workload expectations, or level of market saturation, says Brian Bossard, MD, director of Inpatient Physician Associates in Lincoln, Neb. “Salaries are increasing rapidly because of a rapid increase in the number of groups around the country,” he says.
In its annual survey of programs around the country, the Society of Hospital Medicine documents the normal salaries for different hospital medicine practices. The latest survey suggests the large-chain, independent groups have the highest average salaries. One factor affecting salary is the location: the farther away from an urban area a practice group is, sometimes the greater the salary because of added recruiting difficulties.
As a hospitalist moves from a small group to a large one, interest in the characteristics of an individual physician may be diminished. “The ability to negotiate a better salary by being a ‘good Joe’ is less important in a large group than in a small one,” Dr. Bossard says. In addition, fringe benefits of a small group might not be available in a larger group; in Dr. Bossard’s group of 20 hospitalists, an extra bonus is awarded as an end-of-the-year thanks for hard work. “That’s not part of contract, there’s no qualification for that except being a good member of the group. I doubt that would not happen in a large group,” he says.
If you are considering joining a large HMG, Dr. Hay suggests asking what role you will play in the direction of the organization and whether the possibility exists for eventual partnership or equity in the company.
Shift Coverage
Ease and availability of shift coverage varies greatly between small and large groups. In the latter, for example, physicians experience a good deal of schedule flexibility because more people can cover shifts or do the work. When Donna Beeson, DO, a hospitalist at Kadlec Medical Center in Richland, Wash., worked at the large St. Luke’s Health System in Kansas City, Mo., she had help in most aspects of practice.
“There was interventional radiology for all procedures, eICU [technology] to help with intensive care patients, a more experienced ancillary staff available for emergency situations, more partners to help out when your load gets to be too much,” Dr. Beeson says. She also had strong ancillary support at St. Luke’s, where three nurses were available to the HMG at all times.
Having so many people, however, prevented Dr. Beeson from learning her staff’s strengths and weaknesses. That’s where a smaller group has its advantages. What it lacks in physician and staff availability, it makes up for in operating as a cohesive unit, Dr. Metcalf says. “A small group of physicians is more likely to be more relationally connected and, therefore, more willing to provide help to their colleagues when special needs arise and patient-care assistance is needed,” he says.
The hospital medicine group at Riverside Tappahannock Hospital in Tappahannock, Va., exemplifies the small, cohesive group. Randy Ferrance, MD, medical director there, says having a small group made it easier to work out a three-weeks-on, one-week-off schedule (necessary because the physicians sometimes work 100-hour weeks).
In addition, though there are fewer hands in a smaller program, certain tasks, such as X-rays, reports and lab tests get accomplished with fewer hiccups. Plus, knowing the staff’s idiosyncrasies means understanding when a matter needs immediate attention or when it can be addressed later.
Dr. Beeson believes this phenomenon has made her a stronger doctor. “You know that you cannot always rely on someone else,” she says. “You realize that you have to do something or you have to make the diagnosis, because the consultant may not [do so] and you do not have a willing IR staff to help you with procedures.”
That means wearing many hats, an aspect of working in a small HMG that Dr. Ferrance says he loves. “I get to treat a lot of clinical cases that in a large hospital, a specialist might be called in to treat, whether that is necessary or not.”
One drawback to a smaller HMG is the difficulty transferring patients to bigger hospitals. It is more time consuming and challenging, Dr. Beeson says, and you lose the ability to follow through with a patient to the end of a diagnosis or disease process.
Advancement and Research Opportunities
It may seem like a no-brainer that opportunities for research and career advancement exist more within larger groups. This isn’t always the case, however, says Brian Wolfe, MD, a hospitalist with Cogent Healthcare who practices at Temple University in Philadelphia. “The ability for a group to offer protected time to do research may be more linked to the setting and schedule than whether a group is large or small.”
Of course, it doesn’t hurt to work at an institution that conducts a good deal of research, such as UMass Memorial Medical Center in Worcester Mass. Elizabeth Gundersen, MD, a hospitalist there, says she enjoys the large group’s abundant opportunities to participate in quality projects in areas of medicine that interest her. “I also enjoy having a large and diverse group of colleagues,” she adds. “I get to interact with my fellow hospitalists during the workday, whether it is to bounce ideas off them or just to socialize. There is a great amount of energy within the group.”
On the other end of the spectrum, hospitalists at smaller HMGs may have fewer hoops to jump through to get projects approved. “A smaller institution is often more amenable to the introduction of change,” says Dr. Metcalf, of Faith Regional Health Services, “which may be attractive to a hospitalist who has an interest in medical processes, quality and safety.” Dr. Ferrance adds, “We have very tight control of the hospital’s quality control because there are only four people who have to buy into a policy.”
Plus, a hospitalist at a smaller HMG quickly can establish a strong reputation, “which, in turn, provides venues for influence through involvement in committees,” Dr. Metcalf says. “An interested physician may be offered a position as a committee chairman, chief of medical staff or even as the vice president of medical affairs.”
Social Networking
In any sized group, social networking is key. Before joining the group at Temple, Dr. Wolfe thought physicians in a smaller group would automatically be closer than those in a large one. “I was surprised that we are so inter-relationally dependent and responsible to each other,” Dr. Wolfe says, “but that’s because there are so many inter-service hand-offs and trade-offs, and we see each other so much.”
Scheduling social events for 20-plus doctors and their families can be a challenge. Some, like Dr. Bossard, say it’s a priority, though it could mean orchestrating events for 75 people. “When that social connection is lost in a group,” Dr. Bossard says, “it may reflect burnout on the leader’s part.”
What is most important for any group, no matter its location or size, is having a forward-thinking leadership with operational expertise and a strong infrastructure. “If they don’t have that,” Dr. Hay says, “they may get displaced by big organizations, leaving the hospitalists locked out and scrambling for jobs.” TH
When it comes to hospital medicine groups, size matters. Some physicians, like Jeffrey Hay, MD, senior vice president for medical operations and chief medical officer at Lakeside Comprehensive Healthcare in Glendale, Calif., say larger groups (i.e., those with 20 or more physicians) have the advantages of financial stability, better advancement opportunities and more support for physicians.
But Dr. Hay also sings the praises of smaller groups. A small hospital medicine group (HMG) can be a niche for those who seek particular geographic ties and a long-term commitment, he says.
Then again, a big hospital in an affluent coastal area of California, for example, has had a long-term relationship with its hospitalist group for more than 10 years. “The [hospitalists] made a decision,” Dr. Hay says. “They want to be there, they want to work and retire there. This is it; and it works for everybody.”
Which size works for you? The Hospitalist asked physicians who have experience with both large and small groups to comment about salary, shift coverage, advancement and research opportunities, and social networking. Perhaps their answers can help you decide.
Salary Expectation
Working at a smaller institution doesn’t necessarily mean receiving lower compensation, says Joe D. Metcalf II, MD, director of the five-physician HMG at Faith Regional Health Services in Norfolk, Neb. “Because recruiting hospitalists to any location is competitive, most recruiters understand they must offer a competitive salary and benefit package to their applicants.”
Salary discrepancies could, however, stem from geographic location of the group, differing workload expectations, or level of market saturation, says Brian Bossard, MD, director of Inpatient Physician Associates in Lincoln, Neb. “Salaries are increasing rapidly because of a rapid increase in the number of groups around the country,” he says.
In its annual survey of programs around the country, the Society of Hospital Medicine documents the normal salaries for different hospital medicine practices. The latest survey suggests the large-chain, independent groups have the highest average salaries. One factor affecting salary is the location: the farther away from an urban area a practice group is, sometimes the greater the salary because of added recruiting difficulties.
As a hospitalist moves from a small group to a large one, interest in the characteristics of an individual physician may be diminished. “The ability to negotiate a better salary by being a ‘good Joe’ is less important in a large group than in a small one,” Dr. Bossard says. In addition, fringe benefits of a small group might not be available in a larger group; in Dr. Bossard’s group of 20 hospitalists, an extra bonus is awarded as an end-of-the-year thanks for hard work. “That’s not part of contract, there’s no qualification for that except being a good member of the group. I doubt that would not happen in a large group,” he says.
If you are considering joining a large HMG, Dr. Hay suggests asking what role you will play in the direction of the organization and whether the possibility exists for eventual partnership or equity in the company.
Shift Coverage
Ease and availability of shift coverage varies greatly between small and large groups. In the latter, for example, physicians experience a good deal of schedule flexibility because more people can cover shifts or do the work. When Donna Beeson, DO, a hospitalist at Kadlec Medical Center in Richland, Wash., worked at the large St. Luke’s Health System in Kansas City, Mo., she had help in most aspects of practice.
“There was interventional radiology for all procedures, eICU [technology] to help with intensive care patients, a more experienced ancillary staff available for emergency situations, more partners to help out when your load gets to be too much,” Dr. Beeson says. She also had strong ancillary support at St. Luke’s, where three nurses were available to the HMG at all times.
Having so many people, however, prevented Dr. Beeson from learning her staff’s strengths and weaknesses. That’s where a smaller group has its advantages. What it lacks in physician and staff availability, it makes up for in operating as a cohesive unit, Dr. Metcalf says. “A small group of physicians is more likely to be more relationally connected and, therefore, more willing to provide help to their colleagues when special needs arise and patient-care assistance is needed,” he says.
The hospital medicine group at Riverside Tappahannock Hospital in Tappahannock, Va., exemplifies the small, cohesive group. Randy Ferrance, MD, medical director there, says having a small group made it easier to work out a three-weeks-on, one-week-off schedule (necessary because the physicians sometimes work 100-hour weeks).
In addition, though there are fewer hands in a smaller program, certain tasks, such as X-rays, reports and lab tests get accomplished with fewer hiccups. Plus, knowing the staff’s idiosyncrasies means understanding when a matter needs immediate attention or when it can be addressed later.
Dr. Beeson believes this phenomenon has made her a stronger doctor. “You know that you cannot always rely on someone else,” she says. “You realize that you have to do something or you have to make the diagnosis, because the consultant may not [do so] and you do not have a willing IR staff to help you with procedures.”
That means wearing many hats, an aspect of working in a small HMG that Dr. Ferrance says he loves. “I get to treat a lot of clinical cases that in a large hospital, a specialist might be called in to treat, whether that is necessary or not.”
One drawback to a smaller HMG is the difficulty transferring patients to bigger hospitals. It is more time consuming and challenging, Dr. Beeson says, and you lose the ability to follow through with a patient to the end of a diagnosis or disease process.
Advancement and Research Opportunities
It may seem like a no-brainer that opportunities for research and career advancement exist more within larger groups. This isn’t always the case, however, says Brian Wolfe, MD, a hospitalist with Cogent Healthcare who practices at Temple University in Philadelphia. “The ability for a group to offer protected time to do research may be more linked to the setting and schedule than whether a group is large or small.”
Of course, it doesn’t hurt to work at an institution that conducts a good deal of research, such as UMass Memorial Medical Center in Worcester Mass. Elizabeth Gundersen, MD, a hospitalist there, says she enjoys the large group’s abundant opportunities to participate in quality projects in areas of medicine that interest her. “I also enjoy having a large and diverse group of colleagues,” she adds. “I get to interact with my fellow hospitalists during the workday, whether it is to bounce ideas off them or just to socialize. There is a great amount of energy within the group.”
On the other end of the spectrum, hospitalists at smaller HMGs may have fewer hoops to jump through to get projects approved. “A smaller institution is often more amenable to the introduction of change,” says Dr. Metcalf, of Faith Regional Health Services, “which may be attractive to a hospitalist who has an interest in medical processes, quality and safety.” Dr. Ferrance adds, “We have very tight control of the hospital’s quality control because there are only four people who have to buy into a policy.”
Plus, a hospitalist at a smaller HMG quickly can establish a strong reputation, “which, in turn, provides venues for influence through involvement in committees,” Dr. Metcalf says. “An interested physician may be offered a position as a committee chairman, chief of medical staff or even as the vice president of medical affairs.”
Social Networking
In any sized group, social networking is key. Before joining the group at Temple, Dr. Wolfe thought physicians in a smaller group would automatically be closer than those in a large one. “I was surprised that we are so inter-relationally dependent and responsible to each other,” Dr. Wolfe says, “but that’s because there are so many inter-service hand-offs and trade-offs, and we see each other so much.”
Scheduling social events for 20-plus doctors and their families can be a challenge. Some, like Dr. Bossard, say it’s a priority, though it could mean orchestrating events for 75 people. “When that social connection is lost in a group,” Dr. Bossard says, “it may reflect burnout on the leader’s part.”
What is most important for any group, no matter its location or size, is having a forward-thinking leadership with operational expertise and a strong infrastructure. “If they don’t have that,” Dr. Hay says, “they may get displaced by big organizations, leaving the hospitalists locked out and scrambling for jobs.” TH
When it comes to hospital medicine groups, size matters. Some physicians, like Jeffrey Hay, MD, senior vice president for medical operations and chief medical officer at Lakeside Comprehensive Healthcare in Glendale, Calif., say larger groups (i.e., those with 20 or more physicians) have the advantages of financial stability, better advancement opportunities and more support for physicians.
But Dr. Hay also sings the praises of smaller groups. A small hospital medicine group (HMG) can be a niche for those who seek particular geographic ties and a long-term commitment, he says.
Then again, a big hospital in an affluent coastal area of California, for example, has had a long-term relationship with its hospitalist group for more than 10 years. “The [hospitalists] made a decision,” Dr. Hay says. “They want to be there, they want to work and retire there. This is it; and it works for everybody.”
Which size works for you? The Hospitalist asked physicians who have experience with both large and small groups to comment about salary, shift coverage, advancement and research opportunities, and social networking. Perhaps their answers can help you decide.
Salary Expectation
Working at a smaller institution doesn’t necessarily mean receiving lower compensation, says Joe D. Metcalf II, MD, director of the five-physician HMG at Faith Regional Health Services in Norfolk, Neb. “Because recruiting hospitalists to any location is competitive, most recruiters understand they must offer a competitive salary and benefit package to their applicants.”
Salary discrepancies could, however, stem from geographic location of the group, differing workload expectations, or level of market saturation, says Brian Bossard, MD, director of Inpatient Physician Associates in Lincoln, Neb. “Salaries are increasing rapidly because of a rapid increase in the number of groups around the country,” he says.
In its annual survey of programs around the country, the Society of Hospital Medicine documents the normal salaries for different hospital medicine practices. The latest survey suggests the large-chain, independent groups have the highest average salaries. One factor affecting salary is the location: the farther away from an urban area a practice group is, sometimes the greater the salary because of added recruiting difficulties.
As a hospitalist moves from a small group to a large one, interest in the characteristics of an individual physician may be diminished. “The ability to negotiate a better salary by being a ‘good Joe’ is less important in a large group than in a small one,” Dr. Bossard says. In addition, fringe benefits of a small group might not be available in a larger group; in Dr. Bossard’s group of 20 hospitalists, an extra bonus is awarded as an end-of-the-year thanks for hard work. “That’s not part of contract, there’s no qualification for that except being a good member of the group. I doubt that would not happen in a large group,” he says.
If you are considering joining a large HMG, Dr. Hay suggests asking what role you will play in the direction of the organization and whether the possibility exists for eventual partnership or equity in the company.
Shift Coverage
Ease and availability of shift coverage varies greatly between small and large groups. In the latter, for example, physicians experience a good deal of schedule flexibility because more people can cover shifts or do the work. When Donna Beeson, DO, a hospitalist at Kadlec Medical Center in Richland, Wash., worked at the large St. Luke’s Health System in Kansas City, Mo., she had help in most aspects of practice.
“There was interventional radiology for all procedures, eICU [technology] to help with intensive care patients, a more experienced ancillary staff available for emergency situations, more partners to help out when your load gets to be too much,” Dr. Beeson says. She also had strong ancillary support at St. Luke’s, where three nurses were available to the HMG at all times.
Having so many people, however, prevented Dr. Beeson from learning her staff’s strengths and weaknesses. That’s where a smaller group has its advantages. What it lacks in physician and staff availability, it makes up for in operating as a cohesive unit, Dr. Metcalf says. “A small group of physicians is more likely to be more relationally connected and, therefore, more willing to provide help to their colleagues when special needs arise and patient-care assistance is needed,” he says.
The hospital medicine group at Riverside Tappahannock Hospital in Tappahannock, Va., exemplifies the small, cohesive group. Randy Ferrance, MD, medical director there, says having a small group made it easier to work out a three-weeks-on, one-week-off schedule (necessary because the physicians sometimes work 100-hour weeks).
In addition, though there are fewer hands in a smaller program, certain tasks, such as X-rays, reports and lab tests get accomplished with fewer hiccups. Plus, knowing the staff’s idiosyncrasies means understanding when a matter needs immediate attention or when it can be addressed later.
Dr. Beeson believes this phenomenon has made her a stronger doctor. “You know that you cannot always rely on someone else,” she says. “You realize that you have to do something or you have to make the diagnosis, because the consultant may not [do so] and you do not have a willing IR staff to help you with procedures.”
That means wearing many hats, an aspect of working in a small HMG that Dr. Ferrance says he loves. “I get to treat a lot of clinical cases that in a large hospital, a specialist might be called in to treat, whether that is necessary or not.”
One drawback to a smaller HMG is the difficulty transferring patients to bigger hospitals. It is more time consuming and challenging, Dr. Beeson says, and you lose the ability to follow through with a patient to the end of a diagnosis or disease process.
Advancement and Research Opportunities
It may seem like a no-brainer that opportunities for research and career advancement exist more within larger groups. This isn’t always the case, however, says Brian Wolfe, MD, a hospitalist with Cogent Healthcare who practices at Temple University in Philadelphia. “The ability for a group to offer protected time to do research may be more linked to the setting and schedule than whether a group is large or small.”
Of course, it doesn’t hurt to work at an institution that conducts a good deal of research, such as UMass Memorial Medical Center in Worcester Mass. Elizabeth Gundersen, MD, a hospitalist there, says she enjoys the large group’s abundant opportunities to participate in quality projects in areas of medicine that interest her. “I also enjoy having a large and diverse group of colleagues,” she adds. “I get to interact with my fellow hospitalists during the workday, whether it is to bounce ideas off them or just to socialize. There is a great amount of energy within the group.”
On the other end of the spectrum, hospitalists at smaller HMGs may have fewer hoops to jump through to get projects approved. “A smaller institution is often more amenable to the introduction of change,” says Dr. Metcalf, of Faith Regional Health Services, “which may be attractive to a hospitalist who has an interest in medical processes, quality and safety.” Dr. Ferrance adds, “We have very tight control of the hospital’s quality control because there are only four people who have to buy into a policy.”
Plus, a hospitalist at a smaller HMG quickly can establish a strong reputation, “which, in turn, provides venues for influence through involvement in committees,” Dr. Metcalf says. “An interested physician may be offered a position as a committee chairman, chief of medical staff or even as the vice president of medical affairs.”
Social Networking
In any sized group, social networking is key. Before joining the group at Temple, Dr. Wolfe thought physicians in a smaller group would automatically be closer than those in a large one. “I was surprised that we are so inter-relationally dependent and responsible to each other,” Dr. Wolfe says, “but that’s because there are so many inter-service hand-offs and trade-offs, and we see each other so much.”
Scheduling social events for 20-plus doctors and their families can be a challenge. Some, like Dr. Bossard, say it’s a priority, though it could mean orchestrating events for 75 people. “When that social connection is lost in a group,” Dr. Bossard says, “it may reflect burnout on the leader’s part.”
What is most important for any group, no matter its location or size, is having a forward-thinking leadership with operational expertise and a strong infrastructure. “If they don’t have that,” Dr. Hay says, “they may get displaced by big organizations, leaving the hospitalists locked out and scrambling for jobs.” TH
Patients’ Circumstances Count in Care Planning
Hospitals, insurers, and regulators today direct unparalleled time and resources toward battling medical errors. According to research from Saul Weiner, MD, a teacher and hospitalist at the University of Illinois, Chicago, one type of error is being ignored.
“I found that contextual errors are as least as common and probably even more serious in inpatient care,” Dr. Weiner says. Contextual errors occur when physicians neglect to recognize the crucial role a patient’s life plays in care planning, he says. “I would argue that there are contextual issues in virtually every admission,” he adds.
Dr. Weiner and his team are trying to prove the importance of systematizing how physicians learn to contextualize care. For their research, published in the September 2007 issue of Medical Decision Making, the doctors trained actors to present scenarios in which contextual information was essential to planning appropriate care. They then tested 54 internal medicine residents to see how many would provide contextually appropriate care. More than half made serious errors.1
Why Now?
From the time Dr. Weiner started precepting residents in 1997, he noticed many were quick to fit patients into categories where they could apply evidence-based approaches to care. “But I sometimes sensed that there was something not so straightforward about a particular patient’s situation, some unexplained issue for why the patient wasn’t taking his asthma meds properly, or was coming in today of all days,” he says. When he and the residents would re-question such patients, “key factors often arose that made everything change about the way we wanted to manage them.”
For him, the seminal case occurred in 2002 when a patient who came to the preoperative testing clinic for bariatric surgery. She qualified for surgery, although because of history of adhesions, the surgery was going to be open rather than laparoscopic. When she said she was looking forward to getting the surgery so she could better care for her son, a red flag went up for Dr. Weiner.
“Patients don’t typically offer such reflections,” he says. Further probing revealed that she had a son in his 20s with a fatal disease, she was the sole caregiver, and her husband was an alcoholic. “She really hadn’t processed the fact that she would not be able to do anything for 40 days,” Dr. Weiner says. “Suddenly, when she got that, she wound up canceling surgery.”
The importance of learning a patietn’s contextual factors depends on the setting and the availability of resources, such as case managers, social workers, and outpatient chronic disease teams. Even with those resources, the onus still is on the hospitalist to determine an effective plan of care using context, he says.
How Well Do Hospitalists Spot Red Flags?
Tuning up the radar to prevent these errors comes down to providers asking one question and listening to one answer: What is the best thing I can do for this patient at this time? Watch for red flags, statements patients make or actions they take that may signal something lying beneath the surface that could make a huge difference in outcomes, Dr. Weiner says.
Spotting red flags isn’t always easy for hospitalists, who don’t see the same patients on a regular basis, says William Stinnette, MD, hospitalist with Kaiser Permanente in San Rafael, Calif. “Unless patients are a part of that ‘revolving door,’ with frequent visits to the hospital, we have to work up most of our patients with limited background knowledge,” he says.
Dr. Stinnette, who has worked in hospital medicine groups in both small and large facilities, believes the ability to ferret out contextual factors depends on the setting and teh availability of resources, such as case managers, social workers, and outpatient chornic disease teams. Even with those resources, the onus is still on the hospitalist to determine an effective plan of care using context, he says.
Dr. Weiner agrees. “Clinical decision-making,” he writes in the Medical Decision Making article, “requires two distinct skills: the ability to classify patients’ conditions into diagnostic and management categories that permit the application of research evidence, and the ability to individualize (contextualize) care for patients whose circumstances and needs require variation from a standardized approach.”1
Though most hospitalists recognize the importance of doing this, according to Dr. Weiner, they lack a systematic and coherent way to do so.2
Standardized Training
Physicians are well trained in assessing biomedical information, but not in listening for contextual red flags. “When you need to know what’s unique about a particular patient that might be relevant to the case, you don’t really know what you’re searching for,” Dr. Weiner says. “You just need clarity, and that is theory-building or inductive reasoning, a very different skill.”
Since July, with support from the National Board of Medical Examiners, the University of Illinois, Chicago, team has been testing a contextual-care curriculum for fourth-year medical students to complete during their inpatient medical sub-internships. In the randomized controlled trial, half of the trainees receive the intervention, half do not. Those getting trained learn that when they intuitively feel there is more to a patient’s story, they should return to the patient to find out why.
They also learn to conduct a contextual history by asking simple, straightforward questions, keeping in mind potential areas of context, including the patient’s emotional state and cultural beliefs (see sidebar, “Cases of Context”). Through this process, the residents learn to identify ways to avoid contextual errors in their patients’ care.
At the end of the month-long curriculum, all trainees are tested in the patient laboratory. “The simulated patients are trained to present with complex histories,” Dr. Weiner says. If residents don’t probe properly, the patients don’t reveal the context. Both groups—those who’ve had the intervention and those who have not—interview the patients, and the study is tracking which physicians get the cases ‘correct.’ ”
The Cost of Errors
For a next phase of research, the university has enrolled about 100 physicians from multiple centers in the Chicago/Milwaukee area to participate in visits by undercover actors simulating real patients. The cases require uncovering contextual information to avoid making errors when planning their care.
After each visit, the team downloads and scores the physician’s note, identifying both unnecessary tests and missed opportunities. Using Medicare reimbursement data, the team assigns a dollar amount to these errors that would have occurred had the patients been real. Dr. Weiner predicts publicizing the financial costs will bring more attention to the problem.
Access to Care Issues
Actually, physicians should talk to their patients about the cost of their care, says David O. Meltzer, MD, PhD, associate professor and chief of the Section of Hospital Medicine at the University of Chicago Medical Center. In research published in the Journal of the American Medical Association in 2003, Dr. Meltzer and colleagues found patient costs may be associated with medication nonadherence and considerable economic burden.3
“You have to ask a patient the type of questions that will be most revealing, including the broader questions, such as ‘Are there any challenges in your life to getting the care that we’ve discussed after you leave the hospital?’ ” Dr. Stinnette, of Kaiser, says.
In their study, Dr. Meltzer and colleagues also showed that although physicians and patients agree it is important to talk about money issues, it doesn’t commonly happen.3
“In a public hospital where there are greater numbers of uninsured patients, I expect it is much more a frequent topic of conversation,” Dr. Meltzer says. “My suspicion is that the people at greatest risk are uninsured patients who are hospitalized in settings where most patients are insured, and physicians are not attuned to bringing up this issue.”
Although a great deal of literature now deals with physician-patient communication, the techniques seem too scripted to Dr. Weiner. “When you engage with the patient simply as one person who is concerned about another,” he says, “you much more naturally find out what you could do that might help them.”
References
- Weiner SJ, Schwartz A, Yudkowsky R, et al. Evaluating physician performance at individualizing care: A pilot study tracking contextual errors in medical decision-making. Med Decis Making 2007;27(6):726-34.
- Weiner SJ. Contextualizing medical decisions to individualize care: Lessons from the qualitative sciences. J Gen Intern Med 2004;19(3):281-5.
- Alexander GC, Casalino LP, Meltzer DO. Patient-physician communication about out-of-pocket costs. JAMA 2003;290(7):953-958.
Hospitals, insurers, and regulators today direct unparalleled time and resources toward battling medical errors. According to research from Saul Weiner, MD, a teacher and hospitalist at the University of Illinois, Chicago, one type of error is being ignored.
“I found that contextual errors are as least as common and probably even more serious in inpatient care,” Dr. Weiner says. Contextual errors occur when physicians neglect to recognize the crucial role a patient’s life plays in care planning, he says. “I would argue that there are contextual issues in virtually every admission,” he adds.
Dr. Weiner and his team are trying to prove the importance of systematizing how physicians learn to contextualize care. For their research, published in the September 2007 issue of Medical Decision Making, the doctors trained actors to present scenarios in which contextual information was essential to planning appropriate care. They then tested 54 internal medicine residents to see how many would provide contextually appropriate care. More than half made serious errors.1
Why Now?
From the time Dr. Weiner started precepting residents in 1997, he noticed many were quick to fit patients into categories where they could apply evidence-based approaches to care. “But I sometimes sensed that there was something not so straightforward about a particular patient’s situation, some unexplained issue for why the patient wasn’t taking his asthma meds properly, or was coming in today of all days,” he says. When he and the residents would re-question such patients, “key factors often arose that made everything change about the way we wanted to manage them.”
For him, the seminal case occurred in 2002 when a patient who came to the preoperative testing clinic for bariatric surgery. She qualified for surgery, although because of history of adhesions, the surgery was going to be open rather than laparoscopic. When she said she was looking forward to getting the surgery so she could better care for her son, a red flag went up for Dr. Weiner.
“Patients don’t typically offer such reflections,” he says. Further probing revealed that she had a son in his 20s with a fatal disease, she was the sole caregiver, and her husband was an alcoholic. “She really hadn’t processed the fact that she would not be able to do anything for 40 days,” Dr. Weiner says. “Suddenly, when she got that, she wound up canceling surgery.”
The importance of learning a patietn’s contextual factors depends on the setting and the availability of resources, such as case managers, social workers, and outpatient chronic disease teams. Even with those resources, the onus still is on the hospitalist to determine an effective plan of care using context, he says.
How Well Do Hospitalists Spot Red Flags?
Tuning up the radar to prevent these errors comes down to providers asking one question and listening to one answer: What is the best thing I can do for this patient at this time? Watch for red flags, statements patients make or actions they take that may signal something lying beneath the surface that could make a huge difference in outcomes, Dr. Weiner says.
Spotting red flags isn’t always easy for hospitalists, who don’t see the same patients on a regular basis, says William Stinnette, MD, hospitalist with Kaiser Permanente in San Rafael, Calif. “Unless patients are a part of that ‘revolving door,’ with frequent visits to the hospital, we have to work up most of our patients with limited background knowledge,” he says.
Dr. Stinnette, who has worked in hospital medicine groups in both small and large facilities, believes the ability to ferret out contextual factors depends on the setting and teh availability of resources, such as case managers, social workers, and outpatient chornic disease teams. Even with those resources, the onus is still on the hospitalist to determine an effective plan of care using context, he says.
Dr. Weiner agrees. “Clinical decision-making,” he writes in the Medical Decision Making article, “requires two distinct skills: the ability to classify patients’ conditions into diagnostic and management categories that permit the application of research evidence, and the ability to individualize (contextualize) care for patients whose circumstances and needs require variation from a standardized approach.”1
Though most hospitalists recognize the importance of doing this, according to Dr. Weiner, they lack a systematic and coherent way to do so.2
Standardized Training
Physicians are well trained in assessing biomedical information, but not in listening for contextual red flags. “When you need to know what’s unique about a particular patient that might be relevant to the case, you don’t really know what you’re searching for,” Dr. Weiner says. “You just need clarity, and that is theory-building or inductive reasoning, a very different skill.”
Since July, with support from the National Board of Medical Examiners, the University of Illinois, Chicago, team has been testing a contextual-care curriculum for fourth-year medical students to complete during their inpatient medical sub-internships. In the randomized controlled trial, half of the trainees receive the intervention, half do not. Those getting trained learn that when they intuitively feel there is more to a patient’s story, they should return to the patient to find out why.
They also learn to conduct a contextual history by asking simple, straightforward questions, keeping in mind potential areas of context, including the patient’s emotional state and cultural beliefs (see sidebar, “Cases of Context”). Through this process, the residents learn to identify ways to avoid contextual errors in their patients’ care.
At the end of the month-long curriculum, all trainees are tested in the patient laboratory. “The simulated patients are trained to present with complex histories,” Dr. Weiner says. If residents don’t probe properly, the patients don’t reveal the context. Both groups—those who’ve had the intervention and those who have not—interview the patients, and the study is tracking which physicians get the cases ‘correct.’ ”
The Cost of Errors
For a next phase of research, the university has enrolled about 100 physicians from multiple centers in the Chicago/Milwaukee area to participate in visits by undercover actors simulating real patients. The cases require uncovering contextual information to avoid making errors when planning their care.
After each visit, the team downloads and scores the physician’s note, identifying both unnecessary tests and missed opportunities. Using Medicare reimbursement data, the team assigns a dollar amount to these errors that would have occurred had the patients been real. Dr. Weiner predicts publicizing the financial costs will bring more attention to the problem.
Access to Care Issues
Actually, physicians should talk to their patients about the cost of their care, says David O. Meltzer, MD, PhD, associate professor and chief of the Section of Hospital Medicine at the University of Chicago Medical Center. In research published in the Journal of the American Medical Association in 2003, Dr. Meltzer and colleagues found patient costs may be associated with medication nonadherence and considerable economic burden.3
“You have to ask a patient the type of questions that will be most revealing, including the broader questions, such as ‘Are there any challenges in your life to getting the care that we’ve discussed after you leave the hospital?’ ” Dr. Stinnette, of Kaiser, says.
In their study, Dr. Meltzer and colleagues also showed that although physicians and patients agree it is important to talk about money issues, it doesn’t commonly happen.3
“In a public hospital where there are greater numbers of uninsured patients, I expect it is much more a frequent topic of conversation,” Dr. Meltzer says. “My suspicion is that the people at greatest risk are uninsured patients who are hospitalized in settings where most patients are insured, and physicians are not attuned to bringing up this issue.”
Although a great deal of literature now deals with physician-patient communication, the techniques seem too scripted to Dr. Weiner. “When you engage with the patient simply as one person who is concerned about another,” he says, “you much more naturally find out what you could do that might help them.”
References
- Weiner SJ, Schwartz A, Yudkowsky R, et al. Evaluating physician performance at individualizing care: A pilot study tracking contextual errors in medical decision-making. Med Decis Making 2007;27(6):726-34.
- Weiner SJ. Contextualizing medical decisions to individualize care: Lessons from the qualitative sciences. J Gen Intern Med 2004;19(3):281-5.
- Alexander GC, Casalino LP, Meltzer DO. Patient-physician communication about out-of-pocket costs. JAMA 2003;290(7):953-958.
Hospitals, insurers, and regulators today direct unparalleled time and resources toward battling medical errors. According to research from Saul Weiner, MD, a teacher and hospitalist at the University of Illinois, Chicago, one type of error is being ignored.
“I found that contextual errors are as least as common and probably even more serious in inpatient care,” Dr. Weiner says. Contextual errors occur when physicians neglect to recognize the crucial role a patient’s life plays in care planning, he says. “I would argue that there are contextual issues in virtually every admission,” he adds.
Dr. Weiner and his team are trying to prove the importance of systematizing how physicians learn to contextualize care. For their research, published in the September 2007 issue of Medical Decision Making, the doctors trained actors to present scenarios in which contextual information was essential to planning appropriate care. They then tested 54 internal medicine residents to see how many would provide contextually appropriate care. More than half made serious errors.1
Why Now?
From the time Dr. Weiner started precepting residents in 1997, he noticed many were quick to fit patients into categories where they could apply evidence-based approaches to care. “But I sometimes sensed that there was something not so straightforward about a particular patient’s situation, some unexplained issue for why the patient wasn’t taking his asthma meds properly, or was coming in today of all days,” he says. When he and the residents would re-question such patients, “key factors often arose that made everything change about the way we wanted to manage them.”
For him, the seminal case occurred in 2002 when a patient who came to the preoperative testing clinic for bariatric surgery. She qualified for surgery, although because of history of adhesions, the surgery was going to be open rather than laparoscopic. When she said she was looking forward to getting the surgery so she could better care for her son, a red flag went up for Dr. Weiner.
“Patients don’t typically offer such reflections,” he says. Further probing revealed that she had a son in his 20s with a fatal disease, she was the sole caregiver, and her husband was an alcoholic. “She really hadn’t processed the fact that she would not be able to do anything for 40 days,” Dr. Weiner says. “Suddenly, when she got that, she wound up canceling surgery.”
The importance of learning a patietn’s contextual factors depends on the setting and the availability of resources, such as case managers, social workers, and outpatient chronic disease teams. Even with those resources, the onus still is on the hospitalist to determine an effective plan of care using context, he says.
How Well Do Hospitalists Spot Red Flags?
Tuning up the radar to prevent these errors comes down to providers asking one question and listening to one answer: What is the best thing I can do for this patient at this time? Watch for red flags, statements patients make or actions they take that may signal something lying beneath the surface that could make a huge difference in outcomes, Dr. Weiner says.
Spotting red flags isn’t always easy for hospitalists, who don’t see the same patients on a regular basis, says William Stinnette, MD, hospitalist with Kaiser Permanente in San Rafael, Calif. “Unless patients are a part of that ‘revolving door,’ with frequent visits to the hospital, we have to work up most of our patients with limited background knowledge,” he says.
Dr. Stinnette, who has worked in hospital medicine groups in both small and large facilities, believes the ability to ferret out contextual factors depends on the setting and teh availability of resources, such as case managers, social workers, and outpatient chornic disease teams. Even with those resources, the onus is still on the hospitalist to determine an effective plan of care using context, he says.
Dr. Weiner agrees. “Clinical decision-making,” he writes in the Medical Decision Making article, “requires two distinct skills: the ability to classify patients’ conditions into diagnostic and management categories that permit the application of research evidence, and the ability to individualize (contextualize) care for patients whose circumstances and needs require variation from a standardized approach.”1
Though most hospitalists recognize the importance of doing this, according to Dr. Weiner, they lack a systematic and coherent way to do so.2
Standardized Training
Physicians are well trained in assessing biomedical information, but not in listening for contextual red flags. “When you need to know what’s unique about a particular patient that might be relevant to the case, you don’t really know what you’re searching for,” Dr. Weiner says. “You just need clarity, and that is theory-building or inductive reasoning, a very different skill.”
Since July, with support from the National Board of Medical Examiners, the University of Illinois, Chicago, team has been testing a contextual-care curriculum for fourth-year medical students to complete during their inpatient medical sub-internships. In the randomized controlled trial, half of the trainees receive the intervention, half do not. Those getting trained learn that when they intuitively feel there is more to a patient’s story, they should return to the patient to find out why.
They also learn to conduct a contextual history by asking simple, straightforward questions, keeping in mind potential areas of context, including the patient’s emotional state and cultural beliefs (see sidebar, “Cases of Context”). Through this process, the residents learn to identify ways to avoid contextual errors in their patients’ care.
At the end of the month-long curriculum, all trainees are tested in the patient laboratory. “The simulated patients are trained to present with complex histories,” Dr. Weiner says. If residents don’t probe properly, the patients don’t reveal the context. Both groups—those who’ve had the intervention and those who have not—interview the patients, and the study is tracking which physicians get the cases ‘correct.’ ”
The Cost of Errors
For a next phase of research, the university has enrolled about 100 physicians from multiple centers in the Chicago/Milwaukee area to participate in visits by undercover actors simulating real patients. The cases require uncovering contextual information to avoid making errors when planning their care.
After each visit, the team downloads and scores the physician’s note, identifying both unnecessary tests and missed opportunities. Using Medicare reimbursement data, the team assigns a dollar amount to these errors that would have occurred had the patients been real. Dr. Weiner predicts publicizing the financial costs will bring more attention to the problem.
Access to Care Issues
Actually, physicians should talk to their patients about the cost of their care, says David O. Meltzer, MD, PhD, associate professor and chief of the Section of Hospital Medicine at the University of Chicago Medical Center. In research published in the Journal of the American Medical Association in 2003, Dr. Meltzer and colleagues found patient costs may be associated with medication nonadherence and considerable economic burden.3
“You have to ask a patient the type of questions that will be most revealing, including the broader questions, such as ‘Are there any challenges in your life to getting the care that we’ve discussed after you leave the hospital?’ ” Dr. Stinnette, of Kaiser, says.
In their study, Dr. Meltzer and colleagues also showed that although physicians and patients agree it is important to talk about money issues, it doesn’t commonly happen.3
“In a public hospital where there are greater numbers of uninsured patients, I expect it is much more a frequent topic of conversation,” Dr. Meltzer says. “My suspicion is that the people at greatest risk are uninsured patients who are hospitalized in settings where most patients are insured, and physicians are not attuned to bringing up this issue.”
Although a great deal of literature now deals with physician-patient communication, the techniques seem too scripted to Dr. Weiner. “When you engage with the patient simply as one person who is concerned about another,” he says, “you much more naturally find out what you could do that might help them.”
References
- Weiner SJ, Schwartz A, Yudkowsky R, et al. Evaluating physician performance at individualizing care: A pilot study tracking contextual errors in medical decision-making. Med Decis Making 2007;27(6):726-34.
- Weiner SJ. Contextualizing medical decisions to individualize care: Lessons from the qualitative sciences. J Gen Intern Med 2004;19(3):281-5.
- Alexander GC, Casalino LP, Meltzer DO. Patient-physician communication about out-of-pocket costs. JAMA 2003;290(7):953-958.